BA vs COPD
68
Bronchial Asthma (BA) Bronchial Asthma (BA) vs vs Chronic Obstructive Chronic Obstructive Pulmonary Disease (COPD) Pulmonary Disease (COPD) Dr Chua Keong Tiong Dr Chua Keong Tiong Division of Respiratory Division of Respiratory Medicine Medicine Department of Medicine Department of Medicine
-
Upload
ooi-say-ting -
Category
Documents
-
view
12 -
download
0
description
presentation
Transcript of BA vs COPD
-
Bronchial Asthma (BA) vs Chronic Obstructive Pulmonary Disease (COPD)Dr Chua Keong TiongDivision of Respiratory MedicineDepartment of Medicine
-
Case 124, , feels SOB at night. She gets the symptoms half of the time. The other half of the time, she is very well without limitation to her exercise.
Bronchial AsthmaCOPDCombination of A+BI dont know, thats why I am here
-
Case 260, , feels SOB on exertion. She gets the symptoms all the time. Her SOB is persistent and gradually worsened over a 2-year period. She is a chronic heavy smoker.
Bronchial AsthmaCOPDCombination of A+BI dont know, thats why I am here
-
Case 350, , feels SOB at night. She gets the nocturnal symptoms half of the time. She also has reduced in effort tolerance in the past 2 years. She noticed there was a steady trend towards worsening. She is a chronic heavy smoker.
Bronchial AsthmaCOPDCombination of A+BI dont know, thats why I am here
-
Case 450, , feels SOB on exertion. She has a history of poorly control asthma for 30 years. She usually gets her nocturnal symptoms, but over the past 2 years, she noticed that she was getting the similar symptoms during the daytime especially on exertion. The SOB was persistent and progressive, and it did not seem to respond to her bronchodilator. She is a life-long non smoker.
Bronchial AsthmaCOPDCombination of A+BI dont know, thats why I am here
-
OverviewBronchial AsthmaDefinitionPathophysiologyPathogenesisEpidemiologySymptomologyPhysical SignsInvestigationsTreatment plan
Comparison of BA vs COPDCOPDDefinitionPathophysiologyPathogenesisEpidemiologySymptomologyPhysical SignsInvestigationsTreamtent plan
-
Bronchial AsthmaChronic inflammatory disorder of the airways in which many cells and cellular elements play a role. The chronic inflammation is associated with airway hyperresponsiveness that leads to recurrent episodes of wheezing, breathlessness, chest tightness, and coughing, particularly at night or in the early morning. These episodes are usually associated with widespread, but variable, airflow obstruction within the lung that is often reversible either spontaneously or with treatment.
-
BA - PathophysiologyTriggersExerciseAnimalsPollenAerosol chemicalsDust mitesRespiratory tract infectionSmokeChanges in temperatureDrugsStrong emotional expression
-
BA - PathophysiologyCells in AsthmaMast cellsEosinophilsNeutrophilsT CellsMacrophage and Dendritic CellsAirway Smooth Muscle CellsEpithelial Cells and Goblet Cells
-
Mast Cells and BasophilsExpression of the high-affinity IgE receptorActivated by IgE-allergen complexReleaseHistamineTryptaseLeukotrienesProstaglandinsCytokines
-
EosinophilsActively recruited into the airway by chemokines upon allergen exposureReleaseGranule proteinsLeukotrienesProstaglandinsCytokines
-
BA - PathophysiologyMolecular MediatorsCytokinesChemokinesIgELeukotrienesProstanoidsNitric OxideGranule Proteins
-
CytokinesKey mediators in the pathogenesis of the crhonic inflammationIL-5Activates Eosinophils
-
ChemokinesRecruitment or chemotaxis of inflammatory cellsImportant for localisation of inflammatory cells into the airways
-
IgETriggering mast cells activationHigh level is present especially in allergic asthma
-
MODERN VIEW OF ASTHMAEosinophilMast cellAllergenTh2 cellNeutrophilMacrophage/Dendritic cell
-
BA - EpidemiologyWorldwide, 300 million people of all ages, and all ethnic backgrounds suffer from asthma.
In SouthEast Asia, the number of persons with asthma is around 17.5 million.
Higher in urban compared to rural population
-
Asthma Prevalance and MortalityGINA 2007
-
BA - SymptomologyShortness of breathWheezeChest tightnessCoughVariable and precipitated by non-specific irritantsWorsening at nightRespond to Asthma treatment
-
Questions to Consider in the Diagnosis of BAHas the patient had an attack or recurrent attacks of wheezing?Does the patient have a troublesome cough at night?Does the patient wheeze or cough after exercise?Does the patient experience wheezing, chest tightness, or cough after exposure to airborne allergens or pollutants?Do the patients colds go to the chest or take more than 10 days to clear up?Are symptoms improved by appropriate asthma treatment?
-
BA - Physical examinationWheezingTurbulent airflow through narrowed airwaysUsually expiratoryMaybe absent in very mild or very severe diseaseSigns of rhinitis, sinusitis and nasal polypsDuring acute exacerbationLung hyperinflationUse of accessory muscles of respiration Prolonged expiratory phase of breathing
-
BA - InvestigationsPeak Expiratory Flow RateSpirometryBronchial Challenge TestBlood testsABG, systemic eosinophilia, serum IgE levelsSputum testsEosinophils countsAllergy TestsSkin prick test, Patch test, IgE RAST testsExhaled Nitric Oxide
-
Important Information in PEFR ChartDiurnal VariabilityReversibilityCurrent PEFR / Personal Best PEFR
-
Lung Function Test
-
Important Information in SpirometryFEV1/FVCIndicating airflow obstructionFEV1%Indicating the severity of airflow obstructionReversibility of airflow obstruction FEV1% > 12% FEV1 > 200ml
-
BA - ManagementEducationImprove patient understanding of BAEncourage adherence to treatment Engage patient in self-management practiceAction plan during Asthma exacerbationEnvironmental ControlAvoidance of aeroallergens, viral respiratory pathogens, air pollution and certain drugsVaccinationInfluenza vaccinePneumococcal vaccine
-
BA Management CONTROL
-
OverviewBronchial AsthmaDefinitionPathophysiologyPathogenesisEpidemiologySymptomologyPhysical SignsInvestigationsTreatment plan
Comparison of BA vs COPDCOPDDefinitionPathophysiologyPathogenesisEpidemiologySymptomologyPhysical SignsInvestigationsTreamtent plan
-
What is COPD?Pulmonary Component Airflow limitation which is not fully reversibleMixture of airway disease and parenchymal destructionProgressiveAbnormal inflammatory response Extra-pulmonary ComponentCo-morbidities associated with smoking and aging?Systemic inflammatory disorderPreventable and Treatable
-
Clinical Disorders associated with COPDEmphysemaAirspace enlargment due to disappearance of alveolar septae, leading to loss of elastic recoil, airflow obstruction, hyperinflation and air-trappingChronic BronchitisDaily chronic cough and sputum production for 3 months, two years in a row
-
COPD - Risk factors
-
Fletcher Curve
-
COPD - Risk FactorsTobacco Smoke incl. cigarettes, cigarsOccupational Dust and ChemicalsIndoor and Outdoor Air Pollution?HazeGenderFemale is more susceptibleInfectionChildhood respiratory infectionSocioeconomic Status-1 anti-trypsin deficiency
-
COPD - PathogenesisInflammationProteinase-Antiproteinase ImbalanceOxidant-Antioxidant ImbalanceApoptosisMucus Hypersecretion
-
InflammationRecruitment of inflammatory cells caused by smoking and other irritantsThe inflammation may persist long after smoking cessationMacrophageReleases proteinaseProduces chemotactic factorsProduces matrix metalloproteinasesCD4+, CD8+ and B cells form bronchus-associated lymphoid tissue (BALT)Upregulation of IL-8, MIP 1-, MCP-1 and etc
-
Proteinase-Antiproteinase ImbalanceNeutrophil elastaseMatrix metalloproteinasesEffect of proteinaseDegrading matrix proteinReleasing cell-bound and matrix-bound chemokinesActivating growth factorsInducing expression of mucin genesAntiproteinases : 1-antitrypsin
-
Oxidant-Antioxidant ImbalanceReactive oxygen speciesHydrogen peroxideHydroxyl radicalsSuperoxide radicalsNeutrophil myeloperoxidaseEffects of OxidantInhibit anti-proteinasesAffect lipid and DNAInduce apoptosisFacilitate proteinase-mediated extracellular matrix degradationParticipate in nonenzymatic degradationAntioxidant : Nuclear factor E2-related factor, glutathione peroxidase
-
ApoptosisLost of alveolar tissueAlveolar vascular destructionCigarettes smoking induces apoptosis
-
Mucus HypersecretionHyperplasia of goblet cellsHypertrophy of glands ratio of glandular mucus cells to serous cells acidity mucin glycosylation antimicrobial peptides
-
Muscarinic Receptor Subtypes in AirwaysPre-ganglionic nerveParasympathetic ganglionPost-ganglionic nerveAChAirway smooth muscleNicotinic receptorsM1 receptorsM2 receptors M3 receptorsStimulation causes bronchoconstrictionStimulation causes bronchoconstrictionStimulation inhibits Ach release from cholinergic n. endings
-
Epidemiology of COPD6th leading cause of Death worldwide in 1990? 3rd leading cause by 2020In Malaysia4.7% of population age >30 years old
-
COPD - SymptomologyDyspnoea Effort ToleranceChronic CoughWheezingChest Tightness
Weight loss)Anorexia) Severe COPDDepression / Anxiety)
History tends to be progressive with intermittent exacerbation
-
COPD Physical SignsPhysical ExaminationImportant but rarely diagnosticCyanosisTracheal TugBarrel ChestedIntercostal recessionProlonged Expiratory Phase with RhonchiLoss of Cardiac and Liver DullnessSigns of Cor Pulmonale
-
COPD - InvestigationSpirometry FVC FEV1FEV1/FVC Total Lung Volume Residual Volume DLCO FEF 25%-75%
-
COPD - InvestigationSpirometry FVC FEV1FEV1/FVC < 70% Total Lung Volume Residual Volume DLCO FEF 25%-75%
-
COPD - Other InvestigationCXRABGAlpha-1 Anti-trypsin Level
-
COPD - CXR
-
COPD - CT
-
COPD - Management
-
OverviewBronchial AsthmaDefinitionPathophysiologyPathogenesisEpidemiologySymptomologyPhysical SignsInvestigationsTreatment plan
Comparison of BA vs COPDCOPDDefinitionPathophysiologyPathogenesisEpidemiologySymptomologyPhysical SignsInvestigationsTreamtent plan
-
COPD Asthma
-
COPD is NOT Asthma Different Causes Different Inflammatory Cells Different Mediators Different Inflammatory Consequences Different sites Different response to treatment
-
Different Causes
-
Different Causes
-
Different Causes
-
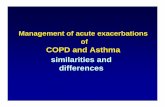
Alveolar macrophageNeutrophilAlveolar wall destructionMucus hypersecretionCytokines (IL-8)Mediators (LTB4)CD8+ lymphocyteProteasesNoxious agent Sensitizing agentAirway thickeningCD4+ lymphocyteMast cellEosinophilHistamineMediators (LTD4)Cytokines (IL-4, IL-5, IL-13) Inflammatory mediatorsAirway hyperreactivityPathophysiology of COPD and Asthma AsthmaCOPDEpithelial sheddingBarnes PJ (1999; 2000)
-
CTS Guidelines Committee Can Respir J 2003; 10 (Suppl A): 11A-33A, p. 16ACTS Guidelines Committee Can Respir J 2003; 10 (Suppl A): 11A-33ACOPD vs ASTHMA Clinical DifferencesPeter J Barnes, 1999
-
CTS Guidelines Committee Can Respir J 2003; 10 (Suppl A): 11A-33A, p. 16ACTS Guidelines Committee Can Respir J 2003; 10 (Suppl A): 11A-33ACOPD vs ASTHMA Clinical DifferencePeter J Barnes, 1999
-
OverviewBronchial AsthmaDefinitionPathophysiologyPathogenesisEpidemiologySymptomologyPhysical SignsInvestigationsTreatment plan
Comparison of BA vs COPDCOPDDefinitionPathophysiologyPathogenesisEpidemiologySymptomologyPhysical SignsInvestigationsTreamtent plan
-
Case 124, , feels SOB at night. She gets the symptoms half of the time. The other half of the time, she is very well without limitation to her exercise.
Bronchial AsthmaCOPDCombination of A+BI dont know, thats why I am here
-
Case 260, , feels SOB on exertion. She gets the symptoms all the time. Her SOB is persistent and gradually worsened over a 2-year period. She is a chronic heavy smoker.
Bronchial AsthmaCOPDCombination of A+BI dont know, thats why I am here
-
Case 350, , feels SOB at night. She gets the nocturnal symptoms half of the time. She also has reduced in effort tolerance in the past 2 years. She noticed there was a steady trend towards worsening. She is a chronic heavy smoker.
Bronchial AsthmaCOPDCombination of A+BI dont know, thats why I am here
-
Case 450, , feels SOB on exertion. She has a history of poorly control asthma for 30 years. She usually gets her nocturnal symptoms, but over the past 2 years, she noticed that she is getting the similar symptoms during the daytime especially on exertion. The SOB is persistent and progressive, and it did not seem to respond to her bronchodilator. She is a life-long non smoker.
Bronchial AsthmaCOPDCombination of A+BI dont know, thats why I am here
-
The End
Five muscarinic receptor subtypes have been identified, of which three subtypes (M1 M3) have been identified in human airways. The function of the three subtypes (M1, M2 and M3) is known.These receptor subtypes serve different regulatory functions. M1 receptors facilitate ganglionic transmission and enhance cholinergic reflex effects in the airways. The bronchoconstrictor and mucous secretory response to acetylcholine and cholinergic nerve stimulation is post-junctionally mediated primarily through M3 receptors.The pre-junctional M2 receptors on post-ganglionic cholinergic nerves have an autoinhibitory effect on acetylcholine release. Barnes PJ. New developments in anticholinergic drugs. Eur Respir Review 1996;6(39):2904COPD and asthma are very different diseases in terms of cellular mechanisms, inflammatory mediators and effects, and response to therapy.7Asthma is usually triggered by a sensitizing agent or stimulus, such as animal hair or exercise, and is characterized by an eosinophilic inflammation, which appears to be influenced by CD4+ lymphocytes (T-helper type 2 cells).7 In COPD, cigarette smoking and other inhaled irritants may initiate the inflammatory response, and in contrast to asthma, it is a neutrophilic inflammation, predominantly involving CD8+ lymphocytes (cytotoxic T-cells).7,8In the asthmatic patient, inflammation affects all of the airways,7 including epithelial shedding, resulting in thickening of the airway wall that encroaches upon the airway lumen. Unless the asthma is very severe, this airway obstruction is completely reversible.The peripheral airways and lung parenchyma are the areas mainly affected in COPD, and the inflammatory process results in tissue destruction, fixed structural narrowing of the airways, and mucus hypersecretion.8
Barnes PJ. Mechanisms in COPD: differences from asthma. Chest. 2000;117:10S-14S.Barnes PJ. Managing Chronic Obstructive Pulmonary Disease. London: Scientific Press Limited, 1999. The result is air trapping and hyperinflation, similar to what occurs in advanced asthma, but in COPD, this hyperinflation tends to be permanent and progressive.
The result is air trapping and hyperinflation, similar to what occurs in advanced asthma, but in COPD, this hyperinflation tends to be permanent and progressive.