AVR: Choice of Prosthesis Tirone E. David University of Toronto.
32
AVR: Choice of Prosthesis Tirone E. David University of Toronto
-
Upload
erica-lloyd -
Category
Documents
-
view
217 -
download
2
Transcript of AVR: Choice of Prosthesis Tirone E. David University of Toronto.

AVR: Choice of Prosthesis
Tirone E. David
University of Toronto

AVR: Choice of Prosthesis
“The perfect heart valve substitute
is yet to be discovered”

AVR: Choice of Prosthesis
Mechanical valves are durable but require life-long anticoagulation
Tissue valves do not require anticoagulation but they are not as durable

AVR: Choice of Prosthesis
Mechanical Valves
Tissue Valves
Bioprosthetic Porcine
Pericardial
Biological:Aortic homograft
Pulmonary autograft
AVR: Choice of Prosthesis
Does the type of heart valve prosthesis affect patients’ survival?
Randomized clinical trials

VA Randomized Trial
Outcomes 15 Years After Valve Replacement With a Mechanical Versus a Bioprosthetic Valve: Final Report of the Veterans Affairs Randomized TrialHammermeister K et al. - J Am Coll Cardiol 2000;36:1152-8
Between 1977 and 1982, 394 men undergoing AVR wererandomized in the OR to receive either the Björk-Shiley spherical disc mechanical prosthesis or a Hancock porcinebioprosthetic valve

VA Randomized TrialLate Mortality After AVR
79±3%
66±3%
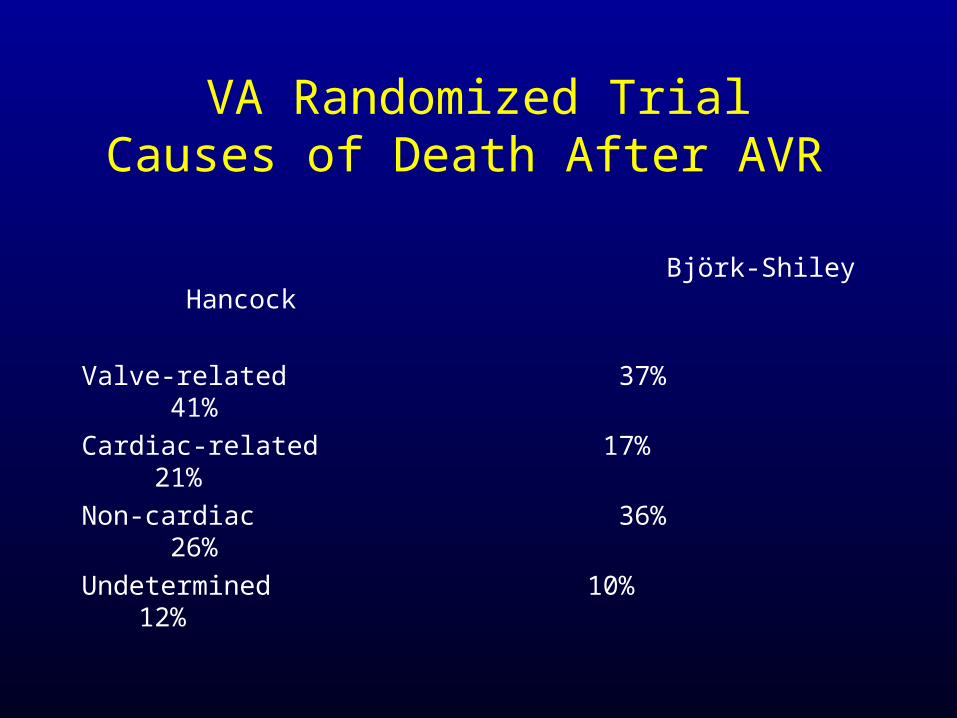
VA Randomized TrialCauses of Death After AVR
Björk-Shiley Hancock
Valve-related 37% 41% Cardiac-related 17% 21% Non-cardiac 36% 26% Undetermined 10% 12%
Edinburgh Randomized Trial
Twenty year comparison of a Björk-Shiley mechanicalheart valve with porcine bioprosthesis
Oxenham H et al. – Heart 2003;89:715-21
Björk-Shiley mechanical vs. porcine bioprosthesis 541 patients ~54±10 years of age 211 – AVR 261 – MVR 61 – AVR+MVR

Edinburgh Randomized TrialPatients’ Survival After AVR
All patients
Survival at 20 years:Mechanical = 28±4%Bioprosthesis = 31±5%

AVR: Choice of Prosthesis
• These two randomized trials used first
generation bioprosthetic heart valves
• The mechanical valve used is no longer available
• Are the findings applicable to our practice today?

1st and 2nd Generation Bioprosthetic Valves
0
20
40
60
80
100
2 4 6 8 10 12 14 16 18 20
Years
% f
ree
from
fai
lure
Hancock Hancock II
Hancock - StanfordHancock II - Toronto

AVR: Choice of Prosthesis
Does the type of heart valve prosthesis affect patients’ survival?
Retrospective clinical studies

Twenty-year comparison of tissue and mechanical valvereplacementKhan S et al - J Thorac Cardiovasc Surg 2001;122:257-69AVR:
666 patients with mechanical ~ 64 years of age725 patients with bioprosthesis ~72 years of age
AVR: Choice of Prosthesis

AVR: Mechanical vs Bioprosthesis
Patients’ Survival
JTCVS 2001;122:257-69

Aortic valve replacement in patients aged 50 to 70 years: Improved outcome with mechanical versus biologic prosthesesBrown ML, Schaff HV, et al – JTCVS 2008;135:878-84
1990 to 2000:510 St. Jude +/- CABG and 257 CE +/- CABG
Matched 1:1 - age, gender, CABG, valve size: 220 in each group
AVR: Choice of Prosthesis
AVR: Choice of Prosthesis
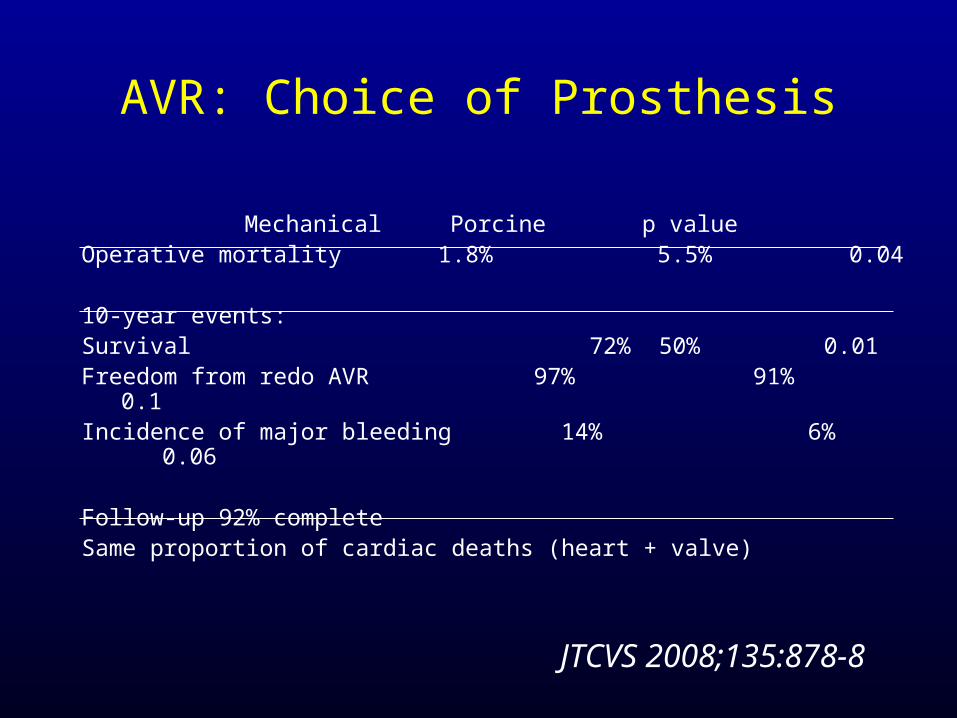
Mechanical Porcine p valueOperative mortality 1.8% 5.5% 0.04
10-year events:Survival 72% 50% 0.01Freedom from redo AVR 97% 91% 0.1Incidence of major bleeding 14% 6% 0.06
Follow-up 92% completeSame proportion of cardiac deaths (heart + valve)
JTCVS 2008;135:878-8

Risk-corrected impact of mechanical versus bioprosthetic valves on long-term mortality after aortic valve replacementOle Lund and Martin Bland – JTCVS 2006;132:20-6 Mechanical BioprostheticNumber of articles 15 23Number of patients 8,578 8,861Mean age in years 58 69 CABG 16% 34% Endocarditis 7% 2% Overall death/year 3.99% 6.33%
AVR: Choice of Prosthesis
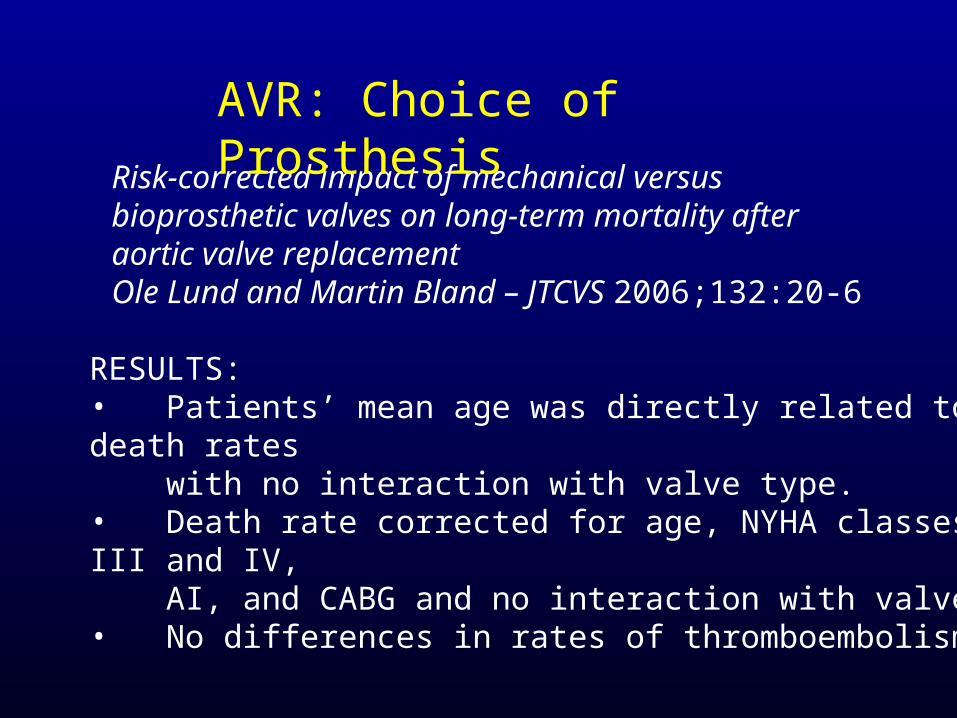
Risk-corrected impact of mechanical versus bioprosthetic valves on long-term mortality after aortic valve replacementOle Lund and Martin Bland – JTCVS 2006;132:20-6
RESULTS: • Patients’ mean age was directly related to death rates with no interaction with valve type. • Death rate corrected for age, NYHA classes III and IV, AI, and CABG and no interaction with valve• No differences in rates of thromboembolism.
AVR: Choice of Prosthesis

AVR: Choice of Prosthesis
Conventional wisdom:
Survival after AVR is not affected by the type of aortic valve prosthesis

AVR: Choice of Prosthesis
• Are valve-related complications dependent on the type of heart valve prosthesis?

VA Randomized TrialAVR: Morbid Events at 15 years
Björk-Shiley Hancock p value
Any valve-related complication 65±4% 66±5% 0.26 Systemic embolism 18±4% 18±4% 0.66 Bleeding 51±4% 30±4% 0.0001Valve thrombosis 2±1% 1±1% 0.33 Endocarditis 7±2% 15±5% 0.45Perivalvular regurgitation 8±2% 2±1% 0.09 Reoperation 10±3% 29±5% 0.004 Primary valve failure 0±0% 23±5% 0.0001

Study end-points:• Valve-related mortality• Valve-related morbidity• Valve-related reoperation
Performance of bioprostheses and mechanical prosthesesAssessed by composites of valve-related complications to15 years after aortic valve replacementV. Chan, WRE Jamieson et al. – J TCVS 2006;131:1267-73
AVR: Choice of Prosthesis

Mechanical vs. Bioprosthesis Freedom from valve-related reoperations 51-60 years
JTCVS 2006;131:1267-73
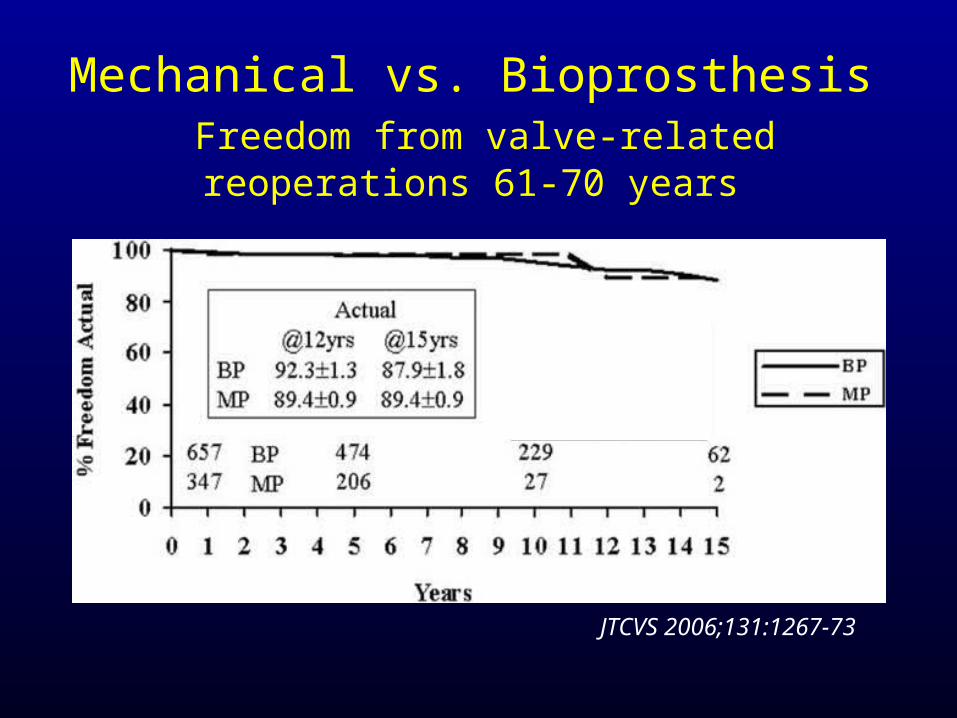
Mechanical vs. Bioprosthesis Freedom from valve-related reoperations 61-70 years
JTCVS 2006;131:1267-73

Mechanical vs. BioprosthesisFreedom from valve-related reoperations >70 years
JTCVS 2006;131:1267-73

Conclusion:
No differences were observed in valve-related reoperation and mortality in patients >60 years. Comparative evaluation givespriority for bioprostheses in patients >60 years based on improvedmorbidity profile.
Performance of bioprostheses and mechanical prosthesesAssessed by composites of valve-related complications to15 years after aortic valve replacementV. Chan, WRE Jamieson et al. – J TCVS 2006;131:1267-73

AVR: Hancock IIFreedom from Failure by Age
0
20
40
60
80
100
0 2 4 6 8 10 12 14 16
Years
Percent free
<65 yrs >65 yrs
Pts at risk306 250 162 61
704 442 202 25
±
Age 10 yr 15yr <65y 94 ± 2 72 ± 5 >65y 99 ± 1 99 ± 1

Quality of LifeMechanical vs Bioprosthesis
“Quality of life in patients with biological and mechanical prostheses. Evaluation of cohorts of patients aged 51 to 65 years at implantation” - Perchinsky et al. Circulation 1998;98:II-81-87.
Study design:
QOL in age and sex matched patients with mechanical and biological valve and general population
SF-12 form & Lamy Smiley Faces form
Quality of LifeMechanical vs Bioprosthesis
• Patients with mechanical valves were troubled with noise, bleeding and blood tests (p<0.01)
• Patients with bioprosthesis were troubled with prospect of reoperation (p<0.01)
• No difference in fear of valve failure• QOL similar in both groups and general
population• 97% would make the same choice of valve
Perchinsky et al. Circulation 1998

Quality of LifeMechanical vs Bioprosthesis
Conclusions:
• Human beings are resilient and adaptable
• Most patients with prosthetic heart valves are well adjusted to their condition
AVR: Choice of Prosthesis
• Patients’ age is probably the most important factor in recommending tissue or mechanical valve
• Bioprosthetic valves are ideally suitable for older patients (>70 years) or those who are not likely to outlive the valve (co-morbidities)
• Mechanical valves should be recommended to younger patients (<60 years)
• If anticoagulation is a perceivable problem, tissue valves can be used in younger patients but the probability of reoperation is high