Avon Breast cancer in LMICs: Meeting the challenge 131011

of 50
-
Upload
presentacionesfk -
Category
Documents
-
view
224 -
download
0
Transcript of Avon Breast cancer in LMICs: Meeting the challenge 131011
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
1/50
Breast Cancer in LMICs:Meeting the Challenge
Felicia Marie KnaulOctober 13, 2011
The 2011 Breast Cancer Global CongressA partnership of the US Department of
State and the Avon Foundation for Women
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
2/50
From anecdote
to evidence
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
3/50
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
4/50
January, 2008
June, 2007
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
5/50
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
6/50
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
7/50
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
8/50
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
9/50
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
10/50
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
11/50
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
12/50
Con jf en harvard
Harvard School of Public Health
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
13/50
Global Task Force on Expanded
Access to Cancer Care and Control
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
14/50
From anecdote
to evidence
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
15/50
Challenge and disprove the
myths about cancerM1. Unnecessary
M2. Unaffordable
M3. Impossible
M4: Inappropriate
Expanding access to cancer careand control in LMICs:
Should, Could, and Can be done
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
16/50
Breast cancer: myths and realities
It is a disease ofdeveloped countries
It is a disease ofolder women
It is of lower prioritythan cervical cancer
The majority of cases anddeaths occur in the
developing world
A large proportion of casesand deathsperhaps the
majorityhappens in
women
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
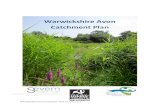
17/50Source: Knaul, Arreola, Mendez. estimates based on IHME, 2011.
The cancer transition in LMICs:
breast and cervical cancer 1980-2010
53%47%
20%24%
19%
-31%
60%
-40%
0%
40%
80%
LMICs High income
BC cases
BC deaths
CC cases
CC deaths
% Change in incidence and mortality
Th i i i LMIC
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
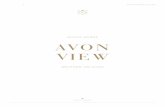
18/50Source: Knaul Arreola Mende . estimates based on IHME 2011.
LMICs as % of global incidence and mortality
Breast
Cervical
The cancer transition in LMICs:
breast and cervical cancer 1980-2010
0%
30%
60%
90%
1980 2010 1980 2010
52%
59%
49%
63%
79%
87%82%
88%
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
19/50
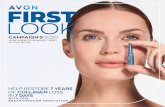
Source: Knaul et al., 2008. Reproductive Health Matters, and updated byKnaul, Arreola-Ornelas and Mndez based on WHO data, WHOSIS (1955-
1978), and Ministry of Health in Mexico (1979-2006)
1995 2000 2005
Costa Rica 1995 - 2005
Breast cancer
Cervical cancerSource: Instituto Nacional de Estadstica y Censos, Ministerio de Salud,Unidad de Estadstica, Registro Nacional de Tumores de Costa Rica.
The Cancer Transition, Mexico and Costa Rica:
breast and cervical cancer, mortality time series.
0
4
8
12
16
1955
1965
1975
1985
1995
2005
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
20/50
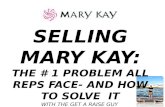
Source: Lozano, Knaul, Gmez-Dants, Arreola-Ornelas y Mndez, 2008, Tendencias en la mortalidad por cncer de Mama en Mxico, 1979-2008.
FUNSALUD, Documento de trabajo. Observatorio de la Salud.
1979
1985 1995
Nuevo Len
2008
0
Oaxaca
5
10
15
20
25
1979 1985 1995
2008
The cancer transition within Mexico:
breast and cervical cancer 1979-2008
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
21/50
Adults
Breast
Cervix Prostate
Testis
HL
N HL
Leukaemia
All cancers
Source: Knaul, Arreola, Mendez. estimates based on IARC, Globocan, 2010.
Children
LOW
INCOME
HIGH
INCOME
Survival
inequalitygap
LOW
INCOME
HIGH
INCOME
100%
The opportunity to survive (M/I)
should not be defined by income.
Yet it is.
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
22/50
The divide is the result of concentrating riskfactors, preventable disease, suffering,impoverishment from ill health and deathamong poor populations.
fueled by progress in cutting-edge science andmedicine in high-income countries.
The Cancer Divide:disparities in outcomes
between poor and rich directly related to inequitiesin access and differences in underlying socio-
economic and health conditions.
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
23/50
Cancer is a disease of both rich and poor;
yet it is increasingly the poor who suffer:
Exposure to risk factors
Cancers of infectious origin
Death from treatable cancer
Stigma and discrimination
Avoidable pain and suffering
Impoverishment
The Cancer Divide:
An Equity Imperative
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
24/50
Challenge and disprove the
minimalists:
myths about cancer
M1. Unnecessary NECESSARY
M2. Unaffordable: .for the poorM3. Impossible
M4: Inappropriate: either/or
Challenging cancer implies taking
resources away from other diseases of
the poor
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
25/50
`5/80 Cancer Disequilibrium
Almost 80% of the DALYs (disability-adjustedlife-years) lost worldwide to cancer are in LMICs,yet these countries have only a very small share of
global resources for cancer ~ 5% or less.
Africa
1% of global spending on health64% of new cancer cases
15% of the global population.
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
26/50
Investing in CCC:
We cannot afford not toHealth is an investment, not a cost
World Economic Forum: chronic disease is 1
of the 3 leading global economic risksEconomic value of lost DALYs: $921 million
VSL losses: $2.5 billion
Total economic cost of cancer, 2010
2-4% global GDP
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
27/50
80% of total
75+% ofbreast
95% of cervical
Avoidable cancer deaths:
1/3 to 1/2 or 2.4-3.7 million
Income Region% of all cancer deaths
considered avoidableBreast
Low income 52% 79%
Lower middle
income44% 73%
Upper middle
income33% 56%
High income 21% 40%
LMICs: Avoidable
deaths
i i CCC
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
28/50
Investing in CCC:
we cannot afford not to
Assuming that between 50% of
deaths are avoidable
Total annual cost: $310 billionInvesting in CCC yields an annual
return on prevention and treatment of
between 1.5:1 to 3.7:1.
Economic cost of inaction, 2009
$US 2010 billion130-850
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
29/50
Second-line TB Drugs
(Farmer, 2009)% Decline in price 1997-9
Amikacin 90%
Ethionamide 84%
Capreomycin 97%
Ofloxacin 98%
Reduced drug and vaccine prices
HPV vaccine in LMICs: Before 2011: from $US 30 to $US 100 per dose PAHO Revolving Fund: decreased from US$ 32 per dose inJanuary 2010 to US$ 14 per dose in April 2011. GAVI: June 2011 Merck offers vaccine at US$ 5 per dose for
low income countries.
Hep B vaccine: decline from a 1982 launch price of over $100to $0.20 a dose has enabled developing countries to dramatically
increase vaccination rates with support from GAVI
Ch ll d di th
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
30/50
Challenge and disprove the
minimalists:
myths about cancer
M1. Unnecessary
M2. Unaffordable:M3. Impossible POSSIBLE
M4: Inappropriate: either/or
Challenging cancer implies taking
resources away from other diseases of
the poor
Harvard Breast Cancer in Developing Countries Nov 4 `09
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
31/50
Harvard, Breast Cancer in Developing Countries, Nov 4, 09
Nobel Laureate Amartya Sen,
Cancer survivor,
diagnosed in India 50 years ago
Drew G Faust
President of Harvard University,
Breast Cancer survivor, 20+ yrs
Initial views on MDR TB treatment
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
32/50
In developing countries, people with multidrug-resistant tuberculosis usually
die, because effective treatment is often impossible in poor countries. WHO 1996
Initial views on MDR-TB treatment,c. 1996-97
Source: Paul Farmer., 2009
cured
83%
abandon
therapy
2%
failed
therapy
8%
died
8%
Mitnick et al, Community-based therapy for multidrug-resistanttuberculosis in Lima, Peru. NEJM 2003; 348(2): 119-28.
Outcomes in MDR-TB patients in Lima,
Peru receiving at least 4 months of therapy
MDR-TB is too expensive to treat in poor
countries; it detracts attention and resources from
treating drug-susceptible disease. WHO 1997
PIH DFCI BWH
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
33/50
Rural Rwanda, Burkitts lymphoma
Source: Paul Farmer., 2009
Regimen ofvincristine,
cyclophosphamide,
intrathecal
methotrexate
Status post-CHOPin Central Haiti:
Still in remission
three years later
Central Haiti
0
oncolo
gists
PIH, DFCI, BWH
M t lit f b t d i l i
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
34/50
Source:Lozano, Knaul, Gmez-Dants, Arreola-Ornelas y Mndez, 2008, Tendencias en la mortalidad por cncer de mama en Mxico, 1979-2007.
FUNSALUD, Documento de trabajo. Observatorio de la Salud, con base en datos de la OMS y la Secretara de Salud de Mxico.
Mortality from breast and cervical cancer inMexico,1955-2008: less death from cervical
Age-adjusted rate per 100,000women
0
4
8
12
16
1955
1965
1975
1985
1995
2005
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
35/50
There are many opportunities and
alternatives for action
~Leth
ality(mortality
/incidence)
Source: Author estimates based on IARC, Globocan 2010
Low income
countries
Lower middleincome
Upper middleincome
High incomecountries
0
20
40
6048%
40% 38%
24%~ Lethality Low income: 48%
Lower middle income: 40%
Upper middle income: 38% High income: 24%
Breast Inequality gapin survival
Mxico
Ch ll d di th
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
36/50
Challenge and disprove the
minimalists:
Myths about cancer& NCD
M1. Unnecessary NECESSARY
M2.Unaffordable AFFORDABLE
M2. Impossible POSSIBLE
M4: Inappropriate: either/or
Challenging cancer implies takingresources away from other diseases of
the poor
Women and mothers are at risk for
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
37/50
LMICs
Mortality ofmothers inchildbirth
(-35% 1980-2008)
342,900
Breast andcervical cancer
166,577+142,744
=309,321
Women and mothers are at risk for
many reasons (15-59)
40% occur in pre menopausal
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
38/50
~40% occur in pre-menopausal
women (55
Age of
Diagnosis
Age ofDeath
Source: Author estimates based on IARC, Globocan, 2008 and 2010.
33%
20%54%
66.6%
34.2% 65%
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
39/50
Cases:
Juanita
Mexico
i
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
40/50
The diagonal approach to
health system strengthening
Rather than focusing on disease-specific vertical
programs or only horizontally on system constraints,
harness synergies that provide opportunities to tackle
disease-specific priorities while addressing systemicgaps.
Optimize available resources so that the whole is more
than the sum of the parts.
Bridge the divides as patients suffer diseases over a
lifetime, most of it chronic.
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
41/50
1. Harness platforms: Integrate prevention,screening and survivorship into MCH, SRH,
HIV/AIDs, social welfare/anti-poverty programs.
2. Delivery: Catalyze, employ and deploycommunity health workers and expert patients.
Harness ICT.
3. Financing: Social protection strategies that
include horizontal and vertical coverage.
4. Stewardship: Improve regulatory frameworks to
remove non-price barriers to pain control.
Diagonal Strategies
Mexico Seguro Popular Insurance
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
42/50
Mexico Seguro Popular Insurance
a diagonal strategy that includes financial
protection for catastrophic illness
Accelerated universal vertical coverage by disease
with a specified package of interventions
2004/5: ALL in children, cervical, HIV/AIDS
2006: All pediatric cancers
2007: Breast cancer
2011: Testicular cancer and NHL
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
43/50
Mexico: summary of facts
Since 2006, breast cancer is the second leading cause ofdeath among women aged 30 to 54 years of age and the
principal cause of death due to tumors.
Seguro Popular: since 2007 all women diagnosed with
breast cancer have very complete access to treatmentwith financial protection
Only 5-10% of cases in Mexico aredetected in Stage 1 or in situ
Stage at diagnosis by level of municipal
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
44/50
Stage at diagnosis by level of municipal
marginalization, Mexico, IMSS 2006(Mxico, IMSS 2006)
Source: Authors estimation based on IMSS data, 2006.
N=221(3.8%)
N=1737(30%)
N=2877(49.8%)
N=946(16.4%)
% diagnosed
in Stage 4
Late detection by state
0%
10%
20%
30%
40%
50%
Poor (High) Middle Low Very low
Stage 1 Stage 2
Stage 3 Stage 4
< low
> mid
> high
Why?
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
45/50
Why?
Social and health systems
barriers to early detection
and
non-price barriers to
treatment
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
46/50
br
Juanita:Advanced metastatic breast
cancer is the result of a series of
missed opportunities
M i H i h i l l f
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
47/50
Mexico: Harnessing the primary level of
care for improving BC detection and care
Challenge and disprove the
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
48/50
Challenge and disprove theminimalists:
Myths about breast cancer,cancer& NCD
M1. Unnecessary NECESSARYM2. Impossible POSSIBLE
M3.Unaffordable AFFORDABLE
M4. Inappropriate : APPROPRIATE
B
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
49/50
Be an
optimistoptimalist.
Economics
of hope.Expanding access to cancer care and control in
LMICs: Should, Could, and Can be done
-
8/2/2019 Avon Breast cancer in LMICs: Meeting the challenge 131011
50/50
Breast Cancer in LMICs:Meeting the Challenge
Felicia Marie KnaulOctober 13, 2011
The 2011 Breast Cancer Global CongressA partnership of the US Department of
State and the Avon Foundation for Women