Available options for keratoconus management
72
Available Options For Keratoconus Management BY Dr. Amr Mounir , Lecturer of Ophthalmology Sohag university
-
Upload
amr-mounir -
Category
Health & Medicine
-
view
565 -
download
1
Transcript of Available options for keratoconus management
Available Options For Keratoconus Management
BY
Dr. Amr Mounir , Lecturer of OphthalmologySohag university


DefinitionKeratoconus is a progressive, noninflammatory, bilateral (but usually asymmetric) ectatic corneal disease, characterized by paraxial stromal thinning and weakening that leads to corneal surface distortion..

Etiology
- History of trauma that causes weakness
- Recurrent trauma due to rubbing from
Blepharitis, Vernal keratoconjuctivitis
- Inflammatory component !!!Decrease proteinase inhibitors
Increase collagenasePremature keratocytic apoptosis
Increase cytokine binding

Pathology-- Epithelial
basement membrane fragmentation and scarring
-- Axial stromal thinning and scarring
- Breaks in and folds close to the Descemet membrane result in
acute hydrops

Clinical Picture
Patients with keratoconus (KC) often report decreasing vision (distortions, glare/flare, and monocular diplopia or ghost images), with multiple unsatisfactory attempts in obtaining optimum spectacle correction

Signs
- Decrease in visual acuity- Progressive myobia ,irrigular
Astigmatism
- Oil droplet sign by direct ophthalmoscope - irregular scissoring by retinoscopy

Slitlamp findings FLEISCHER RING abrupt change in curvature
VOGT’S STRIAE 1st Sign
STROMAL THINNING
STROMAL SCARS
ENLARGED CORNEAL NERVES
ACUTE HYDROPS

FLEISCHER RING

VOGT’S STRIAE

Healed aCUTE HYDROPS

Investigations
1- Old methods :
A- Placido DiscB- Retinoscopy
2- New Methods : A- Corneal topography
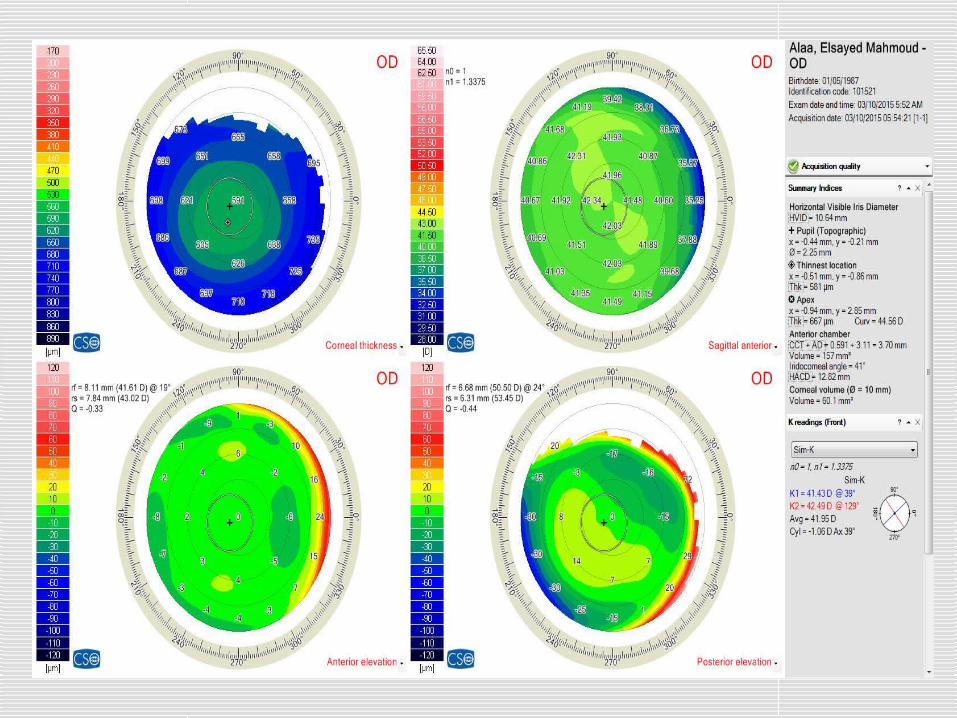
B- Pentacam

What Pentacam says to us???
1- Pachymetry map2- Keratometry map ( K1,K2,Kmax(
3- Cone site and shape
4- Elevation map5- Provisional diagnosis: Keratoconus
Summary ( Sirus device(
6- Aberration map7- Scheimpflug imaging

Keratoconus summary

Scheimpflug imaging

Classifications of keratoconus
Several classifications of keratoconus based on:
1- Morphological Patterns2- Topographical Patterns

Morphological Patterns

Nipple cone

Oval cone

Morphological Patterns

Topographical Patterns
Krumeich Classification of Keratoconus:
Severity of KC is also classified by Krumeich. This classification depends on mean K-readings on the anterior curvature sagittal map, thickness at the thinnest location, and the refractive error of the patient .


Forme Fruste Keratoconus
Forme Fruste Keratoconus (FFKC(:
is a subclinical disease and is not a variant of KC. Although clinicians use many other terms such as mild KC, early KC, and subclinical KC

Recently, there are two opinions regarding the definition of this disease:
1. FFKC is a completely normal cornea with neither clinical nor topographical risk factors, but this cornea is able to develop KC when treated by laser. The fellow eye may be keratoconic or there may be a family history of KC

2. FFKC is an abnormal cornea. Corneal topography or corneal hysteresis or both are abnormal; i.e., there are risk factors but the case is still not a clinically obvious KC.


Another Examble


Pellucid Marginal Degeneration (PMD) and Pellucid-like Keratoconus
- PMD is a bilateral, non-inflammatory, peripheral corneal thinning disorder characterized by a peripheral band of thinning of the inferior cornea. The cornea in and adjacent to the thinned area is ectatic.
- Patients usually are aged 20–40 years at the time of clinical presentation.


Keratoglobus

Options For Treatment

Options For Treatment
Depend on :1- Age
2- Refraction
3- Pachymetry4- Keratometry5- Cone Position
6- Corneal Opacifications.

Options
1- Glasses and follow up.
2- Hard Contact Lens.
3- CXL ( Transepithelial – Epi-off(.
4- Rings ( Kerarings- Myoring(.
5- Keratoplasty(Lamellar – penetrating (

Rules in treatment 1- Non of treatment options is satisfactory for the
patient.2- The disease is progressive by its nature.
3- Follow up is mandatory.4- Combination of treatment options can be done.
5- Keratoplasty can be a final destiny even with treatment.
6- Rings mostly will be followed by glasses.7- Don't judge on improvement of V\A without correction.
6- Financial aspect should be taken into consideration.

Glasses and follow upWhen ?????
1- Age > 28 ys old.2- Stable and low refraction with BCVA
>6/243- Clear cornea
4- Favorable Pentacam: 1( Average Keratometry <46 Ds
2( Thinnest Pachymetry > 480 um

Hard Contact Lens
-- GP lenses are not the same as the old hard lenses. For one thing, GP lens materials allow oxygen to pass through the lens and reach the cornea.
- With advances in manufacturing, GP lenses are made in thinner designs, larger diameters, and with more consistently smooth edges than ever before.

- GP contact lenses are custom made for each individual.
- Parameters which are needed for GP contact lens request.
1( Keratometry: for initial fitting2( Refraction.


- Soft lenses do provide better initial comfort, while GP lenses require a brief adaptation period. But this is due to the size of the lens — not the lens material.
- Soft lenses are larger in diameter than GP lenses and "tuck under" the eyelids. As a result, you don't feel the lens edges when you blink. But since GP lenses are smaller, during blinking your eyelids will experience initial "lens awareness.

Hybrid lenses
This is a lens design combination that has an RGP center surrounded by a soft peripheral “skirt”. Hybrid contact can provide the crisp optics of a GP lens and wearing comfort of soft contact lenses. They are available in a wide variety of parameters to provide a fit that conforms well to the irregular shape of a keratoconic eye.


CXL (Transepithelial – Epi-off(.

Why CXL is important???
- The only actual therapy for keratoconus.
- Main effect is stiffening and flattening.
- Long term effect.
- Minimal optical effect.

1-Transepithelial CXL
Important hints:- Less effective than Epi-off.( Less
flattening effect(
- Less complications rate.
- More comfortable for the patient.

When to do ?????
- Early Keratoconus. 46 Ds<Mean K < 48 Ds
- Middle aged patients.
- Very thin corneas.
- After ICRS.
- Inadequate follow up.


2- Epi-Off CXL
When to do???- In moderate and advanced cases.
- In young patients < 25 ys old.


Intracorneal Rings


Types of Rings

Ideal patient for rings
- High errors.
- Mean Keratometry > 48 Ds- K Max > 50 Ds
- BCVA < 6/30
- High patient motivation

Which type ?????

Kerarings
- Non central cones.
- High cylinder.
- High difference between K1, K2.
- Thickness at insertion site >400 um

Pre and post Kerarings Pentacam

Myoring
- Central cones ( Nipple ,Oval , Globus(
- High K readings K1, K2 with low difference.
- High errors with high sphere.
- Thinnest location > 400 um.
- Epi-off like CXL.
- Eye without refraction.

Pre and post Myoring Pentacam

Central cone - Refraction : -8 Ds -7 Dc- Very high K readings For Myoring implantation

-Shifted cone , Refraction : -9Ds -4.5 Dc- K2 @ 68 For Kerarings implantation

Combined CXL with rings

When to do ???
With Myoring:-It should be done in the same session
( intrapocket CXL(.
- Epi-off like effect as it crosses the epithelium
With Kerarings:-It should be done in the same session or after
ring implantation not before.

Age as a guideline for decision

Young age < 25 ys ---------- be more aggressive Early Keratoconus: Epi-off CXL stabilization and follow upModerate and severe Keratoconus: CXL stabilization + Rings Regularization and Flattening Advanced opacified cornea : Keratoplasty

Middle age > 25 ys ---------- be less aggressive
Early Keratoconus: Epi-on CXL or follow upModerate and severe Keratoconus: Rings Regularization and Flattening with follow up if progression Stabilization by CXL
Advanced opacified cornea : Keratoplasty

Rings in advanced cases

Aim:
- To delay corneal grafting.
- To make the eye refractable.
- To decrease coma aberrations.
N.B: Keratoplasty is still an option



Home message
- Many guidelines affect our decision in keratoconus management.
- Pentacam is an important tool in evaluation of Keratoconus patient.
- Age is a guiding factor in treatment with aggressive attitude in young age.
- Customization should be done for every patient in keratoconus management.

Thank you