Autonomic Disorders of the Urogenital System

of 17
-
Upload
blanca-dora-becerra-diaz -
Category
Documents
-
view
236 -
download
0
Transcript of Autonomic Disorders of the Urogenital System
-
8/11/2019 Autonomic Disorders of the Urogenital System
1/17
AUTONOMIC
DISORDERS OF THEUROGENITAL SYSTEMClare J. Fowler
ABSTRACT
The highly distributed nature of the neural control of the bladder and genitaliameans that disorders of these functions are very likely to occur with many differentneurologic diseases, although the range of symptoms is limited. In this chapter theclinical presentations and recommended management of urogenital symptoms inthree conditions are described: multiple sclerosis, the commonest cause ofneurogenic urogenital dysfunction; multiple system atrophy, a much less commoncondition, but one in which urogenital dysfunction occurs early; and a disorder ofvoiding, which affects neurologically healthy women, now referred to as Fowlerssyndrome.
Continuum Lifelong Learning Neurol 2007;13(6):165181.
INTRODUCTION
The lower urinary tract is peripherallyinnervated by nerves of the autonomicnervous system, but a hierarchy ofhigher centers is involved in the per-ception of bladder fullness and thedecision about the appropriateness of
when to void. In fact, continencedepends on the integrity of the centraland peripheral nervous systems at manydifferent levelspossibly more so thanany other bodily function. Thus, dis-turbances of bladder function can resultfrom disease or disorders of the neo-
cortex, basal ganglia, pons and brainstem, spinal cord, and the peripheralinnervation. But because the repertoireof bladder behavior is limited, the rangeof dysfunction is also restricted. Therecan be abnormalities of the storagephase, ie, incontinence, or abnormali-ties of the voiding phase, ie, retention,or a combination of both problems,
while the neurologic causes are diverse.The neurology of sexual function is
less well defined, but it again depends
on innervation of the genitalia byautonomic system nerves while highercenters modulate that innervation.
In this chapter three disorders thatcause bladder and or sexual dysfunc-tion will be reviewed, with a briefdescription for each condition of theneurologic basis for the urogenitaldysfunction, the clinical presentation,and the recommended management.
MULTIPLE SCLEROSIS
Neurologic Basis ofUrogenital Symptoms
Urogenital symptoms in multiple scle-rosis (MS) are common and resultmainly from spinal cord involvement,so that some correlation betweenlower limb and bladder dysfunction isoften clinically apparent (Betts et al,1993). In health, a complex of brainnetworks is involved in the two pro-cesses of bladder storage and voiding,but the final output of these processesis either activation or inhibition of acenter in the dorsal tegmentum of the
165
KEY POINTS:
A The highly
distributed
nature of the
neural control ofthe bladder and
genitalia means
that disorders of
these functions
are very likely to
occur with many
different
neurologic
diseases,
although the
range of
symptoms
is limited.
A The lower urinary
tract is
peripherally
innervated by
nerves of the
autonomic
nervous system,
but a hierarchy of
higher centers is
involved in the
perception of
bladder fullness
and the decision
about the
appropriateness
of when to void.
A Urogenital
symptoms in MS
are common and
result mainly
from spinal cord
involvement, so
that some
correlationbetween lower
limb and bladder
dysfunction is
often clinically
apparent.
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/11/2019 Autonomic Disorders of the Urogenital System
2/17
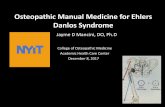
pons, the pontine micturition center(PMC) (Figure 7-1).
From the PMC, direct pathways
project to the sacral segments of thespinal cord (S2-S4) and control para-sympathetic outflow to the detrusorand reciprocal activation of the striatedurethral sphincter. During storage, pa-rasympathetic motor innervation of thedetrusor is inhibited so that the de-trusor pressure does not rise as thebladder fills and tonic firing of themotor units of the striated urethralsphincter and pelvic floor maintain thepressure of the urethra higher than
that within the bladder. At the initia-tion of micturition, a relaxation of thestriated urethral sphincter and pelvicfloor occurs, followed by a coordinatedcontraction of the detrusor muscle.This synergistic activity between thesphincter and the detrusor depends on
connections with the PMC. If theseconnections are damaged or interrup-ted, sphincter contraction may occur as
the detrusor contracts, causing thedisorder known as detrusor sphincterdyssynergia. The most marked abnor-mality, however, which develops fol-lowing disconnection from the PMC, isa newly formed segmental reflex thatcauses reflex detrusor contractions inresponse to bladder distension. Unmy-elinated C fibers, hitherto quiescent(and therefore known as silent Cfibers), become mechanosensitive andrespond to bladder stretch (de Groat
et al, 1990). This afferent activity,through synaptic activity in sacral seg-ments of the cord, causes detrusorcontractions and is responsible for theemergence of the condition of neuro-genic detrusor overactivity (DO) andcomplaints of urinary frequency, ur-gency, and urgency incontinence.
Evidence also points to spinal cordinvolvement as the major cause oferectile dysfunction (ED) in MS (Bettset al, 1994). Cord involvement in MSmay initially result in a partial deficit, sothat ED is variable but with preservedpenile erections nocturnally and onmorning waking (Kirkeby et al, 1988).In the last 20 years the error of thedictum if a man can get an erectionat anytime, impotence is likely to bepsychogenic has been recognized. EDhas been estimated to affect between50% and 75% of men with MS (Zorzonet al, 1999), depending on the severity
of disability of the group studied.Women with MS report sexual dysfunc-tion less frequently than men (Zorzonet al, 1999), but nevertheless, it is aproblem that is thought to affect morethan 50% of women, and incidence in-creases with increasing disability.
Clinical Presentation
Bladder dysfunction. Urinary fre-quency, urgency, and urgency incon-tinence, reflecting the underlying DO
166
FIGURE 7-1 Location of pontine micturitioncenter (PMC). This illustrationhighlights the need for spinal
cord integrity for bladder control since it isparasympathetic and somatic innervation arisesfrom the sacral segments 2-4.
KEY POINT:
A In the last
20 years the
error of the
dictum if aman can get
an erection at
anytime,
impotence is
likely to be
psychogenic
has been
recognized.
"DISORDERS OF THE UROGENITAL SYSTEM
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/11/2019 Autonomic Disorders of the Urogenital System
3/17
and easily demonstrable on cystome-try, are the most common bladdercomplaints in MS. Frequency is due to
the reduced bladder capacity. Urgencyand, if the patient cannot hold on,urgency incontinence, are due to in-
voluntary detrusor contractions. Symp-toms of incomplete bladder emptyingmay be much less prominent, thepatient only admitting to these ifdirectly asked, Do you feel emptyafter voiding? or Can you void againsoon after just doing so? It was foundthat patients who thought they werenot emptying their bladder were often
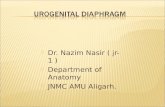
correct, but half of those who thoughtthey were emptying their bladder werelikely to be wrong; hence, the im-portance of measuring the postmictu-rition residual volume with ultrasound(Figure 7-2).
With worsening neurologic diseaseand increasing spinal cord lesions suchthat mobility deteriorates, bladder con-trol is likely to become more difficult totreat. This is a result of worsening ofDO, inefficient emptying of the blad-der, possibly recurrent urinary tractinfections, spasticity, reduction in gen-eral mobility, and sometimes, cognitiveimpairment. Fortunately, however, incontrast to urinary tract dysfunctionfollowing traumatic spinal cord injury,MS rarely causes upper urinary tractinvolvement (Sirls et al, 1994). This istrue even when long-standing MS hasresulted in severe disability and spas-ticity. The reason is not known, but the
implication is that the focus of man-agement should be on symptomaticrelief.
Sexual dysfunction. A study thatanalyzed the type of sexual dysfunc-tion that affected men with MS who
were still ambulant found that ED wasthe most common complaint (63%),followed by ejaculatory dysfunctionand/or orgasmic dysfunction (50%)and reduced libido (40%) (Zorzonet al, 1999). Other nonspecific effects
of MS may also have adverse effects onsexual function, including fatigue, de-pression, spasticity, and anxiety about
incontinence.Although a recent questionnairesurvey of 133 women with mild dis-ability in the United States, of whomhalf reported voiding symptoms, foundthat 70% still enjoyed sexual inter-course, felt aroused, and could expe-rience orgasm (Borello-France et al,
167
FIGURE 7-2 Algorithm for management ofneurogenic incontinence.
PVR = postvoid residual; CISC = cleanintermittent self-catheterization.
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/11/2019 Autonomic Disorders of the Urogenital System
4/17
2004), in women with advancedMS, 62% experienced sensory dysfunc-tion in the genital area (Hulter and
Lundberg, 1995). Loss of orgasmiccapacity is the complaint for whichwomen seek treatment (Dasgupta et al,2004).
Management
Bladder dysfunction. The symptomsof urgency, frequency, and urgency in-continence are due to detrusor over-activity and can, therefore, logically betreated with antimuscarinic agents. Anumber of different preparations are
now available (Table 7-1), and long-acting formulations (extended life[XL]) have the advantage of once-dailyadministration. Patients who have cog-nitive impairment are best treated bythe medications less likely to cross theblood-brain barrier, such as trospiumchloride.
Although it might appear appropri-ate to immediately prescribe an anti-muscarinic for patients complaining ofurinary urgency, a measurement needs
to be made first. If there is any reasonto suspect that the patient is not em-ptying completely, the postmicturition
residual volume should be measured(Fowler, 1996). This can be conve-niently done using a small portableultrasound device, which many special-ist nurse continence advisors haveavailable. It is important to recognizeincomplete emptying because any resi-dual volume in the bladder can trigger
volume-determined reflex detrusorcontractions and thus exacerbate DO.Figure 7-2 shows a simple algorithmfor managing the common symptoms
of bladder dysfunction in MS. Theplace of cystometry and video cysto-metry in the routine investigation ofthese patients is questionable. It hasbeen argued that it is only throughthese investigations that detrusorsphincter dyssynergia can be recog-nized, but since no specific treatment isavailable for that disorder other thanmanaging the consequence, ie, incom-plete emptying and raised detrusorpressure, a pragmatic approach such
168
TABLE 7-1 Oral Antimuscarinic Agents for Treating Symptoms ofDetrusor Overactivity
GenericName
Trade Name inthe United States
Dose(mg) Frequency
EliminationHalf-life ofDrug (Hours)
Propantheline Pro-Banthine 7.515.0 Tid 30 minac and qhs
-
8/11/2019 Autonomic Disorders of the Urogenital System
5/17
as shown in Figure 7-2 has much torecommend it.
If a raised postmicturition residual
volume is demonstrated, some meansof reducing this will be necessary toimprove symptoms. This can be doneby having either the patient or some-times the caregiver perform cleanintermittent catheterization (CIC). CIChas been advocated if the postmictu-rition residual volume is greater than100 mL, a somewhat arbitrary figure,but one about which there seems to begeneral agreement. Teaching the tech-nique is more likely to be successful if
patients are well motivated and havegood cognitive skills and adequatemanual dexterity. Because patients alsoneed to have sufficient mobility to beable to get into a comfortable positionto catheterize efficiently, ideally overthe toilet, severe immobility can pres-ent a problem (Case 7-1).
Unfortunately, little else improvesbladder emptying; although there
were claims that alpha-blockers could
reduce the postmicturition residualvolume, subsequent studies have notconfirmed this. On theoretical grounds
this is not surprising since it is thoughtthe defect of bladder emptying in MSis due to poorly sustained and incoor-dinated relaxation of the striatedsphincter, a muscle on which alpha-blockers are thought to be ineffective.
If patients are performing self-catheterization, urine specimens sentto the laboratory are likely to growmicroorganisms, although other crite-ria that indicate a urinary tract infectionare not present. However, if genuine
recurrent urinary tract infections dooccur with the expected clinical symp-toms of dysuria and change in colorand odor of the urine, investigationsshould be carried out to discover ifthere is a nidus for infection in theurinary tract, and a urologic referral ismandatory. Hematuria is another indi-cation for prompt urologic referral.
An additional therapy that maysometimes be of value is the synthetic
169
Case 7-1A 42-year-old woman, diagnosed with MS 6 years ago when she presentedwith sensory symptoms followed by optic neuritis, has suffered adeterioration of mobility over the last year, such that she now needs a canefor walking. She reports poor bladder control, which has been present forthe past 2 to 3 years but has noticeably worsened in the last year. Herproblems are of urinary frequency, such that she has been restricting fluidintake, but her most troublesome symptom is urinary urgency. With herreduced mobility she finds it difficult to reach a toilet in time and noticesurgency is particularly likely to come on as she rises from a sitting position.On questioning as to whether she empties her bladder, she answers notall the time, saying that she can often void again having just emptied herbladder 30 minutes before.
Using abdominal ultrasound, she is shown to have a postmicturitionresidual volume of 160 mL. She is therefore started on clean intermittentself-catheterization (CISC) and given oral long-acting tolterodine 4 mg oncea day. Taking this medication and using CISC twice a day, she stops havingepisodes of urgency incontinence and feels it safe to drink more liquids.
Comment. This womans case history illustrates the importance ofmeasuring the postmicturition residual volume if effective treatment is tobe achieved.
KEY POINT:
A If genuine
recurrent urinary
tract infections
do occur with theexpected clinical
symptoms of
dysuria and
change in color
and odor of
the urine,
investigations
should be carried
out to discover
if there is a nidus
for infection in
the urinary tract,
and a urologic
referral is
mandatory.
Hematuria is
another
indication
for prompt
urologic referral.
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/11/2019 Autonomic Disorders of the Urogenital System
6/17
antidiuretic hormone desmopressin.Its use in children to treat nocturnalenuresis is well established, and stud-
ies have also demonstrated its efficacyin women with MS and nighttimefrequency. It was shown to be effectiveif taken during the day in providingthe patients with a period up to 6hours during which they were nottroubled by urinary frequency and
were without any rebound nighttimefrequency (Hoverd and Fowler, 1998).However, patients must be cautionedto use desmopressin only once in 24hours despite the convenience of its
effect, and it should not be given tothose with dependent leg edemacaused by immobility who have night-time frequency. Nor should desmo-pressin be prescribed for patients overthe age of 65 years as there is a risk ofits inducing cardiac failure.
There is, however, a point in theprogression of MS where first-linetreatment may be insufficient to con-tain urinary symptoms and yet thepatient does not want to have a long-term indwelling catheter. This point indecline is often reached as the neuro-logic disability, particularly mobility, isdeteriorating and the patient there-fore is not in a robust state of health toundergo bladder augmentation sur-gery, such as a clam cystoplasty. A
very promising treatment that canthen be used at this stage is detrusorinjection of botulinum A toxin. Thediscovery that injection of botulinum
toxin A directly into the smoothmuscle of the detrusor resulted in asignificant alleviation of neurogenicbladder dysfunction (Schurch et al,2000) is having far-reaching conse-quences. Originally proposed on thebasis that botulinum toxin A wouldblock the presynaptic release of para-sympathetic acetylcholine-mediatingdetrusor contraction, the benefits ofthis treatment appear to exceed thoseexpected from an agent that merely
paralyzes the detrusor muscle. Itseems likely that botulinum toxin A isalso affecting the vesicular release
of neurotransmitters involved in theafferent arm of abnormal reflex blad-der contractions (Apostolidis et al,2006).
Many hundreds of patients world-wide have now been successfully treatedby injections of 200-mU to 300-mUbotulinum toxin A (Botox) injected in20 to 30 equally spaced points in thebladder wall. In our department we haveused a minimally invasive technique,performed in 20 minutes as a clinic
procedure under local anesthetic, totreat 43 patients with MS. All benefited,
with their voiding diaries showingremarkable improvements in the re-duction of urinary urgency, frequency,and incontinence. However, they thenall needed to perform CISC, eventhe 30% who had not been doingso prior to treatment. Fortunately, thisdid not appear to affect their qualityof life, which showed highly signifi-cant improvements, with the benefitlasting for a mean of 9.7 months. Cen-ters with the longest experience ofthis treatment have been able toshow that subsequent reinjections areas effective as the initial one andof comparable duration (Grosse et al,2005).
With further neurologic progression,there may become a stage when a long-term indwelling catheter becomes nec-essary. A suprapubic catheter is the
preferred management option. Thisshould be sited by a urologic surgeonwho may want the patient to have ageneral anesthetic so that the bladdercan be distended, facilitating the supra-pubic puncture into the otherwiseshrunken organ.
Sexual dysfunction.Prior to the ad-vent of the oral erectogenic medications,men with MS were successfully treated
with intracavernosal injection therapy(Kirkeby et al, 1988). Subsequently, a
170
KEY POINT:
A The discovery
that injection of
botulinum toxin
A directly intothe smooth
muscle of the
detrusor resulted
in a significant
alleviation of
neurogenic
bladder
dysfunction
is having
far-reaching
consequences.
"DISORDERS OF THE UROGENITAL SYSTEM
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/11/2019 Autonomic Disorders of the Urogenital System
7/17
multicenterplacebo-controlledtrialdem-onstrated an excellent response to sil-denafil citrate in men with MS (Fowler
et al, 2005). Although in that studyorgasmic capacity was also increased, afact that was attributed to the menbeing able to sustain an erection longer,it is known that a significant proportionof men continue to have difficulty withejaculation, for which, as yet, no effec-tive medication is available, although
yohimbine may be tried. Probably thebest recourse is to use a vibrating sexaid.
Following the success of sildenafil
citrate in the treatment of sexualfunction with men, a small placebo-controlled trial in women with sexualdysfunction and MS was carried out. Aquestionnaire was used to measuresexual response, and although there
was a significant improvement in lu-brication and some improvement insensation, there was no overall changein orgasmic response in the active-treatment group compared with thosein the placebo-treated group (Dasguptaet al, 2004). Although disappointing,this was not perhaps surprising.
The pharmaceutical industry con-tinues research to discover agents thatmight be effective in the treatment offemale sexual dysfunction, but despitethe current lack of specific treatment,
women with MS found the oppor-tunity to discuss their problem witha health care professional beneficial(Hulter and Lundberg, 1995).
MULTIPLE SYSTEM ATROPHY
Neurologic Basis ofUrogenital Symptoms
The explanation for the multiple typesof bladder dysfunction that can oc-cur in multiple system atrophy (MSA)probably reflects the neuronal atro-phy in the CNS that occurs at manydifferent sites involved in bladdercontrol (Kirby et al, 1986). It has been
proposed that cells situated in thedorsal tegmentum of the pons, possi-bly those of the PMC, are involved in
the atrophying process. It may be thattheir decline results in loss of in-hibition and thus DO. Involvement ofthe intermediolateral cell columns ofthe spinal cord, which convey thedescending sympathetic and parasym-pathetic innervation of the sacral re-gion, may account for the observedopen bladder neck and impairmentof bladder emptying. Neuronal atrophyof cells in the Onuf nucleus leads tochronic denervation of the striated
sphincters (Sakuta et al, 1978), bothanal and urethral. It is the combi-nation of DO, incomplete emptying,and sphincter weakness that accountsfor the early and severe incontinencethat so often characterizes the onsetof MSA.
Much less is known about theneuropathologic substrate of sexualdysfunction in MSA, but whereas ED
was formerly thought to be secondaryto hypotension, the dissociation ofthese disorders (Kirchhof et al, 2003)and the observation that erectile re-sponses can be restored in men withMSA and hypotension by treatment
with sildenafil citrate argue for adifferent pathophysiology. Erection isknown to result from stimulation ofdopamine receptors in the medialpreoptic area of the hypothalamus,and it has been hypothesized that EDcould result either from impairment
of sacral autonomic innervation orimpairment of dopaminergic-mediatedpathways in the CNS (Kirchhof et al,2003).
Clinical History
The earliest studies of MSA drew at-tention to the premonitory nature ofurogenital symptoms in the condition.The explanation for this remains tobe discovered, but after initial stud-ies that highlighted the fact that
171
KEY POINTS:
A The
pharmaceutical
industry
continuesresearch to
discover agents
that might be
effective in the
treatment of
female sexual
dysfunction,
but despite the
current lack of
specific
treatment,
women with
MS found that
the opportunity
to discuss their
problem with a
health care
professional
was beneficial.
A The explanation
for the multiple
types of bladder
dysfunction that
can occur in
multiple system
atrophy (MSA)
probably reflects
the neuronal
atrophy in the
CNS that occurs
at many different
sites involved in
bladder control.
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/11/2019 Autonomic Disorders of the Urogenital System
8/17
urogenital symptoms were early andalmost invariable in the disease (Becket al, 1994), recent studies have exam-
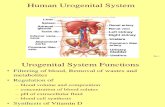
ined the chronology of evolution ofpostural hypotension compared withdisorders of bladder and sexual func-tion. It was clearly shown that, at onset,the incidence of urinary symptoms wasmore than twice that of orthostaticsymptoms (96% compared with 43%)and that no patients had orthostaticsymptoms only, but 53% had urinarysymptoms alone (Sakakibara et al,2000). There were 43% with both uri-nary and orthostatic symptoms, and
in 21% urinary symptoms appearedfirst (Figure 7-3).
A study that looked retrospectivelyat a group of 71 men with a diagnosisof probable MSA who had bladdercomplaints noted that ED was acomplaint in all men who were que-ried. The onset of ED had precededthe onset of bladder symptoms in 58%and the onset of orthostatic hypoten-sion symptoms in 91%. Bladder symp-toms also preceded symptoms oforthostatic hypotension in 76% ofpatients (Kirchhof et al, 2003).
Female sexual dysfunction in MSAhas been little studied, but a single pa-per reported that, when women with
MSA-parkinsonian type or Parkinsonsdisease and healthy controls werequestioned, 47% of the patients withMSA-parkinsonian type, but only 4% ofthe patients with Parkinsons diseaseand 4% of the control group, admittedto reduced genital sensitivity. Further-more, the appearance of this complaintin female patients with MSA showed aclose temporal relation to the onset ofthe disease (Oertel et al, 2003).
Erectile dysfunction is common in
the general population, and its inci-dence is known to increase with age.Likewise, bladder symptoms are alsocommon and often due to under-lying urologic disorders. However,the evidence points to the fact thaturogenital complaints are an early andalmost inevitable component of MSA,be it MSA-parkinsonian type or MSA-cerebellar type, and an absence ofthese symptoms makes the diagno-sis unlikely. Furthermore, urogenitalsymptoms may be valuable in distin-guishing cases of MSA from otherforms of parkinsonism and idiopathicParkinsons disease because in thoseconditions urogenital symptoms occurlate, often in the context of markedneurologic disability.
Clinical Presentation
Urinary incontinence or a fear of im-minent incontinence is the most com-
mon presenting bladder complaint,although other urinary symptoms mayprecede this (Kirby et al,1986; Sakakibaraet al, 2000). Although urinary symp-toms in either men or women are com-mon, the onset of incontinence in thepreceding 4 to 5 years, together withan appropriate neurologic profile, isan ominous portent for a diagnosis ofMSA. Detailed studies of patients us-ing videourodynamics, cystometry, andsphincter EMG (Kirby et al, 1986) have
172
FIGURE 7-3 Timing of urinary and orthostatic symptomsin patients with multiple system atrophy.
Sakakibara R, Hattori T, Uchiyama T, et al. Urinarydysfunction and orthostatic hypotension in multiplesystem atrophy: which is the more common and earliermanifestation? J Neurol Neurosurg Psychiatry2000;68(1):6569. Reprinted with permission fromBMJ Publishing Group Ltd.
KEY POINT:
A A recent study
has clearly shown
that, at onset,
the incidence ofurinary symptoms
was more than
twice that of
orthostatic
symptoms (96%
compared to 43%)
and that no
patients had
orthostatic
symptoms only,
but 53% had
urinary symptoms
alone.
"DISORDERS OF THE UROGENITAL SYSTEM
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/11/2019 Autonomic Disorders of the Urogenital System
9/17
shown that often a combination ofDO and sphincter weakness is pres-ent. The finding of an open bladder
neck, generally an unusual feature ina man, is quite specific in men withMSA. Occasionally a patient may pres-ent with complete urinary retention,but difficulty voiding is much morecommon and the likelihood of raisedpostmicturition residual volume seemsto increase as the disease progresses(Ito et al, 2006). A raised postmictu-rition residual volume is much morecommon in MSA than Parkinsons dis-ease and may even be of diagnostic
value in the differential diagnosis of thetwo conditions (Hahn and Ebersbach,2005).
Management
Some while ago men with MSA andincontinence were often consideredfor prostatectomy, but in recent yearsthis seems to be occurring less often,presumably due to urologists increas-ing awareness of MSA and the more
widespread use of pressure-flow stud-ies to demonstrate obstructed outflow
before surgery. Men with MSA whohave had transurethral prostatectomyseldom report that surgery improves
their bladder symptoms.Preferably, urologic surgery shouldbe avoided, using instead medicalmeans to manage incontinence orincomplete bladder emptying. Themanagement algorithm outlined inFigure 7-2 has also proved highlyeffective in patients with MSA, andmany who had been incontinent at anearly stage of the disease manage tomaintain continence until they becomeseverely disabled (Beck et al, 1994),
when a suprapubic indwelling catheteris the preferred option. Synthetic anti-diuretic hormone (desmopressin) canbe highly effective in reducing night-time frequency and may also have abeneficial effect on postural hypoten-sion (Case 7-2).
In some patients detrusor overactiv-ity predominates and does not re-spond adequately to anticholinergics.It will be interesting to see if the re-cently introduced intervention of de-trusor injections of botulinum toxin(Schurch et al, 2000) proves to have
173
Case 7-2A 57-year-old man was first seen by a urologist 3 years ago, and althoughno urologic abnormality could be found, he was demonstrated on anumber of occasions not to be emptying his bladder fully. He was startedon long-acting tolterodine 4 mg daily and shown how to do CISC. Hehad been taking sildenafil for ED for 5 years.
Two years ago a neurologist made a diagnosis of parkinsonism, and1 year ago a diagnosis of MSA was made on clinical grounds based on hisneurologic deterioration. He was complaining then that his incontinence,particularly at night, was very distressing, so he was advised to do CISCbefore going to bed and to use desmopressin spray at night. When nextseen, he was no longer experiencing nocturnal enuresis and with CISCat eight hourly intervals, his bladder control during the day had greatlyimproved. However, at his most recent examination he was noted to havedeveloped hypophonic slurring dysarthria, akinesia, and rigidity.
Comment.The bladder symptoms of MSA can be significantly alleviatedby appropriate treatment despite continuing deterioration of theunderlying neurologic condition.
A Although urinary
symptoms in
either men or
women are
common, the
onset of
incontinence in
the preceding 4
to 5 years,
together with an
appropriate
neurologic
profile, is an
ominous portent
for a diagnosis
of MSA.
A Men with MSA
who have had
transurethral
prostatectomy
seldom report
that surgery
improves
their bladder
symptoms.
KEY POINTS:
A The evidence
points to the fact
that urogenital
complaints are anearly and almost
inevitable
component of
MSA, be it MSA-
parkinsonian type
or MSA-
cerebellar type,
and an absence
of these
symptoms makes
the diagnosis
unlikely.
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/11/2019 Autonomic Disorders of the Urogenital System
10/17
a role in the management of thesepatients.
The majority of men in the general
population with ED are successfullytreated by oral phosphodiesterase in-hibitors, but a small study of six men
with MSA showed that, in those withpreexisting postural hypotension, sil-denafil citrate exacerbated the bloodpressure fall to a potentially dangerousdegree, whereas those without pos-tural hypotension did not showchanges (Hussain et al, 2001). Fromthis, the recommendation has beenmade that lying and standing blood
pressure should be checked in menwith parkinsonism before prescrib-ing oral phosphodiesterase inhibitors.Furthermore, it would seem prefer-able to use the shorter-acting phospho-diesterase inhibitors such as silden-afil or vardenafil rather than thepopular tadalafil, with its half-life of18 hours.
URINARY RETENTION IN
YOUNG WOMEN(FOWLERS SYNDROME)
Neurologic Basis
Until the latter part of the 20th cen-tury, urinary retention in women wascommonly considered to be psycho-genic. Urologic or gynecologic causesof retention are rare and can be ex-cluded by cystoscopy, leaving a signifi-cant number of women in whomretention is said to have a functional
basis. Past teaching was that urinaryretention was either the presentingsymptom of MS or that it was due tohysteria. However, in 1985 thisauthor recorded an unusual type ofEMG activity from the striated urethralsphincter using a concentric needleelectrode in a series of young women
with urinary retention. The EMG activ-ity consisted of complex repetitivedischarges and a myotonic-like sound-ing component, decelerating bursts,
which was proposed to indicate im-paired urethral relaxation. Detailed anal-
ysis of the EMG activity using single-
fiber electrode techniques showed thatthe jitter of the constituent complexeswas so low that the activity was theresult of ephaptic transmission of im-pulses between muscle fibers. A pro-portion of these young women alsohad a history or clinical features ofpolycystic ovaries (Fowler et al, 1988).It was hypothesized that the hor-monally sensitive striated sphincterhad developed a local muscle mem-brane instability, allowing direct spread
of excitatory impulses and, thus, theinappropriate and involuntary sustainedcontraction of the sphincter (Fowlerand Dasgupta, 2002). In the last 20 years,this condition has been increasinglyreferred to asFowlers syndrome.
In a group of somewhat olderwomen with urinary retention whootherwise have the characteristic fea-tures of Fowlers syndrome, altera-tions of cardiovascular autonomicfunction were discovered. It was thenproposed that the condition is due toan occult dysautonomia (Amarencoet al, 2006). In the authors experi-ence, however, if all possible urologicor neurologic disorders are eliminatedand an abnormally high urethral pres-sure is demonstrated (see below), thecondition does not evolve but remainsan isolated disorder of voiding, benignthough highly inconvenient.
A retrospective study of 247 women
with urinary retention referred to uro-neurology at Queen Square over a4-year period showed that Fowlerssyndrome was the most commondiagnosis, accounting for 58%. Nodiagnosis to explain the urinary reten-tion could be made in 32% of the
women, but in only two of that largeseries of women was urinary retentionthe presenting symptom of a neuro-logic disease (Kavia et al, 2006). Ifurinary retention is due to either
174
KEY POINTS:
A The
recommendation
has been made
that lying andstanding blood
pressure should
be checked in
men with
parkinsonism
before
prescribing oral
phosphodiesterase
inhibitors.
A Urologic or
gynecologic
causes ofretention are
rare and can
be excluded by
cystoscopy,
leaving a
significant
number of
women in
whom retention
is said to have
a functional
basis.
A It was
hypothesized
that the
hormonally
sensitive striated
sphincter had
developed a local
muscle
membrane
instability,
allowing direct
spread of
excitatory
impulses and,
thus, the
inappropriate
and involuntary
sustained
contraction of
the sphincter.
"DISORDERS OF THE UROGENITAL SYSTEM
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/11/2019 Autonomic Disorders of the Urogenital System
11/17
central or peripheral nervous systemdisease, neurologic features with ab-normalities on imaging and CSF exam-
ination are almost invariably presentand often prominent (Sakakibara et al,2006). This is not the case in Fowlerssyndrome.
Clinical Presentation
A retrospective questionnaire surveyof 91 women with Fowlers syndromeshowed that the common clinicalfeatures are painless urinary retention,
with a demonstrated bladder capacityat some stage of the history in excess
of 1 L and difficulty in removingcatheters used for self-catheterization(Swinn et al, 2002). Abdominal strain-ing does not help voiding. A strikingaspect of these womens history is anabsence of the sense of bladderfullness that would be expected withsuch large bladder capacities andgeneral decrease in bladder sensation.
Animal studies indicate that contrac-tion of the striated sphincter has aninhibitory effect on detrusor contrac-tion and on bladder afferent activity(de Groat et al, 2001), and theactivation of comparable neural path-
ways in these women could accountfor the observed clinical features.
In many of the patients a clinicalincident, such as a surgical procedureunder general anesthesia, a urinarytract infection, or childbirth, may havetriggered the onset of retention. In
younger women in particular, the
onset is often apparently spontaneous(Swinn et al, 2002). Sometimes afteracute catheterization voiding abilitymay recover, but retention then recurssome months or even years later. A
young woman with retention mayadmit on direct questioning to havinghad an interrupted urinary stream formany years, although this was unrec-ognized as being abnormal, or recur-rent urinary tract infections, probablyresulting from incomplete emptying.
Intermittent self-catheterization is un-doubtedly more difficult for these
young women than for women with
MS, and it is not uncommon for themto describe difficulty with removingthe catheter, as if something is grip-ping it as it is withdrawn. This isthought to be due to contraction ofthe normally innervated but patholog-ically overactive striated sphincteraround the catheter.
Although the syndrome was origi-nally described on the basis of needleEMG of the striated urethral sphincter(the abnormality is not found in the
anal sphincter), urethral sphincterEMG is not an easy test to perform,and despite the use of local anes-thetic, it is uncomfortable for thepatient. Furthermore, although EMGsampling gives some indication as to
whether or not the abnormality ispresent, the result gives no quanti-tative estimate of dysfunction, unlikethe urethral pressure profile. Usinga pull-through catheter, urethralpressure can be measured at rest withthe expected value derived from thefollowing equation: expected value(cm H2O) = 92 age (in years).
Women with Fowlers syndromecommonly have values in excess of100 cm H2O (Kavia et al, 2006). The
volume of the sphincter muscle esti-mated by a vaginal ultrasound probemay show enlargement, so if there is atypical history and both the urethralpressure profile and the sphincter
volume are abnormally raised, EMGis now less commonly required toconfirm the diagnosis (Kavia et al,2006).
Management
The mainstay of management is CISC,but many women find this uncomfort-able; it is not unusual for a suprapubiccatheter to be required. Psychologi-cally, the prospect of indefinite self-catheterization for a young woman
175
KEY POINTS:
A A retrospective
study of 247
women with
urinary retentionreferred to
uro-neurology at
Queen Square
over a 4-year
period showed
that Fowlers
syndrome was
the most
common
diagnosis,
accounting
for 58%.
A The common
clinical features
of Fowlers
syndrome are
painless urinary
retention with a
demonstrated
bladder capacity
at some stage
of the history
in excess of 1 L
and difficulty
in removing
catheters used
for self-
catheterization.
A Intermittent self-
catheterization
is undoubtedly
more difficult
for young
women with
Fowlers
syndrome than
for women with
MS, and it is not
uncommon for
them to describe
difficulty with
removing the
catheter, as if
something is
gripping it as
it is withdrawn.
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/11/2019 Autonomic Disorders of the Urogenital System
12/17
is understandably distressing. The onlyintervention that has been found torestore voiding is sacral nerve stimu-
lation (SNS), also called sacral neuro-modulation (Swinn et al, 2002). Thisinvolves inserting a unilateral stimu-lating lead into the presacral plexusthrough the third sacral foramenand connecting it to an external bat-tery with its settings adjusted so thatthe patient senses pelvic sensations.The stimulation is then set to sub-threshold intensity so that the sub-
ject rapidly adapts to the continuousstimuli.
Exactly the same intervention is
used to treat intractable urinary fre-quency and urgency, and the paradoxof the same treatment being used totreat clinically opposite conditions isprobably best understood by consider-ing the underlying pathophysiologyof each disorder: in overactive blad-der conditions it seems likely the sti-mulation of afferents is having aninhibitory effect, whereas in Fowlers
176
Case 7-3A 37-year-old nurse was first seen at age 22 after she had undergonean ear, nose, and throat procedure under general anesthetic. Followingthis she was unable to urinate. She had some feeling of pressure whenher bladder was full but had lost normal sensation. In addition, shewas complaining of vague sensory symptoms in her left leg. Clinicalexamination was essentially normal except for some inconsistent sensorydisturbance on the left. However, neurologic investigations, includinga myelogram, MRI of the brain, and visual evoked potentials, were normal.A neurologist suggested her urinary retention might have been ofpsychogenic origin.
A year later, urethral sphincter EMG was highly abnormal. Profusecomplex repetitive discharges and decelerating bursts were recorded,consistent with the diagnosis of Fowlers syndrome.
She remained in complete urinary retention and for 7 years managedto empty her bladder by intermittent self-catheterization. This did notprevent her from working full time, and she spent 1 year backpackingin the Far East. Then 8 years ago an SNS was implanted, and although shepassed urine postoperatively, within 24 hours she developed symptomsand signs of an infection at the stimulator site. The stimulator had tobe removed, and the infective microorganism was the nosocomialmultiresistantStaphylococcus aureus. She was required to avoid contactwith patients and was off work for many months. She remained reluctantto consider a repeat attempt at SNS and continued with intermittentself-catheterization for another 6 years until she accepted the offer ofa stimulator implant using the new 2-stage technique. Fortunately,this was successful, and she was able to urinate spontaneously for the firsttime in 15 years. She no longer needs to self-catheterize.
Comment.The young woman was initially the victim of then prevailingmedical prejudice some 20 years ago, which asserted urinary retentionin women was commonly psychogenic. It is particularly importantthat neurologists are aware of this condition because urologists often referthese patients when their investigations fail to reveal an abnormality.If the diagnosis is recognized, sacral neuromodulation can restorevoiding ability.
KEY POINT:
A The only
intervention
which has been
found to restorevoiding is
sacral nerve
stimulation,
also called sacral
neuromodulation.
"DISORDERS OF THE UROGENITAL SYSTEM
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/11/2019 Autonomic Disorders of the Urogenital System
13/17
-
8/11/2019 Autonomic Disorders of the Urogenital System
14/17
" Betts CD, DMellow MT, Fowler CJ. Urinary symptoms and the neurologicalfeatures of bladder dysfunction in multiple sclerosis. J Neurol NeurosurgPsychiatry 1993;56(3):245250.
Clinical study that showed a clear association between the extent of spinal cord
dysfunction and urinary symptoms in multiple sclerosis (MS).
" Betts CD, Jones SJ, Fowler CG, Fowler CJ. Erectile dysfunction in multiplesclerosis. Associated neurological and neurophysiological deficits, andtreatment of the condition. Brain 1994;117(pt 6):13031310.
The neurologic context of erectile dysfunction in MS.
" Borello-France D, Leng W, OLeary M, et al. Bladder and sexual functionamong women with multiple sclerosis. Mult Scler 2004;10(4):455461.
Women mildly affected by MS are still mostly able to enjoy sexual intercourse.
" Dasgupta R, Critchley HD, Dolan RJ. Fowler CJ. Changes in brain activityfollowing sacral neuromodulation for urinary retention. J Urol2005;174(6):22682272.
A PET study of women examining the central mechanisms of response to sacral
neuromodulation.
" DasGupta R, Fowler CJ. Urodynamic study of women in urinary retentiontreated with sacral neuromodulation. J Urol 2004;171(3):11611164.
Sacral neuromodulation in urinary retention does not work by reversing the sphincter
abnormality.
" Dasgupta R, Wiseman OJ, Kanabar G, et al. Efficacy of sildenafil in thetreatment of female sexual dysfunction due to multiple sclerosis. J Urol2004;171(3):11891193.
Sildenafil citrate had little effect on sexual function in women with MSaplacebo-controlled trial.
" Datta SN, Kavia RB, Gonzales G, Fowler CJ. Results of double-blindplacebo-controlled crossover study of sildenafil citrate (Viagra) in womensuffering from obstructed voiding or retention associated with theprimary disorder of sphincter relaxation (Fowlers Syndrome). Eur Urol2007;51(2):489497.
Sphincter relaxation, which is under nitric oxide control, did not improve with
sildenafil citrate in women with voiding dysfunction.
" de Groat W, Kawatani T, Hisamitsu T, et al. Mechanisms underlying therecovery of urinary bladder function following spinal cord injury. J Auton
Nerv Syst 1990;30(suppl):7177.An important basic science paper that showed the emergence of an unmyelinated
fiber reflex causes detrusor overactivity following spinal injury.
" de Groat WC, Fraser MO, Yoshiyama M, et al. Neural control of the urethra.Scand J Urol Nephrol Suppl 2001;35(207):3543.
Review of the experimental evidence showing the effect of sphincter contraction on
detrusor activity.
178
"DISORDERS OF THE UROGENITAL SYSTEM
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/11/2019 Autonomic Disorders of the Urogenital System
15/17
" De Ridder D, Ost D, Bruyninckx F. The presence of Fowlers syndromepredicts successful long-term outcome of sacral nerve stimulationin women with urinary retention. Eur Urol 2007;51(1):229233.
A study that shows that among all women with retention treated with sacral
neuromodulation, those with Fowlers syndrome do better in the long term.
" Fowler CJ. Investigation of the neurogenic bladder. J Neurol NeurosurgPsychiatry 1996;60(1):613.
A review stressing the importance of measurement of the postvoid residual volume in
the management of neurogenic incontinence.
" Fowler CJ, Christmas TJ, Chapple CR, et al. Abnormal electromyographicactivity of the urethral sphincter, voiding dysfunction, and polycysticovaries: a new syndrome? BMJ 1988;297(6661):14361438.
The original proposal of Fowlers syndrome.
" Fowler CJ, Dasgupta R. Electromyography in urinary retention andobstructed voiding in women. Scand J Urol Nephrol Suppl 2002;(210):5558.
A review explaining more recent thinking about the pathophysiology of urinary
retention in women with Fowlers syndrome.
" Fowler CJ, Miller JR, Sharief MK, et al. A double blind, randomised studyof sildenafil citrate for erectile dysfunction in men with multiple sclerosis.J Neurol Neurosurg Psychiatry 2005;76(5):700705.
Sildenafil citrate was highly effective in treating erectile dysfunction in men with
MSplacebo-controlled trial.
" Grosse J, Kramer G, Stohrer M. Success of repeat detrusor injections of
botulinum a toxin in patients with severe neurogenic detrusoroveractivity and incontinence. Eur Urol 2005;47(5):653659.
The first paper to review the long-term benefits of repeated injections of botulinum
toxin.
" Hahn K, Ebersbach G. Sonographic assessment of urinary retention inmultiple system atrophy and idiopathic Parkinsons disease. Mov Disord2005;20(11):14991502.
Raised postmicturition residual volume may have diagnostic value for the diagnosis of
MSA.
" Hoverd PA, Fowler CJ. Desmopressin in the treatment of daytime urinaryfrequency in patients with multiple sclerosis. J Neurol Neurosurg
Psychiatry 1998;65(5):778780.Desmopressin in patients with MS taken during the day did not result in rebound
nighttime frequency.
" Hulter BM, Lundberg PO. Sexual function in women with advancedmultiple sclerosis. J Neurol Neurosurg Psychiatry 1995;59(1):8386.
An important early study of sexual dysfunction in women with MS.
179
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/11/2019 Autonomic Disorders of the Urogenital System
16/17
" Hussain IF, Brady CM, Swinn MJ, et al. Treatment of erectile dysfunctionwith sildenafil citrate (Viagra) in parkinsonism due to Parkinsons diseaseor multiple system atrophy with observations on orthostatic hypotension.J Neurol Neurosurg Psychiatry 2001;71(3):371374.
Small placebo-controlled study that stressed the importance of measuring blood
pressure in patients with parkinsonism before prescribing sildenafil citrate.
" Ito T, Sakakibara R, Yasuda K, et al. Incomplete emptying and urinaryretention in multiple-system atrophy: when does it occur and how do wemanage it? Mov Disord 2006;21(6):816823.
Repeated measures of postvoid residual volume show that this increased with the
progression of MSA.
" Kavia RB, Datta SN, Dasgupta R, et al. Urinary retention in women: itscauses and management. BJU Int 2006;97(2):281287.
Outcome of investigation of management of a large number of women with urinary
retention referred to a UK tertiary center.
" Kirby R, Fowler C, Gosling J, Bannister R. Urethro-vesical dysfunction inprogressive autonomic failure with multiple system atrophy. J NeurolNeurosurg Psychiatry 1986;49(5):554562.
Early study highlighting the many different types of bladder dysfunction that can occur
in MSA.
" Kirchhof K, Apostolidis AN, Mathias CJ, Fowler CJ. Erectile and urinarydysfunction may be the presenting features in patients with multiplesystem atrophy: a retrospective study. Int J Impot Res 2003;15(4):293298.
A retrospective study.
" Kirkeby HJ, Poulsen EU, Petersen T, Drup J. Erectile dysfunction inmultiple sclerosis. Neurology 1988;38(9):13661371.
Before the advent of sildenafil citrate men with erectile dysfunction and MS were
successfully treated with intracavernosal injections.
" Oertel WH, Wachter T, Quinn NP, et al. Reduced genital sensitivity in femalepatients with multiple system atrophy of parkinsonian type. Mov Disord2003;18(4):430432.
The only report of female sexual dysfunction in MSA.
" Sakakibara R, Hattori T, Uchiyama T, et al. Urinary dysfunction andorthostatic hypotension in multiple system atrophy: which is the morecommon and earlier manifestation? J Neurol Neurosurg Psychiatry
2000;68(1):6569.An important study that shows urinary dysfunction occurs earlier than orthostatic
hypotension in MSA.
" Sakakibara R, Yamanishi T, Uchiyama T, Hattori T. Acute urinary retentiondue to benign inflammatory nervous diseases. J Neurol 2006;253(8):11031110.
A helpful review of the central and peripheral neurologic causes of urinary retention and
the associated neurologic features.
180
"DISORDERS OF THE UROGENITAL SYSTEM
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/11/2019 Autonomic Disorders of the Urogenital System
17/17
" Sakuta M, Nakanishi T, Toyokura Y. Anal muscle electromyograms differin amyotrophic lateral sclerosis and Shy-Drager syndrome. Neurology1978;28(12):12891293.
Remarkably early study giving the basis for sphincter EMG in the diagnosis of MSA.
" Schurch B, Stohrer M, Kramer G, et al. Botulinum-A toxin for treatingdetrusor hyperreflexia in spinal cord injured patients: a new alternativeto anticholinergic drugs? Preliminary results. J Urol 2000;164(3 pt 1):692697.
Much-cited paper, the first report of the benefits of botulinum toxin A treatment for
intractable detrusor overactivity.
" Sirls LT, Zimmern PE, Leach GE. Role of limited evaluation and aggressivemedical management in multiple sclerosis: a review of 113 patients. J Urol1994;151(4):946950.
Postvoid residual volume measurement only, the recommended management in
patients with MS.
" Swinn MJ, Wiseman OJ, Lowe E, Fowler CJ. The cause and natural historyof isolated urinary retention in young women. J Urol 2002;167(1):151156.
A retrospective review of women with Fowlers syndrome, which defined the
clinical history.
" Zorzon M, Zivadinov R, Bosco A, et al. Sexual dysfunction in multiplesclerosis: a case-control study. I. Frequency and comparison of groups.Mult Scler 1999;5(6):418427.
Clinical features of patients with sexual dysfunction due to MS.
181