Refrigeration Dryer Manuel d’utilisation ASD 10 ASD 15 ASD ...

11/29/2019
1
Autism Spectrum DisorderLifespan perspectives on identification, diagnosis, and
behavioural / mental health
Isabel M. Smith PhDJoan & Jack Craig Chair in Autism Research
Department of Pediatrics
1
29 November 2019
No conflicts of interest to declare.
2

11/29/2019
2
Participants will demonstrate increased ability to 1. Recognize signs of ASD in children & youth and refer appropriately for
diagnostic assessment
2. Identify common behavioural and mental health problems in ASD and evidence-based approaches to care
3. Support the transitions of youth with ASD from pediatric to adult health care
Objectives
3
1. Overview of autism spectrum disorder -- current conceptualization
2. Developmental approach to recognizing signs / symptoms
3. Common differential diagnoses / co-morbid conditions
4. Evidence-based approaches to care for common behavioural and mental health problems in ASD
5. Issues relevant to the transition to adult health care
Plan
4

11/29/2019
3
ASD Position StatementsCanadian Pediatric Society Task Force (2019)
1. Early detection of ASD in young children
2. Standards of diagnostic assessment for ASD
3. Post-diagnostic management and follow-up care for ASD
5
Zwaigenbaum et al. (2019)
Brian et al. (2019)
Yip et al. (2019)
https://www.cps.ca/en/documents/tag/autism
Autism Spectrum Disorder
Two core domains• Social-communication behaviour differences
• Restricted / repetitive / inflexible patterns of thinking / behaviour
6

11/29/2019
4
Heterogeneity in ASD• Manifestation of symptoms (mild severe)o Social-communicationo Restricted & repetitive behaviour
• Level of function (less more impaired)o intellectual abilityo language abilityo adaptive behaviour
• Co-existing medical & mental health conditions• Presentation varies with development
7
Spectrum is Multidimensional
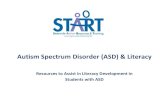
• Canadian multi-site study, Pathways in ASD• Longitudinal cohort study
• Examine, e.g., developmental trajectories of ASD symptoms and adaptive functioning, age 3 to 7 years
8
Szatmari et al. (2015)

11/29/2019
5
0
1
2
3
4
5
6
7
8
9
10
40 45 50 55 60 65 70 75 80
ADOS Severity M
etric
age (months)
Symptom SeverityGroup 1 (11%: low & improving) Group 2 (89%: high & stable)
9Szatmari et al. (2015)
50
60
70
80
90
100
110
40 45 50 55 60 65 70 75 80
VABS II Adap
tive Composite
age (months)
Adaptive FunctioningGroup 1 (29%: low & declining)
Group 2 (49%: medium & slightly improving)
Group 3 (21 %: high & improving)
10Szatmari et al. (2015)

11/29/2019
6
• Symptom severity• Large majority (89%) – ASD symptoms are high & stable• Remainder milder ASD symptoms, improving
• Adaptive functioning• Most (49%) – moderate adaptive functioning, slightly improving• Nearly a third (29%) – lower functioning, declining• Remainder (21%) - higher functioning, improving
11Szatmari et al. (2015)
• Social interaction & communication differences (all 3)• Social – emotional reciprocity• Nonverbal behaviour• Developing / maintaining relationships
• Restricted, repetitive behaviour / interests / activities (2 of 4)• Stereotyped behaviour / speech• Insistence on sameness / resistance to change• Limited / intense interests• Unusual (hypo- / hyper-) reactions to sensations
DSM-5 Criteria APA (2013)
12

11/29/2019
7
• Age of first concern• + / - loss of established skills (i.e., regression)• + / - accompanying intellectual impairment• + / - accompanying structural language impairment• Associated with a known medical or genetic condition or
environmental factor• Associated with another neurodevelopmental, mental, or behavioral
disorder
DSM-5 ASD Specifiers
13
ASD Specifiers - Severity Social Communication Impairment (level 1, 2, or 3)
Restricted interests/Repetitive Behaviors (level 1, 2, or 3)
For each:Level 1 – ‘requiring support’
Level 2 – ‘requiring substantial support’
Level 3 – ‘requiring very substantial support’
14

11/29/2019
8
ASD Epidemiology• Prevalence
• At least 1% worldwide (Fombonne, 2009, Elsabbagh et al., 2012)
• 1 in 66 in Canadian children & youth (1.5%) (PHAC, 2018)
• Is it increasing?• US data suggest yes (CDC, various years) -- but UK data more stable
(Taylor et al., 2013)
• If increasing, why?• Issues of definition / diagnosis as well as etiology
15
Increased rate of diagnosis -- combined effects of
• broadening of diagnostic concepts
• lay and professional awareness of ASD, reduced stigma?• e.g., in very young and / or more able individuals
• service availability
• ‘diagnostic switching’ from other developmental disabilities to ASD• 14 recent population-based studies: 30% - 85% had IQ in average range (historically,
15 to 30%)
16
ASD Epidemiology cont’d

11/29/2019
9
17
U.S. students receiving special education services – Autism vs ID classification Figure adapted by Thurm et al. (2019)
‘Diagnostic switching’
• Social interaction & communication differences (all 3)• Social – emotional reciprocity• Nonverbal behaviour• Developing / maintaining relationships
• Restricted, repetitive behaviour / interests / activities (2 of 4)• Stereotyped behaviour / speech• Insistence on sameness / resistance to change• Limited / intense interests• Unusual (hypo- / hyper-) reactions to sensations
Recognizing ASD – Developmental approach
18

11/29/2019
10
Early Detection of ASDSurveillance for all; closer monitoring of infants at elevated risk • Genetic syndromes• Prenatal factors
• Older parents (35+)• Maternal health problems (obesity, diabetes, hypertension, infections in
pregnancy)• Closely spaced pregnancies
• Low birth weight, extreme prematurity
19
Early Detection of ASDGenetic risk• Canadian Infant Sibling Study Bryson, Zwaigenbaum, et al.
• Autism Observation Scale for Infants Bryson et al. (2000, 2008) - measure of early signs, used in research world-wide
• Recurrence risk in families – 20% in research cohorts Ozonoff et al. (2011)
7% in population studies Grønborg et al. (2013)
20

11/29/2019
11
Signs of ASD in Infants & Toddlers• Early (6 to 12 months)• Recognizable ASD symptoms generally not present
• ASD prodrome -- non-specific signs• EITHER marked passivity OR irritability / reactivity• delayed motor skills• feeding and/or sleeping problems
21
Signs of ASD in Infants & Toddlers• Later (12 to 24 months)• Emerging ASD symptoms more easily recognizedSocial interaction & communication differences:
• orienting to name• eye contact & social referencing• social interest / smiles / joyful play• babbling• gestures• words -- if present, not used socially
22

11/29/2019
12
Videos removed
23
• Emerging restricted, repetitive behaviour / interests / activities
• unusual / intense exploration / examination (tactile, visual)
• repetitive activities with objects
• stereotyped movements (beyond “overflow” seen with excitement)
Signs of ASD in Infants & Toddlers
24

11/29/2019
13
• Parents’ concerns
• Take concerns seriously – but do weigh parental experiences (e.g., other child with ASD?)
• Regression – loss of skills or failure to progress
• Screen when parent or other informant is concerned• Modified Checklist for Autism in Toddlers – Revised with Follow-up
Emerging ASD in Infants & Toddlers
25
https://mchatscreen.com/
ASD in preschoolers• By age 3, symptoms of ASD are recognizable in many -- not all
• ‘Classic’ autism seldom missed – e.g.• Socially aloof / unaware of people• No speech / only echolalic speech • Uses your hand to open / turn on • Stereotyped / repetitive movements
• But presentation is highly variable
26

11/29/2019
14
ASD in preschoolersSocial – Communication• Speech / language may be delayed – in verbal children consider atypical
communicative use of language • Reciprocity – chat / conversation versus monologue• ‘Scripting’ versus spontaneous speech
• Non-verbal communication limited• Little use of gestures, e.g., pointing to draw attention• Limited / unusual gaze & facial expressions
• Poor coordination of verbal & nonverbal
27
ASD in preschoolersRestricted, repetitive inflexible behaviour• Reduced variety of play activities + / - intense and/or unusual interests
• Intense preoccupation with specific toy / topic• ‘Pretending’ may be absent / superficial
• Overly specific routines / upset with changes
• Atypical reactions to sensations – strong interests or aversions (visual, touch, taste, smell)
• Impairment / interference • Does family take extraordinary measures to accommodate the behaviour?
28

11/29/2019
15
Preschool Differential Dx/ Co-morbidity• Global developmental delay (GDD)
• Is social, communication, play behaviour congruent with developmental level?
• e.g., joint attention, gestures, words, pretend play emerge 12 – 18 months
• Are behavioural features present that are atypical at any age?• e.g., atypical movements, sensory fascinations or aversions
• What domains are involved?• e.g., only expressive language delays, nonverbal communication unaffected
29
Preschool Differential Dx/ Co-morbidity• Developmental language disorders
• Assess nonverbal communication, social behaviour, other aspects of adaptive behaviour
• Are behavioural features present that are atypical at any age?• e.g., atypical movements, sensory fascinations or aversions
30

11/29/2019
16
Preschool Differential Dx/ Co-morbidity• ADHD
• Over-activity or impulsivity may affect skill acquisition but not social motivation
• Does communication integrate verbal (talking) and nonverbal (looking, gesturing) means? Is reciprocity evident?
• Although attention may be fleeting, are age-typical social and play interests evident?
31
• Inhibited / anxious temperament• ‘Sticky’ / rigid behaviour may be seen; any other evidence of repetitive, unusual
play / behaviour?
• Complicates in-office observations; seek corroboration of parent concerns if possible
• e.g., preschool educator
• Some preschool girls on pathway to ASD -- social inhibition, rigidity, but less disordered play (may show some pretend play) – warrants monitoring
Preschool Differential Dx/ Co-morbidity
32

11/29/2019
17
ASD in Early School Years• Some children with ASD evade detection until school• Usually, those with without marked language or cognitive difficulties
• Parents may have been unconcerned• More subtle ASD symptoms• Little experience with peers• Other conditions, notably ADHD, may have masked ASD features
• Social, emotional, flexibility demands increase at school• Contrasts with peers’ skills / peer interaction problems become
more evident
33
ASD in Girls (& Women)
• ASD probably under-diagnosed (especially in those without ID)
• Play may appear less atypical / less RRB in young girls with ASDe.g., Duvecote et al. (2016)
• Social ‘camouflage’ may be more successful Dean et al. (2016)
• Later diagnoses are common especially for those without ID
34
Halliday et al. (2015)Kreiser & White (2014)

11/29/2019
18
Differential Dx/ Co-morbidity in School-aged Children• Shift in main differential diagnoses under consideration• Intellectual disability (ID), with or without ASD, usually
identified prior to school• Referrals often for very complex presentations• Often, history of involvement with health and mental health
services• Often, multiple diagnoses considered and/or given
35
Differential Dx/ Co-morbidity in School-aged Children• Much recent interest in boundaries and overlaps among NDDs,
especially between ASD and ADHD• Core domains of impairment are distinct, but …• Structured observations by clinicians may better distinguish
ASD from ADHD symptoms than parent interview• ASD rating scale scores elevated for children with high levels
of behavioural / emotional problems
36
Grzadzinski et al (2016)
e.g., Hus et al (2013)

11/29/2019
19
Differential Dx/ Co-morbidityin School-aged Children• Children with ADHD (& other NDDs) often experience peer interaction
problems• Not associated with poor early fundamental social-communication skills (use of gaze,
facial expressions, quality of social initiations and reciprocity)
• Social behaviour may become more atypical over time• Lack of typical peer interactions, experience• May reduce frequency / quality of reciprocal social interactions
• Not associated with stereotyped, repetitive, inflexible, unusual play and interests
• But -- intense interests may be evident in age-typical activities such as video games
37
Grzadzinski et al (2016)
ASD in Older Children / Adolescents• When ASD is being considered, look to the developmental history
(late preschool, first school years)
• Quality of any behavioural, social concerns?
• Note peer relationships in particular
• Challenging when reliable informants are lacking
38

11/29/2019
20
ASD in Older Children / Adolescents• When ASD is being considered for the first time in older youth,
presentation is usually very complex• Differential diagnosis or co-existing condition?
• ADHD• OCD / Tics / Tourette’s• Early attachment disorder, trauma• Anxiety• Mood disorder• Emerging psychotic illness
39
• Multidisciplinary ax often needed• Depending on history and symptoms, may be primarily behavioural /
mental health or neuropsychological focus
• Coordination needed among family, healthcare providers, school teams, and often social / community services
Complex Presentations
40

11/29/2019
21
Referral for ASD Diagnostic Assessment• Nova Scotia:
• IWK Autism Team (up to age 19)• Children’s MH team in each NSHA zone (preschoolers; capacity for ax of older children
varies)
• Include in referral • Parental concerns (development, behaviour)• Other professionals’ concerns; results of any previous assessments• Risk factors, developmental history• Medical history / results of investigations / conditions confirmed or ruled out• Your own observations – ASD symptoms, other relevant behaviour
41
ASD Diagnostic Assessment• Requires systematic means of
• Eliciting symptoms / behaviour in both domains: social – communication and restricted repetitive behaviour
• Gathering relevant developmental history, ideally from primary caregiver
via
• Observation / interaction protocol (e.g., Autism Diagnostic Interview Schedule)
• Caregiver interviews (structured or semi-structured)+ / - Other caregiver reports (questionnaires, rating scales)
• Collateral information• Interviews, rating forms, reports from other informants (e.g., preschool / school
teachers, other clinicians)42

11/29/2019
22
• Preschoolers are eligible for behavioural intervention programs --EIBI (NS), Preschool Autism Services (NB), IBI (PEI)
• Wait for public EIBI can be very long in NS (depends on age at diagnosis) but short in NB, intermediate in PEI
• In NS, families often already connected with S-LP services (integrated with NS EIBI), perhaps also NSECDIS
After a Diagnosis of ASD
43
CPS ASD Position StatementPost-diagnostic management and follow-up care for ASD
• Support child / parent / family quality of life• Knowledge of local resources – not all communities are equal• Individualization• Routine health care / developmental monitoring• Manage / refer for co-existing conditions (health & behavioural
mental health)
44
Yip et al. (2019)

11/29/2019
23
Ongoing Care for Children / Youth with ASDAssessment & Management / Referral• Nutrition; GI; feeding / eating problems• Dental care• Sleep• ADHD, disruptive behaviour, anxiety, mood difficulties• Other medical conditions
• e.g., epilepsy risk increases at puberty in ASD
45
ASD Resources• Autism Speaks Toolkits - 40 currently available, some in Frenchhttps://www.autismspeaks.ca/science‐services‐resources/resources/tool‐kits/
e.g. Parents - First 100 Days, toileting, sleep, dental visits, puberty/adolescence …
Professionals – Talking to parents about ASD, dental visits, blood draws …
46

11/29/2019
24
Evidence-based Practices for ASD - Cochrane Collaboration• http://www.cochrane.org
• Cochrane standards require RCTs a treatment to claim a strong evidence base
• Much ASD treatment research based on quasi-experimental, pre- / -post-test, and single-subject research designs -- not considered sufficiently rigorous for inclusion
• Behavioural intervention components (e.g., use of task analysis, shaping, reinforcement, prompting) have very strong empirical support from another research tradition (Applied Behaviour Analysis), established using single-subject experimental designs
47
Cochrane Reviews: Educative Interventions• Early intensive behavioural intervention (EIBI)“… evidence supports the use of EIBI for some children with ASD…The current state of the
evidence is limited … due to the lack of RCTs. Additional studies using RCT research designs are needed ....” Reichow et al. (2013)
• Parent-mediated interventionSome evidence of effectiveness in changing parent-child interactions
Note:• NS EIBI – unique model (Pivotal Response Treatment, incl. parent-mediated )• May be as effective as more intensive EIBI (pre-/post- observational study)
48
Smith et al. (2019)

11/29/2019
25
Cochrane Reviews: Educative Interventions
• Social skills groups for individuals aged 6 to 21 years• Some indications of improved social competence and better friendships, compared to no
treatment
• Theory of mind (ToM) interventions• Some evidence that ToM skills can be taught• Poor-quality evidence that skills are maintained or generalized to other settings
• Music therapy• May help to improve skills in … social interaction and communication”
49
Intervention - Anxiety
Modified CBT for anxiety and related symptoms effective in RCTs:• Co-existing anxiety in ASD
• e.g., Facing Your Fears, Reaven et al. (2011)
• Emotion regulation / anxiety (transdiagnostic )• e.g., Weiss et al. (2018)
• Experienced MH providers with knowledge of ASD can implement CBT
50

11/29/2019
26
Intervention – Behavioural Disorders• Disruptive behaviour: parent training / parent-mediated behavioural
interventions• May be combined with medication (e.g., risperidone)
• Insomnia in NDDs: parent-mediated behavioural tx• e.g., Better Nights, Better Days for NDD, Corkum et al.• RCT in progress, recruiting children ages 4 to 12 with ASD, ADHD, CP, FASD
51
www.ndd.betternightsbetterdays.ca/
Aman et al. RUPP Autism Network (2009)
Intervention – Behavioural Disorders• Intensive interventions and comprehensive community supports needed for
the most severely affected individuals with NDDs, with and without intellectual disability
• Limited respite for families, community-based residential care options
• IWK & NSHA MHA intensive behavioural support program for children / youth with ASD - under development
52

11/29/2019
27
Intervention – Social Skills• Greater change seen in social skills programs
• that include parent groups• longer duration / more hours
• Need to distinguish social knowledge from performance
• Peer-mediated social interventions
53
Wolstencroft et al. (2018)
e.g., Chang & Locke (2016)
Cochrane Reviews: Medications• Risperidone: “may be beneficial for various aspects of autism including
irritability, repetition and hyperactivity”
• Aripiprizole: “short-term use may be effective in treating irritability, hyperactivity, and repetitive movements”
• SSRIs: no evidence to support use in children• limited evidence for adults
• Tricyclic antidepressants: limited evidence to support use
• Secretin: no evidence to support use
54
Anagnostou et al. CIHR-funded clinical trial (2019 - )

11/29/2019
28
Cochrane Reviews: Diet and CAM• Gluten and casein-free diet: no evidence to support use• Vitamin B and magnesium combo: cannot currently be supported• Omega-3 fatty acids: insufficient evidence to support use• Polyunsaturated fatty acids: insufficient evidence to support use• Acupuncture: insufficient evidence to support use• Auditory integration therapy: no evidence to support use• Hyperbaric oxygen therapy: no evidence of improved symptoms; minor ear
barotrauma• Chelation: no evidence to support use; risks outweigh benefits
55
Vulnerability
56
• Families of children / youth with ASD are targeted by providers of unproven, ineffective or pseudo-scientific treatments
• Hyperbaric oxygen therapy – US FDA Statement• Homeopathic “vaccines”• Vision therapy• HANDLE• “Miracle Mineral Solution” aka chlorine dioxide• Etc, etc
• Be an advocate for science-based treatment
Smith & MacDonald (2017)

11/29/2019
29
57
• Socialization• social adaptive behaviour; peer and family relationships
• Functional independence• activities of daily living; managing adolescent life tasks; community participation
• School Achievement• academic achievement; feeling of connectedness to school
• Self-determination• setting goals; solving problems; making choices
• Emotional and behavioural regulation
Developmental Health / Well-being in Adolescence ‘Pathways in ASD’ Study
• Increasingly, increased rates reported of GD, non-binary gender identity among individuals with ASD
• Strong research is lacking
• Clinical need to avoid assumptions (as with other teens)
Gender Dysphoria
Øien et al. (2019)
58

11/29/2019
30
CONNECT• CONtiNuity of carE & services for autistiC adulTs• Needs Assessment Survey – Maritimes• 41 self-reporting adults; 63 caregiver reports (18 to 63 years)
• Annual income $11,307Priorities:• employment counselling• housing/residential options• life skills training• provincial disability program
59
https://youtube/kefkHv38OiA
Jose et al. INSAR (2019)
Transition to Adult Care• Families may need cues to begin looking ahead in middle school /
junior high• Setting individualized goals
• Realistic appraisal of abilities, opportunities
• Involve youth as much as possible (“self-determination”)• Autism NS – youth / adult programs
• e.g., social groups, summer camp (6 – 21), Worktopia (pre-employment) program)
60
http://www.autismnovascotia.ca/

11/29/2019
31
Transition to Adult Care• Behavioural / mental health supports are major needs
• In addition to routine care
• Healthcare provider training needs increased attention to NDDs• Ideal area for inter-professional training and collaborative care• BALANCE – educational program for peri-operative healthcare teams
• Formal recognition needed that ASD / NDD care takes more time
61
https://balanceforautism.com/
Transition to Adult Care
• IWK Developmental Pediatrics Clinic• NDD-focused transition-of-care information & support
• Adult Developmental Clinic (> 16 years with NDD / ID)• Dalhousie Family Medicine Spryfield Community Wellness Centre
62
dalfamilymedicineclinics.com

11/29/2019
33
Case 1
• 10-year-old boy referred to IWK Autism Team by Family Physician
• Early language milestones – later end of typical range
• Parents became concerned at age 6 -- teacher spoke to them about behavioural difficulties; followed up with family doctor
• Parents not interested in medication, wanted “full assessment”
Semi‐structured diagnostic interview (ADI‐R)
• Parents’ recall of early behaviour was limited
• Communication– facial expressions and gestures appeared typical, unclear re: pretend play (below cut-off)
• Social – might not offer comfort, limited understanding of relationships, shared enjoyment with others, has friends including a best friend; attention, impulsivity affected social behaviour(above cut-off)
• RRB – intense interest in specific video game, also magic tricks; no repetitive movements or object use nor atypical sensory reactions (below cut-off)

11/29/2019
34
Observation / Interview (ADOS‐2)
• Social Affect – spoke rapidly; prosody typical; no repetitive or pedantic speech; many gestures; reciprocal conversations with examiner; appropriate facial expressions but sometimes undirected; reduced use of gaze; good insight into feelings and relationships
• RRB – no repetitive speech or motor behaviour, no atypical sensory; talked at length about video game with too much detail
• +++ restless and fidgety
• Total score in ASD range (moderate)
Parent‐report Questionnaires
• Child Behaviour Check List• Total – Borderline• Externalizing & Internalizing – Average• Attention Problems – Clinical range
• Autism Spectrum Rating Scales• Total, Self-regulation, Unusual Behaviors - Very Elevated• Social-Communication – Average
• Adaptive Behavior Assessment System, 2nd ed.• General Adaptive Composite, Social, – Low• Conceptual & Practical – Below Average

11/29/2019
35
Teacher‐report Questionnaires
• CBCL TRF • Total & Externalizing – Borderline
• Attention Problems – Borderline• Internalizing - Average
• Autism Spectrum Rating Scales • Total, Social-Communication, Unusual Behaviors – Average• Self-regulation – Slightly elevated • Attention – Elevated
• Adaptive Behavior Assessment System, 2nd ed.• General Adaptive Composite, Conceptual, Practical – Low
Average Social – Average
Other
• Classroom adaptations (inconsistent in past); currently to Learning Centre at times to complete work; good recent progress
• Waiting for psycho-educational assessment
Diagnosis?
ADHD also recommended OT assess for possible DCD

11/29/2019
36
Case 2
• 11-year-old boy with previous diagnosis of ADHD at age 4 or 5 by pediatrician
• Overactive & driven; investigated for possible seizures – negative
• Medications for ADHD and anxiety
• Received group CBT for anxiety; social differences evident in that context prompted referral
• Referred to Autism Team by MHA psychologist
Semi‐structured diagnostic interview (ADI‐R)
• Communication - lacks reciprocity, repetitive (above cut-off)
• Social – atypical gaze, limited facial expressions, difficulty identifying & expressing his feelings (although empathetic), no real friendships, “beat up bullies” but with expressed focus on ‘justice’ (at cut-off)
• RRB – intense interests in science, animals, explosives; many specific sensory aversions (touch, smells, noise) (above cut-off)

11/29/2019
37
Observation / interview (ADOS‐2)
• Social Affect – fleeting eye contact, lack of directed facial expressions, used gestures, no reciprocal conversation, limited understanding of personal relationships
• RRB – struggled with pretense and narrating a story, mentioned interests but not excessive
• Total score in ASD range
Parent‐report Questionnaires
• Child Behavior Check List• Total, Externalizing & Internalizing – All in Clinical range• Rule breaking, Aggressive - Clinical; Anxious/Depressed -
Borderline
• Autism Spectrum Rating Scales• Total, Social-Communication, Unusual Behaviors, Self-
regulation – Very Elevated
• Adaptive Behavior Assessment System, 2nd ed.• 1st percentile

11/29/2019
38
Teacher‐report Questionnaires
• Missing ≈50% of classes, “great sense of justice” but struggling to relate to peers appropriately
• CBCL TRF • Total & Externalizing – Clinical range• Internalizing - Average • Social Problems, Thought Problems, Attention Problems, Rule-breaking,
Aggressive - Clinical range:
• Autism Spectrum Rating Scales• Total, Social-Communication, Unusual Behaviors, Self-regulation – all Very
Elevated
Other
• S-LP assessed in grade 3: average expressive and receptive language; mild-moderate fluency problems; no comment on pragmatics
• No services recommended
• Psycho-educational assessment reportedly done but no report provided at time of ASD assessment
Diagnosis?
ADHD (previously dx’d) + ASD