AUTISM AND ANESTHESIA - oma.org · SLIDE 5 OF 5. Results Healthcare Provider Feedback Exemplar...
35
AUTISM AND ANESTHESIA AMANDA WHIPPEY MD FRCPC PEDIATRIC ANESTHESIOLOGIST MCMASTER UNIVERSITY
Transcript of AUTISM AND ANESTHESIA - oma.org · SLIDE 5 OF 5. Results Healthcare Provider Feedback Exemplar...

AUTISM AND ANESTHESIAAMANDA WHIPPEY MD FRCPC
PEDIATRIC ANESTHESIOLOGIST
MCMASTER UNIVERSITY
OBJECTIVES
1. Review Autism Spectrum Disorder (ASD) its impact on the perioperative experience of patients
2. Discuss current research on Clinical Practice Guidelines that aim to decrease stress, anxiety and improve compliance in patients with ASD coming for surgery

DISCLOSURES
None
“ If you have met one person with autism, you’ve
met ONE person with autism”
- Dr. Stephen Shore

J Dev Behav Pediatr 2016 (37) 457-464
First identified in 1943 by Kanner
1980 - Autism a distinct disorder in DSM IV
2013 – ASD (Autism, Aspergers, PDD)
2017 – Less than 10% of anesthesia deptand 0% pediatric depts in Sweden have specific protocols to address needs of children with ASD
“a mental condition, present from early childhood, characterized by difficulty in communicating and forming relationships with other people and in using language and abstract concepts.”
Autism is Common
CDC Press Release March 2014

DIAGNOSIS Communication
Sensory
ProcessingBehaviour
40-80% ASD have
abnormal sensory
processing
1. Need for
routine
2. Stereotypic
movements
3. Intense special
interests
Visual > Verbal communication
Difficulty interpreting social
interaction
Pediatric Anesthesia 25 (2015)1076-184
*

THE OR IS A SCARY PLACE…
Abnormal responses to sensory stimuli
sound, touch, visual stimuli, pain, or the sensations of hot and cold
Preoperative anxiety = negative postoperative behaviors
sleep disturbances, nightmares, separation anxiety, apathy, general anxiety, withdrawal – up to 1 YR!
Routine dependence can lead to
extreme distress
Paediatr Anaesth. 2003;13(3):188-204
12 parents of patients describe their experience without and without perioperative dialogue

WITHOUT
HOPELESS STRUGGLE
UNSPEAKABLE
SUFFERING
DISGRACEFUL
SCENARIO
WITH
WARM HANDS
KNOWN FACES
INTERPLAY BETWEEN
PATIENT AND
CAREGIVER

Early literature focuses on combative or uncooperative children –NOT ROOT CAUSES
Behaviourally informed interventions are RARE
Individualized plans that minimize known stressors decreased noncompliance at induction from 50 17% WITHOUT premedication
Aim: to survey perioperative management practices for children with ASD
Arch Dis Child 2016 (101) 1090-1094

3 Main Themes:
1) Collaborating with caregiver to inform patient management
2) Developing a process for communicating information gathered from caregivers to perioperative staff
3) Modifying perioperative environment-based on patient-specific needs gathered from caregiver
** Importance of individualized care pervaded all themes**

retrospective chart review - preoperative sedation, stratified by autism spectrum disorder severity level, behavior at induction, caregiver satisfaction
246/251 patients had individual care plans carried out (98%)
45% patients were Aspergers/ Severity Level 1
Need for premedication increased (OR 5.5X) with increasing severity of ASD (level 3 vs level 1)
Cooperation at induction (overall 90%) did not differ between sedated and non sedated patients
Caregiver satisfaction 98%
DO YOU HAVE A PERIOPERATIVE PROGRAM FOR CHILDREN WITH ASD AT YOUR HOSPITAL?
A.Yes
B. No
C. I don’t know
Enhanced Perioperative Management of Children with Autism: a Pilot Study
AMANDA WHIPPEY MD FRCPC LEORA BERNSTEIN MD DESIGEN REDDY MD FRCPC
MCMASTER UNIVERSITY
Autism is increasing 1/68 children is diagnosed with ASD 1
Perioperative stress is high for the autistic child, their families and healthcare workers2
Can we introduce a perioperative care pathway that minimizes perioperative stress and anxiety for children with autism?
Introduction “Nolan would have been screaming, crying and terrified. It would have been a very different
and extremely stressful experience for both of us without the special accommodations.”
– Parent Feedback
1 CDC update Mar 27 20142 Scan J Car Sci 2012; 26 (4) 627-634
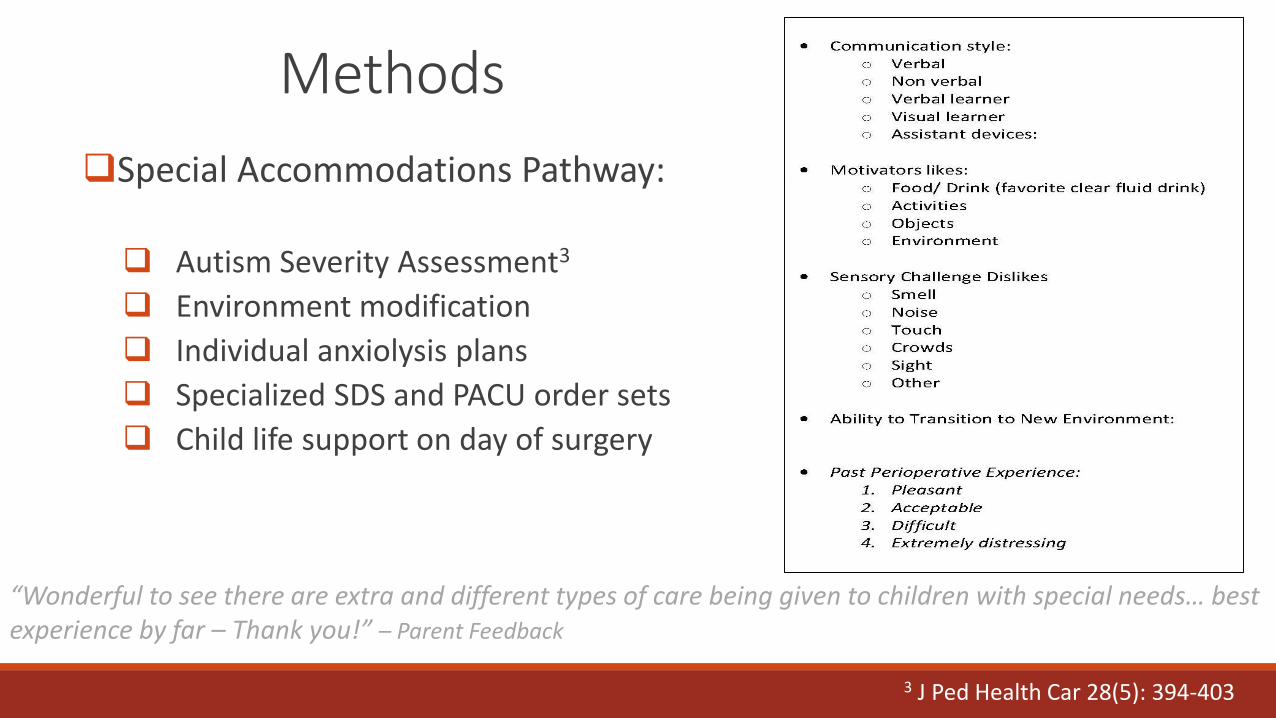
Methods
Special Accommodations Pathway:
Autism Severity Assessment3
Environment modification
Individual anxiolysis plans
Specialized SDS and PACU order sets
Child life support on day of surgery
“Wonderful to see there are extra and different types of care being given to children with special needs… best experience by far – Thank you!” – Parent Feedback
3 J Ped Health Car 28(5): 394-403

Methods Anxiety and sedation scores were recorded at: SDS, induction, PACU
Parental and Healthcare provider feedback used to modify protocol and establish feasiblity
Cases debriefed by sedation team (anesthesia, SDS nurses, CLS, AA) to improve process
“ Amazing program, I hope we learn more about it and it becomes part of our practice” - OR RN
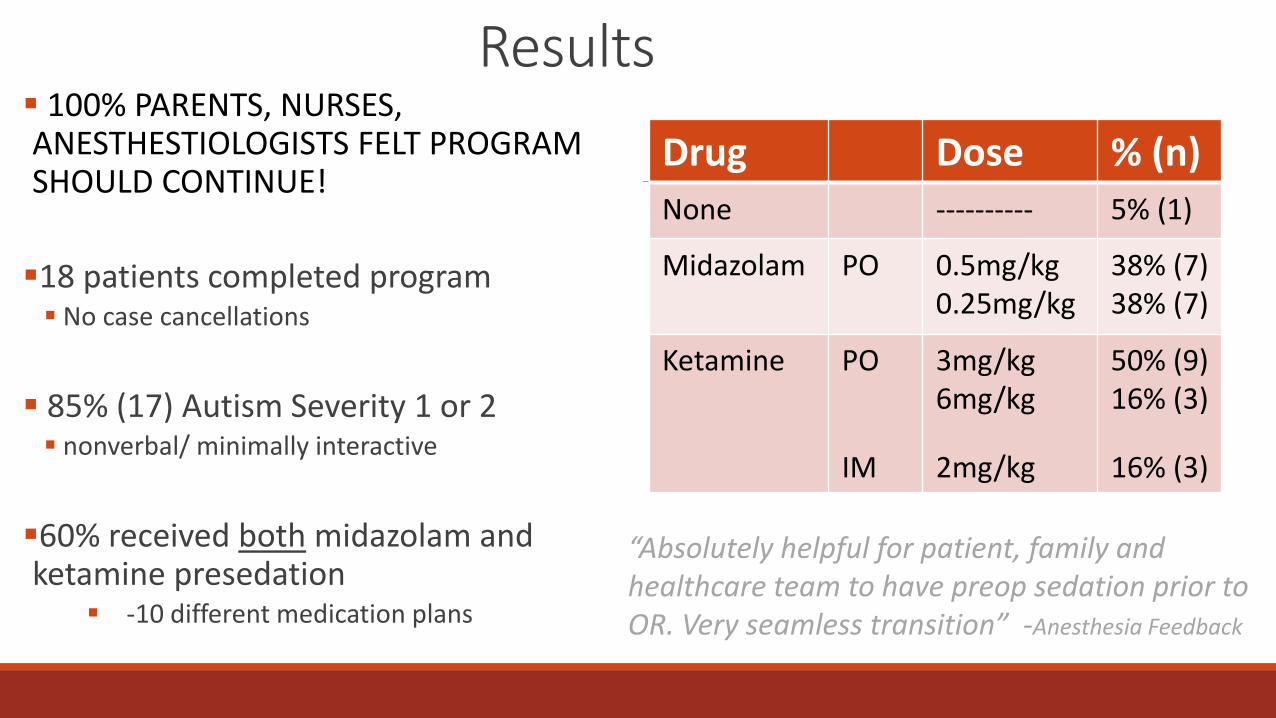
Results 100% PARENTS, NURSES, ANESTHESTIOLOGISTS FELT PROGRAM SHOULD CONTINUE!
18 patients completed program No case cancellations
85% (17) Autism Severity 1 or 2 nonverbal/ minimally interactive
60% received both midazolam and ketamine presedation
-10 different medication plans
Drug Dose % (n)
None ---------- 5% (1)
Midazolam PO 0.5mg/kg0.25mg/kg
38% (7)38% (7)
Ketamine PO
IM
3mg/kg6mg/kg
2mg/kg
50% (9)16% (3)
16% (3)
“Absolutely helpful for patient, family and healthcare team to have preop sedation prior to OR. Very seamless transition” -Anesthesia Feedback

ResultsDemographics Descriptive Statistic (n=18)
Age (yr); mean(SD) 8.1(3.5)
Weight(kg); median (min,max) 28.8(11.1, 100.0)
Gender (male); n (%) 16(89)
Autism Severity Score; n(%)
1. Responds to name/ Aware of others
2. Interacts with toys, Beginning Language
3. Interacts with others, Controls behaviour
4. Maintains control, Verbalizes feelings
Missing
9(56)
6(38)
0
1(6)
2
Sensory Dislikes/ Triggers; n(%)
1. Smell
2. Loud Noises
3. Touch
4. Crowds
5. Bright Lights
6. Other
3 (16)
14 (78)
9 (50)
14 (78)
10 (56)
3 (17)
History of Aggressive/ Combative Behaviour n(%)
Missing
11(73)
3
Type of Surgery n(%)
Ent
Ortho
Dental
Urology
3(17)
1(6)
12(67)
2(11)
Time from admission to surgery (sedation time - 8am
surgery only); mean (SD) 38.6(15.7)
Duration of procedure; mean (min,max) 70 (15, 173)
Time from PACU to discharge; mean (min, max) 95.3(54,186)
• Most common triggers were loud noises and crowds
• 73% patients had a history of aggressive or combative behaviour
• Ave Sedation time was 40min
• Ave Recovery Time 95min

ResultsParental Feedback Exemplar Quote % (n)
Personalized Approach “(Staff) listened to suggestions which is what made this our
best experience ever!”
55% (10)
CLS (distraction, ipad) ”(CL) was encouraging and supportive – could not have
done it without her!”
44% (8)
Preoperative Sedation 33% (6)
Parental Presence ”playing a favourite show, letting him cuddle with mom
were great strategies”
33% (6)
Decreased Wait Times 27% (5)
Accommodating Staff ”Staff were professional and patient..took the time
necessary for our son to complete each step”
27% (5)
Quiet Room 27% (5)
“This program is absolutely necessary for patients and families with special needs!! Thank you so much for all the options!” – Parental Feedback
SLIDE 5 OF 5

ResultsHealthcare Provider Feedback Exemplar Quote
Program should continue “very worthwhile - particularly for family and patient” – PACU
Multidisciplinary Structure is Important
“Appreciated the structure, communication, and support from all services. Everyone had the same plan and expectations” –SDS RN
Preop Sedation can improve experience
“Absolutely helpful for patient, family and health care team to
have this preop sedation prior to the OR. Very seamless transition
into the OR with the child sedated and IV in place” – Anesthesia
Helpful for Families “I think this intervention is very beneficial to the patient as well as the family. It might delay OR time but it is less traumatic to the patient” – OR RN
Increased nursing ratio in PACU “1:1 nursing ratio for 60min … woke up very calm and had no issues” – PACU
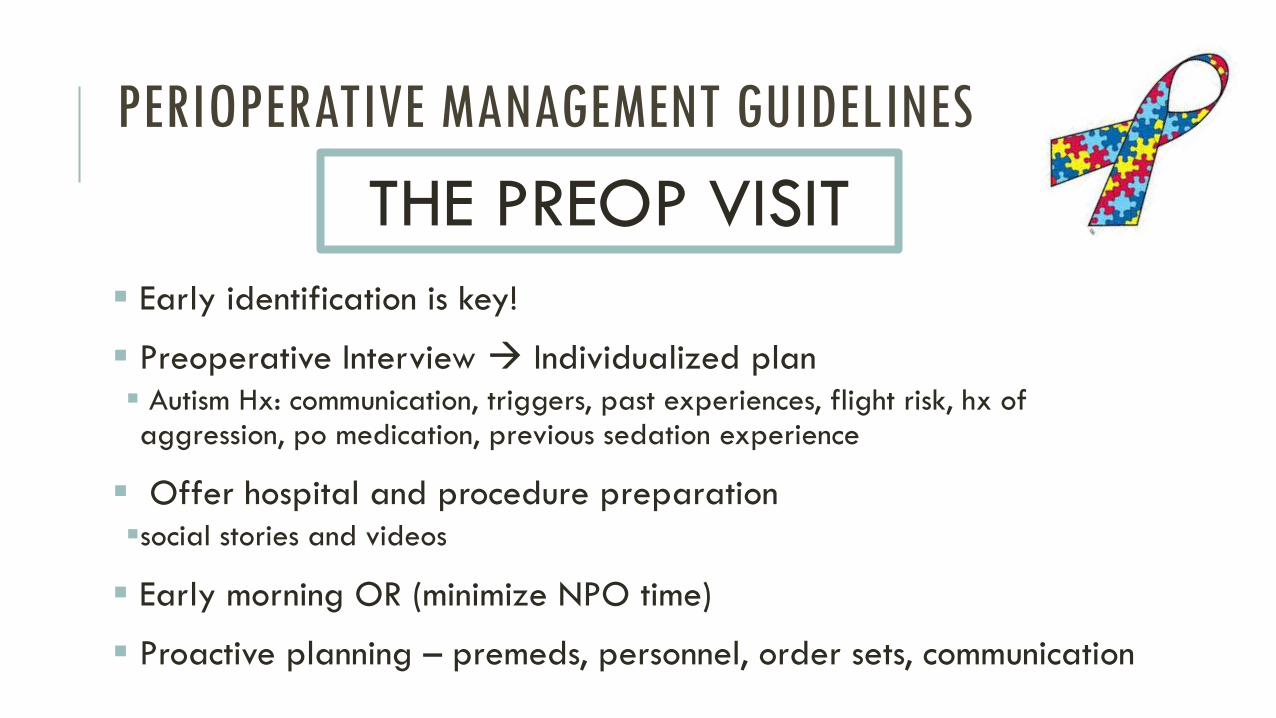
PERIOPERATIVE MANAGEMENT GUIDELINES
Early identification is key!
Preoperative Interview Individualized plan
Autism Hx: communication, triggers, past experiences, flight risk, hx of aggression, po medication, previous sedation experience
Offer hospital and procedure preparation
social stories and videos
Early morning OR (minimize NPO time)
Proactive planning – premeds, personnel, order sets, communication
THE PREOP VISIT
Flexible admission process
Ie. Minimize transitions, wait times
Quiet room – privacy, dim lighting, iPad available, service animals
AVOID changing clothes, multiple health care providers, topical analgesic creams, routine vitals
Premedication on arrival – mix in favourite drink
IV placement if possible
PERIOPERATIVE MANAGEMENT GUIDELINES
Same Day Surgery
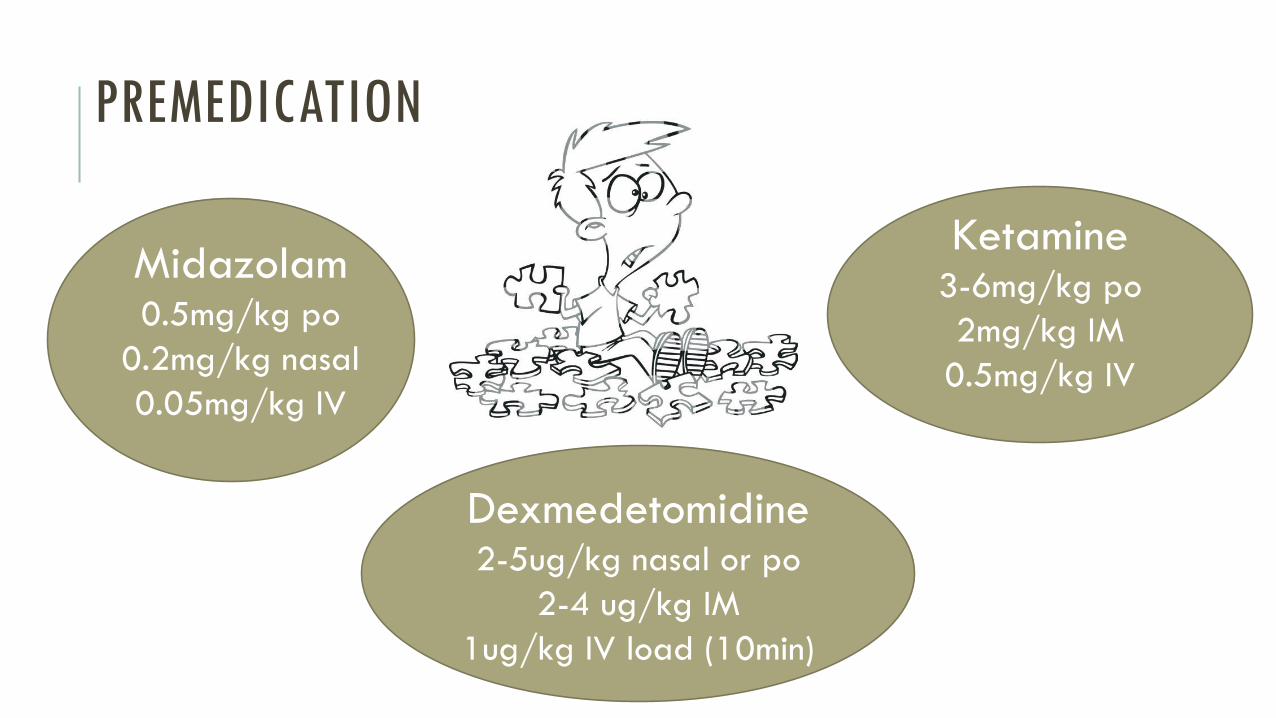
PREMEDICATION
Ketamine3-6mg/kg po
2mg/kg IM
0.5mg/kg IV
Dexmedetomidine2-5ug/kg nasal or po
2-4 ug/kg IM
1ug/kg IV load (10min)
Midazolam0.5mg/kg po
0.2mg/kg nasal
0.05mg/kg IV

DO YOU USE PREMEDICATION TO FACILITATE IV PLACEMENT OR INDUCTION?
A. Routinely
B. For compliance or anxiolysis
C. For compliance only
D. Rarely
E. Never

PREMEDICATION
Midazolam po (0.5mg/kg)
Paradoxical reactions
Tastes gross! – pH 3
Ketamine po (3-6 mg/kg)
emergence phenomenon, disorientation, sensory/ perceptual illusions, vivid dreams, nausea/ vomiting, nystagmus
S/E more common in females, IV administration, excessive stimulation
14% noncompliance with induction vs 30% with midazolam alone
No clear evidence for one
medication over another!
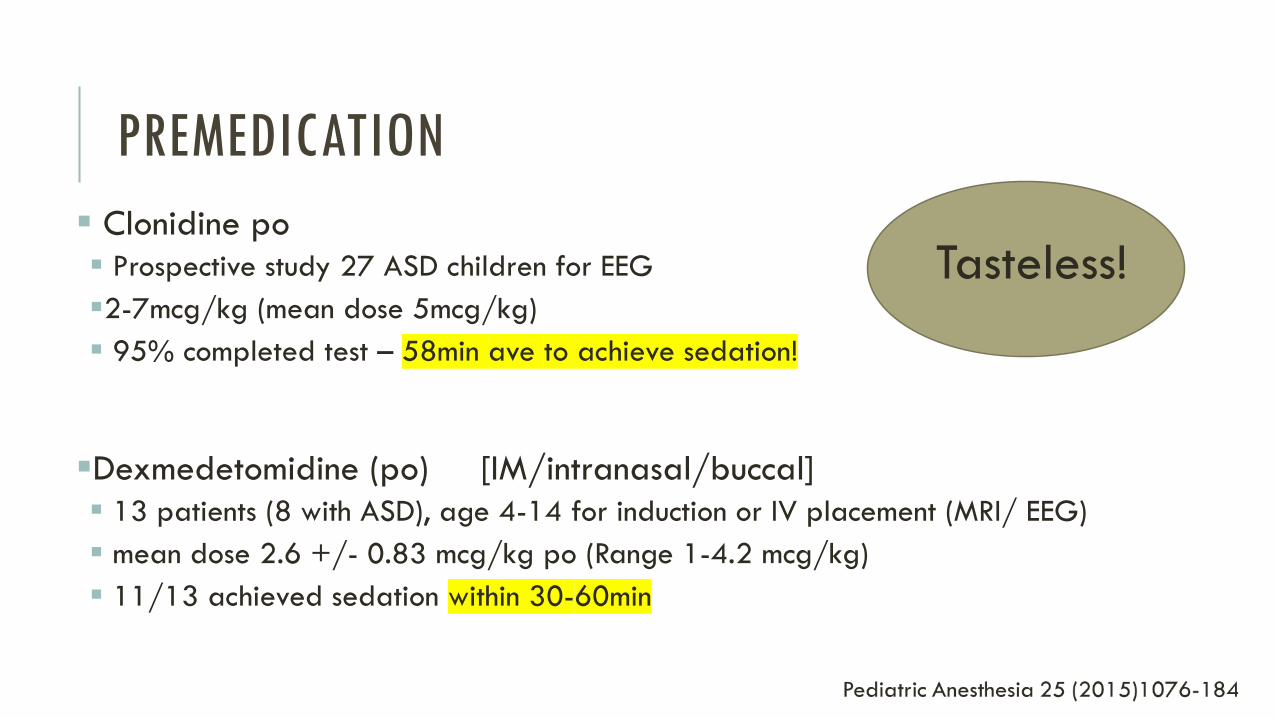
PREMEDICATION
Clonidine po
Prospective study 27 ASD children for EEG
2-7mcg/kg (mean dose 5mcg/kg)
95% completed test – 58min ave to achieve sedation!
Dexmedetomidine (po) [IM/intranasal/buccal]
13 patients (8 with ASD), age 4-14 for induction or IV placement (MRI/ EEG)
mean dose 2.6 +/- 0.83 mcg/kg po (Range 1-4.2 mcg/kg)
11/13 achieved sedation within 30-60min
Tasteless!

Dim lights in OR, minimize personnel, cover equipment/IV supplies
Parental presence/ iPads/ music
Do not delay induction – OR checklist before patient in room or after induction
IV or mask induction may be preferred
Adequate fluid administration, PONV prophylaxis and analgesia S/L IV before leaving OR
PERIOPERATIVE MANAGEMENT GUIDELINES
Anesthesia
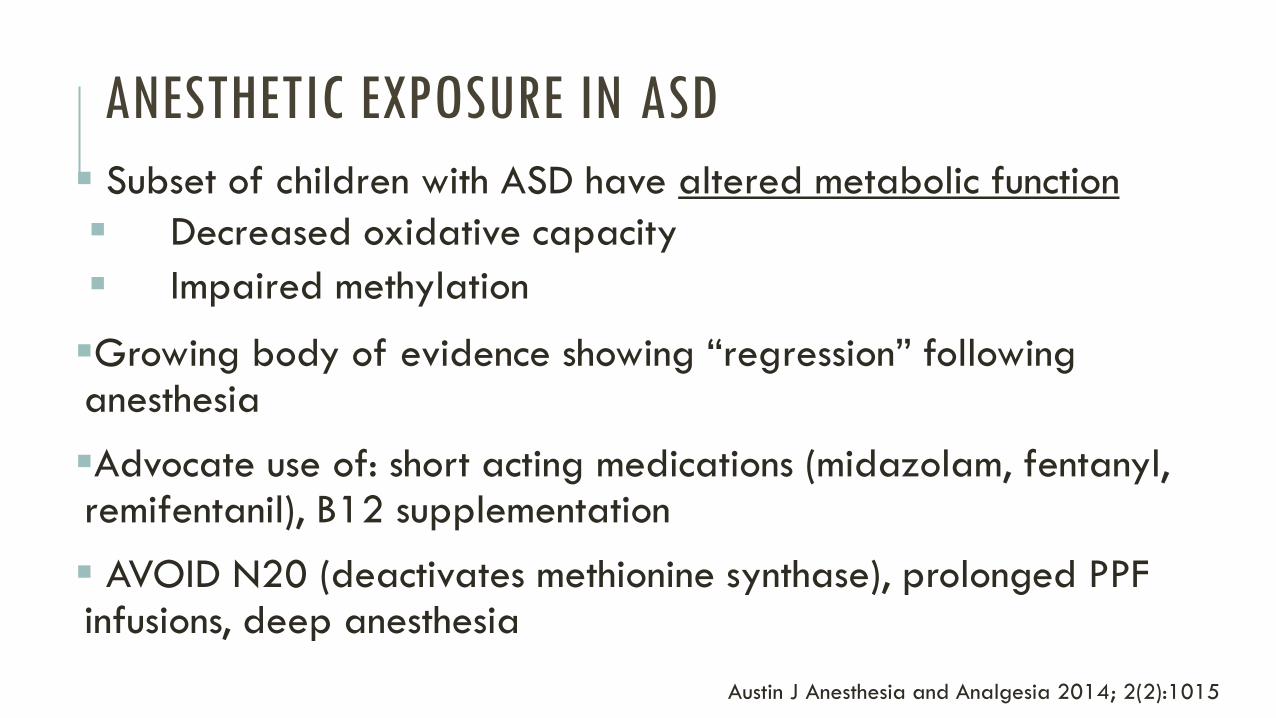
ANESTHETIC EXPOSURE IN ASD
Subset of children with ASD have altered metabolic function
Decreased oxidative capacity
Impaired methylation
Growing body of evidence showing “regression” following anesthesia
Advocate use of: short acting medications (midazolam, fentanyl, remifentanil), B12 supplementation
AVOID N20 (deactivates methionine synthase), prolonged PPF infusions, deep anesthesia
Austin J Anesthesia and Analgesia 2014; 2(2):1015

S/L IV, remove IV early
Quiet recovery area (away from crying babies, loud TVs, turn down monitors)
Early parental presence
Communication boards
Discharge home direct from PACU when patient awake but sedated. Transfer admitted patients ASAP
PERIOPERATIVE MANAGEMENT GUIDELINES
PACU
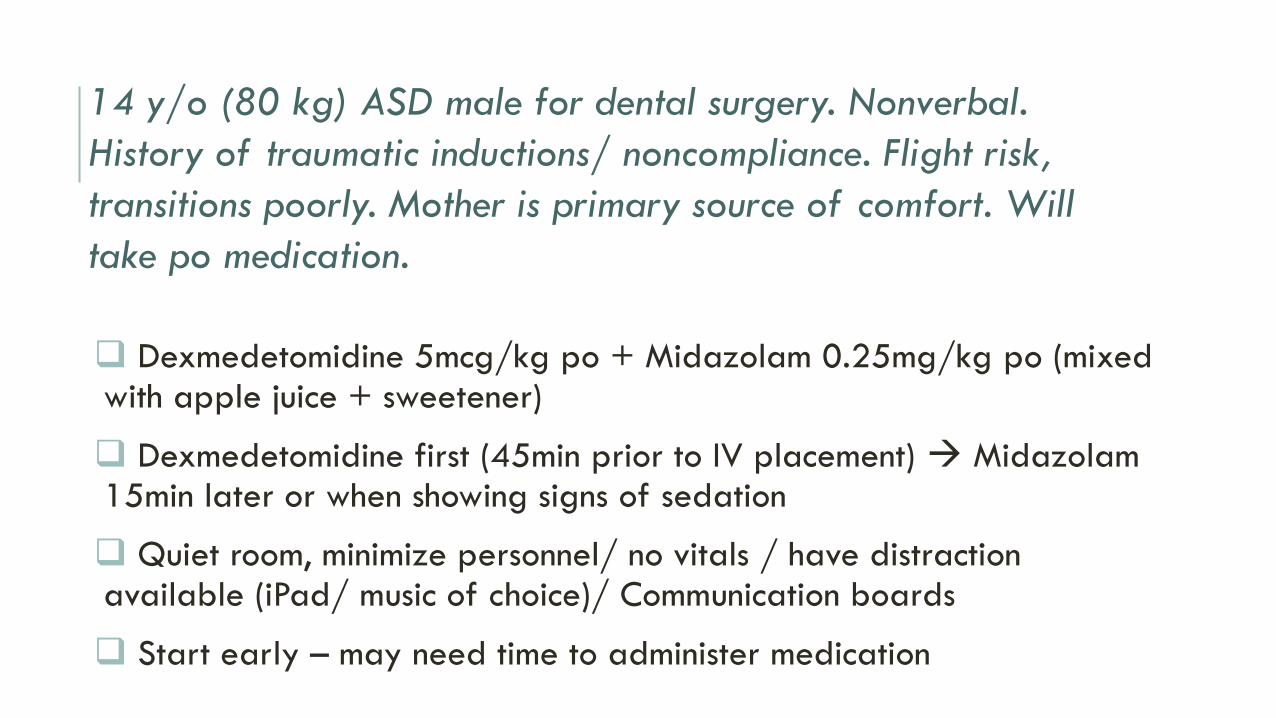
Dexmedetomidine 5mcg/kg po + Midazolam 0.25mg/kg po (mixed with apple juice + sweetener)
Dexmedetomidine first (45min prior to IV placement) Midazolam 15min later or when showing signs of sedation
Quiet room, minimize personnel/ no vitals / have distraction available (iPad/ music of choice)/ Communication boards
Start early – may need time to administer medication
14 y/o (80 kg) ASD male for dental surgery. Nonverbal.
History of traumatic inductions/ noncompliance. Flight risk,
transitions poorly. Mother is primary source of comfort. Will
take po medication.

IV placed when sedated in SDS
Transport to OR on stretcher, lights dimmed, parental presence
IV induction, 10ml/kg RL bolus, PONV prophylaxis, deep extubation, PPF or dex to prevent emergence delirium
S/L IV at end of case
Quiet bay in recovery/ Expedited discharge from PACU
14 y/o (80 kg) ASD male for dental surgery. Nonverbal.
History of traumatic inductions/ noncompliance. Flight risk,
transitions poorly. Mother is primary source of comfort. Will
take po medication.
THE BOTTOM LINE
Autism is common
The perioperative experience can be traumatic and overwhelming
Individual Sedation plans based on the child’s specific needs improve compliance
Perioperative management has moved beyond just premedication
Important to create positive experiences to improve future interactions

Excellent resource for establishing clinical practice guidelines for ASD
Addresses ROOT causes and nonpharmacological approaches to improve compliance and minimize stress to the child and family
Advocates for the use of social stories, distraction (ipad), environment modification (quiet room/ dim lighting), premedication and early discharge.
PREMEDICATION Jannu et al 2016
Oral midazolam (0.75mg/kg) vs dexmedetomidine (4mcg/kg)
RCT 60 children 1-7 yrs
Onset significantly faster with midazolam (18min vs 30min) with equal mask acceptance. Dexmedetomidine produced less postop agitation
Kumari et al 2017 Oral midaz (0.5mg/kg) vs dexmedetomidine (4mcg/kg) vs clonidine (4mcg/kg)
RCT 90 children 4-12yrs
Oral midazolam has significantly faster onset, higher sedation score, lower anxiety and better parental separation and mask acceptance