![A Consumer’s Guide to Chiropractic Care · California Board of ChiropraCtiC ExaminErs [ 3 ] What is a Chiropractic Adjustment and Chiropractic Care? A chiropractic adjustment is](https://static.fdocuments.us/doc/165x107/5afc83ce7f8b9a68498b9600/a-consumers-guide-to-chiropractic-board-of-chiropractic-examiners-3-what.jpg)
Autism and medicationsdepts.washington.edu/lend/pmh-cor/2018/images/autism_and... · 2019-02-26 ·...
21
Autism and medications FEBRUARY 26, 2019 WAVA MCH COR
Transcript of Autism and medicationsdepts.washington.edu/lend/pmh-cor/2018/images/autism_and... · 2019-02-26 ·...

Autism and medications
FEBRUARY 26, 2019 WAVA MCH COR
Agenda TODAY
00:00 Welcome and Announcements00:05 Case by Wendy Schofer (group discussion about screening barriers
in March 2019- stay tuned!)00:30 Didactics: Autism and Medication, Beth Ellen Davis MD00:55 Post session poll
NEXT SESSION is March 26th, Irritability, Dr. Cecilia Margret

Patient DOB 13 MPatient gender Male
Patient race/ethnicity Caucasian
Prior medical or mental health dx none
HPI: Worried, all the time; “always been like this,” leading to issues with attentiveness during classes (no
prior issues with distraction/inattention in the past)
Other settings (school, day care) Still going to lacrosse (new sport for pt, his choice), but staying up late for studies and having difficulties falling asleep, Bedtime around 2300, but won’t fall asleep until after 0100. Awake at 0700. Weekends sleep in til noon after staying up til 0100 (“the time” he feels tired).Prior grades A/B, now B/C. Denies concerns about
Related ROS/HX 4-5 diet/caffeine-free sodas per day (starts with breakfast); denies other stimulant/supplement use
Social (residence, foster care,
finances, trauma, ACES)
Lives with active duty mother (has had GAD diagnosis, treatment on Effexor, no hx of effective therapy
connection), elder brother with dx of ADHD but off of meds electively for the past few years
Medications Melatonin 10mg few evenings per week – no noted response
Other screening: PHQ 9 = 3, GAD7 = , SCARED (pt):SCARED (parent):
CONSULT QUESTION After initial visit, noted diffusely + SCARED on both parent and patient scales. Concerns about degree of symptoms, but with hygiene concerns (caffeine intake, sleep disruption, electronic use), encouraged to address bedtime/electronic turn off and removing sodas while referring to psychology for CBT. Plan to follow-up with PCM in office in 3-4 weeks with anticipated engagement with psychology by then – and assess how doing with hygiene changes/supports.
What is the role for starting meds right away? Not in crisis, but concerned about breadth of symptoms and didn’t want to go to meds right away in light of other contributing lifestyle factors listed above.
Is there a role for starting meds to help with symptoms and perhaps lifestyle contributors will be easier to address if less anxiety symptoms?
Case discussion

Didactics CECILIA MARGRET MD, Ass istant Professor, Chi ld and Adol . Psychiatry
BETH ELLEN DAVIS MD, Professor, Developmental Pediatr ics

AUTISM SPECTRUM DISORDERS AND MEDICINE FOR CHALLENGING BEHAVIORSBETH ELLEN DAVIS MD MPH
DEVELOPMENTAL BEHAVIORAL PEDIATRICS

OBJECTIVESBe clear about goals for medication management: find target symptoms
Be able to list 4 interventions to consider BEFORE medication use.
Be able to discuss the 2 X 2 Table of Safe and Effective interventions

KEY POINTSNo medication to date CURES autism, but many medications help challenging behaviors to allow children with ASD to be in settings where AUTISM is treated: social situations, with peers, in school, on family outings, in learning settings.
Not the same as other children who take medication
Start low !
Go slow !
Lots of kids need special preparations of medication (liquid, dissolvable, sprinkles)

Before we talk meds…..Families who are still considering whether to use medications, direct to the Autism Speaks Toolkit, “Autism: Should My Child Take Medicine For Challenging Behaviors?”
Providers who need a refresher on “challenging behaviors” see October 2018 “Challenging Behaviors”
http://depts.washington.edu/lend/pmh-cor/

Role of provider, BEFORE MEDICATIONS……Look for medical causes of challenging behaviors
◦ GI- constipation? GERD?
◦ Seizure
◦ Dental –impaction?
◦ Sinus/ear-chronic infection?
◦ HA/migraine
◦ Bone fracture
◦ Other medication/supplement
◦ New caregiver? Maltreatment?
Order of interventions◦ R/O medical cause
◦ Evaluate sleep
◦ Caregiver stress
◦ Behavior understood at school and home, with behavior therapy
◦ Is there a co-occurring psychiatric condition?
◦ MEDICATION
“TARGET” ----aggression before sleep before mood, before anxiety/depression before ADHD…..

Target symptomsHyperactivity
Short attention span
Impulsive behaviors
Irritability
Agitation
Aggression
Self-injury
Tantrums
Repeating thoughts interests and behaviors
Sleep problems
Anxiety
Depression
Mood problems
Tics
FINDS: frequency, intensity, number of symptoms, duration, severity, settings* SEE TOOLKIT: AUTISM AND MEDICINE for charts, logs, action plans…

Clusters of symptomsCertain clusters of symptoms bring up the possibility of particular diagnoses. For instance consider:
• ADHD if: inattentive or hyperactive with school difficulty
• Anxiety disorder if: unexplained somatic complaints, general or specific worries
• Autism if: developmental concern with the most severe impairment in social functioning
• Bipolar disorder if: episodic mood changes with manic features
• Depression if: withdrawn, irritable, unexplained somatic complaints
• Eating disorder if: losing weight or odd eating habits
• Conduct or Oppositional Defiant Disorder (ODD) if: oppositional or aggressive behavior

Side effects
Effective Not-effective or insufficientevidence
SAFE MELATONINALPHA-AGONISTS
GLUTEN FREEDIETARYSUPPL.
STIMULANTSSSRIRISPERIDONE
UNSAFE Tricyclics CHELATIONSECRETIN
Use medications with fewer side effects first. Explain “Trial”
START LOW GO SLOW
Do not start or stop more than one medication at a time.
Managing common side effects:
* See Toolkit: Autism and medicine
Target symptoms: hyperactivity, short attention, impulsivity….adhd? Stimulants have most evidence (Ritalin studied most, start at 2.5 mg short acting and increase by 2.5 mg in am, then lunch time to dose between 15-30 mg, usually. More adverse effects such as insomnia, social withdrawal, irritability)
Alpha agonists have least side effects (consider Guanfacine .25 mg bid, increasing by .25 mg/one dose at a time/weekly ‘til 1 mg BID)

Target Symptom: AnxietyAnxiety is really hard in ASD.
◦ 50% have anxiety symptoms that are impairing
◦ Parents of children with ASD are stressed
◦ Anxiety may be very different in this population
SSRIs, guanfacine, Atomoxetine, short acting hydroxyzine, buspirone, …the list goes on, because there are few studies to really inform us. This is the area of ‘Off label’ where shared-decision making, and parent school and therapist communication are needed.

Target symptom: irritability, agitation, self-injury, aggressionRisperidone has evidence, but needs blood monitoring and side effects of weight gain, and rarely movement disorder. Start at 0.25 mg/day and increase by .25 mg/day every two weeks as needed. Effective dose is often around 0.5-1.0 mg.
But you can try Guanfacine? Consider a stimulant or even an SSRI before moving to the anti-psychotics. Remember your box….

Target symptom: SleepSleep hygiene first, second and third. See Toolkit: autism and medicine
Melatonin 1 mg to 6 mg, usually more does not help (ex: 19 year old on 60 mg!)
Guanfacine at night, Clonidine at night (to get to sleep)
Trazadone might help for a while. (has sleep maintenance properties)
Monitoring kids with ASD on medicationsFollow target symptoms and stop one medication before starting another, if possible
Make sure behavior therapies are in place
If on neuroleptic◦ Follow HT WT BMI, metabolic panel (lipids, cholesterol, fasting glucose, +/-CBC)
Check for supplements and other integrative interventions
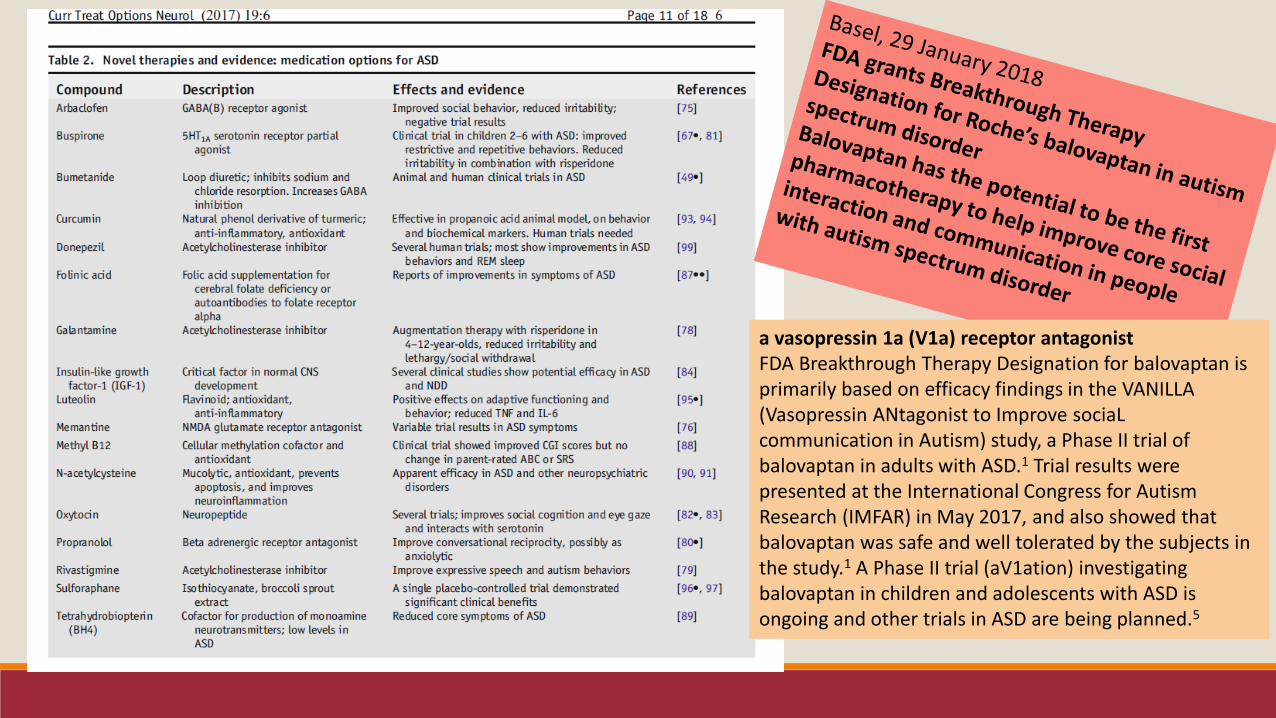
a vasopressin 1a (V1a) receptor antagonistFDA Breakthrough Therapy Designation for balovaptan is primarily based on efficacy findings in the VANILLA (Vasopressin ANtagonist to Improve sociaLcommunication in Autism) study, a Phase II trial of balovaptan in adults with ASD.1 Trial results were presented at the International Congress for Autism Research (IMFAR) in May 2017, and also showed that balovaptan was safe and well tolerated by the subjects in the study.1 A Phase II trial (aV1ation) investigating balovaptan in children and adolescents with ASD is ongoing and other trials in ASD are being planned.5

Complementary and Alternative Medicine (CAM)
➢ 24-74% of children with ASD are given at least one, and usually more than one, complementary therapy➢ Natural products: Herbs, Vitamins, Minerals, and Probiotics
1) Vitamin D, Vitamin B12, Vitamin B6 with magnesium, Omega-3 Fatty Acids, and multivitamin preparations
2) No conclusive evidence exists that people with ASD require different nutrient intake that what is recommended
3) We do not know the long-term risks of high-dose supplementation
4) Melatonin is a safe and effective intervention for sleep in children with ASD
➢ Mind and Body practices: Yoga, Chiropractic, Massage, Acupuncture, progressive relaxation, and guided imagery
1) Emerging evidences supports further study of music therapy, yoga, massage, and equine-assisted therapy
2) No evidence yet supports Auditory Integration training, vision therapy dance therapy, drama therapy, and chiropractic therapy

Questions?

Post-Session EvaluationAs a result of attending the session, to what extent did your Confidence in the learning objectives change?
Autism and medications Much more confident
Somewhat more confident
Confidence unchanged
Less confident
Know interventions to consider before meds
Identify target symptoms and clusters
Discuss safe and effective strategies using 2X2 tool


















