
August 2012, VOL 1, NO 3
60
Facilitating the Next Generation of Precision Medicine in Oncology ..................................Page 43 Which Breast Cancer Patients Should Receive Adjuvant Chemotherapy? ................Page 52 Incorporating Genomics Into Practice: An Interview With Kimberly J. Popovits ..........Page 18 August 2012 Volume 1 • Number 3 A Peer-Reviewed Journal www.PersonalizedMedOnc.com © 2012 Green Hill Healthcare Communications, LLC IMPLEMENTING THE PROMISE OF PROGNOSTIC PRECISION INTO PERSONALIZED CANCER CARE TM REGULATORY ISSUES BREAST CANCER P ERSONALIZED M EDICINE IN O NCOLOGY M O P TM INTERVIEW WITH THE INNOVATORS The official publication of Highlights From the 2012 World Cutaneous Malignancies Congress ................................Page 26 CONTINUING MEDICAL EDUCATION ALSO IN THIS ISSUE… • First-Line Afatinib in Advanced EGFR-Positive NSCLC ....................................................Page 11 • Potential Biomarkers for Response to Lenvatinib Identified ....................................................Page 12
-
Upload
the-oncology-nurse -
Category
Documents
-
view
236 -
download
3
description
August 2012 issue of Personalized Medicine in Oncology
Transcript of August 2012, VOL 1, NO 3

Facilitating the Next Generation of Precision Medicine in Oncology ..................................Page 43
Which Breast Cancer Patients Should Receive Adjuvant Chemotherapy? ................Page 52
Incorporating Genomics Into Practice: An Interview With Kimberly J. Popovits ..........Page 18
August 2012
Volume 1 • Number 3
A Peer-Reviewed Journal
www.PersonalizedMedOnc.com© 2012 Green Hill Healthcare Communications, LLC
IMPLEMENTING THE PROMISE OFPROGNOSTIC PRECISION INTO PERSONALIZED CANCER CARETM
REGULATORY ISSUES
BREAST CANCER
PERSONALIZEDMEDICINE INONCOLOGYM
OP
TM
INTERVIEW WITH THE INNOVATORS
The official publication of
��������������� ��� ���������������� ������ �������������� � ���
��
��
Highlights From the 2012 World Cutaneous Malignancies Congress ................................Page 26
CONTINUING MEDICAL EDUCATION
ALSO IN THIS ISSUE…• First-Line Afatinib in Advanced EGFR-Positive NSCLC ....................................................Page 11
• Potential Biomarkers for Response to Lenvatinib Identified ....................................................Page 12

Are you getting the full picture?
At diagnosis of metastatic colorectal cancer (mCRC)
Name: George Age: 58 Cancer: mCRC Specialty: Storyteller Biomarker Status:
Not an actual patient.

Provides information on a patient’s likelihood of response or non-response to
biomarker-directed treatment1
Approximately 2 out of every 3 patients areKRAS wild-type vs mutant5,7 Approximately 5%-9% of colorectal
cancers are characterized by a specific mutation in the BRAF gene7
May help define the patient’s overall prognosis irrespective of therapy1
At diagnosis of mCRC, testing a patient’s tumors for biomarkers can help determine predictive and/or prognostic information1
Colorectal cancer is the 3rd leading cause of cancer death in men and women in the U.S.2
Understanding the patient’s biomarker profile helps define the characteristics of the patient’s disease and their overall prognosis.1 Knowing a patient’s biomarker status at diagnosis may help guide clinical decisions.3,4
Understanding the biomarker pathways involved in mCRC tumorigenesis can help inform appropriate treatment planning.3,5,6
KRAS and BRAF signaling are involved with colorectal tumorigenesis and tumor progression3
The KRAS gene may be mutated or wild-type. When KRAS is mutated, it is permanently switched on, whereas wild-type KRAS protein is activated when the EGFR is stimulated.3,5 Increased BRAF signaling may occur due to mutations in the BRAF gene.5 BRAF mutations are limited to those tumors that do not have KRAS exon 2 mutations.7
EGFR = epidermal growth factor receptor. *In a CLIA-certified laboratory.
References: 1. Tejpar S, Bertagnolli M, Bosman F, et al. Prognostic and predictive biomarkers in resected colon cancer: current status and future perspectives for integrating genomics into biomarker discovery. Oncologist. 2010;15:390-404. 2. American Cancer Society. Cancer Facts & Figures: 2011. http://www.cancer.org/acs/groups/content/@epidemiologysurveillance/documents/document/acspc-029771.pdf. Accessed March 1, 2012. 3. Monzon FA, Ogino S, Hammond EH, et al. The role of KRAS mutation testing in the management of patients with metastatic colorectal cancer. Arch Pathol Lab Med. 2009;133(10):1600-1606. 4. Grossman AH, Samowitz WS. Epidermal growth factor receptor pathway mutations and colorectal cancer therapy. Arch Pathol Lab Med. 2011;135:1278-1282. 5. Krasinskas AM. EGFR signaling in colorectal carcinoma. Pathol Res Int. 2011;2011:1-6. http://www.hindawi.com/journals/pri/2011/932932/cta. Accessed January 6, 2012. 6. Linardou H, Briasoulis E, Dahabreh IJ, et al. All about KRAS for clinical oncology practice: gene profile, clinical implications and laboratory recommendations for somatic mutational testing in colorectal cancer. Cancer Treat Rev. 2011;37(3):221-233. 7. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Colon Cancer V.3.2012. © 2012 National Comprehensive Cancer Network, Inc. All rights reserved. The NCCN Guidelines® may not be reproduced in any form for any purpose without the express written permission of the NCCN. To view the most recent and complete version of the NCCN Guidelines, go online to NCCN.org. NATIONAL COMPREHENSIVE CANCER NETWORK®, NCCN®, NCCN GUIDELINES®, and all other NCCN Content are trademarks owned by the National Comprehensive Cancer Network, Inc. Accessed March 15, 2012.
T E S T T O P L A N
©2012 Bristol-Myers Squibb. All rights reserved. 693US12AB00106 04/12 Printed in USA.
Testing of biomarkers at diagnosis of mCRC is important for treatment planning3,7*
Strongly recommends KRAS genotyping of CRCtumor tissue (either primary tumor or metastases) inall patients with mCRC at the time of stage IV disease diagnosis. Early establishment of KRAS status is appropriate in order to plan for the treatment continuum.7
BRAF genotyping can be considered for patients with tumors characterized by the wild-type KRAS gene. Such testing is currently optional and not a necessary part of decision making.7

PERSONALIZED MEDICINE IN ONCOLOGY4 Volume 1 • No 3 August 2012
August 2012
Volume 1 • Number 3
MOP
New Targeted Therapies and New BiomarkersExplored at ASCO 2012 PAGE 10
First-Line Afatinib in Advanced EGFR-Positive
NSCLC
Potential Biomarkers for Response to Lenvatinib
Identified
Prostate Cancer Roundup PAGE 146-Gene Model Identifies Lower- Versus
Higher-Risk CRPC Patients
Gene Classifiers Predict Risk of Clinical
Progression Following Prostatectomy
CONFERENCE NEWS
Incorporating Genomics Into Practice: An Interview With Kimberly J. Popovits PAGE 18
PMO talks with the President and CEO of
Genomic Health about their approach to
personalized medicine, her inspiration to
work in this field, and the future of cancer
treatment.
PERSONALIZEDMEDICINE INONCOLOGY™
The Global Biomarkers Consortium™
(GBC) is a community of world-
renowned healthcare professionals who
will convene in multiple educational fo-
rums in order to better understand the
clinical application of predictive molec-
ular biomarkers and advanced personal-
ized care for patients.
Save the date for the Second Annual Conference,
October 4-6, 2013Visit
www.globalbiomarkersconsortium.comto register
Who attends the GBC?INTERVIEW WITH THE INNOVATORS
Highlights From the 2012 World Cutaneous Malignancies Congress PAGE 26
The WCMC focuses on advances in the
fields of cutaneous malignancies and
cutaneous T-cell lymphoma.
CONTINUING MEDICAL EDUCATION
��������������� ��� ���������������� ������ �������������� � ���
��
��
OUR MISSIONThe mission of Personalized Medicine in Oncology is to deliver practice-changing informationto clinicians about customizing healthcare based on molecular profiling technologies, eachpatient’s unique genetic blueprint, and their specific, individual psychosocial profile, prefer-ences, and circumstances relevant to the process of care.
OUR VISION Our vision is to transform the current medical model into a new model of personalized care, wheredecisions and practices are tailored for the individual – beginning with an incremental integrationof personalized techniques into the conventional practice paradigm currently in place.
Academic clinical practice
Academic research only
Communityhospital
Private practice
Pharmaceutical industry
Other
6.4%
12.9%
29%
22.6%
12.9%
16.1%

Decode each patient’s tumor—individualize cancer treatment.
DNA mutations. Gene copy number variations and rearrangements. RNA. Protein expression. Each part of cancer biology reveals relevantbiomarker information. Caris Target Now™ examines them all to illuminate a clearer path through your patients’ treatment options.
CARIS TARGET NOW™
JUST GOT SMARTER
NOW REDESIGNED TO BE SMARTER THAN EVER
• New Select panels for � ve common tumor types• Clinical Trials Connector™
• New “small specimen” friendly technologies• Faster turnaround time
The use of the Caris Target Now service, the use or interpretation of any information provided as part of sus ch servicvice,e, andand/or/or ththe se seleelectict on of any drdrugug ageagentsnts isis sosolellely ay at and withinh n ththe de disciscretretionion of the treating physician’s independent medical judgment. The Caris Target Now services are performed by Cariss LiLife fe SciSciencences,es, aa CLICLIA-cA-certi� �ed ed lablaboraoratortory oy operperatiatingng undunder er thethe U.U.S. S. CliClinicnicalalLaboratory Amendment Act of 1988 and in compliance with all relevant U.S. state and federal regulations. None of f thethe CaCarisris TaTargerget Nt Now ow serservicviceses havhave be beeneen rerevieviewedwed byby ththe Ue Unitniteded StaStatestes FoFoododand Drug Administration. Persons depicted are models and used for illustrative purposes only. ©2012 Caris Life Sciences anand ad a� � lialiatestes. . AllAll rirightghts rs reseeserverved. d. CTCTN06N061311312PM2PMOO
VISIT: CarisTargetNow.com
ON- AND OFF-COMPENDIUM DRUG ASSOCIATIONS AND CLINICAL TRIALS
ON-COMPENDIUM DRUG ASSOCIATIONS AND CLINICAL TRIALS
PERSONALIZED MEDICINE IN ONCOLOGY6 Volume 1 • No 3 August 2012
SENIOR VICE PRESIDENT, SALES AND MARKETINGPhilip Pawelko
PUBLISHERSJohn W. Hennessy
Russell [email protected]
DIRECTOR, CLIENT SERVICESLou Lesperance Jr
MANAGING DIRECTORPam Rattananont Ferris
EDITORIAL DIRECTORKristin Siyahian
STRATEGIC EDITORRobert E. Henry
SENIOR COPY EDITORBJ Hansen
PRODUCTION MANAGERMarie RS Borrelli
QUALITY CONTROL DIRECTORBarbara Marino
BUSINESS MANAGERBlanche Marchitto
CIRCULATION [email protected]
Personalized Medicine in Oncology, ISSN 2166-0166 (print); ISSN ap-plied for (online) is published 6 times a year by Green Hill HealthcareCommunications, LLC, 1249 South River Road, Suite 202A, Cran-bury, NJ 08512. Telephone: 732.656.7935. Fax: 732.656.7938. Copy -right ©2012 by Green Hill Health care Com muni cations, LLC. Allrights reserved. Personalized Medicine in Oncology logo is a trademarkof Green Hill Healthcare Communications, LLC. No part of thispublication may be reproduced or transmitted in any form or by anymeans now or hereafter known, electronic or mechanical, includingphotocopy, recording, or any informational storage and retrieval sys-tem, without written permission from the publisher. Printed in theUnited States of America.
EDITORIAL CORRESPONDENCE should be ad dressed to ED-ITORIAL DIRECTOR, Personalized Medicine in Oncology (PMO),1249 South River Road, Suite 202A, Cranbury, NJ 08512. YEARLYSUBSCRIPTION RATES: United States and possessions: individ-uals, $50.00; institutions, $90.00; single issues, $5.00. Orders will bebilled at individual rate until proof of status is confirmed. Prices aresubject to change without notice. Correspondence regarding permis-sion to reprint all or part of any article published in this journal shouldbe addressed to REPRINT PERMISSIONS DEPART MENT,Green Hill Healthcare Communications, LLC, 1249 South RiverRoad, Suite 202A, Cranbury, NJ 08512. The ideas and opinions ex-pressed in PMO do not necessarily reflect those of the editorial board,the editorial director, or the publishers. Publication of an advertise-ment or other product mention in PMO should not be construed asan endorsement of the product or the manufacturer’s claims. Readersare encouraged to contact the manufacturer with questions about thefeatures or limitations of the products mentioned. Neither the edito-rial board nor the publishers assume any responsibility for any injuryand/or damage to persons or property arising out of or related to anyuse of the material contained in this periodical. The reader is advisedto check the appropriate medical literature and the product informa-tion currently provided by the manufacturer of each drug to be ad-ministered to verify the dosage, the method and duration ofadministration, or contraindications. It is the responsibility of thetreating physician or other healthcare professional, relying on inde-pendent experience and knowledge of the patient, to determine drugdosages and the best treatment for the patient. Every effort has beenmade to check generic and trade names, and to verify dosages. Theultimate responsibility, however, lies with the prescribing physician.Please convey any errors to the editorial director.
PUBLISHING STAFF
MOP PERSONALIZED
MEDICINE INONCOLOGY™
REGULATORY ISSUES
INTERVIEW WITHTHE INNOVATORSAn exclusive PMO series
Personalized Medicine in Oncology™is pleased to offer insightful interviews withleaders in oncology about their approach
to personalized medicine.
To watch our interviews, visit www.PersonalizedMedOnc.com/videolibrary
Facilitating the Next Generation of Precision Medicine in Oncology
PAGE 43
Key stakeholders are increasingly considering
new measures to protect and advance innovation
and investment in diagnostics.
Sheila D. Walcoff, JD
BREAST CANCER
Which Breast Cancer Patients Should Receive Adjuvant Chemotherapy? PAGE 52
A number of decision-making tools have
become available to help clinicians and patients
with early cancer discuss the risks and benefits
of getting adjuvant therapy after surgery.

©Copyright 2012 Agendia. All rights reserved. Agendia, MammaPrint, TargetPrint and TheraPrint are registered trademarks of Agendia. BluePrint and SYMPHONY are trademarks of Agendia.
22 Morgan | Irvine | CA 92618 | p: 888.321.2732 | f: [email protected] | www.agendia.com
Now Availible in ParAffIn
Breast Cancer Recurrence Signature ER/PR/HER2 Expression AssayMolecular Subtyping Signature Therapy Gene Assay
Eliminate the ambiguity in genomic test results.
Here’s why:
All 25,000 genes in human genome analyzed
All 7 metastatic pathways included
Over 10,000 patients tested
Validated in 25 clinical studies
The result is SYMPHONY – the only
molecular diagnostic suite that can give you
100% de�nitive results for breast cancer
tumor pro�ling.
Visit agendia.com or call 1-888-321-2732 today.
SYMPHONY™ delivers 100% de�nitive results – every time.

PERSONALIZED MEDICINE IN ONCOLOGY8 Volume 1 • No 3 August 2012
Editor in ChiefAL B. BENSON III, MDNorthwestern UniversityChicago, Illinois
Editorial Board
Breast CancerEDITH PEREZ, MD Mayo ClinicJacksonville, Florida
Hematologic MalignanciesGAUTAM BORTHAKUR, MDThe University of Texas MD Anderson Cancer CenterHouston, Texas
PathologyDAVID L. RIMM, MD, PHDYale Pathology Tissue Services Yale University School of MedicineNew Haven, Connecticut
Drug DevelopmentIGOR PUZANOV, MDVanderbilt UniversityVanderbilt-Ingram Cancer CenterNashville, Tennessee
Lung CancerVINCENT A. MILLER, MDFoundation MedicineCambridge, Massachusetts
Predictive ModelingMICHAEL KATTAN, PHD Case Western Reserve UniversityCleveland, Ohio
Gastrointestinal CancerEUNICE KWAK, MD Massachusetts General Hospital Cancer CenterHarvard Medical School Boston, Massachusetts
MelanomaDOUG SCHWARTZENTRUBER, MD Indiana University Simon Cancer CenterIndianapolis, Indiana
Prostate CancerOLIVER SARTOR, MD Tulane UniversityNew Orleans, Louisiana
SECTION EDITORS
SANJIV S. AGARWALA, MDSt. Luke’s HospitalBethlehem, Pennsylvania
TONY ALBINO, PHDSignal Genetics LLCNew York, New York
GREGORY D. AYERS, MS Vanderbilt University School of MedicineNashville, Tennessee
LYUDMILA BAZHENOVA, MDUniversity of California, San DiegoSan Diego, California
LEIF BERGSAGEL, MDMayo ClinicScottsdale, Arizona
KENNETH BLOOM, MDClarient Inc.Aliso Viejo, California
MARK S. BOGUSKI, MD, PHDHarvard Medical SchoolBoston, Massachusetts
GILBERTO CASTRO, MDInstituto do Câncer do Estado de São Paulo São Paulo, Brazil
MADELEINE DUVIC, MD The University of TexasMD Anderson Cancer CenterHouston, Texas
BETH FAIMAN, PHD(C), MSN, APRN-BC, AOCNCleveland Clinic Taussig Cancer CenterCleveland, Ohio
STEPHEN GATELY, MDTGen Drug Development (TD2)Scottsdale, Arizona
STEVEN D. GORE, MDThe Johns Hopkins University School of MedicineBaltimore, Maryland
K. PETER HIRTH, PHDPlexxikon, Inc.Berkeley, California
HOWARD L. KAUFMAN, MDRush UniversityChicago, Illinois
KATIE KELLEY, MDUCSF School of MedicineSan Francisco, California
MINETTA LIU, MD Georgetown University HospitalWashington, DC
KIM MARGOLIN, MDUniversity of WashingtonFred Hutchinson Cancer Research CenterSeattle, Washington
GENE MORSE, PHARMDUniversity at BuffaloBuffalo, New York
AFSANEH MOTAMED-KHORASANI, PHDRadient PharmaceuticalsTustin, California
NIKHIL C. MUNSHI, MD Dana-Farber Cancer InstituteBoston, Massachusetts
STEVEN O’DAY, MDJohn Wayne Cancer Institute Santa Monica, California
DAVID A. PROIA, PHDSynta PharmaceuticalsLexington, Massachusetts
RAFAEL ROSELL, MD, PHDCatalan Institute of OncologyBarcelona, Spain
STEVEN T. ROSEN, MD, FACP Northwestern UniversityChicago, Illinois
HOPE S. RUGO, MD University of California, San FranciscoSan Francisco, California
DANIELLE SCELFO, MHSAGenomic HealthRedwood City, California
LEE SCHWARTZBERG, MD The West ClinicMemphis, Tennessee
JOHN SHAUGHNESSY, PHDUniversity of Arkansas for Medical SciencesLittle Rock, Arkansas
LAWRENCE N. SHULMAN, MDDana-Farber Cancer Institute Boston, Massachusetts
JAMIE SHUTTER, MDSouth Beach Medical Consultants, LLCMiami Beach, Florida
DARREN SIGAL, MDScripps Clinic Medical GroupSan Diego, California
DAVID SPIGEL, MDSarah Cannon Research InstituteNashville, Tennessee
MOSHE TALPAZ, MDUniversity of Michigan Medical CenterAnn Arbor, Michigan
SHEILA D. WALCOFF, JDGoldbug Strategies, LLCRockville, Maryland
ANAS YOUNES, MDThe University of Texas MD Anderson Cancer CenterHouston, Texas
EDITORIAL BOARD

WWW.PERSONALIZEDMEDONC.COM 9Volume 1 • No 3 August 2012
Letter From the Board
Dear Reader,
Welcome to this issue of Personalized Medicine in Oncology (PMO), the officialpublication of the Global Biomarkers Consortium (GBC). PMO and GBC arededicated to bringing information to physicians that will support the adoption ofpersonalized medicine into clinical practice.
Personalized medicine is more than just the pairing of biomarkers to biologics. Itencompasses all personal patient conditions in engaging the entire cancer patient.Understanding breeds success, and nothing succeeds in cancer like personalizedmedicine. Thus, there is no turning back. What little we know scientifically or in
terms of patient engagement drivers is continually undergoing expansion. PMO is identifying what canhelp the practicing oncologist now by means of personalized medicine techniques and research findings inthe hope of offering patients their best chances for success.
For now, personalized medicine continues to overlap with conventional treatment. The explanation ofpersonalized medicine techniques and findings comprise an essential stimulus to its expansion, and to thatend we are identifying key applications to make this happen.
In addition to print and online media, we are pleased to host the annual GBC conference. Please save thedate for the 2nd Annual Conference of the Global Biomarkers Consortium on October 4-6, 2013, inBoston, Massachusetts. The conference is designed to educate physicians specializing in hematology/oncology, pathology, and genetics on the state-of-the-art advances in our understanding of tumor biomark-ers and their use in the clinical management of a variety of solid tumors and hematologic malignancies.Early bird registration is open for this important conference. To register, or for more information, pleasevisit www.globalbiomarkersconsortium.com.
On behalf of the entire editorial board, thank you for being part of our PMO community.
Sincerely,
Howard L. Kaufman, MDRush UniversityPMO Editorial Board Member
Understanding Personalized MedicineBreeds Success
Howard L. Kaufman, MD

PERSONALIZED MEDICINE IN ONCOLOGY10 Volume 1 • No 3 August 2012
ASCO Annual Meeting
Below are some highlights of presentations at the2012 ASCO Annual Meeting related to targetedtherapies and personalized (precision) medicine.
T-DM1The anti-body drug conjugate T-DM1 significantly
prolonged progression-free survival (PFS) comparedwith standard capecitabine/lapatinib therapy for treat-ment of advanced HER2-positive breast cancer in theEMILIA trial (Abstract LBA1).Median PFS was 9.6 months in the T-DM1 arm ver-
sus 6.4 months with capecitabine/lapatinib, representinga significant difference favoring the antibody conjugate(P<.0001). T-DM1 reduced the risk of progression by35% compared with capecitabine/lapatinib.
For many patients with HER2-positive breast cancer,trastuzumab has been the mainstay of therapy, eitheralone or in combination with other chemotherapy. T-DM1 goes one step better, linking trastuzumab with apotent cytotoxic agent that is a maytansine derivativeusing a stable linker. The novel compound delivers a po-tent cytotoxic agent to antigen-expressing tumor cells,sparing normal tissue.“This antibody conjugate is significantly better than
the current approved combination in keeping the cancerunder control. T-DM1 demonstrated greater efficacy andsafety compared with capecitabine/lapatinib and shouldoffer an important therapeutic option for advancedHER2-positive breast cancer,” said Kimberly L. Blackwell,MD, Duke Cancer Institute, Durham, North Carolina.
EMILIA was a 3-year, phase 3 trial randomizing 978patients to receive either T-DM1 or capecitabine/lapatinib. T-DM1 was better tolerated than capecitabine/lapatinib. Subgroup analysis showed superiority of T-DM1 in all subgroups except those aged 65 years andolder. Overall survival was improved in the T-DM1group, but median overall survival had not been reachedat the time of the ASCO meeting. At 2 years, 65.4% ofthe T-DM1 group was alive compared with 47.5% of thegroup on standard chemotherapy. The incidence of grade 3 or higher adverse events was
40.8% with T-DM1 versus 57% for capecitabine/ lapatinib. The incidence of adverse events leading totreatment discontinuation was 5.9% versus 10.7%, re-spectively. Death due to toxicity was reported for 1 pa-tient in the T-DM1 arm versus 5 in the capecitabine/lapatinib arm. The most common adverse events grade 3or higher in the T-DM1 arm were thrombocytopenia andincreased hepatic enzymes; in the capecitabine/lapatinibarm, diarrhea, hand/foot syndrome, and vomiting.Formal discussant of this trial, Louis M. Weiner, MD,
Georgetown University Lombardi Comprehensive Can-cer Center, Washington, DC, said EMILIA’s results wereconvincing evidence in support of the potent antitumoractivity of T-DM1, which he called a “magic bullet.”
PD-1 Targeted Immune TherapyThe investigational anti–PD-1 antibody (BMS-
936558) achieved objective responses in 20% to 25%of patients with advanced non–small cell lung cancer(NSCLC), melanoma, and renal cell cancer with ac-ceptable safety in a preliminary study reported at ASCO(Abstract CRA2509) and published simultaneously on-line in the New England Journal of Medicine. Preliminarydata suggest that PD-L1 expression on tumor cells is re-lated to response to the anti–PD-1 antibody.“It’s exciting to see this degree of antitumor activity
New Targeted Therapies and New BiomarkersExplored at ASCO 2012Alice Goodman
For many patients with HER2-positive breast cancer, trastuzumab has been themainstay of therapy, either alone or incombination with other chemotherapy.

WWW.PERSONALIZEDMEDONC.COM 11Volume 1 • No 3 August 2012
ASCO Annual Meeting
from a single agent among patients with a range of can-cers that had progressed despite standard therapies. Wewere especially surprised to see activity in nearly 20%of NSCLC patients, who have been historically unre-sponsive to immune-based therapies. These findingsmark what is probably the strongest anti–lung canceractivity observed to date with any immunotherapy,”commented lead author Suzanne L. Topalian, MD, Pro-fessor of Surgery and Oncology at The Johns HopkinsUniversity School of Medicine, Baltimore, Maryland.The PD-1 antibody targets a key pathway in T-cell
activation that inhibits the body’s immune response tocancer. By blocking this pathway, BMS-936558 isthought to reactivate the immune system to attack can-cer cells.The phase 1 trial included 296 patients with disease
progression despite standard therapies who receivedtreatment through February 2012. Cancers includedwere melanoma (104 patients), NSCLC (122 patients),kidney cancer (34 patients), castrate-resistant prostatecancer (17 patients), and colorectal cancer (19 pa-tients). The majority of patients were heavily pretreated;47% received at least 3 prior regimens.Response rates were as follows: melanoma, 28%;
renal cancer, 27%; and NSCLC, 18%. Responses wereobserved in cancers with both squamous and nonsqua-mous histology. Some responses were quite durable; 20of 31 responses lasted for at least 1 year, and several pa-tients were still in response at the time of the ASCOmeeting.Safety was generally acceptable. Side effects were
similar to those reported with other immunotherapies.The most common treatment-related side effects werefatigue, rash, diarrhea, pruritus, decreased appetite, andnausea. Serious (grades 3 and 4) adverse events were re-ported in 14% of patients. Drug-related serious adverseevents occurred in 11%. Three deaths occurred due topulmonary toxicity.Another goal of the study was to find a biomarker for
response. Subanalysis found that expression of a proteincalled PD-L1 on the tumor cell surface correlated withresponse. Response was seen in more than one-third of
patients with PD-L1–positive tumors, while no responsewas seen in patients with PD-L1–negative tumors. Fur-ther studies are planned to evaluate this potential bio-marker of response to BMS-936558.“This drug has broken the ceiling of durable tumor
response rates of 10% to 15%, which is the highest rateof many of the immunotherapy approaches used overthe past 30 years,” wrote Antoni Ribas, MD, PhD, Jons-son Comprehensive Cancer Center at UCLA in LosAngeles, in his editorial in the New England Journal ofMedicine.
First-Line Afatinib in Advanced EGFR-Positive NSCLCFirst-line therapy with afatinib, a novel investiga-
tional oral epidermal growth factor receptor (EGFR) inhibitor, extended PFS compared with standardchemotherapy (pemetrexed/cisplatin) in EGFR-mu-tated advanced NSCLC, and PFS was prolonged evenfurther in patients whose cancers harbored the 2 mostcommon EGFRmutations (Abstract LBA7500). Thesewere the results from the pivotal phase 3 internationalLUX-Lung 3 trial.Afatinib improved PFS by about 4 months in this ad-
vanced disease population, and PFS benefits were almostdoubled with afatinib in patients with 1 of the 2 mostcommon EGFR mutations: del19 or L858R.Afatinib is an irreversible dual EGFR/HER2 in-
hibitor under development for NSCLC with EGFRmu-tations. Afatinib not only blocks EGFR but also blocksthe ErbB family of receptors associated with the EGFRpathway, including HER2 and HER4. In the UnitedStates no therapy is approved by FDA specifically forEGFR mutation–positive lung cancer.“Afatinib appears to be more potent than other
Afatinib improved PFS by about 4 monthsin this advanced disease population, andPFS benefits were almost doubled withafatinib in patients with 1 of the 2 mostcommon EGFRmutations: del19 or L858R.

PERSONALIZED MEDICINE IN ONCOLOGY12 Volume 1 • No 3 August 2012
ASCO Annual Meeting
EGFR-directed therapies because it blocks the molecu-lar pathways that facilitate growth of these cancers morebroadly and effectively. This new oral therapy may helppatients live longer with no disease progression and re-quires fewer office visits than standard chemotherapy,”said principal investigator James Chih-Hsin Yang, MD,National University of Taiwan, Taipei, Taiwan.
The randomized, open-label, phase 3 LUX-Lung 3trial was conducted at 133 sites in 25 countries, and itis the largest phase 3 trial in the first-line setting for EGFR mutation–positive, advanced, metastaticNSCLC; LUX-Lung 3 was also the first trial to usepemetrexed/cisplatin as the comparator arm. Patients(N=345) were randomized 2:1 to afatinib or standardchemotherapy with pemetrexed/cisplatin. Median PFS in the afatinib arm was 11.1 months ver-
sus 6.9 months for standard chemotherapy, representinga 42% reduced risk of progression for those treated withafatinib (P=.0004). About 90% of patients enrolled inthe trial had cancers that harbored del19 or L858R. Inthe subset of patients with these 2 common mutations,median PFS was 13.6 months with afatinib versus 6.9months in the standard chemotherapy arm, representinga 51% reduced risk of progression with afatinib(P<.0001). Overall survival results will be availablewithin the next 2 years.The most common drug-related adverse events asso-
ciated with afatinib included diarrhea (95%), rash(62%), and paronychia (57%). The most common drug-related adverse events in the chemotherapy arm werenausea (66%), decreased appetite (53%), and vomiting(32%). Rates of discontinuation due to adverse eventswere 7.9% in the afatinib arm and 11.7% in thechemotherapy arm.
Potential Biomarkers for Response toLenvatinib IdentifiedAs part of the effort to identify biomarkers of re-
sponse and outcomes in cancers, a phase 2 study of 58patients with differentiated thyroid cancer treated withthe investigational agent lenvatinib identified severalpotential predictive biomarkers of treatment responseand outcomes (Abstract 5518). The study found thatthe combination of RAS and BRAF mutation with baseline vascular endothelial growth factor (VEGF) andANG-2 or treatment-associated changes in FGF-2 and IL-2 level correlated with treatment response tolenvatinib.Lenvatinib is an oral tyrosine multitargeted inhibitor
that targets VEGFR-3, FGFR-4, RET, KIT, andPDGFRβ. In the study, patients received a starting doseof lenvatinib 24 mg once daily in 28-day cycles. Serumwas collected at baseline, day 8, and day 36; multiplebead assays and enzyme-linked immunoabsorbent assaywere used to measure serum concentrations of 47 cy-tokine and antigenic factors (CAFs). Thirty-three geneswith a total of 443 mutations were examined in archivaltumor samples (n=25).The response rate was 50%. Longer PFS on len -
vatinib was correlated with low baseline VEGF andANG-2 (P=.02). Both baseline and changes in CAFlevels showed an association with gene mutation sta-tus. High baseline levels of VEGF were seen in pa-tients with wild-type RAS and BRAF, whereas highbaseline sTIE-2 levels were associated with RASmutation.Increased levels of IL-10 and FGF-2 on day 8 post-
treatment were associated with RAS and BRAF muta-tion. Combining gene mutation status with baselineCAF levels improved prediction of longer PFS on lenva-tinib treatment than gene mutation status alone. Clustermodeling identified a set of CAFs that could predictlonger PFS and greater tumor shrinkage or longer PFSwithout significant tumor shrinkage.Lead author of this abstract was Douglas Wilmot
Ball, MD, The Johns Hopkins University School ofMedicine, Baltimore, Maryland. u
Afatinib appears to be more potent thanother EGFR-directed therapies because itblocks the molecular pathways thatfacilitate growth of these cancers morebroadly and effectively.

Pancreatic Cancer: Progress and ChallengesJune 18-21, 2012Lake Tahoe, NV
An AACR Special Conference on: Chemical Systems Biology: Assemblingand Interrogating Computational Models ofthe Cancer Cell by Chemical PerturbationsJune 27-30, 2012Marriott Copley PlaceBoston, MA
Eleventh Annual AACR International Conference on Frontiers in Cancer Prevention ResearchOctober 16-19, 2012Anaheim, CA
Fifth Conference on the Science of Cancer Health Disparities in Racial/Ethnic Minorities and theMedically UnderservedOctober 27-30, 2012San Diego, CA
EORTC-NCI-AACR International Symposium on Molecular Targets andCancer TherapeuticsNovember 6-9, 2012Dublin, Ireland
An AACR Special Conference on: Post-GWAS Horizons in MolecularEpidemiology: Digging Deeper into the EnvironmentNovember 11-14, 2012Hollywood, FL
An AACR Special Conference on: Tumor Immunology: MultidisciplinaryScience Driving Basic and Clinical AdvancesDecember 2-5, 2012Miami, FL
CTRC-AACR San Antonio Breast Cancer SymposiumDecember 4-8, 2012San Antonio, TX
An AACR Special Conference on: TumorInvasion and MetastasisJanuary 20-23, 2013San Diego, CA
Ninth AACR-Japanese Cancer AssociationJoint Conference: Breakthroughs in Basicand Translational Cancer ResearchFebruary 21-25, 2013Maui, HI
AACR-Society of Nuclear Medicine JointConference on State-of-the-art MolecularImaging in Cancer Biology and TherapyFebruary 27-March 2, 2013San Diego, CA
Please visit www.aacr.org/meetingscalendar for the complete calendar, as conferences are added and updated on a regular basis

PERSONALIZED MEDICINE IN ONCOLOGY14 Volume 1 • No 3 August 2012
Nearly 3000 abstracts were selected for presen-tation at the recent ASCO 2012 AnnualMeeting, many of them related to some aspect
of personalized medicine. Below are some highlights se-lected from the meeting that focus on potential genomicpredictors of aggressive versus indolent disease and onpotential biomarkers.
6-Gene Model Identifies Lower- VersusHigher-Risk CRPC PatientsA 6-gene model was found to discriminate between
lower-risk patients and higher-risk patients with castra-tion-resistant prostate cancer (CRPC) in both a trainingset and a validation study (Abstract 4516). Current mod-els for risk assessment are based on clinical variables andonly offer moderate predictive discrimination for menwith CRPC who have a heterogeneous range of out-comes. Whole blood offers specific advantages as a bio-marker – it is easy to collect, minimally invasive, can bestandardized, and can be repeatedly collected over time.
“We demonstrated that the 6-gene model predictedsurvival,” stated presenting author William Oh, MD,professor at Mount Sinai School of Medicine in NewYork City.Between August 2006 and June 2008, PAXgene
Blood DNA Tubes were used to collect blood prospec-tively from 62 patients for a training set at Dana-FarberCancer Institute, Oh told listeners. Subsequently, theresearchers collaborated with the Memorial Sloan-Ket-tering Cancer Center (MSKCC), New York, for a vali-dation set from 140 patients who had blood samplesbanked between August 2006 and February 2009. Two
samples were eliminated because of poor-quality RNA.After an extensive review of studies in the literature, theresearchers identified 6 candidate genes that would yieldthe best prediction of survival.“When applied to the training set at Dana-Farber, we
found that the lower-risk patients had a median survivalof 34.9 months, while higher-risk patients had a mediansurvival of 7.8 months (P=.0001),” Oh said. The genemodel was superior to the Halabi nomogram variablesbased on data available for 6 of 7 of the variables,namely, alkaline phosphatase, ECOG performance sta-tus, hemoglobin, visceral metastases, prostate-specificantigen (PSA), and Gleason score. Area under thecurve was 0.90 for the 6-gene model and 0.65 for theclinical model.The MSKCC validation set had a median survival of
18.5 months for lower-risk patients and 9.2 months forthe higher-risk group (P<.0001). As with the trainingset, the results were highly significant. The 6-genemodel maintained its prognostic significance when clin-ical variables were added to it. The authors hope thisstudy will provide models to help assist patient counsel-ing and trial stratification.Patient characteristics were typical for patients with
CRPC. Metastatic disease was present in 87% and 90%of the training and validation cohorts, respectively.The study was funded by Source MDx, which is no
longer in business.
Gene Classifiers Predict Risk of ClinicalProgression Following ProstatectomyThe genomic classifier (GC) and the genomic-clin-
ical classifier (GCC) were validated as predictors of clin-ical progression after radical prostatectomy in prostatecancer patients at high risk for disease progression (Ab-stract 4565). Both GC and the GCC were superior to amultivariable clinical classifier (CC) in this regard, sup-porting the promise of applying GCs in guiding decisionmaking following radical prostatectomy.
ASCO Annual Meeting
Prostate Cancer RoundupAlice Goodman
The MSKCC validation set had a mediansurvival of 18.5 months for lower-riskpatients and 9.2 months for the higher-risk group.

WWW.PERSONALIZEDMEDONC.COM 15Volume 1 • No 3 August 2012
Christine Buerki, PhD, of GenomeDx Biosciences,Vancouver, Canada, reported these results, confirmingthat the GC is able to capture the majority of prognosticinformation.The author believes that the lack of biomarkers, be-
yond clinical and pathologic factors, for predicting riskof clinically significant disease is a barrier to the efficientdelivery of adjuvant therapy following prostatectomy.The GC was developed from the Mayo Clinic radical
prostatectomy registry of routine formalin-fixed, paraf-fin-embedded patient specimens.In the case cohort study of 219 patients from the
Mayo Clinic, clinical progression was defined as a posi-tive bone or CT scan following prostatectomy. C-indices(measures of discrimination for model validation) of0.79, 0.82, and 0.70 were found for GC, GCC, and CC,respectively.Multivariable survival analysis revealed that most of
the prognostic information of GCC was derived from theGC, with only a small contribution from Gleason score.GCC, which is a combination of GC and establishedclinical and pathologic variables, had an overall highernet benefit compared with CC over a wide range of deci-sion-to-treat thresholds for the risk of progression. GCemerged as an independent prognostic factor in this study.The utility of GC and GCC in informing decision
making in the adjuvant setting following radical prosta-tectomy will depend on the results of additional studiesin other prostate cancer risk groups.
FDHT and FDG Potential ImagingBiomarkersBoth 18F-16β-fluoro-5α-dihydrotestosterone (FDHT)
and fludeoxyglucose (FDG) positive emission tomogra-phy (PET) are promising candidates for imaging bio-markers in men with metastatic castrate-resistantprostate cancer (mCRPC), as shown by a study designedto determine if FDHT and FDG PET scans are prognos-tic for survival (Abstract 4517). These findings suggestthat more sophisticated imaging, such as FDHT andFDG, may be helpful in managing mCRPC. Current imaging modalities have limited ability to quan-
tify disease burden and assess response to treatment.Researchers at MSKCC in New York City prospec-
tively scanned 170 patients in the FDG arm and 116 inthe FDHT arm. All patients were diagnosed withmCRPC and had evidence of disease progression at timeof the baseline scan.
Presenting author Karen A. Autio, MD, pointed outsome important differences between the 2 imagingmodalities used in the study. FDG images tumor metab-olism but is not tumor specific and assumes that the lesions are glycolytic. FDHT, a structural analog of dihydrotestosterone, has a high affinity for the androgenreceptor and captures its overexpression in bone, softtissue, and viscera. FDHT measures androgen receptorexpression and is prostate specific, but its utility requiresa castrate state.Each patient was assessed for standardized uptake val-
ues (SUV), specifically, SUVmax (ie, the hottest le-sions) or SUVmaxavg (ie, average of the 5 hottestlesions).“FDHTmaxavg and FDGmaxavg were significantly
associated with survival (P=.049 and P=.0007, respec-tively),” Autio stated. “For FDHT, with a hazard ratioof 1.61, we can say that for every log 1 unit increase inSUV, the risk of death increased by 61%,” Autio said.In comparison, the hazard ratio for FDG was 2.54. In amultivariate model, neither FDHT SUV or FDG SUVwas prognostic of survival, and neither tracer wasstrongly associated with SUVmax.FDHT was superior to PSA and Gleason score as a
prognostic marker of survival.Preliminary data from this study indicate that both
FDG and FDHT are linked to clinical outcome and
ASCO Annual Meeting
Preliminary data from this study indicatethat both FDG and FDHT are linked to clinical outcome and have potential utilityas imaging biomarkers in building anevidence database.

PERSONALIZED MEDICINE IN ONCOLOGY16 Volume 1 • No 3 August 2012
have potential utility as imaging biomarkers in buildingan evidence database.
RT-PCR–Based Technique DiscriminatesBetween Indolent and AggressiveProstate CancerReverse transcriptase-polymerase chain reaction
(RT-PCR) provides a reliable measure of gene expres-sion patterns and biological pathways associated withclinically aggressive prostate cancer in radical prostatec -tomy specimens obtained by needle biopsies, accordingto a study conducted at the Cleveland Clinic, which wasconfirmed by a study presented at a Poster Discussion
Session (Abstract 4560). The technique also discrimi-nated between indolent and aggressive prostate cancer.The study supports the potential value of a biopsy-
based genomic assay to guide the decision between im-mediate treatment and active surveillance for patientswith biopsy-diagnosed prostate cancer. The study was pre-sented by Eric A. Klein, MD, Glickman Urological and
Kidney Institute, Cleveland Clinic, Cleveland, Ohio.The study included 92 low-risk and 75 intermediate-
risk patients who were biopsied and underwent radicalprostatectomy between 1999 and 2010. The investiga-tors used a novel design to assess gene expression in thecontext of tumor heterogeneity assessed by needlebiopsy of tissue obtained from radical prostatectomy.The researchers analyzed the expression of 81
prostate cancer–related genes, which were identified ina prior gene discovery study, and normalized to the av-erage of 5 reference genes. Fifty-eight of the 81 discoverystudy genes (72%) also predicted adverse pathologyand/or nonorgan-confined disease when assayed inbiopsy tumor tissue. These included all stromal responseand androgen genes and most (82%) cellular organiza-tion genes. Proportionately fewer proliferation (40%),stress response (29%), and basal epithelial (25%) geneswere associated with an adverse path.After covariate adjustment for clinical T stage, pre-
treatment PSA, and biopsy Gleason score, the re-searchers found that the predictive genes identified inbiopsy specimens at diagnosis also predicted adversepathology in biopsy tumor tissue.An independent prospective study is currently under
way to validate a clinical-grade multigene assay opti-mized for prostate needle core biopsy tissue. The assayis based on an algorithm incorporating the strongestgenes and gene pathways. u
ASCO Annual Meeting
The study supports the potential value of abiopsy-based genomic assay to guide thedecision between immediate treatmentand active surveillance for patients withbiopsy-diagnosed prostate cancer.
We’re just a click away!Please visit us at www.PersonalizedMedOnc.com

PERSONALIZEDMEDICINE IN ONCOLOGYM
OP
��
� ��� ������������ ����������������������������������������������������������
Personalized Medicine in Oncology’s mission is to deliver practice-changing information to cliniciansabout customizing healthcare based on molecular profiling technologies and each patient’s unique genetic blueprint.
Our vision is to transform the old medical model of stratified medicine into a new model of personalized carewhere all decisions and practices are tailored to the individual.
The goal of Personalized Medicine in Oncology is to sensitize practitioners to the performance realities of new diagnostic and treatment discoveries and to clarify molecular profiling technologies as they relate to diagnostic,prognostic, and predictive medicine. PMOwill feature diagnostic and clinical treatment information concerningthese 3 root aspects of personalized medicine in oncology.
Readers are invited to submit articles for consideration in the following categories:
Biologicals in Trial• Exploring the challenges of clinical trial design and patient enrollment
• Presentation of emerging clinical data
Predictive Models and Diagnostics • A look at available diagnostic technologies andimplementation in the community practice setting
Genetics and Biomarkers• Exploring genetic discoveries and impact on predictors of disease and therapeutic response
The Cost of Personalized Medicine• Personalized medicine policy drivers
• Payer coverage of diagnostics and biologics
Genetic Profiling Technologies• What technologies are available to clinicians and consumers and their impact on diagnostic,prognostic, and predictive medicine
In Practice• A practical guide for community-based oncologists discussing clinical applications and strategies for incorporating personalizedmedicine techniques into practice
• Development of treatment algorithms
N=1 • Case studies, patient-reported outcomes, defining treatment goals, partnering with patientsand caregivers
Submit the entire manuscript and a cover letter stating the objectives of the article to [email protected] should follow the Author Guidelines available at www.PersonalizedMedOnc.com.
CALL FOR PAPERS
�����" � ��
� �� �� � �� �

PERSONALIZED MEDICINE IN ONCOLOGY18 Volume 1 • No 3 August 2012
Interview With the Innovators
PMO How do you define personalized medicine inoncology, particularly as it relates to the treatment ofpatients with breast or colon cancer?
Ms Popovits I think one of the best ways to define per-sonalized medicine is when disease happens to you or tosomebody you love. Oftentimes we hear definitions of get-ting the right drug to the right patient in the right dose atthe right time. I think specific to oncology and the areasthat we’re in, breast, colon, and prostate cancer, it’s reallyabout patients understanding their individual disease.
Cancer is many diseases. One tumor is not like an-other tumor, and it’s really important that patients un-derstand the genomic makeup of their particular tumor.We would actually refer to that as the molecular signa-ture of your breast cancer. Knowing how that is differentfrom somebody else’s breast cancer, and by understand-ing that biology, we’re able to better direct treatment.
PMO It appears that personalized medicine in on-cology is a concept that is implemented mainly at aca-demic centers or initiated by a small set of physicians
Incorporating Genomics Into Practice: An Interview With Kimberly J. PopovitsKimberly J. PopovitsChairman of the Board, Chief Executive Officer, and PresidentGenomic Health, Inc
Genomic Health, Inc, located in Redwood City, California,is a global cancer company
founded in 2000. Genomic Health cur-rently offers patients the Oncotype DXBreast Cancer Assay and the OncotypeDX Colon Cancer Assay. Genomic Healthmaintains that the key to effectivelyusing clinical genomics to improve can-cer treatment and outcomes lies in de-termining which sets of genes and geneinteractions affect different subsets ofcancers. Genomic Health studies whichpatterns of gene expression within a tumor are linked to aresponse to cancer therapy, or to the likelihood that thecancer will return or metastasize. The results of these ge-nomic studies and research can then be used to develop
clinically validated assays that providethe genomic profile of an individual’stumor, helping to understand whetherpatients are likely to benefit from andrespond to cancer therapies, or whetherthose patients are likely to experience arecurrence of their cancer. PersonalizedMedicine in Oncology recently had thepleasure of meeting with the Presidentand CEO of Genomic Health, Ms Kim-berly J. Popovits, to discuss GenomicHealth’s approach to personalized med-icine, her inspiration to work in this
field, and the future of cancer treatment. The followingare excerpts from that interview. To view the interview in its entirety, please go to www.PersonalizedMedOnc.com/videolibrary.
Ms Popovits has served as Chairman of the Board of Genomic Health since 2012, Chief Executive Officer and President since2009, and President and Chief Operating Officer since 2002. Prior to joining Genomic Health, Ms Popovits served as SeniorVice President, Marketing and Sales, at Genentech, Inc. During her 15 years at Genentech, she led the commercialization of14 new therapies, including Herceptin. She was named Woman of the Year in 2008 by the Women Health Care Executivesand as one of the Most Influential Women in the Bay Area by the San Francisco Business Times from 2006-2012. MsPopovits holds a bachelor of arts degree in business from Michigan State University.
Kimberly J. Popovits

WWW.PERSONALIZEDMEDONC.COM 19Volume 1 • No 3 August 2012
Interview With the Innovators
who understand the genetic principles behind molecularbiomarkers and how to assess them appropriately. Howcan personalized medicine be made available to patientsmanaged by community oncologists?
Ms Popovits I think one of the most important goalsin oncology is to make sure that all patients have accessto personalized medicine; that all patients have access tospecific information about their own genome, about theirown genetic makeup; and that their family history is in-corporated into their treatment planning.The dilemma we face is that 80% of patients actually
present in the community and about 20% in the aca-demic setting. We cannot assume that everybody isgoing to be sent to an academic center to get their can-cer treatment.There are a couple of barriers in our way right now,
and a big one is education. We need to make sure thatwe are educating all physicians on the new informationthat’s before us right now. We’re in a world today wherewe have an unprecedented amount of data, and the keyis going to be turning these data into really good action-able information for cancer patients. The tools are here,and folks are using the tools in a lot of places, but I don’tthink it’s necessary that every community physicianhave a sequencer on their desktop. What’s important isthat they have access to those tools through other re-sources, tools that they can present to their patients, sothat the information then gets incorporated into treat-ment planning.We have to work together. It’s going to be a collabo-
rative effort, clearly driven by the academic institutionsand the leading centers, but that information has to getto the community setting so that it’s available to all pa-tients who present with cancer and need to have a per-sonalized treatment plan.
PMO Most of us have been touched by cancer insome way. In fact, the inspiration for Genomic Healthcame from founder Randy Scott’s experience in watch-ing a friend diagnosed with cancer in the late 1990s.Can you tell us what brought you to Genomic Healthand about your inspiration to work in this field?
Ms PopovitsWhen I thought about whether to enter
this whole realm of personalized medicine, and in par-ticular Genomic Health, I was working at Genentechand had the wonderful experience of being involved inthe development of very important cancer therapeutics.What had occurred to me at that time was that we hada number of drugs in our pipeline at Genentech thatmight never see the light of day if we couldn’t figure outhow to target them to the patients that would benefit.We saw that first with Herceptin, a very important
drug for the treatment of breast cancer, and it is a drugthat I’m not sure we would have gotten to market if wehadn’t been able to develop a diagnostic test to findthose patients who overexpress HER2.So when the folks at Genomic Health called me in
the very early days and said they had this idea of how wecould better direct a lot of cancer treatment, and specif-ically chemotherapy, it really touched a cord with me interms of the need for it in medicine, but also on a per-sonal level. I think we are all touched by cancer in someway. It’s hard to run into somebody who doesn’t have afamily member or a friend who’s had to make the reallytough decision about whether to get chemotherapy treat-ment. I went through that with my mother about 19years ago, and I am reluctant to say that she remains asurvivor. My dad was less fortunate in that he died 4 years
Oncotype DX testing is conducted in Genomic Health’s clinicallaboratory in Redwood City, CA.

PERSONALIZED MEDICINE IN ONCOLOGY20 Volume 1 • No 3 August 2012
Interview With the Innovators
ago after a long battle with lung cancer. And I lost a verygood friend to breast cancer just Mother’s Day weekendthis year.All of that is motivation to want to make this dif-
ference, and to really bring personalized medicine to areality.
PMOPlease describe how the gene panels for the breastand colon cancer assays were developed and validated.
Ms Popovits The colon cancer and breast cancer as-says are different in the sense that they look at differentgenes. One of the things that’s really important to thinkabout when we look at breast cancer or colon cancer,and now of course we’re looking at prostate cancer aswell, is that all cancers are not driven by the same ge-netic or genomic profiles.
Starting with the breast cancer assay, we asked our-selves a question, can we figure out who those good andbad actors are that come to the party? What are thegood genes and what are the bad genes playing out inbreast cancer? And so we started with a number of genesin breast cancer. It was several hundred genes that westarted with, and then we pared that number down towhat we thought were the most important genes.We are measuring RNA expression with the Onco-
type DX assays, looking at overexpression and underex-pression of genes. With the breast cancer assay we endedup looking at 21 genes, an algorithm was developed, anda Recurrence Score produced.It’s the same thing with colon cancer except it’s a dif-
ferent number of genes, and they’re different genes. Oneof the things that is at play here is that different path-ways impact different cancers. What we have shownboth in breast cancer and in colon cancer, and what wehope to show in prostate cancer as well, is that looking
at a number of pathways is more powerful than just look-ing at 1 pathway or 1 gene alone.
PMOHow does this differ from the DCIS OncotypeDX score?
Ms Popovits The DCIS score that we developed isbased on the same set of 21 genes as the invasive breastcancer assay, but it’s looking at an earlier stage of breastcancer, using a specific algorithm to determine whetherthat disease is likely to recur over a period of time.
PMOHow does the Recurrence Score correlate withthe likelihood of distant recurrence?
Ms Popovits The Recurrence Score predicts the like-lihood of disease aggressiveness, so what we were at-tempting to do when we did the test for invasive breastcancer was to figure out which women had disease thatwould be more aggressive and could potentially benefitfrom more aggressive treatment. And what we discov-ered when we developed that assay, the 21-gene assay,was that not only could we predict which patients had alikelihood of their disease recurring over a 10-year pe-riod, we did subsequent studies to show that we couldalso predict whether those women would benefit fromchemotherapy.We ended up in a situation where we had 50% of
women in a low-risk group, 25% in an intermediate-riskgroup, and 25% in a high-risk group. Even better thanthat, we were able to give an individual score to eachpatient. When we designed the studies initially, we werehoping to be able to identify risk groups, and we werevery pleased that not only could we identify certain riskgroups, we could actually give women an individualscore to show them their likelihood of recurrence. Forexample, if you get a Recurrence Score of 7, that corre-lates to a specific likelihood of recurrence over a 10-yearperiod. We can also tell you if your cancer is likely tobenefit from chemotherapy.One fact that a lot of people are unaware of is that about
100,000 women are diagnosed each year with early-stagebreast cancer, ie, estrogen receptor–positive, node-negativebreast cancer. Most of those women, prior to OncotypeDXbeing available, would have been recommendedchemotherapy based on cancer practice guidelines.
What we have shown is that...looking at anumber of pathways is more powerfulthan just looking at 1 pathway or 1 gene alone.

WWW.PERSONALIZEDMEDONC.COM 21Volume 1 • No 3 August 2012
Interview With the Innovators
What’s unfortunate there is that while most wouldhave been recommended chemotherapy and most wouldhave received it, most would not have benefited, be-cause we know that only 3% to 4% of women withearly-stage breast cancer actually benefit fromchemotherapy. So we’re treating 100 women to find 3or 4 who get some benefit, and that’s what we were try-ing to change.The OncotypeDX assay allows us to tell 50% of these
women that they have very low-risk disease. Their like-lihood of recurrence is very low, and further, we can tellthem that their disease isn’t likely to be impacted bychemotherapy. Conversely, we can tell those womenwho are in the high-risk group that they have a high riskfor disease recurrence, and while that’s not necessarilygood news, the good thing for these women is thatchemotherapy actually will help them a good bit.
PMO How is the DCIS score result different fromthe Recurrence Score result?
Ms Popovits The DCIS score uses the same 21 genesfrom the invasive assay, with a distinct algorithm opti-mized for this earlier cancer, to predict which women withDCIS have more aggressive disease and which have lessaggressive disease. And we were successful in doing that.
PMO Can you estimate how often the results ofthese assays change treatment decisions?
Ms Popovits One of the most important factors inpersonalized medicine, with the onset of the technologyand the amount of data that are available to us today, isreally making these data actionable. We knew thatwhen we presented the breast cancer assay to physicians,and to payers specifically, some of the questions that wewere going to get were, tell me that this is going to makea difference; tell me that patients are not going to getchemotherapy if they don’t need it.One of the biggest fears was that we would introduce
a diagnostic test into this treatment planning or path-way, and that no decisions would change.We have embarked on over 15 decision impact stud-
ies across the United States, and now also outside theUnited States, to really look at what’s happening. Sowhen patients get a Recurrence Score result and they
are at high risk for recurrence or at low risk of recur-rence, are they following that result? The results of those studies have been amazingly con-
sistent. Treatment decisions are changing on the orderof 30% to 40% of the time when the patients have a Re-currence Score in front of them. That’s a significantchange for a payer.
The other thing that we’ve done is to monitorchemotherapy use across different payer systems and dif-ferent clinical settings, and we are definitely seeing a de-crease in the amount of chemotherapy being used as adirect result of the Recurrence Score being available forpatients to consider in their treatment planning.
PMO What would you say to the breast cancer pa-tient who has a low Recurrence Score but wants to ini-tiate cytotoxic chemotherapy as “insurance”?
Ms Popovits Often we are asked if the RecurrenceScore should be the final deciding factor in whether apatient gets chemotherapy. In personalized medicine,there are so many factors that have to be considered inmaking a treatment decision in any disease, but especiallyin cancer.So you’ll factor in the patient history, patient prefer-
ence, tumor size, tumor grade. What we do know is thatthe Recurrence Score is the most powerful predictor.However, it has to be used in context with everything elsethat’s going on in a patient’s world at that given time.People will ask us, well, if I have a high Recurrence
Score, is it really terrible that I decide not to getchemotherapy? Or, I have a low Recurrence Score, butbecause my mom had breast cancer I am just not goingto be comfortable not getting chemotherapy. And mypersonal feeling is that it’s a good decision if it’s made
We were very pleased that not only couldwe identify certain risk groups, we couldactually give women an individual scoreto show them their likelihood ofrecurrence.

PERSONALIZED MEDICINE IN ONCOLOGY22 Volume 1 • No 3 August 2012
Interview With the Innovators
with all of the relevant information in front of you.So if you decide that you want chemo even though
you have a low Recurrence Score, knowing that the lowscore means that you have a very low likelihood of yourdisease recurring, and further, are not going to get very
much of a benefit from chemotherapy, if you understandthat and you’ve been taken through the data and thosefacts, and you still decide that you want to proceed with
chemotherapy, that’s a personal choice, and that to meis personalized medicine.
PMO Regarding the Genomic Health pipeline,you’re hoping to offer genomic assays in prostate cancer,as well as non–small cell lung cancer, renal cell carci-noma, and melanoma. Regarding an assay for prostatecancer, a test that could provide insight into the indi-vidual biology and behavior of newly diagnosed prostatecancers would be helpful in treatment planning forprostate cancer patients and their physicians, particu-larly to identify patients who are at low risk of diseaseprogression and thus would be ideal candidates for closemonitoring. Where are you in the process of bringingthis assay to patients?
Ms Popovits We have a really exciting pipeline atGenomic Health; we started in breast cancer, and wemoved into colon cancer. I’m happy to say that we havehelped over 300,000 patients make really importanttreatment decisions, but each year over 1.6 million pa-tients are diagnosed with cancer in the United Statesalone.The other big cancer that we haven’t tackled yet is
prostate cancer. We have a validation study under way.We expect to be able to launch that test in 2013, shouldwe be successful in this study, the results of which wehope to be able to announce toward the end of this yearor early next year.The need in prostate cancer is very similar to the
need in breast cancer and colon cancer. Well over200,000 men are diagnosed each year. Most are facedwith a very important decision around how to handletheir disease. Many opt for aggressive surgery, and thatsurgery has very significant lifelong side effects that in-clude incontinence and impotence, which will dramat-ically impact their life.We know prostate cancer is unlikely to present future
problems for most men. Ninety percent of men shoulddo fine with no treatment at all, yet we’re in a situationtoday where 90% of men are actually getting fairly ag-gressive treatment.What we’re really hoping to answer in prostate can-
cer is whether we can tell men that they can be com-
Genomic Health clinical laboratory scientists preparingpatient samples.
What we do know is that the RecurrenceScore is the most powerful predictor.However, it has to be used in context witheverything else…

WWW.PERSONALIZEDMEDONC.COM 23Volume 1 • No 3 August 2012
Interview With the Innovators
fortable that they have a very low-risk disease, and thatthey should be able to monitor that disease accordingto how they and their physician decide to monitor it,but there’s no need for them to go and get aggressivesurgery or treatment at this point.
PMO Given the high incidence of breast, colon,prostate, and lung cancers, will it make sense for GenomicHealth to develop assays that impact smaller patient pop-ulations, such as melanoma or other tumor types?
Ms Popovits There’s a number of things that we arereally excited about getting into as we move forward.Prostate cancer is the big focus right now as we extendour pipeline, but as you know, there are many cancersthat we haven’t touched yet, including melanoma andovarian and bladder cancer. Those are all cancers thatwe’re interested in.What we have started with are the cancers that have
a very low likelihood of presenting significant risks topatients, so it’s early-stage breast cancer, it’s early-stagecolon cancer, it’s prostate cancer. In some of the othercancers that often get detected at a little later stage, ourinterest is to maybe look at therapeutic response, lookat targeted therapies and try to determine if we can doa better job of helping patients choose a particular drug,given that we know that their cancers perhaps are a lit-tle bit more aggressive. So, yes, we’re interested in moving toward other can-
cers, but right now the major ones that we have on ourplate – breast, colon, and prostate cancer – will be ourfocus for the near term. We really hope to be able to saythat we are with patients on their journey; to be able tobe involved in looking at predisposition to cancer, look-ing at diagnosis of cancer, looking at drug monitoringthrough cancer, so that we stay with patients throughtheir entire journey of cancer and cancer treatment.
PMO Genomic Health is transitioning from an RT-PCR [reverse transcriptase-polymerase chain reaction]platform to next-generation sequencing as the basis fordevelopment of its future cancer diagnostic assays. Canyou describe the opportunities and challenges associatedwith this transition?
Ms Popovits This is a really exciting time in the field
of genomics because of how the technology has evolved,and we’re very interested in using next-generation se-quencing, specifically to discover more about the biol-ogy of cancer. We have been using the next-generationsequencing platform in our research area for a numberof years now, and what we’re finding is that we’re ableto see the biology of disease even better than we everhave using RT-PCR as our platform.
As we further our work with next-generation se-quencing, we’re uncovering more and more genes thatare these good and bad actors in cancer, and certainlywe’re going to use this platform to develop more power-ful assays in the future to help treatment decisions forpatients with cancer.
PMO It seems that education of providers, pharma-cists, payers, and patients is vital in achieving personal-ized medicine in oncology. What efforts is GenomicHealth making in educating these stakeholders?
Ms Popovits Education is clearly going to be the cor-nerstone of personalized medicine being successful. Ge-nomic Health has put a tremendous amount of resourcesinto education – educating physicians, payers, and pa-tients. We have worked very closely with the advocacycommunities, and we knew going in that it was going tobe very difficult to move a test like Oncotype DX intostandard of care if we didn’t have payers on board, if weweren’t able to demonstrate that the test was making adifference in treatment planning. Getting payers onboard, getting physicians to embrace the concept of per-sonalized medicine, the understanding of genomics, andhow to present genomics to their patients has been very,very important. Again, we have worked closely with advocacy com-
munities and done a number of educational programs.
Ninety percent of men should do fine withno treatment at all, yet we’re in a situationtoday where 90% of men are actuallygetting fairly aggressive treatment.

PERSONALIZED MEDICINE IN ONCOLOGY24 Volume 1 • No 3 August 2012
Interview With the Innovators
We’re very focused on working with the opinion leaders,both in the academic and in the community setting, tomake sure that this information is available, and to
make sure that we’re doing our job in promoting the ed-ucation around genomics to make sure that personalizedmedicine is successful in the future.
PMO Can you describe the corporate culture of Genomic Health?
Ms PopovitsWell, I’m probably a little biased as the
CEO, but Genomic Health is a pretty special place towork. We have nearly 600 employees now spread acrossthe world, all drawn together with a single purpose. Wereally want to change the way cancer is treated. Wewant to change the way that patients are presented in-formation. We want to change the way physicians usediagnostic tools. We want to change the way molecularpathology is incorporated into cancer treatment. Youcan feel that purpose here every day in our hallways,which makes this a very special place to work. It’s some-thing that I personally guard very carefully. You’ll see pictures of patients in our hallways, you’ll
hear stories of patients at our all-employee meetings be-cause patients are at the center of all we do.Every test result that goes out of our door makes a
significant impact in the life of somebody, and I don’tever want people to forget that. u
We’re very focused on working with theopinion leaders, both in the academicand in the community setting, to makesure that this information is available...
���� ���������� �������� � ������ ����
July 26-28, 2013
Hyatt Regency La Jolla • at Aventine3777 La Jolla Village Drive • San Diego, California
��
• Melanoma• Basal Cell Carcinoma • Cutaneous T-Cell Lymphoma
• Squamous Cell Carcinoma • Merkel Cell Carcinoma
SECOND ANNUAL CONFERENCE
✓
WWW.PERSONALIZEDMEDONC.COM 25Volume 1 • No 1 May 2012
The Next Generation in Oncologic Care
Join us on our journey to realizethe tremendous possibilities ofimproving cancer prevention,diagnosis, and treatment througha new medical model of personalized care.
Where are you on the path?
www.PersonalizedMedOnc.com PMOHouseAd1
MOP PERSONALIZED
MEDICINE IN ONCOLOGY TM
Implementing the Promise of Prognostic Precision into Personalized Cancer CareTM
TM
TM
The official publication of
Global biomarkers ConsortiumClinical Approaches to Targeted Technologies
PERSONALIZED MEDICINE IN ONCOLOGY26 Volume 1 • No 3 August 2012
The World Cutaneous Malignancies Congress,which took place in April 2012 in Montreal,Canada, focused on advances in the fields of cu-
taneous malignancies (ie, malignant melanoma, basal cellcarcinoma) and cutaneous T-cell lymphoma, including bi-ology, pathology, staging, personalized therapy, mainte-nance therapy, novel agents, and ongoing research.
MelanomaEpidemiology: Hereditary Plus Environmental Risk FactorsJulia Newton-Bishop, MD, from the University of
Leeds in the United Kingdom, presented a talk called,“Cutaneous Malignancies: at the Intersection of Genesand the Environment,” in which she discussed what ge-netic epidemiology tells us about the molecular biologyof melanoma and thus about prevention.Melanoma is predominantly genetic; it’s essentially
a cancer of fair-skinned people. Within those groupswith a fair complexion, hereditary factors (eg, red hair,numerous moles, and the propensity to sunburn) con-tribute to risk. However, environmental factors are im-portant because when people with these phenotypeshave immigrated to sunny countries, like Australia and
Continuing Medical Education
Highlights From the 2012 World CutaneousMalignancies CongressTeresa Petrella, BSc, MD, MSc, FRCPCUniversity of Toronto, Toronto, Ontario, Canada
Kim A. Margolin, MD, FACPUniversity of Washington, Seattle, Washington
SponsorsThis activity has been planned and implemented in accordance withthe Essential Areas and policies of the Accreditation Council for Con-tinuing Medical Education (ACCME) through the joint sponsorship ofthe University of Cincinnati, Medical Learning Institute, Inc., Center ofExcellence Media, LLC, and Core Principle Solutions, LLC. The Univer-sity of Cincinnati is accredited by the ACCME to provide continuingmedical education for physicians.
Physician Credit DesignationThe University of Cincinnati designates this enduring material activity for amaximum of 1.25 AMA PRA Category 1 Credits™. Physicians should onlyclaim the credit commensurate with the extent of their participation in theactivity.
Registered Nurse DesignationMedical Learning Institute, Inc.Provider approved by the California Board of Registered Nursing,Provider Number 15106, for 1.25 contact hours.
Registered Pharmacy DesignationMedical Learning Institute (MLI) is accredited by the Accredita-tion Council for Pharmacy Education (ACPE) as a provider of con-
tinuing pharmacy education. Completion of this activity provides for 1.25contact hours (0.125 CEUs) of continuing education credit. The universalactivity number for this activity is 0468-9999-12-025-H01-P.
Commercial Support AcknowledgmentThis activity is supported by an educational grant from Amgen Inc.
Target AudienceThis activity was developed for medical and surgical oncol-ogists, dermatologists, radiation oncologists, nurse practitioners, nurses, physician assistants, pharmacists, and other healthcare professionals involved in the treatment of patients with cutaneous malignancies.
Educational ObjectivesAfter completing this activity, the participants should be better able to:• Review the molecular biology and pathogenesis of cutaneous ma-lignancies as it relates to treatment of CTCL, BCC, or malignantmelanoma
• Compare risk stratification of patients with cutaneous malignan-cies, and how to tailor treatment based on patient and tumor characteristics
• Summarize a personalized treatment strategy that incorporates cur-rent standards of care and emerging treatment options for therapyof patients with cutaneous malignancies
CME/CE Information
To receive credit, complete the posttest at www.mlicme.org/P11080.html.

WWW.PERSONALIZEDMEDONC.COM 27Volume 1 • No 3 August 2012
Instructions for CreditThere is no fee for this activity. To receive credit after reading thisCME/CE activity in its entirety, participants must complete the posttestand evaluation. The posttest and evaluation can be completed onlineat www.mlicme.org/P11080.html. Upon completion of the evaluationand scoring 70% or better on the posttest, you will immediately receiveyour certificate online. If you do not achieve a score of 70% or betteron the posttest, you will be asked to take it again. Please retain a copyof the Certificate for your records.
DisclosuresBefore the activity, all faculty and anyone who is in a position to havecontrol over the content of this activity and their spouse/life partnerwill disclose the existence of any financial interest and/or relationship(s)they might have with any commercial interest producing healthcaregoods/services to be discussed during their presentation(s): honoraria,expenses, grants, consulting roles, speakers bureau membership, stockownership, or other special relationships. Presenters will inform par-ticipants of any off-label discussions. All identified conflicts of interestare thoroughly vetted by University of Cincinnati and Medical LearningInstitute, Inc. for fair balance, scientific objectivity of studies mentionedin the materials or used as the basis for content, and appropriatenessof patient care recommendations.
Planners and Managers DisclosuresRick Ricer, MD, UC CME Content Reviewer, has nothing to disclose.Kathyrn Gada, MSN, MLI Peer Reviewer, has nothing to disclose.Teresa Haile, RPh, MBA, MLI Peer Reviewer, has nothing to disclose.
Faculty DisclosuresKim A. Margolin, MD, FACP, is on the advisory board for Genentechand Roche. Teresa Petrella, BSc, MD, MSc, FRCPC, is on the advisory board forBristol-Myers Squibb, GlaxoSmithKline, Merck, and Roche; is a con-sultant for GlaxoSmithKline, Merck, and Roche; and is on the speakersbureau for Merck and Roche.
The associates of University of Cincinnati, Medical Learning Institute,Inc., the accredited providers for this activity, Center of ExcellenceMedia, LLC, and Core Principle Solutions, LLC, do not have any finan-cial relationships to products or devices with any commercial interestrelated to the content of this CME/CE activity for any amount duringthe past 12 months.
DisclaimerThe information provided at this CME/CE activity is for continuing ed-ucation purposes only and is not meant to substitute for the independ-ent medical judgment of a healthcare provider relative to diagnosticand treatment options of a specific patient’s medical condition. Rec-ommendations for the use of particular therapeutic agents are basedon the best available scientific evidence and current clinical guide-lines. No bias toward or promotion for any agent discussed in this pro-gram should be inferred.
Estimated time to complete this activity: 1.25 hoursInitial Release Date: August 17, 2012Expiration Date: August 17, 2013
To receive credit, complete the posttest at www.mlicme.org/P11080.html.
New Zealand, the risk is greatest. So both ultraviolet exposure and genes are important determinants ofmelanoma risk.The first progress in understanding the molecular bi-
ology of melanoma came from genetic studies of familialmelanoma, which showed that members of a family inthe United Kingdom with many cases of melanomahave an inherited germline mutation in the CDKN2Agene,1 which encodes the tumor suppressor protein p16and also a second tumor suppressor protein – p14ARF.Additional mutations that provide more informationabout the biology of melanoma are slowly being discov-ered. For example, in very rare families, the susceptibil-ity to melanoma is due to mutations in the CDK4 gene,2
and recently a mutation in BAP1 has been reported infamilies with ocular and cutaneous melanoma.3 Theseare genes with high penetrance and a lower environ-mental contribution to risk, but they provide informa-tion about the biology.
Familial mutations explain only a small proportionof melanoma cases. In routine clinical practice, only 2%of melanoma patients will have a CDKN2A mutation(M Harland, unpublished data, 2012). Even when non-
CME/CE Information (continued)
Teresa Petrella, BSc, MD, MSc, FRCPC
FACULTY CHAIRS
Kim A. Margolin, MD, FACP

PERSONALIZED MEDICINE IN ONCOLOGY28 Volume 1 • No 3 August 2012
selected patients present with a family history of 2 ormore additional cases, the majority (88%) will not haveCDKN2Amutations. Mutations are most likely to con-fer susceptibility if the patient has 3 or more primarymelanomas or has more than 1 primary and a family his-tory (M Harland, unpublished data, 2012). The geneticbasis of susceptibility to melanoma remains unknown in30% to 40% of families featuring 4 or more cases!4
The questions remain: What underlies susceptibilityin the rest of the melanoma cases? Is it due to a cluster-ing of lower-risk genes and environmental exposures?Mutations in high-risk genes have yet to be identified.Recently, however, a major international study identi-fied a novel “boutique” mutation that appears to in-crease the risk of both inherited and sporadic cases of
melanoma.5 This germline mutation occurs in the geneencoding MITF, a transcription factor that controls theexpression of several important proteins – some relatedto pigmentation – in melanocytes, the melanoma pre-cursor cells.One puzzling statistic for those studying the epidemi-
ology of melanoma is that outdoor workers do not havean increased risk of melanoma over otherwise similarindividuals who do not work in the sun. Also, a rela-tionship between solar exposure and the risk ofmelanoma has not been demonstrated. In an effort tobetter understand the contribution of the sun to risk ofmelanoma, Newton-Bishop and colleagues performeda pooled analysis of 15 case-control studies correlatingpatterns of sun exposure, sunburn, and solar keratoses(3 studies) with melanoma risk.6 They found thatmelanoma is essentially a cancer of intermittent sun ex-posure rather than of chronic sun exposure. Data froma more recent case-control study by the same investi-gators indicate that paradoxically, sun exposure may beprotective under selected circumstances (Table 1).7 Forexample, individuals who had moderate weekend sunexposure (ie, over 5 hours outdoors on Saturdays andSundays) actually had a lower risk of melanoma. An-other conundrum is the relationship between sun ex-posure and the presence of a large number of nevi(moles). In another study, Chang and colleagues foundthat nevi are strongly related to sunny holidays, but notto sunburn history.8 The researchers concluded thatwhile sunburn history is a robust risk factor formelanoma in all studies, the relationship between sunexposure (and ultraviolet A vs ultraviolet B wavelengthexposure) and risk may be different for “the nevusroute” to melanoma.To investigate genes that explain melanoma risk in in-
dividuals who do not have a family history of melanoma,genome-wide association studies have been conducted bythe Melanoma Genetics Consortium, and 15 genes (in-cluding pigment genes, nevus genes, and some genes re-lated to DNA repair pathways but not associated withat-risk phenotype) have now been identified as low- tomedium-penetrance susceptibility genes.9-11
Continuing Medical Education
OR (95% CI) Factor Controls Cases (adjusted age/sex)
Sunburn ≥20
Never 315 (68%) 511 (58%) 1
At least once 147 (27%) 365 (42%) 1.56 (1.23-1.99)
Average holiday exposure (hours/year)
≤46.2 167 (34%) 345 (38%) 1
46.2-71.3 161 (33%) 259 (28%) 0.75 (0.57-0.98)
>71.3 163 (33%) 312 (34%) 0.87 (0.66-1.15)
Average weekend exposure warm months (hours/day)
≤4 168 (34%) 377 (42%) 1
4.0-5.0 164 (33%) 262 (29%) 0.72 (0.55-0.94)
>5.0 161 (33%) 262 (29%) 0.67 (0.50-0.89)
OR indicates odds ratio.
Table 1. Associations Between Sun Exposure andMelanoma Risk7
What underlies susceptibility in the rest ofthe melanoma cases? Is it due to aclustering of lower-risk genes andenvironmental exposures?

WWW.PERSONALIZEDMEDONC.COM 29Volume 1 • No 3 August 2012
Molecular Alterations in MelanomaBoris C. Bastian, MD, from the University of Cali-
fornia San Francisco School of Medicine, explained thatmelanoma is not a single disease entity; there are differ-ent genetically distinct types of melanoma (Table 2)that differ in their anatomic distribution, age of onset,relationship to ultraviolet radiation, and patterns of so-matic mutations.12 In fact, Bastian pointed out that thestatement “melanoma is primarily a disease of light-skinned people” is only partially true, because although2 genetically distinct forms of melanoma are very com-mon in light-skinned individuals, other types ofmelanoma unrelated to sun exposure occur in dark-skinned individuals. The anatomic distribution of pri-mary melanoma differs between light- and dark-skinnedindividuals. While melanomas manifest on the inter-mittently or chronically sun-exposed skin in light-skinned individuals, dark-skinned people typically gettheir melanomas on acral sites that are not exposed toultraviolet light, ie, the palms, soles, nails, mucosa, andoccasionally, the eye, where it is known as uvealmelanoma.13
The appearance of a lesion on a patient’s skin orunder the microscope is linked to the genetic alterationsfound in its cells. For example, a mutation in the BRAFgene is very common in melanomas originating on skinthat is intermittently exposed to the sun but withoutpathologic evidence of chronic sun damage. Mutationsin KIT occur in a subset of patients with melanoma orig-inating on the hands, the soles of the feet, and the nails(about 10% with c-KITmutations). Around 25% of pa-tients with melanoma originating in the mucous mem-branes of the oral and nasal cavities or the urogenitaltract have a c-KIT mutation, and a small percentage ofpatients with chronically sun-damaged skin, usuallyolder individuals, also have 1 of several c-KITmutationsacting as “drivers” in their melanoma pathogenesis andpossible therapeutic targets.14 NRAS is another onco-gene that is mutated in ~15% of melanomas, althoughalmost never in the same melanomas that harbor aBRAF mutation. For almost half of the cases ofmelanomas, a specific oncogenic “driver” mutation
or genetic aberrancy has not yet been identified.Another type of melanoma is uveal melanoma,
which is the most common intraocular cancer. It is es-timated that 40% of uveal melanomas contain muta-tions in GNAQ, which encodes an alpha subunit ofheterotrimeric G proteins that act downstream of G pro-tein–coupled receptors. A recent study found that 83%of uveal melanomas had somatic mutations in GNAQor GNA11, a closely related gene, concluding that the2 genes appear to be major contributors to uvealmelanoma.15
Thus, mutually exclusive oncogenic mutations inmelanomas involving NRAS, BRAF, KIT, andGNAQ/GNA11 have been identified that provide anew way to molecularly classify melanoma. In this newclassification method, the biologically distinct subsetsshare a common oncogenic mechanism, behave clini-cally in a similar fashion, and require similar clinicalmanagement.
Continuing Medical Education
• Superficial spreading melanoma
• Nodular melanoma
• Lentigo maligna melanoma
• Desmoplastic melanoma
• Nevoid melanoma
• Acral lentiginous melanoma
• Mucosal melanoma
• Uveal melanoma
• Melanoma of childhood
• Melanoma arising from giant congenital nevus
• Melanoma arising from a blue nevus
• Persistent melanoma
Table 2. World Health Organization Classification of Melanoma12
Around 25% of patients with melanomaoriginating in the mucous membranes ofthe oral and nasal cavities or theurogenital tract have a c-KITmutation...

PERSONALIZED MEDICINE IN ONCOLOGY30 Volume 1 • No 3 August 2012
Implications for Testing and TherapyMichael Davies, MD, PhD, from the University of
Texas MD Anderson Cancer Center in Houston, Texas,then discussed, among other topics, the implications ofthe molecular heterogeneity of melanoma on testingand therapy. He began by summarizing the frequencies
of each of the mutations seen in each ofthe melanoma subtypes (Table 3).Davies and colleagues recently pub-
lished their current recommendations formolecular testing in patients who presentwith advanced melanoma (Table 4).17
However, in the future, multipanel testingwill become available, and it will no longerbe necessary to select individual tests.Finally, Davies discussed the implica-
tions of this molecular information ontargeted therapies for melanoma. Thediscovery of BRAF, NRAS, PTEN, andc-KIT mutations in melanoma has sup-ported the development of a variety of
targeted therapies against these proteins and relatedpathways, but approximately 30% of melanoma patientshave no detectable abnormality in these genes. In orderto develop therapeutic approaches for these patients, itwill be necessary to determine if their tumors are acti-vating similar pathways, or if they are dependent oncompletely different signaling cascades.17
Update on Pegylated Interferon in AdjuvantMelanoma TherapyAlexander Eggermont, MD, PhD, Directeur Général
at the Institut de Cancérologie Gustave Roussy in Paris,France, discussed the results of a post hoc meta-analysisof 2 phase 3 adjuvant trials: European Organisation forResearch and Treatment of Cancer (EORTC) trial18952 (intermediate doses of interferon α-2b [IFN] vsobservation in stage IIb/III patients) and EORTC 18991(pegylated [PEG]-IFN vs observation in stage III pa-tients) in melanoma.18 Both trials were stratified forstage (microscopic nonpalpable nodal involvement vspalpable nodal relapse) as well as for the presence of ul-ceration in the primary melanoma.The results of the meta-analysis showed that patients
with stage IIb/III N1 melanoma benefited significantlyfrom IFN or PEG-IFN treatment, while patients withstage III N2 disease did not. Also, patients with an ul-cerated primary tumor benefited significantly from ad-
Continuing Medical Education
Testing Recommendations
Subtype of Melanoma First Step Second Step
Cutaneous (without chronic sun damage) BRAF ± NRAS KIT
Cutaneous (with chronic sun damage) BRAF ± NRAS KIT
Acral BRAF, KIT ± NRAS –
Mucosal BRAF, KIT ± NRAS –
Uveal Gene expression profiling or monosomy 3 determination* –
Melanoma from anunknown primary BRAF, NRAS KIT, GNAQ,
GNA11, monosomy 3 *Tests for metastatic risk.
Table 4. Molecular Testing in Melanoma ClinicalSubtypes17
Melanoma Subtype
Cutaneous Cutaneous Mutations Without Chronic With Chronic
Sun Damage Acral Mucosal Sun Damage UvealBRAFmutations 50% 20% 3% 5% 0NRASmutations 20% 10% 5% 10% 0KITMutations ~1% 20%-40% 20%-40% 20%-40% 0GNAQmutations 0 0 0 0 45%GNA11mutations 0 0 0 0 35%
Table 3. MAPK Pathway Mutations: Prevalence by Site16

WWW.PERSONALIZEDMEDONC.COM 31Volume 1 • No 3 August 2012
juvant IFN or PEG-IFN therapy, while patients with anonulcerated primary tumor did not. Patients with bothfavorable stage (IIb and III N1) and ulcerated primarytumor benefited greatly (hazard ratios [HRs] 0.56-0.69)with regard to relapse-free survival, distant metastasis-free survival, and overall survival. Patients with stage IIIN2 disease did not derive significant benefit for any endpoint, even when they had an ulcerated primary tumor.The authors concluded that both tumor stage and ulcer-ation were predictive factors for the efficacy of adjuvantIFN/PEG-IFN therapy.
Cytotoxic T-Lymphocyte–Associated Antigen 4 BlockadeCaroline Robert, MD, PhD, from the Service de Der-
matologie et INSERM at the Institut Gustave Roussy inVillejuif, France, discussed ipilimumab, a fully humanmonoclonal antibody (IgG1) that blocks the activity ofcytotoxic T-lymphocyte–associated antigen 4. Ipilimumabhas been approved by the FDA for the treatment of unre-sectable or metastatic melanoma. Ipilimumab was studiedin 2 phase 3 trials – 1 in previously treated patients19 and1 in treatment-naive patients.20 In the first study, ipilim -umab, administered with or without a glycoprotein 100(gp100) peptide vaccine, was compared with gp100 alonein 676 HLA-A*0201–positive patients with previouslytreated unresectable stage III or IV metastatic melanomawhose disease had progressed while they were receivingtherapy.19 Patients were randomly assigned in a 3:1:1 ratioto receive ipilimumab plus gp100 (403 patients), ipilim -umab alone (137), or gp100 alone (136). Ipilimumab, ata dose of 3 mg/kg body weight, was administered with orwithout gp100 every 3 weeks for up to 4 treatments (in-duction). The median overall survival (Figure 1) was 10.0months among patients receiving ipilimumab plus gp100,compared with 6.4 months among patients receivinggp100 alone (HR for death, 0.68; P<.001). The medianoverall survival with ipilimumab alone was 10.1 months(HR for death in the comparison with gp100 alone, 0.66;P=.003). No difference in overall survival was detectedbetween the ipilimumab groups (HR with ipilimumab plusgp100, 1.04; P=.76).
In the second study, ipilimumab (10 mg/kg) plusdacarbazine versus dacarbazine plus placebo was studiedin 502 patients with previously untreated metastaticmelanoma. Overall survival (Figure 2) was significantlylonger in the group receiving ipilimumab plus dacar-bazine than in the group receiving dacarbazine plusplacebo (11.2 vs 9.1 months), with higher survival rates
Continuing Medical Education
Figure 1. Overall Survival in Pretreated PatientsReceiving Ipilimumab 3 mg/kg With or Withoutgp10019
Study Group
Ipilimumab Ipilimumab Alone Plus gp100
Adverse Reaction (n=131) (n=380)Enterocolitis 7% 7%EndocrinopathyHypopituitarism 4% 1%Adrenal Insufficiency – 1%
Dermatitis 2% 3%Hepatotoxicity – 2%Hepatitis 1% –Neuropathy 1% –Nephritis 1% –Eosinophilia 1% –Pneumonitis – <1%Meningitis – <1%Pericarditis – <1%gp indicates glycoprotein.
Table 5. Severe to Fatal Immune-Mediated Adverse Reactions Reported With Ipilimumab19
gp indicates glycoprotein; Ipi, ipilimumab.

PERSONALIZED MEDICINE IN ONCOLOGY32 Volume 1 • No 3 August 2012
in the ipilimumab-dacarbazine group at 1 year (47.3%vs 36.3%), 2 years (28.5% vs 17.9%), and 3 years(20.8% vs 12.2%) (HR for death, 0.72; P<.001).20
Brain metastases commonly develop in patients withmelanoma and are a frequent cause of death of patientswith this disease. Ipilimumab was also studied in anopen-label phase 2 trial in 72 patients with melanomaand brain metastases.21 Results showed that ipilimumabhas activity in some patients with advanced melanomaand brain metastases, particularly when metastases aresmall and asymptomatic.Toxicity, including severe to fatal immune-mediated
adverse reactions, was a serious problem in the ipilim -
umab studies (Table 5).19 The most common adversereactions seen with ipilimumab are listed in Table 6. Ipilimumab therapy was discontinued for adverse reac-tions in 10% of patients.19
The benefit/risk ratio associated with ipilimumab canbe optimized either by increasing the efficacy or by theselection of the patients for their likelihood of benefitfrom this treatment. It may be possible to enhance an-titumor activity by modifying the dosing regimen or bycombining therapies (such as ipilimumab plus vemu-rafenib), but none of these approaches can be recom-mended until clinical trials have shown a safe andeffective improvement over what is currently approved.Selection of patients involves increasing the under-standing of tumor/host/therapy interactions, which areunder active investigation and likely to yield insightsover the next few years.
Basal Cell CarcinomaEpidemiology and EtiologyDirk Schadendorf, MD, PhD, Director and Chair of
the Department of Dermatology Skin Cancer Center atthe University Hospital Essen, Essen, Germany, beganhis presentation by reviewing the epidemiology of basalcell carcinoma. The annual global incidence of non-
Continuing Medical Education
Figure 2. Overall Survival in Previously Untreated Patients Receiving Ipilimumab 10 mg/kgWith Dacarbazine20
Patie
nts
Surv
ivin
g (%
)
100
80
90
70
60
40
30
10
50
20
00 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 42 44 46 4840
Months
Placebo–dacarbazine
Ipilimumab–dacarbazine
P
CensoredCensored
Study Group
Ipilimumab Ipilimumab Adverse Alone Plus gp100 gp100 AloneReaction (n=131) (n=380) (n=132)Fatigue 41% 34% 31%Diarrhea 32% 37% 20%Pruritus 31% 21% 11%Rash 29% 25% 8%Colitis 8% 5% 2%gp indicates glycoprotein.
Table 6. Most Common Adverse Reactions Reported With Ipilimumab19

WWW.PERSONALIZEDMEDONC.COM 33Volume 1 • No 3 August 2012
melanoma skin cancer is 2 to 3 million cases,22 and ap-proximately 80% of these are basal cell carcinomas.23,24
Epidemiologic data suggest that the overall incidence ofbasal cell carcinoma is increasing significantly and showmarked geographical variation.23-26 Australia has thehighest incidence rate of basal cell carcinoma in theworld, reporting a rate of 1% to 2% per year.23,24
Basal cell carcinoma develops in the basal layer ofthe epidermis and is the most commonly diagnosed ma-lignancy worldwide.24,27-29 The average lifetime risk forCaucasians to develop basal cell carcinoma is in therange of 5% to 30%, depending in large part on skintype and patterns of sun exposure.24,27 A major cause ofbasal cell carcinoma is exposure to ultraviolet radiation,leading to cumulative DNA damage and acquired genemutations.24,27-30 Most sporadic cases of basal cell carci-noma arise from chronic sun exposure; 80% occur onthe head and neck, 15% on the trunk, and 5% on thearms, legs, or other sites.24,27 Basal cell carcinoma is clas-sified into 3 subtypes (Table 7).27,28,31
Surgical excision is the most common treatment forbasal cell carcinoma and has a high success rate, partic-ularly in uncomplicated cases (Table 8).27,31 However,surgery can be both debilitating and disfiguring.31 Tu-mors that are not appropriate for surgery, or for whichsurgery would result in substantial deformity (ie, in dif-ficult-to-treat locations) require treatment with nonsur-gical approaches, such as radiotherapy,27 photodynamictherapy,32 chemotherapy,33 and topical therapy.34,35
National Comprehensive Cancer Network GuidelinesMark Pittelkow, MD, from the Mayo Clinic College
of Medicine in Rochester, Minnesota, reviewed the National Comprehensive Cancer Network (NCCN)guidelines for treating basal cell carcinomas, in whichtreatment is stratified by risk status.36 According to theNCCN guidelines, high-risk basal cell carcinomas in-clude the following36:• Recurrent or incompletely excised basal cell carcinoma• Primary basal cell carcinoma with clinically indistinctborders
• Lesion in high-risk (known as the “H,” or “mask”)areas, mainly the embryonic fusion planes (eg, eye-lids, nose, ear, nasolabial folds, upper lip, vermillionborder, columella, periorbital region, temples, pre-auricular and postauricular areas, and scalp)
• Lesions that develop in cosmetically and functionallyimportant areas (eg, face, genitals, anal and perianalregions, hands and feet, and the nail unit areas)
• Tumors with aggressive clinical behavior (ie, growingrapidly or >2 cm)
Continuing Medical Education
Nodular Superficial OtherPercentage of Cases 60% 30% 10%Description • Occurs frequently on • Occurs most frequently • For example, morphoeic
sun-exposed areas of the head on the trunk cases, also called sclerosing• Often presents as a papule • Characterized by small buds or fibrosing basal cellor nodule of basaloid tumor cells carcinomas, are aggressive
extending from the epidermis infiltrating subtypes• Often have ill-defined borders, making complete excision a challenge
Table 7. Subtypes of Basal Cell Carcinoma27,28,31
Surgical Technique 5-Year Cure Rate
Surgical excision ≥95%
Curettage and cautery ≥95%
Cryosurgery ≥95%
Mohs micrographic surgery ~99%
Table 8. Cure Rates for Various SurgicalTechniques in Basal Cell Carcinoma27,31

PERSONALIZED MEDICINE IN ONCOLOGY34 Volume 1 • No 3 August 2012
• Tumors with aggressive histologic subtype, includingsclerosing (morpheaform), basosquamous (metatypi-cal or keratinizing), perineural, periappendageal, or perivascular invasion, infiltrating, adenoidal, ormulticentric
• Tumors that develop in sites with previous radiationtherapy
• Tumors that develop in immunosuppressed patients
Treatment Challenges for Advanced Basal Cell CarcinomaNicole Basset-Seguin, MD, PhD, from the Hôpital
Saint-Louis in Paris, France, discussed treatment chal-lenges for patients with various types of basal cell carci-noma, especially advanced disease (Figure 3). Shepointed out that, at present, patients with inoperable,advanced basal cell carcinoma, or those in whom surgi-cal resection would result in substantial deformity, havevery few therapeutic options. There is no standard ther-
apy for advanced basal cell carcinoma.37 Once basal cellcarcinoma has metastasized, it is highly malignant andhas a poor prognosis.38,39 Therefore, new treatment op-tions are needed for advanced basal cell carcinoma.
The Hedgehog Signaling PathwayJoel Claveau, MD, CSPQ, FRCPC, Associate Pro-
fessor of Medicine in the Dermatology Division at LavalUniversity in Quebec, Canada, discussed the molecularpathogenesis of basal cell carcinoma. He provided anoverview of the hedgehog signaling pathway, whichplays a fundamental role in normal embryonic develop-ment. The hedgehog pathway was discovered in thefruit fly (Drosophila) and is conserved in vertebrates (in-cluding humans).42,43 It is involved in cell growth anddifferentiation to control organ formation during em-bryonic development. Hedgehog signaling regulates em-bryonic development, ensuring that tissues reach correctsize and location, maintaining tissue polarity and cellu-
Continuing Medical Education
Figure 3. Classification of Patients With Basal Cell Carcinoma25,27,40,41
Locally advanced basal cell carcinoma• Patients whose lesions are not appropriate for surgery, orwho have medical contraindications to surgery
• Patients for whom surgery would result in substantial morbidity and/or deformity (eg, invasion into skull, limbamputation, or enucleation)
Metastatic basal cell carcinoma• Sometimes occurs in patients with long-standing primarylesions that are large or recurrent
• Rare but serious form of basal cell carcinoma (0.0028%-0.55% of tumors progress to metastatic disease)
• Includes distant metastases (eg, bone, lung, and liver) orlymph node involvement
• Poor prognosis (median survival: 8-14 months; 5-year survival rate: 10%)
Advanced basal cell carcinoma• Locally advanced disease• Metastatic disease
Advanced Basal Cell Carcinoma
Locally advanced basalcell carcinoma
Metastatic basal cellcarcinoma
Basal Cell Carcinoma

WWW.PERSONALIZEDMEDONC.COM 35Volume 1 • No 3 August 2012
lar content.43 In the skin, the hedgehog pathway is crit-ical for regulating hair follicle and sebaceous gland de-velopment.44 Germline mutations in components of thehedgehog signaling pathway result in a number of de-velopmental abnormalities.45,46 Hedgehog signaling nor-mally remains inactive in most adult tissues.Key components involved in hedgehog signaling in-
clude the hedgehog ligand, hedgehog (Hh), which initi-ates signal transduction of the hedgehog pathway; thehedgehog signal transducer, smoothened (SMO), whichis normally suppressed by the hedgehog ligand receptor,patched (PTCH), preventing its activation of thehedgehog signaling cascade; the hedgehog ligand recep-tor, PTCH, which normally suppresses the activity ofSMO; and the hedgehog effectors, which are a cytosoliccomplex of proteins including suppressor of fused andthe Gli family of transcription factors. Activation leadsto expression of specific genes that promote cell prolif-eration and differentiation.43
When the hedgehog pathway is inactive, PTCH in-hibits SMO activity, and the intracellular signaling cas-cade is suppressed.30,47,48 Activation of the pathway isinitiated by the Hh ligand binding to PTCH, releasingits inhibitory effect on SMO, which results in targetgene expression.30,47-49 Abnormal hedgehog pathway sig-naling plays an important role in the pathogenesis ofcertain types of cancer. Different mechanisms drive ab-normal hedgehog pathway signaling in different typesof cancer43,50,51:• Ligand-independent signaling driven by mutations(eg, basal cell carcinoma and medulloblastoma)
• Mutations in key pathway regulators (eg, PTCH orSMO) that cause SMO to be in a constitutively ac-tive state
• Ligand-dependent signaling driven by overexpressionof Hh ligand by tumor cells (eg, ovarian, colorectal,and pancreatic cancer) As a result of inactivating PTCH mutations or acti-
vating SMO mutations, SMO moves to the cell surfaceleading to activation of the Gli family of transcriptionfactors. Activated Gli then moves to the nucleus andinitiates the transcription of target genes.30,43,49,51-56 Ab-
normal activation of the hedgehog signaling pathway isthought to play a critical role in the pathogenesis andprogression of basal cell carcinoma, either by inactivat-ing PTCH mutations or by activating SMO mutations.Hedgehog pathway inhibitors may provide a new treat-ment option for patients with advanced basal cell carcinoma.49
In basal cell carcinoma, abnormal hedgehog pathwaysignaling is the key molecular driver of the disease. Morethan 90% of basal cell carcinomas have abnormal acti-vation of hedgehog pathway signaling. Most basal cellcarcinoma tumors have either inactivating mutations inPTCH or, less commonly, activating mutations in SMO.
Targeted Hedgehog InhibitionAleksandar Sekulic, MD, PhD, from the Mayo Clinic
and the Translational Genomics Institute in Scottsdale,Arizona, presented a keynote lecture on targeted hedge-hog pathway inhibition in basal cell carcinoma. Hepointed out that the hedgehog pathway is aberrantly ac-tivated in virtually all basal cell carcinomas, so there isno need to screen. A number of hedgehog pathway in-
Continuing Medical Education
Drug Status Trials
Erivedge (vismodegib) FDA approved for locally advanced and metastatic basal cell carcinoma
LDE225 Investigational Phase 2LEQ506 Investigational Phase 1BMS-833823 Investigational Phase 1(XL139) Phase 2TAK-441 Investigational Phase 1IPI926 Investigational Phase 1(saridegib) Phase 2PF-04449913 Investigational Phase 1SMO indicates smoothened.
Table 9. New and Investigational SMO Inhibitors57
Abnormal activation of the hedgehogsignaling pathway is thought to play acritical role in the pathogenesis andprogression of basal cell carcinoma.

PERSONALIZED MEDICINE IN ONCOLOGY36 Volume 1 • No 3 August 2012
hibiting agents, mainly SMO inhibitors, are under development (Table 9). Currently, 1 hedgehog pathway inhibitor, vismo -
degib, has been approved by the FDA for the treatmentof adults with metastatic basal cell carcinoma, or withlocally advanced basal cell carcinoma that has recurredfollowing surgery or who are not candidates for surgery,and who are not candidates for radiation. The mostcommon adverse reactions (≥10%) with vismodegibwere muscle spasms, alopecia, dysgeusia, weight loss, fa-tigue, nausea, diarrhea, decreased appetite, constipation,arthralgias, vomiting, and ageusia (Table 10).58 Overall,
these adverse reactions were frequent butmostly mild to moderate. They may be ac-ceptable in advanced and metastatic basalcell carcinoma, but the question remainswhether they would be acceptable in pa-tients who have operable disease. Prelimi-nary data suggest that these adverse effectsare reversible. Selection of patients and ad-verse effect management are key to the useof this agent.
Cutaneous T-Cell LymphomasJoan Guitart, MD, Professor of Derma-
tology and Pathology at the Feinberg Med-ical School in Chicago, Illinois, began hertalk by pointing out that normal humanskin is populated by 20 billion T cells, andthat cutaneous T-cell lymphoma is a malig-nancy of T cells that reside in the skin.59
Guitart then provided a “world tour” ofphotographs of cutaneous T-cell lym-phomas. She organized her presentationbased on the World Health Organizationand European Organisation for Researchand Treatment of Cancer (WHO-EORTC)classification of cutaneous T-cell lym-phomas (Table 11).60
Host Immune ResponseAlain Rook, MD, from the Abramson
Cancer Center and the University of PennsylvaniaSchool of Medicine in Philadelphia, Pennsylvania, dis-cussed the importance of host immune response in thetreatment of cutaneous T-cell lymphoma.Cutaneous T-cell lymphoma is highly responsive to
immune modulation. The malignant CD4+ T cells ob-served in most cases of mycosis fungoides and Sézarysyndrome appear to exhibit a T helper cell type 2(Th2) phenotype (Figure 4). In mycosis fungoides and Sézary syndrome, the malignant T cell (CD4+/CLA+/CCR4+) produces the cytokines IL-4, IL-5, andIL-10 that result in a Th2 predominance and subse-
Continuing Medical Education
All aBCC Patients (N=138)MedDRA Preferred Term All Grades* (%) Grade 3 (%) Grade 4 (%)
Gastrointestinal disordersNausea 42 (30.4%) 1 (0.7%) –Diarrhea 40 (29.0%) 1 (0.7%) –Constipation 29 (21.0%) – –Vomiting 19 (13.8%) – –
General disorders and administration-site conditions Fatigue 55 (39.9%) 7 (5.1%) 1 (0.7%)
InvestigationsWeight loss 62 (44.9%) 10 (7.2%) –
Metabolism and nutritiondisordersDecreased appetite 35 (25.4%) 3 (2.2%) –
Musculoskeletal and connectivetissue disordersMuscle spasms 99 (71.7%) 5 (3.6%) –Arthralgias 22 (15.9%) 1 (0.7%) –
Nervous system disordersDysgeusia 76 (55.1%) – –Ageusia 15 (10.9%) – –
Skin and subcutaneoustissue disordersAlopecia 88 (63.8%) – –
aBCC indicates advanced basal cell carcinoma; MedDRA, Medical Dictionary for Regulatory Activities.*Grading according to NCI-CTCAE v3.0.
Table 10. Adverse Reactions Occurring in ≥10% of AdvancedBasal Cell Carcinoma Patients With Vismodegib in Clinical Trials58

WWW.PERSONALIZEDMEDONC.COM 37Volume 1 • No 3 August 2012
quent multiple abnormalities in cellular immunity.61
Numerous arms of the immune system must cooperateto generate a sufficient host antitumor response such thatthe proliferation of the malignant T-cell population inmycosis fungoides and Sézary syndrome can be controlled.Elimination of the malignant T-cell clone during im-munotherapy leads to restoration of a normal immune response. Studies of numerous patients with Sézary syndrome have demonstrated that induction of completeremission with clearing of the malignant T-cell clone dur-ing multimodality immunotherapy leads to a restorationof normal host immune function (Table 12).
Management of Early-Stage Cutaneous T-Cell Lymphomas (Mycosis Fungoides)Larisa Geskin, MD, from the University of Pittsburgh
Medical Center in Pittsburgh, Pennsylvania, reviewedtreatments for early-stage cutaneous T-cell lymphomas.She explained that skin-directed therapies, including
topical corticosteroids,62 topical chemotherapy (eg, ni-trogen mustard63,64 or carmustine65), topical retinoids,and phototherapy66,67 are used for early-stage (stage Ia,Ib, IIa) disease. Radiation, both localized and total-skinelectron beam radiation,68 as well as photopheresis,69
are used for stage IIb and III, and systemic treatments,such as bexarotene,70-73 interferon-alpha, romidepsin,74
vorinostat,75,76 alemtuzumab, and chemotherapy, areused for stage IVa and IVb disease (Table 13).
Staging/Classification and End Points/Response CriteriaElise A. Olsen, MD, Professor of Dermatology and
Oncology and Director of the Duke Cutaneous Lym-phoma Research and Treatment Center in Durham,North Carolina, discussed staging and classification, aswell as new end points and response criteria.The Mycosis Fungoides Cooperative Group staging
system for cutaneous T-cell lymphoma published in1979 was revised in 2007 by the International Societyfor Cutaneous Lymphomas (ISCL) and the CutaneousLymphoma Task Force of the EORTC.81 The highlightsof the revised system are:
• Include technological advances, including those ofmolecular biology and immunohistochemistry
• Incorporate new data on prognostic variables in my-cosis fungoides and Sézary syndrome
• Exclude other non–mycosis fungoides/non–Sézarysyndrome variants from the staging system
• Identify potential prognostic variables for the purposeof tracking and validation
Continuing Medical Education
• Mycosis fungoides (MF)– Folliculotropic MF– Pagetoid reticulosis – Granulomatous slack skin
• Sézary syndrome• Adult T-cell leukemia/lymphoma• Primary cutaneous CD30+ lymphoproliferative disorders– Primary cutaneous anaplastic large cell lymphoma– Lymphomatoid papulosis
• Subcutaneous panniculitis-like T-cell lymphoma• Extranodal NK/T-cell lymphoma, nasal type• Primary cutaneous peripheral T-cell lymphoma, unspecified• Primary cutaneous aggressive epidermotropic CD8+ T-cell lymphoma (provisional)
• Cutaneous γ/δ T-cell lymphoma • Primary cutaneous CD4+ small/medium-sized pleomorphic T-cell lymphoma (provisional)
EORTC indicates European Organisation for Research and Treatment of Cancer;WHO, World Health Organization.
Table 11. WHO-EORTC Classification of CutaneousT-Cell and Natural Killer (NK) Cell Lymphomas60
Figure 4. Consequences of Malignant T-Cell Cytokine Production61
IgE indicates immunoglobulin E; Th1, T helper cell type 1; Th2, T helper cell type 2.

PERSONALIZED MEDICINE IN ONCOLOGY38 Volume 1 • No 3 August 2012
A comparison of the original and revised staging sys-tems is shown in Table 14.In 2011, the ISCL, the United States Cutaneous
Lymphoma Consortium, and the Cutaneous LymphomaTask Force of the EORTC published consensus recom-mendations for the general conduct of clinical trials ofpatients with mycosis fungoides and Sézary syndrome,as well as methods for standardized assessment of poten-tial disease manifestations in skin, lymph nodes, blood,
and visceral organs, and definition of end points and re-sponse criteria. These guidelines should facilitate col-laboration among investigators and collation of datafrom sponsor-generated or investigator-initiated clinicaltrials involving patients with mycosis fungoides orSézary syndrome.82
New staging for mycosis fungoides and Sézary syn-drome and non–mycosis fungoides/non–Sézary syn-drome primary cutaneous lymphomas allows forincorporation of new molecular data into diagnostic cri-teria as well as standardization of clinical trial inclu-sion/exclusion criteria. New end points and responsecriteria for all types of primary cutaneous lymphomaallow for comparison of data from clinical trials of dif-ferent medications conducted at different time pointsand facilitation of multicenter clinical trials, whetherpharma supported or investigator initiated.
CD30+ Skin LymphomasLauren Pinter-Brown, MD, Clinical Professor of
Medicine in the Division of Hematology-Oncology atthe UCLA Medical Center in Los Angeles, California,discussed new approaches in the management of CD30+skin lymphomas, which include:• Primary cutaneous anaplastic large cell lymphoma• Lymphomatoid papulosis• Mycosis fungoides (transformed)• Secondary cutaneous anaplastic large cell lymphoma• Peripheral T-cell lymphoma (unspecified), adult T-cell leukemia/lymphoma
• Hodgkin lymphomaSGN-30 is a chimeric monoclonal antibody against the
cluster C epitope of CD30. Brentuximab vedotin (formerlyknown as SGN-35) is an antibody-drug conjugate of SGN-30 with an auristatin derivative (tubulin inhibitor). Treatment with single-agent brentuximab vedotin re-
sulted in unprecedented objective response rates andcomplete response rates of 75% and 34%, respectively,in relapsed or refractory Hodgkin lymphoma, and of86% and 57%, respectively, in relapsed or refractory sys-temic anaplastic large cell lymphoma patients. Periph-eral sensory neuropathy and neutropenia were observed
Continuing Medical Education
• Topical corticosteroids• Topical chemotherapy with mechlorethamine (nitrogen mustard) or carmustine
• Psoralen and ultraviolet A radiation• Ultraviolet B radiation• Total-skin electron beam radiation• Radiation of symptomatic skin lesions• Interferon-α or interferon-γ alone or in combination with topical therapy
• Single-agent and multiagent chemotherapy• Bexarotene (topical gel or oral); retinoids• Denileukin diftitox (recombinant fusion protein of diphtheria toxin fragments and interleukin-2 sequences)
• Vorinostat or romidepsin (oral histone deacetylase inhibitors)• Alemtuzumab (a humanized monoclonal antibody targeting the CD52 antigen)
• Combined modality treatment
Table 13. Treatment Options for Patients With Mycosis Fungoides and Sézary Syndrome77-80
Increased Decreased
• CD4+/CLA+/CCR4+ T cells • CD8 T cells
• Th2 cytokines; IL-4, IL-5, IL-10 • Loss of normal T-cell repertoire
• Regulatory T cells (Tregs) • NK cells; Th1 cytokines;IFN-g
• Programmed Death 1 (PD-1) • Dendritic cells (CD123 and CD11c), IL-12, IFN-α
• CD40 ligand expression
IFN indicates interferon; IL, interleukin; NK cells, natural killer cells; Th1, T helpercell type 1; Th2, T helper cell type 2.
Table 12. Immunological Phenotype in Sézary Syndrome

WWW.PERSONALIZEDMEDONC.COM 39Volume 1 • No 3 August 2012
with brentuximab vedotin but were generally grade 1and 2 in severity and manageable.83 In 2011, the FDAgranted accelerated approval for brentuximab vedotinfor the following indications84:• Hodgkin lymphoma after failure of autologous stemcell transplant (ASCT)
• Hodgkin lymphoma in patients who are not ASCTcandidates after failure of at least 2 multiagentchemotherapy regimens
• Systemic anaplastic large cell lymphoma after failureof at least 1 multiagent chemotherapy regimenBrentuximab vedotin is currently being investi-
gated in a number of clinical trials:• Phase 3 trial for patients at high risk of residualHodgkin lymphoma following ASCT
• Phase 3 trial for patients with relapsed CD30+ cuta-neous T-cell lymphoma
• Phase 2 trial for patients with relapsed or refractoryCD30+ non-Hodgkin lymphomas
• Phase 2 trial for patients with CD30+ nonlymphomamalignancies
• Phase 2 trial for retreatment of patients who previ-ously participated in a brentuximab vedotin study
• Phase 1 trial in combination with chemotherapy forfrontline treatment of Hodgkin lymphoma
• Phase 1 trial in combination with chemotherapy for frontline treatment of CD30+ mature T-cell malignancies
ConclusionThe 2012 World Cutaneous Malignancies Congress
covered the biology, pathology, staging, personalized ther-apy, maintenance therapy, novel agents, and ongoing research of a wide range of cutaneous malignancies. Molecular biology and pathogenesis were reviewed as theyrelate to treatment of these cutaneous malignancies. Riskstratification of patients was discussed, along with how totailor treatment based on patient and tumor characteris-tics. At this global forum, experts from around the worldgathered to discuss personalized treatment strategies thatincorporate current standards of care and emerging treat-ment options for the optimal treatment of patients withcutaneous malignancies into oncologists’ practice. u
References1. Goldstein AM, Chan M, Harland M, et al. Features associated withgermline CDKN2A mutations: a GenoMEL study of melanoma-prone fam-ilies from three continents. J Med Genet. 2007;44:99-106.2. Molven A, Grimstvedt MB, Steine SJ, et al. A large Norwegian familywith inherited malignant melanoma, multiple atypical nevi, and CDK4mutation. Genes Chromosomes Cancer. 2005;44:10-18.3. Harbour JW, Onken MD, Roberson ED, et al. Frequent mutation ofBAP1 in metastasizing uveal melanomas. Science. 2010;330:1410-1413.4. Harland M, Meloni R, Gruis N, et al. Germline mutations of the CDKN2gene in UK melanoma families. Hum Mol Genet. 1997;6:2061-2067.5. Yokoyama S, Woods SL, Boyle GM, et al. A novel recurrent mutation inMITF predisposes to familial and sporadic melanoma. Nature. 2011; 480:99-103.6. Chang YM, Barrett JH, Bishop DT, et al. Sun exposure and melanomarisk at different latitudes: a pooled analysis of 5700 cases and 7216 controls.Int J Epidemiol. 2009;38:814-830.7. Newton-Bishop J, Chang YM, Elliott F, et al. Relationship between sunexposure and melanoma risk for tumours in different body sites in a large case-control study in a temperate climate. Int J Epidemiol. 2011;47:732-741.8. Chang YM, Newton-Bishop JA, Bishop DT, et al. A pooled analysis ofmelanocytic nevus phenotype and the risk of cutaneous melanoma at dif-ferent latitudes. Int J Cancer. 2009;24:420-428.
Continuing Medical Education
Table 14. Comparison Between the 1979 Staging System for Cutaneous T-Cell Lymphomas andthe 2007 Revised Staging System for Mycosis Fungoides and Sézary Syndrome81
1979 Staging System for Cutaneous 2007 Revised Staging System for Mycosis Fungoides T-Cell Lymphomas and Sézary Syndrome
Stage T N M Stage T N M BIA 1 0 0 IA 1 0 0 0, 1IB 2 0 0 IB 2 0 0 0, 1IIA 1-2 1 0 IIA 1-2 1-2 0 0, 1IIB 3 0, 1 0 IIB 3 0-2 0 0, 1III 4 0, 1 0 IIIA 4 0-2 0 0
IIIB 4 0-2 0 1IVA 1-4 2-3 0 IVA1 1-4 0-2 0 2IVB 1-4 0-3 1 IVA2 1-4 3 0 0-2
IVB 1-4 0-3 1 0-2

PERSONALIZED MEDICINE IN ONCOLOGY40 Volume 1 • No 3 August 2012
9. Bishop DT, Demenais F, Iles MM, et al. Genome-wide association studyidentifies three loci associated with melanoma risk. Nat Genet. 2009;41:920-925.10. Falchi M, Bataille V, Hayward NK, et al. Genome-wide associationstudy identifies variants at 9p21 and 22q13 associated with developmentof cutaneous nevi. Nat Genet. 2009;41:915-919.11. Barrett JH, Iles MM, Harland M, et al. Genome-wide association studyidentifies three new melanoma susceptibility loci. Nat Genet. 2011;43:1108-1113.12. LeBoit PE, Burg G, Weedon D, Sarasain A, eds. World Health Organi-zation Classification of Tumours. Pathology and Genetics of Skin Tumours.Lyon, France: IARC Press; 2006.13. Krementz ET, Sutherland CM, Carter RD, et al. Malignant melanomain the American Black. Ann Surg. 1976;183:533-542.14. Curtin JA, Fridlyand J, Kageshita T, et al. Distinct sets of genetic al-terations in melanoma. N Engl J Med. 2005;353:2135-2147.15. Herlyn M, Nathanson KL. Taking the guesswork out of uvealmelanoma. N Engl J Med. 2010;363:2256-2257.16. Woodman SE, Lazar AJ, Aldape KD, et al. New strategies in melanoma:molecular testing in advanced disease. Clin Cancer Res. 2012; 18:1195-1200.17. Davies MA, Gershenwald JE. Targeted therapy for melanoma: a primer.Surg Oncol Clin N Am. 2011;20:165-180.18. Eggermont AM, Suciu S, Testori A, et al. Ulceration and stage are pre-dictive of interferon efficacy in melanoma: results of the phase III adjuvanttrials EORTC 18952 and EORTC 18991. Eur J Cancer. 2012;48:218-225.19. Hodi FS, O’Day SJ, McDermott DF, et al. Improved survival with ip-ilimumab in patients with metastatic melanoma. N Engl J Med. 2010;363:711-723.20. Robert C, Thomas L, Bondarenko I, et al. Ipilimumab plus dacarbazinefor previously untreated metastatic melanoma. N Engl J Med. 2011;364:2517-2526.21. Margolin K, Ernstoff MS, Hamid O, et al. Ipilimumab in patients withmelanoma and brain metastases: an open-label, phase 2 trial. Lancet Oncol.2012;13:459-465.22. World Health Organization. www.who.int/uv/faq/skincancer/en/index1.html.23. Diepgen TL, Mahler V. The epidemiology of skin cancer. Br J Dermatol.2002;146(suppl 61):1-6.24. Rubin AI, Chen EH, Ratner D. Basal-cell carcinoma. N Engl J Med.2005;353:2262-2269.25. Ting PT, Kasper R, Arlette JP. Metastatic basal cell carcinoma: reportof two cases and literature review. J Cutan Med Surg. 2005;9:10-15.26. Rogers HW, Weinstock MA, Harris AR, et al. Incidence estimate ofnonmelanoma skin cancer in the United States, 2006. Arch Dermatol.2010;146:283-287.27. Wong CS, Strange RC, Lear JT. Basal cell carcinoma. BMJ. 2003;327:794-798.28. Roewert-Huber J, Lange-Asschenfeldt B, Stockfleth E, et al. Epidemiologyand aetiology of basal cell carcinoma. Br J Dermatol. 2007;157(suppl 2):47-51.29. Lear JT, Harvey I, de Berker D, et al. Basal cell carcinoma. J R SocMed. 1998;91:585-588.30. Caro I, Low JA. The role of the hedgehog signaling pathway in thedevelopment of basal cell carcinoma and opportunities for treatment. ClinCancer Res. 2010;16:3335-3339.31. Walling HW, Fosko SW, Geraminejad PA, et al. Aggressive basal cellcarcinoma: presentation, pathogenesis, and management. Cancer MetastasisRev. 2004;23:389-402.32. Szeimies RM, Morton CA, Sidoroff A, et al. Photodynamic therapyfor non-melanoma skin cancer. Acta Derm Venereol. 2005;85:483-490.33. Tucker SB, Polasek JW, Perri AJ, et al. Long-term follow-up of basalcell carcinomas treated with perilesional interferon alfa 2b as monotherapy.J Am Acad Dermatol. 2006;54:1033-1038.34. Alessi SS, Sanches JA, Oliveira WR, et al. Treatment of cutaneous tumorswith topical 5% imiquimod cream. Clinics (Sao Paulo). 2009;64:961-966.35. Gross K, Kircik L, Kricorian G. 5% 5-Fluorouracil cream for the treat-ment of small superficial basal cell carcinoma: efficacy, tolerability, cos-metic outcome, and patient satisfaction. Dermatol Surg. 2007;33:433-439.36. National Comprehensive Cancer Network (NCCN). Basal Cell andSquamous Cell Skin Cancers. Version 2.2012. www.nccn.org/professionals/physician_gls/pdf/nmsc.pdf. Accessed July 30, 2012.37. Von Hoff DD, LoRusso PM, Rudin CM, et al. Inhibition of the hedge-
hog pathway in advanced basal-cell carcinoma. N Engl J Med. 2009;361:1164-1172.38. Ozbek N, Meydan D, Güneren E, et al. Metastatic basal cell carci-noma. N Z Med J. 2004;117:U874.39. Goldberg LH, Firoz BF, Weiss GJ, et al. Basal cell nevus syndrome: abrave new world. Arch Dermatol. 2010;146:17-19.40. von Domarus H, Stevens PJ. Metastatic basal cell carcinoma. Reportof five cases and review of 170 cases in the literature. J Am Acad Dermatol.1984;10:1043-1060.41. Lo JS, Snow SN, Reizner GT, et al. Metastatic basal cell carcinoma:report of twelve cases with a review of the literature. J Am Acad Dermatol.1991;24(5 Pt 1):715-719.42. Nüsslein-Volhard C, Wieschaus E. Mutations affecting segment num-ber and polarity in Drosophila. Nature. 1980;287:795-801.43. Scales SJ, de Sauvage FJ. Mechanisms of Hedgehog pathway activationin cancer and implications for therapy. Trends Pharmacol Sci. 2009;30:303-312.44. Chiang C, Swan RZ, Grachtchouk M, et al. Essential role for Sonichedgehog during hair follicle morphogenesis. Dev Biol. 1999;205:1-9.45. Wilkie AO, Morriss-Kay GM. Genetics of craniofacial developmentand malformation. Nat Rev Genet. 2001;2:458-468.46. McMahon AP, Ingham PW, Tabin CJ. Developmental roles and clin-ical significance of hedgehog signaling. Curr Top Dev Biol. 2003;53:1-114.47. Rubin LL, de Sauvage FJ. Targeting the Hedgehog pathway in cancer.Nat Rev Drug Discov. 2006;5:1026-1033.48. Beachy PA, Karhadkar SS, Berman DM. Tissue repair and stem cellrenewal in carcinogenesis. Nature. 2004;432:324-331.49. Epstein EH. Basal cell carcinomas: attack of the hedgehog. Nat RevCancer. 2008;8:743-754.50. Low JA, de Sauvage FJ. Clinical experience with Hedgehog pathwayinhibitors. J Clin Oncol. 2010;28:5321-5326.51. Rudin CM. Clinical experience with Hedgehog pathway inhibitors.Cancer Prev Res (Phila). 2010;3:1-3.52. Bale AE, Yu KP. The hedgehog pathway and basal cell carcinomas.Hum Mol Genet. 2001;10:757-762.53. Hutchin ME, Kariapper MS, Grachtchouk M, et al. Sustained Hedge-hog signaling is required for basal cell carcinoma proliferation and survival:conditional skin tumorigenesis recapitulates the hair growth cycle. GenesDev. 2005;19;214-223.54. Teh MT, Blaydon D, Chaplin T, et al. Genomewide single nucleotidepolymorphism microarray mapping in basal cell carcinomas unveils uni-parental disomy as a key somatic event. Cancer Res. 2005;65:8597-8603.55. Kallassy M, Toftgård R, Ueda M, et al. Patched (ptch)-associated pref-erential expression of smoothened (smoh) in human basal cell carcinomaof the skin. Cancer Res. 1997;57:4731-4735.56. Unden AB, Zaphiropoulos PG, Bruce K, et al. Human patched(PTCH) mRNA is overexpressed consistently in tumor cells of both fa-milial and sporadic basal cell carcinoma. Cancer Res. 1997;57:2336-2340.57. www.clinicaltrials.gov.58. Erivedge [package insert]. South San Francisco, CA: Genentech, Inc; 2012.59. Clark RA. Regulation gone wrong: a subset of Sézary patients havemalignant regulatory T cells. J Invest Dermatol. 2009;129:2747-2750.60. Willemze R, Jaffe ES, Burg G, et al. WHO-EORTC classification forcutaneous lymphomas. Blood. 2005;105:3768-3785.61. Kim EJ, Hess S, Richardson SK, et al. Immunopathogenesis and ther-apy of cutaneous T cell lymphoma. J Clin Invest. 2005;115:798-812.62. Zackheim HS. Treatment of patch-stage mycosis fungoides with topicalcorticosteroids. Dermatol Ther. 2003;16:283-287.63. Vonderheid EC, Tan ET, Kantor AF, et al. Long-term efficacy, curativepotential, and carcinogenicity of topical mechlorethamine chemotherapyin cutaneous T cell lymphoma. J Am Acad Dermatol. 1989;20:416-428.64. Kim YH. Management with topical nitrogen mustard in mycosis fun-goides. Dermatol Ther. 2003;16:288-298.65. Zackheim HS. Topical carmustine (BCNU) in the treatment of my-cosis fungoides. Dermatol Ther. 2003;16:299-302.66. Carter J, Zug KA. Phototherapy for cutaneous T-cell lymphoma: onlinesurvey and literature review. J Am Acad Dermatol. 2009;60:39-50.67. Querfeld C, Rosen ST, Kuzel TM, et al. Long-term follow-up of patientswith early-stage cutaneous T-cell lymphoma who achieved complete remissionwith psoralen plus UV-A monotherapy. Arch Dermatol. 2005; 141:305-311.68. Quirós PA, Jones GW, Kacinski BM, et al. Total skin electron beamtherapy followed by adjuvant psoralen/ultraviolet-A light in the manage-
Continuing Medical Education

WWW.PERSONALIZEDMEDONC.COM 41Volume 1 • No 3 August 2012
Continuing Medical Education
ment of patients with T1 and T2 cutaneous T-cell lymphoma (mycosis fun-goides). Int J Radiat Oncol Biol Phys. 1997;38:1027-1035.69. Talpur R, Demierre MF, Geskin L, et al. Multicenter photopheresis in-tervention trial in early-stage mycosis fungoides. Clin Lymphoma MyelomaLeuk. 2011;11:219-227.70. Heald P, Mehlmauer M, Martin AG, et al. Topical bexarotene therapy forpatients with refractory or persistent early-stage cutaneous T-cell lymphoma:results of the phase III clinical trial. J Am Acad Dermatol. 2003; 49:801-815.71. Breneman D, Duvic M, Kuzel T, et al. Phase 1 and 2 trial of bexarotenegel for skin-directed treatment of patients with cutaneous T-cell lym-phoma. Arch Dermatol. 2002;138:325-332.72. Duvic M, Martin AG, Kim Y, et al. Phase 2 and 3 clinical trial of oralbexarotene (Targretin capsules) for the treatment of refractory or persistentearly-stage cutaneous T-cell lymphoma. Arch Dermatol. 2001;137:581-593.73. Duvic M, Hymes K, Heald P, et al. Bexarotene is effective and safe for treatment of refractory advanced-stage cutaneous T-cell lymphoma:multinational phase II-III trial results. J Clin Oncol. 2001;19:2456-2471.74. Whittaker SJ, Demierre MF, Kim EJ, et al. Final results from a multi-center, international, pivotal study of romidepsin in refractory cutaneousT-cell lymphoma. J Clin Oncol. 2010;28:4485-4491.75. Duvic M, Talpur R, Ni X, et al. Phase 2 trial of oral vorinostat (suberoy-lanilide hydroxamic acid, SAHA) for refractory cutaneous T-cell lym-phoma (CTCL). Blood. 2007;109:31-39.76. Olsen EA, Kim YH, Kuzel TM, et al. Phase IIb multicenter trial ofvorinostat in patients with persistent, progressive, or treatment refractorycutaneous T-cell lymphoma. J Clin Oncol. 2007;25:3109-3115.
77. National Cancer Institute. www.cancer.gov/cancertopics/pdq/treatment/mycosisfungoides/healthprofessional/allpages. Accessed July 31, 2012.78. Prince HM, Whittaker S, Hoppe RT. How I treat mycosis fungoidesand Sézary syndrome. Blood. 2009;114:4337-4353.79. Trautinger F, Knobler R, Willemze R, et al. EORTC consensus recom-mendations for the treatment of mycosis fungoides/Sézary syndrome. EurJ Cancer. 2006;42:1014-1030.80. Olsen EA, Rook AH, Zic J, et al. Sézary syndrome: immunopathogen-esis, literature review of therapeutic options, and recommendations fortherapy by the United States Cutaneous Lymphoma Consortium(USCLC). J Am Acad Dermatol. 2011;64:352-404.81. Olsen E, Vonderheid E, Pimpinelli N, et al. Revisions to the stagingand classification of mycosis fungoides and Sezary syndrome: a proposal ofthe International Society for Cutaneous Lymphomas (ISCL) and the cu-taneous lymphoma task force of the European Organization of Researchand Treatment of Cancer (EORTC). Blood. 2007;110:1713-1722.82. Olsen EA, Whittaker S, Kim YH, et al. Clinical end points and re-sponse criteria in mycosis fungoides and Sézary syndrome: a consensusstatement of the International Society for Cutaneous Lymphomas, theUnited States Cutaneous Lymphoma Consortium, and the CutaneousLymphoma Task Force of the European Organisation for Research andTreatment of Cancer. J Clin Oncol. 2011;29:2598-2607.83. Gualberto A. Brentuximab Vedotin (SGN-35), an antibody-drug con-jugate for the treatment of CD30-positive malignancies. Expert Opin Investig Drugs. 2012;21:205-216.84. Adcetris [package insert]. Bothell, WA: Seattle Genetics Inc; 2012.
Deborah Dunsire, MDPresident and Chief Executive OfficerMillennium: The Takeda Oncology Company
Kathy GiustiFounder and Chief Executive OfficerMultiple Myeloma Research FoundationMultiple Myeloma Research Consortium
K. Peter Hirth, PhDChief Executive OfficerPlexxikon, Inc.
Currently featuring:
Kimberly J. PopovitsPresident, Chief Executive OfficerGenomic Health, Inc.
INTERVIEW WITH THE INNOVATORSAn exclusive PMO series
Personalized Medicine in Oncology™ is pleased to offer insightful interviewswith leaders in oncology about their approach to personalized medicine.
To watch our interviews, visit www.PersonalizedMedOnc.com/videolibrary

MAY
2-5
, 201
3��
������
�����
THIRD ANNUAL CONFERENCE
www.AVBCConline.orgFor more information please visit
May 2-5, 2013Westin DiplomatHollywood, Florida
Influencing the Patient-Impact Factor
� � � � �� �� � �� �

WWW.PERSONALIZEDMEDONC.COM 43Volume 1 • No 3 August 2012
Value of Diagnostics in Healthcare –Foundation of Personalized Medicinein Oncology
Clinical laboratory testing hasa tremendous impact on pa-tient outcomes and healtheconomics. Over 7 billion
laboratory tests are performed annually inthe United States,1 and clinical tests con-tribute to an estimated 70% or more of alldecision making in medical practice.2 Yet,the total cost of laboratory services ac-counts for merely 1.8% of all Medicarespending annually and only 2.3% of na-tional healthcare spending.3
Key stakeholders, including industry,patient advocates, regulators, and legislators, are increas-
ingly considering new measures to protect and advanceinnovation and investment in diagnostics. There is par-
ticular interest in so-called advancedpersonalized diagnostics (APDx),which drive greater “precision” inmedical diagnosis and targeted treat-ment. APDx has been defined in draftfederal legislation as in vitro diagnos-tic products that provide “an analysisof deoxyribonucleic acid (DNA), ri-bonucleic acid (RNA), a chromo-some, a protein, or a metabolite…intended principally for use in detect-ing genotypes, mutations, patterns, orchromosomal changes for the purposeof diagnosis, prevention, cure, mitiga-
tion, or treatment of any disease or impairment, includ-
Regulatory Issues
Key Points
• Key stakeholders are increasingly considering new measures to protect and advance innovation and investmentin diagnostics
• Efforts are under way to establish more appropriate and least burdensome regulatory policies to address stake-holder concerns specific to in vitro diagnostic tests
• FDA is concerned with the risk of false-positive and false-negative test results that would be incorporated intoclinical treatment decisions
• FDA has struggled to find the most appropriate way to address regulatory oversight where gaps between CLIAand FDA are perceived
• FDA’s move toward greater oversight of the clinical validity of genomic-based tests has, thus far, not resulted ina path to personalized medicine paved with greater clarity, certainty, and confidence
Sheila D. Walcoff, JD, is a health and science attorney and the founding principal of Goldbug Strategies, LLC, a consultingand law practice offering business strategy, federal legislative and regulatory advocacy, and legal counsel related to personalizedmedicine and FDA-regulated medical products.
Sheila D. Walcoff, JD
Facilitating the Next Generation of Precision Medicinein OncologyThe collision of regulatory paradigms in clinical genomic pathologySheila D. Walcoff, JDFounding Principal, Goldbug Strategies, LLCRockville, Maryland
�
�
� � � �� �� � �� �

PERSONALIZED MEDICINE IN ONCOLOGY44 Volume 1 • No 3 August 2012
Regulatory Issues
ing prognosis or prediction of the outcome of a treat-ment or the assessment of the health of humans” and“…excluding methods of analysis principally comprisingroutine chemistry or routine immunology.”4
The important healthcare and economic benefits ofAPDx include, for example, more accurate and timely di-agnoses (eg, fewer hospital bed days, longer survival, etc);surgery avoidance (eg, organ resection and resulting life-long pharmacotherapy); appropriate therapy selection(eg, pharmacogenomics to optimize therapy selection andtreatment response monitoring); and better avoidance ofineffective therapies (eg, toxic and costly side effects ofchemotherapy). Despite regulatory and reimbursementuncertainty, these tests promise to be even more wide-spread in the very near term as physicians across special-ties overwhelmingly believe genetic testing will improvepatient care and anticipate testing to impact 14% of pa-tients in their own practice within 5 years.5
Evolving Regulation of Diagnostic Tests,Including APDx: CLIA Versus FDAMolecular diagnostic tests performed in clinical lab-
oratories have long been regulated by multiple federaland state agencies. Since the enactment of the federalClinical Laboratory Improvement Amendments of 1988(CLIA), tests developed and performed in clinical lab-
oratories have been regulated chiefly by the Centers forMedicare & Medicaid Services (CMS) and variousstates pursuant to state-by-state laboratory licensurelaws. But certain test components and reagents, whethera single analyte-specific reagent or combinations ofcomponents and reagents packaged together as a “kit,”general-purpose reagents, laboratory equipment, andsoftware offered by manufacturers for sale or distributionto clinical laboratories for research, investigational, or
clinical uses remained regulated by the FDA under theauthority of the Federal Food, Drug and Cosmetic Act(FFDCA) as amended.6 Pursuant to its authority undersection 201(h) of the FFDCA, FDA defines in vitro di-agnostic tests and components as “medical devices.”Specifically, “...reagents, instruments, and systems in-tended for use in the diagnosis of disease or other con-ditions, including a determination of the state of health,in order to cure, mitigate, treat, or prevent disease or itssequelae.” Such products are intended for use in the col-lection, preparation, and examination of specimenstaken from the human body.7 Importantly, state author-ities (rather than the federal government) regulate thepractice of medicine, including laboratory medicine.For tests performed in clinical laboratories, CLIA re-
quires that each clinical laboratory that introduces a testsystem not subject to FDA clearance or approval, or usesa test system for which performance specifications arenot provided by the test kit manufacturer, must establishfor each test system the performance specifications forcertain performance characteristics, including accuracy,precision, analytical sensitivity and specificity, referenceintervals, and reportable ranges for results.8 Addition-ally, clinical laboratories often are accredited by otherindependent organizations, such as the College ofAmerican Pathologists (CAP).9 Clinical test systems aresubject to rigorous certification by state entities as well,for example, the New York State Clinical LaboratoryEvaluation Program (CLEP). Laboratories located inand holding clinical laboratory permits from severalstate programs, including the New York CLEP program,have been granted exempt status by CMS from addi-tional accreditation under CLIA.10 The New York CLEPprogram is a well-known example of a very rigorous statelicensure program designed to ensure the accuracy andreliability of results of laboratory tests on specimens ob-tained within the state. For clinical laboratories andblood banks holding New York state permits, CLEP alsoperforms laboratory inspections, proficiency testing, andevaluation of laboratory personnel.10
In vitro diagnostic tests that are manufactured out-side the clinical laboratory and then distributed to 1 or
Molecular diagnostic tests performedin clinical laboratories have longbeen regulated by multiple federaland state agencies.

WWW.PERSONALIZEDMEDONC.COM 45Volume 1 • No 3 August 2012
more clinical laboratories must be cleared or approvedby the FDA prior to such distribution, although thesetests may be modified later by clinical laboratories underthe CLIA bridge testing and other validation require-ments. FDA also has authority over reagents and instru-mentation labeled for research use or investigationaluse, defined in regulations as in vitro diagnostic prod-ucts. Specifically, the FDA considers products labeledResearch Use Only (RUO) “…to be products that arein the laboratory research phase of development, thatis, either basic research or the initial search for potentialclinical utility, and not represented as an effective invitro diagnostic product.” During this phase, the focusof manufacturer-initiated studies is typically to evaluatelimited-scale performance and potential clinical or in-formational usefulness of the test. These products mustbe labeled “For Research Use Only. Not for use in diag-nostic procedures.”11 FDA does not require RUO prod-ucts to be cleared or approved by FDA since suchproducts are not “intended” to be used for clinical pur-poses. Likewise, no premarket review or notification isrequired by FDA for products labeled for InvestigationalUse Only (IUO) that are intended only for controlledinvestigations to gather performance data on productswith informed consent/Institutional Review Board ap-proval. However, such products have long been used inpractice by CLIA-accredited laboratories in tests offeredby such clinical laboratories and validated pursuant toCLIA standards and requirements in each laboratory.This practice of laboratory validation is widely acceptedand subject to the regulatory rigors of both state and fed-eral laboratory regulations. With regard to tests developed and performed by
clinical laboratories, known as laboratory-developedtests (LDTs), the FDA has long asserted that it has theauthority to require premarket review of LDTs under thelegal definition of “medical device” but has historicallydeferred to CMS to regulate LDTs at the federal levelunder CLIA. FDA’s policy of not requiring CLIA-ac-credited laboratories, including hospital and academicmedical center laboratories, to submit LDTs to FDAprior to offering such tests for clinical purposes is called
“enforcement discretion.” Importantly, FDA has appliedenforcement discretion only to those clinical diagnostictests it defines as LDTs, meaning “…for use in the diag-nosis of disease or other conditions that was developedby [CLIA] certified clinical laboratory for use in thatlaboratory” and are “neither an analyte-specific reagentnor are the components for research use only.”12 No-tably, FDA has taken enforcement action against labo-ratories performing tests as LDTs that have not beenentirely developed and validated in a single facility.13
FDA has asserted that even the provision of customizedreagents with instructions for clinical use or the transferof data alone, such as instructions for use, performance
characteristics, or protocols, between a manufacturer,research entity, CLIA laboratory, or other entity andCLIA laboratory, disqualifies the test as an LDT withenforcement discretion protection and subjects it to theFDA premarket review or notification requirements.13
FDA’s assertion of the existing framework for reviewand approval of traditional medical devices (like heartvalves) is not well suited for both LDTs and distributedin vitro diagnostic kits. Consequently, efforts are underway to establish more appropriate and least burdensomeregulatory policies, including evidentiary requirementsand review standards, to address stakeholder concernsspecific to in vitro diagnostic tests. These proposals rangefrom creating a new category of regulated product forrisk-based review of all in vitro diagnostic products underFDA while retaining CLIA oversight of laboratory op-erations and the actual performance of the test (thepremise of the draft legislation contemplated by US Sen-ator Orrin Hatch), to expanding the regulatory role ofCMS under CLIA and excluding FDA entirely fromLDT oversight (the premise of US House of Represen-tatives Bill 3207 introduced by Representative Michael
Regulatory Issues
FDA does not require RUO products to becleared or approved by FDA since suchproducts are not “intended” to be usedfor clinical purposes.

PERSONALIZED MEDICINE IN ONCOLOGY46 Volume 1 • No 3 August 2012
Regulatory Issues
Burgess), to creating a “transitional” class of novel or“emerging” in vitro diagnostic kits for which manufac-turers could obtain conditional clearance as part of theexisting medical device framework (identified as a po-tential approach in the most recent FDA agreement onreauthorization of medical device user fees).4,14,15
FDA Steps Into the Clinical LaboratoryAs the field of genomic testing began to evolve and
move increasingly into clinical practice, the FDA be-came concerned about the analytical and clinical valid-ity standards for genomic tests. In particular, the FDAis concerned with the risk of false-positive and false-neg-ative test results that would be incorporated into clinicaltreatment decisions for serious and life-threatening dis-eases such as cancer. Although FDA has long limited itspremarket oversight of in vitro diagnostic tests to thosethat constitute “kits” manufactured and sold or distrib-uted to clinical laboratories, in recent years the regula-
tory paradigms have begun to shift dramatically as moremultianalyte assays using algorithmic analysis and newfaster sequencing technologies, such as next-generationsequencing (NGS), have entered the field. The FDAhas struggled to find the most appropriate way to addressregulatory oversight where gaps between CLIA andFDA are perceived, yet, at the same time, avoid erectingfurther barriers to innovation.After failed attempts to target additional premarket
regulation to a more limited class of multianalyte LDTs,FDA announced in 2010 its intent instead to regulateLDTs broadly.16-18 However, the now years-long processFDA has undertaken to develop and publish Draft Guid-ance on LDT regulation has been stalled, first due tosubstantial concerns expressed by both stakeholders andgovernment policy makers regarding the awkward and
ill-defined approach taken by FDA to determine LDTspotentially subject to dual oversight by CLIA and FDA,and later due to broader-based concerns regarding thepotential negative impact the proposed policies wouldhave on the advancement of personalized medicine ingeneral. Nonetheless, the FDA remains committed andhas indicated that the Draft Guidance on LDT policyremains a priority for 2012 publication.19
In the meantime, top FDA officials continue to bevocal in expressing the agency’s distrust of the CLIAregulations to appropriately establish analytical andclinical validity of LDTs, whether single analyte, multi-analyte, or NGS based.20 And although stakeholdersand legal scholars alike have challenged the FDA’s as-sertion of authority over LDTs and the agency’s proposalto require FDA premarket oversight of LDTs absent for-mal rule making by the FDA [guidance documents can-not, as a matter of law, “create or confer any rights foror on any person.” See 21 U.S.C. Sec. 371(h)(1)(A)],the agency has proceeded to develop policies impactingLDTs through “draft” guidance documents, which lacktransparency of process and predictably of policy com-pared with regulations established through formal rulemaking.21
Still, the FDA has moved forward with the publicationof a plethora of other Draft Guidance related to in vitrodiagnostics, 2 of which could have immediate impact onclinical laboratories and LDTs: Draft Guidance for Indus-try and FDA Staff – Commercially Distributed In VitroDiagnostic Products Labeled for Research Use Only or In-vestigational Use Only: Frequently Asked Questions, June1, 2011 (Draft RUO/IUO Guidance); and Draft Guidancefor Industry and Food and Drug Administration Staff – InVitro Companion Diagnostic Devices, July 14, 2011(Draft Companion Diagnostic Guidance).22,23
Clinical Laboratory Use of ProductsLabeled Research or Investigation Use OnlyThe Draft RUO/IUO Guidance suggests that if a
manufacturer of products labeled RUO or IUO sells ordistributes those products to a clinical laboratory, and
Still, the FDA has moved forward withthe publication of a plethora of otherDraft Guidance related to in vitrodiagnostics...

WWW.PERSONALIZEDMEDONC.COM 47Volume 1 • No 3 August 2012
the manufacturer or distributor knows or should haveknown that a CLIA laboratory is using the products inclinical tests beyond research or investigational pur-poses, the manufacturer should “cease sales” to suchCLIA laboratory.23 This proposed requirement has beenwidely viewed as a departure from historic FDA enforce-ment policy, which requires a manufacturer to advertiseor promote the product as validated for clinical use, notmerely sell to a clinical laboratory. Moreover, the sug-gestion that the burden is on manufacturers to under-stand the ultimate use of products sold to third partiesand to cease sales if such “known” use is inconsistentwith the manufacturer’s label, absent unlawful promo-tion or advertising of the product, has caused widespreadconcern among laboratories and other stakeholders.23
Many reagents and components are available to clinicallaboratories only as RUO products, but the FDA has an-nounced its intent to step up enforcement against man-ufacturers that sell products to clinical laboratories withan RUO label rather than seeking separate clearance orapproval for such RUO diagnostic “kits” under theFDA’s medical device regulations.22
Contrary to widely accepted laboratory practiceunder CLIA, the FDA has asserted in this Draft Guid-ance that validation of the performance specificationsof such products as part of a test legally offered to pa-tients by the laboratory under CLIA regulations (or statelicensure laws for those states exempt from CLIA, likeNew York) does not extinguish the responsibility of themanufacturer to properly label its products based on theuse of the product by the laboratory. However, theagency specifically exempted CLIA laboratories fromenforcement action by FDA for using RUO- or IUO-labeled products in clinical tests. This was an importantpublic health decision given the necessity of many ofthese products in widely used clinical tests. Moreover,the FDA made it clear in the guidance that it was notintended to be a mechanism to modify or limit the pol-icy of “enforcement discretion” for LDTs generally.22
Nevertheless, the widespread and accepted use of prod-ucts labeled RUO or IUO by clinical laboratories ascomponents of tests developed and validated in those
CLIA laboratories, uncertainty about the trigger for themanufacturer “awareness” of purchaser use of its prod-ucts, and the related requirement to “cease sales” to lab-oratories when such “knowledge” is achieved, hascreated regulatory uncertainty and confusion. The po-tential disruption of physician orders for thousands ofclinical laboratory tests and the resulting detrimental
impact on public health, as described in public com-ments on this Draft Guidance, has prompted criticismand a congressional inquiry into this FDA policy in par-ticular, and use of Draft Guidance, more generally to es-tablish or modify its enforcement policy.24,25 Consistentwith previous public comments from agency officials,FDA responded to the congressional inquiry by citingits established regulations on labeling requirements formedical devices and suggesting that products labeledRUO/IUO are generally not manufactured under GoodManufacturing Practice guidelines and may lack impor-tant design controls.26 These are important publichealth concerns and of particular importance to theFDA in the context of driving treatment or clinical trialselection decisions in serious or life-threatening diseases like cancer, but it fails to recognize the impor-tant role of CLIA to ensure clinical tests are properlyvalidated for use in patient treatment and management(Figure 1).
Regulatory Issues
Figure 1. FDA Perspective on Companion LDTs
Without Additional FDA Regulatory Oversight“Health care practitioners rely on information from companion di-
agnostic [tests] to help make critical treatment decisions…if companion[test] results are incorrect, it is worse than if there had not been a testat all.” As to enforcement [for companion diagnostic tests], “FDA ex-pects to require compliance with the device regulations, whether the testis lab-developed or distributed as a kit.”27
The agency exempted CLIA laboratoriesfrom enforcement action by FDA for usingRUO- or IUO-labeled products in clinical tests.

PERSONALIZED MEDICINE IN ONCOLOGY48 Volume 1 • No 3 August 2012
“Companion Diagnostics” as EssentialDrivers of Precision OncologyGenomic-based assays have become critical tools and
are more frequently becoming accepted standard of carein clinical guidelines for oncology.28-30 For tests thatFDA has deemed “essential” for the safe and effectiveuse of a novel therapeutic product, its new Draft Com-panion Diagnostics Guidance will require the compan-ion test to be approved by FDA before the drug productcan be approved and labeled, whether developed by aclinical laboratory and offered as an LDT or manufac-
tured and distributed as a “kit” to clinical laboratories.23
Following the publication of this Draft Guidance, FDAquickly approved 2 such companion diagnostics andnovel drugs, illustrating how the FDA considers thesetypes of dual product approvals (Figure 2).�Like the Draft Guidance for products labeled RUO
or IUO, the FDA has continued to maintain the policyof “enforcement discretion” under the Companion Di-agnostics Draft Guidance for LDTs pending the publi-cation of the long-anticipated LDT Draft Guidance.While a companion diagnostic cleared or approved byFDA may be developed as an LDT by a clinical labora-tory or by a manufacturer as a test “kit,” FDA at thistime is only requiring a single test be approved with thetherapeutic.23 This means that all other LDTs offered forthe same purpose by CLIA-accredited laboratories be-
fore, or even after, the FDA approves a companion di-agnostic for the same purpose may remain on the marketand will not be required to seek additional FDA ap-proval as long as the test meets the FDA’s definition ofLDT.23 Additionally, in the practice of medicine, physi-cians are not bound by federal regulatory authorities tochoose a particular test or therapy for any given patient.FDA has complicated the marketplace for companiondiagnostics further by using only a test description in thedrug product labeling rather than the proprietary nameof the FDA-approved test (eg, the drug label requirestesting using an “FDA-approved” BRAF V600E test).23,33
Given the substantial investment necessary to meet theFDA standards for a Class III Premarket Application fora medical device coupled with the lack of requirementsfor CLIA laboratories performing LDT companion di-agnostic testing to seek additional FDA approval, it isunlikely FDA will be flooded with applications for ap-proval of LDTs offered in clinical oncology that are of-fered as a “companion” to an approved drug.FDA has announced it hopes to publish “final” Com-
panion Diagnostics Guidance this year,20 but unless theagency establishes a new framework for LDTs that is not overly burdensome, duplicative of, or contradictoryto CLIA, and physicians find greater medical value intests approved by FDA than those offered by trusted lab-oratories accredited by CLIA or accredited state pro-grams, it will be difficult to discern meaningful impactfrom the FDA review of companion diagnostics on thepractice of medicine.
Implications of New Technologies onCompanion Diagnostics in OncologyThe rapid advances of NGS and other medical infor-
mation processing technologies have created incredibleexcitement in the field of oncology, in particular. At thesame time, FDA remains deeply concerned about thelack of tools to evaluate the accuracy, reliability, andclinical validity of test results based on these rapidly ad-vancing technologies. A senior FDA official describedthe view of the agency as deep concern about “…therapid ability to transfer from research to clinical use.”27
Regulatory Issues
Figure 2. Recent FDA Companion Diagnostics
Approvals
• Pfizer’s Xalkori (crizotinib) for the treatment of locally advanced or metastatic NSCLC in EML4-ALK fusion gene–positive patients— Companion Dx: Abbott Molecular’s Vysis ALK Break Apart FISH Probe Kit for tumor testing to select which patients will respond to this drug31
• Roche’s melanoma drug Zelboraf for BRAF gene mutation–positive patients— Companion Dx: Roche’s BRAF V600E mutation to select which patients will respond to this drug32

WWW.PERSONALIZEDMEDONC.COM 49Volume 1 • No 3 August 2012
FDA has held a public meeting on novel sequencing is-sues and, in addition to companion diagnostics, alsopublished Draft Guidance on Mobile Apps in 2011.34,35
The FDA already regulates certain standalone softwareas a “medical device,” and the agency is working to up-date its policy with respect to regulatory requirementsfor clinical decision support tools that process informa-tion intended for use in the diagnosis, cure, mitigation,treatment, or prevention of disease.With respect to use of these technological advances
in clinical laboratories, while manufacturers and clinicallaboratories continue to await new regulatory require-ments and standards from the FDA, third-party accred-itation entities and professional societies continue topress forward to advance personalized medicine. For ex-ample, CAP published guidelines in 2009 for validatingmolecular tests in clinical laboratories, and the Ameri-can College of Medical Genetics and Genomics pub-lished a policy statement, “Points to Consider in theClinical Application of Genomic Sequencing,” in early2012. These recommendations, in the absence of moredefinitive statements by the FDA on LDTs, in particulartests using NGS and other advanced information tech-nology platforms, will continue to drive best practicesand standards for both analytical and clinical validitythat will usher in the new era of precision media in oncology.36,37
Achieving the Next Generation – theOutlook for Personalized Medicine inOncologyThe FDA’s move toward greater oversight of the
clinical validity of genomic-based tests has, thus far, notresulted in a path to personalized medicine paved withgreater clarity, certainty, and confidence. Regardless,physicians and patients alike continue to seek increas-ingly individualized genomic-based treatment options.Given the accelerated pace of new discoveries in se-quencing and information technologies as well as clini-cal applications, the promise of continued advancementin genomic pathology that will drive greater precisionin medical and clinical oncology likely will continue to
be measured by new regulatory hurdles. The challengefor federal policy makers at both CMS and FDA, Con-gress and, to some extent, the federal courts, will be to
balance new regulatory paradigms to support continuedinvestment in innovative technologies and diagnostictest capabilities without creating overly burdensomebarriers or duplicative and overlapping requirementsthat in practice fail to support public health.
Disclosure StatementS. Walcoff is a consultant to various stakeholders in
genomics and personalized medicine, including clinicallaboratories, biotechnology and pharmaceutical compa-nies, investors, coalitions, and diagnostic device manu-facturers. She has received no financial compensationor other content contribution for this work, and thepaper has not been shared with her clients prior to publication. u
References1. Division of Laboratory Systems, National Center for Preparedness, De-tection, and Control of Infectious Diseases, Centers for Disease Controland Prevention. Laboratory Medicine: A National Status Report. www.futurelabmedicine.org/pdfs/2007%20status%20report%20laboratory_medicine_-_a_national_status_report_from_the_lewin_group.pdf. May 2008.Accessed April 2012.2. Faulkner E. Clinical utility or impossibility? Addressing the moleculardiagnostics health technology assessment and reimbursement conundrum.Journal of Managed Care Medicine. 2009;12:42-55.3. Simon CJ, Wolcott J, Hogan P. Can We Reduce Health Care Spending?Searching for Low-Hanging Fruit in the Garden of Health System Reform.www.optuminsight.com/~/media/Ingenix/Resources/Articles/LewinReportCostDrivers.pdf. October 26, 2009. Accessed April 2012.4. Ray T. Latest draft of Hatch IVD bill contains new regulatory proposals;pricing reforms under discussion. Pharmacogenomics Reporter.www.genomeweb.com/dxpgx/latest-draft-hatch-ivd-bill-contains-new-regulatory-proposals-pricing-reforms-un. July 6, 2011. Accessed April 2012.5.UnitedHealth Group. Personalized Medicine: Trends and prospects for the newscience of genetic testing and molecular diagnostics.www.unitedhealthgroup.com/hrm/UNH_WorkingPaper7.pdf. March 2012. Accessed April 2012.6. 21 U.S.C. § 301 et seq.7. 21 U.S.C. 321(h); see 21 CFR 809.3(a).8. 42 CFR 493.1253(b)(2).9. College of American Pathologists. Accreditation and laboratory im-provement. www.cap.org/apps/cap.portal?_nfpb=true&_pageLabel=accred
Regulatory Issues
FDA has complicated the marketplace forcompanion diagnostics further by usingonly a test description in the drug productlabeling...

PERSONALIZED MEDICINE IN ONCOLOGY50 Volume 1 • No 3 August 2012
itation. Accessed April 2012.10. Wadsworth Center. New York State Department of Health. ClinicalLaboratory Evaluation Program Web site. www.wadsworth.org/labcert/clep/clep.html. Accessed April 2012.11. 21 CFR 809.10 (c)(2)(i).12. US Food and Drug Administration. Product Classification. www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfPCD/PCDSimpleSearch.cfm?db=PCD&id=OQS. Accessed April 2012.13.US Food and Drug Administration. Inspections, Compliance, Enforce-ment, and Criminal Investigation. FDA warning letter on OvaSure.www.fda.gov/ICECI/EnforcementActions/WarningLetters/2008/ucm1048114.htm. Accessed April 2012.14. H.R. 2307: Modernizing Laboratory Test Standards for Patients Actof 2011. www.govtrack.us/congress/bills/112/hr3207.15. US Food and Drug Administration. FDA commitment letter on theMedical Device and User Fee Modernization Act (MDUFMA). www.fda.gov/MedicalDevices/DeviceRegulationandGuidance/Overview/MedicalDeviceUserFeeandModernizationActMDUFMA/ucm293728.htmletter. Ac-cessed April 2012.16.Hamburg MA, Collins FS. The path to personalized medicine. N EnglJ Med. 2010;363:301-304.17.Notice of Public Meeting on FDA Oversight of Laboratory DevelopedTests. Federal Register. June 17, 2010:34463-34464.18. FDA to drop IVDMIA policy. BioCentury Today. www.biocentury.com/dailynews/politics/2010-06-16/fda-to-drop-ivdmia-policy. June 16,2010. Accessed April 2012.19.Documents the Center for Devices and Radiological Health is consid-ering for development (FY12). www.fda.gov/MedicalDevices/DeviceRegulationandGuidance/Overview/MedicalDeviceUserFeeandModernizationActMDUFMA/ucm109196.htm. Accessed April 2012.20. Bureau of National Affairs, Inc. Personalized medicine: co-approvalsaid necessary to market companion diagnostic test, therapeutic. RegulatoryNews. 2012;6:180-181.21. Javitt GH, Garnder KS. Must FDA engage in rulemaking to regulatelaboratory-developed tests? Food and Drug Law Institute Policy Forum.www.sidley.com/f i les /Publicat ion/d83df2d8-e7a8-4159-8cf f -57bc99413ebe/Presentation/PublicationAttachment/9ab25938-f024-4f9d-9535-58be237fd31f/FDLI%20Policy%20Forum%2017.pdf. September 14,2011. Accessed April 2012.22.US Food and Drug Administration. Draft Guidance for Industry and FDAStaff – Commercially Distributed In Vitro Diagnostic Products Labeled forResearch Use Only or Investigational Use Only: Frequently Asked Questions.www.fda.gov/medicaldevices/deviceregulationandguidance/guidancedocuments/ucm253307.htm. June 1, 2011. Accessed April 2012.23. US Food and Drug Administration. Draft Guidance for Industry andFood and Drug Administration Staff – In Vitro Companion Diagnostic De-vices. www.fda.gov/medicaldevices/deviceregulationandguidance/guidancedocuments/ucm262292.htm. July 14, 2011. Accessed April 2012.24. Public comments to FDA Draft Guidance for Industry and FDA Staff:Commercially Distributed In Vitro Diagnostic Products Labeled for Re-search Use Only or Investigational Use Only: Frequently Asked Questions;Availability. www.regulations.gov/#!docketDetail;dct=FR%252BPR%252
BN%252BO%252BSR%252BPS;rpp=25;po=0;D=FDA-2011-D-0305.Accessed April 2012.25.One Hundred Twelfth Congress. Congress of the United States. Houseof Representatives. Committee on Energy and Commerce. Letter to theFDA regarding June 1 draft guidance document. http://Republicans.EnergyCommerce.house.gov/Media/file/Letters/112th/031912FDA.pdf. Ac-cessed April 2012.26. One Hundred Twelfth Congress. Congress of the United States. Houseof Representatives. Committee on Energy and Commerce. FDA responseletter to Energy and Commerce Committee inquiry regarding June 1 draftguidance document. http://republicans.energycommerce.house.gov/news/letters.aspx. Accessed April 2012.27.Mansfield E. Development of the companion diagnostic draft guidance.Presented at: 4th Annual Forum for Payers on Personalized Medicine; March12-13, 2012; Washington, DC. www.cbinet.com/compendiums/FC12020/Presentations/Mansfield_Elizabeth_pres.pdf. Accessed April 2012.28.National Comprehensive Cancer Network. NCCN updates guidelinesfor colorectal cancer. www.nccn.org/about/news/newsinfo.asp?NewsID=194. Accessed April 2012.29.National Comprehensive Cancer Network. NCCN updates breast can-cer guidelines. www.nccn.org/about/news/newsinfo.asp?NewsID=127. Ac-cessed April 2012.30. Harris L, Fritsche H, Mennel R, et al. American Society of ClinicalOncology 2007 update of recommendations for the use of tumor markersin breast cancer. J Clin Oncol. 2007;25:5287-5312.31. US Food and Drug Administration. News & Events. FDA approvesXalkori with companion diagnostic for a type of late-stage lung cancer.www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm269856.htm. August 17, 2011. Accessed April 2012.32. US Food and Drug Administration. News & Events. FDA approvesZelboraf and companion diagnostic test for late-stage skin cancer.www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm268241.htm. August 17, 2011. Accessed April 2012.33. Zelboraf [package insert]. South San Francisco, CA: Roche; 2011.Highlights of prescribing information. www.gene.com/gene/products/information/zelboraf/pdf/pi.pdf. Accessed April 2012.34. US Food and Drug Administration. Medical Devices. Ultra highthroughput sequencing for clinical diagnostic applications – approaches toassess analytical validity, June 23, 2011.www.fda.gov/MedicalDevices/NewsEvents/WorkshopsConferences/ucm255327.htm. Accessed April 2012.35. US Food and Drug Administration. Medical Devices. Draft guidancefor industry and food and drug administration staff – mobile medical ap-plications. www.fda.gov/medicaldevices/deviceregulationandguidance/guidancedocuments/ucm263280.htm. July 21, 2011. Accessed April 2012.36. Jennings L, Van Deerlin VM, Gulley ML; College of American Pathol-ogists Molecular Pathology Resource Committee. Recommended princi-ples and practices for validating clinical molecular pathology tests. ArchPathol Lab Med. 2009;133:743-755.37. American College of Medical Genetics and Genomics. Policy state-ment on clinical application of whole genomic sequencing. www.acmg.net/AM/Template.cfm?Section=Home3&Template=/CM/HTMLDisplay.cfm&ContentID=6980. March 28, 2012. Accessed April 2012.
Regulatory Issues
SECOND ANNUAL CONFERENCE
��������������� ��� �����#
Clinical Approaches to Targeted Technologies#
REGISTER TODAY AT www.globalbiomarkersconsortium.com
October 4-6, 2013The Seaport Boston Hotel • 1 Seaport Lane • Boston, MA 02210
✓
Image: Colored scanning electron micrograph (SEM) of a lung cancer cell.
One focus: a shared commitment to improve the lives of cancer patients everywhere.
Millennium: The Takeda Oncology Company is developing an extensive pipeline — among the top
in oncology worldwide — with more than 17 compounds in development for a broad range of solid
and hematological cancers.
Our pipeline — rich in novel compounds — includes multiple candidates that target seven disease
pathways: protein homeostasis, anti-angiogenesis, growth-signaling inhibition, cell-cycle inhibition,
apoptosis, immunomodulators and hormone regulation.
To make a dramatic impact on cancer therapeutics, we are dedicated to a strong partnership with
the oncology community.
©2012 Millennium Pharmaceuticals, Inc. All rights reserved.
To learn more, visit us at millennium.com.
5:30 PM

PERSONALIZED MEDICINE IN ONCOLOGY52 Volume 1 • No 3 August 2012
Breast Cancer
Prognostication in breast cancer is an inexact sci-ence, with tumor (and patient) heterogeneitylikely contributing to this lack of prognostic pre-
cision. For example, even in patients traditionally con-sidered at low risk for recurrence (ie, those who are T1,N0, ER+), about 15% will have a recurrence within 10years with tamoxifen treatment alone.1 Therefore, muchinterest surrounds the field of personalized medicine,which aims to identify patients at high risk of recurrenceand to tailor therapy specifically for those patients. It ishoped that personalized medicine will bring to the clinicnewer drugs that target this high-risk population and
avoid overtreating patients who have an overall goodprognosis, and avoid costly side effects as well.
Prognostic IndexesOver the past decade, a number of decision-making
tools have become available to help healthcare profes-sionals and patients with early cancer discuss the risksand benefits of getting adjuvant therapy after surgery.One of these tools is Adjuvant! Online 8.0,2 a Web-based validated tool that predicts 10-year outcomes withand without adjuvant systemic therapy for patients withearly breast cancer.3,4 Adjuvant! Online incorporates theupdated St. Gallen consensus guidelines,5 the NationalComprehensive Cancer Network guidelines,6 the Up-date of the Oxford Overview,7 the Early Breast CancerTrialists’ Collaborative Group meta-analysis,8 as well asclinical trial information in the literature and reportedat major breast cancer meetings, including informationon the 7 major aromatase inhibitor trials, the 5 majoradjuvant trastuzumab trials, and the new trials that in-corporate taxanes into adjuvant therapy.When a patient’s data (eg, patient age, tumor size,
nodal involvement, histologic grade, etc) are enteredinto Adjuvant! Online, the program estimates the riskof negative outcome (cancer-related mortality or
Key Points
• A number of decision-making tools have become available to help clinicians and patients with early cancer discuss the risks and benefits of getting adjuvant therapy after surgery
• Adjuvant! Online 8.0 estimates the risk of negative outcome (cancer-related mortality or relapse) without sys-temic adjuvant therapy, the reduction of these risks afforded by therapy, and the risks of side effects of the therapy
• Gene-profiling assays, such as Oncotype DX and MammaPrint, are commercially available to help identify patients at high risk of recurrence
Case• A 52-year-old woman recently underwent surgery for a stageIA, 1.5-cm, right breast tumor (grade 2 invasive ductile car-cinoma, estrogen receptor [ER]-positive, progesterone re-ceptor [PR]-positive, and HER2-negative)
• Her biopsy showed no vascular invasion, negative surgicalmargins, and 2 negative lymph nodes
• You feel she should receive adjuvant radiation therapy andendocrine therapy, but how do you decide whether sheshould receive adjuvant chemotherapy?
Which Breast Cancer Patients Should ReceiveAdjuvant Chemotherapy?Tools to Aid Decision MakingAt the 2012 conference of the Global Biomarkers Consortium, which took place March 9-11, 2012, inOrlando, Florida, Alvaro Moreno-Aspitia, MD, from the Mayo Clinic in Jacksonville, Florida, discussed the useof personalized therapy in the management of breast cancer.

WWW.PERSONALIZEDMEDONC.COM 53Volume 1 • No 3 August 2012
Breast Cancer
Assay Company Description
Oncotype DX Breast Genomic Health A 21-gene assay that provides an individualized prediction ofCancer Assay adjuvant chemotherapy benefit and 10-year distant recurrence.
MammaPrint Agendia Analyzes 70 critical genes that comprise a definitive gene expression signature and stratifies patients into 2 distinct groups – those with low risk or high risk of distant recurrence.
BluePrint Agendia An 80-gene expression signature that classifies breast cancer intobasal-type, luminal-type, and ERBB2-type cancers.
TargetPrint Agendia A microarray-based gene expression test that quantitatively assesses the level of ER, PR and HER2/neu overexpression within the tumor.
TheraPrint Agendia A microarray-based gene expression panel of 56 genes that have been identified as potential targets for prognosis and therapeutic response to a variety of therapies.
PAM50 Breast Cancer ARUP Laboratories A real-time quantitative polymerase chain reaction assay that Intrinsic Classifier measures the expression of 50 classifier genes and 5 control genes
to identify the intrinsic subtypes known as luminal A, luminal B, HER2-enriched, and basal-like.
OncoVue Breast Cancer InterGenetics A genetic-based breast cancer risk test that incorporates bothRisk Test individualized genetic-based single-nucleotide polymorphisms
and personal history measures to estimate a woman’s breast cancer risk.
Pathwork Tissue of Pathwork Diagnostics A gene expression–based test that uses a tumor’s own genomicOrigin Test information to aid in identifying challenging tumors, including
metastatic, poorly differentiated, and undifferentiated tumors.
Pathwork Mutation Tests Pathwork Diagnostics KRAS, BRAF, and EGFR mutation testing to help determine whether patients will respond to targeted therapies.
ER indicates estrogen receptor; PR, progesterone receptor.
Table 1. Commercially Available Genomic Assays
relapse) without systemic adjuvant therapy, the reduc-tion of these risks afforded by therapy, and the risks ofside effects of the therapy. These estimates are then pro-vided on printed sheets in simple graphic and text for-mats to be used in consultations with patients and maybe useful in supporting decision making.
Gene Profiling of TumorBecause the patient’s father had a rough time with
chemo therapy for lung cancer, the patient still wasn’tconvinced, and asked, “Is there anything else that youcan provide to help me make a decision?” Indeed, sev-
eral genomic assays are commercially available (Table1). Among these gene-profiling assays, Oncotype DXand MammaPrint are the most mature.
Oncotype DXThe OncotypeDX assay analyzes the expression of 21
genes by reverse transcriptase-polymerase chain reaction
Indeed, several genomic assays arecommercially available. Among thesegene-profiling assays, Oncotype DX andMammaPrint are the most mature.

PERSONALIZED MEDICINE IN ONCOLOGY54 Volume 1 • No 3 August 2012
Breast Cancer
to provide an individualized Recurrence Score (RS;from 0 to 100) for each patient.9,10 In addition to quan-tifying breast cancer recurrence risk, the Oncotype DXassay also assesses the benefit from chemotherapy.
Node-Negative, ER-Positive Breast CancerThe data from which the assay was developed were
retrospectively analyzed from a prospective randomizedtrial known as the National Surgical Adjuvant Breastand Bowel Project Study B-20, which compared thecombination of chemotherapy (ie, 6 cycles of cyclophos-phamide, methotrexate, and 5-fluorouracil) plus hor-monal therapy (ie, tamoxifen) with hormonal therapyalone in 651 women with lymph node–negative, ER-positive breast cancer. Patients with an RS lower than
18 are categorized as low risk. These patients do well,with over 90% of patients alive at 10 years. Patientswith an RS of 31 or higher are considered as high riskof recurrence. Those with scores in the middle (18 to<31) are classified as intermediate risk (Figure 1).9
When the Oncotype DX assay was used for the pa-tient in this case, an RS of 27 was obtained, which puther in the intermediate-risk group (Figure 2). In thatcase, her risk of distant recurrence is about 17%, whichis actually similar to the estimated recurrence rate foundwith Adjuvant! Online.
Node-Positive, ER-Positive Postmenopausal Breast CancerFor lymph node–positive, ER-positive postmeno -
pausal patients treated with tamoxifen, the OncotypeDX report form now includes data retrospectively ana-lyzed from the prospective randomized Southwest On-
cology Group (SWOG) 8814 study, which evaluatedthe risk of recurrence or death versus the RS result (bothprognosis and likelihood of chemotherapy benefit). Inthe SWOG 8814 study, 1477 women were randomizedto receive either tamoxifen alone for 5 years (n=361),or 6 cycles of chemotherapy with cyclophosphamide,doxorubicin, and fluorouracil (CAF) with concurrenttamoxifen (n=550), or 6 cycles of CAF followed by ta-moxifen (CAF-T).11 Among the groups of women withRS <18 (the low-risk group) or 18 to 30 (intermediate-risk group), CAF-T offered no significant advantageover the 10-year disease-free or overall survival ratesseen among those who received tamoxifen alone. Incontrast, among the women who had RS ≥31, the 10-year disease-free and overall survival rates were signifi-cantly greater with CAF-T than with tamoxifen alone.
Prospective, Randomized Trials Under WayWhile the Oncotype DX is currently based on retro-
spective data from the 2 aforementioned prospectiverandomized clinical trials, prospective studies are ongo-ing. One prospective study, known as the Trial Assign-ing Individualized Options for Treatment (Rx)(TAILORx), is examining whether chemotherapy is re-quired for the intermediate-risk group defined by theRS.12 Another prospective randomized trial, known asthe Rx for Positive Node, Endocrine Responsive BreastCancer (RxPONDER, or SWOG S1007) study, openedin January 2011 and will assess whether chemotherapybenefits patients with node-positive breast cancer whohave low to intermediate RS. The trial will also examinewhether there is an optimal RS cutoff point for thesepatients, above which chemotherapy should be recom-mended. This study includes women with RS ≤25 whohave early-stage, hormone receptor–positive, HER2-
Case (cont)
• What if the patient in our case has 2 macroscop-ically (0.5 cm each without extracapsular exten-sion) involved sentinel lymph nodes?
While the Oncotype DX is currently basedon retrospective data from the 2aforementioned prospective randomizedclinical trials, prospective studies areongoing.

WWW.PERSONALIZEDMEDONC.COM 55Volume 1 • No 3 August 2012
Breast Cancer
negative breast cancer that has been found to involve 1to 3 lymph nodes.
MammaPrintMammaPrint analyzes 70 genes that comprise a de-
finitive gene expression signature and stratifies patientsto 1 of 2 groups: those with low risk of distant recurrence(good signature group) and those with high risk of
distant recurrence (poor signature group).13 WithMammaPrint, there are no intermediate results. Patientswho have a good signature do quite well, with less than20% experiencing a relapse 10 years after their diagno-sis, while patients with a poor signature do poorly over-all, with about 50% to 60% experiencing relapse.14 Keydifferences between MammaPrint and OncotypeDX arelisted in Table 2.
A, all patients; B, low risk (RS <18); C, intermediate risk (RS 18-30); D, high risk (RS ≥31).
RS indicates Recurrence Score.
Paik S, Tang G, Shak S, et al. Gene expression and benefit of chemotherapy in women with node-negative, estrogen receptor–positive breast cancer.J Clin Oncol. 2006;24:3726-3734. Reprinted with permission. © 2006 American Society of Clinical Oncology. All rights reserved.
Figure 1. Kaplan-Meier Plots for Distant Recurrence Comparing Treatment With Tamoxifen (Tam)Alone Versus Treatment With Tamoxifen Plus Chemotherapy (Tam + chemo)

PERSONALIZED MEDICINE IN ONCOLOGY56 Volume 1 • No 3 August 2012
Breast Cancer
MammaPrint is being evaluated in a clinical trialknown as Microarray In Node-negative and 1-3 positivelymph node Disease may Avoid ChemoTherapy (MIN-DACT), which is a randomized European study com-paring MammaPrint with clinical assessment.15
MINDACT has enrolled over 6000 patients, who havebeen classified into high or low genomic risk byMammaPrint and clinicopathologic risk through Adju-vant! Online. Patients with both genomic and clinicalhigh risks are offered adjuvant chemotherapy; thosewith both genomic and clinical low risks do not receivechemotherapy; patients with discordant risk are ran-domized for the decision of adjuvant chemotherapy
based on genomic or clinical risk.15 MINDACT is dueto complete data collection in 2019. u
References1. Fisher B, Redmond C. Systemic therapy in node-negative patients: up-dated findings from NSABP clinical trials. National Surgical AdjuvantBreast and Bowel Project. J Natl Cancer Inst Monogr. 1992;(11):105-116.2. Adjuvant Inc. Adjuvant! Online 8.0. www.adjuvantonline.com/index.jsp. Accessed July 23, 2012. 3. Olivotto IA, Bajdik CD, Ravdin PM, et al. Population-based validationof the prognostic model ADJUVANT! for early breast cancer. J Clin Oncol.2005;23:2716-2725.4. Mook S, Schmidt MK, Rutgers EJ, et al. Calibration and discriminatoryaccuracy of prognosis calculation for breast cancer with the online Adju-vant! program: a hospital-based retrospective cohort study. Lancet Oncol.2009;10:1070-1076.5. Gnant M, Harbeck N, Thomssen C. St. Gallen Consensus Discussion.Breast Care (Basel). 2011;6:136-141.6. National Comprehensive Cancer Network guidelines. www.nccn.org/professionals/physician_gls/pdf/breast.pdf.
Figure 2. Case Example: Patient With Oncotype DX Recurrence Score of 27
From Paik S, Shak S, Tang G, et al. A multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancer. N Engl JMed. 2004;351:2817-2826. Copyright © 2004 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
Recurrence Score as Continuous Predictor
Rate of Distant Recurrence
at 10 Years
0 5 10 15 20 25 30 35 40 45 50
40%
35%
30%
25%
20%
15%
10%
5%
0%
Recurrence Score
Intermediate RiskLow Risk High Risk
Rate95% Confidence Interval
MammaPrint Oncotype DX
Analyzes messenger RNA signals for 70 genes Measures the expression of 21 genes using PCR
Can be used to test patients with any ER status Approved only for ER-positive patients
Predictive (ie, it can be used to predict treatment benefit) Prognostic (ie, it can be used to estimate recurrence risk) and predictive (ie, it can be used to predict treatment benefit)
ER indicates estrogen receptor; PCR, polymerase chain reaction.
Table 2. Key Differences Between MammaPrint and Oncotype DX
WWW.PERSONALIZEDMEDONC.COM 57Volume 1 • No 3 August 2012
Breast Cancer
7. Pritchard KI, Bergh J, Burstein HJ. Update of the Oxford Overview.www.asco.org/ASCOv2/Home/Education%20&%20Training/Educational%20Book/PDF%20Files/2012/zds00112000071.PDF.8. Early Breast Cancer Trialists’ Collaborative Group (EBCTCG), PetoR, Davies C, et al. Comparisons between different polychemotherapy reg-imens for early breast cancer: meta-analyses of long-term outcome among100,000 women in 123 randomised trials. Lancet. 2012;379:432-444.9. Paik S, Tang G, Shak S, et al. Gene expression and benefit ofchemotherapy in women with node-negative, estrogen receptor-positivebreast cancer. J Clin Oncol. 2006;24:3726-3734.10. Paik S, Shak S, Tang G, et al. A multigene assay to predict recurrenceof tamoxifen-treated, node-negative breast cancer. N Engl J Med.2004;351:2817-2826.11. Albain K, Barlow W, Shak S, et al. Prognostic and predictive value ofthe 21-gene recurrence score assay in postmenopausal, node-negative ER-positive breast cancer. Presented at: 30th Annual San Antonio BreastCancer Symposium, San Antonio, TX. 2007. Abstract LBA10.12. Sparano JA, Paik S. Development of the 21-gene assay and its appli-cation in clinical practice and clinical trials. J Clin Oncol. 2008;26:721-728.13. van ’t Veer LJ, Dai H, van de Vijver MJ, et al. Gene expression profil-ing predicts clinical outcome of breast cancer.Nature. 2002;415:530-536.14. van de Vijver MJ, He YD, van ’t Veer LJ, et al. A gene-expression sig-nature as a predictor of survival in breast cancer. N Engl J Med.2002;347:1999-2009.15. Rutgers E, Piccart-Gebhart MJ, Bogaerts J, et al. The EORTC10041/BIG 03-04 MINDACT trial is feasible: results of the pilot phase.Eur J Cancer. 2011;47:2742-2749.
Solution for intravenous infusion Initial U.S. Approval: 2004
WARNING: GASTROINTESTINAL PERFORATIONS, SURGERY AND WOUND HEALING COMPLICATIONS, and HEMORRHAGE
Gastrointestinal PerforationsThe incidence of gastrointestinal perforation, some fatal, in Avastin-treated patients ranges from 0.3 to 2.4%. Discontinue Avastin in patients with gastrointestinal perforation. [See Dosage and Administration (2.4), Warnings and Precautions (5.1).]
Surgery and Wound Healing Complications
The incidence of wound healing and surgical complications, including serious and fatal complications, is increased in Avastin-treated patients. Discontinue Avastin in patients with wound dehiscence. The appropriate interval between termination of Avastin and subsequent elective surgery required to reduce the risks of impaired wound healing/wound dehiscence has not been determined. Discontinue at least 28 days prior to elective surgery. Do not initiate Avastin for at least 28 days after surgery and until the surgical wound is fully healed. [See Dosage and Administration (2.4), Warnings and Precautions (5.2), Adverse Reactions (6.1).]
Hemorrhage
Severe or fatal hemorrhage, including hemoptysis, gastrointestinal bleeding, central nervous systems (CNS) hemorrhage, epistaxis, and vaginal bleeding occurred up to �ve-fold more frequently in patients receiving Avastin. Do not administer Avastin to patients with serious hemorrhage or recent hemoptysis. [See Dosage and Administration (2.4), Warnings and Precautions (5.3), Adverse Reactions (6.1).]
1 INDICATIONS AND USAGE1.1 Metastatic Colorectal Cancer (mCRC)Avastin is indicated for the �rst- or second-line treatment of patients with metastatic carcinoma of the colon or rectum in combination with intravenous 5-�uorouracil–based chemotherapy.
1.2 Non-Squamous Non–Small Cell Lung Cancer (NSCLC)Avastin is indicated for the �rst-line treatment of unresectable, locally advanced, recurrent or metastatic non–squamous non–small cell lung cancer in combination with carboplatin and paclitaxel.
1.3 GlioblastomaAvastin is indicated for the treatment of glioblastoma with progressive disease in adult patients following prior therapy as a single agent.The effectiveness of Avastin in glioblastoma is based on an improvement in objective response rate. There are no data demonstrating an improvement in disease-related symptoms or increased survival with Avastin. [See Clinical Studies (14.3).]
1.4 Metastatic Renal Cell Carcinoma (mRCC)Avastin is indicated for the treatment of metastatic renal cell carcinoma in combination with interferon alfa.
4 CONTRAINDICATIONSNone.
5 WARNINGS AND PRECAUTIONS5.1 Gastrointestinal PerforationsSerious and sometimes fatal gastrointestinal perforation occurs at a higher incidence in Avastin treated patients compared to controls. The incidence of gastrointestinal perforation ranged from 0.3 to 2.4% across clinical studies. [See Adverse Reactions (6.1).]The typical presentation may include abdominal pain, nausea, emesis, constipation, and fever. Perforation can be complicated by intra-abdominal abscess and �stula formation. The majority of cases occurred within the �rst 50 days of initiation of Avastin.Discontinue Avastin in patients with gastrointestinal perforation. [See Boxed Warning, Dosage and Administration (2.4).]
5.2 Surgery and Wound Healing ComplicationsAvastin impairs wound healing in animal models. [See Nonclinical Toxicology (13.2).] In clinical trials, administration of Avastin was not allowed until at least 28 days after surgery. In a controlled clinical trial, the incidence of wound healing complications, including serious and fatal complications, in patients with mCRC who underwent surgery during the course of Avastin treatment was 15% and in patients who did not receive Avastin, was 4%. [See Adverse Reactions (6.1).]Avastin should not be initiated for at least 28 days following surgery and until the surgical wound is fully healed. Discontinue Avastin in patients with wound healing complications requiring medical intervention.The appropriate interval between the last dose of Avastin and elective surgery is unknown; however, the half-life of Avastin is estimated to be 20 days. Suspend Avastin for at least 28 days prior to elective surgery. Do not administer Avastin until the wound is fully healed. [See Boxed Warning, Dosage and Administration (2.4).]
5.3 HemorrhageAvastin can result in two distinct patterns of bleeding: minor hemorrhage, most commonly Grade 1 epistaxis; and serious, and in some cases fatal, hemorrhagic events. Severe or fatal hemorrhage, including hemoptysis, gastrointestinal bleeding, hematemesis, CNS hemorrhage, epistaxis, and vaginal bleeding occurred up to �ve-fold more frequently in patients receiving Avastin compared to patients receiving only chemotherapy. Across indications, the incidence of Grade ≥ 3 hemorrhagic events among patients receiving Avastin ranged from 1.2 to 4.6%. [See Adverse Reactions (6.1).]Serious or fatal pulmonary hemorrhage occurred in four of 13 (31%) patients with squamous cell histology and two of 53 (4%) patients with non-squamous non-small cell lung cancer receiving Avastin and chemotherapy compared to none of the 32 (0%) patients receiving chemotherapy alone.In clinical studies in non–small cell lung cancer where patients with CNS metastases who completed radiation and surgery more than 4 weeks prior to the start of Avastin
AVASTIN® (bevacizumab)
SECOND ANNUALCONFERENCE
�������������� �� �����$
������������������ ������� ���
������������$
�� ������������������������ ��� ����� ��
�������� � ����� �����������
REGISTER TODAY ATwww.globalbiomarkersconsortium.com✓
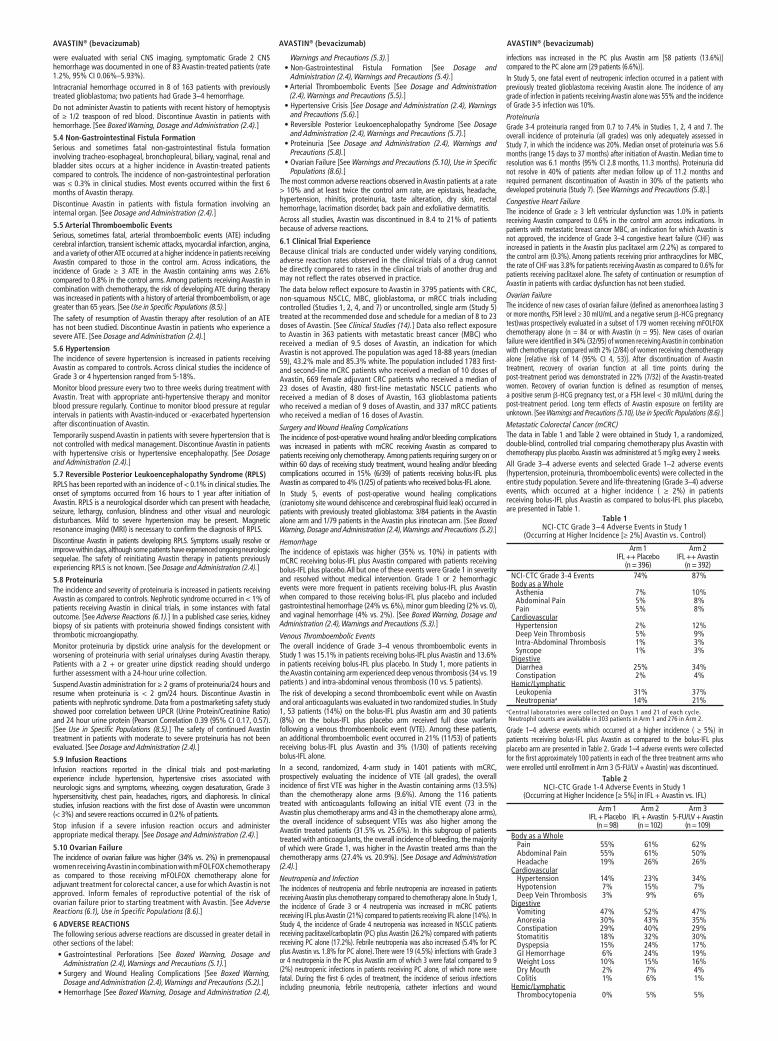
were evaluated with serial CNS imaging, symptomatic Grade 2 CNS hemorrhage was documented in one of 83 Avastin-treated patients (rate 1.2%, 95% CI 0.06%–5.93%).Intracranial hemorrhage occurred in 8 of 163 patients with previously treated glioblastoma; two patients had Grade 3–4 hemorrhage.Do not administer Avastin to patients with recent history of hemoptysis of ≥ 1/2 teaspoon of red blood. Discontinue Avastin in patients with hemorrhage. [See Boxed Warning, Dosage and Administration (2.4).]
5.4 Non-Gastrointestinal Fistula FormationSerious and sometimes fatal non-gastrointestinal �stula formation involving tracheo-esophageal, bronchopleural, biliary, vaginal, renal and bladder sites occurs at a higher incidence in Avastin-treated patients compared to controls. The incidence of non-gastrointestinal perforation was ≤ 0.3% in clinical studies. Most events occurred within the �rst 6 months of Avastin therapy.Discontinue Avastin in patients with �stula formation involving an internal organ. [See Dosage and Administration (2.4).]
5.5 Arterial Thromboembolic EventsSerious, sometimes fatal, arterial thromboembolic events (ATE) including cerebral infarction, transient ischemic attacks, myocardial infarction, angina, and a variety of other ATE occurred at a higher incidence in patients receiving Avastin compared to those in the control arm. Across indications, the incidence of Grade ≥ 3 ATE in the Avastin containing arms was 2.6% compared to 0.8% in the control arms. Among patients receiving Avastin in combination with chemotherapy, the risk of developing ATE during therapy was increased in patients with a history of arterial thromboembolism, or age greater than 65 years. [See Use in Specific Populations (8.5).]The safety of resumption of Avastin therapy after resolution of an ATE has not been studied. Discontinue Avastin in patients who experience a severe ATE. [See Dosage and Administration (2.4).]
5.6 HypertensionThe incidence of severe hypertension is increased in patients receiving Avastin as compared to controls. Across clinical studies the incidence of Grade 3 or 4 hypertension ranged from 5-18%.Monitor blood pressure every two to three weeks during treatment with Avastin. Treat with appropriate anti-hypertensive therapy and monitor blood pressure regularly. Continue to monitor blood pressure at regular intervals in patients with Avastin-induced or -exacerbated hypertension after discontinuation of Avastin.Temporarily suspend Avastin in patients with severe hypertension that is not controlled with medical management. Discontinue Avastin in patients with hypertensive crisis or hypertensive encephalopathy. [See Dosage and Administration (2.4).]
5.7 Reversible Posterior Leukoencephalopathy Syndrome (RPLS)RPLS has been reported with an incidence of < 0.1% in clinical studies. The onset of symptoms occurred from 16 hours to 1 year after initiation of Avastin. RPLS is a neurological disorder which can present with headache, seizure, lethargy, confusion, blindness and other visual and neurologic disturbances. Mild to severe hypertension may be present. Magnetic resonance imaging (MRI) is necessary to con�rm the diagnosis of RPLS.Discontinue Avastin in patients developing RPLS. Symptoms usually resolve or improve within days, although some patients have experienced ongoing neurologic sequelae. The safety of reinitiating Avastin therapy in patients previously experiencing RPLS is not known. [See Dosage and Administration (2.4).]
5.8 ProteinuriaThe incidence and severity of proteinuria is increased in patients receiving Avastin as compared to controls. Nephrotic syndrome occurred in < 1% of patients receiving Avastin in clinical trials, in some instances with fatal outcome. [See Adverse Reactions (6.1).] In a published case series, kidney biopsy of six patients with proteinuria showed �ndings consistent with thrombotic microangiopathy.Monitor proteinuria by dipstick urine analysis for the development or worsening of proteinuria with serial urinalyses during Avastin therapy. Patients with a 2 + or greater urine dipstick reading should undergo further assessment with a 24-hour urine collection.Suspend Avastin administration for ≥ 2 grams of proteinuria/24 hours and resume when proteinuria is < 2 gm/24 hours. Discontinue Avastin in patients with nephrotic syndrome. Data from a postmarketing safety study showed poor correlation between UPCR (Urine Protein/Creatinine Ratio) and 24 hour urine protein (Pearson Correlation 0.39 (95% CI 0.17, 0.57). [See Use in Specific Populations (8.5).] The safety of continued Avastin treatment in patients with moderate to severe proteinuria has not been evaluated. [See Dosage and Administration (2.4).]
5.9 Infusion ReactionsInfusion reactions reported in the clinical trials and post-marketing experience include hypertension, hypertensive crises associated with neurologic signs and symptoms, wheezing, oxygen desaturation, Grade 3 hypersensitivity, chest pain, headaches, rigors, and diaphoresis. In clinical studies, infusion reactions with the �rst dose of Avastin were uncommon (< 3%) and severe reactions occurred in 0.2% of patients.Stop infusion if a severe infusion reaction occurs and administer appropriate medical therapy. [See Dosage and Administration (2.4).]
5.10 Ovarian FailureThe incidence of ovarian failure was higher (34% vs. 2%) in premenopausal women receiving Avastin in combination with mFOLFOX chemotherapy as compared to those receiving mFOLFOX chemotherapy alone for adjuvant treatment for colorectal cancer, a use for which Avastin is not approved. Inform females of reproductive potential of the risk of ovarian failure prior to starting treatment with Avastin. [See Adverse Reactions (6.1), Use in Speci�c Populations (8.6).]
6 ADVERSE REACTIONSThe following serious adverse reactions are discussed in greater detail in other sections of the label:
Gastrointestinal Perforations [See Boxed Warning, Dosage and Administration (2.4), Warnings and Precautions (5.1).] Surgery and Wound Healing Complications [See Boxed Warning, Dosage and Administration (2.4), Warnings and Precautions (5.2).] Hemorrhage [See Boxed Warning, Dosage and Administration (2.4),
Warnings and Precautions (5.3).] Non-Gastrointestinal Fistula Formation [See Dosage and Administration (2.4), Warnings and Precautions (5.4).] Arterial Thromboembolic Events [See Dosage and Administration (2.4), Warnings and Precautions (5.5).] Hypertensive Crisis [See Dosage and Administration (2.4), Warnings and Precautions (5.6).] Reversible Posterior Leukoencephalopathy Syndrome [See Dosage and Administration (2.4), Warnings and Precautions (5.7).] Proteinuria [See Dosage and Administration (2.4), Warnings and Precautions (5.8).] Ovarian Failure [See Warnings and Precautions (5.10), Use in Specific Populations (8.6).]
The most common adverse reactions observed in Avastin patients at a rate > 10% and at least twice the control arm rate, are epistaxis, headache, hypertension, rhinitis, proteinuria, taste alteration, dry skin, rectal hemorrhage, lacrimation disorder, back pain and exfoliative dermatitis.Across all studies, Avastin was discontinued in 8.4 to 21% of patients because of adverse reactions.
6.1 Clinical Trial ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not re�ect the rates observed in practice.The data below re�ect exposure to Avastin in 3795 patients with CRC, non-squamous NSCLC, MBC, glioblastoma, or mRCC trials including controlled (Studies 1, 2, 4, and 7) or uncontrolled, single arm (Study 5) treated at the recommended dose and schedule for a median of 8 to 23 doses of Avastin. [See Clinical Studies (14).] Data also re�ect exposure to Avastin in 363 patients with metastatic breast cancer (MBC) who received a median of 9.5 doses of Avastin, an indication for which Avastin is not approved. The population was aged 18-88 years (median 59), 43.2% male and 85.3% white. The population included 1783 �rst- and second-line mCRC patients who received a median of 10 doses of Avastin, 669 female adjuvant CRC patients who received a median of 23 doses of Avastin, 480 �rst-line metastatic NSCLC patients who received a median of 8 doses of Avastin, 163 glioblastoma patients who received a median of 9 doses of Avastin, and 337 mRCC patients who received a median of 16 doses of Avastin.
Surgery and Wound Healing ComplicationsThe incidence of post-operative wound healing and/or bleeding complications was increased in patients with mCRC receiving Avastin as compared to patients receiving only chemotherapy. Among patients requiring surgery on or within 60 days of receiving study treatment, wound healing and/or bleeding complications occurred in 15% (6/39) of patients receiving bolus-IFL plus Avastin as compared to 4% (1/25) of patients who received bolus-IFL alone.In Study 5, events of post-operative wound healing complications (craniotomy site wound dehiscence and cerebrospinal �uid leak) occurred in patients with previously treated glioblastoma: 3/84 patients in the Avastin alone arm and 1/79 patients in the Avastin plus irinotecan arm. [See Boxed Warning, Dosage and Administration (2.4), Warnings and Precautions (5.2).]
HemorrhageThe incidence of epistaxis was higher (35% vs. 10%) in patients with mCRC receiving bolus-IFL plus Avastin compared with patients receiving bolus-IFL plus placebo. All but one of these events were Grade 1 in severity and resolved without medical intervention. Grade 1 or 2 hemorrhagic events were more frequent in patients receiving bolus-IFL plus Avastin when compared to those receiving bolus-IFL plus placebo and included gastrointestinal hemorrhage (24% vs. 6%), minor gum bleeding (2% vs. 0), and vaginal hemorrhage (4% vs. 2%). [See Boxed Warning, Dosage and Administration (2.4), Warnings and Precautions (5.3).]
Venous Thromboembolic EventsThe overall incidence of Grade 3–4 venous thromboembolic events in Study 1 was 15.1% in patients receiving bolus-IFL plus Avastin and 13.6% in patients receiving bolus-IFL plus placebo. In Study 1, more patients in the Avastin containing arm experienced deep venous thrombosis (34 vs. 19 patients ) and intra-abdominal venous thrombosis (10 vs. 5 patients).The risk of developing a second thromboembolic event while on Avastin and oral anticoagulants was evaluated in two randomized studies. In Study 1, 53 patients (14%) on the bolus-IFL plus Avastin arm and 30 patients (8%) on the bolus-IFL plus placebo arm received full dose warfarin following a venous thromboembolic event (VTE). Among these patients, an additional thromboembolic event occurred in 21% (11/53) of patients receiving bolus-IFL plus Avastin and 3% (1/30) of patients receiving bolus-IFL alone.In a second, randomized, 4-arm study in 1401 patients with mCRC, prospectively evaluating the incidence of VTE (all grades), the overall incidence of �rst VTE was higher in the Avastin containing arms (13.5%) than the chemotherapy alone arms (9.6%). Among the 116 patients treated with anticoagulants following an initial VTE event (73 in the Avastin plus chemotherapy arms and 43 in the chemotherapy alone arms), the overall incidence of subsequent VTEs was also higher among the Avastin treated patients (31.5% vs. 25.6%). In this subgroup of patients treated with anticoagulants, the overall incidence of bleeding, the majority of which were Grade 1, was higher in the Avastin treated arms than the chemotherapy arms (27.4% vs. 20.9%). [See Dosage and Administration (2.4).]
Neutropenia and InfectionThe incidences of neutropenia and febrile neutropenia are increased in patients receiving Avastin plus chemotherapy compared to chemotherapy alone. In Study 1, the incidence of Grade 3 or 4 neutropenia was increased in mCRC patients receiving IFL plus Avastin (21%) compared to patients receiving IFL alone (14%). In Study 4, the incidence of Grade 4 neutropenia was increased in NSCLC patients receiving paclitaxel/carboplatin (PC) plus Avastin (26.2%) compared with patients receiving PC alone (17.2%). Febrile neutropenia was also increased (5.4% for PC plus Avastin vs. 1.8% for PC alone). There were 19 (4.5%) infections with Grade 3 or 4 neutropenia in the PC plus Avastin arm of which 3 were fatal compared to 9 (2%) neutropenic infections in patients receiving PC alone, of which none were fatal. During the �rst 6 cycles of treatment, the incidence of serious infections including pneumonia, febrile neutropenia, catheter infections and wound
infections was increased in the PC plus Avastin arm [58 patients (13.6%)] compared to the PC alone arm [29 patients (6.6%)].In Study 5, one fatal event of neutropenic infection occurred in a patient with previously treated glioblastoma receiving Avastin alone. The incidence of any grade of infection in patients receiving Avastin alone was 55% and the incidence of Grade 3-5 infection was 10%.
ProteinuriaGrade 3-4 proteinuria ranged from 0.7 to 7.4% in Studies 1, 2, 4 and 7. The overall incidence of proteinuria (all grades) was only adequately assessed in Study 7, in which the incidence was 20%. Median onset of proteinuria was 5.6 months (range 15 days to 37 months) after initiation of Avastin. Median time to resolution was 6.1 months (95% CI 2.8 months, 11.3 months). Proteinuria did not resolve in 40% of patients after median follow up of 11.2 months and required permanent discontinuation of Avastin in 30% of the patients who developed proteinuria (Study 7). [See Warnings and Precautions (5.8).]
Congestive Heart FailureThe incidence of Grade ≥ 3 left ventricular dysfunction was 1.0% in patients receiving Avastin compared to 0.6% in the control arm across indications. In patients with metastatic breast cancer MBC, an indication for which Avastin is not approved, the incidence of Grade 3–4 congestive heart failure (CHF) was increased in patients in the Avastin plus paclitaxel arm (2.2%) as compared to the control arm (0.3%). Among patients receiving prior anthracyclines for MBC, the rate of CHF was 3.8% for patients receiving Avastin as compared to 0.6% for patients receiving paclitaxel alone. The safety of continuation or resumption of Avastin in patients with cardiac dysfunction has not been studied.
Ovarian FailureThe incidence of new cases of ovarian failure (de�ned as amenorrhoea lasting 3 or more months, FSH level ≥ 30 mIU/mL and a negative serum β-HCG pregnancy test)was prospectively evaluated in a subset of 179 women receiving mFOLFOX chemotherapy alone (n = 84 or with Avastin (n = 95). New cases of ovarian failure were identi�ed in 34% (32/95) of women receiving Avastin in combination with chemotherapy compared with 2% (2/84) of women receiving chemotherapy alone [relative risk of 14 (95% CI 4, 53)]. After discontinuation of Avastin treatment, recovery of ovarian function at all time points during the post-treatment period was demonstrated in 22% (7/32) of the Avastin-treated women. Recovery of ovarian function is de�ned as resumption of menses, a positive serum β-HCG pregnancy test, or a FSH level < 30 mIU/mL during the post-treatment period. Long term effects of Avastin exposure on fertility are unknown. [See Warnings and Precautions (5.10), Use in Specific Populations (8.6).]
Metastatic Colorectal Cancer (mCRC)The data in Table 1 and Table 2 were obtained in Study 1, a randomized, double-blind, controlled trial comparing chemotherapy plus Avastin with chemotherapy plus placebo. Avastin was administered at 5 mg/kg every 2 weeks.All Grade 3–4 adverse events and selected Grade 1–2 adverse events (hypertension, proteinuria, thromboembolic events) were collected in the entire study population. Severe and life-threatening (Grade 3–4) adverse events, which occurred at a higher incidence ( ≥ 2%) in patients receiving bolus-IFL plus Avastin as compared to bolus-IFL plus placebo, are presented in Table 1.
Table 1 NCI-CTC Grade 3−4 Adverse Events in Study 1
(Occurring at Higher Incidence [≥ 2%] Avastin vs. Control)
Arm 1 Arm 2 IFL ++ Placebo IFL ++ Avastin (n = 396) (n = 392)
NCI-CTC Grade 3-4 Events 74% 87%Body as a Whole Asthenia 7% 10% Abdominal Pain 5% 8% Pain 5% 8%Cardiovascular Hypertension 2% 12% Deep Vein Thrombosis 5% 9% Intra-Abdominal Thrombosis 1% 3% Syncope 1% 3%Digestive Diarrhea 25% 34% Constipation 2% 4%Hemic/Lymphatic Leukopenia 31% 37% Neutropeniaa 14% 21%
a Central laboratories were collected on Days 1 and 21 of each cycle. Neutrophil counts are available in 303 patients in Arm 1 and 276 in Arm 2.
Grade 1–4 adverse events which occurred at a higher incidence ( ≥ 5%) in patients receiving bolus-IFL plus Avastin as compared to the bolus-IFL plus placebo arm are presented in Table 2. Grade 1–4 adverse events were collected for the �rst approximately 100 patients in each of the three treatment arms who were enrolled until enrollment in Arm 3 (5-FU/LV + Avastin) was discontinued.
Table 2 NCI-CTC Grade 1-4 Adverse Events in Study 1
(Occurring at Higher Incidence [≥ 5%] in IFL + Avastin vs. IFL)
Arm 1 Arm 2 Arm 3 IFL + Placebo IFL + Avastin 5-FU/LV + Avastin (n = 98) (n = 102) (n = 109)
Body as a Whole Pain 55% 61% 62% Abdominal Pain 55% 61% 50% Headache 19% 26% 26%Cardiovascular Hypertension 14% 23% 34% Hypotension 7% 15% 7% Deep Vein Thrombosis 3% 9% 6%Digestive Vomiting 47% 52% 47% Anorexia 30% 43% 35% Constipation 29% 40% 29% Stomatitis 18% 32% 30% Dyspepsia 15% 24% 17%
GI Hemorrhage 6% 24% 19% Weight Loss 10% 15% 16% Dry Mouth 2% 7% 4% Colitis 1% 6% 1%
Hemic/Lymphatic Thrombocytopenia 0% 5% 5%
AVASTIN® (bevacizumab) AVASTIN® (bevacizumab) AVASTIN® (bevacizumab)

Table 2 (cont’d)NCI-CTC Grade 1-4 Adverse Events in Study 1
(Occurring at Higher Incidence [≥ 5%] in IFL + Avastin vs. IFL)
Arm 1 Arm 2 Arm 3 IFL + Placebo IFL + Avastin 5-FU/LV + Avastin (n = 98) (n = 102) (n = 109)
Nervous Dizziness 20% 26% 19%Respiratory Upper Respiratory Infection 39% 47% 40% Epistaxis 10% 35% 32% Dyspnea 15% 26% 25% Voice Alteration 2% 9% 6%Skin/Appendages Alopecia 26% 32% 6% Skin Ulcer 1% 6% 6%Special Senses Taste Disorder 9% 14% 21%Urogenital Proteinuria 24% 36% 36%
Avastin in Combination with FOLFOX4 in Second-line mCRCOnly Grade 3-5 non-hematologic and Grade 4–5 hematologic adverse events related to treatment were collected in Study 2. The most frequent adverse events (selected Grade 3–5 non-hematologic and Grade 4–5 hematologic adverse events) occurring at a higher incidence ( ≥ 2%) in 287 patients receiving FOLFOX4 plus Avastin compared to 285 patients receiving FOLFOX4 alone were fatigue (19% vs. 13%), diarrhea (18% vs. 13%), sensory neuropathy (17% vs. 9%), nausea (12% vs. 5%), vomiting (11% vs. 4%), dehydration (10% vs. 5%), hypertension (9% vs. 2%), abdominal pain (8% vs. 5%), hemorrhage (5% vs. 1%), other neurological (5% vs. 3%), ileus (4% vs. 1%) and headache (3% vs. 0%). These data are likely to under-estimate the true adverse event rates due to the reporting mechanisms used in Study 2.
Unresectable Non-Squamous Non-Small Cell Lung Cancer (NSCLC)Only Grade 3-5 non-hematologic and Grade 4-5 hematologic adverse events were collected in Study 4. Grade 3–5 non-hematologic and Grade 4–5 hematologic adverse events (occurring at a higher incidence (≥ 2%) in 427 patients receiving PC plus Avastin compared with 441 patients receiving PC alone were neutropenia (27% vs. 17%), fatigue (16% vs. 13%), hypertension (8% vs. 0.7%), infection without neutropenia (7% vs. 3%), venous thrombus/embolism (5% vs. 3%), febrile neutropenia (5% vs. 2%), pneumonitis/pulmonary in�ltrates (5% vs. 3%), infection with Grade 3 or 4 neutropenia (4% vs. 2%), hyponatremia (4% vs. 1%), headache (3% vs. 1%) and proteinuria (3% vs. 0%).
GlioblastomaAll adverse events were collected in 163 patients enrolled in Study 5 who either received Avastin alone or Avastin plus irinotecan. All patients received prior radiotherapy and temozolomide. Avastin was administered at 10 mg/kg every 2 weeks alone or in combination with irinotecan. Avastin was discontinued due to adverse events in 4.8% of patients treated with Avastin alone. In patients receiving Avastin alone (N = 84), the most frequently reported adverse events of any grade were infection (55%), fatigue (45%), headache (37%), hypertension (30%), epistaxis (19%) and diarrhea (21%). Of these, the incidence of Grade ≥ 3 adverse events was infection (10%), fatigue (4%), headache (4%), hypertension (8%) and diarrhea (1%). Two deaths on study were possibly related to Avastin: one retroperitoneal hemorrhage and one neutropenic infection.In patients receiving Avastin alone or Avastin plus irinotecan (N = 163), the incidence of Avastin-related adverse events (Grade 1– 4) were bleeding/hemorrhage (40%), epistaxis (26%), CNS hemorrhage (5%), hypertension (32%), venous thromboembolic event (8%), arterial thromboembolic event (6%), wound-healing complications (6%), proteinuria (4%), gastrointestinal perforation (2%), and RPLS (1%). The incidence of Grade 3–5 events in these 163 patients were bleeding/hemorrhage (2%), CNS hemorrhage (1%), hypertension (5%), venous thromboembolic event (7%), arterial thromboembolic event (3%), wound-healing complications (3%), proteinuria (1%), and gastrointestinal perforation (2%).
Metastatic Renal Cell Carcinoma (mRCC)All grade adverse events were collected in Study 7. Grade 3–5 adverse events occurring at a higher incidence ( ≥ 2%) in 337 patients receiving interferon alfa (IFN-α) plus Avastin compared to 304 patients receiving IFN-α plus placebo arm were fatigue (13% vs. 8%), asthenia (10% vs. 7%), proteinuria (7% vs. 0%), hypertension (6% vs. 1%; including hypertension and hypertensive crisis), and hemorrhage (3% vs. 0.3%; including epistaxis, small intestinal hemorrhage, aneurysm ruptured, gastric ulcer hemorrhage, gingival bleeding, haemoptysis, hemorrhage intracranial, large intestinal hemorrhage, respiratory tract hemorrhage, and traumatic hematoma).Grade 1–5 adverse events occurring at a higher incidence ( ≥ 5%) in patients receiving IFN-α plus Avastin compared to the IFN-α plus placebo arm are presented in Table 3.
Table 3 NCI-CTC Grades 1−5 Adverse Events in Study 7
(Occurring at Higher Incidence [≥ 5%] in IFN-α + Avastin vs. IFN-α + Placebo)
System Organ Class/ IFN-α + Placebo IFN-α + Avastin Preferred terma (n = 304) (n = 337)Gastrointestinal disorders Diarrhea 16% 21%General disorders and administration site conditions Fatigue 27% 33%Investigations Weight decreased 15% 20%Metabolism and nutrition disorders Anorexia 31% 36%Musculoskeletal and connective tissue disorders Myalgia 14% 19% Back pain 6% 12%Nervous system disorders Headache 16% 24%Renal and urinary disorders Proteinuria 3% 20%Respiratory, thoracic and mediastinal disorders Epistaxis 4% 27% Dysphonia 0% 5%Vascular disorders Hypertension 9% 28%
aAdverse events were encoded using MedDRA, Version 10.1.
The following adverse events were reported at a 5-fold greater incidence in the IFN-α plus Avastin arm compared to IFN-α alone and not represented in Table 3: gingival bleeding (13 patients vs. 1 patient); rhinitis (9 vs.0 ); blurred vision (8 vs. 0); gingivitis (8 vs. 1); gastroesophageal re�ux disease (8 vs.1 ); tinnitus (7 vs. 1); tooth abscess (7 vs.0); mouth ulceration (6 vs. 0); acne (5 vs. 0); deafness (5 vs. 0); gastritis (5 vs. 0); gingival pain (5 vs. 0) and pulmonary embolism (5 vs. 1).
6.2 ImmunogenicityAs with all therapeutic proteins, there is a potential for immunogenicity. The incidence of antibody development in patients receiving Avastin has not been adequately determined because the assay sensitivity was inadequate to reliably detect lower titers. Enzyme-linked immunosorbent assays (ELISAs) were performed on sera from approximately 500 patients treated with Avastin, primarily in combination with chemotherapy. High titer human anti-Avastin antibodies were not detected.Immunogenicity data are highly dependent on the sensitivity and speci�city of the assay. Additionally, the observed incidence of antibody positivity in an assay may be in�uenced by several factors, including sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of the incidence of antibodies to Avastin with the incidence of antibodies to other products may be misleading.
6.3 Postmarketing ExperienceThe following adverse reactions have been identi�ed during post-approval use of Avastin. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.Body as a Whole: PolyserositisCardiovascular: Pulmonary hypertension, RPLS, Mesenteric venous occlusionEye disorders (from unapproved intravitreal use for treatment of various ocular disorders): Permanent loss of vision; Endophthalmitis (infectious and sterile); Intraocular in�ammation; Retinal detachment; Increased intraocular pressure; Hemorrhage including conjunctival, vitreous hemorrhage or retinal hemorrhage; Vitreous �oaters; Ocular hyperemia; Ocular pain or discomfortGastrointestinal: Gastrointestinal ulcer, Intestinal necrosis, Anastomotic ulcerationHemic and lymphatic: PancytopeniaMusculoskeletal: Osteonecrosis of the jawRenal: Renal thrombotic microangiopathy (manifested as severe proteinuria)Respiratory: Nasal septum perforation, dysphoniaSystemic Events (from unapproved intravitreal use for treatment of various ocular disorders): Arterial thromboembolic events, Hypertension, Gastrointestinal perforation, Hemorrhage
7 DRUG INTERACTIONSA drug interaction study was performed in which irinotecan was administered as part of the FOLFIRI regimen with or without Avastin. The results demonstrated no signi�cant effect of bevacizumab on the pharmacokinetics of irinotecan or its active metabolite SN38.In a randomized study in 99 patients with NSCLC, based on limited data, there did not appear to be a difference in the mean exposure of either carboplatin or paclitaxel when each was administered alone or in combination with Avastin. However, 3 of the 8 patients receiving Avastin plus paclitaxel/carboplatin had substantially lower paclitaxel exposure after four cycles of treatment (at Day 63) than those at Day 0, while patients receiving paclitaxel/carboplatin without Avastin had a greater paclitaxel exposure at Day 63 than at Day 0.In Study 7, there was no difference in the mean exposure of interferon alfa administered in combination with Avastin when compared to interferon alfa alone.
8 USE IN SPECIFIC POPULATIONS8.1 PregnancyPregnancy Category CThere are no adequate or well controlled studies of bevacizumab in pregnant women. While it is not known if bevacizumab crosses the placenta, human IgG is known to cross the placenta Reproduction studies in rabbits treated with approximately 1 to 12 times the recommended human dose of bevacizumab demonstrated teratogenicity, including an increased incidence of speci�c gross and skeletal fetal alterations. Adverse fetal outcomes were observed at all doses tested. Other observed effects included decreases in maternal and fetal body weights and an increased number of fetal resorptions. [See Nonclinical Toxicology (13.3).]
Because of the observed teratogenic effects of bevacizumab in animals and of other inhibitors of angiogenesis in humans, bevacizumab should be used during pregnancy only if the potential bene�t to the pregnant woman justi�es the potential risk to the fetus.
8.3 Nursing MothersIt is not known whether Avastin is secreted in human milk. Human IgG is excreted in human milk, but published data suggest that breast milk antibodies do not enter the neonatal and infant circulation in substantial amounts. Because many drugs are secreted in human milk and because of the potential for serious adverse reactions in nursing infants from bevacizumab, a decision should be made whether to discontinue nursing or discontinue drug, taking into account the half-life of the bevacizumab (approximately 20 days [range 11–50 days]) and the importance of the drug to the mother. [See Clinical Pharmacology (12.3).]
8.4 Pediatric UseThe safety, effectiveness and pharmacokinetic pro�le of Avastin in pediatric patients have not been established.Antitumor activity was not observed among eight children with relapsed glioblastoma treated with bevacizumab and irinotecan. There is insuf�cient information to determine the safety and ef�cacy of Avastin in children with glioblastoma.Juvenile cynomolgus monkeys with open growth plates exhibited physeal dysplasia following 4 to 26 weeks exposure at 0.4 to 20 times the recommended human dose (based on mg/kg and exposure). The incidence and severity of physeal dysplasia were dose-related and were partially reversible upon cessation of treatment.
8.5 Geriatric UseIn Study 1, severe adverse events that occurred at a higher incidence ( ≥ 2%) in patients aged ≥ 65 years as compared to younger patients were asthenia, sepsis, deep thrombophlebitis, hypertension, hypotension, myocardial infarction, congestive heart failure, diarrhea, constipation, anorexia, leukopenia, anemia, dehydration, hypokalemia, and hyponatremia. The effect of Avastin on overall survival was similar in elderly patients as compared to younger patients.In Study 2, patients aged ≥ 65 years receiving Avastin plus FOLFOX4 had a greater relative risk as compared to younger patients for the following adverse events: nausea, emesis, ileus, and fatigue.
In Study 4, patients aged ≥ 65 years receiving carboplatin, paclitaxel, and Avastin had a greater relative risk for proteinuria as compared to younger patients. [See Warnings and Precautions (5.8).]
Of the 742 patients enrolled in Genentech-sponsored clinical studies in which all adverse events were captured, 212 (29%) were age 65 or older and 43 (6%) were age 75 or older. Adverse events of any severity that occurred at a higher incidence in the elderly as compared to younger patients, in addition to those described above, were dyspepsia, gastrointestinal hemorrhage, edema, epistaxis, increased cough, and voice alteration.In an exploratory, pooled analysis of 1745 patients treated in �ve randomized, controlled studies, there were 618 (35%) patients aged ≥ 65 years and 1127 patients < 65 years of age. The overall incidence of arterial thromboembolic events was increased in all patients receiving Avastin with chemotherapy as compared to those receiving chemotherapy alone, regardless of age. However, the increase in arterial thromboembolic events incidence was greater in patients aged ≥ 65 years (8.5% vs. 2.9%) as compared to those < 65 years (2.1% vs. 1.4%). [See Warnings and Precautions (5.5).]
8.6 Females of Reproductive PotentialAvastin increases the risk of ovarian failure and may impair fertility. Inform females of reproductive potential of the risk of ovarian failure prior to starting treatment with Avastin. Long term effects of Avastin exposure on fertility are unknown.
In a prospectively designed substudy of 179 premenopausal women randomized to receive chemotherapy with or without Avastin, the incidence of ovarian failure was higher in the Avastin arm (34%) compared to the control arm (2%). After discontinuation of Avastin and chemotherapy, recovery of ovarian function occurred in 22% (7/32) of these Avastin-treated patients. [See Warnings and Precautions (5.10), Adverse Reactions (6.1).]
10 OVERDOSAGEThe highest dose tested in humans (20 mg/kg IV) was associated with headache in nine of 16 patients and with severe headache in three of 16 patients.
AVASTIN® (bevacizumab) AVASTIN® (bevacizumab) AVASTIN® (bevacizumab)
01/12 AVA000075920210127309
Initial U.S.Approval: February 2004Code Revision Date: December 2011Avastin® is a registered trademark
of Genentech, Inc. ©2012 Genentech, Inc.
Avastin® (bevacizumab) Manufactured by:Genentech, Inc.A Member of the Roche Group1 DNA WaySouth San Francisco, CA94080-4990
Think Avastin Clinically meaningful activity in 4 distinct tumor types1
Because anti-angiogenesis mattersAvastin is designed to directly inhibit the VEGF ligand to speci�cally inhibit angiogenesis1*
To confront a common threat across approved indications...
VEGF=vascular endothelial growth factor. * The mechanism of action of Avastin has been elucidated primarily in preclinical models. Its clinical signi�cance is unknown.
IndicationsAvastin is indicated for the treatment of metastatic renal cell carcinoma in combination with interferon alfa. Avastin is indicated for the treatment of glioblastoma as a single agent for adult patients with progressive disease following prior therapy. The effectiveness of Avastin in glioblastoma is based on an improvement in objective response rate. There are no data demonstrating an improvement in disease-related symptoms or increased survival with Avastin.Avastin is indicated for the �rst-line treatment of unresectable, locally advanced, recurrent or metastatic non–squamous non–small cell lung cancer in combination with carboplatin and paclitaxel.Avastin is indicated for the �rst- or second-line treatment of patients with metastatic carcinoma of the colon or rectum in combination with intravenous 5-�uorouracil– based chemotherapy.
Boxed WARNINGS Gastrointestinal (GI) perforation
— Serious and sometimes fatal GI perforation occurs at a higher incidence in Avastin-treated patients compared to controls
— The incidences of GI perforation ranged from 0.3% to 2.4% across clinical studies — Discontinue Avastin in patients with GI perforation
Surgery and wound healing complications — The incidence of wound healing and surgical complications, including serious and
fatal complications, is increased in Avastin-treated patients — Do not initiate Avastin for at least 28 days after surgery and until the surgical wound is
fully healed. The appropriate interval between termination of Avastin and subsequent elective surgery required to reduce the risks of impaired wound healing/wound dehiscence has not been determined
— Discontinue Avastin at least 28 days prior to elective surgery and in patients with wound healing complications requiring medical intervention
Hemorrhage — Severe or fatal hemorrhage, including hemoptysis, GI bleeding, hematemesis,
central nervous system hemorrhage, epistaxis, and vaginal bleeding, occurred up to 5-fold more frequently in patients receiving Avastin. Across indications, the incidence of grade ≥3 hemorrhagic events among patients receiving Avastin ranged from 1.2% to 4.6%
— Do not administer Avastin to patients with serious hemorrhage or recent hemoptysis (≥1/2 tsp of red blood)
— Discontinue Avastin in patients with serious hemorrhage (ie, requiring medical intervention)
Additional serious adverse events Additional serious and sometimes fatal adverse events with increased incidence in the
Avastin-treated arm vs control included — Non-GI �stula formation (≤0.3%) — Arterial thromboembolic events (grade ≥3, 2.6%) — Proteinuria (nephrotic syndrome, <1%)
Additional serious adverse events with increased incidence in the Avastin-treated arm vs control included
— Hypertension (grade 3–4, 5%–18%) — Reversible posterior leukoencephalopathy syndrome (RPLS) (<0.1%)
Infusion reactions with the �rst dose of Avastin were uncommon (<3%), and severe reactions occurred in 0.2% of patients
Inform females of reproductive potential of the risk of ovarian failure prior to starting treatment with Avastin
Most common adverse events Most common adverse reactions observed in Avastin patients at a rate >10% and at least
twice the control arm rate were — Epistaxis — Proteinuria — Lacrimation disorder — Headache — Taste alteration — Back pain — Hypertension — Dry skin — Exfoliative dermatitis — Rhinitis — Rectal hemorrhage
Across all studies, Avastin was discontinued in 8.4% to 21% of patients because of adverse reactions
Pregnancy warning Avastin may impair fertility Based on animal data, Avastin may cause fetal harm Advise patients of the potential risk to the fetus during and following Avastin and the need
to continue adequate contraception for at least 6 months following the last dose of Avastin For nursing mothers, discontinue nursing or Avastin, taking into account the importance
of Avastin to the mother In mRCC, the most common grade 3–5 adverse events in AVOREN, occurring at a ≥2%
higher incidence in Avastin-treated patients vs controls, were fatigue (13% vs 8%), asthenia (10% vs 7%), proteinuria (7% vs 0%), hypertension (6% vs 1%), and hemorrhage (3% vs 0.3%)
In GBM Study AVF3708g, in patients receiving Avastin alone, the most frequently reported adverse events were infection (55%), fatigue (45%), headache (37%), hypertension (30%), epistaxis (19%), and diarrhea (21%). Of these, the incidence of grade ≥3 adverse events was infection (10%), fatigue (4%), headache (4%), hypertension (8%), and diarrhea (1%). Two deaths were possibly related to Avastin: 1 retroperitoneal hemorrhage and 1 neutropenic infection
In GBM patients receiving Avastin alone or Avastin plus irinotecan,† the incidences of Avastin-related adverse events (grade 1–4) were bleeding/hemorrhage (40%), epistaxis (26%), CNS hemorrhage (5%), hypertension (32%), venous thromboembolic events (8%), arterial thromboembolic events (6%), wound healing complications (6%), proteinuria (4%), GI perforation (2%), and RPLS (1%). The incidences of grade 3–5 events in these 163 patients were bleeding/hemorrhage (2%), CNS hemorrhage (1%), hypertension (5%), venous thromboembolic events (7%), arterial thromboembolic events (3%), wound healing complications (3%), proteinuria (1%), and GI perforation (2%). Intracranial hemorrhage occurred in 8 of 163 patients; 2 patients had grade 3–4 hemorrhage
In NSCLC, grade 3–5 (nonhematologic) and grade 4–5 (hematologic) adverse events in Study E4599 occurring at a ≥2% higher incidence in Avastin-treated patients vs controls were neutropenia (27% vs 17%), fatigue (16% vs 13%), hypertension (8% vs 0.7%), infection without neutropenia (7% vs 3%), venous thrombus/embolism (5% vs 3%), febrile neutropenia (5% vs 2%), pneumonitis/pulmonary in�ltrates (5% vs 3%), infection with grade 3 or 4 neutropenia (4% vs 2%), hyponatremia (4% vs 1%), headache (3% vs 1%), and proteinuria (3% vs 0%)
In �rst-line MCRC, the most common grade 3–4 events in Study 2107, which occurred at a ≥2% higher incidence in the Avastin plus IFL vs IFL groups, were asthenia (10% vs 7%), abdominal pain (8% vs 5%), pain (8% vs 5%), hypertension (12% vs 2%), deep vein thrombosis (9% vs 5%), intra-abdominal thrombosis (3% vs 1%), syncope (3% vs 1%), diarrhea (34% vs 25%), constipation (4% vs 2%), leukopenia (37% vs 31%), and neutropenia (21% vs 14%)
In second-line MCRC, the most common grade 3–5 (nonhematologic) and 4–5 (hematologic) events in Study E3200, which occurred at a higher incidence (≥2%) in the Avastin plus FOLFOX4 vs FOLFOX4 groups, were diarrhea (18% vs 13%), nausea (12% vs 5%), vomiting (11% vs 4%), dehydration (10% vs 5%), ileus (4% vs 1%), neuropathy–sensory (17% vs 9%), neurologic–other (5% vs 3%), fatigue (19% vs 13%), abdominal pain (8% vs 5%), headache (3% vs 0%), hypertension (9% vs 2%), and hemorrhage (5% vs 1%)
†Avastin is not approved for use in combination with irinotecan.
Please see accompanying brief summary of Prescribing Information, including Boxed WARNINGS, for additional important safety information.
Reference: 1. Avastin Prescribing Information. Genentech, Inc. December 2011.
www.avastin.com©2012 Genentech USA, Inc. All rights reserved. AVA0000488301 Printed in USA. (01/12)


















