CHRONIC OBSTRUCTIVE PULMONARY DISEASE CHRONIC OBSTRUCTIVE PULMONARY DISEASE.
REVIEW ARTICLE
P
athology and Pathophysiology of Chronic ObstructivePulmonary Disease
Atsushi Nagai
Abstract
A variety of pathological changes have been observed inthe central airways, peripheral airways and lung paren-chyma of patients with chronic obstructive pulmonary dis-ease (COPD). The characteristic changes in the central air-ways include inflammatory cellular infiltration into the air-way wall and mucous gland enlargement. In the periph-eral airways, various morphological changes are observed,including mucous plugging, epithelial abnormalities, in-flammatory cellular infiltrates, fibrosis and distortion ; thesechanges lead to airway narrowing. In the lung parenchyma,emphysema defined as alveolar destruction and airspaceenlargement is present. Although the major sites of airflowlimitation in patients with COPD are most likely the pe-ripheral airways, lesions in both the peripheral airways andthe lung parenchyma contribute to chronic air flow limita-tions.(Internal Medicine 41: 265-269, 2002)
Key words: chronic bronchitis, emphysema, bronchial asthma,
airflow limitation, bronchiolitis, inflammation
Introduction
Chronic obstructive pulmonary disease (COPD) is a lead-ing cause of morbidity and mortality throughout the world ( 1 ).Although the precise prevalence of COPD is unknown, thenumber of patients suffering from this disease is increasing. Inaddition, the development of COPD is related to a past historyof cigarette smoking (2-6). The definition of COPD is basedon functional abnormalities. Most previous definitions havecharacterized the disease as a respiratory condition in whichthe patient's airflow is limited as a result of chronic bronchitisand/or emphysema (7, 8). However, the Global Initiative forChronic Obstructive Lung Disease (GOLD) very recently pub-lished a NHLBI/WHO workshop report in which COPD wasdefined as a disease state that is characterized by a limited air-flow and that is not fully reversible (1). Airflow limitations are
usually both progressive and associated with an abnormal in-flammatory response of the lungs to noxious particles or gases.This workshop report states that chronic bronchitis and em-physema are no longer included in the definition of COPD be-cause the former disease is of minor importance in calculatingthe impact of airflow limitations on the morbidity and mortal-ity rates for COPD and the latter disease is a pathological term.This definition reflects the current knowledge of the pathologyand pathophysiology of COPD.
Pathology
C
entral airways
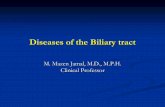
Patients with COPD exhibit enlarged bronchial mucousglands and an increased number of goblet cells (9-1 1) (Figs. 1,2). These morphological changes may lead to mucus hyperse-cretion, although an increase in the number of goblet cells hasnot been consistently observed (12-14). The accepted defini-tion of chronic bronchitis is chronic or recurrent excess secre-tion of mucous into the bronchial tree. Since the main sourceof bronchial mucous was thought to be the submucosal glands,the enlargement of these glands was considered to be a histo-logical hallmark of chronic bronchitis. The degree of mucousgland enlargement is measured as the ratio of the thickness ofthe bronchial mucous glands to the thickness of the bronchialwall; this ratio is referred to as the Reid index (13). An earlierstudy reported a significant difference in the Reid index valuefor patients with chronic bronchitis (0.41-0.79) and nonbron-chitic patients (0.14-0.36). The index was thus thought to bea useful diagnostic tool. However, subsequent works haveshown considerable overlap between the Reid index frequency
distributions for patients with chronic bronchitis and
n
onbronchitic patients ( 15).
Recent developments in bronchoscopy have enabled in-flamed central airways to be more closely observed. Conse-quently, predominant inflammatory cellular infiltrations in thesubepithelial region of the bronchial wall have been identifiedas activated CD8+ T-lymphocytes and macrophages (16). Anumber of neutrophils have been found in the bronchial lu-men, and some neutrophil infiltrates have been identified nearbronchial epithelium and submucosal glands (17). When exac-
From the First Department of Medicine, Tokyo Women's Medical University, TokyoReprint requests should be addressed to Dr. Atsushi Nagai, the First Department of Medicine, Tokyo Women's Medical University, 8- 1 Kawadacho, Shinju-ku,
Tokyo 162-8666
Internal Medicine Vol. 41, No. 4 (April 2002) 265

Nagai
Figure 1. The mucous glands of a patient with COPD form amuch higher proportion of the bronchial wall (HE stain, xl50).
erbated, the number of eosinophils infiltrating the subepithe-lial region increases (1 8).
P
eripheral airways
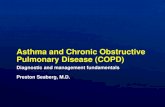
The peripheral airways are considered to be the major sitesof increased airway resistance in patients with COPD (19).Various structural changes can be observed in these regions,including goblet cell metaplasia, squamous metaplasia, inflam-matory cellular infiltrations, an increased amount of smoothmuscle, fibrosis and pigmentation (19-24). Mucous pluggingis also frequently observed in the airway lumen. These patho-logical changes may lead to an increase in airway wall thick-ness and the subsequent narrowing of the airway lumen (Fig.
3)(25).
Knowledge of how inflammation leads to structural changesis important for an understanding of the relationship betweenpathological changes and the severity of air flow limitation.Inflammation appears to be the earliest stage of lesion forma-tionand, by itself, can cause mild chronic airflow limitations(26). Fibrosis and goblet cell metaplasia are thought to follow
i
nflammation (27) and cause irreversible airflow limitations.
Recent studies focusing on the nature of the inflammatory
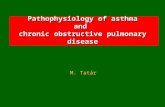
Figure 2. Scanning electron micrograph showing secretion ofmucous (arrow) from increased goblet cells (x6,000).
Figure 3. Light micrograph of lung parenchyma region in a pa-tient with severe COPD. The narrowed lumens in the airwaysand vessels are observed in the emphysematous lesions (HE stain,
x8).
cells have identified the infiltration of CD8+ T-lymphocytesinto the walls of the peripheral and central airways (16, 28).These findings suggest that a similar inflammatory processoccurs in both types of airways in COPD patients. The periph-eral airways are infiltrated by a number of macrophages that
a
re recruited via transforming growth factor-p l (29).On the basis of morphologic studies, the loss of alveolar
attachments (radial traction) around bronchioles has been pro-posed as the mechanism responsible for chronic airflow ob-struction (30, 3 1). Airway narrowing and bronchiolar deformi-ties have been associated with a loss of alveolar attachment(3 1-33), and a significant relationship between the loss of nor-mal attachments and the severity of emphysema has been iden-
266 Internal Medicine Vol. 41, No. 4 (April 2002)

Pathology and Pathophysiology of COPD
tified (33).
L ung parenchyma
In patients with emphysema, the lung parenchyma is char-acterized by an enlargement of the air spaces accompanied byalveolar destruction. Conventionally, three types of emphysemahave been described: centriacinar emphysema, panacinar em-physema and distal acinar emphysema. As distal acinar em-physema is not associated with air flow limitations, onlycentriacinar and panacinar emphysema will be described here.Centriacinar emphysema is characterized by alveolar destruc-tion in the respiratory bronchioles in the central area of theacinus. These lesions are predominantly found in the upperlobes of smokers. Panacinar emphysema involves the dilata-tion of the entire acinus, with the lower lobe dilated to a largerdegree than the upper lobe, deficiency of al -antitrypsin andan early onset are associated with panacinar emphysema. Bothtypes of emphysema are characterized by alveolar destructionwith loss of the capillary bed. The mechanism responsible for the development of emphy-sematous lesions is thought to be an imbalance in protease andantiprotease enzymes in the lung. Oxidative stress has also beenproposed as a potential mechanism (34), although this hypoth-esis has yet to be proven. Inflammation is assumed to causethe characteristic alveolar destruction seen in emphysematouslesions. Both neutrophils and macrophages play an importantrole in increasing protease activity in the lung. However, therewas no difference between the upper and lower lobes in thenumbers and types of inflammatory cells, whereas the severityof the emphysematous lesions is more extreme in the upperlobe (35, 36). Recently, the predominance of T-lymphocytes inemphysematous lungs has been reported. One study describeda significant association between alveolar wall destruction andthe number of CD8+ T-lymphocytes (37). However, our data
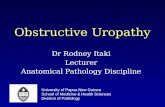
using specimens obtained from lung volume reduction surgeryhave shown a relationship between the number of CD4+ T-lymphocytes and alveolar wall destruction (unpublished ob-servation) (Fig. 4). Further study is necessary to determine the
p
recise role of T-lymphocytes in alveolar destruction.In summary, lesions develop when central airways are irri-
tated and respond with mucus hypersecretion and mucous glandenlargement. The peripheral airways respond by becoming in-flamed, leading to fibrosis and airway narrowing. In the paren-chyma, the inflammation results in alveolar wall destructionand emphysema.
Pathophysiology
Most patients with chronic airflow limitations have centralairway lesions, peripheral airway lesions, and emphysema invarying combinations of severity. Many reports have describedthe presence of peripheral airway lesions in patients with se-verechronicairflow limitations. However, the great majority
of these reports describe the patients as having either emphy-sema or chronic bronchitis; assessing the functional signifi-cance of individual morphological abnormalities is thus diffi-cult. To clarify the relative importance of central airway le-sions, peripheral airway lesions, and emphysema in expiratoryairflowabnormalities, quantitative functional-structural correla-
t
ive studies have been performed.
The clinico-pathological correlative studies showed thatperipheral airway lesions resulting in airway narrowing play asignificant role in causing airflow limitation. Emphysematouslesions were also found to limit expiratory airflow. The largeststudy, involving a wide range of airflow limitations, indicatedthat in patients with moderate to severe emphysema, the lossof elastic recoil induced by the emphysematous lungs has astronger effect on airflow limitation than that of the peripheral
C D 4
C O P D S m o k e r N o n s m o k e r1 2 1 2 1 2
1 0 1 0 1 0
S o 8 8
C D
o 61- I
6 6
^ 4CDo
2
0
0
- 4 - E
4 2
�"�"�".r *
4
ォ . . I�": i v : ~ . . ' } : ' 2
* *.�".�" 0 * -
.0 0 .2 0 .4 0 .6 0 .8 0 .0 0 .2 0 .4 0 .6 0 .8 1 .0 0 .0 0 .2 0 .4 0 .6 0 .8 1 .0V a lv / V v V a l v / V v V a l v / V v
m p h y s e m a F ib r o s is 蝣
Figure 4. Morphometric study shows the relationship between the number of CD4+ T-lymphocytes and the extent of emphy-semaby the lower volume density of the lung parenchyma (Vvalv).
Internal Medicine Vol. 41, No. 4 (April 2002) 267

Nagai
Figure 5. Scanning electron micrograph shows that the loss ofalveolar attachments around peripheral airways contributes tothe narrowing of the lumen in the peripheral airways (x38).
lesions (24). When the emphysema is mild, however, the pe-ripheral lesions are most likely the primary cause of the air-
f
low limitation.
The loss of alveolar attachments around peripheral airwayscan contribute to the narrowing of the lumen in the peripheralairways, leading to airflow limitation (Fig. 5) (38). This effectmay occur as a result of emphysema, since the loss of alveolarattachments reflects the severity of emphysema which in turnis related to airflow limitation. A recent study using computedtomography of the chest to assess emphysema clearly showedthat the prevalence of grossly visible emphysema increases asFEV1 declines (Fig. 6), although the authors concluded that
a
irflow limitations and emphysema were not related (39).In summary, functional-morphologic correlative studies in-
volving quantitative assessments of the airways and lung pa-renchyma have indicated that emphysema may be the most sig-nificant factor in cases of moderate and severe chronic airflowlimitation; peripheral airway lesions also cause airflow limita-tion, but these lesions are likely to play a secondary role in thecase of serious COPD. In addition, central airway lesions areprobably not very important in airflow limitation. Concomi-tant lesions in the peripheral airways and lung parenchyma arethus responsible for chronic airflow limitations in the periph-eral airway regions.
References
1 ) NHLBI/WHO workshop report. Global initiative for chronic obstructivelung disease. National Institutes of Health, National Heart, Lung, andBlood Institute, Publication No. 2701, April, 2001.
2) U.S. Surgeon General. The Health Consequences of Smoking: Chronicobstructive lung disease. U.S. Department of Health and HumanServices,Washington, D.C. DHHS Publication No. 8450205, 1984.
3) Fletcher C, Peto R. The natural history of chronic airflow obstruction. BrMed J l: 1645-1648, 1977.
50^ 40CJc<D 30ua 20<Dw>サJl 10tf 0n
< 5 0 5 0 - 6 9 7 0 - 8 9 0 - 1 1 0 1 1 0 <
FEV: ( % p r e d ic t e d )
Figure 6. The prevalence of grossly visible emphysema increasesas FEV1 declines.
4
) Burrows B, Knudson RJ, Cline MG, Lebowitz MD.Quantitative rela-tionships between cigarette smoking and ventilatory function. AmRevRespir Dis 115: 195-205, 1977.
5
) Auerbach O, Hammond EC, Garfinkel L, Benante C. Relation of smok-
ing and age to emphysema. Whole-lung section study. N Engl J Med 286:853-857, 1972.
6
) Higgins MW,Keller JB, Becker M et al. An index of risk for obstructiveairways disease. AmRev Respir Dis 125: 144-151, 1982.
7
) American Thoracic Society. Standards for the diagnosis and care of pa-tients with chronic obstructive pulmonary disease. AmJ Respir Crit CareMed l52: S77-S120, 1995.
8
) Siafakas NM, Vermeire P, Pride NB, et al. and The European RespiratorySociety Task Force. Optimal assessment and management of chronic ob-structive pulmonary disease (COPD). Eur Respir J 8: 1398-1420, 1995.
9) Reid L. Pathology of chronic bronchitis. Lancet 1: 275-278, 1954.
1
0) Jamal K, Cooney TP, Fleetham JA, Thurlbeck WM.Chronic bronchitis.Correlation of morphologic findings to sputum production and flow rates.Am^RevRespir Dis 129: 719-722, 1984.
1
1) Nagai A, West WW,Paul JL, Thurlbeck WM.The National Institutes ofHealth Intermittent Positive-pressure Breathing Trial : Pathology studies.
I. Interrelationship between morphologic lesions. AmRev Respir Dis 132:937-945, 1985.
1
2) Niewoehner DE, Kleinerman J, Knoke JD. Regional chronic bronchitis.AmRev Respir Dis 105: 586-593, 1972.
1
3) Reid L. Measurement of the bronchial mucous gland layer: a diagnosticyardstick in chronic bronchitis. Thorax 15: 132-141, 1960.
1
4) Mullen JB, Wright JL, Wiggs BR, Pare PD, Hogg JC. Reassessment ofinflammation of airways in chronic bronchitis. Br Med J 291: 1235-1239,1985.
1
5) Thurlbeck WM.Aspects of chronic airflow obstruction. Chest 72: 341-349, 1977.
1
6) O'Shaughnessy TC, Ansari TW, Barnes NC, Jeffery PK. Inflammation inbronchial biopsies of subjects with chronic bronchitis: inverse relation-ship of CD8+ T lymphocytes with FEV1. AmJ Respir Crit Care Med155: 852-857, 1997.
1
7) Saetta M, Turato G, Facchini FM, et al. Inflammatory cells in the bron-chial glands of smokers with chronic bronchitis. AmJ Respir Crit CareMed 156: 1633-1639, 1997.
1
8) Saetta M, Di Stefano A, Maestrelli P, et al. Airway eosinophilia in chronicbronchitis during exacerbations. AmJ Respir Crit Care Med 150: 1646-
1652, 1994.
19) Hogg JC, Macklem PT, Thurlbeck WM. Site and nature of airway ob-
268 InternalMedicineVol. 41, No. 4 (April 2002)

Pathology and Pathophysiology of COPD
struction in chronic obstructive lung disease. N Engl J Med 278: 1355-1360, 1968.
2
0) Niewoehner DE, Kleinerman J, Rice DP. Pathologic changes in the pe-ripheral airways of young cigarette smokers. N Engl J Med 291: 755-758, 1974.
2
1) Cosio MG, Hale KA, Niewoehner DE. Morphologic and morphometriceffects of prolonged cigarette smoking on the small airways. AmRevRespir Dis 122: 265-271, 1980.
2
2) Wright JL, Lawson LM, Pare PD, Kennedy S, Wiggs B, Hogg JC. Thedetection of small airways disease. Am Rev Respir Dis 129: 989-994,1984.
2
3) Mitchell RS, Stan ford RE, Johnson JM, Silvers GW, Dart G, George MS.The morphologic features of the bronchi, bronchioles and alveoli in chronicairway obstruction: A clinicopathological study. Am Rev Respir Dis 114:137-145, 1976.
2
4) Nagai A, West WW,Thurlbeck WM.The National Institutes of HealthIntermittent Positive-pressure Breathing Trial: Pathology studies. II Cor-relation between morphologic findings, clinical findings, and evidence ofexpiratory airflow obstruction. AmRev Respir Dis 132: 946-953, 1985.
2
5) Nagai A, Yamawaki I, Thurlbeck WM,Takizawa T. Assessment of lungparenchymal destruction by using routine histologic tissue sections. AmRev Respir Dis 139: 313-319, 1989.
2
6) Cosio MG, Ghezzo H, Hogg JC, et al. The relations between structuralchanges in small airways and pulmonary function tests. N Engl J Med298: 1277-1281, 1978.
2
7) Hogg JC, Cosio M. The Pathophysiology of Small Airways, in: Sadoul P,Milic-Emili J, Simonsson BG, Clark TJH, Eds. Small Airways in Healthand Disease. Excerpta Medica, New York, 1979: 33-39.
2
8) Saetta M, Di Stefano A, Turato G, et al. CD8+ T lymphocytes in theperipheral airways of smokers with chronic obstructive pulmonary dis-ease. AmJ Respir Crit Care Med 157: 822-826, 1998.
2
9) de Boer WI, van Schadewijk A, Sont JK, et al. Transforming growth fac-tor beta 1 and recruitment of macrophages and mast cells in airways inchronic obstructive pulmonary disease. AmJ Respir Crit Care Med 158:1951-1957, 1998.
3
0) Pratt PC, Haque A, Klugh GA. Correlation of postmortem function andstructure in normal and emphysematous lungs. AmRev Respir Dis 83:856-865, 1961. j
3
1) Anderson AE, Foraker AG. Relative dimensions of bronchioles and pa-renchymal spaces in lungs from normal subjects and emphysematouspatients. AmJ Med 32: 218-226, 1962.
3
2) Linhartova A, Anderson AE, Foraker AG. Further observation on luminaldeformity and stenosis of non-respiratory bronchioles in pulmonary em-physema. Thorax 32: 53-59, 1977.
3
3) Nagai A, Yamawaki I, Takizawa T, Thurlbeck WM.Alveolar attachment^in emphysema of human lungs. AmRev Respir Dis 144: 888-891, 1991.
3
4) Repine JE, Bast A, Lankhorst I, and Oxidative Stress Study Group. Oxi-dative stress in chronic obstructive pulmonary disease. AmJ Respir CritCare Med 156: 341-357, 1997.
3
5) Wright JL. Airway inflammatory cells in upper and lower lobes in lungsof patients with and without emphysema. Pathol Res Pract 183: 297-300,1988.
3
6) Wright JL, Wiggs BJ, Hogg JC. Airway disease in upper and lower lobesin lungs of patients with and without emphysema. Thorax 39: 282-285,1984.
3
7) Saetta M, Baraldo S, Corbino L, et al. CD8+ve cells in the lungs of smok-ers with chronic obstructive pulmonary disease. Am J Respir Crit CareMed 160: 711-717, 1999.
3
8) Nagai A, Thurlbeck WM.Scanning electron microscopic observations ofemphysema in humans. AmRev Respir Dis 144: 901-908, 1991.
3
9) Hogg JC, Wright JL, Wiggs BR, Coxson HO, Saez AO, Pare PD. Lungstructure and function in cigarette smokers. Thorax 49: 473-478, 1994.
Internal Medicine Vol. 41, No. 4 (April 2002) 269