Atherosclerosis, Stenosis and Ischemia
77
Atherosclerosis, Stenosis and Ischemia: One Primary, One Secondary, One Tertiary James K. Min, MD Professor of Radiology and Medicine Weill Cornell Medicine Director, Dalio Institute of Cardiovascular Imaging NewYork-Presbyterian Hospital Editor-in-Chief Journal of Cardiovascular Computed Tomography
Transcript of Atherosclerosis, Stenosis and Ischemia

Atherosclerosis, Stenosis and Ischemia:
One Primary, One Secondary, One Tertiary
James K. Min, MD Professor of Radiology and Medicine
Weill Cornell Medicine
Director, Dalio Institute of Cardiovascular Imaging
NewYork-Presbyterian Hospital
Editor-in-Chief
Journal of Cardiovascular Computed Tomography
• Research Support: National Institutes of Health, Dalio Foundation,
General Electric, Michael Wolk Foundation
• Medical Advisory Board: General Electric, Arineta
• Ownership Interest: Cleerly
Disclosures

• Quote
• Premise
• Patient
• Prediction
Outline

If I had an hour to solve a problem and my life depended on it,
I would use the first 55 minutes determining the proper questions to ask.
- Albert Einstein
Quote
• Atherosclerosis evaluation should be the primary objective to define (a)
clinical risk, (b) identify ischemia, and (c) guide therapeutic decision
making to improve patient-centered outcomes.
• Atherosclerosis = primary disease process
• Stenosis = secondary anatomic consequence of atherosclerosis
• Ischemia = tertiary physiologic consequence of atherosclerosis plus stenosis
Premise
We are asking the right questions . . . in the wrong order

Left anterior descending artery1st Diagonal Branch
Left circumflex artery Right coronary artery
• “Obstructive”
• “Obstructive”
• “Non-obstructive”
• Normal
63 y/o man with chest pain on exertion
What is the question that we are trying answer?

Diagnostic Performance of CT versus Cath for High-Grade Stenosis
N Prevalence Sensitivity Specificity PPV NPV
ACCURACY1 230 25% 94 83 48 99
Stable Chest Pain; No known CAD; No exclusion for calcium score, heart rate or body mass
index
Europe2 360 68% 99 64 85 97
Acute and Stable Chest Pain; No known CAD
CorE643 291 56% 85 90 91 83
Stable Chest Pain; No known / Known CAD; Exclusion for coronary calcium score >600
Source: 1Budoff et al. J Am Cardiol 2008; 2Meijboom et al. J Am Coll Cardiol 2009; 3Miller et al. N Engl J Med 2008;
• Prospective multicenter studies comparing CT to invasive coronary angiography for
identification and exclusion of >50% stenosis
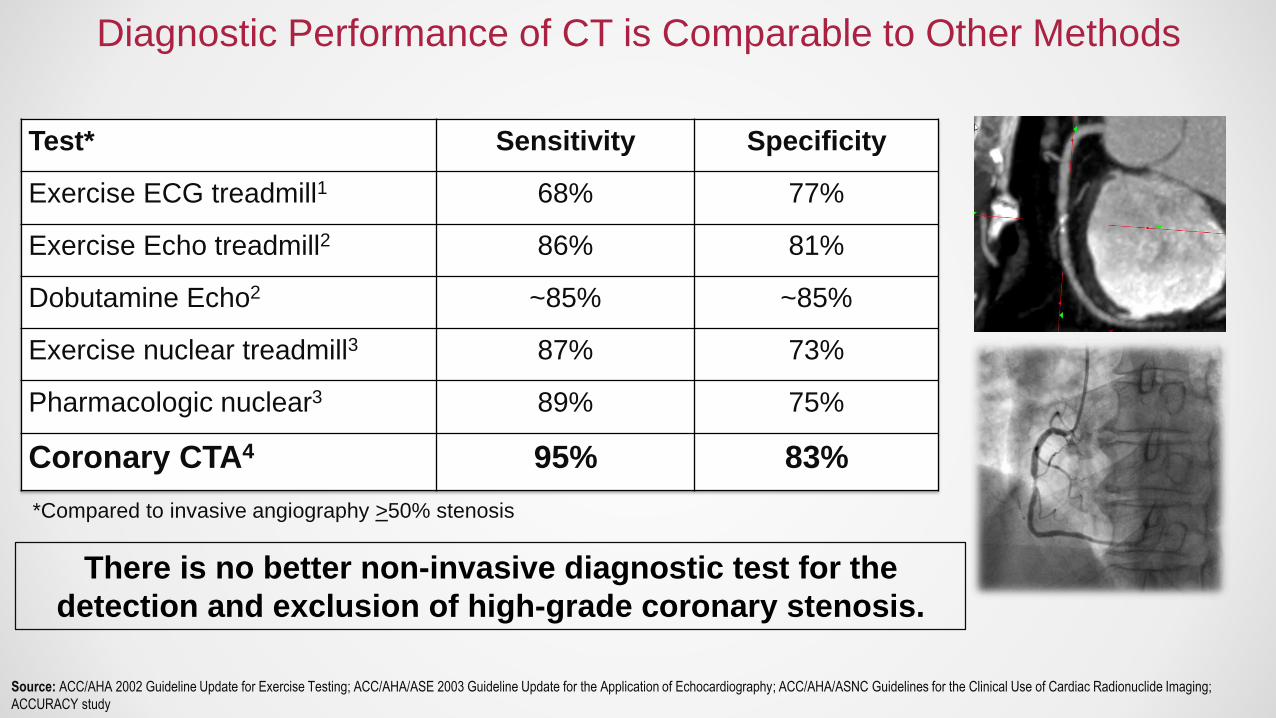
Diagnostic Performance of CT is Comparable to Other Methods
Test* Sensitivity Specificity
Exercise ECG treadmill1 68% 77%
Exercise Echo treadmill2 86% 81%
Dobutamine Echo2 ~85% ~85%
Exercise nuclear treadmill3 87% 73%
Pharmacologic nuclear3 89% 75%
Coronary CTA4 95% 83%
Source: ACC/AHA 2002 Guideline Update for Exercise Testing; ACC/AHA/ASE 2003 Guideline Update for the Application of Echocardiography; ACC/AHA/ASNC Guidelines for the Clinical Use of Cardiac Radionuclide Imaging;
ACCURACY study
*Compared to invasive angiography >50% stenosis
There is no better non-invasive diagnostic test for the
detection and exclusion of high-grade coronary stenosis.
Source: Min JK et al. JACC 2011; Leipsic J et al. Radiology 2013
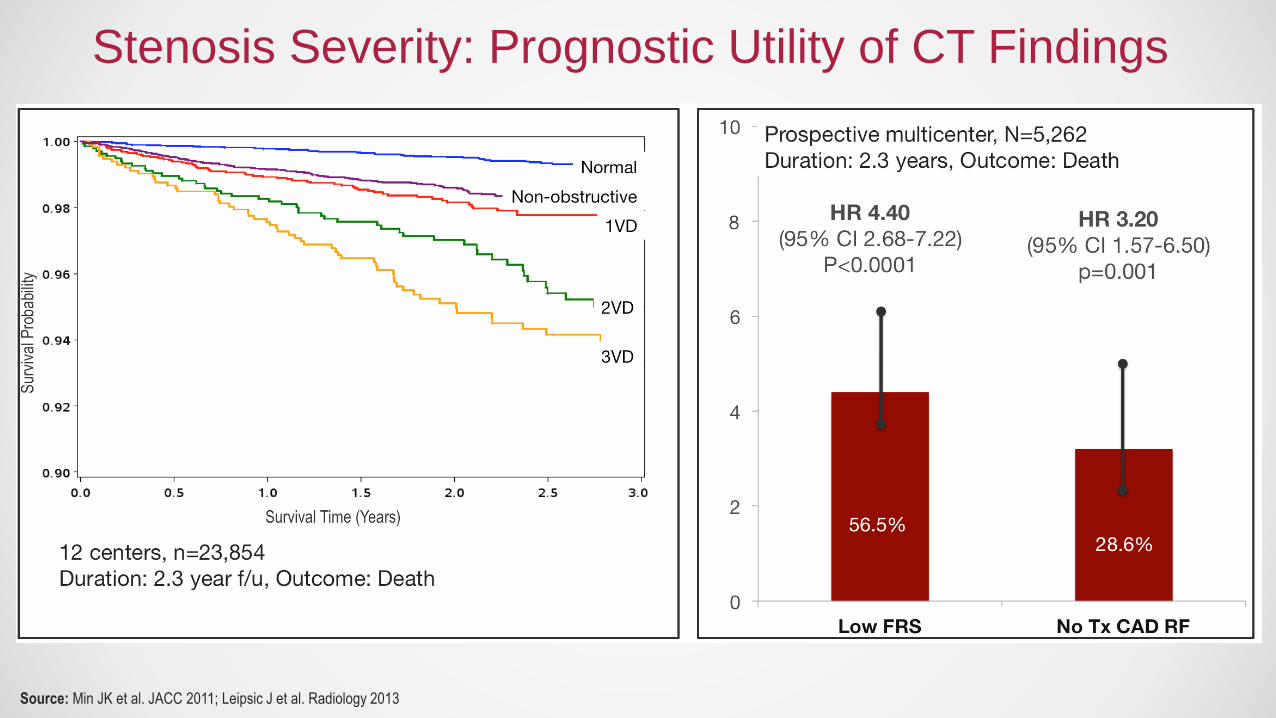
Stenosis Severity: Prognostic Utility of CT Findings

0
2
4
6
8
10
12
14
16
1VD 2VD 3VD
HR 1.93 HR 2.74 HR 6.09
>6-fold higher mortality for patients with 3V “mild” CAD
n=2,583, all with <50% stenosis
Followed for 3.1 years for ACM
“Mild” Stenoses Prognosticate Events in Dose-Dependent Fashion.
Source: Lin FY et al. J Am Coll Cardiol 2008

Source: Ostrom et al. J Am Coll Cardiol 2008; Andreini et al. JACC Imaging 2012; Hadamitzky et al. Eur Heart J 2013; CONFIRM
The Absence of Stenosis Confirms the Absence of Risk“Warranty Period” of Normal CT >10 Years

Extent/Severity of CAD Findings
Ris
k*
*Adjusted or unadjusted • Elderly
• Men and Women
• No Hx CAD
• CAC=0
• No modifiable risk
factors
• Known CAD
• Post-CABG
• Post-PTCA
• Ethnicity
• Diabetes
• Young
• Family history
• LV dysfunction
• Known CAD
• Chronic total
occlusion
• CKD
Stenosis Severity: Prognostic Utility of CT Findings
Source: Min et al. J Am Coll Cardiol 2011; Chow et al. Circ CV Imaging 2011; Villines et al. J Am Coll Cardiol 2011; Cheng et al. Circulation 2011; Cho et al. Circulation 2012; Chow et al. J Am Coll Cardiol 2011;
Villines et al. Am J Cardiol 2012; Shaw et al. J Am Coll Cardiol 2012; Min et al. Eur Heart J 2012; Nakazato et al. Atherosclerosis 2012; Rana et al. Diabetes Care 2012; Otaki et al. J Nucl Cardiol 2012; Hadamitzky M
et al. J Am Coll Cardiol 2013; Al-Mallah MH et al. Eur Heart J Cardiovasc Imaging 2014; Shah S et al. J Nucl Cardiol 2014; Nakazato R et al. Eur Heart J Cardiovasc Imaging 2014; Arsanjani R et al. Radiology 2014;
Leipsic J et al. Radiology 2014; Cho I et al. Eur Heart J 2015; Schulman-Marcus J et al. Atherosclerosis 2015; Otaki Y et al. Eur Heart J Cardiovasc Imaging 2015; Chow BJ et al. Arterioscler Thromb Vasc Biol 2015;
Ahmadi A et al. PLoS One 2015; Gebhard C et al. Eur Heart J Cardiovasc Imaging 2015; Cheruvu C et al. J Cardiovasc Comput Tomogr 2016; Schulman-Marcus J et al. JACC Cardiovasc Imaging 2016; Gebhard C et
al. Eur Heart J Cardiovasc Imaging 2017; Blanke P et al. JACC Cardiovasc Imaging 2016; Andreini D et al. Int J Cardiol 2017; Naoum C et al. Circ Cardiovasc Imaging 2017; Schulman-Marcus J et al. Eur Heart J
Cardiovasc Imaging 2017; Deseive S et al. Eur Heart J Cardiovasc Imaging 2017; Nakanishi R et al. Hypertension 2017; Xie JX et al. Circ Cardiovasc Imaging 2017

Source: Schulman-Marcus J et al. Atherosclerosis 2015; Min JK et al. Eur Heart J 2012
Aspirin StatinsBeta
BlockerAce
Inhibitor
% Difference -26 -43 5 38
-26-43
5
38
-100
-50
0
50
100
% D
iffe
ren
ce
in
MA
CE
1° Prevention
2° Prevention
• N=1,637 patients with >50% stenosis
• Outcome: MACE @ 3 years
Medical Therapy
*
*p<0.05
• N=15,223 (high risk vs. non-high risk dx)
• Outcome: Mortality @ 2.1 years
Revascularization
Effective Stenosis-Guided Therapy Improves Survival

• Hypothesis: Use of a CT-based strategy will improve the diagnosis of angina
pectoris secondary to CHD at 6 weeks
RANDOMIZE
Standard of CareStandard of Care
plus CCTA
Suspected angina from CHD
(n-4146)
Additional Endpoints
• Diagnosis of any CHD
• Changes in planned
investigations
• Changes in therapy
Source: SCOT-HEART Investigators, Lancet 2015
Effective Stenosis-Guided Therapy Improves Survival
SCOT-HEART Randomized Controlled Trial

Source: SCOT-HEART Investigators, Lancet 2015
27
1518
9
1 14
10
5
10
15
20
25
30
Dx of CHD Planned testing Preventive Med Tx Anti-anginal
CT Stress Testing
% R
ecla
ssific
ation C
hange
38% Reduction in Fatal / Non-Fatal MI at 1.7 years (p=0.06)
Effective Stenosis-Guided Therapy Improves Survival
SCOT-HEART Randomized Controlled Trial

Source: SCOT-HEART Investigators, Lancet 2015
Effective Stenosis-Guided Therapy Improves Survival
SCOT-HEART 3-Year Follow-Up
• CCTA performed
• Results reviewed
• Management changes
• Preventive therapy initiated
• Coronary revascularization
Implementation Delay
HR 0.50
p=0.020
Impact of Alterations
in Therapy
• Equal revasc
• More preventive Tx
(HR 4.03, p<0.01)

0
-40
-33
-50 -61
-100
-80
-60
-40
-20
0
Hosp for AMI Death or MI Death or MI Death
Reduction in A
dvers
e E
vents
(n=282,830),
CMS
(n=10,003),
PROMISE
(n=4146),
SCOT-Heart
(n=4244),
Observational
Time 180 d 12 months 20 months 80 months
Source: Hlatky MA et al. JAMA 2011; Douglas P et al NEJM 2015; Newby D et al. Lancet 2015, Budoff MJ et al. Atherosclerosis 2014
SCOT-HEART is consistent with all other studies to date.

RANDOMIZE
1600 Stable Patients with Suspected Coronary Heart Disease
Referred to Cath Based Upon ACC / AHA Class II Guideline
Direct Cath StrategyInvasive
Coronary Angiography
Physician Discretion
Selective Cath StrategyNon-invasive
Coronary CT Angiography
Physician Discretion
Source: Chang HJ et al. Late-Breaking Clinical Trials, European Society of Cardiology, August 2016
CONSERVE RCTCan CT serve as a safe, non-invasive, economically efficient “gatekeeper”?

Source: Chang HJ et al. Late-Breaking Clinical Trials, European Society of Cardiology, August 2016
-78
-45-50
-100
-80
-60
-40
-20
0
%
CONSERVE RCTCan CT serve as a safe, non-invasive, economically efficient “gatekeeper”?
Cath Rates Revasc Cardiovascular Costs
Selective Cath Strategy vs. Direct Cath Strategy
CT alone results in ~80% reduction in invasive coronary angiography.

Source: Chang HJ et al. Late-Breaking Clinical Trials, European Society of Cardiology, August 2016
Direct ICA Selective ICA
MACE Rates4.6%
(33/719)
4.6%
(36/784)
Hazards Ratio for MACE
(p=0.99)
31
1 2
8
02
33
2 2
9
02
0
10
20
30
40
50
CV Hosp CV Death MI UA Urgentrevasc
Stroke
No
. o
f E
ven
ts
No differences in any individual MACE
p=1.00 p=1.00 p=1.00 p=1.00 p=1.00 p=1.00
CONSERVE RCTCan CT serve as a safe, non-invasive, economically efficient “gatekeeper”?

Left anterior descending artery1st Diagonal Branch
Left circumflex artery Right coronary artery
• Ischemic?
• Ischemic?
• Non-ischemic?
• Normal
63 y/o man with chest pain on exertion
What is the question that we are trying answer?
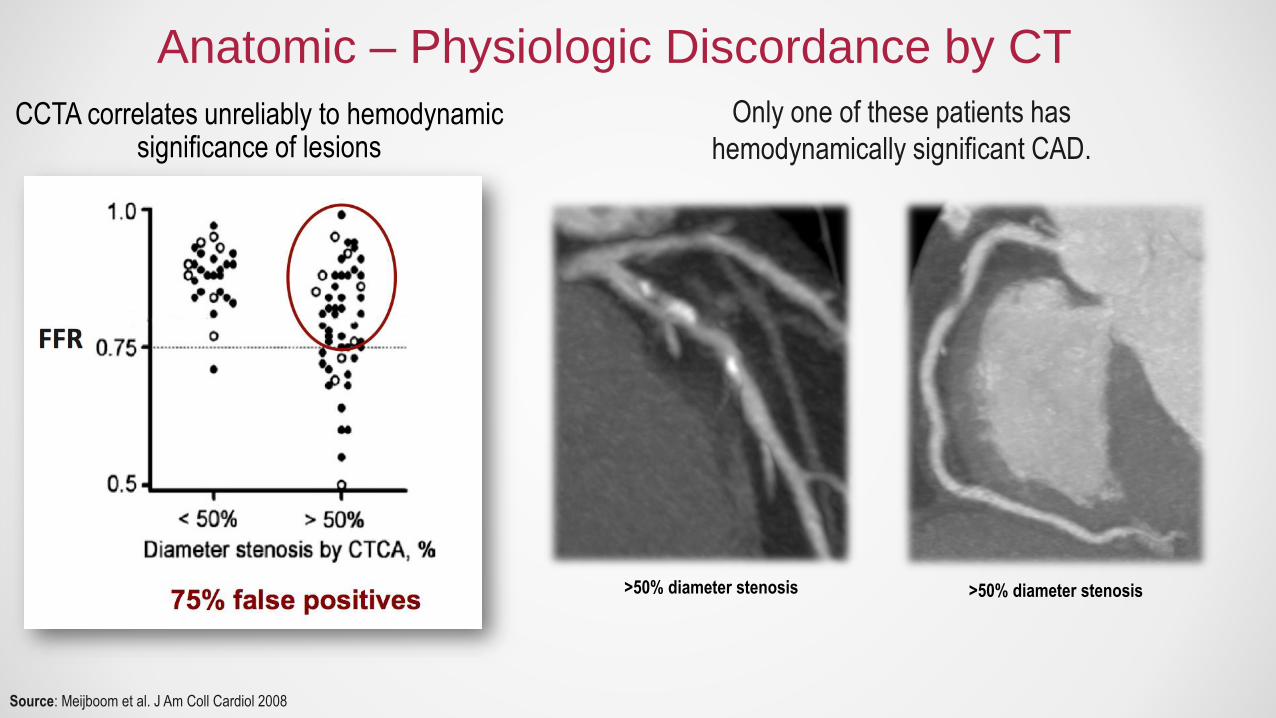
Anatomic – Physiologic Discordance by CT
CCTA correlates unreliably to hemodynamic significance of lesions
>50% diameter stenosis >50% diameter stenosis
Only one of these patients has
hemodynamically significant CAD.
Source: Meijboom et al. J Am Coll Cardiol 2008

Maximal MBF through a diseased artery
MBF in the hypothetical case the artery is normal
Lesion-specific ischemia: FFR <0.80
• Only method to pinpoint ischemia-causing lesions
• Only method to guide revascularization to improve event-free survival
Source: Pijls NH et al. J Am Coll Cardiol. 2007; Pijls NH et al. J. Am. Coll. Cardiol. 2010
FAME RCT, N=1,005
“Gold” standard for vessel-based ischemia
Invasive fractional flow reserve (FFR)

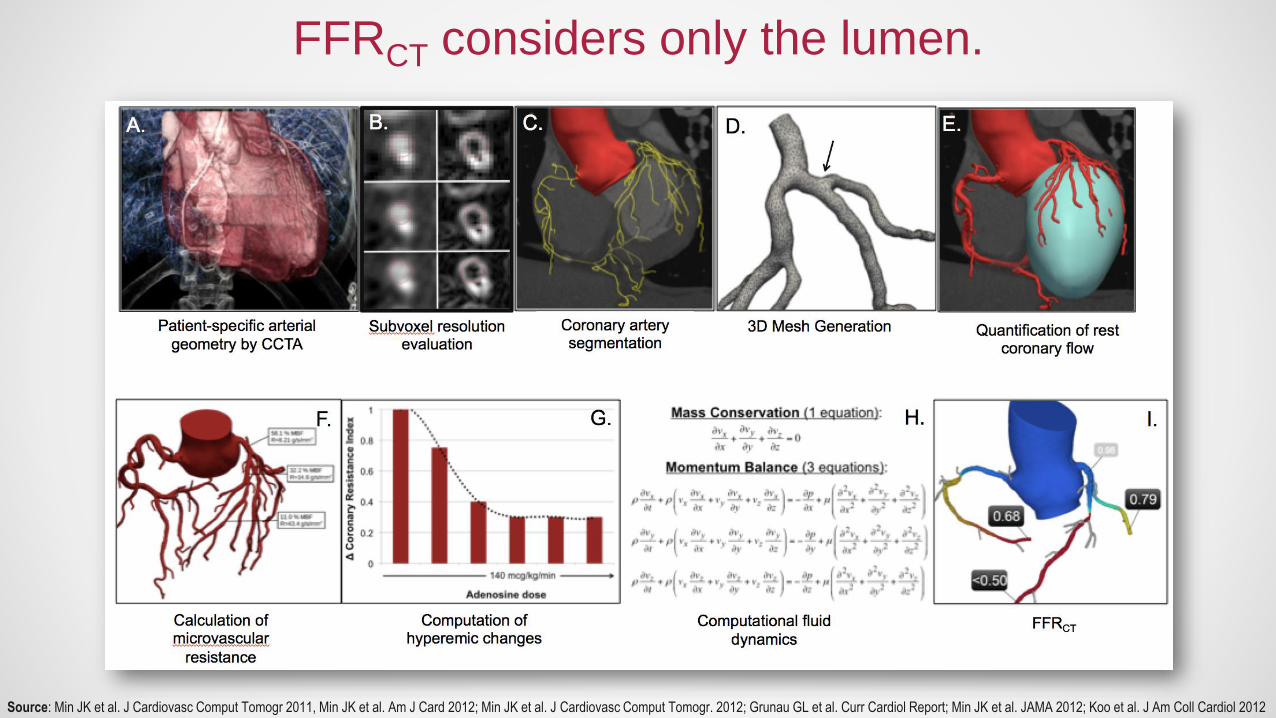
• From typically acquired CCTA
• No additional radiation
• No modification to imaging protocols
• No administration of medications
Source: Min JK et al. J Cardiovasc Comput Tomogr 2011, Min JK et al. Am J Card 2012; Min JK et al. J Cardiovasc Comput Tomogr. 2012; Grunau GL et al. Curr Cardiol Report; Min JK et al. JAMA 2012; Koo et al. J Am Coll Cardiol 2012
FFR from CT

FFRCT: Three (3) Prospective Multicenter Trials
DISCOVER-FLOW DeFACTO NXT
Principal Investigator Min (JACC) Min (JAMA) Norgaard (JACC)
Primary end point Per pt. diag accuracy Per pt. diag accuracy; lower
limit 95% CI 0.7
Per pt. AUC
Study sites/ countries 4 / 3 17 / 5 10 / 8
Site expertise qualification FFR CT or FFR CT plus FFR
CT training of site Yes No Yes
FFR training of site No No Yes
CT quality check No No Yes
CT results reading Core lab Core lab Site
FFR results report Site Site Site with core lab overview
Vessel size for inclusion ≥ 2.0 mm ≥ 1.5 mm ≥ 2.0 mm
Software version* V 1.0 manual V 1.2 partial automation ~6
hrs
V 1.4 automation; <4 hours
Source: Koo et al. JACC 2011; Min JK et al. JAMA 2012; Norgaard BL et al. JACC 2014

FFR from CT: Severe LAD Stenosis
Source: Min JK et al. JAMA 2012
CT: Severe Stenosis FFRCT: Lesion-specific Ischemia FFR: Ischemia

FFR from CT: Severe RCA Stenosis
Source: Min JK et al. JAMA 2012
CT: Severe Stenosis FFRCT: No Ischemia FFR: No Ischemia

FFR from CT
• 5 studies, n=539 (908 vessels)
• Only 13% with intermediate stenosis
Source: Cook CM et al. JAMA Cardiology 2017
• Accurate at the extremes
• Between 0.7-0.9 values – ~50%
Source: Min JK et al. J Cardiovasc Comput Tomogr 2011, Min JK et al. Am J Card 2012; Min JK et al. J Cardiovasc Comput Tomogr. 2012; Grunau GL et al. Curr Cardiol Report; Min JK et al. JAMA 2012; Koo et al. J Am Coll Cardiol 2012
FFRCT considers only the lumen.

• Stenosis alone
Source: Cook CM et al. JAMA Cardiology 2017
• Atherosclerosis
Sparse feature set Rich feature set
FFRCT considers only the lumen.
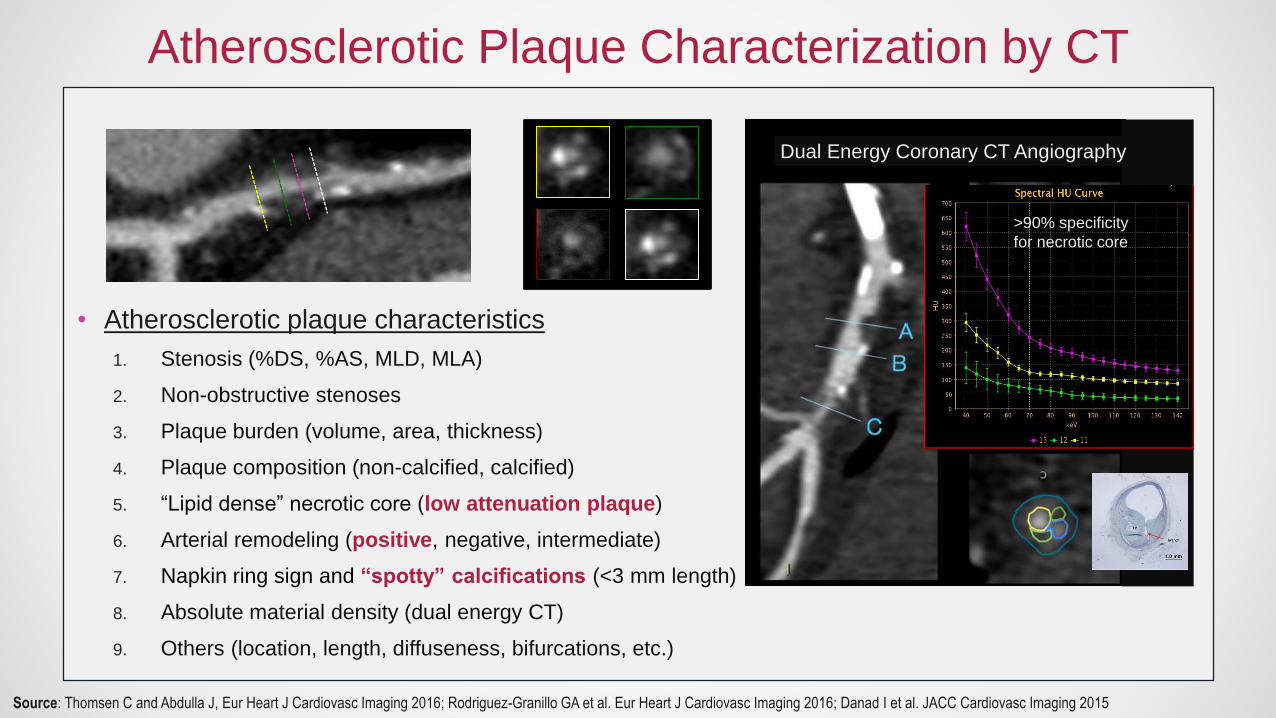
• Atherosclerotic plaque characteristics
1. Stenosis (%DS, %AS, MLD, MLA)
2. Non-obstructive stenoses
3. Plaque burden (volume, area, thickness)
4. Plaque composition (non-calcified, calcified)
5. “Lipid dense” necrotic core (low attenuation plaque)
6. Arterial remodeling (positive, negative, intermediate)
7. Napkin ring sign and “spotty” calcifications (<3 mm length)
8. Absolute material density (dual energy CT)
9. Others (location, length, diffuseness, bifurcations, etc.)
>90% specificity
for necrotic core
Dual Energy Coronary CT Angiography
Source: Thomsen C and Abdulla J, Eur Heart J Cardiovasc Imaging 2016; Rodriguez-Granillo GA et al. Eur Heart J Cardiovasc Imaging 2016; Danad I et al. JACC Cardiovasc Imaging 2015
Atherosclerotic Plaque Characterization by CT
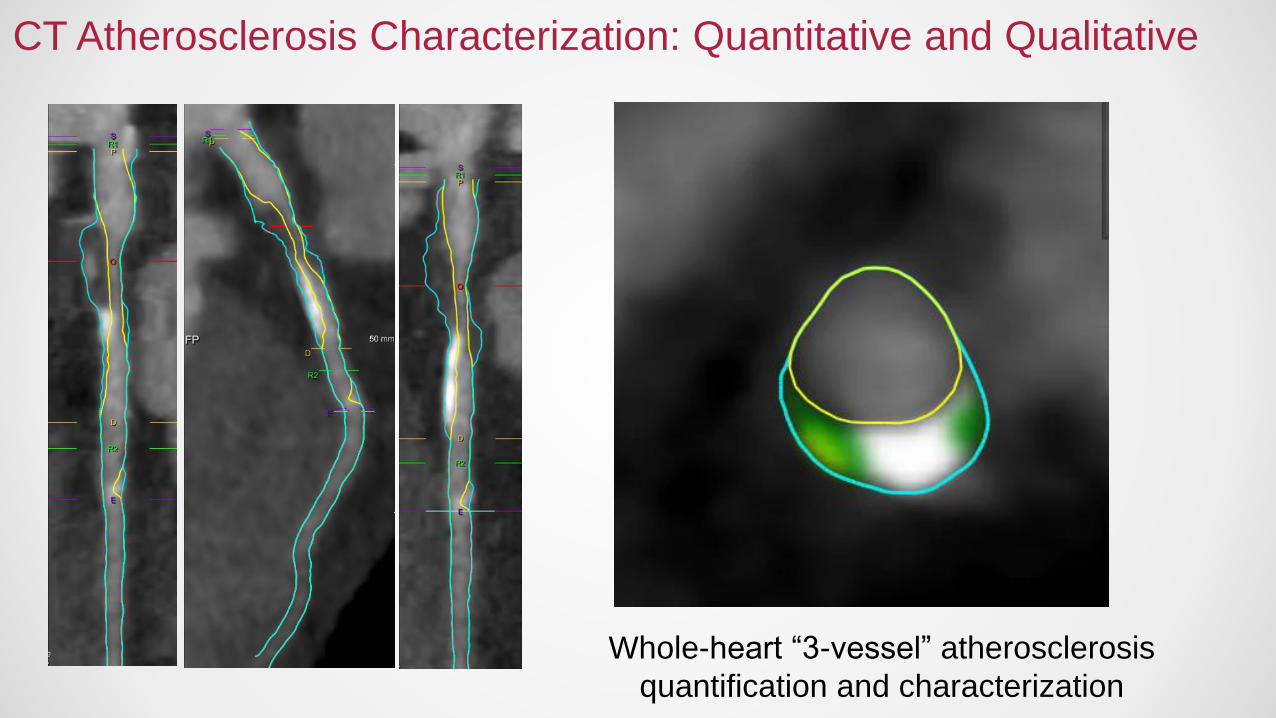
CT Atherosclerosis Characterization: Quantitative and Qualitative
Whole-heart “3-vessel” atherosclerosis
quantification and characterization

Source: Nakazato R et al. J Am Coll Cardiol 2012
Quantifying Plaque Burden Identifies Ischemia: Aggregate Plaque Volume

Source: Nakazato R et al. J Am Coll Cardiol 2012
• DS: 55.6%
• AS 59.5%
• APV 60.2%
• DS 63.3%
• AS 72.2%
• APV 27.8%
Ischemic Lesion Non-Ischemic Lesion
Quantifying Plaque Burden Identifies Ischemia: Aggregate Plaque Volume

Atherosclerosis Defines IschemiaPlaques look different because they act different.
A B C
C D E
The type of atherosclerosis is more important than the presence of atherosclerosis.

Source: Park HB et al. JACC Imaging 2015; Nakazato R et al. Eurointervention 2015
252 patients undergoing CT, ICA and FFR
Plaque Composition Identifies Ischemia
Agnostic to Stenosis Severity

Source: Park HB et al. JACC Imaging 2015; Nakazato R et al. Eurointervention 2015
Plaque Composition Identifies Ischemia
Agnostic to Stenosis Severity
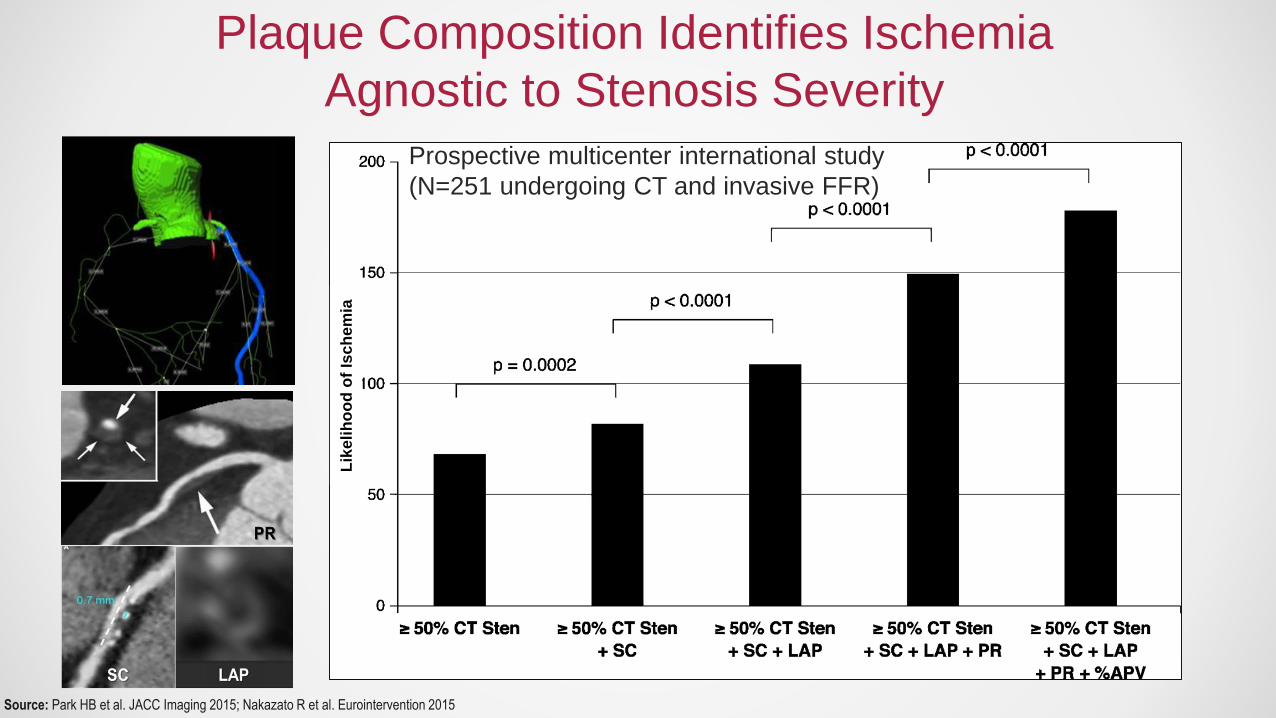
Prospective multicenter international study
(N=251 undergoing CT and invasive FFR)
Source: Park HB et al. JACC Imaging 2015; Nakazato R et al. Eurointervention 2015
Lik
eli
ho
od
of
Isc
he
mia
Plaque Composition Identifies Ischemia
Agnostic to Stenosis Severity
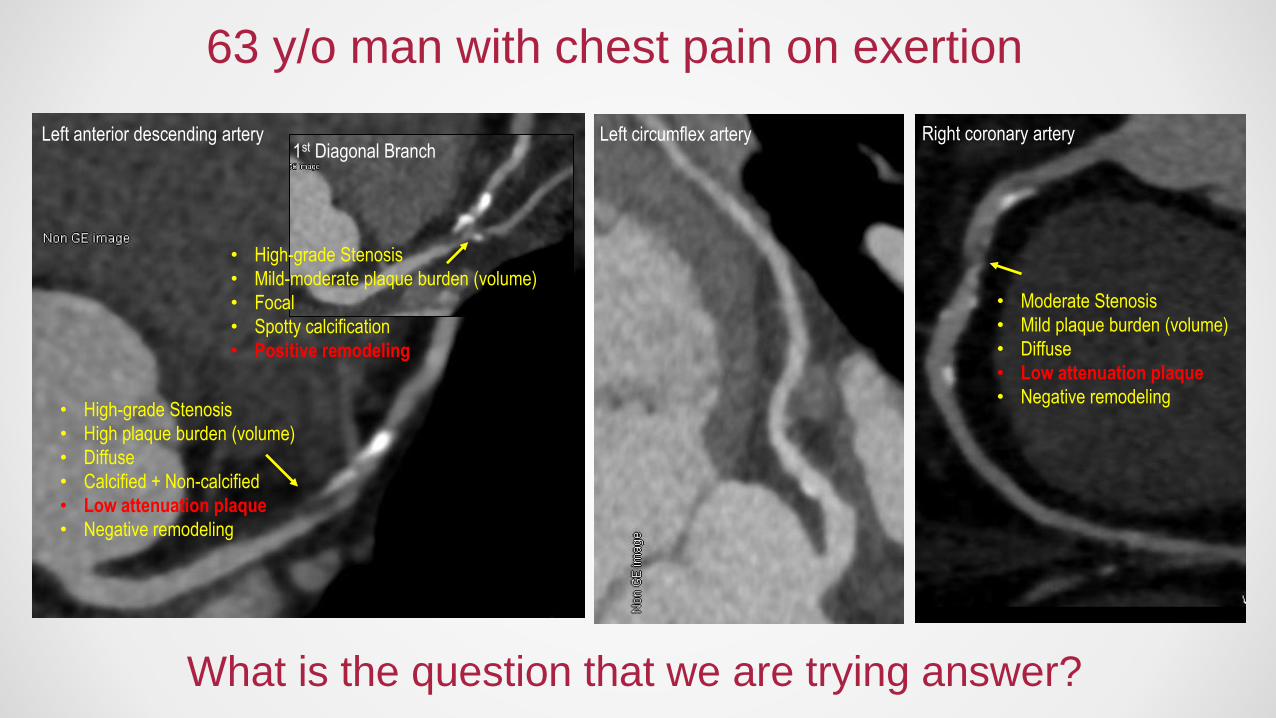
Left anterior descending artery1st Diagonal Branch
Left circumflex artery Right coronary artery
• High-grade Stenosis
• High plaque burden (volume)
• Diffuse
• Calcified + Non-calcified
• Low attenuation plaque
• Negative remodeling
• High-grade Stenosis
• Mild-moderate plaque burden (volume)
• Focal
• Spotty calcification
• Positive remodeling
• Moderate Stenosis
• Mild plaque burden (volume)
• Diffuse
• Low attenuation plaque
• Negative remodeling
63 y/o man with chest pain on exertion
What is the question that we are trying answer?

Source: Pooled data from 4 studies: Ambrose et al, 1988; Little et al, 1988; Nobuyoshi et al, 1991; and Giroud et al, 1992. (Adapted from Falk et al.)
Most Myocardial Infarctions Are Caused By Low Grade Stenoses
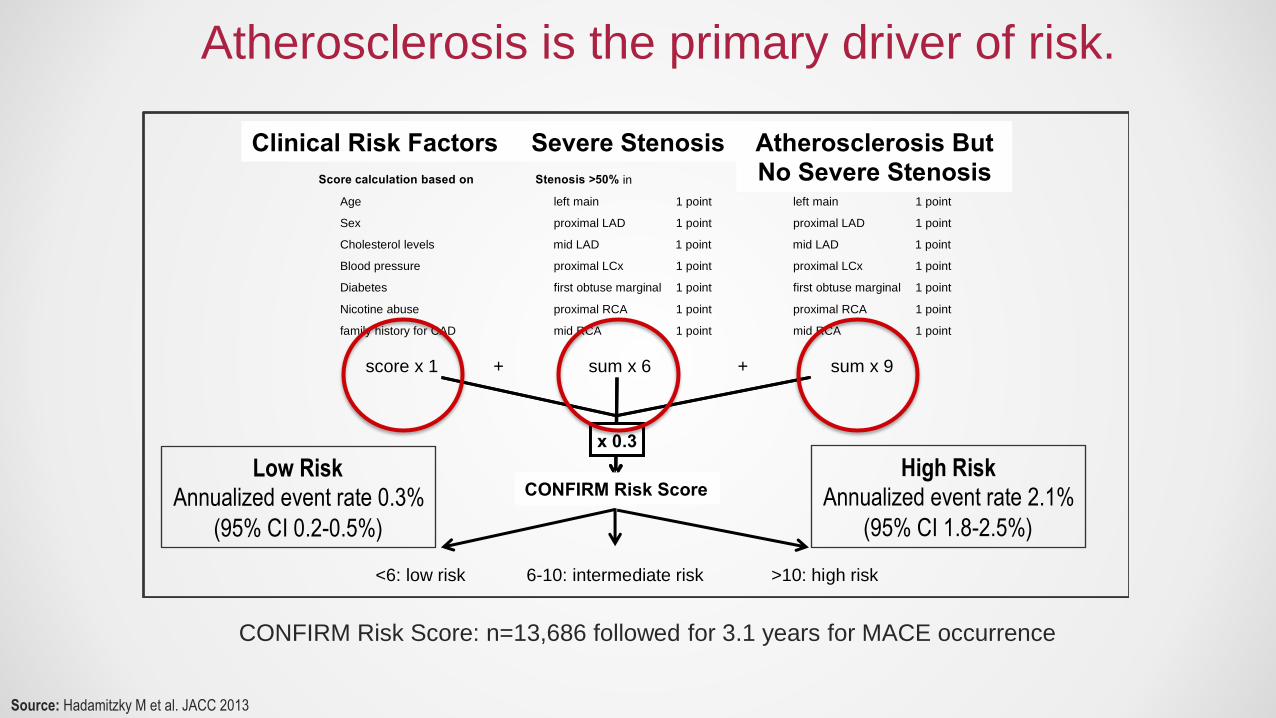
Atherosclerosis is the primary driver of risk.
CONFIRM Risk Score: n=13,686 followed for 3.1 years for MACE occurrence
Framingham Stenosis Plaque
Calcified or mixed plaque in
left main 1 point
proximal LAD 1 point
proximal LCx 1 point
first obtuse marginal 1 point
proximal RCA 1 point
mid RCA 1 point
Score calculation based on
Age
Sex
Cholesterol levels
Blood pressure
Diabetes
Nicotine abuse
family history for CAD
score x 1 sum x 6 sum x 9+ +
Confirm-Score
Stenosis >50% in
left main 1 point
proximal LAD 1 point
proximal LCx 1 point
first obtuse marginal 1 point
proximal RCA 1 point
mid RCA 1 point
x 0.3
mid LAD 1 pointmid LAD 1 point
<6: low risk 6-10: intermediate risk >10: high risk
Clinical Risk Factors
CONFIRM Risk Score Low Risk
Annualized event rate 0.3%
(95% CI 0.2-0.5%)
High Risk Annualized event rate 2.1%
(95% CI 1.8-2.5%)
Severe Stenosis Atherosclerosis But No Severe Stenosis
Source: Hadamitzky M et al. JACC 2013

Risk Increases With Atherosclerosis In the Absence of Stenosis.
Source: Cho I et al. Atherosclerosis 2017 (online before print)
N=6,656 followed for 5.1 years
All-cause mortality (n=456)
1.4
2.5
2.2
2
2.9
0
1
2
3
CAC 1-99 CAC >100 <50%Stenosis
Plaque, 0%Stenosis
>50%Stenosis
Ha
za
rds R
atio

High-risk Plaques: Positive Remodeling & Low Attenuation Plaque Qualitative atherosclerosis characterization portends ACS risk
Source: Motoyama S et al. J Am Coll Cardiol 2009
No APCs
PR, LAP, SC
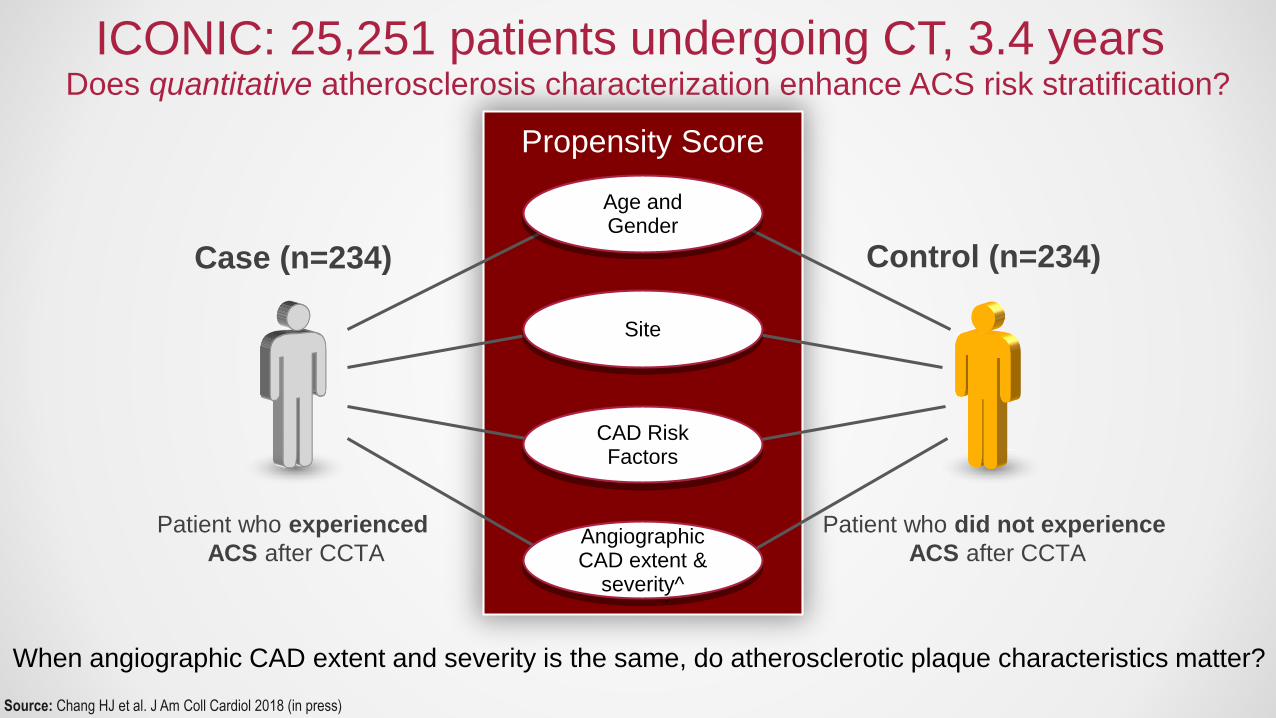
ICONIC: 25,251 patients undergoing CT, 3.4 years
Propensity Score
Age and Gender
Site
CAD Risk Factors
Angiographic CAD extent &
severity^
Patient who experienced
ACS after CCTA
Case (n=234)
Patient who did not experience
ACS after CCTA
Control (n=234)
Source: Chang HJ et al. J Am Coll Cardiol 2018 (in press)
When angiographic CAD extent and severity is the same, do atherosclerotic plaque characteristics matter?
Does quantitative atherosclerosis characterization enhance ACS risk stratification?

ICONIC Results: Maximal % stenosis at time of CT
<50% stenosis
65.4%21.8%
12.8%
Patient
(n=234)
50-70% stenosis >70% stenosis
Source: Chang HJ et al. J Am Coll Cardiol 2018 (in press)
75.2%20.1%
4.7%
Culprit Lesion
(n=129)

ICONIC Evaluation: High Risk Plaque (%)
52.1
43.2
87.6
30.833.3
27.4
79.9
20.1
0
10
20
30
40
50
60
70
80
90
100
HRP (> or = 2) Low Attenuation Positive Remodeling Spotty Calcification
p=0.003
58% higher
p<0.001
58% higher
p=0.026
9.6% higher
p=0.013
53.2% higher
ACS No ACS
Source: Chang HJ et al. J Am Coll Cardiol 2018 (in press)

ICONIC Evaluation: Plaque Volume (mm3)
Total
127
112
0
20
40
60
80
100
120
140
Fibrous
p=NSp=NS
ACS No ACS
98
109
0
20
40
60
80
100
120
Calcified
p=NS
290
267
0
50
100
150
200
250
300
350
Total
p=NS
Source: Chang HJ et al. J Am Coll Cardiol 2018 (in press)

ICONIC Evaluation: Plaque Volume (mm3)
290
267
255
260
265
270
275
280
285
290
295
Total
98
109
92
94
96
98
100
102
104
106
108
110
Calcified
p=NS
127
112
50
60
70
80
90
100
110
120
130
140
Fibrous
p=NS
6.5
4.2
3
3.5
4
4.5
5
5.5
6
6.5
7
Necrotic Core
p=0.026
55% higherp=NS
ACS No ACS
59
41
30
35
40
45
50
55
60
65
Fibrofatty
p=0.009
43% higher
Source: Chang HJ et al. J Am Coll Cardiol 2018 (in press)
Purely calcified plaques never cause ACS.

The Vulnerable Patient: Characterizing Atherosclerosis
Distance from ostium (mm)
Area (m
m2)
Remodeling index: 1.6
Left Anterior Descending Artery
Spotty Calcifications / Positive Remodeling
Source: Chang HJ et al. J Am Coll Cardiol 2018 (in press)
975 days later

What is the Most Important Feature of Atherosclerosis?
12/1/09
37% area stenosis
08/08/2013
67% area stenosis
How A Plaques Progresses Over Time

High-Risk Atherosclerotic Plaque Plus Plaque Progression
N=449, 4 years
Source: Motoyama S et al. J Am Coll Cardiol 2015; Ito H et al. Heart Vessels 2014
8.2
1.6 2.1
0
5
10
HRP >70% Stenosis Prior ACS
1.30.11
13.1
17.2
0
5
10
15
20
None >70%Stenosis
HRP Both
8.3
33.4
0
10
20
30
40
Prior ACS Progression
Timepoint 1 Timepoint 2

PARADIGM: Evolution of Atherosclerosis
CT#1MACE
3.8 years
CT#2
• Prospective observational cohort study
• N=1,255, 13 sites, 7 countries
• Quantitative CT evaluation for APCs
• Lab testing, including lipid panels
9 years
Source: Lee SE et al. JACC CV Imaging 2018 (in press)
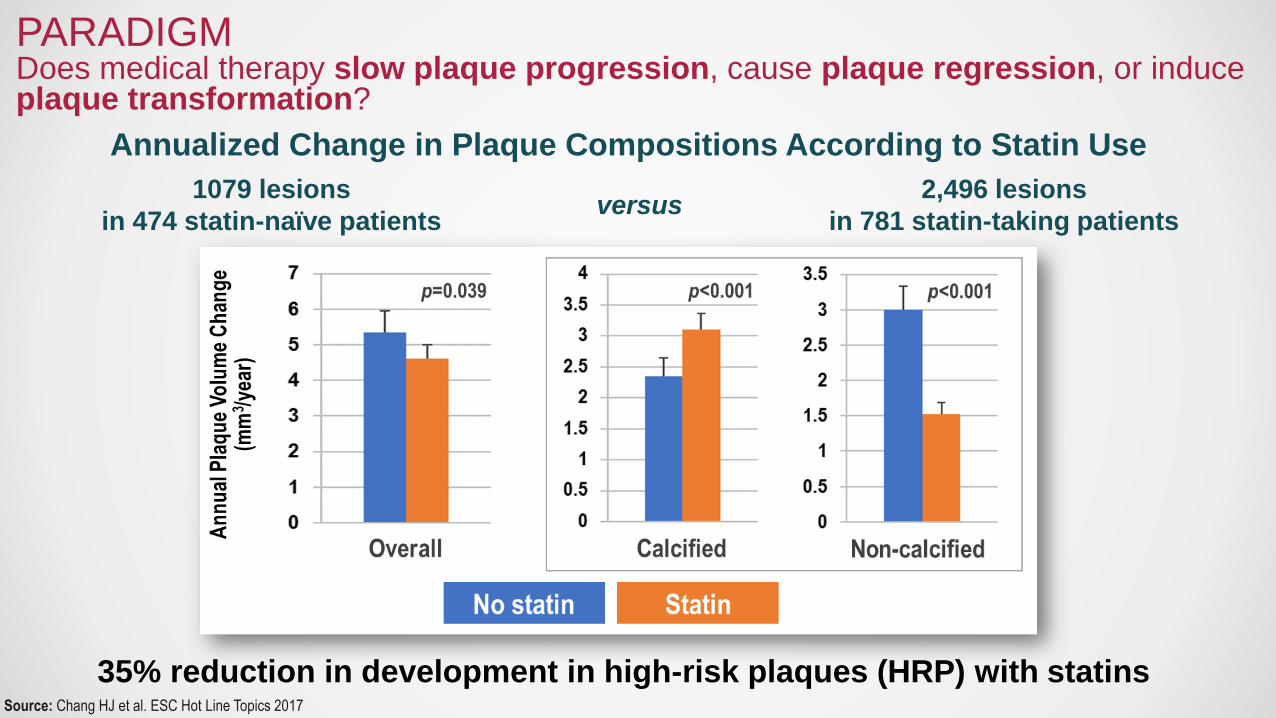
Source: Chang HJ et al. ESC Hot Line Topics 2017
35% reduction in development in high-risk plaques (HRP) with statins
PARADIGM Does medical therapy slow plaque progression, cause plaque regression, or induce plaque transformation?
1079 lesions
in 474 statin-naïve patients
2,496 lesions
in 781 statin-taking patientsversus
Annualized Change in Plaque Compositions According to Statin Use

Left anterior descending artery1st Diagonal Branch
Left circumflex artery Right coronary artery
• High-grade Stenosis
• High plaque burden (volume)
• Diffuse
• Calcified + Non-calcified
• Low attenuation plaque
• Negative remodeling
• High-grade Stenosis
• Mild-moderate plaque burden (volume)
• Focal
• Spotty calcification
• Positive remodeling
• Moderate Stenosis
• Mild plaque burden (volume)
• Diffuse
• Low attenuation plaque
• Negative remodeling
63 y/o man with chest pain on exertion
Atherosclerosis quantifies risk, identifies ischemia, and improves
therapeutic decision making.
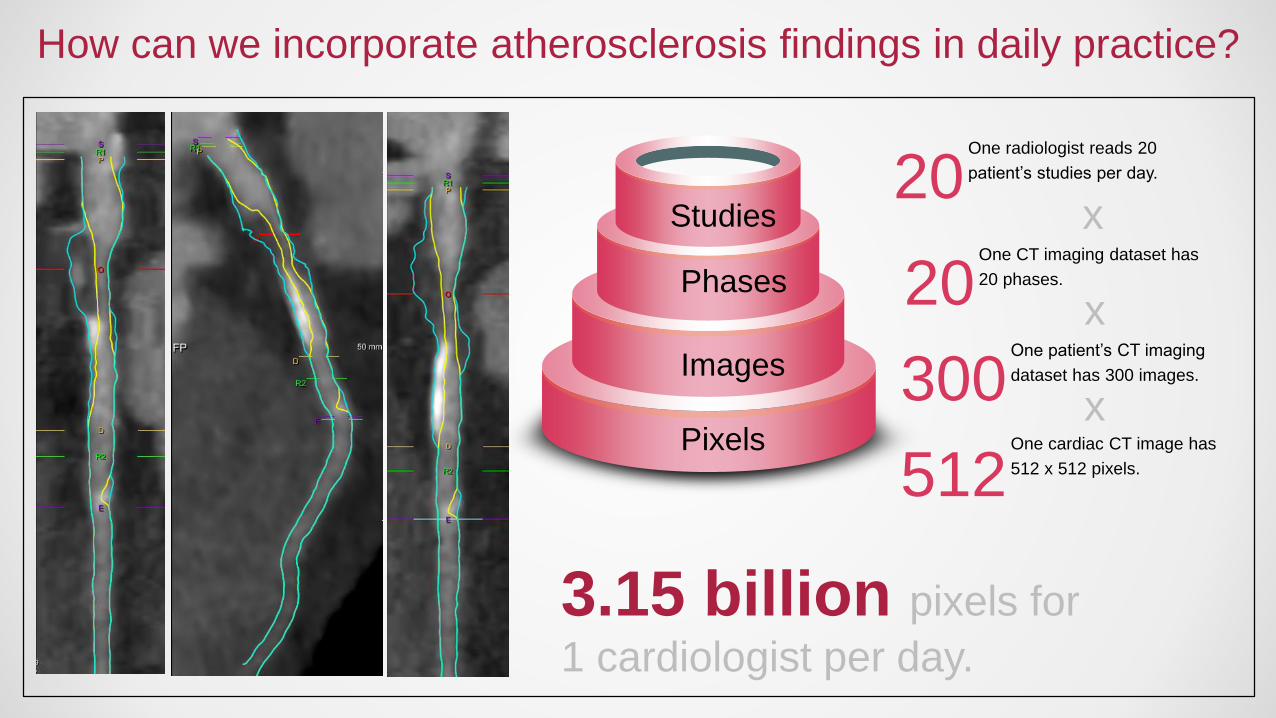
How can we incorporate atherosclerosis findings in daily practice?
512One cardiac CT image has
512 x 512 pixels.
300One patient’s CT imaging
dataset has 300 images.
20One CT imaging dataset has
20 phases.
20One radiologist reads 20
patient’s studies per day.
x
x
xPixels
Images
Phases
Studies
3.15 billion pixels for
1 cardiologist per day.

• “By 2025, 80% of the functions doctors do will be done much better and
much more cheaply by machines and machine learned algorithms.”
--Vinod Khosla
--Founder, Sun Microsystems
The Very Near-term Future

Machine Learning: Superhuman In Every Field To Date
Browsing
Shopping
“Liking”
(Personal
Preferences)
Meteorology
and
Farming
Credit Card
Fraud
SEARCH
“BIG DATA”
Drones
Self-driving
Cars
Voice
Recognition
Gunshot
Detection
HEARING
Oil
Refineries
AUTOMATION
Go
Jeopardy
Game Show
THINKING
Empathy
and
Ethics
SEEING
Facial
Recognition
Medical Imaging?
FEELING

Machines are particularly good at imaging.
• Classification
• Clustering
• Regression
• Association rules
• Ranking
• Grammar induction
• Feature learning

Machines are particularly good at imaging.
• Classification
• Clustering
• Regression
• Association rules
• Ranking
• Grammar induction
• Feature learning
Which stenosis is >70%?
Which plaques cause heart attacks?
Which plaques have necrotic cores?
Which plaque features together increase risk of heart attack?
Which plaques are most dangerous?
How should these findings be reported?
What features are most important?

Machines process images better and faster than we can.

Machines process images better and faster than we can.
Source: https://www.youtube.com/watch?v=VG68SKoG7vE

Machine can foresee outcomes better than we can.
Number of possible moves in Go = 10120
Number of atoms in universe = 1080
Source: nature.com (January 27 2016)
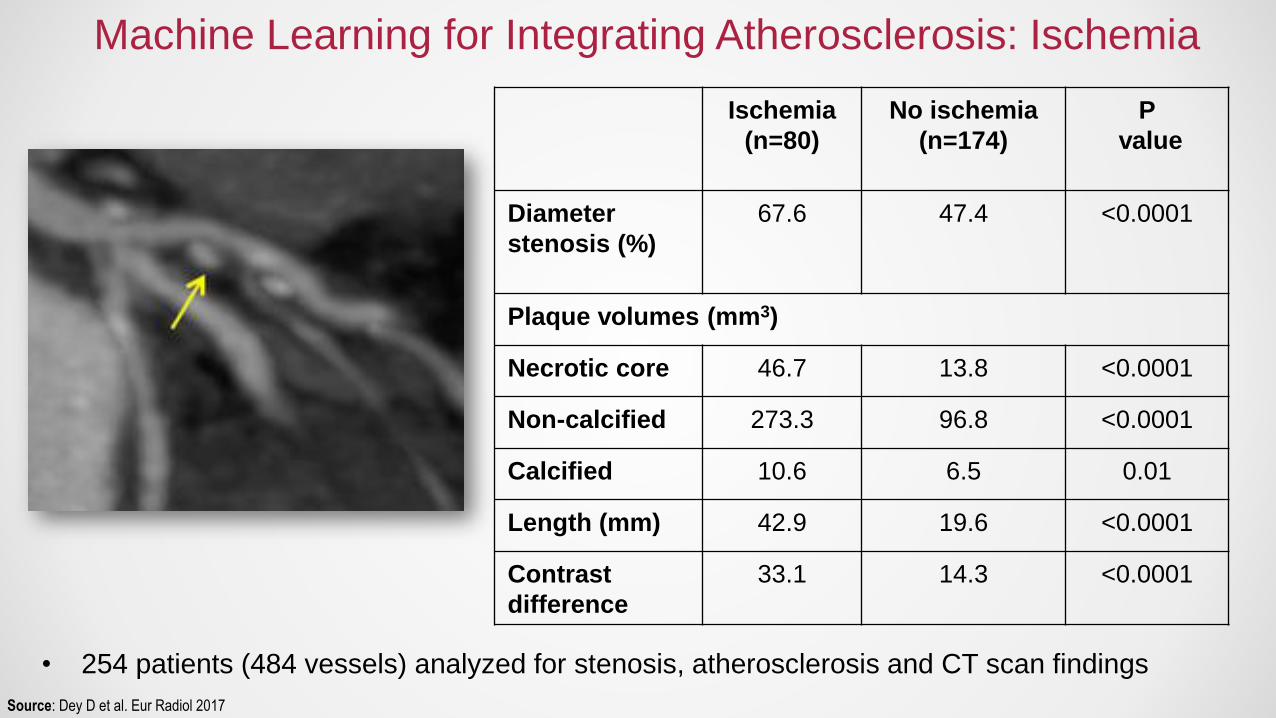
Machine Learning for Integrating Atherosclerosis: Ischemia
Source: Dey D et al. Eur Radiol 2017
• 254 patients (484 vessels) analyzed for stenosis, atherosclerosis and CT scan findings
Ischemia
(n=80)
No ischemia
(n=174)
P
value
Diameter
stenosis (%)
67.6 47.4 <0.0001
Plaque volumes (mm3)
Necrotic core 46.7 13.8 <0.0001
Non-calcified 273.3 96.8 <0.0001
Calcified 10.6 6.5 0.01
Length (mm) 42.9 19.6 <0.0001
Contrast
difference
33.1 14.3 <0.0001

• 254 patients (484 vessels) analyzed for stenosis, atherosclerosis and scan findings
• Highest predictive value for contrast density differences and low attenuation plaque
Source: Dey D et al. Eur Radiol 2017
Machine Learning for Integrating Atherosclerosis: Ischemia

Machine Learning for Atherosclerosis Risk Prediction
LAD Diag 1
Diag 2
RCALCX
Source: Motwani M et al. Eur H Journal 2017
10,030 patients followed for 5 years
44 CT + 25 clinical parameters
Conclusion
1. Atherosclerosis is primary; Stenosis is secondary; and Ischemia is tertiary
2. Atherosclerosis is the primary driver of future adverse events, and its treatment
improves event-free survival
3. Atherosclerosis-Defined Ischemia is a robust method for determining the ischemia-
causing nature of coronary artery lesions
4. Machine learning will transform the way we evaluate coronary artery disease.

Thank you.
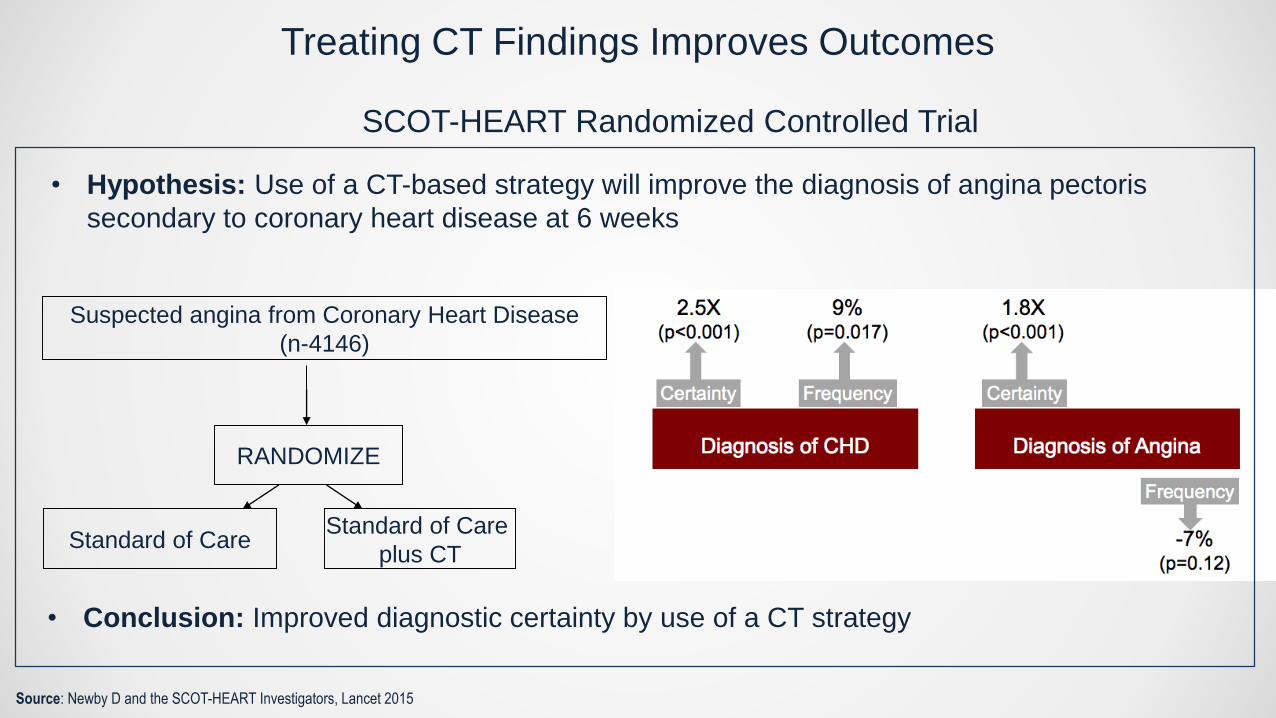
Treating CT Findings Improves Outcomes
RANDOMIZE
Standard of CareStandard of Care
plus CT
Suspected angina from Coronary Heart Disease
(n-4146)
Source: Newby D and the SCOT-HEART Investigators, Lancet 2015
• Conclusion: Improved diagnostic certainty by use of a CT strategy
• Hypothesis: Use of a CT-based strategy will improve the diagnosis of angina pectoris
secondary to coronary heart disease at 6 weeks
SCOT-HEART Randomized Controlled Trial

(2) Identify and Reduce Risk of Cardiac Events
• Identify coronary artery lesions that may cause future
cardiac events
• Institute medical therapy and to reduce risk
Source: Pooled data from 4 studies: Ambrose et al, 1988; Little et al, 1988; Nobuyoshi et al, 1991; and Giroud et al, 1992. (Adapted from Falk et al.)
(1) Identify and Relieve Myocardial ischemia
• Determine hemodynamic significance of CAD
• Identify high-grade stenosis (that may benefit from
revascularization)
Two (2) Major Goals for For Patients With Coronary Artery Disease
• Atherosclerosis = primary disease process
• Stenosis = secondary anatomic consequence of atherosclerosis
• Ischemia = tertiary physiologic consequence of atherosclerosis plus stenosis
Atherosclerosis Defines Ischemia

Plaque Volume (r=0.95, p<0.0001)
(105.0 vs. 109.4 mm3, p=NS)
1 mm cross-sections
• No Differences (Interobserver correlation, r=0.94, p<0.001)
- Plaque Burden: Volume, MLA, MLD, %AS, %DS
- Positive Remodeling
- Lipid-rich (Low Attenuation Plaque)
- Spotty Calcification
Source: Nakazato R et al. Eur Radiol 2013
CT Atherosclerosis Characterization: Comparison to IVUS

The Effect of Atherosclerosis on Perivascular Adipose Tissue Defines Risk.
• 453 patients undergoing cardiac surgery: related ex vivo images with CT scan
• FAI (Fat attenuation index) that describes adipocyte lipid content and size
• Identifies CAD
• A/w 18F-FDG PET inflammation
Source: Antoniades C et al. Science Transl Med 2017

ATHEROSCLEROSIS

Improved methods for atherosclerosis evaluation
>50% stenosis High-risk plaque Important
findings?
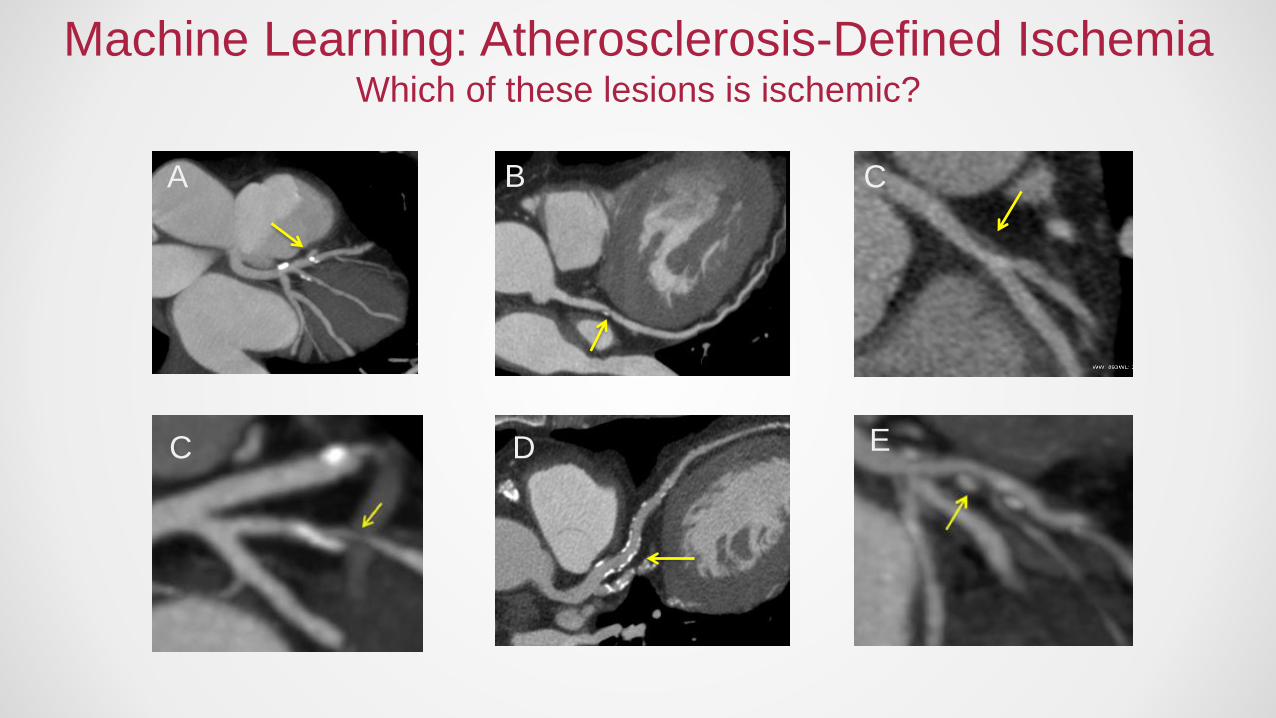
Machine Learning: Atherosclerosis-Defined IschemiaWhich of these lesions is ischemic?
A B C
C D E

Source: Mancini GB et al. JACC CV Interventions 2014
Atherosclerosis explains the relationship of ischemia to events.
Perc
en
t w
ith D
eath
, M
I or
NS
TE
-AC
S
Ischemic Myocardium
Angiographic
CAD Burden
(% stenosis)
COURAGE Trial
Ischemia does not improve risk stratification over anatomy.

Source: Park HB et al. JACC Imaging 2015; Nakazato R et al. Eurointervention 2015
Right coronary artery Left anterior descending
No ischemia(FFR 0.94)
Ischemia(FFR 0.79)
17% of CT lesions <50% stenosis exhibit ischemia by invasive FFR.
Plaque Composition Identifies Ischemia:Identification of Ischemia Agnostic to Stenosis Severity