Asymptomatic Aortic Regurgitation...Anatomy of aortic leaflets and root! Presence and severity of...
47
Asymptomatic Aortic Regurgitation Theodora Zaglavara, MD, PhD Euromedica Kyanous Stavros Hospital Thessaloniki, GREECE Wednesday, March 4, 15
Transcript of Asymptomatic Aortic Regurgitation...Anatomy of aortic leaflets and root! Presence and severity of...

Asymptomatic Aortic Regurgitation
Theodora Zaglavara, MD, PhDEuromedica Kyanous Stavros Hospital
Thessaloniki, GREECE
Wednesday, March 4, 15

No Disclosures
Wednesday, March 4, 15

Wednesday, March 4, 15

Pathophysiology of Chronic Aortic
Wednesday, March 4, 15

Pathophysiology of Chronic Aortic
Wednesday, March 4, 15

Pathophysiology of Chronic Aortic
Wednesday, March 4, 15

2 Major Questions: - Is Aortic Regurgitation Severe? - Does the Patient have
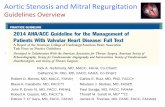
Survival Free of Surgery for AR after Diagnosis in Asymptomatic Patients. Patients are Stratified According to Quantitative Criteria of the ASE for AR Grading
Survival without Surgery in 242 Patients with Chronic AR Demonstrating the Importance of Symptoms in Determining Outcome
Dujardin et al. Circulation 1999J Am Coll Cardiol Img 2008
Wednesday, March 4, 15

! Anatomy of aortic leaflets and root! Presence and severity of AR! Additional echo findings ! Assessment of LV size and function! Assessment of the aorta
Wednesday, March 4, 15

Valve Anatomy/Aetiology and Mechanisms of AR/Functional Classification Calcification Grade/Suitability for Repair in Pure AR/Aortic Root Assessment
! Congenital (bicuspid unicuspid)! Degenerative (fibrosis/sclerosis)! Rheumatic! Endocaritis! Miscellaneous
! Hypertension! Bicuspid valve! Annuloaortic ectasia! Marfan syndrome! Aortic dissection
Leaflet AbnormalitiesAortic Root Abnormalities
• Aortic dissection• Trauma• Infective endocaritis• Post – balloon or surgical
valvotomy
Acute events
Wednesday, March 4, 15

Valve Anatomy/Aetiology and Mechanisms of AR/Functional Classification Calcification Grade/Suitability for Repair in Pure AR/Aortic Root Assessment
! Congenital (bicuspid unicuspid)! Degenerative (fibrosis/sclerosis)! Rheumatic! Endocaritis! Miscellaneous
! Hypertension! Bicuspid valve! Annuloaortic ectasia! Marfan syndrome! Aortic dissection
Leaflet AbnormalitiesAortic Root Abnormalities
• Aortic dissection• Trauma• Infective endocaritis• Post – balloon or surgical
valvotomy
Acute events
Wednesday, March 4, 15

Valve Anatomy/Aetiology and Mechanisms of AR/Functional Classification Calcification Grade/Suitability for Repair in Pure AR/Aortic Root Assessment
! Congenital (bicuspid unicuspid)! Degenerative (fibrosis/sclerosis)! Rheumatic! Endocaritis! Miscellaneous
! Hypertension! Bicuspid valve! Annuloaortic ectasia! Marfan syndrome! Aortic dissection
Leaflet AbnormalitiesAortic Root Abnormalities
• Aortic dissection• Trauma• Infective endocaritis• Post – balloon or surgical
valvotomy
Acute events
Wednesday, March 4, 15

Valve Anatomy/Aetiology and Mechanisms of AR/Functional Classification Calcification Grade/Suitability for Repair in Pure AR/Aortic Root Assessment
! Congenital (bicuspid unicuspid)! Degenerative (fibrosis/sclerosis)! Rheumatic! Endocaritis! Miscellaneous
! Hypertension! Bicuspid valve! Annuloaortic ectasia! Marfan syndrome! Aortic dissection
Leaflet AbnormalitiesAortic Root Abnormalities
• Aortic dissection• Trauma• Infective endocaritis• Post – balloon or surgical
valvotomy
Acute events
Wednesday, March 4, 15

Valve Anatomy/Aetiology and Mechanisms of AR/Functional Classification Calcification Grade/Suitability for Repair in Pure AR/Aortic Root Assessment
! Congenital (bicuspid unicuspid)! Degenerative (fibrosis/sclerosis)! Rheumatic! Endocaritis! Miscellaneous
! Hypertension! Bicuspid valve! Annuloaortic ectasia! Marfan syndrome! Aortic dissection
Leaflet AbnormalitiesAortic Root Abnormalities
• Aortic dissection• Trauma• Infective endocaritis• Post – balloon or surgical
valvotomy
Acute events
Wednesday, March 4, 15

Valve Anatomy/Aetiology and Mechanisms of AR/Functional Classification Calcification Grade/Suitability for Repair in Pure AR/Aortic Root Assessment
! Congenital (bicuspid unicuspid)! Degenerative (fibrosis/sclerosis)! Rheumatic! Endocaritis! Miscellaneous
! Hypertension! Bicuspid valve! Annuloaortic ectasia! Marfan syndrome! Aortic dissection
Leaflet AbnormalitiesAortic Root Abnormalities
• Aortic dissection• Trauma• Infective endocaritis• Post – balloon or surgical
valvotomy
Acute events
Wednesday, March 4, 15

Valve Anatomy/Aetiology and Mechanisms of AR/Functional Classification Calcification Grade/Suitability for Repair in Pure AR/Aortic Root Assessment
! Congenital (bicuspid unicuspid)! Degenerative (fibrosis/sclerosis)! Rheumatic! Endocaritis! Miscellaneous
! Hypertension! Bicuspid valve! Annuloaortic ectasia! Marfan syndrome! Aortic dissection
Leaflet AbnormalitiesAortic Root Abnormalities
• Aortic dissection• Trauma• Infective endocaritis• Post – balloon or surgical
valvotomy
Acute events
Wednesday, March 4, 15

Caution with Eccentric Jets!!
Wednesday, March 4, 15

Caution with Eccentric Jets!!
Wednesday, March 4, 15

Vena Contracta! The narrowest portion of the flow region at
or just below valve level ! Provides an estimate of the size of EROA! Simple, quantitative, highly feasible! Less sensitive to haemodynamic changes
or instrument settings! Not useful for multiple or irregular AR jets! < 0.3 not severe AR! > 0.6 severe AR (Nyquist Limit of 50-60 cm/
s)
Wednesday, March 4, 15

How to do PISA Measurements in AR! Use apical views! Zoom on supravalvular region! Shift colour doppler baseline upwards to obtain a rounded
and measurable PISA! Select frame with largest PISA and measure aliasing radius! Obtain CW Doppler recording of the regurgitant flow and
measure AR VTI! EROA and RV will be automatically calculated by most current
ultrasound systems
The thresholds for severe AR are an EROA ≥ 30 mm² and RV ≥ 60 ml and for mild AR an EROA < 10 mm² and RV < 30 ml
Wednesday, March 4, 15

Aortic Diastolic Flow Reversal
ED vel > 0.2 m/s
Wednesday, March 4, 15

Aortic Diastolic Flow Reversal
ED vel > 0.2 m/s
Wednesday, March 4, 15

Aortic Diastolic Flow Reversal
ED vel > 0.2 m/s
Wednesday, March 4, 15

Aortic Diastolic Flow Reversal
ED vel > 0.2 m/s
Wednesday, March 4, 15

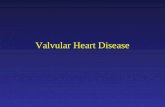
Consequences of Aortic Regurgitation
LVEDV: 229 ml, LVESV: 142 ml, EF: 38%
Wednesday, March 4, 15

Consequences of Aortic Regurgitation
LVEDV: 229 ml, LVESV: 142 ml, EF: 38%
Wednesday, March 4, 15

Consequences of Aortic Regurgitation
LVEDV: 229 ml, LVESV: 142 ml, EF: 38%
Wednesday, March 4, 15

New 2015!!!!!!!
Wealth of published data!!
Established prognostic value!Vendor dependent!
Global Longitudinal Strain
3-D Volumes
Less published data on normal values!!
Wednesday, March 4, 15

?????
Wednesday, March 4, 15

Natural History of Asymptomatic Aortic Regurgitation
Wednesday, March 4, 15

>65 mm IIb AHA 20014
Indications for Surgery in Chronic Severe Aortic Regurgitation
Wednesday, March 4, 15

J Am Coll Cardiol, 47 (2006), pp. 1012–1017
Survival After Aortic Valve Replacement for Aortic RegurgitationLong-term survival after valve replacement for aortic regurgitation demonstrating improved outcome with early surgery.
Wednesday, March 4, 15

Long-term Post-operative Survival in Patients with AR, Stratified According to the Severity of Preoperative Symptoms and Preoperative LVEF
Klodas E et al. J Am Coll Cardio 1997
Wednesday, March 4, 15

The Management of Asymptomatic AR Remains Challenging ! A balance needs to be reached between the competing risks
of chronic AR and having an artificial valve.
! Even if the risks of surgery were negligible, the need of either long-term anticoagulation for mechanical prosthesis or redo surgery for inevitable bioprosthetic valve degeneration imposes a significant disease burden.
! In contrast to MV repair AoV repair is limited to specific valve
Wednesday, March 4, 15

Aortic Valve and/or Root Repair for ARKvitting JP et al. J Thorac Cardiovasc Surg 2013
Surgical Results for Aortic Valve Repair and Aortic Valve Replacement with A Bioprosthesis
A. Bovine B. Porcine Pericardial Bioprosthesis
B. Annals Thorac Surgery 1998Annals Thorac Surgey 2001
Wednesday, March 4, 15

EF ≤ 50 %
LVDD >70 mm
LVSD > 50 mm (25 mm/m² BSA)
Wednesday, March 4, 15

Impact of ESVI Level on Cardiac Events Rates after Diagnosis of Asymptomatic
Wednesday, March 4, 15

LVESD : 53 mmSymptoms with Exercise
Lancellotti et al.Circulation: Cardiovascular Imaging. 2013; 6: 840-849
Limited Data Support the Use of Exercise Echocardiography in Patients with AR
Wednesday, March 4, 15

Global LV StrainGlobal RV StrainExercise TAPSE
Wednesday, March 4, 15

Survey in 120 departments performing Stress Echocardiography in the United Kingdom
Wednesday, March 4, 15

Cut off value GLS< -18%
Wednesday, March 4, 15

ACC/AHA 2014 Stages of Chronic Aortic Regurgitation A: At Risk of AR
B: Progressive AR
- Mild AR- Moderate AR
C: Asymptomatic severe AR1. Normal LVEF >50%, LVESD< 50 mm2. Abnormal LVEF <50%, LVESD>50 mm
Consider Exercise Testing to assess symptoms and haemodynamic response to exercise.
D: Symptomatic severe AR
Evidence of LV DilatationSymptomatic
Wednesday, March 4, 15

ACC/AHA 2014
Consider Exercise Testing
Consider Strain
Measurements
Wednesday, March 4, 15

34 year old patient: First diagnosis of bicuspid AoV and severe AR with mildly dilated LV and aorta in 2007.
2008 2010 2013
Wednesday, March 4, 15

34 year old patient: First diagnosis of bicuspid AoV and severe AR with mildly dilated LV and aorta in 2007.
2008 2010 2013
Wednesday, March 4, 15

34 year old patient: First diagnosis of bicuspid AoV and severe AR with mildly dilated LV and aorta in 2007.
2008 2010 2013
Wednesday, March 4, 15

34 year old patient: First diagnosis of bicuspid AoV and severe AR with mildly dilated LV and aorta in 2007.
2008 2010 2013
Wednesday, March 4, 15

NOT Too Early….BUT Early Enough!
Timing of Surgery in Asymptomatic Severe Aortic Regurgitation
The Anatomy Lesson of Dr. Nicolaes Tulp Rembrandt 1632, The Hague Netherlands
Wednesday, March 4, 15