Asthma lecture
27
ASTHMA
Transcript of Asthma lecture

ASTHMA

Case Definitions
“Reversible airway obstruction with airway inflammation and increased airways responsiveness to a variety of stimuli”
Samet JM, Marbury MC, Spengler JD. Health effects and sources of indoor air pollution. Part II. Am Rev Respir Dis. 1988 Jan;137(1):221–242.

Measuring airway obstruction: Spirometry
• PEF = Peak Expiratory Flow– Greatest flow sustained 10 milliseconds with a forced
expiration• FEV1 = Forced Expiratory Volume
– Volume of air expelled in 1st second of forced expiration
• FVC = Forced Vital Capacity– Maximum volume of air exhaled with forced expiration
after a maximum inhalation• FEF25-75 = Forced Expiratory Flow between 25%
and 75% of FVC– Detects small-airways obstruction

Reversible airway obstruction
http://www.sbpt.org.br/downloads/arquivos/Dir_Asma_Int/Practical_Guide_Diagnosis_Management_Asthma_NIH_2002.pdf

Council of State and Territorial Epidemiologists
Asthma Surveillance Case Definition Work Group

Mortality/Hospitalization Case Definition
Confirmed: · No confirmed case classification for mortality and hospital discharge data.
Probable: · death certificates/records listing the asthma diagnostic code (ICD-9 Code: 493; or ICD-10 Codes: J45, J46) as the underlying cause of death.· hospital records listing the asthma diagnostic code (ICD-9-CM Codes: 493.0- 493.9;ICD-10-CM Codes: J45.0-J45.9) as the primary diagnosis.
Possible:· death certificates/records listing the asthma diagnostic code as a contributing cause of death.· hospital records listing the asthma diagnostic code as a secondary diagnosis. · 466(acute bronchitis and bronchiolitis), *** in children < 12 years***· 491.20 and 491.21 (chronic bronchitis), *** in children < 12 years***

Prevalent Case Definition
Confirmed: · There is no confirmed case classification for self-report.
Probable: · A positive response:
“Did a doctor (or other health professional) ever tell you that you had asthma?” and “Do you still have asthma?” OR “Have you taken prescription medications for asthma (such as albuterol, inhaled steroids, cromolyn, theophylline, etc) during the past year?” OR “Have you had a wheeze episode in the past year?”
Possible: · A positive response
“Have you used over-the-counter medications for asthma during the past year?”, OR
“Have you experienced episodes of wheezing during the past year?

Clinical and functional criteria
• Clinical criteria– Wheezing 2 consecutive days– Chronic cough persisting 3-6 weeks responding to
bronchodilators in absence of allergic rhinitis or sinusitis
– Nocturnal awakening with dyspnea, cough/wheezing (w/o other medical condition)
• Laboratory criteria – Spirometry (FEV1, FVC)– 12% > short-acting bronchodilator challenge– 20% FEV1 w/histamine/methacholine/exercise/cold– 20% diurnal variation in PEF over 1-2 weeks

Clinical and functional case definitionsConfirmed: any of the clinical symptoms at least 3 times during the past
year AND at least one of the laboratory criteria.
Probable: In the absence of supporting · laboratory criteria, presence of any of the clinical symptoms which have been reversed by physician treatment with asthma medications and have occurred at least 3 times during the past year.· clinical criteria, at least one of the laboratory criteria during the past year.· laboratory or clinical criteria, taken medications in the past year that were prescribed by a physician for asthma.
Possible: the presence of any of the following during the past year:· shortness of breath on exertion, presence of wheezing or chronic cough in the absence of obvious respiratory infection, presence of increased nasal secretion, mucosal swelling, nasal polyps, or chronic sinusitis, hyper expansion of the thorax, sounds of wheezing during normal breathing, prolonged phase of forced exhalation, chest x ray showing hyper expansion, FEV1 less than 80% of predicted value

Asthma Case Definition Epidemiologic Issues
• Overlap with other COPD’s• Partially a diagnosis of exclusion• Different etiologies?• Continuum of symptoms?• More difficult to diagnose in young children• Symptoms & lung function change over time,
related to environmental triggers, medication, and age
• Definitions based on self-report or medical records depend on physician diagnosis– Diagnostic criteria not standardized

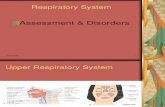
Pathogenesis of Asthma:IgE-mediated Inflammation
Allergen
IgE Antibodies
Activate Inflammatory Cells Mast cells Lymphocytes Eosinophils Platelets Macrophages
Inflammatory Mediators Released Histamine Leukotrines Cytokines
Early Response Bronchospasm Edema Airflow Obstruction
Late Response Airway Inflammation Airflow Obstruction Airway Hyperresponsiveness Remodelling
Adapted from Busse WW, Lemanske RF NEJM 2001;344


Asthma Risk Factors
• Genetic– Atopy : IgE-mediated response to common
environmental allergens• Strong genetic component• 50% of asthma attributable to atopy
– Family history of asthma• Environmental
– House dust mites, cat dander – Environmental tobacco smoke in pre-school children– Ambient air pollution (RR<2)– Fungi– Cockroaches

Primary Prevention?:Clinical Trials in High-Risk Infants
• Prenatal intervention (allergen avoidance) in infants from birth through one year of age with first-degree relatives who have diagnosed asthma(Chan-Yeung et al. Archives of Ped Adol Med
2000;54:667-63)• Primary prevention of asthma and atopy during
childhood by allergen avoidance in infancy (birth through age 8 years)(Arshad et al. Thorax 2003;58:489-93)

Primary Prevention?:Hygiene Hypothesis
• Newborn immune system skewed to type 2 T-helper cell type (Th2)
• Need timely and appropriate environmental stimuli to create balanced immune response– Th1: cellular defense, autoimmune diseases
• Viral & bacterial infections, older siblings, early day care, rural environments
– Th2: humoral defense, allergies, IgE• Antibiotics, parasites, house-dust mites, cockroaches, urban
environment, diet• Vaccination, antibiotics, hygiene, fewer siblings
=> Skewed to Th2 => increased atopy / asthma

Risk Factors for Asthma Exacerbations
• Biologic– Causal: cat, cockroach, house dust mite, pollens– Associated: dog, fungi/molds, rhinovirus– Suggestive: domestic birds, respiratory infections
• Chemical– Causal: environmental tobacco smoke (pre-school)– Associated: pollutants– Suggestive: ETS (older children, adults),
formaldehyde, fragrances• Other
– Exercise, cold air
IOM 2000, Clearing the Air: Asthma and Indoor Air Exposures

Environmental Epidemiology• Indoor environment (Chapman, NHANES)
– Self-report of smokers in family, use of gas stove, having a dog or cat
• Occupational airborne exposure (Bakke)– Self-report on survey of past or present dust or gas
exposure– Imputation based on occupational titles
• Low-level ozone – Gent et al. JAMA 2003– Longitudinal study of asthma exacerbations– Hourly ozone concentrations from monitoring sites– Asthmatic children vulnerable to ozone at levels
below current EPA air quality standards

Source: CDC. Surveillance for asthma – United States, 1980-2004. MMWR 2007;56(SS-08)

Source: CDC. Surveillance for asthma – United States, 1980-2004. MMWR 2007;56(SS-08)

Source: CDC. Surveillance for asthma – United States, 1980-2004. MMWR 2007;56(SS-08)


Source: CDC. Surveillance for asthma – United States, 1980-2004. MMWR 2007;56(SS-08)

Source: CDC. Surveillance for asthma – United States, 1980-2004. MMWR 2007;56(SS-08)


Societal Impact of Asthma
Source: CDC. Surveillance for asthma – United States, 1980-1999. MMWR 2002;51(SS-01)
• In 1998, the cost of asthma to the U.S. economy was estimated to be $12.7 billion

Primary Prevention?:NIH RFA 2003
• Hypothesis: early life changes in immune function induced by environmental factors determine likelihood of developing asthma– Early cellular/molecular markers of asthma
onset– Effect of timing, dose and route of antigen
exposure on asthma susceptibility– Effects of maternal & environmental asthma
risk factors on immune function early in life– Etc.

Secondary Prevention of Asthma: • Expert Panel Report 2: Guidelines for the Diagnosis and
Management of Asthma (NHLBI 1997, 2002)– Stepwise approach based on symptom severity
• Quick-acting bronchodilator (e.g. ß-agonists)• Prophylactic anti-inflammatory (e.g., steroids)
– Control factors contributing to asthma severity• Avoid triggers (allergens, tobacco smoke, • Annual influenza vaccination with persistent asthma
– Assessment and monitoring– Patient involvement– written plan for self-management, PEF monitoring
• Environmental controls (e.g. reduced air pollution – see Gent et al.)• What proportion of medically-attended asthma-related exacerbations
are preventable through proper management?• How does access to and quality of asthma management vary by
region, socioeconomic status, and race/ethnicity?