
Asthma Champions Webinar OACHC final - cdn.ymaws.com fileWe integrated elements of the original...
46
GOOD Afternoon! 1
Transcript of Asthma Champions Webinar OACHC final - cdn.ymaws.com fileWe integrated elements of the original...

GOOD Afternoon!
1

NO disclosures
2

3

With effective outpatient care, most asthma related hospital and emergency department episodes are preventable2
2 National Heart, Lung and Blood Institute, 2007
4

Have you ever been told you have asthma? Do you still have asthma?
5

6

7
8

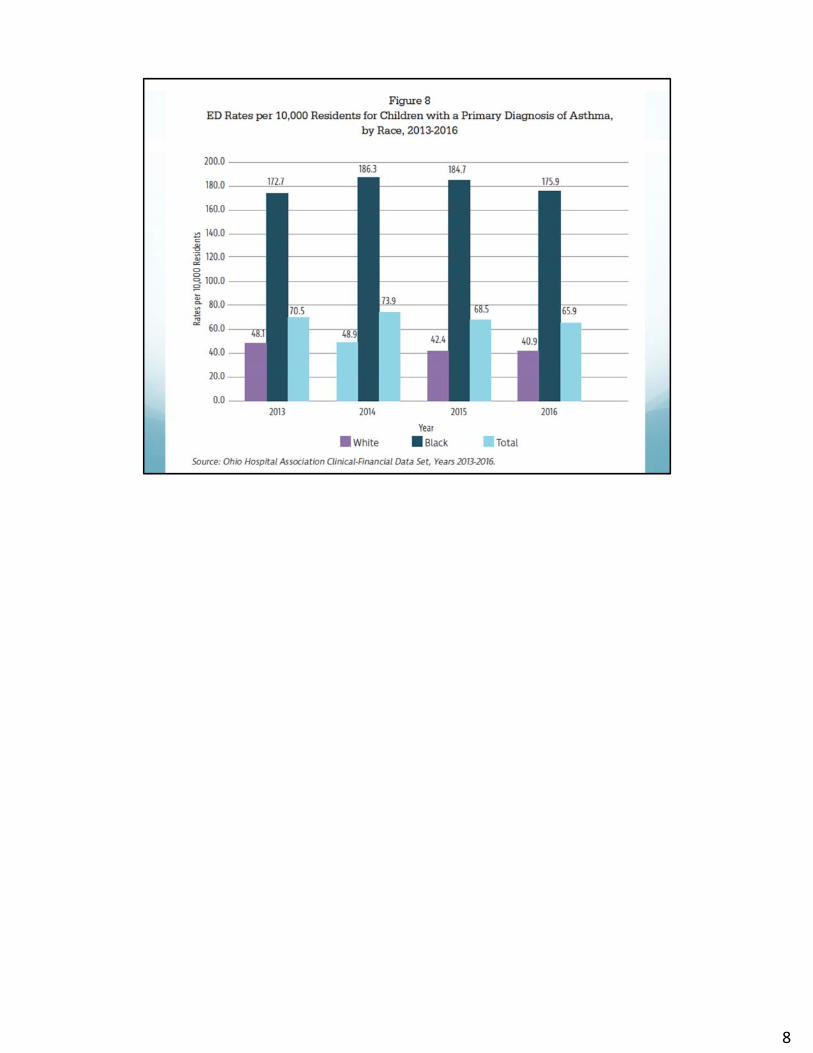
Recent report from the Ohio Hospital Association provides data for 2016 using the ICD‐10 definition of asthma will serve as the baseline going forward. The data shows changes in ICD 9 (2014) to ICD 10 coding (2016) contributed shows a 60% lower hospitalization rate and a 15% lower emergency department visit rate
The International Classification of Diseases, Tenth Revision, Clinical Modification (ICD‐10) is a morbidity classificationpublished by the United States for classifying diagnoses and reason for visits in all health care settings. This document isthe statistical classification of disease published by the World Health Organization (WHO). Deaths have been coded usingthese asthma diagnostic codes (ICD‐10 Codes: J45, J46) as the underlying causes of death since 1999. However, a clinicalmodification of the classification for morbidity purposes has been developed by the National Center for Health Statistics(NCHS), the federal agency responsible for use of the International Statistical Classification of Diseases and Related HealthProblems, 10th revision (ICD‐10) in the United States (National Center for Health Statistics, 2017).
9

10

https://www.nhlbi.nih.gov/files/docs/guidelines/asthma_qrg.pdf
11

12

Why Asthma?It is the most common chronic illness in children. Our patient population, students in Cincinnati Public Schools have a higher than national average prevalence of asthma. Across our 10 participating sites there were over 1500 asthma students with an average prevalence rate of 17%. Our patients are at higher risk for poorly controlled asthma due to health care disparities, social determinants of health high prevalence of poverty, most of our sites have Free/reduced lunch rates of near 100%!
13

Background for our project:Beginning in late 2015, the Cincinnati Health Dept. partnered with Xavier University School of Nursing in a HRSA Grant to promote Interprofessional Collaborative Practice (IPCP). The Asthma CHAMPIONS project began in May of 2017
The purpose of the grant is to promote and enhance Interprofessional Collaborative Practice.
Our asthma project is the largest multi‐site endeavor utilizing this grant support to date – a GRAND FINALE to our learning with IPCP teams!
14

The Asthma CHAMPIONS team was comprised of: nurse practitioners, nurses, medical assistants, casework associates, home health nurses, pharmacist, health educator, and a registered sanitarian. This project was designed to engage all these professionals in optimizing our asthma care.
We additionally partnered with Spirometry 360, American Lung Association, Thermo Fischer Scientific and ndd Medical Technologies.
15

The team created a hybrid program recognizing our unique situation – as a Primary Care Clinic located in a School!! Our framework was based on CHAMPS. CHAMPS is the acronym for Community Healthcare for Asthma Management and Prevention of Symptoms which is a family‐centered, patient‐tailored, evidence‐based, pediatric asthma intervention.
The CHAMPS intervention includes asthma counseling and in‐home mitigation of environmental triggers for children with poorly‐controlled or moderate‐to‐severe asthma in primary care settings.
The CHAMPS intervention is effective for – and can be tailored to fit – any practice or patient population where pediatric asthma is common.
16

>1500 students in CPS schools with 10 participating SBHCs are recorded as having asthma, classifications ranging from intermittent – severe persistent asthma.
We integrated elements of the original CHAMPS program with our current asthma care tools i.e. ACT vs. CHAMPS ‐ ASTHMA SYMPTOMS & UTILIZATIONKeeping CHAMPS forms for CHILD ASTHMA RISK ASSESSMENT TOOL (CARAT) and HOME ENVIRONMENT OBSERVATION used by Home Health RN.Patients for home visit were triaged by asthma control status/HX, allergy test results and OK from family to visit Based on school health records there were >1500 students in CPS schools at our 10 participating SBHCs recorded as having asthma, classifications ranging from intermittent severe persistent asthma.PowerSchool data reveals that:• 40% are classified as intermittent (As of 6/18/18 41% if rounded up)• 29% in persistent range – mild severe (As of 6/18/18 32%)• 31% are currently un‐classified (As of 6/18/18 27% if rounded up)We expect to see a shift in classification with implementation of spirometry as an additional tool in asthma assessment and management. It was most likely more students would be classified in the persistent range.Prevalence rates vary between sites which we hope to learn and understand more about ‐ if this is a true variance or due to record discrepancies.
17

Our Nurse Practitioners, RNs, and MAs are participated in an online spirometry training program – Spirometry 360 from the University of Washington to learn “how‐to” perform quality spirometry and interpret the results. The program also provides feedback on completed spirometry reports as an integral part of our learning.
I worked with our Home Health Department to assemble an asthma visit kit that included the Home Environmental Risk Assessment and CARAT (Child Asthma Risk Assessment Tool). One of our Health Educators on the Team is also a Sanitarian and was available accompany the Home Health Nurse for the first few visits until the nurse is comfortable with the environmental assessment. She also provided in‐service training for Home Health staff.We initially thought that our Home Health Nurses would be able to make up to 4 visits to the home for initial assessment and follow‐up. We anticipated that adding the home visit will be helpful in engaging families and providing vital information to our providers. Due to the size of our Home Health Dept., patients were selected for a home visit through a triage process based on asthma control status/HX, allergy test results and finally an OK from the family to visit. As a “side effect” of this work we hoped to find evidence and support to adding additional Home Health nurses and Community Health Workers!
We have been working with our Cincinnati branch of the American Lung Association for education materials. The ALA Health Educator provided our School Nurses an Asthma Basics presentation to cover the most current asthma information. We planned to utilize the ALA’s Open Airway curriculum at our Elementary sites and continue to look for the best options for adolescent format – perhaps using the ALA’s Asthma 101 program. We were supportive of each site’s unique staffing and populations and their determination of what might work best for them. We hoped to provide options and resources that could work in any situation.
We have also formed a partnership with the regional representative from Thermo‐Fisher Scientific, the maker of equipment and assays for Immunocap allergy testing. He worked with us to bring additional resources and support to the project.
We continued to pursue establishing connections with our Medicaid Managed Care Organizations to see what support they might be able to offer – especially for allergen reduction items such as pillow and mattress covers.
17

18
The quadruple aim helped shape our outcome goals.To improve clinical outcomes & lower costs as evidenced by:• reduced # of ER/hospital stays• Improved ACT scores
We applied all project innovations to all patients seen but narrowed our detailed study to 100 randomly selected patients (about 10 per site).Selection was based on ACT scores < 20 in the first 6 weeks of the school year.
How the quadruple aim has helped shape our desired outcome goals:Improve patient/family satisfaction
Improve patient clinical outcomes
Decrease healthcare costs
Improved team satisfaction
To achieve Clinical outcomes of: • reduced ER/hospital stays• Improved ACT scoresBy implementing comprehensive asthma care

Our plan meant that we would provide comprehensive asthma care by adding spirometry, allergy testing and home visits to our current care model. We added objective measures to better manage our patients’ asthma – putting pieces of the care puzzle together! We offered this model of care to all of our consented SBHC asthma patients.
19

For data purposes we randomly selected approx. 10 patients from each site for “deeper dive” into data = “select 100”Aggregate data was obtained from all sites = “Big Ten”
19

LOW ACT SCORES: Our goal was to reduce the # of students with sub‐optimal asthma control and follow them with NP and RN visits until stable.
Results from the “Select 100” patientsWe “Lost” 10 – they were not seen again for their asthma during the school year.We were able to decrease our # of low ACTs• From 34 to 5 for younger students• From 66 to 13 for students ages 12‐18
In total:
72 of 90 had ACT scores >20 by May!
20

3,865 Asthma visits were completed at the 10 sites!!!! This was 502 more visits than the previous school year. All 10 sites increased the # of asthma visits.
About our Aim to reduce the # of ER/HOSPITAL ADMISSIONS: Out of the “Select 100” at Baseline 10 had documented ER/Hospital stays by the end of year there were only 3! From ALL sites there were 21 fewer reported ER/Hospital stays.
21

SPIROMETRY TESTING: guidelines recommend any student 6 yrs or older with asthma have spirometry annually. What is it? = Objective measure of lung function which can assist in determining severity and control
Why use it? • Up to 1/3 of patients with mild or severe asthma are identified
by spirometry who would be missed by history alone.• Patients’ perceptions of obstruction are notoriously inaccurate.• Significant obstruction can be present even when the chest is
clear on physical examination.• Spirometry can demonstrate obstruction and assess
reversibility in patients 5 years of age or older. • Diagnosis of Asthma because the medical history and physical
examination are not reliable means of excluding other diagnoses or of assessing lung status.
22

• Establishing asthma severity and control levels:
22

THANKS to Dr. James Stout @ University of Washington for sharing these slides
23

The foundation of asthma care Establishing asthma severity and control levels: Assessing Asthma Severity utilizing Lung Function
Based on age and
• Impairment (frequency/intensity of symptoms, lung function, functional
limitations over past 2‐4 weeks)
• Risk (exacerbations over the past year)
Levels of severity:
• Intermittent
• Persistent/Mild
• Persistent/Moderate
• Persistent/Severe
24

Assessing Asthma Control
Control looks at severity metrics over time, once treatment is initiated. Based on:
• Impairment (frequency/intensity of symptoms, lung function, functional limitations over past 2‐4 weeks, questionnaire, e.g., Asthma Control Test)
• Risk (exacerbations requiring oral systemic corticosteroids, reduced lung growth, adverse effects of meds)
Levels of control:
• Well Controlled
• Not Well Controlled
• Very Poorly Controlled
25

26
NCICAS = National Cooperative Inner‐City Asthma StudyJ Allergy Clin Immunol. 1999 Mar;103(3 Pt 1):501-6.Results of the National Cooperative Inner-City Asthma Study (NCICAS) environmental intervention to reduce cockroach allergen exposure in inner-city homes.Gergen PJ1, Mortimer KM, Eggleston PA, Rosenstreich D, Mitchell H, OwnbyD, Kattan M, Baker D, Wright EC, Slavin R, Malveaux F.
ICAS = Inner-City Asthma StudyInner City Asthma Study: Relationships among sensitivity, allergen exposure, and asthma morbidityGruchalla, Rebecca S. et al.Journal of Allergy and Clinical Immunology , Volume 115 , Issue 3 , 478 - 485

27
Conclusions:1. Using FEV1 in addition to symptom
frequency, one‐third of participants were reclassified into higher severity categories.
2. In certain populations, under‐use of spirometry may have direct implications for the under‐treatment of asthma.

Only 5 sites had spirometers before the 2017‐2018 school year – in the prior school year 51 tests were done across those 5 sites.
By the end of 2017‐2018 school year 760 tests were
completed!With the online spirometry training and 5 months of feedback reports we were able to build confidence in our coaching and results interpretation. We continue to monitor our use of spirometry – YTD (AUG FEB) = 484 test
28

Prior to CHAMPIONS NO allergy testing was being done. For our 10 sites, we chose to use ImunoCAP Specific IgEblood test for Area V respiratory allergens common to the Southwest Ohio region: dust mites, mold, cockroaches, dog and cat dander, mouse, grasses, trees, and weeds
29

At our SBHCS, we use: ImmunoCap blood test for respiratory allergens
Done in officeTests for environmental allergens common to the Southwest Ohio region: dust mites, mold, cockroaches, dog and cat dander, mouse, grasses, trees, and weedsNo need to be off antihistamines prior to testingNo test preparation neededSingle blood draw vs. multiple skin prick testNo potential for uncomfortable allergic reaction to testing
Our goal: was to test patients with persistent asthma
30

What it means for an individualA study by Morgan et al. in the New England Journal of Medicine looked at the impact of targeted exposure reduction. The study examined over 900 inner-city children with asthma and allergies, identified their allergic triggers, and reduced the exposure to these triggers only in their bedrooms. The targeted exposure reduction led to fewer symptom days, fewer missed school days, and fewer trips to the emergency department or unscheduled doctor’s office visits. By including this component of the guidelines into asthma management, patients can experience improvement in their chronic condition.
21.3 symptom free days = 3 week vacation from their symptoms/chronic condition4.4 missed school = 1 week = better attendance2 fewer Urgent/ER visits
31

16 year old male student with Severe Persistent Asthma. He has low Asthma Action Scores with asthma exacerbations in the spring and fall. He has had 3 reported visits to the emergency department for asthma in the past year. He gets allergic rhinitis and asthma problems during the spring and fall. He also has a history of atopic dermatitis.
Asthma medications include: Singulair 10 mg daily, Dulera 200‐5 mcg 2 puffs 2 times a day, and albuterol rescue inhaler 2 puffs every 4 hours as neededAllergy medications include: cetirizine 10 mg daily and flonase 1 puff per nostril dailyPatient reports his allergies are trees, dogs, cats, grass but has never been tested for these allergies
32

Remember – results are individualized cannot compare one patient’s result for an allergen to another’s, rather the largest number for an allergen result for a patient is their “worst”
Dermatophagoides farinae, Dermatophagoides pteronyssinus, and Euroglyphusmaynei
33

Allergies add up and eventually reach a threshold where symptoms start – by reducing exposure to as many allergens/triggers as possible, symptoms are reduced.
Allergen 3 “seasonal allergen” – patient already has elevated level of allergen exposure, so when the seasonal allergen hits, patient goes above his/her symptom threshold and can experience allergy symptoms and exacerbation of asthma. By reducing exposure to all with bed coverings, keeping cat out of BR, and avoiding high pollen days, etc.
Other important thing to note…we can also decrease medications a patient uses if we find out allergies are NOT the cause of their symptoms/exacerbations! (yay!)
34

• 224 tests were completed. • Covered by all Medicaid HMOs , CHD had a
negotiated price with LabCorps for uninsuredpatients.
Challenges were:• Initial provider hesitancy due to perceived high cost• Difficulty contacting parent to OK blood draw
Late in the school year we enlisted additional support for calling parents, still struggling to have providers order.
35

Asthma Education ‐We emphasized key educational messages: to teach and reinforce at every opportunity :Basic Facts About Asthma ■ Role of inflammation. ■What happens to the airways during an asthma attack. Understanding the Difference Between: ■ Long‐term control medications: and Quick‐relief medications■ Inhaler technique ■ Identifying and avoiding environmental exposures ■ Self‐monitoring symptoms■ Recognize early signs and symptoms of worsening asthma. ■ Using a written asthma action plan■ Seeking medical care as appropriate
36

HOME HEALTH REFERRAL: any student with + household allergens was a candidate for a home visit which included an environmental observation. Also eligible were students with poorly controlled asthma regardless of allergies.
Lessons learned ‐ just because we had plenty of candidates for a home visit didn’t mean it actually happened.• Most frequently a parent declined our initial offer • OR a parent expressed an interest and Oked the visit, then declined when Home Health called to schedule
• OR parent scheduled a visit BUT “No show/not home”
For the 9 that received a home visit – it was very helpful to family and care team with Home Health nurse as the bridge from home to school.
37

Lessons LearnedProvide training• Spirometry 360 training for coaching and interpretation provided
CEUs for completion• Training from partners at Thermo Fischer Scientific on allergy testing,
interpreting results• Asthma refresher/review by American Lung Association Educator
Provide equipment• Spirometer provided to each site• Appropriate lab equipment was obtained
Provide resources and support• Resource Manual for each site with lists of resources, expanded
information on allergy testing, home health referral process, EPIC efficiencies and screenshots of documentation
• Site visits to offer hands‐ on support • Support for Sites‐ based on monthly data/report review
38

• Cheerleader and site CHAMPION
38

We Learned …. IT TOOK TIME• It took 4 months to have all teams complete online spirometry training
• To develop confidence in doing spirometry both coaching and interpreting
• Improve communication with family and obtain OK for allergy testing• Developing best communication methods between facilitators and care teams
LEARNED TO UTILIZE TEAM SKILLS • Available experienced team members – NP and MA with extensive
prior experience in spirometry• Early adopters and promoters• Feedback reports reviewed to help improve test quality
DELAYED DUE TO “NOT ENOUGH TIME”• Open Airways education as group visit for first year • School Staff and coach asthma education• Asthma Friendly school assessment
39

THANK YOU!!!!TO all the SBHC Teams for working so
hard to provide ComprehensiveAsthma Care!!
&Xavier University for the opportunity
40

41

42


















