Asthivikara ss-mys
216
I “CONCEPT OF ASTHI PRADOSHAJA VIKARAS W.S.R TO MANAGEMENT OF SANDHIGATAVATA” By DR. RANJITH KUMAR SHETTY, B.A.M.S. Dissertation submitted to the Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore. In the partial fulfillment of the requirements for the degree of DOCTOR OF MEDICINE (AYURVEDA) in AYURVEDA SIDDHANTA Under The Guidance of Dr. N.ANJANEYA MURTHY M.D. (Ayu) Professor, Department of Post-Graduate Studies in Ayurveda Siddhanta, G.A.M.C., Mysore. Co-Guide DR.VASUDEV A. CHATE , M.D. (Ayu) Lecturer, Department of Post-Graduate Studies in Ayurveda Siddhanta GAMC Mysore – 570021 & DR.KIRAN KALAIH , M.S. (Ortho) Professor and Orthopedic surgeon, Mysore Medical College and Research center, Mysore – 570021 DEPARTMENT OF POST GRADUATE STUDIES IN AYURVEDA SIDDHANTA, GOVERNMENT AYURVEDA MEDICAL COLLEGE, MYSORE. 2010
-
date post
19-Oct-2014 -
Category
Health & Medicine
-
view
3.738 -
download
20
description
RANJITH KUMAR SHETTY, CONCEPT OF ASTHI PRADOSHAJA VIKARAS W.S.R TO MANAGEMENT OF SANDHIGATAVATA, DEPARTMENT OF POST GRADUATE STUDIES IN AYURVEDA SIDDHANTA, GOVERNMENT AYURVEDA MEDICAL COLLEGE, MYSORE. 2010
Transcript of Asthivikara ss-mys
I
“CONCEPT OF ASTHI PRADOSHAJA VIKARAS W.S.R TO
MANAGEMENT OF SANDHIGATAVATA”
By
DR. RANJITH KUMAR SHETTY, B.A.M.S.
Dissertation submitted to the Rajiv Gandhi University of Health Sciences,
Karnataka, Bangalore.
In the partial fulfillment of the requirements for the degree of
DOCTOR OF MEDICINE (AYURVEDA)
in
AYURVEDA SIDDHANTA
Under The Guidance of
Dr. N.ANJANEYA MURTHY M.D. (Ayu)
Professor, Department of Post-Graduate Studies in Ayurveda Siddhanta,
G.A.M.C., Mysore.
Co-Guide DR.VASUDEV A. CHATE, M.D. (Ayu)
Lecturer, Department of Post-Graduate Studies in Ayurveda Siddhanta
GAMC Mysore – 570021 &
DR.KIRAN KALAIH, M.S. (Ortho)
Professor and Orthopedic surgeon, Mysore Medical College and Research center,
Mysore – 570021
DEPARTMENT OF POST GRADUATE STUDIES IN AYURVEDA SIDDHANTA,
GOVERNMENT AYURVEDA MEDICAL COLLEGE,
MYSORE.
2010
Ayurmitra
TAyComprehended
II
III
IV

V

VI

VII
VIII
ACKNOWLEDGEMENT
I bow to the sacred feet of Almighty, without the blessings of whom this study would
not have been completed.
I sincerely express my indebtedness and profound gratitude to my Guide
Dr. N. Anjaneya Murthy, Professor, Department of PG Studies in Ayurveda
Siddhanta, Government Ayurveda Medical College, Mysore for his valuable guidance
& encouragement throughout my study.
I sincerely acknowledge my reverend teacher and Co- guide Dr.Vasudev A Chate,
Lecturer, Department of PG Studies in Ayurveda Siddhanta, Government Ayurveda
Medical College, Mysore and another Co-guide Dr.Kiran Kalaih, Professor &
Orthopedic surgeon, Mysore Medical College and Research center, Mysore for his
valuable guidance and support throughout my study.
I am highly thankful to Dr. K.Naseema Akhtar, Professor and HOD, Department of
PG Studies in Ayurveda Siddhanta, Government Ayurveda Medical College, Mysore,
for her constant support and encouragement at every stage of this study.
I am highly thankful to Late. Dr.G.N.Shakuntala, Former HOD, Department of PG
Studies in Ayurveda Siddhanta, Government Ayurveda Medical College, Mysore, for
her constant guidance, continuous supervision and help at every stage of this study.
I am grateful to Principal Dr.Ashok D.Satpute, Principal, Government Ayurveda
Medical College, and Mysore for his support and encouragement.
I owe my deep sense of gratitude to all my teachers Dr.T.D.Ksheera Sagar,
Dr.H.M.Chandramouli, Dr.G.Gopinath, Dr.Shantaram, Dr.Rajendra, Dr.T.R.Shantala
Priyadarshini, Dr.Shrivathsa, Dr.Mythrey, Dr. Anand Katti, Dr.Ananth Desai, Dr.
Nalini, Dr.Adarsh and all other teachers for their support in this study.
I am thankful to physician Dr.Anuradha Nadakarni and all other hospital staffs for
their help during the course of study.
IX
I owe my special thanks to my classmates and friends Dr.Kalyani, Dr.Geetha,
Dr.Ramesh and Dr.Kavitha for their comments, cooperation and timely advises, they
stood beside and inspired me through out the completion of this study.
I thank my younger colleagues Dr. Athika Jan, Dr. Aravind B.S, Dr.Pallavi G,
Dr.Rekha A.R Dr.Preetha and Dr.Arhanth for their help and support throughout my
work.
I am thankful to my senior colleagues Dr.Savitha Shenoy, Dr.Soubhagya, Dr.Kedar
Sharma, Dr. Vijayalakshmi, Dr.Yogesh, Dr.Aparna, Dr.Annapoorani, Dr.Pankaj
Pathak and Dr.Rajesh Bhat for their help.
I acknowledge my special thanks to my friend Dr.Kiran Kumar Agadi, for his support
and encouragement throughout my study.
I am thankful to my colleagues Dr.Vyasaraj Tantry, Dr.Parveen, Dr.Pallavi,
Dr.Ranjani, Dr.Ananthshayan, Dr.Sameena and to my younger colleagues Dr.Mahesh,
Dr.Adhitya, Dr.Sowmya, Dr.Shubharani, Dr.Geetha and Dr.Sridharmurthy,
Department of P.G.studies in Kayachikitsa, for their help.
I wish to place my sincere gratitude to my friends Dr.Rajaram, Dr.Ravi, Dr.Sowmya
M.D and Dr.Sharif for their support.
I also owe my heart felt gratitude to my teacher Dr.Hariprasad Shetty and all other
teachers of under graduation who initiated and instilled in me the knowledge of this
holy science.
This acknowledgement would not be complete without paying obeisance to my
parents Mr. Ramayya Shetty and Late. Jyothi R Shetty. Their constant
encouragement and guidance propelled me to achieve my goal.
I convey my special thanks enveloped with affection to my beloved younger sisters
Ms.Rajani Kumari and Ms.Nisha Shetty and younger brother Mr. Vignesh Shetty
for their valuable timely help and support.
I wish to convey my thanks to U.G. and PG Librarian Mrs Varalakshmi and Mr
Somasundar for providing library facilities.

X
I thank Dr.Lancy D’souza for his valuable help and guidance in the statistical
analysis and interpretations.
I convey my heartfelt thanks to Manager, M/s SDM Ayurveda Pharmacy , Kuthpady
Udupi who helped me in procuring drugs for my dissertation.
I thank Mr.Mahesh C, Maneesh printers Mysore, for bringing this work in a
documented form.
Last but not the least, I express my thanks to all my patients , without whom I
wouldn’t have completed this dissertation and I thank all those who helped me
directly or indirectly in my studies with apologies for my inability to identify and
thank them individually.
Date:
Place: Mysore Dr. Ranjith Kumar Shetty
XI
LIST OF ABBREVATIONS
A.H: Ashtanga Hrudaya
A.K: Amara Kosha
A.S: Ashtanga Sangraha
B.P:Bhava Prakasha
B.S: Bhela Samhita
C.D: Chakradatta
C.S: Charaka Samhita
H.S: Harita Samhita
M.N: Madhava Nidana
S.K.D: Shabda kalpa Druma
S.S: Sushruta Samhita
Sha.Sa: Sharangdhara Samhita
Y.R: Yoga Ratnakara

XII
ABSTRACT
Background of the Study
Asthi pradoshaja vikara is a condition in which Asthi gets vitiated extremely
by the doshas and changes its natural form and leads to many disorders like adhyasthi
adhidanta etc. Classical texts mention that tikta ksheera sarpi is the best line of
treatment for Asthi pradoshaja vikaras. Sandhi mainly constitutes Asthi. Hence this
research is undertaken to study the concept of Asthi pradoshaja vikaras and to
evaluate the efficacy of tikta ksheera sarpi in Janusandhigatavata.
Objectives of the study
To review in detail about Asthi and Asthi pradoshaja vikaras.
To assess the involvement of Asthi with the help of radiology (x-ray).
To assess the role of Asthi in manifestation of sandhigatavata.
To study the role of tiktaka dravyas in the management of sandhigatavata.
Method
A Comparative Single Blind Clinical Study was conducted with pre and post
design. Patients of janusandhigatavata were categorised into two groups namely
Group A and Group B, consisting of 15 patients each.
Intervention
The intervention of clinical study was carried according to the individual group as
mentioned below.
Group-A
Trikatu churna was administered for ama pachana.
After attaining niramavastha patients were subjected to abhyanga with
ksheerabala taila followed by nadi sweda.
XIII
The sequence of 15 bastis in the form of kala basti was administered starting from
anuvasana with panchatikta ghrita (total 9 anuvasana bastis) and niruha basti with
panchatikta ksheera sarpi (total 6 niruha bastis) .
Group-B
Trikatu churna was administered for ama pachana.
After attaining niramavastha patients were subjected to abhyanga with
ksheerabala taila followed by nadi sweda.
The sequence of 15 bastis in the form of kala basti was administered starting from
anuvasana with bala ghrita (total 9 anuvasana bastis) and niruha basti with bala
sadhita ksheera sarpi (total 6 niruha bastis) .
Results
All the patients considered for the study showed improvement in both the
groups, which is statistically significant. But comparatively Group A showed good
result clinically when compared to Group B.
Interpretation and Conclusion
Based on both the literary and clinical aspects of the study, Janusandhigatavata
was considered under Asthi pradoshaja vikaras.
Group A showed good result with statistical significance ( p value 0.042 )
compared to Group B with no statistical significance ( p value 0.819).
Keywords Asthi pradoshaja vikaras
Janusandhigatavata
Kala basti
Panchatikta ghrita
Bala ghrita

XIV
CONTENTS
Sl. No Particular Page No.
1. Introduction 1-2
2. Objectives 3
3. Review of literature
4. Review on Asthi Pradoshaja vikaras 4-42
5. Review on Sandhigatavata 43-64
6. Review on Basti 65-72
7. Drug review 73-79
8. Materials and methods 80-94
9. Observation and results 95-130
10. Discussion 131-162
11. Conclusion
Recommendations for further study
163-164
12. Summary 165-166
13. Bibliographic reference 167-184
14 Annexure I-XI
XV
List of Tables
Table No
Particular Page No.
1 Showing the Paryayas of Asthi 6
2 Showing the Panchabhoutika sanghatana of Asthi 7
3 Showing the Sroto mulas of Asthi 8
4 Showing the Numbers of Asthi 8
5 Showing the Types of Asthi 9
6 Showing the Malas of Asthi 10
7 Showing the Vruddhi lakshanas of Asthi 11
8 Showing the Kshaya lakshanas of Asthi 12
9 Showing the different Asthi pradoshaja vikaras 14
10 Showing the Nidanas for Janusandhigatavata 45
11 Showing the Lakshanas of Janusandhigatavata 49
12 Showing the Saapeksha nidanas for Janusandhigatavata 51
13 Showing the Chikitsa for Janusandhigatavata 53
14 Showing Differential diagnosis of Knee osteoarthritis 61
15 Showing Differential diagnosis of Knee osteoarthritis 62
16 Showing the Properties of Trikatu 73
17 Showing the Properties of Panchatikta & Bala 74
18 Showing distribution of patients according to Age 95
19 Showing distribution of patients according to Sex 96
20 Showing distribution of patients according to Marital status 96
21 Showing distribution of patients according to Education 96
22 Showing distribution of patients according to Religion 97
23 Showing distribution of patients according to Socio-economic status
97
XVI
24 Showing distribution of patients according to Occupation 98
25 Showing distribution of patients according to Habitat 98
26 Shows distribution of patients according to Diet 99
27 Showing distribution of patients according to Prakruti 99
28 Showing distribution of patients according to Samhanana 100
29 Showing distribution of patients according to Pramana 100
30 Showing distribution of patients according to Sattva 100
31 Showing distribution of patients according to Koshtha 101
32 Showing distribution of patients according to Agni 101
33 Showing distribution of patients according to Bala 102
34 Showing distribution of patients according to Vyayama 102
35 Showing distribution of patients according to Joint involvement 103
36 Showing results of Joint pain ( Rt Knee ) 112
37 Showing Systemic measures in Joint pain (Rt Knee)
113
38 Showing results of Joint pain ( Lt knee ) 114
39 Showing Systemic measures in Joint pain (Lt Knee) 114
40 Showing results of Joint stiffness ( Rt knee ) 115
41 Showing Systemic measures in Joint stiffness (Rt Knee) 116
42 Showing results of Joint stiffness ( Lt knee ) 117
43 Showing Systemic measures in Joint stiffness ( Lt knee ) 117
44 Showing results of Joint swelling ( Rt knee ) 118
45 Showing Systemic measures in Joint swelling ( Rt knee ) 119
46 Showing results of Joint swelling ( Lt knee ) 120
47 Showing Systemic measures in Joint swelling ( Lt knee ) 120
48 Showing results of Joint crepitus ( Rt knee ) 121
49 Showing Systemic measures in Joint crepitus ( Rt knee ) 121
50 Showing results of Joint crepitus (Lt Knee) 122
XVII
51 Showing Systemic measures in Joint crepitus (Lt Knee) 123
52 Showing the Overall results within the groups 124
53 Showing the Overall results of the groups 125
54 Showing the significance of overall results 125
55 Showing sadhyaasadhyata of Asthi pradoshaja vikaras 139
56 Showing the chikitsa of Asthi Pradoshaja Vikaras 141
List of Illustrations
Sl.No Particulars Page No.
1 Showing Age wise distribution of 30 patients 104
2 Showing Sex wise distribution of 30 patients 104
3 Showing Marital status wise distribution of 30 patients 104
4 Showing Education wise distribution of 30 patients 105
5 Showing Religion wise distribution of 30 patients 105
6 Showing Occupation wise distribution of 30 patients 105
7 Showing Habitat wise distribution of 30 patients 106
8 Showing Diet wise distribution of 30 patients 106
9 Showing Prakruti wise distribution of 30 patients 106
10 Showing Samhanana wise distribution of 30 patients 107
11 Showing Pramana wise distribution of 30 patients 107
12 Showing Sattva wise distribution of 30 patients 107
13 Showing Koshtha wise distribution of 30 patients 108
14 Showing Agni wise distribution of 30 patients 108
15 Showing Bala wise distribution of 30 patients 108
XVIII
16 Showing Vyayamashakti wise distribution of 30 patients 109
17 Showing joint involvement wise distribution of 30 patients 109
18 Showing results of Joint pain (Rt Knee) 126
19 Showing results of Joint pain (Lt Knee) 126
20 Showing results of Joint stiffness (Rt Knee) 127
21 Showing results of Joint stiffness (Lt Knee) 127
22 Showing results of Joint swelling (Rt Knee) 128
23 Showing results of Joint swelling (Lt Knee) 128
24 Showing results of Joint crepitus (Rt Knee) 129
25 Showing results of Joint crepitus (Lt Knee) 129
26 Showing overall results within the groups 130
27 Showing overall results in 30 patients 130
List of flow charts
Chart No.
Particular Page No.
1 Showing Samanya Samprapti of Asthi Pradoshaja Vikaras 23
2 Showing the Vishesha Samprapti of Asthi pradoshaja vikaras
138
3 Showing the probable Samprapti of Janusandhigatavata 146

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 1
INTRODUCTION
Being an eternal science, 'Ayurveda', the 'science of human life', deals with
physical, psychological as well as spiritual well being of an individual. It covers all
the spheres of human life. It is not merely a materialistic science, but a philosophical
and factful truth, which our great ancestral sages, through their experience, logic and
power of wisdom, had found true and proved it to the truth of time. To keep it in pace
with advancing or so called modern age or scientific age is the present day task. To
proceed with such an incredibly rewarding task, is not more a challenge but an
exhaustive endeavour.
Human creatures have emerged as specialized species in the process of
evolution. The study of human being includes both physiological & pathological
entities. Ancient seers of Ayurveda have classified the elements of the body under
three fundamental components- Dosha, Dhatu and Mala. These three entities are
responsible for the maintenance of structural and functional integrity of the body.
Among these basic elements Dhatus are especially meant for dharana & poshana of
shareera. The equilibrium state of these dhatus results in arogya, where as any
imbalance in it produces vikara.
Dhatu pradoshaja vikara is a condition in which the dhatus are in vitiated state.
Among the dhatu pradoshaja vikaras, Asthi pradoshaja vikaras include adhyasthi,
asthibheda, asthishula etc. Acharya Charaka mentions that Panchakarma ,ksheera,
sarpi & tikta dravya basti are the treatment modalities for Asthi pradoshaja vikaras.
Sandhigatavata is a vata vyadhi, with characteristic features of Vatapurna
dhruti sparsha, shotha, vedana, sandhi shaithilyata & atopa. Here sandhi means asthi
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 2
melana, so in pathological condition, Asthi is also found to be vitiated & it can be
correlated to osteoarthritis as per the contemporary science.
According to World Health Organization, OA is the second commonest
musculoskeletal problem in the world (30%). The reported prevalence of OA from a
study in rural India is 5.78%. The major risk factors associated with knee OA seen in
population study were; age, females, obesity, smoking, occupational knee bending,
physical labor and chondrocalcinosis. Symptomatic and radiographic OA increases
with age.
Osteoarthritis is defined as degenerative condition of the articular surfaces of
the joint, particularly weight bearing joints. The clinical features are joint stiffness,
diminished mobility, discomfort & pain. The pathological changes occur in articular
cartilages, adjacent bones & synovium.
Evidence based medicine is the mantra of the modern era. So revalidation &
revitalization is essential through research in both fundamental & applied aspect of
Ayurveda. Asthi is one entity which can be visualized easily by radiology. The
revalidation of Asthi pradoshaja vikaras is possible with the help of radiological
investigations.
Hence, this work is undertaken to study the Asthi pradoshaja vikaras w.s.r.to
role of Asthi in manifestation of sandhigatavata & its management with tikta ksheera
sneha basti.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 3
OBJECTIVES OF THE STUDY
To review in detail about Asthi and Asthi pradoshaja vikaras.
To assess the involvement of Asthi with the help of radiology (X-ray).
To assess the role of Asthi in manifestation of sandhigatavata.
To study the role of tiktaka dravyas in the management of sandhigatavata.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 4
ASTHI PRADOSHAJA VIKARAS
The shareera is made up of dosha, dhatu and mala. Among them dhatu is
meant for deha dharana. When this dhatu gets vitiated by doshas it leads to a specific
condition known as dhatu pradoshaja vikara. Among the dhatu pradushaja vikaras,
Asthi pradoshaja vikara is one.
Derivation
The term ‘Asthi pradoshaja vikaras’ consists of three terms. They are Asthi,
Pradoshaja and Vikara.
1. AÎxjÉ
The term ‘asthi’ is a napumsaka linga pada. The vyutpatti of which is as follows:
AxÉç + YÍjÉlÉç AÎxjÉ 1
It is derived from the mula dhatu ‘AxÉç’ and ‘YÍjÉlÉç’suffix.
AÎxjÉ: MüÐMüxÉ, MÑüsrÉqÉç, MümÉÉsÉ.2
Dictionary meanings: hard or firm, a bone, skull bones.3
2. mÉëSÉåwÉeÉ: mÉë+SÉåwÉ+eÉ 4
The term ‘mÉëSÉåwÉeÉ’ is a pullinga pada. The vyutpatti of which is as follows.
mÉë: mÉëM×ü¹ålÉ, EiMüwÉåï, AÉUqpÉ.5
Dictionary meanings: excessively, commencement, beginning.6
SÉåwÉ: SÉåwÉhÉqÉç, SÒ¹qÉç, mÉÉmÉqÉç.7,8
Dictionary meanings: a fault, defect, sinfulness. 9
eÉ: eÉlrÉiuÉÉiÉç, eÉlqÉÌlÉ,eÉlÉɬïlÉå.10,11
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 5
Dictionary meanings: born from, produced, caused by.
3. ÌuÉMüÉU
The term ‘ÌuÉMüÉU’ is a pullinga pada .The vyutpatti of which is as follows.
ÌuÉ+M×ü+bÉgÉç ÌuÉMüÉU.12
The term ÌuÉMüÉU is derived from moola dhatu ‘M×ü’ with ‘ÌuÉ’ upasarga and ‘bÉgÉç’
pratyaya.
ÌuÉMüÉU: mÉËUhÉÉqÉ, ÌuÉM×üÌiÉ, ÌuÉÌ¢ürÉÉ.13
Dictionary meanings: change of form or nature, an alteration, transformation.14
Collectively Asthi pradoshaja vikaras means the excessively vitiated doshas
takes shelter in the asthi and changes its natural form and produces different disorders.
Asthi Pradoshaja Vikaras have been selected for the applied study of this
work. These diseases occur due to vitiation of Asthi Dhatu, so it is important to know
the Asthi Dhatu, before describing Pradoshaja Vikara. Therefore now in the sequence
of concepts, concept of Asthi has been described here.
Asthi dhatu
Definition
zÉUÏUxjÉxÉmiÉkÉÉiuÉliÉaÉïiÉ kÉÉiÉÑÌuÉzÉåwÉ |15
It is one among the sapta dhatus which are present in the shareera.
qÉÉÇxÉÉprÉliÉUxjÉå (WûÉQèû) CÌiÉ ZrÉÉiÉå kÉÉiÉÑpÉåSå |16
Form of dhatu which is present inside the mamsa dhatu is known as Asthi.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 6
Synonyms
Following synonyms are used for Asthi; 17,18,19
Keekasa = hard, firm.
Kulyam = a bone.
Kapala = the skull, cranium, skull bone.
Astri = not feminine, masculine.
Medojam = which is produced from meda.
Table No.1: Showing the Paryayas of Asthi
Sl.no Paryaya S.K.D A.K
1. Keekasa + +
2. Kulyam + +
3. Medojam + -
4. Kapala - +
5. Astri - +
Asthi Utpatti and Poshana
The formation of dhatu takes place in the following order- from annarasa rasa
will form, then rasa to rakta, rakta to mamsa, mamsa to meda, meda to asthi, asthi to
majja, from majja shukra will form, in this way uttarottara dhatu will be formed by
the previous dhatu. During this process heat produced by the combination of pruthvi,
agni and vayu acts on medas giving rise to kharatva (hardness) and thus produces the
asthi. This is in the form of krama parinama paksha or theory of transformation. The
uttarottara dhatu is nourished by the previous dhatu. 20
Food composed of Panchabhutas which is predominantly composed of Pruthvi, Tejas
and Vayu does poshana of the asthi dhatu. 21
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 7
Time taken for asthi formation
There are two opinions regarding formation of Asthi depending upon the time factor.
Asthi is formed on the 6th day. 22
Asthi is formed on 20th day. 23
Asthi swarupa (nature)
‘Kathina’ and ‘sthira’ are the swarupa of Asthi. 24
Asthi Panchabhoutika sanghatana
The panchabhoutika sanghatana of asthi which are mentioned in different samhitas
are tabulated below. 25,26
Table No.2: Showing the Panchabhoutika sanghatana of Asthi
Sl.no Panchabhutas C.S S.S
1. Pruthvi + +
2. Agni/ tejas + +
3. Anila + +
Asthidhara kala
Purishadhara kala is considered as asthidhara kala. 27
Asthivaha sroto mula28, 29, 30
The asthivaha sroto mulas which are mentioned in different samhitas are listed below.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 8
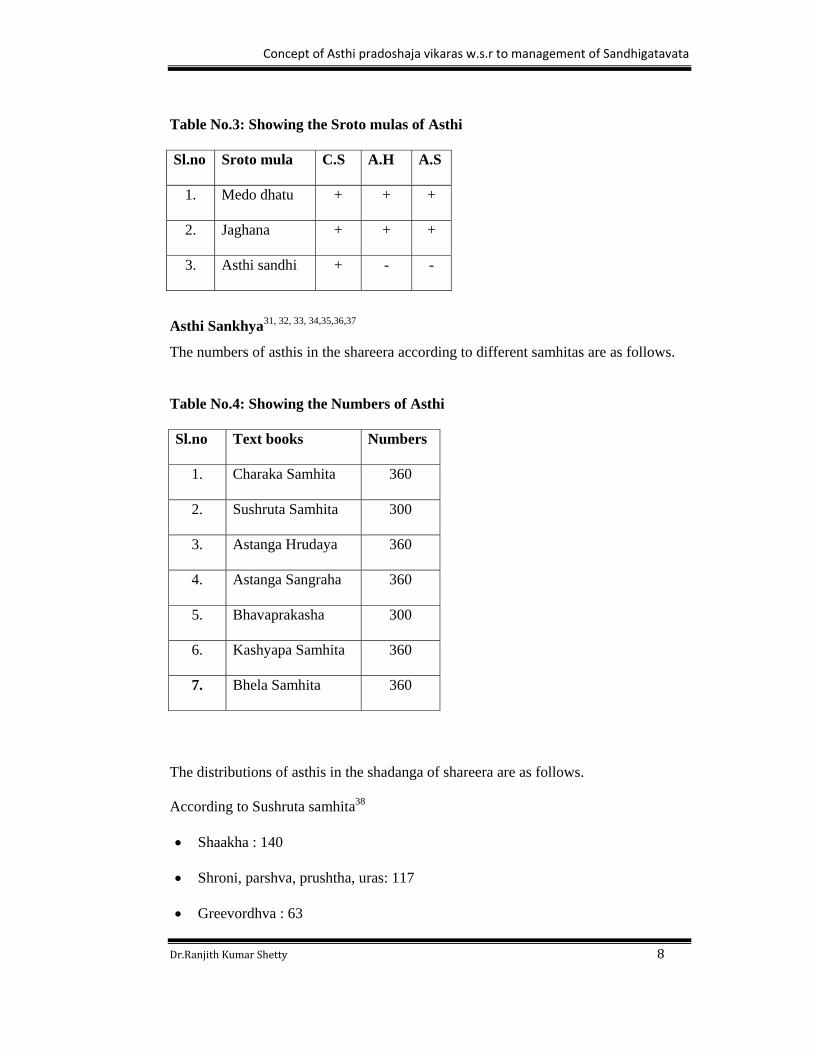
Table No.3: Showing the Sroto mulas of Asthi
Sl.no Sroto mula C.S A.H A.S
1. Medo dhatu + + +
2. Jaghana + + +
3. Asthi sandhi + - -
Asthi Sankhya31, 32, 33, 34,35,36,37
The numbers of asthis in the shareera according to different samhitas are as follows.
Table No.4: Showing the Numbers of Asthi
Sl.no Text books Numbers
1. Charaka Samhita 360
2. Sushruta Samhita 300
3. Astanga Hrudaya 360
4. Astanga Sangraha 360
5. Bhavaprakasha 300
6. Kashyapa Samhita 360
7. Bhela Samhita 360
The distributions of asthis in the shadanga of shareera are as follows.
According to Sushruta samhita38
Shaakha : 140
Shroni, parshva, prushtha, uras: 117
Greevordhva : 63
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 9
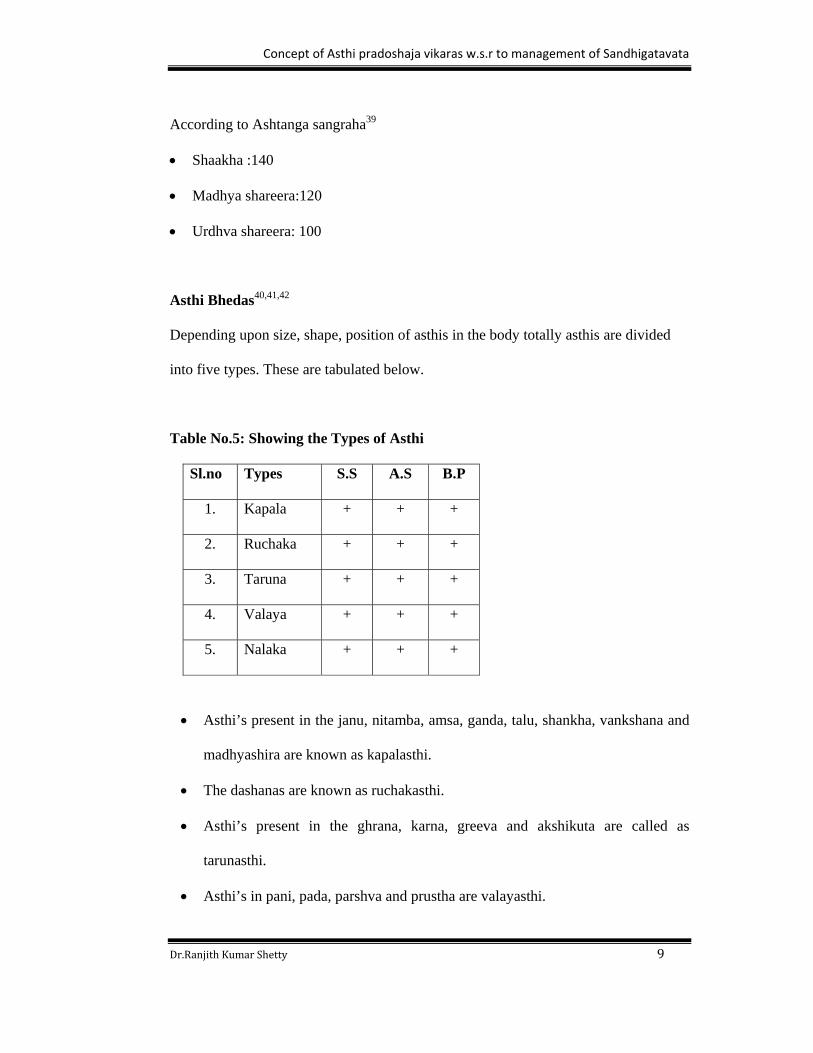
According to Ashtanga sangraha39
Shaakha :140
Madhya shareera:120
Urdhva shareera: 100
Asthi Bhedas40,41,42
Depending upon size, shape, position of asthis in the body totally asthis are divided
into five types. These are tabulated below.
Table No.5: Showing the Types of Asthi
Sl.no Types S.S A.S B.P
1. Kapala + + +
2. Ruchaka + + +
3. Taruna + + +
4. Valaya + + +
5. Nalaka + + +
Asthi’s present in the janu, nitamba, amsa, ganda, talu, shankha, vankshana and
madhyashira are known as kapalasthi.
The dashanas are known as ruchakasthi.
Asthi’s present in the ghrana, karna, greeva and akshikuta are called as
tarunasthi.
Asthi’s in pani, pada, parshva and prustha are valayasthi.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 10
The remaining asthi’s are nalakasthi.
Asthi Karmas
The asthi karmas are as follows
Deha dharana. 43
Majja pushti. 44
Asthi supports the mamsa, sira and snayu. 45
Asthi Upadhatu
The upadhatu of Asthi is danta 46.
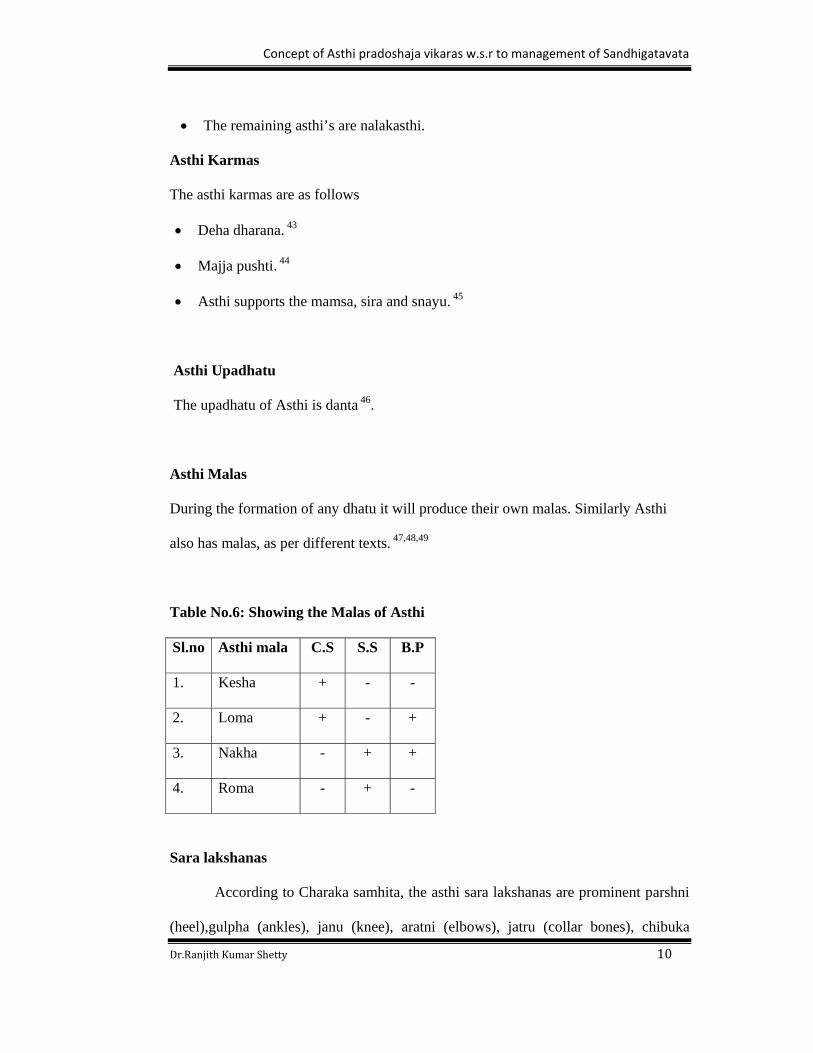
Asthi Malas
During the formation of any dhatu it will produce their own malas. Similarly Asthi
also has malas, as per different texts. 47,48,49
Table No.6: Showing the Malas of Asthi
Sl.no Asthi mala C.S S.S B.P
1. Kesha + - -
2. Loma + - +
3. Nakha - + +
4. Roma - + -
Sara lakshanas
According to Charaka samhita, the asthi sara lakshanas are prominent parshni
(heel),gulpha (ankles), janu (knee), aratni (elbows), jatru (collar bones), chibuka
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 11
(chin), shira (head) and parva (joints) and also asthi (bone), nakha (nails) and danta
(teeth). Such individuals are endowed with qualities such as mahotsaha (enthusiastic),
kriyavanta (active), kleshasaha (enduring), sarasthi and shareera (having strong &
firm body) as well as ayushmanta (longivity). 50
As per Sushruta samhita, asthisara purusha lakshanas are mahashira (big
head), mahaskandha (big shoulders) and drudha danta (strong teeth), drudha hanu
(strong jaws), drudha asthi (strong bones) and drudha nakha (strong nails). 51
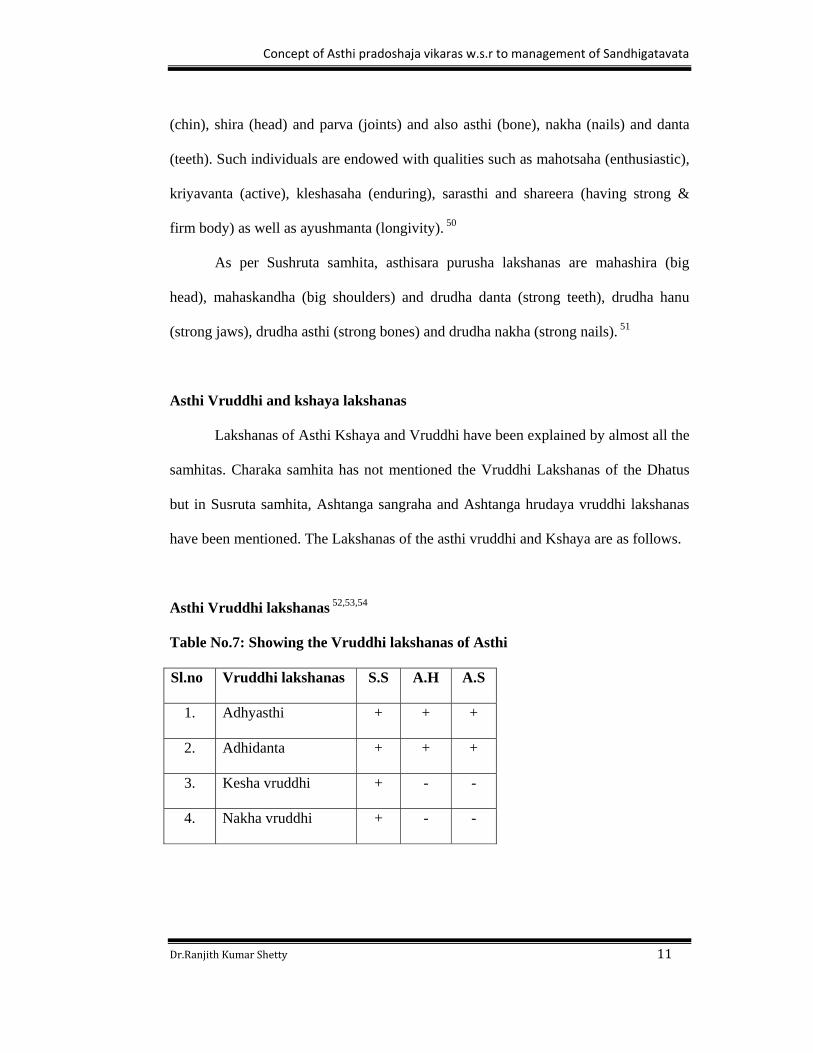
Asthi Vruddhi and kshaya lakshanas
Lakshanas of Asthi Kshaya and Vruddhi have been explained by almost all the
samhitas. Charaka samhita has not mentioned the Vruddhi Lakshanas of the Dhatus
but in Susruta samhita, Ashtanga sangraha and Ashtanga hrudaya vruddhi lakshanas
have been mentioned. The Lakshanas of the asthi vruddhi and Kshaya are as follows.
Asthi Vruddhi lakshanas 52,53,54
Table No.7: Showing the Vruddhi lakshanas of Asthi
Sl.no Vruddhi lakshanas S.S A.H A.S
1. Adhyasthi + + +
2. Adhidanta + + +
3. Kesha vruddhi + - -
4. Nakha vruddhi + - -
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 12
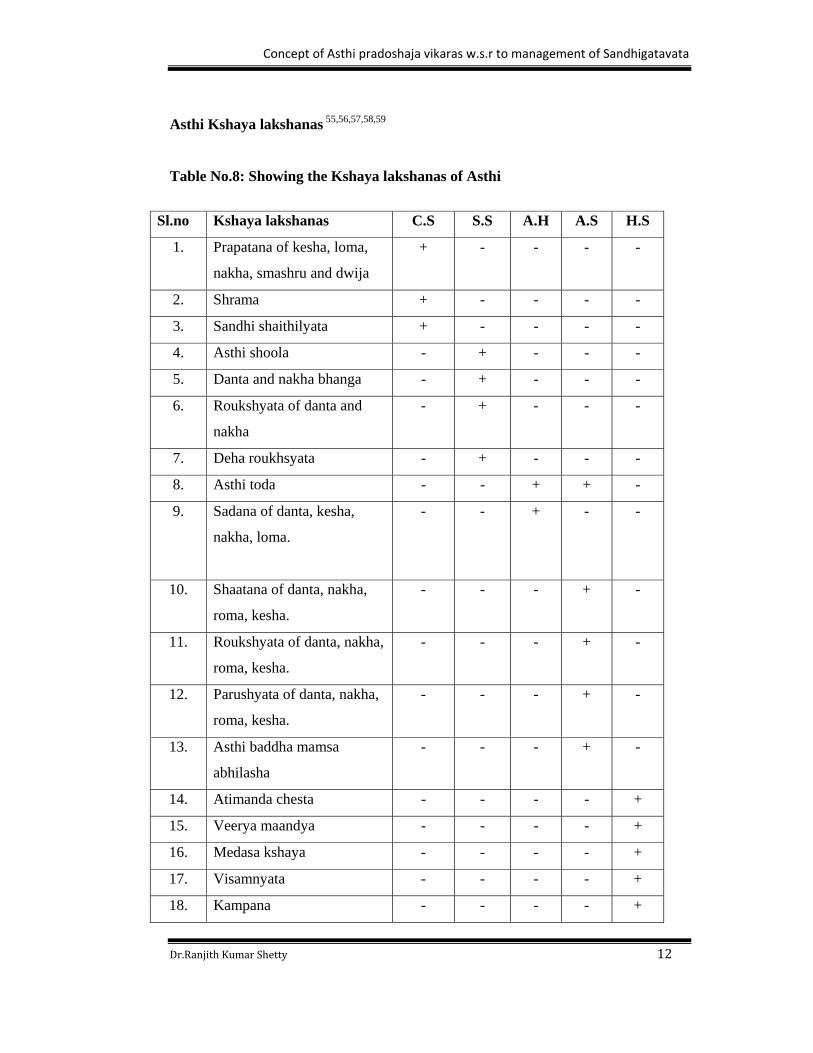
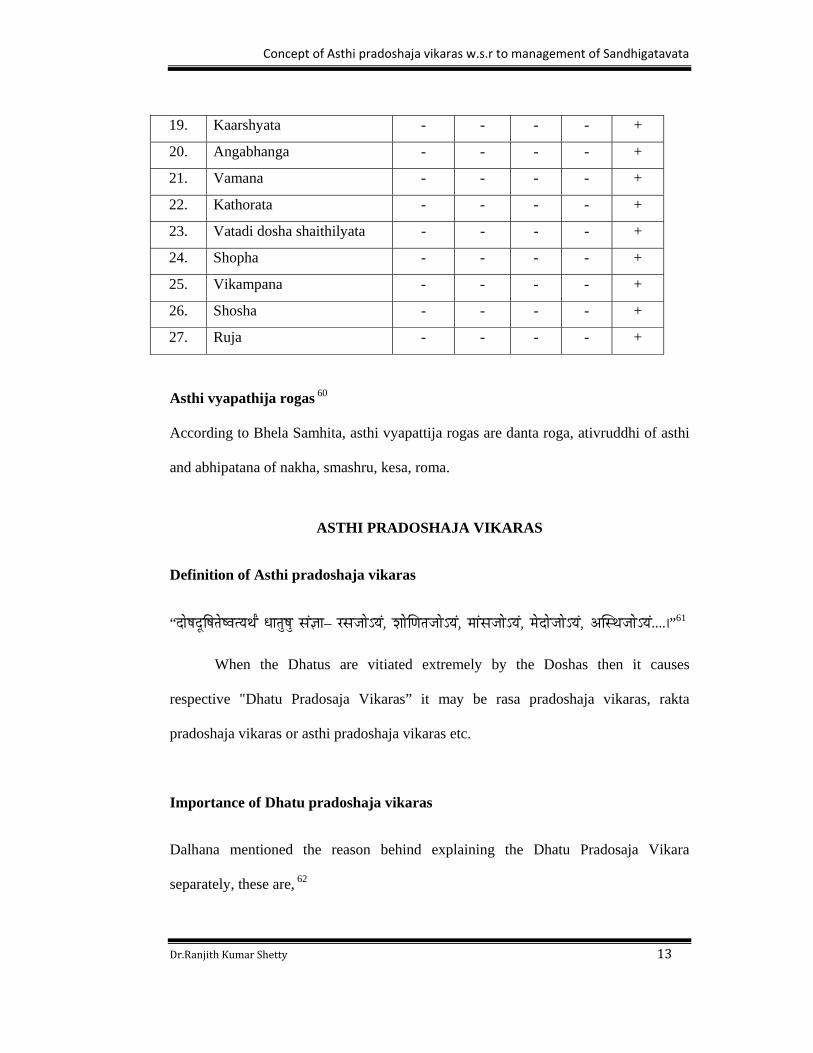
Asthi Kshaya lakshanas 55,56,57,58,59
Table No.8: Showing the Kshaya lakshanas of Asthi
Sl.no Kshaya lakshanas C.S S.S A.H A.S H.S
1. Prapatana of kesha, loma,
nakha, smashru and dwija
+ - - - -
2. Shrama + - - - -
3. Sandhi shaithilyata + - - - -
4. Asthi shoola - + - - -
5. Danta and nakha bhanga - + - - -
6. Roukshyata of danta and
nakha
- + - - -
7. Deha roukhsyata - + - - -
8. Asthi toda - - + + -
9. Sadana of danta, kesha,
nakha, loma.
- - + - -
10. Shaatana of danta, nakha,
roma, kesha.
- - - + -
11. Roukshyata of danta, nakha,
roma, kesha.
- - - + -
12. Parushyata of danta, nakha,
roma, kesha.
- - - + -
13. Asthi baddha mamsa
abhilasha
- - - + -
14. Atimanda chesta - - - - +
15. Veerya maandya - - - - +
16. Medasa kshaya - - - - +
17. Visamnyata - - - - +
18. Kampana - - - - +
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 13
Asthi vyapathija rogas 60
According to Bhela Samhita, asthi vyapattija rogas are danta roga, ativruddhi of asthi
and abhipatana of nakha, smashru, kesa, roma.
ASTHI PRADOSHAJA VIKARAS
Definition of Asthi pradoshaja vikaras
“SÉåwÉSÕÌwÉiÉåwuÉirÉjÉïÇ kÉÉiÉÑwÉÑ xÉÇ¥ÉÉ– UxÉeÉÉåÅrÉÇ, zÉÉåÍhÉiÉeÉÉåÅrÉÇ, qÉÉÇxÉeÉÉåÅrÉÇ, qÉåSÉåeÉÉåÅrÉÇ, AÎxjÉeÉÉåÅrÉÇ....|”61
When the Dhatus are vitiated extremely by the Doshas then it causes
respective "Dhatu Pradosaja Vikaras” it may be rasa pradoshaja vikaras, rakta
pradoshaja vikaras or asthi pradoshaja vikaras etc.
Importance of Dhatu pradoshaja vikaras
Dalhana mentioned the reason behind explaining the Dhatu Pradosaja Vikara
separately, these are, 62
19. Kaarshyata - - - - +
20. Angabhanga - - - - +
21. Vamana - - - - +
22. Kathorata - - - - +
23. Vatadi dosha shaithilyata - - - - +
24. Shopha - - - - +
25. Vikampana - - - - +
26. Shosha - - - - +
27. Ruja - - - - +
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 14
1. Chikitsa Vishesa Vijnanartha
2. Sukhasadhyatvadi Karma Bodhartham
Knowledge of these two is very much essential for a Vaidya, to avoid failure
in practice. Chakrapani distinctly revealed that in some cases only dosha viparita
chikitsa will not bring complete relief to the patient. One should treat dhatu also
because of ashraya prabhava.
“ mÉëuÉ×®zÉÉåÍhÉiÉÉ´ÉrÉÉxiÉÑ uÉÉiÉÉSrÉ AÉ´ÉrÉmÉëpÉÉuÉÉ³É xuÉÍcÉÌMüixÉÉqÉɧÉåhÉ mÉëzÉÉqrÉÌiÉ||” 63
Chakrapani has used the term "Ashraya Prabhava" to indicate the significance of
Dhatu in the treatment.
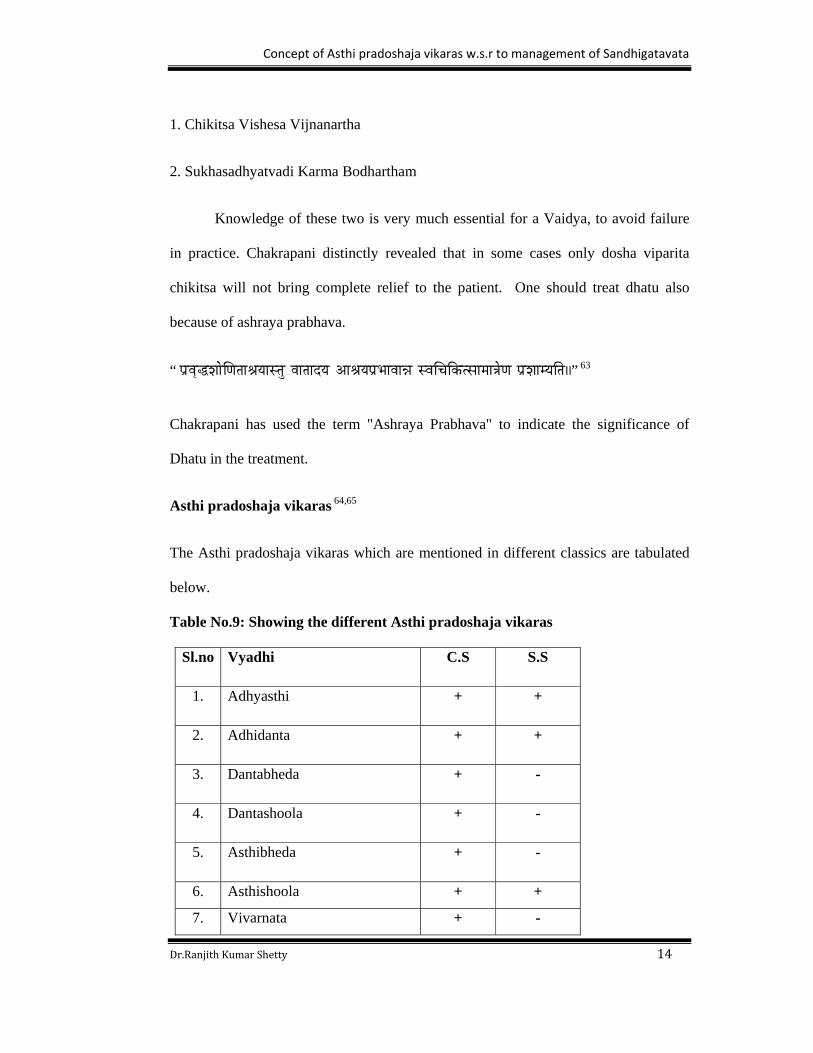
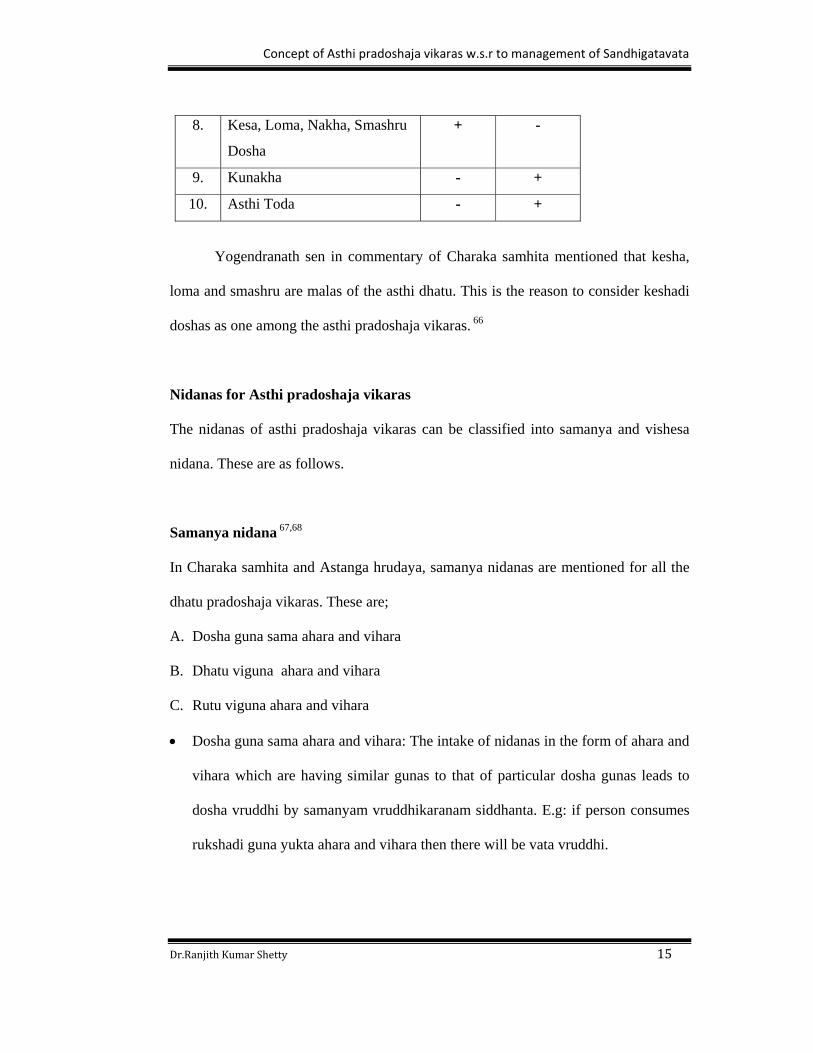
Asthi pradoshaja vikaras 64,65
The Asthi pradoshaja vikaras which are mentioned in different classics are tabulated
below.
Table No.9: Showing the different Asthi pradoshaja vikaras
Sl.no Vyadhi C.S S.S
1. Adhyasthi + +
2. Adhidanta + +
3. Dantabheda + -
4. Dantashoola + -
5. Asthibheda + -
6. Asthishoola + +
7. Vivarnata + -
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 15
8. Kesa, Loma, Nakha, Smashru
Dosha
+ -
9. Kunakha - +
10. Asthi Toda - +
Yogendranath sen in commentary of Charaka samhita mentioned that kesha,
loma and smashru are malas of the asthi dhatu. This is the reason to consider keshadi
doshas as one among the asthi pradoshaja vikaras. 66
Nidanas for Asthi pradoshaja vikaras
The nidanas of asthi pradoshaja vikaras can be classified into samanya and vishesa
nidana. These are as follows.
Samanya nidana 67,68
In Charaka samhita and Astanga hrudaya, samanya nidanas are mentioned for all the
dhatu pradoshaja vikaras. These are;
A. Dosha guna sama ahara and vihara
B. Dhatu viguna ahara and vihara
C. Rutu viguna ahara and vihara
Dosha guna sama ahara and vihara: The intake of nidanas in the form of ahara and
vihara which are having similar gunas to that of particular dosha gunas leads to
dosha vruddhi by samanyam vruddhikaranam siddhanta. E.g: if person consumes
rukshadi guna yukta ahara and vihara then there will be vata vruddhi.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 16
Dhatu viguna ahara and vihara: The intake of nidanas in the form of ahara and
vihara which are having dissimilar gunas to that of particular dhatu gunas i.e dhatu
virodhaka swabhava by vishesa siddhanta.
Rutu viguna ahara and vihara: The particular ahara and vihara which are dealt for
each rutu if not followed leads to dosha vitiation i.e. vipareeta to rutucharya
palana.
Vishesa nidana 69,70,71
In Charaka samhita some specific nidanas are mentioned for Asthi pradoshaja vikaras.
These are;
A. Ativyayama
B. Ati sankshobha
C. Ati vighattana
D. Vatala ahara and vihara
Ativyayama: ativyayama means excessive shareera ayasa janaka karma.
Atisankshobha: Atisankshobha means abhighata (Yogindranath sen). It means
injury or excessive jerk or violence or commotion.
Ativigattana: Ativighattana means atichaalana (Yogindranath sen). It means
excessive movements or separated or loosened or shaking.
Vatala ahara and vihara sevana: Vata guna samana ahara and vihara sevana. For
e.g,
Vatala ahara: ruksha – sheeta- laghu guna pradhana ahara sevana, alpa matra
ahara sevana, mudga, masoora, vaartaaka, kalinga, harenuka etc.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 17
Vatala vihara: ativyavaya, ati jagarana, krodha, bhaya, vegadharana, abhighata,
upavasa, shoka, plavana etc.
Poorvarupa 72
None of the Ayurvedic classics have mentioned poorvarupa of Asthi
pradoshaja vikaras. Avyakta lakshanas or alpa vyakta lakshanas are considered as
poorvarupa.
Rupa
Each Asthi pradoshaja vikara is having its own lakshana. These are as follows.
Adhyasthi 73
Adyasthi means adhika asthi i.e, additional bone or extra bone.
Adhidanta 74
Adhidanta means adhika danta i.e, additional tooth or extra tooth.
Dosha: Vata
Characteristic features: There will be an extra tooth eruption over the tooth and during
the eruption pain associates and after the eruption pain subsides. This condition is
called adhidanta.
Dantabheda 75,76
It is a condition were cutting type of pain in danta is seen and is called as dantabheda.
It is also called as ‘bhanjanaka’.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 18
Dosha: Vata (Vagbhata)
Vata + Kapha (Sushruta)
Characteristic features: It is a vataja vyadhi and there will be toda, bheda, ruk and
sphutana in the danta. This is known as dantabheda.
It is a kapha- vataja vyadhi in which teeth falls down due to mukha vaktrata and
associated with teevra ruja. This is known as bhanjanaka.
Dantashoola 77,78
There will be a severe or acute pain in the tooth is called as dantashoola.
Other names: Dalhana (Sushruta)
Sheetadanta (Vagbhata)
Dosha: Vata
Characteristic features: The vitiated vata dosha causes untolerable cutting type of pain
in the teeth and is called dalana.
Ashtanga hrudaya also opines same, but called it as sheeta danta because the patient is
not able to eat or drink sheeta padarthas.
Asthibheda 79
It is a condition in which bhidhyamanasya vyatha (cutting type or splitting type of
pain) will be present in asthi. This is known as asthibheda.
Asthishoola 80
It is a condition in which severe or acute pain in asthi like shanka sphutanavat. This is
known as asthishoola.

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 19
Asthitoda 81
It is a condition in which vicchinna shoola (pricking or breaking type of pain) will be
present in asthi. This is known as asthitoda.
Vivarnata
These disorders are two in number. They are shyavadanta and krimidanta.
Shyavadanta 82,83
The blackish discoloration of tooth is called as shyavadanta.
Dosha: Rakta + Pitta (Sushruta)
Rakta + Pitta + Vata (Vagbhata)
Characteristic features: The vitiated rakta along with pitta, burns the danta twacha and
causes the shyavata (blackish) or neela (blue) varnata of danta. This is known as
shyavadanta.
The danta becomes shyava varna due to the vitiation of rakta, pitta and vata is known
as shyavadanta.
Krimidanta 84,85
The condition in which decaying of tooth takes place is called as krimidanta.
Dosha: Vata
Characteristic features: Due to the vitiation of vata dosha, danta becomes krishna
varna, chidra yukta, chalayukta, sravayukta, teevra rujayukta or sometime intermittent
shoola. This is known as krimi danta.
Ashtanga hrudaya explained krimidanta in a more ellaborate manner, which is as
follows.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 20
Vata vitiation danta moola shotha
Danta kshata sushira
Danta majja shosha production of krimi
Danta shoola, srava chala danta
Puya rakta srava danta vidradi
Kesha, loma and smashru vikaras
The kesha, loma and smasru vikaras are indralupta, ruhya, khalitya and palitya.
Indralupta 86,87,88
The partial or complete loss of hair from all over the body is called as indralupta.
Synonyms: Ruhya, Chacha
Dosha: Tridosha + Rakta
Characteristic features: The vitiated vata and pitta affects the roma kupas and causes
roma patana, then the vitiated kapha and rakta obstructs the roma kupas. So there is
no chance for regrowth of hairs. This condition is called as indralupta.
Ashtanga hrudaya also opines same.
Karteeka opines that if hair loss is from all over the body is called as Ruhya and fall
of smashru is known as indralupta.
Khalitya 89,90,91
The condition in which gradual loss of hair takes place in the scalp is called as
khalitya.
Dosha: Tridosha (Charaka)
Tridosha + Rakta (Sushruta & Vagbhata)

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 21
Characteristic features: The vitiated vatadi doshas along with increased shareera
ushnata removes the snigdata in kesha moolas leading to gradual hair loss is called as
khalitya.
The vitiated vata and pitta affects the roma kupas and causes roma patana, then the
vitiated kapha and rakta obstructs the roma kupas. So there is no chance for regrowth
of hairs. The complete loss of scalp hair is called khalitya.
The pathology of khalitya is like indralupta i.e, vata and pitta causes kesha shatana,
kapha and rakta obstructs the kesha moolas so there is no chance of re growth of hair
but in khalitya kesha shatan is g radual or slow, not sudden as in indralupta.
Palitya 92,93,94
The condition in which discoloration of hair takes place is called as palitya.
Dosha: Tridosha (Charaka)
Pitta (Sushruta & Vagbhata)
Characteristic features: The vitiated vatadi doshas and increased shareera ushnata
removes the snigdhata in kesha moolas causing discoloration of hair, it becomes
kapila varna.
Due to krodha, shoka and shrama the increased shaeera ushnata and vitiated pitta
causes pachana or discoloration of keshas in the shiras which is called as palitya.
Ashtanga hrudaya also opines same as Sushruta samhita and mentions some other
lakshanas depending upon predominance of doshas.
In vata predominance, hair becomes shyava varna, ruksha, khara and jalaprabha.
In pitta predominance, hair becomes peetabha with daha.
In kapha predominance, hair becomes snigdayukta, shukla varna and sthula.

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 22
In tridosha vitiation all the above symptoms together present.
Kunakha 95,96
A disease of the nails which is ugly in appearance. This condition is called as
kunakha.
Syonyms: Kuleena (Sushruta)
Dosha: Pitta +Vata
Characteristic features: The vitiated pitta and vata localizes at the sides of the nail
beds producing daha, paka and vedana and is called as chippa. When this condition is
in mild form, it is known as kunkha and nakha attains rukshatva, kharatva and asita
varna. Other causes for kunakha include abhighata.
Ashtanga hrudaya also opines same and added one more lakshana i.e, jwara.
Samprapti 97
The nidanas of the asthi pradoshaja vikara are ativyayama, atisankshobha,
ativighattana and vatala ahara- vihara which leads to agni dushti and is the cause of
production of abnormal asthi. In such conditions if the patient continues the intake of
causative factors (Nidana Sevana), there will be excessive vitiation of doshas as they
have been already vitiated earlier. These excessive vitiated doshas when lodges in
asthi dhatu, the manifestation of asthi pradosaja vikara takes place at various sites in
the body according to sthana dusti or Khavaigunya.

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 23
Flow chart No.1: Showing Samanya Samprapti of AsthiPradoshaja Vikara
Sadhyasadhyata 98,99
Among the Asthi pradoshaja vikaras, some are considered as asadhya vyadhis
and some are considered as yapya vyadhis and some are kashta sadhya vyadhis.
Dalana, bhanjanaka, shyavadanta, tridoshaja khalitya, tridoshaja palitya and
dantashoola are considered as asadhya vyadhis. Indralupta, ekadoshaja khalitya and
Nidana sevana
Dosha gunasama
ahara‐vihara
Dhatu viguna ahara‐
vihara
Rutu vigunaa ahara‐vihara
Dhatu dushti
Dosha dushti Dosha dushti
Asthi dhatu dushti
Khavaigunya
Dosha‐dushya sammurchana
Particular Asthi pradoshaja vikaras
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 24
ekadoshaja palitya are considered as yapya vyadhis. The remaining diseases are
considered as kashtasadhya vyadhis i.e adhyasthi, adhidanta, dantabheda, asthibheda,
asthi toda, asthishoola and kunakha.
Upadrava
None of the Ayurvedic classics have mentioned upadravas of Asthi pradoshaja
vikaras.
Arishta lakshanas
Regarding arishta lakshanas, there is no direct reference in the context of Asthi
prradoshaja vikaras.
Chikitsa
According to Charaka Samhita, Asthyashrita vyadhis are treated by
Panchakarma, especially by Basti, which is prepared out of Ksheera, Sarpi, and Tikta
Dravyas. While commenting on chikitsa sutra Chakrapani opines that tikta ksheera
sarpi basti is ‘hita’ for asthi pradoshaja vikaras. 100
Other treatment modalities which are expalined in different classical texts can be
adopted to treat Asthi pradoshaja vikaras. These are as follows.
According to Sushruta Samhita, snayu and sandhyasthi gata rogas are treated by
sneha, upanaha, agnikarma, bandhana and unmardana. 101

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 25
According to Ashtanga hrudaya, diseases due to vitiation of Asthidhatu are treated
by basti, which is prepared by Ksheera, Sarpi, and Tikta Dravyas. Ashtanga
sangrahakara also opines same treatment. 102,103
According to Yogaratnakara, bahya and abhyantara snehana karma are adopted to
treat asthimajjagata rogas. 104
According to Harita Samhita, asthi kshaya is treated by processed ghrita, usage of
different types of ksheeras, chandana, drakshadi churna, all types of jangala desha
praani mamsa sevana and all types of Madura pradhana annas. 105
Chikitsa for Adhidanta 106,107
Kshara karma
When danta is jarjarita, then krimidantavat chikitsa is to be adopted i.e. swedana,
rakta visravana, gandusha, nasya, agnikarma.
Danta nirharana, then vranavat chikitsa.
Chikitsa for Danta bheda108
All the vata-kapha nashaka kriya.
Arditavat chikitsa
Abhyanga with narayana taila.
Swedana and vasti.
Kavala with aakara karabhadi yoga.
Eranda taila pana.
Gandusha dharana: ksheera prepared out of tila + yashtimadhu.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 26
Chikitsa for Danta shoola109
According to Sushruta samhita, it is an asadhya vyadhi.
Gandusha with hingvadi taila or eranda + dvivyaghri + bhukadamba siddha taila
or yastimadhu taila.
Danta nirharana with danta nirgatana yantra.
Danta pali lekhana, then agni karma with ushna taila.
Danta pali gharshana or pratisarana with fine powders of musta, saindhava,
dadima tvacha, triphala, rasanjana, shunti + madhu.
Kavala with ksheeri vruksha kashaya
Nasya with anu taila or ksheera prepared out of yashtimadhu + vidari +
shrungataka + kasheru.
Chikitsa for Krimidanta110,111
Immovable teeth: swedana, rakta mokshana, vataghna avapeeda nasya, sneha
gandusha, bhadradarvadi lepa, snigdha bhojana.
Movable teeth: danta nirharana and agni karma.
If tooth is perforated: filling the gap with guda or madhuchista and agnikarma,
filling the gap with the milk of saptacchada or arka.
Chikitsa for Indralupta112,113
First siravyadhana is done at the nearer site of lesion, then application of the paste
which is prepared by kaseesa, manashila, tuttha and maricha or pippali to the
head.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 27
Application of bhrungaraja taila or bruhati taila + gunja moola or bhrungaraja
swarasa + taila (pakwa) or gomutra + japa pushpa or root and fruit of gunja or
langali moola + ksheera or karaveera patra swarasa or kantakari swarasa + madhu
or dhattura patra swarasa with madhu or ghrita, bhallataka rasa with madhu or
ghrita, tila pushpa + gokshura with madhu or ghrita, hastidanta masi with tila taila.
Upto completion of treatment snana is not adviced.
Chikitsa for Khalitya and Palitya114,115,116
Shareera shodana : vamana and virechana
Nasya karma with vidarigandhadi taila or sahacharadi taila or bhrungaraja taila or
prapoundarikadi taila or mahaneela taila or laghupanchamooladi taila or nimba
taila or bhruhatyadi taila or jeevaniya gana taila.
Shiroabhyanga with mahaneela taila or bhrungaraja taila
Lepa with priyaladi yoga or tiladi yoga.
Palitanashaka loha yoga for oral administration.
Application of jatamamsi + kushta + tila + Krishna sariva + neelotpala + gomutra
+ madhu.
Oral intake of ksheera daily.
Bramhacharya palana.
Chikitsa for Kunakha117
Shastra karma: swedana with the part being immersed in ushna jala and nail has
to be removed.

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 28
Agni karma
Chakra taila for application.
Sarja churna for application
Madhuroushadha siddha taila for application.
Application of haridra + agaru and kalimaka kalka.

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 29
BONE AND BONE DISORDERS
Bone is essentially a highly vascular, living, constantly changing mineralized
connective tissue. It is remarkable for its hardness, resilience and regenerative
capacity, as well as its characteristic growth mechanisms. 118
Synonyms of bones: bone, off-white, os, pearl, ivory, osseous tissue. 119
Number of bones120
The human skeleton consists of 206 bones.
Upper limbs- 64
Lower limbs- 62
Vertebrae- 26(33)
Skull- 29
Ribs- 24
Sternum- 1
Classification of bones121
(A). According to position
1. Axial: bones forming the axis of the body. e.g, skull, ribs, sternum and vertebrae.
2. Appendicular: bones forming the skeleton of limbs.
(B). According to size and shape
1. Long bones: present in upper and lower limbs.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 30
2. Short long bones: same as above but are miniature in size. e.g, metacarpals,
metatarsals and phalanges.
3. Short bones: small, polyhedral and generally cuboidal in shape.e.g, carpel and
tarsal bones.
4. Flat bones: expanded and plate like. e.g, scapula, sternum, ribs, parietal and
frontal bones.
5. Irregular bones: irregular in general outline and do not fit in any of the categaries.
e.g, vertebrae and some skull bones.
6. Pneumatic bones: flat or irregular bones possessing a hollow space within their
body which contains air. e.g, ethmoid, maxilla, mastoid part of temporal bone.
7. Sesamoid bones: sesamoid means ‘seed- like’. They are nodules of bones. e.g,
pisiform, patella.
(C). According to gross structure
1. Compact bone: the outer cortical part of long bones, which is hard and has a
homogenous appearance.
2. Spongy bone: the inner part of bone which is less hard and presents a spongy
appearance. E.g, flat, short and irregular bones and ends of long bones.
3. Diploic bone: consists of inner and outer tables of compact bone with an
intervening porous layer which is occupied by a spongy substance consisting of
bone marrow and diploic veins. Eg, most of cranial bones.
(D). According to development
1. Membranous bones: which develop in membrane.
2. Cartilaginous bones: which develop in cartilage.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 31
Development of bones122
Both cartilages and bones are mesodermal in origin. They develop from the
embryonic mesenchyme which is the loose cellular connective tissue with a fluid
matrix.
Structure of cartilage and bone123
1. Cartilage: Cartilage is a variety of hard connective tissue.
Characteristic feature: translucent, firm (less hard than bone) and elastic. It is
compressible and can withstand considerable pressure, pull and torsion.
Histological structure: Cartilage consists of two basic structures
i. Chondrocytes: usually large, rounded and encapsulated. They are embedded in
the matrix.
ii. Matrix: it depends upon the character and properties of the cartilage of a gel
like ground substance which makes the cartilage solid. It contains cartilage
cells and fibres.
Types of cartilage: Depending upon the type of fibers in the matrix and number of
cells cartilages are divided into 3 types. (a) Hyaline cartilage
(b) White fibro cartilage
(c) Elastic cartilage
(2) Bone: Bone is a type of hard connective tissue and is the hardest structure in the
body

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 32
Composition of bone124
i. Organic matter: Forms1/3 weight of bone; consists of fibrous material and
cells; responsible for the toughness and resilience of bone.
ii. Inorganic matter: Forms 2/3 weight of bone; consists of the following minerals
salts-calcium phosphate, calcium carbonate, calcium fluoride and magnesium
phosphate; responsible for the rigidity and hardness of bone.
Bone cells: These are (i) Osteoblasts (ii) Osteocytes (iii) Osteoclasts. 125
Osteoblasts: These are ovoid cells with basophilic cytoplasm and an oval nucleus.
They lie against the surface of bone in the inner layer of periosteum and the
endosteum i.e. at the sites where active bone formation is in progress. They form
protein elements of the matrix and control deposition of mineral salts in relation to
collagen fibres. They produce alkaline phosphatase which helps in precipitation of
calcium phosphate and other salts.
Osteocytes: Osteoblasts becomes Osteocytes by forming matrix around itself and
becoming dormant when active bone formation is not required. They occupy the
lacunae.
Osteoclasts: These are large multi nucleated giant cells with acidophilic cytoplasm,
which contains many vacuoles. They arise by fusion of Osteoblasts and Osteocytes
and are concerned with resorption of bone during growth and remodeling of skeleton.
They produce acid phosphatase which dissolves inorganic constituents of bone.

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 33
Periosteum: It is a thick layer of fibrous tissue which covers bone surfaces except
over its articular surfaces where it is replaced by articular cartilage. Through its blood
vessels it nourishes the bone and if torn, the underlying bone dies. Periosteum has
bone forming activity in times of need.
Endosteum: It is highly vascular membrane which lines the medullary cavity on the
inner surface of a compact bone.
Bone minerals, Calcitropic hormones and bone mineral homeostasis126
Three major ions, calcium, phosphorous and magnesium; three major Calcitropic
hormones, parathyroid hormone (PTH), 1,25dihydro vitamin D3 and calcitonin; and
three major target organs, bone, kidney and gut are involved in the metabolism of
bone, bone mineral and bone growth.
Minerals
Calcium: The total body content of calcium is about 1000gms. More than 99% of this
is in the bone. Normally, 90% of the filtered calcium is reabsorbed in the proximal
tubule and loop of henley and 8% in the distal tubule and collecting duct.
Reabsorption at the latter site is increased by PTH and decreased by metabolic
acidosisand phosphate depletion. Tubular intestinal absorption of calcium adjusts so
that the plasma level set by the prevailing secretion rate of PTH can be maintained
without the loss of calcium from bone.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 34
Phosphate: The total body content of phosphate is about 700gms, of which 85% is in
bone and most of the remainder is inside cells. Inorganic phosphate is an integral part
of bone mineral. The concentrations of inorganic phosphate in glomerular filtrate are
similar to that in plasma. Normally, about 85% of the filtered load is reabsorbed, 75%
in the proximal tubules and 10% in the distal tubules. Both proximal and distal
reabsorption of phosphate is decreased by PTH and calcium.
Magnesium: The total body content of magnesium is about 20gm, of which 65% in
bone and most of the remainder is intracellular. Net gastrointestinal absorption of
magnesium is about 40% intake. Normally, about 96% of filtered magnesium is
reabsorbed. Magnesium is an important component of the adenylate cyclase system
and is required in the process of vitamin-D activation. Severe and prolonged
hypomagnesaemia inhibits PTH release and induces resistance to the action of PTH
on bone.
Calcitropic hormones
Vitamin-D: Intestinal absorption of dietary vitamin-D occurs mainly in jejunum.
Both viaminD2 and vitamin D3 are prohormonal forms and are inert until activated in
the liver and kidney through sequential hydroxylations. The production of
1,25(OH)2D3 is directly related to body needs; its formation is enhanced by vitamin D
depletion,PTH, hypocalcaemia and hypophosphataemia. The effect 1,25(OH)2D3 on
the intestineis to increase the absorption of calcium and phosphorus. In the skeleton
1,25(OH)2D3 has two actions; mobilization of calcium and phosphorus from
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 35
previously formed bone and probably promotion of maturation and mineralization of
the organic matrix.
Parathyroid hormone: The function of PTH is to maintain ionized calcium
concemtration in the ECF. PTH secretion increases with a fall and decreases with a
rise in plasma ionized calcium. The extracellular concentration of ionized calcium is
the most important physiological regulator minute to minute secretion of PTH. PTH
has a dual action on bone, of calcium release and bone remodeling. PTH increases
osteoclastic bone resorption by first acting on Osteoblasts or stromal fibroblasts,
which release osteoclast activating cytokines.
Calcitonin: Calcitonin is the only hormone in humans capable of actively lowering
serum calcium. The hypocalcimic action of CT results from the inhibition of bone
resorption and decreased in the absolute number of Osteoclasts and increased bone
mineral deposition. It also affects Osteocytes causing decreased calcium ion flux
across the cell membranes. These effects are opposite of PTH. Calcitonin secretion is
stimulated by hypercalcaemia and inhibited by hypocalcaemia. Calcitonin protects
against hypercalcaemia. Calcitonin levels are lowered by oestrogen deficiency.
Oestrogen: The limited number of estrogen binding sites is on Osteoblasts as well as
Osteoclasts. Its decline at menopause results in a rapid bone loss, associated with
increased osteoclastic bone resorption, particularly trabecular.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 36
Other systemic hormones: Other hormones, which regulate bone growth and
metabolism, include growth hormone, somatomedins, insulin, glucocorticoids, thyroid
hormones, prolactin and gonadotropins.
Local factors: Most of the local regulators of bone remodeling are synthesized by
skeletal cells and include growth factors, cytokines and prostaglandins.
Functions of bones: 127
Constitute framework of the body and hence gives shape and form to the body.
Forms central axis of the body.
Supports and transmits weight of the body.
Provides the levers essential for locomotion by forming articulations and giving
attachment to muscles and ligaments.
Provide mechanical protection to vital organs such as brain, heart and lungs.
Stores calcium.
Forms blood in their marrow.
Blood supply of bones: Derived from 4 sources. They are; 128
i. Nutrient artery
ii. Periosteal artery
iii. Metaphyseal artery
iv. Epiphysial artery
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 37
Lymphatic drainage of bones: The lymphatics of the haversian systems drain into
the periosteal lymph vessels. 129
Nerve supply of bones: They apparently consist of both sensory and motor
(autonomic) fibres. 130
Bone disorders131,132
Some of the bone disorders are as follows.
Bone Spur
A bone spur (osteophyte) is a bony growth formed on normal bone. Bone spur is just
extra bone. It’s usually smooth, but it can cause wear and tear or pain if it presses or
rubs on other bones or soft tissues such as ligaments, tendons, or nerves in the body.
Common places for bone spurs include the spine, shoulders, hands, hips, knees, and
feet.
Bone pain
Chronic bone pain: Subacute or chronic bone pain usually has the following
characteristics.
Localized to the affected bone, rather than the joint
Present at rest and worse at night-time
Not clearly worsened by movement or usage (unlike joint or periarticular pain)
Not readily reproduced by joint movement
Focal tenderness on local pressure.
Other features in the enquiry usually points to the most likely cause. For example;
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 38
Slowly but relentlessly progressive pain suggests a destructive disease like
malignancy or chronic infection. Malignancy is usually associated with weight
loss, fatigue and symptoms relating to the primary site.
Pain that is experienced over a wider area of a bone and accompanied by
deformity strongly suggests Paget's disease.
Osteomalacia is associated with bone tenderness and limb girdle weakness.
Pain from osteonecrosis is initially bony and progressive but then may develop
superadded features of joint pain (worse on usage or weight-bearing, with or
without radiation, reproduced by examination) as the adjacent joint cartilage
collapses and the joint is involved (mainly hips, shoulders or elbows).
Severe arthropathy with subchondral bone attrition and collapse most commonly
osteoarthritis, may also cause bone pain, though this inevitably superimposed
upon a chronic history of usage –related joint pain.
Acute bone pain: Fracture
Sudden onset pain that is very well localized, severe and worsened by even slight
movement should always suggest a fracture. This is the major clinical manifestation
of metabolic bone disease.
Fragility fractures occur spontaneously or as the result of relatively minor trauma;
they are typical of osteoporosis.
Pathological fractures occur in bone that is structurally abnormal, such as in
Paget's disease, osteomalacia, bone metastasis and parathyroid bone disease. Like
fragility fractures, they can occur spontaneously or follow minor trauma.
High-energy fractures result from major trauma (e.g. car crash, falls from a
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 39
height) and can affect normal bones. The same is true of stress (fatigue) fractures
in healthy individuals, such as athletes and military recruits, who are exposed to
repetitive trauma.
Toothache
A toothache, also known as odontalgia or, less frequently, as odontalgy, is an aching
pain in or around a tooth. In most cases toothaches are caused by problems in the
tooth or jaw, such as cavities, gum disease, the emergence of wisdom teeth, a
marginally cracked tooth, infected dental pulp (necessitating root canal treatment or
extraction of the tooth), jaw disease, or exposed tooth root. Causes of a toothache may
also be a symptom of diseases of the heart, such as angina or a myocardial infarction,
due to referred pain.
Dental caries
Dental caries, also known as tooth decay or a cavity, is a disease where bacterial
processes damage hard tooth structure (enamel, dentin, and cementum). These tissues
progressively break down, producing dental caries (cavities, holes in the teeth). Two
groups of bacteria are responsible for initiating caries: Streptococcus mutans and
Lactobacillus. If left untreated, the disease can lead to pain, tooth loss, infection, and,
in severe cases, death.
Hyperdontia
Hyperdontia is the condition of having supernumerary teeth, or teeth which appear in
addition to the regular number of teeth. The most common supernumerary tooth is a
mesiodens, which is a mal-formed, peg-like tooth that occurs between the maxillary
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 40
central incisors. Fourth and fifth molars that form behind the third molars are another
kind of supernumerary teeth.
Fissure or cracked teeth
The deep pits and fissures in teeth are where some 80% of cavities begin. In reference
to the teeth, fissures are thin grooves in the biting surfaces (frequently extending onto
the sides). They are significant because of their tendency to accumulate food and
bacterial plaque. It may not be possible to remove plaque from deep pits and fissures
in teeth, and some 80% of cavities are believed to originate there.
Tooth discoloration
Tooth discoloration is caused by multiple local and systemic conditions. Extrinsic
dental stains are caused by predisposing factors(poor oral hygiene) and other factors
such as dental plaque and calculus, foods and beverages, tobacco, chromogenic
bacteria, metallic compounds, and topical medications. Intrinsic dental stains are
caused by dental materials (eg, tooth restorations), dental conditions and caries,
trauma, infections, medications, nutritional deficiencies and other disorders (eg,
complications of pregnancy, anemia and bleeding disorders, bile duct problems), and
genetic defects and hereditary diseases. (eg, those affecting enamel and dentin
development or maturation).
Onychogryphosis
Onychogryphosis is a thickening and distortion of the toenails usually due to tight or
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 41
ill fitting shoes. These types of nails are caused by damage to the cells that grow the
nail. This can be sudden acute damage such as dropping a heavy object onto the toe or
can be due to a gradual damage over the years with the toes impacting into the toe box
of the shoes or with various sporting activities.
Alopecia areata
Alopecia areata is a condition affecting humans, in which hair is lost from some or all
areas of the body, usually from the scalp. Because it causes bald spots on the scalp,
especially in the primary stages, it is sometimes called spot baldness. In 1%–2% of
cases, the condition can spread to the entire scalp (Alopecia totalis) or to the entire
epidermis (Alopecia universalis).
Hair may also be lost more diffusely over the whole scalp, in which case the
condition is called diffuse alopecia areata.
Alopecia areata monolocularis describes baldness in only one spot. It may occur
anywhere on the head.
Alopecia areata multilocularis refers to multiple areas of hair loss.
The disease may be limited only to the beard, in which case it is called Alopecia
areata barbae.
If the patient loses all the hair on his/her scalp, the disease is then called Alopecia
areata totalis.
If all body hair, including pubic hair, is lost, the diagnosis then becomes Alopecia
areata universalis.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 42
Grey Hair
Grey hair is usually associated with ageing, but this is not always the case. Early
greying of the hair is basically hereditary, and can inherit it from one of our parents or
grandparents. Grey hair can also be influenced by stress. A person experiencing a
prolonged period of stress and anxiety may notice, over a period of time, white hairs
gradually appearing. Malnutrition, worry, shock, deep sorrow, tension and other
similar conditions may also slow down the production of melanin resulting in grey
hair.
Investigations 133
The following investigations are usually done in bone disorders.
Bone mineral profile
Calcitropic hormone assay
Imaging technique
Plain radiography
Bone scan or Scintigraphy
Bone densitometry
Quantitative ultrasound
Quantitative computed tomography
Magnetic resonance imaging
Bone biopsy and Histomorphometry

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 43
SANDHIGATAVATA
Sandhigatavata is mentioned under Vatavyadhi by all the samhitas.
Janusandhigatavata represents the variety of sandhigatavata. The knowledge of
disease is obtained by the study of Nidana, Purvarupa, Rupa, Upashaya and Samprapti
which are termed as Nidana Panchaka.
Derivation
JanuSandhigata vata is a compound word with 4 words combined. Janu, Sandhi, Gata
and Vata.
Janu
Vyutpatti: eÉlÉç +gÉÑhÉç 134
The term ‘janu’ is derived from the mula dhatu ‘eÉlÉç’ and ‘lÉÑhÉç’ suffix.
Nirukti: EÂ eÉÇbÉrÉÉåUç qÉkrÉ pÉÉaÉ:| 135
The region between the uru and jangha is called janu.
Sandhi
Vyutpatti: xÉÇ+ kÉÉ+ ÌMü: 136
The term is derived from ‘sam’ upasarga and ‘dhaa’ dhatu. It means that which does
the sandhaana is nothing but sandhi.
Nirukti: AxjlÉÉÇ iÉÑ xÉlkÉrÉÉå ¾ûÉåiÉå MåüuÉsÉ: mÉËUMüÐÌiÉïiÉÉ:| 137
Place where the joining of bone takes place is known as sandhi.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 44
Gata
Vyutpatti: aÉÇ + £ü: 138
The term gata is derived from ‘gam’ dhatu and ‘kta’ upasarga.
Nirukti: aÉqÉç- aÉqÉlÉå|139
This is approached or situated.
Vata
Vyutpatti : uÉÉ + iÉlÉç 140
The term vata is derived from mula dhatu ‘vaa’ and ‘tan’ suffix.
Nirukti: uÉÉ aÉÌiÉ aÉlkÉlÉrÉÉå: CÌiÉ| 141
Which is having mobility or movement is called vata.
The vitiated vata when gets lodged in janu sandhi leads to the manifestation of
janusandhigatavata.
Paryaya of Sandhigata vata. 142
Sandhivata
Sandhigatavata
Khudavata
Jeerna vata
Nidana
There are no special set of nidanas mentioned in classics for sandhigatavata or
janusandhigatavata. The set of nidanas mentioned for vatavyadhi can be considered
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 45
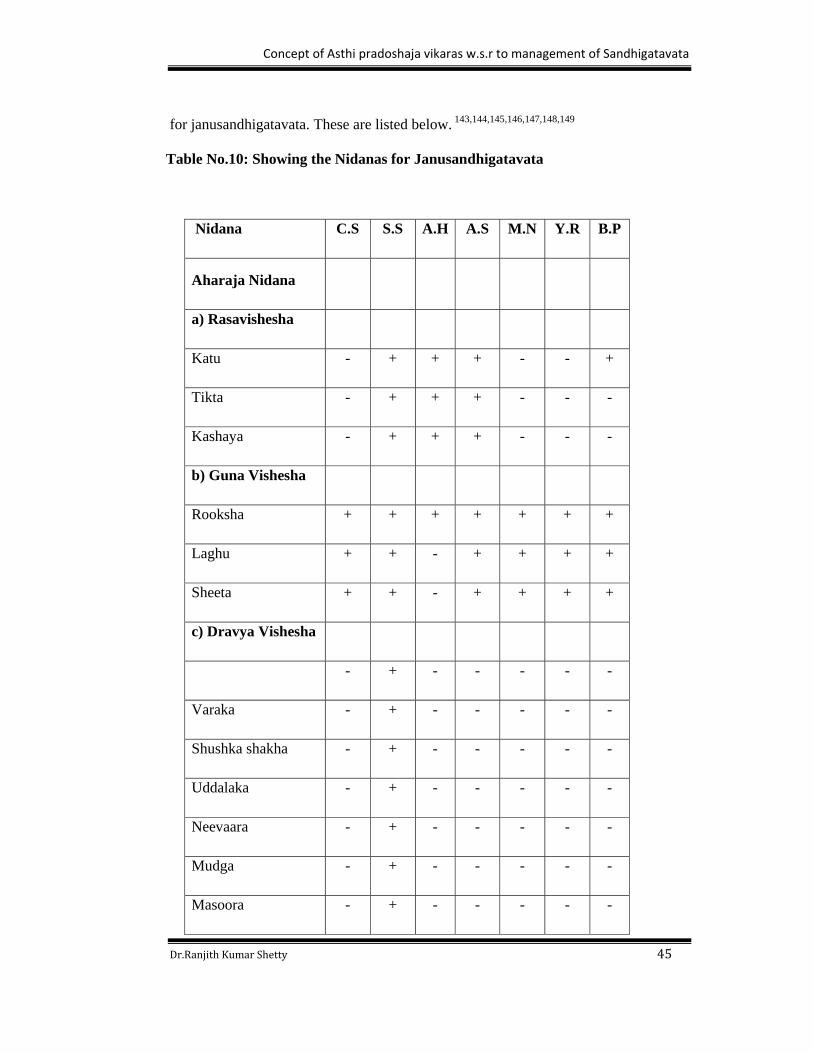
for janusandhigatavata. These are listed below. 143,144,145,146,147,148,149
Table No.10: Showing the Nidanas for Janusandhigatavata
Nidana C.S S.S A.H A.S M.N Y.R B.P
Aharaja Nidana
a) Rasavishesha
Katu - + + + - - +
Tikta - + + + - - -
Kashaya - + + + - - -
b) Guna Vishesha
Rooksha + + + + + + +
Laghu + + - + + + +
Sheeta + + - + + + +
c) Dravya Vishesha
- + - - - - -
Varaka - + - - - - -
Shushka shakha - + - - - - -
Uddalaka - + - - - - -
Neevaara - + - - - - -
Mudga - + - - - - -
Masoora - + - - - - -

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 46
Harenu - + - - - - -
Kalaaya - + - + - - -
Nishpaava - + - - - - -
Virudhaka dhanya - - - + - - -
Vistambhi dhanya - - - + - - -
Trina dhanya - - - + - - -
Chanaka - - - + - - -
Kareera - - - + - - -
Thumba - - - + - - -
Kalinga - - - + - - -
Chirbhata - - - + - - -
Bisa - - - + - - -
Shabooka - - - + - - -
Jambava - - - + - - -
Tinduka - - - + - - -
Vihara
Ativyayama + + + + + + +
Langhana + + - + + + -
Plavana + + - + + + -
Atyadhwa + + - + + + -
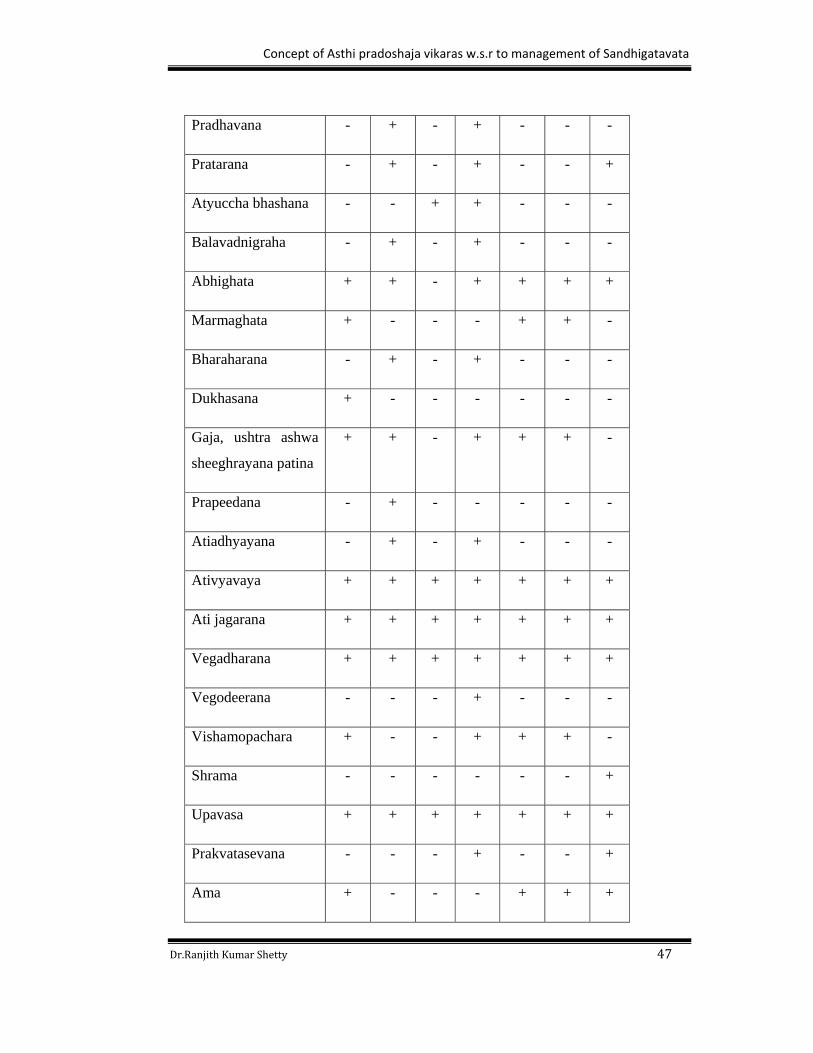
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 47
Pradhavana - + - + - - -
Pratarana - + - + - - +
Atyuccha bhashana - - + + - - -
Balavadnigraha - + - + - - -
Abhighata + + - + + + +
Marmaghata + - - - + + -
Bharaharana - + - + - - -
Dukhasana + - - - - - -
Gaja, ushtra ashwa
sheeghrayana patina
+ + - + + + -
Prapeedana - + - - - - -
Atiadhyayana - + - + - - -
Ativyavaya + + + + + + +
Ati jagarana + + + + + + +
Vegadharana + + + + + + +
Vegodeerana - - - + - - -
Vishamopachara + - - + + + -
Shrama - - - - - - +
Upavasa + + + + + + +
Prakvatasevana - - - + - - +
Ama + - - - + + +
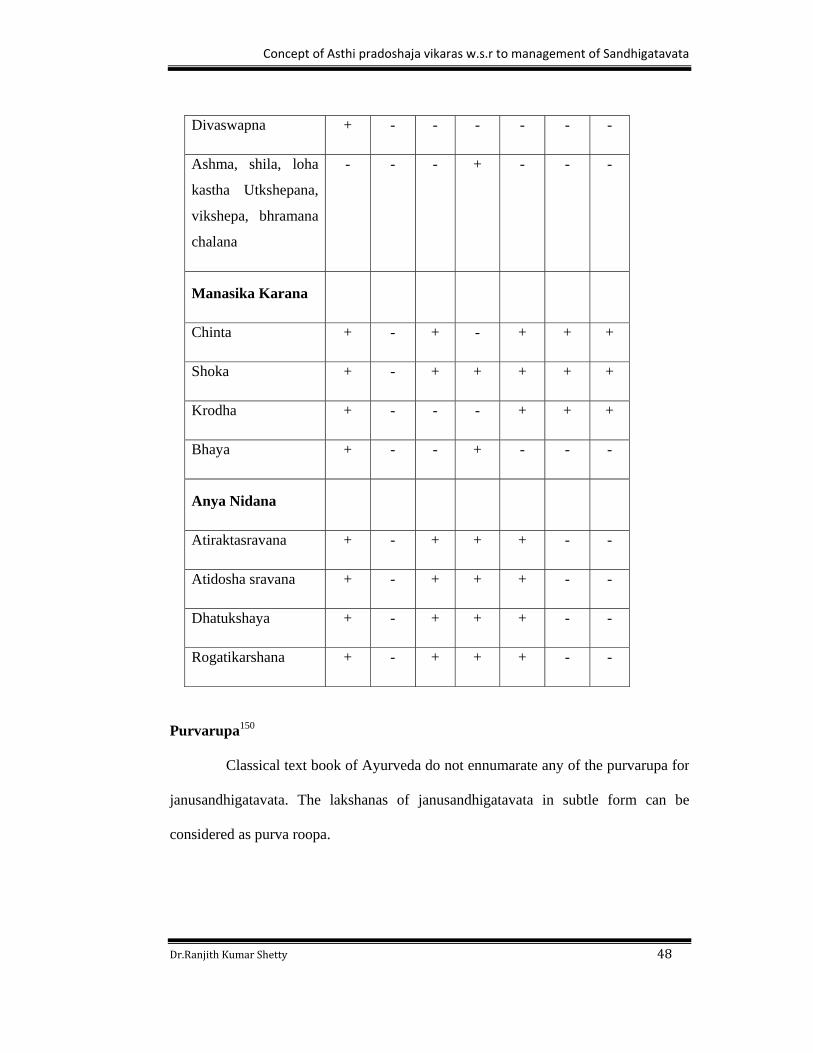
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 48
Divaswapna + - - - - - -
Ashma, shila, loha
kastha Utkshepana,
vikshepa, bhramana
chalana
- - - + - - -
Manasika Karana
Chinta + - + - + + +
Shoka + - + + + + +
Krodha + - - - + + +
Bhaya + - - + - - -
Anya Nidana
Atiraktasravana + - + + + - -
Atidosha sravana + - + + + - -
Dhatukshaya + - + + + - -
Rogatikarshana + - + + + - -
Purvarupa150
Classical text book of Ayurveda do not ennumarate any of the purvarupa for
janusandhigatavata. The lakshanas of janusandhigatavata in subtle form can be
considered as purva roopa.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 49
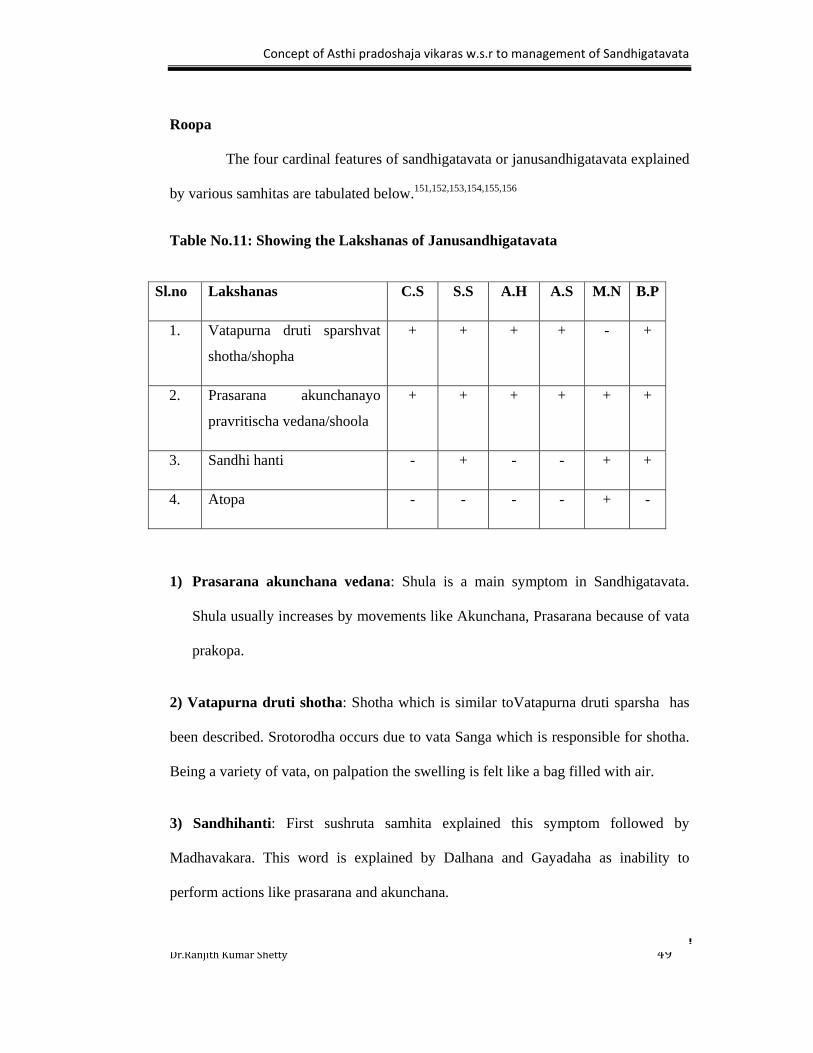
Roopa
The four cardinal features of sandhigatavata or janusandhigatavata explained
by various samhitas are tabulated below.151,152,153,154,155,156
Table No.11: Showing the Lakshanas of Janusandhigatavata
1) Prasarana akunchana vedana: Shula is a main symptom in Sandhigatavata.
Shula usually increases by movements like Akunchana, Prasarana because of vata
prakopa.
2) Vatapurna druti shotha: Shotha which is similar toVatapurna druti sparsha has
been described. Srotorodha occurs due to vata Sanga which is responsible for shotha.
Being a variety of vata, on palpation the swelling is felt like a bag filled with air.
3) Sandhihanti: First sushruta samhita explained this symptom followed by
Madhavakara. This word is explained by Dalhana and Gayadaha as inability to
perform actions like prasarana and akunchana.
Sl.no Lakshanas C.S S.S A.H A.S M.N B.P
1. Vatapurna druti sparshvat
shotha/shopha
+ + + + - +
2. Prasarana akunchanayo
pravritischa vedana/shoola
+ + + + + +
3. Sandhi hanti - + - - + +
4. Atopa - - - - + -
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 50
4) Atopa: Atopa means gud-gudaya shabda. That means there will be peculiar type
of sound in the sandhi during movemensts. This is mentioned in madhava nidana.
Samprapti 157,158
Sandhigatavata has not been explained in classics of ayurveda. It is explained
under the heading of the Vata Vyadhi. So samanya samprapti of vatavyadhi can be
considered the samprapti of sandhigatavata or janusandhigatavata.
The aggravated vata pervades into the rikta srotus in the body and produces various
disorders either generalized (pertaining to entire body) or localized (single part of
body). Here the term rikta srotus refers to snehadiguna shunya.
According to Ashtanga hrudaya, dhatukshaya aggravates vata and also
responsible for to produce rikta srotus. Vitiated vata travels throughout the body and
settles in the rikta srotus and further vitiates the srotus leading to the manifestation of
vatavyadhi. When this type of process occurs in the janu sandhi it leads to the
manifestation of janusandhigatavata.
Upashaya
All drugs, diet and regimen which give long lasting relief in Sandhigatavata
may be taken as Upashaya. For example; Abhyanga, Swedana, Ushna Ahara, Ushna
Ritu etc.
Anupashaya
All drugs, diet and regimen which exaggerate the disease are taken as
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 51
Anupashaya for that disease. Also Hetus of that disease can also be taken as
Anupashaya. The diet having Laghu, Ruksha, Sheeta Gunas, Anashana, Alpashana,
Sheeta Ritu, can be considered as Anupashaya.
Sadhyasadhyata159
Sandhigata Vata is a kashta sadhya vyadhi.
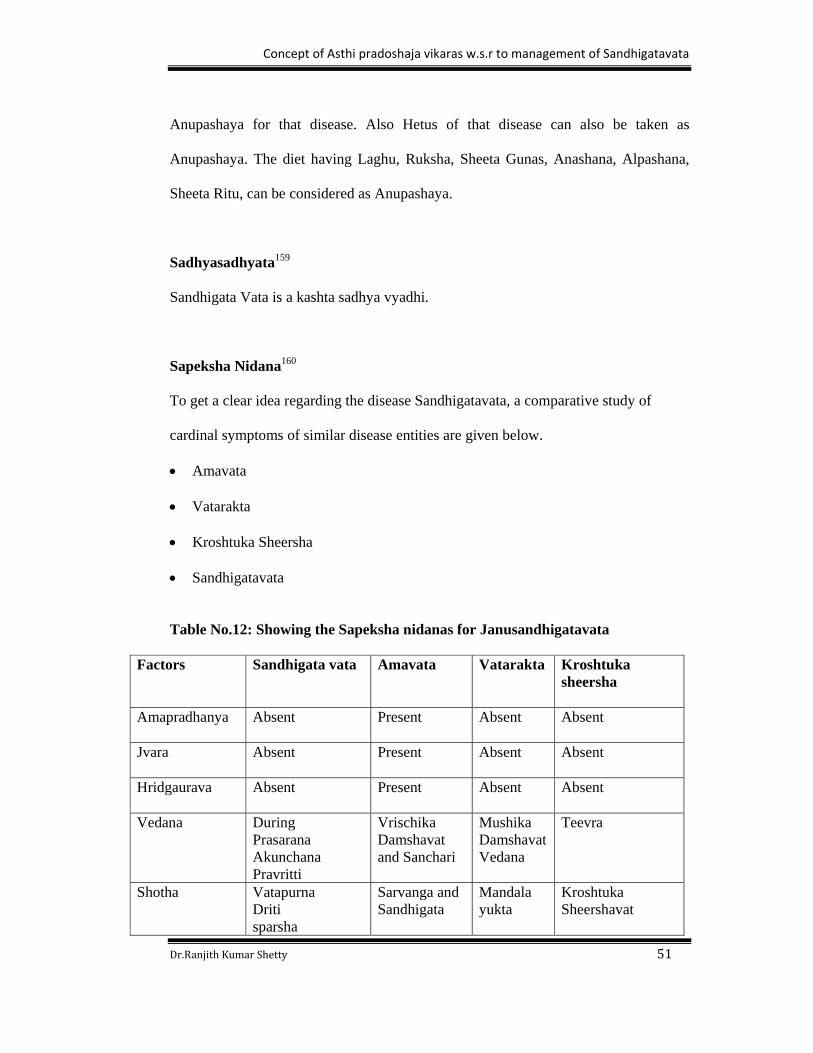
Sapeksha Nidana160
To get a clear idea regarding the disease Sandhigatavata, a comparative study of
cardinal symptoms of similar disease entities are given below.
Amavata
Vatarakta
Kroshtuka Sheersha
Sandhigatavata
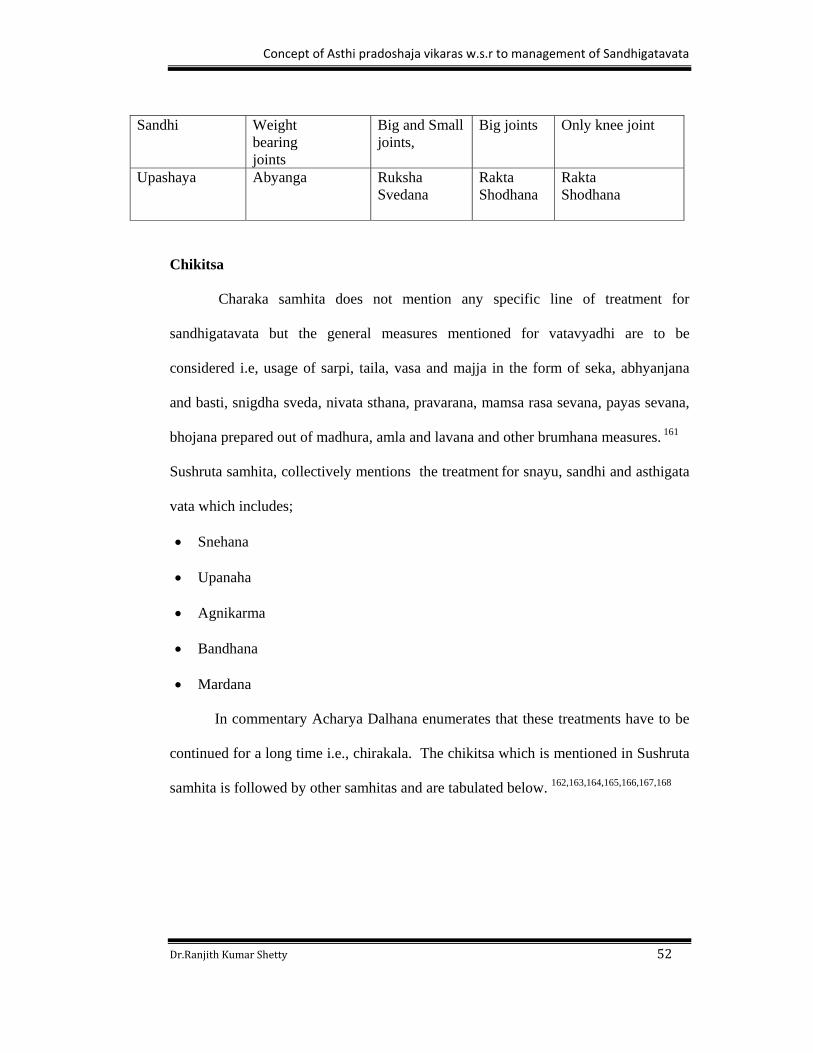
Table No.12: Showing the Sapeksha nidanas for Janusandhigatavata
Factors
Sandhigata vata Amavata Vatarakta Kroshtuka sheersha
Amapradhanya
Absent Present Absent Absent
Jvara
Absent Present Absent Absent
Hridgaurava
Absent Present Absent Absent
Vedana
During Prasarana Akunchana Pravritti
Vrischika Damshavat and Sanchari
Mushika Damshavat Vedana
Teevra
Shotha
Vatapurna Driti sparsha
Sarvanga and Sandhigata
Mandala yukta
Kroshtuka Sheershavat
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 52
Sandhi
Weight bearing joints
Big and Small joints,
Big joints
Only knee joint
Upashaya
Abyanga Ruksha Svedana
Rakta Shodhana
Rakta Shodhana
Chikitsa
Charaka samhita does not mention any specific line of treatment for
sandhigatavata but the general measures mentioned for vatavyadhi are to be
considered i.e, usage of sarpi, taila, vasa and majja in the form of seka, abhyanjana
and basti, snigdha sveda, nivata sthana, pravarana, mamsa rasa sevana, payas sevana,
bhojana prepared out of madhura, amla and lavana and other brumhana measures. 161
Sushruta samhita, collectively mentions the treatment for snayu, sandhi and asthigata
vata which includes;
Snehana
Upanaha
Agnikarma
Bandhana
Mardana
In commentary Acharya Dalhana enumerates that these treatments have to be
continued for a long time i.e., chirakala. The chikitsa which is mentioned in Sushruta
samhita is followed by other samhitas and are tabulated below. 162,163,164,165,166,167,168
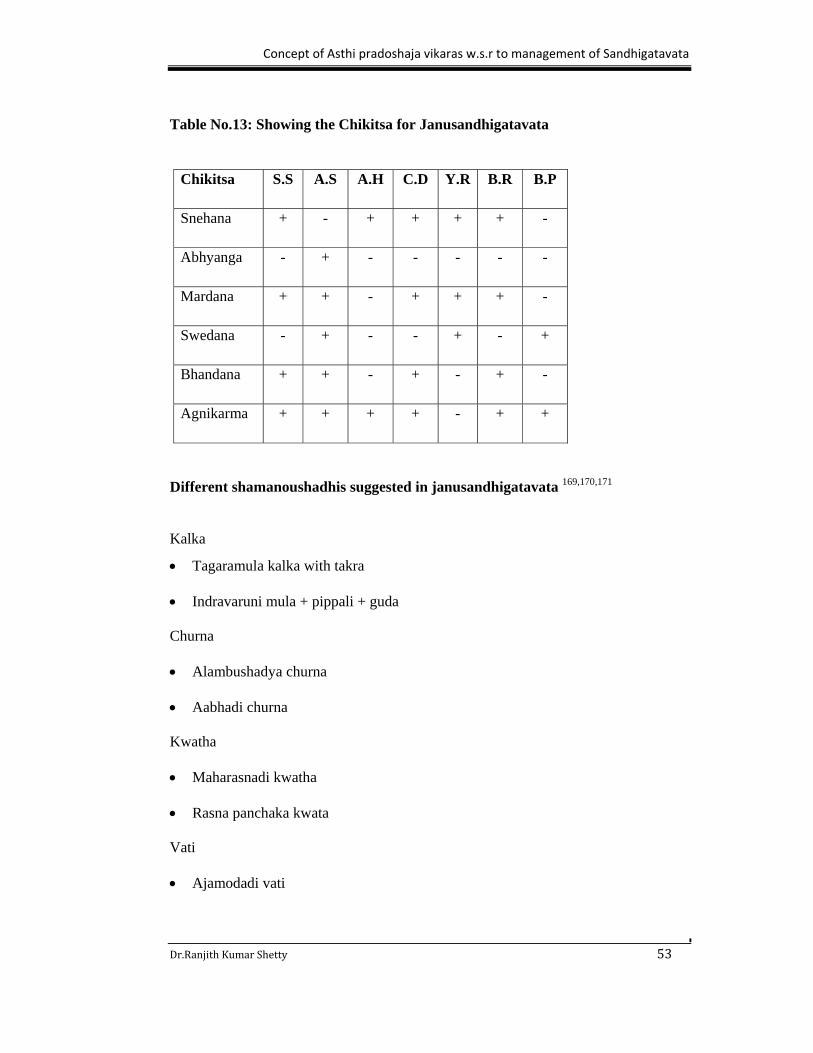
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 53
Table No.13: Showing the Chikitsa for Janusandhigatavata
Different shamanoushadhis suggested in janusandhigatavata 169,170,171
Kalka
Tagaramula kalka with takra
Indravaruni mula + pippali + guda
Churna
Alambushadya churna
Aabhadi churna
Kwatha
Maharasnadi kwatha
Rasna panchaka kwata
Vati
Ajamodadi vati
Chikitsa S.S A.S A.H C.D Y.R B.R B.P
Snehana + - + + + + -
Abhyanga - + - - - - -
Mardana + + - + + + -
Swedana - + - - + - +
Bhandana + + - + - + -
Agnikarma + + + + - + +
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 54
Guggulu
Adityapaka guggulu
Trayodashanga guggulu
Yogaraja guggulu
Yogaraja guggulu brihat
Shodasheeti guggulu
Simhanada guggulu
Rasaushadi
Panchananarasa lauha
Vatarakshasa rasa
Sneha
Phalatrikadi sneha
Dashamula siddamajja sneha
Majja sneha
Panchatikta guggulu ghrita
Prasarani taila
Vishnu taila
Siddartha taila
Pathyapathya172,173
According to this general rule of Pathyapathya, the nidanas, which cause the diseases,

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 55
are to be considered as apathya. Hence in this study the nidanas, which have been
described earlier, are apathya for the patients of janusandhigatavata.
Pathya Ahara – Internal and external use of Sneha, viz. ghrita, taila, vasa and
majja, mamsarasa, ksheera, mamsa, snehanvita bhojana, fruits having amla rasa
like dadima, recipes having madhura, amla and lavana Rasa.
Pathya Vihara – Nirvatasthana, atapa Sevana, garbhagriha, agnisantapa,
gurupravarana, mrudu shayya, brahmacharya .
Pathya Ausadha – Sukhoshna parisheka, abhyanga, snigdha sveda, basti, sneha
virechana, shiro basti, shirah sneha, snaihika dhumapana, snaihika nasya,
sukhoshna sneha gandusha, samvahana . Drugs like kumkum, agaru, tejapatra,
kustha, ela, tagara.

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 56
OSTEOARTHRITIS
Osteoarthritis is one among the common musculoskeletal diseases affecting
the human being making an important cause of disability. There is no simple
definition of osteoarthritis as it requires consideration of 3 overlapping areas-
pathological changes, radiological changes & clinical consequences. Pathologically
there is an alteration in cartilage structure; radiologically there are osteophytes & joint
space narrowing and clinically pain, disability.
Knee osteoarthritis is the most common form of osteoarthritis. It is usually
unilateral in the beginning but becomes bilateral over a period of time. Obesity,
female gender and knee bending are predominant risk factors. .It may involve
predominantly medial femorotibial, lateral femorotibial or patellofemoral
compartment.174,175
Etymology176
The term osteoarthritis is composed of two terms i.e, osteo and arthritis.
Osteo-The world Osteo comes from the Greek word ‘Osteon’.
The word osteo means bone.
Arthritis-The prefix ‘Arth’ means joint. The suffix ‘itis’ is defined as inflammation.
Hence, Arthritis means inflammation of joint.
So, Osteoarthritis can be defined as inflammation of the bony part of the joint.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 57
Synonyms177,178
The osteoarthritis has following synonyms.
Osteoarthritis
Arthrosis
Degenerative Joint Disease
Wear and Tear Arthritis
Hypertrophic Osteoarthritis.
Classification 179
1. Primary OA - is the most common form of the disease, no predisposing factor is
apparent.
2. Secondary OA- is pathologically indistinguishable from idiopathic OA. but is
attributable to an underlying cause.
Causes of osteoarthritis180
Primary OA:
No known cause.
Secondary OA
Pre-existing joint damage;
Rheumatoid arthritis
Gout
Seronegative spondyloarthropathy
Septic arthritis

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 58
Paget’s disease
Avascular necrosis e.g; corticosteroid therapy
Metabolic disease;
Chondrocalcinosis
Hereditary haem0chromatosis
Acromegaly
Systemic diseases;
Haemophilia- recurrent haemoarthrosis
Haemoglobinopathies e.g; sickle cell disease
Neuropathies
Factors predisposing to osteoarthritis181
Obesity: predicts later risk of radiological and symptomatic OA.
Hereditary: familial tendency to develop nodal and generalized OA.
Gender: polyarticular OA is more common in women; a higher prevalence after
the menopause suggests a role of sex hormones.
Hypermobility: increased range of joint movements and reduced stability leads to
OA.
Osteoporosis: commonest risk factor for OA.
Trauma: a fracture through any joint. Meniscal and cruciate ligament tears cause
OA of the knee.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 59
Congenital joint dysplasia: alters joint biomechanics and leads to OA.
Joint congruity: congenital dislocation of the hip or a slipped femoral epiphysis or
osteonecrosis causes early onset of OA.
Occupation: miners develop OA of the hip, knee and shoulder.
Sports: repetitive use and injury in some sports causes a high incidence of lower
limb OA.e.g; football.
Pathogenesis 182
Normal hyaline cartilage consists of chondrocytes embedded in extracelluar
matrix composed of water, type II collagen and proteoglycon. The cartilage remains
stable with active degeneration and regeneration occurring in equilibrium. OA results
from excessive degeneration compared to regeneration.
Earliest identifiable changes are loss of proteoglycons and decreased
metachromasia in cartilage. There is focal loss of cartilage, associated with reactive
proliferation of chondrocytes to form clusters. Progression of these changes leads to
breach of surface integrity, fissures, pitting, flaking of cartilage and development of
vertical clefts. This fissure deepens and may expose to subchondral bone, which
becomes ivory like, due to thickening and vascularisation. Associated bone growth in
subchondral region leads to sclerosis, while growth in the margin leads to the
formation of osteophytes which alters the contour of the joint and may restrict
movement.

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 60
Clinical features183
Symptoms
Joint pain
Joint gelling (stiffening & pain after immobility)
Crepitus
Joint instability
Loss of function
Signs
Joint tenderness
Crepitus on movement
Limitation of range of movement
Joint instability
Joint effusion
Wasting of muscles
Differential diagnosis184
Osteoarthritis of the knee has to be differentiated from following conditions.
Acute suppurative arthritis
Gonococcal arthritis
Tubercular arthritis
Rheumatoid arthritis
Gout
Rheumatic fever
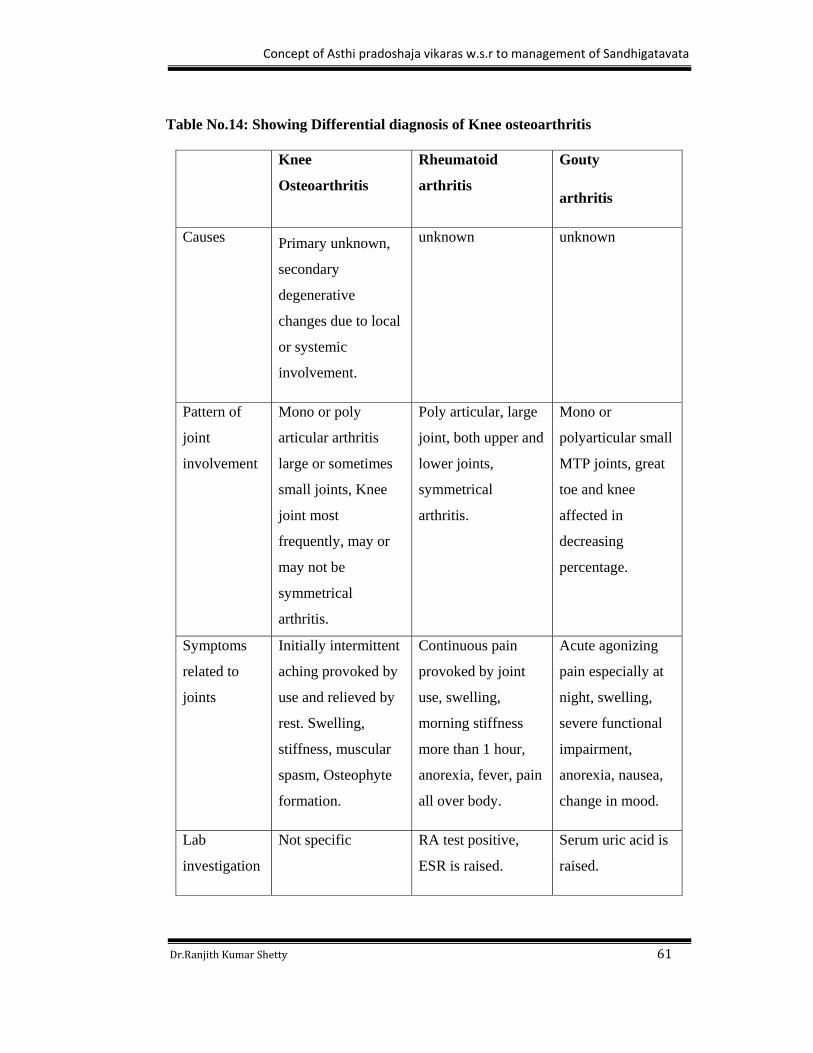
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 61
Table No.14: Showing Differential diagnosis of Knee osteoarthritis
Knee
Osteoarthritis
Rheumatoid
arthritis
Gouty
arthritis
Causes Primary unknown,
secondary
degenerative
changes due to local
or systemic
involvement.
unknown unknown
Pattern of
joint
involvement
Mono or poly
articular arthritis
large or sometimes
small joints, Knee
joint most
frequently, may or
may not be
symmetrical
arthritis.
Poly articular, large
joint, both upper and
lower joints,
symmetrical
arthritis.
Mono or
polyarticular small
MTP joints, great
toe and knee
affected in
decreasing
percentage.
Symptoms
related to
joints
Initially intermittent
aching provoked by
use and relieved by
rest. Swelling,
stiffness, muscular
spasm, Osteophyte
formation.
Continuous pain
provoked by joint
use, swelling,
morning stiffness
more than 1 hour,
anorexia, fever, pain
all over body.
Acute agonizing
pain especially at
night, swelling,
severe functional
impairment,
anorexia, nausea,
change in mood.
Lab
investigation
Not specific RA test positive,
ESR is raised.
Serum uric acid is
raised.
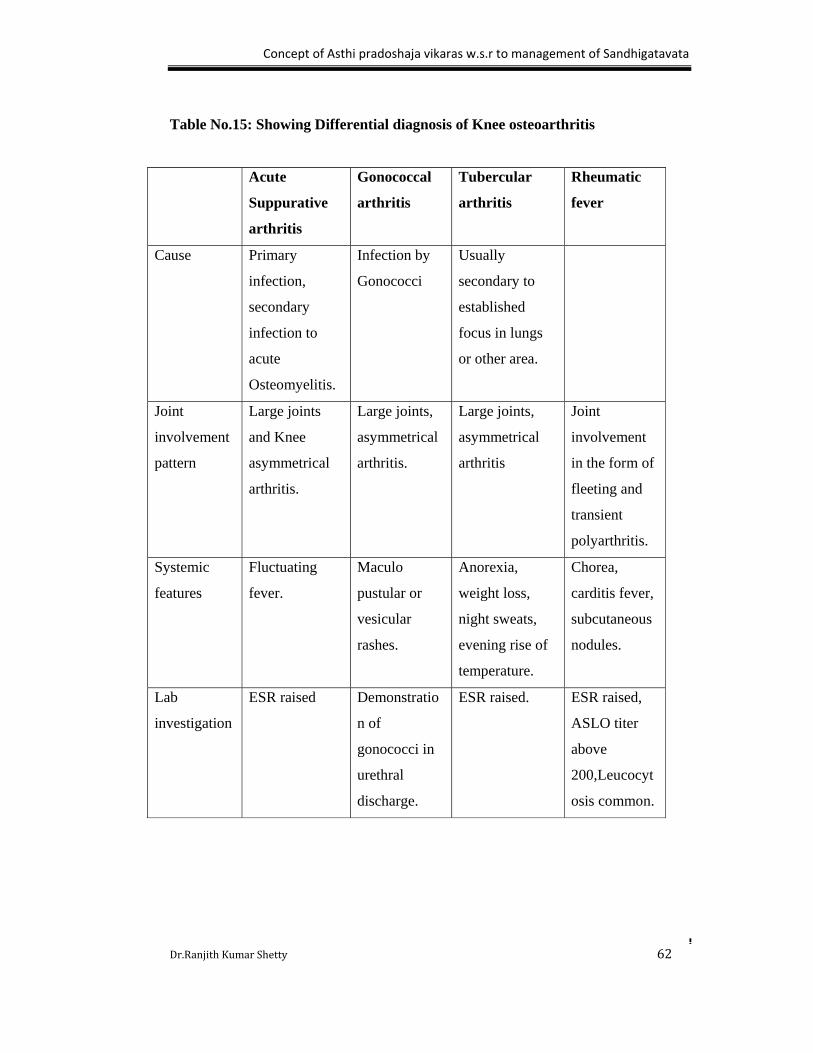
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 62
Table No.15: Showing Differential diagnosis of Knee osteoarthritis
Acute
Suppurative
arthritis
Gonococcal
arthritis
Tubercular
arthritis
Rheumatic
fever
Cause Primary
infection,
secondary
infection to
acute
Osteomyelitis.
Infection by
Gonococci
Usually
secondary to
established
focus in lungs
or other area.
Joint
involvement
pattern
Large joints
and Knee
asymmetrical
arthritis.
Large joints,
asymmetrical
arthritis.
Large joints,
asymmetrical
arthritis
Joint
involvement
in the form of
fleeting and
transient
polyarthritis.
Systemic
features
Fluctuating
fever.
Maculo
pustular or
vesicular
rashes.
Anorexia,
weight loss,
night sweats,
evening rise of
temperature.
Chorea,
carditis fever,
subcutaneous
nodules.
Lab
investigation
ESR raised Demonstratio
n of
gonococci in
urethral
discharge.
ESR raised. ESR raised,
ASLO titer
above
200,Leucocyt
osis common.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 63
Investigations 185
Primary investigations
X-rays are abnormal only when the damage is advanced; joint space narrowing
and osteophytes.
MRI demonstrates early cartilage & subchondral bone damages.
Arthroscopy reveals early fissuring & surface erosion of the cartilage.
Secondary investigations
Blood tests: there is specific tests; the ESR, rheumatoid factor & nuclear
antibodies are negative.
Management186
The treatment of OA is aimed at minimizing pain, optimizing function and reducing
disability. Management of OA requires a comprehensive approach involving non
pharmacological, pharmacological and surgical therapies.
Non – pharmocolgical therapy
Education: e.g; avoidance of poor posture.
Weight reduction
Exercises
Application of hot pack, ice pack, hydrotherapy, massage.
Uses of devices like knee brace.
Pharmacological therapy
Non steroidal anti inflammatory drugs like aceclofenac, acetaminophen celecixib.
Intra-articular steroid injections.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 64
Chondroitin and glucosamine were used as nutritional agents.
Surgical therapy
Arthroplasty; total or unicompartmental knee replacement.
Arthrodesis
Osteotomy

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 65
BASTI
Basti is the one among the major procedures in panchakarma. The classical
literatures attaches a great significance to this form of treatment and points out the
vivid scope of its applicability. Depending upon the uses of different drugs, basti act
as a dosha shodhaka, dosha shamaka, restoration of shukra, brumhana in krusha
individuals, karshana in obese individuals, improvement in vision, prevention of
aging, improvement in lusture, strength and longevity. 187
Derivation188
“ uÉxÉÑ – ÌlÉuÉxÉå oÉxÉç-AÉcNûÉSlÉå uÉxÉç –uÉÉxÉlÉå xÉÑUÍpÉMüUhÉå,
oÉÎxiÉ-uÉxiÉå: AÉuÉ×hÉÉãÌiÉ qÉÔ§ÉÇ| uÉxÉç-ÌiÉcÉç|
lÉÉpÉåUkÉÉåpÉÉaÉå qÉÔ§ÉÉkÉÉUå xjÉÉlÉ å(mÉÑ.)||
AÉæwÉkÉ SÉlÉÉjÉåï SìurÉpÉåSå|” (uÉÉcÉxmÉirÉqÉç)
The word Basti is derived from the root 'Vas' by adding 'Tich' Pratyaya and it belongs
to pullinga pada.
Means to reside, to stay or to dwell.
Means to cover/to coat.
Coating of Sneha for the elimination.
Gandha denotes bad smell hence it refers to Mala and verb 'Ardane'is derived
from Ardagatau "Yachane Cha" denotes the movement (in the colon) and to beg
(drawing of waste material in the colon from all over the body).
To produce the effect of pleasant smell.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 66
It denotes an organ, which covers the urine.
It denotes an organ situated below the umbilicus, which hold the urine.
It denotes an instrument used for the administration of the medicine.
Definition:
1. oÉÎxiÉlÉÉ SÏrÉiÉå CÌiÉ oÉÎxiÉ:| 189
2. oÉÎxiÉÍpÉ: SÏrÉiÉå rÉxqÉÉiÉç iÉxqÉÉiÉç oÉÎxiÉËUÌiÉ xqÉ×iÉ:| 190
Basti means urinary bladder of animal which were being used to introduce medication
through different routes.
Classification191
A. Depending upon Adhishthana bheda
a. Pakvashayagata
b. Garbhashyagata
c. Mutrashayagata
d. Vranagata
B. Depending upon Dravya bheda
a. Niruha basti
b. Anuvasana basti
i. Sneha basti
ii. Anuvasana basti
iii.Matra basti

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 67
C. Depending upon kaarmukata
According to Charaka samhita
a. Vataghna basti
b. Balavarnakrut basti
c. Snehaneeya basti
d. Shukrakrut basti
e. Krimighna basti
f. Vrushyatvakrut basti
According to Sushruta samhita
a. Shodhana basti
b. Lekhana basti
c. Snehana basti
d. Brhumana basti
According to Ashtanga sangraha
a. Uthkleshana basti
b. Doshahara basti
c. Shaman basti
D. Depending upon sankhya bheda
a. Karma basti
b. Kala basti
c. Yoga basti
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 68
E. Depending upon anushangika bheda
a. Yaapana basti
b. Siddha basti
c. Prasruta yogika basti
d. Dvadasha prasrutika basti
e. Paada heena basti
Kala basti
This is is a form of basti which is classified depending upon the number of
bastis, which includes both anuvasana and niruha basti.
Charaka samhita opines that Kala Basti includes half the number of Basti to that of
Karma Basti. Here, Chakrapani opines that it includes 16 Basti. On the first day 1
anuvasana is to be given then afterwards 6 anuvasana and 6 niruha can be given
alternatively. Lastly, 3 anuvasana are to be given. 192 Ashtanga hrudaya opines that
Kala Basti includes the group of 15 Basti. i.e, a group of 15 bastis, with one
anuvasana basti at the beginning and 3at the end, with 6 niruha bastis and 5 anuvasana
bastis alternatively in the middle. 193
Niruha basti
xÉ SÉåwÉ ÌlÉWïûUåiÉç zÉUÏUå SÉåwÉ WûUhÉÉSè lÉÏUÉåWû uÉÉxjÉmÉlÉqÉç AÉrÉÑ xjÉÉmÉlÉÉiÉç AxjÉÉmÉlÉqÉç|194
That which expels the doshas from the body is called as niruha, due to its
vayasthapana karma it is called as asthapana.

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 69
Anuvasana basti
AlÉÑuÉÉxÉlÉ iÉ§É rÉjÉÉ mÉëqÉÉhÉqÉç aÉÑhÉ ÌuÉÌWûiÉ: xlÉåWû oÉÎxiÉÌWû ÌuÉMüsmÉÉå AlÉÑuÉÉxÉlÉ: mÉÉSuÉM×ü¹:|195
This is the vikalpa of niruha basti but it contains more quantity of sneha hence it is
called as a sneha basti and basti dravya is quarter of niruha basti.
Yogyayogya for basti 196,197,198
Indications of niruha basti
Vataja roga, sarvanga roga, kukshi roga, bala mamsa kshaya, mutra-vata-mala sanga,
janu shoola, hrudroga, parva asthi shoola etc.
Contraindications of niruha basti
Ajeerna, athisnigdha, kshudhartha, vamita, virikta, pandu, arochaka, amadosha, kshata
ksheena, alpavarcha etc.
Indications of anuvasana basti
Which are already mentioned under the indications of niruha basti.
Contraindications of anuvasana basti
Anasthapya, navajwara, pandu, pleehodara, vishapeeta, shleepada, sthoulya, kushta,
prameha etc.
Basti yantra199
Basti yantra contains two parts. They are;
i.Basti netra
ii.Basti putaka

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 70
Basti netra
This is nalika which is connected to the basti putaka, is measures about 12 angulis (for
more than 20 years aged patients and for bellow 20 years different size is mentioned)
and it is having 2-3 karnikas.
Basti putaka
It is made up of bladder of animals or plastic bags or thick cloth or rubber bag.
Yoga-ayoga-atiyoga lakshanas of basti200,201
Niruha basti
Samyak niruha lakshanas
Prasrushta vit-mutra-vata, ruchi vriddhi, agni vriddhi, ashaya laghuta, roga upashanti,
prakruti sthapanashareera laghuta, upachaya.
Ayoga niruha lakshanas
Ruja in shira-hrudaya-nabhi-basti-guda-medhra or yoni, shotha, pratishyaya, guda
kartika, hrullasa, vata-mutra sanga, aruchi, shareera jadyata.
Atiyoga niruha lakshanas
Angasupti, angamarda, klama, kampa, nidra, dourbalya, tama pravesha, unmada,
hikka.
Anuvasana basti
Samyak anuvasana lakshanas
Snehayukta shakrut pravritti, raktadi dhatu vruddhi, indriya prasada, samyak swapna,
shareera laghuta, bala vrudhi, vega swapravruti, na osha and chosha.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 71
Ayoga anuvasana lakshanas
Ruja in adhoshareera- udara- baahu-prushta, rukshata and kharatva of shareera,
avarodha of mutra and vata, vishtabdhata of anila-vata-mutra.
Atiyoga anuvasana lakshanas
Hrullasa, moha, klama, sada, murcha, vikartika, daha, pravahana, arti, pipasa.
Basti karmukata
The basti karmukata which is explained in different classics are as follows.
When Basti is administered, the basti dravyas enters the pakwashaya which is the
main Sthana of Vata Dosha, there by sub siding the vitiated vata and destroys vikaras,
since vata dosha is responsible for all the vikaras. By sub siding the Vata, all Vikaras
located in the other parts of the body are also destroyed. This is better understood with
the help of a simile that when the root of a plant is destroyed then naturally the stem,
branches, sprouts, fruits, leaves are destroyed.
Commentator Chakrapani has quoted that Guda is the Mula of the body where all
Siras are located. So the basti dravyaas reaches siras and performs its functions. 202
The action of basti dravyas are illustrated with a simile, just as a tree fed with water at
its roots, puts forth green leaves and delicate sprouts, and in due course of time grows
into a big tree, full of blossom and fruits, similarly the basti dravyas reaches all parts
of the body and does its functions.This is further elaborated in sushruta samhita and
states that The veerya of basti dravya reachs all over the body through the srotas in the
same way as the water poured at the root of the plant reaches upto leaves. Even
though basti dravyas quickly comes out alone or with mala, their veerya acts over the
whole body by the action of Apana and the other Vayu. This action takes place just
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 72
like sun draws moisture from the earth. The method of administration of anuvasana
basti is as follows. The administration of 1st basti does the snehana of basti and
vankshana. The properly administered 2nd basti tends to restore the vayu in the
murdha bhaga to its normalcy. The 3rd basti increases the bala and varna. The 4th and
5th anuvasana basti does the snehana of rasa and rakta. The 6th and 7th basti then
nourishes the mamsa and meda. The 8th and 9th bastis nourishes the asthi and majja.
During the intervals the niruha basti should be given. 203
Basti dravyas in Pakvashaya acts on whole body in the same way as that of sun, though
placed in the sky, causes evaporation of water on the earth.The Virya (potency) of
collective Basti drug is first taken up by Apana Vayu, i.e. it acts or influences the Gunas
of Apana Vayu with which it comes in contact first.Consequently the Samana Vayu isalso
affected followed by Vyana, Prana and Udana. By the Gunas of Basti Dravya, thevitiated
Vayu regains their normal state and supports the body. They also bring vitiatedPitta and
Kapha in their normal state, and the five types of Vayu nourishs their respective Sharira-
Bhuta Guna.The Virya (potency) of Dravya (substance) is propogated by the Vyana in
Tiryak or lateral direction, by the Apana in downward direction and in upward direction
by Prana, just as water pipes carry water to the different parts of the field similarly
the“Harini” (Channels) carry the Gunas of the Basti Dravya to every part the body, hence
Basti which is appropriate will with the help of Vata, Pitta and Kapha through the Siras
will spread all over the body and cures even the most difficult disease. 204
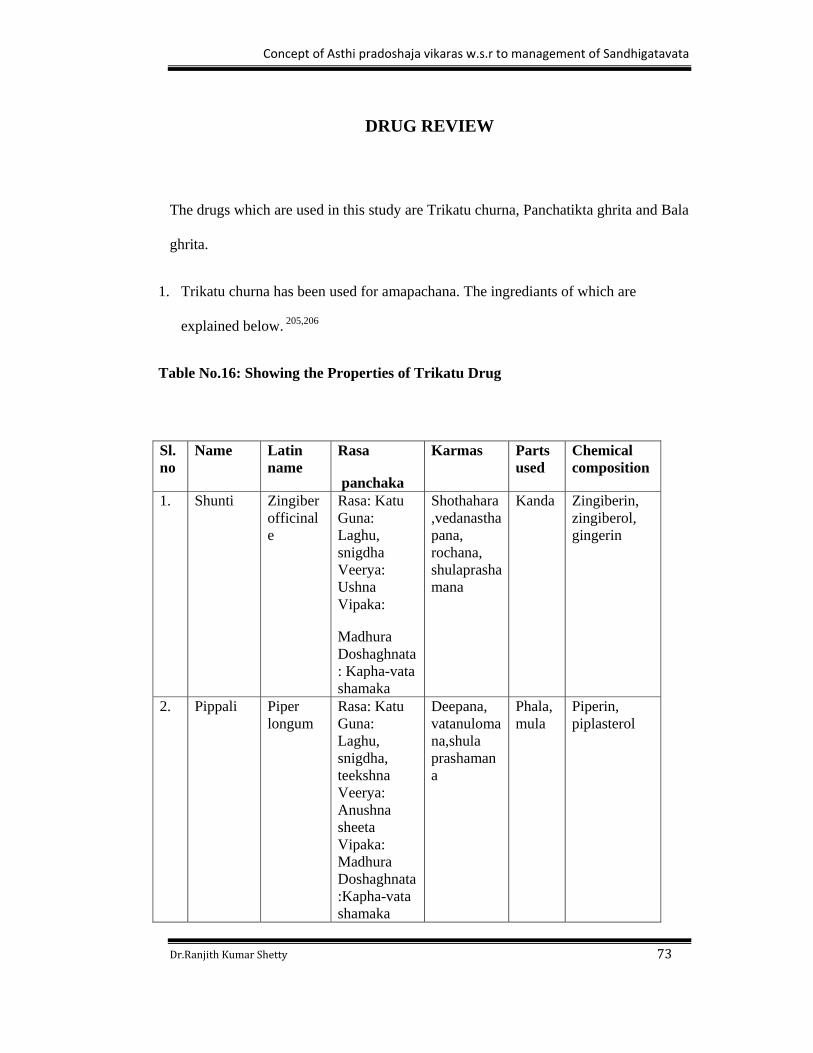
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 73
DRUG REVIEW
The drugs which are used in this study are Trikatu churna, Panchatikta ghrita and Bala
ghrita.
1. Trikatu churna has been used for amapachana. The ingrediants of which are
explained below. 205,206
Table No.16: Showing the Properties of Trikatu Drug
Sl.no
Name Latin name
Rasa
panchaka
Karmas Parts used
Chemical composition
1. Shunti Zingiber officinale
Rasa: Katu Guna: Laghu, snigdha Veerya: Ushna Vipaka:
Madhura Doshaghnata: Kapha-vata shamaka
Shothahara,vedanasthapana, rochana, shulaprashamana
Kanda Zingiberin, zingiberol, gingerin
2. Pippali Piper longum
Rasa: Katu Guna: Laghu, snigdha, teekshna Veerya: Anushna sheeta Vipaka: Madhura Doshaghnata:Kapha-vata shamaka
Deepana, vatanulomana,shula prashamana
Phala, mula
Piperin, piplasterol
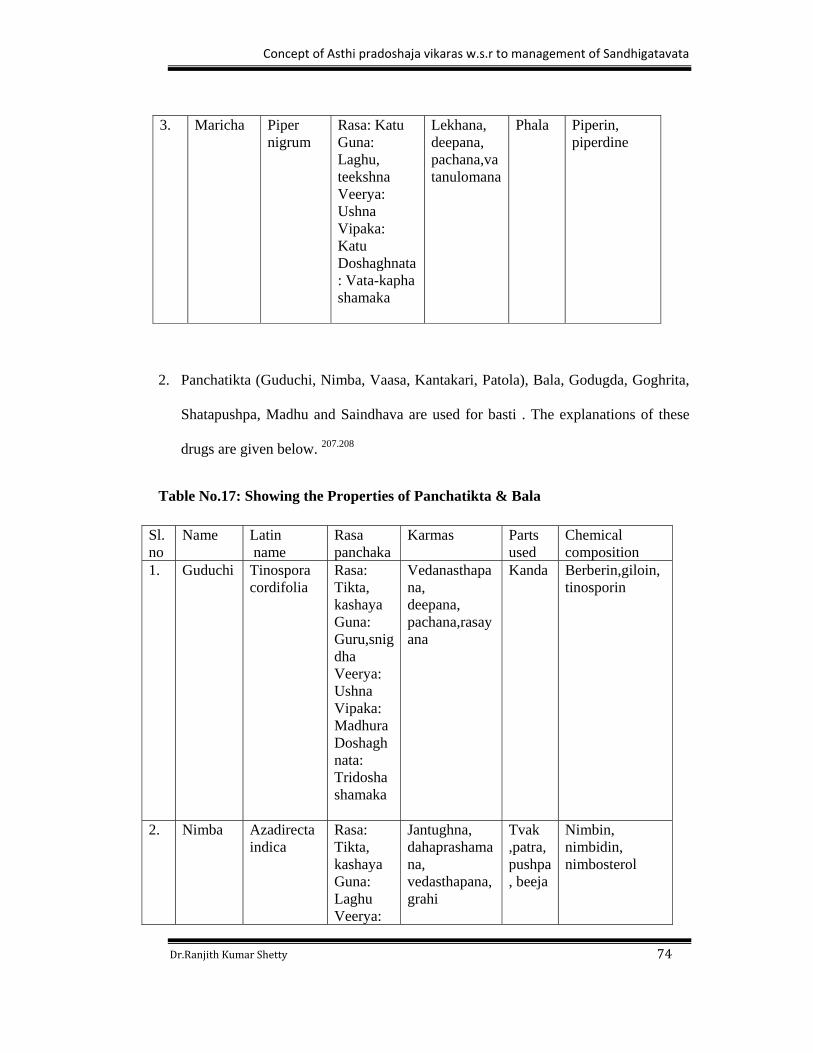
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 74
3. Maricha Piper nigrum
Rasa: Katu Guna: Laghu, teekshna Veerya: Ushna Vipaka: Katu Doshaghnata: Vata-kapha shamaka
Lekhana, deepana, pachana,vatanulomana
Phala Piperin, piperdine
2. Panchatikta (Guduchi, Nimba, Vaasa, Kantakari, Patola), Bala, Godugda, Goghrita,
Shatapushpa, Madhu and Saindhava are used for basti . The explanations of these
drugs are given below. 207.208
Table No.17: Showing the Properties of Panchatikta & Bala
Sl.no
Name Latin name
Rasa panchaka
Karmas Parts used
Chemical composition
1. Guduchi
Tinospora cordifolia
Rasa: Tikta, kashaya Guna: Guru,snigdha Veerya: Ushna Vipaka: Madhura Doshaghnata: Tridosha shamaka
Vedanasthapana, deepana, pachana,rasayana
Kanda Berberin,giloin, tinosporin
2. Nimba
Azadirecta indica
Rasa: Tikta, kashaya Guna: Laghu Veerya:
Jantughna, dahaprashamana, vedasthapana,grahi
Tvak ,patra, pushpa, beeja
Nimbin, nimbidin, nimbosterol
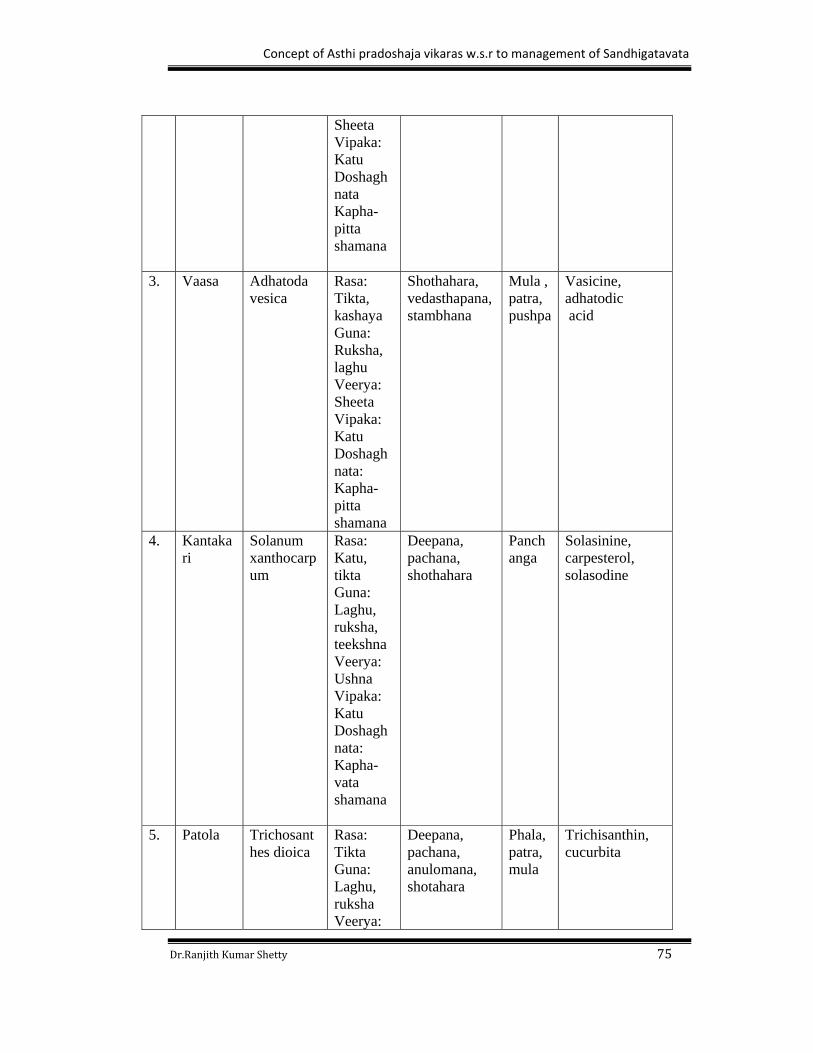
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 75
Sheeta Vipaka: Katu Doshaghnata Kapha-pitta shamana
3. Vaasa
Adhatoda vesica
Rasa: Tikta, kashaya Guna: Ruksha, laghu Veerya: Sheeta Vipaka: Katu Doshaghnata: Kapha-pitta shamana
Shothahara, vedasthapana, stambhana
Mula , patra, pushpa
Vasicine, adhatodic acid
4. Kantakari
Solanum xanthocarpum
Rasa: Katu, tikta Guna: Laghu, ruksha, teekshna Veerya: Ushna Vipaka: Katu Doshaghnata: Kapha-vata shamana
Deepana, pachana, shothahara
Panchanga
Solasinine, carpesterol, solasodine
5. Patola
Trichosanthes dioica
Rasa: Tikta Guna: Laghu, ruksha Veerya:
Deepana, pachana, anulomana, shotahara
Phala, patra, mula
Trichisanthin, cucurbita
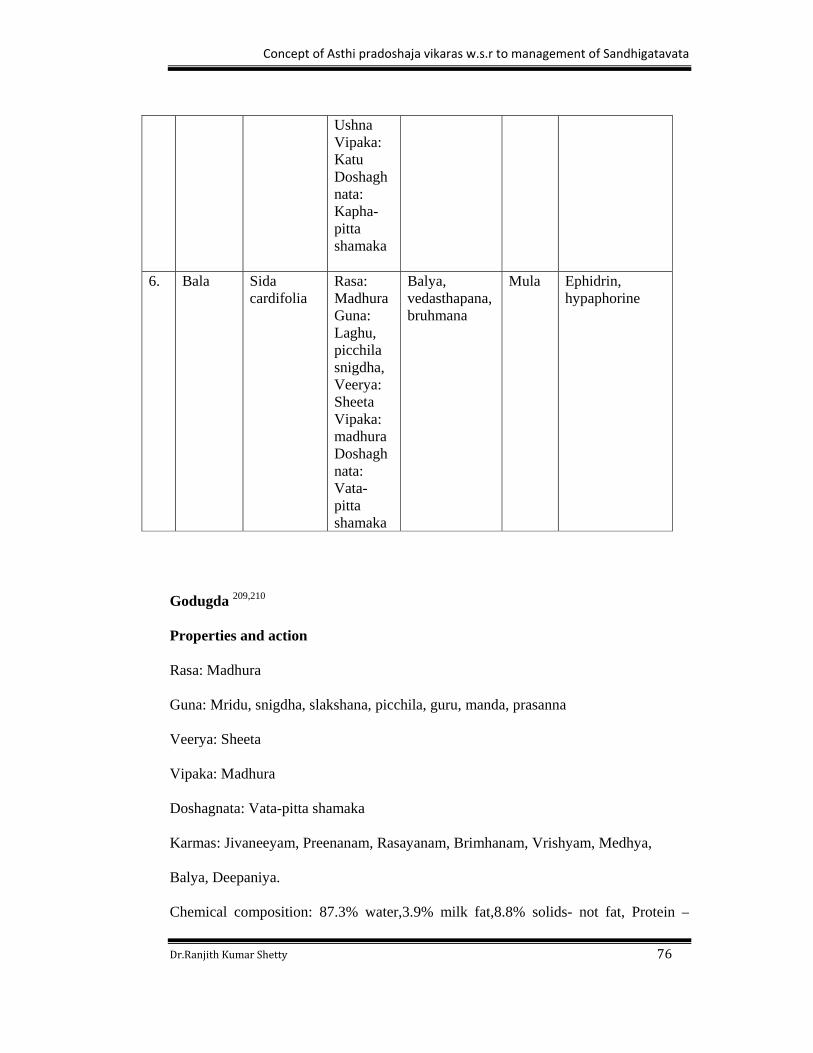
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 76
Ushna Vipaka: Katu Doshaghnata: Kapha-pitta shamaka
6. Bala Sida
cardifolia
Rasa: Madhura Guna: Laghu, picchila snigdha, Veerya: Sheeta Vipaka: madhura Doshaghnata: Vata-pitta shamaka
Balya, vedasthapana, bruhmana
Mula Ephidrin, hypaphorine
Godugda 209,210
Properties and action
Rasa: Madhura
Guna: Mridu, snigdha, slakshana, picchila, guru, manda, prasanna
Veerya: Sheeta
Vipaka: Madhura
Doshagnata: Vata-pitta shamaka
Karmas: Jivaneeyam, Preenanam, Rasayanam, Brimhanam, Vrishyam, Medhya,
Balya, Deepaniya.
Chemical composition: 87.3% water,3.9% milk fat,8.8% solids- not fat, Protein –
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 77
3.25%, Lactose – 4.6%, Minerals – 0.65% - Ca, P, Mg, K, Na, Zn, CO, Fe, Cu,
sulphates, bicarbonates, Acid – 0.18% - citrates, formates, acetate, lactate, oxalate.,
Enzymes – peroxidase, catalase, phosphatase, lipase., Gases – oxygen, nitrogen.,
Vitamins – A, C, D, thiamine, riboflavin, others.
Goghrita211,212
Biological name: Bos taurus
Properties and action
Rasa: Madhura
Guna: ,Guru, Snigdha, Mrudu, Yoghavahi,
Veerya: Sheeta
Vipaka: Madhura
Doshagnata: Vata-pitta shamaka
Karmas: Jeevaniyam, Rasayanam, Medhya, Vishanashaka, Chakshushya,
Arogyakara,Vrushya,
Chemical composition: Triglyceride (1) Saturated: Short chain (%) 37.6 Butyric 8.8,
Long chain (%) 62.4 Caproic 3.5Trisaturated (%) 39.0 Caprylic 2.2, High Melting 4.9
Capric 3.0, Partial glyceride : Lauric 8.8Diglycerides (%) 4.3 Myristic 9.9,
Monoglycerides (%) 0.7Palmitic 26.1, Phospholipids : Stearic 9.1Total cholesterol
(mg%) 330.0 High Sat 1.0, Lanosterol (mg%) 9.32 (2) Unsaturated, Lutein
(microg/g 4.2 Lower unsaturated 1.8, Squalene (microg/g 59.2 Hexadecenoic 2.8,
Carotene 7.2 Oleic 24.7,Vit. A 9.2 Unsat. Polyethenoid 3.5, Vit. E 30.5.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 78
Shatapushpa 213,214
Botanical name: Anethum sowa
Properties and action
Rasa: Katu
Guna: Laghu, Teekshna,
Veerya: Ushna
Vipaka: Katu
Doshaghnata: Vata-kapha shamaka
Karmas: Deepana, vedanasthapana, shothahara, anulomana
Parts used:Phala
Chemical composition: Carvone, limonene, cugenol.
Madhu215,216
Bilological name: Apis
Properties and action
Rasa: Madhura, kashaya
Guna: Sheeta, Laghu, ruksha,
Veerya: Ushna
Vipaka: Katu
Doshaghnata: Tridosha shamaka
Karmas: Chakshushya, vishahara
Chemical composition: glucose, sucrose, alkaloids, iron, wax volatile oil, water.

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 79
Saindhava 217,218
Biological name: Rock salt
Properties and action
Rasa: Lavana
Guna: Laghu, snigdha
Veerya: Sheeta
Vipaka: Madhura
Doshagnata: Tridosha shamaka
Karmas: Deepana, pachana, rochaka, chakshushya, hrudya.
Chemical composition: Potassium, Chlorides.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 80
MATERIALS AND METHODS
It is essential to mention the materials and methods used for the study based on
which the literary and clinical work has been carried out. The materials used for the
study were categorized in to following three headings.
Materials
1. Literary
2. Drugs
a. Deepana- Pachana: Trikatu churna
b. Abhyangartha : Ksheerabala taila
c. Avuvasanartha :i. Panchtikta ghrita (Group-A)
ii.Bala ghrita (Group-B)
d. Niruhartha: Group-A: Madhu
Saindhava
Panchatikta ghrita
Shatapushpa kalka
Panchatikta ksheera paka
Group -B: Madhu
Saindhava
Bala ghrita
Shatapushpa kalka
Balamula ksheera paka
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 81
3. Instruments : i. Douche set
ii.Enema Syringe
iii.Rubber catheter
Collection of materials
A) Literary: The literary source for the present study was obtained from vedic
scriptures, classical texts of Ayurveda, western medical text books, published articles
in reputed journals and also from the various media like internet followed by
retrospective study of related research works.
B) Drugs
Panchatikta ghrita, bala ghrita, panchatikta kwatha churna, balamula kwatha
churna and shatapushpa kalka was purchased from Sri Dharmasthala
Manjunatheshwara Ayurveda Pharmacy, Kuthpady, Udupi – 574 118.
Trikatu churna and ksheerabala taila was taken from Government Ayurveda
Medical College & Hospital, Mysore.
Honey was purchased from B.R. hills, Chamarajanagar district.
Saindhava lavana was purchased from Govindraj setty & sons, D.D.Urs. Road
Mysore.
Fresh Ksheera was purchased from Nandini dairy Mysore.
C) Instruments
Douche set (Basti pranidhanartha)
Douche set contents:
1. Douche can- with 1000ml capacity
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 82
2. Douche tube with 2 openings and length about 41/2 inches long and 6mm diameter.
3. Douche F set containing two units 1st unit which is attached to the douche tube, it
has a valve at proximal end to maintain the flow.
4. Second unit which is attached to the 1st unit at proximal end and distal end is blunt
and is has got two lateral and one distal openings, both will measure about four
inches long and one and half mm diameter.
5. Assembly and calibrations of douche set.
i. All the units of douche set were properly sterilized and dried.
ii. Douche tube is connected firmly to the exit nozzle at the bottom of the douche can.
iii. The distal end of the tube was properly conncted to the 1st unit of ‘F’ set which
connects the wall.
iv. Nozzle part of the douche ‘F’ set was connected with 1st unit of the ‘F’ set.
Collabartion of the Douche set
1. The prepared basti dravya was carefully poured into the douche can and held it
vertically.
2. The valve was opened and the drawn basti dravya was allowed to flow through the
tube and ‘F’ set easily.
3. Precaution was taken to remove all the air present in tube and ‘F’ set.
4. Keeping it vertical the basti dravya was made to flow till it reaches the required
level marked on douche can.
5. Then the valve was closed.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 83
Methodology
Basti dana vidhi- Basti dana vidhi includes purva karma, pradhana karma and paschat
karma.
Purva karma
1. Examination of patients: Dosha, oushadha, desha, kala, satmya, agni, sattva, oka,
vaya and bala, are examined before administration of basti.
2. Preparation of the medicine.
3. Matra nirnaya: Matra of anuvasana and niruha basti was fixed to 80ml and 600ml
respectively. The ingredients are as follow.
Anuvasanartha dravya
i.For Group A: Panchatikta ghrita - 80ml
ii. For Group B: Balaghrita -80ml.
Niruhartha dravya
i.For Group-A
Madhu- 50ml
Saindhava- 5gm
Panchatikta ghrita- 80ml
Shatapushpa kalka- 5gm
Panchatikta ksheera paka- 450ml
Total -600ml
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 84
ii. For Group-B
Madhu- 50ml
Saindhava- 5gm
Bala ghrita- 80ml
Shatapushpa kalka- 5gm
Balamula ksheera paka- 450ml
Total – 600ml
Mixing of basti dravya
Mixing of basti dravya is done according to the quotation
‘makshikam lavanam sneham kalkam kwatham’.
Deepana – Pachana
The amapachana is essential before administration of basti. Trikatu churna was
administered for ama pachana to all the patients.
Pradhana karma
This includes basti pranidhana vidhi.
Anuvasana bastipranidana vidhi
Snehana & swedana
Patient was subjected for abhyanga by ksheerabala taila for 15 mins and swedana for
10 mins.
Basti poorva bhojana
Specially cooked rice was administered in precise quantity before administration of
anuvasana basti.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 85
Procedures of basti pranidhana
Anuvasana basti procedure
Position
Patient was made to lie on the table in left lateral position with left lower
extremity straight and right lower extremity flexed on knee and hip joint and
asked the patient was asked to keep head on his flexed left hand.
Oleation of anus was done by applying the ghrita.
Patient was asked to take deep breath while administration of basti.
Assembled and clabbered douche set was taken and the douche can was kept 4ft
height from the patient.
Ghrita was applied to the 2nd unit of douche F set and was slowly introduced in to
the anus and valve was opened.
Valve was closed when can becomes empty and some quantity of medicine was in
tube.
Precautions were taken to avoid shivering of hands, quicker insertion and too slow
insertion.
The douche F set 2nd unit was removed slowly and asked the patient was asked to
remain in the same posture for 1min.
After that, patient was asked to lie down in supine position and mardana was done
over the udara, paada and hasta.
Then patients were advised to take rest and eliminate mala when there is an urge
and time was recorded.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 86
Paschat karma
Basti pratyagamana and nireekshana
a. Duration of elimination of basti is known as basti pratyagamana kala
(Su.chi.38/5). The kala is one muhurtha (48 mins) for niruha basti and for
anuvasana upto 24 hours and patient was kept under observation for any
complication.
b. Patients were advised to take prescribed food on feeling hungry.
c. Patients were asked to avoid the following.
i.Aharaja: apathya, adhika matrayukta, guru, sheeta and ati snigdha etc.
ii.Vihara: maithuna, apathya vihara.
Niruha basti procedure
On next day morning patients were asked to eliminate mala and mootra.
The patients were examined for complications if any.
Ksheerabala taila abhyanga was done properly for 15mins and swedana by nadi
sweda for 10 mins.
Niruha basti medicines were properly prepared mixed in the manner of
makshikam lavanam sneha kalka & kwatha.
Procedure of administration of basti- the anuvasana basti procedure was followed
by the niruha basti, only basti poorva ahara was not administered.
Like above procedure on 3rd, 5th, 7th, 9th, 11th, 13th, 14th, 15th day anuvasana basti
was administered and on 2nd, 4th, 6th, 8th,10th and 12th day niruha basti was
administered.

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 87
Samsarjana karma
For basti karma there is no such reference of samsarjana karma as advised in vamana
and virechana, but patients were advised to take restricted ahara and vihara and avoid
the pariharya vishayas for 30 days. Advised ahara are only laghu and ushna ahara,
mainly dugda yukta yavagu or dugda yukta anna. Vihara – bed rest and pariharya
vishayas- to avoid astamaha doshakara vishayas i.e;
i.Avoid sitting, standing posture for long time.
ii.Avoid excessive talking, travelling, day sleep, vega dharana, sheetopachara, atapa
sevana.
iii. Avoid shoka, krodha.
iv.Avoid akala and ahita ahara.
v.Avoid astanga maithuna.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 88
METHODS
Aim
The present work was under taken for the analytical study of asthi pradoshaja vikaras
supported by the study on the effect of panchatikta ksheera sarpi and bala sadhita
ksheera sarpi in sandhigatavata.
Objectives of the study
To review in detail about asthi and asthi pradoshaja vikaras.
To assess the involvement of asthi with the help of radiology (x-ray).
To assess the role of asthi in manifestation of sandhigatavata.
To study the role of tiktaka dravyas in the management of sandhigatavata.
Research Design
A comparative literary study of Ayurvedic literature on asthipradoshaja vikaras
with current updated view (western medicine).
A comparative clinical study where the incidentally selected patients were
systematically allotted to Group A and B respectively.
Source of the patients
Patients of either sex diagnosed as janusandhigatavata were selected from the O.P.D
and I.P.D of GAMC Hospital Mysore. A special free camp was conducted for
janusandhigatavata in the campus of GAMC Hospital Mysore.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 89
Selection criteria
Patients were diagnosed as janusandhigatavata after preliminary examination.
Patients were selected with respect to age and irrespective of sex, caste,
occupation and socioeconomic status.
Patients fulfilling inclusion criteria.
Patients willing to participate in the study were selected by explaining them the
intervention in detail.
Inclusion criteria
The individuals having janusandhigatavata lakshanas will be selected.
The individuals yogya for basti will be selected.
The individuals of either sex between the age group 30-60 years will be selected.
Exclusion criteria
Any other systemic disorders which interferes the course of treatment will be
excluded.
Pregnant women will be excluded.
Diagnostic criteria
Subjective parameters
Vedana
Shotha
Atopa
Stabdhata
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 90
Objective parameters
Antalogic gait
Osteophytes
Bony swelling around the joint
Sampling Method
Systemic method was adopted for group A and B, patients No.1 and 2 respectively
were fixed as a starting number and uniform difference of the two patients were
maintained for each group till the required size of 15 patients for each group was
attained.
Investigation
Following investigation was performed before treatment, after treatment and at the
end of the follow up to assess the severity and clinical improvement respectively.
X-ray of knee joint.
Intervention
The intervention of clinical study was carried according to the individual group as
mentioned below.
Group-A
The patients of group A were administered with trikatu churna in appropriate
doses for deepana and pachana till niramavastha was attained.
After attaining niramavastha patient was aubjected to abhyanga (udara, kati and
janusandhi) with ksheerabala taila followed by nadi sweda.

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 91
The sequence of 15 bastis in the form of kala basti was administered starting from
anuvasana with panchatikta ghrita (total 9 anuvasana basti) and niruha basti with
panchatikta ksheera sarpi (total 6 niruha basti) by maintaining the proper duration
between them and performing abhyanga and swedana before each basti. After
pratyagamana of each basti patients were advised to take cooked rice and maintain
the pariharya vishayas.
Group-B
The patients of group B were administered with trikatu churna in appropriate
doses for deepana and pachana till niramavastha was attained.
After attaining niramavastha patients were subjected to abhyanga (udara, kati and
janusandhi) with ksheerabala taila followed by nadi sweda.
The sequence of 15 bastis in the form of kala basti were administered starting
from anuvasana with bala ghrita (total 9 anuvasana basti) and niruha basti with
bala sadhita ksheera sarpi (total 6 niruha basti) by maintaining the proper duration
between them and performing abhyanga and swedana before each basti. After
pratyagamana of each basti patients were advised to take cooked rice and maintain
the pariharya vishayas.
Assessment criteria
The results were evaluated by subjective and objective criteria mainly based on
clinical observation by grading method.
Shoola /pain
Grade0: No pain.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 92
Grade1: Mild pain (working for 8hrs pain starts & reduces after 1/2hr rest)
Grade2: Moderate pain (working for 4hrs pain starts & reduces after 1hr rest)
Grade3: Severe pain (working for an 1hr pain starts &does not subside even after
taking rest)
Shotha/swelling
Grade0: No swelling.
Grade1: Mild swelling (working for 8hrs swelling starts & reduces after 1/2hr rest)
Grade2: Moderate swelling (working for 4hr swelling starts & reduces after 1hr rest)
Grade3: Severe swelling (working for an 1hrs swelling starts &does not subsides even
after taking rest)
Stabdatha/stiffness
Grade0: No stiffness.
Grade1: Mild stiffness (knee flexion upto 100-120 degree & no difficulty in walking)
Grade2: Moderate stiffness (knee flexion upto 80-100 degree & slight difficulty in
walking)
Grade3: Severe stiffness ((knee flexion upto 60-80 degree & difficulty in walking)
Atopa/crepitus
Grade0: No crepitation.
Grade1: Palpable crepitus
Grade2: Palpable + Audible crepitus
Grade3: Crepitus always audible
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 93
X-ray changes
Grade0: Normal knee joint (no loss of cartilage & no deformation).
Grade1: Mild changes (some loss of articular cartilage, minute osteophytes, joint
space narrowing <3mm)
Grade2: Moderate changes (rough edges, definite osteophytes, moderate bone
attrition <5mm)
Grade3: Severe changes (definite deformity of bone ends, definite osteophytes with
severe joint space >5mm)
Overall assessment
Based on the grading given in the assessment criteria the improvement will be
assessed as below.
Complete remission, all signs and symptoms relieved.
Marked improvement, all signs and symptoms brought to the lower grading than
before.
Moderate improvement, at least three signs and symptoms brought to the lower
grade than before.
Minor improvement, at least two signs and symptoms brought to the lower grade
than before.
No improvement, all signs and symptoms persisting.
Statistical Analysis to assess Individual and comparative effects of the groups was
done using Chi- Square test, Contingency Co-efficient Test and Descriptive statistics.
All the statistical methods were carried out through the SPSS (Statistical presentation
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 94
system software) for Windows (version 16.0).
Data Collection
Data was collected before treatment, after treatment and at the end of follow up.

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 95
OBSERVATIONS
Total 30 patients coming under the inclusion criteria were randomly taken for the
clinical study and made into group A and B. Observations in the present study were
done in three stages.
i) General Observations for all the patients
ii) Observations during intervention
iii) Observation on results
General observations
In the present study total 32 patients were registered, out of which 2 patients
discontinued the treatment during various stages of the clinical study and with 30
patients the clinical study was completed.
Age
Table No.18: Showing distribution of patients according to Age
Age No. of patients Percentage (%)
30-40yrs 5 16.7%
41-50yrs 15 50.0%
51-60yrs 10 33.3%
In present study there was limitation for age. The patients of the age between 30-60
years were selected. It was found that the patients of age group between 30-40 years
were 5 (16.77%) 41-50 years were 15 (50.0%) and 51-60years were 10(33.3%).

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 96
Sex
Table No.19: Showing distribution of patients according to Sex
Sex No. of patients Percentage (%)
Males 9 30.0%
Females 21 70.0%
In the present study it was observed that more number of patients were females i.e.21,
(70.0%) and male patients were 9 (30.0%).
Marital status
Table No.20: Showing distribution of patients according to Marital status
Marital status No. of patients Percentage (%)
Married 29 96.66%
Unmarried 1 3.33%
In the present study it was observed that majority of patients were married .i.e. 29
(96.66%) and unmarried were only 1 (3.33%).
Education
Table No.21: Showing distribution of patients according to Education
Education No of patients Percentage (%)
Illiterate 8 26.66%
Primary school 7 23.33%
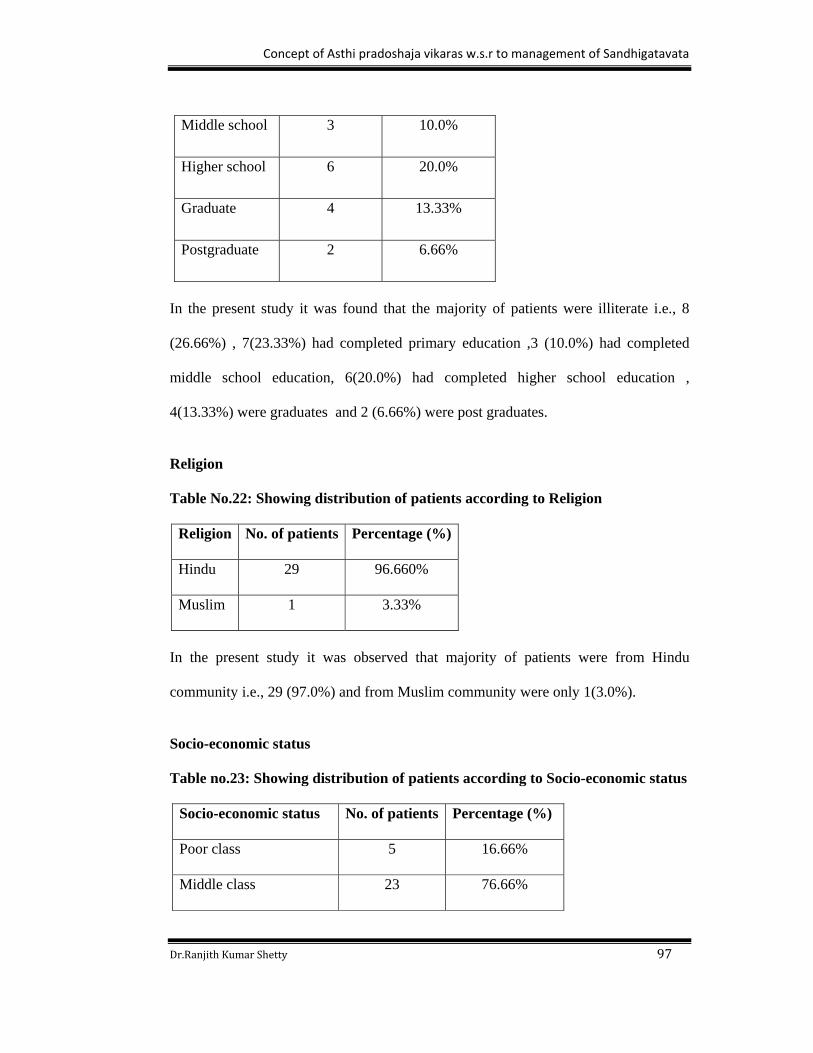
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 97
Middle school 3 10.0%
Higher school 6 20.0%
Graduate 4 13.33%
Postgraduate 2 6.66%
In the present study it was found that the majority of patients were illiterate i.e., 8
(26.66%) , 7(23.33%) had completed primary education ,3 (10.0%) had completed
middle school education, 6(20.0%) had completed higher school education ,
4(13.33%) were graduates and 2 (6.66%) were post graduates.
Religion Table No.22: Showing distribution of patients according to Religion
Religion No. of patients Percentage (%)
Hindu 29 96.660%
Muslim 1 3.33%
In the present study it was observed that majority of patients were from Hindu
community i.e., 29 (97.0%) and from Muslim community were only 1(3.0%).
Socio-economic status
Table no.23: Showing distribution of patients according to Socio-economic status
Socio-economic status No. of patients Percentage (%)
Poor class 5 16.66%
Middle class 23 76.66%
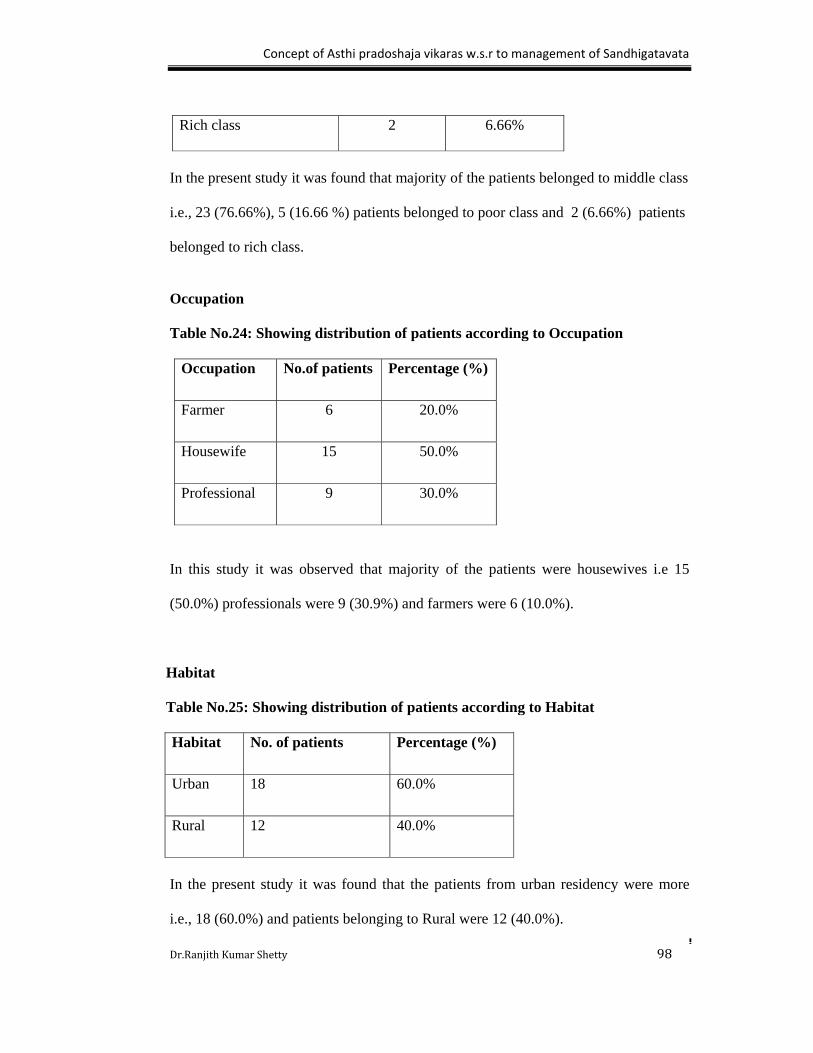
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 98
Rich class 2 6.66%
In the present study it was found that majority of the patients belonged to middle class
i.e., 23 (76.66%), 5 (16.66 %) patients belonged to poor class and 2 (6.66%) patients
belonged to rich class.
Occupation
Table No.24: Showing distribution of patients according to Occupation
Occupation No.of patients Percentage (%)
Farmer 6 20.0%
Housewife 15 50.0%
Professional 9 30.0%
In this study it was observed that majority of the patients were housewives i.e 15
(50.0%) professionals were 9 (30.9%) and farmers were 6 (10.0%).
Habitat
Table No.25: Showing distribution of patients according to Habitat
Habitat No. of patients Percentage (%)
Urban 18 60.0%
Rural 12 40.0%
In the present study it was found that the patients from urban residency were more
i.e., 18 (60.0%) and patients belonging to Rural were 12 (40.0%).
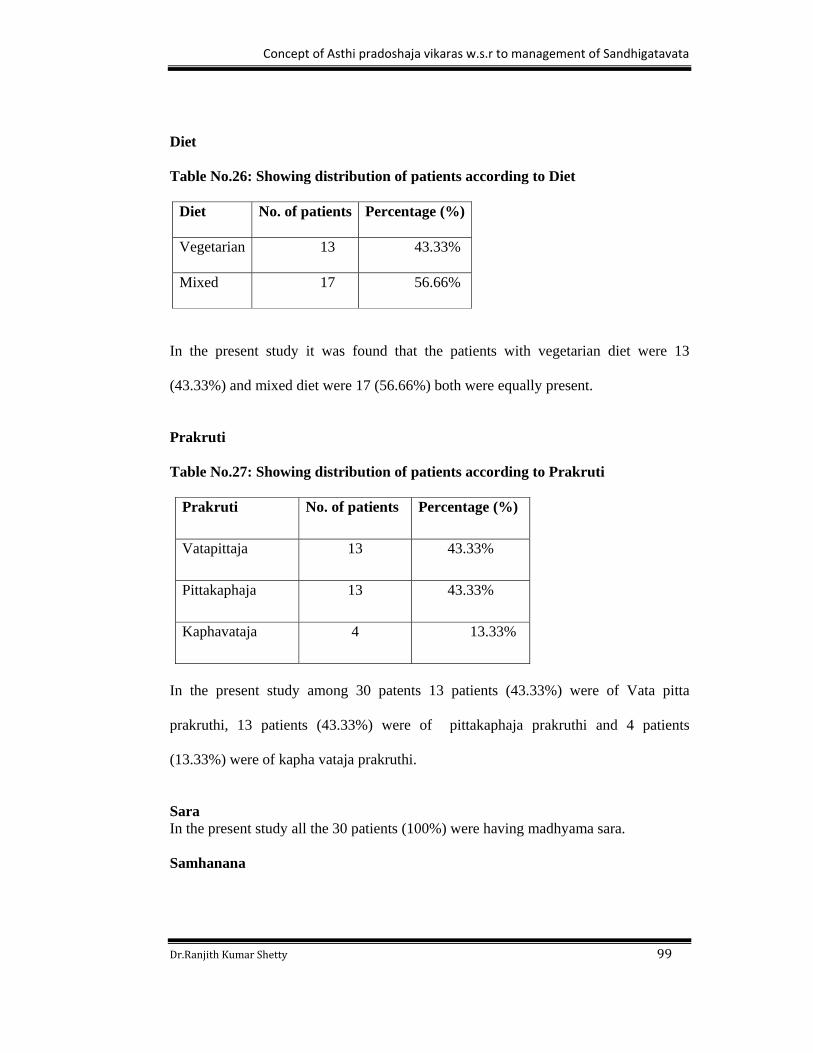
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 99
Diet Table No.26: Showing distribution of patients according to Diet
Diet No. of patients Percentage (%)
Vegetarian 13 43.33%
Mixed 17 56.66%
In the present study it was found that the patients with vegetarian diet were 13
(43.33%) and mixed diet were 17 (56.66%) both were equally present.
Prakruti
Table No.27: Showing distribution of patients according to Prakruti
Prakruti No. of patients Percentage (%)
Vatapittaja 13 43.33%
Pittakaphaja 13 43.33%
Kaphavataja 4 13.33%
In the present study among 30 patents 13 patients (43.33%) were of Vata pitta
prakruthi, 13 patients (43.33%) were of pittakaphaja prakruthi and 4 patients
(13.33%) were of kapha vataja prakruthi.
Sara In the present study all the 30 patients (100%) were having madhyama sara.
Samhanana

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 100
Table No.28: Showing distribution of patients according to Samhanana
Samhanana No.of patients Percentage(%)
Pravara 2 6.66%
Madhyama 21 70.0%
Avara 2 6.66%
Among 30 patients 21 patients (70.0%) were of madhyama samhanana, 2 patients
(6.66%) were of avara samhanana and 2 patients (6.66%) were of pravara
samhanana.
Pramana Table No.29: Showing distribution of patients according to Pramana
Pramana No. of patients Percentage (%)
Madhyama 26 86.66%
Avara 4 13.33%
In the present study among the 30 patients 26 patients (86.66%) were having
madhyama pramana and 4 patients (13.33%) were having avara pramana.
Satva
Table No.30: Showing distribution of patients according to Satva
Satva No. of patients Percentage (%)
Pravara 1 3.33%
Madhyama 23 76.66%
Avara 6 20.0%
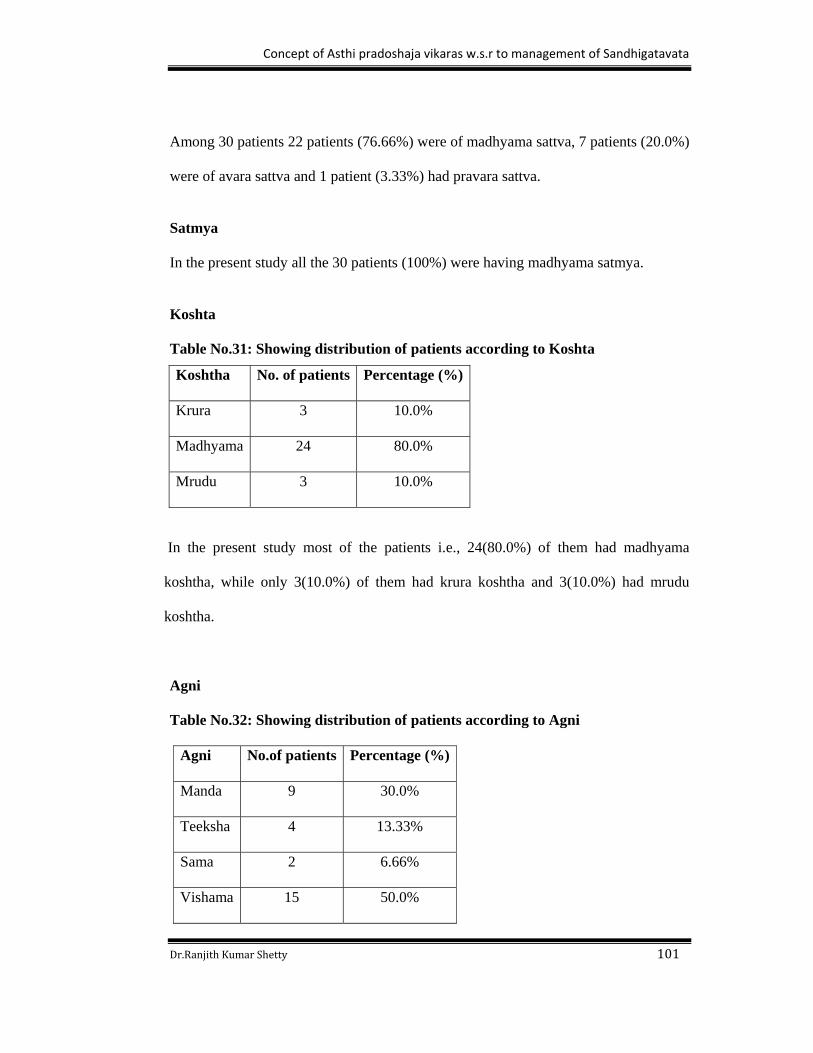
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 101
Among 30 patients 22 patients (76.66%) were of madhyama sattva, 7 patients (20.0%)
were of avara sattva and 1 patient (3.33%) had pravara sattva.
Satmya
In the present study all the 30 patients (100%) were having madhyama satmya.
Koshta Table No.31: Showing distribution of patients according to Koshta
In the present study most of the patients i.e., 24(80.0%) of them had madhyama
koshtha, while only 3(10.0%) of them had krura koshtha and 3(10.0%) had mrudu
koshtha.
Agni
Table No.32: Showing distribution of patients according to Agni
Agni No.of patients Percentage (%)
Manda 9 30.0%
Teeksha 4 13.33%
Sama 2 6.66%
Vishama 15 50.0%
Koshtha No. of patients Percentage (%)
Krura 3 10.0%
Madhyama 24 80.0%
Mrudu 3 10.0%

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 102
Among 30 patients 15 patients (50.0%) had Vishamagni, 9 patients (30.0%) had
mandagni and 4 patients (13.33%) had teekshna agni and 2 patients (6.66%) had
samagni.
Bala Table No.33: Showing distribution of patients according to Bala
Bala No.of patients Percentage (%)
Pravara 1 3.33%
Madhyama 28 93.33%
Avara 1 3.33%
In the present study most of the patients i.e., 28(93.33%) of them had madhyama bala,
while only 1 patient (3.33%) of them had pravara bala and 1patient (3.33%) had avara
bala.
Vyayama shakti
Table No.34: Showing distribution of patients according to Vyayama Vyayama shakti No.of patients Percentage (%)
Pravara 1 3.33%
Madhyama 28 93.33%
Avara 1 3.33%
Among 30 patients, 28 patients (93.33%) had madhyama vyayama shakti, 1 patient
(3.33%) had avara vyayama shakti and 1 patient (3.33%) had pravara vyayama
shakti.

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 103
Joint involvement Table No.35: Showing distribution of patients according to Joint involvement
Side involvement No. of patients Percentage (%)
Unilateral 2 13.33%
Bilateral 28 86.66%
Among 30 patients, 28 patients (86.6%) had bilateral joint involvement and only 2
patients (13.3%) had unilateral involvement of joint.
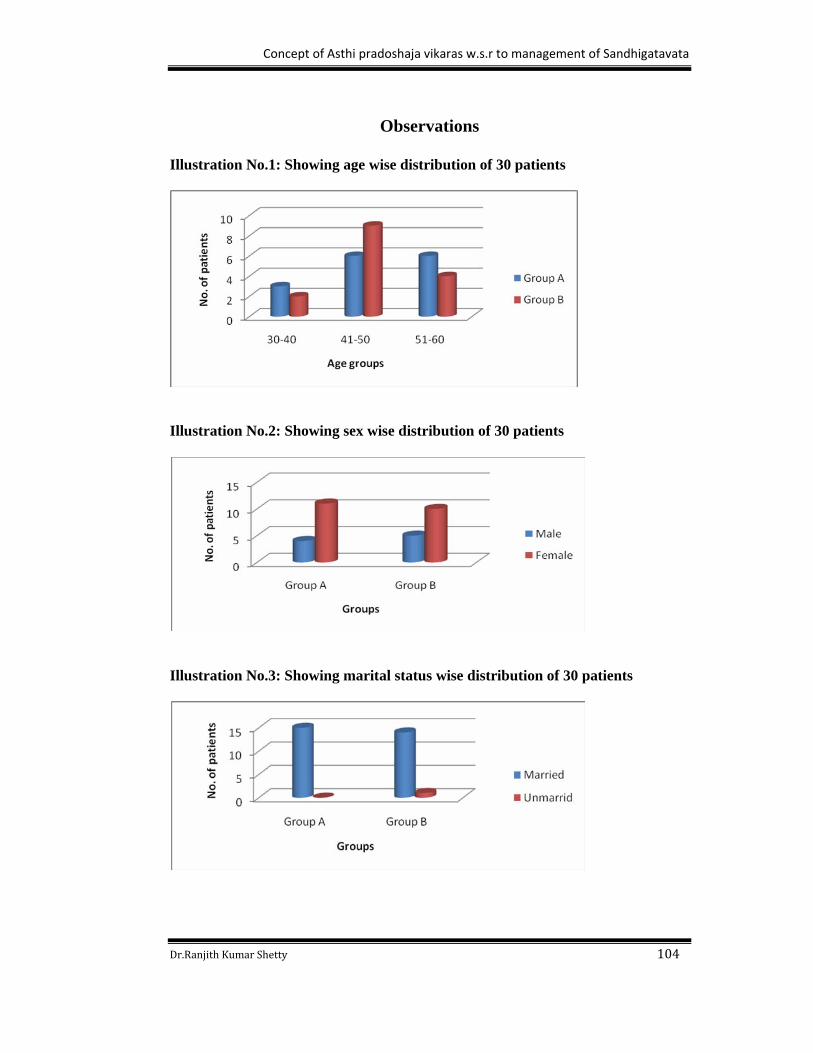
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 104
Observations
Illustration No.1: Showing age wise distribution of 30 patients
Illustration No.2: Showing sex wise distribution of 30 patients
Illustration No.3: Showing marital status wise distribution of 30 patients

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 105
Illustration No.4: Showing education wise distribution of 30 patients
Illustration No.5: Showing religion wise distribution of 30 patients
Illustration No.6: Showing occupation wise distribution of 30 patients

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 106
Illustration No.7: Showing habitat wise distribution of 30 patients
Illustration No.8: Showing diet wise distribution of 30 patients
Illustration No.9: Showing prakruti wise distribution of 30 patients

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 107
Illustration No.10: Showing samhanana wise distribution of 30 patients
Illustration No.11: Showing pramana wise distribution of 30 patients
Illustration No.12: Showing satva wise distribution of 30 patients
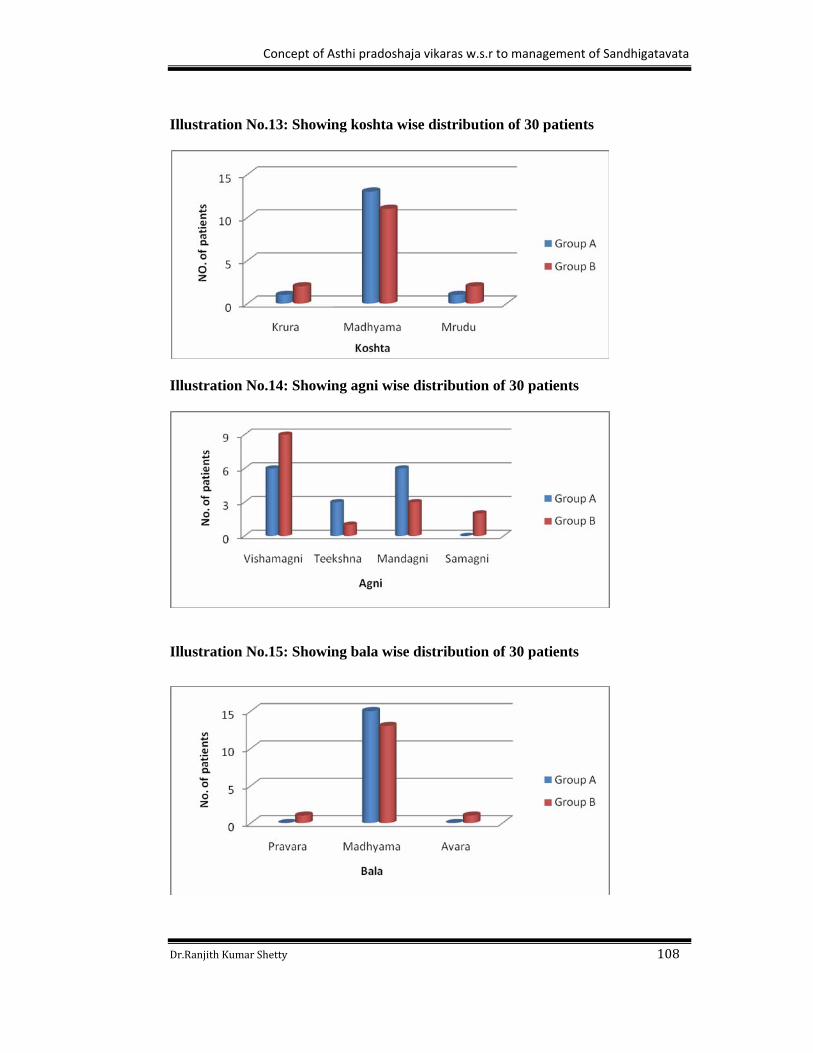
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 108
Illustration No.13: Showing koshta wise distribution of 30 patients
Illustration No.14: Showing agni wise distribution of 30 patients
Illustration No.15: Showing bala wise distribution of 30 patients

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 109
Illustration No.16: Showing vyayamashakti wise distribution of 30 patients
Illustration No.17: Showing joint involvement wise distribution of 30 patients
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 110
Observations during intervention
Group-A
All the patients were presenting with varied degree of sama lakshanas.
Patients received trikatu churna; thrice daily in a dose of 4gm till niramavastha was
attained.
It was observed that the duration taken to attain niramavastha was 2-3 days.
All the patients received Kalabasti regularly for 15 days.
All the patients received panchatiktaka ghrita for anuvasana basti and pancatikta
ksheera sarpi for niruha basti.
The dose was adjusted to 80ml for anuvasana and 600ml for niruha basti.
It was observed that pratyagamana kala was 30mins to 24 hrs for anuvasana basti
and 5mins to 40 mins for niruha basti.
Patients were comfortable at the end of the treatment.
There were no complications observed.
Patients received samsarjana karma (pathyapathya) for 30 days.
Group-B
All the patients were presenting with varied degree of sama lakshanas.
Patients received trikatu churna; thrice daily in a dose of 4gm till niramavastha was
attained.
It was observed that the duration taken to attain niramavastha was 2-3 days.
All the patients received Kalabasti regularly for 15 days.

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 111
All the patients received bala ghrita for anuvasana basti and bala sadhita ksheera
sarpi for niruha basti.
The dose was adjusted to 80ml for anuvasana and 600ml for niruha basti.
It was observed that pratyagamana kala was 30mins to 24 hrs for anuvasana basti and
5mins to 40 mins for niruha basti.
Patients were comfortable at the end of the treatment.
There were no complications observed.
Patients received samsarjana karma (pathyapathya) for 30 days.
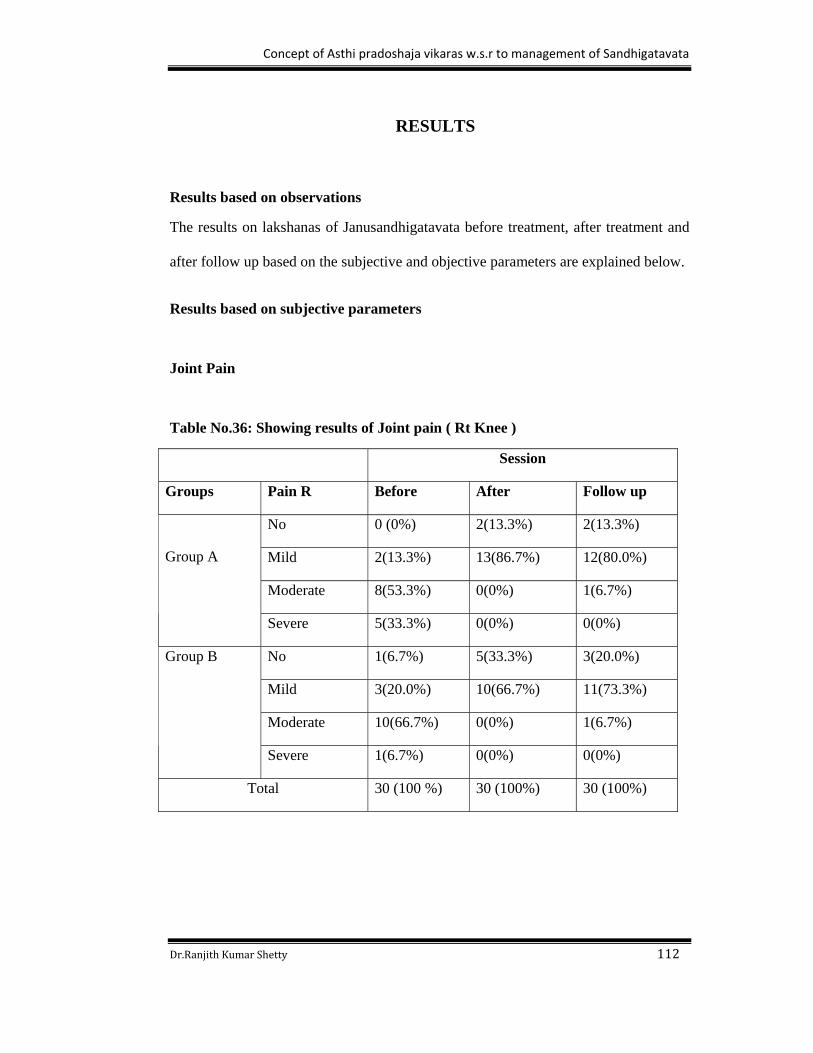
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 112
RESULTS
Results based on observations
The results on lakshanas of Janusandhigatavata before treatment, after treatment and
after follow up based on the subjective and objective parameters are explained below.
Results based on subjective parameters
Joint Pain
Table No.36: Showing results of Joint pain ( Rt Knee )
Session
Groups Pain R Before After Follow up
No 0 (0%) 2(13.3%) 2(13.3%)
Mild 2(13.3%) 13(86.7%) 12(80.0%)
Moderate 8(53.3%) 0(0%) 1(6.7%)
Group A
Severe 5(33.3%) 0(0%) 0(0%)
No 1(6.7%) 5(33.3%) 3(20.0%)
Mild 3(20.0%) 10(66.7%) 11(73.3%)
Moderate 10(66.7%) 0(0%) 1(6.7%)
Group B
Severe 1(6.7%) 0(0%) 0(0%)
Total 30 (100 %) 30 (100%) 30 (100%)

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 113
Table No.37: Showing Systemic measures in Joint pain (Rt Knee)
Groups Value Approx sig
Group A Nominal by Nominal Contingency Coefficient
N of Valid cases
650
45
.000
Group B Nominal by Nominal Contingency Coefficient
N of Valid cases
605
45
.000
In Group A before treatment 5 patients had severe pain, 8 patients had moderate pain
and 2 patients had mild pain. After treatment 13 patients attained mild pain and 2
patients attained no pain. After the follow up, 12 patients’ attained mild pain, 1patient
attained moderate pain and 2 patients attained no pain.
In Group B before treatment 1 patient had severe pain, 10 patients had moderate pain,
3 patients had mild pain and 1 patient had no pain. After treatment 10 patients attained
mild pain and 5 patients attained no pain. After follow up, 1 patient attained moderate
pain, 11 patients had mild pain and 3 patients attained no pain.
By observing the results, it has been noted that there was improvement seen in both
the groups and statistically highly significant with P value 0.000 in the both groups.
But comparatively Group A shows high significance than Group B.
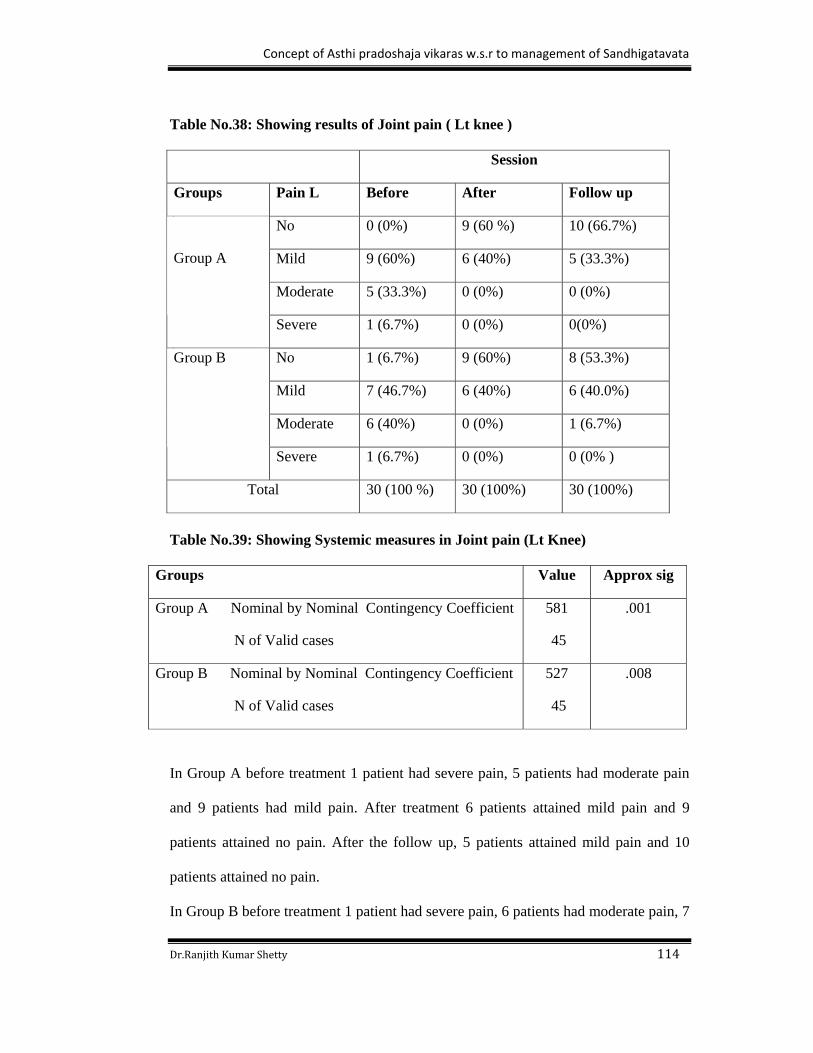
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 114
Table No.38: Showing results of Joint pain ( Lt knee ) Session
Groups Pain L Before After Follow up
No 0 (0%) 9 (60 %) 10 (66.7%)
Mild 9 (60%) 6 (40%) 5 (33.3%)
Moderate 5 (33.3%) 0 (0%) 0 (0%)
Group A
Severe 1 (6.7%) 0 (0%) 0(0%)
No 1 (6.7%) 9 (60%) 8 (53.3%)
Mild 7 (46.7%) 6 (40%) 6 (40.0%)
Moderate 6 (40%) 0 (0%) 1 (6.7%)
Group B
Severe 1 (6.7%) 0 (0%) 0 (0% )
Total 30 (100 %) 30 (100%) 30 (100%)
Table No.39: Showing Systemic measures in Joint pain (Lt Knee)
Groups Value Approx sig
Group A Nominal by Nominal Contingency Coefficient
N of Valid cases
581
45
.001
Group B Nominal by Nominal Contingency Coefficient
N of Valid cases
527
45
.008
In Group A before treatment 1 patient had severe pain, 5 patients had moderate pain
and 9 patients had mild pain. After treatment 6 patients attained mild pain and 9
patients attained no pain. After the follow up, 5 patients attained mild pain and 10
patients attained no pain.
In Group B before treatment 1 patient had severe pain, 6 patients had moderate pain, 7
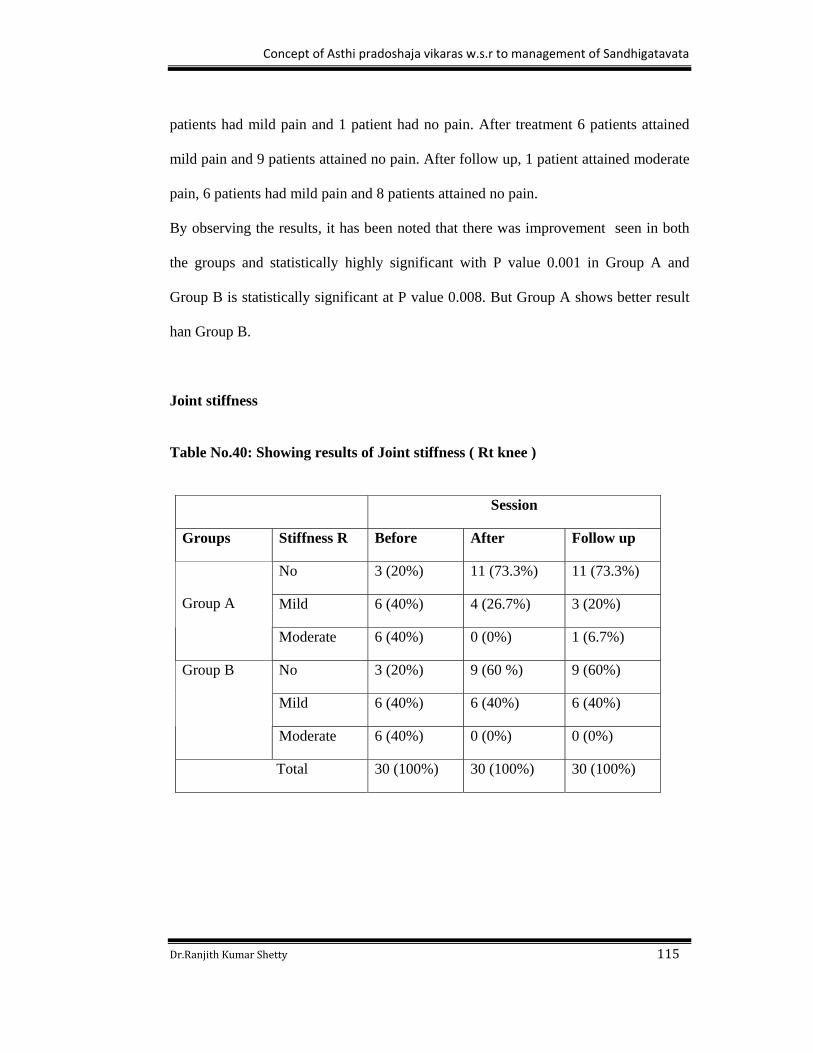
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 115
patients had mild pain and 1 patient had no pain. After treatment 6 patients attained
mild pain and 9 patients attained no pain. After follow up, 1 patient attained moderate
pain, 6 patients had mild pain and 8 patients attained no pain.
By observing the results, it has been noted that there was improvement seen in both
the groups and statistically highly significant with P value 0.001 in Group A and
Group B is statistically significant at P value 0.008. But Group A shows better result
han Group B.
Joint stiffness Table No.40: Showing results of Joint stiffness ( Rt knee )
Session
Groups Stiffness R Before After Follow up
No 3 (20%) 11 (73.3%) 11 (73.3%)
Mild 6 (40%) 4 (26.7%) 3 (20%)
Group A
Moderate 6 (40%) 0 (0%) 1 (6.7%)
No 3 (20%) 9 (60 %) 9 (60%)
Mild 6 (40%) 6 (40%) 6 (40%)
Group B
Moderate 6 (40%) 0 (0%) 0 (0%)
Total 30 (100%) 30 (100%) 30 (100%)
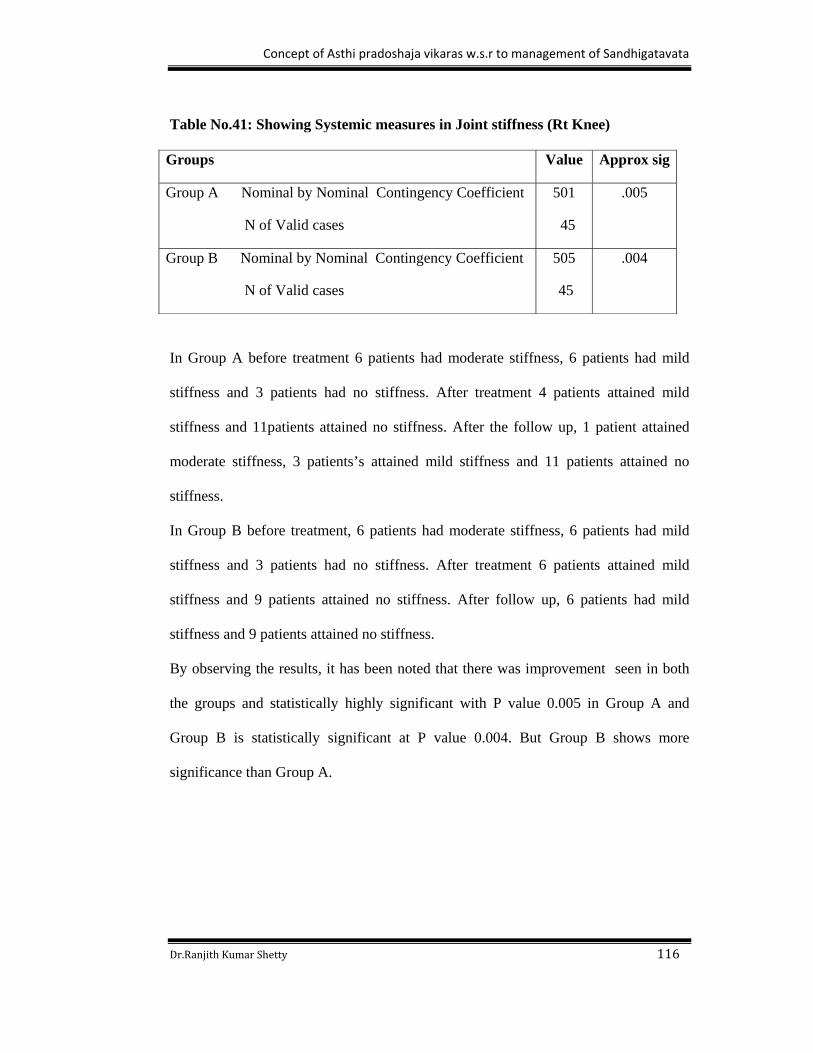
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 116
Table No.41: Showing Systemic measures in Joint stiffness (Rt Knee)
Groups Value Approx sig
Group A Nominal by Nominal Contingency Coefficient
N of Valid cases
501
45
.005
Group B Nominal by Nominal Contingency Coefficient
N of Valid cases
505
45
.004
In Group A before treatment 6 patients had moderate stiffness, 6 patients had mild
stiffness and 3 patients had no stiffness. After treatment 4 patients attained mild
stiffness and 11patients attained no stiffness. After the follow up, 1 patient attained
moderate stiffness, 3 patients’s attained mild stiffness and 11 patients attained no
stiffness.
In Group B before treatment, 6 patients had moderate stiffness, 6 patients had mild
stiffness and 3 patients had no stiffness. After treatment 6 patients attained mild
stiffness and 9 patients attained no stiffness. After follow up, 6 patients had mild
stiffness and 9 patients attained no stiffness.
By observing the results, it has been noted that there was improvement seen in both
the groups and statistically highly significant with P value 0.005 in Group A and
Group B is statistically significant at P value 0.004. But Group B shows more
significance than Group A.

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 117
Table No.42: Showing results of Joint stiffness ( Lt knee )
Session
Groups Stiffness L Before After Follow up
No 5 (33.3%) 13 (86.7 %) 12 (80%)
Mild 9 (60%) 2 (13.3 %) 3 (20%)
Group A
Moderate 1 (6.7%) 0 (0%) 0 (0%)
No 3 (20%) 12 (80%) 14 (93.3%)
Mild 10 (66.7 %) 3 (20%) 1(6.7%)
Moderate 1 (6.7 %) 0 (0%) 0 (0%)
Group B
Severe 1 (6.7 %) 0 (0%) 0 (0%)
Total 30 (100%) 30 (100%) 30 (100%)
Table No.43: Showing Systemic measures in Joint stiffness ( Lt knee )
Groups Value Approx sig
Group A Nominal by Nominal Contingency Coefficient
N of Valid cases
458
45
.018
Group B Nominal by Nominal Contingency Coefficient
N of Valid cases
561
45
.002
In Group A before treatment 1 patient had moderate stiffness, 9 patients had mild
stiffness and 5 patients had no stiffness. After treatment 2 patients attained mild
stiffness and 13 patients attained no stiffness. After the follow up, 3 patients attained
mild stiffness and 12 patients attained no stiffness.
In Group B before treatment 1 patient had severe stiffness, 1 patient had moderate
stiffness, 10 patients had mild stiffness and 3 patients had no stiffness. After treatment

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 118
3 patients attained mild stiffness and 12 patients attained no stiffness. After follow up,
1 patient had mild stiffness and 14 patients attained no stiffness.
By observing the results, it has been noted that there was improvement seen in both
the groups and statistically highly significant with P value 0.002 in Group B and
Group A is statistically significant with P value 0.018. But Group B shows significant
value than Group A.
Joint Swelling Table No.44: Showing results of Joint swelling ( Rt knee )
Session
Groups Swelling R Before After Follow up
No 8 (53.3%) 13 (86.7%) 15 (100%)
Mild 5 (33.3%) 2 (13.3%) 0 (0%)
Group A
Moderate 2 (13.3%) 0 (0%) 0 (0%)
No 9 (60%) 14 (93.3%) 15 (100%)
Mild 5 (33.3%) 1 (6.7%) 0 (0%)
Group B
Moderate 1 (6.7%) 0 (0%) 0 (0%)
Total 30 (100%) 30 (100%) 30 (100%)

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 119
Table No.45: Showing Systemic measures in Joint swelling ( Rt knee )
Groups Value Approx sig
Group A Nominal by Nominal Contingency Coefficient
N of Valid cases
453
45
.021
Group B Nominal by Nominal Contingency Coefficient
N of Valid cases
437
45
.031
In Group A before treatment 2 patients had moderate swelling, 5 patients had mild
swelling, and 8 patients had no swelling. After treatment 2 patients attained mild
swelling and 13 patients attained no swelling. After the follow up all the 15 patients
attained no swelling.
In Group B before treatment 1 patient had moderate swelling, 5 patients had mild
swelling and 9 patients had no swelling. After treatment 1 patients attained mild
swelling and 9 patients attained no swelling. After follow up all the 15 patients
attained no swelling.
By observing the results, it has been noted that there was improvement seen in both
the groups and statistically highly significant with P value 0.021 in Group A and
Group B is statistically significant with P value 0.031. But Group A shows
significance than Group B.
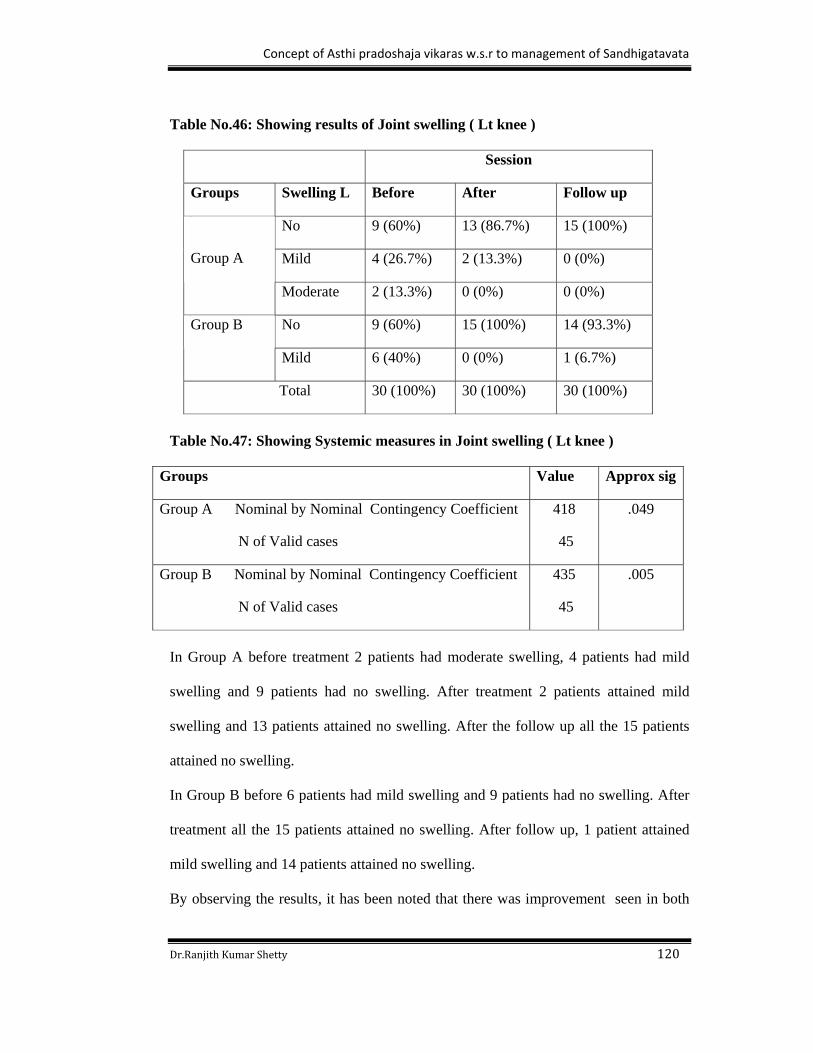
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 120
Table No.46: Showing results of Joint swelling ( Lt knee )
Session
Groups Swelling L Before After Follow up
No 9 (60%) 13 (86.7%) 15 (100%)
Mild 4 (26.7%) 2 (13.3%) 0 (0%)
Group A
Moderate 2 (13.3%) 0 (0%) 0 (0%)
No 9 (60%) 15 (100%) 14 (93.3%) Group B
Mild 6 (40%) 0 (0%) 1 (6.7%)
Total 30 (100%) 30 (100%) 30 (100%)
Table No.47: Showing Systemic measures in Joint swelling ( Lt knee )
Groups Value Approx sig
Group A Nominal by Nominal Contingency Coefficient
N of Valid cases
418
45
.049
Group B Nominal by Nominal Contingency Coefficient
N of Valid cases
435
45
.005
In Group A before treatment 2 patients had moderate swelling, 4 patients had mild
swelling and 9 patients had no swelling. After treatment 2 patients attained mild
swelling and 13 patients attained no swelling. After the follow up all the 15 patients
attained no swelling.
In Group B before 6 patients had mild swelling and 9 patients had no swelling. After
treatment all the 15 patients attained no swelling. After follow up, 1 patient attained
mild swelling and 14 patients attained no swelling.
By observing the results, it has been noted that there was improvement seen in both
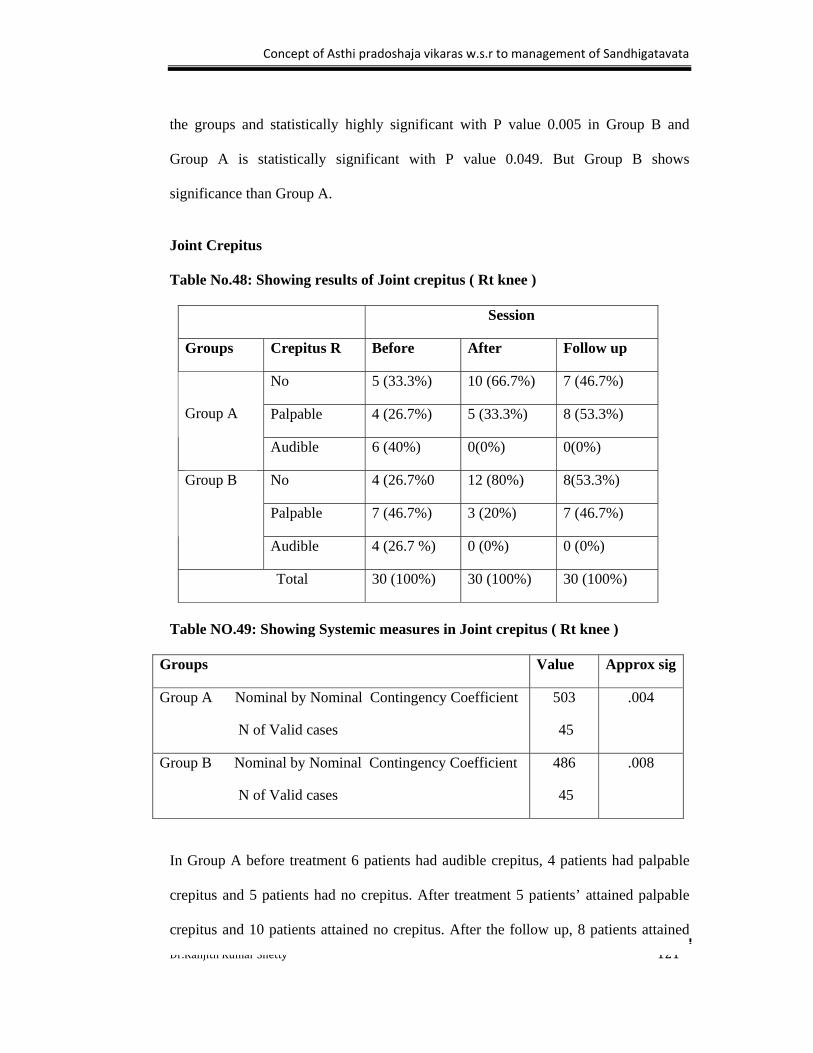
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 121
the groups and statistically highly significant with P value 0.005 in Group B and
Group A is statistically significant with P value 0.049. But Group B shows
significance than Group A.
Joint Crepitus Table No.48: Showing results of Joint crepitus ( Rt knee )
Session
Groups Crepitus R Before After Follow up
No 5 (33.3%) 10 (66.7%) 7 (46.7%)
Palpable 4 (26.7%) 5 (33.3%) 8 (53.3%)
Group A
Audible 6 (40%) 0(0%) 0(0%)
No 4 (26.7%0 12 (80%) 8(53.3%)
Palpable 7 (46.7%) 3 (20%) 7 (46.7%)
Group B
Audible 4 (26.7 %) 0 (0%) 0 (0%)
Total 30 (100%) 30 (100%) 30 (100%)
Table NO.49: Showing Systemic measures in Joint crepitus ( Rt knee )
Groups Value Approx sig
Group A Nominal by Nominal Contingency Coefficient
N of Valid cases
503
45
.004
Group B Nominal by Nominal Contingency Coefficient
N of Valid cases
486
45
.008
In Group A before treatment 6 patients had audible crepitus, 4 patients had palpable
crepitus and 5 patients had no crepitus. After treatment 5 patients’ attained palpable
crepitus and 10 patients attained no crepitus. After the follow up, 8 patients attained
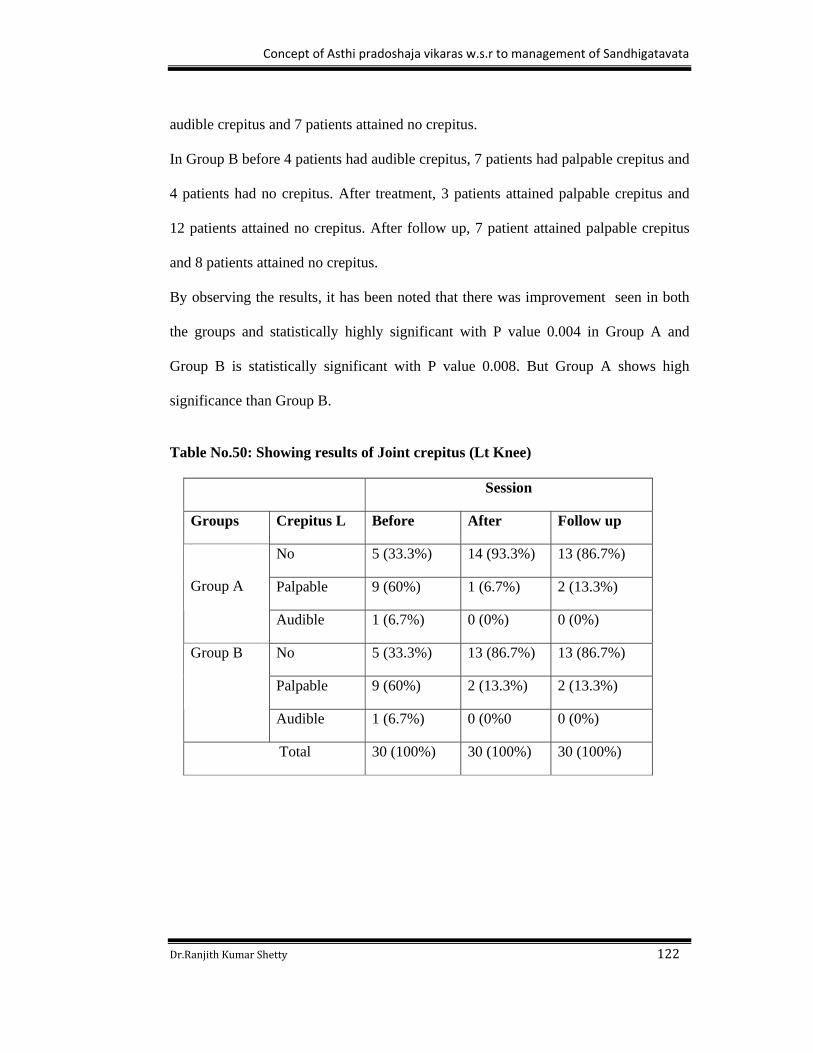
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 122
audible crepitus and 7 patients attained no crepitus.
In Group B before 4 patients had audible crepitus, 7 patients had palpable crepitus and
4 patients had no crepitus. After treatment, 3 patients attained palpable crepitus and
12 patients attained no crepitus. After follow up, 7 patient attained palpable crepitus
and 8 patients attained no crepitus.
By observing the results, it has been noted that there was improvement seen in both
the groups and statistically highly significant with P value 0.004 in Group A and
Group B is statistically significant with P value 0.008. But Group A shows high
significance than Group B.
Table No.50: Showing results of Joint crepitus (Lt Knee)
Session
Groups Crepitus L Before After Follow up
No 5 (33.3%) 14 (93.3%) 13 (86.7%)
Palpable 9 (60%) 1 (6.7%) 2 (13.3%)
Group A
Audible 1 (6.7%) 0 (0%) 0 (0%)
No 5 (33.3%) 13 (86.7%) 13 (86.7%)
Palpable 9 (60%) 2 (13.3%) 2 (13.3%)
Group B
Audible 1 (6.7%) 0 (0%0 0 (0%)
Total 30 (100%) 30 (100%) 30 (100%)

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 123
Table No.51: Showing Systemic measures in Joint crepitus (Lt Knee)
Groups Value Approx sig
Group A Nominal by Nominal Contingency Coefficient
N of Valid cases
513
45
.003
Group B Nominal by Nominal Contingency Coefficient
N of Valid cases
483
45
.008
In Group A before treatment 1 patient had audible crepitus, 9 patients had palpable
crepitus and 5 patients had no crepitus. After treatment 1 patient attained palpable
crepitus and 14 patients attained no crepitus. After the follow up, 2 patients attained
audible crepitus and 13 patients attained no crepitus.
In Group B before 1 patient had audible crepitus, 9 patients had palpable crepitus and
5 patients had no crepitus. After treatment, 2 patients attained palpable crepitus and
13 patients attained no crepitus. After follow up, 2 patient attained palpable crepitus
and 13 patients attained no crepitus.
By observing the results, it has been noted that there was improvement seen in both
the groups and statistically highly significant with P value 0.003 in Group A and
Group B is statistically significant at P value 0.008. But Group A shows significance
than Group B.
Result based on the Objective parameter
Radiological findings
X-ray was done before treatment, after treatment and after the end of follow up in
Group A and Group B. But no changes were observed radiologically in both the
groups after the treatment and after the end of follow up.
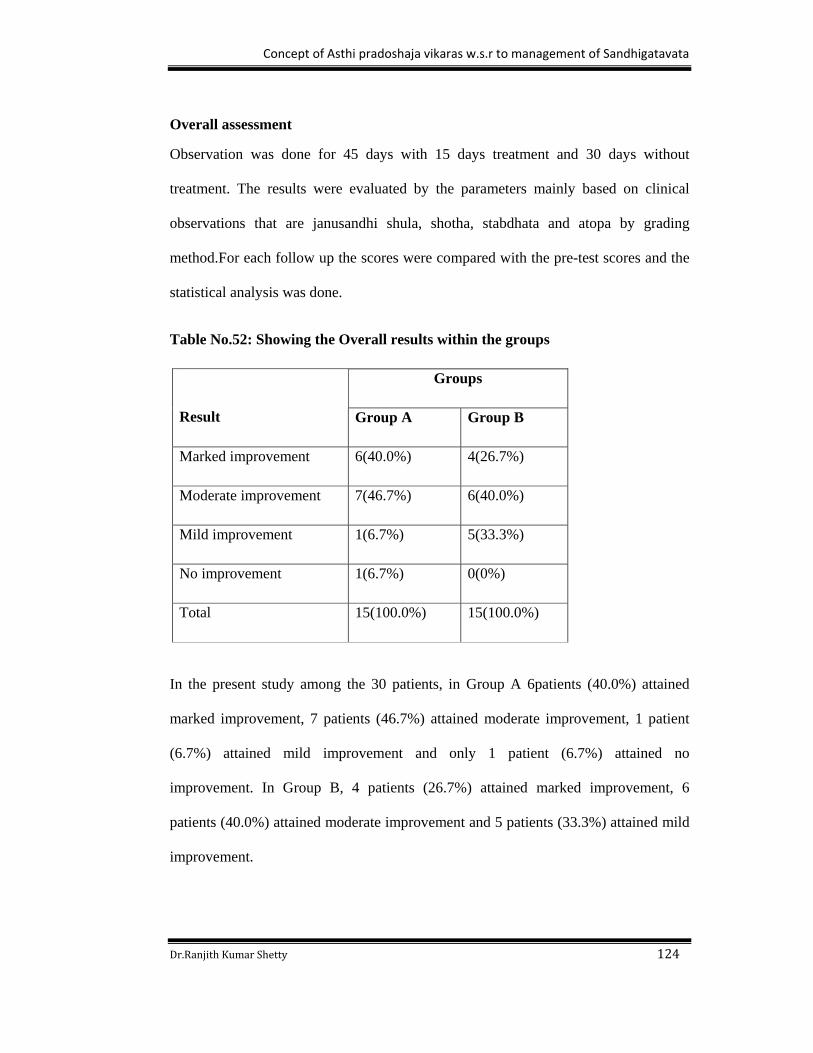
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 124
Overall assessment
Observation was done for 45 days with 15 days treatment and 30 days without
treatment. The results were evaluated by the parameters mainly based on clinical
observations that are janusandhi shula, shotha, stabdhata and atopa by grading
method.For each follow up the scores were compared with the pre-test scores and the
statistical analysis was done.
Table No.52: Showing the Overall results within the groups
Groups
Result Group A Group B
Marked improvement 6(40.0%) 4(26.7%)
Moderate improvement 7(46.7%) 6(40.0%)
Mild improvement 1(6.7%) 5(33.3%)
No improvement 1(6.7%) 0(0%)
Total 15(100.0%) 15(100.0%)
In the present study among the 30 patients, in Group A 6patients (40.0%) attained
marked improvement, 7 patients (46.7%) attained moderate improvement, 1 patient
(6.7%) attained mild improvement and only 1 patient (6.7%) attained no
improvement. In Group B, 4 patients (26.7%) attained marked improvement, 6
patients (40.0%) attained moderate improvement and 5 patients (33.3%) attained mild
improvement.
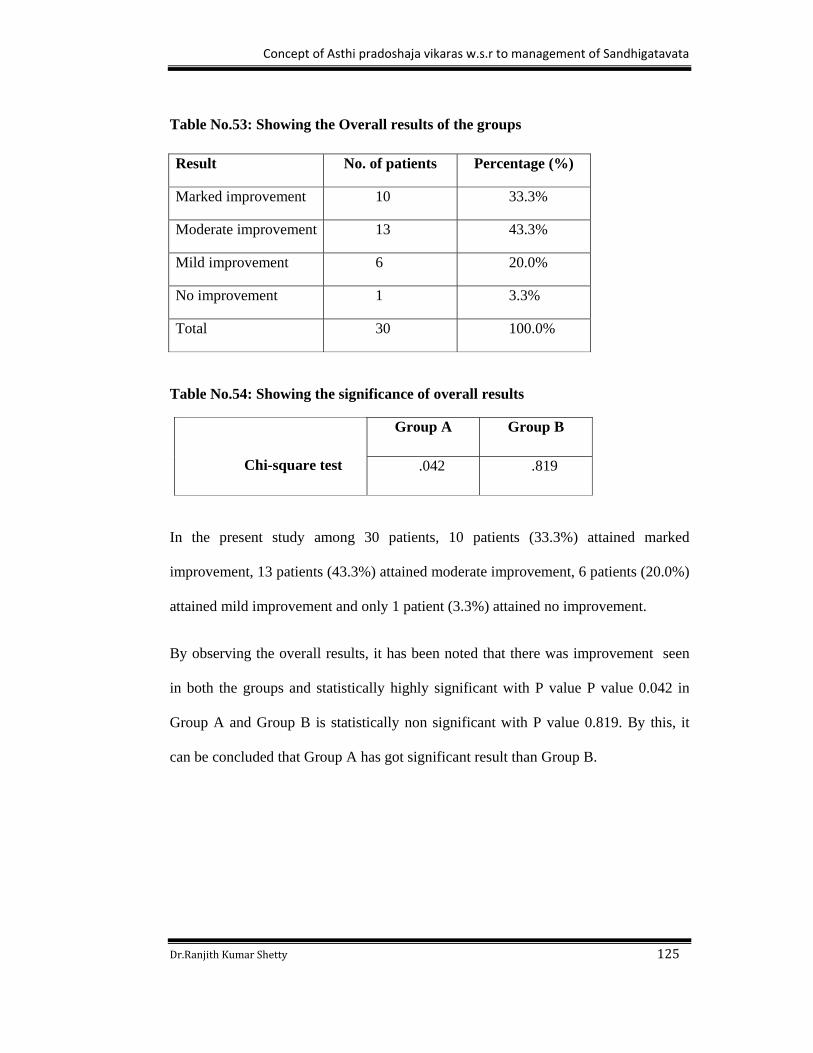
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 125
Table No.53: Showing the Overall results of the groups
Result No. of patients Percentage (%)
Marked improvement 10 33.3%
Moderate improvement 13 43.3%
Mild improvement 6 20.0%
No improvement 1 3.3%
Total 30 100.0%
Table No.54: Showing the significance of overall results
Group A Group B
Chi-square test .042 .819
In the present study among 30 patients, 10 patients (33.3%) attained marked
improvement, 13 patients (43.3%) attained moderate improvement, 6 patients (20.0%)
attained mild improvement and only 1 patient (3.3%) attained no improvement.
By observing the overall results, it has been noted that there was improvement seen
in both the groups and statistically highly significant with P value P value 0.042 in
Group A and Group B is statistically non significant with P value 0.819. By this, it
can be concluded that Group A has got significant result than Group B.
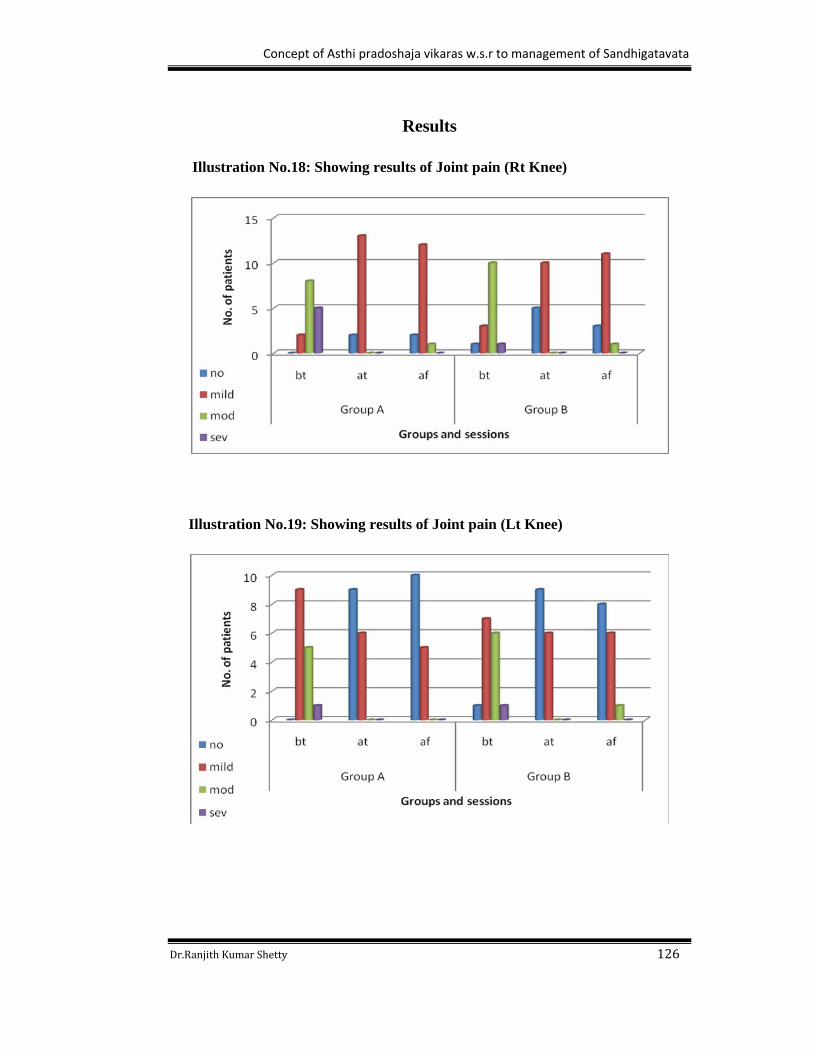
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 126
Results
Illustration No.18: Showing results of Joint pain (Rt Knee)
Illustration No.19: Showing results of Joint pain (Lt Knee)
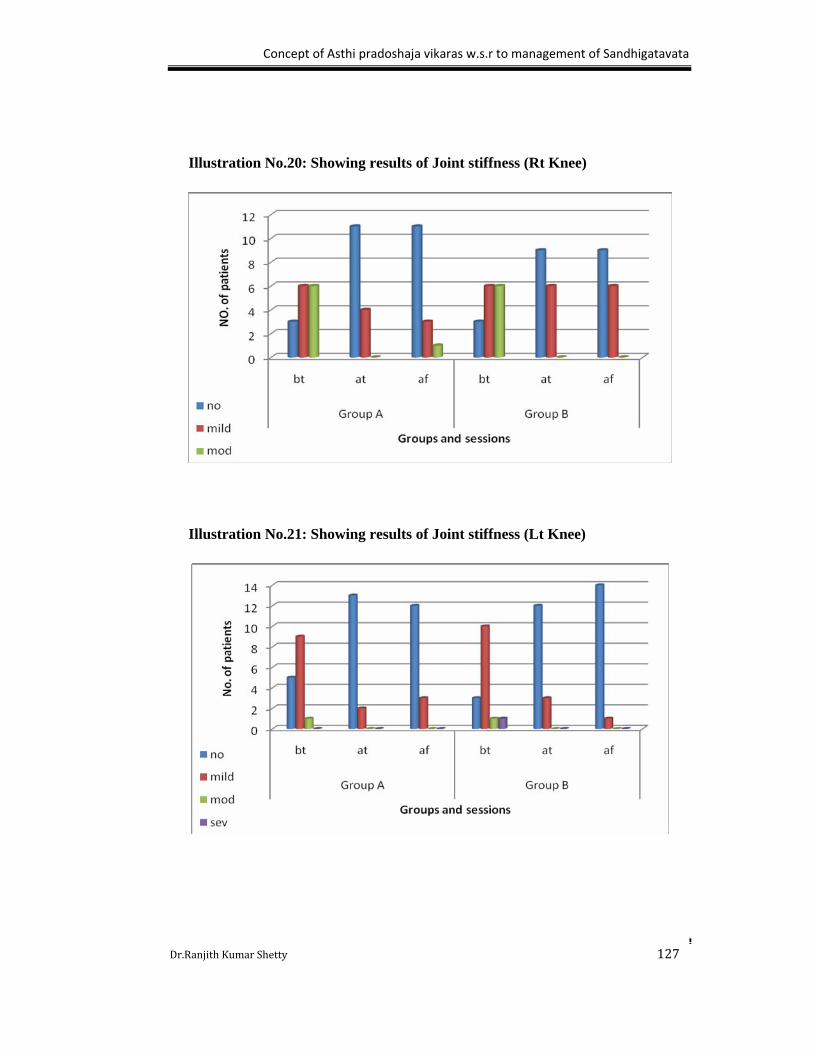
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 127
Illustration No.20: Showing results of Joint stiffness (Rt Knee)
Illustration No.21: Showing results of Joint stiffness (Lt Knee)

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 128
Illustration No.22: Showing results of Joint swelling (Rt Knee)
Illustration No.23: Showing results of Joint swelling (Lt Knee)
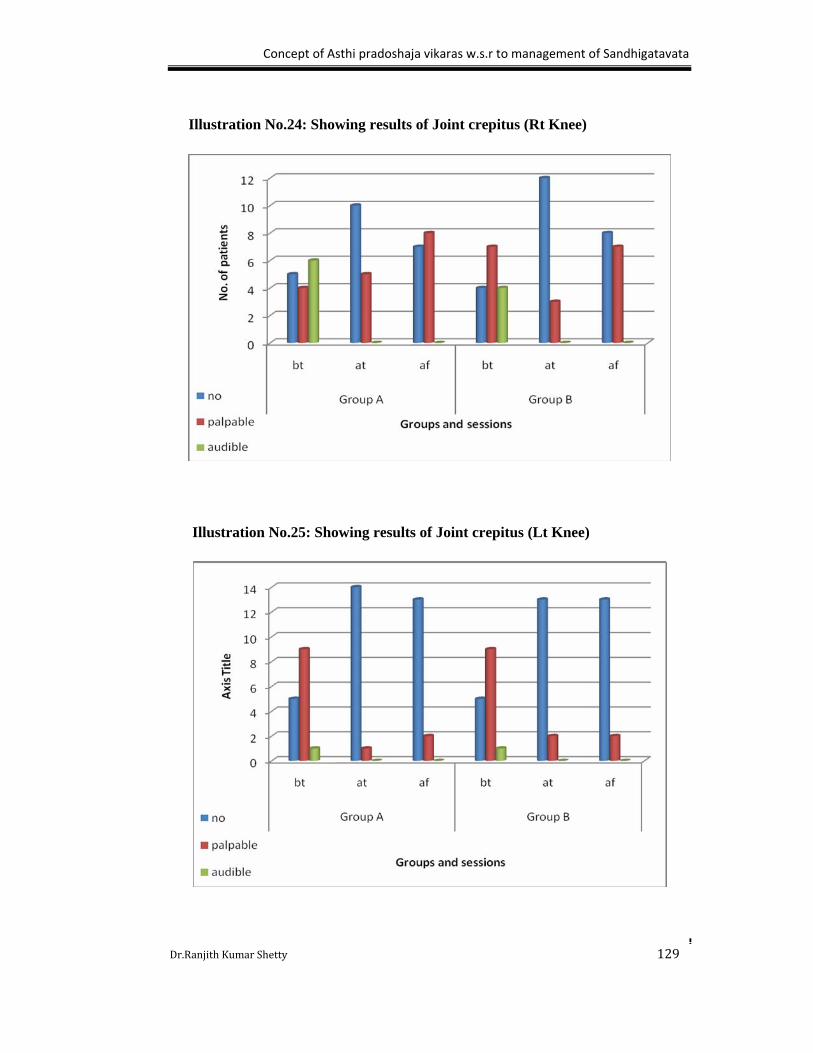
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 129
Illustration No.24: Showing results of Joint crepitus (Rt Knee)
Illustration No.25: Showing results of Joint crepitus (Lt Knee)
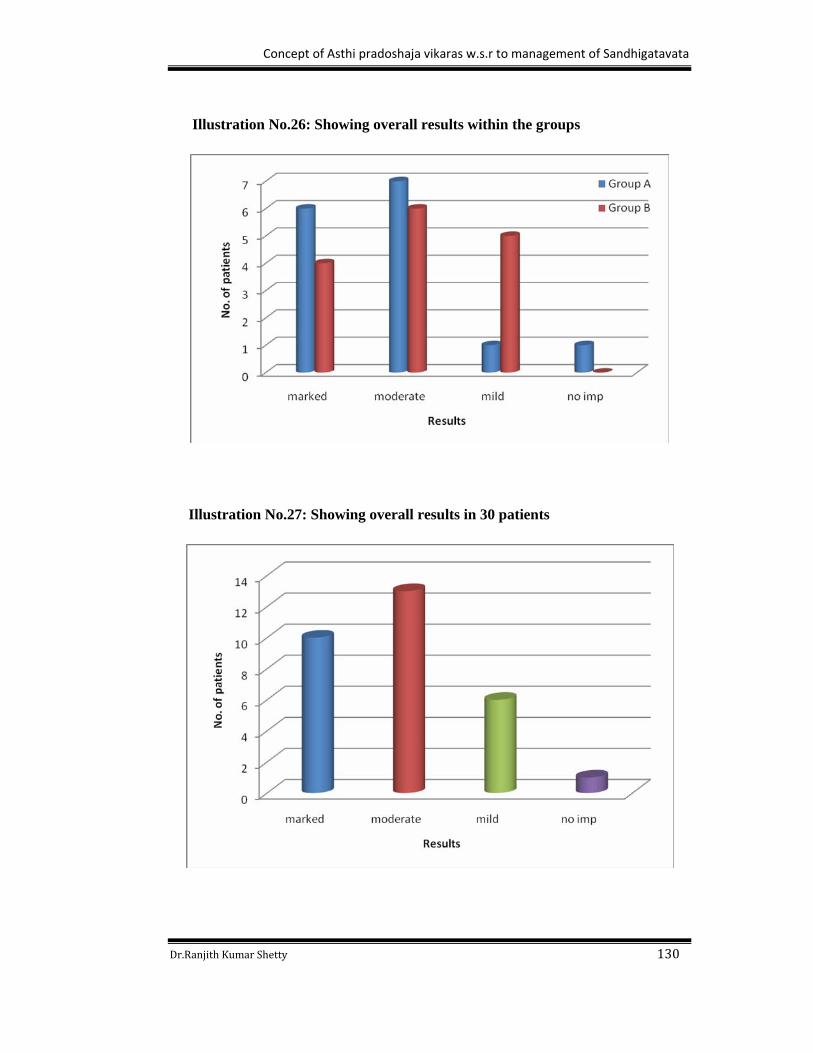
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 130
Illustration No.26: Showing overall results within the groups
Illustration No.27: Showing overall results in 30 patients

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 131
DISCUSSION
Discussion is the interpretation of observations and results obtained from the
clinical study along with the review. So the relevant points are discussed here.
Discussion on the title
“Concept of Asthi Pradoshaja vikaras w.s.r to Management of Sandhigatavata.”
Ayurveda is a science of life, which is framed on many concepts. All these concepts
are proved and established facts. The methodology adopted to establish these facts was
holds good for that respective era. In the present era due to globalization of Ayurveda
and to easily convince the common people, these olden techniques are not sufficient.so
these old principles should be restablished with the help of modern advanced technology.
As Asthi is one among the sapta dhatu and it does the function of dharana. The normalcy
and abnormalcy of Asthi can easily be visualized with the help of so many techniques,
one among them is X-ray. By this extra growth, fracture, increase of porocity,
calcification etc deformities which can be ruled out and this is one among best technology
to rule out sandhigatavata. Sandhigatavata is a common joint disorder occurs due to the
deformity mainly in the Asthi. As per the World Health Organization OA is the second
commonest musculoskeletal problem in the world. The reported prevalence of OA from a
study in rural India is 5.78%. Hence the present study is undertaken to restablish the
concept of Asthi pradoshaja vikaras with the help of radiology and supported by
considering sandhigatavata as an Asthi pradoshaja vikara treating as per the chikitsa sutra
explained in the Asthi pradoshaja vikaras.
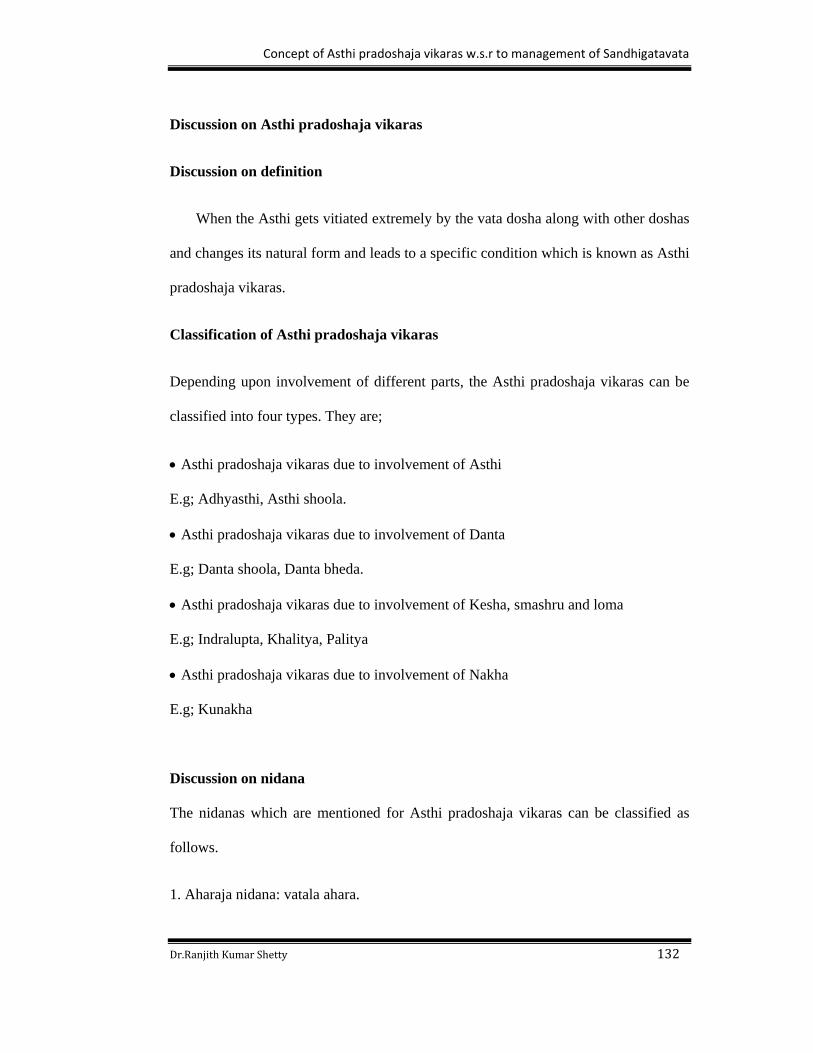
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 132
Discussion on Asthi pradoshaja vikaras
Discussion on definition
When the Asthi gets vitiated extremely by the vata dosha along with other doshas
and changes its natural form and leads to a specific condition which is known as Asthi
pradoshaja vikaras.
Classification of Asthi pradoshaja vikaras
Depending upon involvement of different parts, the Asthi pradoshaja vikaras can be
classified into four types. They are;
Asthi pradoshaja vikaras due to involvement of Asthi
E.g; Adhyasthi, Asthi shoola.
Asthi pradoshaja vikaras due to involvement of Danta
E.g; Danta shoola, Danta bheda.
Asthi pradoshaja vikaras due to involvement of Kesha, smashru and loma
E.g; Indralupta, Khalitya, Palitya
Asthi pradoshaja vikaras due to involvement of Nakha
E.g; Kunakha
Discussion on nidana
The nidanas which are mentioned for Asthi pradoshaja vikaras can be classified as
follows.
1. Aharaja nidana: vatala ahara.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 133
2. Viharaja nidana: ativyayama, ati vighattana.
3. Manasika nidana: ati sankshobha
Aharaja nidana
Vatala ahara and vihara sevana: Over indulgence in ruksha, laghu and alpa matra
ahara aggravates vata in the shareera. The chief qualities of vata are ruksha, laghu,
sukshma etc. these are similar to each other. So it will lead to vata vitiation. Viharas
like ati chesta, abhigata, etc cause the vata vitiation. When the vitiated vata gets
lodges in Asthi, it leads to different disorders.
Viharaja nidana
Ati vyayama: Ativyayama means excessive shareera ayasa janaka karma i.e more
than ardha shakti vyayama. When person performs the ati vyayama continuously it
leads to the increase in laghu, ruksha, sukshma, teekshna guna in the shareera. Later it
invariably leads to vata vitiation. Because vata havs the same gunas like laghu,
ruksha, sukshma etc on the basis of samanya siddhanta. As per the contemporary
science, excessive exercise causes the injury to the body like bone fracture, bone pain
etc.
Ati vighattana: ati vighattana means excessive movements or separation or injury. It
directly affects the particular part of the body. It is considered as the abhighataja
nidana. Here it directly affects the Asthi dhatu initially later vitiation of vata dosha
takes place due to ashraya ashrayee bhava. Then it leads to different disorders like
Asthi bheda, Asthi shoola etc. even in the contemporary science, it is mentioned that
external injury is one of the main causative factor for the manifestation of bone
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 134
disorders like osteoarthritis etc.
Manasika nidana
Ati sankshobha: ati sankshobha means excessive manasika kshobha (mental stress or
disturbance). When the person is under mental stress, then it will leads to increase in
rajo guna in the shareera. As per the classics, rajo guna is one among the vata guna.
So it invariably increases the vata dosha in the shareera. As per the contemporary
science mental disturbance is the cause for all most all the disorders.
Discussion on poorvarupa
All the Asthi pradoshaja vikaras have avyakta or alpa vyakta lakshanas as
poorvarupa. So it is difficult to consider particular poorvarupa for all Asthi pradoshaja
vikaras.
e.g, Danta shoola: mild tooth ache can be considered has a poorva rupa for danta
shoola.
Kunakha: mild discoloration can be considered has a poorva rupa for kunaka.
Discussion on rupa
Adhyasthi (Bone spur): It refers to additional bone or extra bone. It generally forms
in response to pressure, rubbing, or stress that continues over a long period of time. It
is usually smooth, but it can cause wear and tear or pain if it presses on the other
bones or soft tissues. Bone spurs usually limit joint movement and typically cause
pain. Has such bone spur may originate anywhere in the body like ankle, knee,
shoulder etc. e.g; calcaneal spur.

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 135
Adhidanta (Hyperdontia): It refers to additional or extra teeth. Which appear in
addition to the regular number of teeth and is mal-formed. There is evidence of
hereditary factors along with some evidence of environmental factors leading to this
condition. Many supernumerary teeth never erupt, but they may delay eruption of
nearby teeth or cause other dental problems.
Danta bheda and Danta shoola (Odontalgia): As per Ayurvedic classics these are
two different disorders. Here patient suffers from different form of pain like cutting;
pricking etc. This pain can often be aggravated somewhat by chewing or by hot or
cold temperature. Causes of tooth ache may also be a symptom of the heart, such as
angina or myocardial infarction due to referred pain.
Asthi bheda, Asthi shoola and Asthi toda (Bone pain): As per Ayurvedic classics
these are the different Asthi pradoshaja vikaras. Details regarding each disorder are
not available in any of the classics. The individual feels different forms of pain in the
bone due to different disorders. In the contemporary science there are conditions
characterized by bony pain which includes both acute and chronic. Chronic pain will
be present in some disorders like Osteoarthritis; Paget’s disease etc. Acute pain will
be present in the fractures.
Shyavadanta (Tooth discoloration): The blackish or kapila varnata of the tooth is
called as shyavadanta. Tooth discoloration is caused by multiple local and systemic
conditions. Extrinsic dental strains are caused by poor oral hygiene etc. Intrinsic
dental strains are caused by dental materials (eg, tooth restorations), dental conditions
and caries, trauma, infections, medications, nutritional deficiencies and other
disorders (eg, complications of pregnancy, anemia and bleeding disorders, bile duct
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 136
problems), and genetic defects and hereditary diseases (eg, those affecting enamel and
dentin development or maturation).
Krimidanta (Dental caries): In this condition danta becomes Krishna varnata, chidra
yukta, sravayukta or sometimes with shoola. When it is neglected then it leads to
complications like danta vidradi. Dental caries is a disease where bacterial processes
damage hard tooth structure, if left untreated, the disease can lead to pain, infection
and in severe cases death may occur. When the pH at the surface of the tooth drops
below 5.5, demineralization proceeds faster than remineralization (meaning that there
is a net loss of mineral structure on the tooth's surface). This results in the ensuing
decay.
Indralupta (Alopecia areata): The partial or complete loss of hair from all over the
body is called as indralupta. It can be correlated to alopecia areata or some times it is
called as spot baldness, in which hair is lost from the localized area or all areas of the
body, usually from the scalp. This disease may be limited only to the beard, in which
case it is called alopecia areata barbae. The area of hair loss may tingle or be very
slightly painful. It occurs more frequently in individuals who have affected family
members, suggesting that heredity may be a factor.
Khalitya (Alopecia areata universalis): The condition in which partial loss of hair
takes place in the scalp and there is no chance for regrowth of hair. This condition can
be correlated to alopecia universalis. If all body hair, including pubic hair is lost then
it called s alopecia areata universalis. Alopecia universalis can occur at any age, and is
currently believed to be an autoimmune disorder. Alopecia Universalis may be acute
and short-lived or remain permanently.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 137
Palitya (Grey hair): When the hair becomes kapila varna in the early age then it is
called as palitya. This condition can be correlated to the premature grey hair. Early or
premature greying of hair is basically hereditary and other causes are stress, anxiety
and malnutrition. An individual who is under a prolonged period of stress and anxiety
may notice, over a period of time, white hairs gradually appearing. Malnutrition,
worry, shock, deep sorrow, tension and other similar conditions may also slow down
the production of melanin resulting in grey hair.
Kunakha (Onychogyphosis): This is a condition in which daha, paka, vedana and
asita varnata will be present in the nakha. This can be correlated to the
onychogryphosis. These types of nails are caused due to damage to the cells that grow
the nail. Discomfort can result when footwear or even bed sheets press on thickened
nails, because the surface beneath the nails (the nail plate) is also thickened and
tender. The thickening of a nail, which is common in older people, may be caused by
several factors including injury (such as that caused by ill-fitting shoes), infection,
poor blood supply, diabetes, or inadequate intake of nutrients.
Discussion on samprapti
Probabal pathogenesis which is involved in the manifestation of Asthi pradoshaja
vikaras can be understood by this flow chart.

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 138
Flow chart No.2: Showing the vishesha samprapti of Asthi pradoshaja vikaras
Nidana
Ati vyayama Ati sankshobha Ati vighattana Vatala ahara & vihara
Vata dushti Vata dushti Asthi dushti Vata dushti
Asthi dhatu dusti
Dosha dushya sammurchana
Sthaana samshraya in particular angaavayava (Asthi, Danta, Kesha, Nakha)
Particular Asthi pradoshaja vikaras (Adhyasthi, Danta shoola, Khalitya, Kunakha)
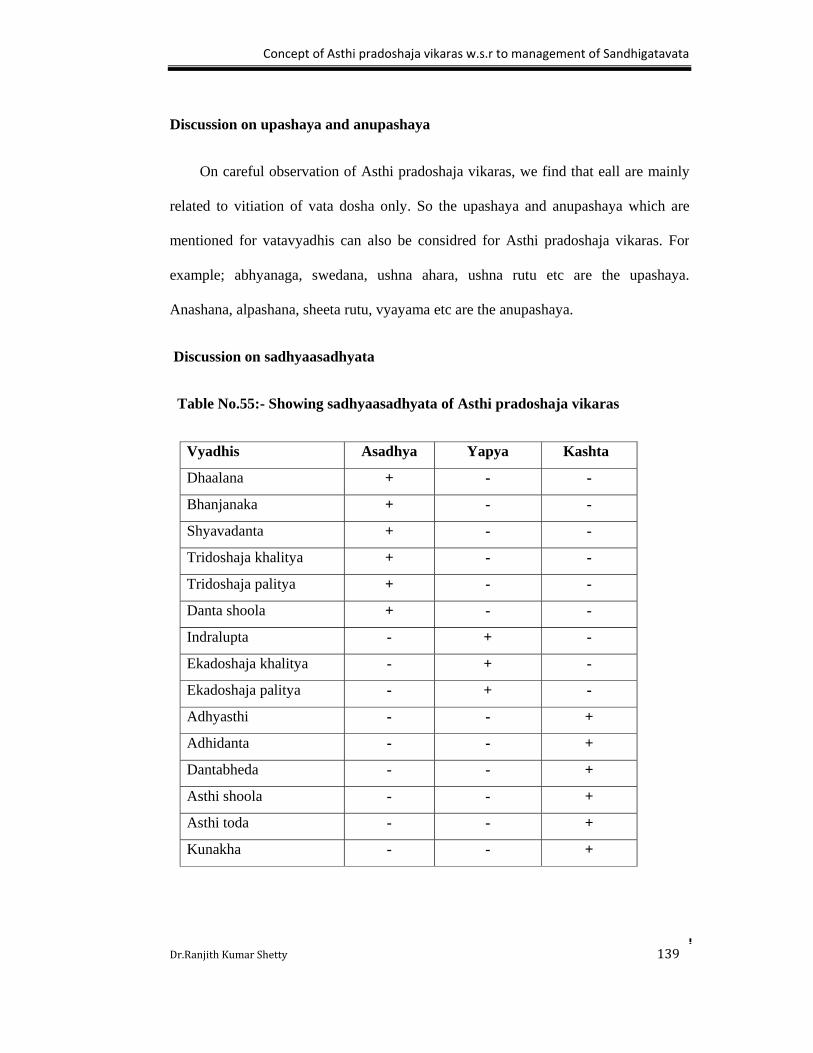
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 139
Discussion on upashaya and anupashaya
On careful observation of Asthi pradoshaja vikaras, we find that eall are mainly
related to vitiation of vata dosha only. So the upashaya and anupashaya which are
mentioned for vatavyadhis can also be considred for Asthi pradoshaja vikaras. For
example; abhyanaga, swedana, ushna ahara, ushna rutu etc are the upashaya.
Anashana, alpashana, sheeta rutu, vyayama etc are the anupashaya.
Discussion on sadhyaasadhyata
Table No.55:- Showing sadhyaasadhyata of Asthi pradoshaja vikaras
Vyadhis Asadhya Yapya Kashta
Dhaalana + - -
Bhanjanaka + - -
Shyavadanta + - -
Tridoshaja khalitya + - -
Tridoshaja palitya + - -
Danta shoola + - -
Indralupta - + -
Ekadoshaja khalitya - + -
Ekadoshaja palitya - + -
Adhyasthi - - +
Adhidanta - - +
Dantabheda - - +
Asthi shoola - - +
Asthi toda - - +
Kunakha - - +
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 140
Among the Asthi pradoshaja vikaras dhaalana, bhanjanaka, shyavadanta, tridoshaja
khalitya, tridoshaja palitya and dantashoola are considered as asadhya vyadhis
because these are tridoshaja vyadhis and treatment modality in such cases are not
satisfactory and prognosis is very poor. The diseases like indralupta, ekadoshaja
khalitya and ekadoshaja palitya are considered as yapya vyadhis because it requires
long duration of treatment and some times it gets may cured but chances of
reccurrence are more. Other diseases like adhyasthi, adhidanta, dantabheda, Asthi
shoola, Asthi toda and kunaka are considered as kashta sadhya vyadhis because it
requires both shamana aoushadhis and shastra karma.
Discussion on treatment
In Charaka samhita the treatment principles are explained for Asthi pradoshaja
vikaras. But in other samhitas like sushruta samhita, Ashtanga hrudaya, Ashtanga
sangraha the direct reference for the treatment of Asthi pradoshaja vikaras is not
available, but treatment principles explained for Asthi kshaya and vruddi looks similar
as explained in Charaka samhita. The treatment modalities are panchakarama (tikta
ksheera sarpi basti) and vatahara ahara-vihara.
Panchakarma: This is the major treatment modality, which is always used to
eradicate the diseases which are located in shaakha, marma, asthisandhi and this is is
the best treatment for chronic disorders. By adopting panchakarma one can subside
the doshas which are located all over the body and by this diseases can be eradicated
completely. Ability of evacuation, superiority and enormity of the procedures ,target
of dosha eradication and multitude of action are characterstics of pachakarma. Bones
are present all over the body and are the hardest structures in the body. Due to these

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 141
reasons panchakarma is the major procedure for Asthi pradoshaja vikaras.
Basti: Basti is the best treatment modality for vata and the vitiated doshas located
below the nabhi pradesha. The administered basti reaches the pakvashaya which is the
place of purushadhara kala. Pakvashaya and Asthi are the main seats of vata dosha,
therefore increased or decreased formation of vata affects all the sites of vata
especially Asthi. Hence purishadhara kala is also considered Asthidhara kala. So it
invariably nourishes the Asthi also.
Especially tikta sadhita ksheera sarpi basti is indicated in Asthi pradoshaja vikaras.
Tikta rasa has predomonently vayu and akasha mahabhuta and as per arunadatta tikta
rasa has a unique property to maintain the kharatva of Asthi dhatu. Asthi also has
preodominently pruthvi, vayu and teja mahabhuta.so tikta invariably increases the
kharatva in the Asthi. Ksheera and sarpi has predominantly pruthvi, jala mahabhuta
and madhura rasa yukta. These properties will check the vitiated vata dosha. The
provocation of Vata will result into Asthi Dhatu dushti Basti is the best treatment
explained for Vata Dosha so the Tikta Rasa in combination with Sneha Dravyas in the
form of Basti have a bifold nature i.e it provides sufficient nourishment to the Asthi
Dhatu as well as check the Vata Dosha also.
Table No.56:- Showing the chikitsa of Asthi Pradoshaja Vikaras
Chikitsa
Asthi pradoshaja
vikaras
Panchakarma Shastra karma Shamana karma
Adhidanta Rakta mokshana,
Nasya
Kshara karma,
Agni karma,
Danta nirharana
Gandusha

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 142
Danta bheda Vasti - Kavala
Gandusha
Abhyanga
Swedana
Danta shoola Nasya Danta nirharana
Dantapali lekhana
Gandusha
Pratisarana
Kavala
Krimidanta Rakta mokshana
Avapeeda nasya
Danta nirharana
Agni karma
Gandusha
Lepa
Indralupta Rakta mokshana Siravyadha Lepa
Shiroabhyanga
Khalitya & Palitya Nasya - Shiroabhyanga
Lepa
Adhyasthi,
Asthi shoola
Asthi bheda
Asthi toda
Basti - Abhyanga
Swedana
Among the Asthi pradoshaja vikaras adhidanta, danta bheda, danta shoola,
krimidanta, indralupta, khalitya and palitya occurs in the jatru urdhva pradesha. So
nasya, kavala, gandusha, shiroabhyanga are considered to be the main treatment
modalities. Asthi shoola, Asthi bheda, Asthi toda and adhyasthi are may manifest any
where in the body, so basti is considered as main treatment principle.
Discussion on Janusandhigatavata
Sandhigata Vata is described in all Samhitas and Sangraha Granthas as a
separate clinical entity under the heading of Vata Vyadhi. While commenting on the
word “Khudavata” Chakrapani explains the meaning of Khudavata as “Gulpha Vata”
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 143
or Sandhigata Vata. Hence, it can be said that according to Chakarapani, Sandhigata
Vata (janusandhigatavata) is the Nanatmaja Vata Vikara.
Discussion on definition
The disease Janusandhigatavata can be defined as a disease of Janu Sandhi
(Joint) with symptoms of Sandhishula, Sandhishotha and pain during akunchana and
prasarana and in the later stage affects the joint (Hanti Sandhi). In contemporary
science a similar condition is explained and is called as Osteoarthritis which is a
degenerative joint disorder with the symptoms of Joint Pain, Joint Swelling,
Restricted and Painful Movements of the Joints and Joint Instability.
Discussion on nidana
The nidanas of janusandhigatavata are vatakara and kapha-majjahara.
Shleshaka kapha is the major component of sandhi and performs the normal function
of sandhi. Due to the above said nidana sevana, the rukshatva and achalatva guna
increases. Simultaneously these properties also influences the kapha ashraya sthana
and majja dhatu which is present within the Asthi. Due to majja kshaya Asthi
soushiryata occurs. In another way as Asthi and vata are ashraya ashrayee, whenever
Asthi increases vata decreases and vice versa. Due to above said nidana sevana the
vata dosha increases which is present in the Asthi. By this vitiation occurs in the
Asthi. In this way these nidanas will lead to the manifestation of janusandhigatavata.
Discussion on purvarupa
Jansandhigatavata is one among the vatavyadhi, so avyakta or alpavyakta
lakshanas are considered as poorvrupa. Mild sandhi shula or shotha prior to the
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 144
manifestation of disease janusandhigatavata may be taken as its Purvarupa.
Discussion on rupa
The janusandhigatvata lakshanas can be classified as follows.
Sandhishula: Shula is the main symptom of prakupita vata. Shula usally increases by
movements like akunchana, prasarana because of vata prakopa. It is worst during
evening because of the tendency of vata which naturally aggravates at evening period,
hence the shula. It can be correlated te joint pain, which occurs due to bone attrition
and pressure of osteophytes over the soft tissues.
Sandhishotha: Due to nidana sevana vata gets prakupita and affects the srotus by
decreasing kapha, creates the shotha in the sandhi pradesha so it senses like a
vatapoorna druti. It means on palpation the swelling is felt like a bag filed with air.
Contemporary science mentions that joint swelling occurs due to inflammation.
Sandhiatopa: Janusandhigatavata is a localized vatavyadhi in which prakupita vayu
affects janusandhi which means akasha mahabhuta is increased at the site of
janusandhi and shabda is a guna of akasha. Hence shabda is heard or palpated.
Contemporary science, mentions clearly regarding crepitations due to the rubbing of
adjacent bony surface against each other during movement.
Sandhihanti: This occurs in the chronic stage of janusandhigatavata. In the
preliminary stage of janusandhigatavata due to above said symptoms there is
restriction of movements. Due to this reason the sanga in the srotus increases the vata

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 145
dosha, by that the sandhi loses movement . This condition is called as sandhihanti.
This can be correlated to the knock knee deformity.
Discussion on samprapti
The Vata Dosha is aggravated due to different factors and Vata moves out of
its Ashaya to circulate in the entire body and its constituents. During circulation it
gets localized in the roots of Asthivaha and Majjavaha Srotas. i.e. Asthi Sandhi. In the
Asthi and Majjavaha Srotas. The chief qualities of Vata are Khara, Ruksha, Vishada,
and Laghu. Sandhi gives Ashraya to Shleshaka Kapha which has Guru, Snigdha and
Mrudu guna. When aggravated Vata gets localized in Sandhi, it over powers all the
qualities of Kapha. The chief task of Kapha is dharana or to sustain. This chief aim of
kapha is destroyed by the influence of aggravated Vata. When aggravated Vata is
localized into a single joint, the disease will be reflected in only one Joint but if Vata
is localised in many joints, the disease may be presented by multiple joint
involvements.
Samprapti Ghataka
Dosha - Vata -Vyana vata vruddhi
Kapha - Sleshaka kapha kshaya
Dushya - Asthi, Majja, Snayu, Peshi.
Srotas - Asthivaha, majjavaha
Rogamarga - Madhyama
Udbhava sthana - Pakwashaya
Sanchara sthana - Rasayani
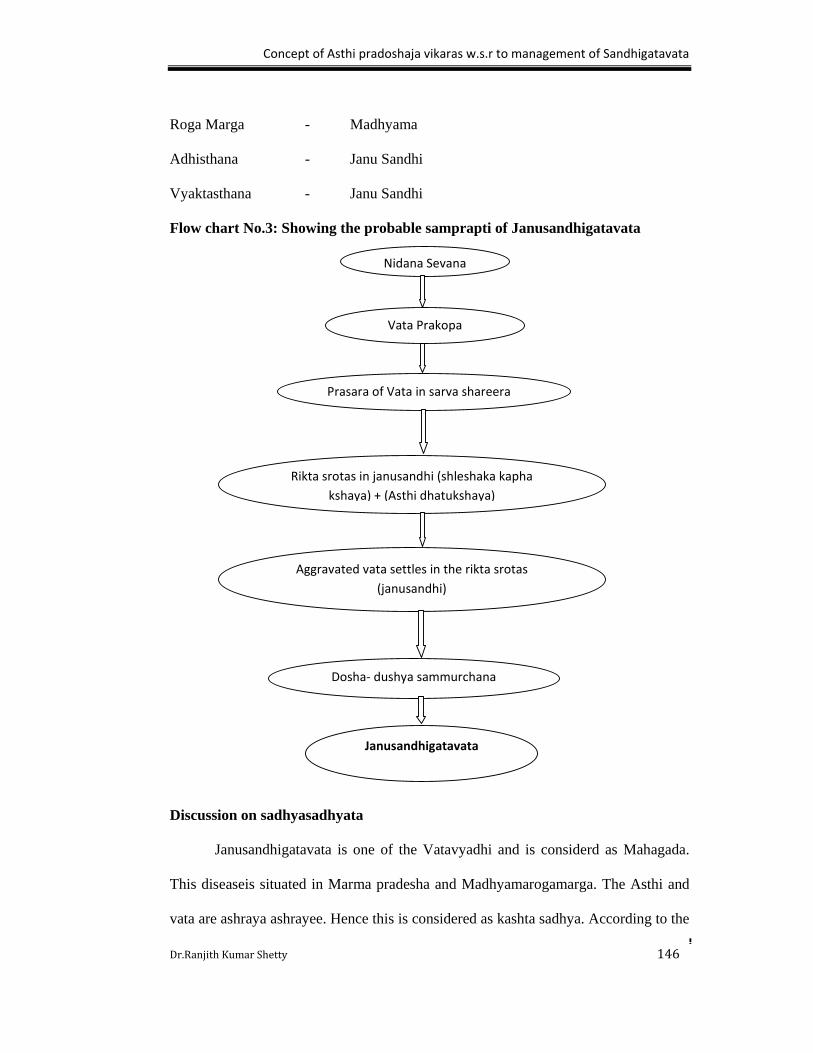
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 146
Roga Marga - Madhyama
Adhisthana - Janu Sandhi
Vyaktasthana - Janu Sandhi
Flow chart No.3: Showing the probable samprapti of Janusandhigatavata
Discussion on sadhyasadhyata
Janusandhigatavata is one of the Vatavyadhi and is considerd as Mahagada.
This diseaseis situated in Marma pradesha and Madhyamarogamarga. The Asthi and
vata are ashraya ashrayee. Hence this is considered as kashta sadhya. According to the
Nidana Sevana
Vata Prakopa
Prasara of Vata in sarva shareera
Rikta srotas in janusandhi (shleshaka kapha
kshaya) + (Asthi dhatukshaya)
Aggravated vata settles in the rikta srotas
(janusandhi)
Dosha‐ dushya sammurchana
Janusandhigatavata
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 147
contemparary science, Knee Osteoarthritis is very difficult to cure till date. No
treatment which can reverse the degenerative process is available. Only palliative
treatment is available which acts as analgesic and medications given helps to slow
down the degenerative process.
Discussion on chikitsa
The treatment principles for janusandhigatavata are snehana, upanaha,
agnikarma, bandhana, unmardana and basti.
Sneha Dravya possesses Drava, Sukshma, Sara, Snigdha, Manda, Mrudu and
Guru gunas which are just opposite to those of Vata so it alleviates Vata. Snehana
helps in the promotion and regulation of the proper functioning of Vayu. It is stated
that by the regular use of Abhyanga all changes occurring due to old age could be
prevented and cured, if already manifested. Svedana is the procedure which relieves
Stiffness, Heaviness, Cold and which induces sweat. Upanaha is bandaging. The Paste
should be hot and mixed with Sneha. The application of heat causes relaxation of the
muscles and tendons, improves the blood supply. It relieves pain in the affected joints.
To perform Agnikarma on Sandhi, Kshoudra, Guda and Sneha are to be used. By
Agnikarma on Mamsa, diseases located in Shira, Snayu and Asthi gets alleviated.
Bandha is bandaging tightly, the leaves of Vatashamaka drugs on affected Sandhi.
This bandaging does not leave any scope for Vata to inflate the Sandhi. In
januandhigatavata, Shotha appears like a bag inflated with air. Bandhana causes
abatement in Shotha. Unmardana is a type of massage in which pressure is exerted on
diseased Sandhi. It relieves Shotha and enhances blood circulation. And lastly basti
as discussed earlier is the best mode of treatment for janu sandhigata vata.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 148
Discussion on Asthi pradoshaja vikaras vs Sandhigatavata
In the present study, janusandhigatavata is considered one among the Asthi
pradoshaja vikaras due to these following reasons.
Sandhi is Asthi melana sthana. Though there are so many other structures in the
formation of sandhi,but asthi plays a major role in its formation. Hence if there is
any defect in the sandhi i.e, mainly due to the Asthi only. This is has been
identified this clinical work.
The sroto mulas of Asthi are meda, jaghana and Asthi sandhi. Hence asthivaha
sroto dusti definitely affects the sandhi.
The causative factors responsible for the manifestation of janusandhigatavata and
Asthi pradoshaja vikaras are looks similar i.e, in both conditions vata is the
predominant dosha and vatala ahara- viharas like ruksha, alpa matra ahara,
abhighata, ati vyayama, ati sankshobha etc nidanas are similar for
janusandhigatavata and Asthi pradoshaja vikaras.
There is no specific porvarupa observed in both the conditions i.e,
janusandhigatavata and Asthi pradoshaja vikaras. Avyakta or alpa vyakta
lakshanas can be considered as poorvarupa for both janusandhigatavata and Asthi
pradoshaja vikaras.
Among the lakshanas of janusandhigatavata, there are some symptoms which can
be correlated with the lakshanas of Asthi pradoshaja vikaras and these are related
to Asthi. They are adhyasthi which can be co-related to osteophytes, Asthi shoola,
Asthi bheda and Asthi toda which can be correlated to those different forms of pain
occuring in the joint.
The pathological changes occur in the manifestation of Asthi pradoshaja vikaras
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 149
and janusandhigatavata are similar. i.e, doshas: vata pradhana, dushya: Asthi and
sroto mula: Asthi sandhi.
The methodology adopted to subside the vitiation in the Asthi pradoshaja vikaras
and janusandhigatavata are similar. i.e, the main line of treatment for Asthi
pradoshaja vikaras are panchakarma, tikta sadhita ksheera sarpi yukta basti,
sthanika abhyanga-sweda, vatahara ahara-vihara and same modalities are utilized
in the treatment of janusandhigatavata.
Hence due to the reasons, janusandhigatavata is considered as one among Asthi
pradoshaja vikaras and it is treated by adopting the treatment principles explained for
Asthi pradoshaja vikaras.
Probable mode of action of basti
Tikta ksheera Basti, regarding this Arunadatta opines that the combination of
Snigdha and Shoshana guna produces Khara guna which is also the guna of Asthi.
This nourishes the Asthi as per the Samanya Siddhanta. The Pachabhoutika
composition of ingredients of basti is similar to Asthi. The ingredients will reach the
asthivaha srotas and will be acted upon by Parthivagni, Vayavagni, and Tejasagni and
gets transformed into Asthi poshakamshas on which the Asthi dhatwagni will act
upon and converts it into sthayi Asthi dhatu. Hence there will be increase of decreased
Asthi.
Cow’s milk is the richest natural source of calcium present on the earth. The
ratio in which calcium and phosphorus are present is ideal for their proper absorption
and assimilation and consequently for bone formation along with vitamin D. Vitamin
D present in cows milk helps in bone formation by maintaining the proper levels of
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 150
calcium in the blood along with the parathyroid hormone. Vitamin K activates
osteocalcin the major non collagen protein in the bone. Cow’s milk also contains
lactoferin an iron binding protein that boosts the growth and activity of the
osteoblasts, the cells that build bone and reduces the rate at which these cells die by
up to 50-70%. These also decrease the formation of osteoclasts, the cells responsible
for breaking down of the bone, thus helping to build the bone and prevent
osteoporosis.
Step wise mode of action of Basti
Ama Pachana- To clear the obstruction (Sanga) in asthivaha srotas caused by
ama and to combat the other lakshanas of Ama, ama pachana was done with trikatu
churna. When Amapachana is achieved (Pakat) the srotomukaha becomes clear and
the stage is set to bring back the vitiated Doshas from Shaakha to Koshtha.
Snehana- Sneha is said to reach the Asthi Dhatu by performing Abhyanga for
800 Matra kala approximately 15 minutes. Sneha enyters the body through minute
pores of skin by the virtue of its Anupravana bhava. Thus entering the Asthivaha
srotas, it causes Vishyandana. It destroys the obstruction in Asthivaha Srotas
(Malanam Vinihanti Sangam ). Sneha is Vata Nashaka (Sneho anilam hanti). So it
pacifies vata.
Swedana- Swedana also pacifies Vata especially, when performed after
Snehana. If Swedana is done after proper Snehana, it liquefies the Doshas which
causes obstruction in the minute channels. Hence by the combined effect of
Amapachana, Snehana and Swedana the morbid Doshas are brought to Koshtha. The
Pharmacodynamics of these three procedures is nothing but Paka, Vishyandana,
Srotomuka Vishodhana and Vayu nigrahana.These factors are responsible for the
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 151
movement of doshas from Shaakha to koshtha. Here paka is by Amapachana and
swedana, Vishyanadana is by snehana and swedana; Sroto mukha vishodhana is done
by amapachana, Snehana and swedana and Vayu nigraha is achieved by Snehana and
swedana.
Basti- After proper Snehana and Swedana, when the doshas come from
Shakaha to Koshtha, Tikta Ksheera Basti is given to expel these Doshas from the
body to nourish the Kshina Asthi Dhatu. Sushruta opines that eighth basti enters the
Asthi Dhatu. Thus entering the Asthi its action can be explained on the following
factors.
The action of tikta ksheera basti on Asthi Dhatu can also be explained on the
basis of Pancha Mahabhoutika composition. Predominance wise the Panchabhoutika
composition of Asthi is Prithvi, Vayu, Agni, Akasha and Jala Mahabhuta. The Basti
contains Ksheera , Ghrita Madhu, Guggulu, and Tikta dravya as its main ingredients.
Anuvasana basti mainly contains tikta rasa and madhura rasa where as Niruha basti
contains katu rasa along with tikta rasa and madhura rasa. If we analyze the
Panchabhoutika composition of Madhura, Tikta and Katu rasa it is Prithvi+ Jala,
Vayu+ Akasha, and Agni+ Vayu respectively. Hence the total Panchabhoutika
composition of Basti dravya is similar to the Asthi dhatu and hence nourishes the
Asthi.
Due to the Vataghna property of Niruha and Anuvasana basti there is shaman
of aggravated Vata, by this the ksheena Asthi Dhatu returns to normalcy. The Ksheera
Basti reaches the Pakwashaya which is Purishadhara kala and the ingredients of basti
ie Ksheera, Ghrita and Madhu nourishes the Purishadhara kala and thus also nourishes
the Asthidhara kala. According to Modern embryology both bone tissue and the large
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 152
intestine are formed by the mesenchymal cells of the mesoderm.
Probable Pharmacokinetics and Pharmacodynamics of Tikta Ksheera Basti
according to scientific parameters.
According to modern science basti is a process which can be compared with enema.
There are 2 types of enemas. 1. Evacuation enema and 2. Retention enema. Ksheera
basti may be considered as the nourishing retention enema.
Retention enema:- The fluid containing the drugs is retained in the rectum so that the
drug may act locally e.g. steroid enema in ulcerative colitis. The rectum has rich
blood and lymph supply and drugs can cross the rectal mucosa like the other lipid
membranes; thus unionized and lipid soluble substances are readily absorbed from the
rectum, through the rectal venous plexus. The portion of the absorbed drugs from the
upper rectal mucosa is carried to the portal circulation where as that absorbed from
the lower rectum enters directly into the systemic circulation.
The absorption of the drug from the rectum follows the laws of transfer of the
molecules across the biological membranes. Most drugs are absorbed by passive
diffusion, a few by active transport or carrier mediated transport. Pinocytosis is a
mechanism for transport of molecules across membranes. Usually unionized and lipid
soluble substances are absorbed by simple diffusion or passive diffusion. “Diffusion is
a law of transport of molecules from the region of higher concentration to the region
of lower concentration”. The absorption of the basti dravya is also by diffusion and
many factors influence this rate of diffusion and thus absorption. These factors are as
follows.
Physical state: Liquids are absorbed better than solids.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 153
Ingredients of basti, their solubility and their homogenous mixing : Lipids and lipid
soluble drugs penetrate into the cell more rapidly than the water soluble drugs. The
homogenous mixture of basti dravyaa is important.
Temperature- Luke warm solutions are rapidlu absorbed because of vasodilatation,
whereas cold solutions are absorbed slowly.
Size of the molecule, its disintegration time and dissolution time: Simpler and
smaller the size of the molecule, faster is the absorption. If the disintegration and
dissolution time of the compound is less then the absorption is faster.
Quantity and concentration gradient of the basti dravya : Higher the quantity
lesser is the retention time. Concentrated solutions are absorbed more rapidly than the
weak solutions.
pH of the GI fluid- Alkaline drugs are absorbed in the alkaline medium i.e distal
ileum and large intestine, where as acidic drugs are absorbed in the stomach and
proximal part of the small intestines.
Ionization: Unionized component predominantly lipid soluble are absorbed rapidly.
Surface area of absorption- Absorption is more in intestines than in stomach, because
of the larger surface area of the former .
Vascularity- Richer the vascularity greater the absorption.
Structural and functional status of the rectum:
In the healthy and empty rectum the absorption is more and in the diseased condition,
the presence of stool delays the absorption.
The concentration of the basti dravyas is higher in the lumen of the rectum and
in the cells surrounding the rectum. Hence the molecules of basti move from higher

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 154
concentration to the lower concentration i.e from the rectum to the surrounding cells
and there, they are absorbed into the rectal veins. The lipid soluble substances like
vitamin- A D and K and essential minerals such as calcium, phosphorus , magnesium,
sodium, and chlorine etc present in the milk are in unionized form and hence absorbed
rapidly. The surface area of the small intestine and rectum is more and it has very rich
blood supply, moreover the basti was given in the morning after the patient has passed
the stool i.e when the rectum was empty. Hence all these factors enhance the
absorption of the basti dravyas from the rectum through the rectal mucosa.
The cow’s milk which is the main ingredient of the Ksheera Basti is rich in
calcium, phosphorus, magnesium, potassium, sodium, chlorine etc. It also contains fat
soluble vitamins like vitamin –A, D and K. These minerals and vitamins help in bone
formation. A study conducted by Finnish researchres, published in November-2005
issue of American Journal of Clinical nutrition revealed that, only dairy calcium is
better than synthetic calcium supplements for growing girl’s bones. The superiority of
milk over other calcium supplements is because the bone health is not a mono-
nutrient issue and milk contains all the essential vitamins and mineral nutrients
required for bone formation. Apart from this the ghee contains phospholipids which
plays an important role in the mineralization of bones.
Discussion on Materials and Methods
Discussion on selection of drugs
Trikatu churna is attributed with like deepana, pachana, vatanulomana,
shothahara, shula prashamana. This is easily available and cost effective also very
less.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 155
Panchatikta is said to be shreshta among the tikta rasa pradhana dravyas. These drugs
are attributed with karmas like vedanasthapana, shothahara, anulomana, rasayana,
deepana, pachana
Bala has the karmas like vatahara, balya, vedanasthapana and brumhana.
Godugdha and goghrita possess the karmas like vata nashaka, jeevaniya, balya,
bruhmana, and rasayana. The chemical composition of godugdha includes calcium,
magnesium, potassium etc.
Saindhava, madhu and shatapushpa are mainly used in administration of basti. These
facilitate the drug absorption. Hence, these drugs are selected for the present study.
Discussion on Instruments
There are many devices to administer basti but in present study douche set,
enema syringe and rubber catheter were selected because they are easily available
and it can be used very safely.
Discussion on Aims
The present work was under taken for the analytical study of asthi pradoshaja
vikaras supported by the study on the effect of panchatikta ksheera sarpi and bala
sadhita ksheera sarpi in sandhigatavata.
The contemporary science aids us to understanding Ayurvedic concepts better, hence
in the present work sandhigatavata was taken for the study.
Discussion on Inclusion criteria
Individuals of either sex between the age group 30-60 years were selected, as
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 156
the degeneration of articular cartilage in primary OA starts with the process of ageing
i.e. after 30 years. OA is seen in the lower age groups are usually secondary. The
individuals willing for the treatment were selected because the duration of the
treatment is long.
Discussion on Exclusion criteria
Pregnant women were excluded because the kala basti is contraindicated
during this period and also to avoid the complications. Individuals with other systemic
disorders like bleeding piles etc were excluded to avoid the interference in the action
of drug and also to avoid complications.
Discussion on Diagnostic criteria
Pain, stiffness, crepitus and swelling were considered as the diagnostic criteria
as there is no evidence of inflammatory infiltration in all cases of OA. Osteoarthritis
with radiological changes were taken , because in most of the pathologies of the knee
joint, X-ray fails to show any abnormality as the cartilaginous pathologies outnumber
the bony pathologies. Therefore in order to maintain the homologenesity in between
the groups, radiological changes were considered under diagnostic criteria.
Discussion on Intervention
The study was designed in such way so as to get a clear picture regarding efficacies of
the drugs which were used in the present study.
Discussion on Statistical Analysis -
Contingency Co-efficient: It is applied when Categorical Data Analysis is to be done.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 157
Then a contingency table can be used to express the relationship between the variables
Descriptive statistics: The Descriptive procedure displays univariate summary statistics
for several variables in a single table and calculates standardized values (z scores).
Variables can be ordered by the size of their means (in ascending or descending order),
alphabetically, or by the order in which one selects the variables (the default).
Chi-square test: The Chi-Square Test procedure tabulates a variable into categories and
computes a chi-square statistic. This goodness-of-fit test compares the observed and
expected frequencies in each category to test either that all categories contain the same
proportion of values or that each category contains a user-specified proportion of values.
Discussion on Observations and Results
Discussion on General observations
Age: In the present series of 30 cases, it has been observed that this disease most
commonly manifests in the 4th decade (50.0%). Increase in age is one of the risk
factor for OA observed in the study. Especially patients belonging to the age group
41–50 years were engaged in their household and other jobs.
Sex: In the present study, it has been observed that the incidence of this disease more
in females. Here the lack of female hormone (oestrogen) in the peri-menopausal
period also plays an important role. Biosynthesis of articular cartilage is influenced by
sex hormone in females.
Marital status: Married patients showed more susceptiblity (96.6%) for
janusandhigatavata. Though it is not a risk factor for Sandhigata Vata, but the disease
was prevalent in the post marital age.

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 158
Education: In this study, maximum numbers of patients i.e. 26.7% were illiterate. It
was revealed from the study that due to illiteracy, people had to involve in more
strenuous work and were not taking nutritious diet, which lead to Dhatukshaya.
Religion: In this clinical study, most of the patients i.e. 96.7% were Hindus. This data
indicates that there is predominance of hindu population in Mysore district.
Habitat: In this clinical study, maximum numbers of patients i.e. 60.0% were from
urban area. It may because the study was carried out on urban population.
Socio-economical status: Middle class patients were more susceptible (76.7%) to
janusandhigatavata. It is quite natural that the people from middle class are exposed to
more physical stress and strain which acts as a risk factor for OA.
Occupation: In the present series of 30 cases, it has been observed that, the incidence
of this disease was more in housewives (50.0%). This percentage of patients implies
that mostly they were performing household work for long duration in standing
posture and had to lift heavy loads.
Diet: The present study revealed that, the patients who were consuming mixed diet
were more susceptible (56.7%) to janusandhigatavata. The study however could not
generalize the fact that vegetarians are on safer side from the disease as the sample
size taken was very small.
Prakruti: Patients belonging to Vata pitta prakruti (43.3%) and pitta kapha prakruti
(43.3%) showed equal incidence in the manifestation of janusandhigatavata. The
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 159
study however could not generalize, as the sample size taken was very small.
Sara: In the present study all the 30 patients (100%) were having madhyama sara.
Samhanana: Among 30 patients, 21 patients (70.0%) were of madhyama samhananain the present study. Pramana: Among 30 patients 26 patients (86.66%) were of madhyama pramana.
Sattva: Among 30 patients, 22 patients (76.66%) were of madhyama sattva in the present study.
Satmya: In the present study all the 30 patients (100%) were of madhyama satmya.
Koshta: In the present study among 30 patients, 24 patients (80.0%) were of
madhyama koshta.
Agni: Among 30 patients 15 patients (50.0%) had Vishamagni in the present study.
Bala: In the present study among the 30 patients, 28 patients (93.33%) of them had
madhyama bala.
Vyayama shakti: Among 30 patients, 28 patients (93.33%) had madhyama vyayama
shakti in the present study.
Joint involvement: Among the 30 patients, 28 patients (86.6%) had bilateral joint
involvement in the present study. This shows the Chronicity of the disease.

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 160
Discussion on Results
Joint pain
On observing the results, it was noted that there was improvement in both the groups
and statistically highly significant with P value 0.001 in Group A and Group B is
statistically significant with P value 0.008. But comparatively Group A shows high
significance than Group B. (Rt Knee)
On observing the results, it was noted that there was improvement seen in both the
groups and statistically highly significant with P value 0.000 in the both groups. But
Group A shows high significance than Group B. (Lt Knee)
Hence it can be said that panchatikta ksheera sarpi had good effect on joint pain due
to vedanasthapana and vatahara properties.
Joint stiffness
On observing the results, it was noted that there was improvement in both the groups
and statistically highly significant with P value 0.005 in Group A and Group B is
statistically significant with P value 0.004. But comparatively Group B shows
significance than Group A. (Rt Knee)
On observing the results, it was noted that there was improvement in both the groups
and statistically highly significant with P value 0.002 in Group B and Group A is
statistically significant with P value 0.018. But comparatively Group B shows
significant result than Group A. (Lt Knee)
Hence it can be said that bala ksheera sarpi had good effect on joint stiffness due to
snehana and vatahara properties.

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 161
Joint swelling
On observing the results, it was noted that there was improvement in both the groups
and statistically highly significant with P value 0.021 in Group A and Group B is
statistically significant with P value 0.031. But comparatively Group A shows
significant result than Group B. (Rt Knee)
Hence it can be said that panchatikta ksheera sarpi had good effect on joint stiffness
due to shothahara property.
On observing the results, it was noted that there was improvement in both the groups
and statistically highly significant with P value 0.005 in Group A and Group B is
statistically significant with P value 0.049. But comparatively Group B shows
significant result than Group A. (Lt Knee)
Hence it can be said that bala ksheera sarpi had good effect on joint stiffness due to
shothahara property.
Joint crepitus
On observing the results, it was noted that there was improvement in both the groups
and statistically highly significant with P value 0.004 in Group A and Group B is
statistically significant with P value 0.008. But comparatively Group A shows
significant result than Group B.
On observing the results, it was noted that there was improvement in both the groups
and statistically highly significant with P value 0.003 in Group A and Group B is
statistically significant with P value 0.008. But comparatively Group A shows
significant result than Group B.
Hence it can be said that panchatikta ksheera sarpi had effect on joint crepitus due to
snehana and vatahara properties.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 162
Overall assessment
On observing overall results, it was noted that there was improvement in both the
groups and statistically significant with P value 0.042 in Group A and Group B is
statistically non significant with P value 0.819. But comparatively Group A has got
significant result than Group B.
The above findings support the statement of Charaka samhita regarding superiority of
tikta ksheera sarpi basti. Finally it can be concluded that panchatikta ksheera sarpi has
a better result in janusandhigatavata
Radiological findings
In the present study radiology (X-ray) was used to restablish the involvment of Asthi
in janusandhigatavata and also to observe the changes occurinng in the Asthi, after the
kala basti. Due to this reason X-ray was taken for all the 30 patients, before treatment
to rule out the involvement of Asthi and after the treatment and after the end of follow
up to find out the changes. In radiological findings of before treatment all the 30
patients showed the osteophytes and joint space narrowing in the Asthi. But after the
treatment and at the end of follow up there were no marked changes in the
osteophytes which imply that there is no increase of osteophytes in the Asthi. It may
need longer observation to find the osteophytes changes (reduction in osteophytes) in
the Asthi.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 163
RECOMMENDATION FOR FURTHER STUDY
Same study can be done in a larger sample and for a long duration.
An experimental study can be carried out ,to identify the exact action of
panchatikta ghrita on various components of the body
The same study can be done in different age groups so as to assess the efficacy
of the drug.
With other investigations like BMD the same study can be carried out to
evaluate the efficacy of panchatikta ghrita.

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 164
CONCLUSION
Asthi pradoshaja vikara is a condition in which Asthi gets vitiated extremely by
the vata dosha and changes its natural form and leads to many disorders.
Ativyayama, ati sankshobha, ati vighattana and vatala ahara-vihara are the four
nidanas for Asthi pradoshaja vikaras.
Avyakta or alpavyakta lakshanas of Asthi pradoshaja vikaras are considered as
poorvarupa.
Asthi pradoshaja vikaras are classified into various types based on the
involvement of Asthi, danta, kesha and nakha.
As Asthi pradoshaja vikaras are marmasthigata vyadhis, so panchakarma is the
best choice of treatment.
Janusandhigatavata is one among the Asthi pradoshaja vikaras.
Vata is the main dosha involved in the manifestation of janusandhigatavata.
Prevalence of janusandhigatavata was more in females, housewives and between
the age group of 41-50 years.
The panchatikta ksheera sarpi was more effective in subsiding joint pain, joint
crepitation and joint swelling and bala sadhita ksheera sarpi was effective in
reducing joint stiffness and swelling.
The overall effect of thearapy was significant in Group A with p value 0.042
when compared to Group B at the p value 0.819.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 165
SUMMARY
The Present study entitled “Concept of Asthi pradoshaja vikaras w.s.r.to
management of Sandhigtavata” was aimed at understanding the concept of Asthi
pradoshaja vikaras and applying the concept of chikitsa Siddhanta of Asthi pradoshaja
vikaras i.e, tikta ksheera basti in the management of janusandhigatavata.
The present dissertation work was divided into 2 parts. The first chapter deals
with the introduction and concept of Asthi pradoshaja vikaras supported by the
contemporary science view. In the second chapter, concepts of Janusandhigatavata
contemporary view in detail are explained. In the third chapter, concept of basti
especially Kala basti is explained. The fourth chapter deals with the, Drug review
(trikatu, panchatikta, bala, godugdha, goghrita, shatapushpa, madhu and saindhava)
was dealt.
In the second part, Materials & Methods, Observation of clinical trials, Results,
Statistical tables & graphs, Discussion, Conclusions along with recommendation for
future study were dealt. A total of 30 Patients in two groups (each group contains
15patients each) were selected for the study.
The patients of group A were administered with trikatu churna for ama
pachana. After attaining niramavastha patients were subjected to abhyanga with
ksheerabala taila followed by nadi sweda. The sequence of 15 bastis in the form of
kala basti administered starting from anuvasana with panchatikta ghrita (9 anuvasana)
and niruha basti with panchatikta ksheera sarpi (6 niruha) and were advised 30 days
parihara kala. The patients of group B were administered with trikatu churna for ama
pachana. After attaining niramavastha patients were subjected to abhyanga with
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 166
ksheerabala taila followed by nadi sweda. The sequence of 15 bastis in the form of
kala basti administered starting from anuvasana with bala ghrita (9 anuvasana) and
niruha basti with bala sadhita ksheera sarpi (6 niruha) and adviced 30 days parihara
kala.
The different parameters of the study were observed and recorded before
treatment, after treatment and after the follow up. The observations and results were
statistically analyzed for better interpretation. Based on result statistical analysis and
general observations, Group A showed significant result with p value 0.042 and with
no statistical significance in Group B with p value 0.819. Radiological changes were
not seen in both the groups after the treatment and follow up.
The conclusion was derived on the basis of observations & results. Future
perspective of the study is highlighted as an aid for the future research workers.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 167
BIBLIOGRAPHY
1. Raja Radha Kantha Deva, Shabda Kalpa Druma, part one, 3rd
Edition,Varanasi,The Choukhamba Sanskrit Series Office,1967,PP:155.
2. Raja Radha Kantha Deva, Shabda Kalpa Druma, part one, 3rd
Edition,Varanasi,The Choukhamba Sanskrit Series Office,1967,PP:155.
3. Williams M.M, Sanskrit-English Dictionary, Varanasi, Motilal Banarsidass,
Reprinted 1990, PP: 122.
4. Taranath Tarkavachaspathy Bhattacharya, Vachaspathyam, part four, Varanasi,
Chowkambha Sanskrit Series Office, 1969, PP: 4468.
5. Raja Radha Kantha Deva, Shabda Kalpa Druma, part three, 3rd
Edition,Varanasi,The Choukhamba Sanskrit Series Office,1967,PP:275.
6. V.S.Apte, Sanskrit English Dictionary, Varanasi, Motilal Banarsidass, 1968, PP: 350.
7. Raja Radha Kantha Deva, Shabda Kalpa Druma, part two, 3rd
Edition,Varanasi,The Choukhamba Sanskrit Series Office,1967,PP:753.
8. Taranath Tarkavachaspathy Bhattacharya, Vachaspathyam, part five, Varanasi,
Chowkambha Sanskria Series Office, 1969, PP: 3793.
9. V.S.Apte, Sanskrit English Dictionary, Varanasi, Motilal Banarsidass, 1968, PP: 261.
10. Raja Radha Kantha Deva, Shabda Kalpa Druma, part two, 3rd
Edition,Varanasi,The Choukhamba Sanskrit Series Office,1967,PP:496.
11. Taranath Tarkavachaspathy Bhattacharya, Vachaspathyam, part four, Varanasi,
Chowkambha Sanskrit Series Office, 1969, PP: 3003.
12. Raja Radha Kantha Deva, Shabda Kalpa Druma, part four, 3rd
Edition,Varanasi,The Choukhamba Sanskrit Series Office,1967,PP:372.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 168
13. Raja Radha Kantha Deva, Shabda Kalpa Druma, part two, 3rd
Edition,Varanasi,The Choukhamba Sanskrit Series Office,1967,PP:372.
14. V.S.Apte, Sanskrit English Dictionary, Varanasi, Motilal Banarsidass, 1968, PP: 506.
15. Raja Radha Kantha Deva, Shabda Kalpa Druma, part one, 3rd
Edition,Varanasi,The Choukhamba Sanskrit Series Office,1967,PP:155.
16. Taranath Tarkavachaspathy Bhattacharya, Vachaspathyam, part one, Varanasi,
Chowkambha Sanskria Series Office, 1969, PP: 568.
17. Raja Radha Kantha Deva, Shabda Kalpa Druma, part one, 3rd
Edition,Varanasi,The Choukhamba Sanskrit Series Office,1967,PP:155.
18. Laxman Sastri Pansikar, Amarakosha, 7th Edition, Bombay, Nirnaya Sagar Press,
1934, PP: 1210.
19. Williams M.M, Sanskrit-English Dictionary, Varanasi, Motilal Banarsidass,
Reprinted 1990, PP: 122, 250,289,296.
20. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 514.
21. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 59.
22. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 516.
23. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 59.
24. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 187.
25. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 169
Chaukhambha Prakashan, 2007, PP: 515.
26. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 69.
27. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 574.
28. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 250.
29. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 392.
30. Shivprasad Sharma, Ashtanga Sangraha of Vagbhata, 1st edition, Varanasi,
Choukhamba Sanskrit Series Office, 2006, PP: 314.
31. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 337.
32. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 365-366.
33. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 360.
34. Shivprasad Sharma, Ashtanga Sangraha of Vagbhata, 1st edition, Varanasi,
Choukhamba Sanskrit Series Office, 2006, PP: 68.
35. Brahma Sankara Misra, Bhavaprakasha of Bhavamishra Vol 2, 11th Edition,
Varanasi, Chaukhambha Sanskrit Sansthan, 2009, PP: 48-49.
36. Satyapala, Kasyapa Samhita of Vriddha Jivaka, Varanasi, Chaukambha Sanskrit
Sansthan, 2006, PP: 75.
37. Giriraja Dhayalu Shukla, Bhela Samhita of Bhela, 1st Edition, Varanasi,
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 170
Chowkamba Vidya Bhavan, 1959, PP: 100.
38. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 365.
39. Shivprasad Sharma, Ashtanga Sangraha of Vagbhata, 1st edition, Varanasi,
Choukhamba Sanskrit Series Office, 2006, PP: 305.
40. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 366.
41. Shivprasad Sharma, Ashtanga Sangraha of Vagbhata, 1st edition, Varanasi,
Choukhamba Sanskrit Series Office, 2006, PP: 69.
42. Brahma Sankara Misra, Bhavaprakasha of Bhavamishra Vol 2, 11th Edition,
Varanasi, Chaukhambha Sanskrit Sansthan, 2009, PP: 49.
43. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 67.
44. Shivprasad Sharma, Ashtanga Sangraha of Vagbhata, 1st edition, Varanasi,
Choukhamba Sanskrit Series Office, 2006, PP: 69.
45. Brahma Sankara Misra, Bhavaprakasha of Bhavamishra Vol 2, 11th Edition,
Varanasi, Chaukhambha Sanskrit Sansthan, 2009, PP: 46.
46. Parashuram Shastri Vidyasagar, Sarngadhara Samhita of Sarngadhara, Varanasi,
Chaukhamba Surbharati Prakashan, 2006, PP: 46.
47. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 515.
48. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 253.
49. Brahma Sankara Misra, Bhavaprakasha of Bhavamishra Vol 2, 11th Edition,

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 171
Varanasi, Chaukhambha Sanskrit Sansthan, 2009, PP: 64.
50. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 278.
51. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 152.
52. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 70.
53. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 174.
54. Shivprasad Sharma, Ashtanga Sangraha of Vagbhata, 1st edition, Varanasi,
Choukhamba Sanskrit Series Office, 2006, PP: 150.
55. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 103.
56. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 69.
57. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 185.
58. Shivprasad Sharma, Ashtanga Sangraha of Vagbhata, 1st edition, Varanasi,
Choukhamba Sanskrit Series Office, 2006, PP: 150.
59. Kshemaraj Shri Krishnadas, Harita Samhita of Harita, Mumbai, Vunkateshwar
Mudranalaya, 1984, PP: 267-268.
60. Giriraja Dhayalu Shukla, Bhela Samhita of Bhela, 1st Edition, Varanasi,
Chowkamba Vidya Bhavan, 1959, PP: 21.
61. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 172
Surabharati Prakashan, Reprinted 2008, PP: 115.
62. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 116.
63. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 125.
64. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 179.
65. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 116.
66. Yogindra Nath Sen, Charaka Samhita of Charaka, 2nd Vol, Banaras, Chowkhamba
Sanskrit Series Office, 1922, PP: 988.
67. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 252.
68. Yogindra Nath Sen, Charaka Samhita of Charaka, 2nd Vol, Banaras, Chowkhamba
Sanskrit Series Office, 1922, PP: 989.
69. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 251.
70. Yogindra Nath Sen, Charaka Samhita of Charaka, 2nd Vol, Banaras, Chowkhamba
Sanskrit Series Office, 1922, PP: 988.
71. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 617.
72. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 617.
73. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 173
Chaukhambha Prakashan, 2007, PP: 179.
74. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 846.
75. Vaidhya Harishatri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 846.
76. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 332.
77. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 332.
78. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 846.
79. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 201.
80. Yadunandana Upadhyaya, Madava Nidana Vol 1, Varanasi, Chaukhambha
Sanskrit Sansthan, 2003, PP: 513.
81. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 201.
82. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 332.
83. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 849.
84. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 332.
85. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 174
Varanasi, Chaukhambha Orientalia, 2009, PP: 847.
86. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 322.
87. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 859.
88. Yadunandana Upadhyaya, Madava Nidana Vol 1, Varanasi, Chaukhambha
Sanskrit Sansthan, 2003, PP: 204.
89. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 606.
90. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 322.
91. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 860.
92. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 606.
93. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 322.
94. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 860.
95. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 320.
96. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 889.
97. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 175
Chaukhambha Prakashan, 2007, PP: 617.
98. Dingari Lakshmana Chary, Shalakya Tantra, Reprinted, Delhi, Chuakhamba
Sanskrit Pratishthan, 2007, PP: 253-253.
99. Dingari Lakshmana Chary, Shalakya Tantra, Reprinted, Delhi, Chuakhamba
Sanskrit Pratishthan, 2007, PP: 29-31.
100. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 180.
101. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 420.
102. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 187.
103. Shivprasad Sharma, Ashtanga Sangraha of Vagbhata, 1st edition, Varanasi,
Choukhamba Sanskrit Series Office, 2006, PP: 152.
104. Indradev Tripathi & Dayashankar Tripati, Yogaratnakara, 1st Edition, Varanasi,
KrishnadasAcademy, 1998, PP: 412.
105. Kshemaraj Shri Krishnadas, Harita Samhita of Harita, Mumbai, Vunkateshwar
Mudranalaya, 1984, PP: 267-268.
106. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 482.
107. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 852.
108. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 851.
109. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 176
Varanasi, Chaukhambha Orientalia, 2009, PP: 852.
110. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 483.
111. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 852.
112. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 479.
113. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 862.
114. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 611.
115. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 479.
116. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 862.
117. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 479.
118. Siddharth N Shah, API Text book of Medicine, 8th Edition, Mumbai, The
Association of Physicians of India, 2008, PP: 214.
119. Catherine Soanes, Oxford Dictionary Theaurus and Worldwide Guide, 25th
Edition, New Delhi, Oxford University Press, 2005, PP: 90.
120. Poddar S, Ajay Bhagat, Handbook of Osteology, 11th Edition, Patna, Scientific
Book Company, 2002, PP: 1.
121. Poddar S, Ajay Bhagat, Handbook of Osteology, 11th Edition, Patna, Scientific
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 177
Book Company, 2002, PP: 1-3.
122. Poddar S, Ajay Bhagat, Handbook of Osteology, 11th Edition, Patna, Scientific
Book Company, 2002, PP: 15.
123. Poddar S, Ajay Bhagat, Handbook of Osteology, 11th Edition, Patna, Scientific
Book Company, 2002, PP: 4-5.
124. Poddar S, Ajay Bhagat, Handbook of Osteology, 11th Edition, Patna, Scientific
Book Company, 2002, PP: 7.
125. Poddar S, Ajay Bhagat, Handbook of Osteology, 11th Edition, Patna, Scientific
Book Company, 2002, PP: 9.
126. Siddharth N Shah, API Text book of Medicine, 8th Edition, Mumbai, The
Association of Physicians of India, 2008, PP: 215-217.
127. Poddar S, Ajay Bhagat, Handbook of Osteology, 11th Edition, Patna, Scientific
Book Company, 2002, PP: 1.
128. Poddar S, Ajay Bhagat, Handbook of Osteology, 11th Edition, Patna, Scientific
Book Company, 2002, PP: 11.
129. Poddar S, Ajay Bhagat, Handbook of Osteology, 11th Edition, Patna, Scientific
Book Company, 2002, PP: 15.
130. Poddar S, Ajay Bhagat, Handbook of Osteology, 11th Edition, Patna, Scientific
Book Company, 2002, PP: 15.
131. www.ncbi.nlm.nih.gov/pubmed
132. Davidson’s Principles and Practice of Medicine, 19th Edition, Churchill
Livingstone, 2002, PP: 985.
133. Siddharth N Shah, API Text book of Medicine, 8th Edition, Mumbai, The
Association of Physicians of India, 2008, PP: 218-223.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 178
134. Taranath Tarkavachaspathy Bhattacharya, Vachaspathyam, part four, Varanasi,
Chowkambha Sanskria Series Office, 1969, PP: 3113.
135. Taranath Tarkavachaspathy Bhattacharya, Vachaspathyam, part two, Varanasi,
Chowkambha Sanskria Series Office, 1969, PP: 1365.
136. Raja Radha Kantha Deva, Shabda Kalpa Druma, part five, 3rd
Edition,Varanasi,The Choukhamba Sanskrit Series Office,1967,PP:240.
137. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 367.
138. Raja Radha Kantha Deva, Shabda Kalpa Druma, part two, 3rd
Edition,Varanasi,The Choukhamba Sanskrit Series Office,1967,PP:298.
139. Raja Radha Kantha Deva, Shabda Kalpa Druma, part two, 3rd
Edition,Varanasi,The Choukhamba Sanskrit Series Office,1967,PP:285.
140. Raja Radha Kantha Deva, Shabda Kalpa Druma, part four, 3rd
Edition,Varanasi,The Choukhamba Sanskrit Series Office,1967,PP:325.
141. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 99.
142. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 620.
143. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 617.
144. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 99.
145. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 530.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 179
146. Shivprasad Sharma, Ashtanga Sangraha of Vagbhata, 1st edition, Varanasi,
Choukhamba Sanskrit Series Office, 2006, PP: 355.
147. Yadunandana Upadhyaya, Madava Nidana Vol 1, Varanasi, Chaukhambha
Sanskrit Sansthan, 2003, PP: 511.
148. Indradev Tripathi & Dayashankar Tripati, Yogaratnakara, 1st Edition, Varanasi,
KrishnadasAcademy, 1998, PP: 400.
149. Brahma Sankara Misra, Bhavaprakasha of Bhavamishra Vol 2, 11th Edition,
Varanasi, Chaukhambha Sanskrit Sansthan, 2009, PP: 227.
150. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 617.
151. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 618.
152. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 261.
153. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 531.
154. Shivprasad Sharma, Ashtanga Sangraha of Vagbhata, 1st edition, Varanasi,
Choukhamba Sanskrit Series Office, 2006, PP: 414.
155. Yadunandana Upadhyaya, Madava Nidana Vol 1, Varanasi, Chaukhambha
Sanskrit Sansthan, 2003, PP: 420.
156. Brahma Sankara Misra, Bhavaprakasha of Bhavamishra Vol 2, 11th Edition,
Varanasi, Chaukhambha Sanskrit Sansthan, 2009, PP: 228.
157. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 617.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 180
158. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 530-531.
159. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 617.
160. Yadunandana Upadhyaya, Madava Nidana Vol 1, Varanasi, Chaukhambha
Sanskrit Sansthan, 2003, PP: 575, 560-561, 541, 520.
161. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 621.
162. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 420.
163. Shivprasad Sharma, Ashtanga Sangraha of Vagbhata, 1st edition, Varanasi,
Choukhamba Sanskrit Series Office, 2006, PP: 414.
164. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 722.
165. Ravidatta Shastry, Chakradatta of Chakrapanidataa, 4th edition, Varanasi,
Chaukhamba Surbharati Prakashan, 2006, PP:
166. Indradev Tripathi & Dayashankar Tripati, Yogaratnakara, 1st Edition, Varanasi,
KrishnadasAcademy, 1998, PP: 410.
167. Siddhi Nandan Mishra, Bhaisajya Ratnavali of Kaviraj Govind Das Sen,
Reprinted, Varanasi, Chaukhamba Surbharati Prakashan, 2007, PP: 527.
168. Brahma Sankara Misra, Bhavaprakasha of Bhavamishra Vol 2, 11th Edition,
Varanasi, Chaukhambha Sanskrit Sansthan, 2009, PP: 228.
169. Indradev Tripathi & Dayashankar Tripati, Yogaratnakara, 1st Edition, Varanasi,
KrishnadasAcademy, 1998, PP: 434, 437, 418, 420-423.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 181
170. Siddhi Nandan Mishra, Bhaisajya Ratnavali of Kaviraj Govind Das Sen,
Reprinted, Varanasi, Chaukhamba Surbharati Prakashan, 2007, PP: 546, 610, 604-
605,608.
171. Ravidatta Shastry, Chakradatta of Chakrapanidataa, 4th Edition, Varanasi,
Chaukhamba Surbharati Prakashan, 2006, PP: 139, 148, 150,153.
172. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 621.
173. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 422.
174. Kumar & Clark, Clinical Medicine, 6th Edition, Elsevier Limited, 2005, PP: 550.
175. Siddharth N Shah, API Text book of Medicine, 8th Edition, Mumbai, The
Association of Physicians of India, 2008, PP: 279.
176. www.wiktionary.com
177. www.thefreedictionary.com
178. www.dictionary.sensagent.com
179. Kumar & Clark, Clinical Medicine, 6th Edition, Elsevier Limited, 2005, PP: 551.
180. Kumar & Clark, Clinical Medicine, 6th Edition, Elsevier Limited, 2005, PP: 552.
181. Kumar & Clark, Clinical Medicine, 6th Edition, Elsevier Limited, 2005, PP: 552.
182. Siddharth N Shah, API Text book of Medicine, 8th Edition, Mumbai, The
Association of Physicians of India, 2008, PP: 280.
183. Kumar & Clark, Clinical Medicine, 6th Edition, Elsevier Limited, 2005, PP: 552.
184. L.C.Gupta etl, Differential Diagnosis, 7th Edition, New Delhi, Jaypee Brothers
Medical Publishers (P) Ltd, 2005, PP: 121-123.
185. Kumar & Clark, Clinical Medicine, 6th Edition, Elsevier Limited, 2005, PP: 553.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 182
186. Siddharth N Shah, API Text book of Medicine, 8th Edition, Mumbai, The
Association of Physicians of India, 2008, PP: 282.
187. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 525.
188. H.S.Kasture, Ayurvediya Panchakarma Vignana, 8th Edition, Patna, Shri
Bhaidyanath Ayurveda Bhavan Ltd, 2005, PP: 187.
189. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 270.
190. Parashuram Shastri Vidyasagar, Sarngadhara Samhita of Sarngadhara, Varanasi,
Chaukhamba Surbharati Prakashan, 2006, PP: 319.
191. H.S.Kasture, Ayurvediya Panchakarma Vignana, 8th Edition, Patna, Shri
Bhaidyanath Ayurveda Bhavan Ltd, 2005, PP: 346-350.
192. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 684.
193. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 282.
194. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 526.
195. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 526.
196. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 688-689.
197. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 525,527.

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 183
198. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 271-272.
199. Vaidhya Harishastri Paradakara, Ashtanga Hrudaya of Vagbhata, 9th Edition,
Varanasi, Chaukhambha Orientalia, 2009, PP: 273.
200. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 684.
201. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 540,535.
202. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 114-115,682.
203. Acharya Y.T, Acharya NR, Sushruta Samhita of Sushruta, Varanasi, Chaukhamba
Surabharati Prakashan, Reprinted 2008, PP: 527-528,535.
204. Shivprasad Sharma, Ashtanga Sangraha of Vagbhata, 1st edition, Varanasi,
Choukhamba Sanskrit Series Office, 2006, PP: 605.
205. P.V.Sharma, Dravya Guna Vignana, part two, 16th Edition, Varanasi,
Chowkhamba Vishwabharati, 1994, PP: 331,275,362.
206. J.L.N.Shastry, Illustrated Dravya Guna Vignana, 2nd Edition, Varanasi,
Chaukhamba Orientalia, 2005, PP: 871, 448, 452.
207. P.V.Sharma, Dravya Guna Vignana, part two, 16th Edition, Varanasi,
Chowkhamba Vishwabharati, 1994, PP: 761,149,242,280,697,735.
208. J.L.N.Shastry, Illustrated Dravya Guna Vignana, 2nd Edition, Varanasi,
Chaukhamba Orientalia, 2005, PP: 265, 123, 407, 367, 250, 93.
209. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 165.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigatavata
Dr.Ranjith Kumar Shetty 184
210. www.milkfacts.org
211. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 166.
212. www.indiadiets.com
213. P.V.Sharma, Dravya Guna Vignana, part two, 16th Edition, Varanasi,
Chowkhamba Vishwabharati, 1994, PP: 403.
214. J.L.N.Shastry, Illustrated Dravya Guna Vignana, 2nd Edition, Varanasi,
Chaukhamba Orientalia, 2005, PP: 258.
215. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 167.
216. www.indiadiets.com
217. Acharya Y.T, Charaka Samhita of Agnivesha, 5th Edition, Varanasi,
Chaukhambha Prakashan, 2007, PP: 170.
218. Vishwanath Dwiedi, Bharatiya Rasashastra, 2nd Edition, Varanasi, Sharma
Ayurveda Mandir, 1987, PP: 376.
219. Sanjay Kadlimatti,P.G Subbanna gouda- Clinical Evaluation of the role of tikta
ksheera basti and ajasthi bhasma in the management of Asthi kshaya vis-a-vis
Osteoporosis- Ayu Journal Vol-30 N0-2 (April-June) 2009 PP-131-141.
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigata vata
Dr.Ranjith Kumar Shetty I
CASESHEET
DEPARTMENT OF POST GRADUATE STUDIES IN AYURVEDA SIDDHANTA
GOVERNMENT AYURVEDA MEDICAL COLLEGE,
MYSORE.
“CONCEPT OF ASTHI PRADOSHAJA VIKARAS W.S.R TO MANAGEMENT OF SANDHIGATA VATA.”
HEAD OF THE DEPARTMENT : Dr. N.Anjaneya Murthy M.D. (Ayu) GUIDE : Dr. N.Anjaneya Murthy M.D. (Ayu) CO-GUIDE : Dr. Kiran Kalaiah M.S (Ortho) CO-GUIDE : Dr. V.A.Chate M.D.(Ayu) RESEARCHER : Dr.Ranjith Kumar Shetty B.A.M.S
Part A- History taking and Examination Sl. No: Name of the patient: Case No: Age: O.P. No: Sex: Male/female I.P No: Religion: H/M/C/Others Ward No: Marital Status: M/UM/W/D Bed No: Socio-economic class: VP/P/LM/M/UM/R Date of Commencement: Education: UE/PS/MS/HS/G/PG Date of Completion: Occupation: Result: Address: Phone No:

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigata vata
Dr.Ranjith Kumar Shetty II
I. VEDANA VRITTANTA:
A. PRADHANA VEDANA: DURATION
Janu sandhi shoola
Janu sandhi shotha
Atopa
Stabdhatha
Others
B. ANUBANDHA VEDANA: DURATION
Difficulty in walking
Disturbed sleep
Others
II. ADYATANA VYADHI VRITTANTA:
A. JANU SANDHI SHOOLA
1. Presentation: Unilateral ( ) Bilateral ( )
2. Mode of Onset : Gradual ( ) Sudden ( )
3. Severity of Pain: Deep ache ( ) Dull ache ( )
4. Duration of pain : Lasts for minutes ( ), Hours ( )
5. Aggravating factors : Aahara:
Vihara:
Kala:
B. JANU SANDHI SHOTHA
1. Mode of Onset: Gradual ( ) , Sudden ( )
2. Time of onset: Precedes pain ( ), Recedes pain ( )
3. Inflammatory changes : Present ( ), Absent ( )
C. ATOPA
Present ( ) Absent ( )
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigata vata
Dr.Ranjith Kumar Shetty III
D. STABDHATA
Range of different movements of knee joints: Restricted ( ), Not Restricted ( )
Time:
E. OTHERS
III. POORVA VYADHI VRITTANTA
A. H/O Previous illness
B. H/O Previous treatment
IV. KULAJA VRITTANTA
A. Pitruja: Present ( ) , Absent ( )
B. Matrija: Present ( ), Absent ( )
V. VAYAKTIKA VRITTANTA
A. Occupation : Hard ( ), Moderate ( ), Sedentary ( )
B. Diet: Veg/Non veg ( Regular/ Irregular )
C. Appetite: Poor ( ), Moderate ( ) , Good ( )
D. Habits: Tea ( ) Beedi ( )
Coffee ( ) Tobacco chewing ( )
Cigarette ( ) Alcohol ( )
Others:
VI. GYNAECOLOGICAL & OBSTETRIC HISTORY
A. Gynecological history
Menstrual Cycle: Regular/ Irregular intervals
B. Obstetric history: G P D A L
VII. EXAMINATION
A. Asta sthana pareeksha:
Nadi: V/P/K/VP/VK/VPK
Mutra: __ times per day, __ times at night
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigata vata
Dr.Ranjith Kumar Shetty IV
Mala: Drava/Baddha/samyak
Jihwa: Alipta/Alpa lipta/ Lipta
Shabda: Prakruta /Vikruta
Sparsha: Prakruta/Vikruta
Druk: Prakruta/Vikruta
Aakruti: Pravara/Madhyama/Avara
B. Janu sandhi pareeksha
Darshana:
Gait- Swinging gait ( ), Limping gait ( )
Swelling: Present ( ), Absent ( )
Muscle wasting: Present ( ), absent ( )
Sparshana
Local temperature: Present ( ), Absent ( )
Local tenderness: Present ( ), Absent ( )
Swelling
Fluctuation: Positive ( ) , Negative ( )
Patellar tap: Positive ( ), Negative ( )
Crepitus: Audible ( ), Palpable ( )
Sandhi Chalana
Flexion:
Extension:
External Rotation:
Internal rotation:
Maana
Apparent shortening:
True shortening:
C. Dashavidha pareeksha
i. Prakruti: V/P/K/VP/PK/KV/VPK
ii. Vikruti: a) Dosha: V/P/K/VP/PK/KV/VPK
b) Dushya: R/Ra/Ma/Me/As/Mj/Sh/Others
iii Sara: Pravara ( ), Madhyama ( ), Avara ( )
iv Samhanana : Pravara ( ), Madhyama ( ), Avara ( )

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigata vata
Dr.Ranjith Kumar Shetty V
v Pramana: Pravara ( ), Madhyama ( ), Avara ( )
vi Satmya : Pravara ( ), Madhyama ( ), Avara ( )
vii Sattva: Pravara ( ), Madhyama ( ), Avara ( )
viii Ahara Shakti
a) Abhyavaharana : Pravara ( ), Madhyama ( ), Avara ( )
b) Jarana: Pravara ( ), Madhyama ( ), Avara ( )
ix Vyayama Shakti: Pravara ( ), Madhyama ( ), Avara ( )
x Vaya: Bala ( ) , Madhyama ( ), Vruddha ( )
D. Prayogashala pareeksha
X-ray of knee joint
Part –B Interpretation
1. Nidana
Aharaja:
Viharaja:
Manasika:
2. Poorvarupa:
3. Rupa :
4. Upashaya- Anupashaya:
5. Samprapti ghataka
a. Dosha
b. Dushya
c. Ama
d. Srotas
e. Sroto dushti prakara
f. Udhbhava sthana
g. Sanchara sthana
h. Adhisthana
i. Roga marga
6. Vyadhi vinishchaya
Chikitsa:
Type of Basti: Kala basti
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigata vata
Dr.Ranjith Kumar Shetty VI
POORVAKARMA
Deepana pachana from ______ to ______
Yoga: Trikatu Churna
Matra: 12gm
Kala: Morning ( ). Afternoon ( ), Evening ( )
Anupana: Ushna jala
Nirama lakshana attained on ______ day
Ama lakshana
Jeerna lakshana
Stimita koshta
Guru koshta
Annaabhilasha
Angamarda
Snehana: Bahya abhyanaga
Dravya:
Sthana:
Kala:
Swedana
Kala:
Bastipoorva ahara
Bastipoorva vihara
Basti dravya prepared properly.
PRADHANA KARMA
Sthiti- Vama parshwa
Group A ( )
Yoga : Anuvasana: Pancha tiktaka ghrita
Niruha:Madhu
Saindhava
Pancha tiktaka ghrita
Shatapushpa Kalka

Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigata vata
Dr.Ranjith Kumar Shetty VII
Pancha tikta saadhita ksheera paka
Duration : 15days, from _________ to ________
Follow up: 30 days from _________ to ________
Group B ( )
Yoga: Anuvasana : Bala ghrita
Niruha : Madhu
Saindhava
Bala ghrita
Shatapushpa kalka
Bala saadhita ksheera paka
Duration :15days from __________ to __________
Follow up : 30 days from __________ to _________
Basti A N A N A N A N A N A N A A A
Date
Bastidana kala
Basti pratyagamana kala
PASCHAT KARMA
Pathya: Aahara Vihara
Part C- Observation and Assessment Subjective Parameters
Before treatment After treatment After follow up
Lakshanas Rt Lt Rt Lt Rt Lt
Sandhishula Sandhishotha Sandhi stabdhata Atopa
Concept of Asthi pradoshaja vikaras w.s.r to management of Sandhigata vata
Dr.Ranjith Kumar Shetty VIII
Objective parameters: X-ray examination
X-ray Before treatment
After treatment
After follow up
Normal Mild changes of OA Moderate changes of OA Severe changes of OA Signature of the Researcher Signature of the Observer
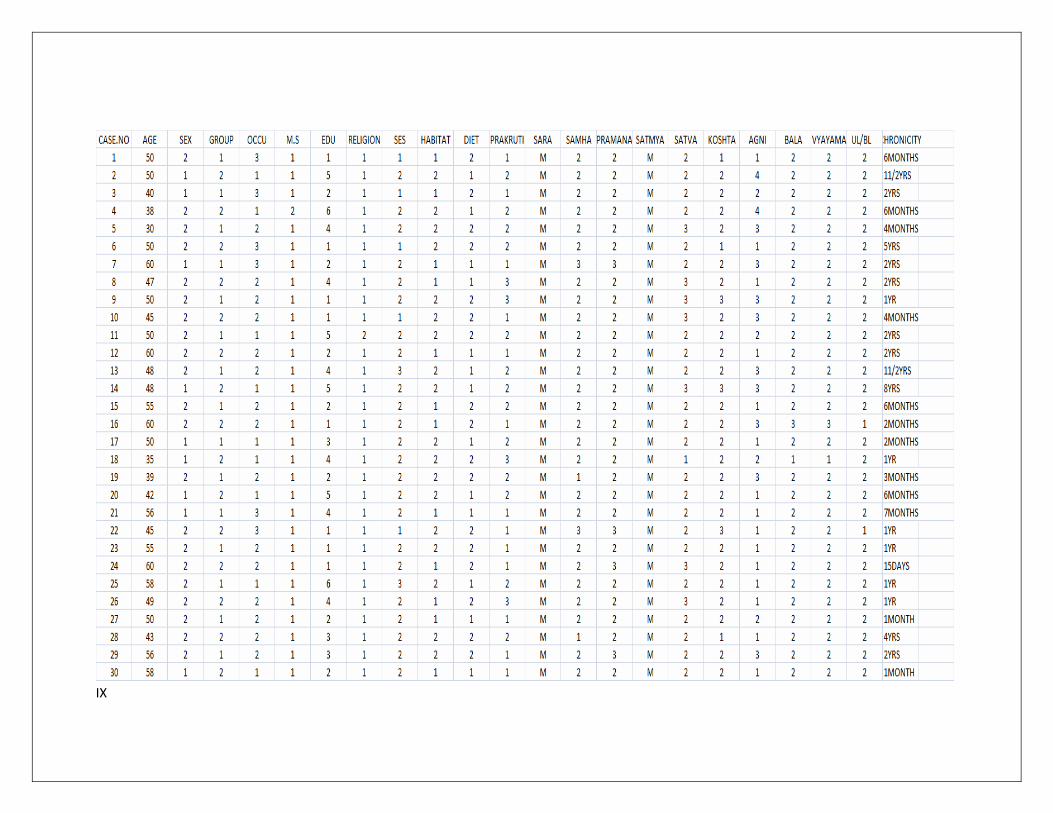
IX
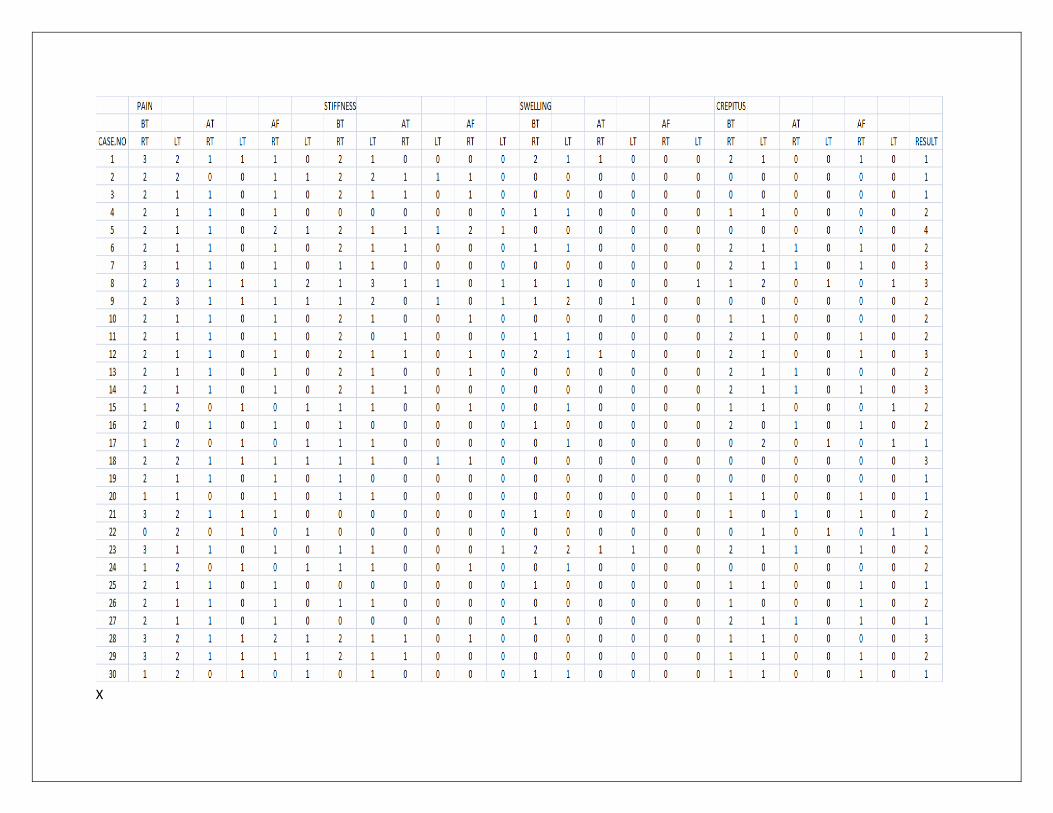
X
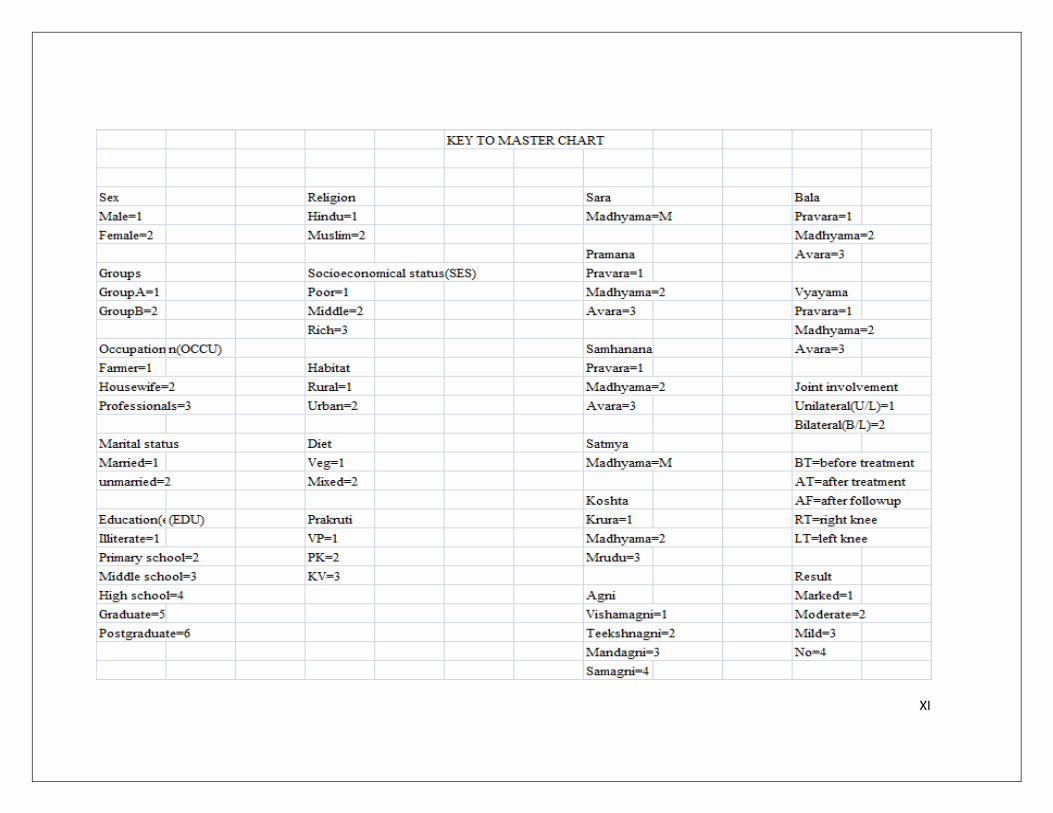
XI

Bala Ghrita Panchatikta Ghrita Panchtikta kwatha churna Balamula kwatha churna
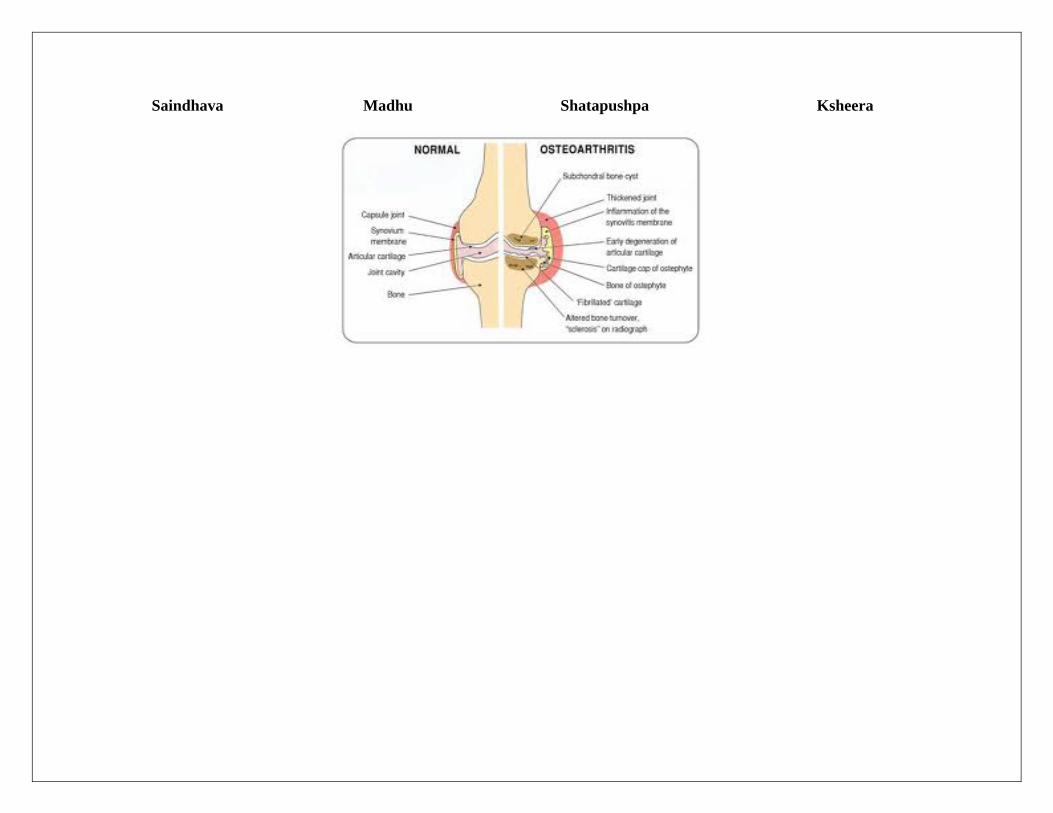
Saindhava Madhu Shatapushpa Ksheera