assisting clients with complex PTSD - Baltimore, MD PTSD.pdf · Complex PTSD: A syndrome in...
28
Interventions LaShaun Williams, PsyD ASSISTING CLIENTS WITH COMPLEX PTSD
Transcript of assisting clients with complex PTSD - Baltimore, MD PTSD.pdf · Complex PTSD: A syndrome in...
Interventions
LaShaun Williams, PsyD
ASSISTING CLIENTS WITH COMPLEX PTSD
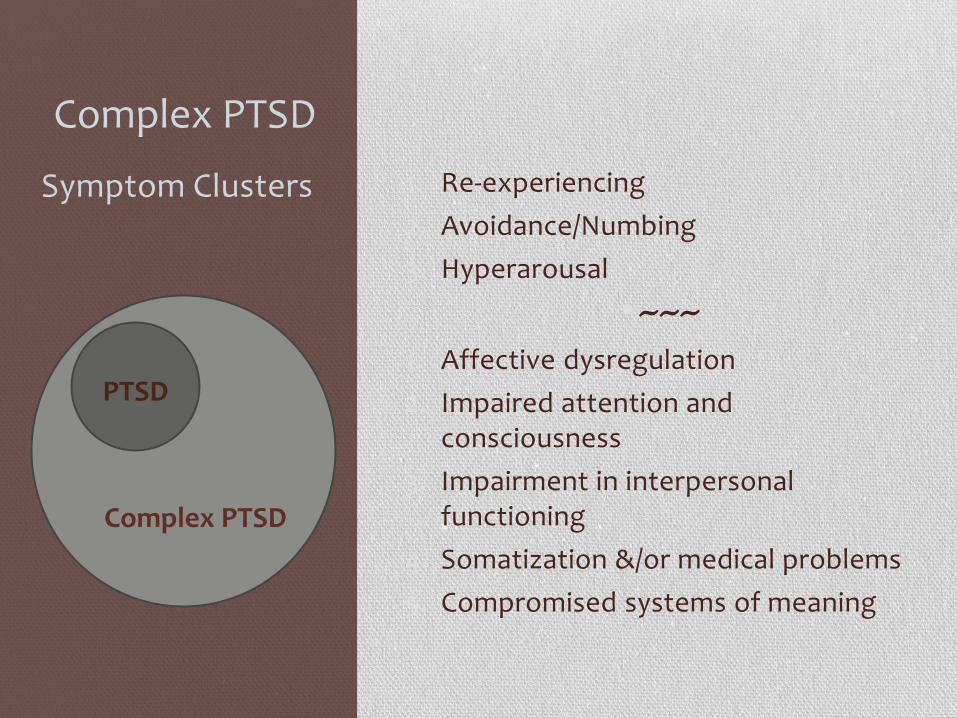
Complex PTSD
1. Re-experiencing
2. Avoidance/Numbing
3. Hyperarousal
•~~~ 1. Affective dysregulation
2. Impaired attention and consciousness
3. Impairment in interpersonal functioning
4. Somatization &/or medical problems
5. Compromised systems of meaning
Symptom Clusters
PTSD
Complex PTSD

Phasic Treatment
• PHASE I
• Stabilizing safety
• Psychoeducation
• Effects of trauma
• Responses as adaptations
• Cummulative nature
• Treatment process
• Develop therapeutic alliance
• Reducing symptom acuity
• PHASE II
• Review and reconstruction of trauma memories
• PHASE III
• Engagement in community life
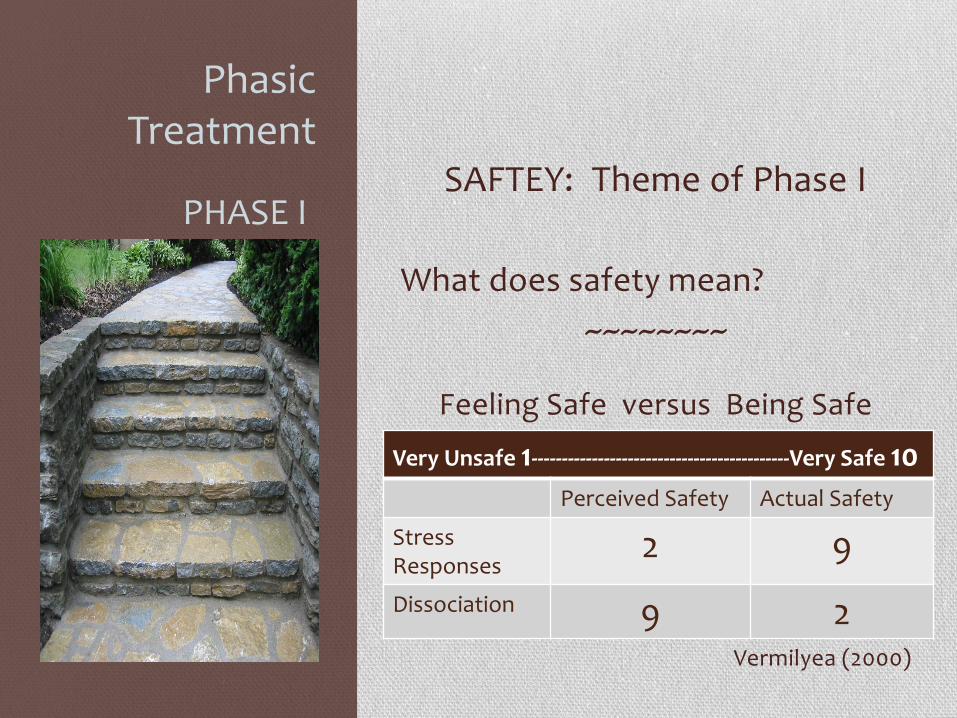
Phasic Treatment
SAFTEY: Theme of Phase I
What does safety mean?
~~~~~~~~
Feeling Safe versus Being Safe
Vermilyea (2000)
PHASE I
Very Unsafe 1-------------------------------------------Very Safe 10
Perceived Safety Actual Safety
Stress Responses
2 9
Dissociation 9 2

Phasic Treatment
SAFTEY: Theme of Phase I
Survival Mode
• Need to react
• No time to think
Recovery Mode
• Need to respond
• Must Reflect & Consider
PHASE I

Psychoeduation
• Ongoing process
• Facilitates transparency
• Facilitates collaboration
• Reinforces differences in
therapeutic relationship
• OK to ask “Why?”
• OK to expect explanation
• OK to expect thoughtfulness
• OK to question the rationale
• OK to disagree

Grounding
SIGHT SOUND TOUCH SMELL TASTE
Look around the room Look at a specific object Notice a specific features (e.g. How many blue things?)
Notice sounds in the room (e.g. fan) Listen to soft music Nature sounds
Pillow Rock Frozen orange Pets
Lotions Scented candles Essential oils Clean laundry
Tea Gum Mints Ginger candy
Using the 5 Senses

Grounding • Orienting Self to Present
• “I am safe.”
• “Today is Monday, May 20th, 2013”
• “I’m at my therapist’s office.”
• Observation Games
• How many windows in this room?
• How many brown things are there?
• How many circular things?
• What’s the distance between me and the bookshelf?
• What’s the length of the table top?
Mentally

Comparisons
SIMILARITIES DIFFERENCES
In You Feel scared Feel alone Could get disappointed
Adult Have help More able to handle it
In the Environment
Wish it’s different Cramped
Pictures on wall Lots of people around
In the Situation
Feel attacked Feel trapped
I made the decision to be here Not trapped
In Others Have power over me Couldn’t disagree
People listen Can find out the reason why
Separating Past and Present Orienting to Present

Containment Skills
• temporarily put experiences aside, rather than allowing them to remain unconscious
Physical

Containment Skills
Removing Yourself from the Situation
Safe Places
Using Imagery

Containment Skills
Removing the Distressing Material
Using Imagery
Containment Skills
• Contains experiences
• Facilitates Other Treatment Activities
• Grounding
• Developing awareness
• Exploration
• Pro’s versus Con’s
Journaling

Containment Skills
Level 1: surface, factual
• Grounding
• Managing time loss
• Increase awareness of day to day events
Level 2: present thoughts, feelings, impulses
• Therapy assignments
• Containment
• Self soothing
Level 3: present-focused writing related to trauma material
Journaling

Cognitive Restructuring
• Systematically identifying and challenging cognitive distortions and replacing them with more positive and accurate thoughts.
• Can be simple consideration of evidence for and against the thought.
• Can be a more involved process…
Challenging Trauma Based Distortions
ghts
“Just because we think it doesn’t make it true.”

Assessing Thoughts: Accurate? DATE
/TIME
SITUATION AUTOMATIC
THOUGHTS
EMOTIONS RATIONAL
RESPONSE
OUTCOME
-At the shelter.
No money in
my pocket.
-Thinking about
some people I
used to hang
with.
-Start craving
cocaine.
“There is
nothing to
do.”
(85%)
“I can’t
stand this
boredom.”
(80%)
Bored
(90%)
Anxious
(95%)
“Actually, there
are plenty of
things I could do;
for example go
to a meeting,
write in my
journal.”
“It is not true that
there is nothing
to do but the
pain of boredom
makes it hard to
see other things
I could do.”
Belief in
automatic
thoughts
(10%)
Bored
(30%)
Anxious
(20%)
Adapted from Beck, et al (1993)

Assessing Thoughts: Functional? Helpful Thinking Harmful Thinking
Constructive
Puts you together
“I can learn.”
Necessary
Helps you do what you need to.
“To find out if I am HIV +, I need a
blood test.”
Positive
Makes you feel better.
“I can focus on what is good in my
life or what I can do.”
Destructive
Tears you apart & destroys you.
“I don’t know anything.”
Unnecessary
Does not change anything.
“What if I’m HIV +?”
Negative
Makes you feel worse.
“There’s so many things wrong with
my life, and there’s nothing that I
do about it.”

Label Dysfunctional Thinking Patterns
•Overgeneralizations “She cut me off
when I was talking. No one wants to
listen to what I have to say.”
• Personalizations Taking responsibility for
negative events, beyond your control. “I ruined
the evening because I chose the restaurant
with the bad service.”
• Dichotomous (All or Nothing) Thinking “If I
can’t make money like I used to, what’s the
point in living.”

Label Dysfunctional Thinking Patterns
•Mind Reading “The counselor doesn’t like
me,… he ignored my question in group.”
•Negative Future Telling Thinking that you
can see how things will be in the future and
its bad.
• Negative Mental Filter Focusing
solely on the negative and
ignoring the positive.

Dialectical Behavior Therapy
(DBT) Skills
•Mindfulness
•Affect Regulation
•Distress Tolerance
• Interpersonal Effectiveness
Identifying and Managing Triggers
“Small things set me off, and before I know it, I’m thinking of
suicide.”
“When I see someone light up, the world narrows and all I can feel is
the need to get high.”
Najavits (2002)

Dialectical Behavior Therapy (DBT)
1. Describe the specific TARGET EVENT
2. Identify the specific PRECIPITATING EVENTS
3. Explain in general the VULNERABILITY FACTORS influencing the event
4. Describe the CHAIN OF EVENTS leading to the TARGET EVENT
5. Identify the CONSEQUENCES of the event
6. Describe in detail alternative SOLUTIONS
7. Outline in detail PREVENTION STRATEGIES
8. Identify REPAIR options
Behavior Chain Analysis
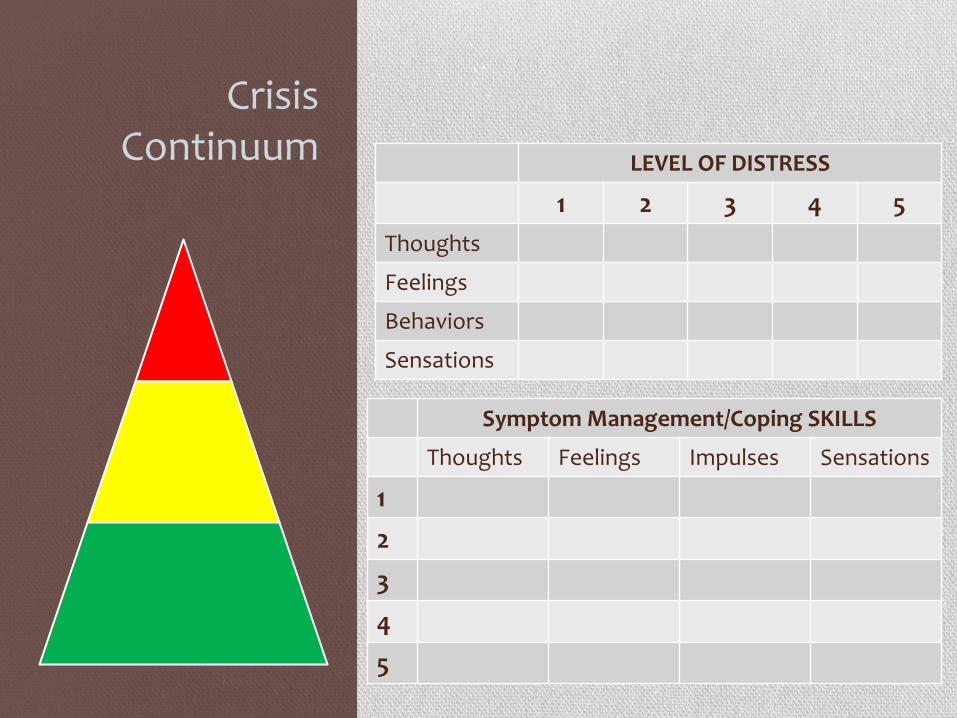
Crisis Continuum LEVEL OF DISTRESS
1 2 3 4 5
Thoughts
Feelings
Behaviors
Sensations
Symptom Management/Coping SKILLS
Thoughts Feelings Impulses Sensations
1
2
3
4
5
.
.
.

Between Trigger and Reaction “Between stimulus and response
there is a space. In that space is our power to choose our
response. In our response lies our growth and our freedom.”
-Victor Frankl (Man’s Search for Meaning)

Bibliography Adams, K. (1998). The Way of the Journal: A Journal Therapy Workbook for
Healing. Lutherville, MD: Sidran Press.
Beck, J. S. (1995). Cognitive Therapy: Basics and Beyond. New York, NY: Guilford Press
Beck, A. T., Wright, F. D., Liese, B. S. (1993). Cognitive Therapy of Substance Abuse. New York, NY: Guilford Press
Braun, B. G. (1988). The BASK (behavior, affect, sensation, knowledge) model of dissociation. Dissociation, 1, 4-23.
Herman, J. L. (1992). Trauma and Recovery. New York: Basic Books.
Herman, J. L. (1992). Complex PTSD: A syndrome in survivors of prolonged and repeated trauma. Journal of Traumatic Stress, 5, 377-391.
Cloitre, M., Courtois, C. A., Ford, J. D., Green, B. L., Alexander, P., Briere, J., Herman, J. L., Lanius, R., Stolbach, B. C., Spinazzola, J., Van der Kolk, B. A., Van der Hart, O., (2012). The ISTSS Expert Consensus Treatment Guidelines for Complex PTSD in Adults. Retrieved from http://www.istss.org [www.istss.org/AM/Template.cfm?Section=ISTSS_Complex_PTSD_Treatment_Guidelines&Template=/CM/ContentDisplay.cfm&ContentID=5185
Courtois, C. (2004). Complex Trauma, Complex Reactions: Assessment and Treatment. Psychotherapy: Research, Practice, Training. Vol 41, No. 4, 412-425.
Bibliography International Society for the Study of Dissociation. (2005). [Chu, J.A.,
Loewenstein, R., Dell, P.F., Barach, P.M., Somer, E., Kluft, R.P., Gelinas, D.J., Van der Hart, O., Dalenberg, C.J., Nijenhuis, E.R.S., Bowman, E.S., Boon, S., Goodwin, J., Jacobson, M., Ross, C.A., Sar, V, Fine, C.G., Frankel, A.S., Coons, P.M., Courtois, C.A., Gold, S.N., & Howell, E.]. Guidelines for treating Dissociative Identity Disorder in adults. Journal of Trauma & Dissociation, 6(4) pp. 69-149. Journal of Trauma & Dissociation, Vol. 6(4) 2005 Available online at www.informaworld.com doi:10.1300/J229v06n04_05)
Kluft, R. P. (1994). Treatment trajectories in multiple personality disorder. Dissociation, 7, 63 – 76.
Kluft, R. P. & Loewenstein, R. J. (2007). Dissociative disorders and depersonalization. In G. O. Gabbard (ed.), Gabbord’s treatment of psychiatric disorders. 4th edn. (pp. 547-572). Washington, DC: American Psychiatric Press.
Linehan, M. M. (1993). Cognitive-Behavioral Treatment of Borderline Personality Disorder. New York, NY: Guilford Press.
Loewenstein, R. L. & Welzant, V. (2010). Pragmatic approaches to stage-oriented treatment for early life trauma-related complex post-traumatic stress and dissociative disorders. The Impact of Early Life Trauma on Health and Disease: The Hidden Epidemic. Lanius, R. A., Vermetten, E. & Pain, C. Eds. Cambridge University Press.

Bibliography Nathanson, D. L. (1989). Understanding what is hidden: Shame in Sexual
Abuse. Psychiatric Clinics of North America, 12 (2), 381 – 388.
Nathanson, D. L. (1992). Shame and pride: affect, sex, and the birth of the self. New York, NY: W. W. Norton & Company, Inc.
Najavits, L. M. (2002). Seeking Safety: A Treatment Manual for PTSD and Substance Abuse. New York, NY: Guilford Press.
Ogden, P., Minton, K., & Pain, C. (2006). Trauma and the Body: A Sensorimotor Approach to Psychotherapy. New York, NY: W. W. Norton & Company, Inc.
Saakvitne, K. W., Gamble, S. G., Pearlman, L.A., & Lev, B. (2000). Risking Connection: A training curriculum for working with survivors of childhood abuse. Lutherville, MD: Sidran Foundation Press.
Salter, A. (1995). Transforming Trauma. Thousand Oaks, CA: Sage Publications, Inc.
Schwarz, R. (2002). Tools for Transforming Trauma. New York, NY: Routledge.
Vermilyea, E. G. (2000). Growing Beyond Survival: A Self-Help Toolkit for Managing Traumatic Stress. Baltimore, MD: Sidran Foundation Press.

LaShaun Annette Williams, PsyD
(202) 361-5992
Drlashaunwilliams.com
THANK YOU
Image from Louisiana Tech University Counseling

Phasic Treatment
There is general agreement that effective treatment of complex post‐traumatic stress and dissociative
disorders follows a phasic process (Courtois, 2004; Herman, 1992; Lowenstein & Welzant, 2010;
Schwarz, 2002). The structure of this conference reflects that consensus with the morning sessions
focusing on phase I issues including the stabilization of safety and engagement. In addition, affect
regulation, skill building, psychoeducation and the development of the treatment alliance are the tasks
of phase I. The second phase includes the processing of traumatic experiences and the third phase
addresses living well in the present. These phases serve as general guideposts for the work. Treatment
of complex posttraumatic stress and dissociative disorders is seldom a linear process, but rather a spiral
in which we return again and again for deeper and more nuanced understanding and resolution.
The over‐aching framework for treatment of complex posttraumatic stress and dissociative disorders
has been described by Courtois (2004) as “multimodal and transtheoretical” due to the applicability of
various treatment approaches and strategies and the multiplicity of treatment issues to be addressed.
Trauma informed means understanding that there is a logic to the client’s symptoms and ways of being
that relate to experiences of trauma. Loewenstein and Welzant (2010) describe the sometimes
incomprehensible presentation of our clients as “chronic adaptations to recurring, coercive
interpersonal trauma” (p. 257).
Even when we’re getting it right, we can be getting it wrong. An accurate reflection of the client’s
experience may set off a series of negative reactions. For example the client’s response to being seen
and understood by the therapist may not be experienced as validating. As Nathanson (1989) points out,
there is a relationship between shame and all exposure and there is “an inherently shameful quality of
psychotherapeutic disclosure” (p. 384). Also, as noted by Salter (1995), for clients abused by sadistic
perpetrators, their thoughts and feelings were used as an instrument of abuse. Therefore, the
therapist’s efforts to know the client better are extremely threatening and terrifying. Likewise,
entreaties to clients to open up and share their internal experiences are similarly fraught with danger.
For such clients, deception and hiding one’s true feelings was essential for survival (Salter, 1995).
Psychoeducation
Psychoeducation is a tool that is used regularly throughout the treatment. Beginning in the first session,
the client is taught what it means to be in treatment. As part of gaining informed consent it is important
to explain that since difficult issues are discussed, sessions may feel uncomfortable. However, they
should not be re‐traumatizing. “We won’t be talking in depth about the details of traumatic experiences
in the beginning. We’re going to make sure that it’s not overwhelming to be here.” Ensuring that the
client remains within the “window of tolerance” [see Ogden, 2006], in which the client is neither hyper‐
or hypo‐ aroused allows for the client to engage optimally in sessions. What kind of relationship is a
therapeutic one? A collaborative relationship, in which we work together to make things better. I
explain that I have no interest in controlling the client, which then gives me the opportunity to address

disbelief. I explain that I don’t expect the client to believe me and that it’s actually appropriate not to
just take at face value what you’re told by someone you’ve just met. “I invite you to check me out.”
DBT
My clients have found DBT Skills training extremely helpful. The approach addresses many of the
associated symptoms of repeated and ongoing trauma, such as affective and cognitive dysregulation,
impaired interpersonal functioning, hyperarousal, impaired attention and consciousness as well as
somatization. It is recommended that careful attention be paid to maintaining the integrity of the
treatment approach. It is not altogether clear which aspects are responsible for particular treatment
gains, so adaptations must be made with care.