Assessment of Memory Processes Milton J. Dehn, Ed.D. MASP Conference: Day I October 22, 2015.
150
Assessment of Memory Processes Milton J. Dehn, Ed.D. MASP Conference: Day I October 22, 2015
-
Upload
garry-lamb -
Category
Documents
-
view
218 -
download
1
Transcript of Assessment of Memory Processes Milton J. Dehn, Ed.D. MASP Conference: Day I October 22, 2015.

Assessment of Memory Processes
Milton J. Dehn, Ed.D.MASP Conference: Day I
October 22, 2015

Notice of Copyright 2015
This PowerPoint presentation and accompanying materials are copyrighted by Milton J. Dehn and Schoolhouse Educational Services, LLC. The PowerPoint and materials are not to be reprinted, copied, presented, or electronically disseminated without written permission. To obtain permission, email [email protected].

Workshop Information Sources
1. Essentials of Working Memory Assessment2. Long-Term Memory Problems in Children3. Essentials of Processing Assessment, 2nd Ed.4. Working Memory in the Classroom5. www.psychprocesses.com6. www.SchoolhouseEducationalServices.com7. www.workingmemoryonline.com8. Presenter Contact: [email protected]

Workshop Content
1. Memory processes2. Related cognitive processes3. Neuropsychology of memory and
processing4. Risk factors5. WM Assessment6. LTM Assessment7. Processing Assessment and Analysis8. Using MPA and PPA software to determine
strengths and weaknesses

Need for Memory Assessmentand Interventions
1. Under-identified in children & adolescents2. 10% have a WM impairment-Alloway3. 6% of average children have LTM deficits (UK)4. Half of LD have a memory deficit (Dehn)5. LTM impairments are a growing problem, e.g,
juvenile diabetes and concussions6. Intervention expertise is lacking; identified
children not served7. Memory deficits are “The elephant in the
classroom”

Why the Under-Identification?
1. Not considered during assessment or assessment knowledge lacking
2. Misattributions1. Teachers report WM as inattentiveness2. Test anxiety, motivation, study skills for LTM
3. Viewed as a “learning” problem4. Lack of knowledge about memory functions5. Lack of knowledge about interventions

Working Memory Definition
1. ST retention + processing = WM2. “WM: the limited capacity to retain
information while simultaneously manipulating the same or other information for a short period of time”
3. Keeping information in mind from moment to moment
4. STM is part of WM; WM “manages” STM as needed
Signs of WM Overload in Daily Life
• “What was I going to say?”• “What did I walk in here to get?”• Not noticing you made a mistake• Reaching for the calculator• Having to switch back and forth from one
computer screen to another to remember• Having difficulty focusing or dividing attention• Unrelated thoughts getting in the way

Why WM is So Important
1. WM is a core cognitive process2. Also, an important executive process3. It’s the interface between STM and LTM4. WM predicts academic learning5. Deficit predicts need for special ed.6. WM deficits seen in several disabilities7. Important in daily functioning
WM Capacity
1. STM adult span of 7; Digit span of 80?2. WM limit of 4 “chunks”3. Can be as little as one chunk in children4. Processing & storage use same WM resource5. Processing referred to as “cognitive load”6. Concurrent processing lowers span7. Strategies can increase span8. Duration affected by rehearsal & amount of
interference Human limitations

Dehn’s Integrated Model of WMIntegrated Model of Working Memory
Verbal WM
Executive WM
Visual-spatial
WM
Active Verbal LTM
Visual-spatial STM
Phono-logical STM
Active Visual LTM

WM Processes to Assess & Why
1. Assess: Phonological STM, Visual-Spatial STM, Verbal WM, Visual-Spatial WM, and Executive WM
2. They each have different functions3. Each has a different neurological basis4. To identify strengths and weaknesses for
intervention purposes
Phonological STM (Auditory)
1. Holds & manipulates speech-based info.2. The coding is phonological3. A loop of about 2 seconds4. Span equals amount articulated in 2 sec.
1. Span increases with speech rate increases5. Includes a subvocal rehearsal process6. Similarity/rhyming reduces span (interference)7. Related to phonological processing & language
development & basic reading skills

Visuospatial STM
1. Visual (object) and spatial (location); these are separate neurologically, e.g. dorsal (spatial) and ventral (visual) stream and thus should be considered separately
2. Is automatically updating3. Concrete, nameable images are consciously
recoded verbally after age 8; tendency to “abandon” visual-spatial

Verbal Working Memory
1. Processing plus storage; complex span2. Effortful processing, manipulating,
transforming, while maintaining verbal information
3. Meaningful processing, semantic information4. Examples: Taking notes, reading
comprehension, mental arithmetic

Visuospatial Working Memory
1. Both mental imagery and visual stimuli2. Maintaining visual images during processing3. Manipulating, restructuring images4. Necessary for dealing with rotation5. Example: On-going awareness of location of
automobiles in motion on a crowded freeway
6. Related with math

Executive WM
1. The essence of working memory2. Combines storage and processing3. Integrates visual and verbal4. Controls and coordinates other components 5. Allocates/focuses attention 6. Inhibiting, shifting, updating7. Involves strategy use8. Often where the deficiency lies 9. Close relationship with executive functions

The Big Three Executive WM Processes
1. Inhibiting: Suppressing distractors and interference
2. Shifting: Alternating between different processing tasks or between processing and storage (rehearsal)
3. Updating: Continual replacement of no longer relevant information with current information
Distinction Between Executive WM and Verbal and Visual-Spatial WM
1. This is Dehn’s model/definition2. Executive is doing additional processing not
necessary for verbal and visual-spatial WM3. Both have processing and deal with
interference4. When the interference is not specific to the
task, it is primarily executive WM5. For example, processing language is verbal
WM, but not executive

Activated LTM Processes
1. Recently activated LTM representations2. WM works with these, going back and forth3. Up to 20 at a time4. Effectively expands capacity of WM because
these are not stored in STM/WM5. Are part of verbal and visual-spatial WM6. WM may draw from these more than STM7. Problem: No way to easily assess these

Working Memory and RelatedCognitive Processes
Should be considered when WM is deficient:1. Attention2. Executive functions3. Fluid Reasoning4. Language5. Long-term memory6. Processing speed7. Phonological processing

WM and Related Cognitive Processes*
General Intellectual Ability .72Fluid Reasoning .54Processing Speed .42Auditory Processing .56Long-Term Retrieval .40Visual-Spatial Processing .37*From WJ IV COG manual
What WM and AttentionHave in Common
1. Both are in dorsolateral prefrontal cortex2. Both part of general executive functions3. Both involve controlled attention4. Inhibition deficit underlies both ADHD and WM5. Both respond to Ritalin6. Problems manifest in similar ways7. When a student has a WM deficit, the number
one thing reported by teachers is that the student has an attention problem

WM and Attention
1. The control of attention is part of WM2. Paying attention is a necessary but
insufficient condition for processing and retention in STM and WM
3. If child is paying attention and still can’t remember in the moment, it’s probably WM
4. Attention problems diminish WM performance in a normal WM

WM vs ADHD
1. The majority with ADHD have a WM problem2. ADHD behavior issues have little to do with WM,
except for poor decision-making3. Attention involves arousal & motor inhibition4. WM deficit closely related to Inattentive ADHD,
not Hyperactive/Impulsive type5. ADHD involves mainly visuospatial WM6. Divided attention closest to WM7. As WM load increases, hyperactivity increases
WM vs Executive Processing
1. WM is one of the executive functions2. General executive processing controls and
coordinates all cognitive functions3. WM has it’s own executive control4. STM functions well without executive5. Inhibition is an overlapping function
1. General executive---resisting distraction2. Working memory---inhibiting old information
6. Strategy selection is also overlapping
WM & Fluid Reasoning
1. Correlations as high as .902. Both require focused, controlled attention3. Reasoning is more the logic; relations4. WM maintains the content used in the
reasoning process5. Novel situations: with little long-term
knowledge or automaticity require more fluid reasoning & working memory
WM & Oral Language
1. L1 and L2 development depend on Phonological STM and Verbal WM
2. Communication (thoughts into words with appropriate structure) depend on WM
3. Language development facilitates WM processing of information (they’re reciprocal)
4. Example: Following directions

WM & Phonological Processing
1. Correlation of .85 with phonological STM2. As reading develops, more differentiation3. Phonological awareness and processing
places demands on STM and WM4. Phonological processing deficit is primary
cause of reading disabilities
WM & Processing Speed
1. Processing speed accounts for most of the variance in STM span (up to 90%)
2. Slow: Information lost before processing and task completed
3. Slow: Poorer encoding into LTM4. Faster rehearsal maintains more info.5. Less of a relationship in adults6. Case study example

Discussion
How does the new information on working memory change your concept of it?
LTM Importance & Misconceptions
1. Everyone agrees on its importance for learning, identity, & daily functioning
2. People assume it’s okay when it’s not3. Assume only head injuries harm it
1. Even then, memory functions often ignored
4. Assume nothing much can be done about it5. When recognized, the specific memory
process deficit is not identified

STM/WM vs LTM• STM LTM• Very limited capacity Extensive capacity• Retention for seconds Retention for minutes to years• Conscious access to all content Limited conscious access• Depends on attention Less dependent on attention• Immediate retrieval only Retrieval can be extended • Forgetting is immediate Forgetting is gradual• Amenable to simple strategies Amenable to elaborate strategies• Easy to assess Difficult to assess• Less susceptible to brain injury Very susceptible to injury• Frontal & parietal lobes Medial temporal lobe• Electrical activity Neuronal and synaptic changes
Long-term memory encoding changes the brain, WM and STM processing does not.

Long-Term Memory
Mem
Implicit Memory
Explicit Memory
Semantic Episodic Priming Procedural Learning
Classical Conditioning

LTM Memory Systems1. Explicit/declarative
1. Episodic---episodes, events, autobiographical1. Organized by scripts
2. Semantic---factual, knowledge, academic1. Organized by schemas
2. Implicit/nondeclarative1. Priming---unconscious associations (example)2. Procedural learning--- “how to” learning3. Classical conditioning---e.g., phobias
3. Prospective Memory (not really a separate memory system)
Explicit vs Implicit• Explicit Implicit• Conscious Unconscious• Knowledge Skills• Flexible expression Rigid expression• Hippocampus-dependent Non-hippocampus• Recollection expresses Performance expresses• Cognitive only Non-cognitive also• Effortful retrieval also Automatic retrieval only• Develops until adulthood Developed by age 3 • Vulnerable to injury Resistant to injury

Episodic vs Semantic• Episodic Semantic• Memory for events Memory for facts• Remembering Knowing• Context dependent Context free• Subjective focus Objective focus• Vulnerable to pathology Resistant to pathology• Develops later Develops first• Known source Unknown source• Mostly visuospatial Mostly verbal• Unintentional encoding More intentional• Chronological Categorical• Organized spatiotemporally Organized by
meaning• Subject to rapid forgetting Less rapid forgetting• Few demands on WM Requires WM

Episodic-Semantic Interactions
1. Semantic slowly accrues from episodic2. School learning is initially episodic but
eventually semantic3. Episodic helps build the semantic4. Semantic provides the schemas and scripts for
the episodic5. Episodic provides context cues for semantic6. Memory tests are primarily episodic

LTM Processes
• Encoding• Consolidation• Storage• Retrieval

Encoding
1. Requires attention2. Associated with “learning”3. All other LT memory depends on4. Enhanced by strategies5. Hippocampus dependent6. STM and WM deficits reduce encoding
opportunities
Consolidation
1. Memories become more stable and resistant to interference over time
2. Memories are forgotten because they are not consolidated
3. LT memories are initially and temporarily stored in the hippocampus and adjoining medial temporal lobe structures
4. Over time they are transferred to the cortex for more “permanent” storage

Consolidation Details
1. Neuroscience construct; not cognitive psych.2. Evidence from TBI, amnesia, & sleep studies
1. Ribot’s gradient3. Takes time: hours to several days4. Unconscious mostly5. Much of it occurs during sleep6. Especially important for semantic memory7. Reactivations improve consolidation

Sleep and Consolidation
1. During both types of sleep2. Hippocampus “replays” experiences/learning
1. “Organizes” information; Strengthens connections2. “Moves” information to cortical areas
3. Sleep also reduces interference4. Sleep accounts for 69% of next day
improvement in procedural tasks5. Immediate sleep: 81% recall; delayed: 66%

Storage of Memories
1. The connections (synapses) more important than the cellular changes
2. In networks of interconnected neurons, with associated items linked more closely
1. Logical linking at the neurological level may result from thinking about two things at the same time (associations) (“fire together; wire together” principle)
3. Memories end up being stored in same areas that sensed, perceived, and processed info.

Retrieval
1. Mostly automatic; strengthens memories2. WM involved in effortful retrieval3. We know more than we can retrieve4. Hippocampus reintegrates information5. Reasoning involved in reconstruction6. During assessment, compare with
recognition to determine whether it is a retrieval or a storage problem

Recognition
1. Should be better than uncued retrieval2. If not, there is an encoding or a storage
problem3. When significantly better, there is a retrieval
problem1. Slow retrieval2. Ineffective retrieval

Causes of Retrieval Problems
1. Blocking or interference2. Slow processing speed3. Poor or no associations at time of encoding4. Wrong cues or lack of cues5. Has not been consolidated; is not in storage

Forgetting (Permanent)
1. Lost from storage; not a retrieval problem2. Lack of consolidation3. Fast at first, then reaches asymptote4. 20 to 80% forgotten within 24 hours5. Some retain well within 30 minutes or first
day but then have very poor retention afterwards (poor consolidation)
6. Is it gone or not retrievable at moment?

Interference
1. Proactive---previous learning interferes with current learning
2. Retroactive---current learning interferences with previous learning
3. Related information is the most interfering4. Controlled somewhat through inhibition5. Spread out instruction; different material
1. Block scheduling?
Interference
1. The primary cause of forgetting2. Memory improves when interference
reduced3. Amnesic individuals benefit from delaying
interference (dark room example)4. “Every time I learn something new, it pushes
some old stuff out of my brain” Homer Simpson
Discussion
How does the new information on long-term memory change your concept of it?
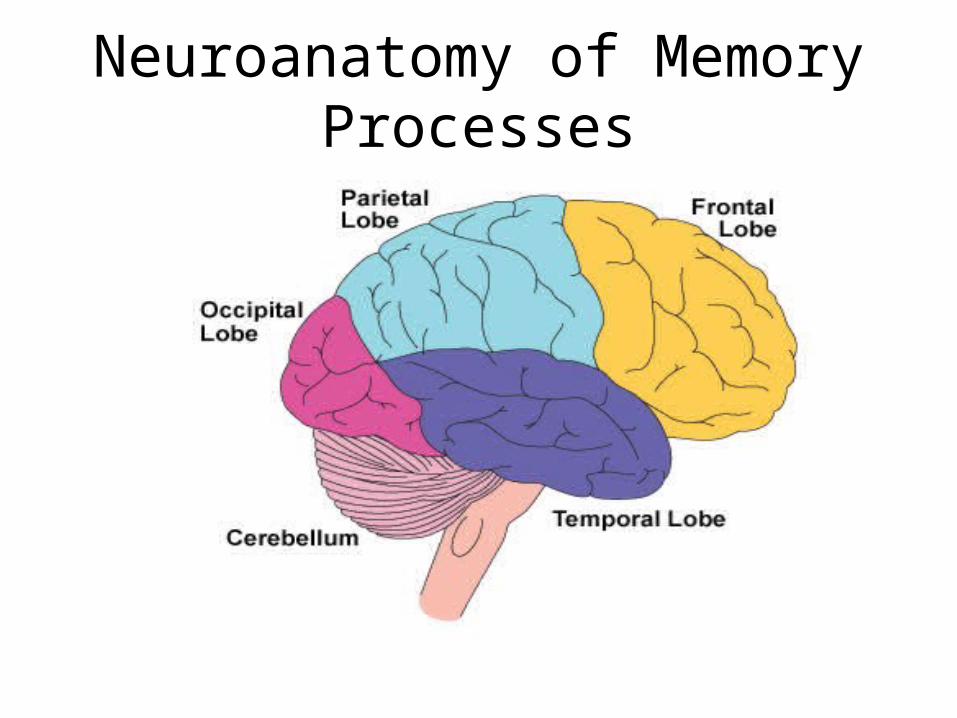
Neuroanatomy of Memory Processes
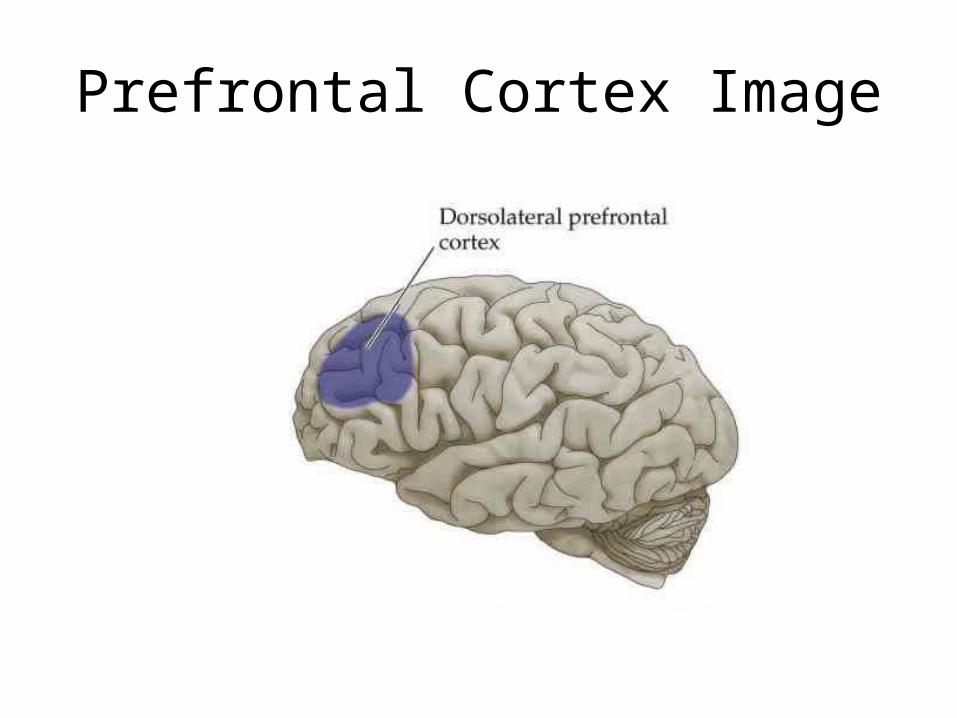
Prefrontal Cortex Image
WM Neuroanatomy Evidence
1. Evidence for each of the five WM components/processes, even phonological storage vs rehearsal
2. Executive WM: dorsolateral prefrontal cortex (dPFC)---shared with attentional control
3. STM processes mainly in parietal and occipital lobes
4. WM processes mainly frontal, temporal, parietal
Brain Lobes and STM & WM
1. Frontal (Dorsolateral Prefrontal Cortex): Executive WM
2. Temporal: Episodic WM (especially during LTM encoding and retrieval)
3. Parietal Lobes: Phonological STM and Verbal WM in language processing areas
4. Occipital Lobes: Visuospatial STM and WM

Neuropsychology of WM
“working memory can be viewed as neither a unitary nor a dedicated system. Thus, working memory is not localized to a single brain region but probably is an emergent property of the functional interactions between the PFC and the rest of the brain” (D’Esposito, 2007)
WM Neurological Basis
1. Individual differences in WM capacity are correlated with the structural integrity of white matter pathways connecting domain general regions with the fronto-parietal network
2. Thus, WM is related to integrity (strength) and extent of myelinated axons
3. WM training increases the integrity of white matter (Takeuchi et al., 2010)

Other Brain Involvement in General WM
1. Striatum: part of the forebrain and the basal ganglia system. Mainly involved with planning movement.
2. Anterior cingulate: a “collar” around the corpus callosum involved in decision making
3. Dopamine level is important for WM. A deficiency in dopamine can impair WM performance.
LTM and the Brain Lobes
1. Temporal lobes---encoding, retrieval, consolidation, temporary storage of long-term episodic memories, semantic storage
2. Frontal lobes---memory strategies for encoding and retrieval (no actual storage of long-term memories)
3. Parietal---auditory and spatial storage4. Occipital---visuospatial storage

Prefrontal Cortex and LTM
1. Interacts with medial temporal lobe and hippocampus
2. Involved during conscious encoding and retrieval1. Application of strategies
3. Prospective memory & source memory4. Development of metamemory

The Hippocampus
Hippocampus Image

The Hippocampus
1. Seahorse shape in temporal lobe2. Necessary for STM-LTM transfer3. Encodes, consolidates, retrieves,
reintegrates4. May hold some episodic permanently5. Explicit memory only6. Sensitive to injury, glucose, oxygen, &
cortisol levels

The Hippocampus
1. Responsible for transferring memories to cortex (consolidation); active during sleep
2. Has a spatial side and a verbal side3. Spatial memory depends on it (more than
verbal memory); London’s taxi drivers4. Large EEG signals5. High levels of glucocorticoid receptors6. Size matters; bigger is better

The Hippocampus
1. Clearly necessary for episodic memory2. May not be as essential for semantic memory3. More involved with automatic retrieval;
conscious retrieval may depend more on the prefrontal cortex
4. The hippocampus primarily stores associations between memories rather than the memories themselves; holds the key to the connections
The Hippocampus
1. Hippocampus contains stem cells2. Hippocampus can grow (London taxi drivers)3. New neurons can be created from stem cells;
up to six weeks to mature4. Rats given Prozac had a 70 percent increase
in hippocampi cells after three weeks5. Humans who recover from depression have
more hippocampal volume than those who are chronically depressed
What the Hippocampus Needs
1. Oxygen2. Glucose3. Sleep (no permanent damage from lack of)4. No cortisol5. No impact6. No electricitySee YouTube Video: “Hippocampus Damage”
Non-Hippocampal LTM Structures
1. Thalamus (sensory relay station)2. Amygdala (emotions strengthen memories)3. Ventral visual stream (RAN)4. Parahippocampal cortex (surrounds
hippocampus; memory encoding)5. Entorhinal cortex (interface between
hippocampus and neocortex) 6. Perirhinal cortex (visual recognition)

HM: Classic Case of No Hippocampus
1. Hippocampus, parahippocampal gyrus, entorhinal cortex, and amygdala were surgically removed in 1957 at age 27 because of epilepsy
2. Anterograde amnesia but STM and WM fine; could modify some semantic knowledge, such as celebrities’ names, but no new episodic memory
3. Some retrograde amnesia: Most events 1-2 years prior to surgery forgotten but prior semantic memory was good

HM
1. Performed normally on intellectual tests2. Could learn new motor skills (implicit,
procedural memory) but could not remember that he had learned them
3. He could draw a map of the house he was living in (that he moved to after the surgery), maybe from locomotion recall
4. His case had strong influence on memory theories and brain mapping of memory

Implicit Memory
1. Does not appear to depend on the hippocampus
2. Not consciously accessible3. Demonstrated through performance, not
recall4. Precedes development of explicit memory5. Example of implicit memory without explicit
Implicit Memory Structures
1. Generally not in medial temporal lobe but parietal and occipital
2. Cerebellum---conditioning3. Striatum---procedural learning4. Also, temporal cortices, amygdala, basal
ganglia, and motor cortex5. Range of structures may serve a protective
function

Organization of LTM Memories from Cognitive Perspective
1. Schemas1. Logical linking at the neurological level may
result from thinking about two things at the same time (associations) (“fire together; wire together”)
2. Scripts3. Memory traces4. Associations
Organization and Storage of Memories
1. The connections more important and better understood than the cellular changes
2. Memory traces (pathways): synapses1. New memories: new synapses or changes in strength
3. In networks of interconnected neurons, with associated items linked more closely
4. Memories end up being stored in same areas that sensed, perceived, and processed info
5. Different components of a memory stored separately; then reintegrated during retrieval

Neuroanatomy of Other Processes
1. Most in more than one brain lobe2. Illustrates the interconnectivity of processes3. Most have specific structures within a lobe4. Processing speed is a function of
interconnectivity; does not have a specific structure

Occipital Lobe
1. Dedicated to vision and visual-spatial processing
2. Receives sensory data from the thalamus3. Visual and spatial processing are separate4. Dorsal stream (upper) sends spatial
information to parietal lobe5. Ventral stream (lower) sends visual
information to temporal lobe
Temporal Lobe
1. Auditory processing2. Long-term memory processing in the
hippocampus3. Some visual processing4. Semantic memory storage

Parietal Lobe
1. Integrates sensory information2. Language processing3. Phonological processing

Frontal Lobe
1. The “output” lobe; others are input2. Executive functions---prefrontal cortex3. Working memory---prefrontal cortex4. Attentional control---prefrontal cortex5. Fluid reasoning6. Fine motor7. Oral expression8. No storage of long-term memories

Discussion
How does the new information on neuroanatomy change your concept of memory, processing, and learning problems?

Risk Factors for Memory Impairments
1. Anything that harms the brain or cognitive functioning impacts LTM
2. All involve risk of damage to hippocampus 3. The hippocampus is a vulnerable structure4. Damage to prefrontal cortex also impacts LTM5. Prenatal, perinatal, neonatal, any point in life6. Some temporary with recovery, some stable,
some progressively worse7. See Table

Risk Factors: TBI
1. .25% of youth acquire a TBI each year2. Severe TBI: 36 – 53% have ongoing LTM impairment3. Implicit more resistant to injury4. More verbal problems than visuospatial5. Most mild cases recover within a month
1. But some can have persistent problems
6. Most moderate cases within 1-2 years7. Frontal lobes: Metamemory and strategies8. Very susceptible to interference9. Require some different types of interventions

Concussions
1. 19% chance for school athletes per year2. Likely memory problems: few days/weeks3. Loss of consciousness, orientation, increases risk4. Possibility of persistent LTM problems should be
considered5. Athletes will deny so they can play again6. Pre-season baseline testing important (IMPACT)7. Temporal window of vulnerability when second
injury results in magnified cognitive deficits (case)

Post-Concussion Syndrome
1. These are acute effects2. Headaches, dizziness/vertigo, nausea, light
and noise sensitivity, fatigue, hypersomnia/insomnia, irritability, emotional dysregulation, dysmnesia, attention problems, processing speed, working memory
3. There can be long-term effects, such as vertigo

Concussion Case Study
1. Soccer player; kick to head2. No loss of consciousness3. Some amnesia first few days4. Serious and persistent concussion symptoms5. 30 days later
1. Verbal and visuospatial WM down 1 SD2. Verbal and visuospatial LTM down, esp. visual-
spatial6. Six months later; all recovered except visual-
spatial LTM

Extreme Prematurity
1. Hypoxia due to poorly developed lungs can damage hippocampus
2. Myelination adds to memory problems3. Those born prior to 32 weeks have significant
risk of memory problems4. Episodic and “everyday” memory problems
may be more serious than semantic memory problems
Type I Diabetes
1. Hippocampus sensitive to glucose levels2. Growing numbers of diabetic children3. Greater risk with earlier onset4. Greater risk with poorly controlled insulin5. Hypoglycemia damages hippocampus6. Memory functions decline over time7. Children of diabetic mothers also at risk8. Even nondiabetics with poor insulin control9. Adequate glucose also important for WM

Epilepsy
1. 10% have significant memory impairment2. Depends on type, severity, frequency, and
location of seizures3. Temporal lobe type most devastating4. Especially known for “accelerated forgetting”5. Seizures disrupt consolidation6. Six-year old case from Session I update
PTSD
1. Due to abuse, trauma or witnessing violence2. Do not need actual PTSD diagnosis for impact3. More PTSD symptoms, more LTM deficits4. Vietnam PTSD; 26% hippocampal reduction5. Cortisol damages hippocampus6. Temporarily elevated cortisol reduces
encoding7. Chronic stress causes LTM problems

Depression and Anxiety
1. Depressed adults have a 12 – 15% reduction in hippocampal volume
2. Depends on the number and duration of depressive episodes
3. Hippocampus damage is less when depression is treated
4. Anxiety primarily affects encoding

FAS and Alcohol Consumption
1. FAS children have a smaller hippocampus2. Even mild alcohol consumption increases risk
for LTM problems, which usually go undetected
3. Effects are dose-dependent4. Difficulty inhibiting interference
Anorexia and Memory
1. Problems during and after illness2. Working memory3. Verbal recall and Visual-spatial recall
1. Due to reduced cerebral blood flow and high levels of stress hormones (corticosteroids) and glucose and nutritional deficiencies, e.g. vitamin B.1
4. Have enhanced memory for maladaptive perceptions of food
1. Evidence that memories are of what you perceive
Disorders with High Risk of Memory Impairment
1. Learning disability2. Language impairment3. ADHD (semantic memory and strategy
deficits)4. Autism (semantic memory, strategy, facial
memory deficits)5. Down syndrome (interference)

Discussion
What are the assessment and intervention implications of the risk factors?
WM Assessment Challenges
1. Other processes interrelated2. Interrelated with LTM3. No standardized inclusive composites4. Can’t easily separate some components5. No complete batteries6. No easy way to assess strategy use7. Examinee’s expertise/automaticity8. Ecological validity; tests well but doesn’t
perform well in classroom and daily life

LTM Memory Assessment Challenges
1. Time consuming2. Memory abilities versus strategy usage3. Everyday mem. vs formal test activities4. Episodic vs semantic5. Can’t control learning opportunities6. Difficult to isolate memory processes7. Difficult to test consolidation8. Poor labeling on standardized measures9. Influence of STM, WM, other processes

Working Memory Assessment
1. Test all 5 WM/STM components1. To identify strengths and weaknesses2. To understand learning & WM problems3. Because they are neurologically separable4. More testing = higher reliability & validity
2. Observations and interviews important3. Rating scales helpful

LTM Processes to Test
1. Verbal Episodic2. Visual-Spatial Episodic3. Encoding4. Consolidation (must have 24+ delayed recall)5. Storage/Recognition6. Retrieval Fluency
Health and Developmental History
1. History of any at-risk conditions, e.g. diabetes2. Complete history, beginning pre-natal3. Health risk factors
1. Age of onset2. Episodes leading to hospitalization3. Any treatment
4. Developmental concerns, e.g. language development
Academic and Learning History
1. Academic markers1. Diagnosed disorders 2. Learning problems3. Grade retention4. Progress worse as memory demands increase5. Studies but performs poorly on exams
2. Memory concerns reported by teachers

Interviews
1. Include memory items in teacher interviews 2. With parents, adapt teacher items for home
environment 3. Directly question older students 4. Assess metamemory5. Elicit their hypotheses about learning and
memory problemsLink

Observations: General Findings Regarding WM
1. WM failure leads to abandonment of activity without completing it
2. Reserved in group activities3. Short attention spans4. Poor monitoring of work quality5. Loses place in complicated tasks6. Examples of evidence-based WM behaviors7. LTM Observations
Metamemory Link
1. Understanding memory functions2. Self-awareness of strengths/weaknesses3. Regulating/controlling memory4. Strategy knowledge and monitoring5. Simple strategy use by age 36. Conditional knowledge (why a strategy works)7. Metamemory development is an essential
intervention piece; so, it needs to be assessed8. Metamemory interview items

Signs of Poor Metamemory Development
1. Not aware of existing memory problems2. No understanding of how memory works3. Poor estimates of how much will be
remembered (usually over estimates)4. Has no realistic idea of how to make a
memory stronger5. Has no memorization strategies6. Not aware of different types of memories
Strategy Development
1. Strategies enhance memory performance2. Strategies more important for LTM than WM3. Do children have memory problems because
they lack strategy development?1. Usually not (Swanson regarding WM)
4. Driven by the demands of the environment

Metamemory and Strategy Assessment
1. A standardized measure is lacking2. Assess:
1. Knowledge of memory functions2. Knowledge of LTM strengths/weaknesses3. Accuracy of JOL’s4. Knowledge of strategies and use of strategies 5. Try CVLT for semantic clustering6. After testing, ask what strategies were used
Informal Strategy Assessment
1. Question student during interview2. Observe during testing
1. Rehearsing2. Recoding3. Chunking
3. Question after all testing completed4. Try n-back with cards and see if examinee
develops a strategy

Rehearsal Ability
1. Give child a series of words and ask him/her to repeat 5 times rapidly
2. Children with significant memory problems have difficulty maintaining the sequence during rehearsal
3. Will avoid using rehearsal when directed to do so

Consider Related Processes
1. Test other processes that are closely linked with memory components
2. Test memory when related processes are weak
3. Link

Testing WM with Cognitive Scales: Advantages
1. No need to buy separate scales2. Usually do not confound learning/LTM
encoding with STM or WM components3. Tend to use traditional, purer measures of
STM and WM4. Correlations with other cognitive processes
are known5. Correlations with achievement scales
Cognitive Scales Disadvantages
1. Some measure only auditory/verbal2. Some classify visual-spatial STM and WM
under visual processing3. Some confound STM and WM4. Some do not have pure visual-spatial5. Multi-battery testing necessary

Intellectual/Cognitive Tests withWorking Memory Subtests
1. May be better than memory batteries
2. Most do not assess all WM components
3. Go by what is measured; not by subtest title or test author’s classification
See selective tables for cognitive and other scales

WM Components in Broad Memory Batteries
Pros:• Comprehensive assessment of most memory
systems• Include learning measures, learning rateCons:• STM subtests often confounded with learning• Misleading test names Link• See comprehensive list in MPA manual

Advantages to Testing with Memory Batteries
1. Can compare with STM and WM directly2. Fewer confounds with other cog. processes3. More in-depth memory assessment4. Include recognition (retrieval) measures
1. Memory battery required for this
5. Include learning (encoding) measures6. Both visual and verbal

Disadvantages to Testing with Memory Batteries
1. No semantic memory measures2. No measures of consolidation3. Do not measure “everyday” memory4. No metacognitive or strategy measures5. Maybe too much structure6. Measures of STM and WM are “messy”
Dehn: Task Analysis/Classificationof Subtests
1. Consider definition of the process2. Consider factor analytic information3. What is the primary process being measured
by the subtest? (not just input or output)4. Which primary process allows the examinee
to successfully complete the task5. Consider what the task is typically used to
measure
Selective & Multi-Battery Testing
1. Start with batteries you have2. Try to limit number of supplemental batteries3. Avoid redundancies4. Tests should be normed about the same time5. Only selected subtests administered6. Composites are preferred, or two subtests7. May include rating scales8. Use multi-battery analysis procedures

WM Case Study: “Jacob”
1. Age 13; 7th grade2. Foster care; special ed placement3. 3 months premature; failure to thrive4. Early elementary IQ of 70; recent IQ of 955. ADHD diagnosis; poor organization6. Social skills problems7. Difficulty completing homework8. Moderately high test anxiety

Case Study Continued
1. Likes to read2. Struggles with Math and Written Lang. 3. Reading Composite – 1064. Math Composite – 885. Wr. Lang. Composite – 736. Oral Lang Composite - 877. Group Task: Generate WM deficit hypotheses
and related processing deficit hypotheses

Planning a Processing Assessment
1. Complete the processing assessment planner on case study
2. Consider concern3. Hypothesize which processes involved4. Consider non-processing hypotheses5. Fill in all processes tested by primary scale6. Find other scales to cover remaining
processes See Partially Completed Example

Memory Analysis Worksheet
1. Composite scores from test manual when possible
2. Convert all scores to standard scores3. Compute clinical scores by averaging4. Compute processing or memory mean or
use IQ5. Calculate discrepancies6. Determine weaknesses and deficits7. Do pairwise comparisons
1. Opposites and those closely related
Weaknesses vs Deficits
1. Scores below 90 are normative weaknesses2. Intra-individual strengths & weaknesses use
12 points 3. Deficit = both normative and intra-individual
weakness (deficit is a “strong” weakness)1. A deficit is rare2. Indicates underlying neurological impairment3. Learners with deficits really need interventions

Non-Unitary Scores
1. When standard score difference is greater than 22 points
2. Something different is being measured or something is different about the task
3. Investigate further with more testing if cannot be explained

Hypothesis Testing
1. Consider deficit hypotheses proposed prior to testing
2. Examine scores: support or not3. Consider other data4. Give weight to functional evidence5. Be wary of confirmation bias or Type I errors:
Seeing a weakness/deficit where there is none

Consistency Approach
1. With processing and memory assessment, use a consistency approach, not a discrepancy approach
1. Low WM + low academic skill = SLD
2. NOT high WM + low academic skill

When Does a WM Deficit Support an SLD Diagnosis?
1. When the memory or processing component is one that is related to the academic skill deficiency
2. When both the academic skill and WM component are similarly low (consistency approach)
3. When WM is significantly higher, it may not be SLD or there could be some other cause of poor skills
Pairwise Comparisons
1. More for intervention planning, not diagnosis2. Pay most attention to:
1. Opposites2. Those that are closely related
3. A greater discrepancy is required for significance
4. Significant when confidence intervals do not overlap

Discuss Jacob’s Results
LinkDo his memory and processing deficits account for his learning problems?

Psych Report Components
1. Explain cross-battery selective testing2. Explain how analysis was conducted3. Explain what is being used to predict scores4. Integrate results by memory components5. Define each component6. Explain how it relates to academics7. See Labeling example
Discussion
What new assessment procedure or analysis procedure did you learn about today that you plan to use in the future when conducting assessments or analyzing data?

Psychological Processing Analyzer (PPA) 4.0
& Memory Processing Analyzer (MPA) 2.01. Download software packages that apply
statistical procedures to PSW analysis2. Conducts PSW among 11 psychological
processes or 11 memory processes 3. Conducts PSW among 8 achievement areas4. Identifies statistically significant intra-individual
strengths, weaknesses, deficits, and assets and significant pair differences
5. Identifies consistency between low processes and related areas of low achievement
Composites and Subtests
1. Can enter composite and/or subtest scores2. Allows scores from cognitive, achievement,
rating, and processing scalesSee Lists
3. Includes latest tests, updated every year; pre-1999 excluded
Processes Analyzed by the PPA
1. Attention2. Auditory Processing3. Executive Functions4. Fine Motor5. Fluid Reasoning6. Long-Term Recall7. Oral Language8. Phonological Processing9. Processing Speed10.Visual-Spatial Processing11.Working Memory (WM)

Achievement Areas on the PPA 4.0
1. Basic Reading Skills2. Reading Fluency3. Reading Comprehension4. Math Calculation5. Math Problem Solving6. Written Expression7. Oral Expression8. Listening Comprehension

Memory Processes
• Phonological Short-Term Memory• Visual-Spatial Short-Term Memory• Verbal Working Memory• Visual-Spatial Working Memory• Executive Working Memory• Long-Term Memory Verbal Recall• Long-Term Memory Visual-Spatial Recall• Long-Term Memory Encoding/Learning• Long-Term Memory Consolidation• Long-Term Memory Storage/Recognition• Long-Term Memory Retrieval Fluency
Composites and Subtests
1. Does not include all composites and subtests in each battery
2. Composite and subtests are limited to those that primarily are measuring that process
3. Some are re-classified based on the primary demands of the task
4. Crystallized intelligence excluded on the PPA

Main Equations1. Converts all scores (except raw scores) to standard
scores with a mean of 100/SD of 152. .01 or .05 level of significance3. Normative weakness cutoff options: 80, 85, and 904. Difference formulas based on reliability coefficients of
composites/subtests5. Regression toward the mean 6. Predicted score based on mean of other 107. Non-unitary scores are flagged8. Checks processes and achievement for consistency
using difference formula
Using the PPA and MPA
1. Select and administer tests for processes Link2. No minimum number of processes required3. Enter scaled scores, T-scores, standard scores4. Program transforms scores to standard scores5. Option of entering unlisted composites &
subtests 6. IQ can be used as predictor

Normative Weakness Options
1. Can select the average range2. Will apply to all entries3. Options:
1. 90-1092. 85-1143. 80-119
4. This will determine what is identified as normative weaknesses and also the deficits
5. If using the deficit rule, then use 90-109
Using the Mean or IQ/Cognitive Composite as Predictor of Processes
1. Okay to use IQ as predictor because it has high correlations with most processes
2. Is technically more appropriate because it has known reliability and SEM
3. Use when only weak processes tested4. Use when only a few processes tested5. Use when a legal challenge is anticipated6. Do not use when processes pull down IQ
Entering Unlisted Scores
1. If a composite, type it in uppercase2. Must know the reliability coefficient and
enter it3. Only one unlisted entry per area4. Cannot combine with listed scores5. More entries and combining entries will be
allowed in next update in winter 2016

Entering Process, Memory, and Achievement Scores
1. In first column select composites, subtests, or unlisted score
2. Up to 4 of each or only 1 unlisted score3. Within same area cannot mix composite and
subtest scores4. In second column click on the composite or
subtest5. In third column enter score
Non-Unitary Scores
1. When standard score difference is greater than 22 points
1. Can use a difference of 15 points 2. PPA software uses 22 points
2. Something different is being measured or something is different about the task
3. Investigate further with more testing if it cannot be explained

PPA PSW Achievement Analysis
1. This is a within achievement PSW analysis: what are the strengths and weaknesses among achievement
2. IQ or the mean of the processes is not allowed as the predictor of the achievement scores
3. The mean of the achievement scores is the predictor
4. Other PPA analysis criteria and procedures apply

Checking Pairs for Significance
1. Pairwise comparisons of process scores is not diagnostic but provides more details and intervention ideas
1. Only logically connected process pairs included2. Achievement and Process pairs are
diagnostic1. Only related pairs included2. The “no’s” are diagnostic 3. “No” means they are not significantly different
and therefore consistent See Example

Processing-Achievement Consistency
1. When the process score and achievement score are consistent, this is evidence that the processing weakness is causing the achievement deficiency
2. When process score significantly higher than achievement, something other than the process is causing the achievement deficiency
3. When the process score is significantly weaker than the achievement, the student is overachieving or other strong processes are being used to compensate

PPA and MPA Reports
1. Results tables, graphs, and a narrative2. Pairwise comparisons also provided 3. Narrative and colored score charts can be
saved to Word document4. See sample report

Purchasing the PPA 4.0• Available at www.psychprocesses.com• For individual use: $129– A download to your computer– Unlimited use
• Five-year site license available based on total student population in district– Cost effective when 10 or more users– Free updates for 5 years– Free training via webinar– Technical support

Entering Unlisted Scores
1. If a composite, type it in uppercase2. Must know the reliability coefficient and
enter it3. Only one unlisted entry per area4. Cannot combine with listed scores5. More entries and combining entries will be
allowed in next update in winter 2016