Assessment, Feedback and Evaluation Vinod Patel & John Morrissey 1.
81
Assessment, Feedback and Evaluation Vinod Patel & John Morrissey 1
-
Upload
emery-kennedy -
Category
Documents
-
view
222 -
download
1
Transcript of Assessment, Feedback and Evaluation Vinod Patel & John Morrissey 1.
Assessment, Feedback and
Evaluation Vinod Patel & John Morrissey
1
By the end of this session you will be able to :
• Define assessment, feedback and evaluation
• Discuss how these are related and how they differ
• Discuss the application of each in clinical education.
• Begin to apply them in practice
Learning outcomes
2
• Definitions
• Assessment : theory & practice
• Tea break
• Feedback
• Evaluation : theory & practice
• Questions and close
Lesson Plan
3
• Assessment ?
• Feedback
• Evaluation ?
Definitions ?
4
Assessment : definition
“The processes and instruments applied to measure the learner’s achievements, normally after they have worked through a learning programme of one sort or another”
Mohanna K et al (2004) Teaching Made Easy – a manual for health professionals
5
Feedback : definition
“Specific information about the comparison between a trainee’s observed performance and a standard, given with the intent to improve the trainee’s performance”
Van de Ridder JM et al (2008) Med Educ 42(2): 189
6

Evaluation : definition
“A systematic approach to the collection, analysis and interpretation of information about any aspect of the conceptualisation, design, implementation and utility of educational programmes”
Mohanna K et al (2004) Teaching Made Easy – a manual for health professionals
7
AssessmentPart 1
8

In this section:
• Purposes of assessment
• Miller’s pyramid
• The utility function
9

Why assess ?
10

Why assess ? 1 of 2
• To inform students of strengths and weaknesses.
• To ensure adequate progress has been made before students move to the next level.
• To provide certification of a standard of performance.
11
Why assess ? 2 of 2
• To indicate to students which parts of the curriculum are considered
important.
• To select for a course or career.
• To motivate students in their studies.
• To measure the effectiveness of teaching and to identify weaknesses in the curriculum.
12
Summative
Formative13
Clinical Education : Assessment Methods
• Written Assessments
• Observed clinical practice
• Others :
• Vivas
• Portfolios
• …
14
How a skill is acquired
• Cognitive phase
• Fixative phase• Practice
• Feedback
• Autonomous phase
Fitts P & Posner M (1967) Human Performance
15
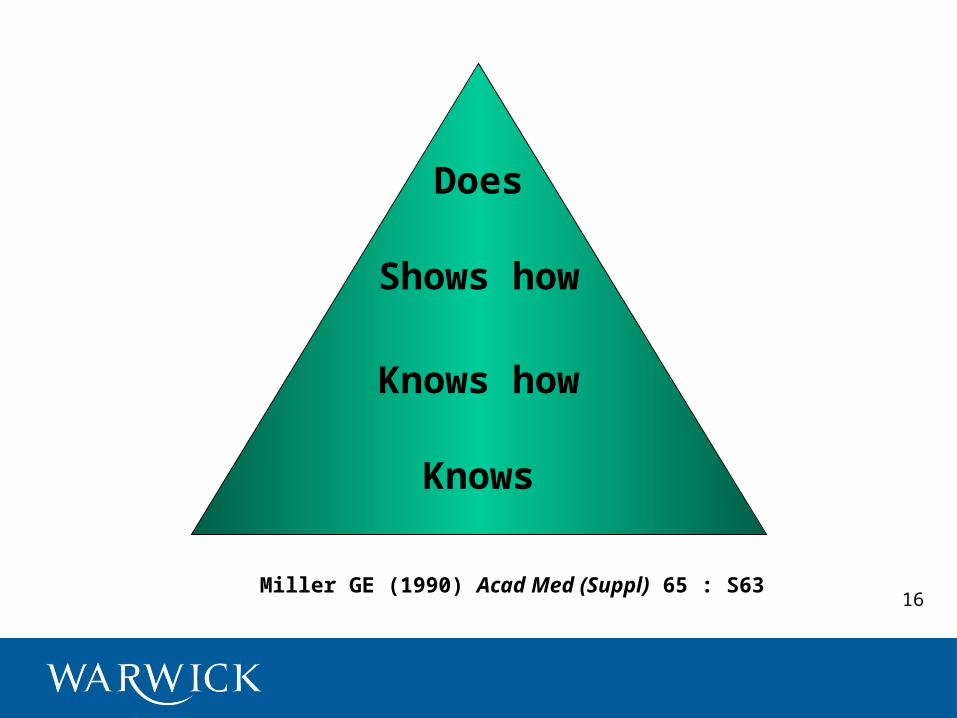
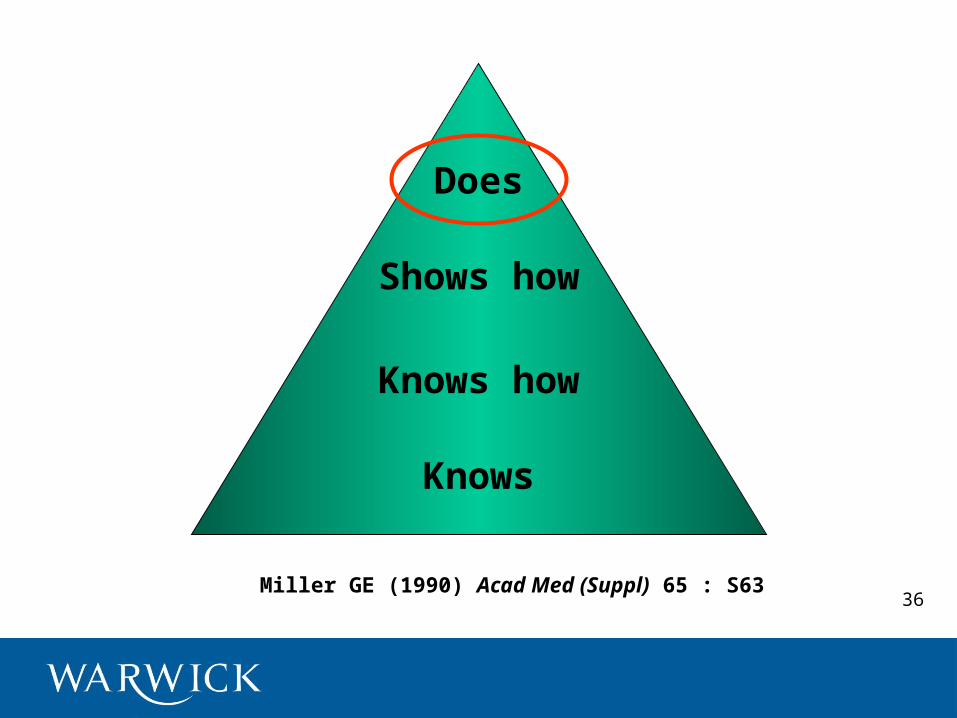
Miller GE (1990) Acad Med (Suppl) 65 : S63
Does
Shows how
Knows how
Knows
16
17

18
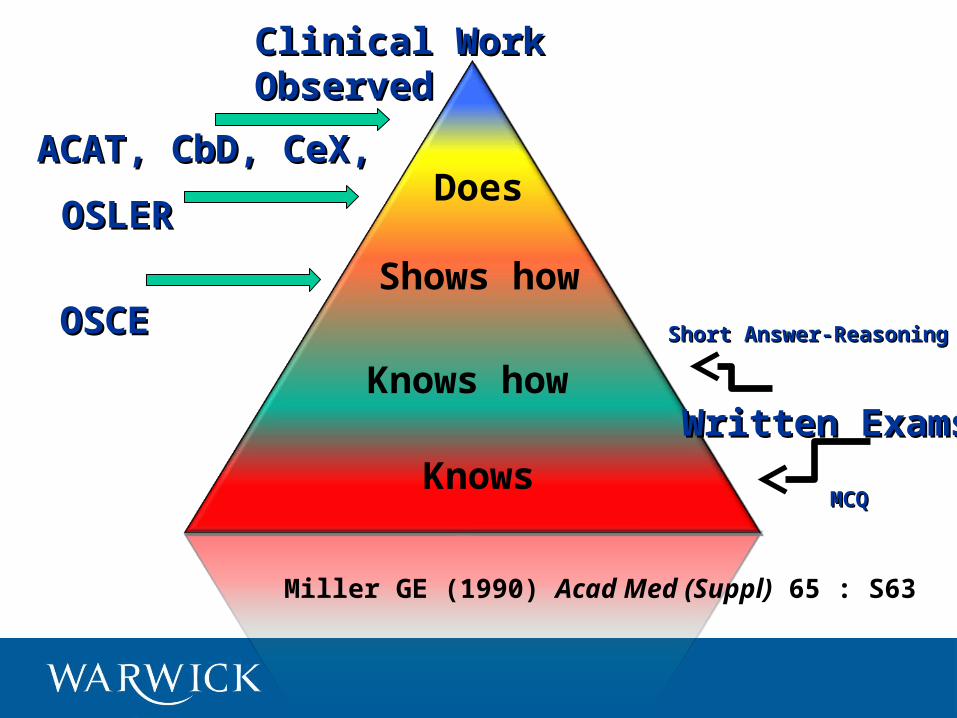
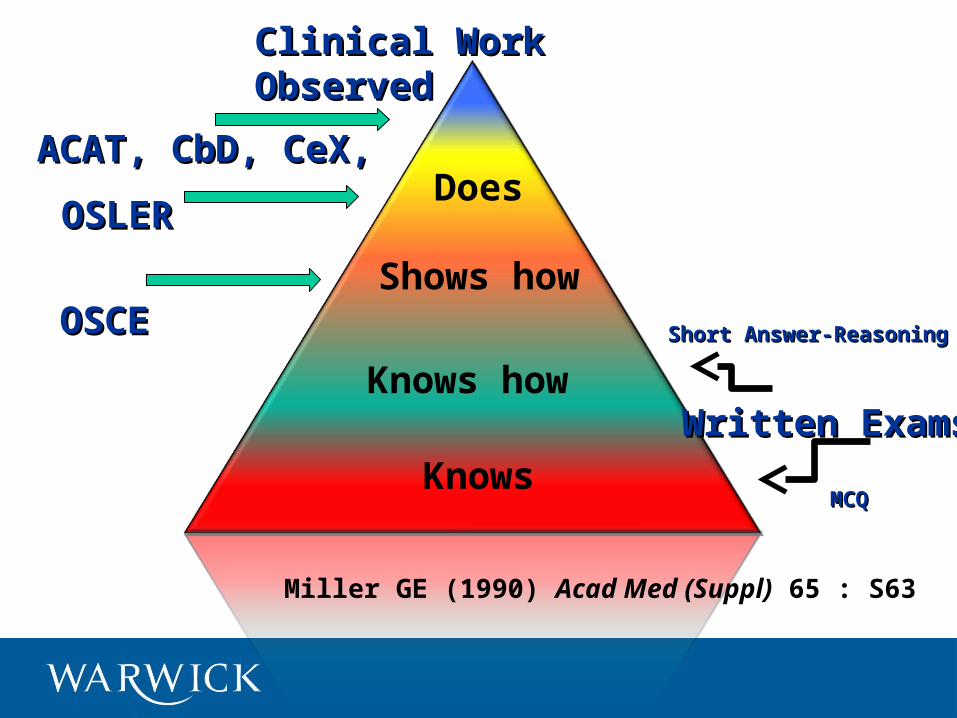
Miller GE (1990) Acad Med (Suppl) 65 : S63
Does
Shows how
Knows how
Knows
OSCEOSCE
Written Exams Written Exams
OSLEROSLER
Clinical Work ObservedClinical Work Observed
ACAT, CbD, CeX, ACAT, CbD, CeX,
Short Answer-Reasoning Short Answer-Reasoning
MCQMCQ

Question :
How can we tell whether these tests are any good or not ?
Answer :
We do the maths .
20
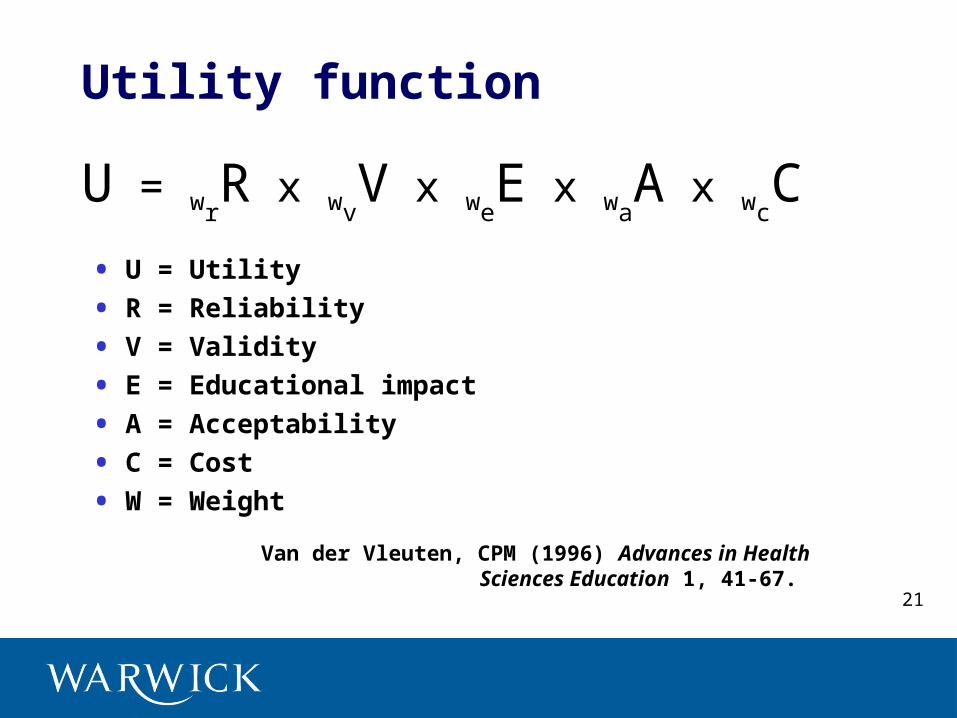
Utility function
• U = Utility
• R = Reliability
• V = Validity
• E = Educational impact
• A = Acceptability
• C = Cost
• W = Weight
U = wrR x wv
V x weE x wa
A x wcC
Van der Vleuten, CPM (1996) Advances in Health Sciences Education 1, 41-67.
21
The Assessment Pentagram
Validity Reliability
Feasibility Acceptability
Educational Impact
22
Validity & reliability
• Validity : the extent to which the competence that the test claims to measure is actually being measured.
• Reliability : the extent to which a test yields reproducible results.
Schuwirth & van der Vleuten (2006) How to design a useful test : the principles of assessment
23
Messick (1994) Educational Researcher 23 : 13
“The degree to which empirical evidence and theoretical rationales support the adequacy and appropriateness of inferences and actions based on test scores or other modes of assessment.”
Validity : another definition
24
Some causes of low validity
• Vague or misleading instructions to candidates.
• Inappropriate or overcomplicated wording.
• Too few test items.
• Insufficient time.
• Inappropriate content.
• Items too easy or too difficult.
McAleer (2005) Choosing Assessment Instruments
25
Some causes of low reliability
• Inadequate sampling.
• Lack of objectivity in scoring.
• Environmental factors.
• Processing errors.
• Classification errors.
• Generalisation errors.
• Examiner bias.
McAleer (2005) Choosing Assessment Instruments
26
Types of validity
• Face
• Predictive
• Concurrent
• Content
• Construct
27
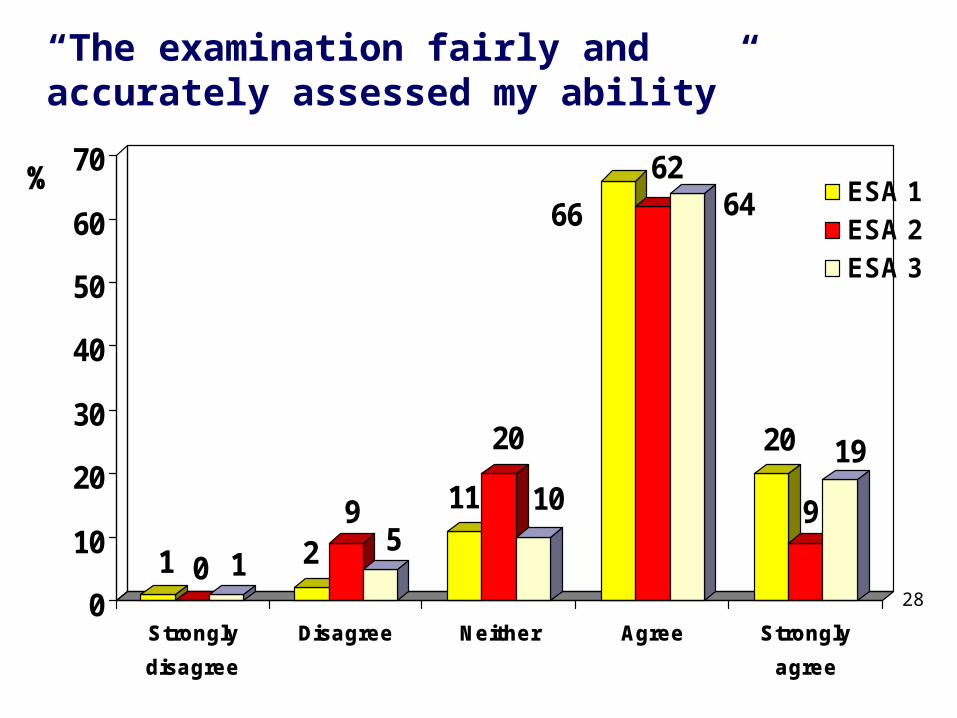
1 0 1 29
511
20
10
66
6264
20
9
19
0
10
20
30
40
50
60
70%
Strongly
disagree
Disagree Neither Agree Strongly
agree
ESA 1ESA 2ESA 3
“The examination fairly and accurately assessed my ability”
28
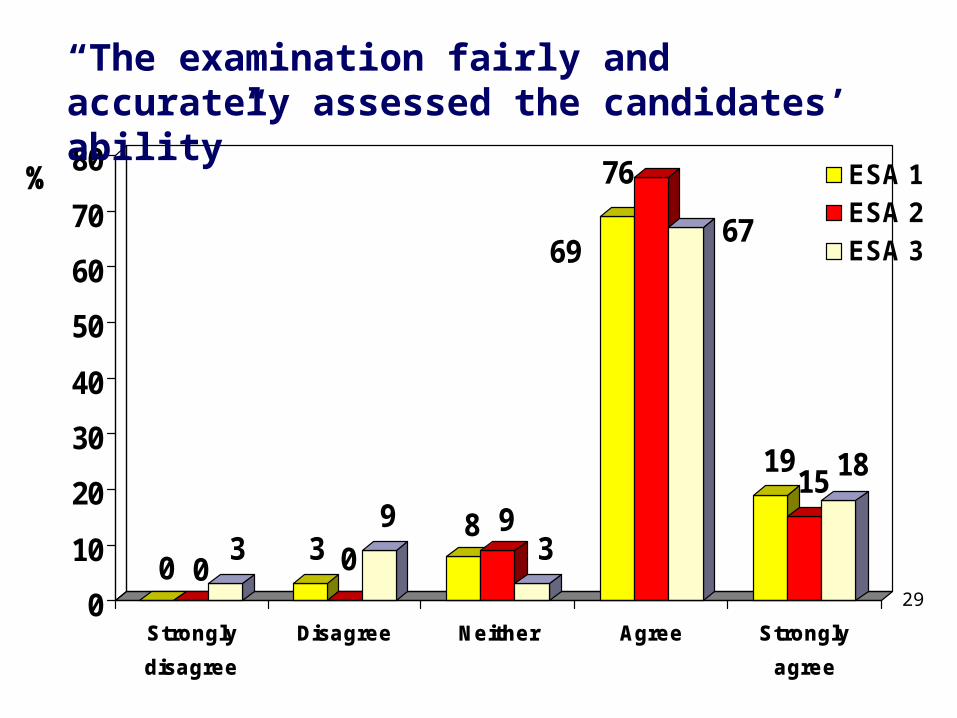
0 03 3 0
9 8 93
69
76
67
1915 18
0
10
20
30
40
50
60
70
80%
Strongly
disagree
Disagree Neither Agree Strongly
agree
ESA 1ESA 2ESA 3
“The examination fairly and accurately assessed the candidates’ ability”
29
Problem :
Appearances can be deceptive.
30
Types of reliability
• Test-retest
• Equivalent forms
• Split-half
• Interrater and intrarater
31
32

33
The Assessment Pentagram
Validity Reliability
Feasibility Acceptability
Educational Impact
34
Utility function
• U = Utility
• R = Reliability
• V = Validity
• E = Educational impact
• A = Acceptability
• C = Cost
• W = Weight
U = wrR x wv
V x weE x wa
A x wcC
Van der Vleuten, CPM (1996) Advances in Health Sciences Education 1, 41-67.
35
Miller GE (1990) Acad Med (Suppl) 65 : S63
Does
Shows how
Knows how
Knows
36
Miller GE (1990) Acad Med (Suppl) 65 : S63
Does
Shows how
Knows how
Knows
OSCEOSCE
Written Exams Written Exams
OSLEROSLER
Clinical Work ObservedClinical Work Observed
ACAT, CbD, CeX, ACAT, CbD, CeX,
Short Answer-Reasoning Short Answer-Reasoning
MCQMCQ

FY Workplace Assessment
• Mini-CEX (from USA): Clinical Examination
• DOPS (developed by RCP): Direct Observation of Procedural Skills
• CBD (based on GMC performance procedures): Case-based Discussion
• MSF (from industry): Multi-Source Feedback
Carr (2006) Postgrad Med J 82: 57638
Practical Exercise
39
Educational interventions
• How will we assess?
• How will we feedback?
• How will we evaluate?
40
Educational interventions
• Communication skills for cancer specialists
• 2nd year medical speciality training
• Medical humanities SSM for medical students
• Masters-level pharmacology module
• Procedural skills for medical students
• Clinical Officers: ETATMBA 41
Communication skills
Learning outcome
To improve communication skills of HCPs working with individuals with cancer, e.g. with respect to breaking bad news, discussion of management plans, end of life care
Duration 2 days
Students Mostly specialist cancer nurses, including Macmillan nurses, also consultants and trainee medics. N = 30.
Teaching & learning
Mainly consultations with simulated patients
42
Speciality training
Learning outcome
To ensure trainees have reached the appropriate stage in the acquisition of the knowledge, skills and attitudes necessary to independent medical practice
Duration 1 year
Students Second-year GP trainees. N = 50.
Teaching & learning
Clinical apprenticeship, protected training days
43
Medical humanities SSM
Learning outcome
By a reading of Middlemarch by George Eliot, to enhance students ability to reflect on medical practice and to enter imaginatively into the lives of others
Duration 90-minute sessions weekly for 10 weeks
Students Second-year medical students. N = 20.
Teaching & learning
Small group teaching and discussion
44

M-level pharmacology moduleLearning outcome
To enhance knowledge and understanding of pharmacotherapies used in diabetes and its complications, and to develop the ability to apply this knowledge in clinical practice
Duration 200 hours, i.e. 20 CATS points
Students Mostly DSNs, a few GPs and endocrinology trainees, some from overseas. N = 20.
Teaching & learning
20 hours directed learning – small group teaching and discussion – and 180 hours self-directed learning
45
Procedural skillsLearning outcome
To ensure newly-qualified doctors are competent in all the bedside and near-patient procedures listed in Tomorrow’s Doctors
Duration 4 years
Students Medical students. N = 200.
Teaching & learning
Small group teaching sessions distributed across three hospitals
46

Clinical Officers Learning outcome
To……………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………..
Duration x………
Students y…………………….
Teaching & learning
z…….
47
The ideal assessment instrument :
• Totally valid.
• Perfectly reliable.
• Entirely feasible.
• Wholly acceptable.
• Huge educational impact.
48
FeedbackPart 2
49
Feedback : definition
“Specific information about the comparison between a trainee’s observed performance and a standard, given with the intent to improve the trainee’s performance”
Van de Ridder JM et al (2008) Med Educ 42(2): 189
50

Feedback : definition
“Specific information about the comparison between a trainee’s observed performance and a standard, given with the intent to improve the trainee’s performance”
Van de Ridder JM et al (2008) Med Educ 42(2): 189
51
Feedback : definition
“Specific information about the comparison between a trainee’s observed performance and a standard, given with the intent to improve the trainee’s performance”
Van de Ridder JM et al (2008) Med Educ 42(2): 189
52
Feedback : definition
“Specific information about the comparison between a trainee’s observed performance and a standard, given with the intent to improve the trainee’s performance”
Van de Ridder JM et al (2008) Med Educ 42(2): 189
53
In this section:
• Importance of feedback
• How to give feedback: models
• How to improve feedback
54

Experiential learning
Feedback
• Its value is self-evident : experiential learning cannot take place without it
• It is often infrequent, untimely, unhelpful or incomplete
• It is often not acted upon to improve performance
56
How to give feedback
• Establish appropriate interpersonal climate
• Use appropriate location
• Establish mutually agreed goals
• Elicit learner’s thoughts and feelings
• Reflect on observed behaviours
• Be non-judgmental
• Relate feedback to specific behaviours
• Offer right amount of feedback
• Offer suggestions for improvement
Hewson MG & Little ML (1998) J Gen Int Med 13 (2) : 111 57

Practical Exercise
58

Pendleton’s Rules
• Clarification of matters of fact
• Trainee identifies what went well
• Trainer identifies what went well
• Trainee discusses what did not do well and how to improve
• Trainer identifies areas for improvement
• Agreement on areas for improvement and formulation of action plan
Pendleton D et al (1984) in The Consultation : an Approach to Learning and Teaching
60
Difficulties with Pendleton ?
• The strict format may inhibit spontaneous discussion.
• Unhelpful polarisation between “good points” and “bad points”
• Opening comments may seem predictable, insincere and a merely a prelude to criticism.
Carr (2006) Postgrad Med J 82: 576
61

Chicago• Review aims and objectives of the job at the start.
• Give interim feedback of a positive nature.
• Ask the learner to give a self-assessment of their progress.
• Give feedback on behaviours rather than personality.
• Give specific examples to illustrate your views.
• Suggest specific strategies to the learner to improve performance.
65
Improving feedback
• Recognise that we all need feedback to learn and improve
• Ask for feedback yourself and model this process for learners
• Inform learners that you expect them to ask for feedback
• Make feedback a routine activity
• Discuss the need of feedback with colleagues
Sergeant J & Mann K in Cantillon P & Wood D (eds) ABC of Learning and Teaching in Medicine 2nd edn (2010)
66
EvaluationPart 3
67

Evaluation : definition
“A systematic approach to the collection, analysis and interpretation of information about any aspect of the conceptualisation, design, implementation and utility of educational programmes”
Mohanna K et al (2004) Teaching Made Easy – a manual for health professionals
68
In this section:
• Purposes of evaluation
• Data sources
• Kirkpatrick’s heirarchy
69

The Audit Cycle
Action plan
Re-audit Review literature
Set criteria & standards
Design audit
Feed back findings Collect data
Analyse data
Ask question(s)
Review standards
Wakley G & Chambers R (2005) Clinical Audit in Primary Care70

Why evaluate ?
• To ensure teaching is meeting students’ needs.
• To identify areas where teaching can be improved.
• To inform the allocation of faculty resources.
• To provide feedback and encouragement to teachers
• To support applications for promotion by teachers.
• To identify and articulate what is valued by medical schools.
• To facilitate development of the curriculum.Morrison (2003) Br Med J 326 : 385
71

Evaluation
• Scale : micro macro
• Formative summative
• Internal external
• Can you evaluate an assessment ?
72

Evaluation : data sources
Student ratings Employer ratings
Peer ratings Video recordings
Self-ratings Administrator ratings
Assessment scores Teacher scholarship
Expert ratings Teacher awards
Student interviews Teaching portfolios
Exit ratings
Based on : Berk RA (2006) Thirteen Strategies to Measure College Teaching73

74
75
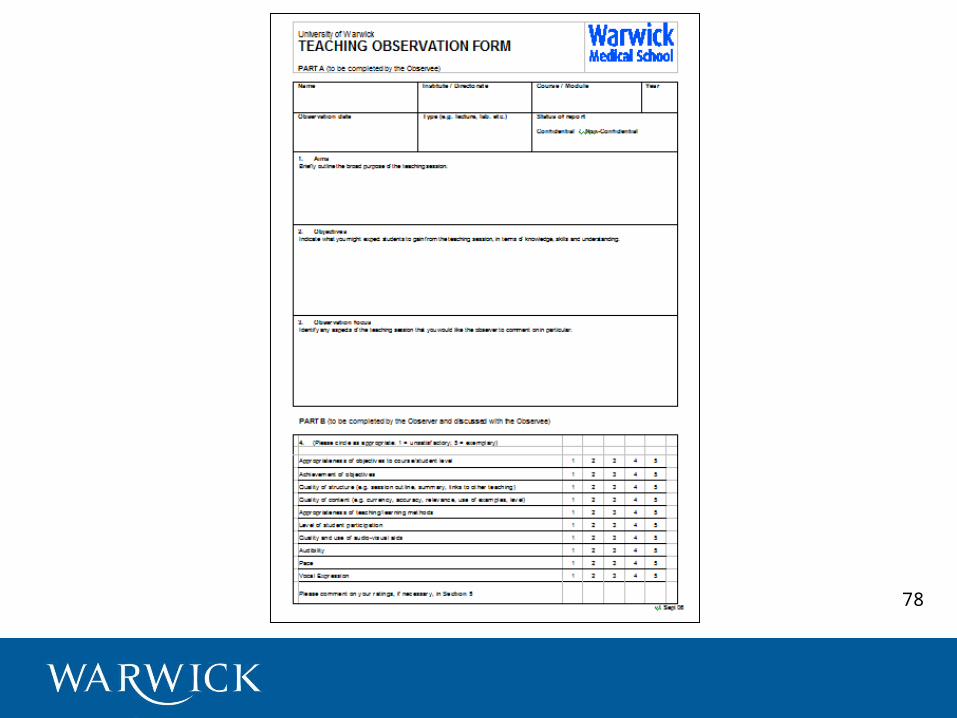
• A method of evaluating teaching
• Different models and purposes
• Three stages: pre-observation, observation, post-observation
• Form (instrument) for recording the information, observation and feedback
Siddiqui ZS, Jonas-Dwyer D & Carr SE (2007) Twelve tips for peer observation of teaching. Medical Teacher 29:297-300
Teaching Observation
76

• Evaluation : authority / summative
• Developmental : expert / formative
• Peer review : collaborative / mutual learning
Teaching Observation : purposes
77
78

Evaluation : triangulation
Self Peers
Students79
Practical Exercise
80

Results
Behaviour
Learning
Reaction
Kirkpatrick’s Hierarchy
Complexity of behaviour
Time elapsed
Reliable measures
Confounding factors
Hutchinson (1999) Br Med J 318 : 1267 81

What’s the point ?
82
83
Issues with Kirkpatrick
• Is it a hierarchy ?
• Omissions : learning objectives ?
• Linkages between levels ?
• “Kirkpatrick plus”
Tamkin P et al (2002) Kirkpatrick and Beyond, IES
84

• There is no perfect assessment instrument
• Feedback to students is essential to experiential learning
• The ultimate purpose of evaluation is to improve clinical outcomes
Conclusions
85