
CHM-II-CHP-01.docx CHM-II-CHP-03.docx CHM-II-CHP-04.docx ...
Upload
revie-iglesiasCategory
view
219download
0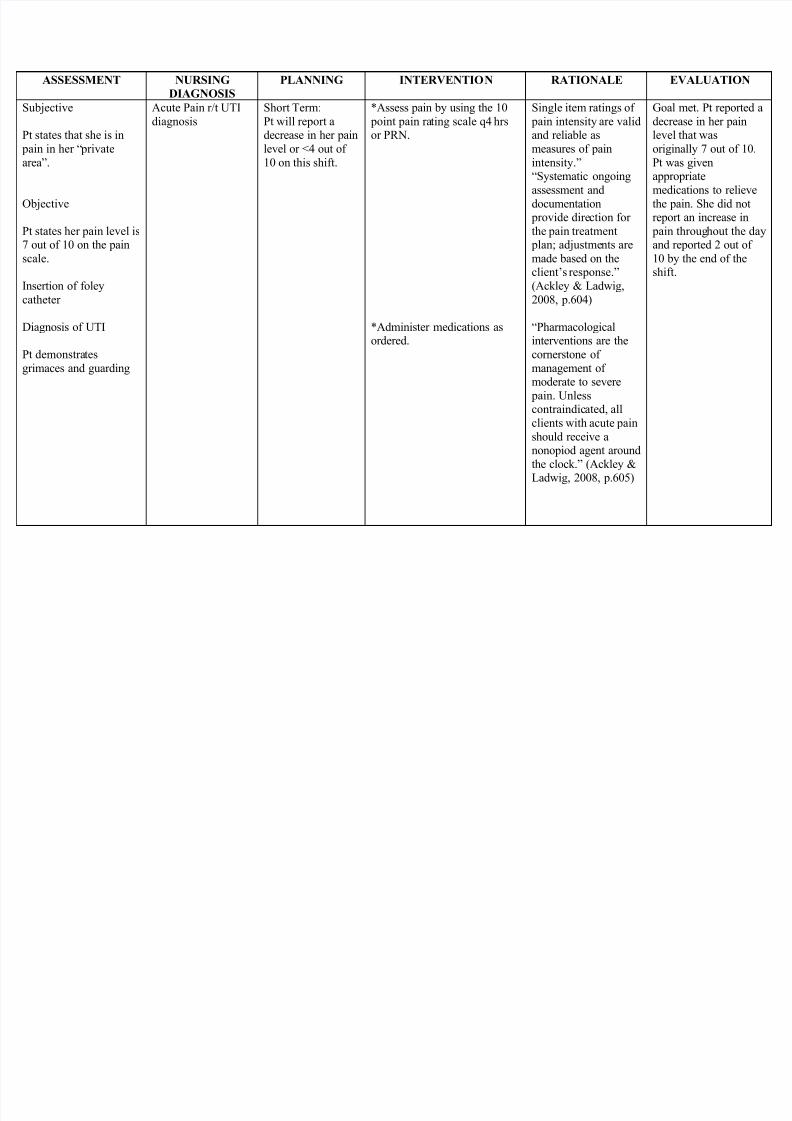
8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 1/31
ASSESSMENT NURSINGDIAGNOSIS
PLANNING INTERVENTION RATIONALE EVALUATION
Subjective
Pt states that she is in pain in her ―privatearea .
Objective
Pt states her pain level is7 out of 10 on the painscale.
Insertion of foleycatheter
Diagnosis of UTI
Pt demonstratesgrimaces and guarding
Acute Pain r/t UTIdiagnosis
Short Term:Pt will report a
decrease in her painlevel or <4 out of10 on this shift.
*Assess pain by using the 10 point pain rating scale q4 hrs
or PRN.
*Administer medications asordered.
Single item ratings of pain intensity are valid
and reliable asmeasures of painintensity. ―Systematic ongoingassessment anddocumentation
provide direction forthe pain treatment
plan; adjustments aremade based on the
client’s response.(Ackley & Ladwig,2008, p.604)
―Pharmacologicalinterventions are thecornerstone ofmanagement ofmoderate to severe
pain. Unless
contraindicated, allclients with acute painshould receive anonopiod agent aroundthe clock. (Ackley &Ladwig, 2008, p.605)
Goal met. Pt reported adecrease in her pain
level that wasoriginally 7 out of 10.Pt was givenappropriatemedications to relievethe pain. She did notreport an increase in
pain throughout the dayand reported 2 out of10 by the end of the
shift.

8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 2/31
*Explain to the pt the painmanagement approach that has
been ordered.
―One of the mostimportant steps towardimproved control of
pain is a better clientunderstanding of thenature of pain, itstreatment, and the rolethe client needs to playin pain control.(Ackley & Ladwig,2008, p.606)

8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 3/31
Glomerulonephritis
ASSESSMENT NURSINGDIAGNOSIS
PLANNING INTERVENTION RATIONALE EVALUATION
Subjective Data:―I felt mutatedwith this enlargedarms and feet sinceif suffered fromthis illness, asverbalized by the
patient.
Objective Data:- +3 edema
on bothfoot
- +2 edemaon bothhands
- (+) periorbitaledema
- (+) proteinuria
- 30 ml urineoutput forthe last 8hours
- Vital signs:BP — 140/90
PR — 120 bpm
Fluid volumeexcess r/tdecreasedglomerularfiltration rate
Short termgoal:
Client willhave anincreased urineoutput of 70-80ml for the next6 hours.
Long termgoal:
Client willhave asustainedminimum urineoutput of 20 ml
per hour andmanifest lesseredema (+) 1.
Assessment: Obtain complete physicalassessment.
Monitor daily weight.
Monitor fluid intake andoutput every 4 hours.
Monitor BP and PR everyhour.
Assess for adventitious breath sounds.
Monitor laboratory valuesespecially for the proteinlevel in the urine.
Treatment:1. Maintain dietary restrictionsduring
acute phase.a. sodium
b. protein
To have baseline data onthe progress of fluidelimination through
physical appearance. To have a measurable
account on the fluidelimination.
To know progressingcondition via glomerularfiltration.
To know progression ofhypertension and basisfor further nursingintervention or referral.
To know for possible progression in the lungs.
To know the extent of protein loss which led toedema.
a. to help prevent fluid retentionvia absorption.
b. it helps prevent fast elevationof BUN level.
Helps prevent further fluidaccumulation while there is
Client had a totalurine output of 72ml 4 hours aftertheimplementation ofthe nursinginterventions.
Client had edemaof (+) 1 the secondday of nursingintervention.Patient also had anaverage of 24 mlof urine output forthe last 10 hours.

8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 4/31
2. Maintain fluid restriction
3. Elevate extremities with pillowswhen at rest or at lying position.4. Administer diuretics as ordered.
5. Administer antibiotics as ordered.6. Administer anti hypertensive drugsas ordered.
Educative:
1. Encourage ambulation and nonstrenuous exercises.2. Teach on the importance ofelevating extremities when at rest.3. Encouraged to maintain clean andmoist skin.
4. Encouraged to stick on dietary andfluid restrictions.
decreased glumerular filtration.
Helps fluid excretion via
gravity.
Helps excrete excess fluidsthrough pharmacologicalreaction.
Fights infection and progressionof scarring.Controls hypertension as caused
by excessive fluid.
1.Helps increase blood and fluidcirculation.
2. Reinforces awareness on itseffect on fluid excretion.
3. Helps prevent skin breakdownand further infection arisingfrom the skin.
4. For client cooperation even inthe absence of any medical
practitioner.

8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 5/31
Nephrolithiasis/Urolithiasis
ASSESSMENT NURSINGDIAGNOSIS
PLANNING INTERVENTION RATIONALE EVALUATION
S> ―masakit anglikod ko as
verbalized
O> with facial
grimace
Irritable at times
Slightly weak inappearance
With guarding
behavior
Pain scale=8/10
BP=110/80
Alteration incomfort; flank painsecondary to diseasecondition
At the end of nursingintervention the
patient will be able to
demonstrate ways
and technique on how
to reduce pain to a
tolerable level
Assessed severity of pain using pain scale
Monitor VS esp. BP
Provided comfort
measures such as
positioning
Provided diversional
activities such as listeningto music or talking to S.O.
Instructed S.O. not to
leave the patient alone
Provided therapeutic
touch
Demonstrated and
encouraged to do deep
breathing exercise
Encouraged back
tapping
For baseline data
For baseline data
To promote comfort
and relaxation
To divert focus of
attention to pain
To prevent pain
stimulation
To promote comfort
and relaxation
For pharmacologic
intervention
―Medyo nawala naung sakit ng likod ko as
verbalized
Pain scale= 6/10
BP=90/60

8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 6/31
Avoid abrupt
movements
Provided adequate rest
and sleep periods
Administered analgesics
as ordered
8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 7/31
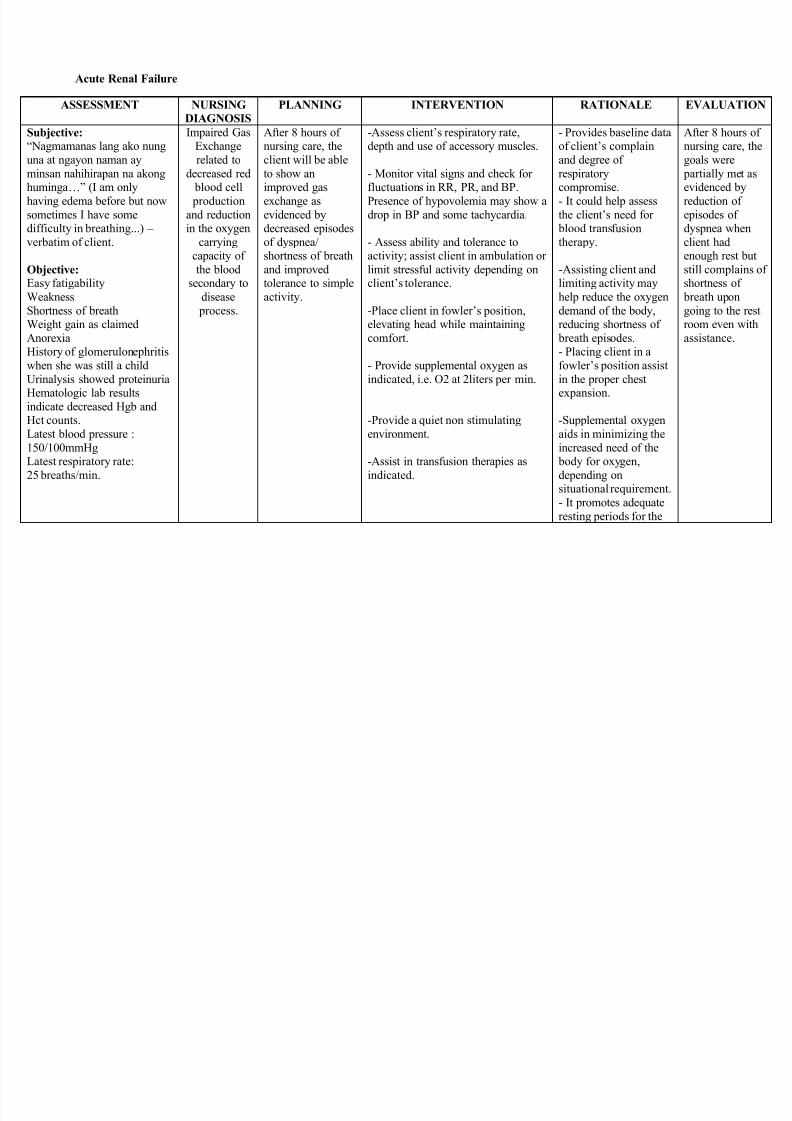
Acute Renal Failure
ASSESSMENT NURSINGDIAGNOSIS
PLANNING INTERVENTION RATIONALE EVALUATION
Subjective:―Nagmamanas lang ako nunguna at ngayon naman ayminsan nahihirapan na akonghuminga … (I am onlyhaving edema before but nowsometimes I have somedifficulty in breathing...) – verbatim of client.
Objective:Easy fatigabilityWeaknessShortness of breathWeight gain as claimedAnorexiaHistory of glomerulonephritiswhen she was still a childUrinalysis showed proteinuriaHematologic lab resultsindicate decreased Hgb andHct counts.Latest blood pressure :150/100mmHgLatest respiratory rate:25 breaths/min.
Impaired GasExchangerelated to
decreased red blood cell production
and reductionin the oxygen
carryingcapacity ofthe blood
secondary todisease
process.
After 8 hours ofnursing care, theclient will be ableto show animproved gasexchange asevidenced bydecreased episodesof dyspnea/shortness of breathand improvedtolerance to simpleactivity.
-Assess client’s respiratory rate,depth and use of accessory muscles.
- Monitor vital signs and check forfluctuations in RR, PR, and BP.Presence of hypovolemia may show adrop in BP and some tachycardia.
- Assess ability and tolerance toactivity; assist client in ambulation orlimit stressful activity depending onclient’s tolerance.
-Place client in fowler’s position,elevating head while maintainingcomfort.
- Provide supplemental oxygen asindicated, i.e. O2 at 2liters per min.
-Provide a quiet non stimulatingenvironment.
-Assist in transfusion therapies asindicated.
- Provides baseline dataof client’s complainand degree ofrespiratorycompromise.- It could help assessthe client’s need for
blood transfusiontherapy.
-Assisting client andlimiting activity mayhelp reduce the oxygendemand of the body,reducing shortness of
breath episodes.- Placing client in afowler’s position assistin the proper chestexpansion.
-Supplemental oxygenaids in minimizing theincreased need of the
body for oxygen,depending onsituational requirement.- It promotes adequateresting periods for the
After 8 hours ofnursing care, thegoals were
partially met asevidenced byreduction ofepisodes ofdyspnea whenclient hadenough rest butstill complains ofshortness of
breath upongoing to the restroom even withassistance.

8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 8/31

8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 9/31
Chronic Renal Failure
ASSESSMENT NURSINGDIAGNOSIS
PLANNING INTERVENTION RATIONALE EVALUATION
Objective:Patient manifested: Edema Hypertension Weight gain Pulmonary
congestion (SOB,DOB)
Oliguria Distended jugular
vein Changes in mental
status
Fluid VolumeExcess R/T decreaseGlomerular filtrationRate and sodiumretention
Short Term :After 4-8 hours ofnursing interventions,
patient willdemonstrate
behaviors to monitorfluid status andreduce recurrence offluid excess
Long Term :After 3 days ofnursing interventionthe patient willmanifest stabilizefluid volume AEB
balance I & O,normal VS, stableweight, and free fromsigns of edema.
1. Establish rapport
2. Monitor and recordvital signs
3. Assess possible riskfactors
4. Monitor and recordvital signs.
5. Assess patient’sappetite
6. Note amount/rate offluid intake from allsources
7. Compare currentweight gain withadmission or previous
1. To assess precipitatingand causative factors.
2. To obtain baseline data
3. To obtain baseline data
4. To note for presence ofnausea and vomiting
5. To prevent fluidoverload and monitorintake and output
6. To monitor fluidretention and evaluatedegree of excess
7. For presence of cracklesor congestion
8. To evaluate degree ofexcess
9. To determine fluidretention
Short Term :The patient shall havedemonstrated behaviorsto monitor fluid statusand reduce recurrenceof fluid excess
Long Term :The patient shall havemanifested stabilizedfluid volume AEB
balance I & O, normalVS, stable weight, andfree from signs ofedema.

8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 10/31
stated weight8. Auscultate breath
sounds
9. Record occurrence ofdyspnea
10. Note presence ofedema.
11. Measure abdominalgirth for changes.
12. Evaluate mentationfor confusion and
personality changes.
13. Observe skin mucousmembrane.
14. Change position ofclient timely.
15. Review lab data likeBUN, Creatinine,Serum electrolyte.
16. Restrict sodium andfluid intake ifindicated
17. Record I&O
10. May indicate increase influid retention
11. May indicate cerebraledema.
12. To evaluate degree offluid excess.
13. To prevent pressureulcers.
14. To monitor fluid andelectrolyte imbalances
15. To lessen fluid retentionand overload.
16. To monitor kidneyfunction and fluidretention.
17. Weight gain indicatesfluid retention or edema.
18. Weight gain mayindicate fluid retention

8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 11/31
accurately andcalculate fluid volume
balance
18. Weigh client
19. Encourage quiet,restful atmosphere.
20. Promote overallhealth measure.
and edema.19. To conserve energy and
lower tissue oxygendemand.
20. To promote wellness.

8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 12/31
Hemodialysis
ASSESSMENT NURSING DIAGNOSIS PLANNING INTERVENTION RATIONALE EVALUATIONSUBJECTIVE:
“Nanghihina ako” asverbalized by thepatient.
OBJECTIVE:
Loss of weight Restlessness Weakness
V/S taken asfollows
T: 36.8 ˚C P: 73R: 18BP: 110/ 80
Risk for deficient fluidvolume. Risk factor mayinclude ultrafiltration, fluidrestriction and actual bloodloss such as systemicheparinization ordisconnection of the shunt
After 8 hours ofnursinginterventions, thepatient will maintainfluid balance asevidenced by stablevital signs, goodskin turgor, moistmucousmembranes,absence ofbleeding, andappropriate weight.
Independent Measure all
sources ofintake andoutput. Havepatient to keepa diary.
Weigh daily aswell as beforeand afterdialysis run.
Monitor vitalsigns duringdialysis.
Ascertainwhetherdiuretics andantihypertensives are to bewithheld.
Verify continuityof shunt or
Aids in evaluatingstatus, especially whencompared with weight.
Weight loss overprecisely measuredtime is a measure ofultrafiltration and fluidremoval.
Hypotension,tachycardia, and fallinghemodynamicpressures suggestsvolume depletion.
Dialysis potentiateshypotensive effects ifthese drugs have beenadministered.
Disconnected shunt oropen access permitsexsanguination.
Minimizes stress on
cannula insertion siteto reduce inadvertentdislodgement andbleeding from site.
Maximizes venousreturn if hypotensionoccurs.
After 8 hours of nursinginterventions, the patientwas able to maintain fluidbalance as evidenced bystable vital signs, goodskin turgor, moistmucous membranes,absence of bleeding, andappropriate weight.

8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 13/31
access catheter.
Apply externalshunt dressing.Permit nopuncture ofshunt.
Place patient ina supine ortrendelenburgposition, asnecessary.
Collaborative Monitor
laboratorystudies asindicated.
Reduce rate ofultrafiltrationduring dialysis,as indicated.
To monitor closely toprevent futurecomplications.
Reduces the amount ofwater being removedand may correcthypotension orhypovolemia.

8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 14/31
Peritoneal Dialysis
ASSESSMENT NURSINGDIAGNOSIS
PLANNING INTERVENTION RATIONALE EVALUATION
O:>cyanosis>rr- 10bpm>shallow
breathing
Risk forIneffectiveBreathingPattern r/tinflammatory
process
After 8 hours ofnursing interventionthe client will displayan effectiverespiratory patternwith clear breathsounds, ABGs within
patient’s normalrange.
1. Monitor respiratoryrate/effort. Reduce infusionrate if dyspnea is present.
2. Auscultate lungs, notingdecreased, absent, oradventitious breath sounds,e.g.,crackles/wheezes/rhonchi.
3. Note character, amount, andcolor of secretions.
4. Elevate head of bed or have patient sit up inchair. Promote deep-
breathing exercises andcoughing
5. Review ABGs/pulseoximetry and serial chest x-rays.
6. Administer supplemental O2as indicated.
7. Administer analgesics asindicated.
1. Tachypnea, dyspnea,shortness of breath, andshallow breathingduring dialysis suggestdiaphragmatic
pressure from distended peritoneal cavity or mayindicate developingcomplications.
2. Decreased areas ofventilation suggest
presence of atelectasis,whereas adventitioussounds maysuggest fluid overload,retained secretions, orinfection.
3. Patient is susceptible to pulmonary infections asa result of depressedcough reflex andrespiratoryeffort, increasedviscosity of secretions,as well as alteredimmune response andchronic/debilitatingdisease.
4. Facilitates chest
After 8 hours ofnursingintervention theclient displayed aneffectiverespiratory patternwith clear breathsounds, ABGswithin patient’snormal range.
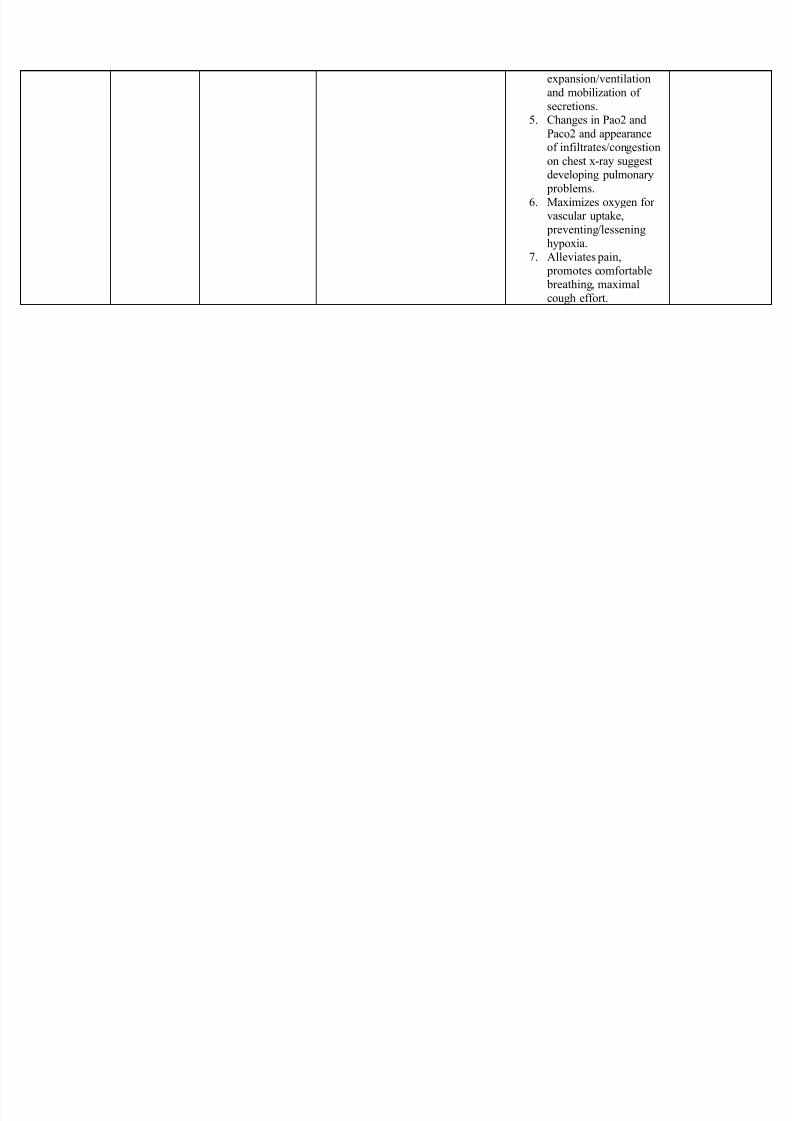
8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 15/31
expansion/ventilationand mobilization ofsecretions.
5. Changes in Pao2 andPaco2 and appearanceof infiltrates/congestionon chest x-ray suggestdeveloping pulmonary
problems.6. Maximizes oxygen for
vascular uptake, preventing/lesseninghypoxia.
7. Alleviates pain, promotes comfortable breathing, maximalcough effort.

8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 16/31

8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 17/31
BloodPressure:130/90mmHg
Collaborative
1. Catheterize forresidual urine and leaveindwelling catheter asindicated.
2. Administermedications as indicated.
term. Antibiotics aregiven to combatinfection.

8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 18/31
Nasopharyngeal Cancer
ASSESSMENT NURSINGDIAGNOSIS
PLANNING INTERVENTION RATIONALE EVALUATION
Subjective:―Masaki tanglalamunan ko lalo na
pag nagsasalita. Asverbalized by theclient.
Objective: Dyspnea Restlessness Use of accessorymuscle Cough Nasal flaring
Prolonged expiratory phase
Ineffective airwayclearance r/ttissue necrosislocated in nasalarea AEBdyspnea,restlessness, useof accessorymuscle, cough,and nasal flaring.
After 3 hours of NI, pt will be able to verbalizeunderstanding of cause andtherapeutic managementregimen and demonstrate
behaviors to improve ormaintain clear airway.
Establish rapport
Position head to facilitateairway
Elevate head of bed
Encourage deep-breathingand coughing exercise
Increase fluid intake
Supportreduction/cessation ofsmoking
To get the trust of the pt. To open or maintainopen airway in at-restor com promisedindividual To take advantage ofgravity decreasing
pressure on thediaphragm andenhancing drainage To maximize effort inexpectoratingsecretions Hydration can helpliquefy viscoussecretions and improvesecretion clearance
To improve lungfunction
After 3 hours of NI, pt was able toverbalizeunderstanding ofcause andtherapeuticmanagementregimen anddemonstrate
behaviors toimprove ormaintain clearairway.

8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 19/31
Ovarian Cancer
ASSESSMENT NURSINGDIAGNOSIS
PLANNING INTERVENTION RATIONALE EVALUATION
Subjective:
―Mabilis akongmapagod ngayon,tingin kokailangan ko pa ngsapat na lakas paramagawa ko yungmga karaniwangginagawa ko asverbalized by theclient.
Objective:
Limitedmovement
Activityintolerancerelated togeneralizedweaknesssecondary tounderlyingdisease process
After 6 hours ofnursingintervention, theclient will stateunderstanding ofand willingness tocooperate inmaximizingactivity level
Independent:
1. Note presence of factorscontributing to fatigue
2. Evaluate current limitations
3. Have patient perform self-careactivities. Begin slowly and increasedaily, as tolerated.
4. Provide emotional support andencouragement
5. Note treatment-related factors,such as side effects/interactions ofmedications
6. Adjust activities
7. Plan care with rest periods betweenactivities
8. Assist with activities and provideclient’s use of assistive devices
- To identify causative factors
- Provides comparative baseline
- Activities will help patientregain health
- To help improve patient’sself-concept and motivation to
perform activities of dailyliving.
- To identify precipitatingfactors
- To prevent overexertion
- To reduce fatigue
- To protect client from injury
After 6 hours ofnursingintervention,goal met, asevidence by client’sable to stateunderstanding ofand willingness tocooperate inmaximizing activitylevel

8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 20/31
9. Encourage client to maintain positive attitude; suggest use ofrelaxation techniques
- To enhance sense of well- being

8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 21/31
Retinoblastoma
ASSESSMENT NURSINGDIAGNOSIS
PLANNING INTERVENTION RATIONALE EVALUATION
Objective:-Eye is opened inhorizontal plane
-Cloudy cornea thatmeasures 10mm x9mm and isedematous
-Anterior chamber isobliterated
-Vitreous cavitycontains granularwhite material
-Sclera is thickenedand fibrotic
-Choroid and focalarea of sclera arediffusely invaded bytumor
DISTURBEDSENSORYPERCEPTIONrelated toaltered status ofsense organ(eyes)secondary toretinoblastoma
Goal:After 8 hours of nursingintervention, the patientwill be able tocompensate for sensoryimpairments.
Independent:Assess ability to speak, hear, interpretand respond to simple commands.
Evaluate sensory awareness: stimulusof hot/cold, dull/sharp, smell, taste,hearing, and location/function of body
parts.
Determine response to painful stimuli.
Provide means of communication and promote stable environment withcontinuity of care by same personnelas much as possible. And reorient to
person, place, time and events, asnecessary.
Avoid isolation of client, physically oremotionally.
Interpret stimuli and offer feedback.
To obtain anoverview ofclient’s mentaland cognitivestatus and abilityto interpretstimuli.
To assess degreeof impairment.
To note whetherresponse isappropriate tostimulus,immediate ordelayed.
To promotenormalization orresponse tostimuli.
After 8 hours of nursingintervention, the patientwas able to compensatefor sensoryimpairments.

8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 22/31
Speak to visually impaired clientduring care.
Provide tactile stimulation as care isgiven.
Provide safety measures as needed.
Position doors and furniture so theyare out of travel path for client withimpaired vision.
Collaborative:Collaborate with and involve otherhealth team members in providingrehabilitative therapies andstimulating modalities
To preventsensorydeprivation andlimit confusion.
To assist client toseparate realityfrom fantasy andaltered
perception.
To provideauditorystimulation and
prevent startlereflex.
Touching is animportant part ofcaring and a deep
psychologicalneedcommunicating
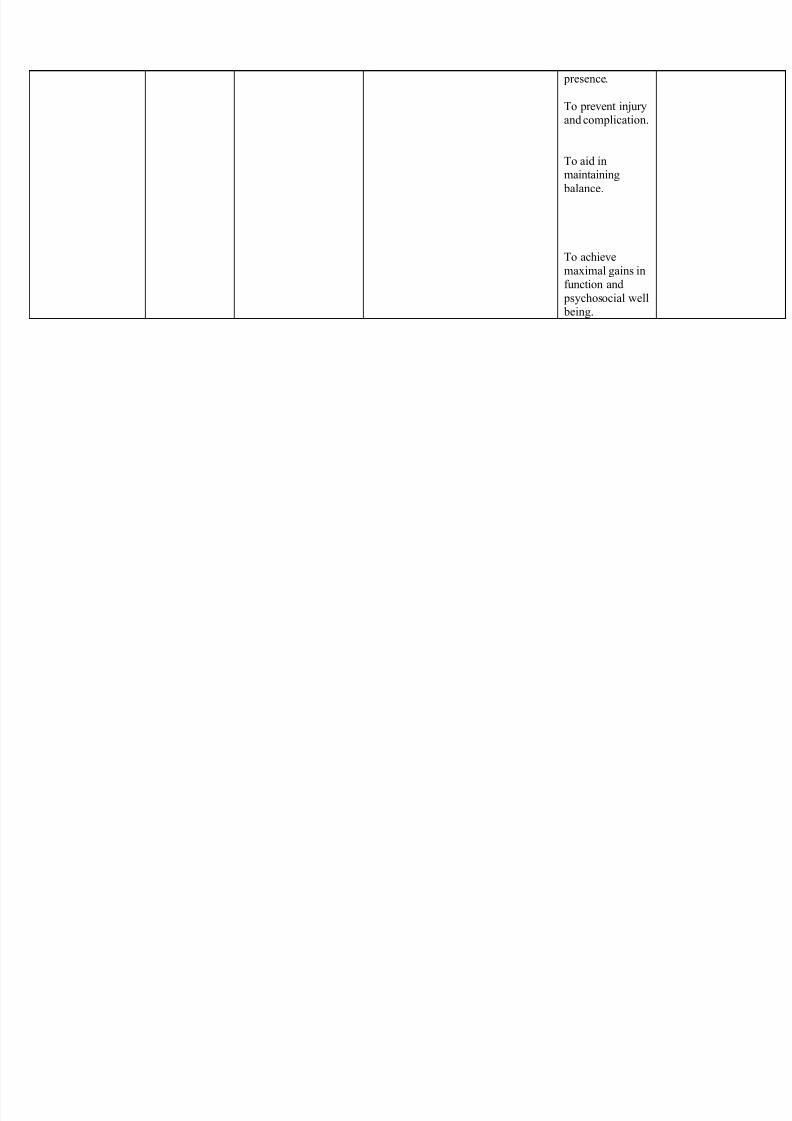
8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 23/31
presence.
To prevent injuryand complication.
To aid inmaintaining
balance.
To achievemaximal gains infunction and
psychosocial well being.

8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 24/31
Oral Cancer
ASSESSMENT NURSINGDIAGNOSIS
PLANNING INTERVENTION RATIONALE EVALUATION
O: PHYSICALEXAMINATION- Vital signs:
RR – 20 breaths/min BP – 120/70mmHg, Larm
PR- 67/min, L arm,radial
T-35.9^C- Skin graft over mouthextending to neck- Mark from tracheostomy,midline, neck, 0.5 cmdiameter- Lateral mouth erosions- Decreased intake of food,difficulty swallowing(blenderized feeding)
LABORATORY RESULTS(02/14/11) Hgb: 84 g/L LOWRBC: 2.80 10^12/L LOWHCT: 0.249% LOW
WBC: 6.88 10^9/L NORMAL Neutrophil 0.745 HIGHLymphocyte = 0.112 LOWMono = 0.103 NORMAL
Risk for Infectionr/t compromisedimmune defensessecondary to cancer
By the end ofthe nursingintervention,the client will:
1. Not developfurther breaksfrom primarydefenses
1. Maintain strictasepsis when
performing procedures toclient .
2. Exercisemeticuloushandwashing
before and afterhandling patient.
3. Check presence ofinvasive devicesand monitor their
present condition.
4. Monitor vitalsigns especiallytemperature every4 hours.
5. Check incisions/wounds for signsof infection.
6. Cleanse mouth
R: Asepsis will preventclient from entry oorganisms thus, protectingher from infection.
R: Frequent, meticuloushandwashing greatlydecreases the chanced of
spreaing infection.
R: Checking of condition oflines or devices, theirduration of attachment willhelp the nurse identify
possible sources ofinfection, which she thencan remove.
R: Fever or hypothermiamay indicate presence ofinfection.
R: Skin and mucosa provide first line defenseagainst microorganisms.
By the end of the shift,the client will be able to:
1. Not acquire anyinfective organism.
2. Cleanliness andhygiene are maintainedat wound sites and bedsides.
3. Developed resistanceto infection throughtechniques

8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 25/31
Eoso = 0.300 NORMALBaso = 0.001 NORMAL
2. Achievetimely woundhealing withno infection.
erosions, if notcontraindicated.
7. Providemeticulous skincare (cleansing
bath)
8. Assist with oralcare (Orahex) ifneeded.
9. Promote frequentand adequate fluidintake.
10. Encourage toapply lubricant(petroleum jelly)to lips and skingraft.
11. Encouragefrequent positionchanges/ambulation, coughing, anddeep breathingexercises. 12.Provide healthteaching on:
R: Ensures that wound is free from infection- causingorganisms and is kept cleanto prevent infections.
R: To prevent skinbreakdown which is a
possible way of infection.
R: Provides care if client isunable.
To liquefy secretions and facilitate expectorations to prevent stasis of body fluidsand promotes moist mucusmembranes.
R: Keeps areas moist.
R: To promote ventilationin all lung segments andaids in mobilizing
secretions to prevent pneumonia.

8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 26/31
Testicular Cancer
ASSESSMENT NURSINGDIAGNOSIS
PLANNING INTERVENTION RATIONALE EVALUATION
Anxietyrelated to crisissituations (cancer),health change,socio-economics,the role andfunctions,form interaction ,
preparation ofdeath, separation offamilies.
After 8 hours ofnursing intervention:
Clientscan relieve anxiety.
Relax and beable to see himselfobjectively.
Demonstrateeffective coping andable to participate intreatment.
Determine the client'sexperience prior to the illness.
Provide accurateinformation about prognosis.
Give the client anopportunity to express anger,fear, confrontation. Givereasonable information to theemotions and expressions
accordingly. Explain the treatment,
the purpose and side effects.Help clients prepare fortreatment.
Note the ineffectivecoping such as lack ofsocial interaction, helpless.
Encourage todevelop interaction with thesupport system.
Provide a quiet andcomfortable environment.
Maintain contact withclients, talk and touch with thefair.
Data about previousclient experience will
provide a basis forcounseling and avoidduplication.
Provision ofinformation to assist clientsin understanding the disease
process.
Can reduceclient anxiety.
Assist clients inunderstanding the need fortreatment and side effects.
Knowing the client'scoping patterns and exploreand resolve / providesolutions in an effort toincrease the strength indealing withanxiety.
So that clients getthe support from the nearest
person / family.
Providing theopportunity for clients to
After 8 hours of nursingintervention:
Clients relievesanxiety
Relax and ableto see himselfobjectively.
Demonstrateeffective coping andable to participate intreatment.

8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 27/31

8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 28/31
Throat Cancer
ASSESSMENT NURSING DIAGNOSIS PLANNING INTERVENTION RATIONALE EVALUATIONO:>difficulty ofswallowing>pain of 7 out of 10>irritability
Ineffective airwayclearance r/t to trachealobstruction and swelling
After 8 hours ofnursingintervention clientwill be able tomaintain patentairway withaspiration
prevented
Monitor respiratory rate, depth,and work of breathing.
Auscultate breath sounds,noting presence of rhonchi.
Assess for dyspnea, stridor,―crowing, and cyanosis. Notequality of voice.
Caution patient to avoid bending neck; support headwith pillows.
Assist with repositioning, deep breathing exercises, and/orcoughing as indicated.
Suction mouth and trachea asindicated, noting color andcharacteristics of sputum.
Respirations may remainsomewhat rapid, butdevelopment ofrespiratory distress isindicative of trachealcompression from edemaor hemorrhage
Rhonchi may indicateairway obstruction/accumulation of copiousthick secretions.
Indicators of trachealobstruction/laryngealspasm, requiring promptevaluation andintervention.
Reduces likelihood oftension on surgicalwound.
Maintains clear airwayand ventilation. Although―routine coughing is notencouraged and may be
painful, it may be neededto clear secretions.
After 8 hours ofnursingintervention clientwas able tomaintain patentairway withaspiration
prevented
8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 29/31
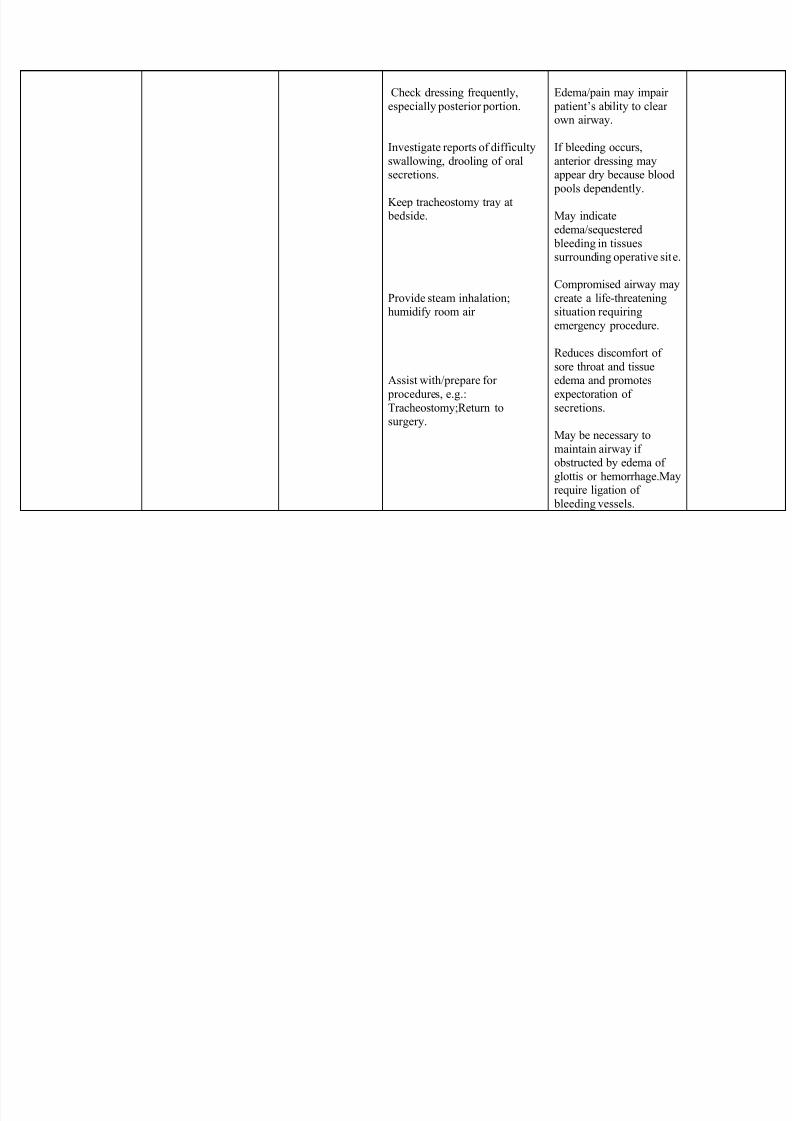
Check dressing frequently,
especially posterior portion.
Investigate reports of difficultyswallowing, drooling of oralsecretions.
Keep tracheostomy tray at bedside.
Provide steam inhalation;humidify room air
Assist with/prepare for procedures, e.g.:Tracheostomy;Return tosurgery.
Edema/pain may impair patient’s ability to clearown airway.
If bleeding occurs,anterior dressing mayappear dry because blood
pools dependently.
May indicateedema/sequestered
bleeding in tissuessurrounding operative site.
Compromised airway maycreate a life-threateningsituation requiringemergency procedure.
Reduces discomfort ofsore throat and tissueedema and promotesexpectoration ofsecretions.
May be necessary tomaintain airway ifobstructed by edema ofglottis or hemorrhage.Mayrequire ligation of
bleeding vessels.

8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 30/31
Pancreatic Cancer
ASSESSMENT NURSING DIAGNOSIS PLANNING INTERVENTION RATIONALE EVALUATIONS: ― Medyokinakabahan
siyempre. I think thatis normal. We do notknow what to expect.
― I just use prayers tocalm down .
― Client cried whenthe nun said that shecould not administerthe holy sacrament theday of her surgery. ”
O: BP = 120/60RR = 24/minPR = 64/min
(+) sleep disturbances,
weakness, faintness,fatigue
Gastroscopy results:Post-endoscopicdiagnosis: duodenalmass probablymalignant, 1 ° VSinfiltration, hiatal
Anxiety (moderate) relatedto actual or perceivedthreat to biologic integritysecondary to invasive
procedures
Anxiety is a state ofmentaluneasiness,apprehension,dread, orforeboding or afeeling ofhelplessnessrelated to animpending oranticipatedunidentifiedthreat to self orsignificantrelationships.
Anxiety on theunkniwn,especially
surgery, isnatural andcommon.
Moderate painincreases in thearousal state toa point wherethe person
GOAL:At the end of thenursingintervention, Mrs.Xxx will relate anincrease in
psychological and physiologiccomfort.
OBJECTIVES:
After the nursingintervention, Mrs.Xxx will:
1. Explain theimportance of
preoperativelaboratory tests in
her own words.
2. Verbalizeunderstanding of
bowel and skin preparation andneed to remove allmake-up and
jewelry prior to
The student nurse will:
1. Explain the need for preoperative laboratorytests
R: The moreinformation a clienthas, the more she isreassured.
2. Discuss bowel andskin preparation andthe need to remove all
jewelry, nail polish,make-up, etc. prior tosurgery.
R: Discuss preparations toempower client.
3. Briefly discuss the procedure to be doneand what the clientcould expect from it.
R: The moreinformation a clienthas, the more she isreassured.
After the nursing intervention,Ms. xxx will:
1. Explain the importance of preoperative laboratory testsin her own words.
2. Verbalize understanding of bowel and skin preparationand need to remove all make-up and jewelry prior tosurgery.
3. State her ownunderstanding of the
procedure to be done andwhat could be expected
4. State the need forrestriction food and oral fluids
for at least 8 hours prior tosurgery.
5. Demonstrate ambulation,leg exercises, deep breathingand coughing exercises.

8/11/2019 ASSESSMEN3.docx
http://slidepdf.com/reader/full/assessmen3docx 31/31
hernia expressesfeelings oftensions,nervousness orconcern.
SOURCE:
Kozier, B., Erb,G., Berman,A. &Snyder, S.(2004).Fundamentals of nursing(7 th ed).Philippines:PearsonPrentice Hall
surgery.
3. State her ownunderstanding of the
procedure to bedone and whatcould be expected
4. State the need forrestriction food andoral fluids for atleast 8 hours priorto surgery.
5. Demonstrateambulation, legexercises, deep
breathing andcoughing exercises.
4. Explain the need forrestriction of food andoral fluids for at least8hours prior to surgery.
R: The moreinformation a clienthas, the more she isreassured.
5. Demonstrate theneed for ambulation,leg exercises, deep
breathing and coughingexercises.
R: This arenonpharmacologicalmethods used to lessenanxiety.









![[MS DOCX]: Word Extensions to the Office Open XML (.docx ......[MS-DOCX] — Word Extensions to the Office Open XML (.docx) File Format 2.2.4.](https://static.fdocuments.us/doc/165x107/6139ff100051793c8c00cb27/ms-docx-word-extensions-to-the-office-open-xml-docx-ms-docx-a-word.jpg)
![[MS-DOCX]: Word Extensions to the Office Open XML (.docx…interoperability.blob.core.windows.net/files/MS-DOCX/[… · · 2017-12-12Word Extensions to the Office Open XML (.docx)](https://static.fdocuments.us/doc/165x107/5a7556437f8b9aa3618c60c7/ms-docx-word-extensions-to-the-office-open-xml-docx-2017-12-12word.jpg)







