Assessing Abilities and Capacities: Sensation Nisrin Alqatarneh MSc. Occupational therapy Assessment...
20
Assessing Abilities and Capacities: Sensation Nisrin Alqatarneh MSc. Occupational therapy Assessment 2015 1
-
Upload
miranda-harrison -
Category
Documents
-
view
217 -
download
0
Transcript of Assessing Abilities and Capacities: Sensation Nisrin Alqatarneh MSc. Occupational therapy Assessment...

Assessment 2015
1
Assessing Abilities and Capacities: SensationNisrin Alqatarneh
MSc. Occupational therapy
Assessment 2015
2
Purposes of sensory evaluation:
• Assess the type and extent of the sensory loss• Evaluate and document sensory recovery• Assist in diagnosis• Determine impairment and functional limitation• Provide direction for OT intervention:• Determine time to begin sensory reeducation• Determine need for education to prevent injury during
occupational functioning• Determine need for desensitization
Assessment 2015
3
Somatosensory deficit patterns:
• Any interruption at the ascending sensory pathways or in the sensory areas of the cortex can lead to decrease or loss of sensation
• The extent and severity of the sensory deficit can be determined by the mechanism and location of the lesion or injury
• Types of injury:
1. Cortical injury
2. Spinal cord injury
3. Peripheral nerve injury

Assessment 2015
4
Guidelines of assessment for patients with cortical injury:
• Screen areas of the body to identify areas for thorough evaluation if a deficit is found
• Assess more thoroughly the areas that are expected to be affected which are the side contralateral to the injury
• For patients with mild cortical impairment; start assessment of the light touch and proprioception, if they are intact we expect temperature and pain to be intact as well
• For patients with severe cortical impairment; start with pain and temperature assessment, if they are absent then light touch and/or proprioception are absent as well
• To reassess recovery start with pain and temperature before light touch and proprioception

Assessment 2015
5Spinal cord injury
• Patients with complete lesions of the spinal cord demonstrate a total absence of sensation in the dermatomes below the level of injury
• Paresthesia: is tingling or pins or needles sensation, it MAY occur in dermatomes associated with the level of the lesion
• Incomplete spinal cord lesions result in loss of sensation related to damage within specific spinal tracts.

Assessment 2015
6
• Damage to anterior part of the spinal cord usually result in loss of pain and temperature sensations below the level of lesion, while touch, vibration, and proprioception remain intact.
• Damage to posterior part of the spinal cord usually affect light touch and vibration, but patient can feel differences between temperatures and painful stimuli

Assessment 2015
7
• Patients with damage to one side of the spinal cord display loss of touch, vibration, and proprioception on the side of lesion, and loss of temperature and pain sensation on the opposite side.
• Mild to moderate compression of the spinal cord may result in decreased or absent sensation in the single dermatome at the level of the compression or could also involve dermatomes below the level of compression.
• Any sensory recovery after traumatic spinal cord injury happens within the first year, most recovery within the first 6 months

Assessment 2015
8
Guidelines of assessment for patients with spinal cord injury:
• Use a test with a strong stimulus (pinprick or cotton ball) to determine the level of the injury.
• Bilateral testing is necessary because results may differ from one side to the other.
• With patients with known complete lesions there is no need to test multiple sensory modalities.
• For incomplete lesions, test using multiple sensory modalities, with at least one measure for pain or temperature, and one for touch, vibration, or proprioception.
Assessment 2015
9
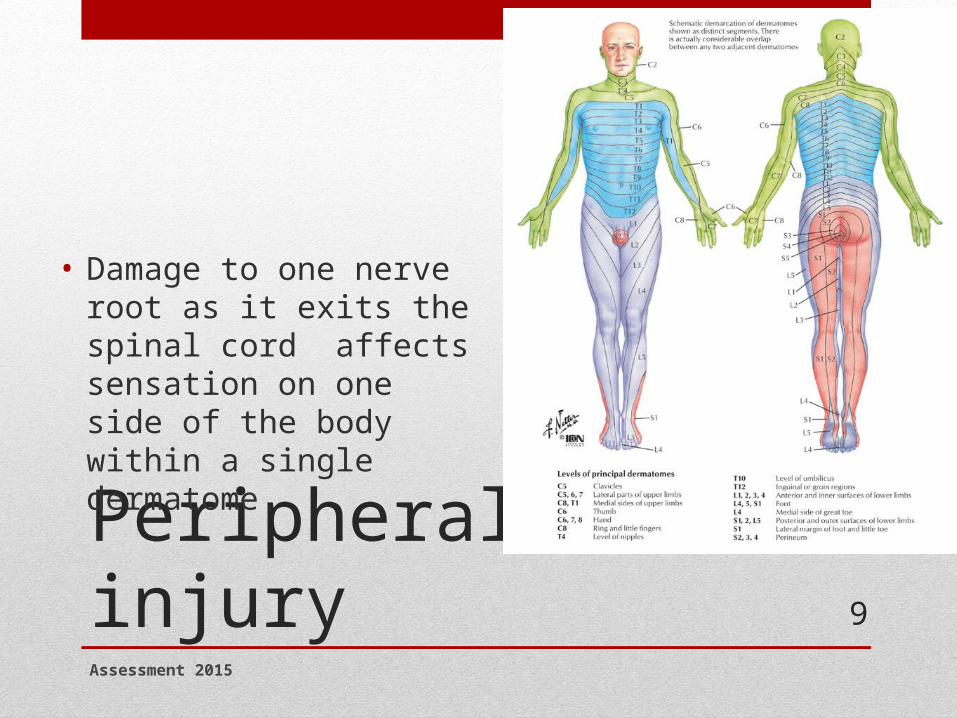
Peripheral nerve injury
• Damage to one nerve root as it exits the spinal cord affects sensation on one side of the body within a single dermatome
Assessment 2015
10
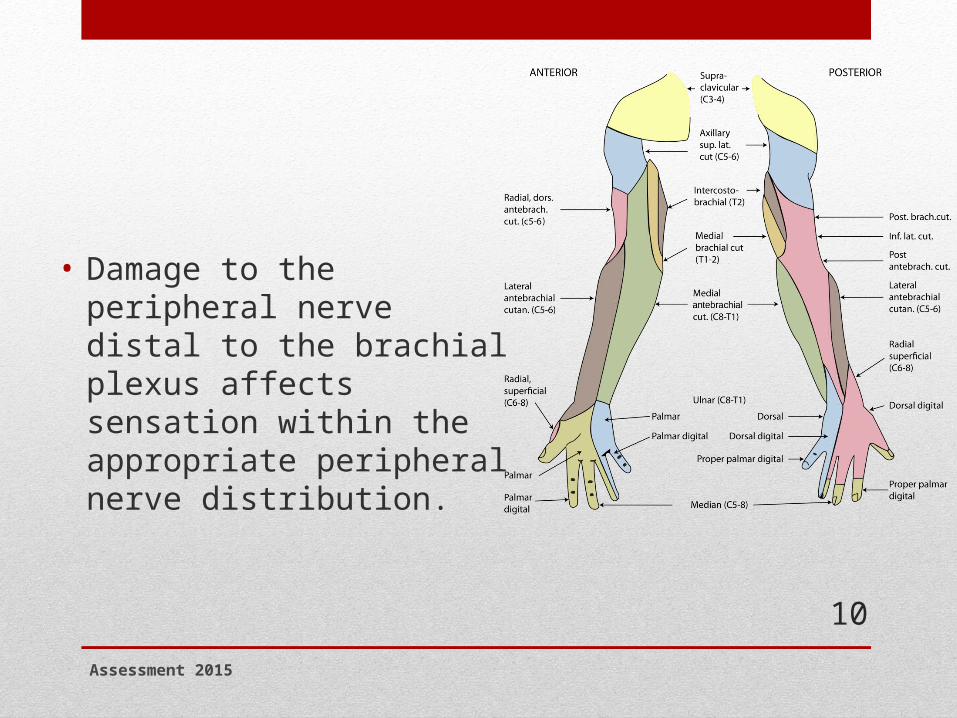
• Damage to the peripheral nerve distal to the brachial plexus affects sensation within the appropriate peripheral nerve distribution.

Assessment 2015
11
• With peripheral nerve compression injuries we sometimes use provocative testing; this is when we put the hand in a position that will provoke the compression (as in median nerve compression; we put the wrist in flexion at the carpal tunnel)
• Manual pressure on the nerve can be combined with the provocative position to further increase stress on the nerve

Assessment 2015
12
Guidelines of assessment for patients with Peripheral nerve injury:
• With patients who has peripheral polyneuropathy, the goal is to establish the impact of the disease on protective sensation
• With patients with a single peripheral nerve injury, the goal is to make a map of both the body area and severity of sensory loss.
• With recovery or nerve compression we use highly sensitive tests to notice small changes in sensation
• Recovery sequence is: pain moving touch light touch touch localization

Assessment 2015
13
Evaluation techniques:
• There are different types of sensory tests:
1. Those that test the use of sensation in skills that support occupational functioning (example, stereognosis)
2. Or to detect very small changes in sensory reception such as touch threshold (example, monofilaments)

Assessment 2015
14
Types of sensory tests:
• Threshold tests: determine the smallest stimuli the patient can observe and is sensitive to change
• Two point discrimination: measures innervation density in the fingers and is sensitive to change
• Touch localization: evaluates not only the sensation but also if it is correctly perceived
• Touch, pain, vibration and temperature awareness: simple to administer but are not sensitive to change
• Kinesthetic and proprioception: less commonly used, not sensitive to change, and is believed to be related to specific type of sensory feedback for coordinated movement
• The picking up and stereognosis: more functional, requires combined motor and sensory function in the hand

Assessment 2015
15
Procedures of sensory testing:
• Choose an environment with minimal distractions• Ensure your patient is comfortable and relaxed• Determine areas of body to test• Stabilize the limb or body part to be tested• Note any differences in color or thickness of skin • Describe the test to your patient and give clear instructions• Demonstrate the test procedures on an intact skin• Occlude the patient’s vision for the test• Apply stimuli at irregular intervals, or insert catch trials in which no
stimulus is given• Observe the patient for discomfort related to the stimuli that may signal
hypersensitivity
Assessment 2015
16
Interpreting of evaluation findings:
• Compare the results with those expected based on the patient’s diagnosis
• Note that although body graphs for sensory distribution is useful but not all humans have the exact borders of sensation, variation are normal
• Always compare to the other side if this is possible (as in peripheral nerve injuries)
• Use clinical reasoning to decide if the results are different enough from expected to suggest neural damage

Assessment 2015
17
• With decreased light touch threshold, patients may not be aware of the sensory problem as their motor is unaffected
• With diminished protective sensation; we see decreased motor coordination (such as dropping objects from the hand, slower manipulation)
• Loss of protective sensation cause an inability to use the hand when it is not in view

Assessment 2015
18
Planning treatment:
• Diminished or loss of protective sensation, or absence of sensation indicate that the patient may be at risk of injuring the limb
• Patient must be taught to rely on vision and adapted environment to compensate for the loss and avoid injury
• If there is hypersensitive of the body part we use a desensitization program
• if there is a decrease only in sensation we use a sensory retraining program, but only if the diagnostic prognosis indicate potential for improvement
Assessment 2015
19
How to chose a sensory assessment method?
• Decide why is the test necessary and what information is needed
• Consider the diagnosis and what the patient’s description of the problem
• Example: in spinal cord injuries we need to know if the sensation is present or absent in each area of the skin, so we may use a touch awareness or pinprick test and record the result on a drawing of the body

Assessment 2015
20
Any questions??