Aspiration pneumonia in older people
36
Aspiration pneumonia in older people Ayman Morish, M.D. Internal medicine, Critical care Medicine and Geriatrics Fellow. .
Transcript of Aspiration pneumonia in older people

Aspiration pneumonia in older people
Ayman Morish, M.D. Internal medicine, Critical care Medicine and Geriatrics Fellow.
.
.

Contents
Epidemiology
Causes of aspiration pneumoniaIssues of older ageManagement
Prevention
.
.

Case 1: admission Jan 26
CHIEF COMPLAINT(S): weakness and feeling unwell
HPI: 90-year-old gentleman. Came from an assisted living facility feeling weak for the past 4 days.
PMH: ESRD on HD, AFib, COPD, CHF, HTN, CAD.
SHx: Assisted living facility. Independent in most of his ADLs and need moderate support with transfer and mobilities.
.
.

P/E VITALS: tachycardia 121,
others unremarkable.
CVS: S1+S2, Irregularly irregular, holo-systolic murmur. No JVD.
Chest: reduced air entry, nwheezing or crackles.
o
Abd: + BS, soft, non-tender, no masses.
Neuro: AAOX3, grossly intact, able to move UE and LE
Extremity: No pitting edema, normal pulses.
.
.

Lab and Imagining
WBC 6.93Na 138 K 3.9BUN 19Creat 2.9BNP 2687
CXR: Left LL infiltrate / atelectasis. Hyperinflated lung suggesting COPD.
.
.

What do you think is going on?
Hold your thoughts for now ..
.
.

Case 2: Admission Feb 14 CHIEF COMPLAINT(S): Weakness, cough, nausea and vomiting. HPI: 90-year-old gentleman. Came from an assisted living facility
complaining of vomiting 3-4 times, chocking and coughing with eating.
Had a recent history of pneumonia 3 weeks ago and was treated with antibiotics. PMH: ESRD on HD, AFib, COPD, CHF, HTN, CAD.
SHx: Assisted living facility. Independent in most of his ADLs and need moderate support with transfer and mobilities.
.
.

P/E
VITALS: stable
Gen: cachectic and ill appearing
Mouth: dry oral mucosa
CVS: S1+S2, Irregularly irregular, 3/6 murmur in the mitral area.
Chest: b/l crackles , left>right
Abd: + BS, soft, non-tender, no rigidity
Neuro: AAOX3, No gross motor or sensory deficit
Extremities: pitting edema, normal pulses.
.
.

Lab and Imagining
WBC 7.76 K 6.2 BUN 71 Cr 5.7 BNP 4357
CXR: interstitial prominence, left lower lobe airspace opacity consistent with atelectasis or consolidation. Left pleural effusion.
.
.

What do you think is going on?
Hold your thoughts for now ..
.
.

Definitions and mechanisms
Aspiration is the misdirection of oropharyngeal or gastric contents into the larynx and lower respiratory tract
Aspiration Pneumonitis is a chemical injury by inhalation of gastric contents.
Aspiration pneumonia is an infection caused by inhalation of bacteria colonized oropharyngeal contents
.
.

Epidemiology
Adults age 65 years and older account for >50 percent of all pneumonia
Incidence of pneumonia increases with aging and frailty
Hospitalisations per year for pneumonia1.1 /1000 young adults12 /1000 old adults 32 /1000 nursing home residents
https://www.uptodate.com
.
.

Epidemiology: cont..
Rate of bacteremia: 1/1000 between age 35-44. 25/1000 at age > 75
Rate of nosocomial pneumonia:<2/1000 between 30-40 17/1000 at age > 70
*Kaplan et al. Arch Intern Med 163:317, 2003, ** Johnstone et al. Medicine 87: 329, 2008
.
.

Bacteriology:
anaerobic bacteria is less common than previously thought. Hard to distinct. Aspiration pneumonia represents a distinct entity from typical
pneumonia? Pneumonia occurs from micro aspiration of oropharyngeal
contents. Similar microbiology and clinical course as aspiration
pneumonia
.
.

Bacteriology: cont...
CAPYoung adult S. pneumoniae; Mycoplasma; Chlamydia
Older adultS. pneumoniae; H. influenza; Chlamydia; S. aureus; Gram-negative rods
.
.

Bacteriology: cont...
NHS. pneumoniaeGram-negative rods S. Aureus
Aspiration PneumoniaSame as NH with anaerobes it was isolated from patients with long-standing processes such as lung abscess; and it is unclear what role they play in early infection
.
.

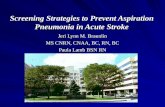
Work up:
https://www.uptodate.com/contents/image?imageKey=RADIOL%2F100988&topicKey=ID%2F7024&source=outline_link
.
.

Indications for extensive workup .
.

Diagnosis:
new hypoxemia pulmonary infiltrates on imaging, particularly in gravity-
dependent lung regions on chest imagingposterior-segments of the upper lobes, basilar segments of the lower lobes
fever leukocytosis tachypnea
.
.

LimitLimitatatiionons:s:
Diagnosis is made in <50% of cases
Insufficient sample.
Gram-negative pathogens and Staph aureus are common.
Strep pneumoniae remains the most common pathogen.
.
.

Risk factors – aspiration pneumonia in older people altered mental status Dysphagia in residents of long-term care facilities
Difficulty swallowing food (OR 2.0) and medication (OR 8.3)Swallowing dysfunction, e.g. in patients with COPD or after
stroke. prolonged supine positionGastroparesis and high residual gastric volumes Aspirations: 71% of patients with CAP compared to 10% in
controls
.
.

Healthy aging and the swallow
Older people swallow more slowlyLaryngeal closure is delayedUpper oesophageal sphincter opening delayedOral bolus transport time prolonged
Safety of oropharyngeal swallowing is not compromisedThere is no increase in aspiration comparing to younger
adults in radiographic studies
.
.

Dysphagia
50% of acute stroke patients have clinical dysphagiaMost (80%) resolve in the first 7-10 days
Associated with big strokes and aphasia Dementia Parkinson diseaseMultiple sclerosis
Mann et al, Stroke 1999; 30:744
.
.

Poor oral health + oropharyngeal bacterial colonization
Can’t do oral hygiene!• Reduced consciousness level• Impaired hand / arm function
Can’t ask for oral hygiene!• Communication barriers
DysphasiaDeliriumDementia
Increased oral vulnerability• Dysphagia• Nil by mouth (NPO)• Drugs (PPI and antiH2)• Nutritional status
.
.

Back to our patients
Did they meet the criteria for diagnosis of aspiration pneumonia?
What are their risk factors
.
.

First case was treated with Unasyn(Ampicillin / Sulbactam)
Second case treated with ceftriaxone
.
.

When to treat?
Prophylactic antibiotics are not recommended Antibiotics are discouraged shortly after aspiration even with
fever, leukocytosis or pulmonary infiltrate. Recommend antibiotics in:1. Aspiration in high risk patients with colonized gastric contents2. Aspiration pneumonitis that fails to resolve within 48 hrs3. Unstable patient with witnessed aspiration
.
.

Treatment:
For nursing home residents, patients with antibiotics use in the last 3 months or patients with comorbidities: Fluoroquinolone (respiratory) alone : moxifloxacin,
levofloxacin, or Gemifloxacin or Macrolides (Azithromycin, clarithromycin, or erythromycin)
plus β-lactams (amoxicillin (high dose) or amoxicillin-clavulanate acid)
Alternative β-lactams: ceftriaxone, cefpodoxime or cefuroxime. Alternative to a Macrolide: doxycycline.
Amoxicillin-clavulanate acid if need anaerobic bacterial coverage.
.
.

Treatment: cont..
Nursing-home or Hospital-acquired Pneumonia Requiring Parenteral Treatment: Antipseudomonal cephalosporin (cefepime or ceftazidime) or
Antipseudomonal carbapenem (imipenem or meropenem) or ß-lactam/ß-lactamase inhibitor (piperacillin-tazobactam)
plus Antipseudomonal fluoroquinolone (ciprofloxacin or levofloxacin) or
Aminoglycoside (amikacin, gentamicin, or tobramycin) plus MRSA Linezolid or vancomycin Ampicillin-sulbactam if need anaerobic bacterial coverage.
.
.

Duration of Treatment:A minimum of 5 days plus no fever for 48 h and should
have no CAP associated sign of clinical instability:
HR >100 bpmRespiratory rate 225/minSBP 00 mmHg02 saturation <90% or Pa02 mmHgAbility to maintain oral intakeabnormal mental status
.
.

Maintain therapy:
Switch from parenteral to oral antibiotics when patient is hemodynamically stable, shows clinical improvement, is afebrile for 16 h, and can tolerate oral medications;
Average duration of 7—14 d depending on clinical response.
Long-term care facility—usually 10—14 d
.
.

Recommendations:
Start early (<4hrs) in critically ill. Target the causative organism. If no infiltrates develop 48 to 72 hours after an aspiration,
it is appropriate to stop antibiotics.
.
.

Management strategies to reduce the risk of aspiration pneumonia
Assistance with regular oral hygiene Screening / investigation for dysphagia
High risk subgroups e.g. stroke, dementia, pneumonia, witnessed aspiration
Nil-by-mouth during high risk periods Postural interventions. Hand-feeding Small amounts frequentlyModified diet / thickened fluids / food supplements
.
.

Swallowing assessment after a stroke:
Routine assessment Look in the mouth!No impaired consciousnessWater swallow test Bedside swallow assessmentSelected patients NasoscopeModified Barium swallow
(video-fluoroscopy)
.
.

Conclusions
Aspiration is the main cause of pneumonia in later life The risk increased with;
dysphagia with oropharyngeal bacterial colonisation Frailty, cognitive impairment and multi-morbidity
AP has non-specific presentation Potential for prevention of AP
multi-modal / multi-disciplinary strategies
.
.

Thank you
.
.