![[XLS] committee 2013.xls · Web viewA double blind, placebo controlled trial of Asenapine in the prevention of recurrence of a mood episode after stabilisation of an acute manic/mixed](https://static.fdocuments.us/doc/165x107/5ac07aee7f8b9a4e7c8be7ec/xls-committee-2013xlsweb-viewa-double-blind-placebo-controlled-trial-of-asenapine.jpg)
Asenapine & agomelatine
51
Asenapine & Agomelatine 1 Dr. Jervin Mano, MD
-
Upload
jervinm -
Category
Health & Medicine
-
view
136 -
download
2
Transcript of Asenapine & agomelatine

Asenapine & Agomelatine
1
Dr. Jervin Mano, MD
Asenapine
2

Introduction
Schizophrenia : mental disorder characterized by problems with thought processes and by poor emotional responses
– Positive symptoms : hallucination
– Negative symptoms : lack of motivation
– Cognitive disturbances : memory disorders
Bipolar disorder: mood disorder with episodes of an elevated or agitated mood known as mania alternating with episodes of depression
3
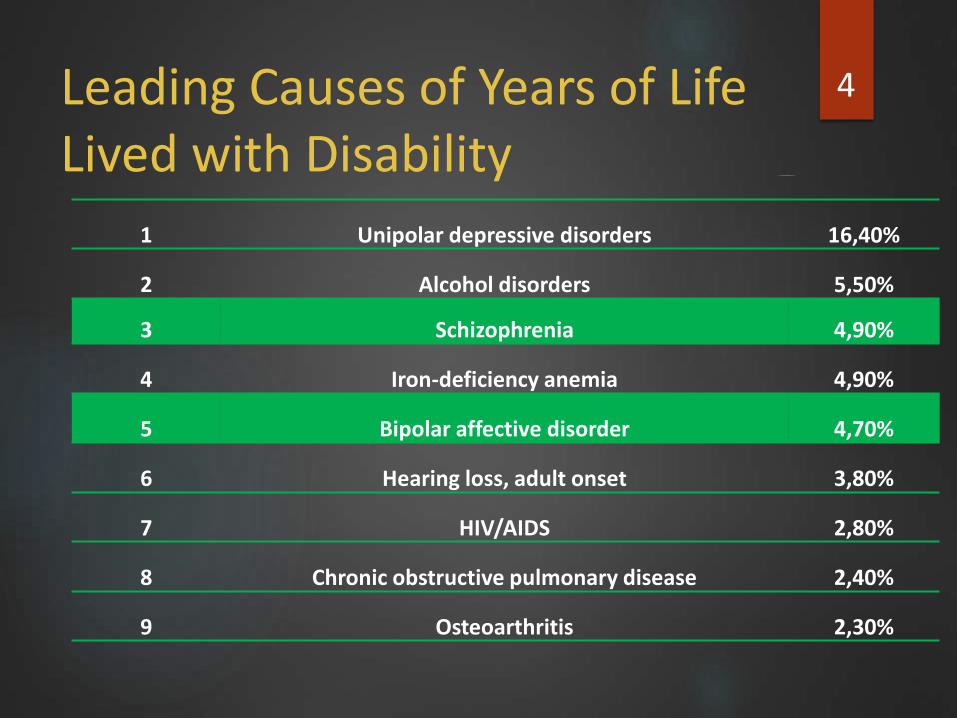
Leading Causes of Years of Life Lived with Disability
1 Unipolar depressive disorders 16,40%
2 Alcohol disorders 5,50%
3 Schizophrenia 4,90%
4 Iron-deficiency anemia 4,90%
5 Bipolar affective disorder 4,70%
6 Hearing loss, adult onset 3,80%
7 HIV/AIDS 2,80%
8 Chronic obstructive pulmonary disease 2,40%
9 Osteoarthritis 2,30%
4

Past historic of anti-psychotics : 5
Limitations with Current Treatment
Effective only in a subset of patients
Prediction of individual treatment response not possible
Are associated with safety and tolerability issues
Extrapyramidal symptoms and akathisia (Haloperidol)
Prolactin increases (Risperidone)
Metabolic changes (Olanzapine)
Weight gain (Olanzapine/Risperidone)
Cardiovascular risk factors (QTc prolongation) (Quetiapine)
Clinical practice: a high rate of switching due to limited efficacy and/ or tolerability
6
ASENAPINE
Important new treatment option for patients with schizophrenia and bipolar disorder
Psychotropic agent belonging to class of dibenzo-oxepino pyrroles
Approved by FDA in Aug 2009
7
MOA
The mechanism of action is unclear
Acts on receptors:
Serotonin :5-HT1A , 5-HT1B , 5-HT2A , 5-HT2B, 5-HT2C , 5-HT5A , 5-HT6 , and 5-HT7
Adrenergic: α1, α2A , α2B, and α2C
Dopamine :D1 , D2 , D3 and D4
Histamine :H1 and H2
No appreciable affinity for muscarinic cholinergic receptors
8

Pharmacokinetics
Absorption
Bioavailability: SL, 35%; swallowed, ≤2%
Peak plasma time: 0.5-1.5 hr
Peak plasma concentration: 4 ng/mL
Distribution
Protein bound: 95%
Vd: 20-25 L/kg
9

Pharmacokinetics
Metabolism
Metabolized by UGT1A4 and CYP450 (predominantly isoenzyme 1A2)
Enzymes inhibited: CYP2D6 (weakly)
Elimination
Half-life: 24 hr
Clearance: 52 L/hr
Excretion: Urine (50%), faeces (40%)
10
TRADE NAME & COST
US/EUROPE
Saphris, Sycrest
INDIA
Asenapt marketed by Sun pharmaceuticals
5mg 10 tabs - ₹55
11

DOSAGE FORMS
5mg sublingual tablets
10 mg sublingual tablets
12

INDICATIONS & DOSAGES 13

Patient Counselling Information
1.Gently remove tablet
Do not crush tablet.
2.Place tablet under tongue and allow it to dissolve completely.
Do not chew or swallow tablet.
Do not eat or drink for 10 minutes.
14

WARNINGS
Mortality
Drug comes with boxed warning of increased mortality in elderly patients with dementia-related psychosis
C/I in patients with dementia-related psychosis
Hypersensitivity
Sep 2011, FDA issues warning of serious hypersensitivity reactions following drug administerations
To be administered with caution
15
ADVERSE DRUG REACTIONS
Neuroleptic Malignant Syndrome
hyperpyrexia, muscle rigidity, altered mental status, and evidence of autonomic instability
1) immediate discontinuation of antipsychotic drugs and other drugs not essential to concurrent therapy
2) intensive symptomatic treatment and medical monitoring
3) treatment of any concomitant serious medical problems
Hypersensitivity Reactions
anaphylaxis, angioedema, hypotension, tachycardia, swollen tongue, dyspnea, wheezing and rash
16
ADVERSE DRUG REACTIONS
Oral hypoesthesia
Reverses in half to one hour after taking the drug
Tardive Dyskinesia
irreversible, involuntary, dyskinetic movements
Weight Gain
regular monitoring of weight
Orthostatic Hypotension
Due to the α1-adrenergic antagonist activity
Application site reactions including oral ulcers, blisters, peeling/sloughing and inflammation
17
ADVERSE DRUG REACTIONS
Leukopenia, Neutropenia, and Agranulocytosis
QT Prolongation
should be avoided in combination with other drugs known to prolong QTc
Hyperprolactinemia
D 2 receptor antagonist
Seizures
Somnolence
Dysphagia
18

ADVERSE DRUG REACTIONS
Hyperglycemia and Diabetes Mellitus
Risk of hyperglycemia-related adverse events
Patients with an established diagnosis of diabetes mellitus who are started on atypical antipsychotics should be monitored regularly for worsening of glucose control
Extra pyramidal syndrome
Lesser incidence than other antipsychotic drugs
19
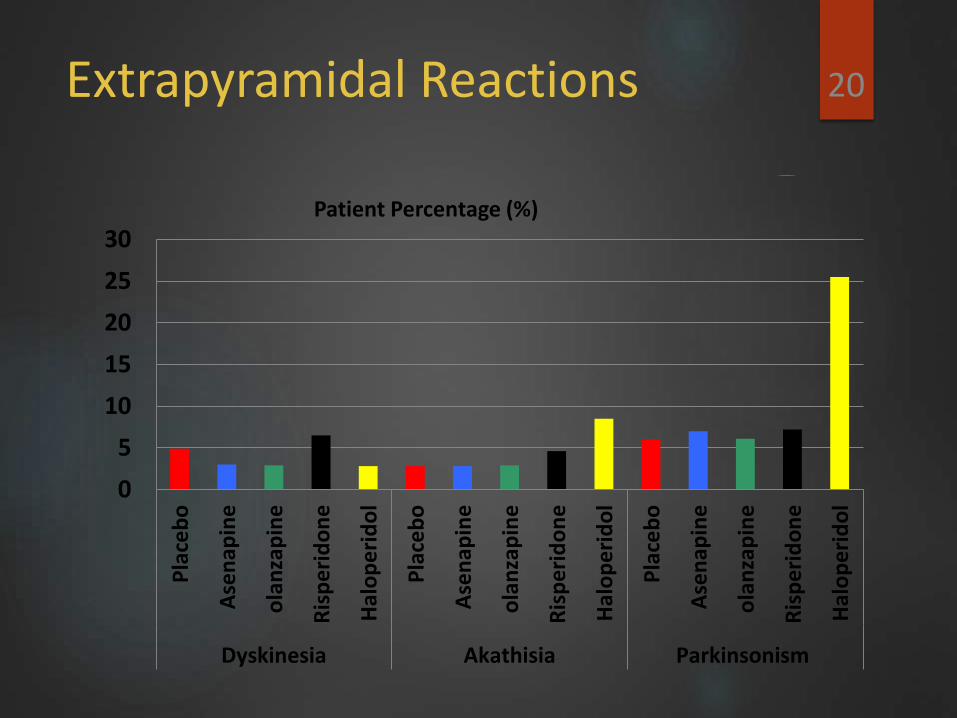
Extrapyramidal Reactions 20
0
5
10
15
20
25
30
Pla
ceb
o
Ase
nap
ine
ola
nza
pin
e
Ris
pe
rid
on
e
Hal
op
eri
do
l
Pla
ceb
o
Ase
nap
ine
ola
nza
pin
e
Ris
pe
rid
on
e
Hal
op
eri
do
l
Pla
ceb
o
Ase
nap
ine
ola
nza
pin
e
Ris
pe
rid
on
e
Hal
op
eri
do
l
Dyskinesia Akathisia Parkinsonism
Patient Percentage (%)
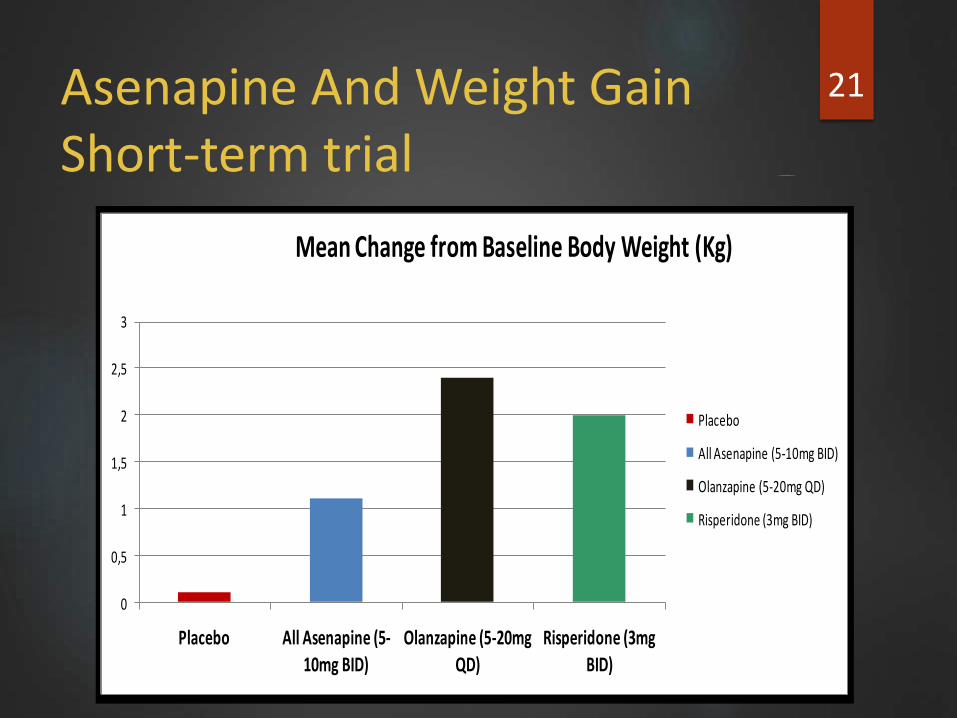
Asenapine And Weight GainShort-term trial
21
0
0,5
1
1,5
2
2,5
3
Placebo All Asenapine (5-
10mg BID)Olanzapine (5-20mg
QD)Risperidone (3mg
BID)
Mean Change from Baseline Body Weight (Kg)
Placebo
All Asenapine (5-10mg BID)
Olanzapine (5-20mg QD)
Risperidone (3mg BID)
Baseline (kg):
P=81.7
A=78.5
R=86.8
O=78.4
21
Drug Interactions
Asenapine weakly inhibits CYP2D6.
Should be coadministered cautiously with drugs that are both substrates and inhibitors for CYP2D6
22
SPECIAL POPULATIONS
Pregnancy: Risk of foetal toxicity category C
Lactation : Excretion in is unknown
Paediatric : Safety and effectiveness have not been established
Caution advised in geriatric age group
Renal Impairment: No dose adjustment needed
Hepatic Impairment:
Mild to moderate impairment (Child-Pugh class A or B): Dose adjustment not necessary
Severe impairment (Child-Pugh class C): Not recommended
OVERDOSAGE
Reported adverse reactions at the highest dosage included agitation and confusion.
No specific antidote available
Management
ECG taken to evaluate arrhythmias
Haemodynamic compromise: intravenous fluids and/or sympathomimetic agents
In case of severe extrapyramidal symptoms, anticholinergic medication should be administered.
CLINICAL TRIALS
SCHIZOPHRENIA
Adult patients who met DSM-IV criteria for schizophrenia were included
Primary efficacy rating scale was the Positive and Negative Syndrome Scale (PANSS).
Trial OneThis study enrolled 174 subjects and compared Asenapine (5 mg twice daily) to placebo, Asenapine was statistically superior to placebo on the PANSS total score.Trial TwoThis trial enrolled 448 subjects and compared two fixed doses of Asenapine (5mg and 10mg twice daily) to placebo. Asenapine 5 mg twice daily was statistically superior to placebo on the PANSS total score.
Trial ThreeAsenapine could not be distinguished from placebo

BIPOLAR DISORDER
3-week, randomized, double-blind, placebo-controlled, and active-controlled (olanzapine) trial
Adult patients who met DSM-IV criteria for Bipolar Disorder were included
Asenapine was statistically superior to placebo on the YMRS total score and the CGI-BP Severity of Illness score

ADVANTAGES DISADVANTAGES
Sublingual form convinient to take
Mechanism of action is unclear
Rapid onset of action Serious ADR of mortality in geraiatric patients with dementia related psychosis
Promising safety and efficacy Limited clinical information available
REFERENCES
Potkin SG, Cohen M, Panagides J Efficacy and tolerability of asenapine in acute schizophrenia: a placebo- and risperidone-controlled trial. The Journal of Clinical Psychiatry 2007 Oct;68(10):1492-500
Marston HM, Young JW, Martin FD, Serpa KA, Moore CL, Wong EH, Gold L, Meltzer LT, Azar MR, Geyer MA, ShahidM Asenapine effects in animal models of psychosis and cognitive function. Psychopharmacology 2009 May 22

Agomelatine
Depression
Mood disorders is a major public health problem
Ranked 2nd by WHO to all diseases in 2010.
Depression : a major mood disorders affecting 340 million people worldwide
Chronic and recurrent depression : disrupts the normal physical & social well being , drives individual to suicide

Goal of treatment of MDD: Remission of all symptoms
Complete recovery of social & vocational dysfunction
Rx available SSRIs
SNRIs
TCAs

A new drug !!…but... Y?
TCAs –
poor tolerability & lethargy in high dose
Reserved for non-responders to SSRIs, SNRIs
SSRIs
Mild to moderate depression
Safe in overdose & cost effective
ADRs – discontinuation , sexual dysfunction , GI disturbances & wt. gain. – only 30-40% achieve remission – increased risk of relapsing , worsening of long term prognosis
Pathogenesis of depression
Monoamine hypothesis :
Depletion of monoamines in hippocampus , limbic system & frontal cortex
SSRIs, SNRIs , TCAs – increases monoamines – only effective in 50% of patients.
Melatonin hypothesis
New evidence – disruption of circadian rhythm –predisposes to depression
Melatonin – hormone from pineal gland – regulates circadian rhythm
Patients with depression
Low levels of melatonin
Delayed onset of sleep
Difficulty in maintaining sleep
Early morning awakening

MT1 & MT2 Rs
MT1 – acute inhibition of neuronal firing within SCN
MT2 – induces phase shifting of circadian rhythm

Chemistry
Synthetic analog of the hormone melatonin
N-[2-(7-methoxynaphthalen-1-yl) ethyl] acetamide
Mechanism of action
Synthetic analogue of human hormone melatonin
Actions on – MT1 & MT2 Rs
Seratonin rs antagonists (5HT-2C)
Neurogenesis
Pharmacokinetics
Metabolism :
Metabolized by Cytochrome P450 1A2 to 7-O –demethylated and hydroxylated inactive metabolites
Excretion :
60-80% excreted as metabolites in urine
Metabolised to 3,4 dihydrodiol which is excreted in faeces
Dosage
25 mg / day
Given once at bed time for 2 weeks
Dose increased to 50 mg if response is inadequate
Sublingual agomelatine 0.5-2mg – under trial
Precautions
Hepatic impairment - ↑plasma levels upto 100 times
Renal impairment - ↑ plasma levels by 25 %
Pregnancy & lactation
Pediatric
≥ 60 yrs of age
Drug interactions
Does not inhibit or induce Cytochrome p450 enzymes
Enzyme inducers like omeprazole and nicotine decrease the serum levels of agomelatine.
Enzyme inhibitors like Fluoxamine and oestrogens increase the serum levels

Uses
Major depressive disorder especially in non-responders and intolerant to SSRIs
Generalized anxiety disorder
Bipolar depression
Sleep disturbances
Migraine and cluster headaches
Adverse drug reactions
Well tolerated
Adverse effect profile similar to placebo
Headache, nausea, dry mouth, fatigue
Dizziness †
Diarrhea / constipation
Insomnia, somnolence
Upper abdominal pain
Overdose
Well tolerated
Reported overdoses up to 525mg have not resulted in significant or serious sequelae.
1200mg was taken in earliest clinical sstudies
800mg – maximum tolerated dose
LD50 in animals was 100 times greater than the human dose

Brands in India
Brand NameComposition Company Packing MRP Rs
AGOTINE Agomelatine 25mg UNICHEM 10 70
AGOVIZ Agomelatine 25mg ABBOTT 10 69.5
CIRCALTIN Agomelatine 25mgZYDUS NEUROSCIENCE 7 49
NOVELTIN Agomelatine 25mg INTAS 10 79.5
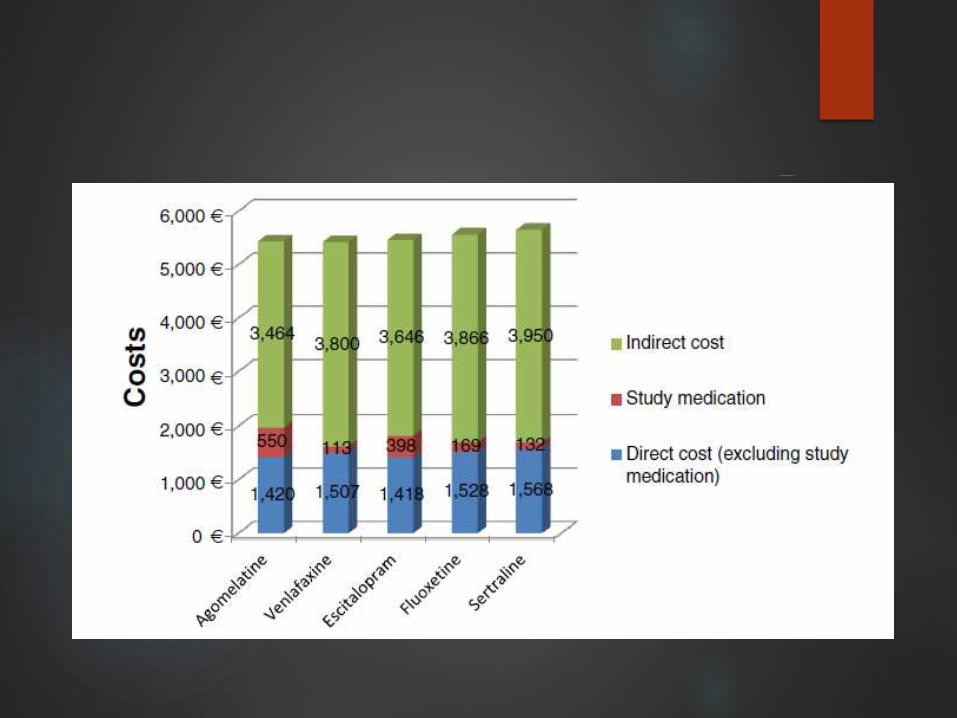
Pharmacoeconomics
Agomelatine with venlafaxine, sertraline, fluoxetine or escitalopram
Provides greater benefit and is less costly compared to escitalopram, generic fluoxetine and generic sertraline
Cost-effective alternate to generic venlafaxine
Advantages
Good tolerability profile
No discontinuation symptoms
Serotonin syndrome, suicidal tendencies, cardiovascular effects and weight gain have not been observed
Minimal GI disturbance and sexual dysfunction
Efficacy is similar to SSRIs and relapse rate is less compared to all the other antidepressants
Improves the quality of sleep without daytime sedation
Limitations
Lack of long term active comparator controlled studies.

Approval status
Europe & Australia – 2006 for major depression
USA – yet to be approved
Clinical Trials
Dose finding and efficacy study: 25mg – 50mg bed time dose
Early onset of efficacy: Agomelatine has quick onset of action detectable from 7th day after starting treatment as compared to venlafaxine
With active comparators: Agomelatine demonstrated greater efficacy than venlafaxine and sertraline at 6 months
Sleep and day time functioning: Agomelatine was superior to venlafaxine and sertraline in “getting to sleep and quality of sleep”.
Relapse and remission: Goodwin et al have shown significantly lower relapse and remission rate vs placebo. An insignificant difference between agomelatine and sertraline or venlafaxine was observed
51


















