ASEeXAM Review Course - American Society of...
40
Michael D. Pettersen M.D. Director, Echocardiography Rocky Mountain Hospital for Children Denver, CO [email protected] ASEeXAM Review Course
-
Upload
truongduong -
Category
Documents
-
view
214 -
download
1
Transcript of ASEeXAM Review Course - American Society of...
Michael D. Pettersen M.D.
Director, Echocardiography
Rocky Mountain Hospital for Children
Denver, CO
ASEeXAM
Review Course
Congenital Heart Disease for the Adult Echocardiographer The vast majority of congenital heart defects are currently detected within the first several years of life.
Therefore, the term “adult congenital heart disease” is something of an oxymoron. In the “ancient” days
before diagnostic ultrasound, there was less precision in early diagnosis. Improvements in surgical
techniques for correcting most congenital cardiac defects have progressed along with our diagnostic skills,
making early diagnosis easier and necessary. For all of these reasons, congenital heart disease is more
commonly recognized and more frequently diagnosed today than in years past. The result of this is a
declining population of adult patients with undiagnosed congenital heart defects. However, the
improvements in the success of medical management and surgical repair has led to the growing number of
patients who reach adulthood. The clinical course, natural history, and outcome for many of these patients
is uncertain because of the time has not allowed for collection of the “unnatural history” of the repaired
defects.
The ASEexam® will probably deal mainly with issues of unrepaired congenital heart disease. Therefore,
these items will be emphasized in this manual and talk. However, questions may appear which deal with
knowledge of congenital operations in terms of “what they do”, although the imaging issues are apparently
not addressed in detail.
Basics Principles of Congenital Heart Disease
An understanding of the incidence and frequency of congenital heart disease will aid the clinician in
developing an index of suspicion for variation types of defects.
Perspective
The science of pediatric cardiology is almost 50 years old. Prior to about 1947, there was very little to offer
patients with congenital heart disease and many died. In the last 40 years and particularly the last 15-20,
great strides have been made in imaging, surgery and interventional techniques which have significantly
improved the outcome. However, since we are dealing with children who have a whole lifetime to live, we
still do not know what the distant future may hold for many of our successes. This unknown perspective
should be emphasized when counseling the patients and parents of children with congenital heart disease.
Incidence
The incidence of congenital heart disease is approximately 0.5-0.8% of live births. The incidence may be
higher in premature babies than in full-term infants if PDA is included, and congenital cardiac malformations
are much more common in stillbirths than in live births. Heart disease remains the most common lethal
anomaly in the newborn. About 32,000 infants are born each year with congenital heart disease.
Approximately 960,000 Americans with heart defects are alive today. 1993 death rates for congenital heart
disease is about 2 per 100,000 people.
The figures quoted above do not include mitral valve prolapse (MVP) or the congenitally bicuspid aortic
valve, (BAV) which occur in 4-6% and 1-2% of the population, respectively.
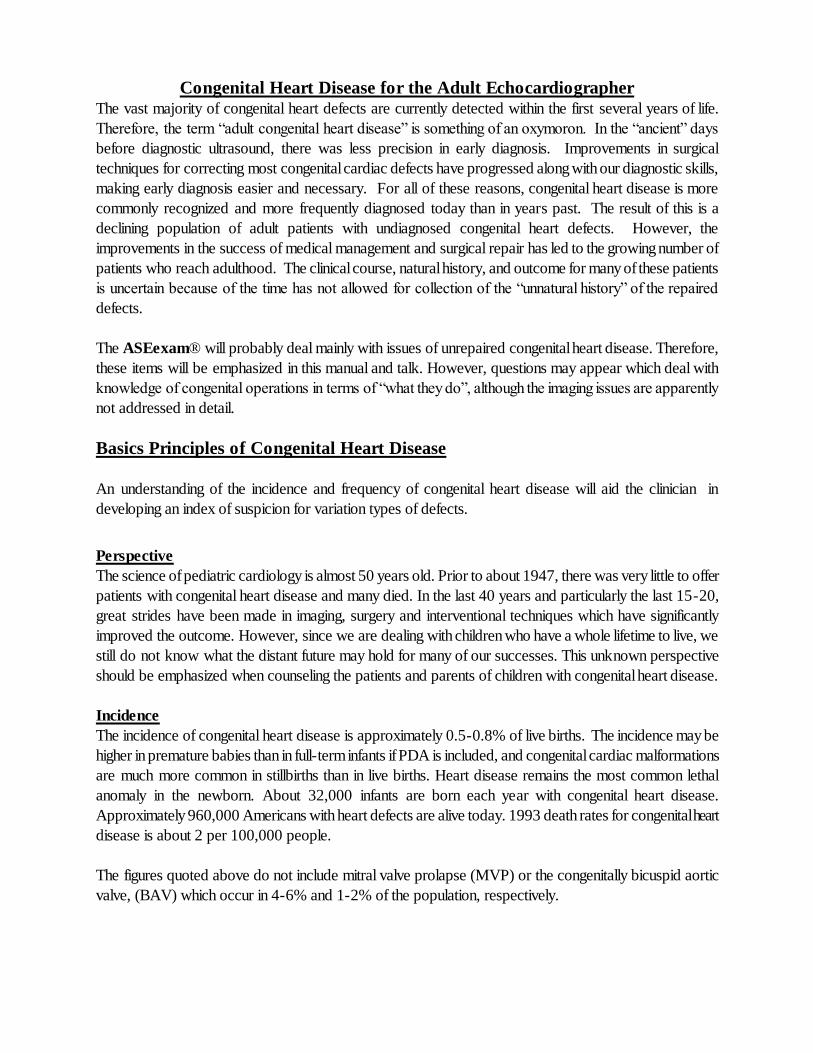
Frequency of Congenital Heart Defects Congenital defects
%CHD
Simple shunts (ASD, VSD, PDA)
50
Simple obstruction (AS, PS, coarctation)
20
Complex (combination lesions, tetralogy, etc.)
30
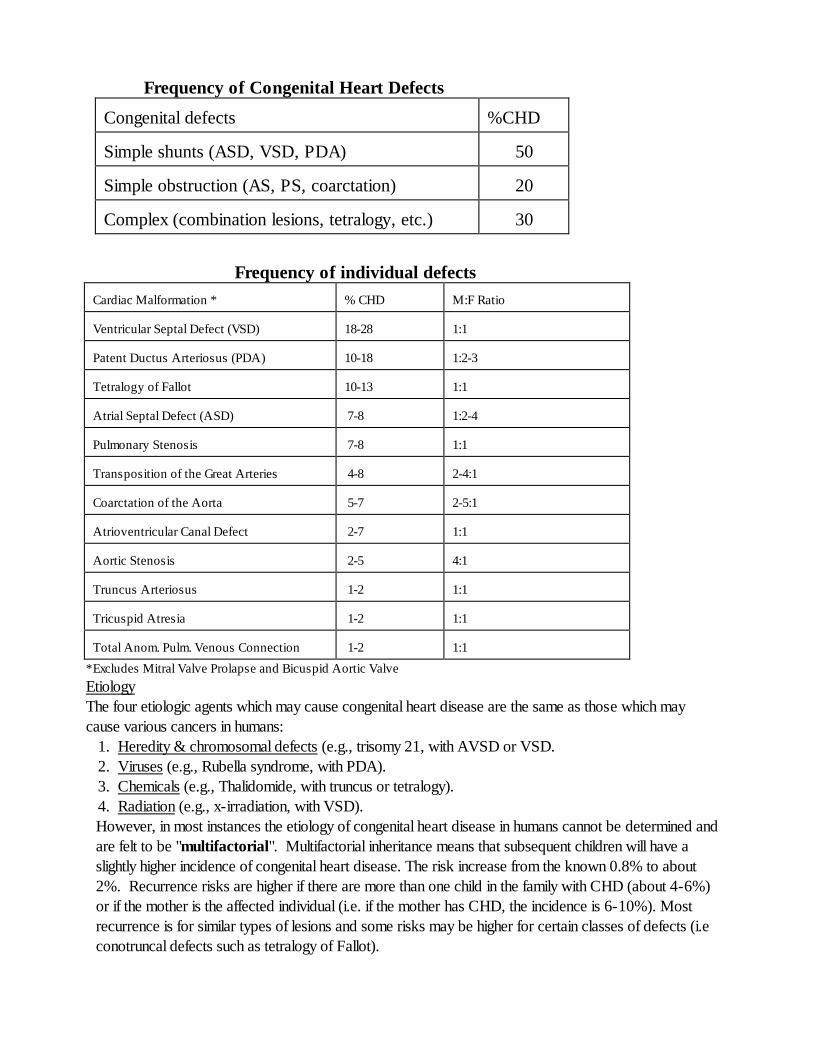
Frequency of individual defects
Cardiac Malformation *
% CHD
M:F Ratio
Ventricular Septal Defect (VSD)
18-28
1:1
Patent Ductus Arteriosus (PDA)
10-18
1:2-3
Tetralogy of Fallot
10-13
1:1
Atrial Septal Defect (ASD)
7-8
1:2-4
Pulmonary Stenosis
7-8
1:1
Transposition of the Great Arteries
4-8
2-4:1
Coarctation of the Aorta
5-7
2-5:1
Atrioventricular Canal Defect
2-7
1:1
Aortic Stenosis
2-5
4:1
Truncus Arteriosus
1-2
1:1
Tricuspid Atresia
1-2
1:1
Total Anom. Pulm. Venous Connection
1-2
1:1
*Excludes Mitral Valve Prolapse and Bicuspid Aortic Valve
Etiology
The four etiologic agents which may cause congenital heart disease are the same as those which may
cause various cancers in humans:
1. Heredity & chromosomal defects (e.g., trisomy 21, with AVSD or VSD.
2. Viruses (e.g., Rubella syndrome, with PDA).
3. Chemicals (e.g., Thalidomide, with truncus or tetralogy).
4. Radiation (e.g., x-irradiation, with VSD).
However, in most instances the etiology of congenital heart disease in humans cannot be determined and
are felt to be "multifactorial". Multifactorial inheritance means that subsequent children will have a
slightly higher incidence of congenital heart disease. The risk increase from the known 0.8% to about
2%. Recurrence risks are higher if there are more than one child in the family with CHD (about 4-6%)
or if the mother is the affected individual (i.e. if the mother has CHD, the incidence is 6-10%). Most
recurrence is for similar types of lesions and some risks may be higher for certain classes of defects (i.e
conotruncal defects such as tetralogy of Fallot).
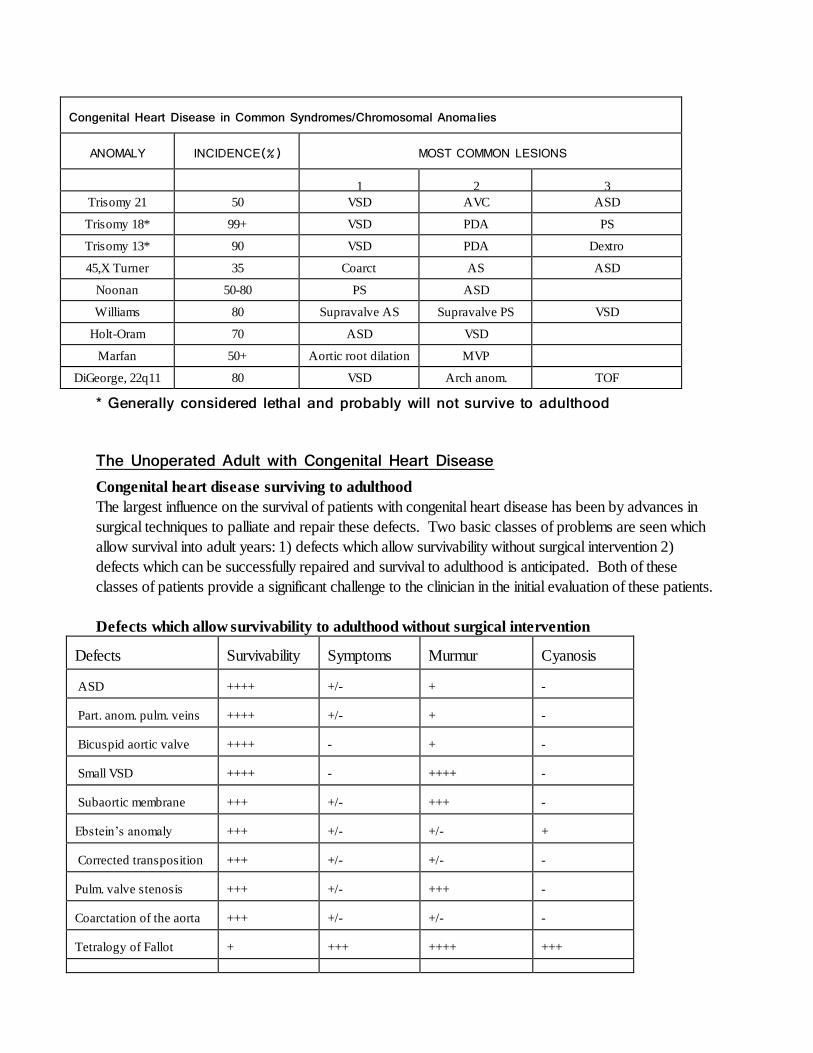
Congenital Heart Disease in Common Syndromes/Chromosomal Anomalies
ANOMALY
INCIDENCE(%)
MOST COMMON LESIONS
1
2
3
Trisomy 21 50 VSD AVC ASD
Trisomy 18* 99+ VSD PDA PS
Trisomy 13* 90 VSD PDA Dextro
45,X Turner 35 Coarct AS ASD
Noonan 50-80 PS ASD
Williams 80 Supravalve AS Supravalve PS VSD
Holt-Oram 70 ASD VSD
Marfan 50+ Aortic root dilation MVP
DiGeorge, 22q11 80 VSD Arch anom. TOF
* Generally considered lethal and probably will not survive to adulthood
The Unoperated Adult with Congenital Heart Disease
Congenital heart disease surviving to adulthood
The largest influence on the survival of patients with congenital heart disease has been by advances in
surgical techniques to palliate and repair these defects. Two basic classes of problems are seen which
allow survival into adult years: 1) defects which allow survivability without surgical intervention 2)
defects which can be successfully repaired and survival to adulthood is anticipated. Both of these
classes of patients provide a significant challenge to the clinician in the initial evaluation of these patients.
Defects which allow survivability to adulthood without surgical intervention Defects
Survivability
Symptoms
Murmur
Cyanosis
ASD
++++
+/-
+
-
Part. anom. pulm. veins
++++
+/-
+
-
Bicuspid aortic valve
++++
-
+
-
Small VSD
++++
-
++++
-
Subaortic membrane
+++
+/-
+++
-
Ebstein’s anomaly
+++
+/-
+/-
+
Corrected transposition
+++
+/-
+/-
-
Pulm. valve stenosis
+++
+/-
+++
-
Coarctation of the aorta
+++
+/-
+/-
-
Tetralogy of Fallot
+
+++
++++
+++
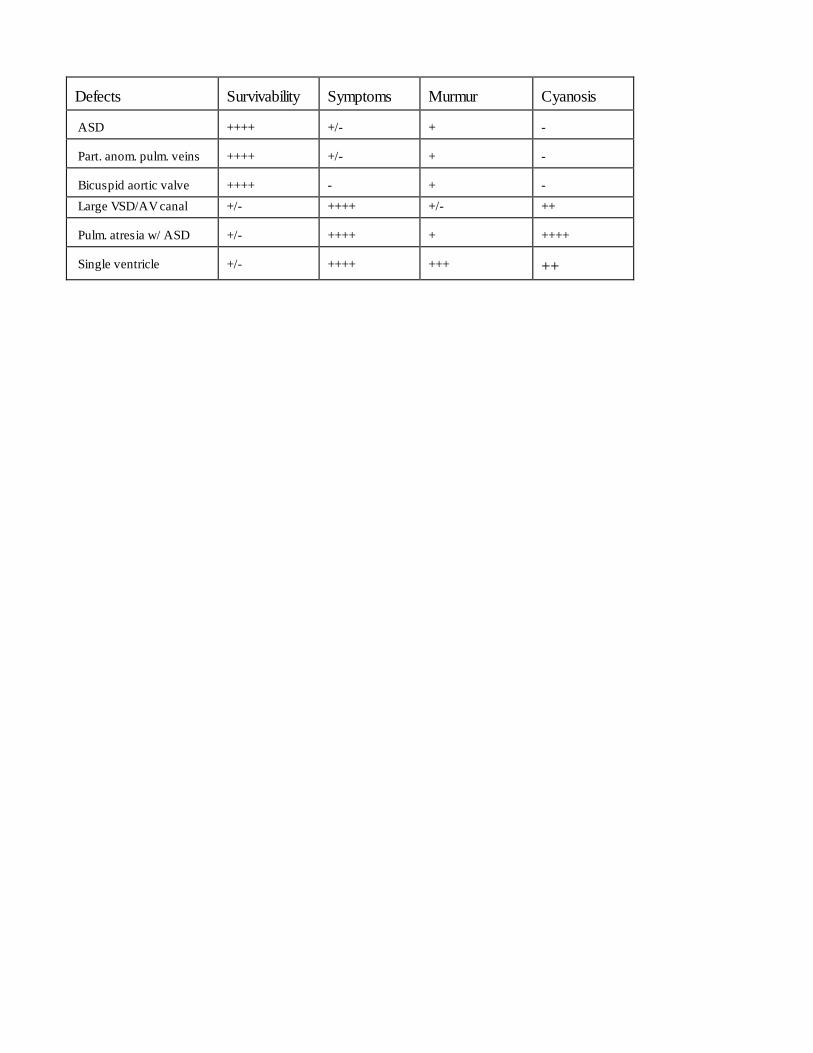
Defects
Survivability
Symptoms
Murmur
Cyanosis
ASD
++++
+/-
+
-
Part. anom. pulm. veins
++++
+/-
+
-
Bicuspid aortic valve
++++
-
+
-
Large VSD/AV canal +/- ++++ +/- ++
Pulm. atresia w/ ASD
+/-
++++
+
++++
Single ventricle
+/-
++++
+++
++
Fetal Echocardiography (not discussed in lecture)
Fetal echocardiography may be used to detect most major and minor cardiac defects. This test is
generally performed as early as 18-20 weeks gestation. This timing allows for optimal visualization of
cardiac structures by balancing fetal size with the relative amount of amniotic fluid and bony rib density.
The heart has completed its development by 8 weeks of gestation.
Established indications for fetal echo:
1. Previous child with heart disease
2. Personal (maternal) history of heart disease
3. Suspected heart rhythm problem in the baby
4. Fluid around the baby's heart (hydrops)
5. Suspected heart defect in the baby/abnormal OB ultrasound
6. Suspected non-cardiac defect in baby with potential related cardiac disease
7. Maternal history of diabetes
8. History of drug/medicine/teratogen use
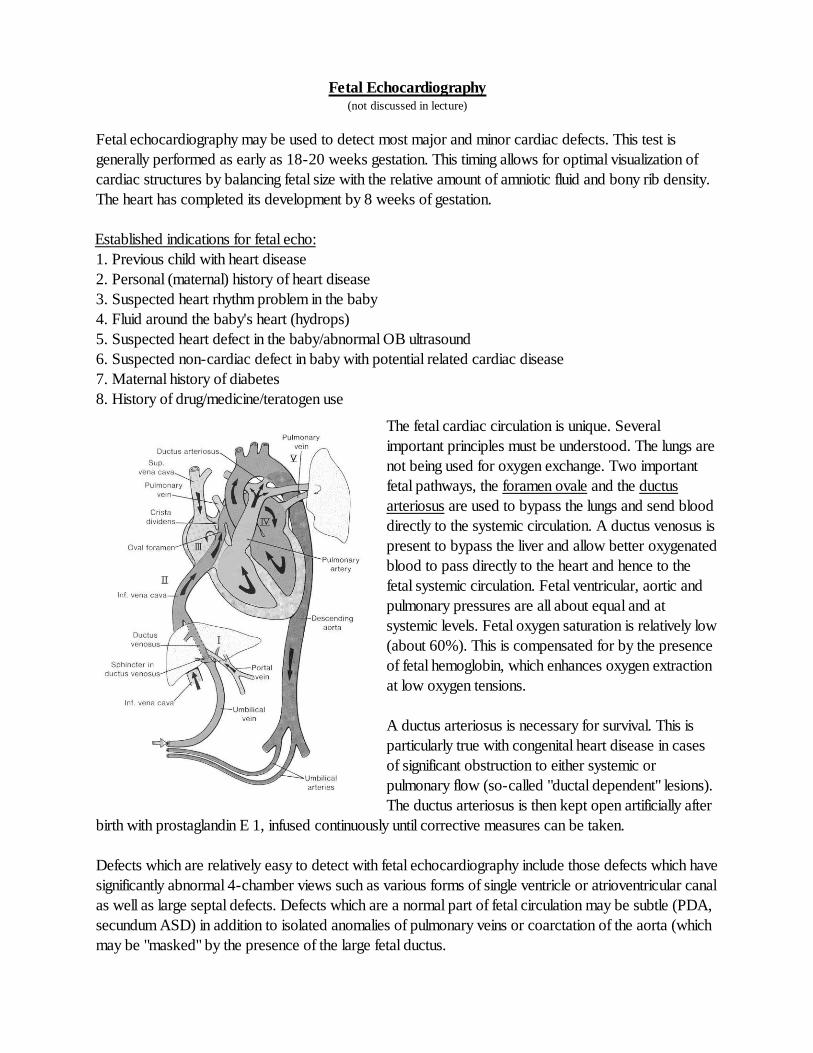
The fetal cardiac circulation is unique. Several
important principles must be understood. The lungs are
not being used for oxygen exchange. Two important
fetal pathways, the foramen ovale and the ductus
arteriosus are used to bypass the lungs and send blood
directly to the systemic circulation. A ductus venosus is
present to bypass the liver and allow better oxygenated
blood to pass directly to the heart and hence to the
fetal systemic circulation. Fetal ventricular, aortic and
pulmonary pressures are all about equal and at
systemic levels. Fetal oxygen saturation is relatively low
(about 60%). This is compensated for by the presence
of fetal hemoglobin, which enhances oxygen extraction
at low oxygen tensions.
A ductus arteriosus is necessary for survival. This is
particularly true with congenital heart disease in cases
of significant obstruction to either systemic or
pulmonary flow (so-called "ductal dependent" lesions).
The ductus arteriosus is then kept open artificially after
birth with prostaglandin E 1, infused continuously until corrective measures can be taken.
Defects which are relatively easy to detect with fetal echocardiography include those defects which have
significantly abnormal 4-chamber views such as various forms of single ventricle or atrioventricular canal
as well as large septal defects. Defects which are a normal part of fetal circulation may be subtle (PDA,
secundum ASD) in addition to isolated anomalies of pulmonary veins or coarctation of the aorta (which
may be "masked" by the presence of the large fetal ductus.
Pregnancy and Maternal Congenital Heart Disease (not discussed in lecture)
Maternal congenital heart disease poses a new set of problems for the clinician and
echocardiographer. A thorough knowledge of the hemodynamics of each individual’s congenital heart
disease should be present before making generalizations about any individual clinical problem.
Patients who have grown up with CHD, even those with multiple operative procedures, are often very
ignorant of the specifics of their own hear problem. This is because the pediatric cardiologist usually
directs the discussion to the responsible parent during many informative discussions. OLD RECORDS
are essential in this type of evaluation so that incorrect diagnoses may be rejected.
Prior to pregnancy:
1. Pregnancy should be planned. Appropriate non-invasive or invasive evaluation of pregnancy risk
should be sought.
2. Contraception should be considered. In many forms of CHD, standard-dose estrogen oral agents
may increase the risk of thrombosis and should be avoided.
3. The increased recurrence risk of the offspring of affected individuals should be mentioned.
Effects of pregnancy:
1. Volume expansion: Cardiac output and total blood volume increases until about 30 weeks gestation.
2. Systemic hypertension may be present in later stages of pregnancy and may profoundly effect
hemodynamics.
3. The risk of SBE is generally low.
4. Patients with obligatory intracardiac shunts are at increased risk for embolic phenomena.
Defects not found above probably fall into a moderate risk category clinically. Tetralogy of Fallot is a
good example. However, obstetricians and perinatologists do not have "moderate risk" categories, so
many of these patients will be classified as high risk. More data is being collected regularly on the risk
and outcome of these types of pregnancies.
Cardiac defects which are low risk:
Post repair of a simple shunt
Simple, mild valvular abnormalities
(Bicuspid AV, mild PS)
Cardiac defects which are high risk:
Eisenmengers/pulmonary hypertension -Pregnancy contraindicated
. Single ventricle- Fontan
Marfan syndrome
Significant aortic stenosis, coarctation
Ventricular failure
Clinical and Anatomic Aspects of Congenital Heart Lesions
1) Ventricular Septal Defect (VSD)
Definition. A ventricular septal defect is an abnormal opening in the ventricular septum, which allows
communication between the right and left ventricles. It is the most common form of congenital heart
disease, accounting for about 25% of defects.
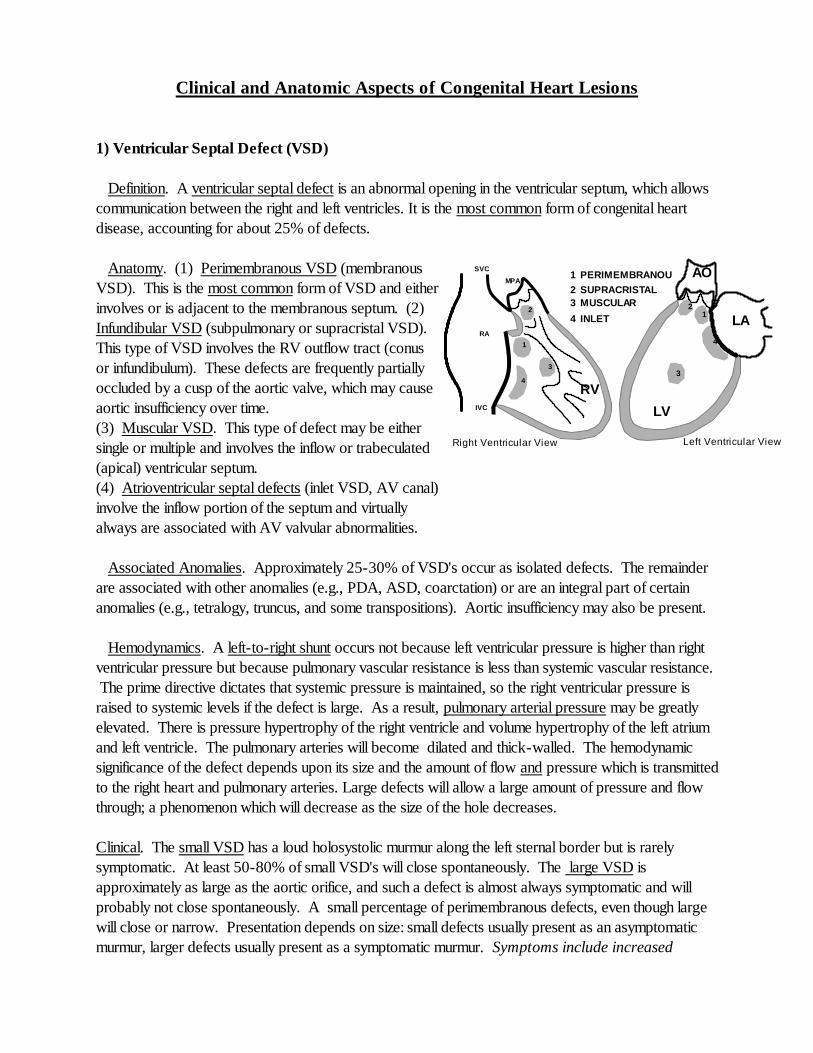
Anatomy. (1) Perimembranous VSD (membranous
VSD). This is the most common form of VSD and either
involves or is adjacent to the membranous septum. (2)
Infundibular VSD (subpulmonary or supracristal VSD).
This type of VSD involves the RV outflow tract (conus
or infundibulum). These defects are frequently partially
occluded by a cusp of the aortic valve, which may cause
aortic insufficiency over time.
(3) Muscular VSD. This type of defect may be either
single or multiple and involves the inflow or trabeculated
(apical) ventricular septum.
(4) Atrioventricular septal defects (inlet VSD, AV canal)
involve the inflow portion of the septum and virtually
always are associated with AV valvular abnormalities.
Associated Anomalies. Approximately 25-30% of VSD's occur as isolated defects. The remainder
are associated with other anomalies (e.g., PDA, ASD, coarctation) or are an integral part of certain
anomalies (e.g., tetralogy, truncus, and some transpositions). Aortic insufficiency may also be present.
Hemodynamics. A left-to-right shunt occurs not because left ventricular pressure is higher than right
ventricular pressure but because pulmonary vascular resistance is less than systemic vascular resistance.
The prime directive dictates that systemic pressure is maintained, so the right ventricular pressure is
raised to systemic levels if the defect is large. As a result, pulmonary arterial pressure may be greatly
elevated. There is pressure hypertrophy of the right ventricle and volume hypertrophy of the left atrium
and left ventricle. The pulmonary arteries will become dilated and thick-walled. The hemodynamic
significance of the defect depends upon its size and the amount of flow and pressure which is transmitted
to the right heart and pulmonary arteries. Large defects will allow a large amount of pressure and flow
through; a phenomenon which will decrease as the size of the hole decreases.
Clinical. The small VSD has a loud holosystolic murmur along the left sternal border but is rarely
symptomatic. At least 50-80% of small VSD's will close spontaneously. The large VSD is
approximately as large as the aortic orifice, and such a defect is almost always symptomatic and will
probably not close spontaneously. A small percentage of perimembranous defects, even though large
will close or narrow. Presentation depends on size: small defects usually present as an asymptomatic
murmur, larger defects usually present as a symptomatic murmur. Symptoms include increased
AO
LA
LV
Left Ventricular View
1 2
3
4
Right Ventricular View
IVC
SVC
RV
MPA
RA
1
1 PERIMEMBRANOU
S
2
2 SUPRACRISTAL
3
3 MUSCULAR
4
4 INLET
respiratory effort and/or feeding difficulties. The additional presence of an apical mitral diastolic
flow rumble from the defect represents significantly increased flow.
In most unoperated patients with a large VSD, obstructive pulmonary vascular disease eventually
develops, and a right-to-left shunt (shunt reversal) with cyanosis becomes evident (Eisenmengers
syndrome). Once irreversible pulmonary hypertension is present, the VSD is considered inoperable.
Even in large VSD's, Eisenmengers syndrome is uncommon under 1 year.
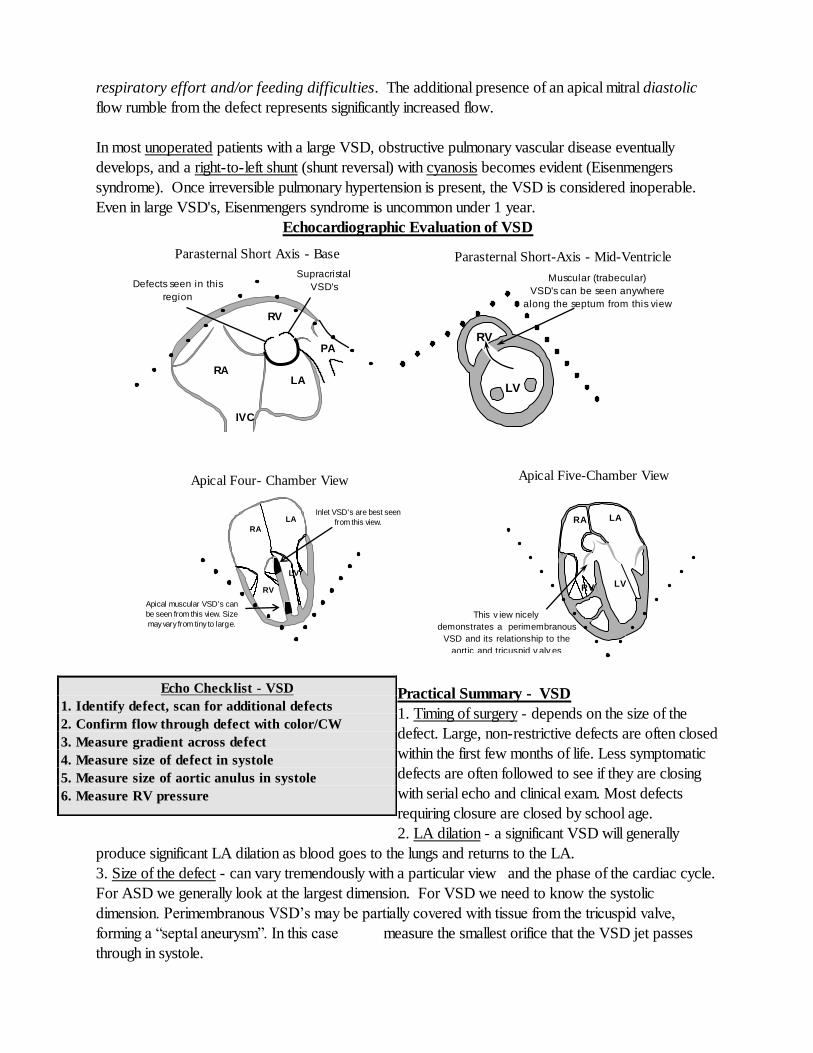
Echocardiographic Evaluation of VSD
Practical Summary - VSD
1. Timing of surgery - depends on the size of the
defect. Large, non-restrictive defects are often closed
within the first few months of life. Less symptomatic
defects are often followed to see if they are closing
with serial echo and clinical exam. Most defects
requiring closure are closed by school age.
2. LA dilation - a significant VSD will generally
produce significant LA dilation as blood goes to the lungs and returns to the LA.
3. Size of the defect - can vary tremendously with a particular view and the phase of the cardiac cycle.
For ASD we generally look at the largest dimension. For VSD we need to know the systolic
dimension. Perimembranous VSD’s may be partially covered with tissue from the tricuspid valve,
forming a “septal aneurysm”. In this case measure the smallest orifice that the VSD jet passes
through in systole.
Echo Checklist - VSD
1. Identify defect, scan for additional defects
2. Confirm flow through defect with color/CW
3. Measure gradient across defect
4. Measure size of defect in systole
5. Measure size of aortic anulus in systole
6. Measure RV pressure
Parasternal Short Axis - Base
RV
LA RA
IVC
PA
Defects seen in this
region
are perimembranous
Supracristal
VSD's
are seen here
Parasternal Short-Axis - Mid-Ventricle
LV
RV
Muscular (trabecular)
VSD's can be seen anywhere
along the septum from this view
Apical Four- Chamber View
Apical muscular VSD's can
be seen from this view. Size
may vary from tiny to large.
RA
LA
LV
RV
Inlet VSD's are best seen
from this view.
Apical Five-Chamber View
This v iew nicely
demonstrates a perimembranous
VSD and its relationship to the
aortic and tricuspid v alv es
LA
LV RV
RA
4. Aortic regurgitation - supracristal defects and some perimembranous defects can distort the aortic
valve and cause aortic regurgitation, particularly in older children.
5. Type of surgical closure - this is an open heart procedure, median sternotomy, usually with patch
closure. The patch is sewn to the RV side of the septum and may be difficult to distinguish from normal
tissue after many years. Usually it is echo-bright.
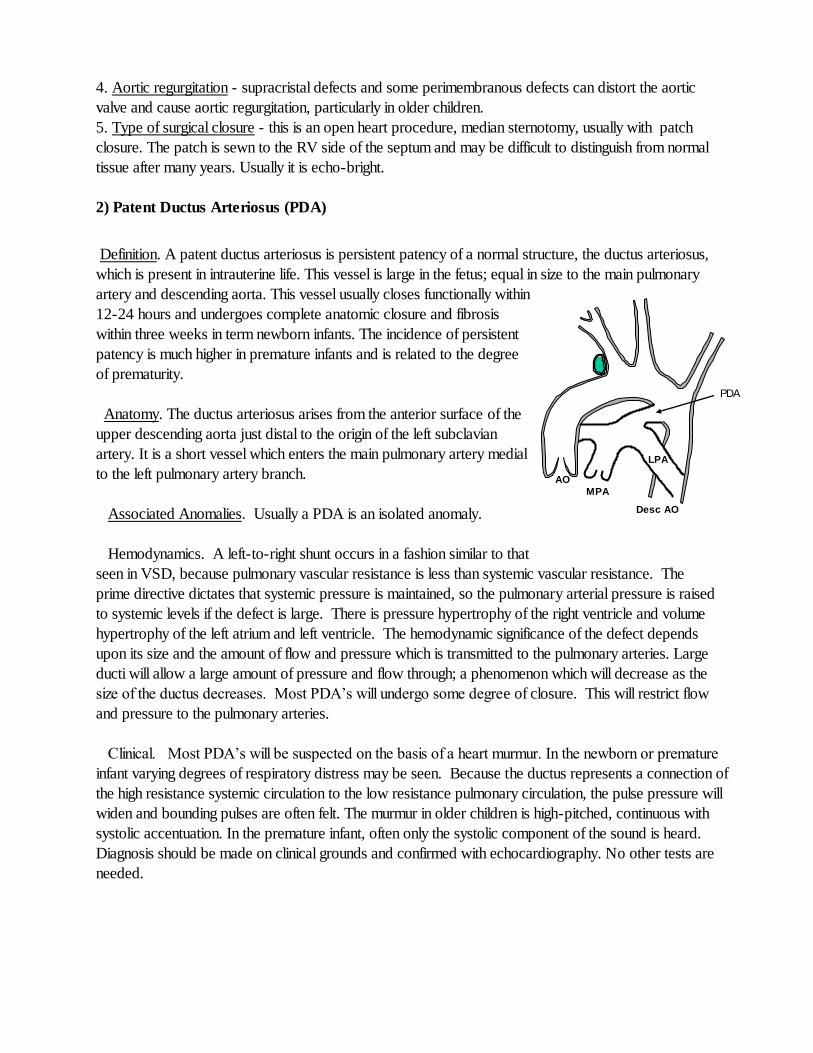
2) Patent Ductus Arteriosus (PDA) Definition. A patent ductus arteriosus is persistent patency of a normal structure, the ductus arteriosus,
which is present in intrauterine life. This vessel is large in the fetus; equal in size to the main pulmonary
artery and descending aorta. This vessel usually closes functionally within
12-24 hours and undergoes complete anatomic closure and fibrosis
within three weeks in term newborn infants. The incidence of persistent
patency is much higher in premature infants and is related to the degree
of prematurity.
Anatomy. The ductus arteriosus arises from the anterior surface of the
upper descending aorta just distal to the origin of the left subclavian
artery. It is a short vessel which enters the main pulmonary artery medial
to the left pulmonary artery branch.
Associated Anomalies. Usually a PDA is an isolated anomaly.
Hemodynamics. A left-to-right shunt occurs in a fashion similar to that
seen in VSD, because pulmonary vascular resistance is less than systemic vascular resistance. The
prime directive dictates that systemic pressure is maintained, so the pulmonary arterial pressure is raised
to systemic levels if the defect is large. There is pressure hypertrophy of the right ventricle and volume
hypertrophy of the left atrium and left ventricle. The hemodynamic significance of the defect depends
upon its size and the amount of flow and pressure which is transmitted to the pulmonary arteries. Large
ducti will allow a large amount of pressure and flow through; a phenomenon which will decrease as the
size of the ductus decreases. Most PDA’s will undergo some degree of closure. This will restrict flow
and pressure to the pulmonary arteries.
Clinical. Most PDA’s will be suspected on the basis of a heart murmur. In the newborn or premature
infant varying degrees of respiratory distress may be seen. Because the ductus represents a connection of
the high resistance systemic circulation to the low resistance pulmonary circulation, the pulse pressure will
widen and bounding pulses are often felt. The murmur in older children is high-pitched, continuous with
systolic accentuation. In the premature infant, often only the systolic component of the sound is heard.
Diagnosis should be made on clinical grounds and confirmed with echocardiography. No other tests are
needed.
PDA
AO
MPA
LPA
Desc AO
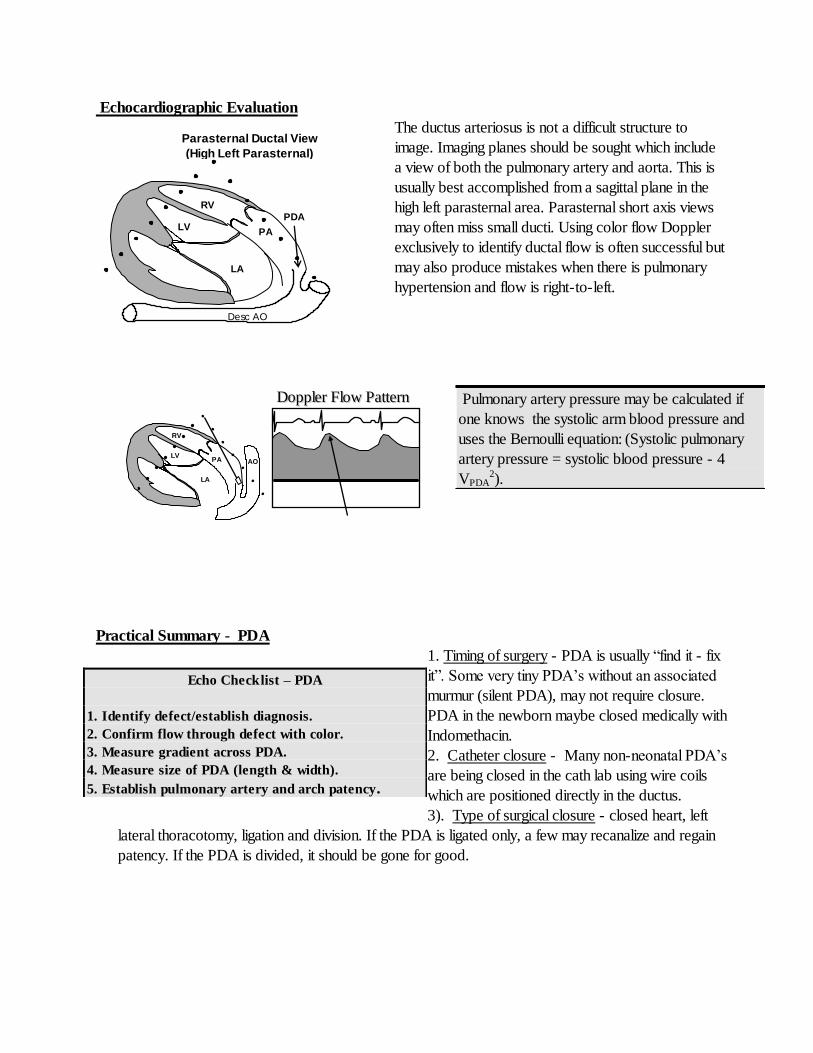
Echocardiographic Evaluation
The ductus arteriosus is not a difficult structure to
image. Imaging planes should be sought which include
a view of both the pulmonary artery and aorta. This is
usually best accomplished from a sagittal plane in the
high left parasternal area. Parasternal short axis views
may often miss small ducti. Using color flow Doppler
exclusively to identify ductal flow is often successful but
may also produce mistakes when there is pulmonary
hypertension and flow is right-to-left.
Practical Summary - PDA
1. Timing of surgery - PDA is usually “find it - fix
it”. Some very tiny PDA’s without an associated
murmur (silent PDA), may not require closure.
PDA in the newborn maybe closed medically with
Indomethacin.
2. Catheter closure - Many non-neonatal PDA’s
are being closed in the cath lab using wire coils
which are positioned directly in the ductus.
3). Type of surgical closure - closed heart, left
lateral thoracotomy, ligation and division. If the PDA is ligated only, a few may recanalize and regain
patency. If the PDA is divided, it should be gone for good.
Pulmonary artery pressure may be calculated if
one knows the systolic arm blood pressure and
uses the Bernoulli equation: (Systolic pulmonary
artery pressure = systolic blood pressure - 4
VPDA2).
Echo Checklist – PDA
1. Identify defect/establish diagnosis.
2. Confirm flow through defect with color.
3. Measure gradient across PDA.
4. Measure size of PDA (length & width).
5. Establish pulmonary artery and arch patency.
PA
LA
LV
RV
Desc AO
PDA
Parasternal Ductal View
(High Left Parasternal)
LV
RV
DDoopppplleerr FFllooww PPaatttteerrnn
PA
LA
AO
IVC
SVC
RV
MPA
1
1 SECUNDUM
2
2 PRIMUM 3
3 SINUS VENOSUS
4
4 CORONARY SINUS
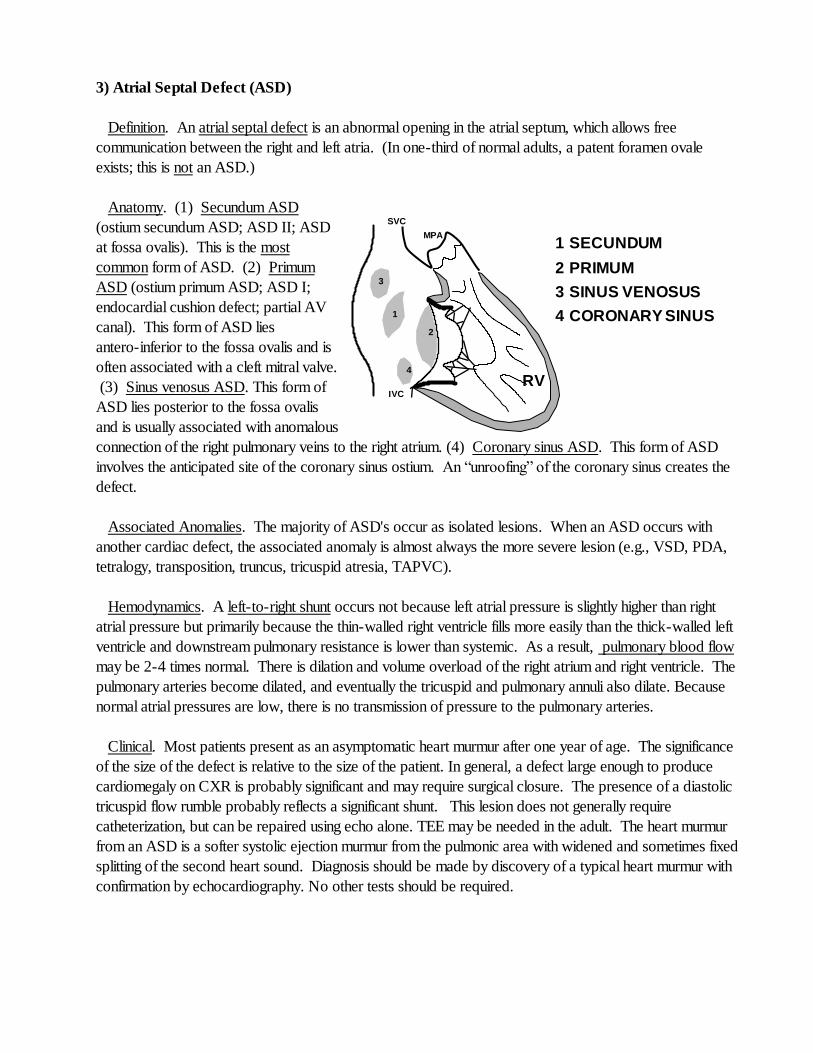
3) Atrial Septal Defect (ASD)
Definition. An atrial septal defect is an abnormal opening in the atrial septum, which allows free
communication between the right and left atria. (In one-third of normal adults, a patent foramen ovale
exists; this is not an ASD.)
Anatomy. (1) Secundum ASD
(ostium secundum ASD; ASD II; ASD
at fossa ovalis). This is the most
common form of ASD. (2) Primum
ASD (ostium primum ASD; ASD I;
endocardial cushion defect; partial AV
canal). This form of ASD lies
antero-inferior to the fossa ovalis and is
often associated with a cleft mitral valve.
(3) Sinus venosus ASD. This form of
ASD lies posterior to the fossa ovalis
and is usually associated with anomalous
connection of the right pulmonary veins to the right atrium. (4) Coronary sinus ASD. This form of ASD
involves the anticipated site of the coronary sinus ostium. An “unroofing” of the coronary sinus creates the
defect.
Associated Anomalies. The majority of ASD's occur as isolated lesions. When an ASD occurs with
another cardiac defect, the associated anomaly is almost always the more severe lesion (e.g., VSD, PDA,
tetralogy, transposition, truncus, tricuspid atresia, TAPVC).
Hemodynamics. A left-to-right shunt occurs not because left atrial pressure is slightly higher than right
atrial pressure but primarily because the thin-walled right ventricle fills more easily than the thick-walled left
ventricle and downstream pulmonary resistance is lower than systemic. As a result, pulmonary blood flow
may be 2-4 times normal. There is dilation and volume overload of the right atrium and right ventricle. The
pulmonary arteries become dilated, and eventually the tricuspid and pulmonary annuli also dilate. Because
normal atrial pressures are low, there is no transmission of pressure to the pulmonary arteries.
Clinical. Most patients present as an asymptomatic heart murmur after one year of age. The significance
of the size of the defect is relative to the size of the patient. In general, a defect large enough to produce
cardiomegaly on CXR is probably significant and may require surgical closure. The presence of a diastolic
tricuspid flow rumble probably reflects a significant shunt. This lesion does not generally require
catheterization, but can be repaired using echo alone. TEE may be needed in the adult. The heart murmur
from an ASD is a softer systolic ejection murmur from the pulmonic area with widened and sometimes fixed
splitting of the second heart sound. Diagnosis should be made by discovery of a typical heart murmur with
confirmation by echocardiography. No other tests should be required.
SSuubbccooss tt aall FFoouurr--CChhaammbbeerr VViieeww
LA
RA LV
RV
SV ASD Sec. ASD
Primum ASD
SSuubbccooss tt aall CCaavvaall VViieeww
RA
LA
IVC
SVC
RV
Sinus Venosus ASD
Secundum ASD
PPaarraass tt eerrnnaall SShhoorrtt AAxxiiss -- BBaassee
Secundum (and primum)
ASD's may be seen from
this view if the angle
is right
RV
RA
LA
MP
A
AV
Dilated RV
AApp iiccaall FFoouurr--CChhaammbbeerr VViieeww
RA LA
RV
LV
Secundum ASD
Primum ASD
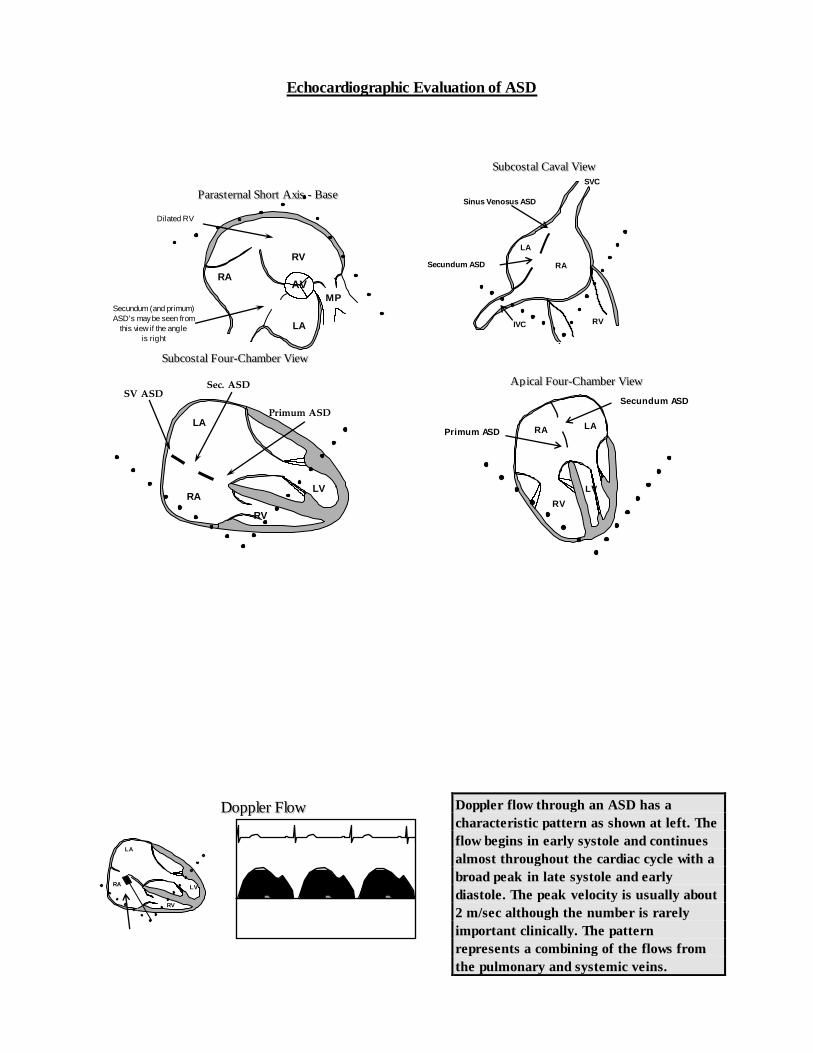
Echocardiographic Evaluation of ASD
Doppler flow through an ASD has a
characteristic pattern as shown at left. The
flow begins in early systole and continues
almost throughout the cardiac cycle with a
broad peak in late systole and early
diastole. The peak velocity is usually about
2 m/sec although the number is rarely
important clinically. The pattern
represents a combining of the flows from
the pulmonary and systemic veins.
DDoopppplleerr FFllooww
LA
RA LV
RV
Practical Summary - ASD
1. Timing of surgery - usually after age 2 years,
unless symptoms are present.
2. RV dilation - a significant ASD will generally
produce RV dilation, a general indicator of the need to
close the defect.
3. Non-surgical options - expect to see more
device closures of secundum defects in the future.
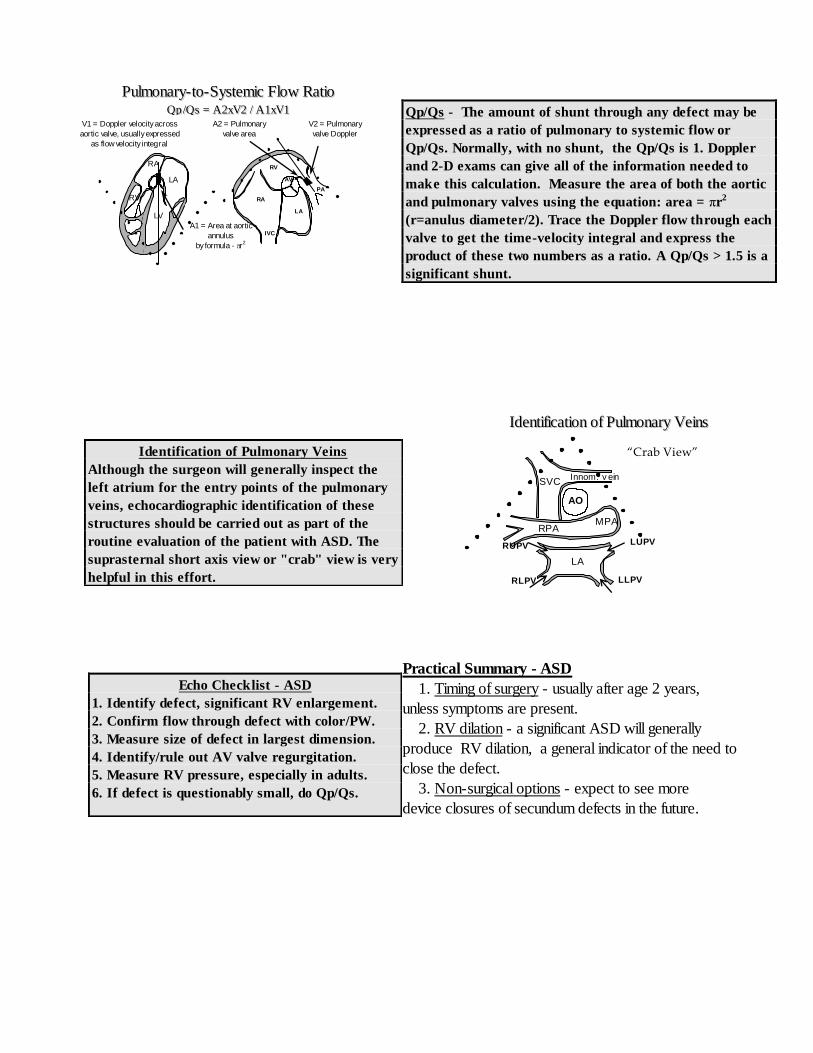
Qp/Qs - The amount of shunt through any defect may be
expressed as a ratio of pulmonary to systemic flow or
Qp/Qs. Normally, with no shunt, the Qp/Qs is 1. Doppler
and 2-D exams can give all of the information needed to
make this calculation. Measure the area of both the aortic
and pulmonary valves using the equation: area = πr2
(r=anulus diameter/2). Trace the Doppler flow through each
valve to get the time-velocity integral and express the
product of these two numbers as a ratio. A Qp/Qs > 1.5 is a
significant shunt.
Echo Checklist - ASD
1. Identify defect, significant RV enlargement.
2. Confirm flow through defect with color/PW.
3. Measure size of defect in largest dimension.
4. Identify/rule out AV valve regurgitation.
5. Measure RV pressure, especially in adults.
6. If defect is questionably small, do Qp/Qs.
Identification of Pulmonary Veins
Although the surgeon will generally inspect the
left atrium for the entry points of the pulmonary
veins, echocardiographic identification of these
structures should be carried out as part of the
routine evaluation of the patient with ASD. The
suprasternal short axis view or "crab" view is very
helpful in this effort.
PPuullmmoonnaarryy-- ttoo--SSyysstteemmiicc FFllooww RRaattiioo
QQpp //QQss == AA22xxVV22 // AA11xxVV11
RV
LA
RA
IVC
PA
AV
V2 = Pulmonary
valve Doppler
A2 = Pulmonary
valve area
A1 = Area at aortic
annulus
by formula - r2
RA
LV
RV
LA
V1 = Doppler velocity across
aortic valve, usually expressed
as flow velocity integral
LA
SVC
RPA
AO
MPA
Innom. v ein
LUPV
LLPV
RUPV
RLPV
IIddeennttiiffiiccaattiioonn ooff PPuullmmoonnaarryy VVeeiinnss
“Crab View”
4) Tetralogy of Fallot (TOF)
Definition/Anatomy. Tetralogy of Fallot is classically defined as: 1) right ventricular hypertrophy 2)
ventricular septal defect 3) overriding aorta 4) pulmonary stenosis, but is actually a spectrum of defects
probably resulting from abnormal conotruncal septation. This leads to anterior deviation of the infundibular
septum which in turn "crowds" the right ventricular outflow tract leading to sub-pulmonary stenosis or atresia.
The anterior deviation of the infundibular septum also is responsible for the malalignment ventricular septal
defect and dextroposition of the aorta. Tetralogy occurs in approximately 9% of children born with congenital
heart defects.
Associated Anomalies. In addition to the “tetrad” the following anomalies may co-exist: Valvular pulmonary
stenosis (50-60%), Right aortic arch (25%) - usually mirror image branching, Atrial septal defect (15%),
Coronary anomalies (esp. LAD from right coronary 5%) Additional muscular VSD (2%), Unilateral absent
pulmonary artery (rare).
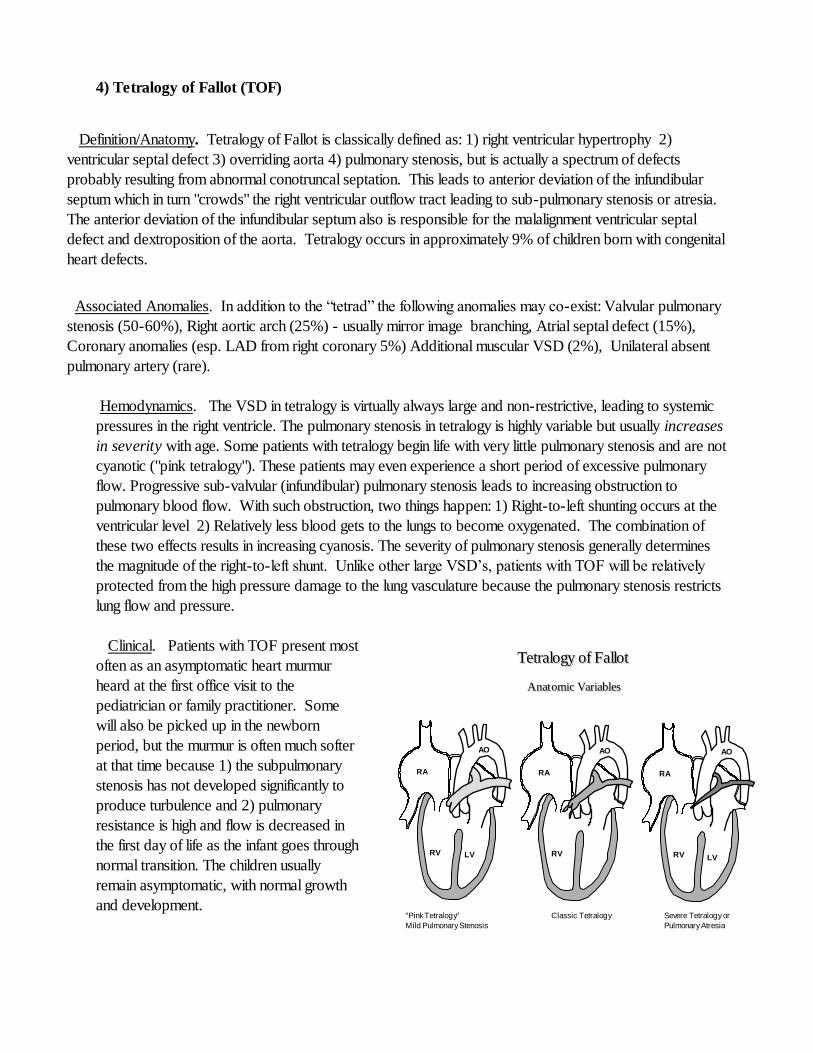
Hemodynamics. The VSD in tetralogy is virtually always large and non-restrictive, leading to systemic
pressures in the right ventricle. The pulmonary stenosis in tetralogy is highly variable but usually increases
in severity with age. Some patients with tetralogy begin life with very little pulmonary stenosis and are not
cyanotic ("pink tetralogy"). These patients may even experience a short period of excessive pulmonary
flow. Progressive sub-valvular (infundibular) pulmonary stenosis leads to increasing obstruction to
pulmonary blood flow. With such obstruction, two things happen: 1) Right-to-left shunting occurs at the
ventricular level 2) Relatively less blood gets to the lungs to become oxygenated. The combination of
these two effects results in increasing cyanosis. The severity of pulmonary stenosis generally determines
the magnitude of the right-to-left shunt. Unlike other large VSD’s, patients with TOF will be relatively
protected from the high pressure damage to the lung vasculature because the pulmonary stenosis restricts
lung flow and pressure.
Clinical. Patients with TOF present most
often as an asymptomatic heart murmur
heard at the first office visit to the
pediatrician or family practitioner. Some
will also be picked up in the newborn
period, but the murmur is often much softer
at that time because 1) the subpulmonary
stenosis has not developed significantly to
produce turbulence and 2) pulmonary
resistance is high and flow is decreased in
the first day of life as the infant goes through
normal transition. The children usually
remain asymptomatic, with normal growth
and development.
RA
RV LV
AO
RA
RV
LV
AO
RA
RV LV
AO
"Pink Tetralogy"
Mild Pulmonary Stenosis
Classic Tetralogy Severe Tetralogy or
Pulmonary Atresia
AAnnaatt oommiicc VVaarriiaabblleess
TTeettrraallooggyy ooff FFaalllloott
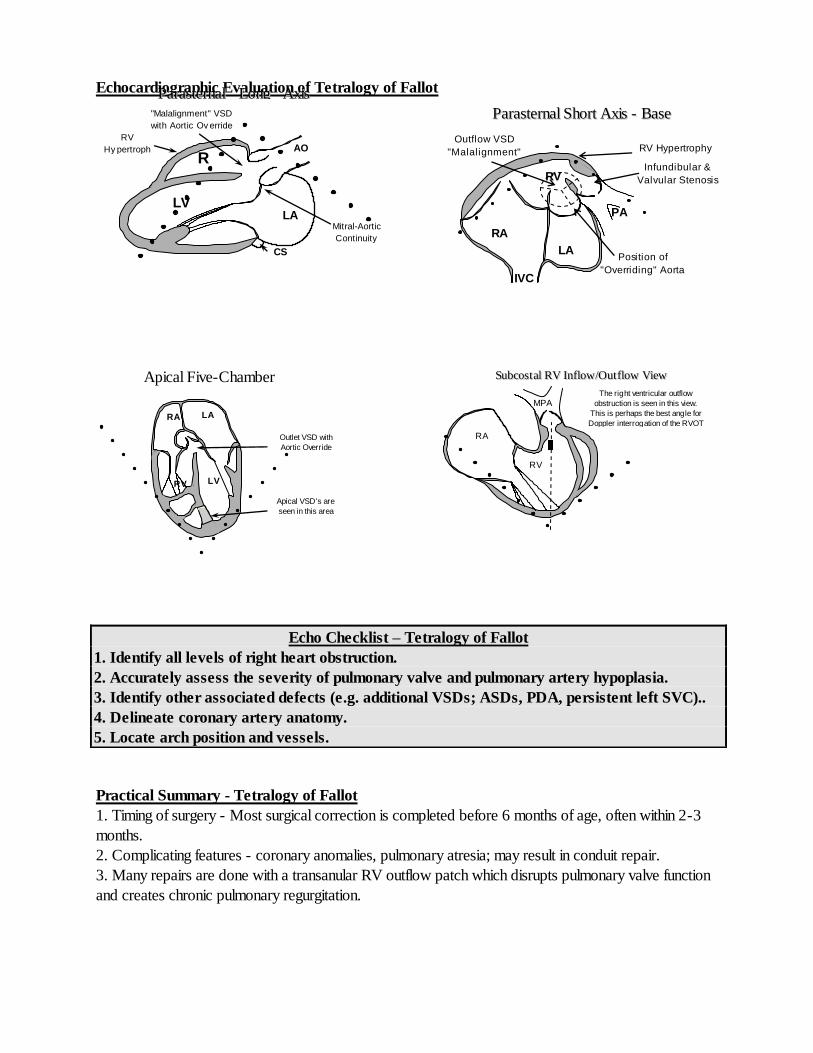
Echocardiographic Evaluation of Tetralogy of Fallot
Practical Summary - Tetralogy of Fallot
1. Timing of surgery - Most surgical correction is completed before 6 months of age, often within 2-3
months.
2. Complicating features - coronary anomalies, pulmonary atresia; may result in conduit repair.
3. Many repairs are done with a transanular RV outflow patch which disrupts pulmonary valve function
and creates chronic pulmonary regurgitation.
Echo Checklist – Tetralogy of Fallot
1. Identify all levels of right heart obstruction.
2. Accurately assess the severity of pulmonary valve and pulmonary artery hypoplasia.
3. Identify other associated defects (e.g. additional VSDs; ASDs, PDA, persistent left SVC)..
4. Delineate coronary artery anatomy.
5. Locate arch position and vessels.
PPaarraasstteerrnnaall LLoonngg AAxxiiss
VViieeww
LV LA
AO
CS
R
V
"Malalignment" VSD
with Aortic Ov erride
Mitral-Aortic
Continuity
RV
Hy pertroph
y
PPaarraasstteerrnnaall SShhoorrtt AAxxiiss -- BBaassee
RV
LA
RA
IVC
PA
Outflow VSD
"Malalignment"
type
RV Hypertrophy
Infundibular &
Valvular Stenosis
Position of
"Overriding" Aorta
Apical Five-Chamber
LA
LV RV
RA
Outlet VSD with
Aortic Override
Apical VSD's are
seen in this area
SSuubbccooss tt aall RRVV IInnffllooww//OOuutt ffllooww VViieeww
RA
RV
MPA The right ventricular outflow
obstruction is seen in this view.
This is perhaps the best angle for
Doppler interrogation of the RVOT

5) Pulmonary Valve Stenosis
Definition. Pulmonary stenosis refers to obstruction in the region of either the pulmonary valve or the
subpulmonary ventricular outflow tract.
Associated Anomalies. Most pulmonary valve stenoses are isolated lesions, but a few may be
associated with a patent ductus arteriosus or aortic coarctation. Bicuspid or unicommissural pulmonary
valves may be associated with subpulmonary stenosis in tetralogy or transposition or may rarely coexist
with a ventricular septal defect or bicuspid aortic valve.
Hemodynamics. Due to pulmonary valvular obstruction, there is pressure hypertrophy of the right
ventricle and post-stenotic dilatation of the pulmonary trunk. If subpulmonary stenosis is present (as in
tetralogy), the pulmonary trunk usually is not dilated; the stenotic subpulmonary channel offers resistance
to blood flow so that the high right ventricular pressure is not fully transmitted to the pulmonary valve
and, as a result, no high pressure jet is forced across the valve and against the wall of the pulmonary
trunk.
Clinical. Pulmonary valve stenosis usually presents as an asymptomatic systolic murmur heard best at
the upper left sternal border. Even severe PS in older children rarely produces symptoms. Critical PS
in the newborn may present as cyanosis and/or shock after the ductus arteriosus closes. Mild
pulmonary stenosis found in the infant may become progressively worse with time, but may also get
better and even resolve over several years. The process which occurs to accomplish this “cure” is not
understood.
Practical Summary - Pulmonary
Stenosis
1. Timing of intervention - gradients of >40-50 mm Hg.
Balloon valvuloplasty is the procedure of first choice.
2. Secondary infundibular or supravalvular stenosis may
be present.
Echo Checklist – Pulmonary Stenosis
1. The size of the annulus - is it normal or hypoplastic?
2. The thickness of the valve leaflets - how dysplastic are they?
3. The leaflet excursion - how well does the valve open; do the
leaflets "dome?"
4. The main pulmonary artery - is it hypoplastic? Is there post
stenotic dilatation?
5. The subvalvular area - is there hypertrophy of the
infundibulum and subvalvular stenosis?
6. Is a patent ductus arteriosus present?
PPuullmmoonnaarryy SStteennoossiiss
RV
LA
RA
IVC
PA
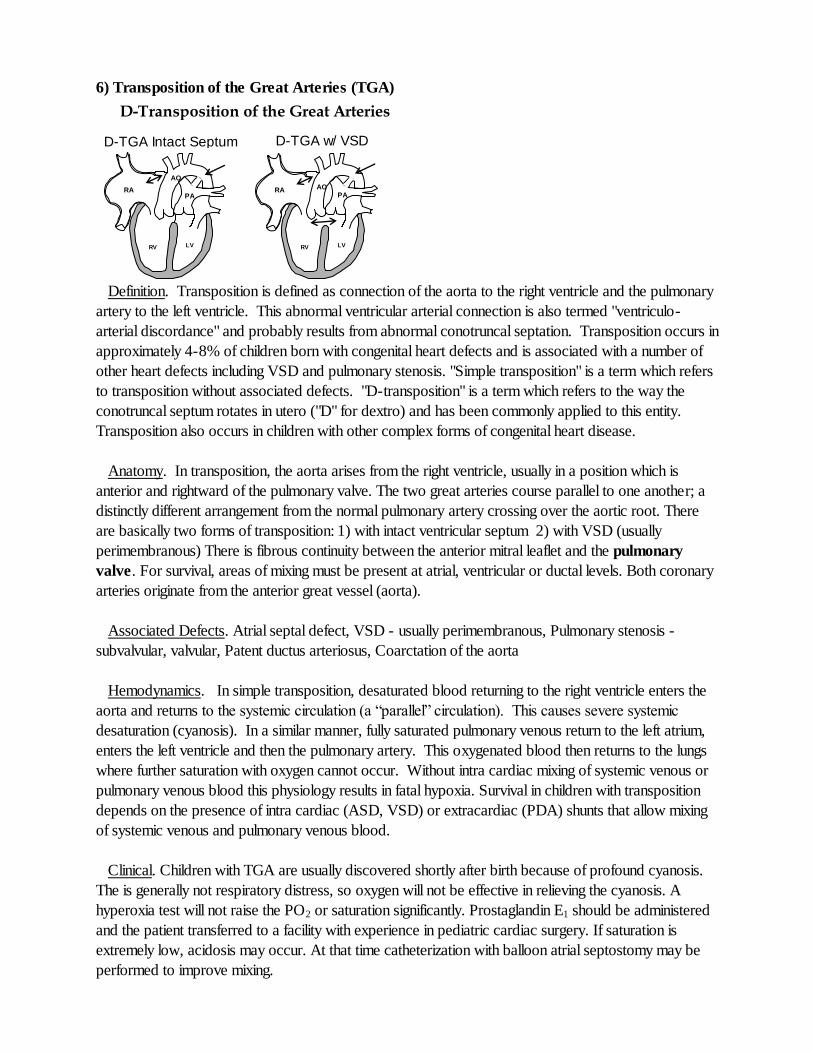
6) Transposition of the Great Arteries (TGA)
Definition. Transposition is defined as connection of the aorta to the right ventricle and the pulmonary
artery to the left ventricle. This abnormal ventricular arterial connection is also termed "ventriculo-
arterial discordance" and probably results from abnormal conotruncal septation. Transposition occurs in
approximately 4-8% of children born with congenital heart defects and is associated with a number of
other heart defects including VSD and pulmonary stenosis. "Simple transposition" is a term which refers
to transposition without associated defects. "D-transposition" is a term which refers to the way the
conotruncal septum rotates in utero ("D" for dextro) and has been commonly applied to this entity.
Transposition also occurs in children with other complex forms of congenital heart disease.
Anatomy. In transposition, the aorta arises from the right ventricle, usually in a position which is
anterior and rightward of the pulmonary valve. The two great arteries course parallel to one another; a
distinctly different arrangement from the normal pulmonary artery crossing over the aortic root. There
are basically two forms of transposition: 1) with intact ventricular septum 2) with VSD (usually
perimembranous) There is fibrous continuity between the anterior mitral leaflet and the pulmonary
valve. For survival, areas of mixing must be present at atrial, ventricular or ductal levels. Both coronary
arteries originate from the anterior great vessel (aorta).
Associated Defects. Atrial septal defect, VSD - usually perimembranous, Pulmonary stenosis -
subvalvular, valvular, Patent ductus arteriosus, Coarctation of the aorta
Hemodynamics. In simple transposition, desaturated blood returning to the right ventricle enters the
aorta and returns to the systemic circulation (a “parallel” circulation). This causes severe systemic
desaturation (cyanosis). In a similar manner, fully saturated pulmonary venous return to the left atrium,
enters the left ventricle and then the pulmonary artery. This oxygenated blood then returns to the lungs
where further saturation with oxygen cannot occur. Without intra cardiac mixing of systemic venous or
pulmonary venous blood this physiology results in fatal hypoxia. Survival in children with transposition
depends on the presence of intra cardiac (ASD, VSD) or extracardiac (PDA) shunts that allow mixing
of systemic venous and pulmonary venous blood.
Clinical. Children with TGA are usually discovered shortly after birth because of profound cyanosis.
The is generally not respiratory distress, so oxygen will not be effective in relieving the cyanosis. A
hyperoxia test will not raise the PO2 or saturation significantly. Prostaglandin E1 should be administered
and the patient transferred to a facility with experience in pediatric cardiac surgery. If saturation is
extremely low, acidosis may occur. At that time catheterization with balloon atrial septostomy may be
performed to improve mixing.
D-Transposition of the Great Arteries
D-TGA Intact Septum D-TGA w/ VSD
RV LV
RA AO PA
RV LV
RA
AO
PA
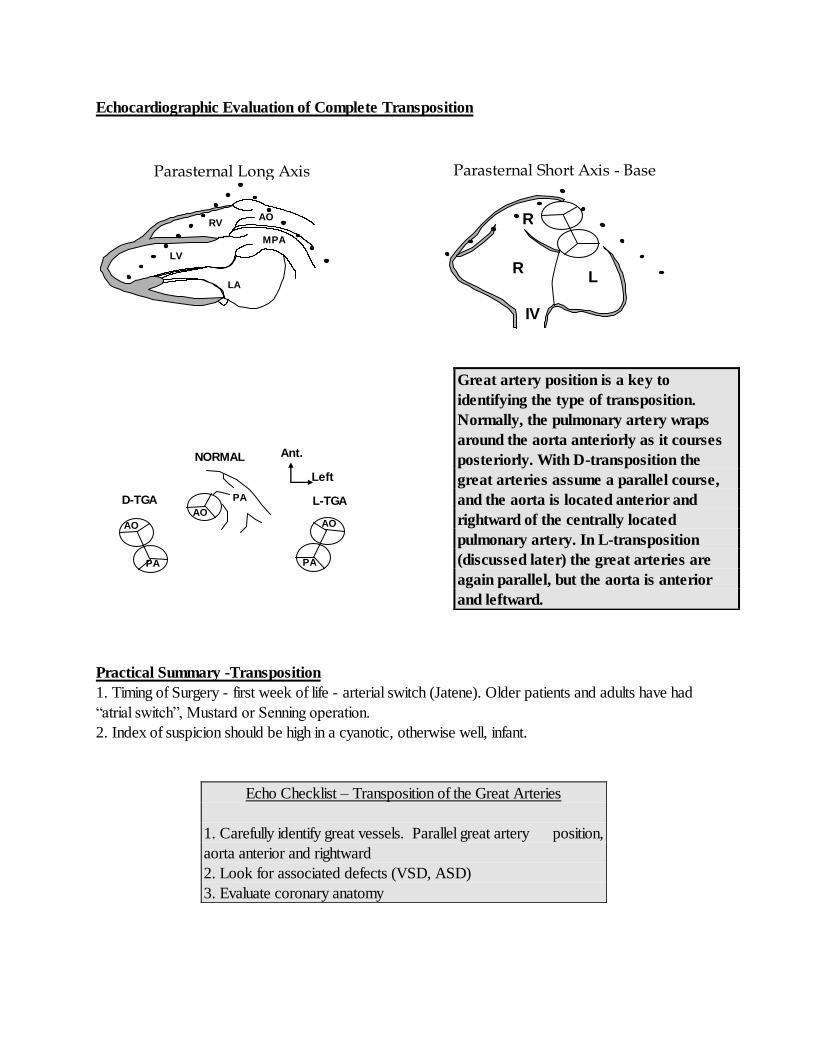
Echocardiographic Evaluation of Complete Transposition
Practical Summary -Transposition
1. Timing of Surgery - first week of life - arterial switch (Jatene). Older patients and adults have had
“atrial switch”, Mustard or Senning operation.
2. Index of suspicion should be high in a cyanotic, otherwise well, infant.
Great artery position is a key to
identifying the type of transposition.
Normally, the pulmonary artery wraps
around the aorta anteriorly as it courses
posteriorly. With D-transposition the
great arteries assume a parallel course,
and the aorta is located anterior and
rightward of the centrally located
pulmonary artery. In L-transposition
(discussed later) the great arteries are
again parallel, but the aorta is anterior
and leftward.
Echo Checklist – Transposition of the Great Arteries
1. Carefully identify great vessels. Parallel great artery position,
aorta anterior and rightward
2. Look for associated defects (VSD, ASD)
3. Evaluate coronary anatomy
Parasternal Long Axis View
LA
LV
RV
MPA
AO
Parasternal Short Axis - Base
R
V
L
A
R
A
IV
C
AO
PA
AO
PA
AO
PA L-TGA
NORMAL
D-TGA
Ant.
Left
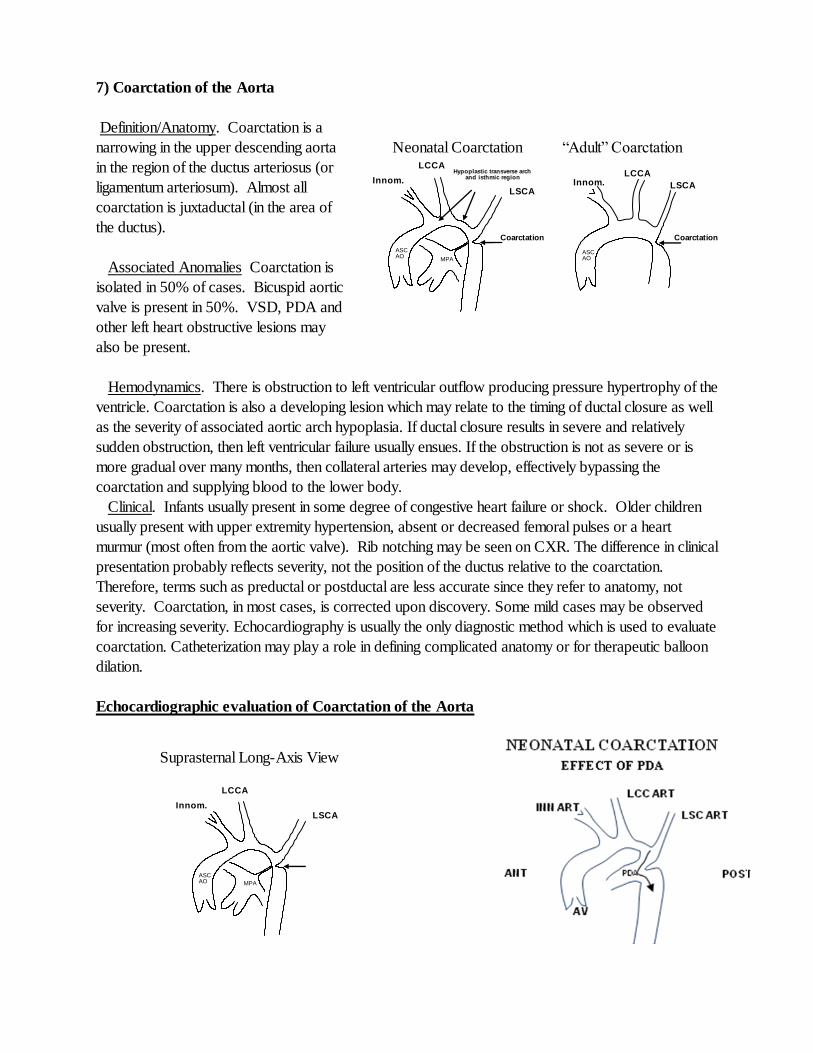
7) Coarctation of the Aorta
Definition/Anatomy. Coarctation is a
narrowing in the upper descending aorta
in the region of the ductus arteriosus (or
ligamentum arteriosum). Almost all
coarctation is juxtaductal (in the area of
the ductus).
Associated Anomalies Coarctation is
isolated in 50% of cases. Bicuspid aortic
valve is present in 50%. VSD, PDA and
other left heart obstructive lesions may
also be present.
Hemodynamics. There is obstruction to left ventricular outflow producing pressure hypertrophy of the
ventricle. Coarctation is also a developing lesion which may relate to the timing of ductal closure as well
as the severity of associated aortic arch hypoplasia. If ductal closure results in severe and relatively
sudden obstruction, then left ventricular failure usually ensues. If the obstruction is not as severe or is
more gradual over many months, then collateral arteries may develop, effectively bypassing the
coarctation and supplying blood to the lower body.
Clinical. Infants usually present in some degree of congestive heart failure or shock. Older children
usually present with upper extremity hypertension, absent or decreased femoral pulses or a heart
murmur (most often from the aortic valve). Rib notching may be seen on CXR. The difference in clinical
presentation probably reflects severity, not the position of the ductus relative to the coarctation.
Therefore, terms such as preductal or postductal are less accurate since they refer to anatomy, not
severity. Coarctation, in most cases, is corrected upon discovery. Some mild cases may be observed
for increasing severity. Echocardiography is usually the only diagnostic method which is used to evaluate
coarctation. Catheterization may play a role in defining complicated anatomy or for therapeutic balloon
dilation.
Echocardiographic evaluation of Coarctation of the Aorta
Innom.
Art. LSCA
ASC AO
MPA
Coarctation
Hypoplastic transverse arch and isthmic region
LCCA
Neonatal Coarctation “Adult” Coarctation
Coarctation
ASC AO
LSCA
LCCA Innom.
Art.
Innom.
Art. LSCA
ASC AO MPA
LCCA
Suprasternal Long-Axis View
NEONATAL COARCTATION
EFFECT OF PDA
ANT POST
AV
INN ART LSC ART
LCC ART
PDA
Practical Summary - Coarctation of the Aorta
1. Timing of Surgery - usually at time of diagnosis regardless of age.
2. Gradient may be low despite severe obstruction due to collateral flow.
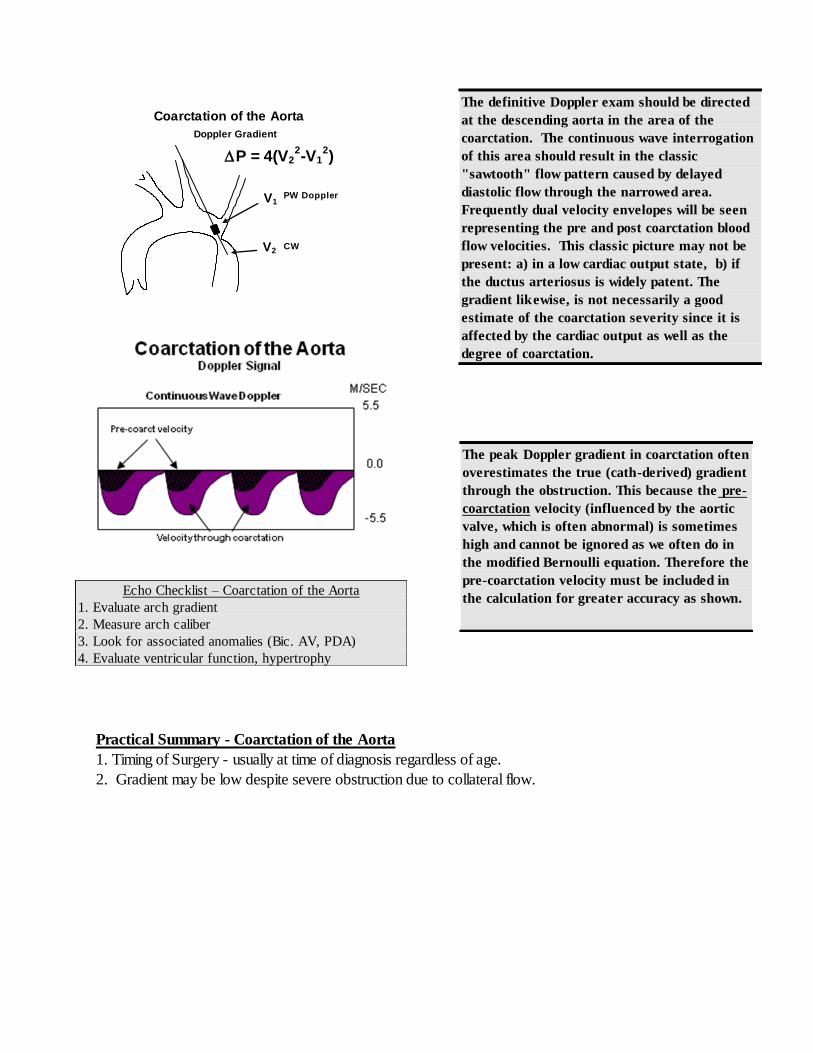
The definitive Doppler exam should be directed
at the descending aorta in the area of the
coarctation. The continuous wave interrogation
of this area should result in the classic
"sawtooth" flow pattern caused by delayed
diastolic flow through the narrowed area.
Frequently dual velocity envelopes will be seen
representing the pre and post coarctation blood
flow velocities. This classic picture may not be
present: a) in a low cardiac output state, b) if
the ductus arteriosus is widely patent. The
gradient likewise, is not necessarily a good
estimate of the coarctation severity since it is
affected by the cardiac output as well as the
degree of coarctation.
The peak Doppler gradient in coarctation often
overestimates the true (cath-derived) gradient
through the obstruction. This because the pre-
coarctation velocity (influenced by the aortic
valve, which is often abnormal) is sometimes
high and cannot be ignored as we often do in
the modified Bernoulli equation. Therefore the
pre-coarctation velocity must be included in
the calculation for greater accuracy as shown. Echo Checklist – Coarctation of the Aorta
1. Evaluate arch gradient
2. Measure arch caliber
3. Look for associated anomalies (Bic. AV, PDA)
4. Evaluate ventricular function, hypertrophy
Coarctation of the Aorta
PW Doppler
CW
Doppler
V1
V2
P = 4(V22-V1
2)
Doppler Gradient
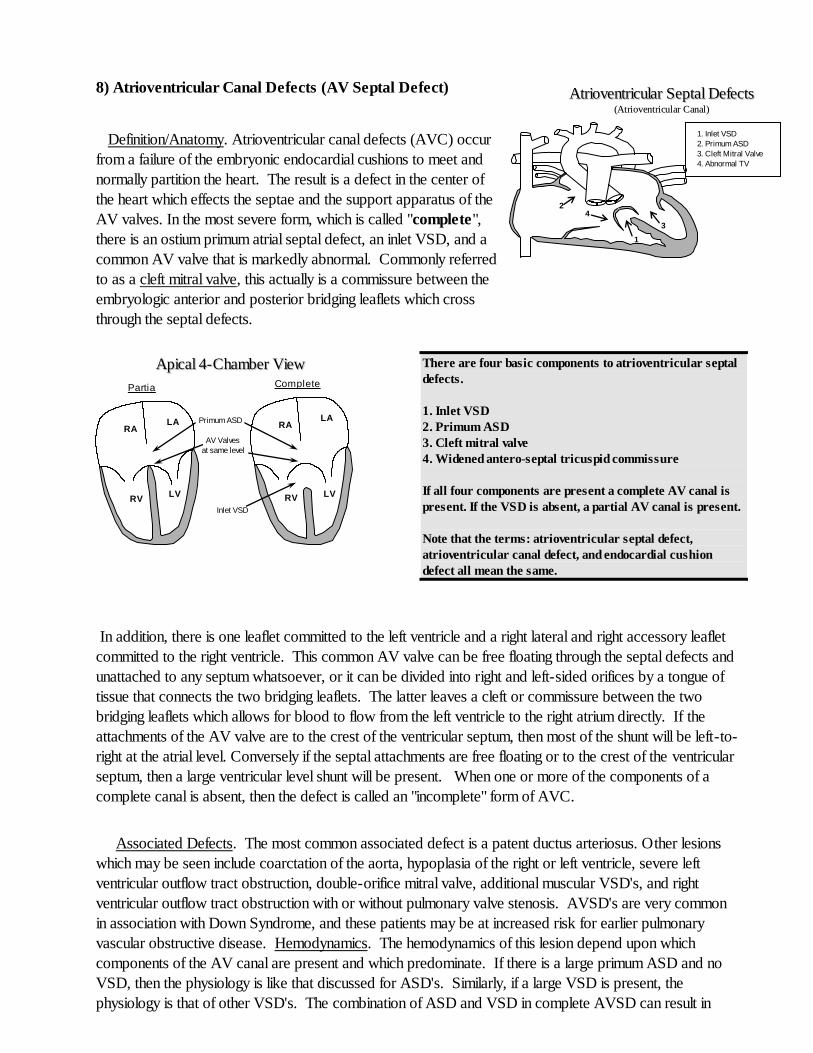
8) Atrioventricular Canal Defects (AV Septal Defect) Definition/Anatomy. Atrioventricular canal defects (AVC) occur
from a failure of the embryonic endocardial cushions to meet and
normally partition the heart. The result is a defect in the center of
the heart which effects the septae and the support apparatus of the
AV valves. In the most severe form, which is called "complete",
there is an ostium primum atrial septal defect, an inlet VSD, and a
common AV valve that is markedly abnormal. Commonly referred
to as a cleft mitral valve, this actually is a commissure between the
embryologic anterior and posterior bridging leaflets which cross
through the septal defects.
In addition, there is one leaflet committed to the left ventricle and a right lateral and right accessory leaflet
committed to the right ventricle. This common AV valve can be free floating through the septal defects and
unattached to any septum whatsoever, or it can be divided into right and left-sided orifices by a tongue of
tissue that connects the two bridging leaflets. The latter leaves a cleft or commissure between the two
bridging leaflets which allows for blood to flow from the left ventricle to the right atrium directly. If the
attachments of the AV valve are to the crest of the ventricular septum, then most of the shunt will be left-to-
right at the atrial level. Conversely if the septal attachments are free floating or to the crest of the ventricular
septum, then a large ventricular level shunt will be present. When one or more of the components of a
complete canal is absent, then the defect is called an "incomplete" form of AVC.
Associated Defects. The most common associated defect is a patent ductus arteriosus. Other lesions
which may be seen include coarctation of the aorta, hypoplasia of the right or left ventricle, severe left
ventricular outflow tract obstruction, double-orifice mitral valve, additional muscular VSD's, and right
ventricular outflow tract obstruction with or without pulmonary valve stenosis. AVSD's are very common
in association with Down Syndrome, and these patients may be at increased risk for earlier pulmonary
vascular obstructive disease. Hemodynamics. The hemodynamics of this lesion depend upon which
components of the AV canal are present and which predominate. If there is a large primum ASD and no
VSD, then the physiology is like that discussed for ASD's. Similarly, if a large VSD is present, the
physiology is that of other VSD's. The combination of ASD and VSD in complete AVSD can result in
There are four basic components to atrioventricular septal
defects.
1. Inlet VSD
2. Primum ASD
3. Cleft mitral valve
4. Widened antero-septal tricuspid commissure
If all four components are present a complete AV canal is
present. If the VSD is absent, a partial AV canal is present.
Note that the terms: atrioventricular septal defect,
atrioventricular canal defect, and endocardial cushion
defect all mean the same.
AAppiiccaall 44--CChhaammbbeerr VViieeww
RA
RV
LA
LV
RA
RV
LA
LV
Primum ASD
Inlet VSD
Partia
l
Complete
AV Valves
at same level
AAttrriioovveennttrriiccuullaarr SSeeppttaall DDeeffeeccttss
((AAttrriioovveennttrriiccuullaarr CCaannaall))
2
1
1. Inlet VSD
2. Primum ASD
3. Cleft Mitral Valve
4. Abnormal TV
3
4
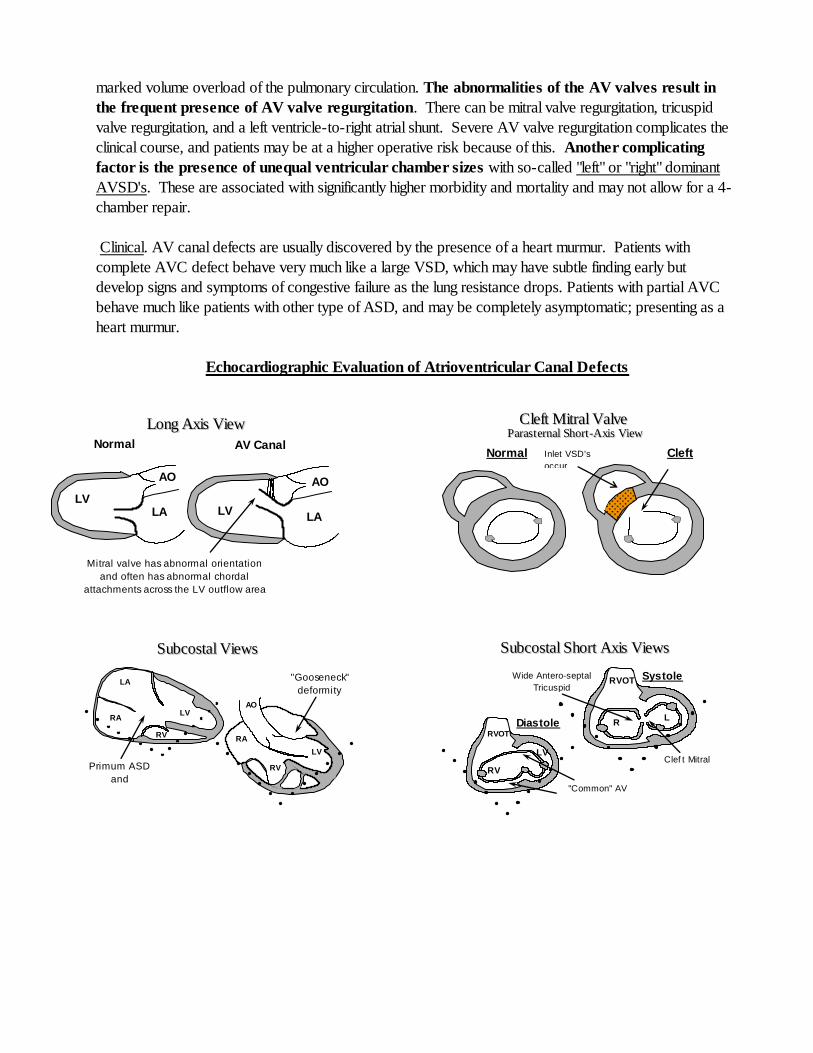
marked volume overload of the pulmonary circulation. The abnormalities of the AV valves result in
the frequent presence of AV valve regurgitation. There can be mitral valve regurgitation, tricuspid
valve regurgitation, and a left ventricle-to-right atrial shunt. Severe AV valve regurgitation complicates the
clinical course, and patients may be at a higher operative risk because of this. Another complicating
factor is the presence of unequal ventricular chamber sizes with so-called "left" or "right" dominant
AVSD's. These are associated with significantly higher morbidity and mortality and may not allow for a 4-
chamber repair.
Clinical. AV canal defects are usually discovered by the presence of a heart murmur. Patients with
complete AVC defect behave very much like a large VSD, which may have subtle finding early but
develop signs and symptoms of congestive failure as the lung resistance drops. Patients with partial AVC
behave much like patients with other type of ASD, and may be completely asymptomatic; presenting as a
heart murmur.
Echocardiographic Evaluation of Atrioventricular Canal Defects
LLoonngg AAxxiiss VViieeww
LV LA
AO
LV LA
AO
Normal AV Canal
Mitral valve has abnormal orientation
and often has abnormal chordal
attachments across the LV outflow area
CClleefftt MMiittrraall VVaallvvee PPaarraass tt eerrnnaall SShhoorrtt --AAxxiiss VViieeww
Normal Cleft Inlet VSD's
occur
in this location
SSuubbccoossttaall SShhoorrtt AAxxiiss VViieewwss
Diastole
Systole
RV
LV
RVOT
R
V
L
V
RVOT
Clef t Mitral
Valv e
Wide Antero-septal
Tricuspid
Commissure
"Common" AV
Valv e
SSuubbccoossttaall VViieewwss
LA
RA LV
RV
LV
RV
RA
AO
"Gooseneck"
deformity
Primum ASD
and
Inlet VSD
Practical summary - AV Canal
1. Timing of surgery - most often done within the first few months of life because the VSD is usually large
and non-restrictive. If the ventricles are unbalanced (one ventricle hypoplastic), a pulmonary band is often
done early followed by a Fontan-type repair.
2.Type of surgical closure - open heart, midline sternotomy, patch closure of defects with often some
repair of the mitral valve cleft. Transesophageal echo is commonly used to evaluate the repair in the
operating room.
9) Aortic Valve Stenosis
The clinical and echocardiographic issues of aortic stenosis in adults and children are approximately the
same, and will not be discussed in detail in this section.
The biggest clinical problem faced by the pediatric cardiologist occurs when a valve replacement is
contemplated for aortic valve disease in a small child. This complicates the situation because of the lack of
small mechanical prostheses and because of the potential for growth (patients would “outgrow”) even a
successful valve replacement.
The current solution to this clinical dilemma is to wait as long as possible, balancing ventricular
performance against gradient and risk. Surgical solutions which are more frequently encountered in
pediatrics are a Konno procedure, where the aortic annulus is enlarged through the ventricular septum and
patched open to accept a larger aortic prosthesis or a Ross procedure, where the patients native
pulmonary valve is excised and placed in the aortic position (the pulmonary valve is replaced by a
homograft prosthesis). In the Ross procedure, the coronary artery origins must be explanted and
reimplanted into the aortic root.
Echo Checklist – Atrioventricular Septal Defects
1. Identify defect/establish diagnosis.
2. Confirm flow through defect with color.
3. Measure gradient across VSD.
4. Measure size of ASD/VSD.
5. AV valve commitment and attachments.
6. Measure relative sizes of ventricles.
7. Measure RV pressure.
8. Evaluate LV outflow tract.
9. Look for associated anomalies.
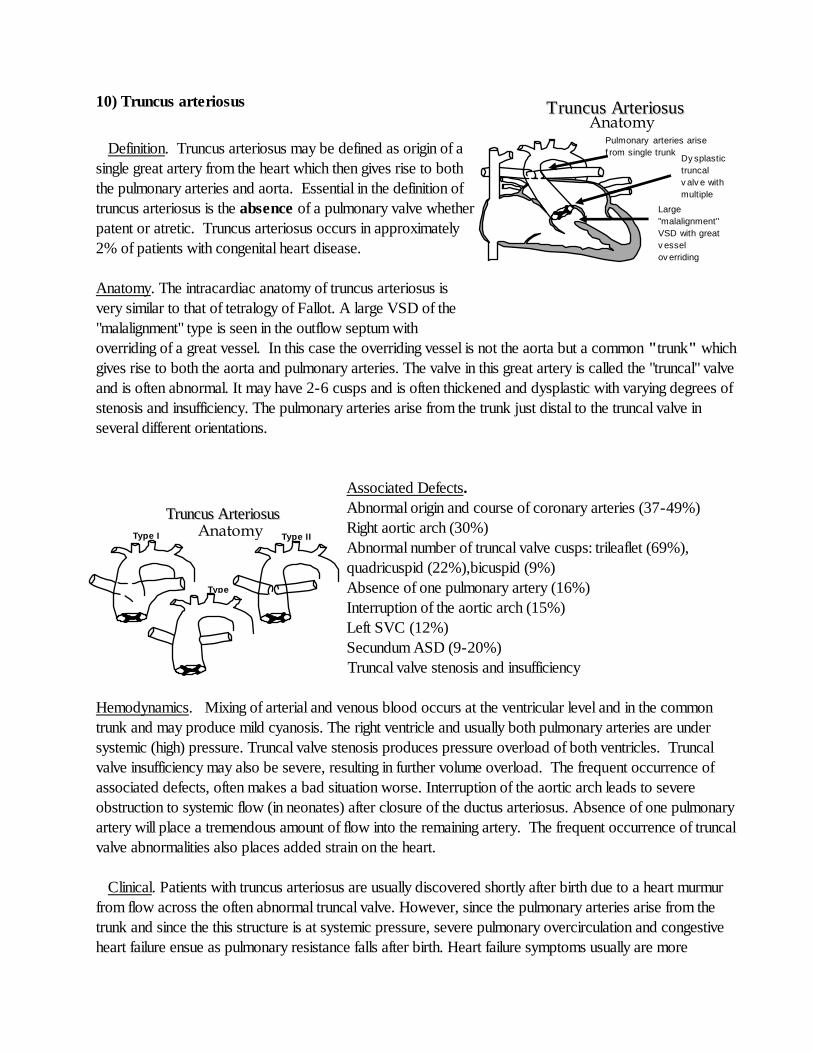
10) Truncus arteriosus
Definition. Truncus arteriosus may be defined as origin of a
single great artery from the heart which then gives rise to both
the pulmonary arteries and aorta. Essential in the definition of
truncus arteriosus is the absence of a pulmonary valve whether
patent or atretic. Truncus arteriosus occurs in approximately
2% of patients with congenital heart disease.
Anatomy. The intracardiac anatomy of truncus arteriosus is
very similar to that of tetralogy of Fallot. A large VSD of the
"malalignment" type is seen in the outflow septum with
overriding of a great vessel. In this case the overriding vessel is not the aorta but a common "trunk" which
gives rise to both the aorta and pulmonary arteries. The valve in this great artery is called the "truncal" valve
and is often abnormal. It may have 2-6 cusps and is often thickened and dysplastic with varying degrees of
stenosis and insufficiency. The pulmonary arteries arise from the trunk just distal to the truncal valve in
several different orientations.
Associated Defects.
Abnormal origin and course of coronary arteries (37-49%)
Right aortic arch (30%)
Abnormal number of truncal valve cusps: trileaflet (69%),
quadricuspid (22%),bicuspid (9%)
Absence of one pulmonary artery (16%)
Interruption of the aortic arch (15%)
Left SVC (12%)
Secundum ASD (9-20%)
Truncal valve stenosis and insufficiency
Hemodynamics. Mixing of arterial and venous blood occurs at the ventricular level and in the common
trunk and may produce mild cyanosis. The right ventricle and usually both pulmonary arteries are under
systemic (high) pressure. Truncal valve stenosis produces pressure overload of both ventricles. Truncal
valve insufficiency may also be severe, resulting in further volume overload. The frequent occurrence of
associated defects, often makes a bad situation worse. Interruption of the aortic arch leads to severe
obstruction to systemic flow (in neonates) after closure of the ductus arteriosus. Absence of one pulmonary
artery will place a tremendous amount of flow into the remaining artery. The frequent occurrence of truncal
valve abnormalities also places added strain on the heart.
Clinical. Patients with truncus arteriosus are usually discovered shortly after birth due to a heart murmur
from flow across the often abnormal truncal valve. However, since the pulmonary arteries arise from the
trunk and since the this structure is at systemic pressure, severe pulmonary overcirculation and congestive
heart failure ensue as pulmonary resistance falls after birth. Heart failure symptoms usually are more
Large
"malalignment"
VSD with great
v essel
ov erriding
Pulmonary arteries arise
f rom single trunk
TTrruunnccuuss AArrtteerriioossuuss Anatomy
Dy splastic
truncal
v alv e with
multiple
cusps
Type I Type II
Type
III
TTrruunnccuuss AArrtteerriioossuuss Anatomy
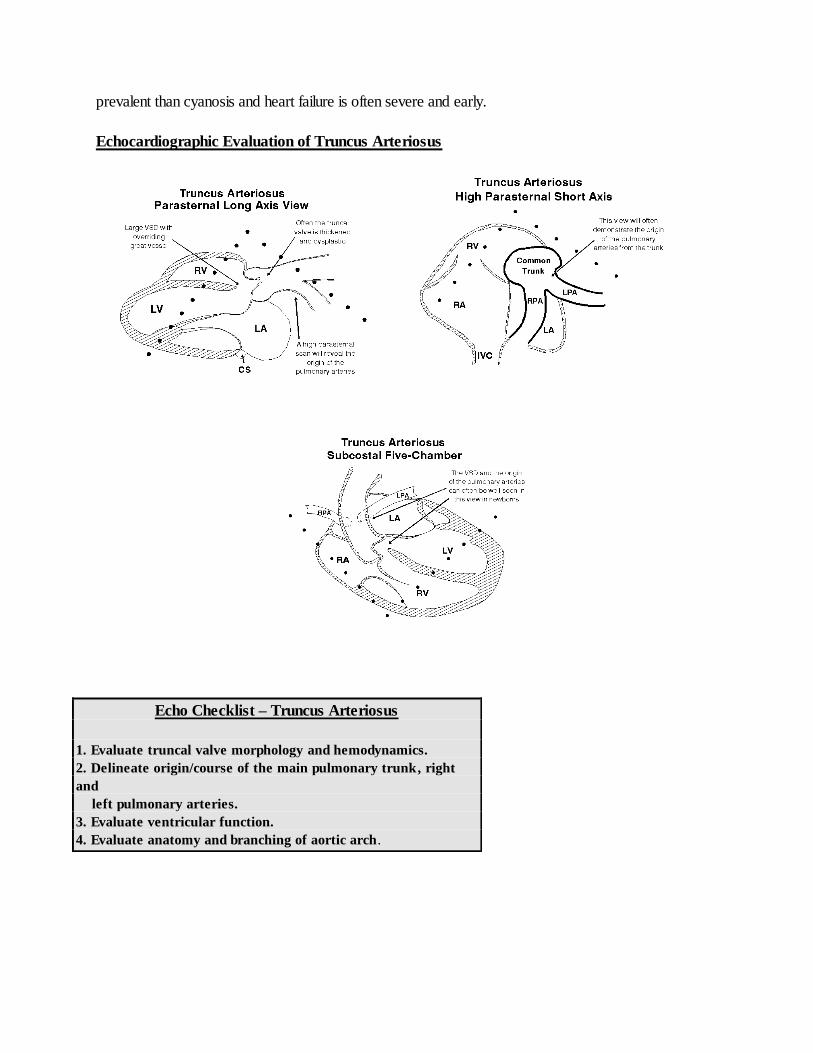
prevalent than cyanosis and heart failure is often severe and early.
Echocardiographic Evaluation of Truncus Arteriosus
Echo Checklist – Truncus Arteriosus
1. Evaluate truncal valve morphology and hemodynamics.
2. Delineate origin/course of the main pulmonary trunk, right
and
left pulmonary arteries.
3. Evaluate ventricular function.
4. Evaluate anatomy and branching of aortic arch.
RA
LA
RV
LV
Corrected Transposition
Anatomy
Practical Summary - Truncus Arteriosus
1. Timing of surgery - usually as a newborn or within the first month.
2. The repair utilizes an extra-cardiac conduit (RV-PA) which will require multiple re-operations for conduit
changes with growth and age.
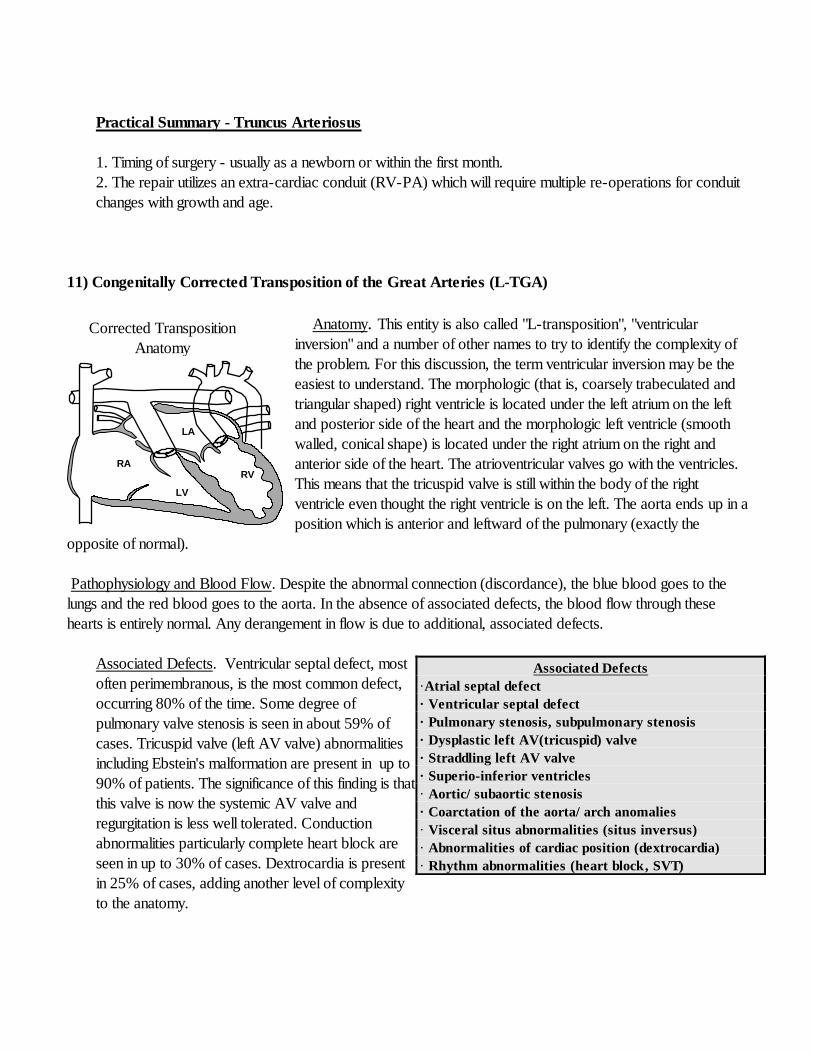
11) Congenitally Corrected Transposition of the Great Arteries (L-TGA)
Anatomy. This entity is also called "L-transposition", "ventricular
inversion" and a number of other names to try to identify the complexity of
the problem. For this discussion, the term ventricular inversion may be the
easiest to understand. The morphologic (that is, coarsely trabeculated and
triangular shaped) right ventricle is located under the left atrium on the left
and posterior side of the heart and the morphologic left ventricle (smooth
walled, conical shape) is located under the right atrium on the right and
anterior side of the heart. The atrioventricular valves go with the ventricles.
This means that the tricuspid valve is still within the body of the right
ventricle even thought the right ventricle is on the left. The aorta ends up in a
position which is anterior and leftward of the pulmonary (exactly the
opposite of normal).
Pathophysiology and Blood Flow. Despite the abnormal connection (discordance), the blue blood goes to the
lungs and the red blood goes to the aorta. In the absence of associated defects, the blood flow through these
hearts is entirely normal. Any derangement in flow is due to additional, associated defects.
Associated Defects. Ventricular septal defect, most
often perimembranous, is the most common defect,
occurring 80% of the time. Some degree of
pulmonary valve stenosis is seen in about 59% of
cases. Tricuspid valve (left AV valve) abnormalities
including Ebstein's malformation are present in up to
90% of patients. The significance of this finding is that
this valve is now the systemic AV valve and
regurgitation is less well tolerated. Conduction
abnormalities particularly complete heart block are
seen in up to 30% of cases. Dextrocardia is present
in 25% of cases, adding another level of complexity
to the anatomy.
Associated Defects
·Atrial septal defect
· Ventricular septal defect
· Pulmonary stenosis, subpulmonary stenosis
· Dysplastic left AV(tricuspid) valve
· Straddling left AV valve
· Superio-inferior ventricles
· Aortic/ subaortic stenosis
· Coarctation of the aorta/ arch anomalies
· Visceral situs abnormalities (situs inversus)
· Abnormalities of cardiac position (dextrocardia)
· Rhythm abnormalities (heart block, SVT)
RA
RV
LV
LA
The septal tricuspid
leaf let is displaced
apically creating an
"atrialized" right
v entricle.
The anterior
tricuspid leaf let is
large and
"sail-like".
An ASD is present in a large
percentage of cases.
Ebstein’s Anomaly Anatomy
Practical Summary - Corrected Transposition
1. Timing of surgery - depends upon the nature of the associated defects (VSD, PS).
2. High incidence of complete heart block, either spontaneous or post-operative.
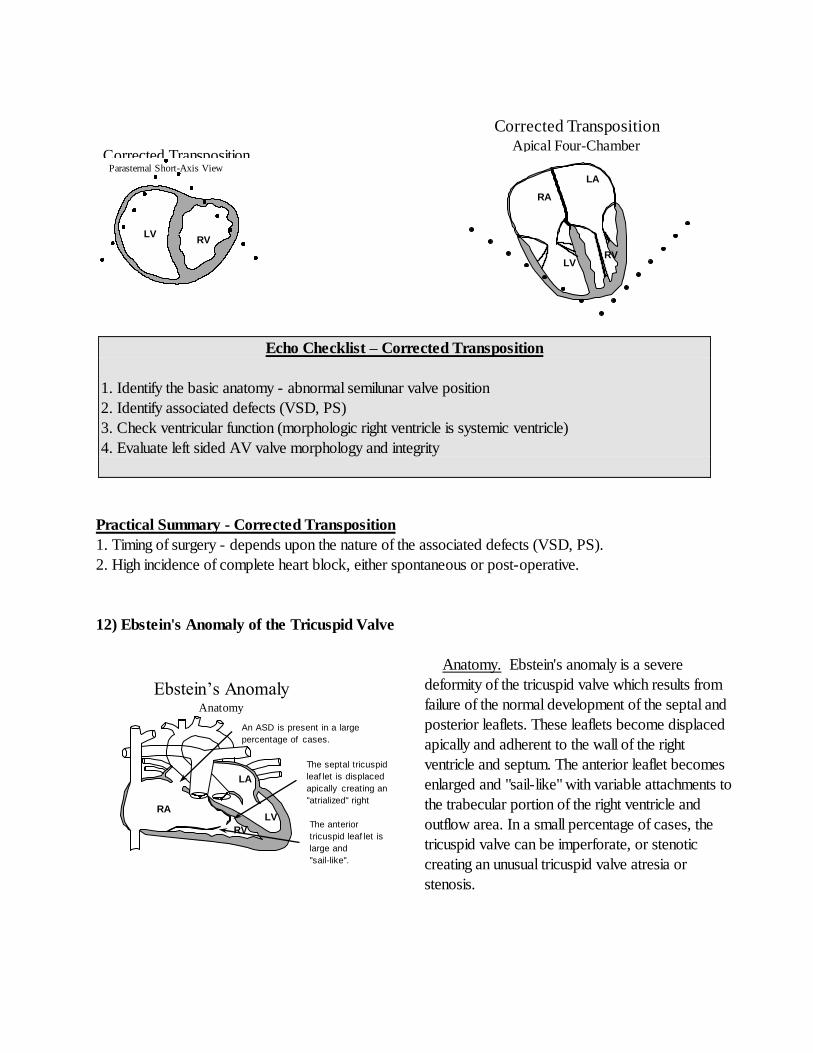
12) Ebstein's Anomaly of the Tricuspid Valve
Anatomy. Ebstein's anomaly is a severe
deformity of the tricuspid valve which results from
failure of the normal development of the septal and
posterior leaflets. These leaflets become displaced
apically and adherent to the wall of the right
ventricle and septum. The anterior leaflet becomes
enlarged and "sail-like" with variable attachments to
the trabecular portion of the right ventricle and
outflow area. In a small percentage of cases, the
tricuspid valve can be imperforate, or stenotic
creating an unusual tricuspid valve atresia or
stenosis.
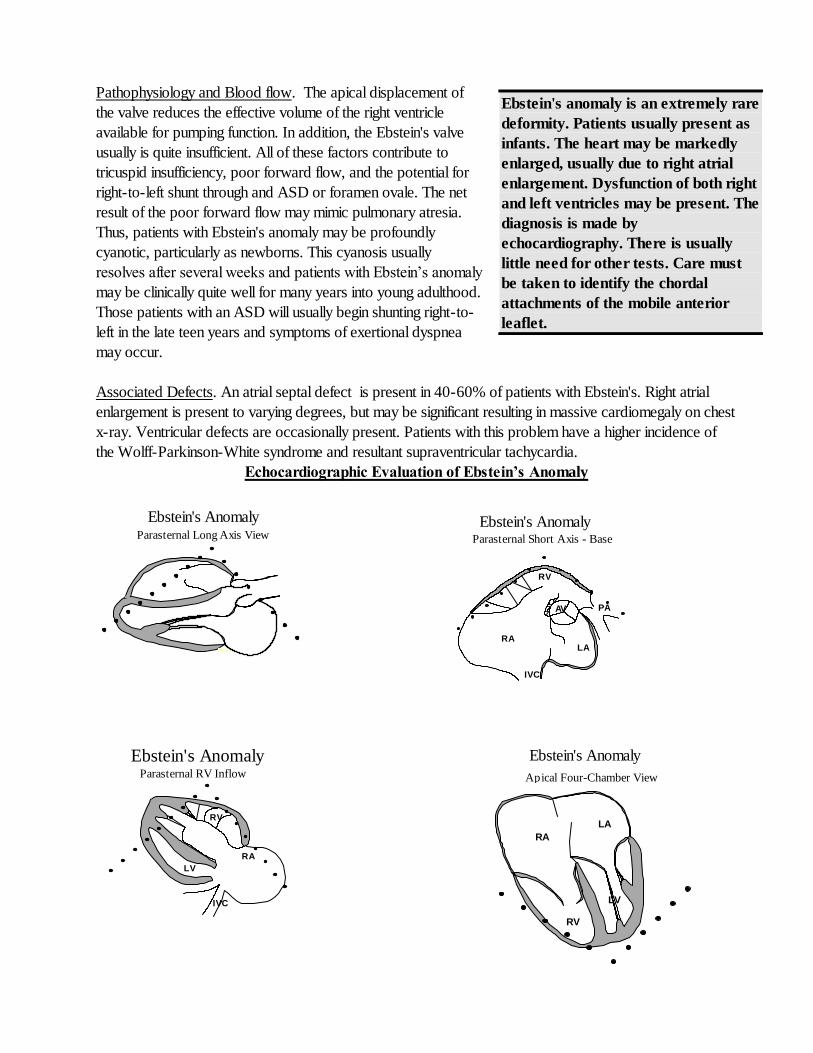
Echo Checklist – Corrected Transposition
1. Identify the basic anatomy - abnormal semilunar valve position
2. Identify associated defects (VSD, PS)
3. Check ventricular function (morphologic right ventricle is systemic ventricle)
4. Evaluate left sided AV valve morphology and integrity
LV RV
RA
LA
LV RV
Apical Four-Chamber
View
Corrected Transposition
Corrected Transposition Parasternal Short-Axis View
Pathophysiology and Blood flow. The apical displacement of
the valve reduces the effective volume of the right ventricle
available for pumping function. In addition, the Ebstein's valve
usually is quite insufficient. All of these factors contribute to
tricuspid insufficiency, poor forward flow, and the potential for
right-to-left shunt through and ASD or foramen ovale. The net
result of the poor forward flow may mimic pulmonary atresia.
Thus, patients with Ebstein's anomaly may be profoundly
cyanotic, particularly as newborns. This cyanosis usually
resolves after several weeks and patients with Ebstein’s anomaly
may be clinically quite well for many years into young adulthood.
Those patients with an ASD will usually begin shunting right-to-
left in the late teen years and symptoms of exertional dyspnea
may occur.
Associated Defects. An atrial septal defect is present in 40-60% of patients with Ebstein's. Right atrial
enlargement is present to varying degrees, but may be significant resulting in massive cardiomegaly on chest
x-ray. Ventricular defects are occasionally present. Patients with this problem have a higher incidence of
the Wolff-Parkinson-White syndrome and resultant supraventricular tachycardia.
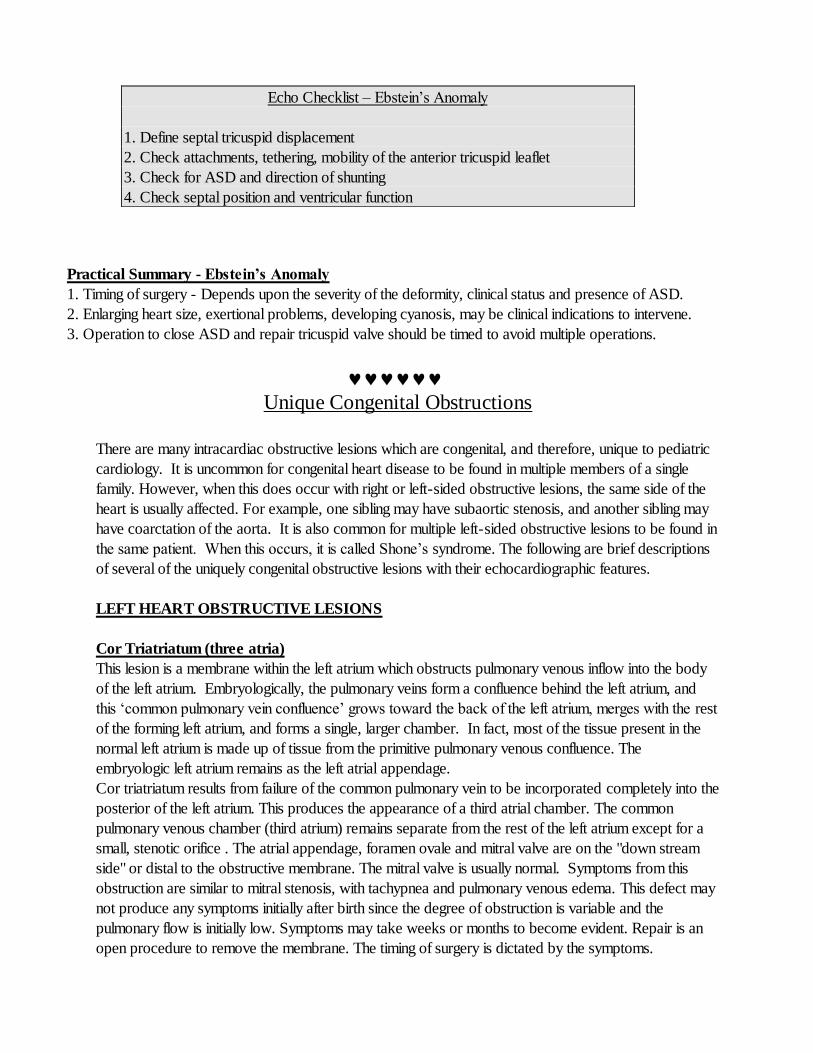
Echocardiographic Evaluation of Ebstein’s Anomaly
Ebstein's anomaly is an extremely rare
deformity. Patients usually present as
infants. The heart may be markedly
enlarged, usually due to right atrial
enlargement. Dysfunction of both right
and left ventricles may be present. The
diagnosis is made by
echocardiography. There is usually
little need for other tests. Care must
be taken to identify the chordal
attachments of the mobile anterior
leaflet.
Parasternal Long Axis View
Ebstein's Anomaly
Parasternal RV Inflow
Ebstein's Anomaly
RV
RA
IVC
LV
RV
LA RA
IVC
PA AV
Parasternal Short Axis - Base
Ebstein's Anomaly
Apical Four-Chamber View
Ebstein's Anomaly
RA
LA
LV
RV
Practical Summary - Ebstein’s Anomaly
1. Timing of surgery - Depends upon the severity of the deformity, clinical status and presence of ASD.
2. Enlarging heart size, exertional problems, developing cyanosis, may be clinical indications to intervene.
3. Operation to close ASD and repair tricuspid valve should be timed to avoid multiple operations.
Unique Congenital Obstructions
There are many intracardiac obstructive lesions which are congenital, and therefore, unique to pediatric
cardiology. It is uncommon for congenital heart disease to be found in multiple members of a single
family. However, when this does occur with right or left-sided obstructive lesions, the same side of the
heart is usually affected. For example, one sibling may have subaortic stenosis, and another sibling may
have coarctation of the aorta. It is also common for multiple left-sided obstructive lesions to be found in
the same patient. When this occurs, it is called Shone’s syndrome. The following are brief descriptions
of several of the uniquely congenital obstructive lesions with their echocardiographic features.
LEFT HEART OBSTRUCTIVE LESIONS
Cor Triatriatum (three atria)
This lesion is a membrane within the left atrium which obstructs pulmonary venous inflow into the body
of the left atrium. Embryologically, the pulmonary veins form a confluence behind the left atrium, and
this ‘common pulmonary vein confluence’ grows toward the back of the left atrium, merges with the rest
of the forming left atrium, and forms a single, larger chamber. In fact, most of the tissue present in the
normal left atrium is made up of tissue from the primitive pulmonary venous confluence. The
embryologic left atrium remains as the left atrial appendage.
Cor triatriatum results from failure of the common pulmonary vein to be incorporated completely into the
posterior of the left atrium. This produces the appearance of a third atrial chamber. The common
pulmonary venous chamber (third atrium) remains separate from the rest of the left atrium except for a
small, stenotic orifice . The atrial appendage, foramen ovale and mitral valve are on the "down stream
side" or distal to the obstructive membrane. The mitral valve is usually normal. Symptoms from this
obstruction are similar to mitral stenosis, with tachypnea and pulmonary venous edema. This defect may
not produce any symptoms initially after birth since the degree of obstruction is variable and the
pulmonary flow is initially low. Symptoms may take weeks or months to become evident. Repair is an
open procedure to remove the membrane. The timing of surgery is dictated by the symptoms.
Echo Checklist – Ebstein’s Anomaly
1. Define septal tricuspid displacement
2. Check attachments, tethering, mobility of the anterior tricuspid leaflet
3. Check for ASD and direction of shunting
4. Check septal position and ventricular function
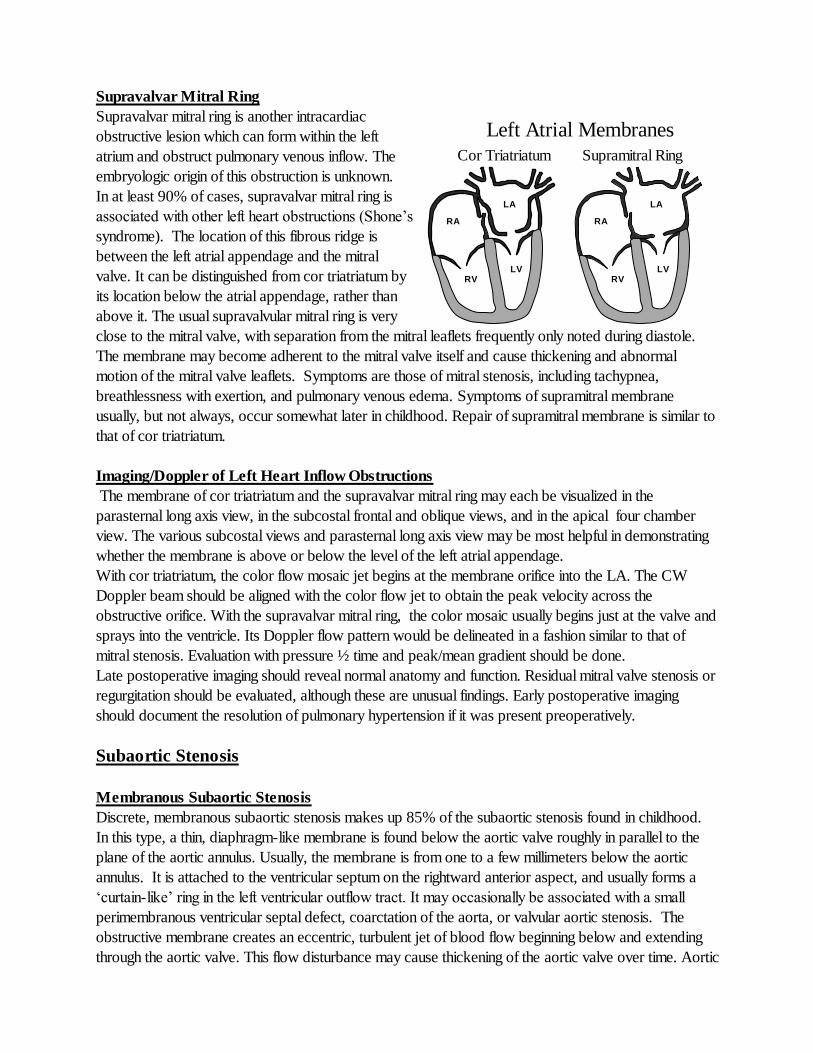
Supravalvar Mitral Ring
Supravalvar mitral ring is another intracardiac
obstructive lesion which can form within the left
atrium and obstruct pulmonary venous inflow. The
embryologic origin of this obstruction is unknown.
In at least 90% of cases, supravalvar mitral ring is
associated with other left heart obstructions (Shone’s
syndrome). The location of this fibrous ridge is
between the left atrial appendage and the mitral
valve. It can be distinguished from cor triatriatum by
its location below the atrial appendage, rather than
above it. The usual supravalvular mitral ring is very
close to the mitral valve, with separation from the mitral leaflets frequently only noted during diastole.
The membrane may become adherent to the mitral valve itself and cause thickening and abnormal
motion of the mitral valve leaflets. Symptoms are those of mitral stenosis, including tachypnea,
breathlessness with exertion, and pulmonary venous edema. Symptoms of supramitral membrane
usually, but not always, occur somewhat later in childhood. Repair of supramitral membrane is similar to
that of cor triatriatum.
Imaging/Doppler of Left Heart Inflow Obstructions
The membrane of cor triatriatum and the supravalvar mitral ring may each be visualized in the
parasternal long axis view, in the subcostal frontal and oblique views, and in the apical four chamber
view. The various subcostal views and parasternal long axis view may be most helpful in demonstrating
whether the membrane is above or below the level of the left atrial appendage.
With cor triatriatum, the color flow mosaic jet begins at the membrane orifice into the LA. The CW
Doppler beam should be aligned with the color flow jet to obtain the peak velocity across the
obstructive orifice. With the supravalvar mitral ring, the color mosaic usually begins just at the valve and
sprays into the ventricle. Its Doppler flow pattern would be delineated in a fashion similar to that of
mitral stenosis. Evaluation with pressure ½ time and peak/mean gradient should be done.
Late postoperative imaging should reveal normal anatomy and function. Residual mitral valve stenosis or
regurgitation should be evaluated, although these are unusual findings. Early postoperative imaging
should document the resolution of pulmonary hypertension if it was present preoperatively.
Subaortic Stenosis
Membranous Subaortic Stenosis
Discrete, membranous subaortic stenosis makes up 85% of the subaortic stenosis found in childhood.
In this type, a thin, diaphragm-like membrane is found below the aortic valve roughly in parallel to the
plane of the aortic annulus. Usually, the membrane is from one to a few millimeters below the aortic
annulus. It is attached to the ventricular septum on the rightward anterior aspect, and usually forms a
‘curtain-like’ ring in the left ventricular outflow tract. It may occasionally be associated with a small
perimembranous ventricular septal defect, coarctation of the aorta, or valvular aortic stenosis. The
obstructive membrane creates an eccentric, turbulent jet of blood flow beginning below and extending
through the aortic valve. This flow disturbance may cause thickening of the aortic valve over time. Aortic
RV
LA
LV
RA
RV
LA
LV
RA
Cor Triatriatum Supramitral Ring
Left Atrial Membranes
insufficiency frequently develops since the membrane blocks part of the aortic valve but allows
accelerated flow across the rest of the valve. Aortic regurgitation is rarely severe. Symptoms and clinical
findings are similar to those of aortic valve stenosis.
Tunnel Subaortic Stenosis
Tunnel subaortic stenosis makes up the other 15% of subaortic stenosis. Many authors believe that
there is a spectrum of disease between the thin membrane described above and tunnel subaortic
stenosis. In tunnel subaortic stenosis, a fibrous or fibromuscular cuff of obstructive tissue of variable
length develops below the aortic valve in the left ventricular outflow tract. It is often associated with
concentric left ventricular hypertrophy, and less commonly with asymmetric septal hypertrophy and
hypercontractility of the LV. It may also be found in patients with multiple left heart obstructions
(Shone’s syndrome). Symptoms and clinical findings are similar to those of aortic valve stenosis.
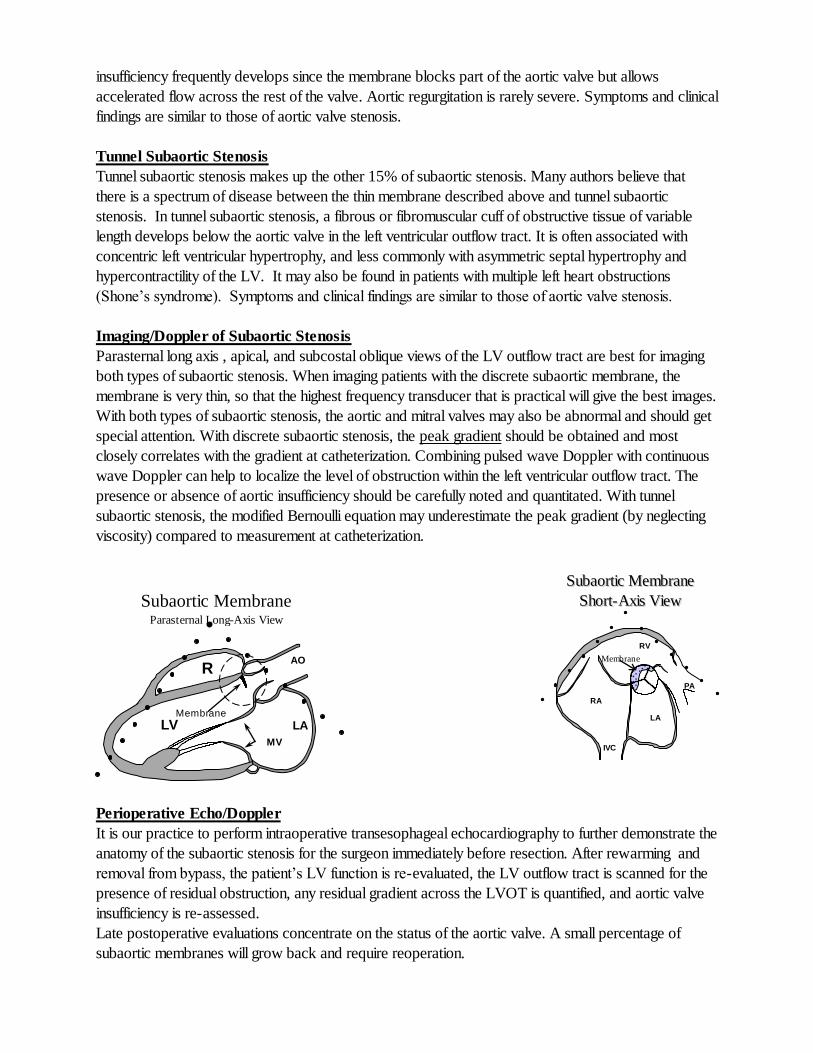
Imaging/Doppler of Subaortic Stenosis
Parasternal long axis , apical, and subcostal oblique views of the LV outflow tract are best for imaging
both types of subaortic stenosis. When imaging patients with the discrete subaortic membrane, the
membrane is very thin, so that the highest frequency transducer that is practical will give the best images.
With both types of subaortic stenosis, the aortic and mitral valves may also be abnormal and should get
special attention. With discrete subaortic stenosis, the peak gradient should be obtained and most
closely correlates with the gradient at catheterization. Combining pulsed wave Doppler with continuous
wave Doppler can help to localize the level of obstruction within the left ventricular outflow tract. The
presence or absence of aortic insufficiency should be carefully noted and quantitated. With tunnel
subaortic stenosis, the modified Bernoulli equation may underestimate the peak gradient (by neglecting
viscosity) compared to measurement at catheterization.
Perioperative Echo/Doppler
It is our practice to perform intraoperative transesophageal echocardiography to further demonstrate the
anatomy of the subaortic stenosis for the surgeon immediately before resection. After rewarming and
removal from bypass, the patient’s LV function is re-evaluated, the LV outflow tract is scanned for the
presence of residual obstruction, any residual gradient across the LVOT is quantified, and aortic valve
insufficiency is re-assessed.
Late postoperative evaluations concentrate on the status of the aortic valve. A small percentage of
subaortic membranes will grow back and require reoperation.
LV LA
AO
MV
R
V
Membrane
Subaortic Membrane Parasternal Long-Axis View
SSuubbaaoorrttiicc MMeemmbbrraannee
SShhoorrtt--AAxxiiss VViieeww
RV
LA
RA
IVC
PA
Membrane
Coronary Arteries
Coronary artery anomalies may be classified into:
1) Abnormalities of clinical importance 2) Abnormalities of surgical importance
Abnormalities of Clinical Importance
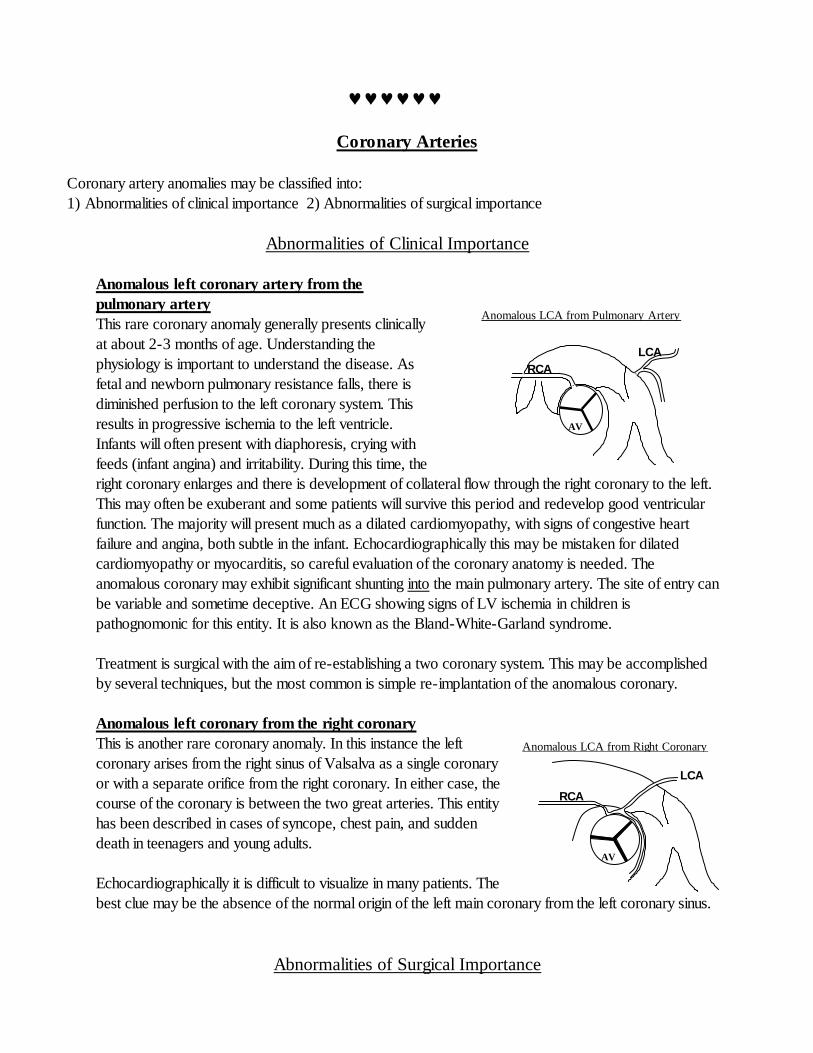
Anomalous left coronary artery from the
pulmonary artery
This rare coronary anomaly generally presents clinically
at about 2-3 months of age. Understanding the
physiology is important to understand the disease. As
fetal and newborn pulmonary resistance falls, there is
diminished perfusion to the left coronary system. This
results in progressive ischemia to the left ventricle.
Infants will often present with diaphoresis, crying with
feeds (infant angina) and irritability. During this time, the
right coronary enlarges and there is development of collateral flow through the right coronary to the left.
This may often be exuberant and some patients will survive this period and redevelop good ventricular
function. The majority will present much as a dilated cardiomyopathy, with signs of congestive heart
failure and angina, both subtle in the infant. Echocardiographically this may be mistaken for dilated
cardiomyopathy or myocarditis, so careful evaluation of the coronary anatomy is needed. The
anomalous coronary may exhibit significant shunting into the main pulmonary artery. The site of entry can
be variable and sometime deceptive. An ECG showing signs of LV ischemia in children is
pathognomonic for this entity. It is also known as the Bland-White-Garland syndrome.
Treatment is surgical with the aim of re-establishing a two coronary system. This may be accomplished
by several techniques, but the most common is simple re-implantation of the anomalous coronary.
Anomalous left coronary from the right coronary
This is another rare coronary anomaly. In this instance the left
coronary arises from the right sinus of Valsalva as a single coronary
or with a separate orifice from the right coronary. In either case, the
course of the coronary is between the two great arteries. This entity
has been described in cases of syncope, chest pain, and sudden
death in teenagers and young adults.
Echocardiographically it is difficult to visualize in many patients. The
best clue may be the absence of the normal origin of the left main coronary from the left coronary sinus.
Abnormalities of Surgical Importance
RCA
LCA
Anomalous LCA from Pulmonary Artery
(ALCAPA)
AV
RCA
LCA
Anomalous LCA from Right Coronary
AV
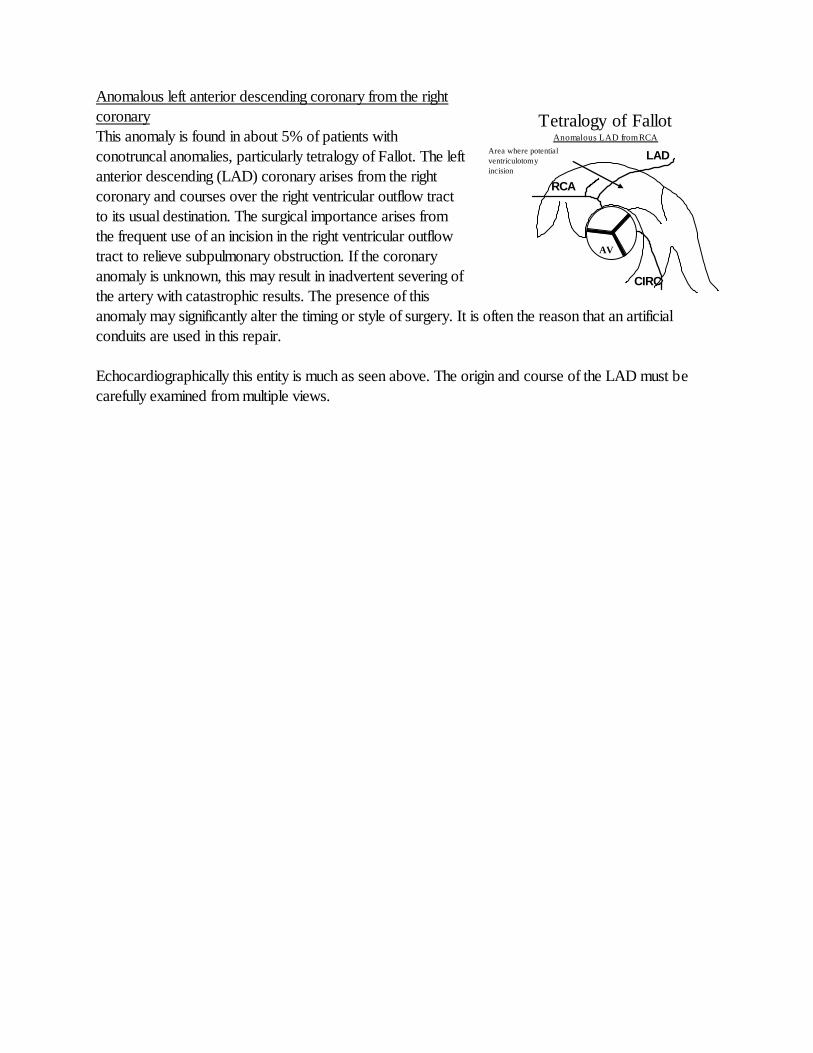
Anomalous left anterior descending coronary from the right
coronary
This anomaly is found in about 5% of patients with
conotruncal anomalies, particularly tetralogy of Fallot. The left
anterior descending (LAD) coronary arises from the right
coronary and courses over the right ventricular outflow tract
to its usual destination. The surgical importance arises from
the frequent use of an incision in the right ventricular outflow
tract to relieve subpulmonary obstruction. If the coronary
anomaly is unknown, this may result in inadvertent severing of
the artery with catastrophic results. The presence of this
anomaly may significantly alter the timing or style of surgery. It is often the reason that an artificial
conduits are used in this repair.
Echocardiographically this entity is much as seen above. The origin and course of the LAD must be
carefully examined from multiple views.
RCA
LAD
CIRC
Tetralogy of Fallot Anomalous LAD from RCA
AV
Area where potential
ventriculotomy
incision
would be.
Anomalous Pulmonary Venous Return
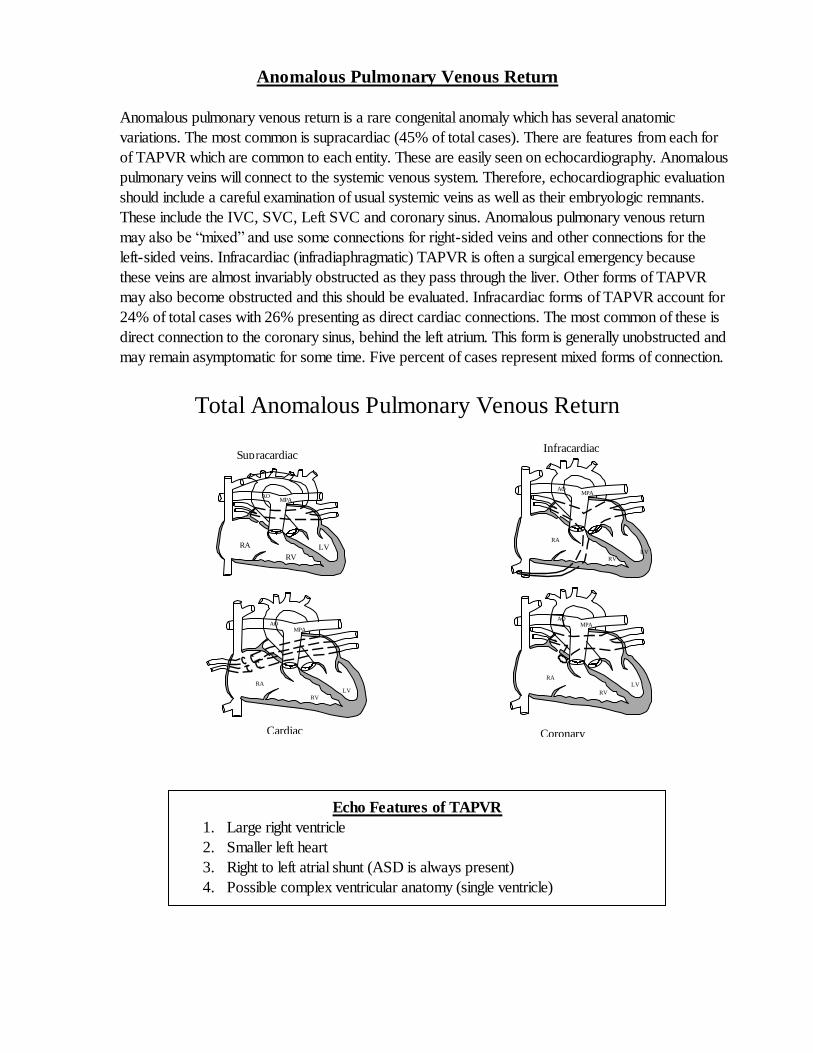
Anomalous pulmonary venous return is a rare congenital anomaly which has several anatomic
variations. The most common is supracardiac (45% of total cases). There are features from each for
of TAPVR which are common to each entity. These are easily seen on echocardiography. Anomalous
pulmonary veins will connect to the systemic venous system. Therefore, echocardiographic evaluation
should include a careful examination of usual systemic veins as well as their embryologic remnants.
These include the IVC, SVC, Left SVC and coronary sinus. Anomalous pulmonary venous return
may also be “mixed” and use some connections for right-sided veins and other connections for the
left-sided veins. Infracardiac (infradiaphragmatic) TAPVR is often a surgical emergency because
these veins are almost invariably obstructed as they pass through the liver. Other forms of TAPVR
may also become obstructed and this should be evaluated. Infracardiac forms of TAPVR account for
24% of total cases with 26% presenting as direct cardiac connections. The most common of these is
direct connection to the coronary sinus, behind the left atrium. This form is generally unobstructed and
may remain asymptomatic for some time. Five percent of cases represent mixed forms of connection.
RA
RV
LV
MPA AO
Infracardiac Supracardiac
RA
RV
LV
MPA AO
Coronary
sinus
RA
RV
LV
MPA AO
Cardiac
RA
RV
LV
MPA AO
Total Anomalous Pulmonary Venous Return Anatomic Types
Echo Features of TAPVR
1. Large right ventricle
2. Smaller left heart
3. Right to left atrial shunt (ASD is always present)
4. Possible complex ventricular anatomy (single ventricle)
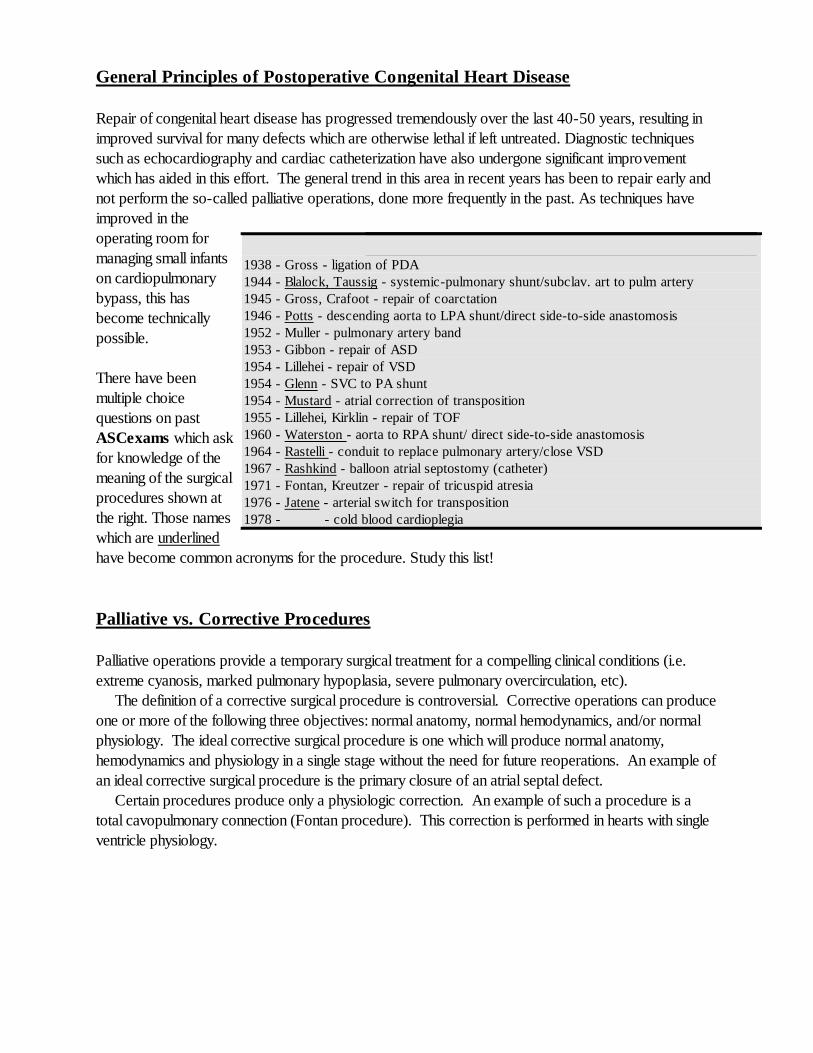
General Principles of Postoperative Congenital Heart Disease
Repair of congenital heart disease has progressed tremendously over the last 40-50 years, resulting in
improved survival for many defects which are otherwise lethal if left untreated. Diagnostic techniques
such as echocardiography and cardiac catheterization have also undergone significant improvement
which has aided in this effort. The general trend in this area in recent years has been to repair early and
not perform the so-called palliative operations, done more frequently in the past. As techniques have
improved in the
operating room for
managing small infants
on cardiopulmonary
bypass, this has
become technically
possible.
There have been
multiple choice
questions on past
ASCexams which ask
for knowledge of the
meaning of the surgical
procedures shown at
the right. Those names
which are underlined
have become common acronyms for the procedure. Study this list!
Palliative vs. Corrective Procedures
Palliative operations provide a temporary surgical treatment for a compelling clinical conditions (i.e.
extreme cyanosis, marked pulmonary hypoplasia, severe pulmonary overcirculation, etc).
The definition of a corrective surgical procedure is controversial. Corrective operations can produce
one or more of the following three objectives: normal anatomy, normal hemodynamics, and/or normal
physiology. The ideal corrective surgical procedure is one which will produce normal anatomy,
hemodynamics and physiology in a single stage without the need for future reoperations. An example of
an ideal corrective surgical procedure is the primary closure of an atrial septal defect.
Certain procedures produce only a physiologic correction. An example of such a procedure is a
total cavopulmonary connection (Fontan procedure). This correction is performed in hearts with single
ventricle physiology.
A Brief History of Congenital Heart Disease Operations 1938 - Gross - ligation of PDA
1944 - Blalock, Taussig - systemic-pulmonary shunt/subclav. art to pulm artery
1945 - Gross, Crafoot - repair of coarctation
1946 - Potts - descending aorta to LPA shunt/direct side-to-side anastomosis
1952 - Muller - pulmonary artery band
1953 - Gibbon - repair of ASD
1954 - Lillehei - repair of VSD
1954 - Glenn - SVC to PA shunt
1954 - Mustard - atrial correction of transposition
1955 - Lillehei, Kirklin - repair of TOF
1960 - Waterston - aorta to RPA shunt/ direct side-to-side anastomosis
1964 - Rastelli - conduit to replace pulmonary artery/close VSD
1967 - Rashkind - balloon atrial septostomy (catheter)
1971 - Fontan, Kreutzer - repair of tricuspid atresia
1976 - Jatene - arterial switch for transposition
1978 - - cold blood cardioplegia
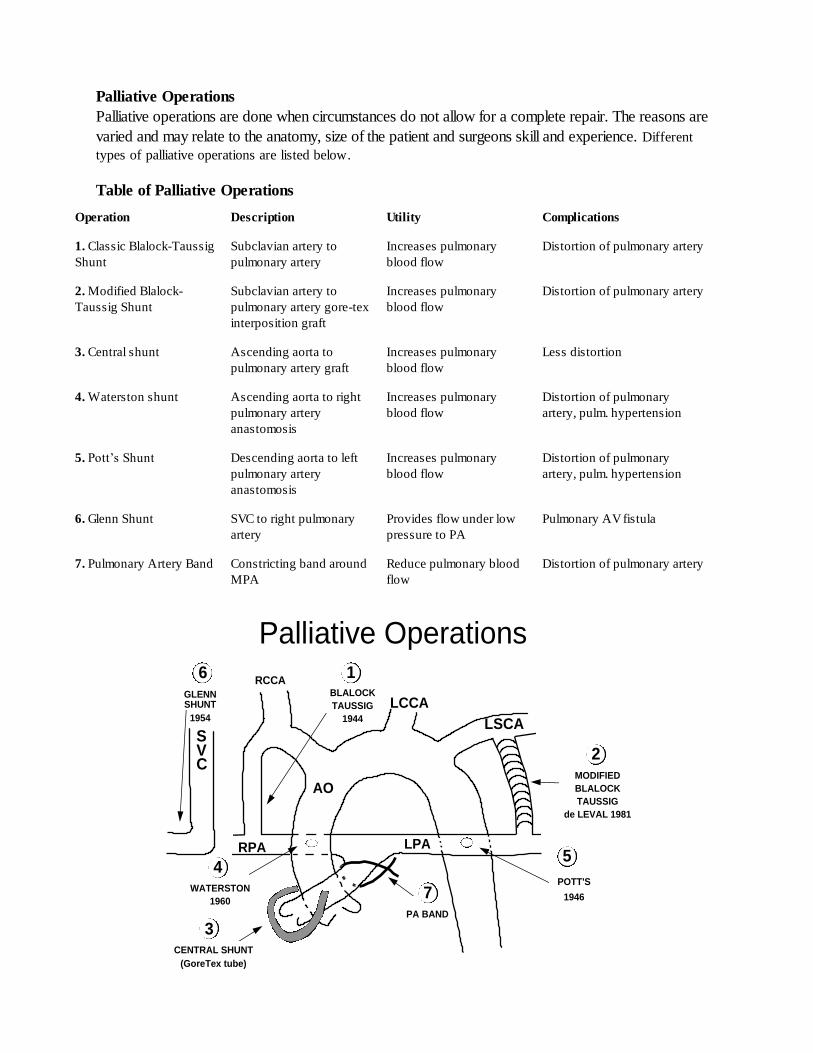
Palliative Operations
Palliative operations are done when circumstances do not allow for a complete repair. The reasons are
varied and may relate to the anatomy, size of the patient and surgeons skill and experience. Different
types of palliative operations are listed below.
Table of Palliative Operations Operation
Description
Utility
Complications
1. Classic Blalock-Taussig
Shunt
Subclavian artery to
pulmonary artery
Increases pulmonary
blood flow
Distortion of pulmonary artery
2. Modified Blalock-
Taussig Shunt
Subclavian artery to
pulmonary artery gore-tex
interposition graft
Increases pulmonary
blood flow
Distortion of pulmonary artery
3. Central shunt
Ascending aorta to
pulmonary artery graft
Increases pulmonary
blood flow
Less distortion
4. Waterston shunt
Ascending aorta to right
pulmonary artery
anastomosis
Increases pulmonary
blood flow
Distortion of pulmonary
artery, pulm. hypertension
5. Pott’s Shunt
Descending aorta to left
pulmonary artery
anastomosis
Increases pulmonary
blood flow
Distortion of pulmonary
artery, pulm. hypertension
6. Glenn Shunt
SVC to right pulmonary
artery
Provides flow under low
pressure to PA
Pulmonary AV fistula
7. Pulmonary Artery Band
Constricting band around
MPA
Reduce pulmonary blood
flow
Distortion of pulmonary artery
Palliative Operations
BLALOCK
TAUSSIG
1944
CENTRAL SHUNT
(GoreTex tube)
WATERSTON
1960
LSCA
LPARPA
LCCA
RCCA
AO
SVC
POTT'S
1946
MODIFIED
BLALOCK
TAUSSIG
de LEVAL 1981
GLENNSHUNT
1954
6
54
3
2
1
PA BAND
7
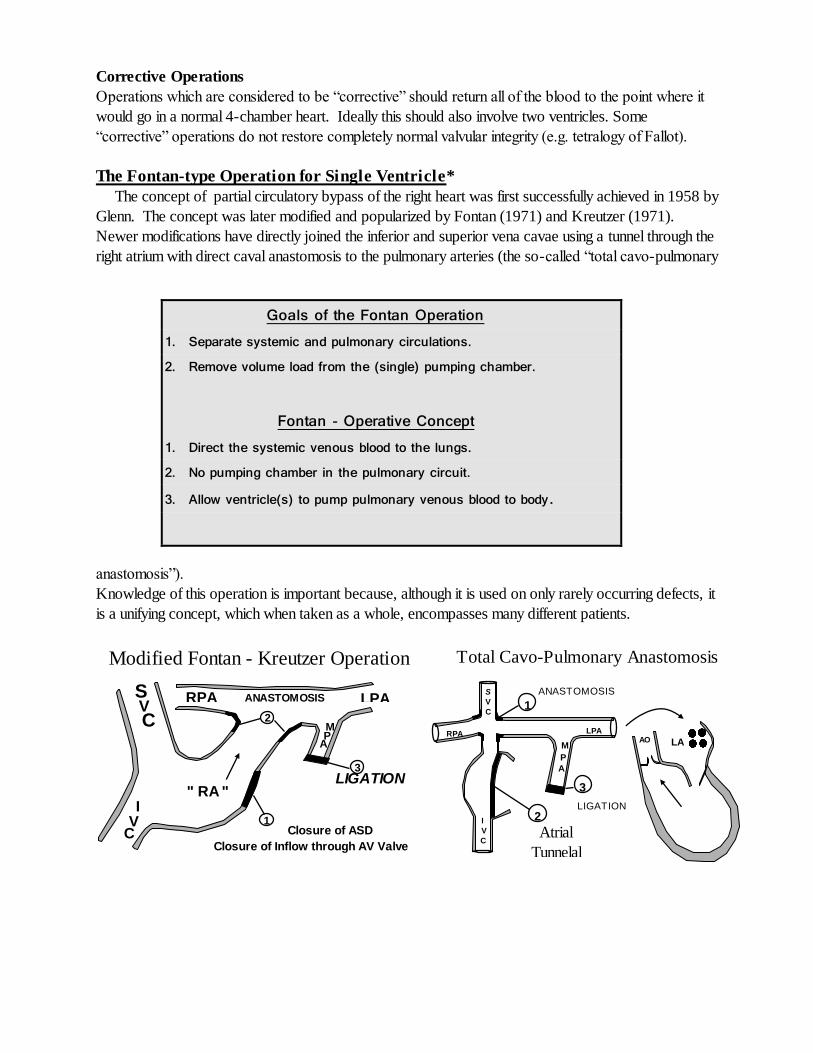
Modified Fontan - Kreutzer Operation
S V C
I V
C
" RA "
Closure of ASD
Closure of Inflow through AV Valve
RPA LPA
M P
A
ANASTOMOSIS
LIGATION
1
2
3
Total Cavo-Pulmonary Anastomosis
S
V
C
I
V
C
RPA LPA
M
P
A
1
2
3
LA AO
ANASTOMOSIS
Atrial
Tunnelal
LIGATION
Corrective Operations
Operations which are considered to be “corrective” should return all of the blood to the point where it
would go in a normal 4-chamber heart. Ideally this should also involve two ventricles. Some
“corrective” operations do not restore completely normal valvular integrity (e.g. tetralogy of Fallot).
The Fontan-type Operation for Single Ventricle*
The concept of partial circulatory bypass of the right heart was first successfully achieved in 1958 by
Glenn. The concept was later modified and popularized by Fontan (1971) and Kreutzer (1971).
Newer modifications have directly joined the inferior and superior vena cavae using a tunnel through the
right atrium with direct caval anastomosis to the pulmonary arteries (the so-called “total cavo-pulmonary
anastomosis”).
Knowledge of this operation is important because, although it is used on only rarely occurring defects, it
is a unifying concept, which when taken as a whole, encompasses many different patients.
Goals of the Fontan Operation 1. Separate systemic and pulmonary circulations. 2. Remove volume load from the (single) pumping chamber. Fontan - Operative Concept 1. Direct the systemic venous blood to the lungs. 2. No pumping chamber in the pulmonary circuit. 3. Allow ventricle(s) to pump pulmonary venous blood to body.
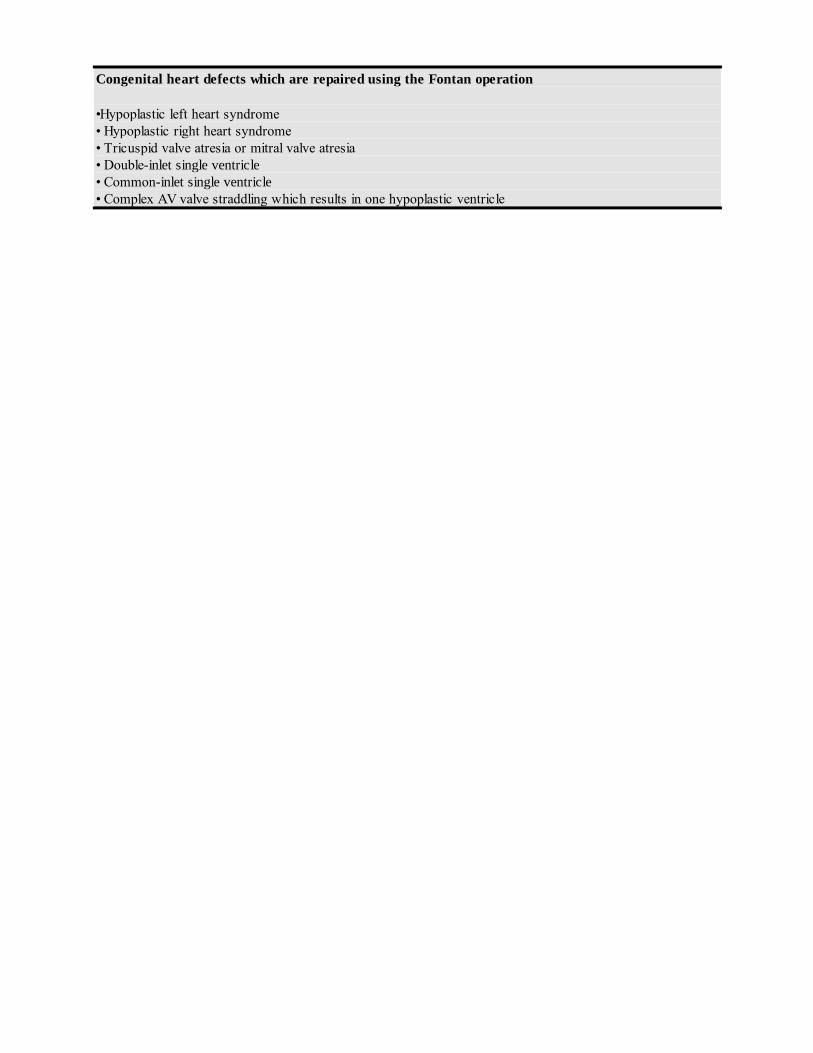
Congenital heart defects which are repaired using the Fontan operation
•Hypoplastic left heart syndrome
• Hypoplastic right heart syndrome
• Tricuspid valve atresia or mitral valve atresia
• Double-inlet single ventricle
• Common-inlet single ventricle
• Complex AV valve straddling which results in one hypoplastic ventricle
Exam Tips
Exam items which have previously appeared are no guarantee that they will be on every exam. The
exam writers choose from a question bank and each year’s exam differs from previous exams.
Like most board exams, questions are evaluated after each exam for validity and some are
discarded if the answers clearly do not produce a consensus. The following represent some tips
which have been given by previous examinees based on their experience to give course
participants an idea of the type of questions which they might face.
Congenital things which have appeared on previous exams:
Video Test
VSD w/ aneurysm vs. ruptured sinus of Valsalva
Supracristal VSD with aortic regurgitation
Secundum ASD demonstrated by negative contrast
Written Test
Description of Ebstein’s anomaly
Associated problems w/ bicuspid aortic valve
– Post-stenotic dilation, coarctation, degeneration
– Bicuspid vs. unicommissural
Picture of sub-aortic membrane
Picture of tricuspid atresia
Picture of L-Transposition – a favorite question
Knowledge of AV canal defects
Anomalous left coronary artery from the pulmonary artery (ALCAPA)
Associations w/ primum ASD – know cleft MV
QP/QS calculations – usually with an ASD
Sinus venosus ASD – TEE picture and common associations – know PAPVR
Timing of fetal echocardiography
– Know what might be hard to spot in a 20-week fetus – perimembranous
VSD
– Easy things to spot are hypoplastic chambers or big VSD’s, AV canal,
conotruncal defects
Knowledge of associations with supracristal VSD – aortic cusp prolapse
Look-alikes for DORV and VSD – tetralogy of Fallot
Case of adult w/ PO tetralogy and increased RV pressure – think peripheral PS
Noonan’s, William’s, Turner’s, Marfan’s syndromes – associated anomalies
Common associated lesions with coarctation (other left heart obstructions)
Uhls’ Anomaly
Uhl’s anomaly is a very rare anomaly with parchment-like right ventricle and
almost complete absence of RV muscle fibers. In appearance it has similarities
to Ebstein’s anomaly, except that the tricuspid valve is anatomically normal. It
has been associated with arrythmogenic right ventricular dysplasia.