Refrigeration Dryer Manuel d’utilisation ASD 10 ASD 15 ASD ...

Jassin M. Jouria, MD
Dr. Jassin M. Jouria is a medical doctor, professor of
academic medicine, and medical author. He graduated from
Ross University School of Medicine and has completed his
clinical clerkship training in various teaching hospitals
throughout New York, including King’s County Hospital Center and Brookdale Medical Center,
among others. Dr. Jouria has passed all USMLE medical board exams, and has served as a test
prep tutor and instructor for Kaplan. He has developed several medical courses and curricula for a
variety of educational institutions. Dr. Jouria has also served on multiple levels in the academic field
including faculty member and Department Chair. Dr. Jouria continues to serves as a Subject Matter
Expert for several continuing education organizations covering multiple basic medical sciences. He
has also developed several continuing medical education courses covering various topics in clinical
medicine. Recently, Dr. Jouria has been contracted by the University of Miami/Jackson Memorial
Hospital’s Department of Surgery to develop an e-module training series for trauma patient
management. Dr. Jouria is currently authoring an academic textbook on Human Anatomy &
Physiology.
ABSTRACT
The U.S. Center for Disease Control estimates that 1 in 88 children are on the autism
spectrum; meaning some degree of a complex brain disorder exists, characterized by
difficulties in social interaction and communication, as well as a tendency toward
repetitive behaviors. In its mildest form, autism spectrum disorder (ASD) can present
minor communication challenges in children who are at or above normal intelligence. In
its most severe form, comprehensive cognitive deficits and a total lack of
communication create permanent dependence. Currently, there is no cure for ASD, and
the focus is on research to develop effective management and prevention strategies.
Nursece4less.com 1
AUTISM SPECTRUM DISORDER
Continuing Nursing Education Course Director & Planners
William A. Cook, PhD, Director, Douglas Lawrence, MS, Webmaster,
Susan DePasquale, CGRN, MSN, FPMHNP-BC, Lead Nurse Planner
Accreditation Statement
This activity has been planned and implemented in accordance with the policies of
NurseCe4Less.com and the continuing nursing education requirements of the American
Nurses Credentialing Center's Commission on Accreditation for registered nurses.
Credit Designation
This educational activity is credited for 12.5 hours. Nurses may only claim credit
commensurate with the credit awarded for completion of this course activity.
Course Author & Planner Disclosure Policy Statements
It is the policy of NurseCe4Less.com to ensure objectivity, transparency, and best
practice for all nursing educational activities. All authors and course planners
participating in the planning or implementation of an educational activity are expected to
disclose to course participants any relevant conflict of interest that may arise.
Statement of Need
Nurses often participate on an autism treatment team, involved in the diagnosis and
ongoing health care of the individual child or adult with ASD as well as their families.
Mental health and school nurses are required to perform an evidence-based evaluation
and treatment plan to promote the best quality of life for the individual with ASD.
Course Purpose
This course will provide advanced learning for nurses interested in the diagnosis and
treatment plan for the individual with autism, and for their families.
Nursece4less.com 2

Learning Objectives
Identify the disorders included within the ASD.
Explain the historical etiology of autism.
Identify domains that are evaluated when diagnosing ASD according to the DSM-5.
Identify common characteristics of ASD.
Describe the gradual onset course and the regression course of ASD.
Explain the effects of early intervention in ASD patients.
Describe risk factors that may influence the occurrence of ASD.
Describe common neuroanatomical abnormalities that may occur in ASD patients.
Define the two levels of initial diagnosis for ASD.
List common psychological assessment tools for diagnosis ASD.
List common co-morbidities of ASD.
Explain the primary goals of ASD treatment.
Explain the controversy relating to autism and vaccines.
Target AudienceAdvanced Practice Registered Nurses, Registered Nurses, Licensed Practical Nurses,
and Associates
Course Author & Director Disclosures
Jassin M. Jouria, MD, William S. Cook, PhD, Douglas Lawrence, MS,
Susan DePasquale, CGRN, MSN, FPMHNP-BC – all have no disclosures
Acknowledgement of Commercial Support
There is no commercial support for this course.
Activity Review Information
Reviewed by Susan DePasquale, CGRN, MSN, FPMHNP-BC.
Release Date: 1/1/2015 Termination Date: 10/24/2016
Please take time to complete the self-assessment Knowledge Questions before reading the article. Opportunity to complete a self-assessment of knowledge learned will be
provided at the end of the course.
Nursece4less.com 3

1. The primary goals of ASD treatments are to:a. lessen deficits and family stresses
b. treatment through use of medication
c. educating family and other caregivers about unique challenges of an
individual with ASD
d. all of the above
2. True of False. ASD is understood to be the result of a combination of genetic and non-genetic factors.
a. True
b. False
3. Secondary ASD can be caused by:
a. Fragile X syndrome
b. Tuberculosis
c. Rett Syndrome
d. Answers a and c above
4. Rett syndrome predominantly affects:
a. males
b. females
c. individuals during adolescence
d. those of African descent
5. Repetitive behaviors in individuals with ASD can include:
a. arm and hand flapping
b. rocking or other unusual body movements
c. head banging
d. all of the above
Nursece4less.com 4
6. True or False. Pregnancy and increased risk of ASD with a combined diagnosis of ADHD or ADHD symptoms includes use of valproic acid.
a. True
b. False
7. Individuals with ASD often have ADHD-like symptoms, which include:
a. hyperactivity, distractibility, excitability, difficulty concentrating
b. impulsivity, short term memory loss, aggression, tension
c. distractibility, fatigue, poor concentration and insomnia
d. poor performance in school, conflict with peers, hyperactivity
8. True or False. Treatment for children with both ASD and anxiety is evolving and more research is needed on how to adapt traditional approaches with cognitive behavioral therapy.
a. True
b. False
9. Individuals with ASD thrive best in very well organized and highly structured environments, which include those that:a. promote a clear understanding of schedules
b. provide activities
c. establish expectations
d. all of the above
10.True or False. Treatment with SSRIs is uncommon for children with ASD.a. True
b. False
Nursece4less.com 5

INTRODUCTION
Autism Spectrum Disorders (ASD) encompass a group of developmental disorders
whose symptoms range on a continuum that runs from mild to severe in expression [1].
ASD is typically present early in life, anytime from infancy or early childhood; however,
in the new DSM-V, there are changes in place for diagnostic age criteria in that deficits
from ASD may not be detected until later on in life. This later detection may result from
lower social demands placed on an individual as a result of assistance from parents or
caregivers earlier on in life.
The onset of ASD has been intensively studied [2-4], and it is largely accepted that the
time of diagnosis may occur far after the time of onset. Additionally, the time between
where parents indicate that the child shows early signs or symptoms of ASD or
abnormal development and the time until diagnosis may be quite lengthy. It is important
to note here that detecting early signs of ASD has been indicated to be quite difficult [5].
This is why ASD is sometimes only diagnosed once a child is put into situations that
require social abilities, and a lack is seen in these situations.
More than 500,000 people in the United States have some form of diagnosed autism [6].
Autism may keep a child from forming effective relationships with other people, due in
part to an inability to properly interpret facial expressions or emotions. Children with
autism spectrum disorders may be resistant to cuddling or change, and they may play
alone or have delays in speech development. People with autism also frequently repeat
body movements or have extreme attachments to certain objects. However, there are
positive aspects to autism, such as the fact that many people with autism excel on
certain mental levels, such as counting and measuring, or at art, music, or memory.
The precise causes of ASD are not known. However, it is known that genetic factors
play a role in ASD. It is also known that non-genetic, environmental factors play a role in
the development of ASD. It is thought that ASD is the result of a combination of genetic
and non-genetic factors. What basically happens is that non-genetic, environmental
factors come into play to make those who are genetically susceptible to ASD more likely
Nursece4less.com 6

to develop ASD. ASD may then develop gradually, or the individual may experience
what is known as regression, where he or she may lose some or all of their acquired
skills. The loss of skills can happen suddenly or gradually. Overall, there are a number
of risk factors for ASD, including gender – boys are more likely than are girls to develop
ASD – genetics, certain prenatal and perinatal factors, neuroanatomical abnormalities
such as enlargement of the brain, and environmental factors.
There is no cure for ASD. The primary goals of ASD treatments are to lessen deficits
and to lessen family stresses. There are a number of ways to do these things, including
applied behavioral therapy, structured teaching, speech and language therapy, social
skills therapy, occupational therapy, and the use of medication. Additionally, educating
parents, caregivers, and siblings and providing these individuals with ways to cope with
the unique challenges that having an individual with ASD in the household brings helps
in alleviating the inevitable resulting family stress.
INCLUDED DISORDERS
AutismThe American Psychiatric Association has put forth a
new definition for autism as a part of the revisions made
for the new Diagnostic and Statistical Manual of Mental
Disorders (DSM). Autism will be seen as part of a
continuum of disorders termed autism spectrum disorder,
involving a range of disorders, such as autistic disorder,
Asperger’s syndrome, childhood disintegrative disorder,
and pervasive developmental disorder not otherwise specified. Dr. James Scully of the
APA has stated that the criteria will “lead to more accurate diagnosis and will help
physicians and therapists design better treatment interventions” [8].
Autistic disorder is also known as autism or mindblindness. This disorder generally
presents sometime in the first three years of life, and the child appears to live within its
own world. The child also appears to show little interest in other people and displays
Nursece4less.com 7
[7]

poor social skills. The focus of a child with autistic disorder is on a consistent routine,
with repetitive odd or peculiar behaviors. Children with autism frequently have problems
communicating, and they often will avoid making eye contact with others or will avoid
attaching to others.
Autistic disorder may be associated with a number of infirmities, including difficulties
with motor coordination and attention, intellectual disability, and physical health issues
such as gastrointestinal issues or sleep issues. However, despite difficulties, some
people with autistic disorder often excel in music, art, math, or with visual skills.
Autistic disorder seems to have roots in the early development of the brain, although the
most obvious signs and symptoms emerge between 2 – 3 years of age. Approximately
1 out of every 88 children in the United States will have an ASD; this has been a huge
increase in prevalence over the past 40 years. The increase is due in part to
improvements made in diagnostic tools as well as disease awareness. Another reason
for the increase may be environmental influence. Autistic disorder is much more
common in boys than it is in girls: approximately 1 out of every 54 boys and 1 out of
every 252 girls is diagnosed with an ASD in the U.S., with ASD affecting over 2 million
individuals in the U.S., and millions are affected worldwide.
There is no one cause for ASD, although a genetic predisposition appears to play a
role, as do environmental, or non-genetic, factors. Most cases of ASD appear to be the
result of a combination of both genetic and non-genetic factors, with environmental
stressors increasing the risk of development of ASD in children who already have a
genetic predisposition. The clearest evidence of these types of risk factors includes
events that happen before or during birth, such as maternal illness or birthing difficulties.
Asperger Syndrome
Asperger Syndrome is considered a sub-type of autism spectrum disorder. The cause of
Asperger Syndrome is unknown, and presents 4 times more frequently in boys than it
does in girls [9].
Nursece4less.com 8

Many consider Asperger syndrome to be the mildest form of autism; therefore, many
with Asperger’s are considered to be the highest functioning autistic individuals.
However, even though many individuals with Asperger’s may be high functioning, they
still share certain key symptoms with others who suffer from autism spectrum disorders,
such as a lack of normal social conversation, lack of normal eye contact, deficits in body
language and facial expression, and difficulties in maintaining social relationships.
Those with Asperger syndrome also frequently engage in repetitive behaviors and may
become excessively attached to objects or routines.
The prevalence of Asperger syndrome is not well known. It is not even well recognized
prior to the age of 5 or 6, primarily because the individual has normal language
development. Asperger syndrome occurs in all ethnic groups and affects every age
group [10]. Additionally, it does not just affect the child during childhood; studies indicate
that children who suffer from Asperger syndrome carry their problems with them into
adulthood and some develop further psychiatric problems in adulthood.
Some of the common signs or symptoms of those with Asperger syndrome are having
monotone speech or lack of rhythm in speaking. Additionally, an individual with
Asperger syndrome may have problems modulating the volume in his or her voice and
may need to be continually reminded to talk more softly. Individuals with Asperger’s are
not generally isolated from the rest of the world as a result of their own withdrawal, but
rather they are isolated because they have poor social skills or because their interests
are narrow. For example, they may approach conversations by speaking only about
their own very narrow interests, making a normal conversation difficult.
Current research [10] indicates that brain abnormalities may be to blame, as some
research has indicated that those children who have Asperger syndrome have
differences in structure and function than do those children who are not affected.
Researchers posit that these differences could be caused by an abnormal migration of
embryonic cells that in turn affects brain structure in early childhood. This then goes on
to affect the brain circuitry that affects thought and behavior. Scientists have also
suspected that there is a strong genetic component to Asperger syndrome, although no
Nursece4less.com 9

specific gene for Asperger syndrome has ever been identified. Recent research has
indicated that Asperger syndrome is most likely the result of a grouping of genes in
which variations or deletions cause the individual to become vulnerable to the
development of Asperger syndrome. When combined with environmental factors, this
also determines the severity and the specific symptoms that each individual suffers.
Pervasive Developmental Disorder Not Otherwise Specified (PDD-NOS)
Pervasive Developmental Disorder Not Otherwise Specified (PDD-NOS) is sometimes
simply called pervasive developmental disorder, or may be used interchangeably with
autism spectrum disorder. There are some health professionals who refer to PDD-NOS
as sub threshold autism. PDD-NOS is a relatively new diagnosis, having been around
for only about 15 years. PDD-NOS is the diagnosis that has come to be commonly
applied to those who are on the autism spectrum but do not generally meet the criteria
for some other autism spectrum disorder in full, such as Asperger Syndrome.
Defining features of PDD-NOS are challenges in language development and social
functioning. Repetitive behaviors are frequently seen with PDD-NOS. Not all children
with PDD-NOS have the same symptoms. Symptoms may sometimes be mild, where
the individual exhibits only a few symptoms while at home or at school. Other
individuals may exhibit severe symptoms in all areas of their lives but still may not
qualify for a diagnosis of autistic disorder.
The signs and symptoms of PDD-NOS are divided into several categories, as outlined
below:
Social Signs and Symptoms:
Children with PDD-NOS have a desire to make and have friends, but they have
no idea how to make that happen. If there are language delays this may hinder
the ability to socialize with other people. There is frequently difficulty in
understanding body language, tone of voice, and facial expression in others, as
well as difficulty understanding emotions. Children with PDD-NOS often have
trouble distinguishing between emotions such as sadness, happiness and anger.
Nursece4less.com 10

Communication Signs and Symptoms:
Those with PDD-NOS frequently have language or communication issues. Those
with PDD-NOS may not babble as babies. They also frequently take language
literally and do not have an understanding of things such as sarcasm or joking
language. It is easier to expand language skills in those children who have some
language skills than it is in those children who are entirely nonverbal.
Behavioral Signs and Symptoms:
Children with PDD-NOS may exhibit tantrums or emotional outbursts. These
children may also have a great need for routine. Additionally, individuals with
PDD-NOS can often misinterpret what is happening in a situation and in turn
become easily frustrated. Tantrums are the result of fear and anxiety. Another
common behavioral symptom is perseveration, which means the child will tend to
dwell on certain events or subjects. Individuals with PDD-NOS may become
fixated on one topic or play only with one toy that is associated with a particular
area.
Given the newness of this diagnosis, there has been some disagreement on how to
apply a diagnosis of PDD-NOS. Recently, some studies [11] have suggested that PDD-
NOS may best be utilized by placing individuals into one of three subgroupings of
diagnosis, as explained below:
High functioning PDD-NOS:
This involves approximately 25% of those with PDD-NOS); and, these individuals
generally have symptoms that overlap Asperger’s, but they may differ slightly in
that they have delays in language development or slight cognitive impairment.
Mid-function PDD-NOS:
This involves approximately 25% of those with PDD-NOS; and, these individuals
generally have symptoms that resemble those with autistic disorder.
Nursece4less.com 11

Low function PDD-NOS:
This involves approximately 50% of those with PDD-NOS; and, these individuals
meet all of the criteria for autistic disorder, however, some of their symptoms are
noticeably mild.
Another way to diagnose PDD-NOS may be by placing individuals into one of five
subgroupings [12]:
Atypical autism: this category is for young children who may not have developed
a full-blown autistic disorder yet; these are individuals who almost, but not quite,
meet the criteria for autistic disorder.
Residual autism: this category is for individuals who have a history of having
autistic disorder yet may not at present meet the criteria; they therefore still have
some autistic features but as a result of interventions or development they do not
meet the criteria for autistic disorder.
Atypical Asperger syndrome: this category is for young children who may not
have developed full-blown Asperger syndrome as well as for individuals who are
almost, but not quite, to the point of meeting the full criteria for Asperger
syndrome.
Mixed clinical features of atypical Asperger syndrome: this category is for
children with an atypical autistic disorder.
Comorbid autism: this category is for children who have a medical or neurological
disorder, such as tuberous sclerosis, that is associated with some ASD-like
features.
Those who have PDD-NOS respond best to combined therapies. Therapies that have
been demonstrated to work well on PDD-NOS are applied behavioral analysis (ABA),
sensory integration therapy, play therapy, and social skills training. It is important for the
practitioner to pay attention to the child who may not be as easily diagnosed; the Yale
Developmental Disabilities Clinic [13] indicates that children who have PDD-NOS may
not get the treatment they need as easily as do those diagnosed with autistic disorder.
Additionally, many education systems in the United States do not have a special
education category for those individuals who have PDD-NOS, leaving these individuals
Nursece4less.com 12

to be placed into programs designed for students with other problems, such as
intellectual disabilities, emotional disturbances, or behavior disorders. This can lead to
the individual getting lost in the crowd and not having their needs met. It is therefore
essential that the practitioner work closely with parents and caregivers to ensure that
the individual with PDD-NOS is getting his or her needs met in all areas.
Childhood Disintegrative Disorder
Childhood disintegrative disorder (CDD), also called Heller’s syndrome, is a condition
wherein children develop normally until approximately age 3 or 4. They then lose all of
the skills they have learned. This includes motor, language, social, and other skills. To
be diagnosed with CDD the child must lack or lose normal function in at least two
developmental skills areas that include: social interaction, communication, and repetitive
or stereotyped patterns of interest and behavior/activities. CDD may be caught at
developmental screenings performed at well-child check-ups; these screenings should
always be performed, although parents should also be encouraged to voice concerns
about their child’s development at other times as well. The cause of CDD is not known,
but a link to the brain and nervous system has been made [14].
Symptoms of CDD include the following: a delay or lack of language, impaired
nonverbal behavior, an inability to start or to maintain conversation, failure to play, loss
of control of the bladder or bowels, loss of previously established language or
communication skills, loss or motor or skills, and; problems forming relationships with
others have been identified. The loss of skills may occur abruptly or it may occur over a
period of time that is extended. Parents should express concerns to a practitioner when
a child loses any developmental skill, whether it is gradual or sudden loss.
Outcome for CDD is poor. Many children with CDD are as severely impaired as those
with severe autistic disorder. Those with CDD almost always need support for the
duration of their lifetime and may need residential care in facilities such as group homes
or long-term care residential living. There is no cure for CDD, although there are some
Nursece4less.com 13
treatments that may be used to lessen or relieve symptoms. These treatments include
the following:
Medication:
While there are not any medications that treat this disorder directly, some
medications may be used to treat the behaviors that result, such as anxiety or
depression. Additionally, epilepsy is highly co-occurring with CDD, and
anticonvulsant drugs may be utilized to control seizures.
Behavior therapy:
Behavior therapy programs are frequently utilized to help the individual with ASD
learn language or to help minimize language loss, as well as social skills and
self-care skills. Behavioral therapy programs use systems of reward and
discipline to reinforce behavior that is desirable and to discourage behavior that
is not desirable. It is important that the approach in behavior therapy is consistent
among all practitioners, caregivers, and teachers.
Rett Syndrome
Rett Syndrome is a neurodevelopmental disease that is seen almost entirely in females,
although it may sometimes rarely be seen in males. Rett Syndrome presents in infancy
or early childhood, and is caused by a mutation in the MECP2 gene on the X
chromosome [15]. Since boys have a different combination of chromosomes than do
females, males who have the mutation that causes the syndrome are generally affected
in ways that are devastating. Many die prior to birth or very early in infancy.
Symptoms vary in type and severity. Generally the child may appear to be developing
normally, up until about 6 months of age, and then symptoms begin to appear. This is
also when the rate of growth of the head as well as progress of certain skills such as
communication may start to slow. The most notable changes usually occur at around 12
– 18 months and occur over weeks to months. There are a number of signs and
symptoms that occur with Rett syndrome, including those listed below:
Slowed growth: the brain slows in growth following birth. One of the first signs
that a child has Rett syndrome is that the child has a smaller than usual head
Nursece4less.com 14

size. Then, as the child ages, it becomes evident that there are delays in growth
in other body parts as well.
Loss of normal coordination and movement: the individual begins to lose a
significant amount of motor skills. This generally begins between 12 to 18 months
of age and includes a decreased ability to control the hands as well as a
decreased ability to crawl and walk in a normal way. This occurs rapidly at first
and then continues in a more gradual manner.
Loss of communication and the ability to think: individuals who have Rett
syndrome will lose their ability to communicate as well as to speak. They may
also become uninterested in toys, in people, and in their surroundings. The
change may be rapid in some children; for example, some children may
experience a sudden loss of their speech skills. Most children regain skills such
as eye contact over time as well as develop skills such as nonverbal
communication.
Abnormal hand movements: children who have Rett syndrome have stereotyped
hand patterns individual to each child; these may include wringing, clapping,
rubbing, squeezing, or tapping.
Unusual eye movements: those with Rett syndrome may have eye movements
that are unusual, such as blinking, staring intensely, or closing one eye.
Breathing problems: individuals with Rett syndrome may have breathing
problems that include apnea, forceful exhalation of air (or saliva), or rapid
breathing that is abnormal. These types of problems are likely to occur during
waking hours but not during sleep hours.
Irritability: Rett syndrome may cause individuals to become more and more
irritable and agitated as they age, having spells of screaming that can begin
suddenly and last for hours.
Abnormal behaviors: abnormal behaviors may include sudden and odd facial
expressions or extended bouts of screaming or laughter that occurs for no
reason. Abnormal behaviors also include such behaviors as hand licking or
grasping clothing or hair.
Nursece4less.com 15
Seizures: many who have Rett syndrome also experience seizures at some point
in their lifetime. The symptoms of these seizures vary, but they can range from
having a periodic muscle spasm to being struck with full-blown epilepsy.
Abnormal spinal curvature: this is also known as scoliosis. Scoliosis commonly
co-occurs with Rett syndrome, and generally begins at around 8 – 11 years of
age.
Irregular heartbeat, or dysrhythmia: many individuals with Rett syndrome
experience this life-threatening issue.
Constipation: constipation is a common issue for those who suffer from Rett
syndrome.
Rett syndrome is generally divided into 4 stages:
Stage I: In this stage the signs and symptoms of the disease may be easily
overlooked, as this stage begins between 6 – 18 months of age. Children who
are in this stage may begin to show less eye contact or begin to lose interest in
their toys. There may also be delays in sitting up or in crawling.
Stage II: Stage II occurs between 1 – 4 years of age. In this stage the child
begins to lose his or her speaking ability as well as the ability to use his or her
hands. Additionally, repetitive and purposeless hand motions begin. Some
children also start to hyperventilate or hold their breath as well as cry or scream
for no reason. It is also frequently difficult for the child to move on his or her own.
Stage III: Stage III is considered a plateau that starts between 2 – 10 years of
age. This stage may last for years. Even though issues with movement may
continue, behavior can improve. Children in this stage frequently cry less often,
and become less irritable.
Stage IV: This last stage shows extremely reduced mobility as well as muscle
weakness and scoliosis. Communication skills, understanding, and hand skills
usually won’t decline any further in this stage.
Most people who suffer from Rett Syndrome require daily assistance with everyday
tasks. They can usually live moderately long lives, extending to 50 years of age or
longer.
Nursece4less.com 16
EARLY ETIOLOGY
The precise causes of ASD are not known. However, many think that it is a complex
combination of genetic and environmental components that cause ASD symptoms.
ASD causes may be described in two ways: [16]
Primary ASD, which is also known as idiopathic ASD. This means that there is no
underlying medical condition, which can explain why there are symptoms of ASD.
Ninety percent of all ASD cases are primary ASD.
Secondary ASD, which means that there is an underlying medical condition that is
thought to be responsible – or at the very least, partially responsible – for the ASD
symptoms. Ten percent of all ASD cases are secondary ASD.
Primary ASD
Researchers have examined four possible causes to primary ASD. These causes are
outlined below:
Genetic causes:
There are certain genetic mutations, which may lead to a child being more likely to
develop ASD. ASD has been known to run in families, and there is 5 – 6% likelihood
that younger children born into families with an older child with ASD will also themselves
have ASD. Identical twins are also at risk for developing ASD. For example, if one twin
develops ASD, there is 60% likelihood that the other will develop ASD as well. However,
it is important to note that there are currently no specific genes that have been linked to
the development of ASD, and there is no way to currently test for the genetic
predisposition toward ASD.
Environmental causes:
A child may be exposed to certain environmental factors during the mother’s pregnancy
that may lead to the development of ASD. Some researchers think that ASD is caused
Nursece4less.com 17

more by environment than by genetics, and that certain people may be born with a
predisposition toward ASD that is only triggered if exposed to certain environmental
stimuli. Some of the suggested environmental stimuli include: a mother who had a viral
or bacterial infection while pregnant; a mother who smoked while pregnant; an older
father; air pollution; and, pesticide exposure.
There is evidence to support some of these environmental factors. For example, women
who were exposed to the rubella infection while they were pregnant have a 7% risk of
giving birth to a child who develops an ASD. Additionally, women who smoked while
pregnant were 40% more likely to have a child who developed an ASD. Also, fathers
over 40 years of age were 6 times more likely to have a child who developed an ASD.
Researchers posit that this may be the case because a father’s genetic material
becomes more vulnerable to mutation as he ages. There is less evidence to support the
idea that air pollution or pesticide exposure causes the development of ASD; however,
studies are currently examining this idea under the CHARGE study [16].
Psychological causes:
A child may have thought processes that contribute to the expression of symptoms of
ASD. A great deal of the research behind the psychological factors that may contribute
to ASD is rooted in a psychological concept called “theory of mind” (TOM) [16]. TOM is
an individual’s ability to understand others’ emotional states; and, at its core involves
seeing the world through the eyes of the other person. The majority of children who do
not have ASD possess a full understanding of TOM by the time they are approximately
4 years of age. Children who have ASD possess a limited or no understanding of TOM.
This may be one of the causes of the social problems that children with ASD
experience.
Neurological causes:
There are certain problems with how the brain and nervous system develops that may
contribute to ASD symptoms. A great deal of the research into neurological causes has
Nursece4less.com 18

focused on the amygdala, which is the section of the brain that matches emotions to the
situation the individual is placed in. The amygdala selects emotional responses from the
limbic system and relays them to the cerebral cortex.
Brain studies that have been conducted on people with ASD indicate that the
connections between these systems are not fully functional. The result is that people
with ASD can suddenly experience extreme emotional reactions even to trivial objects
or events. This may explain why people who have ASD favor routines, since routines
and patterns tend not to promote extreme responses. An additional area of research
has been focused on mirror neurons, which enable an individual to mirror another
individual’s actions. For example, a mirror neuron is what allows a baby to smile in
reaction to a mother’s smile. Mirror neurons create more elaborate pathways in the
brain that may contribute to higher brain functions such as language, learning from
others, and the ability to recognize emotional states in others as an individual grows
older. Studies of children with ASD have discovered that mirror neurons in ASD
individuals do not respond in the ways they do those without ASD. Difficulties with
mirror neurons may contribute to the problems that some individuals with ASD
experience with learning and social interaction.
Secondary ASDSometimes another medical condition may be the cause of ASD. Some of these
conditions that can cause symptoms of ASD are listed below:
Fragile X syndrome:
This is an uncommon condition that occurs more frequently in boys than it does in girls.
It occurs in about 1 in every 3600 boys, and in about 1 in every 6000 girls [16], and
presents with certain distinct characteristics such as a long face, larger ears, and
flexible joints.
Tuberous sclerosis:
Nursece4less.com 19

This is a rare condition that results in multiple tumors to grow throughout the body. The
tumors are not cancerous. This condition occurs in approximately 1 in every 6000
children.
Rett syndrome: This condition, also discussed above, is included here as a rare
secondary ASD and almost always occurs in girls. It causes extreme difficulty with
physical movement, and the individual suffering from Rett syndrome nearly always
requires full assistance with daily tasks. Approximately 1 in every 20,000 girls has Rett
syndrome.
RECENT CHANGES TO THE DSM-V
There have been several refinements made to the diagnostic criteria found in the
Diagnostic and Statistical Manual (DSM), with suggestions based on limitations found in
previous diagnostic criteria [1]. The fourth edition of the DSM (DSM-IV) contained a large
number of diagnoses [17], including a large number of not otherwise specified (NOS)
diagnoses. Additionally, practice has changed in recent years to include the
consideration of the contribution of various comorbidities.
Autism Spectrum Disorders in the DSM-V
ASD in the DSM-V is an umbrella term that will include such disorders as pervasive
developmental disorders, autistic disorder, Asperger syndrome, childhood disintegrative
disorder, and not otherwise specified disorders. ASD’s will consist of these groups of
developmental disorders that are seen on a continuum that ranges from mild to severe
and present in infancy or early childhood. However, in the new DSM-V, the age criteria
for diagnosis will be different; it will not be specified that diagnosis must occur during
childhood and that diagnosis may occur later on in life. Because caregivers might
compensate for a child’s lack of social intelligence, in school and other social
interactions, a diagnosis of ASD might not be made until later in the child’s life.
Onset of ASD has been extensively studied [2-4], and it is accepted by the majority of
practitioners that diagnosis may occur much later than the time the disorder begins
Nursece4less.com 20

presenting itself. Additionally, parents and caregivers do not always acknowledge
symptoms immediately as signs of a problem, and the time at which they acknowledge
symptoms is important as well. It is not always easy to detect specific signs and
symptoms of ASD, particularly the early ones [5]. This aspect of ASD is, in particular,
important to the changes in the new DSM-V because onset of symptoms prior to age 3
has been removed. The deletion of the age criteria in the diagnosis of ASD in general
highlights the fact that some individuals are diagnosed later in life, as adolescents or
adults.
It has been suggested that the presence of language delays not be utilized as criteria
for applying a diagnosis of autistic disorder. This is because it has been well established
that a language delay is not a symptom that is specific to ASD. Further, children who
suffer from ASD may develop fluency of speech as they grow even if they suffered from
language delay as a younger child. However, it is important to note that the
development of language is crucial where it regards outcome because a severe
language delay in early childhood seems to predict poor outcome [18].
Considerations regarding specific disorders in the DSM-V are outlined below:
Asperger disorder:
A highly debated change to the revision of the DSM-V is the suggestion to remove
Asperger syndrome. However, the suggestion to remove Asperger syndrome is based
on study evidence that indicates that there is no clear difference between Asperger’s
and autistic disorder where outcome is concerned [1].
Disintegrative disorder:
While the validity of disintegrative disorder has been debated recently, the debate
focuses on the problems that stem from precisely defining developmental regressions
as well as pinpointing the time of onset of the regression. Additionally, there is the
problem of defining whether developmental delays were present prior to regression.
Further, consideration has been given to whether symptoms or changes present
Nursece4less.com 21

gradually or suddenly. Due to these ambiguities, the DSM-V therefore suggests removal
of the category of childhood disintegrative disorders.
A goal of this new criterion is to stabilize validity of diagnostic criteria across types of
ASD. Earlier studies have indicated that various types of ASD are not easily
distinguishable from one another [19, 20], which was supported by a recent review [21],
which concluded that criteria for various types of ASD indeed overlap. One study [22]
indicated that this led to differing definitions between such disorders as autistic disorder
and Asperger syndrome between assessment sites, which compromised diagnostic
validity. The conclusion was that distinctions between various types of ASD’s are often
dependent upon the severity of symptoms such as the presence of a learning disability
or language skills. Utilizing an umbrella term such as autistic spectrum disorders helps
place symptoms on a continuum and provides one clear, concise defining term,
therefore preserving diagnostic validity. The major goal of changes to the diagnostic
criteria in the new DSM-V is to make criteria for ASD’s more clear as well as increase
validity of diagnosis.
CHARACTERISTICS OF ASD
Social deficits
Infants and children with ASD are
different from typical infants when it
comes to social development [24].
Typically developing infants are very
social. They gaze toward faces, turn
toward speaking voices, grasp
fingers extended towards them, and
smile by the time they are 2 – 3
months old. Conversely, children
who develop ASD have difficulty with
social interactions with other human
Nursece4less.com 22
[23]

beings. By 8 – 10 months of age, infants who go on to develop ASD are generally
showing some symptoms such as the failure to respond to their names, a reduced
interest in other people, and a delay in babbling. By the time they are toddlers, many of
these children have difficulties playing socially with other children. Additionally, they
don’t imitate others and they often prefer to play on their own instead of with other
children. They may not seek comfort from parents or caregivers as well as show a
failure to respond to anger or affection in ways that are typical.
Research has indicated that children with ASD are attached to caregivers. However, the
way this attachment is expressed is often unusual, and caregivers frequently interpret
the child’s expressions as disconnected or emotionless. It is important to remember that
both children and adults who suffer from ASD have difficulty determining what others
are thinking or feeling. Where children who develop normally learn to accurately
interpret such social cues as smiling, waving or grimacing, these social cues hold little
meaning for the individual who suffers from autism. Individuals with ASD also have
difficulty seeing things from another person’s perspective, meaning that they have little
empathy. While most normally developing five year olds have learned to see things from
another person’s perspective, the person suffering from ASD has not learned this skill,
leading to poor understanding. This may interfere with an ability to predict or understand
actions as well as lead to an inability to understand why another person is feeling the
way they are feeling.
Finally, it is common for individuals who suffer ASD to have difficulty regulating their
emotions. They may come across as emotionally immature, having crying outbursts or
displaying emotions that are inappropriate for the situation. They may also be disruptive
or physically aggressive. These expressions may be particularly pronounced if the
individual with ASD is feeling overwhelmed or frustrated, and can lead to self-injurious
behaviors such as biting or head banging.
Nursece4less.com 23
Communication difficulties
Infants and children with ASD are different from typical children when it comes to
communication [24]. The majority of children pass predictable milestones to learning
language by 3 years of age. The earliest of these is babbling; and, by the age of 1, most
typically developing children will say a few words, acknowledge their names, and point
to or display objects they want. Additionally, children of this age have the ability to
communicate clearly either through sounds or expression when they do not want
something that is given to them. Conversely, children suffering from ASD generally
experience delayed babbling and speaking and may also experience delays in learning
how to utilize gestures to indicate their preferences. Some individuals who develop ASD
may possess these abilities early on and then lose them. Others experience delays and
then gain language ability later on in life.
With therapy, many with ASD do learn how to use spoken language and all with ASD
can learn how to communicate in some way, either verbally or nonverbally. Those who
communicate nonverbally or nearly nonverbally learn to use systems such as pictures,
sign language, word processors, or devices such as speech-generators.
When language does begin to develop, an individual with ASD may utilize speech in
ways that are unusual. For example, some individuals have difficulty forming complete
or meaningful sentences. They may speak single words or phrases or repeat the same
word or phrase over and over again. Others may experience a stage where they repeat
everything they hear word for word, a condition called echolalia. There are others who
have difficulty sustaining conversation despite developing large vocabularies. Still
others carry on long monologues on favorite subjects, giving those listening little
opportunity to respond and having little understanding of the give and take of social
conversation.
Another common communication difficulty is the inability to interpret body language and
tone of voice. For example, sarcasm is particularly difficult for those with ASD to
interpret. An individual who has developed normally may accurately interpret the
sarcasm in a comment such as “Oh, that’s just great!” whereas the individual with ASD
Nursece4less.com 24

would miss it and interpret the comment as referencing something that actually is just
great. The individual with ASD may also not exhibit typical body language himself or
herself. For instance, their body language may not match what they are saying.
Tone of voice may not reflect the emotion and individual with ASD is trying to convey.
Some individuals suffering from ASD utilize flat or robotic sounding voices. These
displays make it difficult for others to understand what individuals with ASD need or
want. This failure in communication can in turn lead to frustration and inappropriate
displays made by the person suffering ASD, such as screaming or grabbing.
Stereotyped or repetitive behaviors and interests
Infants and children with ASD are different from typical children when it comes to
behaviors and interests [24]. Individuals who develop ASD generally engage in repetitive
behaviors as well as have a tendency to engage in a range of activity that is tightly
restricted. Common repetitive behavior includes hand flapping, jumping, rocking,
twirling, arranging or rearranging objects, and the repetition of sounds, words, or
sentences. Occasionally the repetition involves behaviors such as wiggling the hands or
fingers.
Restrictive activities can be clearly seen in the ways children with ASD play with their
toys. Instead of actually playing with their toys, these children will often spend hours
lining the toys up in a specific order. In adults this is seen in the way the individual is
preoccupied with having certain objects lined up in a certain order. Repetitive behavior
may be intensely obsessive and very unusual. It can take any form, including unusual
content or knowledge. This is why some individuals with ASD develop extreme interest
and knowledge of numbers or scientific topics. Individuals with restrictive activities can
become extremely upset if someone or something disrupts the order of their things. This
shows how essential consistency is for many individuals with ASD. Even the slightest
changes in environment or routine can prove very stressful for individuals suffering from
ASD and may lead to outbursts.
Nursece4less.com 25

Individuals with ASD may have many different obsessions or behaviors, however there
are some that are particularly common among those with ASD. Activities where these
behaviors become notable include: identifying historical dates and events, computers,
certain television programs, trains, and science. Children with ASD in particular like
playing with toys such as Thomas the Train and dinosaurs. Older individuals with ASD
may develop repetitive obsessive interests with things like car registration numbers,
traffic lights, shapes, or body parts. Individuals with ASD are also frequently quite
interested in collecting objects; this may be collecting something that seems quite
common, such as a certain toy, or something that seems uncommon, such as leaves.
What marks the behavior as unusual is the duration and intensity that the person with
ASD shows. People with ASD will frequently learn a great deal about the thing they are
obsessed with, be intensely interested in it for an extended period of time, and feel very
strongly about the object or objects in question. There are a number of reasons that
people with ASD develop obsessions, including the fact that obsessions help provide
structure and order, obsessions offer a way to start conversations when social
interactions prove difficult, obsessions help the individual relax or feel happy, and
obsessions offer enjoyment and the opportunity to learn.
Repetitive behaviors can include arm and hand flapping, finger flicking, rocking,
jumping, twirling, spinning, head banging, and more complex body movements.
Repetitive movements also include the repetitive usage of an object, such as the
repetitive flick of a rubber band or repetitively stroking a piece of fabric. Many individuals
with ASD have what is called sensory sensitivity; this means that they are over or under
sensitive to sights, smells, touch, sounds, and tastes. Their balance and body
awareness may also be affected by this sensitivity, and the repetitive behavior is a way
to deal with the sensitivity. There are a number of reasons that people with ASD utilize
repetitive behavior, including attempts to obtain or reduce sensory input, finding ways to
deal with anxiety or stress, or as a way to obtain enjoyment or to occupy one self.
Routines and sameness are also important for the individual with ASD. Routines are
important because they bring order and predictability to the individual’s life and help to
Nursece4less.com 26

manage anxiety. Repetitive behaviors and obsessions offer routine and order to the
individual who suffers from ASD. However, the need for repetition and routine and order
may extend beyond repetitive behaviors. Some individuals with ASD may have issues
with changes such as those to their physical environment. For instance, if a chair is
moved in a room or a new person enters the room, this could be difficult for some
individuals with ASD to handle. Some individuals with ASD may also have very rigid
preferences when it comes to things such as food. For example, they may only eat food
that is a certain color or begins with a certain letter of the alphabet. This may extend to
other areas of life, such as clothing (for example, only wearing clothing made of certain
fabrics) or even to everything objects (for example, only utilizing certain brands of soap
of toilet paper).
Some individuals with ASD may also develop a need to have a routine around daily
activities such as bedtime or meals. These routines may become nearly ritualistic.
Verbal rituals in addition to physically repetitive behaviors may also be seen in the
individual with ASD; and, they may repeat the same question over and over again or
need to hear a specific answer repeatedly. There may also be compulsive behavior in
addition to obsessive behavior that is developed. This means that the individual may do
things like wash their hands or check locks constantly. This behavior is not the same as
having obsessive-compulsive disorder (OCD), although it strongly mirrors it.
Cognitive delays
Children with ASD are different from typical children when it comes to cognitive
development [25]. While cognitive abilities vary, a great many children who have ASD
also have some level of mental retardation. About 75% of people who have ASD have a
non-verbal IQ that is below 70, although ASD may also occur in individuals who are of
normal or high intelligence. There are some children with ASD who also have a high
level of giftedness in a certain area, such as art, music, or math. However, this category
or individuals typically referred to as savants is typically very small and is estimated to
comprise less than 1% of ASD children [25]. If a child with ASD has abilities such as
these they usually manifest by the age of 10.
Nursece4less.com 27

Children with cognitive delay often present with other delays as well. They also miss
general developmental milestones, particularly the following [26]:
Speaking their first words, generally at age 10 – 18 months
Responding to simple instructions, exploring on one’s own, utilizing trial and
error, generally at age 12 months
Walking without aid, generally at age 12 – 18 months
Naming body parts, generally at 18 months
Utilizing phrase speech, generally before the age of 24 – 30 months
Some studies indicate that cognitive delays may be in part the result of drug usage. One
study, the Neurodevelopmental Effects of Antiepileptic Drugs (NEAD), confirmed that
fetal exposure to the drug valproate impairs a child’s IQ well into childhood [25]. This
study was conducted on 310 pregnant women in the United States and the United
Kingdom, with the purpose being to determine if there were differential long-term
neurodevelopmental effects across four frequently utilized drugs: carbamazepine,
phenytoin, lamotrigine, and valproate. Researchers indicate that the use of valproate
during pregnancy led to significant cognitive effects in children, with the child IQ being 8
– 11 points lower (as compared with the other drugs). Valproate was therefore
considered a very poor choice for women who were of childbearing age. While these
results seem to indicate one possible culprit of cognitive delay in those with ASD, further
study is needed to determine how drugs could be contributing to cognitive delays.
A child with ASD may also experience additional mental health conditions or learning
disabilities. For example, they may experience attention difficulties, problems controlling
emotions, or have difficulties learning. There may also be mood or anxiety disorders
present. For example, children with ASD sometimes suffer specific phobias in addition
to ASD. It is also important to note that medication that is utilized to treat symptoms may
affect a child with ASD cognitively. For example, children with ASD who also have
attention deficits do not respond predictably to stimulant medications (i.e.
methylphenidate) that may be prescribed for children with attention deficit disorder.
Keeping in mind that medication may affect the ASD child in unpredictable ways allows
for customization of treatment protocol.
Nursece4less.com 28
ASSOCIATED FEATURES OF ASD
Genetic disordersOne of the biggest advances in understanding the pathophysiology of ASD has been
appreciating the significance of the contribution genetics makes to the etiology of ASD.
There are three main areas of evidence that support this genetic contribution: twin
studies, which compare monozygotic twins (MZ) and dizygotic twins (DZ); family
studies, which compare the rates of ASD in the first-degree relatives versus the general
population; and, studies of genetic syndromes that also co-occur with a diagnosis of
ASD [27]. Each of these will be addressed in turn in the following sections.
Since MZ twins share 100% of genetic material, and DZ twins share 50% of genetic
material (which is similar to siblings who are not twins), and both of these types of twins
share an environment in utero, the higher disease occurrence in MZ twins as opposed
to DZ twins supports the genetic etiology. This has been supported in more than one
twin study and is overall consistent with estimates of heritability at around 70 – 80% [28,
29]. Studies in families indicate that first-degree relatives of those who are autistic have a
marked increased risk of developing ASD as compared to those in the general
population. This is consistent with the strong familial, genetic tie that was observed in
the twin studies [30]. This is not to say that environment does not play a role, but rather
to display that genetics also plays an important role as well. Further, first degree
relatives of those with ASD display an increase in the behavioral and cognitive features
that are associated with ASD, such as language deficits or autistic-like social
impairments [31]; however these often manifest in lesser forms. This is as compared to
the general population [32].
It has also been common knowledge for several decades that there are a number of
medical and genetic conditions that are associated with ASD. For instance, conditions
such as Joubert syndrome, Smith-Lemli-Opitz syndrome, Tuberous Sclerosis, and
Fragile X are all known to cause ASD, although many of these with a lower than 50%
penetrance [33, 34]. Many genes have been identified for ASD; however, few of these
Nursece4less.com 29

genes are specific to ASD but instead contribute to a genetic risk for an associated
disorder that causes ASD.
EpilepsyEpilepsy is very common in those who suffer from ASD, and increasingly, practitioners
are recognizing it as a problem that must be dealt with in addition to the problems that
come with an ASD diagnosis. Approximately 20 – 30% of those who suffer ASD will
develop epilepsy by the time they become adults [35]. However, actual rates of
comorbidity vary with age and the type of disorder.
Major risk factors for occurrence of a seizure are mental retardation as well as the
presence of additional neurological disorders [36]. Therapeutic approaches to epilepsy in
ASD include conventional treatments; however, should seizures not be evident, there is
controversy as to what treatments should be utilized. Anticonvulsant medication may
interfere with moods or behaviors, and disturbances in moods and behaviors are often
observed in those patients with ASD. There is currently limited understanding regarding
the link between ASD and epilepsy; however, from a clinical standpoint this link should
not be dismissed.
Intellectual disordersRecent findings [37] indicate that those with ASD also have a high prevalence of
intellectual disorders. Intellectual disabilities are characterized by cognitive, social, and
adaptive deficits, leading to the co-occurrence with other disorders, such as ADHD,
mood disorders, and catatonia and repetitive behaviors, which further complicate
matters. These problems may be problematic not only for the individual suffering from
the disability but also for parents, caregivers, and providers. The disorder may be so
severe as to be debilitating [38].
Matson [39] divides individuals into three distinct groups: those with intellectual disability
(ID), those with ASD, and those with both ASD and ID. Matson states that it is important
for the practitioner to know which type of person he or she is treating, as that will
Nursece4less.com 30

determine the best course of treatment. For instance, an individual with both ID and
ASD will have different needs than the individual who only has ASD.
The combination of intellectual disorders and ASD presents a number of challenges as
well as deficits across a wide range of behaviors or skills that are not seen in those
individuals who have only ID or only ASD. For example, it has been observed [40] that
those individuals with severe autism had more feeding problems that were behaviorally
based, in particular with selecting or refusing food, as compared with those who only
had ID. The combination also increases challenging behaviors. For example, as IQ
goes down, the severity of challenging behaviors in ASD increases. Murphy et al [41]
discovered that self-injury in particular increased. Further, those with ASD tend to not
“grow out” of these types of behaviors; rather, they continue to present significant
challenges over the lifespan, as observed by Murphy et al [41] in a 12-year follow-up
conducted on 141 individuals with severe ASD and ID.
DEVELOPMENTAL COURSE OF ASD
It is commonly believed that those with ASD fall into one of two major developmental
categories [42]. One category involves early onset of impairment and signs and
symptoms of ASD without signs of regression. This is termed gradual onset course. The
other category involves a rather typical development. This typical development is then
followed by loss of language or social skills, sometimes with loss of both, that is paired
with an emergence of ASD-type behaviors such as repetitive or stereotypical behaviors.
This is termed regression course. There is mixed evidence when it comes to prognostic
implications where the regression course is concerned. Some studies indicate that the
regression course is associated with worse outcomes than is the gradual onset course
[43]. Both of these courses may be diagnosed in early to late infancy [44].
There are two approaches that have been taken in order to understand the
development of ASD. These approaches are retrospective and prospective.
Retrospective approaches are mainly based on information gained from reviews of
medical records, parental recall, or observational coding of videotapes made in the
Nursece4less.com 31
home environment during the first or second year of life prior to the ASD diagnosis.
Retrospective studies have generated information that indicates that the core deficits of
ASD are social functioning [45]; however, they also indicate that children who suffer from
ASD also exhibit disruptions in other areas of their lives within the first year of life,
including motor skills, attention, and temperament.
Prospective studies are considered optimal to investigate the timing and nature of how
ASD emerges [42] because prospective, longitudinal studies conducted from infancy
would provide a means of determining patterns of development in those children who
are later diagnosed with ASD. This would later eliminate such confounds as recall bias.
There have been five prospective studies to date that have provided longitudinal data
before the third birthday in children who have ASD as well as in children who are not
affected [46-50]. These studies have all indicated that the development of cognitive,
motor, language, and social skills all appear to be fine at age 6 months. Development
then slows. By the time the children enter pre-school, those with ASD frequently display
motor delays.
Gradual Onset CourseThe gradual onset course occurs just as its name suggests; signs and symptoms
present themselves gradually. Parents or caregivers may notice increasing delays in
development or strange behavior, such as an unwillingness to communicate or
communicating in odd ways. One example of this would be a failure to look a person
who is speaking in the face. Other examples include failure to turn when the child’s
name is called or failure to display interests by pointing to objects the child desires.
Stereotypical behaviors may also develop, such as tapping or hand flapping. All of these
behaviors are early warning signs that a child is developmentally delayed and may need
to be screened for ASD.
Regression CourseThe regression course occurs when a child is following a pattern of normal
development, generally for the first 12 – 24 months of life, and then he or she appears
to lose skills he or she has acquired. Language regression is considered the most
Nursece4less.com 32
obvious form of regression, but it may also be accompanied by more global regression,
which can involve a loss of social skills or social interest. There is a late-onset
regression course that may occur after the age of 3, but the more common course
occurs prior to the age of 3.
Regression is thought to lead to the more severe course of autism [51], particularly when
young children abruptly lose acquired skills, according to a study published in the
Journal of Autism and Developmental Disorders [52]. There is a particular debate among
scientists as to whether children who regress form a distinct grouping of autistic
individuals, as some studies have indicated that those with regression have poorer
outcomes [53].
The study published in the Journal of Autism and Developmental Disorders surveyed
the parents of 2,720 children and found that those children who regress were more
likely to display more severe symptoms than were those children who had early onset
delays. This was as measured through two standard questionnaires: the Social
Responsiveness Scale and the Social Communication Questionnaire. Children in the
regression group were more likely to receive a diagnosis of autistic disorder as opposed
to a diagnosis that was on the milder end of the spectrum, such as Asperger syndrome,
as compared to their earlier onset peers. Additionally, in a school setting, approximately
70% of children who regress are put into special education settings, with 56% needing a
professional aid.
Communication
Research indicates that regression in communication, particularly in speech and
gestures occurs in approximately 22 – 50% of those children with ASD [54]. The rate is
so variable because the definition for regression is fairly loose and can mean anything
from the loss of a minimum of five words for a period of 3 months to the loss of the
consistent usage of one word used in standard communication. Approximately 30% of
children who experience regression never manage conversational speech.
Social
Nursece4less.com 33

Loss of social skills can mean that the child stops returning the caregiver’s gaze, for
example, or displays a lack of interest in other people when they are in the same space
with him or her. An increased disinterest in social games that the child previously
enjoyed, such as patty cake or peek-a-boo, may become obvious. One meta-analysis
[55] indicates that approximately 38% of children suffer from social regression.
Cognitive
Cognitive decline in ASD manifests as more than a child simply losing what he or she
has learned to date. However, one of the manifestations most clearly seen in cognitive
decline is the loss of language skills. The individual may have been learning language
skills perfectly well and then suddenly loses the ability to learn new skills. Other features
of cognitive decline are the inability to learn new material as well as the development of
associated mental impairments. An example of an associated impairment would be
epilepsy, a common impairment associated with ASD.
Self-help skills
The loss of self-help skills occurs when a child loses the ability to continue to develop
independence. This means that the child fails to develop the ability to feed, clean, and
dress oneself. Children who regress lose the ability to understand how to complete
these tasks and can lack or lose the physical coordination necessary to complete these
tasks. Additionally, the child may lose or not develop an understanding of how or when
to ask for assistance with tasks. These types of tasks help children become socialized
into his or her culture; without them the child is poorly socialized. The fact that many
individuals with ASD are lacking in this area is one reason why they appear to be so
poorly socialized.
EFFECTS OF EARLY INTERVENTION
Early detection of ASD allows for practitioners to intervene in a more timely way with
behavioral therapies that may then improve outcomes. Currently, the American
Academy of Pediatrics guidelines call for the screening of all toddlers at the ages of 18
and 24 months [56]. These are the ages at which the existing screening methods are
most able to identify children at risk for ASD.
Nursece4less.com 34

However, research has shown that a brief questionnaire administered to parents at their
child’s one year well-baby screening may help practitioners identify those children who
have ASD or who are at higher risk for the development of ASD. One study involving
137 pediatricians who administered a 24-item checklist to all caregivers bringing in
children for routine one-year check-ups indicated that about 346 of the 10,500 children
screened were at risk for autism. These children were all referred to an autism clinic to
be evaluated further. Of these children, approximately 50% were followed to age 3; and,
32 of these children received a diagnosis of ASD. Another 56 children were diagnosed
with having a language delay. Of those children diagnosed with delayed language skills,
9 children were diagnosed with having a developmental delay, and; 36 children were
diagnosed with other conditions.
The screening utilized for autism in childhood – called the Communication and Symbolic
Behavior Scales Developmental Profile Infant-Toddler Checklist, took the parents
approximately 5 minutes to complete; and, the screening test predicted autism and
other developmental delays approximately 75% of the time. This indicates that this
questionnaire – or one similar – could be useful in identifying ASD earlier so that more
timely intervention methods may be put to use. Although most pediatricians do not
routinely screen early for ASD and other developmental delays (indeed, prior to the
study, only 30 of the 137 pediatricians participating (22%) had routinely screened for
ASD at 1 year of a child’s life) there seems to be some good evidence that early
intervention efforts do benefit those who suffer from ASD.
The Early Start Denver Model (ESDM), which is a behavioral intervention program
appropriate for children as young as 12 months who are suffering from ASD, has been
found in more than one study to be effective in improving brain response as well as
social skills. ESDM combines applied behavioral analysis (ABA) along with a
developmental relationship based approach to achieve gains in language, cognition,
and everyday living skills. ESDM is a unique approach in part because it works with
children who are very young, but also because it blends ABA with routines that are
based in play and focus on building relationships.
Nursece4less.com 35

One study [57] utilizing ESDM examined 48 children with ASD between 18 and 30
months of age. The children were randomly assigned to either receive ESDM or a
community based intervention regimen for a two-year period. Electroencephalogram
(EEG) activity was measured at the close of the two-year period. The hypothesis was
that children receiving ESDM would show higher levels of brain activity when viewing
faces than when viewing objects than would children who were receiving the typical
community regimen. The children were paired with typically developing children at the
time of their EEG assessment. Additionally a group of typical 4-year-old children was
tested as a comparison group. The children who were receiving the ESDM intervention
regimen were given therapy services for 20 hours per week and parents were also
trained to deliver the intervention regimen. Children who were in the community based
regimen received treatment per usual in their community and were given evaluation,
referrals, as well as resources and reading material at the start of services as well as
two times annually.
On the individual level, the study mentioned above showed that 11 of 15 children in the
ESDM group (73%) and 12 of 17 children (71%) in the control group had higher levels
of brain activity on their EEG assessment when viewing faces as opposed to viewing
objects. This is compared to 5 of 14 (36%) children in the community regimen group. At
the close of the study, the children in the ESDM group exhibited brain activity that was
comparable to typically developing children and that was significantly different from
those children who had received the community regimen. Dr. Geraldine Dawson, a
developer of the ESDM intervention and one of the researchers on the study, stated the
following: “For the first time, parents and practitioners have evidence that early
intervention can result in an improved course of both brain and behavioral development
in young children. It is crucial that all children with autism have access to early
intervention which can promote the most positive long-term outcomes” [57].
Another study [57], also examining the ESDM, found that this same model minimizes the
need for required therapy following the intervention as well as achieves the best
possible outcomes for the individual in terms of IQ, social interactions, and brain activity.
Nursece4less.com 36

The study compared 21 children who received ESDM to 18 children who received a
community intervention regimen during the two years they received their early
intervention regimen as well as the subsequent four years post-intervention. ESDM is
more expensive to deliver in the early years of intervention; there was an average
monthly cost of about $10,000 per child. Children on the community regimen had an
average monthly cost of approximately $5,200. However, the hypothesis was that
despite this greater up-front cost, ESDM would pay off greater dividends on the back
end of things, promoting higher IQ, greater ease in social interactions, increased brain
activity, and reduced therapy, leading to an overall reduced cost.
In the four years following the early intervention, the children who had received the
ESDM required an average of approximately $4,450 in related services such as speech,
physical, and occupational therapy, as well as ABA. The children who received the
community regimen required an average of approximately $5,550 in related speech,
physical, and occupational therapy, as well as ABA. Study researchers believe this is
very telling and differences in cost may be even broader than study results suggest, as
the defining factors for related expenses were kept fairly narrow. David S. Mandell,
study researcher expressed the following: “I believe the cost efficiencies would become
even more pronounced if there had been an evaluation on health costs and overall
family economics such as the ability of both parents to continue to work and earn
income while their child received services” [57].
These two studies offer powerful evidence for the idea that early intervention such as
early screening as well as methods such as ESDM may prove to offer better outcomes
for those individuals who suffer from ASD, and in turn offer parents and caregivers a
better outcome as well. Early intervention may help a child in the form of increased
cognitive and social skills, and a family in terms of long-term financial savings.
Therefore, there is strong evidence to suggest that early intervention benefits everyone
involved with ASD.
RISK FACTORS
Nursece4less.com 37

There are a number of risk factors that contribute to ASD. There are both heritable and
non-heritable risk factors. These risk factors are discussed below.
GenderWhile ASDs occur in all racial, ethnic, socioeconomic, and gender groupings, it is well
known that males have a greater likelihood than do females of developing an ASD. The
ratio is as high as 5:1 [58]. It is not known or well understood why there is this
discrepancy. It is also not known if concrete differences in development or presentation
occur between genders. Males with ASD do have certain advantages over females with
ASD. Research indicates that females with ASD tend to have lower Intelligence
Quotients (IQ) than do males [59]. Males also show stronger verbal, motor, and social
skills. However, when controlling for language, females display stronger nonverbal
problem solving abilities.
A recent study published in JAMA Pediatrics [60] that examined the records of more than
625,000 births indicated that birth that involved both augmented and induced labor was
linked to a 35% higher instance of ASD as compared with labor that did not receive
either treatment. The study further indicates that augmented or induced labor was linked
with a smaller increased risk in boys. In girls, only the augmented birth was linked with a
small increased risk. The researchers did control for a number of associated factors that
have been shown to increase the risk of autism, such as the health or age of the
mother. Researchers in the study added that the study results did not necessarily
indicate cause and effect; rather, there could be other factors at play that have as yet
been unidentified. One of these factors may be the usage of Pitocin (oxytocin) that is
utilized to induce or augment labor. Approximately 50 – 70% of women who undergo
induction in the United States receive Pitocin injections. There are other contributors
that may be a factor, such as pregnancy conditions or delivery events that lead up to the
need to induce labor. Further study is needed to determine why augmented and
induced labor is leading to this increased the risk of ASD in boys.
Genetics
Nursece4less.com 38
Twin studies provide evidence to support that there is a heritable component to ASD
etiology, although there has not been any particular gene discovered that predisposes
an individual to ASD [61]. Twin studies have been done on both monozygotic (identical)
and dizygotic (fraternal) twins. Monozygotic twins share all of their genes, whereas
dizygotic twins share half of their genes, on the average. Studies have indicated that
there are increased disease concordance rates among monozygotic twins as compared
to dizygotic twins. A recent study indicated that there is a 60% monozygotic
concordance among 25 sets of twins as compared to a 0% dizygotic concordance
among 20 sets of twins [62]. This data suggests that there is a high rate of heritability.
However, the suggestion has been made that estimations from twin studies may be
overstated. Still, the large heritability discovered in twin studies is supported through
familial aggregation studies [63].
Several studies have also shown a heightened risk for ASD amongst siblings of cases.
This is termed “sibling relative risk” [61] and is estimated as the “ratio of the risk for ASD
among siblings of cases to the risk, or prevalence, in the general population” [61]. The
probability that a sibling of a case will develop ASD is estimated at between 2 % and
6% [64, 65], although there are some estimates that are as high as 7% for siblings of male
cases and 14% of siblings for female cases [66]. It is important to remember, however,
that these numbers are entirely dependent on the population prevalence estimates at
the time of sampling, leading to higher or lower estimations, depending on what is
happening in the population.
There is also another avenue of support for genetic association, and this is the overlap
of ASD with certain genetic disorders such as tuberous sclerosis [67], neurofibromatosis
[68], and Fragile X syndrome [69, 70]. To that end, abnormalities on nearly every
chromosome have been associated with one form or another of ASD phenotype, most
notably on chromosomes 7, 15, and X [71]. The most frequently cited of these are
duplications and deletions of the proximal area of chromosome 15 [72-75]. Breakpoints for
chromosomal inversions that result in features of ASD frequently lie in fragile regions of
chromosomes, which lead to speculations about the possible role of unstable regions of
DNA and submicroscopic chromosomal deletions [76, 77].
Nursece4less.com 39

Prenatal and Perinatal FactorsThere are specific prenatal factors that may contribute to development of ASD. One
such factor is maternal infections. In several studies [61], maternal infections were
measured with non-specific indicators, which included maternal recall of symptoms such
as fever as well as information archived in medical records. While the studies did not
attain statistical significance for the infection measure, each reported a ratio of odds that
were above 1.0 [78-80].
There are specific infections that are known to affect developing brains; of these that
have been most commonly known to affect the developing brain as well as to be
commonly associated with ASD is rubella. However, it has also been shown that other
infections, such as herpes, syphilis, and varicella, as well as the flu, also have a higher
than normal association with ASD. Another factor is prenatal and intrapartum
pharmaceutical usage. For example, utilizing thalidomide during days 20-24 of gestation
has been associated with increased risk of ASD [81, 82]. This suggests that xenobiotics
may play a role in the etiology of ASD. Animal studies [83, 84] and case studies [85, 86]
reflect findings that valproic acid as well as other anticonvulsants may increase ASD
risk. This is an interesting association, as these same drugs may prove therapeutic for
non-epileptic children who suffer from ASD [87-89].
There are also some preconception factors that may be associated with development of
ASD. For instance, in the 1970s the idea that environmental exposure to certain
chemicals arose [90]. This hypothesis was revisited in the 1990s when parents without
incidence of ASD who lived close to plastic manufacturing plants appeared to have a
higher incidence of children with ASD [91]. However, upon examination, the
Massachusetts Department of Public Health concluded that further investigation of the
cases in question was not needed [92].
While preconception chemical exposure factors have not been thoroughly explored,
hypotheses of postnatal chemical exposures have been more thoroughly investigated,
primarily through looking at case studies. However, epidemiologic evidence for specific
Nursece4less.com 40

postnatal environmental exposure that in turn leads to development of ASD is not
substantial. One of the more comprehensive investigations into the matter was
conducted in Brick Township, New Jersey, where there was a high local presence of
ASD near local landfills. This raised concerns that landfills were leaching chemicals into
the drinking water or into local swimming areas. The Agency for Toxic Substances and
Disease Registry looked into the possible exposure pathways, as well as evaluated data
on levels of trihalomethanes, tetrachloroethylene, and thrichloroethylene. While these
chemicals were present in the drinking water at various times during the study, the
levels were found to be low or in locations that did not correspond with the locations
being studied or with the timing of the pregnancies being studied [93, 94].
Neuroanatomical AbnormalitiesNeuroanatomical abnormalities in the brains of individuals with ASD provide concrete
evidence that there is a neurobiological component to ASD [95], that the disease is more
than just a behavioral disorder with purely environmental contributions.
The neurobiology of the disorder has been examined since the dawn of the disorder,
and both genetic and non-genetic factors have been shown [96]. However, particular
etiologic factors are as yet undefined. Frontal lobe volume does appear to be decreased
in individuals with autism [97]; there also appears to be a decrease in gray matter (GM)
volume in the orbitofrontal cortex [98] as well as an abnormally thin frontotemporal cortex
[99]. However, conflicting studies [100-102] have reported that GM volume and thickness is
actually enlarged in these areas.
An increase in GM volume has also been indicated in areas involved in communicative
and social functions, to include the dorsal and medial prefrontal regions, the lateral and
medial temporal area, the parietal regions, and the auditory and visual association
cortices [103-106]. Likewise, discrepant white matter (WM) have been indicated in autism,
including regional increases [107-109], as have decreases in cross-sectional areas and the
microstructure of the corpus callosum [110, 111]. Concomitant WM disruptions have been
indicated in prefrontal, superior temporal, temporoparietal cortices and the corpus
callosum, but there have also been observations of an increase in whole brain WM [101,
109]. It is not clear how these anatomic abnormalities related to domain specific cognitive
Nursece4less.com 41

impairment in social functioning, emotional functioning, language deficits,
communication deficits, and deficient executive function.
Microscopic observations of the brains of individuals with ASD have discovered reduced
cell size as well as increased cell-packing density (meaning an increased number of
nerve cells per unit volume) in the hippocampus, amygdala, mammillary body, anterior
cingulate gyrus, and medial septal nucleus [112]. These structures are recognized as
being connected to one another by interrelated circuits. They also comprise a major
portion of the limbic system. The limbic system is acknowledged to be important to
emotion and behavior, as well as learning and memory. It also plays a large role in the
integration, processing, and generalization of information. Abnormalities of the limbic
system may account for a lot of the major clinical features of ASD, including language
dysfunction as well as social deficits.
Additionally, abnormalities have
been located in the cerebellum,
where the amount of Purkinje cells
is much reduced, particularly in the
posterior and inferior parts of the
hemispheres bilaterally. The vermis
microscopically appears normal.
Abnormalities have also been seen
in the deep cerebellar nuclei.
These findings appear to vary
along with the age of the patient.
Comparable observations have
been seen in the inferior olivary
nucleus neurons as well as the
neurons of the nucleus of the Diagonal Band of Broca. The fact the the olivary neurons
are preserved even in the face of such markedly reduced number of Purkinje cells
indicates that these brain lesions are likely of prenatal origin.
Nursece4less.com 42
[113]

The role of the cerebellum in ASD is not certain. Some studies [112] show that it may play
a role in the modulation of language, attention, emotional affect, mental imagery,
cognition, and anticipatory planning. Therefore, it is likely that the abnormalities in both
the limbic system and the cerebellum are important to understanding the clinical
features of ASD.
Brain enlargement
Brain changes prior to the age of 2 may lead to brain enlargement that in turn leads to
ASD. One study conducted by University of North Carolina (UNC) researchers found
that children with ASD who had enlarged brains at the age of 2 years also had enlarged
brains at the ages of 4 and 5. However, their brain growth was not markedly different
than it had been at 2 years old.
Researchers conducted their original study in 2005, with a follow-up study conducted in
2011. In 2005, researchers discovered that 2-year-old participants with ASD had brains
that were up to 10% larger than those of children at the same age that did not have
ASD. The follow-up study indicated that the children with ASD continued to have brain
enlargement in subsequent years, but at the same level they had it at 2 years old. This
finding led researchers to conclude that the changes they detected at the age of 2 were
due to growth prior to that time period. Additionally, the study discovered that the
enlargement was affiliated with an increase in folding on the surface of the brain, not an
increase in gray matter. Researchers posit that this increase is more than likely genetic
and results from “an increase in the proliferation of neurons in the developing brain” [114].
The researchers suggest that the brain overgrowth may be occurring around the child’s
first birthday.
Another study conducted by the University of California Davis MIND Institute indicated
that those children who were later diagnosed with ASD were found to have an excess of
cerebrospinal fluid as well as enlarged brains in infancy. This brought up the possibility
that these types of brain abnormalities may serve “as potential biomarkers for the early
identification of the neurodevelopmental disorder” [115]. The study is the first to link the
excess of cerebrospinal fluid that existed during infancy to the development of ASD. A
Nursece4less.com 43

potential positive outcome to the study is that it would offer practitioners a new way to
positively screen for ASD, because the brain anomaly would be detectable utilizing a
conventional MRI. Therefore, early detection would be possible; this is crucial in
children who have ASD because it allows for timely intervention.
Early intervention offers the most hope in decreasing the behavioral and cognitive
impairments associated with ASD and increasing positive long-term outcomes. This
study was conducted on 55 children who were between 6 – 26 months of age. Thirty-
three of these children had an older sibling who had an ASD. Twenty-two were children
who had no family history of ASD. Researchers indicated that the brain anomaly was
more significantly detected in those infants who were high risk and who were later
diagnosed with ASD between 24 and 26 months of age.
Another study [116] examined abnormal brain growth and onset status: early onset or
regressive onset. This particular study examined 2 – 4 year olds whose status was
either non-regressive (n = 53) or regressive (n = 61). There was also a control group of
non-affected 2 – 4 year olds (n = 66). Researchers discovered that abnormal brain
enlargement was most commonly discovered in boys with regressive ASD. Brain size in
boys who were non-regressive did was not different from the control group.
Retrospective head circumference measurements were also taken, and it was
discovered that head circumference in boys with regressive ASD is normal at birth but
then diverges at around 4 – 6 months of age. Girls who have autism do not have any
difference in brain size from those in the control group. Researchers posit that these
results indicate that there could be certain neural phenotypes that are associated with
the different types of onset of ASD. For instance, the rapid head growth may be a risk
factor for regressive type ASD.
Environmental FactorsThere are several environmental factors that may be associated with the development
of ASD. One of these is childhood infection. There have been reports of sudden onset
Nursece4less.com 44

of ASD symptoms in older children following herpes encephalitis [117-119]. There are other
infections that can result in secondary hydrocephalus; for example, meningitis. These
infections may lead to development of ASD [120]. One study indicated that mumps,
chicken pox, fever of unknown origin, and ear infections were significantly associated
with an increased risk of development of ASD [121].
Some vaccinations may also increase the risk for development of ASD. A paper
published in 1998 indicated that the measles-mumps-rubella vaccine might be linked to
ASD development [122]. However, epidemiologic studies have not provided evidence that
supports a link between the vaccine and the risk of developing ASD [123-127]. Similarly,
case study comparisons do not find any indication of post-vaccination increase in risk of
developing ASD [123, 128]. Further, a population based retrospective study that included
more than half a million children from Denmark who were born between 1991 and 1998,
82% who had received the measles-mumps-rubella vaccine, discovered no association
between the vaccine and development of ASD [129].
There are additional concerns over vaccines and ASD, which stem from the usage of
thimerosal, which is a preservative that contains ethylmercury. Ethylmercury is itself
similar to methylmercury, which is a known fetal neurotoxin that can cause severe brain
injury at high doses and leads to developmental delays and dysfunction at lower doses
[130]. There is limited data that suggests that higher doses of ethylmercury is similar to
higher doses of methylmercury [131, 132], and there is no data on low dose exposure to
ethylmercury. There is not much data on the association to date.
Data from the Vaccine Safety Datalink of the Centers for Disease Control and
Prevention indicates weak association between thimerosol related exposure to mercury
and related neurodevelopmental disorders, but not association to ASD itself [133].
Existing evidence is considered to be inconclusive. Although Thimerosal has been
removed from vaccines, there are still many individuals alive with ASD who have
received vaccinations that contained thimerosal.
Nursece4less.com 45

Other environmental factors include birth complications, including umbilical cord
complications, fetal distress, injury or trauma during birth, multiple births, maternal
hemorrhage, summer births, low birth weights, congenital malformations, low 5-minute
Apgar score, feeding difficulty, neonatal anemia, meconium aspiration,
hyperbilirubenemia, and ABO or Rh incompatibility [134]. Parental age at the time of
conception is also a factor; and, this includes the age of both parents. One study [135]
indicated that firstborn children of 2 parents who were older were 3 times more likely to
develop ASD than were third or later born children of mothers who were 20 – 34 years
of age and fathers who were <40 years of age. Therefore, the risk of ASD increases
with both maternal and paternal age.
Another environmental risk factor may be waiting less than a year between
pregnancies. One study [136] indicated that pregnancies that are closely spaced are
associated with an increase in ASD. The study examined pairs of first and second born
siblings in California that occurred between 1992 and 2002 and examined ASD
diagnoses in these siblings. Results of the study indicated that children who were born
after shorter intervals between the pregnancies were at an increased risk of developing
an ASD, with the highest risk being associated with pregnancies that were spaced less
than a year apart.
One more environmental risk factor may be not taking prenatal vitamins, as taking
prenatal vitamins has been shown to slightly reduce the odds that a child will develop
ASD. One study examining Northern California families enrolled in the Childhood
Autism Risks from Genetics and Environment (CHARGE) study [137] concluded that
mothers who had children with ASD were less likely than were mothers of non-affected
children to have taken a prenatal vitamin during the 3 months prior to pregnancy or in
the first month of pregnancy. This led researchers to conclude that the peri-conceptional
use of prenatal vitamins may reduce risk of birthing a child with ASD, particularly in
those who are already genetically susceptible to ASD.
What is important to note regarding environmental risk factors is they do not affect a
child in a vacuum. Many children are exposed to environmental risk factors without
Nursece4less.com 46

developing ASD. This leads researchers to conclude that if a child is genetically
predisposed to ASD, for example, then these types of environmental risk factors may
increase the risk of development of an ASD. Studies have indicated that there are other
environmental factors - such as the maternal use of antipsychotics and mood
stabilizers – that may increase the risk of development of ASD. However, the risk must
also be weighed against the mother’s need, which can also affect the health of the child
she will be having. Additionally, most risk factors that are not yet well documented may
only increase the risk of development of ASD slightly as compared with other risk
factors, such as genetic predisposition, making it difficult to pinpoint how, exactly,
environmental factors contribute to the larger overall picture of each single ASD
diagnosis.
DIAGNOSIS
Differential DiagnosisDiagnosing ASD is no easy task, particularly since ASD may mimic other disorders, and
vice versa. Hence, what is required of practitioners is making a differential diagnosis, or
differentiating between conditions that share symptoms. One such example is ASD and
ADHD, which look remarkably similar.
The CDC [138] has released a handout outlining differences to allow practitioners to
make a differential diagnosis between ASD and commonly confused conditions. These
conditions are as follows:
Developmental delays and intellectual disabilities:
Those with intellectual disabilities or developmental delays may display autistic features
but may not meet the criteria for ASD. Those with ASD may have an intellectual
disability or be of normal intelligence. Those with intellectual disability generally have
better social and communication skills than do those with ASD who are of the same
cognitive level.
Fetal alcohol syndrome disorders:
There is an increase in risk of ASD as well as other neurodevelopmental disorders in
those children who were exposed to alcohol in utero.
Nursece4less.com 47
Genetic syndrome:
There may or may not be a family history, although this is dependent upon the specific
disorder. Should dysmorphic features be present, genetic disorders should be
considered. There are certain neurogenetic disorders that tend to be associated with
ASD; and, these include the following:
Fragile X – this includes intellectual disability, large ears, macrocephaly, large
testicles, hyptonia, and joint hyperextensibilty.
Tuberous sclerosis – this includes hypopigmented macules, seizures, central
nervous system hamartomas, and intellectual disability.
Angelman syndrome – this includes developmental delays, wide-based ataxic
gait, progressive spasticity, hypotonia, and seizures.
Rett syndrome – this is a disorder mainly seen in girls. There is an apparently
normal development over the first 5 – 48 months of life that then results in
microcephaly. The child then loses the previously acquired hand skills and often
develops hand wringing stereotypies. Frequently seizures develop.
Hearing impairment:
Often this can be due to a history of fluid or recurrent otitis media. Those with hearing
impairments frequently have speech delays but typically may use a compensatory
nonverbal type of communication. These children will make eye contact and utilize facial
expression. Those with ASD however can sometimes be described as having selective
hearing (they may not respond if someone calls their name, but they become overly
sensitive to other noise). Those with hearing impairments are generally under-
responsive to all noises, although this may be somewhat variable dependent upon the
degree of hearing loss.
Mental Health Disorders:
Nursece4less.com 48

Mental health disorders is a fairly broad category of differential diagnoses with variable
symptomology that depends upon the specific diagnosis. Some of the diagnoses not
uncommonly seen in individuals with ASD are outlined below:
Obsessive compulsive disorder (OCD) – The obsessive thoughts and repetitive
actions seen in obsessive compulsive disorder may appear very similar to the
kinds of ritualistic behaviors and motor stereotypies seen in ASD.
Anxiety disorders – those with anxiety problems may be hesitant to interact with
other people. They may have problems with change or transitions. Those with
anxiety are still socially related, however, and they still have appropriate social
insight, whereas someone with ASD does not.
Depression – Depression may present in a variety of ways, and particularly in
children. Children may be withdrawn or they may isolate themselves from others.
They may display a blunted affect and avoid eye contact, which are all signs of
ASD as well.
Attention deficit hyperactivity disorder (ADHD) – Those with ADHD can have
impairments in social skills as a result of hyperactivity or impulsivity. They may
have a hard time sustaining a conversation as a result of inattention. Those with
ASD also often have issues with hyperactivity, impulsivity, and inattention.
Oppositional defiant disorder (ODD) – The behavioral problems seen in those
children with ODD are generally intentional. Many children will have temper
tantrums at some point; however, children who have ASD are more likely to have
tantrums that are associated with anxiety that results from transitions or tantrums
that appear to be for no reason.
Tourette syndrome - The tics seen with Tourette syndrome may appear to be
similar to some of the motor stereotypies seen with ASD. Those with Tourette
syndrome will generally not have the social or communication problems seen
Nursece4less.com 49

with ASD though. However, there may still be some isolation due to
embarrassment or avoidance of peers, which should be taken into account.
Psychosocial factors are important to consider when evaluating individuals with ASD
and co-occurring mental illness, for example, issues of abuse and neglect. Those who
have a history of psychosocial factors such as neglect or abuse may be very withdrawn
or hesitant to interact with other people. They may also display skills regression, such
as a loss of language, or they may display behavioral problems.
Sensory problems:
Those with ASD often times have sensory issues such as being hypersensitive to loud
noises or avoiding certain textures in foods. A person without ASD but who has sensory
impairments will not have the accompanying social and communication impairments.
Speech and language disorders:
Those with speech and language disorders will compensate with nonverbal forms or
communication. These nonverbal compensations include pointing and gestures. There
is a lack of severe social deficits, although there may be some social impairment that
results from communication difficulties. In a person with ASD, nonverbal communication
and social skills is often lacking.
Level 1 ScreeningEvidence based recommendations for routine Level 1 developmental screening for ASD
are important in the evaluation and treatment planning phases [139]. Providers and
nurses need to be knowledgeable and consistent about the following when caring for
the individual with ASD:
Developmental observation should be conducted at all well child visits from
infancy on through school age and at any age thereafter if there are concerns
that are aroused regarding social interactions, learning, or behavior.
Nursece4less.com 50

The recommended developmental screening tools include: Ages and Stages
Questionnaire, BRIGANCE(R) Screens, the Child Development Inventories, and
the Parents’ Evaluations of Developmental Status.
Further evaluation is needed should a child fail to meet any of the following
milestones:
o Failure to babble by 12 months
o Failure to gesture – such as pointing or waving goodbye by 12
months
o Failure to speak in single words by 16 months
o Failure to speak in two word spontaneous phrases by 24 months
o Loss of language or social skills at any age
Siblings of those children who have ASD must be carefully monitored for
acquisition of social, play, and communication skills as well as the occurrence of
maladaptive behavior. Screenings should be conducted not only for ASD related
symptoms but also for learning difficulties, language delays, social problems, and
anxiety and depressive symptoms.
ASD screening should be conducted on all children who have failed routine
developmental screening procedures utilizing one of the validated instruments:
the Checklist for Autism in Toddlers (CHAT) or the Autism Screening
Questionnaire.
Laboratory investigations that are recommended for all children with
developmental delays or ASD include audiological assessments and screening
for lead exposure. Early referrals for assessments should include behavioral
measures, assessments of middle ear function, and electrophysiological
procedures. Lead screening should be conducted in any child who has
developmental delay and pica, and additional periodic screening should be
conducted if the pica (an abnormal craving for non-food substances, i.e. dirt,
paint or clay) persists.
Nursece4less.com 51

Level 2 EvaluationEvidence based recommendations for routine Level 2 diagnosis and evaluation for ASD
involve the following [139]:
Genetic testing in children with ASD, in particular high-resolution chromosome
studies and DNA analysis for Fragile X should be performed should there be a
presence of mental retardation or if there is a family history of Fragile X or an
undiagnosed mental retardation, or if there are dysmorphic features present.
Selective metabolic testing should be performed if the following are present:
lethargy, cyclic vomiting, or early seizures, or if evidence of mental retardation is
evident or cannot be ruled out.
There is no evidence at the moment to indicate that routine clinical neuroimaging
can assist in evaluating or diagnosing ASD. Additionally, there is not sufficient
evidence to support the idea that hair analysis, celiac antibodies, allergy test,
thyroid function tests, or erythrocyte glutathione peroxidase studies can assist in
evaluation or diagnosis.
Another important consideration in the evaluation and treatment of individuals with ASD
relate to Consensus Based Principles of Management [139]. There are some
recommendations that are based on consensus agreement, and, these are listed below.
Surveillance and Screening:
In the United States, states are required to follow Public Law 105-17, the Individuals
with Disabilities Education Act Amendments of 1997-IDEA’97, which orders “immediate
referral for a free appropriate public education for eligible children with disabilities from
the age of 36 months, and early intervention services for infants and toddlers with
disabilities from birth through 35 months of age” [139].
Diagnosis:
The diagnosis of ASD should include the usage of an instrument that has at the least a
good specificity for ASD and a moderate sensitivity. Sufficient time should be allotted for
standardized parental or caregiver interviews regarding concerns and child behavioral
Nursece4less.com 52

history, as well as time given to direct and structured observation or social and
communication interactions and play.
Recommended instruments include the use of rating scales and diagnostic parental
interviews; examples are outlined below:
The Gilliam Autism Rating Scale:
This is an instrument that assists both parents/caregivers and practitioners in
identifying and diagnosing ASD by examining stereotyped behaviors,
communication, and social interaction in individuals. This assessment consists of
42 items that describe behaviors characteristic of individuals with ASD. The
assessment is utilized for identification of ASD in individuals, of the ages 3
through 22 years.
The Parent Interview for Autism:
This assessment was designed to measure ASD symptom severity across a wide
range of behavioral domains. The main point of this assessment is to assess
behavioral change in young children.
The Pervasive Developmental Disorders Screening Test – Stage 3:
This assessment may actually screen for several ASD disorders in children as
young as 18 months. This assessment is designed to be a parental reporting
measure, and the assessment facilitates early identification in order to offer
parents, caregivers, and practitioners the opportunity to implement early
intervention methods.
The Autism Diagnostic Interview-Revised:
This assessment is a structured interview that is utilized for diagnosing ASD as
well as distinguishing ASD from other developmental disorders and planning
treatment. The assessment is designed for children and adults with a mental age
above 2 years.
Diagnostic Observation Instruments (these are differentiated further as):
Nursece4less.com 53

o The Childhood Autism Rating Scale:
This is a behavioral rating scale frequently utilized to diagnose ASD. The
scale rates children on a scale of 1 through 4 on various criteria and
comes up with a composite score that rates the child from non-autistic to
severely autistic.
o The Screening Tool for Autism in Two-Year-Olds:
The STAT is an empirically based, interactive measure developed to
screen for autism in children between 24 and 36 months of age. It is
designed for use by community service providers who work with young
children in assessment or intervention settings and who have experience
with autism.
o The Autism Diagnostic Observation Schedule-Generic:
This assessment is observation based and examines the social and
communication based behaviors that are frequently delayed in those that
have ASD. The assessment consists of four 30-minute observational
sessions that contain communication, socially interactive, play, and
imaginative elements to test the child.
Medical and neurologic evaluation of the individual with ASD should include the
childhood developmental history and milestones. Also, the history should reflect if there
was regression in early childhood or later on in life; encephalopathic events, attention
deficits, seizure disorders, depression or mania, behaviors such as irritability, self-injury,
sleep or eating disturbances, or pica. A neurologic and physical examination in the child
should include: longitudinal measurements of the circumference of the head as well as
examination of the head for unusual features that may suggest a need for a genetic
evaluation, neurocutaneous abnormalities, gait, reflexes, tone, cranial nerves, and a
determination of mental status that includes verbal and nonverbal language and play.
Evaluation and monitoring of ASD involves multivariate considerations and approaches,
as well as interdisciplinary ASD specialists to ensure best outcomes. Both the
Nursece4less.com 54

immediate and long term evaluative and monitoring approach of those who suffer from
ASD requires a multi-disciplinary approach which may include one or more of the
following professionals: psychologists, speech-language therapists, neurologists,
audiologists, pediatricians, occupational therapists, child psychiatrists, and physical
therapists. In addition, educators or special educators may also be involved. Those
individuals who have mild ASD must also receive adequate assessment and diagnosis.
Re-evaluation within 1 year of the initial diagnosis and continual monitoring is one
expected aspect of clinical practice. While there is not a need to repeat extensive
diagnostic tests, follow-up visits may be helpful when it comes to addressing behavioral,
environmental, and developmental concerns. Common and helpful evaluations and
developmental tests for ASD are highlighted below:
Speech, language, and communication evaluation:
A speech, language, and communication evaluation should be conducted on all
children who fail a language developmental screening conducted by a speech-
language therapist who is trained in evaluating children who have developmental
disabilities. Comprehensive assessments of pre-verbal and verbal individuals
should take into account such factors as age, cognitive level, and socio-
emotional ability. These assessments should examine receptive language and
communication, expressive language and communication, voice and speech
production, and the collection and analysis of spontaneous language.
Cognitive and adaptive behavioral evaluations:
A psychologist or other trained practitioner should conduct cognitive evaluation
on all children with ASD. Cognitive instruments must be appropriate for both the
chronological and mental age and provide a full range of standard scores and
current norms that are independent of social ability, include independent
measures of both nonverbal and verbal abilities, and provide a full index of
ability. A measure of adaptive functioning must be collected for any child who has
been evaluated as having an associated cognitive handicap.
Nursece4less.com 55

Sensorimotor and occupational therapy evaluations:
An evaluation of sensorimotor skills should be considered. A qualified
professional such as an occupational therapist or physical therapist should
conduct this assessment. The assessment should include an examination of both
gross and fine motor skills, sensory processing abilities, praxis, unusual and
stereotyped mannerisms, and the impact of all of these on the individual’s life.
An occupational therapy evaluation is suggested when the deficits that are
present exist in functional skills or in the areas of leisure/play, self-maintenance
in daily living activities, or in productive school or work tasks. Sensory Integration
and Praxis Tests may be utilized on a case-by-case basis to detect certain
patterns of sensory integrative dysfunction, although these are not always
routinely warranted in all evaluations of those children who suffer from ASD.
Sensory Integration and Praxis Test (SIPT):
This assessment is a battery of 17 subtests that require children to perform a
variety of motor tasks, either visual, tactile, kinesthetic, or motor, to assess
sensory integration. The assessment is intended for ages 4 years through 8
years, 11 months [139].
Neuropsychological, behavioral, and academic assessment:
These types of assessments should be performed on an as needed basis in
addition to cognitive assessments. These assessments should include
relationships and social skills, educational functioning, learning style, problematic
behaviors, sensory functioning, self-regulation, motivation and reinforcement.
There should also be an assessment of family resources performed by a
qualified psychologist or other professional to include an assessment of the
parent or caregiver’s understanding of their child’s condition as well as familial
strength and talents, stressors and adaptations, and supports and resources.
This also offers the practitioner the opportunity to offer the family the proper
counseling and education.
Nursece4less.com 56

Psychological Assessment Tools
Autism Diagnostic Interview – Revised (ADI-R)
The Autism Diagnostic Interview – Revised (ADI-R) is a clinical diagnostic tool utilized to
assess autistic disorder in both children and adults [140]. The ADI-R offers a diagnostic
algorithm for autism that is described in the ICD-10 and in the DSM. This diagnostic tool
focuses on autistic behaviors in 3 primary areas: qualities of reciprocal social
interactions; communication and language, and; restricted and repetitive stereotyped
interests and behavior. The ADI-R is appropriate for use in with children and adults who
have a mental age of 18 months and older.
The tool contains 93 items. Beyond the three main areas of focus the tool also includes
other areas relevant for treatment planning; for example, self-injury or over-activity.
Responses to items are scored by a clinician, which is based on the parent or caregiver
description of the child or adult individual behavior. Items are organized around content
area, with definitions of behavioral items being provided. For example, in the area of
communication, “Delay or total lack of language not compensated by gesture” [140] is
broken down further into behavioral items that are specific, such as pointing to items or
expressing interest, nodding or the head, or expressing conventional gestures.
All items in the ADI-R ask about current behavior. The exception to this is found with a
few behaviors that only occur within specific age periods. In these items, specific age
limitations are given. For instance, items that ask about group play are referring only to
behavior displayed between ages 4 and 10. In addition to inquiring about current
behavior, items focus on time periods in which behaviors are likely to be pronounced –
this is generally between the ages of 4 to 5 years of age.
The tool begins with an introductory question that is followed by questions about the
participants’ early development. After the introductory question, the following 41
questions regard verbal and nonverbal communication. Questions 50 – 66 specifically
regard social development and play. There are included questions that regard interests
and behaviors; and, there are 14 questions that regard “general behavior”. The final 14
Nursece4less.com 57
questions in the ADI-R include questions about motor skills, memory skills, over-activity
and fainting.
The ADI-R tool generates scores in each of the three main content areas as stated
above. Elevated scores are indicative of problematic behavior in that particular area.
Scores are based on a clinicians’ judgment, with a clinician giving a score of 0 – 3 for
each item: a score of 0 is awarded when “behavior of the type specified in the coding is
not present”; a score of 1 is awarded when “behavior of the typed specified is present in
an abnormal form, but not sufficiently severe or frequent to meet the criteria for a 2”; a
score of 2 is indicative of “definite abnormal behavior”, and; a score of 3 indicated
“extreme severity” of the behavior in question [140]. Additionally, there are also scores of
7, which indicates “definite abnormality in the general area of the coding, but not of the
type specified; scores of 8, which indicates “not applicable”, and; scores of 9, which
indicates “not known or asked” [140]. All of these scores are converted to 0 in the
algorithm.
A child is classified as autistic when the scores in all three main content areas meet or
exceed certain specified cutoffs and the onset of autistic spectrum disorder is evident by
36 months of age. The same algorithm is utilized for children who have mental ages of
18 months through adulthood, with 3 versions that contain minor modifications, which
are:
A life-time version
Version that is based on current behavior
Version utilized for children under age 4
This algorithm specifies a minimum score in each main content area to lead to a
diagnosis of autism.
There are some practical issues to consider when utilizing this diagnostic tool; such as,
this interviewer-based tool requires quite a bit of training in both administration and
scoring. The test, however, when administered by a well-trained professional, only takes
approximately 90 minutes for children and slightly longer for adults. The test has a
strong background of internal validity as well as inter-rater and test-retest reliability [140].
Nursece4less.com 58
Autism Diagnostic Observation Schedule (ADOS)
The Autism Diagnostic Observation Schedule (ADOS) is a semi-structured assessment
tool that examines communication, social interaction, and play in individuals who are
suspected of having autism spectrum disorders [141]. ADOS consists of four different
modules, each of which is appropriate for use for testing on children and adults of
different developmental and language levels.
The ADOS is a standardized testing tools and is comprised of standardized activities
that allows the administrator to observe the presence or non-presence of behaviors that
have been determined to be important to extending a diagnosis of ASD. The test is
administered through the administrator selecting the module that is most appropriate for
the individual’s language level and chronological age. The participant’s response is then
recorded within each module and overall ratings are made at the end of each schedule.
The ratings may then be utilized to formulate a diagnosis by way of utilizing an algorithm
for each module.
The ADOS basically provides a 30 – 45 minute observation period in which the
administrator of the test presents the participant with a number of opportunities to
exhibit typical ASD behaviors by pressing the individual to communicate through social
interaction and language skills [141]. The modules offer social-communicative sequences
that unite a series of both unstructured and structured situations, each of which offers a
different combinations of the above-mentioned presses for social behaviors.
Module 1 is designed for individuals who do not regularly utilize “phrase speech” [141].
Materials in this module have been selected for younger children, although materials
from other modules may be substituted if the administrator so desires. Module 2 is
designed for individuals who have some phrase speech but do not possess verbal
fluency. Module 3 is designed for individuals who are verbally fluent, which is defined as
“having the expressive language of a typical four-year-old child” [141]. Module 3 also
includes tasks such as playing with age appropriate toys – this typically encompasses
up to ages 12 – 16. Module 4 is much the same as module and includes many of the
same tasks; and, Module 4 is intended primarily for verbally fluent adolescents and
Nursece4less.com 59

adults. The biggest difference between module 3 and module 4 is in whether
information about social communication is more suitably acquired during playtime or
during a conversational interview.
The four modules overlap in terms of activities and together they contain a variety of
tasks. These tasks range from observing the way a young child requests that the
administrator continue to blow up a balloon in Module 1 to a conversation about a social
relationship in Module 4. Modules 1 and 2 are frequently conducted whilst moving about
different places in a room whereas Modules 3 and 4 are frequently conducted whilst
sitting at a table and consist of more conversation and language that do not come along
with physical context. The superficial appearance of each of the different modules may
seem quite varied; however, the general principles involved in the deliberate variation of
the administrator’s behavior when it comes to utilizing a hierarchy of both structured and
unstructured behavior remain the same. Standardization lies in this hierarchy of
behavior that is employed by the administrator and the types of behaviors that are taken
into consideration in each activity during the ratings. The activities work to structure the
interaction.
The ADOS offers practitioners the opportunity to observe social and communication
behaviors in standardized and well documented contexts, and the primary goal of the
ADOS is to provide a standardized context in which to observe social and
communicative behaviors of participants across the life span in order to aid with
diagnosis. For diagnostic purposes, use of the ADOS should also be accompanied by
other information, in particular a detailed observational history from parents or
caregivers when possible.
Other questionnaires
There are a number of other developmental and behavioral screening tools available.
These include the following:
Ages and Stages Questionnaire (ASQ-3):
Nursece4less.com 60
The ASQ-3 covers ages 1 month through 66 months. There are 21
questionnaires and scoring sheets for the following childhood ages: at 2, 4, 6, 8,
9, 10, 12, 14, 16, 18, 20, 22, 24, 27, 30, 33, 36, 42, 48, 54, and 60 months of
age. The ASQ-3 screens several different areas, which include communication,
fine motor, gross motor, personal and social skills, and problem solving. The
ASQ-3 is completed by parents and caregivers and is scored by a professional or
clerical worker trained at scoring the assessment [142].
Ages and Stage Questionnaire: Social-Emotional (ASQ:SE):
The ASQ:SE covers ages 3 through 66 months. There are 8 questionnaires for
use at 6, 12, 18, 24, 30, 36, 48, and 60 months of age. The ASQ:SE screens
several different areas, including self-regulation, communication, autonomy,
interaction with people, compliance, adaptive behaviors, and affect. The ASQ:SE
is completed by parents or caregivers and is scored by a professional [143].
Brief-Infant-Toddler Social-Emotional Assessment (BITSEA):
The BITSEA covers ages 12 months through 36 months. The BITSEA is a social
emotional screener that may be administered by a parent or caregiver and is
scored by a professional with a minimum qualification of a Master’s degree in a
related field [144].
Child Development Inventory
The Child Development Inventory covers ages 0 through 6 years and is a 300-
item questionnaire that parents may complete either in the home or in a
professional’s office. The purpose of this assessment is to record observations of
the child’s behavior. This assessment screens several different behavioral areas,
including social, gross motor, fine motor, self-help, language comprehension,
expressive language, numbers, and letter.
The assessment also includes a General Development Scale as well as 30 items
designed to identify a parent or caregiver’s concerns about their child’s growth,
health, hearing, vision, behavior, and general development [145].
Nursece4less.com 61
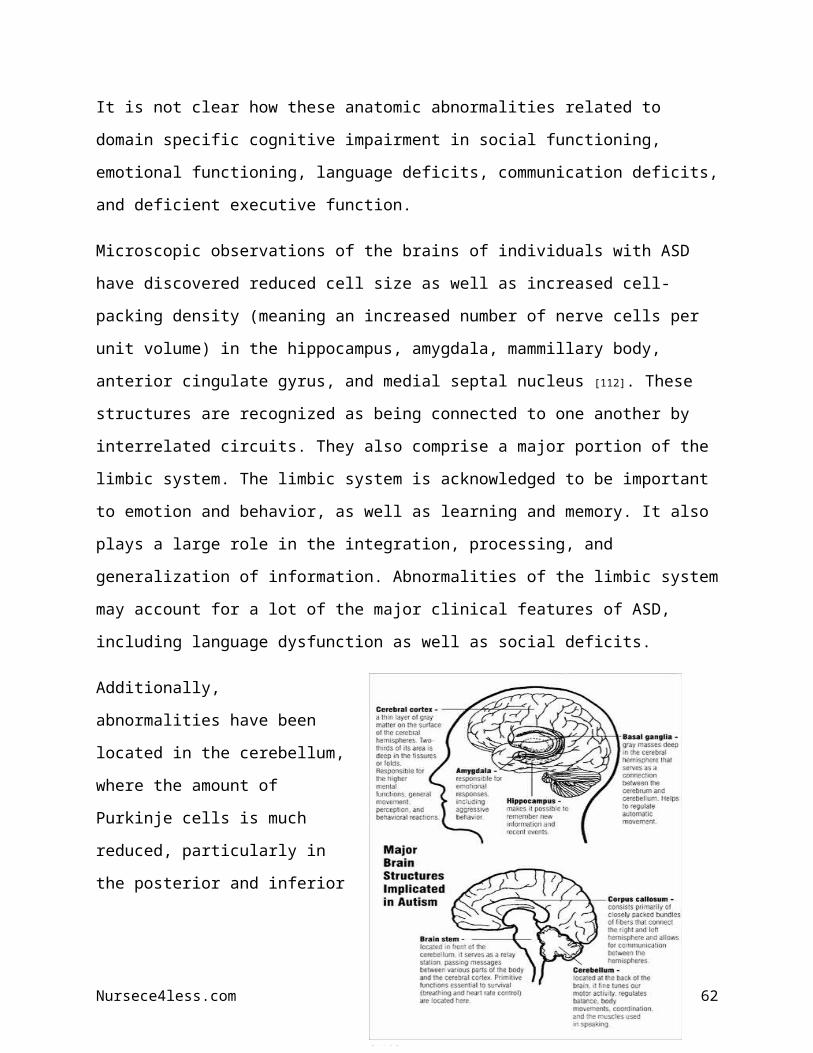
CSBS DP Infant-Toddler Checklist:
The CSBS DP Infant-Toddler Checklist is designed to assess children ages 6
months through 24 months. Components include a 1 page Infant-Toddler
Checklist, a 4 page Caregiver Questionnaire, and a Behavior Sample, which is
conducted while the parent and child interact. The CSBS DP Infant-Toddler
Checklist screens several different language predictors, including emotion and
eye gaze, gestures, words, object use, communication, sounds, and
understanding. Caregivers or professionals who are trained to assess young
children, such as speech language therapists or early interventionists, conduct
the assessment; a professional scores the results [146].
Parents Evaluation of Developmental Status (PEDS):
PEDS is an assessment designed for children ranging in age from 0 through 8
years. PEDS is considered one of the most brief, yet accurate, methods for early
detection of ASD. The screening consists of 10 short questions that parents
complete. PEDS helps parents decide the following:
o If a child needs a developmental or mental health assessment, and if they
do, then a determination is made of the kind of testing needed.
o If parents need advice, a determination is made on what topics for which
advice is required.
o If a child needs to be watched over time to offer prompt attention for
emerging potential problems.
o Whether or not reassurance and monitoring is what is required or if there
is something more that is required.
All children at high risk on PEDS should be referred and monitored. PEDS takes
only approximately 2 minutes to complete and may be completed even in
practitioners’ waiting rooms. There is a high specificity to this assessment.
Further, PEDS is an assessment that may be administered online [147].
Parents Evaluation of Developmental Status-Developmental Milestones
(PEDS:DM):
Nursece4less.com 62

The PEDS:DM is an assessment designed for children from 0 to 7-11 years of
age. This assessment may be used either with the original PEDS assessment or
on its own. Each item assesses a different developmental domain, including fine
motor and gross motor skills, expressive and receptive language skills, self-help,
social-emotional skills, and for those children who are older, skills such as
reading and math. If there is failure on an item it often predicts difficulties in that
domain.
The assessment is designed with a high specificity and to provide clear criteria
regarding when to refer. There is value in utilizing the PEDS and PEDS:DM
together, as the two assessments combined have only 16 to 18 questions to
answer per visit. The assessment is designed to address parental or caregiver
concern as well as focus the visit. It also helps ensure collaboration between the
parent and the practitioner in that it puts the two together on the same page in
terms of where treatment is headed [148].
Social-Emotional Growth Chart
The Social-Emotional Growth Chart takes approximately 10 minutes to
administer and is appropriate for ages 0 through 42 months. The assessment
consists of a questionnaire that is to be completed by the parent, caregiver or
educator in order to help the practitioner come to an understanding about how
the child utilizes all of his or her capacities to deal with feelings, meet needs,
think, and communicate with others. The questionnaire contains 35 items that are
ordered developmentally and according to the age at which the item is usually
mastered. The items are rated utilizing a 5-point scale. This assessment is given
as a preliminary step and is utilized for early identification of ASD. It may be
utilized to determine if further assessment or a referral is needed and may also
help in monitoring growth or in planning intervention [149].
Modified Checklist for Autism in Toddlers (M-CHAT):
The M-CHAT is designed for children ages 16 through 30 months. This
assessment is administered to assess a toddler’s risk of development of ASD
Nursece4less.com 63

and may be administered by parents, caregivers, or practitioners. The main fault
of the M-CHAT is that it has a high rate of false positives; this stems from the fact
that one of the main goals of the assessment is to maximize specificity.
Therefore, not all children who score as being at risk for ASD will actually be
diagnosed with ASD. To adequately address this issue, a structured follow-up
interview should be conducted following the administration of this test [150].
Autism Spectrum Screening Questionnaire (ASSQ):
The ASSQ is a 27-item checklist that may be completed by parents or caregivers
that is designed to assess children ages 7 through 16. This assessment is
designed to examine symptoms that are characteristic of high functioning ASD,
such as Asperger syndrome, in those children who have either normal
intelligence or mild mental disability [151].
Social Communication Questionnaire (SCQ):
This assessment is designed to assess children ages 4 and older and is a cost
effective way to screen for ASD, so long as the individual’s mental age exceeds 2
years of age. The SCQ assists in evaluating communication skills as well as
social functioning in those children who may have ASD. A parent or caregiver
completes the assessment. This assessment may be completed under ten
minutes. The SCQ is available in two formats – Lifetime format and Current
format. Each of these formats is composed of 40 yes or no questions.
The Lifetime format focuses on the child’s developmental history. The Current
format moves from developmental history to the child’s present status and
examines the child’s behavior over the most recent previous 3 months. The
purpose of the Lifetime format is to aid in screening and referral. The purpose of
the Current format is to aid in treatment planning, educational intervention, and to
map and measure changes over time. The SCQ may also be utilized to compare
symptoms across groups – for example, to compare symptoms across groups of
children with a variety of language disorders [152].
Nursece4less.com 64

ASD AND CO-MORBIDITIES
EpilepsyASD and epilepsy often co-occur. Approximately 30% of those children with autism
have epilepsy, and approximately 30% of those children with epilepsy have autism [153].
When these two disorders co-occur they are often also associated with intellectual
disability. While both ASD and epilepsy are considered heterogeneous disorders with
multiple pathophysiologies and etiologies, there may still be some common underlying
pathophysiological mechanisms that can help to explain why these two conditions
frequently co-occur. For example, it has been proposed that both ASD and epilepsy are
disorders of synaptic plasticity that result in excitation and inhibition imbalances in the
developing brain. Synaptic plasticity refers to the process where synapses, which are
the connections between two neurons, get strengthened through experience or practice.
Synaptic plasticity relies on a variety of proteins whose genes are interrupted in certain
genetic conditions that are associated with autism and epilepsy. Many of these
conditions are also co-morbid with ASD and epilepsy and include such conditions as
Rett Syndrome, Fragile X, and tuberous sclerosis [154].
The effect of seizures and epileptogenesis on the developing brain is important to
understand. There are a number of possible effects of seizures and epileptogenesis on
the developing brain on synaptic plasticity. Emerging evidence indicates that seizures
that occur early on in life may alter the functioning of neurotransmitters and intrinsic
neuronal properties of the brain, which may possibly contribute to cognitive impairments
as well as learning impairments.
Gamma-Aminobutyric acid (GABA) is the primary inhibitory neurotransmitter in the
brain, and the GABA-A receptors are those that mediate most fast synaptic inhibition.
Changes in inhibitory neurotransmission have been known to affect learning, a common
difficulty seen in those with ASD [155, 156]. Changes in excitatory neurotransmission can
also lead to behavioral or learning differences after seizures early in life.
Nursece4less.com 65
Glutamate is the main excitatory neurotransmitter in the brain, whose activity is
mediated by a number of receptor subtypes, including N-Methyl-D-aspartate (NMDA)
and non-NMDA, ionotropic receptors and metabotropic receptors. Excitatory signaling is
critical for different types of long-term potentiation (LTP) and hippocampal learning. It
has been found in some studies [157, 158] that mutant mice that lack subtypes of α-Amino-
3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA) or NMDA receptors have
impaired learning. Further, changes in neuromodulatory pathways can also contribute to
behavioral or learning differences following early-life seizures.
Tuberous SclerosisTuberous sclerosis also frequently co-occurs with both ASD; a high co-occurrence is
also seen with epilepsy. Tuberous sclerosis is a neurocutaneous disorder that is
characterized by benign tumors and mental retardation, as well as epilepsy and autistic
disorder. This syndrome results from mutations of tuberin or hamartin; together these
inhibit the phosphatidyl inositol 3-kinase (PI3) signaling pathway involving the
mammalian target of rapamycin (mTOR) as well as a cascade of other downstream
kinases that stimulate cell growth and proliferation, and protein translation [154].
Mutations of tuberin of hamartin in tuberous sclerosis lead to a hyperactivation of mTOR
and downstream signaling pathways, and results in increased cell growth and
proliferation and abnormal gene expression. The precise mechanisms of ASD in
tuberous sclerosis are not known at this time. However, it is believed that ASD may
stem from persistent seizures that occur early in the development of certain regions of
the brain, such as those responsible for social perception and communication, located
in the left temporal lobe [159]. Further, alterations in expression of certain glutamate and
GABA-A receptor subunit as well as decreases in glutamate transporter GLT-1 may
help bring about imbalances in excitation and inhibition [160, 161].
Sensory Processing DisorderUnusual sensory processing has been reported in ASD [162]; however, most of the
research has been focused on sensory processing disorders in children. Previous
studies show that unusual sensory responses are present in most children who have
Nursece4less.com 66

ASD [163]; this has been identified since the earliest description of ASD [164]. These
sensory abnormalities have primarily been described in relation to vision, taste, sound,
touch, and smell [165], to include hyper and hypo sensitivity as well as general sensitivity
overload. Additionally, responses have been reported as early as 6 – 12 months of age
and are considered one of the earliest indicators of ASD in young childhood.
It is accurate that many individuals with ASD focus on details. One study indicates [166]
that this particular trait may lie beneath stereotyped routines as well as repetitive
interests and behaviors. The study examined 29 children who were diagnosed with
either high functioning autistic disorder or Asperger syndrome who had completed the
Embedded Figured Test (EFT). Parents or caregivers completed the Short Sensory
Profile and Childhood Routines Inventory. The study found significant correlation
between the degree of the amount of restricted and repetitive behaviour that was
reported by parents or caregivers and the degree of sensory abnormalities.
Another study that examine sensory processing in adults utilizing the Adult/Adolescent
Sensory Profile (AASP) indicated that 94.4% of the participants being studied reported
extreme levels of sensory processing [162] in at least one sensory quadrant of the profile.
Further, analysis of the patterns of sensory processing impairments suggests that
individuals with ASD may experience extremely different, although severe sensory
processing abnormalities. It is important to note that sensory processing abnormalities
in ASD extend across the lifespan; they are not simply present only in childhood.
Therefore, it is essential that the practitioner treat these issues with care in both children
and adults.
Fragile X SyndromeFragile X syndrome is considered the most frequent form of inherited mental retardation
[154]. Further, those with Fragile X and ASD may have a significantly lower IQ than do
those with Fragile X who do not have ASD. Fragile X frequently presents with ASD as
well as epilepsy. A hallmark of Fragile X pathology is a hyperabundance of dendritic
spines with long, thin and immature morphology [167, 168], and Fragile X is a result of an
expanded triplet repeat in the FMR1 gene.
Nursece4less.com 67
Fragile X is a genetic, and therefore medical, diagnosis. This is an important distinction
from ASD, which is a behavioral diagnosis. However, when it is associated with Fragile
X, autism is caused by the genetic changes in the Fragile X gene [169]. This may be
compared to other genetic conditions such as Down syndrome; individuals with Down
syndrome may have related conditions such as autism or hearing loss. If a child is first
diagnosed with ASD and then subsequently diagnosed with Fragile X syndrome, it is
considered that the cause of the ASD is known, the cause being Fragile X.
It is estimated that between 15 – 33% of children who have Fragile X also have ASD
[169]. Many of these children are considered high functioning, as while they do not meet
the criteria for full autistic disorder, they do exhibit autistic like symptoms, such as social
anxiety, poor eye contact, sensory issues, hand flapping, and shyness. ASD is more
common in males with Fragile X than it is in girls with Fragile X. In comparison, it is
estimated between 2 – 6% of children who have ASD also are diagnosed with Fragile X.
This leads researchers to believe that all children with ASD, both male and female,
should be genetically tested for Fragile X as well as other genetic causes of ASD.
Anxiety DisordersThe relationship between ASD and anxiety is not well understood at the moment.
However, it is evident that anxiety is a big problem for a large number of those
individuals who suffer from ASD. One review [170] estimates that comorbidity ranges
from 11 – 84%. Certain variables have an influence on each individual’s experience of
anxiety; these include the type of ASD diagnosis, cognitive function, and level of social
impairment.
There are a number of questions about the presentation and the course of anxiety in
children with ASD, as the development and the course of specific types of anxiety as
seen in ASD patients is not well understood. While the presentation of anxiety in
children with ASD is in some ways similar to the presentation in children without ASD,
some studies [171] have found marked differences. For instance, phobias may be more
common among younger children who have ASD, whereas disorders such as social
phobia or OCD may be more common in adolescents with ASD.
Nursece4less.com 68

It is also thought that anxiety symptoms are often overlooked or mislabeled in children
with ASD, primarily because children with ASD frequently lack the ability to express
themselves in an emotionally accurate way. Additionally, it is thought that children with
ASD face unique and considerable challenges as they transition from childhood into
adolescence, as difficulties with social interactions and an awareness that they are
different from others may lead to problems with anxiety, depression, or hostility [172].
Also, for teens with ASD, the new environments and quickly changing routines that
come with high school as well as hormonal and physical changes may prove to be
overwhelming and lead to anxiety [170]. Therefore, it is essential to understand that
anxiety in children and teens with ASD is not only unique but a constantly shifting and
changing dynamic. Understanding this concept will allow for informed development of
adequate treatment options.
It is also essential to consider the degree to which anxiety in children who suffer from
ASD affects relationships with parents and caregivers, as the quality of these
relationships may in turn have an effect on the child’s mood. For example, if the parent
or caregiver of an ASD child handles anxiety in a positive and calm manner, the
relationship may remain positive, lessening the child’s overall anxiety as opposed to
perpetuating it. In other words, there may be a bi-directional influence [172].
Treatment for children with both ASD and anxiety is woefully inadequate. Further
research is needed in this area, in particular in such areas as adapting traditional
approaches such as cognitive behavioral therapy (CBT) to ASD populations. Further,
more thought should be put into the ways individuals with ASD think, behave, and feel
in order to provide them with the very best and most effective treatment [173]. Of the
treatments that are available, a multimodal approach is often considered the best
approach, taking into consideration the child’s learning style, as well as strengths and
limitations. The multimodal approach would include such approaches as individual
therapy, occupational therapy (for children with sensory sensitivities or sensory-seeking
behavior), and school consultations (to add structure), just to name a few approaches.
Medications can sometimes help alleviate severe anxiety as well as complement
Nursece4less.com 69

therapy, although medications can affect the ASD brain differently than the normal
brain. Parent education and parental support groups sometimes also help by providing
a stable foundation for the anxious ASD child.
One review maintains that issues with anxiety “likely cause additional social and
developmental impairment above and beyond the impairment caused by the core
difficulties associated with ASD” [170]. The review further points out that ASD conditions
are lifelong conditions and that a large number of individuals with ASD will need
psychiatric care as they progress toward adulthood. Therefore, the need for accurate
diagnosis and treatment of psychiatric conditions in those individuals with ASD is
essential.
Parents and caregivers can assist in diagnosis by being observant of their child’s
behavior at home and school. For instance, the child may start to act out more at home
or school, or may display an increase in repetitive behavior or restrict more. The child
may not be able to report symptoms accurately or could deny feeling anxious, despite
showing symptoms that clearly display a problem, so it is essential that practitioners
instruct parents to be observant to behaviors that are normal or abnormal for their child,
as a child with ASD may not have insight into his or her inner feelings or anxious
thoughts.
Intellectual DisordersIntellectual disorders and ASD co-occur at very high rates. It should also be noted that
the greater the severity of one of these disorders, the more the effect there appears to
be on the other [38]. Intellectual disorders (ID) present cognitive, social, and adaptive
skills deficits. Also, ID is frequently accompanied by stereotyped and challenging
behaviors, such as repetitive behaviors [174]. Comorbid psychopathologies of a number
of types – for example, depression, anxiety, or schizophrenia – may also present
themselves [175]. All of these issues may be problematic for both the individual suffering
from ASD and the practitioner, and these issues can prove to be debilitating [176].
One study [177] speculates that a great deal of the recent advances in ASD treatment
has been with people who have ASD and are intellectually normal. Further, they posit
Nursece4less.com 70
that as a consequent, many of those individuals with ID may be overlooked. This is the
case despite the fact that there is knowledge that ID co-occurs with ASD, and this
knowledge has existed for several decades.
It should be noted that those with co-occurrent ID and ASD have different needs than
those individuals who simply have ID or ASD alone. There are therefore 3 distinct
groups present: those with ID, those with ASD, and those with co-occurrent ID and ASD
[178]. Currently, it is difficult to make a clear distinction between symptoms in these
groups. More scale development is required to make this distinction easier.
The combination of ASD and ID offers a number of challenges and deficits across a
range of skills and behaviors that are not only seen in ASD or ID. For example, in
individuals who had “severe and profound” ID with co-occurrent ASD, one study [179]
found that these individuals had greater behaviorally based feeding issues, particularly
where food refusal and selectivity were concerned, as compared to those individuals
who had ID on its own.
Challenging behaviors have also recently seen a great amount of increased study. For
example, researchers have discovered that as IQ decreases, the severity of ASD and
challenging behaviors increases, making ASD and ID major risk factors [180]. Murphy et
al [39] discovered that severe IQ and ASD were correlated with higher rates of
challenging behaviors, but these correlations were not across the board. In particular,
self-injury was correlated to severity of autism [180]. For those children with autism,
functional assessment for challenging behaviors indicated that these behaviors were
maintained through escape or retention of tangible items.
Those children who have co-occurrent ASD and ID do not tend to grow out of
challenging behavior; rather, the challenging behaviors tend to persist of the life span
with persons who have the highest rates of challenging behaviors early in life still having
the highest rates of challenging behaviors later in life. Murphy et al [181] observed this to
be the case in a study of 141 people who suffered severe ID and autistic disorder in a
12-year follow-up study. Practitioners should consider patterns of challenging behavior
to be a high priority, as these problem behaviors occur at a very high rate. However, it is
Nursece4less.com 71

important to note that there is still much to be learned. The available research on this
topic is small at the moment but is promising.
Attention deficit hyperactivity disorder (ADHD)Children who have ASD and ADHD have some of the same features, which may
complicate diagnosis [183]. For example, both experience attention deficit and over
activity, behavior problems, and social difficulties. Often, the child is simply diagnosed
with ADHD and a diagnosis of ASD is missed.
To further complicate matters, according to the DSM as well as the ICD-10, a diagnosis
of either autism or Asperger syndrome automatically precludes a diagnosis of ADHD
[184]. However, there is most certainly symptom overlap, as seen in population-based
twin studies [185, 186] as well as a recent epidemiologically based study that reported a
high rate of ADHD in autism and ASD [187]. In the DSM-V the diagnosis of ASD will no
longer preclude a diagnosis of ADHD.
It is estimated that there is an approximate 30% prevalence of ADHD in individuals with
ASD. This is about 6 times higher than the prevalence of ADHD in children and
adolescents worldwide [188]. Further, autistic-like symptoms in those with ADHD are
higher than in children who are healthy [189]. These findings preclude a co-occurrence of
the disorders by chance.
There are risk factors for the development of the combination of ASD and ADHD. One
risk factor is genetics. Both ASD and ADHD are highly heritable neurodevelopmental
disorders. It is estimated that approximately 70 – 80% of the phenotypic variance of
each of these disorders can be explained by genetic factors [190, 191]. Family studies
indicated increased ASD-like symptoms in both affected and non-affected siblings of
ADHD patients, which signifies a familiarity of the co-occurrence of ADHD and ASD
symptoms [189]. Further, according to twin studies, which utilized questionnaire data on
ASD and ADHD symptoms, approximately 50 – 70% of the co-variance of ASD and
ADHD symptoms can be explained by shared genetic factors [185, 186].
Nursece4less.com 72

Non-genetic biologic factors also pose a risk. Some studies have started to focus on the
relevance of environmental risk factors for both ASD and ADHD [191]. Some
environmental biologic risk factors increase the risk of both ASD as well as ADHD, and
this supports the thought that both of these disorders may be alternate manifestations of
the same risk factors. Recent studies reported increased rates of ASD-like symptoms in
11 year old, previously pre-term children below 26 weeks of pregnancy [182]. This study
was replicated in adults with ADHD [192]. Additionally, several risk factors related to
pregnancy seemed to simultaneously increase the risk of ASD with a combined
diagnosis of ADHD or ADHD symptoms, such as the use of valproic acid [193], maternal
diabetes [194], pre-eclampsia [195], and viral or bacterial infections [196, 197] during
pregnancy. The majority of these risk factors has only been examined recently and is
not yet well replicated.
Well-replicated factors that are specific to ADHD are pre-pregnancy obesity, which
increases the risk of inattention symptoms [198], and smoking during pregnancy, which in
particular is a risk factor for hyperactive and impulsive behavior. This risk factor also
increases the risk of a comorbid conduct disorder with aggressive behavior in children
who have ADHD [199-201]. Smoking during pregnancy has been excluded as a risk factor
for ASD however. For ASD, increase in paternal age has been shown to be a particular
risk factor [202]. On the other side, younger maternal age seems to be a risk factor
specific to ADHD [200]. The exact mechanism of how these risk factors influence the
developing brain is not yet determined.
Finally, non-genetic psychosocial factors pose a risk. For ASD, these factors have not
yet been adequately defined, whereas for ADHD, several of these risk factors have
been very strongly replicated in longitudinal studies. For example, an association exists
between family conflicts and divorce, maternal depression, paternal antisocial
personality disorder, and lowered familial socio-economic status with increased rates of
ADHD as well as increased symptoms of inattentiveness and hyperactivity and
impulsivity [200, 201]. Therefore, these risk factors appear to be specific to ADHD and may
also increase ADHD symptomology in those children who suffer from ASD.
Nursece4less.com 73

In regard to psychosocial risk, the relevance of psychosocial risk factors for comorbid
ASD and ADHD has been indicated by population-based study, wherein a higher area
of deprivation was a specific risk factor for co-occurring ADHD in children who have
ASH [187]. In children with ADHD who also have increased ASD-like symptoms, family
risk factors in one study were predictive of increased ASD-like symptoms [203], which
indicates one of two things: either there is some relevance of psychosocial risk factors
to ASD symptoms in general or there is the possibility that an increase in ASD
symptoms in ADHD may represent a particular ADHD subtype but not the same
disorder as ASD with no ADHD. Therefore, it may be concluded that there are
overlapping factors at play that lead to the comorbid diagnosis of ASD and ADHD.
In examining the new DSM-V rules that allow for a joint diagnosis of ASD and ADHD
[204] the following are highlighted:
Previous versions of the DSM forced practitioners to choose between a diagnosis
of ASD or ADHD, which may have prevented those with both disorders from
receiving the course of treatment they really needed.
The DSM-V is going to allow for a dual diagnosis of ASD and ADHD.
Practitioners will no longer have to qualify symptoms of one disorder or the other;
for example, diagnosing an individual with ASD and calling his or her ADHD
symptoms “ADHD-like” in order to offer treatment for ADHD.
Under the new guidelines, practitioners will be able to directly analyze whether or
not those with a primary diagnosis of ADHD and some ASD symptoms may
benefit from the strategies designed for treating ASD, for example, social,
speech, or occupational therapy. Also, on the other side of things, those who are
diagnosed with ASD but show symptoms such as hyperactivity, inattentiveness,
or impulsivity could benefit from treatment protocols designed to treat ADHD [205].
The new guidelines will allow practitioners to treat children with drugs such as
Ritalin for conditions they can actually diagnose them with. Until now,
Nursece4less.com 74

practitioners could not dual diagnose and prescriptions for ADHD medications for
those who have ASD were prescribed as off-label medications being given for
“ADHD-like” symptoms.
In addition to the above a benefit may be seen in clinical studies. Studying those who
have both ASD and ADHD may help researchers identify and design treatments specific
to this group.
MANAGEMENT AND PROGNOSIS
Treatment Goals
Lessen deficits
Once the child has been diagnosed with ASD, the treatment program should begin at
once. As indicated above, over the past 15 years there is evidence that has shown early
intervention programs result in much improved outcomes, particularly when started in
very young children. The reason for this is because a younger child’s brain is more able
to change [206]. However, there is really no single best program for children with ASD to
lessen deficits. The key is to combine interventions, with the goal being to engage the
child’s unique combination of special interests in an effort to keep the child involved with
tasks. Good behaviors should also be positively reinforced.
One key factor to lessening deficits is parental involvement, which is instrumental to the
success of treatment. Its important for parents to work side by side with practitioners in
an effort to learn how therapeutic practices may be continued outside of a clinical
setting. This is because parents are the child’s primary teachers. Therefore, impressing
on the parents how important it is that they remain active and involved in their child’s
care is crucial.
Some common interdisciplinary approaches that are utilized to lessen deficits for
individuals with ASD are listed and explained below:
Nursece4less.com 75

Speech therapy:
Speech therapy is conducted by a professionally trained speech therapist. This
therapy involves a great deal more than just teaching a child how to speak. The
therapist may work with the ASD individual on a number of skills, including skills
such as:
o Nonverbal language skills: Nonverbal language involves communication
such as gestures, PECS (picture exchange communication system),
electronic talking devices, or utilizing other alternative devices such as
iPads or iPhones.
o Speech pragmatics: Speech pragmatics involves training regarding the
suitable speech context.
o Conversational skills: Speech therapists may instruct individuals with ASD
on how to have a back and forth conversation. This is called joint
attention.
o Concept skills: A speech therapist may help an individual with ASD
understand abstract ideas, as they relate to communication.
Occupational Therapy:
Occupational therapy helps those with ASD work on the basic personal and
social skills that are necessary to live independently, as many individuals who
suffer from ASD lack these skills. Some of the things that an occupational
therapist may work on are:
o Provide interventional therapy to assist a child in responding appropriately
to information and stimuli that enters through the senses. Interventions
may include brushing, playing in a ball pit, or other activities that are
aimed at assisting the child who suffers from ASD to better manage how
their body operates in space.
Nursece4less.com 76

o Facilitates play activities that offer instruction as well as assist in teaching
a child in interaction and communication with other people. For an
occupational therapist who specializes in treating those with ASD, this
may mean designing specific structured play therapies, for example,
Floortime, that are developed to building emotional, intellectual, and
physical skills.
o Comes up with strategies to assist the child with transitioning from one
type of setting to another and from one person to another, as well as from
one phase of life to another. For the child who has ASD, this may involve
self-soothing strategies to manage transitions from home to school; for
adults with the condition it could involve learning vocational skills.
o Develops adaptive strategies and techniques to maneuver around
disabilities. One example of this would be teaching the individual typing
should he or she find handwriting too difficult.
Behavioral Therapy:
Amongst those behavioral therapies that are most effective for working with
children who suffer from ASD are the kinds that engage a child’s intrinsic
motivation to learn. This type of motivation utilizes the child’s inner interest in a
topic to encourage the individual to seek more and more knowledge in that
particular area. Behavioral therapists who utilize intrinsic motivators may use a
child’s interest in dinosaurs, for example, to create a story that includes
dinosaurs as the main topic of the story, making learning a reward of the story.
Two of the most frequently used behavioral play therapy interventions utilized
with children who have ASD are Floortime and Relationship Development
Integration (RDI). These are therapies that assist the child in integrating
emotional, intellectual, and social capabilities, as opposed to simply focusing on
skills or isolated behaviors. Both of these types of therapies allow for the
individual’s particular interests in order to encourage learning and to engage the
Nursece4less.com 77
child in their own physical environment as well as at their current level of
cognitive and emotional development.
Another therapy that is frequently utilized, and is considered the gold standard of
behavioral therapy, is Applied Behavioral Analysis (ABA). This behavioral
therapy is a technique that is utilized to reduce inappropriate behavior while
increasing communication and increasing appropriate social behaviors. ABA
frequently utilizes confrontational techniques as well as punishment (i.e. time
outs from preferred objects or activities, or removal of a token) in attempts to
decrease behaviors that are unwanted. Many psychologists and therapists who
work with those who have ASD utilize ABA, making this the most likely therapy to
be utilized in most schools and clinical settings.
Social Skills Training:
Social skills therapists are psychologists, social workers, occupational therapists,
or speech and language therapists whose specialty is working with those who
have ASD. Drama therapists may also teach social skills by working with those
with ASD through scripted scenarios or through improving or critiquing practiced
interactions.
In school settings, social skills therapy can consist of group activities with those
with ASD and those who are not affected. These activities are generally games
and conversation. These activities are generally overseen by social workers or
school psychologists, and can be held in the classroom, playground, or
lunchroom. Social skills groups held at school generally focus on game playing,
conversation, or sharing.
Groups that are held outside of school may have a similar style, but are often
paid for privately. Children may be grouped by similar age and ability, and they
make use of a particular social skill curriculum that is developed by trained
practitioners in social skills therapy. Social skills therapy that is effective provides
those with ASD the opportunity to share, play, converse, and work with their non-
affected peers.
Nursece4less.com 78

Dietary Interventions:
ASD is sometimes caused by a genetic predisposition that is combined with an
environmental trigger. It is thought that this trigger may be a sensitivity to a
particular food that the individual with ASD consumes on a regular basis, such as
gluten, casein, corn, nightshade vegetables such as tomatoes or potatoes, soy,
or food dyes or preservatives.
The individual must be given an IgG food sensitivity test to determine food
sensitivities. This is a blood test that is given by a food allergist. The
recommended treatment for food sensitivities is to cease consumption of the food
that the individual is reacting to, commonly termed a food exclusion diet. Many
parents indicate that their child with ASD became less moody and better
behaved as well as less sensitive to light, sound and touch upon adoption of the
food exclusion diet.
Lessen family stress
For many families, the stress of ASD – whether the diagnosis comes earlier or later –
starts immediately. There is no aspect of family functioning that is not affected, from
having to cope with the affected child’s temper tantrums to dealing with the financial
burden ASD brings or the social isolation that frequently results. Research conducted by
the Interactive Autism Network (IAN) [207] examined the many aspects of stress that
families experience as well as the responses to stress and the feelings that result.
Families answered questionnaires that gauged stress on several measures. Fathers
reported slightly lower overall stress levels than did mothers. The first aspect assessed
was child behaviors. Parents were asked in the Parental Depression History
Questionnaire to determine to what extent their child’s challenging behaviors had a
detrimental impact on their lives. Seventy-two percent of participants indicated that
challenging behaviors had a moderate or great detrimental impact on their lives.
Nursece4less.com 79

Two of the most frequently mentioned contributors of stress that were associated with
challenging behaviors were meltdowns and aggression. Both of these behaviors
required the parent to be hyper-vigilant and made interaction with the world at large
difficult. One of the greatest consequences of challenging behaviors was social isolation
for the whole family. Additionally, parental self-esteem suffered as a result of the child’s
challenging behaviors.
Another aspect assessed was sleep disruption. Parents of children with ASD indicate
that they do not sleep as long and often have sleep that is poorer in quality when
compared to parents of other children, including those who are parents of children with
other types of disabilities [208, 209]. One study that was conducted in Philadelphia stated
that the accumulated poor sleep quality and shorter sleep duration contributes to the
stress of raising a child who suffers from ASD [210]. Children with ASD do themselves
have unusual sleep patterns, including a refusal to sleep, awakening in the middle of the
night, and prolonged rituals at bedtime. Forty-eight percent of parents indicated that
they experienced exhaustion as a result of these sorts of issues, and that these issues
had a moderate or great deal of impact on their stress level.
One other aspect that was assessed involved issues with treatment. A great number of
children with ASD need therapy for issues that are associated not only with ASD but
also with other co-occurring conditions, such as ADHD, depression, or anxiety. It may
cause extreme stress on the parent or caregiver to have to obtain and manage multiple
treatments, which may include physical, speech and language therapy, occupational
therapy, social skills therapy, medication, and ABA, just to name a few. Additionally, all
of these therapies can put a financial burden on the family in addition to placing a
logistical burden on the person coordinating the therapy [211]. Further, many parents and
caregivers feel that they are largely unsupported in seeking and obtaining adequate
treatment for their child, and that quality treatment options are not always readily
available. This adds to the stress of obtaining treatment.
In the aforementioned study, nearly 70% of participants indicated that managing
multiple therapies, including attempting to obtain treatment – either on their own or
Nursece4less.com 80

through insurance – created a moderate or great negative impact. Treatments may also
prove to be disappointing, and it can prove stressful when the family has invested their
time, energy, and money in a treatment option that has not been fruitful. Forty-six
percent of participants indicated that disappointments in treatment outcomes have had
a moderate to great negative impact on their lives. Another aspect that was assessed
was child setbacks. Parents and caregivers can find child setbacks very disheartening,
particularly because they help their children to work so hard to make progress.
The IAN research determined two categories into which setbacks fell: 1) classic
regression, in which the child acquired a skill and then lost that skill, and; 2) more
general setbacks wherein new negative behavior emerged. More than 70% of
respondents indicated that there was a moderate or great deal of negative impact when
the child experienced “a major problem or reversal in progress at school or in some
other area of life” [207]. In other words, setbacks were highly stressful. Some parents
even reported feeling “traumatized” by the setback experience.
One other aspect that was assessed was parental worry about the future. Parents worry
about a number of different factors pertaining to their ASD child’s future. For example,
when the child is young, the parent worries about whether or not the child will be bullied
in the future. As the child grows up, the parent starts to worry about such things as
independent living and employment prospects. Parents also worry about how other
family members will fare. Eighty-nine percent of study respondents indicate that stress
over worrying about the future has a moderate or great negative impact on their lives,
with some respondents indicating that this is an issue they think about every single day.
Despite this stress, many parents and caregivers indicate that they have feelings of
hope for their children.
Another aspect that was assessed was the impact on career and continuing education.
Participants were asked, “What impact, if any, has raising a child with an ASD had on
your own career or continuing education?” [212] Mothers and fathers answered this
question differently. Fathers felt more often than mothers did that there had been no
impact on their education or career, with 44% versus 28%. While many fathers reported
Nursece4less.com 81

that there was a negative impact (46%), more mothers reported that there was a
negative impact (59%). Researchers believe that the reason for this may be because
women are more likely to stay home with children than are men.
Studies show that gender roles are more likely to become more traditional after men
and women make the transition to parenthood [213, 214]. Mothers take on the bulk share of
the domestic duties, even if they work outside the home [215]. Additionally, there is still a
disparity in pay between what men earn and what women earn [216, 217]. Therefore,
women end up more often than men being titled the homemaker. Also, many women
plan on returning to work after having the child, but may not be able to because the
child has extensive needs. Those women who were planning to return to work may
have discovered that having a child with ASD meant missing work or performing below
the standards they had set for themselves, resulting in a negative impact on their
careers.
Many parents reported that challenging child behaviors were one of the major problems
standing in the way to fully achieving at work – these led to phone calls from schools or
care centers that interrupted the work day and contributed to stress at the job.
Additionally, childcare was often an issue. Many parents had issues finding or
maintaining consistent childcare options for their child. These issues often interfered
with work, leading to the parent having difficulty or inability in holding down a job. In one
study that compared families of children with ASD to families of children who were not
affected, parents of children with ASD were nearly 7 times more likely to leave a job as
a result of issues with child care than were parents of children who were not affected
[218].
In addition, in another study conducted by the University of Rochester, researchers
indicated that 39% of parents of those with ASD stated that they had quit a job, changed
a job, or not accepted a job as a result of childcare issues that were related to having a
child who suffered from ASD – this is more than 4 times the 9% that is reported by
families who are raising a child who is not affected [219]. However, not all parents
indicate that raising a child with ASD has had a negative impact. Nine percent of fathers
Nursece4less.com 82

and 13% of mothers indicate that raising a child with ASD has had a positive impact on
their education or career. This did vary somewhat dependent on the parent’s level of
education. A number of these individuals had simply found new careers, many of them
in areas such as autism advocacy, ABA, social work, special education, or a related
field.
One other question asked parents in the IAN research related to the impact, if any, that
raising a child with an ASD had
on their financial situation; nearly
80% of participants indicated that
the impact was a negative one.
One reason for the negative
impact was that many parents
were required to cut back on or
change employment. Additionally,
the cost of evaluation, treatment,
and therapies adds up quickly
and can create financial hardship.
Expenses can be of all kinds, and
can include various types of
therapies.
Many parents reported feeling desperate, with adequate treatment options always
feeling just out of reach. A negative impact was reported by parents of children with
every type of ASD, with 75% of those parents of children suffering from Asperger
syndrome, 78% of those parents of children suffering from PDD-NOS, and 80% of those
parents of children suffering from autistic disorder reporting negative impact. For many
parents, immediate needs are pressing, and adding to the stress and negative impact is
the constant worry of how to pay for future needs.
Nursece4less.com 83
[212]
Average per year expenditures for different ASD
diagnoses.

Another area assessed was how friendships and social networks are impacted, with
nearly 60% of participants indicating that having a child with ASD had a negative impact
on friendships and social networks [221]. Many parents mentioned that getting out into
the social world at large at all could be difficult, in particular if their child suffered from
temper tantrums or from meltdowns, as these tended to draw negative reactions from
other people, particularly strangers. This is particularly true because children with ASD
often appear to be physically fine, unlike many other children with mental or physical
disabilities, making it appear as though the child is simply acting out. This means that
others may be less understanding about what the parent must deal with when the child
acts out, and that the child’s challenges may be attributed to lax parenting as opposed
to an actual disability.
Further to the above, parents indicated that it is not only strangers that make socializing
difficult; parents conveyed that they have sometimes been asked to leave organizations
such as playgroups or churches as a result of their child’s challenges. Therefore, it is no
surprise that feelings such as loneliness or isolation are common amongst those
parents who have children who suffer from ASD. These parents tend to begin to avoid
social situations. In fact, a study indicated that families with children ages 3 – 5 who
have ASD were 70% less likely to attend church services as compared with children
who have ADHD or were not affected [222]. Another study that focused on quality of life
with families who have children with disabilities indicated that those parents who have
children with ASD had more difficulty with social relationships than did parents of
children who had cerebral palsy or mental retardation or parents of children who were
not affected [222]. Further, in a Canadian study where parents were interviewed
regarding their experience raising a child with ASD, many described that they were
made to “live in a world of their own”, or a world that was isolated [223].
Some of the parents interviewed for the IAN research indicated that they themselves
exhibited ASD-like traits, for example, social anxiety [224-226]. This made the social
situation even more difficult for these parents, as they started the situation feeling
socially awkward and then found the situation compounded by their child’s challenges.
Parents also found that friendships, which they had enjoyed previous to having a child
Nursece4less.com 84

with ASD, were strained upon having to care for their child’s challenges. Basically, the
majority of participants in the IAN study indicated that having a child with ASD is a
situation that reveals who one’s true friends are, and while they often found new
friendships, often with those experiencing the same hardships, they also lost friendships
they had previously valued.
Relationships with extended family also suffered. Forty three percent of fathers and
50% of mothers responding to the IAN research indicated that raising a child with ASD
had a negative impact on their relationships with their extended family. For many of the
families, the impact was mixed, with many relatives in denial or dismissive of the ASD
child’s diagnosis. Other relatives were helpful or supportive. Still, an ASD diagnosis may
bring barriers to the typical family interaction, as a child with ASD may have unusual
needs that a non-affected child may not have, such as a particular need for quiet or
routine. This can make events such as birthdays or weddings particularly trying or
isolating for family members who must care for the child who has ASD, not to mention
exhausting, as some participants indicated.
Some study participants indicated that they avoided family functions to avoid the
accompanying stress. Others indicated that they avoided events to avoid the
accompanying critical remarks made by other family members who did not believe the
child had ASD. However, stress with extended family was not without its positive
aspects. Participants indicated that stress helped them focus on who the real supporters
in their journey were and avoid those who would be critical and negative to progress.
The relationship between the parents/caregivers was also researched. Parents who are
raising a child with ASD face challenges that are in addition to balancing work and
family demands, paying bills, and doing chores. These families must also cope with
additional tasks to manage their child, for example, they must investigate treatments,
find providers, wrangle with insurance providers, shuttle their child to appointments, and
prepare for Individualized Education Plan (IEP) meetings. Additionally, there is also an
emotional toll that is exacted on the couple once they learn that their child has ASD.
Nursece4less.com 85

How the couple adapts and copes has implications for the ongoing health of their
relationship. Participants in the IAN research indicated that 60% of mothers and 54% of
fathers stated that raising a child with ASD had a somewhat or very negative impact on
their relationship with each other. However, despite this research finding, couples
raising a child who is suffering from ASD are not all that different from those couples
who are raising an unaffected child when it comes to respect for partner, commitment,
or support [227]. There also is no support for the previously reported 80% divorce rate of
80% for those families who have a child suffering from ASD [228, 229]. One study that
examined the divorce rates for families with children who suffered from a number of
disabilities indicated an average increased rate of 5.97% over the rate of couples for
non-affected children [230].
Researchers have reported a number of different areas of marriage difficulty for parents
with a child with ASD. One study of couples that were raising children with ASD
indicated that these couples experienced lower relationship satisfaction and less social
support than did parents of children who were not affected [231]. Another study that
examined families of children with developmental disabilities, mental health problems,
or no issues over a number of years to determine adaptation and coping mechanisms
found that parents with developmental challenges themselves had lower instances of
employment as well as social participation. However, these parents were the same as
the parents without developmental challenges when it came to such factors as physical
health, psychological health, and marital status. Those parents who had a child with a
mental health issue fared a bit worse. They were also the same as the normal parents
when it came to marital status; however, they experienced a greater instance of
depression and physical issues [232].
Such a research study is particularly important to pay note to, because many children
with ASD also have mental health issues [233-235]. One issue that couples frequently
mentioned was a lack of time together or being too exhausted to make time together.
Additionally, marital conflicts often arose from such issues as division of labor, or if one
of the two parents remained in denial of the child’s diagnosis of ASD. It should be noted
though, that a conflict over division of labor in the household might occur even amongst
Nursece4less.com 86

those couples that have a non-affected child [236]; the issue only becomes more difficult
to navigate when a child with a disability is involved. Gender differences may contribute
in how division of labor occurs, as many men see care of the child as the mother’s
purview. Some participants in the IAN research were deeply involved in meeting their
child’s needs; however, many others were not, and the most common strategy
employed by fathers in dealing with their child’s ASD needs – and a source of stress on
the couple – was avoidance [237].
Conflict and stress need not result in tragedy, however; families, as it turns out, can be
extremely resilient [238, 239]. Families may discover many positive aspects to having a
child with ASD, such as finding pleasure in caring for the child, finding a sense of
accomplishment in progress the child makes, coming to a sense that the marriage and
family has been strengthened by what the family unit has gone through as a whole as a
result of the diagnosis, and increased spirituality. Families may also gain a new
perspective on what is truly important about life.
One last important grouping of note is siblings of those with ASD. Raising a child who
suffers from ASD places a high demand on the time and resources of parents not only
as individuals but also on the family as a whole. Oftentimes, other members of the
family do not get their needs attended to in the same way that the ASD individual gets
his or her needs attended to. Many parents feel that even as they are giving their all in
caring for the child who suffers from ASD, they struggle in caring for the rest of their
family as well as caring for themselves – the feeling is compared to putting the rest of
life on hold while they care for the autistic individual. What results is a constant tension
between the needs of the child with ASD and the needs of the other family members.
While research indicates that the majority of siblings of those who have ASD cope well
with having an autistic brother or sister, these individuals still encounter specific
challenges as they learn how they must deal with having a sibling with ASD.
Some of the top sources of stress for siblings are covered below, and these include [240]:
Embarrassments around their peers as well as jealousy regarding the amount of
time parents spend with the child with ASD.
Nursece4less.com 87

Feelings of frustration over not being able to get a response or engage with the
child with ASD.
Being the target of aggression.
An attempt to make up for the deficits the child with ASD suffers.
Feelings of concern regarding parental stress or grief.
Feelings of concern regarding their own role for caregiving in the future.
There are things that parents – and practitioners as well – can do to help siblings
understand ASD, as well as to help improve sibling interaction and to ensure that all
children in the family feel loved and attended to. First, ASD must be explained to
children early and often, and the information should be given to them in ways that is
appropriate to their developmental age and level of understanding. For example,
preschool age children may need an explanation that will help them comprehend how
the behavior concerns them: saying that the child with ASD doesn’t talk is an
appropriate way to explain this.
An older child may want an explanation that is more interpersonal in nature, for
example, an explanation of how to explain autism to his or her friends. The role is to
listen carefully and pay attention to the unique needs and concerns of the child at every
age, adjusting explanations to fit those needs and concerns. Additionally, explanations
need to be offered again and again. Offering constant opportunities for education allow
the sibling repeated chances to have open conversations where questions and
concerns may be raised. A parent, caregiver, or practitioner may conduct these
conversations.
Secondly, parents and caregivers should work to help their children form a bond with
each other. This is difficult because of the nature of ASD. Many siblings become
discouraged at forming bonds with their ASD siblings; however, they can often be
taught simple skills that will help them engage with their sibling who is suffering from
ASD. Some of these skills include ensuring that the sibling has the ASD child’s
attention, offering simple instructions, and praising good play.
Nursece4less.com 88
Thirdly, to help alleviate sibling stress, it is important to teach parents that they must
make family time special for all family members. Parents frequently work very hard to
make certain that the individual with ASD is fully integrated into family life, but they work
less hard to make certain that this is the case for the other children. One way families
can make certain the non-affected children feel special is by setting aside time for non-
affected children that is separate from time spent together as a family unit.
Fourth, it is important for parents to recognize that being the sibling of a child with ASD
does not end when the sibling reaches adulthood. The sibling of a child with ASD is a
lifelong commitment, just as being the parent of a child with ASD is. Therefore,
practitioners should prepare parents for how to address sibling concerns as siblings
enter early adulthood. For example, young adults may be concerned about the genetics
of ASD and whether or not there is a chance that they themselves may have a child with
ASD. They may also be concerned about whether or not they will end up taking care of
their ASD sibling as he or she ages, particularly when questions of parental aging are
also involved.
All of these questions can create stress, but this stress can be adequately managed by
having open – and consistent – conversations, as siblings grow older. While it is true
that growing up the sibling of an individual with ASD can by challenging, most siblings
handle the challenge very well.
Applied Behavior AnalysisApplied Behavior Analysis (ABA) is the design, implementation, and evaluation of
modification of the individual’s environment in order to produce a socially significant
improvement in the individual’s behavior [241]. ABA includes the usage of direct
observation and measurements as well as the functional analysis of the relationship
between environment and behavior. ABA utilizes changes in environmental events to
produce both practical and significant changes in the individual’s behavior. These
environmental events are generally identified through a number of specialized
assessment methods.
Nursece4less.com 89

ABA is based on the idea that the individual’s behavior is determined by both the past
and current environmental events that are in play with certain organic variables, such as
genetics, as well as ongoing physiological changes. The focus of ABA is on treating
behavioral difficulties by changing the environment as opposed to focusing on variables
that are beyond the direct control of the practitioner. ABA is considered the standard of
care for treatment of ASD [241].
Contributions made by ABA to people who have ASD have been studied; ASD has
previously been considered to be a disorder that has been associated with a poor
prognosis, with only 50% of those individuals affected expected to develop spoken
language skills [242]. Behavioral intervention has been shown to be the most effective
method at addressing the needs of those who have ASD [243]. One early behavioral
intervention study that was conducted by Lovaas in 1987 discovered that 40 hours per
week of early intensive behavioral intervention (EIBI) that involved a curriculum that
emphasized language skills as well as intensively applied behavioral procedures,
resulted in nearly 50% of participants achieving IQs in excess of 100. Participants also
greatly improved their social development and were able to successfully mainstream.
This study is considered monumental in this area of research, as it was the first in
history to produce such incredibly encouraging outcomes for those with autism. The
gains produced in this study were replicated and maintained through several follow-up
studies.
To determine if the gains that were shown in the Lovaas study could be maintained over
an extended time period, McEachin, Smith, and Lovaas [244] conducted a longer-term
study of the same children by studying intelligence and adaptive function 4.5 years later.
Results indicated that the outcome of EIBI was better in relation to gains made by a
control group that received minimal treatment. Sallows and Graupner [245] provided
further validation of the results through a four-year long-term study that demonstrated a
replication of the EIBI success when parent directed and intensive treatment was
utilized. The Lovaas study [246] was met with methodological criticism, however, one
criticism of which was that it lacked randomization. Others have made efforts to
Nursece4less.com 90

replicate the findings of this study while addressing the problems of randomization.
Smith, Groen, and Wynn [247] published the first randomized study that evaluated less
intensive treatment at 20 hours per week; results indicated that even when it was
delivered with less intensity, EIBI showed improvement over parent training on its own.
Although a dose effect, indicated by Smith et al [248], had been raised there was a
question that remained about a need for adherence to the ABA principles, as to whether
intensity alone was a significant variable. Studies that followed worked to validate the
necessity to adhere to ABA versus more eclectic approaches that may be more
common in the early intervention programs. One study [249] validated Lovaas’ style of
EIBI in those children of autism who received Lovaas style of treatment for a period of
one year. The participants in the treatment possessed superior skills as compared with
a control group who had received more eclectic procedures that were considered
generally well regarded. The group that received the Lovaas treatment showed gains
that were evident in areas of language, intelligence, and adaptive behavior. These
findings were later supported in a study by Howard et al [250], which indicated that
classic eclectic approaches did not produce the same type of favorable results that the
Lovaas method resulted in.
Even though the Lovaas method proved to be remarkably successful, there has always
been a focus on improving the quality of treatment methods. Additionally, ABA
practitioners criticized the Lovaas method of EIBI because it did not utilize B.F.
Skinner’s (a psychologist that studied human behavior and language) analysis of verbal
behavior [251]. There are two examples of efforts that did utilize Skinner’s analysis, in
Bondy and Frost’s [252] and Partington and Sundberg’s [253] research. These efforts
resulted in the development of technology as well as teaching procedures that include
the Picture Exchange Communication System [254] and a treatment pack referred to as
the Applied Verbal Behavior pack [255]. It does still remain unclear whether or not
approaches that are based on Skinner’s analysis of verbal behavior are superior to the
Lovaas method. However, regardless of whether this is the case or not, ABA treatments
of all types assist individuals with ASD in living more fulfilling lives. ABA is a wonderful
Nursece4less.com 91

treatment for people with autism. It also is true that people with ASD have been good for
ABA, as elaborated on below.
How have individuals with ASD contributed to ABA and to Society? Those who have
received ABA as well as parents and caregivers who are advocates have made great
strides in efforts to provide those who need this valuable therapy with behavioral
intervention in both home and school environments. Efforts to bring ABA into these
environments have had many favorable impacts on education of those with ASD as well
as on the image of ABA.
Improving the image of behaviorism is important, as there have been common
misconceptions and contentions that misrepresent the significance and achievements of
behaviorism. B.F. Skinner himself identified 20 such contentions [251], which ranged from
the idea that behaviorism ignores the idea of conscious and feelings or states of mind,
the thought the behaviorism formulates behavior as a set of responses to stimuli that
are limited to the prediction and control of behavior that basically present the person as
a machine or robot, the idea that behaviorism works with animals but not people, the
notion that behaviorism is dehumanizing and confined to a laboratory setting instead of
being applicable to real life, and the thought that behaviorism is more concerned with
general principles instead of being focused on the uniqueness of each individual. All of
these ideas are damaging, but as more individuals have become consumers of ABA,
ABA’s image as a discipline has been improved, and its practitioners have come to be
seen as effective and humane teachers. This is one contribution that the ASD world has
made to ABA.
Another way in which those with ASD have helped the world of ABA is by permitting
practitioners to understand whether or not Skinner’s analysis of verbal behavior is valid
and practical. Dixon et al [256] indicate that Skinner’s analysis offered the first overall
accounting of language acquisition from “a naturalistic perspective” [242] and also made
a conceptual and empirical contribution to ABA that is enduring.
Nursece4less.com 92

Children with ASD have also shown the importance of early intervention methods such
as the Lovaas method. Methods such as EIBI may accelerate the learning process in all
children, including those without ASD. For example, if one considers the history of those
children who have been labeled as geniuses, such as Mozart, one may be struck by the
fact that these individuals are often the beneficiaries of large amounts of early training
[242]. Since methods such as EIBI benefit those with ASD so greatly, they may also
benefit those in other populations, such as those with Down syndrome, fetal alcohol
syndrome, and even those who are not disabled.
ABA has a history of focusing on addressing serious problems that affect those who
have severe disabilities [257] and have majorly benefited those who have ASD. While
ABA has not been integrated into mainstream science and remains in a niche in the
special education system, there is no denying the benefits it has produced for those
who suffer from ASD.
Structured TeachingThose who suffer from ASD thrive best in very well organized and highly structured
environments. Structured environments are considered those that promote a clear
understanding of schedules, activities, and expectations not just for the individual who
suffers from ASD but also for their caregivers and teachers. Specifically, the structured
environment allows the individual with ASD to [258]:
Understand and predict what is going on in the environment around them
Predict what is expected of them
Acquire new skills
Generalize the skills they acquire from one setting to another [259]
Structured teaching is generally a visually-based approach designed to create a
structured environment that will in turn support individuals with ASD in a number of
educational, community, and home or living environments [260]. The goal of structured
teaching is to create this environment that promotes independence – and ultimately a
decreased need for caregiver support – through incorporating an increased
understanding of the characteristics of ASD and the strengths and interests of the
Nursece4less.com 93

individual [260]. External organization and visual support serves as the basis for
intervention in the structured environment.
Structured teaching has certain specific components, and these are outlined below:
Physical organization and visual boundaries:
This is the usage of visual supports such as furniture, labels, icons, and so on to
make the learning environment more comprehensible and manageable to the
individual. An environment that is physically organized clearly indicates the types
of activities that occurs in each area; this helps promote increased understanding
and attention to each task. Visual boundaries help students understand the rules
of the space, the specific types of activities they should complete in each space,
as well as the behavioral expectations of each space.
Schedules:
Visual schedules offer a visual representation of planned activities in the order in
which they will occur utilizing symbols, pictures, words, photos, icons, or even
actual objects.
Routines:
Routines, when combined with visual schedules, help by assisting individuals
with understanding their environment and becoming more flexible. Predictable
routines serve as another form of structure, meaning that students with ASD
experience decreased anxiety in routine situations. When their anxiety is
lowered, students frequently demonstrate increased attention to tasks. In
addition, once an individual with ASD learns the routine, he or she will increase in
independence.
The primary goal of routines is to offer a framework for activities that will occur
within the individual’s schedule. Once the framework is established, the specific
context details may continually change [260]. For instance, once an individual
understands the basic routine of their language arts lessons, the teacher may
change the specific content. Since the individual with ASD may have difficulty
Nursece4less.com 94

paying attention, it is often helpful to provide each individual with his or her own
set of directions. An individual schedule placed into the individual’s agenda will
increase the individual’s chances of success in following a schedule or directions.
When routine is consistent and expectations are made clear, independence is
increased and level of learning is often higher.
Work systems:
Work systems are sequences that are visually structured and provide
opportunities to practice skills, activities, or concepts that have been previously
taught. The key here is that these are visually structured to increase
independence.
Task organization:
Visually structured tasks are highly incorporated and organized visual
instructions. These structured activities clearly indicate what activity the individual
should complete, the steps for completing the task, as well as the important and
essential features of the task. Tasks are selected based on assessment
information utilizing emerging skills. Tasks are developed so that the person
utilizing the system knows what to do simply by looking at the materials and the
design. There may be a picture or written instructions. Also, limiting the work
area by utilizing a box tray or folder assists the individual with ASD in knowing
what to focus on in a particular task. It is important to make certain that all
materials are secure; this lessens frustration. To know what is important, the task
may have highlighting in certain important parts, a limited number of items, be
color coded, or labeled.
There are several ways to create highly organized learning environments; these should
all be adapted to meet the needs of the individual suffering from ASD. These include:
Paying attention to individual consideration:
a. Consider the interests, strengths and needs of the individuals in
the particular setting at hand
b. Consider safety issues
Nursece4less.com 95

Designing the physical space and developing the visual boundaries:
a. Link the physical set up to the needs of the individuals in that
particular setting
Developing the schedules
Creating the work system
Organizing the tasks
a. Choose the tasks based on an assessment of the individual
b. Design the tasks to indicate direction
Implementing and monitoring progress
a. Make sure to teach the particular steps of the system. Utilize
strategies such as prompting, modeling, and reinforcement in
the teaching process.
b. Make sure to collect data on each individual’s ability to remain
actively engaged in the environment.
Structured teaching may be used in any setting or may be utilized to support any
individual with ASD. Further, any caregiver, educator, or practitioner, may use the
principles of structured teaching to support an individual suffering from ASD. These
strategies may be used at home, in educational environments, and in community living
settings, as well as to promote success at work.
Speech and Language TherapyMost ASD behavior intensive therapy programs include a speech-language component.
This is because many individuals with ASD experience language difficulties. With a
number of techniques, speech-language therapy addresses a number of challenges
faced by those individuals who suffer ASD. For example, some individuals who suffer
ASD do not speak, while others enjoy speaking but have problems utilizing
conversational speech or even understanding language or nonverbal cues when others
are speaking.
Speech-language therapy is made to coordinate with the mechanics of speech as well
as with the meaning and social usage of language. Speech-language therapy programs
Nursece4less.com 96
start with an individual evaluation by a speech-language therapist to assess the
individual’s verbal aptitude and to determine where the individual may be challenged.
From this evaluation, the therapist then sets goals based on the individual’s challenge
areas. In every case, the goal is to assist the person in communication in more effective
ways.
Even if a person is nonverbal, they can benefit from the skills of a speech-language
therapist. These individuals may benefit from augmentative and alternative
communicative (AAC) devices or methods. The Picture Exchange and Communication
System (PECS) is one of the most commonly utilized methods with children or adults
who have little or no verbal language skills. This method allows children or adults with
ASD to develop a vocabulary through which they may articulate desires, observations,
or feelings. This system may be taught and utilized at home, in classrooms, or in a
number of other settings.
Augmentative and Alternative Communication
At the beginning of the PECS program, the instructor teaches the individual to exchange
a photo for the object – for example,
the adult would exchange the picture
of the apple for the apple itself. With
further instruction, the individual then
learns to distinguish pictures as well
as symbols and utilizes them to form
sentences. Even though PECS is a
visually based system, the program
reinforces and emphasizes verbal
communications. Caregivers may purchase standard PECS systems as part of a
manual or put together their own by gathering photos from everyday sources, for
example, magazines, newspapers, and books.
Nursece4less.com 97
[261]

Other augmentative and alternative communicative devices include devices that may be
specially programmed, such as iPads and iPhones. A speech-language therapist may
provide therapy in a one on one setting, in small groups or in a classroom setting.
Social Skills TherapySocial skills are considered “socially acceptable learned behaviors that enable a person
to interact with others in ways that elicit positive responses that assist in avoiding
negative responses” [262]. One of the biggest areas that those who suffer from ASD
experience deficits is the area of social skills. There are five basic tenets of social skills
programming in individuals with ASD:
Individuals who suffer ASD have a desire to establish meaningful social
relationships.
If those with ASD are to be successful socially, then they must be given the skills
to be successful.
Successful social behaviors are not always “appropriate” social behaviors.
Social success is dependent upon the individual’s ability to adapt to his or her
environment.
Social interaction skills are not the equivalent of academic skills.
There are 3 integrated components that form up the essence of social interaction.
These are: thinking, feeling, and doing.
In order to approach social skills therapy in those with ASD, a five-stage approach must
be taken. This approach includes:
Identifying and assessing areas of need
Discerning between skill acquisition deficits and performance deficits
Selecting appropriate intervention strategies
Implementing intervention strategies
Evaluating the selected program and modifying the program as needed
Nursece4less.com 98

The social skills assessment is by far the most essential piece of this approach. The
purpose of the assessment is to discover: a child’s current level of performance; current
strengths as well as limitations; identify skills to teach, and; answer the important
question, “What is precluding the child from establishing and maintaining social
relationships?” [262].
The most common social skills difficulties that social skills therapy addresses are
difficulties in social initiation, difficulties with reciprocity and terminating interaction,
difficulties with non-verbal communication, difficulties with social cognition, difficulties
with perspective and self-awareness, and difficulties with social anxiety or social
withdrawal.
Occupational TherapyOccupational therapy addresses engagement in “activities…of everyday life, named,
organized, and given value and meaning by individuals and a culture” [263]. Occupational
therapy services focus primarily on enhancing participation in these activities, based on
an individual’s own goals and priorities for participation in these activities.
Occupational therapy focuses on a number of skills, including cognitive, physical, and
motor skills. The goal is to assist in helping the child or adult gain independence that is
age-appropriate and allow the individual to participate more fully in life. For an individual
with ASD, occupational therapy frequently focuses on skills for appropriate play or
leisure, learning, or caring for oneself.
Therapy starts with a therapist certified in the area of occupational therapy evaluating
the individual’s developmental level as well as their learning styles and social abilities.
The individual’s environmental needs are also assessed. Based on the evaluation, the
therapist selects strategies and goals designed to enhance certain skills. For example, a
goal may include dressing independently, feeding or grooming oneself, or using the
toilet on one’s own. Occupational therapy typically involves half-hour or one-hour
sessions, with the frequency of sessions determined by each individual’s needs.
Nursece4less.com 99

Additionally, the individual suffering ASD practices the skills with guidance at home or in
other settings, such as school.
PHARMCOLOGY
Current MedicationsEven though prescription medication is common for the treatment of ASD, there is not
much evidence that medications do much good. Surveys indicate that as many as 50%
of children with ASD take some psychiatric medications – most often these are
antidepressants, antipsychotics, or stimulants [264].
In one recent survey of 2853 children in the Autism Treatment Network, 27% of
respondents were using at least one psychotropic medication. Use of medication
ranged from 11% in children ages 3 – 5 years to 66% in those 12 – 17 years of age.
Most of the use was related to comorbid psychiatric diagnoses, which included
diagnoses such as ADHD or ADHD-like symptoms, bipolar disorder, obsessive-
compulsive disorder, anxiety, and depression. Despite the fact that there are a wide
number of medications utilized to treat patients with ASD, there is little evidence that
exists to show that medication is effective.
Educational interventions are still considered the cornerstones of treatment. These
typically involve behavioural or rehabilitative components to address the deficits that
exist with ASD. The components may involve occupational therapy, behaviour
modification, or speech and language therapy. However, medication may be considered
in the treatment of ASD if non-pharmacologic interventions have failed or if maladaptive
behaviours are severe. Medications are not intended to treat the core symptoms or
ASD; they also cannot cure ASD. Medications are considered adjuncts, and they may
be utilized to decrease the severity of symptoms as well as to help patients participate
Nursece4less.com 100
in more active ways in educational interventions or to assist patients in living outside of
institutional settings.
Patients with ASD are more sensitive to the side effects of medications, so practitioners
must take care to observe that the benefits of utilizing medications in ASD patients
outweigh the risks of the development of adverse reactions to such drugs. Medication
often utilized to treat symptoms related to ASD was frequently chosen based on their
ability to treat the same symptoms in other psychiatric disorders. For instance, Selective
Serotonin Reuptake Inhibitors (SSRIs) are utilized to treat stereotypical behaviour
based on the use of these medications in obsessive-compulsive disorder. Many
medications utilized in the treatment of ASD symptoms do not carry any sort of FDA
indication for the usage of treatment in ASD.
Studies of medication usage in ASD populations are sparse and often have small
sample sizes. Trials are often also complicated by the concomitant usage of other
medications utilized to treat symptoms related to ASD. Frequently, researchers have
difficulty recruiting enough study participants. The medications most commonly used to
treat ASD are listed below [264]:
Antipsychotics:
These are the most studied type of medication when it comes to the use of medication
in the treatment of ASD. The primary usage is for the aggression, irritability, and the
self-injurious behaviours that are associated with ASD. However, antipsychotics may
also be used to treat stereotypical behaviours and ADHD-like behaviours.
Haloperidol is one antipsychotic that has been utilized and studied for usage in treating
ASD. An average dosage of 1.12 mg/d has been shown in 2 clinical trials to decrease
maladaptive behaviours [265]. Doses exceeding this dosage show no additional
effectiveness. Usage of this antipsychotic was associated with a high incidence of side
effects. These side effects included sedation, increases in irritability, and dystonia. At
doses of 1.75 mg/d, 1/3 of patients developed dyskinesia that primarily affected the face
and mouth.
Nursece4less.com 101

Over 90% of the antipsychotics prescribed to children are second-generation atypicals
(SGAs). Risperidone is the most well studied SGA in ASD and is considered one of the
most commonly prescribed of the antipsychotics in children. Risperidone and
aripiprazole are the only two SGAs that carry an FDA indication for treating associated
irritability in children with ASD. Risperidone has been shown to reduce maladaptive
behaviour in ASD. The Research Units on Pediatric Psychopharmacology (RUPP)
Autism Network studies convey strong evidence for the efficacy of risperidone in
treatment of ASD [266]. In an 8-week double-blind, randomized, placebo-controlled study
of 101 children who ranged in age from 5 – 17 years, a mean dosage of 1.8 mg/d of
risperidone resulted in a 14.9 decrease in the ABC-irritability (ABC-I) subscale. This was
versus -3.6 points for the placebo group.
Risperidone does come with some side effects. These include fatigue, drowsiness, and
tremor. Aripiprazole was shown to reduce symptoms of irritability in those with ASD in
some small studies. The strongest evidence for the efficacy of this treatment comes
from two manufacturer-sponsored trials that led to the drug’s approval by the FDA for
treatment of symptoms associated with ASD. Both trials were 8-week trials on children
ages 6 – 17 years [267, 268]. Participants had to have both a diagnosis of ASD as well as
irritability-type behaviours such as aggression, tantrums, or self-injurious behaviours.
The first trial consisted of a flexible dosage schedule that started at 2 mg/d that
increased weekly to a maximum dosage of 15 mg/d by 6 weeks. In 98 participants with
a mean age of 9.3 years, there was a between group change in the ABC-I scale of -7.9
[267]. Side effects to the medication were seen in 91.5% of participants. The most
common side effects of this medication were fatigue, sedation, somnolence, drooling,
vomiting, diarrhea, and tremor. The second trial consisted of fixed-dosage aripiprazole,
with dosage being 5 mg, 10 mg, or 15 mg daily, given to 218 patients with a mean age
of 9.7 years [268]. Decreased in ABC-I were statistically significant across all doses as
compared to placebo. In the group receiving the 5 mg dosage, the total change was -
4.0; in the group receiving the 10 mg dosage, the total change was -4.8, and; in the
group receiving the 15 mg dosage, the total change was -6.0. Side effects were
Nursece4less.com 102

experienced by 85.2 – 89.8% of all of the participants on the medication and resulted in
17 withdrawals from the study.
Evidence for the usage of other SGAs is fairly sparse. Olanzapine and ziprasidone have
each had 1 clinical trial that demonstrate that they may reduce maladaptive behaviours
in those who suffer from ASD; however, the sample sizes in both trials were very small
(<20). In other small trials, quetiapine showed some mixed results. These medications
remain unproven [265, 269].
Selective Serotonin Reuptake Inhibitors (SSRIs):
Treatment with SSRIs is common. This is because the maladaptive and repetitive
behaviors frequently exhibited by those with ASD resemble those with obsessive-
compulsive disorder. Research evidence has shown mixed results. One trial of
citalopram in 149 children did not find any benefit [269].
In early trials, fluvoxamine was shown to improve repetitive behaviours and language
use in 8 out of 15 adults, but a trial that followed did not find similar responses in
children [265]. Another trial of paroxetine in 15 patients was initially shown to have
positive benefits on aggressive and self-injurious behaviours, but the effects waned
after 4 weeks of treatment [270]. One small trial of escitalopram in 28 participants
indicated improvement in the ABC-I scale [265].
There are two medications that have shown promise. These medications are sertraline
and fluoxetine. Setraline has been shown to improve aggression and self-injurious
behaviour. In one study, sertraline improved both of these behaviours in 8 out of 9
patients [265]. In another trial, 57% of ASD patients displayed significant decreases in
aggression and repetitive behaviours when given a mean dosage of 122 mg/d of
sertraline [270]. However, those with Asperger syndrome did not show any response to
the medication. In a study of fluoxetine in 34 children ranging in age from 5 – 17 years,
fluoxetine given at mean dosages of 0.38 mg/kg/d decreased the compulsion subscale
of the Yale-Brown Obsessive Compulsive Scale by 1.55 points. This was as compared
to 0.25 points for placebo [271]. In another study of 37 adult patients with ASD, a mean
Nursece4less.com 103

dosage of 64.75 mg/d of fluoxetine led to a decrease in the Yale-Brown Obsessive
Compulsive Scale of 3.7 points [272]. Side effects for fluoxetine were generally mild, and
included vivid dreams, insomnia, dry mouth, and headache.
Stimulants and Atomexetine:
Individuals who suffer from ASD often also have ADHD-like symptoms. These
symptoms may include symptoms such as hyperactivity, distractibility, excitability, and
difficulty concentrating. Psychostimulants and often considered the first line to treat
these types of symptoms. However, unlike children who have ADHD, children who have
ASD are not as responsive to stimulants and may have an increased sensitivity to side
effects such as emotionality or agitation.
Methylphenidate is the preferred medication, mostly because it has been used in most
of the clinical research. Short acting formulas should be used first so as to gauge
tolerance [273]. Although there are a number of trials that demonstrate the efficacy of
methylphenidate in treating the ADHD-like symptoms in children who have ASD, the
strongest evidence to this point comes from RUPP trials. In a 4-week trial of 72 children
ranging in age from 5 – 14 years who were treated with low dosages (0.125/mg/kg/d),
medium dosages (0.25/mg/kg/d) and high dosages (0.5/mg/kg/d) of methylphenidate in
3 divided dosages. During the first phase, forty-nine percent were found to respond to
the medication. However, 18% stopped the medication because they were unable to
tolerate it.
During the crossover phase, the ABC-I decreased from 30.9 – 33.2 to 17.2 – 20.1
(dependent upon the evaluator) [274]. In the second phase, which was conducted as an
open label, 8-week trial of 34 responders who were dosed on what was determined to
be their best response dosage, response was maintained. Side effects were most
commonly irritability, sadness, lethargy, dullness, and social withdrawal. In a follow-up
analysis of 33 participants from this study, it was indicated that there was substantial
improvement in self-regulation, joint attention, and the ability to regulate one’s emotions
[275].
Nursece4less.com 104

Two small studies indicate that there are potentially minor benefits of atomoxetine in
those children with ASD and ADHD-like symptoms. The first study was a crossover
study that consisted of 16 participants ranging in age from 5 – 15 years. Over 6 weeks
the patients were given a mean atomoxetine dosage of 44.2 + 21.9 mg/d; patients
experienced a mean decrease of 5 points on the ABC-I hyperactivity scale as compared
to 0.1 point for placebo [276]. In the second study, 97 participants ranging in age from 6 –
17 years were assigned randomly to either a fixed dose atomoxetine regimen (1.2
mg/kg/d) or a placebo regimen. After 8 weeks, participants on the atomoxetine
experienced an 8.2-point decrease in the 5-point ADHD Rating Scale (ADHD-RS) score
as compared with 1.2 for placebo [277].
In both trials, atomoxetine was well tolerated. The most common side effects were
decreased appetite, nausea, fatigue, and early morning awakening. The drug’s
manufacturer sponsored both of these trials. Although they do suggest that there is a
possible benefit in this drug in the treatment of ADHD-like symptoms in those individuals
who suffer from ASD, further research is needed before this medication may be
considered a first line therapy.
Even though clonidine and guanfacine have been utilized to treat ADHD, there is sparse
data on their usage in ASD. Both risperidone and aripiprazole have been shown to
decrease ADHD-like symptoms in those children who also have ASD. However, there is
a risk of weight gain and movement disorders with these medications. Therefore, these
medications are not recommended unless there is a high degree of impulsivity that
threatens the child’s life, for example, the child displays dangerous or impulsive running
or jumping. Another example would be a child who displays excessive irritability or
aggression [273].
Cholinesterase Inhibitors and Glutamatergic Antagonist (Memantine):
Medication typically utilized to treat Alzheimer’s Disease that may be added to their
treatment plan. There has been increased interest in utilizing both cholinesterase
inhibitors and the glutamatergic antagonist memantine to improve executive level
functional deficits such as decision making, problem solving, and social deficits in those
Nursece4less.com 105

patients with ASD. The interest in this avenue of treatment stems from findings in
autopsies that indicate a deficit of cholinergic receptors as well as abnormal functioning
of those receptors in the prefrontal regions and cerebral cortex. There have only been
small trials of these types of agents and these agents are not yet proven [278].
One 10-week trial conducted with 34 participants with donepezil at 10 mg/d indicated
that participants did not show any difference on tests that were made to measure
cognitive functions such as verbal ability or problem solving [279]. In another open label,
12 week study conducted with 32 participants ranging in age from 2 – 12 years,
rivastigmine dosed at 0.8 mg twice a day was shown to improve expressive speech and
autistic behaviour, as indicated by a 3 point drop in the Childhood Autism Rating Scale
Score [278]. Galantamine has been shown to bring about mild improvement in such
behaviour as hyperactivity, eye contact, and inappropriate speech, but these results are
limited [280, 281].
Additional autopsy findings have shown a decreased neuronal size in the greatly
interconnected structures in the limbic system. This indicates neuronal immaturity,
which impacts the ability to form memories. An “excitotoxicity” state may occur which
might then lead to high levels of the neurotransmitter glutamate, which in turn may lead
to neuronal death. Small studies of both amantadine, which is related structurally to
memantine, and D-cycloserine, which behaves as a partial agonist at the NMDA
receptor, indicated positive effects on those with ASD. These indications have in turn
led to an interest in memantine as a treatment for ASD [282].
In one 8-week open label study of 14 participants ranging in age from 3 – 12 years,
memantine dosed at 0.4 mg/kg (up to 20 mg/d) culminated in a small improvement on
simple memory tests. Improvements were not seen on other cognitive measurements.
However, participants did show improvements on all ABC subscales [282]. In a second
trial of 18 participants ranging in age from 6 – 19 years, with a mean dosage of
memantine of 10.1 mg/d and over a treatment period that averaged 19.3 weeks,
participants were “much improved” or “very much improved” as indicated on the Clinical
Global Impression [283].
Nursece4less.com 106

The results of studies that use galantamine, rivastigmine, and memantine do show
promise, but they must be confirmed before these medications may be utilized in routine
treatment.
Behavioural Interventions:
Behavioural interventions are still considered the best option. Many early intervention
therapies utilized in treating those with ASD are based on the principles of ABA, which
utilized positive reinforcement as well as other techniques to encourage a behavioural
change. Research suggests that high intensity intervention – considered to be at least
30 hours per week for one to three years – may help improve behaviour and thinking
ability as well as broaden the individual’s language skills, as compared to other, more
broad treatment options.
Future TherapiesFuture therapies for treating ASD may take many paths. Researcher Jeffrey Bradstreet
is examining how neuronal stem cells may help treat ASD [284]. His research is currently
being tested on mice models of autism.
Additional therapies are also being explored. For example, trials on mice utilizing
metabotropic glutamate receptor 5 (mGluR5) blockers have shown promise [285]. It has
been commonly thought that a glutamate imbalance could lead to many of the core
symptoms of ASD; therefore, balancing glutamate may lead to alleviating these
symptoms.
Other therapies involve more individualized behavioral therapies and a more away from
a one size fits all approach to therapy. Since ASDs sit on a wide spectrum, allowing for
a wide spectrum of treatment options that may be tailored to each individual also allows
for optimum treatment, ensuring that each individual may get his or her needs met fully.
VACCINE CONTROVERSY
Nursece4less.com 107

Vaccines are considered one of the great advances in health care. However, many
parents have questions about the possible link between vaccinations and ASD. These
questions persist even after science has debunked connections between vaccinations
and autistic disorder [287].
The concern over autism and vaccines first arose after Wakefield and colleagues
published a small and controversial study in The Lancet in 1998 that suggested that
autism is related to the MMR (measles, mumps and rubella) vaccine. This led to a
media frenzy that in turn led to widespread public concern and a decrease in MMR
vaccination rates as well as several measles outbreaks. The link between the MMR
vaccine and ASD was never substantiated, and The Lancet has since issued a
retraction [288]. Additionally, Wakefield was found guilty of professional misconduct and
lost his license to practice medicine in the U.K. [289]. Nevertheless, the idea that
vaccines and ASD are linked continues to receive a fair amount of public and media
attention. In addition, there has more recently been speculation that thimerosal and
other preservatives are responsible for the rise in autism in spite of the removal of
thimerosal from vaccinations.
Scientifically speaking, vaccinations are safe. The benefits of vaccines far outweigh the
risks they bring. There is not evidence of a relationship between ASD and vaccinations.
Vaccinations in fact save millions of lives as well as prevent long-term complications
from life threatening diseases. Legally speaking, vaccinations have also been found
safe [290]. However, the decision to vaccinate continues to be a hotly debated and highly
emotional issue.
The rise in the incidence of ASD is a public health concern; therefore, it is prudent to
ask if there is any remaining scientific evidence for the concern associating vaccinations
and ASD. Some parents believe that the rise in ASD is due to vaccinations; however,
some researchers believe that the rise in ASD diagnoses is because diagnostic tools
have become more finely honed and specified, allowing for more precise diagnosis than
in previous years, where individuals may have been diagnosed incorrectly. Additionally,
practitioners are receiving a greater level of education on ASD in recent years than they
Nursece4less.com 108

received previously, increasing awareness as well as allowing for more accurate
diagnosis.
In 2009, Fombonne reviewed 43 studies on the epidemiology of ASD, and concluded
that “there is evidence that the broadening of the concept [of autism], the expansion of
the diagnostic criteria, the development of services, and the improved awareness of the
condition have played a major role in explaining this increase, although it cannot be
ruled out that other factors might have also contributed to that trend” [291].
There have been a number of studies that have examined beliefs about immunizations
in families who have individuals who suffer from ASD, and these studies reflect that
beliefs that vaccinations are related to ASD persist. For example, one study that
examined 486 families registered on the Interactive Autism Network [292] found that
26.4% of the families who had at least one child with ASD delayed vaccinations for
other children; 18.9% declined vaccinating their other children. When asked for their
reasons for delaying or declining vaccinations, the degree of belief in the link between
the vaccine and autism was the largest associated factor. In another study of 197
children with ASD in western Los Angeles County, researchers discovered half of
caregivers stopped or altered vaccinations based on the belief that the vaccinations
contributed to ASD [293]. This indicated to researchers that there is still a large gap
between parental belief and practices as well as medical practice and recommendations
for childhood immunizations.
It is important to note that parental beliefs have the power to adversely affect
vaccination practices and rates. In particular, those who are parents of children with
ASD may be more likely than others to change their vaccination practices. These
parents may also serve as sources of trusted information for other families in their
communities who fear ASD. Since there is a high prevalence of ASD, it is important to
understand the concerns and vaccination practices of parents of children with ASD so
that these concerns and practices may be adequately addressed. Researchers in the
Los Angeles County study believe that the large proportion of parents who think that
vaccines cause their child’s ASD is indicative of a communication barrier between
Nursece4less.com 109

practitioners and parents, in addition to the powerful effect the media has on vaccine
practices. This communication barrier may exist for a couple reasons. For example,
physicians may believe that parents of children with ASD might not be open to
discussion about vaccination or that education will not cause a change in beliefs, and
parents may be fearful to ask questions or think that practitioners do not value what they
believe. One study [294] found that those parents who chose not to vaccinate felt
estranged from and untrusting of their doctors, and another study [295] indicated that
those caregivers who had refused the MMR vaccine felt that their good intentions were
not recognized.
Those parents of children with ASD often feel very guilty over the idea that in
vaccinating their child that they may have caused their child’s disorder. They then may
be more likely to decline vaccines because they may be concerned that they could
make their child’s ASD worse or cause ASD in their other children. Parents frequently
perceive that practitioners underestimate safety concerns as well as the impact of ASD
on their family. However, although parents frequently turn to outer sources such as
media for information, it is likely that they will continue to ask their practitioners for
information. Therefore, it is essential for practitioners to advance open discussion as
well as make it clear that both parent and practitioner share the concern for the child’s
welfare.
SUMMARY
Autism Spectrum Disorders (ASD) includes a group of developmental disorders whose
symptoms range on a continuum that runs from mild to severe in expression. ASD is
typically present early in life, anytime from infancy or early childhood. More than
500,000 people in the United States have some form of diagnosed autism. Autism may
keep a child from forming effective relationships with other people, due in part to an
inability to properly interpret facial expressions or emotions. Children with autism
spectrum disorders may be resistant to cuddling or change, and they may play alone or
have delays in speech development. People with ASD also frequently repeat body
movements or have extreme attachments to certain objects.
Nursece4less.com 110
It is not known what causes ASD. However, it is known that there are strong genetic
factors that play a role in causing ASDs to develop. Additionally, non-genetic,
environmental factors play a role in the development of ASD. Most researchers agree
that ASD is a combination of genetic and non-genetic factors, with the individual who is
genetically predisposed having been exposed to factors that then make him or her more
vulnerable to developing an ASD. ASD may develop gradually, or there may be a
regression course, where the individual starts out developing normally and then loses
the skills he or she acquires. There are a number of risk factors for the development of
ASD, including gender, prenatal and perinatal factors, and neuroanatomical anomalies.
The diagnosis of ASD is of utmost important, and it is important that ASD be diagnosed
early. There are many testing tools available for the diagnosis of ASD, and these tools
allow parents and practitioners to assess children to allow for early intervention. While
there is no cure for ASD, early intervention research indicates that early intervention
allows for better outcomes than does standard treatment protocols. The main goals of
treatment in ASD are to lessen individual deficits and to lessen stress on the family.
There are several ways to do this, including structured teaching, behavioral therapy,
speech and language therapy, occupational therapy, social skills therapy, and the use
of medication. In addition, educating family members offers valuable ways to cope.
However, it is important to remember that there are positive aspects to autism, such as
the fact that many people with ASD excel on certain mental levels, such as counting
and measuring, or at art, music, or memory. Many family members also report feeling
accomplished in caring for the individual in their family who has autism, and feeling a
deep sense of fulfillment in being around their ASD sibling or child. Although there is no
cure for ASD, ASD is not a hopeless diagnosis. There is hope for progress both in
research and for those who have an ASD. ASD affects the entire family unit, but with
the proper education and coping tools, the entire family unit can be well equipped to
handle the ASD diagnosis.
Nursece4less.com 111

Please take time to help the NURSECE4LESS.COM course planners evaluate nursing knowledge needs met following completion of this course by completing the self-assessment knowledge
questions after reading the article. Correct answers on page 114.
1. The primary goals of ASD treatments are to:a. lessen deficits and family stresses
b. treatment through use of medication
c. educating family and other caregivers about unique challenges of an
individual with ASD
d. all of the above
2. True of False. ASD is understood to be the result of a combination of genetic and non-genetic factors.
a. Trueb. False
3. Secondary ASD can be caused by:
a. Fragile X syndrome
b. Tuberculosis
c. Rett Syndrome
d. Answers a and c above
4. Rett syndrome predominantly affects:a. males
b. females
c. individuals during adolescence
d. those of African descent
5. Repetitive behaviors in individuals with ASD can include:a. arm and hand flapping
b. rocking or other unusual body movements
Nursece4less.com 112

c. head banging
d. all of the above
6. True or False. Pregnancy and increased risk of ASD with a combined diagnosis of ADHD or ADHD symptoms includes use of valproic acid.a. True
b. False
7. Individuals with ASD often have ADHD-like symptoms, which include:a. hyperactivity, distractibility, excitability, difficulty concentrating
b. impulsivity, short term memory loss, aggression, tension
c. distractibility, fatigue, poor concentration and insomnia
d. poor performance in school, conflict with peers, hyperactivity
8. True or False. Treatment for children with both ASD and anxiety is evolving and more research is needed on how to adapt traditional approaches with cognitive behavioral therapy.a. True
b. False
9. Individuals with ASD thrive best in very well organized and highly structured environments, which include those that:a. promote a clear understanding of schedules
b. provide activities
c. establish expectations
d. all of the above
10.True or False. Treatment with SSRIs is uncommon for children with ASD.a. True
b. False
Nursece4less.com 113

Correct Answers:
1. d
2. a
3. d
4. b
5. d
6. a
7. a
8. a
9. d
10. b
Footnotes:1. Lauritson MB. Autism spectrum disorders. Ear Child Adolesc Psychiatry 2013; 22(Supp1):S37-S42.
2. Ozonoff S, Heung K, Byrd R, Hansen R, Hertz-Picciotto. The onset of autism: patterns of symptom
emergence in the first years of life. Autism Res 2008; 1:320–328.
3. Barbaro J, Dissanayake C. Autism spectrum disorders in infancy and toddlerhood: a review of the
evidence on early signs, early identification tools, and early diagnosis. J Dev Behav Pediatr
2009;30:447–459.
4. Yirmiya N, Charman T. The prodrome of autism: early behavioral and biological signs, regression,
peri- and post-natal development and genetics. J Child Psychol Psychiatry 2010;51:432–458.
5. Rogers SJ. What are infant siblings teaching us about autism in infancy? Autism Res 2009;2:125–
137.
6. Children’s Hospital of Wisconsin. Autistic disorder. Obtained October 14, 2013 from
http://www.chw.org/display/PPF/DocID/22122/router.asp
Nursece4less.com 114

7. Bryce L. Analyzing the 2012 CDC numbers on autism rates. 2012. Picture obtained October 14,
2013 from http://thautcast.com/drupal5/category/tags/race
8. CMAJ. 2012;184(4):E219.
9. Hayes S. A look at Asperger’s Syndrome. Scol Parent & Child 2009;17,2:86-88.
10. National Institute of Neurological Disorders and Stroke. Asperger syndrome fact sheet. Obtained
October 14, 2013 from http://www.ninds.nih.gov/disorders/asperger/detail_asperger.htm
11. Autism Speaks. PDD-NOS. Obtained October 14, 2013 from http://www.autismspeaks.org/what-
autism/pdd-nos
12. American Academy of Child & Adolescent Psychiatry. Bullying Resource Center. Obtained October
14, 2013 from
http://www.aacap.org/AACAP/Families_and_Youth/Resource_Centers/Autism_Resource_Center/
FAQ.aspx
13. National Autism Resources. PDD-NOS signs, symptoms and treatments. Obtained October 14,
2013 from http://www.nationalautismresources.com/autismsymptoms.html
14. MedlinePlus. Childhood disintegrative disorder. Obtained October 14, 2013 from
http://www.nlm.nih.gov/medlineplus/ency/article/001535.htm
15. International Rett Syndrome Foundation. About Rett Syndrome. Obtained October 14, 2013 from
http://www.rettsyndrome.org/about-us/about-rett-syndrome/frequently-asked-questions#001
16. NHS Choices. Autism and Asperger syndrome – causes. Obtained October 14, 2013 from
http://www.nhs.uk/Conditions/Autistic-spectrum-disorder/Pages/Causes.aspx
17. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. American
Psychiatric Association, Washington, DC, USA. 1994.
18. Howlin P. Outcome in high-functioning adults with autism with and without early language delays:
implications for the differentiation between autism and Asperger syndrome. J Autism Dev Disord
2003;33:3–13.
19. Walker DR, Thompson A, Zwaigenbaum L, et al. Specifying PDD-NOS: a comparison of PDD-
NOS, Asperger syndrome, and autism. J Am Acad Child Adolesc Psychiatry 2004;43:172–180.
20. Witwer AN, Lecavalier L. Examining the validity of autism spectrum disorder subtypes. J Autism
Dev Disord 2008;38:1611–1624.
Nursece4less.com 115

21. Sharma S, Woolfson LM, Hunter SC. Confusion and inconsistency in diagnosis of Asperger
syndrome: a review of studies from 1981 to 2010. Autism 2011;16:465–486
22. Lord C, Petkova E, Hus V, Gan W, et al. A multisite study of the clinical diagnosis of different
autism spectrum disorders. Arch Gen Psychiatry 2012;69:306–13.
23. Fein E. German tech company seeks to hire people with autism. Photo obtained from
http://wondergressive.com/news/4991/german-tech-company-seeks-to-hire-people-with-autism/
24. Autism Speaks. Symptoms. Obtained October 14, 2013 from http://www.autismspeaks.org/what-
autism/symptoms
25. Massachusetts General Hospital. Autism Spectrum Disorders. Obtained October 14, 2013 from
http://www2.massgeneral.org/schoolpsychiatry/info_autism.asp
26. BMJ. Learning difficulty and cognitive delay. Obtained October 14, 2013 from
http://www.bestpractice.bmj.com/best-practice/monograph/884/diagnosis/html
27. Geschwind DH. Genetics of autism spectrum disorders. Trends in Cog Sciences 2011;15(9):409-
16.
28. Bailey A, et al. Autism as a strongly genetic disorder: evidence from a British twin study. Psychol
Med 1995;25:63–77.
29. Rosenberg RE, et al. Characteristics and concordance of autism spectrum disorders among 277
twin pairs. Arch Pediatr Adolesc Med 2009;163:907–14.
30. Bolton P, et al. A case-control family history study of autism. J Child Psychol. Psychiatry
1994;35:877–900.
31. Constantino JN, Todd RD. Intergenerational transmission of subthreshold autistic traits in the
general population. Biol Psychiatry 2005:57:655–60.
32. Losh M, et al. Neuropsychological profile of autism and the broad autism phenotype. Arch Gen
Psychiatry 2009;66:518–26.
33. Abrahams BS and Geschwind DH. Advances in autism genetics: on the threshold of a new
neurobiology. Nat Rev Genet 2008;9:341–55.
34. Wang K, et al. Common genetic variants on 5p14.1 associate with autism spectrum disorders.
Nature 2009;459:528–33.
35. Autism Speaks. Autism and epilepsy resources. Obtained October 14, 2013 from
http://www.autismspeaks.org/family-services/epilepsy
Nursece4less.com 116

36. Canitano R. Epilepsy in autism spectrum disorders. Eur Child Adolesc Psychiatry 2007;16(1):61-6.
37. McCarthy J. Children with autism spectrum disorders and intellectual disability. Curr Opin
Psychiatry 2007;20:472-76.
38. Matson JL, Shoemaker M. Intellectual disability and its relationship to autism spectrum disorders.
Res in Dev Disabil 2009;30:1107-14.
39. Matson JL, Dempsey T, LoVullo SV. Characteristics of social skills for adults with intellectual
disability, autism, and PDD-NOS. Research in Autism Spectrum Disorders 2009;3:207–13.
40. Fodstad JC, Matson JL. A comparison of feeding and mealtime problems in adults with intellectual
disabilities with and without autism. J Dev and Phys Disabil 2008;20:541–50.
41. Murphy O, Healy O, Leader G. Risk factors for challenging behaviors among 157 children with
autism spectrum disorders in Ireland. Research in Autism Spectrum Disorders, 2009;3:474–82.
42. Landa RJ et al. Developmental trajectories in children with and without autism spectrum disorders:
the first 3 years. Child Dev 2013;84(2):429-42.
43. Kalb LG, Law JK, Landa R, et al. Onset patterns prior to 36 months in autism spectrum disorders.
Journal of Autism and Developmental Disorders 2010;40:1389–1402.
44. Werner E, Dawson G. Validation of the phenomenon of autistic regression using home videotapes.
Archives of General Psychiatry 2005;62(8):889-95.
45. Pelphrey KA, Carter EJ. Charting the typical and atypical development of the social brain.
Development and Psychopathology 2008:20:1081–1102.
46. Landa R, Garrett-Mayer E. Development in infants with autism spectrum disorders: A prospective
study. J of Child Psychology and Psychiatry 2006;47:629–38.
47. Landa RJ, Holman KC, Garrett-Mayer E. Social and communication development in toddlers with
early and later diagnosis of autism spectrum disorders. Archives of General Psychiatry
2007;64:853–64.
48. Ozonoff S, Young GS, Carter A, et al. Recurrence risk for autism spectrum disorders: A Baby
Siblings Research Consortium study. Pediatrics 2011;128:e488–e495.
49. Sullivan M, Finelli J, Marvin A, et al. Response to joint attention in toddlers at risk for autism
spectrum disorder: A prospective study. J Aut and Dev Disord 2007;37:37–48.
50. Zwaigenbaum L, Bryson S, Rogers T, et al. Behavioral manifestations of autism in the first year of
life. Int J Dev Neuroscience, 2005;23:143–52.
51. deWeerdt S. Dramatic regression leads to severe autism, study finds. SFARI. Obtained October
14, 2013 from http://sfari.org/news-and-opinion/news/2010/dramatic-regression-leads-to-severe-
autism-study-finds.
52. Kalb L. G. et al. J. Autism Dev. Disord. Epub.
53. Bernabei P. et al. J. Autism Dev. Disord. 2007;37:580-588
54. Brereton AV. Regression in autism. ACT-NOW Fact Sheet 54. 2010.
Nursece4less.com 117

55. Barger BD, Campbell JM, McDonough JD. Prevalence and onset of regression within autism
spectrum disorders: a met-analytic review. J Autism Dev Disord. 2013;43(4)817-28.
56. Pierce K, Carter C, Weinfeld M, et al. Detecting, studying, and treating autism early: the one-year
well-baby check-up approach. J Pediatr 2011;159(3):458-65.
57. Autism Speaks. The Early Start Denver Model (ESDM). Obtained October 14, 2013 from
http://www.autismspeaks.org/what-autism/treatment/early-start-denver-model-esdm
58. CDC. Facts about ASDs. Obtained October 14, 2013 from
http://www.cdc.gov/ncbddd/autism/facts.htm.
59. Johnston A, Tam C, Doerr J, et al. Gender differences in presentation of autism spectrum
disorders. Developmental Research Program, Children’s Hospital Boston, Harvard Medical School.
60. Autism Speaks. Study links inducing/augmenting labor with modestly higher autism risk. Obtained
October 14, 2013 from http://www.autismspeaks.org/science/science-news/study-links-
inducingaugmenting-labor-modestly-higher-autism-risk
61. Newschaffer CJ, Fallin D, Lee NL. Heritable and nonheritable risk factors for autism spectrum
disorders. Epidemiol Rev 2002;24(2):137-53
62. Bailey A, Le Couteur A, Gottesman I, et al. Autism as a strongly genetic disorder: evidence from a
British twin study. Psychol Med 1995;25:63–77.
63. Jorde LB, Mason-Brothers A, Waldmann R, et al. The UCLA University of Utah epidemiologic
survey of autism: genealogical analysis of familial aggregation. Am J Med Genet 1990;36:85–8.
64. Smalley SL, Asarnow RF, Spence MA. Autism and genetics. A decade of research. Arch Gen
Psychiatry 1988;45:953–61.
65. Jorde LB, Hasstedt SJ, Ritvo ER, et al. Complex segregation analysis of autism. Am J Hum Genet
1991;49:932–8.
66. Ritvo ER, Jorde LB, Mason-Brothers A, et al. The UCLA University of Utah epidemiologic survey of
autism: recurrence risk estimates and genetic counseling. Am J Psychiatry 1989;146:1032–6.
67. Smalley SL. Autism and tuberous sclerosis. J Autism Dev Disord 1998;28:407–14.
68. Folstein SE, Rutter ML. Autism: familial aggregation and genetic implications. J Autism Dev Disord
1988;18:3–30.
69. Brown WT, Jenkins EC, Cohen IL, et al. Fragile X and autism: a multicenter survey. Am J Med
Genet 1986;23:341–52.
70. Folstein SE, Piven J. Etiology of autism: genetic influences. Pediatrics 1991;87:767–73.
71. Gillberg C. Chromosomal disorders and autism. J Autism Dev Disord 1998;28:415–25.
72. Martinsson T, Johannesson T, Vujic M, et al. Maternal origin of inv dup (15) chromosomes in
infantile autism. Eur Child Adolesc Psychiatry 1996;5:185–92.
73. Cook EH Jr, Lindgren V, Leventhal BL, et al. Autism or atypical autism in maternally but not
paternally derived proximal 15q duplication. Am J Hum Genet 1997;60:928–34.
Nursece4less.com 118

74. Schroer RJ, Phelan MC, Michaelis RC, et al. Autism and maternally derived aberration of
chromosome 15q. Am J Med Genet 1998;76:327–33.
75. Wassink TH, Piven J, Patil SR. Chromosomal abnormalities in a clinic sample of individuals with
autistic disorder. Psychiatr Genet 2001;11:57–63.
76. Ashley-Koch A, Wolpert CM, Menold MM, et al. Genetic studies of autistic disorder and
chromosome 7. Genomics 1999;61:227–36.
77. Bass MP, Menold MM, Wolpert CM, et al. Genetic studies in autistic disorder and chromosome 15.
Neurogenetics 2000;2:219–26.
78. Deykin EY, MacMahon B. Pregnancy, delivery, and neonatal complications among autistic children.
Am J Dis Child 1980;134:860–4.
79. Mason-Brothers A, Ritvo ER, Pingree C, et al. The UCLA University of Utah epidemiologic survey
of autism: prenatal, perinatal, and postnatal factors. Pediatrics 1990;86:514–19.
80. Juul-Dam N, Townsend J, Courchesne E. Prenatal, perinatal, and neonatal factors in autism,
pervasive developmental disorder-not otherwise specified, and the general population. Pediatrics
2001;107:E63.
81. Stromland K, Nordin V, Miller M, et al. Autism in thalidomide embryopathy: a population study. Dev
Med Child Neurol 1994;36:351–6.
82. Miller MT, Stromland K. Teratogen update: a review, with a focus on ocular findings and new
potential uses. Teratology 1999;60:306–21.
83. Rodier PM, Ingram JL, Tisdale B, et al. Linking etiologies in humans and animal models: studies of
autism. Reprod Toxicol 1997;11:417–22.
84. Ingram JL, Peckham SM, Tisdale B, et al. Prenatal exposure of rats to valproic acid reproduces the
cerebellar anomalies associated with autism. Neurotoxicol Teratol 2000;22:319–24.
85. Moore SJ, Turnpenny P, Quinn A, et al. A clinical study of 57 children with fetal anticonvulsant
syndromes. J Med Genet 2000;37:489–97
86. Bescoby-Chambers N, Forster P, Bates G. Foetal valproate syndrome and autism: additional
evidence of an association. Dev Med Child Neurol 2001;43:847–8.
87. DiMartino A, Tuchman RF. Antiepileptic drugs: affective use in autism spectrum disorders. Pediatr
Neurol 2001;25:199–207.
88. Hollander E, Dolgoff-Kaspar R, Cartwright C, et al. An open trial of divalproex sodium in autism
spectrum disorders. J Clin Psychiatry 2001;62:530–4.
89. Plioplys AV. Autism: electroencephalogram abnormalities and clinical improvement with valproic
acid. Arch Pediatr Adolesc Med 1994;148:220–2.
90. The autistic syndromes. New York, NY: American Elsevier Publishing Company, Inc, 1976.
91. Spiker D, Lotspeich L, Hallmayer J, et al. Failure to find cytogenetic abnormalities in autistic
children whose parents grew up near plastics manufacturing sites. J Autism Dev Disord
1993;23:681–2.
Nursece4less.com 119
92. Massachusetts Department of Public Health. Leominster environment and health investigation.
Boston, MA: Environmental Epidemiology Program, The Bureau of Environmental Health
Assessment, Massachusetts Department of Public Health, 1997.
93. Agency for Toxic Substances and Disease Registry. Chemical specific consultation: hazardous
substance exposures and autism. Atlanta, GA: Agency for Toxic Substances and Disease Registry,
Division of Toxicology, Emergency Response and Scientific Assessment Branch, 1999.
94. Agency for Toxic Substances and Disease Registry. Public health assessment: Brick Township
investigation, Brick Township, Ocean County, New Jersey. Atlanta, GA: Agency for Toxic
Substances and Disease Registry, Division of Health Assessment and Consultation, Superfund
Site Assessment Branch, 2000.
95. Bauman ML, Kemper TL. Neuroanatomic observations of the brain in autism: a review and future
directions. Intl J Dev Neuroscience 2005;23(2-3)183-7.
96. Zeilinski BA, Anderson JS, Froehlich AL, et al. scMRI reveals large-sclae brain network
abnormalities in autism. Obtained on October 10, 2013 from: http://www.plosone.org/article/info
%3Adoi
%2F10.1371%2Fjournal.pone.0049172;jsessionid=60B73ECF39A9FFCA4E2B243DC0BDDC83.
97. Schmitz N, Daly E, Murphy D. Frontal anatomy and reaction time in autism. Neurosci Lett
2007;412:12–17.
98. Hardan AY, Girgis RR, Lacerda AL, et al. Magnetic resonance imaging study of the orbitofrontal
cortex in autism. J Child Neurol 2006;21:866–71.
99. Hadjikhani N, Joseph RM, Snyder J, et al. Anatomical differences in the mirror neuron system and
social cognition network in autism. Cereb Cortex 2006;16:1276–82.
100. Hazlett HC, Poe MD, Gerig G, et al. Cortical gray and white brain tissue volume in adolescents and
adults with autism. Biol Psychiatry 2006;59:1–6.
101. Schumann CM, Bloss CS, Barnes CC, et al. Longitudinal magnetic resonance imaging study of
cortical development through early childhood in autism. J Neurosci 2010;30:4419–27.
102. Hardan AY, Muddasani S, Vemulapalli M, et al. An MRI study of increased cortical thickness in
autism. Am J Psychiatry 2006;163:1290–92.
103. Bonilha L, Cendes F, Rorden C, et al. Gray and white matter imbalance–typical structural
abnormality underlying classic autism? Brain Dev 2008;30:396–401.
104. Mitchell SR, Reiss AL, Tatusko DH, et al. Neuroanatomic alterations and social and communication
deficits in monozygotic twins discordant for autism disorder. Am J Psychiatry 2009;166:917–25.
105. Carper RA, Courchesne E. Localized enlargement of the frontal cortex in early autism. Biol
Psychiatry 2005;57:126–33.
106. Hyde KL, Samson F, Evans AC, et al. Neuroanatomical differences in brain areas implicated in
perceptual and other core features of autism revealed by cortical thickness analysis and voxel-
based morphometry. Hum Brain Mapp 2010;31:556–66.
Nursece4less.com 120

107. Herbert MR, Ziegler DA, Makris N, et al. Localization of white matter volume increase in autism and
developmental language disorder. Ann Neurol 2004;55:530–40.
108. Amaral DG, Schumann CM, Nordahl CW. Neuroanatomy of autism. Trends Neurosci 2008;31:137–
45.
109. Hazlett HC, Poe M, Gerig G, et al. Magnetic resonance imaging and head circumference study of
brain size in autism: birth through age 2 years. Arch Gen Psychiatry 2005;62:1366–76.
110. Vidal CN, Nicolson R, DeVito TJ, et al. Mapping corpus callosum deficits in autism: an index of
aberrant cortical connectivity. Biol Psychiatry 2006;60:218–25.
111. Alexander AL, Lee JE, Lazar M, et al. Diffusion tensor imaging of the corpus callosum in Autism.
Neuroimage 2007;34:61–73.
112. Bauman M, Kemper T. ASD. 2010.
113. Strock M. Autism spectrum disorders (pervasive developmental disorders).2007. Photo obtained
October 14, 2013 from http://en.wikipedia.org/wiki/File:Autismbrain.jpg
114. UNC School of Medicine. Brain enlargement in autism due to brain changes occurring before age
2. 2011. Obtained October 14, 2013 from
http://www.med.unc.edu/www/newsarchive/2011/may/brain-enlargement-in-autism-due-to-brain-
changes-occurring-before-age-2
115. UC Davis Health System. Excessive cerebrospinal fluid and enlarged brain size in infancy are
potential biomarkers for autism. 2013. Obtained October 14, 2013 from
http://www.ucdmc.ucdavis.edu/publish/news/newsroom/7884
116. Nordahl CW, Lange N, Li DD, et al. Brain enlargement is associated with regression in preschool-
age boys with autism spectrum disorders. PNAS. 1-6.
117. Delong GR, Bean SC, Brown FR. Acquired reversible autistic syndrome in acute encephalopathic
illness in children. Arch Neurol 1981;38:191–4.
118. Gillberg C. Onset at age 14 of a typical autistic syndrome. A case report of a girl with herpes
simplex encephalitis. J Autism Dev Disord 1986;16:369–75.
119. Gillberg IC. Autistic syndrome with onset at age 31 years herpes encephalitis as a possible model
for childhood autism. Dev Med Child Neurol 1991;33:920–4.
120. Gillberg C, Coleman M. Infectious diseases. The biology of the autistic syndromes. London, United
Kingdom: Mac Keith Press, 1992:218–25.
121. Deykin EY, MacMahon B. Viral exposure and autism. Am J Epidemiol 1979;109:628–38.
122. Birmingham K, Cimons M. Reactions to MMR immunization scare. Nat Med 1998;4:478–9.
123. Taylor B, Miller E, Farrington CP, et al. Autism and measles, mumps, and rubella vaccine: no
epidemiological evidence for a causal association. Lancet 1999;353:2026–9.
124. Fombonne E, Chakrabarti S. No evidence for a new variant of measles-mumps-rubella-induced
autism. Pediatrics 2001;108:E58.
Nursece4less.com 121

125. Dales L, Hammer SJ, Smith NJ. Time trends in autism and in MMR immunization coverage in
California. JAMA 2001;285:1183–5.
126. Kaye JA, Melero-Montez MDM, Jick H. Mumps, measles, and rubella vaccine and the incidence of
autism recorded by general practitioners: a time trend analysis. BMJ 2001;322:460–3.
127. Gillberg C, Heijbel H. MMR and autism. Autism 1998;2:423–4.
128. Farrington CP, Miller E, Taylor B. MMR and autism: further evidence against a causal association.
Vaccine 2001;19:3632–5.
129. Madsen K, Hvid A, Vestergaard M, et al. A population-based study of measles, mumps, and rubella
vaccination and autism. N Engl J Med 2002;347:1477–82.
130. US Food and Drug Administration. Thimerosal in vaccines. Rockville, MD: Center for Biologics
Evaluation and Research, US Food and Drug Administration, 2002.
131. Magos L, Brown AW, Sparrow S, et al. The comparative toxicology of ethyl- and methylmercury.
Arch Toxicol 1985;57:260–7.
132. Zhang J. Clinical observations in ethyl mercury chloride poisoning. Am J Ind Med 1984;5:251–8.
133. Immunization Safety Review Committee, Board on Health Promotion and Disease Prevention,
Institute of Medicine. Immunization safety review: thimerosal-containing vaccines and
neurodevelopmental disorders. Washington, DC: National Academy Press, 2001.
134. Gardener H, Spiegelman D, Buka SL. Perinatal and neonatal risk factors for autism: a
comprehensive meta-analysis. Pediatrics 2011;128(2)344-55.
135. Durkin MS, Maenner MJ, Newschaffer CJ. Advanced parental age and the risk of autism spectrum
disorder. Am J Epidemiol 2008;168(11):1268-76.
136. Cheslak-Postova K, Liu K, Bearman PS. Closely spaced pregnancies are associated with
increased odds of autism in California sibling births. Pediatrics 2011;127(2)246-53.
137. Schmidt RJ, Hansen RL, Hartiala J. Prenatal vtamins, one-carbon metabolism gene variants, and
risk for autism. Epidemiol 2011;22(4)476-85.
138. CDC Autism spectrum disorders – data and statistics. Obtained October 14, 2013 from
http://www.cdc.gov/ncbddd/autism/data.html
139. Le Couteur A, Lord C, Rutter M, et al. Autism diagnostic interview – revised (ADI-R). Western
Psychological Services. 2003.
140. Autism Genetic Resource Exchange. About the ADOS. Obtained October 14, 2013 from
http://research.agre.org/program/aboutados.cfm
141. Brookes Publishing Co. ASQ. Obtained October 13, 2013 from
http://www.brookespublishing.com/resource-center/screening-and-assessment/asq/
142. Brookes Publishing Co. ASQ:SE. Obtained October 13, 2013 from
http://www.brookespublishing.com/resource-center/screening-and-assessment/asq/asq-se/
Nursece4less.com 122

143. Minnesota Department of Health. Brief infant toddler social emotional assessment. (BITSEA).
Obtained October 13, 2013 from
http://www.health.state.mn.us/divs/fh/mch/devscrn/instr/bitsea.html
144. Child Development Review. Child development inventory. Obtained October 13, 2013 from
http://www.childdevrev.com/page15/page17/cdi.html
145. Brookes Publishing Co. CSBS. Obtained October 13, 2013 from
http://www.brookespublishing.com/resource-center/screening-and-assessment/csbs/csbs-dp/
146. Pedstest. Parents’ evaluation of developmental status (PEDS). Obtained October 13, 2013 from
http://www.pedstest.com/LearnAboutPEDS/IntroductiontoPEDS.aspx
147. Pedstest. Parents’ evaluation of developmental status – developmental milestones (PEDS:DM).
Obtained October 13, 2013 from
http://www.pedstest.com/AboutOurTools/LearnAboutPEDSDM.aspx
148. Pearson. Greenspan social-emotional growth chart. Obtained October 13, 2013 from
http://pearsonassessments.com/HAIWEB/Cultures/en-us/Productdetail.htm?Pid=015-8280-
229&Mode=summary
149. Robins, DL. M-CHAT. Obtained October 13, 2013 from
http://www2.gsu.edu/~psydlr/Diana_L._Robins,_Ph.D..html
150. Ehlers S, Gillberg C, Wing L. A screening questionnaire for Asperger syndrome and other high-
functioning autism spectrum disorders in school age children. J Aut Dev Disord 1999;29(2)129-41.
151. WPS. Social communication questionnaire (SCQ). Obtained October 13, 2013 from
http://portal.wpspublish.com/portal/page?_pageid=53,70432&_dad=portal&_schema=PORTAL
152. Tuchman R, Moshe SL, Rapin I. Convulsing toward the pathophysiology of autism. Brain Dev
2009;31:95–103.
153. Brooks-Kayal A. Epilepsy and autism spectrum disorders: are there common developmental
mechanisms? Brain & Dev 2010;32:731-8.
154. del Cerro S, Jung M, Lynch G. Benzodiazepines block long-term potentiation in slices of
hippocampus and piriform cortex. Neuroscience 1992;49:1–6.
155. Seabrook GR, Easter A, Dawson GR, Bowery BJ. Modulation of long-term potentiation in CA1
region of mouse hippocampal brain slices by GABAA receptor benzodiazepine site ligands.
Neuropharmacology 1997;36:823–30.
156. Nakazawa K, Quirk MC, Chitwood RA, et al. Requirement for hippocampal CA3 NMDA receptors in
associative memory recall. Science 2002;297:211–8.
157. Mead AN, Stephens DN. Involvement of AMPA receptor GluR2 subunits in stimulus-reward
learning: evidence from glutamate receptor gria2 knock-out mice. J Neurosci 2003;23:9500–7.
158. Numis AL, Major P, Montenegro MA, et al. Identification of risk factors for autism spectrum
disorders in tuberous sclerosis complex. Massachussetts General Hospital M.A.P. 2011.
Nursece4less.com 123
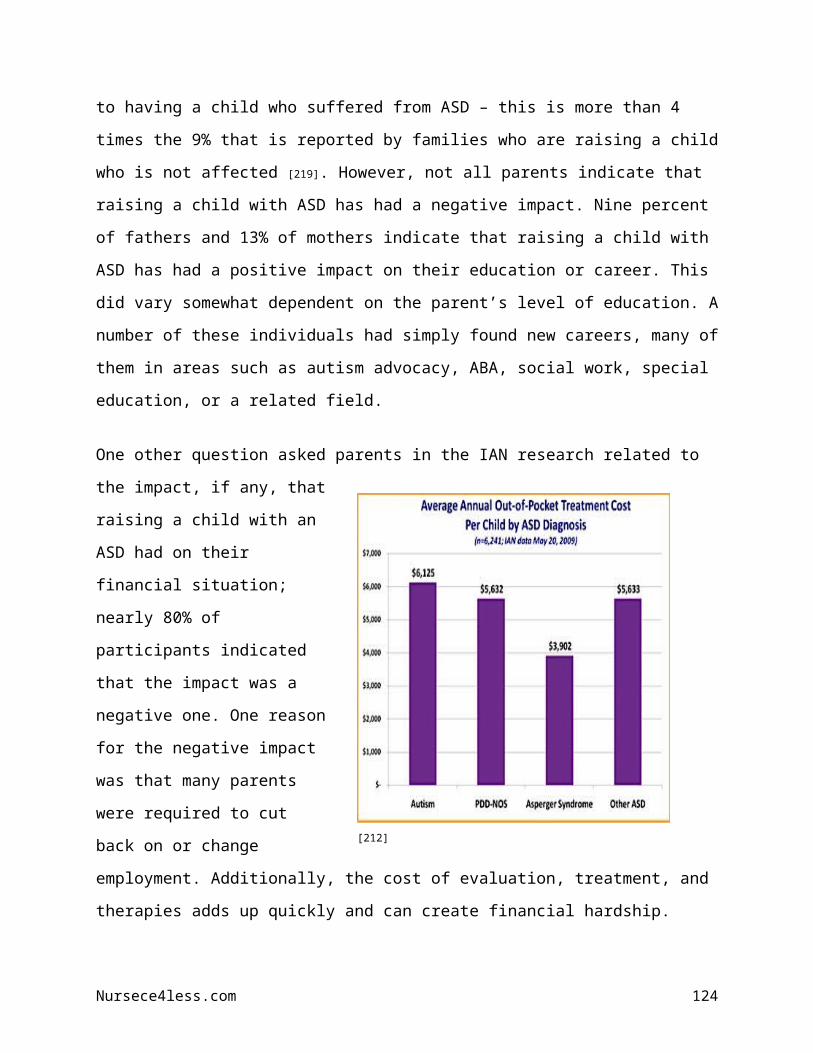
159. White R, Hua Y, Scheithauer B, et al. Selective alterations in glutamate and GABA receptor subunit
mRNA expression in dysplastic neurons and giant cells of cortical tubers. Ann Neurol 2001;49:67–
78.
160. Wong M, Ess KC, Uhlmann EJ, et al. Impaired glial glutamate transport in a mouse tuberous
sclerosis epilepsy model. Ann Neurol 2003;54:251–6.
161. Crane L, Goddard L, Pring L. Sensory processing in adults with autism spectrum disorders. Autism.
2009;13(3):215-28.
162. Rogers SJ, Hepburn S, Wehner E. Parent Reports of Sensory Symptoms in Toddlers with Autism
and Those with Other Developmental Disorders. J Aut and Dev Disord 2003;33(6):631–42.
163. Asperger H. “Autistic Psychopathy in Childhood” in U. Frith (ed.) Autism and Asperger Syndrome.
Cambridge: Cambridge University Press. 1944/1991;37-92.
164. O’Neill M, Jones RS. Sensory-perceptual abnormalities in autism: a case for more research? J Aut
and Dev Disord 1997:27(3):283–93.
165. Chen Y, Rodgers J, McConachle H. Restricted and repetitive behaviours, sensory processing and
cognitive style in children with autism spectrum disorders. J Aut Dev Disord. 2009;39:635-42.
166. Grossman AW, Aldridge GM, Weiler IJ, et al. Local protein synthesis and spine morphogenesis:
fragile X syndrome and beyond. J Neurosci 2006;26:7151–5.
167. Irwin SA, Galvez R, Greenough WT. Dendritic spine structural anomalies in fragile-X mental
retardation syndrome. Cereb Cortex 2000;10:1038–44.
168. National Fragile X Foundation. Autism and Fragile X syndrome. Obtained October 14, 2013 from
http://www.fragilex.org/fragile-x-associated-disorders/fragile-x-syndrome/autism-and-fragile-x-
syndrome/
169. White SW, Oswald D, Ollendick T, et al. Anxiety in children and adolescents with autism spectrum
disorders. Clin Psych Rev. 2009;29:216-29.
170. Farrugia S, Hudson J. Anxiety in adolescents with Asperger syndrome: negative thoughts,
behavioral problems, and life interference. Focus on Autism and Other Developmental Disabilities,
2006;21:25−35.
171. Tantam D. The challenge of adolescents and adults with asperger syndrome. Child Adolesc
Psychiatric Clin N Am 2003:12:143−63.
172. Jennet HK, Hagopian LP. Identifying empirically supported treatments for phobic avoidance in
individuals with intellectual disabilities. Behavior Therapy 2008;39:151−61.
173. Lee LC, Harrington RA, Chang JJ et al. Increased risk of injury in children with developmental
disabilities. Research in Developmental Disabilities 2008;29:247–55.
174. Holden B, Gitlesen JP. The relationship between psychiatric symptomatology and motivation of
challenging behaviour: A preliminary study. Research in Developmental Disabilities 2008:29:408–
13.
Nursece4less.com 124

175. Wilkins J, Matson JL. A comparison of social skills profiles in intellectually disabled adults with and
without ASD. Behavior Modification 2009;33:143–55.
176. Hurley AD, Levitas AS. The importance of recognizing autism spectrum disorders in intellectual
disability. Mental Health Aspects of Developmental Disabilities 2007;10:157–61.
177. Noterdaeme M, Euders A. Autistic disorders and mental retardation: How to recognize and
differentiate? Tagliche Praxis 2009;50:111–21.
178. Fodstad JC, Matson JL. A comparison of feeding and mealtime problems in adults with intellectual
disabilities with and without autism. Journal of Developmental and Physical Disabilities
2008;20:541–50.
179. Goldmon S, Wang C, Salgado MW, et al. Motor stereotypies in children with autism and other
developmental disorders. Developmental Medicine and Child Neurology 2009;51:30–8.
180. Murphy GH, Beadle-Brown J, Wing L, et al. Chronicity of challenging behaviours in people with
severe intellectual disabilities and/or autism: A total population sample. Journal of Autism and
Developmental Disorders 2005;35:405–18.
181. Johnson S, Hollis C, Kochhar P, et al. Psychiatric disorders in extremely preterm children:
longitudinal finding at age 11 years in the EPICure study. J Am Acad Child Adolesc Psychiatry
2010;49:453–63.
182. Mayes SD, Calhoun SL, Mayes RD, et al. Autism and ADHD: Overlapping and discriminating
symptoms. Res in Aut Spect Disord. 2012;6:277-85.
183. Taurines R, Schwenck C, Westerwald E, et al. ADHD and autism: differential diagnosis or
overlapping traits? A selective review. ADHD Atten Def Hyp Disord. 2012;4:115-39.
184. Reiersen AM, Constantino JN, Grimmer M, et al. Evidence for shared genetic influences on self-
reported ADHD and autistic symptoms in young adult Australian twins. Twin Res Hum Genet
2008;11:579–85.
185. Ronald A, Simonoff E, Kuntsi J, et al. Evidence for overlapping genetic influences on autistic and
ADHD behaviours in a community twin sample. J Child Psychol Psychiatry 2008;49:535–42.
186. Simonoff E, Pickles A, Charman T, et al. Psychiatric disorders in children with autism spectrum
disorders: prevalence, comorbidity, and associated factors in a population-derived sample. J Am
Acad Child Adolesc Psychiatry 2008;47:921–29.
187. Polanczyk G, de Lima MS, Horta BL, et al. The worldwide prevalence of ADHD: a systematic
review and metaregression analysis. Am J Psychiatry 2007;164:942–48.
188. Mulligan A, Anney RJ, O’Regan M, et al. Autism symptoms in attention-deficit/hyperactivity
disorder: a familial trait which correlates with conduct, oppositional defiant, language and motor
disorders. J Autism Dev Disord 2009;39:197–209.
189. Freitag CM, Hanig S, Schneider A, et al. Biological and psychosocial environmental risk factors
influence symptom severity and psychiatric comorbidity in children with ADHD. J Neural Transm
2012b;119:81–94.
Nursece4less.com 125

190. Lichtenstein P, Carlstrom E, Rastam M, et al. The genetics of autism spectrum disorders and
related neuropsychiatric disorders in childhood. Am J Psychiatry 2010.
191. Halmoy A, Klungsoyr K, Skjaerven R, et al. Pre- and perinatal risk factors in adults with attention-
deficit/hyperactivity disorder. Biol Psychiatry. 2011.
192. Cohen MJ, Meador KJ, Browning N, et al. Fetal antiepileptic drug exposure: motor, adaptive, and
emotional/behavioral functioning at age 3 years. Epilepsy Behav 2011;22:240–46.
193. Lyall K, Pauls DL, Spiegelman D, et al. Pregnancy complications and obstetric suboptimality in
association with autism spectrum disorders in children of the Nurses’ Health Study II. Autism Res
2011;epub.
194. Mann JR, McDermott S, Bao H, et al. Preeclampsia, birth weight, and autism spectrum disorders. J
Autism Dev Disord 2010;40:548–54.
195. Atladottir HO, Thorsen P, Ostergaard L, et al. Maternal infection requiring hospitalization during
pregnancy and autism spectrum disorders. J Autism Dev Disord 2010a;40:1423–30.
196. Mann JR, McDermott S. Are maternal genitourinary infection and pre-eclampsia associated with
ADHD in school-aged children? J Atten Disord 2011;15:667–73.
197. Rodriguez A. Maternal pre-pregnancy obesity and risk for inattention and negative emotionality in
children. J Child Psychol Psychiatry 2010;51:134–43.
198. Freitag CM, Staal W, Klauck SM, et al. Genetics of autistic disorders: review and clinical
implications. Eur Child Adolesc Psychiatry 2010b;19:169–78.
199. Galera C, Cote SM, Bouvard MP, et al. Early risk factors for hyperactivity-impulsivity and
inattention trajectories from age 17 months to 8 years. Arch Gen Psychiatry 2011;68:1267–75.
200. Sciberras E, Ukoumunne OC, Efron D. Predictors of parentreported attention-deficit/hyperactivity
disorder in children aged 6–7 years: a national longitudinal study. J Abnorm Child Psychol
2011;39:1025–34.
201. Hultman CM, Sandin S, Levine SZ, et al. Advancing paternal age and risk of autism: new evidence
from a population-based study and a meta-analysis of epidemiological studies. Mol Psychiatry
2011;16:1203–12.
202. Kroger A, Hanig S, Seitz C, et al. Risk factors of autistic symptoms in children with ADHD. Eur
Child Adolesc Psychiatry 2011;20:561–70.
203. Johnson M. New rules allow joint diagnosis of autism, attention deficit. October 2012. Obtained
October 10, 2013 from: http://sfari.org/news-and-opinion/news/2012/new-rules-allow-joint-
diagnosis-of-autism-attention-deficit.
204. Cortese S. et al. Expert Rev. Neurother. 2012;12:461-73.
205. The Advisory Board on Autism and Related Disorders (ABOARD). Treatment goals for autism.
Obtained October 10, 2013 from: http://autism-support.org/characteristics-for-autism/treatment-
goals-autism/.
Nursece4less.com 126

206. Autism Speaks, Inc. IAN Research Report – Part I. Obtained October 10, 2013 from:
http://www.autismspeaks.org/news/news-item/ian-research-report-family-stress-%E2%80%94-part-
1.
207. Meltzer LJ. Brief report: Sleep in parents of children with autism spectrum disorders. J Pediatr
Psychology, 2008;33(4):380-86.
208. Cotton S, Richdale A. Brief report: parental descriptions of sleep problems in children with autism,
Down syndrome, and Prader-Willi syndrome. Research in Developmental Disabilities
2006;27(2):151-61.
209. Meltzer LJ. Brief report: Sleep in parents of children with autism spectrum disorders. Journal of
Pediatric Psychology 2008;33(4):380-86.
210. Kogan MD, Strickland BB, Blumberg SJ, et al. A national profile of the health care experiences and
family impact of autism spectrum disorder among children in the United States, 2005-2006.
Pediatrics 2008;122:e1149-e1158.
211. Autism Speaks, Inc. IAN Research Report – Part II. Obtained October 10, 2013 from:
http://www.autismspeaks.org/news/news-item/ian-research-report-family-stress-%E2%80%94-part-
2.
212. Cowan CP, Cowan PA, Heming G, et al. Transitions to parenthood: His, hers, and theirs. Journal of
Family Issues 1985;6:451-81.
213. Kluwer ES, Heesink JA, Van de Vliert E. The division of labor across the transition to parenthood: A
justice perspective. Journal of Marriage and Family 2002;64:930-43.
214. Hochschild A, Machung A. The second shift. Penguin Books: New York 2003.
215. Lips HM. The gender pay gap: Concrete indicator of women's progress toward equality. Analyses
of Social Issues and Public Policy 2003;3(1):87-109.
216. Institute for Women's Policy Research. Fact sheet: The gender wage gap: 2008.
217. Lee LC, Harrington RA, Louie BB, et al. Children with autism: Quality of life and parental concerns.
J Aut and Dev Disord 2008;38:1147-60.
218. Montes G, Halterman JS. Child care problems and employment among families with preschool-
aged children with autism in the United States. Pediatrics 2008;122:e202-e208.
219. Montes G, Halterman JS. Association of childhood autism spectrum disorders and loss of family
income. Pediatrics 2008;121(4):e821-e826.
220. Autism Speaks, Inc. IAN Research Report – Part III. Obtained October 10, 2013 from:
http://www.autismspeaks.org/news/news-item/ian-research-report.
221. Mugno D, Ruta L, D'Arrigo VG, et al. Impairment of quality of life in parents of children and
adolescents with pervasive developmental disorder. Health and Quality of Life Outcomes
2007;5:22.
222. Woodgate RL, Ateah C, Secco L. Living in a world of our own: The experience of parents who have
a child with autism. Qualitative Health Research 2008;18(8):1075-83.
Nursece4less.com 127

223. Smalley SL, McCracken J, Tanguay P. Autism, affective disorders, and social phobia. Am J of
Medical Genetics 1995;60(1):19-26.
224. Bishop DV, Maybery M, Maley A, Wong D, Hill, et al. Using self-report to identify the broad
phenotype in parents of children with autistic spectrum disorders: A study using the autism-
spectrum quotient. J of Child Psychology and Psychiatry, and Allied Disciplines 2004;45(8):1431-
36.
225. Losh M, Childress D, Lam K, et al. Defining key features of the broad autism phenotype: A
comparison across parents of multiple and single-incidence autism families. Am J of Medical
Genetics. Part B, Neuropsychiatric Genetics 2008;147B(4):424-33.
226. Brobst JB, Clopton JR, Hendrick SS. Parenting children with autism spectrum disorders: The
couple's relationship. Focus on Autism and Other Developmental Disabilities 2009;24(1):38-49.
227. Rudy LJ. Does autism in the family lead to divorce? Obtained October 10, 2013 from
http://autism.about.com/b/2008/10/13/does-autism-in-the-family-lead-to-divorce.htm.
228. Finke B. Data on autism and divorce. Obtained October 10, 2013 from
http://autismblog.easterseals.com/tag/divorce/
229. Risdal D, Singer GH. Marital adjustment in parents of children with disabilities: A historical review
and meta-analysis. Research & Practice for Persons with Severe Disabilities 2004;29(2):95-103.
230. Brobst JB, Clopton JR, Hendrick SS. Parenting children with autism spectrum disorders: the
couple's relationship. Focus on Autism and Other Developmental Disabilities 2009;24(1):38-49.
231. Seltzer MM, Greenberg JS, Floyd FJ, et al. Life course impacts of parenting a child with a disability.
Am J of Mental Retardation 2001;106(3):265-86.
232. Ghaziuddin M, Ghaziuddin N, Greden J. Depression in persons with autism: Implications for
research and clinical care. J of Aut and Dev Disord 2002;32(4):299-306.
233. Leyfer OT, Folstein SE, Bacalman S, et al. Comorbid psychiatric disorders in children with autism:
Interview development and rates of disorders. J of Aut and Dev Disord 2006;36(7):849-61.
234. Rosenberg R, Kaufmann W, Law JK, et al. Factors associated with psychiatric co-morbidity in
autism spectrum disorders. Autism Research.
235. Simonoff E, Pickles A, Charman T, et al. Psychiatric disorders in children with autism spectrum
disorders: Prevalence, comorbidity, and associated factors in a population-derived sample. J of the
Am Acad of Child and Adolesc Psychiatry 2008;47(8):921-29.
236. Pelchat D, Lefebvre H, Levert MJ. Gender differences and similarities in the experience of
parenting a child with a health problem: current state of knowledge. J of Child Health Care
2007;11(2):112-31.
237. Van Riper M. Families of children with down syndrome: Responding to "a change in plans" with
resilience. J of Pediatr Nurs 2007;22(2):116-28.
Nursece4less.com 128

238. Havens CA. Becoming a resilient family: child disability and the family system. Access Today
2005(17). Obtained October 10, 2013 from
http://www.indiana.edu/~nca/monographs/17family.shtml.
239. Autism Society. Siblings. Obtained October 13, 2013 from: http://www.autism-society.org/living-
with-autism/family-issues/siblings.html
240. Behavior Analyst Certification Board. Health plan coverage of applied behavior analysis treatment
for autism spectrum disorder. 2012;1.1
241. Axelrod S, McElrath KK, Wine B. Applied behavior analysis: autism and beyond. Behav Intervent
2012;27:1-15.
242. Bailey J, Burch M. 25 Essential skills and strategies for the professional behavior analyst:expert
tips for maximizing consulting effectiveness. NY, NY: Routledge, 2010.
243. Lovaas OI. Behavioral treatment and normal educational and intellectual functioning in young
autistic children. J of Consult and Clin Psychol 1987;55:3–9.
244. Sallows GO, Graupner TD. Intensive behavioral treatment for children with autism: four year
outcome and predictors. Am J Mental Retardation 2005;6:417–38.
245. McEachin JJ, Smith T, Lovaas OI. Long-term outcome for children with autism who received early
intensive behavioral treatment. Am J Mental Retardation 1993;97:359–72.
246. Smith T, Groen AD, Wynn JW. Randomized trial of intensive early intervention forchildren with
pervasive developmental disorder. Am J Mental Retardation 2000;(105):269–85.
247. Smith LK, Fowler SA. Positive peer pressure: the effects of peer monitoring on children’s disruptive
behavior. J Applied Behav Analysis 1984;17:213–27.
248. Eikeseth S, Smith T, Jahr E, et al. Intensive behavioral treatment at school for 4- to 7-year-old
children with autism: A 1-year comparison controlled study. Behavior Modification 2002;26:49–68.
249. Howard JS, Sparkman CR, Cohen HG, et al. A comparison of intensive behavior analytic and
eclectic treatments for young children with autism. Research in Dev Disabil 2005;26:359–83.
250. Skinner BF. Verbal behavior. New York: Appleton-Century-Crofts. 1957.
251. Bondy AS, Frost LA. The picture exchange communication system. Focus on Autistic Behavior
1994;9:1–19.
252. Partington JW, Sundberg ML. The assessment of basic language and learning skills: an
assessment, curriculum guide, and tracking system for children with autism or other developmental
disabilities. Danville, CA: Behavior Analysts, Inc. 1998.
253. Frost L, Bondy A. The picture exchange communication system training manual. Cherry Hill, NJ:
PECs, Inc. 1994.
254. Evans VE, Wilde NC, Axelrod S. Classroom management: an overview. In E. M.Anderson, & L. H.
Anderson (Eds.), Psychology of classroom learning: An encyclopedia.Farmington Hills, MI: Cenage
Learning. 2008:162-66.
Nursece4less.com 129

255. Dixon MR, Small SL, Rosales R. Extended analysis of empirical citations with Skinner’s verbal
behavior: 1984–2004. Behavior Analyst 2007;30:197–209.
256. Friman PC. The future of applied behavior analysis is under the dome. Association for Behavior
Analysis International Newsletter 2006;29.
257. Carnahan C. Structured teaching: Online training module (Columbus, OH: OCALI). In Ohio Center
for Autism and Low Incidence (OCALI), Autism Internet Modules, www.autisminternetmodules.org.
Columbus, OH: OCALI. 2009.
258. Iovannone R, Dunlap G, Huber H, et al. Effective educational practices for students identified as
having autism spectrum disorders. Focus on Autism and Other Developmental Disabilities
2003;18(3):150-65.
259. Mesibov G, Shea V, Schopler E. The TEACCH approach to autism spectrum disorders. New York:
Kluwer Academic/Plenum Publishers. 2005.
260. Autism Speaks. What treatments are available for speech, language and motor issues? Obtained
October 10, 2013 from: http://www.autismspeaks.org/what-autism/treatment/what-treatments-are-
available-speech-language-and-motor-impairments
261. Bellini, S. (2011). Overview of Social Skills Functioning and Programming (Columbus, OH: OCALI).
In Ohio Center for Autism and Low Incidence (OCALI), Autism Internet Modules,
www.autisminternetmodules.org. Columbus, OH: OCALI.
262. AOTA. What is occupational therapy’s role is supporting persons with an autism spectrum
disorder? 2010:1-6.
263. Cauffield JS. Medication use in autism spectrum disorders: what is the evidence? Formulary.
2013;48:161-8.
264. Leskovec TJ, Rowles BM, Findling RL. Pharmacological treatment options for autism spectrum
disorders in children and adolescents. Harv Rev Psychiatry. 2008;16:97–112.
265. Research Units on Pediatric Psychopharmacology Autism Network. Risperidone in children with
autism and serious behavioral problems. N Engl J Med 2002;347:314–21.
266. Owen R, Sikich L, Marcus RN, et al. Aripiprazole in the treatment of irritability in children and
adolescents with autistic disorder. Pediatrics 2009;124:1533–40.
267. Marcus RN, Owen R, Kamen L, et al. A placebo-controlled, fixed-dose study of aripiprazole in
children and adolescents with irritability associated with autistic disorder. J Am Acad Child Adolesc
Psychiatry 2009;48:1110–19.
268. Canitano R, Scandurra V. Psychopharmacology in autism: an update. Progr Neuro
Psychopharmacol Biol Psychiatry 2011;35:18–28.
269. Davanzo PA, Belin TR, Widawski MH, et al. Paroxetine treatment of aggression and self-injury in
persons with mental retardation. Am J Ment Retard 1998;102:427–37.
Nursece4less.com 130
270. Hollander E, Phillips A, Chaplin W, et al. A placebo controlled crossover trial of liquid fuoxetine on
repetitive behaviors in childhood and adolescent autism. Neuropsychopharmacology 2005;30:582–
89.
271. Hollander E, Soorya I, Chaplin W, et al. A double-blind placebo-controlled trial of fuoxetine for
repetitive behaviors and global severity in adult autism spectrum disorders. Am J Psychiatry
2012;169:292–99.
272. Mahajan R, Bernal MP, Panzer R, et al. Clinical practice pathways for evaluation and medication
choice for attention-deficit/hyperactivity disorder symptoms in autism spectrum disorders.
Pediatrics 2012;130:S125–S138.
273. Research Units on Pediatric Psychopharmacology (RUPP) Autism Network. Randomized,
controlled, crossover trial of methylphenidate in pervasive developmental disorders with
hyperactivity. Arch Gen Psychiatry 2005;62:1266-74.
274. Jahromi LB, Kasari CL, McCracken JT, et al. Positive effects of methylphenidate on social
communication and self-regulation in children with pervasive developmental disorders and
hyperactivity. J Autism Dev Disord 2009;39:395–404.
275. Arnold LE, Aman MG, Cook AM, et al. Atomoxetine for hyperactivity in autism spectrum disorders:
placebo-controlled crossover pilot trial. J Am Acad Child Adolesc Psychiatry 2006;45:1196–1205.
276. Harfterkamp M, van de Loo-Neus G, Minderaa RB, et al. A randomized double-blind study of
atomoxetine versus placebo for attention-deficit/hyperactivity disorder symptoms in children with
autism spectrum disorder. J Am Acad Child Adolesc Psychiatry 2009;51:733–41.
277. Chez MG, Aimonovitch M, Buchanan T, et al. Treating autism spectrum disorders in children: utility
of the cholinesterase inhibitor rivastigmine tartrate. J Child Neurol 2004;19:165–69.
278. Handen BL, Johnson CR, McAuliffe-Bellin S, et al. Safety and efficacy of donepezil in children and
adolescents with autism: neuropsychological measures. J Child Adolesc Psychopharmacol
2011;21:43–50.
279. Hertzman M. Galantamine in the treatment of adult autism: a report of three clinical cases. Int J
Psychiatry Med 2003;33:395–98.
280. Niederhofer H, Staffen W, Mair A. Galantamine may be effective in treating autistic disorder. BMJ
2002;325:1422.
281. OwleyT, Salt J, Guter S, et al. A prospective, open-label trial of memantine in the treatment of
cognitive, behavioral, and memory dysfunction in pervasive developmental disorders. J Child
Adolesc Psychopharmacol 2006;16:517–24.
282. Erickson CA, Posey DJ, Stigler KA, et al. A retrospective study of memantine in children and
adolescents with pervasive developmental disorders. Psychopharmacology 2007;191:141–47.
283. Autism One. Are stem cells the future of autism biomedical therapies? 2012. Obtained October 14,
2013 from http://www.autismone.org/content/are-stem-cells-future-autism-biomedical-therapies
284. Kong X, Chen L, Wang X. Future directions on autism treatment. NAJ Med Sci 2012;5(3)185-8.
Nursece4less.com 131

285. APA. Individualized treatments are future of autism therapies, according to psychologist. 2012.
Obtained October 14, 2013 from http://www.apa.org/news/press/releases/2012/04/autism-
therapies.aspx
286. McGuinness TM, Lewis S. Update on autism and vaccines. J Psychosocial Nurs 2010;48:15-18.
287. Retraction—Ileal-lymphoid-nodular hypoplasia, non-specific colitis, and pervasive developmental
disorder. Lancet 2010;375:445
288. Burns JF. British medical council bars doctor who linked vaccine with autism. The New York Times
2010;A4.
289. Dyer C. Thimerosal does not cause autism, U.S. court finds. BMJ;2010b;340:c1518.
290. Fombonne E. Thimerosal disappears but autism remains. Archives of General Psychiatry
2008;65(1):15–6.
291. Rosenburg RE, Law JK, Anderson C, et al. Survey of vaccine beliefs and practices among families
affected by autism spectrum disorders. Clin Pediatr. 2012;52(9):871-4.
292. Bazzano A, Zeldin A, Schuster E, et al. Vaccine-related beliefs and practices of parents of children
with autism spectrum disorders. Am J on Intellect and Dev Disabil. 2012;117(3):233-42.
293. Benin AL, Wisler-Scher DJ, Colson E, et al. Qualitative analysis of mother’s decisionmaking about
vaccines for infants: The importance of trust. Pediatrics 2006;117:1532–41.
294. Casiday R, Cresswell T, Wilson D, et al. A survey of UK parental attitudes to the
MMR vaccine and trust in medical authority. Vaccine 2006;24(2):177–84.
Nursece4less.com 132

The information presented in this course is intended solely for the use of healthcare professionals taking this course, for credit, from NurseCe4Less.com. The information is designed to assist healthcare professionals, including nurses, in addressing issues associated with healthcare.
The information provided in this course is general in nature, and is not designed to address any specific situation. This publication in no way absolves facilities of their responsibility for the appropriate orientation of healthcare professionals. Hospitals or other organizations using this publication as a part of their own orientation processes should review the contents of this publication to ensure accuracy and compliance before using this publication.
Hospitals and facilities that use this publication agree to defend and indemnify, and shall hold NurseCe4Less.com, including its parent(s), subsidiaries, affiliates, officers/directors, and employees from liability resulting from the use of this publication.
The contents of this publication may not be reproduced without written permission from NurseCe4Less.com.
Nursece4less.com 133