ASCO GU Oncology 2009 · ASCO GU Oncology 2009 Robert Dreicer, M.D., M.S., FACP Chair Dept of Solid...
54
ASCO GU Oncology 2009 Robert Dreicer, M.D., M.S., FACP Chair Dept of Solid Tumor Oncology Taussig Cancer Institute Professor of Medicine Cleveland Clinic Lerner College of Medicine
Transcript of ASCO GU Oncology 2009 · ASCO GU Oncology 2009 Robert Dreicer, M.D., M.S., FACP Chair Dept of Solid...

ASCO GU Oncology 2009
Robert Dreicer, M.D., M.S., FACP
Chair Dept of Solid Tumor Oncology
Taussig Cancer Institute
Professor of Medicine
Cleveland Clinic Lerner College of Medicine

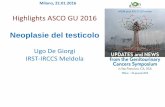
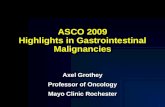
Inclusion Criteria
• mRCC with component of
clear cell histology
• Measurable or evaluable
disease
Exclusion Criteria
• Prior systemic therapy
• Evidence of CNS
metastases
Stratification:
• Nephrectomy status
• MSKCC risk group
•Primary objective: OS
•Secondary objectives: PFS, ORR, and safety
IFN-/Bevacizumab (n=369)
IFN- 9 MU s.c. 3x/week
Bevacizumab 10 mg/kg IV q2w
IFN- (n=363)
IFN- 9 MU s.c. 3x/week
(n = 732)
R
A
N
D
O
M
I
Z
E
Phase III CALGB 90206 Trial: Study
Design (abstract LBA5019)
Rini et al. J Clin Oncol 2009; 27(suppl):239s

Adverse event
Bevacizumab + IFN
(n=366)
IFN
(n=352)
Any grade 3/4 adverse event 79% 61%
Fatigue/asthenia/malaise 37% 30%
Anorexia 17% 8%
Proteinuria 15% <1%
Hypertension 11% 0%
Hemorrhage 2% <1%
Venous thromboembolism 2% 1%
Gastrointestinal perforation <1% 0%
Arterial ischemia 1% 0%
Frequency of selected grade 3 or 4 AEs
LBA5019

Objective Response
Note: patients with measurable disease only
Bev + IFN (n=325) IFN (n=314)
Overall Response rate 25.5%
[95% CI = 20.9-30.6]
13.1%
[95% CI = 9.5-17.3]
CR 3.7% 1.9%
PR 23.4% 12.7%
p < 0.0001
Duration of response 11.9 months
[95% CI = 8.3 – 14.8]
9.7 months
[95% CI = 7.6 – 19.8]
p = 0.362
LBA5019

Time(months)
Ove
rall
Su
rviv
al (p
rob
ab
ility)
IFN BEV/IFNStratified log-rank p=0.069
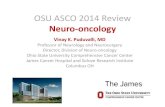
Kaplan-Meier Overall Survival Curves by Treatment Arm
0 6 12 18 24 30 36 42 48 54 60
0.0
0.2
0.4
0.6
0.8
1.0
363 286 221 177 148 118 98 64 37 10 1
369 314 242 190 160 139 116 94 42 17 2
IFN
BEV/IFN
Number of Patients at Risk
---- BEV/IFN: Median OS 18.3 months
IFN: Median OS 17.4 months
Kaplan-Meier Overall Survival by Treatment Arm
LBA5019

Median OS (months) according to treatment
arm and subsequent therapy (LBA5019)
Bevacizumab +
Interferon
Interferon Total(unstratified log-rank
p comparing arms)
Stratified HR
Received
2nd-line
therapy
(n=408)
31.4 26.8 28.2(p=0.079)
0.80 (p=0.055)
Did not
receive 2nd-
line therapy
(n=324)
13.1 9.1 10.2(p=0.059)
0.82 (p=0.108)
Total 18.3 17.4 18.1 (p=0.097)
0.86 (p=0.069)

Authors Conclusions LBA5019
Overall survival is greater in patients with metastatic clear cell RCC receiving bevacizumab plus interferon as initial systemic therapy compared to interferon alone, but does not meet pre-defined criteria for significance
Although the favorable effect of bevacizumab plus IFN on OS is preserved regardless of subsequent treatment, the most robust OS is achieved in patients with favorable underlying disease biology who are able to receive subsequent therapy
The combination of bevacizumab and IFN as initial therapy in metastatic RCC patients results in a significantly greater progression-free survival and objective response rate versus IFNA monotherapy
Toxicity is greater in the combination therapy arm, including more fatigue, anorexia, hypertension and proteinuria

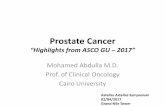
Nephrectomized patients
with advanced RCC
Stratification:
Country
MSKCC risk group
•Primary objective: OS
•Secondary objectives: PFS, TTP, TTF, ORR, and safety
•Median follow-up: 22 months
IFN-2a/Bevacizumab (n=327)
IFN- 9 MIU s.c. 3x/week*
Bevacizumab 10 mg/kg IV q2w
until progression
IFN-/placebo (n=322)
IFN- 9 MIU s.c. 3x/week*
placebo 10 mg/kg IV q2w until
progression(n = 649)
R
A
N
D
O
M
I
Z
E
Phase III AVOREN Trial: Study
design
Escudier et al. J Clin Oncol 2009; 27(suppl):239s
(abstract 5020).
*Dose reduction allowed

Phase III AVOREN Trial : Final OS results
Multiple Cox regression analysis for OS:
− HR 0.78 (0.63-0.96); P = .0219
OS not affected by reduction of IFN dose:
− OS 26 months with reduced-dose IFN and 23.3 months
with standard IFNEscudier et al. J Clin Oncol 2009; 27(suppl):239s
(abstract 5020)).
IFN+placebo
(n=322)
IFN+bev
(n=327)HR
Log rank
P Value
Median OS (months)
Unstratified NR NR 0.91 (0.76-1.10) .3360
Stratified 21.3 23.3 0.86 (0.72-1.04) .1291
Median OS after
censoring patients at
time of crossover
(months)
20.8 23.3 0.84 (0.70-1.02) .0766

Phase III AVOREN trial of interferon alpha plus bevacizumab
or placebo in nephrectomized advanced RCC: Final OS results
Subgroup analysis demonstrated similar benefit regardless of age,
Motzer score, baseline VEGF levels, and number of metastatic sites
However, patients without liver metastases demonstrated significant
OS benefit from the addition of bevacizumab (27.5 vs. 21.4 months,
HR 0.76; P = .0155)
Escudier et al. J Clin Oncol 2009;
27(suppl):239s (abstract 5020)
Post-protocol
therapy
N
IFN+plac vs.
IFN+bev
Median OS (months)
HRIFN+placebo IFN+bev
Subsequent TKI 120 vs. 113 33.6 38.6 0.80 (0.56-1.13)
Subsequent
sunitinib92 vs. 83 39.7 43.6 0.88 (0.58-1.35)
Subsequent
sorafenib50 vs. 60 30.7 38.6 0.73 (0.44-1.20)

Phase III study of pazopanib in treatment-naïve or
cytokine-pretreated advanced RCC
Sternberg et al. J Clin Oncol 2009; 27(suppl):240s
(abstract 5021)
Eligibility:
• Locally advanced or
metastatic RCC
• Clear cell histology
• Treatment naive or
failure of 1 prior
cytokine therapy
Stratification:
ECOG PS
Prior nephrectomy
Rx naive (n=233) vs. 1
cytokine failure (n=202)
•Primary objective: PFS
•Secondary objectives: OS, ORR, duration of response, safety, health-related QOL
Pazopanib 800mg qd
Placebo*
(n = 435)
R
A
N
D
O
M
I
Z
E
2:1
(n = 290)
(n = 145)
*Option to crossover via an
open label study at progression

Phase III study of pazopanib in treatment-naïve or
cytokine-pretreated advanced RCC: Efficacy
48% of patients on placebo arm received pazopanib at disease
progressionSternberg et al. J Clin Oncol 2009; 27(suppl):240s
(abstract 5021).
Patient populationplacebo
(n=145)
pazopanib
(n=290)HR P Value
ORR (%)
Overall population 3 30 NR NR
Treatment-naïve* 4 32 NR NR
Cytokine-pretreated† 3 29 NR NR
Median PFS (months)
Overall population 4.2 9.2 0.46 (0.34-0.62) <.0000001
Treatment-naïve* 2.8 11.1 0.40 (0.27-0.60) <.0000001
Cytokine-pretreated† 4.2 7.4 0.54 (0.35-0.84) <.001
Median OS (months) 18.7 21.1 0.73 (0.47-1.12) .02‡
* n = 78 for placebo and 155 for pazopanib; † n = 67 for placebo and 135 for pazopanib
‡ one-sided P value

Phase III study of pazopanib in treatment-naïve or
cytokine-pretreated advanced RCC: Safety
4% of pts in the pazopanib arm and 3% in the placebo arm
experienced grade 5 adverse events
Sternberg et al. J Clin Oncol 2009;
27(suppl):240s (abstract 5021)
Grade 3/4 Adverse Eventsplacebo
(n=145) (%)
pazopanib
(n=290) (%)
Hypertension <1 4
Diarrhea <1 4
Anorexia <1 2
Vomiting 2 3
Fatigue 2 2
Asthenia 0 3
Hemorrhage 0 2
ALT abnormalities 1 12
AST abnormalities <1 8
ALT = alanine transferase; AST = aspartate aminotransferase

RCC Treatment Algorithm: 2009
Setting Patients Therapy
(level 1)
Other Options
(≥ level 2)
Untreated
Good or
Intermediate risk
Sunitinib
Bevacizumab +
IFN
HD IL-2
Sorafenib
Clinical trial
Observation
Poor risk Temsirolimus Sunitinib
Clinical trial
Cytokine-
refractory
Sorafenib
Pazopanib
Sunitinib
Bevacizumab
VEGF-R
refractory
Everolimus
Clinical trial
Sunitinib
Sorafenib
mTOR-refractory Clinical trial Clinical trial
*Adapted from M Atkins, ASCO 2006 & R Bukowski ASCO 2007

Randomized Trial of p53 Targeted
Adjuvant Therapy for Patients with
Organ- Confined Node-Negative
Urothelial Bladder Cancer
Abstract 5017Walter M. Stadler, Seth P. Lerner, Susan Groshen, John P. Stein†, Ellenie Tuazon, David Quinn, Donald G. Skinner, Derek Raghavan, David Esrig, Gary Steinberg, David Wood, Laurence Klotz, Craig Hall, Richard Cote
†Deceased

Years from Cystectomy
Pro
bab
ilit
y o
f N
ot
Recu
rrin
g
p53 negative( n=142)
p53 positive( n=101)
p< 0.001
Esrig, et al NEJM 1994; 1259-64
p53 Status May be Prognostic

STUDY DESIGN
Radical Cystectomy (P1, P2a, P2b, NO, MO)
Registration - Consent to p53 Analysis and
Randomized Trial
IHC, p53 Altered
(>10% nuclear +)
IHC, p53 Wild type
(≤10% nuclear +)
Consent for
Randomization Re-
Confirmed
Consent for
Randomization Not Re-
Confirmed
MVAC x 3
Arm I
Observ.
Arm II
Observ.
Arm IV
Observ.
Arm III
Abstract 5017

Overall Survival: MVAC vs.
Observation (Arm 2)
0.00
0.10
0.20
0.30
0.40
0.50
0.60
0.70
0.80
0.90
1.00
0 12 24 36 48 60 72 84 96 108 120 132
Months Since Randomization
Estim
ate
d
Pro
bab
ility
o
f
Su
rviv
al
MVAC (n=58)
Observed (n=56)
p=0.75
Abstract 5017

Abstract 5017
Authors Conclusions
Unable to confirm prognostic value of p53
Centrally performed IHC may not be analytically valid
Stage migration led to better than expected outcomes
Preliminary data based on too small of a cohort
p53 mutation and pathway analysis pending
Unable to confirm predictive value of p53
See above
Randomization challenges led to underpowered trial

A Multicenter Study of Cisplatin,
Gemcitabine and bevacizumab As First Line
Therapy for Metastatic Urothelial Cancer:
Hoosier Oncology Group Protocol GU04-75
ABSTRACT 5018
N. M. Hahn, W. M. Stadler, R. T. Zon, D. Waterhouse, J. Picus, S. Nattam, C. S. Johnson, S. M. Perkins, M. J. Waddell, C. J. Sweeney

Study Design
Primary Endpoint
Progression Free Survival (PFS)
Secondary Endpoints
Response Rates
Toxicity
Overall Survival (OS)
Abstract 5018

• Maximum of 8 cycles of Cisplatin and Gemcitabine• Maximum 1 year of Bevacizumab therapy*Gemcitabine reduced to 1000 mg/m2 iv d1,8 after first 17 patients due to 7 DVT/PE events
Eligibility Criteria•Metastatic UC (mUC)•ECOG PS 0-1•Cr < 1.5 mg/dl•No prior CTx for mUC•No anticoagulation•No CNS mets
E
N
R
O
L
L
M
E
N
T
Cisplatin 70 mg/m2 iv d1
Gemcitabine* 1250 mg/m2 iv d1,8
Bevacizumab 15 mg/kg iv d1
Cycle length = 21 days
Abstract 5018
STUDY SCHEMA

Median chemotherapy cycles – 6 (2-8)
30% patients entered Bevacizumab maintenance portion
60% patients required dose modifications
42% discontinued therapy due to toxicity
21% discontinued Bevacizumab due DVT/PE
Therapy Administration
Abstract 5018

Cisplatin/Gemcitabine + Bevacizumab in
Metastatic Urothelial Cancer: Results
Hahn et al. J Clin Oncol 2009; 27(suppl):239s
(abstract 5018)
Adverse events (n = 43):
− 60% of patients required dose adjustments
• 42% discontinued therapy due to toxicity
• 21% discontinued bevacizumab due to DVT/PE
− DVT/PE incidence
• Gemcitabine 1250 mg/m2 (n = 18) – 39%
• Gemcitabine 1000 mg/m2 (n = 25) – 8%
− 3 treatment-related deaths (all at 1000 mg/m2 dose)
• Cerebral hemorrhage, aortic dissection, sudden cardiac
death
Objective response rate: 25 (58%)

Progression Free SurvivalP
ro
bab
ilit
y o
f n
ot
Pro
gressin
g
Months
Median PFS = 8.2 m (95% CI 6.5 – 10.0)
Median follow-up = 14.6 m (Range 2-37)
12-month PFS = 29%
Abstract 5018

Overall Survival
Median OS = 19.1 m (95% CI 11.5 – 23.4)
Median follow-up = 14.6 m (Range 2-37)
12-month OS = 65%
Abstract 5018

Bevacizumab is associated with significant toxicity in metastatic urothelial carcinoma patients
The PFS of 8.2 months did not meet the designed primary endpoint
The OS of 19.1 months is beyond that expected from cisplatin plus gemcitabine alone
Authors Conclusions
Abstract 5018

Proposed Intergroup Phase III Trial

Antitumor Activity of MDV3100 in a
Phase 1-2 Study of Castration-Resistant
Prostate Cancer
Abstract No: 5011
H. I. Scher, T. Beer, C. Higano, M. Taplin, E. Efstathiou, A. Anand,
D. Hung, M. Hirmand, M. Fleisher, C. SawyersProstate Cancer Clinical Trials Consortium

MDV3100
A Second-Generation Antiandrogen
1. Engineered for activity in prostate cancer cells that
overexpress the androgen receptor (AR).
2. Binds the AR more potently than bicalutamide.
3. Unlike bicalutamide, MDV3100 inhibits nuclear
translocation of the AR and its binding to DNA.
4. Induces apoptosis in prostate cancer cells.
Abstract 5011


Ligand
1. AR Binding Affinity• DHT ~ 5nM
• Bicalutamide ~160 nM
• MDV3100 ~35 nM
2. Nuclear Import• DHT: ++++
• Bicalutamide: ++++
• MDV3100: ++
3. DNA Binding• DHT: ++++
• Bicalutamide: ++
• MDV3100: -
4. Coactivator recruitment• DHT: ++++
• Bicalutamide: ++
• MDV3100: -
The Effects of MDV3100 on the
Androgen Receptor Are Distinct from Bicalutamide
1
2
Chen, Clegg and Scher
3
4
DNA
POL
II
HS
P 9
0
LB
D
HD
DBD
NTD

Phase 1-2 Multicenter Trial in CRPC
Determine safety
Determine pharmacokinetics (PK)
Assess antitumor activity:
Exploratory:
Circulating tumor cells
PET: FDG - 18-fluorodeoxyglucose
PET: FDHT - 18-fluorodihydrotestosterone
Abstract 5011

Key Inclusion Criteria
1. Pathologic confirmation of adenocarcinoma of
prostate
2. Serum testosterone level <50 ng/dL
3. Progressive disease defined as one or more of:
3 rising PSA levels; screening PSA >2 ng/mL
RECIST
Two or more new lesions on bone scan
4. No more than 2 prior chemotherapy regimens,
at least one of which contained docetaxel
Abstract 5011

Trial Design
Single
Dose
6 days
Continuous Dosing
Assess Monthly;
Q3 Month Imaging
Long-Term
Dosing
Indefinite
Cohort 1
Single
Dose
6 days
Continuous Dosing
Assess Monthly;
Q3 Month Imaging
Long-Term
Dosing
Indefinite
Cohort 2
After 28
Day Safety
Subsequent Dose Levels
Cohort expansion at > 60 mg/day12 pre- and 12 post-chemotherapyPost-chemotherapy only at > 480 mg/day Abstract 5011

Demographics/Prior Therapy (N=140)
Med. (range)
AGE (years) 68 (44–93)
PSA (ng/mL) 50 (2–2,159)
N (%)
PRIOR HORMONE THERAPY 140 (100%)
1 line 32 (23%)
2 lines 42 (30%)
>3 lines 66 (47%)
CHEMOTHERAPY 75 (54%)
Abstract 5011

MDV3100 Was Generally Well-Tolerated
Adverse Event All Doses
(N = 140)
240 mg/day
(N = 60)
G2 G3 G2 G3
Fatigue
Nausea
Anorexia
Seizure
29 (21%)
11 ( 8%)
4 ( 3%)
12 (9%)
3 (2%)
8 (13%)
2 ( 3%)
3 (5%)
1. Only one subject discontinued treatment due to fatigue which coincided with
disease progression
2. Two witnessed seizures (one each at 600 and 360 mg/day) and a possible
unwitnessed seizure (at 480 mg/day) were reported
Both patients with witnessed seizures were taking concomitant medications
that can cause seizure
3. MTD determined to be 240 mg/day; patients at higher doses were lowered to
240 mg/day
Possibly Related Grade 2/3 Adverse Events in >2 Patients
Abstract 5011

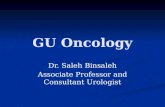
Waterfall Plot of Best Percent PSA Change
from BaselineChemotherapy-Naïve (N=65) Post-Chemotherapy (N=75)
62% (40/65)
>50% Decline
51% (38/75)
>50% Decline

Authors Conclusions
MDV3100 is a second-generation antiandrogen
engineered for activity in cells that overexpress AR,
unique from bicalutamide
The drug active in CRPC both before and following
chemotherapy as demonstrated by declines in PSA,
imaging, CTC conversion rates, and PET
MDV3100 is generally well-tolerated
Phase III trial will open this year
Abstract 5011

Southwest Oncology Group S9921:
Prolonged Event Free Survival in High
Risk Prostate Cancer (PC) Patients
Receiving Adjuvant Androgen Deprivation
Abstract 5009
L. Michael Glode, Cathy M. Tangen, Maha H.A. Hussain, David P. Wood, Jr. , Gregory P. Swanson, David I. Quinn, Nancy Dawson, Naomi Balzer-Haas, E. David Crawford, Benjamin Ely, Ian M. Thompson

Background
Study conceived 1997-98
Mitoxantrone approved 1996 by FDA for
palliative treatment of HRPC
Canadian Palliation trial (JCO 14:1756)
CALGB 9182 (JCO 17:2506)
Improved QOL compared to hydrocortisone alone
Improved time to treatment failure
No difference in survival
Abstract 5009

SWOG 9921
Intergroup Participants: CALGB, ECOG
Eligibility
Prostatectomy ≤ 120 days prior to registration and one or
more of the following:
Path Gleason sum > 8
pT3b (seminal vesicle) or pT4 or N1
Path Gleason’s sum 7 and positive margin
Preop PSA >15ng/ml, or biopsy Gleason >7, or PSA
>10ng/ml with biopsy Gleason > 6
Abstract 5009

PSA>20,T3b, T4 or N1 or
Gleason > 8,or T3a, + margin,
and Gleason 7
RA
ND
OM
IZE
CAB X 24 months
Mitoxantrone 12 mg/m2 d1+ Prednisone 5 mg BID d1-21
Q 3 Weeks X 6 andCAB x 24 months
983496
487
Trial Design
Abstract 5009

Causes of Death (17 total)
Prostate Cancer – 7
Other Cancers – 4
Cardiovascular Disease – 1
Other Causes – 5
Abstract 5009

Testosterone (T) Recovery (> 50ng/ml)
• Per protocol, T measured every 6 month intervals until > ILLN.
• Patients included in analysis: ≥1 T measurement within the first 12
months after completing CAB
Median
T Recovery
Time*
(95% CI)
6 Month*
Overall
T Recovery
(95% CI)
12 Month*
Overall
T Recovery
(95% CI)
18 Month*
Overall
T Recovery
(95% CI)
9.5 Months
(8.7, 10.5)
27.8%
(5.6, 71.4)
75.3%
(50.8, 90.0)
89.5%
(69.8,96.9)
* Recovery time measured from completion of CAB
Abstract 5009

Authors Conclusions
S9921 shows better than predicted DF-survival in high risk prostate cancer patients who received 2 years of CAB Potential causes: stage migration, patient selection,
lead time bias, effects of CAB itself. Comparable survival data are seen in selected
contemporary studies
75% of patients have testosterone recovery to above castrate level within one year of stopping CAB
Much longer follow-up of S9921 will be required to observe any differences in survival due to mitoxantrone
Abstract 5009

Phase II Trials of Abiraterone Acetate in Castration
Resistant Prostate Cancer
1Ryan et al. J Clin Oncol 2009; 27(suppl):245s (abstract
5046)2Reid et al. J Clin Oncol 2009; 27(suppl):246s (abstract 5047)
3Danila et al. J Clin Oncol 2009; 27(suppl):246s (abstract
5048)
Patient population NPSA decline ≥
50%
Tumor
response
(RECIST)
ECOG PS
Improvement
(at least one level)
CRPC: Chemotherapy
naïve1 33 24 (73%)PR: 9 (27%)
SD: 19 (58%)8 (61.5%)
CRPC: Prior docetaxel247 24 (51%)
PR: 6 (13%)
SD: 25 (53%)11 (35%)
CRPC: Prior docetaxel3
No prior ketoconazole
Prior ketoconazole
31
27
16 (52%)
8 (30%)
(n = 18)
PR: 3 (17%)
SD: 11 (61%)
16 (48%)

Phase II Trials of Abiraterone Acetate in Castration Resistant
Prostate Cancer: Grade 3/4 Adverse Events
1Ryan et al. J Clin Oncol 2009; 27(suppl):245s (abstract 5046)2Reid et al. J Clin Oncol 2009; 27(suppl):246s (abstract 5047)
3Danila et al. J Clin Oncol 2009; 27(suppl):246s (abstract 5048)
Ryan (n = 33) Reid (n = 47)* Danila (n = 58)*
Hematological
Lymphopenia NR 2 (4%) 5 (9%)
Anemia NR 3 (6%) NR
Nonhematologic
Peripheral edema 1 (3%) 0 NR
Fatigue 0 4 (8.5%) NR
Nausea NR 3 (6%) NR
Vomiting NR 3 (6%) NR
•Common toxicities (all grades) in at least two trials: peripheral
edema, fatigue, hypokalemia, arthralgia
*Experienced by ≥ 2 patients

Fleisher H, et al. abstract 5049
Circulating tumor cells (CTC) in patients with metastatic castration-
resistant prostate cancer (CRPC) receiving abiraterone acetate (AA) after
failure of docetaxel –based chemotherapy
Preliminary findings suggest correlation with
CTC decline and PSA decline
Prospectively built into phase III abiraterone
program

IMPACT Overall Survival: Primary Endpoint
Intent-to-Treat Population
0 6 12 18 24 30 36 42 48 54 60 660
25
50
75
100
Perc
ent
Surv
ival
Survival (Months)
P = 0.032 (Cox model)
HR = 0.775 [95% CI: 0.614, 0.979]
Median Survival Benefit = 4.1 Mos.
Sipuleucel-T (n = 341)
Median Survival: 25.8 Mos.
Placebo (n = 171)
Median Survival: 21.7 Mos.
PF Schellhammer, et al. LBA 9 AUA 2009

LocallyAdvancedDisease
Rising PSAHormone
Naive
Rising PSACastrate
MetastasesCastrate
Asymptomatic
MetastasesCastrate
Symptomatic
OrganConfined
Metastatic Disease
(De novo)
Clinical States In Prostate Cancer
MetastasesCastrate
SymptomaticPost Docetaxel
Modified from Scher H, et al.

Conclusions: Renal Cancer
Lots of active agents, need to sort out optimal
sequence taking into account efficacy, cost,
toxicity
New generations of TKI’s may be equally
effective but perhaps less toxic- cant
emphasize how important that may be
Combination therapy is going to be difficult,
toxicity remains significant impediment to
further development

Conclusions: Urothelial Cancer
Progress remains painfully slow
Gemcitabine/cisplatin/bevacizumab of
interest, but toxicity remains SIGNIFICANT
CONCERN
Phase III will have real time toxicity
monitoring by CALGB

Conclusions: Prostate Cancer
Near term future for advanced prostate
cancer therapeutics, is much brighter—BUT
WILL BE VERY EXPENSIVE
Androgen receptor targeting therapy IS
HERE- STOP USING TERM HORMONE
REFRACTORY/ANDROGEN
INDEPENDENT
CASTRATE RESISTANT