
Arthroscopic Shoulder Procedures - AHN space lidocaine with epi injection Systolic blood pressure...
32
Arthroscopic Shoulder Procedures David C. Neuschwander MD Allegheny Health Network Orthopedic Associates of Pittsburgh Shoulder Instability Anterior Instability Posterior Instability
Transcript of Arthroscopic Shoulder Procedures - AHN space lidocaine with epi injection Systolic blood pressure...
Arthroscopic Shoulder
Procedures
David C. Neuschwander MD
Allegheny Health Network
Orthopedic Associates of
Pittsburgh
Shoulder Instability
Anterior Instability
Posterior Instability

Glenohumeral Joint Stability
Dependent upon the bony geometry and soft
tissues about the shoulder
Success rates of Open Anterior stabilization
procedures 90-95%
Despite low recurrence rates with open
procedures, there can be important losses
in external rotation, surgical morbidity and
difficult rehab


Shoulder Arthroscopy
Has a learning curve which is specific to
each procedure
Needs to duplicate the techniques which
have been done with an open technique
Measures to Limit Bleeding
Subacromial space lidocaine with epi
injection
Systolic blood pressure about 100 if
tolerated medically
Use of arthroscopic pump
Epi in fluid
Initial Evaluation
Scalene block or General Anesthesia
Assess range of motion and stability testing
Portal placement (Poster, Anterior) for evaluation of GH joint
Subacromial space portal placement (posterior, anterior, and lateral)
Use of accessory portals and anchor portals as necessary

Anterior Instability
Preop
Clinical
Exam
Assess Tissue Quality
Determine if the
tissue has moved
medially along the
glenoid neck
Determine how far the
tissue can be moved
to get desired effect
on the tension of the
repair
Anchor Placement
Along the glenoid
face-neck junction
Placed 5-7 mm apart
Recreate the “bumper
effect”

Anterior Instability
Postop
Exam
Anterior Instability
Initial Shoulder
Arthroscopic
Evaluation
Anterior Instability
Anterior Superior
Lateral Portal

Anterior Instability
Anchor Hole
Placement
Anterior Instability
Knot Tying
Anterior Instability
Final Evaluation

Anterior Instability
Another Case
Anterior Soft
Tissue
Bankart
Lesion
Anterior Instability
Anterior
Capsule
T Split
Anterior Instability
Preop
Arthroscopic
Exam

Anterior Instability
Initial
Probe
Eval
Anterior Instability
Elevate
Anterior
Labrum
Anterior Instability
Place
Anchor

Anterior Instability
Tie
Knot
Anterior Instability
Replace
Blue
Suture
Anterior Instability
Knot
Tying

Anterior Instability
Test
Stability
Anterior Instability
Evaluate
Final
Repair
Another Case

Retracted Anterior Labrum
Elevate Anterior Labrum
Shoulder Instability and
Rotator Cuff Repairs
March 29, 2014
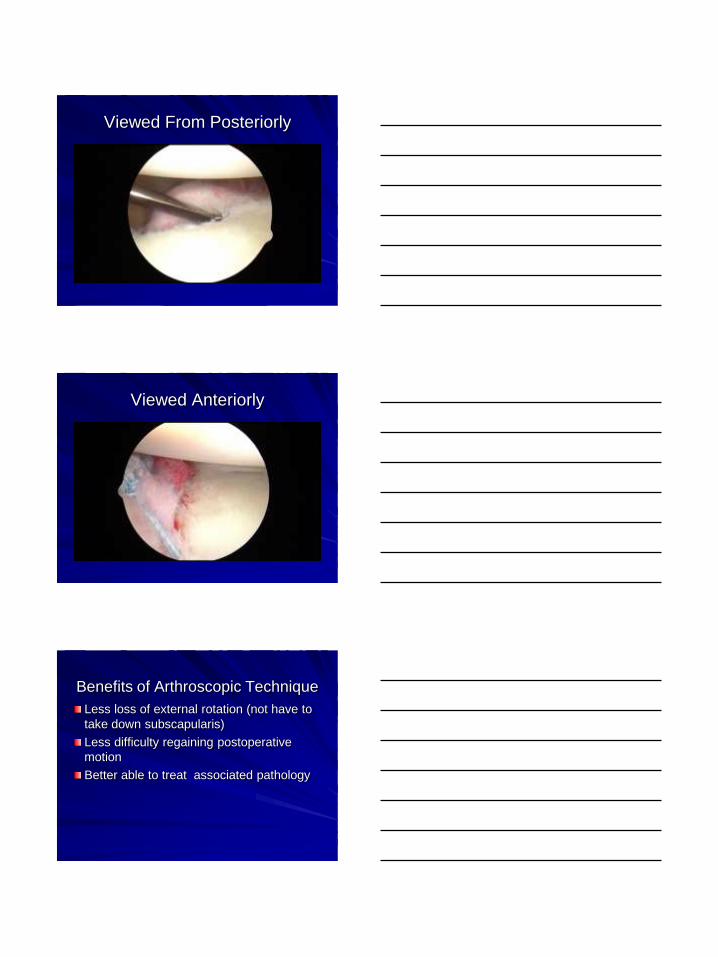
Viewed From Posteriorly
Viewed Anteriorly
Benefits of Arthroscopic Technique
Less loss of external rotation (not have to
take down subscapularis)
Less difficulty regaining postoperative
motion
Better able to treat associated pathology

Refined Arthroscopic Technique
Anchors placed on the anterior glenoid
face-neck junction to recreate labral
“bumper” that deepens glenoid concavity
Plication sutures
Rotator Interval closure
Analysis of Athroscopic Instability
Failures
Too short a period of immobilization (< 3
weeks)
Use of too few anchors
Anterior placement of anchors on glenoid
neck rather than edge of the articular
surface
Participation in contact sports
Young Age
Analysis of Arthroscopic Failures
Glenohumeral Ligament Quality
Generalized ligamentous laxity
Engaging Hill-Sachs lesion
Bony Bankart (inverted pear shaped
glenoid)
Capsular attenuation

Posterior Shoulder Instability
2-10% of all instability cases
50% due to trauma
Athletes usually have subluxation rather
than dislocation
Most common in overhead throwers,
tennis players, butterfly and freestyle
swimmers, weightlifters, and football
lineman
History
Symptoms with forward flexion, adduction,
and internal rotation
Throwers (follow-through)
Swimmers (pull-through)
Location of pain variable
Often describe crepitation or click
Posterior Instability
Improvements in diagnosis and treatment
of athletes and other individuals has
shown posterior instability to be more
common than once thought

Posterior Instability
Symptoms
Pain, weakness and loss of function with
the arm in a forwardly flexed position
Many patients improve with conservative
treatment
Physical Exam
Posterior Joint Line Tenderness
Load and shift test (sitting and supine)
Posterior Instability

Posterior Instability
Loose Body

Posterior Instability
Viewed From Anterior
Portal
Viewed From Posterior
Portal
Viewed Posteriorly Viewed Anteriorly

Knot Tying
Anchor Placement Evaluate Knot Security
Suture Anchor for Anterior
Labral Tear
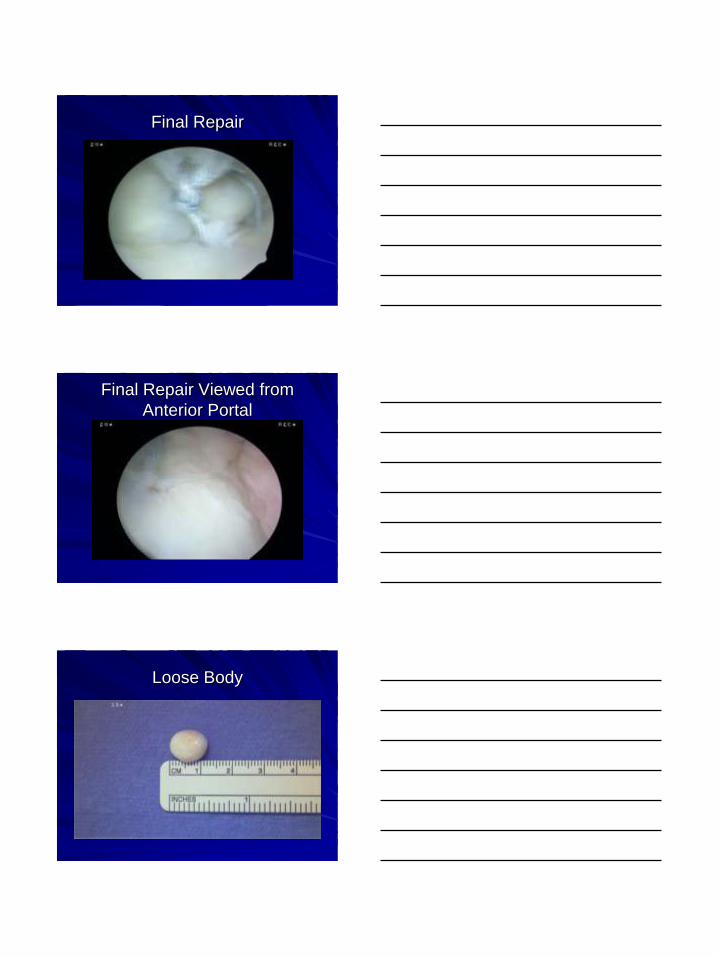
Final Repair
Final Repair Viewed from
Anterior Portal
Loose Body
Rotator Cuff
Rotator Cuff
Tendinitis
Partial Thickness Tears
Full Thickness Tears
Rotator Cuff Tendons
Supraspinatus
Infraspinatus
Teres Minor
Subscapularis
Operative Procedure
Visualization
Preparation
Execution
Visualization
Glenohumeral Evaluation
Humeral Head and Glenoid
Labrum
Biceps Tendon
Rotator Cuff ( all 4 Tendons)
Subacromial Space Evaluation
Bursal Side of Rotator Cuff
Preparation
Remove Thickened Bursal Tissue
Remove Thickened CA Ligament
Remove Acromial Spur
Evaluate Rotator Cuff Tear
Size
Tendons Involved
Configuration of Tear

Execution
Undertake Rotator Cuff Repair
Side to Side Rotator Cuff Repair

Second Suture
Reevaluate Tear
Single Row Repair

Single Row Repair
Single Row Repair
Single Row Repair
Single Row Evaluation
Double Row Repair
Evaluate Tear

Medial Row Anchor

Footprint Cuff Insertion
Thank You

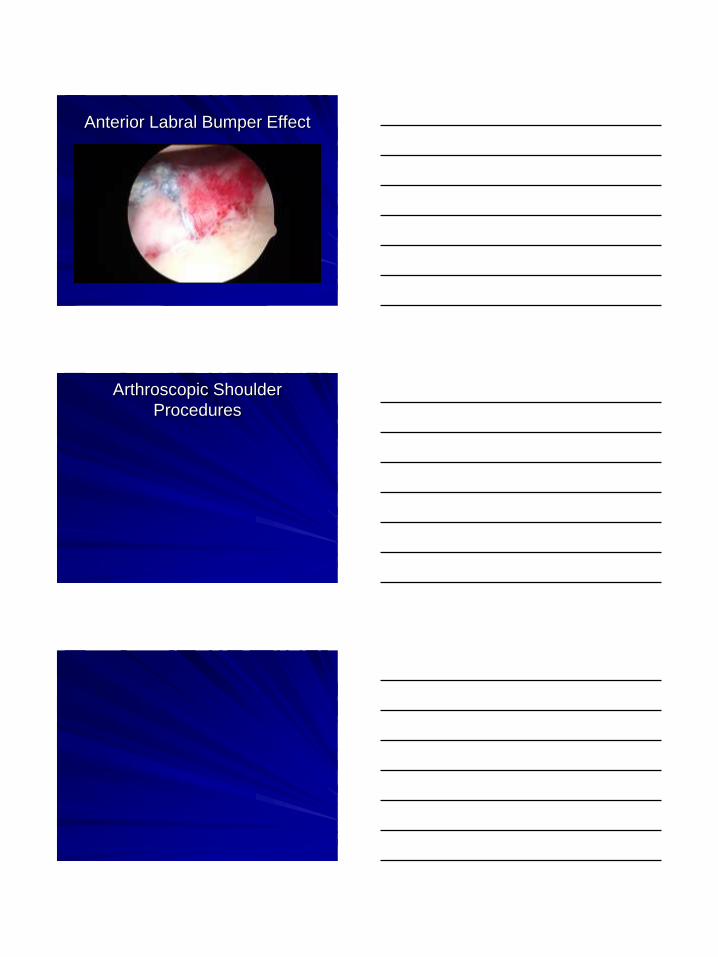
Anterior Labral Bumper Effect
Arthroscopic Shoulder
Procedures


















