
Arterial Tortuosity and Cardiovascular Outcomes in ...€¦ · Arterial Tortuosity and...
28
2/25/2017 1 Arterial Tortuosity and Cardiovascular Outcomes in Thoracic Aortic Disease Disease Shaine A Morris MD MPH Pediatric Cardiology Texas Children’s Hospital Baylor College of Medicine Background • Patients with genetically- mediated aortic disease like Marfan syndrome (MFS) and Marfan syndrome (MFS) and Loeys-Dietz syndrome (LDS) are at high risk of adverse cardiovascular outcomes • Valve dysfunction xxx00.#####.ppt 2/25/2017 9:26:33 PM • Aortic aneurysm • Aortic dissection
Transcript of Arterial Tortuosity and Cardiovascular Outcomes in ...€¦ · Arterial Tortuosity and...

2 / 2 5 / 2 0 1 7
1
Arterial Tortuosity andCardiovascular Outcomesin Thoracic AorticDiseaseDisease
Shaine A Morris MD MPH
Pediatric Cardiology
Texas Children’s Hospital
Baylor College of Medicine
Background
• Patients with genetically-mediated aortic disease likeMarfan syndrome (MFS) andMarfan syndrome (MFS) andLoeys-Dietz syndrome (LDS)are at high risk of adversecardiovascular outcomes
• Valve dysfunction
xxx00.#####.ppt 2/25/2017 9:26:33 PM
• Aortic aneurysm
• Aortic dissection
2 / 2 5 / 2 0 1 7
2
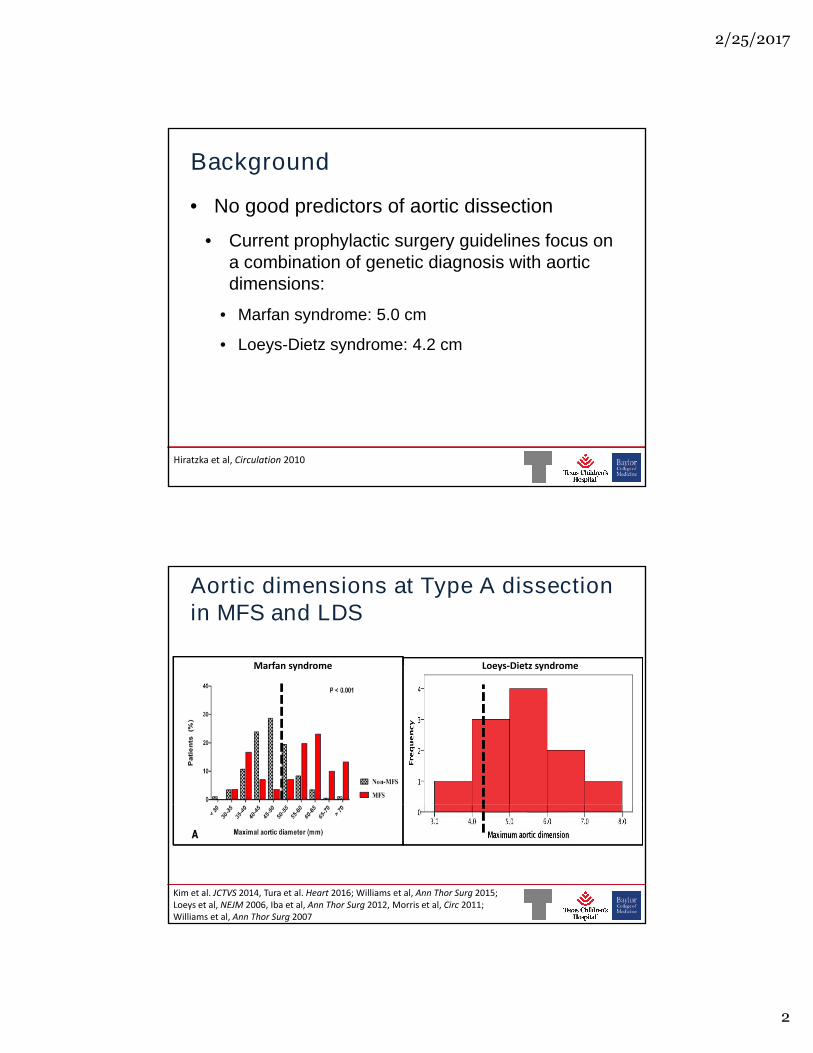
Background
• No good predictors of aortic dissection
• Current prophylactic surgery guidelines focus on• Current prophylactic surgery guidelines focus ona combination of genetic diagnosis with aorticdimensions:
• Marfan syndrome: 5.0 cm
• Loeys-Dietz syndrome: 4.2 cm
xxx00.#####.ppt 2/25/2017 9:26:33 PM
Hiratzkaetal,Circulation2010
M arfansyndrom e
Aortic dimensions at Type A dissectionin MFS and LDS
L oeys-Dietzsyndrom e
xxx00.#####.ppt 2/25/2017 9:26:33 PM
Kim etal.JCT VS 2014,T uraetal.Heart2016;W illiam setal,AnnT horS urg2015;L oeysetal,N EJM 2006,Ibaetal,AnnT horS urg2012,M orrisetal,Circ2011;W illiam setal,AnnT horS urg2007

2 / 2 5 / 2 0 1 7
3
Arterial tortuosity
• Arterial tortuosity is a common featurewith TGFBR1/2 mutations1
• Arterial tortuosity has since been
T GFBR 2
• Arterial tortuosity has since beendescribed with many other genemutations associated with dissection:
• FBN1 2
• SMAD3 3
• TGFB2 4
FBN 1X O
xxx00.#####.ppt 2/25/2017 9:26:33 PM
• TGFB2
• PRKG1 5
and
• Turner syndrome 6
1. Loeys BL, et al. N Engl J Med 20062. Morris et al. Circulation 20113. Vad de Laar et al. Nature Genetics 2011
4. Lindsay et al. Nat Genetics 20125. Guo et al. Am J Hum Genetics 20136. Morris et al. J Cardiovasc Magn Reson 2014
xxx00.#####.ppt 2/25/2017 9:26:33 PM
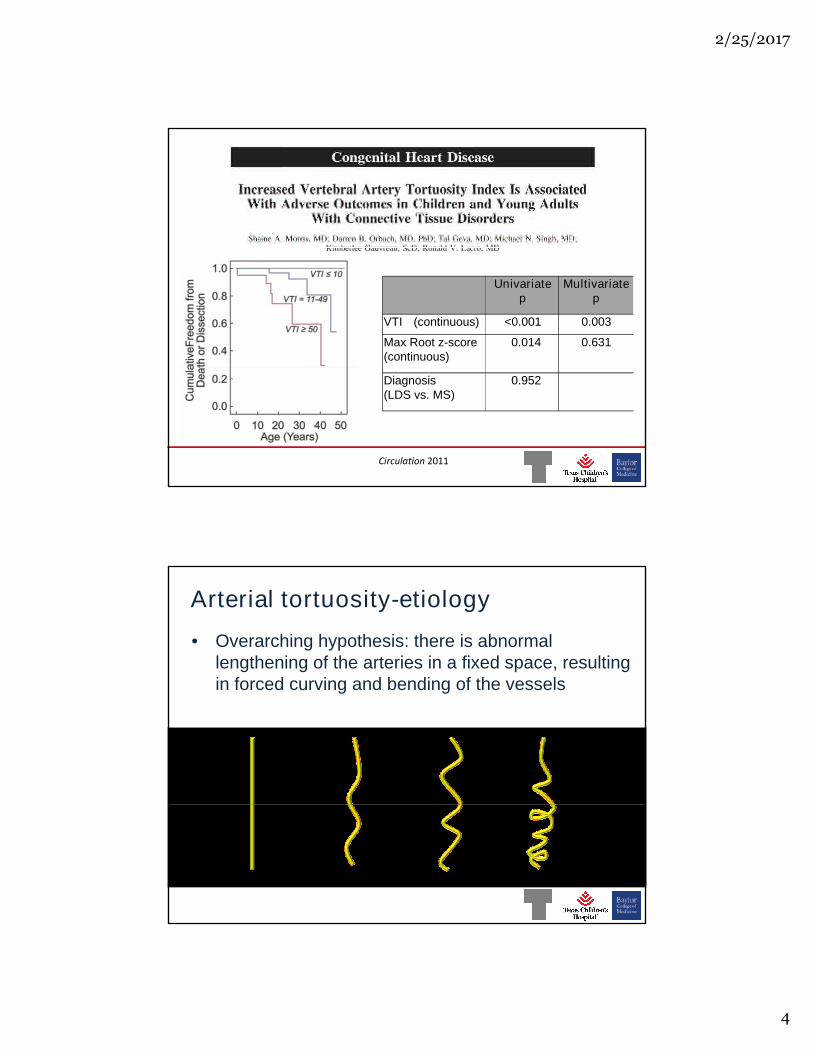
Circulation2011
2 / 2 5 / 2 0 1 7
4
Univariatep
Multivariatep
VTI (continuous) <0.001 0.003
Max Root z-score(continuous)
0.014 0.631
xxx00.#####.ppt 2/25/2017 9:26:33 PM
Circulation2011
Diagnosis(LDS vs. MS)
0.952
Arterial tortuosity-etiology
• Overarching hypothesis: there is abnormallengthening of the arteries in a fixed space, resultingin forced curving and bending of the vesselsin forced curving and bending of the vessels
xxx00.#####.ppt 2/25/2017 9:26:33 PM
2 / 2 5 / 2 0 1 7
5
Arterial tortuosity- theories
• Vessel has maladaptation to axial stress,lengthens as an intrinsic effort to reduce stressalong the vessel1.along the vessel1.
• Increased TGFb activity has also been postulatedto affect the degree of arterial tortuosity3
xxx00.#####.ppt 2/25/2017 9:26:33 PM
1.Hum phrey Jetal.JBiom ech20092.Jacksonetal.ArteriosclerT hrom bVascBiol2005
3.Frankenetal.IntJCard2015
New Study
Study populations: Marfan, TGFBR1, TGFBR2
• National Registry of Genetically Triggered ThoracicAortic Aneurysms and Cardiovascular ConditionsAortic Aneurysms and Cardiovascular Conditions(GenTAC)
• Texas Children’s Hospital patients, followedbetween 1980 and May 30, 2016
xxx00.#####.ppt 2/25/2017 9:26:33 PM

2 / 2 5 / 2 0 1 7
6
Methods• Predictor variable: VTI
xxx00.#####.ppt 2/25/2017 9:26:33 PM
• Primary outcomes• Stanford type A aortic dissection• Stanford type B aortic dissection
Results: Study population
153
51
153
xxx00.#####.ppt 2/25/2017 9:26:33 PM
2 / 2 5 / 2 0 1 7
7
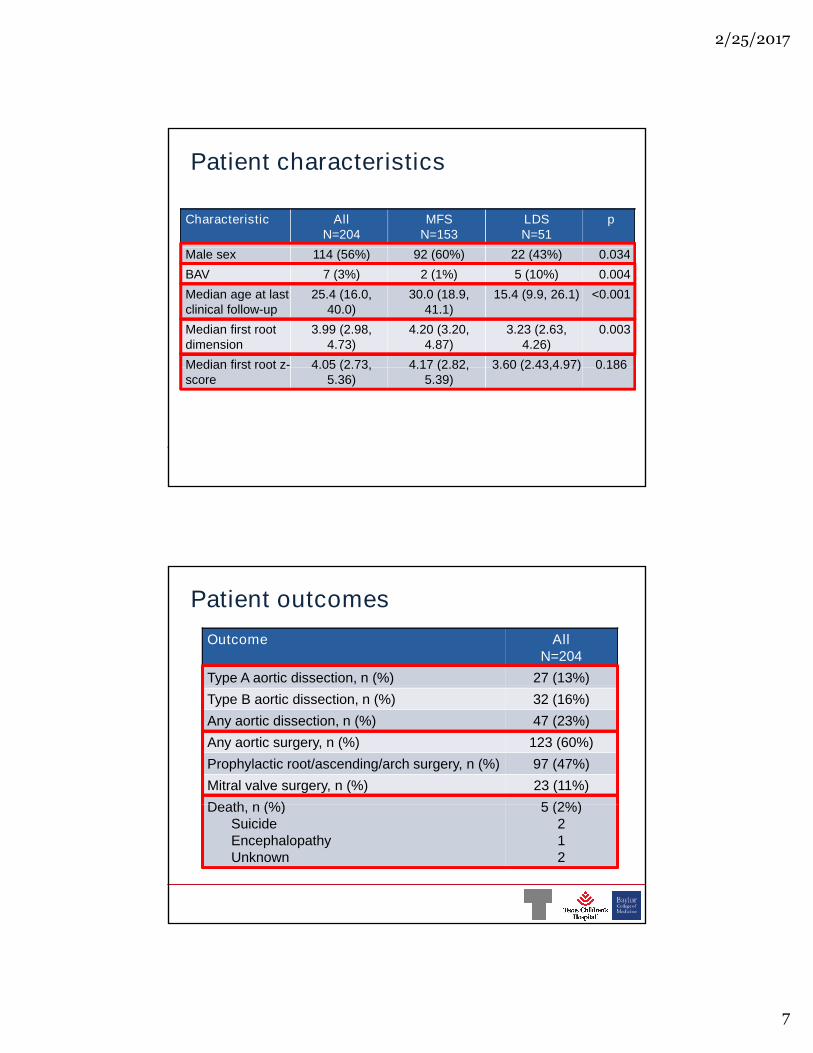
Patient characteristics
Characteristic AllN=204
MFSN=153
LDSN=51
p
Male sex 114 (56%) 92 (60%) 22 (43%) 0.034Male sex 114 (56%) 92 (60%) 22 (43%) 0.034
BAV 7 (3%) 2 (1%) 5 (10%) 0.004
Median age at lastclinical follow-up
25.4 (16.0,40.0)
30.0 (18.9,41.1)
15.4 (9.9, 26.1) <0.001
Median first rootdimension
3.99 (2.98,4.73)
4.20 (3.20,4.87)
3.23 (2.63,4.26)
0.003
Median first root z- 4.05 (2.73, 4.17 (2.82, 3.60 (2.43,4.97) 0.186
xxx00.#####.ppt 2/25/2017 9:26:33 PM
Median first root z-score
4.05 (2.73,5.36)
4.17 (2.82,5.39)
3.60 (2.43,4.97) 0.186
Patient outcomes
Outcome AllN=204
Type A aortic dissection, n (%) 27 (13%)Type A aortic dissection, n (%) 27 (13%)
Type B aortic dissection, n (%) 32 (16%)
Any aortic dissection, n (%) 47 (23%)
Any aortic surgery, n (%) 123 (60%)
Prophylactic root/ascending/arch surgery, n (%) 97 (47%)
Mitral valve surgery, n (%) 23 (11%)
Death, n (%) 5 (2%)
xxx00.#####.ppt 2/25/2017 9:26:33 PM
Death, n (%)SuicideEncephalopathyUnknown
5 (2%)212

2 / 2 5 / 2 0 1 7
8
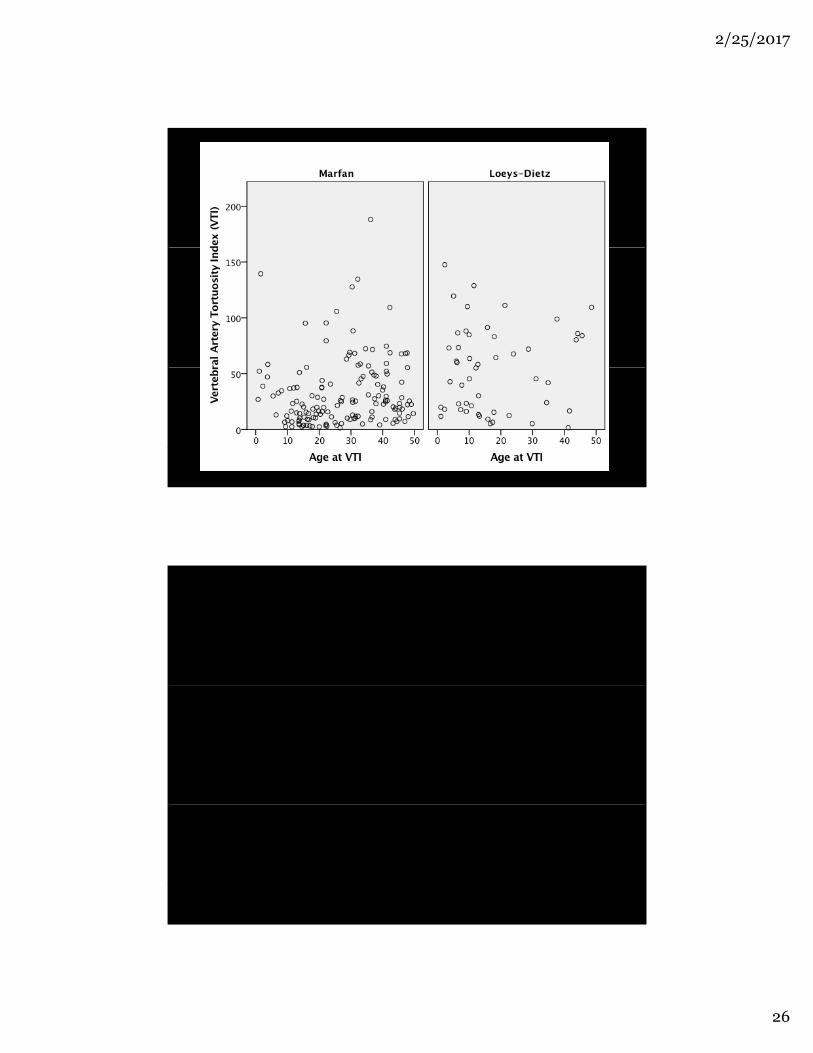
VTI by gene mutation
xxx00.#####.ppt 2/25/2017 9:26:33 PM
Freedom from Type A dissection
P =0.304
DiagnosisM arfanL oeys-Dietz
xxx00.#####.ppt 2/25/2017 9:26:33 PM
2 / 2 5 / 2 0 1 7
9
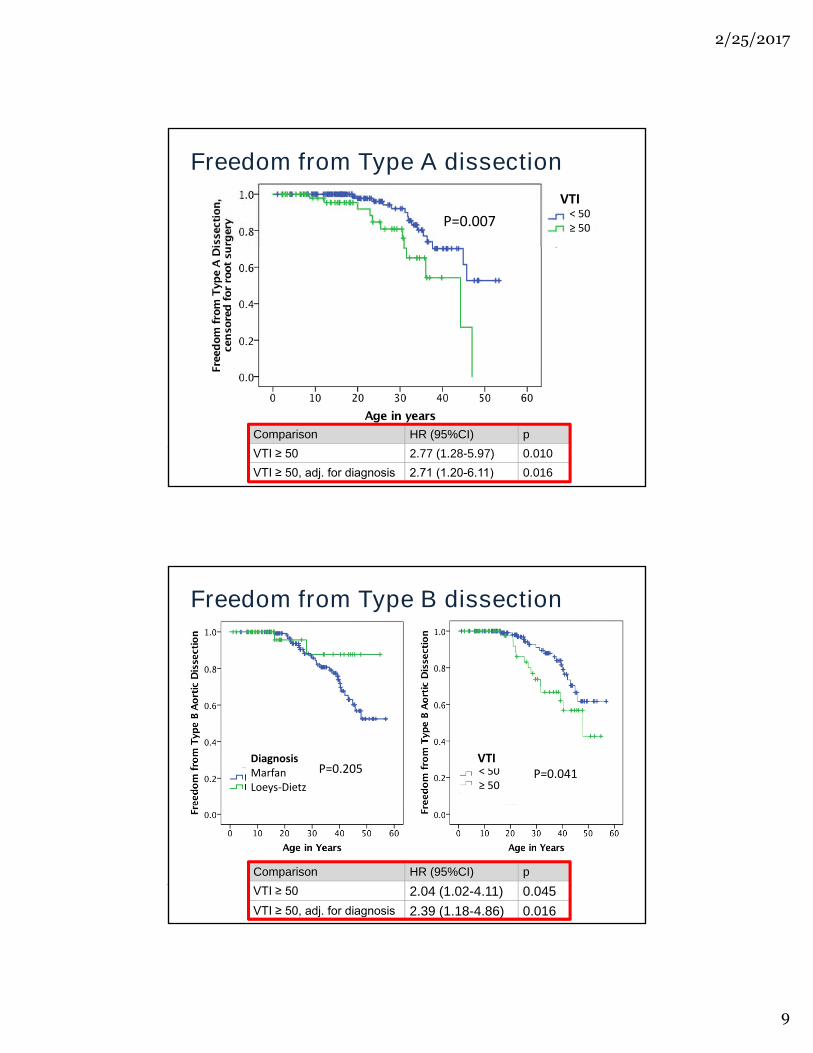
Freedom from Type A dissection
P =0.007< 50≥ 50
VT I
xxx00.#####.ppt 2/25/2017 9:26:33 PM
Comparison HR (95%CI) p
VTI ≥ 50 2.77 (1.28-5.97) 0.010
VTI ≥ 50, adj. for diagnosis 2.71 (1.20-6.11) 0.016
Freedom from Type B dissection
P =0.205DiagnosisM arfanL oeys-Dietz
< 50≥ 50
VT IP =0.041
xxx00.#####.ppt 2/25/2017 9:26:33 PM
Comparison HR (95%CI) p
VTI ≥ 50 2.04 (1.02-4.11) 0.045
VTI ≥ 50, adj. for diagnosis 2.39 (1.18-4.86) 0.016
2 / 2 5 / 2 0 1 7
1 0
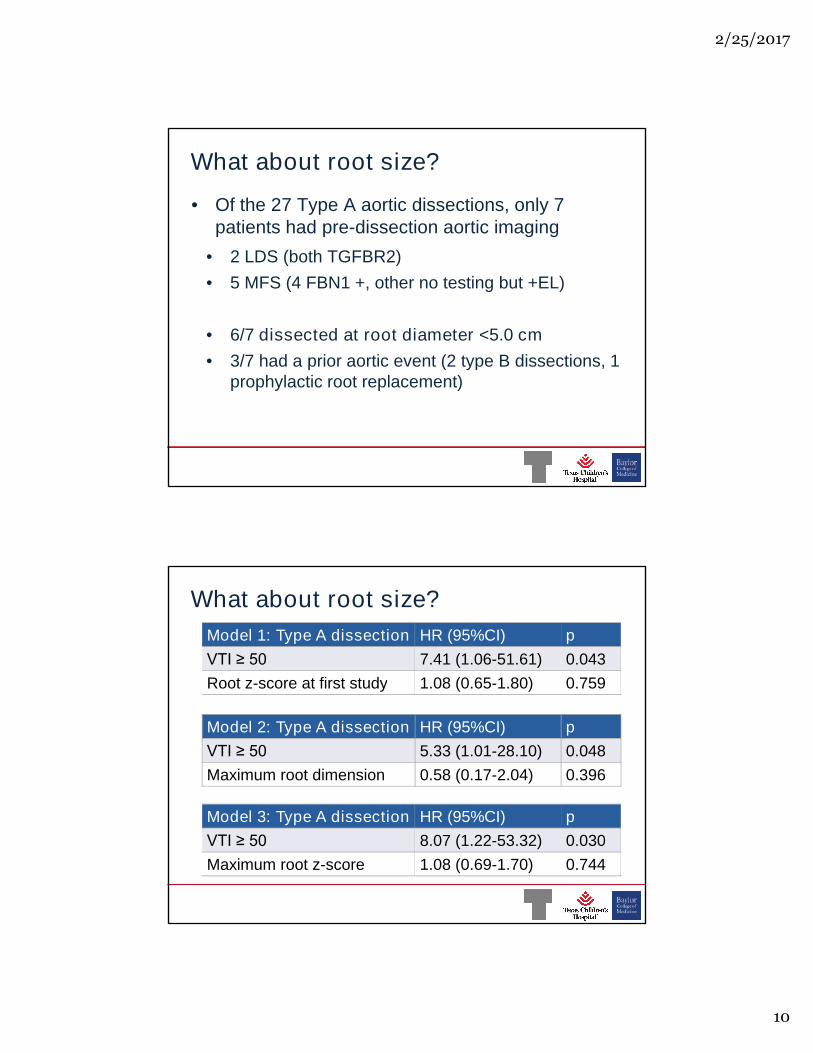
What about root size?
• Of the 27 Type A aortic dissections, only 7patients had pre-dissection aortic imaging
• 2 LDS (both TGFBR2)• 2 LDS (both TGFBR2)
• 5 MFS (4 FBN1 +, other no testing but +EL)
• 6/7 dissected at root diameter <5.0 cm
• 3/7 had a prior aortic event (2 type B dissections, 1
xxx00.#####.ppt 2/25/2017 9:26:33 PM
• 3/7 had a prior aortic event (2 type B dissections, 1prophylactic root replacement)
What about root size?
Model 1: Type A dissection HR (95%CI) p
VTI ≥ 50 7.41 (1.06-51.61) 0.043
Root z-score at first study 1.08 (0.65-1.80) 0.759Root z-score at first study 1.08 (0.65-1.80) 0.759
Model 2: Type A dissection HR (95%CI) p
VTI ≥ 50 5.33 (1.01-28.10) 0.048
Maximum root dimension 0.58 (0.17-2.04) 0.396
xxx00.#####.ppt 2/25/2017 9:26:33 PM
Model 3: Type A dissection HR (95%CI) p
VTI ≥ 50 8.07 (1.22-53.32) 0.030
Maximum root z-score 1.08 (0.69-1.70) 0.744
2 / 2 5 / 2 0 1 7
1 1
Summary
• Arterial tortuosity, as assessed by VTI is present inmany conditions associated with aortic dissection
• A VTI ≥ 50 is independently associated with earlier adverse cardiovascular outcomes, and has greaterprognostic value than genetic diagnosis
• VTI should be taken into account when counselingand managing patients with MFS and LDS
xxx00.#####.ppt 2/25/2017 9:26:33 PM
and managing patients with MFS and LDS
Thank you!
Fundingby N HL BIR 21HL 121630,K23HL 127266,HHS N 268200648199C and
HHS N 26821000048CHHS N 26821000048C
xxx00.#####.ppt 2/25/2017 9:26:33 PM
2 / 2 5 / 2 0 1 7
1 2
xxx00.#####.ppt 2/25/2017 9:26:33 PM
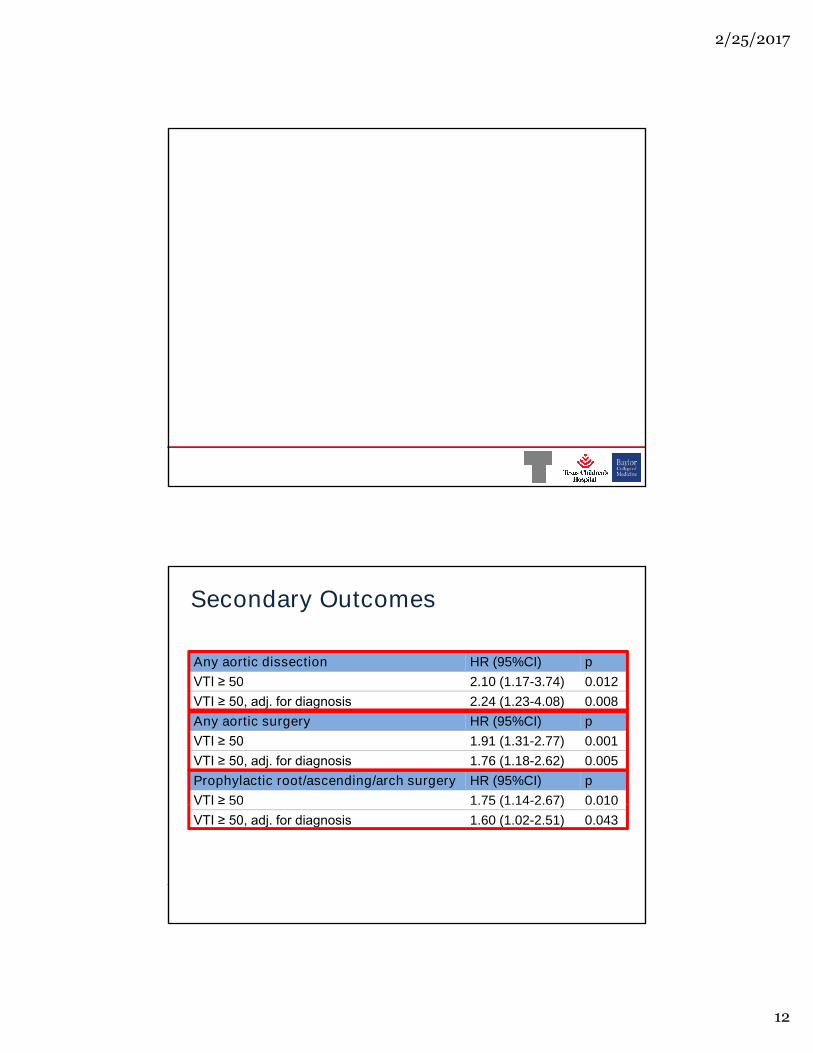
Secondary Outcomes
Any aortic dissection HR (95%CI) p
VTI ≥ 50 2.10 (1.17-3.74) 0.012VTI ≥ 50 2.10 (1.17-3.74) 0.012
VTI ≥ 50, adj. for diagnosis 2.24 (1.23-4.08) 0.008
Any aortic surgery HR (95%CI) p
VTI ≥ 50 1.91 (1.31-2.77) 0.001
VTI ≥ 50, adj. for diagnosis 1.76 (1.18-2.62) 0.005
Prophylactic root/ascending/arch surgery HR (95%CI) p
VTI ≥ 50 1.75 (1.14-2.67) 0.010
xxx00.#####.ppt 2/25/2017 9:26:33 PM
VTI ≥ 50 1.75 (1.14-2.67) 0.010
VTI ≥ 50, adj. for diagnosis 1.60 (1.02-2.51) 0.043
2 / 2 5 / 2 0 1 7
1 3
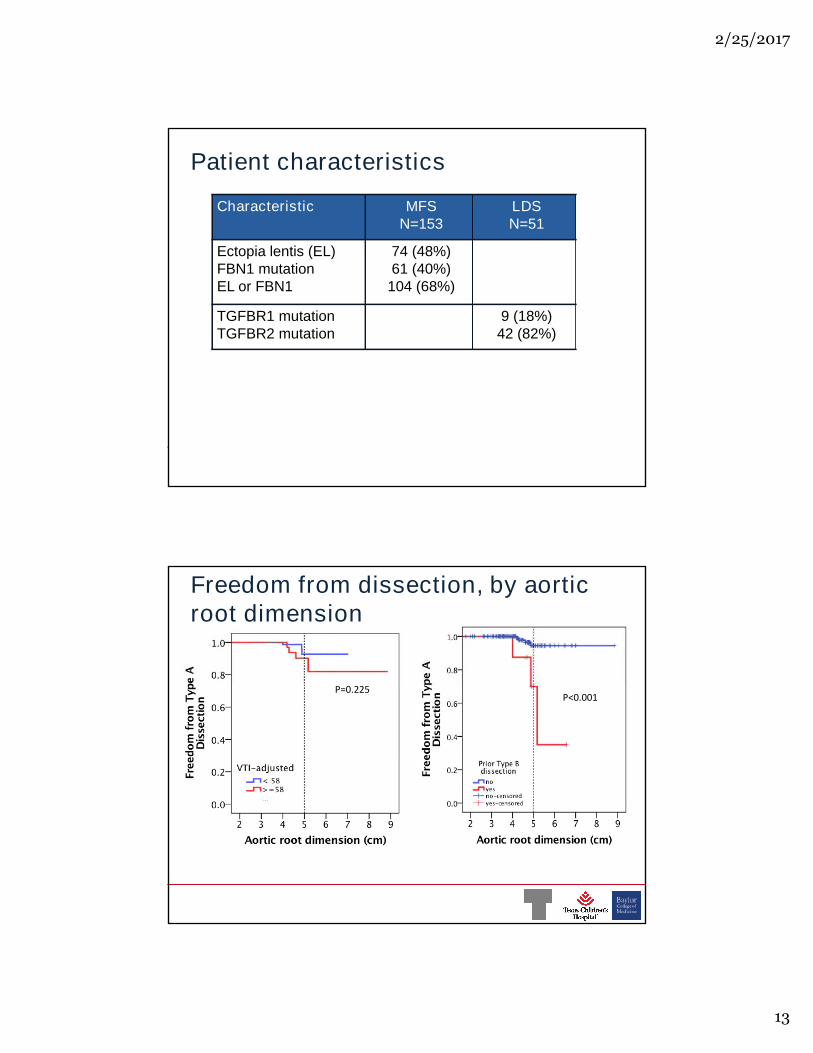
Patient characteristics
Characteristic MFSN=153
LDSN=51
Ectopia lentis (EL) 74 (48%)Ectopia lentis (EL)FBN1 mutationEL or FBN1
74 (48%)61 (40%)
104 (68%)
TGFBR1 mutationTGFBR2 mutation
9 (18%)42 (82%)
xxx00.#####.ppt 2/25/2017 9:26:33 PM
Freedom from dissection, by aorticroot dimension
P =0.225P =0.225P <0.001
xxx00.#####.ppt 2/25/2017 9:26:33 PM
2 / 2 5 / 2 0 1 7
1 4
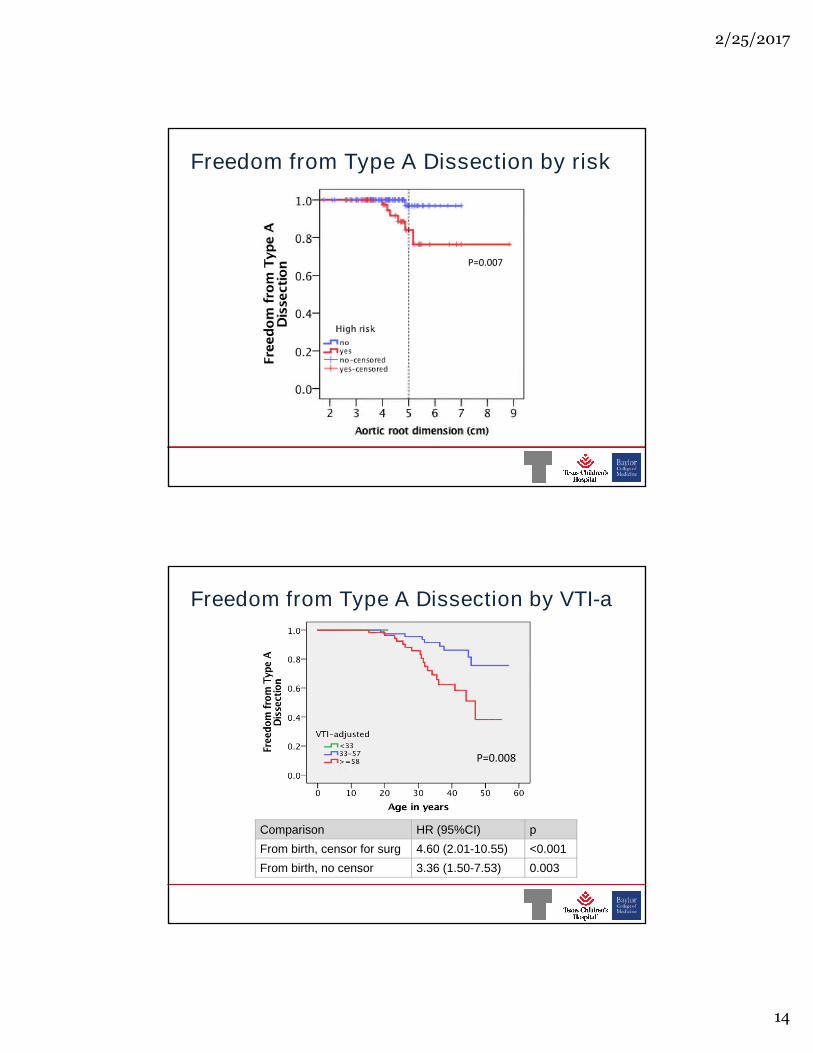
Freedom from Type A Dissection by risk
P =0.007
xxx00.#####.ppt 2/25/2017 9:26:33 PM
Freedom from Type A Dissection by VTI-a
P =0.008
xxx00.#####.ppt 2/25/2017 9:26:33 PM
Comparison HR (95%CI) p
From birth, censor for surg 4.60 (2.01-10.55) <0.001
From birth, no censor 3.36 (1.50-7.53) 0.003

2 / 2 5 / 2 0 1 7
1 5
Freedom from Type A Dissection by VTI-a
xxx00.#####.ppt 2/25/2017 9:26:33 PM
Comparison MFS HR (95%CI) MFS p LDS HR (95%CI) LDS p
From birth, censor for surg 4.71 (1.90-11.66) 0.001 2.10 (0.21-20.63) 0.524
From birth, no censor 3.46 (1.44-8.34) 0.006 1.90 (0.90-18.31) 0.580
Multivariable analysis
Model 1 HR (95%CI) pModel 1 HR (95%CI) p
VTI-adjusted>58
4.98 (2.08-11.96)
<0.001
LDS vs. MFS 1.11 (0.40-3.10) 0.844
Male vs Female 1.54 (0.69-3.46) 0.294
xxx00.#####.ppt 2/25/2017 9:26:33 PM

2 / 2 5 / 2 0 1 7
1 6
Age =25 y Root = 4 cm (mild) Desc aorta=2.2cm (upper nl)
Supports waiting for surgery
Given:
xxx00.#####.ppt 2/25/2017 9:26:33 PM
No surgery If surgery now
Median survival in years 46.5 (95%CI 43-50) years 35 (95%CI 30-45)years
Median survival without Type Adissection
24 (95%CI 21-30) years 44.5 (95%CI 39-50)years
Mean Quality-adjusted life years(estimated)
40.7 ± 13.6 years 28.6 ± 16.6 years
P <0.0001P =0.116
A ge=25y R oot= 4 cm (m ild) Descaorta=2.2 cm(uppernl)
S upportsw aitingforsurgery
Given:
N osurgery Ifsurgery now
M ediansurvivalinyears 46.5 (95% CI43-50)years 35 (95% CI30-45)years
M ediansurvivalw ithoutT ypeA dissection 24 (95% CI21-30)years 44.5 (95% CI39-50)years
M eanQ uality-adjustedlifeyears(estim ated) 40.7± 13.6 years 28.6 ± 16.6 years
P <0.0001P =0.116
2 / 2 5 / 2 0 1 7
1 7
xxx00.#####.ppt 2/25/2017 9:26:33 PM
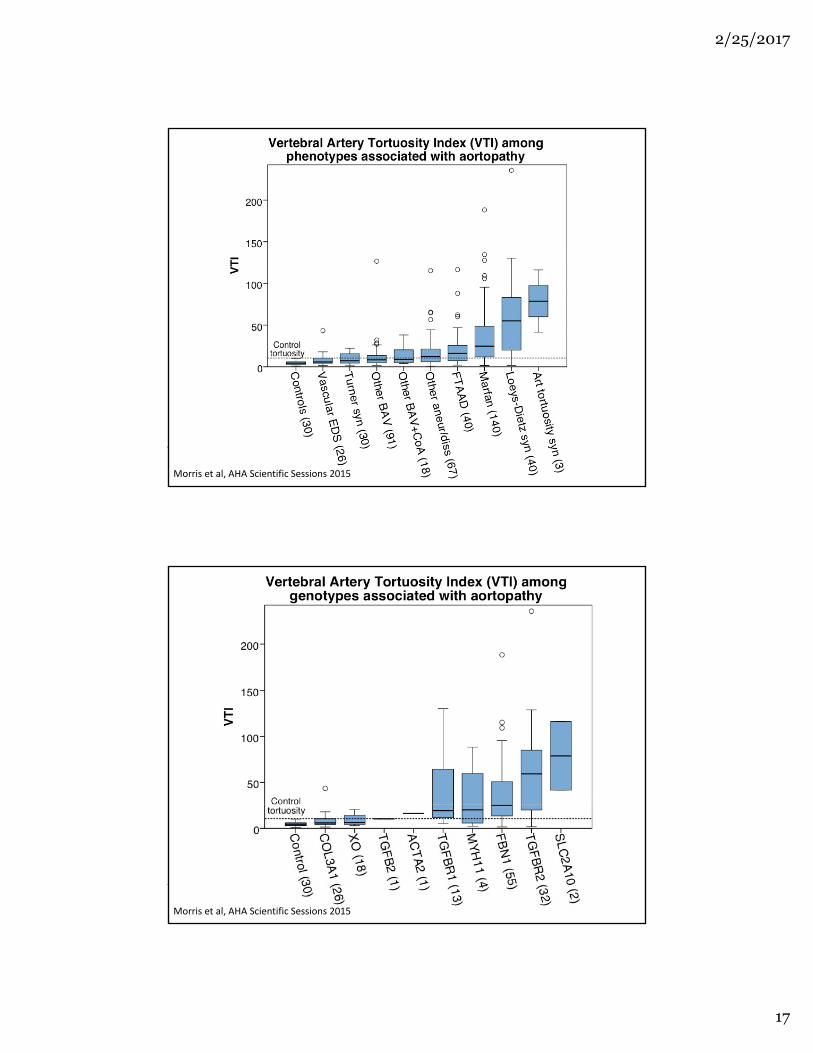
M orrisetal,AHA S cientificS essions2015
xxx00.#####.ppt 2/25/2017 9:26:33 PM
M orrisetal,AHA S cientificS essions2015
2 / 2 5 / 2 0 1 7
1 8
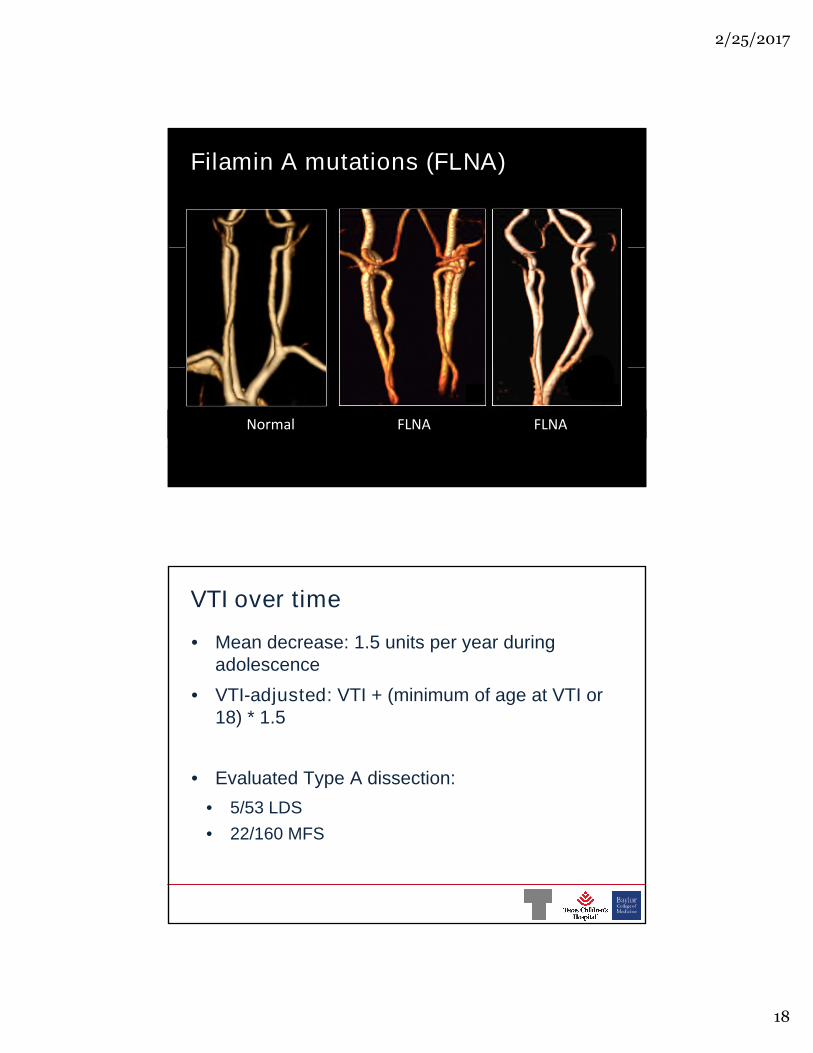
Filamin A mutations (FLNA)
xxx00.#####.ppt 2/25/2017 9:26:33 PM
N orm al FL N A FL N A
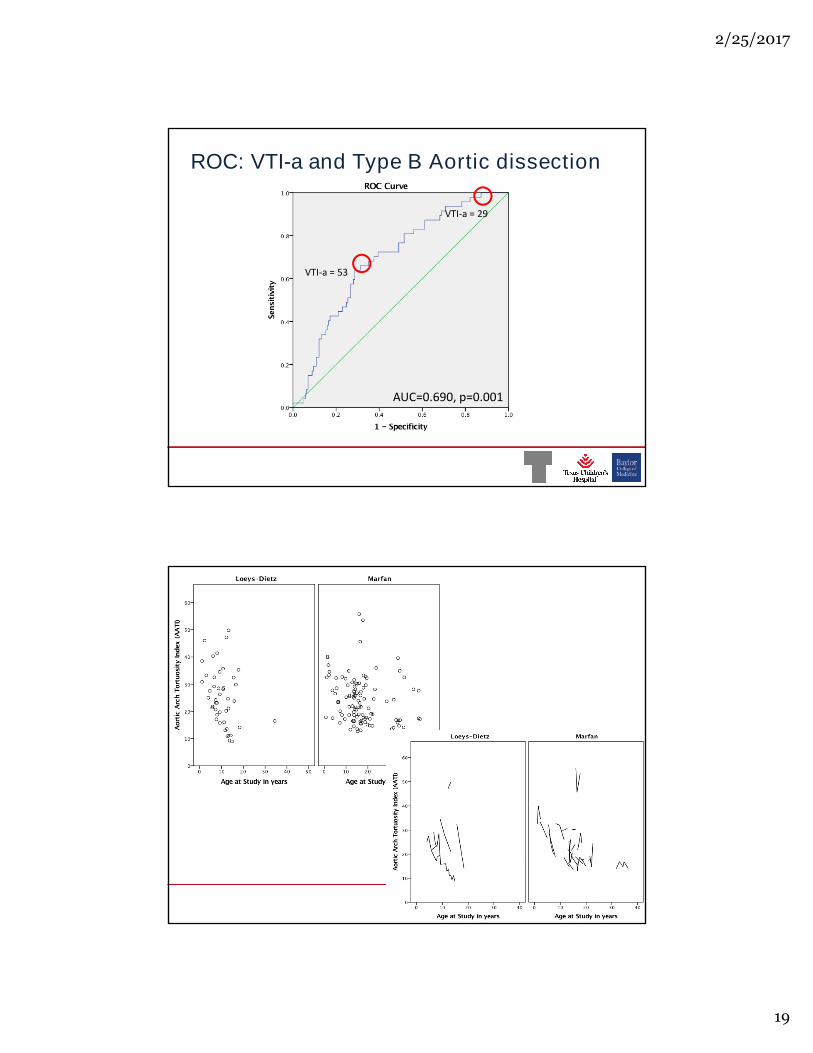
VTI over time
• Mean decrease: 1.5 units per year duringadolescence
• VTI-adjusted: VTI + (minimum of age at VTI or• VTI-adjusted: VTI + (minimum of age at VTI or18) * 1.5
• Evaluated Type A dissection:
• 5/53 LDS
xxx00.#####.ppt 2/25/2017 9:26:33 PM
• 5/53 LDS
• 22/160 MFS
2 / 2 5 / 2 0 1 7
1 9
ROC: VTI-a and Type B Aortic dissection
VT I-a= 29
VT I-a= 53
xxx00.#####.ppt 2/25/2017 9:26:33 PM
AU C=0.690,p=0.001
Extra Slides
xxx00.#####.ppt 2/25/2017 9:26:33 PM

2 / 2 5 / 2 0 1 7
2 0
Extra Slides
xxx00.#####.ppt 2/25/2017 9:26:33 PM
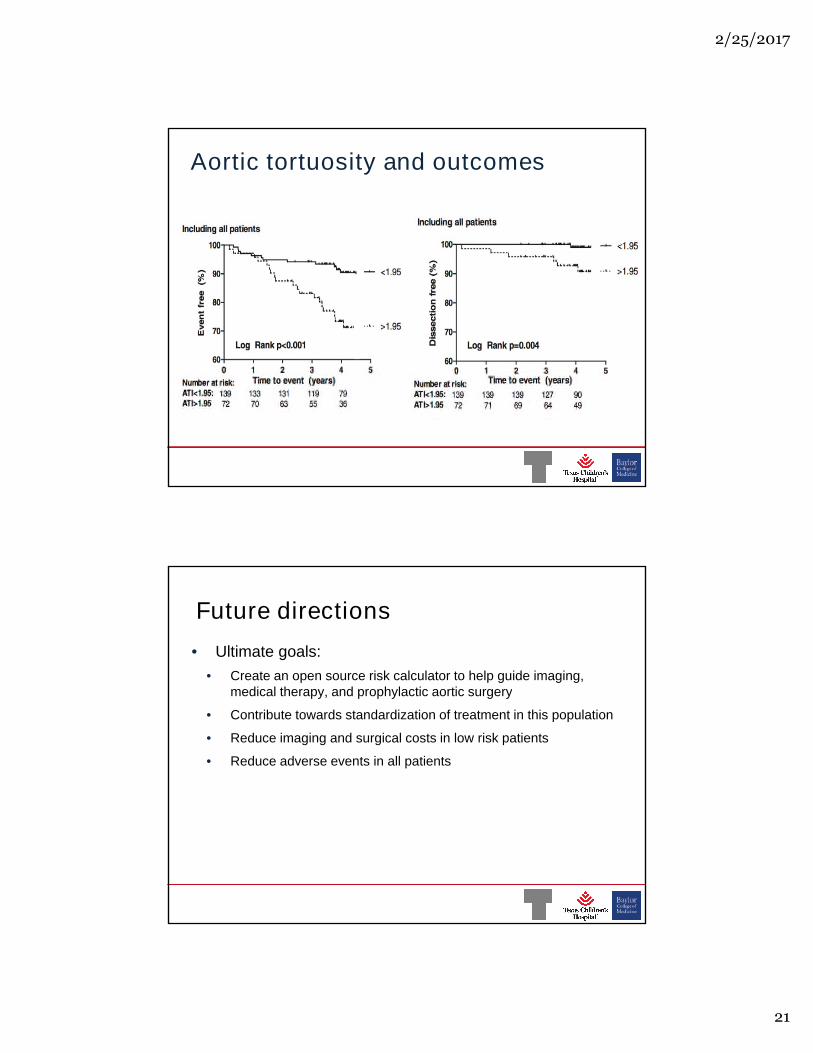
Aortic tortuosity and outcomes
• Franken et al.
• Secondary analysis of Dutch RCT
xxx00.#####.ppt 2/25/2017 9:26:33 PM
Frankenetal.IntJCardiology,2015
2 / 2 5 / 2 0 1 7
2 1
Aortic tortuosity and outcomes
xxx00.#####.ppt 2/25/2017 9:26:33 PM
Future directions
• Ultimate goals:
• Create an open source risk calculator to help guide imaging,medical therapy, and prophylactic aortic surgerymedical therapy, and prophylactic aortic surgery
• Contribute towards standardization of treatment in this population
• Reduce imaging and surgical costs in low risk patients
• Reduce adverse events in all patients
xxx00.#####.ppt 2/25/2017 9:26:33 PM

2 / 2 5 / 2 0 1 7
2 2
Concept of Static and Dynamic predictors
• Static predictors-Do not change with age• Gene affected
• Mutation• Mutation
• Sex
• Aortic z-score (usually)
• Dynamic (time-dependent) predictors- Changewith age
• Aortic dimension
xxx00.#####.ppt 2/25/2017 9:26:33 PM
• Aortic dimension
• Aortic surgery history
• Aortic dissection history
Aortic dimension/z-score
Dynamic Static
xxx00.#####.ppt 2/25/2017 9:26:33 PM
Tierney et al. J Peds 2007
2 / 2 5 / 2 0 1 7
2 3
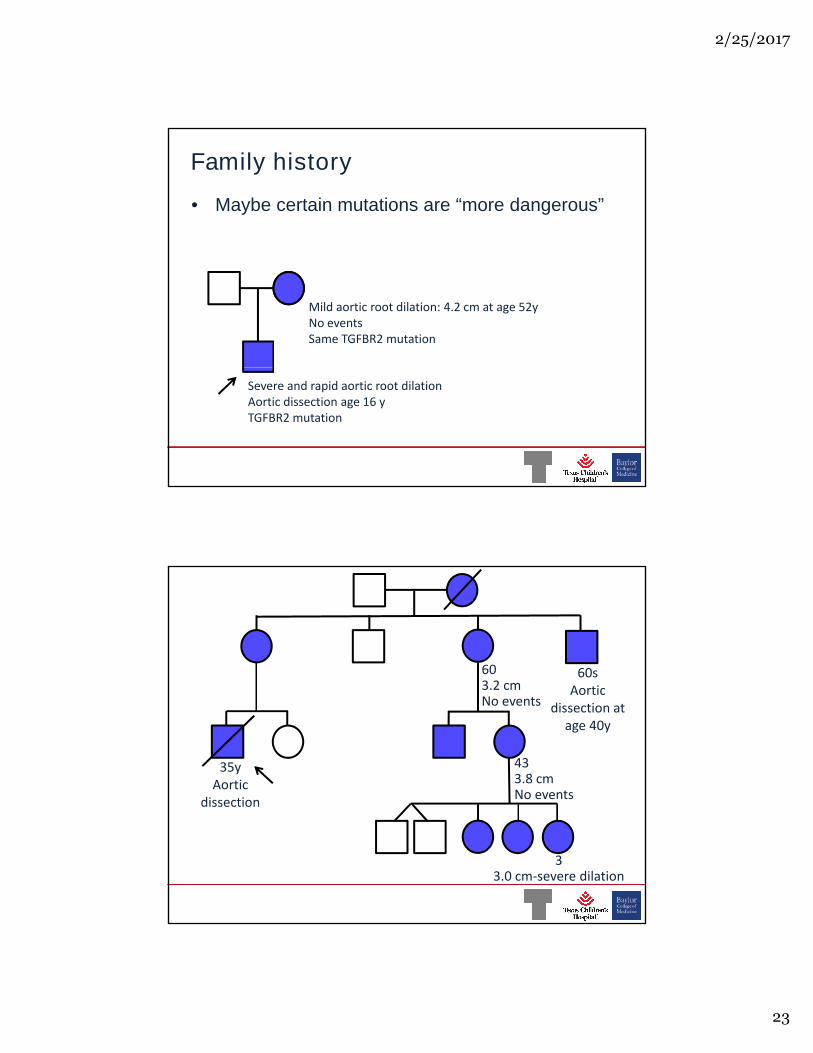
Family history
• Maybe certain mutations are “more dangerous”
M ildaorticrootdilation:4.2 cm atage52yN oeventsS am eT GFBR 2 m utation
xxx00.#####.ppt 2/25/2017 9:26:33 PM
S evereandrapidaorticrootdilationAorticdissectionage16 yT GFBR 2 m utation
60sAortic
603.2 cm
35yAortic
dissection
Aorticdissectionat
age40y
3.2 cmN oevents
433.8cmN oevents
xxx00.#####.ppt 2/25/2017 9:26:33 PM
dissection
33.0 cm -severedilation
2 / 2 5 / 2 0 1 7
2 4
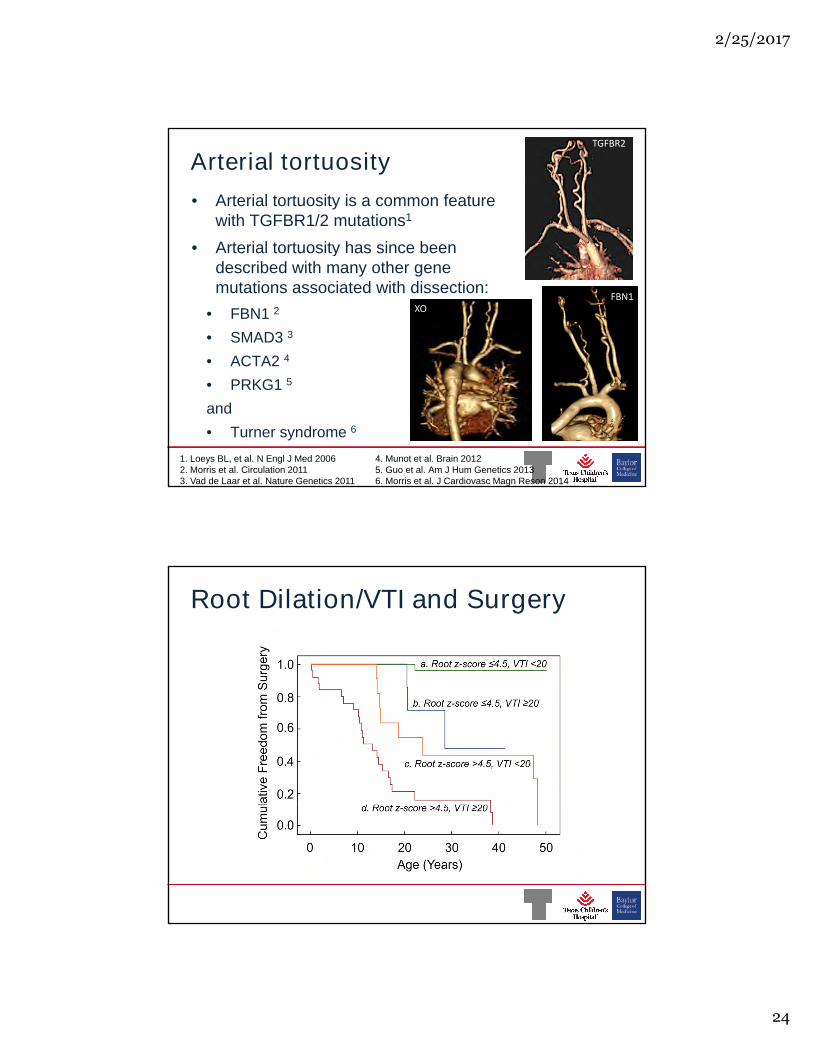
Arterial tortuosity
• Arterial tortuosity is a common featurewith TGFBR1/2 mutations1
• Arterial tortuosity has since been
T GFBR 2
• Arterial tortuosity has since beendescribed with many other genemutations associated with dissection:
• FBN1 2
• SMAD3 3
• ACTA2 4
FBN 1X O
xxx00.#####.ppt 2/25/2017 9:26:33 PM
• ACTA2
• PRKG1 5
and
• Turner syndrome 6
1. Loeys BL, et al. N Engl J Med 20062. Morris et al. Circulation 20113. Vad de Laar et al. Nature Genetics 2011
4. Munot et al. Brain 20125. Guo et al. Am J Hum Genetics 20136. Morris et al. J Cardiovasc Magn Reson 2014
Root Dilation/VTI and Surgery
xxx00.#####.ppt 2/25/2017 9:26:33 PM

2 / 2 5 / 2 0 1 7
2 5
xxx00.#####.ppt 2/25/2017 9:26:33 PM
Arterial tortuosity-etiology
• Overarching hypothesis: there is abnormallengthening of the arteries in a fixed space, resultingin forced curving and bending of the vesselsin forced curving and bending of the vessels
xxx00.#####.ppt 2/25/2017 9:26:33 PM
2 / 2 5 / 2 0 1 7
2 6
xxx00.#####.ppt 2/25/2017 9:26:33 PM
xxx00.#####.ppt 2/25/2017 9:26:33 PM

2 / 2 5 / 2 0 1 7
2 7
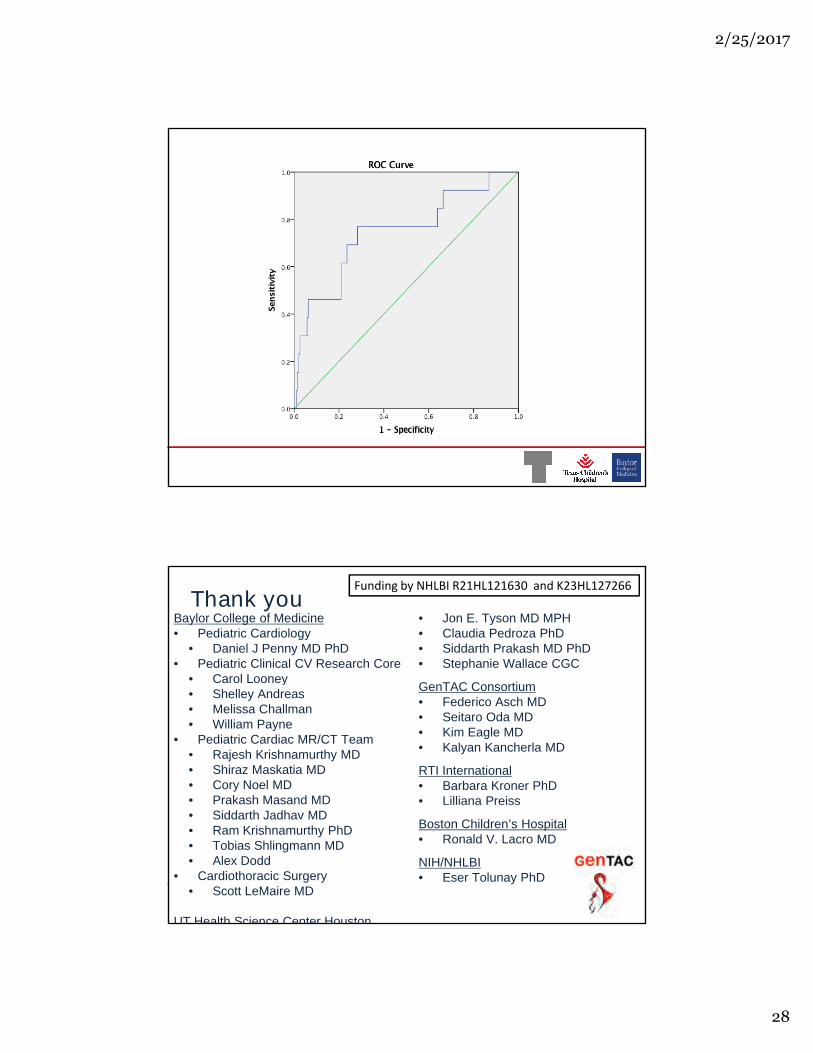
ROC: VTI-a and Type A Aortic dissection
VT I-a= 32
VT I-a= 58
xxx00.#####.ppt 2/25/2017 9:26:33 PM
AU C=0.679,p=0.003
Gene as a predictor• Some conditions seem to have a higher risk of
dissection at smaller dimensions
• TGFBR1/TGFBR2• TGFBR1/TGFBR2
• ACTA2“ Clinicaloutcom esappearsim ilarbetw eentreatedpatientsw ith T GFBR 2 m utationsandindividualsw ith
FBN 1 m utations.P rognosisdependsonclinicaldiseaseexpressionandtreatm entratherthansim ply the
presenceofaT GFBR 2 genem utation.”
xxx00.#####.ppt 2/25/2017 9:26:33 PM
presenceofaT GFBR 2 genem utation.”
Attiasetal.Circulation2009
2 / 2 5 / 2 0 1 7
2 8
xxx00.#####.ppt 2/25/2017 9:26:33 PM
Thank youBaylor College of Medicine• Pediatric Cardiology
• Daniel J Penny MD PhD• Pediatric Clinical CV Research Core
• Carol Looney
• Jon E. Tyson MD MPH• Claudia Pedroza PhD• Siddarth Prakash MD PhD• Stephanie Wallace CGC
GenTAC Consortium
Fundingby N HL BIR 21HL 121630 andK23HL 127266
• Carol Looney• Shelley Andreas• Melissa Challman• William Payne
• Pediatric Cardiac MR/CT Team• Rajesh Krishnamurthy MD• Shiraz Maskatia MD• Cory Noel MD• Prakash Masand MD
GenTAC Consortium• Federico Asch MD• Seitaro Oda MD• Kim Eagle MD• Kalyan Kancherla MD
RTI International• Barbara Kroner PhD• Lilliana Preiss
xxx00.#####.ppt 2/25/2017 9:26:33 PM
• Prakash Masand MD• Siddarth Jadhav MD• Ram Krishnamurthy PhD• Tobias Shlingmann MD• Alex Dodd
• Cardiothoracic Surgery• Scott LeMaire MD
UT Health Science Center Houston
• Lilliana Preiss
Boston Children’s Hospital• Ronald V. Lacro MD
NIH/NHLBI• Eser Tolunay PhD











![ARTERIAL PERIPHERAL VASCULAR DISEASES.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000113-cardiovascular-system/… · arterial peripheral vascular diseases acute arterial occlusion](https://static.fdocuments.us/doc/165x107/604e83caf1418f71db611c5a/arterial-peripheral-vascular-read-onlyocwusuacidcoursedownload1110000113-cardiovascular-system.jpg)





