
Arsenic (PIM G042) Página 1 de 47 - Pan American Health … · · 2002-01-29Arsenic (PIM G042)...
47
Arsenic (PIM G042) Página 1 de 4 http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/0 ARSENIC, INORGANIC International Programme on Chemical Safety Poisons Information Monograph 042 Chemical 1. NAME 1.1 Substance Arsenic, inorganic 1.2 Group 1.3 Synonyms Table 1 Arsenic and salts: synonyms, structure and identification numbers (IPCS, 1992) Chemical Relative Structural Identification numbers name molecular formula mass CAS RTECS UN INORGANIC (III) Arsenic sulfide 246,02 As 2 S 3 1303-33-9 CG2638000 1557 Synonyms and trade names * Arsenic sesquisulfide * Arsenic tersulphide * Arsenic trisulphide * Arsenic yellow * Arsenious sulphide * Arsenous sulphide * Auripigment * C.I. 77086 * C.I. pigment yellow * Diarsenic trisulphide * Kings Gold
Transcript of Arsenic (PIM G042) Página 1 de 47 - Pan American Health … · · 2002-01-29Arsenic (PIM G042)...

Arsenic (PIM G042) Página 1 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
ARSENIC, INORGANIC
International Programme on Chemical Safety Poisons Information Monograph 042 Chemical
1. NAME
1.1 Substance
Arsenic, inorganic
1.2 Group
1.3 Synonyms Table 1 Arsenic and salts: synonyms, structure and identification numbers (IPCS, 1992)
Chemical Relative Structural Identification numbers name molecular formula mass CAS RTECS UN
INORGANIC (III)
Arsenic sulfide 246,02 As2S3 1303-33-9 CG2638000 1557
Synonyms and trade names
* Arsenic sesquisulfide * Arsenic tersulphide * Arsenic trisulphide * Arsenic yellow * Arsenious sulphide * Arsenous sulphide * Auripigment * C.I. 77086 * C.I. pigment yellow * Diarsenic trisulphide * Kings Gold

Arsenic (PIM G042) Página 2 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
* Orpiment
Chemical Relative Structural Identification numbers name molecular formula mass CAS RTECS UN
Arsenic 181,27 AsCl3 7784-34-1 CG1750000 1560 trichloride
Synonyms and trade names
* Arsenic butter * Arsenious chloride * Arsenous chloride * Caustic arsenic chloride * Caustic oil of arsenic * Fuming liquid arsenic
Arsenic 197,82 As2O3 1327-53-3 CG3325000 1561 trioxide
Synonyms and trade names
* Arsenic oxide * Arsenic (III)oxide * Arsenic sesqui oxide * Arsenicum album * Arsenious acid * Arsenious oxide * Arsenious trioxide * Arsenite * Arsenolite * Arsenous acid
* Arsenous

Arsenic (PIM G042) Página 3 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
anhydride * Arsenous oxide * Arsenous oxide anhydride * Arsodent * Claudelite * Crude arsenic * Diarsenic trioxide * White arsenic
Chemical Relative Structural Identification numbers name molecular formula mass CAS RTECS UN
Cupric 187,46 CuHAsO3 10290-12-7 CG3385000 1586 arsenide
Synonyms and trade names
* Schelle's green
Gallium 144,64 AsGa 1303-00-0 LW8800000 n.a. arsenide
Synonyms and trade names
* Gallium monoarsenide
Potassium 399,65 KH(AsO2)2 10124-50-2 38000000 1678 arsenite
Synonyms and trade names
* Arsenenous acid, potassium salt * Arsenious acid
potassium salt * Arsonic

Arsenic (PIM G042) Página 4 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
acid, potassium salt * Fowlers solution * Potassium metaarsenite
Chemical Relative Structural Identification numbers name molecular formula mass CAS RTECS UN
Sodium 129,9 NaAsO2 7784-46-5 CG367500 1686 arsenite 2027
Synonyms and trade names
* Arsenenous acid, sodium salt * Arsenious acid, sodium salt * Prodalumnol * Sodanit * Sodium metaarsenite
INORGANIC (V)
Arsenic pentoxide 229,84 As2O5 1303-28-2 GC2275000 1559
Synonyms and trade names
* Arsenic acid * Arsenic acid anhydride * Arsenic oxide * Arsenic (V) oxide
* Diarsenic pentoxide
Chemical Relative Structural Identification numbers name molecular formula

Arsenic (PIM G042) Página 5 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
mass CAS RTECS UN
Calcium 398,06 Ca3(AsO4)2 7778-44-1 CG0830000 1573 arsenate
Synonyms and trade names
* Arsenic acid calcium salt * Calcium orthoarsenate * Chipcal * Pencal * Spracal * Tricalcium arsenate
Lead 347,12 PbHAsO4 7784-40-9 CG0980000 1617 arsenate
Synonyms and trade names
* Acid lead arsenate * Acid lead orthoarsenate * Arsenate of lead * Arsenic acid lead salt * Arsinette * Gypsine * Lead acid arsenate * Plumbous arsenate * Schultenite * Soprabel
* Standard lead arsenate * Talbot
Chemical Relative Structural Identification numbers name molecular formula mass CAS RTECS UN
Arsenic (PIM G042) Página 6 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
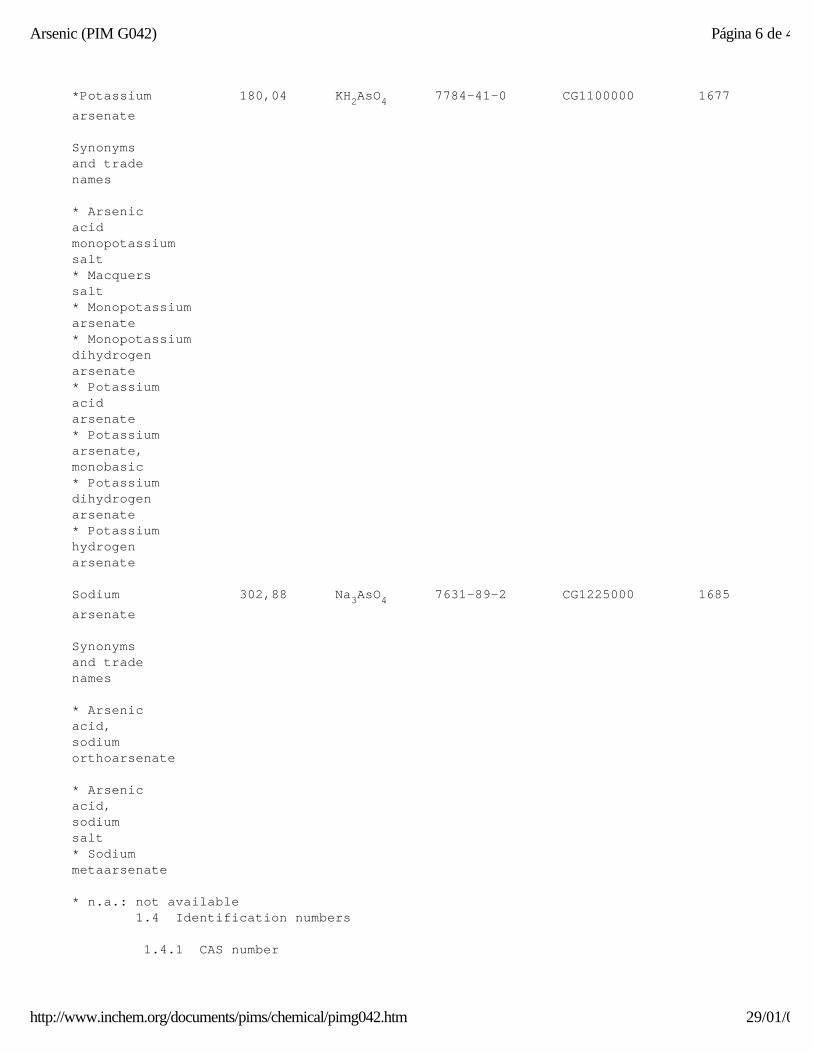
*Potassium 180,04 KH2AsO4 7784-41-0 CG1100000 1677 arsenate
Synonyms and trade names
* Arsenic acid monopotassium salt * Macquers salt * Monopotassium arsenate * Monopotassium dihydrogen arsenate * Potassium acid arsenate * Potassium arsenate, monobasic * Potassium dihydrogen arsenate * Potassium hydrogen arsenate
Sodium 302,88 Na3AsO4 7631-89-2 CG1225000 1685 arsenate
Synonyms and trade names
* Arsenic acid, sodium orthoarsenate
* Arsenic acid, sodium salt * Sodium metaarsenate
* n.a.: not available 1.4 Identification numbers
1.4.1 CAS number

Arsenic (PIM G042) Página 7 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
See table 1.3
1.4.2 Other numbers
See table 1.3
1.5 Main brand names, main trade names
1.6 Main manufactures, main importers
2. SUMMARY
2.1 Main risks and target organs
After absorption, arsenic may cause multi-organ failure. The primary target organs initially are gastrointestinal tract, the heart, brain and kidneys. The skin, bone marrow and peripheral nervous system may be affected. In severe poisoning, the patient may die early of cardiovascular disturbances, mainly intravascular volume depletion and severe shock.
2.2 Summary of clinical effects
In acute poisoning, symptoms begin usually within the first hours following ingestion. Garlic-like odour of breath, gastric content and faeces may be indicative. Gastrointestinal disturbances (vomiting, gastrointestinal pain, diarrhoea) are the main clinical effects. After an apparent remission (1 to 2 days), several organs are affected by the systemic action of inorganic arsenic (cardiovascular, renal, hepatic and cutaneous manifestations). This will produce hypotension, tachycardia, ECG modifications of QT and T wave, airway irritation, pulmonary oedema, haematuria, acute renal failure, acute haemolysis, altered mental status, confusion, delirium, convulsions, encephalopathy. If the patient survives the cardiovascular failure, and after a long convalescence, sequelae are observed, mainly peripheral neuropathy and Mee's lines on nails.
2.3 Diagnosis
Diagnosis is based on history, symptoms, signs and laboratory investigations, but treatment should start on suspicion of poisoning. The diagnosis may be confirmed by quantification of arsenic in urine in acute cases and hair in chronic exposure. In acute, massive arsenic ingestion, barium-like opacities on abdominal X-ray may be demonstrated.
2.4 First-aid measures and management principles

Arsenic (PIM G042) Página 8 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
Due to the toxic action of inorganic arsenic on the gastrointestinal tract in acute poisoning, and the subsequent liquid losses, special care to the fluid-electrolyte balance is required to prevent cardiovascular toxicity. Hypovolemia, cardiac arrhythmias and cardiovascular failure are the main cause of early death. Transport of the patient to an hospital and monitoring of vital functions in an intensive care department is therefore mandatory. Gastric decontamination using gastric lavage and activated charcoal is highly recommended. Whole bowel irrigation should be considered if the presence of arsenic in the lower gastro-intestinal tract is observed by X-ray. Maintain high urine output with an alkaline pH. Chelation therapy using BAL or DMSA or DMSP should be rapidly envisaged. In the meantime, first aid should be commenced.
3. PHYSICO-CHEMICAL PROPERTIES
3.1 Origin of the substance
Arsenic is an ubiquitous element mainly present in the lithosphere as arsenic minerals or arsenic impurities in minerals or as arsenic in various rock types and fossil fuels (NRCC, 1978). In soils, arsenic is present as arsenite (As(III)) and arsenate (As(V)) and in an organic form. Industrial and agricultural sources of arsenic may enhance, sometimes in a dramatic way, the natural levels of arsenic: mining activities, smelters, coal and coal combustion by-products, withdrawal sludges, pesticides (Bhumbla, 1994; NRCC, 1978).
3.2 Chemical structure
Chemical name : See table 1.3 Relative molecular mass : See table 1.3 Structural formula : See table 1.3 Table 2 Arsenic and salts: physico-chemical properties (IPCS, 1992) Arsenic Normal state Colour Odour Soluble Insoluble compound (at room (g/litre) temperature) INORGANIC (III) * Arsenic * Powder * Yellow-red n.a. * Hot water * Water sulphide (slightly) (cold) * Alkali

Arsenic (PIM G042) Página 9 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
* Acids * Ethanol * Arsenic * Liquid * Colourless Acrid * Ethanol * (decomposed trichloride (oily) smell * Ether by water) * Concentrated mineral acids * Arsenic * Powder * White Odour * Water * Alcohol trioxide (amorphous or less - cold (12) * Chloroform crystalline) - 20EC (37) * Ether - hot (115) * Alkali * HCl
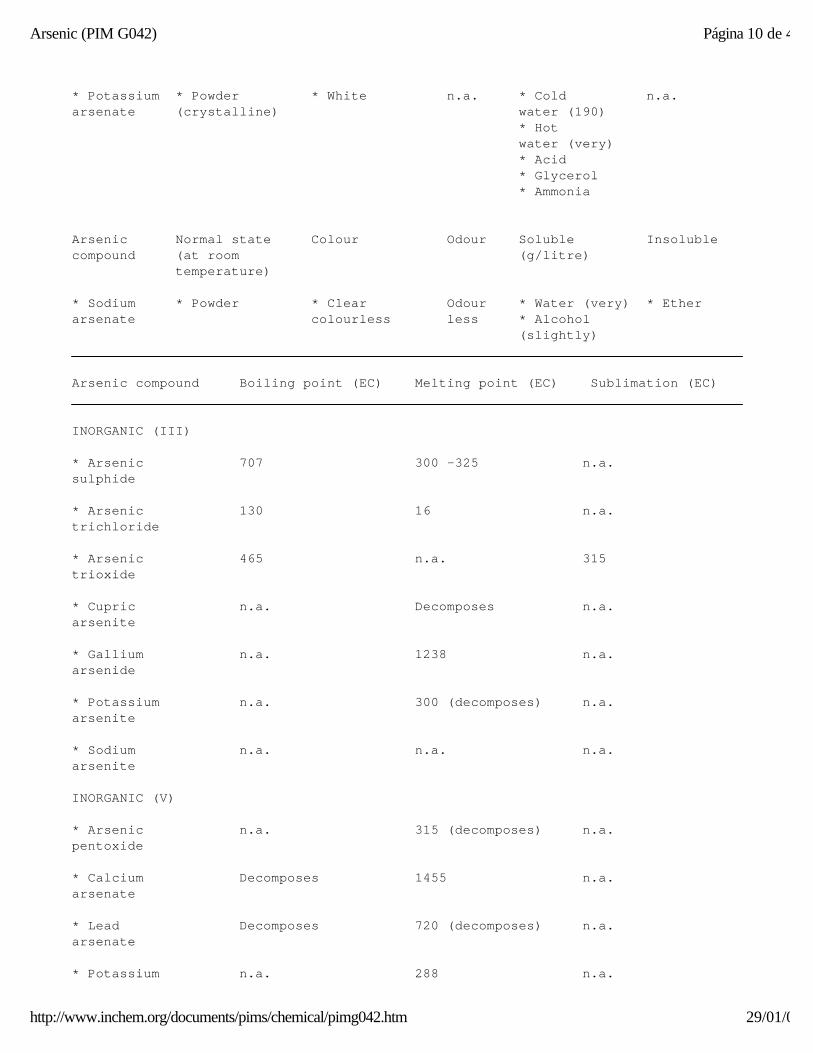
Arsenic Normal state Colour Odour Soluble Insoluble compound (at room (g/litre) temperature) * Cupric * Powder * Yellowish- n.a. * Acids * Water arsenite green * Ammonia * Alcohol * Gallium * Solid * Dark grey n.a. n.a. * Water arsenide (cubic with crystals) metallic sheen * Potassium * Powder * White n.a. * Water n.a. arsenite * Ethanol (Slightly) * Sodium * Powder * White n.a. * Water n.a. arsenite or greyish- (very) white * Ethyl alcohol (slightly) INORGANIC (V) * Arsenic Powder * White n.a. * Cold n.a. pentoxide (hygroscopic) water (1500) * Hot water (767) * Calcium Powder * Colourless Odour- * Water n.a. arsenate (amorphous) less (slightly) * Dilute acids * Lead * Powder * White n.a. * Hot water arsenate or solid (slightly) n.a. (crystalline) * Dilute nitric acid * Caustic alkalis
Arsenic (PIM G042) Página 10 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
* Potassium * Powder * White n.a. * Cold n.a. arsenate (crystalline) water (190) * Hot water (very) * Acid * Glycerol * Ammonia
Arsenic Normal state Colour Odour Soluble Insoluble compound (at room (g/litre) temperature) * Sodium * Powder * Clear Odour * Water (very) * Ether arsenate colourless less * Alcohol (slightly) Arsenic compound Boiling point (EC) Melting point (EC) Sublimation (EC) INORGANIC (III) * Arsenic 707 300 -325 n.a. sulphide * Arsenic 130 16 n.a. trichloride
* Arsenic 465 n.a. 315 trioxide * Cupric n.a. Decomposes n.a. arsenite * Gallium n.a. 1238 n.a. arsenide * Potassium n.a. 300 (decomposes) n.a. arsenite * Sodium n.a. n.a. n.a. arsenite INORGANIC (V) * Arsenic n.a. 315 (decomposes) n.a. pentoxide * Calcium Decomposes 1455 n.a. arsenate * Lead Decomposes 720 (decomposes) n.a. arsenate * Potassium n.a. 288 n.a.
Arsenic (PIM G042) Página 11 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
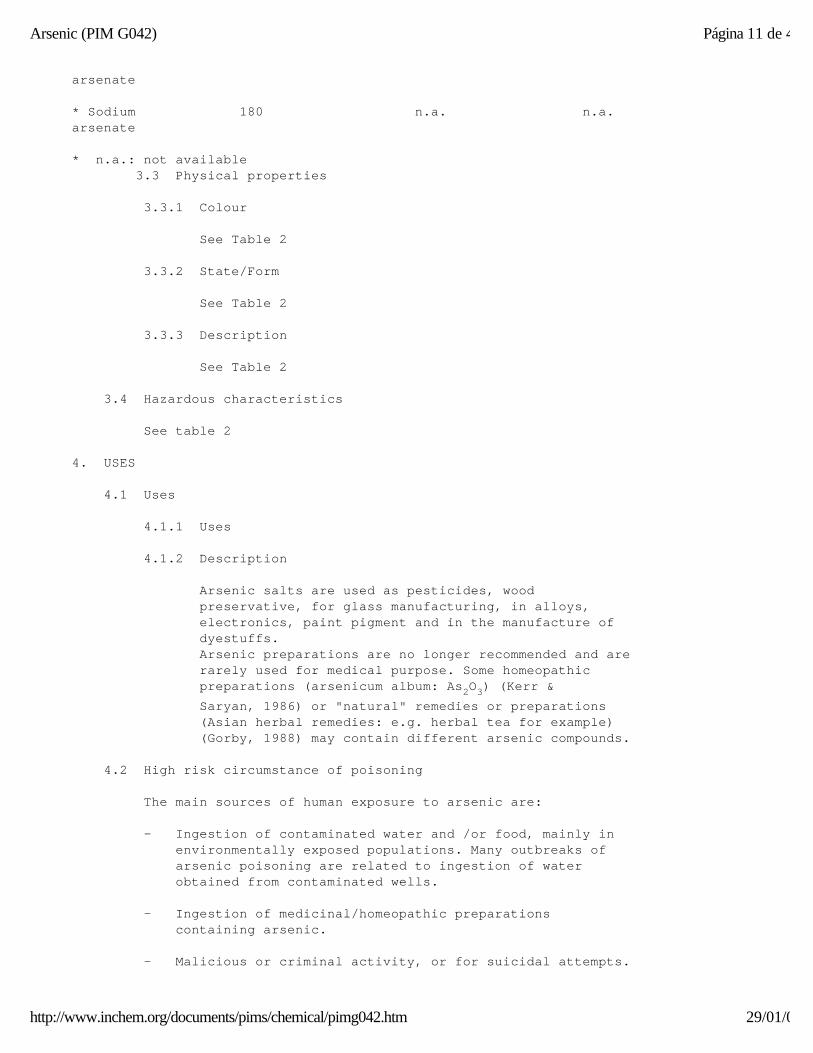
arsenate * Sodium 180 n.a. n.a. arsenate * n.a.: not available 3.3 Physical properties
3.3.1 Colour
See Table 2
3.3.2 State/Form
See Table 2
3.3.3 Description
See Table 2
3.4 Hazardous characteristics
See table 2
4. USES
4.1 Uses
4.1.1 Uses
4.1.2 Description
Arsenic salts are used as pesticides, wood preservative, for glass manufacturing, in alloys, electronics, paint pigment and in the manufacture of dyestuffs. Arsenic preparations are no longer recommended and are rarely used for medical purpose. Some homeopathic preparations (arsenicum album: As2O3) (Kerr & Saryan, 1986) or "natural" remedies or preparations (Asian herbal remedies: e.g. herbal tea for example) (Gorby, 1988) may contain different arsenic compounds.
4.2 High risk circumstance of poisoning
The main sources of human exposure to arsenic are: - Ingestion of contaminated water and /or food, mainly in environmentally exposed populations. Many outbreaks of arsenic poisoning are related to ingestion of water obtained from contaminated wells. - Ingestion of medicinal/homeopathic preparations containing arsenic. - Malicious or criminal activity, or for suicidal attempts.
Arsenic (PIM G042) Página 12 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
4.3 Occupationally exposed populations
Inhalation of arsenic containing dusts or volatile arsenicals during industrial or agricultural exposures. Absorption through skin and mucous membranes during the handling of arsenicals or through prolonged therapeutic usage of arsenical preparations. Main occupational exposures are the following: - Workers (mainly roaster workers) engaged in the smelting industries: copper, gold, lead, silver and zinc ores, where arsenic is present as a contaminant or by-product. - Workers engaged in the manufacturing of pesticides, herbicides and other agricultural products using arsenic preparations and industrial or agricultural workers using them.
- Arsenic in wood processing plants. - Arsenic as desiccant or defoliant for the preparation of cotton fields for harvesting. - Various metallurgical or industrial activities like the electrolysis of copper, or cadmium, with arsenic as a contaminant.
5. ROUTES OF EXPOSURE
5.1 Oral
Oral absorption of arsenic is the main route of exposure for the general population and may be accidental (ingestion of arsenical pesticides by children) or, more rarely, voluntary or criminal. During occupational exposure, ingestion of inhaled arsenic dusts or direct contamination through lack of occupational hygiene.
5.2 Inhalation
Inhalation exposure to dusts or aerosols containing arsenic occurs mainly in industry (smelting of ores) or agriculture (mixing and/or spraying pesticides) and can produce toxic effects on the respiratory tract along with systemic effects.
5.3 Dermal
Dermal absorption can result from topical application of arsenical agents or from accidental contact with arsenicals (eg. arsenic acid: Garb & Hine, 1977) and may result in systemic toxicity.
Arsenic (PIM G042) Página 13 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
5.4 Eye
Ocular contact with dusts or accidental splashing has occurred in industry (Grant, 1986), resulting in local toxic effects.
5.5 Parenteral
No data available.
5.6 Others
No data available.
6. KINETICS
6.1 Absorption by route of exposure
Oral absorption Pentavalent arsenic compounds are almost totally absorbed (till 90%) in most species. The absorption of trivalent arsenic is limited, although the toxicity is greater because of the high lipid solubility (Mahieu et al., 1981; Schoolmeester & White, 1980). Absorption by inhalation Animals studies indicate a wide range of absorption according to species, chemical form and particle size of arsenicals; the clearance half-life from the lungs being from 30 minutes to several days. Several studies, involving workers exposed to inorganic arsenic, indicate a rather good relationship between airborne concentrations of inorganic arsenic and urinary excretion of arsenic and its metabolites. Skin absorption Systemic poisoning involving prolonged cutaneous application of arsenical agents (Robinson, 1975) or splashing on the skin of arsenic acid (Garb & Hine, 1977) indicate an absorption of inorganic arsenic through the skin.
6.2 Distribution by route of exposure
Once absorbed, arsenic is bound to haemoglobin, leucocytes, and plasma proteins. It is cleared from the intravascular space within 24 hours, and distributed in most tissues (Jolliffee, 1991; Schoolmeester & White, 1980). The ratio between red cell and plasma arsenic concentrations increases with the level of exposure: from 1/1 for low exposures to 3/1 for high environmental exposures (Vahter, 1983).
Arsenic (PIM G042) Página 14 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
Soluble inorganic compounds, well absorbed by gastro-intestinal tract or by lungs, are rapidly distributed to organs or tissues rich in proteins containing sulfhydryl groups, and accumulate mainly in liver, kidneys, spleen and adrenal gland (Quatrehomme, 1992).
In humans, not exposed occupationally or environmentally to arsenic compounds, arsenic binds to the sulfhydryl groups in keratin and can be detected in hair, nails, and skin 2 to 4 weeks after exposure. After 4 weeks, arsenic localizes in bone, coinciding with decreasing levels in the liver and kidneys (Jolliffe et al., 1991; Schoolmeester & White, 1980; Winship, 1984). Arsenic compounds can cross the placental barrier (Lugo, 1969).
6.3 Biological half-life by route of exposure
Blood clearance of arsenic occurs in three phases. In phase 1, a rapid decline occurs within 2 to 3 hours; some estimate that greater than 90% of arsenic clears from the blood, with a half-life of 1 to 2 hours (Vahter, 1980; McKinney, 1992). For the remaining arsenic, a more gradual decline occurs in phase 2, from 3 hours to 7 days (estimated half-life is 30 hours), followed by phase 3, a slower elimination phase with an estimated half-life of 200 hours (Vahter, 1980; Mealey, 1959)
6.4 Metabolism
After absorption inorganic arsenic is biotransformed into two organic methylated derivatives: - Monomethylarsenic (MMA) and - Dimethylarsenic acid (DMA) DMA seems to be produced by a subsequent methylation of the MMA precursor (Buchet et al., 1981; Buchet & Lauwerys, 1985). The methylation process is dose dependent and as the dose of arsenic increases, a reduction of the percentage of DMA is observed in urine while retention of arsenic is higher (EPA, 1984; Vahter, 1983). Unusual metabolic processes have been reported in literature: - Case of methylenetetrahydrofolate reductase deficiency, with increased neurotoxicity of arsenic, in a 16-year-old girl, exposed to arsenic from CCA, in Suriname (Brouwer et al., 1992).
- Very little excretion of arsenic in urine, as MMA (about 2%), in native Andean women exposed to high levels of arsenic in water (Vahter et al., 1995). In this case, a

Arsenic (PIM G042) Página 15 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
genetic polymorphism in the control of the methyltransferase activity has been postulated.
Compared with inorganic As, the methylated metabolites are less reactive with tissue constituents, less acutely toxic, less cytotoxic, and more readily excreted in the urine (ATSDR, 1998).
6.5 Elimination by route of exposure
Inorganic arsenic compounds are mainly excreted via the kidneys but the rate of urinary arsenic excretion depends upon the chemical form of the compound ingested, the route of exposure and the dose level (Vahter, 1983). Other secondary routes of elimination are hair, nails, sweat and faeces. Urinary excretion Following absorption of inorganic arsenic, arsenic is excreted in the urine as DMA (60%) MMA (20%) and inorganic arsenic (20%) (Crecelius, 1977; Tam et al., 1979). One day after an ingestion of an oral dose (10 µg of arsenic as main pentavalent compound, i.e. arsenic acid 90%), 22.4% is recovered in urine; 57.9% after 5 days (Tam et al., 1979). In the presence of insoluble inorganic compounds like arsenic selenite, there is no urinary excretion (Mappes, 1977). When multiple doses are administered, at steady state, 60% of the dose is excreted in urine (Buchet et al., 1981). It has been estimated that the daily excretion of arsenic metabolites is 30 - 60% of the inhaled amount (ATSDR, 1998). Other routes of excretion - Faecal/biliary excretion Only a few percent is excreted in faeces (Ishinishi et al., 1986). This small faecal excretion (< 10%) is probably related to a reabsorption by intestines of arsenic eliminated by the bile. - Sweat Sweat in a hot, humid environment can eliminate 2 µg of As per hour (Vahter, 1983). - Skin Desquamation of skin can contribute to an elimination of 0,1 to 0,2 µg of As per day (Molin, 1976).
- Hair and nails
Arsenic (PIM G042) Página 16 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
Inorganic arsenic is incorporated to hairs or nails (Winship, 1984).
7. TOXICOLOGY
7.1 Mode of action
The toxicity of arsenic compounds is generally linked to the soluble inorganic trivalent forms. The toxicity of pentavalent inorganic compounds seems related to the in vivo reduction of As(V) to As(III) (Harvey, 1970). Inorganic arsenic compounds react with sulfhydryl (-SH) groups of cellular proteins, thereby inhibiting cellular oxidative processes (pyruvate and succinate oxidative pathways) (Arena & Drew, 1986; Harvey, 1970; Schoolmeester & White, 1980). Competition with phosphorus in the oxidative phosphorylation process is caused by inorganic compounds (Dickerson, 1994), mainly in the pentavalent form (Harvey, 1970). The diffuse toxic process of arsenic poisoning causes widespread endothelial cellular toxicity, resulting in capillary damage and tissue hypoxia precipitating generalized vasodilatation and transudation of plasma. Gastrointestinal, cardiac, renal, bone marrow, central nervous system, and hepatic damage may be noted at different stages of arsenic poisoning (Donofrio et al., 1987; Fincher & Koeker, 1987; Jolliffe et al., 1991; Schoolmeester & White, 1980; Winship, 1984).
7.2 Toxicity
7.2.1 Human data
7.2.1.1 Adults
A certain tolerance is believed to develop upon repeated long term exposure with low doses as seen in arsenic-eaters in Austria and Styria, in last century (Tardieu, 1867). Though not well documented in the scientific literature, that tolerance could be seen against acute poisoning (Foa, 1987). In adults, the estimated lethal dose varies from 50 to 300 mg of inorganic compounds (Armstrong et al., 1984; Hindmarsh, 1986; Vallee, 1960; Zaloga et al., 1985).
For As2O3, the lowest reported lethal dose is about 120 mg (Arena, 1967). The fatal dose of ingested arsenic trioxide has also
Arsenic (PIM G042) Página 17 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
been reported to lie between 70 and 180 mg (Vallee, 1960). Severe toxicity has been reported with the ingestion of as little as 1 mg As203, but as little as 20 mg can be life threatening (Schoolmeester et al., 1980; Winship, 1984).
7.2.1.2 Children
Subchronic oral exposure to only 3 mg/day was fatal in a number of children exposed to arsenic via contaminated milk (Hamamoto, 1955).
7.2.2 Relevant animal data
Experimental data suggest that animals are not as sensitive to inorganic arsenic compounds as humans, and that this difference is not due entirely to differences in gastro-intestinal absorption (ATSDR, 1989).
7.2.3 Relevant in vitro data
No relevant data.
7.2.4 Workplace standards
American conference of Governmental Industrial Hygienists (ACGIH) - ACGIH (1995) consider arsenic, elemental (7440-38-2) and inorganic arsenic compounds (except arsine) as a confirmed human carcinogen, and has set up the standard for arsenic at 0,01 mg/m3 (TLV-TWA: Threshold Limit Value - Time - Weighted Average). - ACGIH (1995) has adopted also a Biological Exposure Indice (BEI) for arsenic and soluble compounds including arsine (7784-42-1) of 50 µg/g creatinine (inorganic arsenic metabolites in urine), for a sampling time at the end of the workweek.
7.2.5 Acceptable daily intake (ADI) and other guideline levels
International standards
- Provisional tolerable weekly intake (PTWI)
0.015 mg/kg/body weight for inorganic arsenic. There is a narrow margin between the PTWI and intakes
Arsenic (PIM G042) Página 18 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
reported in epidemiological studies to have toxic effects (FAO/WHO, 1989).
- Reference dose (RfD)
0.0003 mg/kg/day is the oral reference dose established by the EPA for inorganic arsenic (IRIS, 1996)
- Drinking water guidelines
0.01 mg/As (total)/L is the provisional guideline value recommended by the World Health Organization (WHO, 1996).
- Air quality guidelines
No safe level for arsenic can be recommended, because there is no known safe threshold (WHO, 1987).
7.3 Carcinogenicity
American Conference of Governmental Industrial Hygienists (ACGIH) ACGIH (1995) consider As elemental (7440-38-2) and inorganic compounds (except arsine) as confirmed human carcinogen. Environmental Protection Agency (EPA) Inorganic arsenic is classified by EPA as a group A carcinogen (a known human carcinogen), under the EPA classification (ATSDR, 1989) International Agency for Research on Cancer (IARC) In humans, exposure to inorganic arsenic via drinking water (contaminated wells), drugs (Fowler's solution) and pesticides can lead to skin cancers. Respiratory cancers have been observed in workers manufacturing arsenical pesticides and among copper smelter workers, exposed to inorganic arsenic, but also to other toxic substances (IARC, 1990).
There is inadequate evidence for the carcinogenicity of arsenic compounds in animals (IARC, 1990). There is sufficient evidence that inorganic arsenic compounds are skin and lung carcinogens in humans. The data suggesting an increased risk for cancer at other sites are inadequate for evaluation (IARC, 1990). Arsenic and arsenic compounds are classified by IARC in the group 1: "The agent is carcinogenic to humans".

Arsenic (PIM G042) Página 19 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
7.4 Teratogenicity
In animals, inorganic arsenic compounds are embryo lethal or teratogenic (Barlow & Sullivan, 1982): - sodium arsenate: hamster, mouse, rat - sodium arsenite: mouse Although sodium arsenate has been shown to be teratogenic and embryo toxic in several experimental animals, intravenous and intra peritoneal doses to produce this effect are greater than or equal to 20 mg/kg (Beaudouin, 1974; Ferm et al., 1971; Ferm & Carpenter, 1968). In humans, arsenic can cross the placental barrier. Some studies indicate an accumulation of arsenic in infant tissues with age and a more sensitivity of infants to arsenic, with long term brain damage (Barlow & Sullivan, 1982). There is however, little evidence concerning effects of arsenic in pregnancy (Barlow & Sullivan, 1982). Spontaneous abortions and low weight babies reported in people working or living close to a smelter can be linked to arsenic but also to many other toxic compounds (Nordström, 1979). In many experimental studies on reproductive effects of inorganic arsenical compounds, maternal and developmental toxicity occur at the same dose administered. But various evidence from the basic science literature indicates that developmental toxicity is not secondary to maternal toxicity (Golub, 1994).
7.5 Mutagenicity
There is limited evidence that arsenic may be mutagenic in people exposed to inorganic arsenic compounds (drugs, occupational exposure) with effects persisting for many years (Barlow & Sullivan, 1982). Inorganic arsenic compounds can produce detectable cytogenetic changes, in vivo, in human somatic cells (Hantson et al., 1996); but theses changes, seen with sister chromatid exchanges (SCEs), occur at very high doses.
7.6 Interactions
Phosphorus (P) Arsenic can compete with phosphorus in the oxidative phosphorylation process and this can lead to the replacement of phosphorus in the bone, where it may remain for many years (Arena & Drew, 1986; Ellenhorn & Barceloux, 1988). Selenium (Se) It has been suggested that arsenic could form complexes with GSH-peroxidase, Se-dependent enzyme, thereby depleting body stores of enzymatically active selenium.
8. TOXICOLOGICAL AND BIOMEDICAL INVESTIGATIONS

Arsenic (PIM G042) Página 20 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
8.1 Material sampling plan
8.1.1 Sampling and specimen collection
8.1.1.1 Toxicological analyses
8.1.1.2 Biomedical analyses
8.1.1.3 Arterial blood gas analysis
8.1.1.4 Haematological analyses
8.1.1.5 Other (unspecified) analyses
8.1.2 Storage of laboratory samples and specimens
8.1.2.1 Toxicological analyses
8.1.2.2 Biomedical analyses
8.1.2.3 Arterial blood gas analysis
8.1.2.4 Haematological analyses
8.1.2.5 Other (unspecified) analyses
8.1.3 Transport of laboratory samples and specimens
8.1.3.1 Toxicological analyses
8.1.3.2 Biomedical analyses
8.1.3.3 Arterial blood gas analysis
8.1.3.4 Haematological analyses
8.1.3.5 Other (unspecified) analyses
8.2 Toxicological analyses and their interpretation
8.2.1 Tests on toxic ingredient(s) of material
8.2.1.1 Simple qualitative test(s)
8.2.1.2 Advanced qualitative confirmation test(s)
8.2.1.3 Simple quantitative method(s)
8.2.1.4 Advanced quantitative method(s)
8.2.2 Tests for biological specimens
8.2.2.1 Simple qualitative test(s)
8.2.2.2 Advanced qualitative confirmation test(s)

Arsenic (PIM G042) Página 21 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
8.2.2.3 Simple quantitative method(s)
8.2.2.4 Advanced quantitative method(s)
8.2.2.5 Other dedicated method(s)
8.2.3 Interpretation of toxicological analyses
8.3 Biomedical investigations and their interpretation
8.3.1 Biochemical analysis
8.3.1.1 Blood, plasma or serum
8.3.1.2 Urine
8.3.1.3 Other fluids
8.3.2 Arterial blood gas analyses
8.3.3 Haematological analyses
8.3.4 Interpretation of biomedical investigations
8.4 Other biomedical (diagnostic) investigations and their interpretation
In acute, massive ingestions, barium like opacities may be demonstrated by abdominal X-ray (Adelson et al., 1961; Gousios & Adelson, 1959; Gray et al., 1989; Hilfer & Mandel, 1962; Levin-Scherz et al., 1987; Lee et al., 1995).
8.5 Overall interpretation of all toxicological analyses and toxicological investigations
Interpretation: The use of urinary arsenic excretion as the sole determinant for chelation therapy may lead to inaccurate assessment of tissue burden and over estimate the risk of toxicity. Less toxic, water soluble forms of arsenic such as organoarsenicals or sodium arsenate are excreted rapidly after acute exposure and urinary arsenic levels obtained shortly after exposure may not accurately reflect tissue or target organ levels (Hayes, 1982; Monier-Williams, 1949; Schoolmeester & White, 1980; Schroeder & Balassa, 1966).
Recent ingestion of seafood rich in organic arsenic may lead to false positive diagnosis of arsenic poisoning, especially if no speciation is done of the type of arsenic measured in urine. Biomedical analysis A slightly increased liver enzymatic activity is observed in severe acute poisoning.

Arsenic (PIM G042) Página 22 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
Fluid losses are often accompanied by electrolyte disturbances. Acid-base disturbances may occur. Oliguria, anuria are observed in severe cases. Monitor renal functions (serum creatinine). Other investigations As inorganic arsenic compounds are radio-opaque, an X-ray of the abdomen will be useful, in all cases of acute inorganic arsenic ingestion.
9. CLINICAL EFFECTS
9.1 Acute poisoning
9.1.1 Ingestion
Symptoms begin usually within the first hour following ingestion. Gastrointestinal disturbances are the main clinical effects: vomiting, oesophageal and abdominal pain, bloody rice water diarrhoea (Quatrehomme, 1992). Metallic taste and garlic odour of breath or faeces can be noted (Lee, 1995). After an apparent remission (1 to 2 days), several organs are affected by the systemic action of inorganic arsenic, resulting in the following delayed effects: Cardiovascular: hypotension, tachycardia, dysrrhythmia, prolonged QT interval, torsades de pointes, myocarditis, cardiovascular failure and coma; Renal: albuminuria, haematuria, oliguria, anuria, renal failure; Hepatic: toxic hepatitis; Cutaneous: various eruptions; Neurological: hyperpyrexia, toxic delirium, convulsions, tremor, coma; Respiratory: pulmonary oedema, ARDS, respiratory failure. If patient survives the cardiovascular failure, hepatic and renal impairment and central and peripheral nervous system damage may develop (Armstrong, 1984; Goldsmith, 1980; Bolliger et al.,1992; Greenberg et al., 1979; Ellenhorn, 1997). After a long convalescence, sequelae may be observed: Sensorimotor polyneuropathy, usually symmetrical, may occur one to three weeks after the beginning of the intoxication (Campbell, 1989; Donofrio, 1987; Bansal, 1991; Wesbey, 1981). The encephalopathy may be stated (Fincher & Koerker, 1987) Mee's lines i.e. transverse white striae on the nails appear several weeks after absorption (Aldrich, 1904; Mees, 1919; Sass, 1993).

Arsenic (PIM G042) Página 23 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
9.1.2 Inhalation
Irritation of the respiratory tract: dyspnoea, accompanied by cough, thoracic pain during inspiration (Hathaway et al., 1991).
9.1.3 Skin exposure
Following accidental splashing of an arsenic acid solution, local effects (pain and swelling at the site of contact) were noted, followed several hours later by gastrointestinal disturbances: nausea, vomiting, diarrhoea, stomach pains. In the next days, neurological effects and peripheral neuropathy were reported (Garb & Hine, 1977).
9.1.4 Eye contact
Ocular irritation: eyelids dermatitis, conjunctivitis. Corneal necrosis has been observed with exposition to arsenic trichloride: AsCl3 (Grant, 1986).
9.1.5 Parenteral exposure
No data available.
9.1.6 Other
No data available.
9.2 Chronic poisoning
9.2.1 Ingestion
During chronic ingestion of inorganic arsenic compounds, the following effects are noted: gastrointestinal disturbances: nausea, vomiting, diarrhoea, metallic taste; Sensorimotor symmetrical polyneuropathy, polyneuritis, psychiatric disturbances are the more frequent effects. Haematological effects: anaemia; aplastic anaemia was reported in one case (Kjeldsberg & Ward, 1972). More rarely, cardiovascular, renal, hepatic problems occur. Cutaneous signs: hyperkeratosis, melanosis, Mee's lines.
9.2.2 Inhalation
Local effects on mucous membranes - irritation, perforation of the nasal septum are noted. Systemic effects are rarely observed.
Arsenic (PIM G042) Página 24 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
9.2.3 Skin exposure
Local irritation signs are observed with chronic cutaneous contact: ulcerations, vesiculation (Zaloga et al., 1985). Inorganic arsenic compounds may act as contact allergens (ATSDR, 1989).
9.2.4 Eye contact
Dermatitis of the eyelids and conjunctivitis have been reported in the literature.
9.2.5 Parenteral exposure
No data available.
9.2.6 Other
No data available.
9.3 Course, prognosis, cause of death
After absorption, arsenic may cause multi-organ failure. The primary target organs initially are gastrointestinal tract, the heart, brain and kidneys. The skin, bone marrow and peripheral nervous system may be affected. In case of severe acute poisoning by ingestion, gastrointestinal disturbances begin within the first 20 to 30 minutes and are marked: diffuse capillary damage results in haemorrhagic gastroenteritis. Nausea, vomiting abdominal pain and watery, profuse diarrhoea is noted; sometimes the term "arsenical cholera" has been used. Intense thirst, retrosternal pain, dysphagia, marked dyspnea, fluid- electrolyte disturbances, oligo-anuria, delirium are observed. In severe cases, extensive tissue third spacing of fluids combined with fluid loss from gastroenteritis may lead to hypotension, cardiovascular failure and death. If prompt treatment is not initiated, death may occur within 12 to 24 hours and the mortality rate is high, 50 to 75% (Evreux et al., 1968, Gosselin et al., 1984) Survivors of severe poisoning (after a vigorous fluid replacement therapy) may develop a peripheral neuropathy and skin lesions, which were only seen formerly in chronic poisoning (Gosselin et al., 1984). Recovery from arsenical neuropathy is generally poor, even after treatment with chelating agents (Kew et al., 1993; Murphy et al., 1981).
9.4 Systematic description of clinical effects
9.4.1 Cardiovascular
Cardiac effects Acute poisoning:

Arsenic (PIM G042) Página 25 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
Cardiotoxicity may manifest itself as non-specific ECG changes: QT prolongation, ST depression, or T wave inversion. Minor ECG changes may remain for as long as 6 to 8 weeks. Cases of torsade de pointes, ventricular tachycardia, ventricular fibrillation, asystole have been reported by Beckman et al., 1991; Campbell & Alvarez, 1989; Goldsmith, 1980; 1990; Levin-Scherz et al., 1987; Poklis & Saady, 1990, Schoolmeester & White, 1980; St-Petery et al., 1970; Wang & Mazzia, 1969). Death may occur secondary to dysrrhythmias. Chronic poisoning: An increase of the frequency of mortality by cardiovascular diseases has been observed in workers exposed to As2O3 in a copper smelter (Axelson et al., 1978). Myocardial infarction and arterial thickening has been observed in children exposed to inorganic arsenic via drinking water (Rosenberg, 1974; Zaldivar, 1974). Toxic myocardial action of inorganic arsenic was reported in vineyard workers, exposed chronically to arsenic pesticides with electrocardiographic abnormalities: QT prolongation, T wave depression or inversion (Haguenoer & Furon, 1982). Interstial myocarditis resulting in fatal ventricular arrhythmias has been reported after chronic exposure to arsenic (Hall & Robertson, 1990). Vascular effects Acute poisoning The toxic action of arsenic on blood vessels result in fluid leakage into the intestinal space with subsequent intravascular volume depletion and severe hypotension (Hall & Robertson, 1990). Chronic exposure Raynaud's syndrome was observed in Chile, infants and children showing more severe symptoms than adults (Rosenberg, 1974; Zaldivar, 1980) exposed to high inorganic arsenic concentrations in drinking water.
In vineyard workers, peripheral vascular disturbances have been reported: endoangiitis, gangrene of the extremities, atrophic acrodermatitis, peripheral circulatory troubles (Ishinishi et al., 1986; Grobe, 1976). Black-foot disease, as described in Taiwan, is a gangrene of the extremities, due to peripheral vascular disorders (Tseng, 1977), prevalence of the disease being 8.9 per 1000. Hypertension has been linked to long-term arsenic exposure (Chen et al., 1995) and increased prevalence of cerebrovascular disease, particularly cerebral infarction was observed

Arsenic (PIM G042) Página 26 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
9.4.2 Respiratory
Local effects in acute poisoning by inhalation are irritation of the respiratory tract: rhinitis, pharyngitis, laryngitis and tracheobronchitis, with cough, pain during inspiration and dyspnoea (Hathaway, 1991). Massive inhalation and swallowing of substantial amounts of crude arsenic dust (more than 80% As2O3) has been responsible for the death, within several hours, of a worker. At autopsy, trachea and main bronchi showed widespread mucosal and submucosal haemorrhages and there was intense visceral congestion (Gerhardsson et al., 1988). Acute respiratory failure occurs infrequently in acute arsenic poisoning and is usually due to the muscle weakness. Pulmonary oedema, either noncardiogenic from capillary leaking, or cardiogenic from myocardial depression may occur. Adult respiratory distress syndrome (ARDS) has been reported (Bolliger, 1992; Greenberg, 1979; Schoolmeester & White, 1980; Zaloga et al., 1985).
9.4.3 Neurological
9.4.3.1 Central Nervous System (CNS)
Neurological symptoms range from vertigo or altered mental status to seizures or toxic encephalopathy (Campbell & Alvarez, 1989; Poklis & Saady, 1990; Schoolmeester & White, 1980). Encephalopathy has been observed in acute or subacute poisoning by ingestion contaminated drinking water from well (Armstrong, 1984) and deliberated ingestion of arsenic trioxide (Danan et al., 1985).
In chronic poisoning encephalopathy was observed after ingestion (Freeman & Couch, 1978), inhalation of fumes during a smelting process of antimony ore (Beckett et al., 1986) or from wood treated with ammoniated copper arsenate (Morton & Caron, 1989).
9.4.3.2 Peripheral nervous system
The most common long-term sequela associated with arsenic poisoning, occurring usually 7 to 14 days after ingestion, is a polyneuropathy, which is the result of a direct toxic effect leading to damage of the peripheral nerve bodies (Bansal et al., 1991; Campbell & Alvarez, 1989; Donofrio et al.,

Arsenic (PIM G042) Página 27 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
1978; Wesbey & Kunis, 1981). Peripheral neuropathy occur in acute or in chronic poisonings. It is frequently a progressive ascending and painful polyneuritis, involving both sensory and motor neurons. It is due to a demyelimination of axons. Paresthesias, numbness, tingling sensations, pain in extremities. Muscular weakness is commonly observed. Electromyographic disturbances are observed (Hindmarsh et al., 1977) and the reduction of nerve conduction velocity, without symptoms, has been noted (Feldman et al., 1979). In severe poisoning, motor palsy may predominate.
9.4.3.3 Autonomic nervous system
No data available.
9.4.3.4 Skeletal and smooth muscle
In a case of acute massive arsenic poisoning a severe rhabdomyolysis was observed (Fernandez-Sola et al., 1991).
9.4.4 Gastrointestinal
Gastrointestinal disturbances, such as severe gastritis or gastroenteritis are the first and prominent manifestations of acute toxicity by ingestion. These gastrointestinal effects can lead to a choleriform syndrome ("arsenical cholera").
Digestive lesions are not due to a corrosive effect on the gastrointestinal mucosa, but are the consequence of vascular damage of the mucosa with subsequent fluid loss. Thus, the first symptoms may be delayed for several hours. Symptoms are the following: nausea, vomiting, severe gastroenteric pain, sensation of burning in the mouth and thorax, profuse and sometimes bloody diarrhoea, dehydration. If fluid losses are important, the clinical course may be cardiovascular collapse, shock and death. (Quatrehomme, 1992, Moore, 1994) Stools and emesis may have a garlic like odour. In cases of poisoning by inhalation, these gastrointestinal effects are delayed later and less prominent than after ingestion. During chronic occupational exposure, gastrointestinal disturbances are not common.
9.4.5 Hepatic

Arsenic (PIM G042) Página 28 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
Patients may develop hepatomegaly, jaundice, portal hypertension or pancreatitis caused by the direct effect of arsenic. However, Labadie et al. (1990) suggested that arsenic induced hepatic injury is caused by vascular and not hepatocellular damage. In chronic occupational exposures, hepatomegaly with jaundice may be observed, evolving in some cases toward cirrhosis, as seen in vineyard workers (Haguenoer & Furon, 1982) or in copper smelter workers (Axelson et al., 1978). Jaundice, with sometimes ascites, has been described after prolonged arsenical medication (Haguenoer & Furon, 1982; Ishinishi et al., 1986). Non-cirrhotic portal hypertension has been observed in chronic arsenic intake (Guha Mazumdar & Das Gupta, 1991; Nevens et al., 1990). Hepatic angiosarcoma and hepatocellular carcinomata have been reported (Lander et al., 1975; Regelson et al., 1968; Roth, 1957).
9.4.6 Urinary
9.4.6.1 Renal
Renal failure is caused by vasodilatation leading to increased glomerular filtration and capillary permeability. The resulting protein leakage may cause acute tubular necrosis or diffuse interstitial fibrosis (Cullen et al., 1995). Acute renal tubular necrosis and also cortical necrosis (Gerhardt et al., 1978) have been reported in severe acute poisoning (ATSDR, 1989). Tubulo-interstitial nephritis has been reported in chronic poisoning (Prasad & Rossi, 1995).
9.4.6.2 Other
No data available.
9.4.7 Endocrine and reproductive systems
9.4.7.1 Endocrine system
Chronic oral exposure to inorganic arsenic has been linked to the induction of diabetes mellitus (Lai et al., 1994).
9.4.7.2 Reproductive system

Arsenic (PIM G042) Página 29 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
See 7.4 Teratogenicity
9.4.8 Dermatological
In acute poisoning, melanosis, hyperpigmentation and exfoliative dermatitis have been described, but dermatologic effects are mainly seen after chronic ingestion or inhalation exposure (Zaloga et al, 1985; Schoolmeester & White, 1980;) Chronic local effects include local irritation - erythema, painful ulcerations, dermatitis (neck, face, eyelids, forearms, hands), vesiculation (Zaloga et al., 1985). Skin lesions, occurring in environmentally, medically or occupationally exposed populations are frequently observed:
melanosis, generally seen on eyelids, temples, neck, nipples, axillae and, in severe cases, on chest, back and abdomen (Ishinishi et al., 1986; ATSDR, 1989); sometimes accompanied by punctiform leucoderma ("raindrop" pigmentation). hyperkeratosis, commonly seen on the palms and soles, either as warts or diffuse plaque and characterised by thickening of corneal layer (Sass et al., 1993). other skin lesions may evolve to a Bowen's disease (Haguenoer & Furon, 1982). Skin lesions are now rare in industry: only one case of hyperkeratosis was described during the last decades (Frost, 1967). However, skin alterations, skin malignant tumors and Bowen's disease have been found frequent among wine growers, during the 1960-1977 period (Lüchtrath, 1983).
9.4.9 Eye, ears, nose, throat: local effects
Dermatitis of the eyelids and conjunctivitis characterised by redness, swelling and pain is seen in acute or chronic exposure by inhalation. No valid evidence of injury of the optic nerve by inorganic arsenic can be found in the literature (Grant, 1986). Irritation of the nose and pharynx, causing acute or chronic rhino-pharyngo-tracheo-bronchitis has been observed (Buchanan, 1962). Perforation of the nasal septum has been observed in arsenic-exposed workers (Ishinishi et al., 1986).
9.4.10 Haematological
Arsenic (PIM G042) Página 30 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
<9.4.10>Bone marrow depression/failure and haemolysis may develop. The peripheral haematologic abnormalities associated with arsenic intoxication include leucopenia, anemia and thrombocytopenia (Kyle & Pease, 1965; Lerman et al., 1980; Selzer & Ancel, 1983; Rezuke et al., 1991; Terada et al., 1962; Van Tongeren et al., 1965; Westhoff et al., 1975). The anemia, usually associated with arsenic, has normocytic indices (Kyle & Pease, 1965; Terada et al., 1962). Megaloblastic anaemia has been reported rarely (Lerman et al., 1980; Westhoff et al., 1975).
Macrocytosis without anaemia has been reported by Heaven et al., 1994. Severe dyserythropoiesis has been reported after ingestion of kelp supplements (Pye et al., 1992).
9.4.11 Immunological
<9.4.11>An immunosuppressive effect has been elicited on mice exposed to sodium arsenite at doses of 0,5 ppm to 10 ppm via drinking water (Blakely, 1980). No data available in humans.
9.2.12 Metabolic
9.4.12.1 Acid-base disturbances
<9.4.12.1>No data available.
9.4.12.2 Fluid and electrolyte disturbances
<9.4.12.2>In acute poisoning by ingestion, fluid losses are severe and are followed by electrolyte disturbances.
9.4.12.3 Others
<9.4.12.3>Hyperthermia can be seen in the acute phase of the intoxication.
9.4.13 Allergic reactions
<9.4.13>Contact dermatitis have been observed in workers exposed to As2O3 (Ishinishi et al., 1986). Positive dermal patch tests have been observed in workers (ATSDR, 1989; Haguenoer & Furon, 1982).

Arsenic (PIM G042) Página 31 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
9.4.14 Other clinical effects
<9.4.14>In chronic exposure, the presence of white striae in fingernails, i.e. Mee's lines is frequently observed. Cases of alopecia would have been observed (Haguenoer & Furon, 1982). Breath, perspiration, and stools of poisoned patients intoxicated may have a garlic like odour.
9.4.15 Special risks
<9.4.15>Pregnancy Inorganic arsenic crosses the placental barrier. A case of neonatal death has been reported, following acute maternal intoxication (Lugo et al., 1969). Breast-feeding Arsenic can be present in human milk (WHO, 1989).
9.5 Others
No data available.
9.6 Summary
10. MANAGEMENT
10.1 General principles
After ingestion, aggressive decontamination by gastric lavage is recommended. Activated charcoal should be left in the stomach. Due to the toxic action of inorganic arsenic on the gastrointestinal tract in acute poisoning, and the subsequent fluid losses, special care to the fluid-electrolyte balance is required to prevent cardiovascular toxicity (hypovolemia, arrhythmias, cardiogenic shock). Admission of the patient into the intensive care unit of the hospital is therefore mandatory in order to allow close monitoring of vital signs. Antidote treatment with BAL or DMSA or DMSP should be initiated as soon as the diagnosis is reasonably established.
10.2 Life supportive procedures and symptomatic treatment In case of hypotension, place patient in Trendelenburg position and administer IV fluids. If the response is inadequate, administer dopamine or norepinephrine (levarterenol) at the dosage required (See IPCS-INTOX Treatment Guide on shock and hypotension).

Arsenic (PIM G042) Página 32 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
If gastrointestinal hemorrhage occurs, blood products may be necessary. Arrhythmias, may be controlled by standard measures. Morphine may be necessary to control abdominal pain.
10.3 Decontamination
Ingestion Aggressive decontamination with gastric lavage is recommended. Prior control of convulsions and protection of airway is required. Activated charcoal, has been suggested, although its efficacy has not been proven. Cathartics do not seem useful. Whole bowel irrigation may be useful if arsenic is visible using abdominal X-ray (Mahieu et al., 1987; Lee et al., 1995).
Skin If material has been spilled on the skin, immediately remove the patient from the source of contamination, remove all contaminated clothing, and wash affected areas with soap and water (IPCS, 1992). Eye If the material is in the eyes, flush with clean water for at least 15 minutes (IPCS, 1992).
10.4 Enhanced elimination
Haemodialysis may enhance elimination of free inorganic arsenic or arsenic-BAL chelate (Mahieu et al., 1987; Winchester, 1977). Especially in cases of early anuria, haemodialysis is an effective arsenic elimination method (Mathieu et al., 1992). If a combination with chelator therapy is chosen, then BAL should be used because it has been shown that arsenic-BAL complexe cross dialyser membranes (Varizi et al., 1980), while for instance arsenic-DMSA complexes do not pass the dialyser membrane (Sheabar et al., 1989). But its use has been recommended essentially in situations of concomitant renal failure (Vaziri, 1980).
10.5 Antidote treatment
10.5.1 Adults

Arsenic (PIM G042) Página 33 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
<10.5.1>Dimercaprol (BAL): 3 to 5 mg/kg intramuscularly every 4 hours for 2 days, then every 12 hours for 7 to 10 days until recovery or until oral therapy can be started (Gorby, 1988). Caution must be taken to avoid decreased urine pH, which may result in dissociation of the BAL-arsenic complex, increasing the risk of renal failure (Poklis & Sandy, 1990; Reynolds, 1996). Urine alkalization reduces the risk of renal failure and also promotes the excretion of the BAL-arsenic complex (Reynolds, 1996).
BAL has many side effects a.o. painful injection, nausea, vomiting, chest- and abdominal pain, headaches, fever, hypertension, central nervous system depression, and seizures. Peak side effects are noted 10 to 30 minutes after injection and usually subside in 30 to 50 minutes. It is contraindicated in patients with renal or hepatic impairment, pregnant patients, and in patients with glucose-6-phosphate dehydrogenase (G6PD) deficiency (Schoolmeester & White, 1980). Besides its many side effects, it has been suggested that the lipophilic BAL could serve as a carrier for arsenic across the blood-brain barrier. Some authors indeed found in the brain of the rabbits treated with BAL higher arsenic concentrations than in the control animals (Aposhian, 1984; Kreppel et al., 1990). However Tsutsumi et al., (1983) found the arsenic content in the brain following BAL treatment unchanged, while Graziano et al. (1978) found the arsenic concentration in the brain even decreased, compared to controls. D-Penicillamine: 25 mg/kg four times per day for a total of 5 days with a maximum of 2 g/day. Although it has been advocated for the treatment of As, based on anecdotal case reports, Kreppel et al. (1989, 1990) using a controlled experimental model, demonstrated that it was ineffective in preventing the lethal action of arsenic. The findings of Aposhian et al. (1983) confirmed this experiment. Also many side effects are reported: Hypersensitivity reactions, leucopenia, eosinophilia, thrombocytopenia, optic neuritis, and nephrotoxicity. Dimercaptosuccinic acid (DMSA): 10 mg/kg every 8 hours for 5 days. Side effects are rare, but include reversible

Arsenic (PIM G042) Página 34 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
elevation in serum transaminases, gastrointestinal symptoms, leucopenia, and hypersensitivity. DMSA is 20 to 30 times less toxic than BAL and can be given to patients with G6PD deficiency without causing haemolysis. 2,3-dimercaptopropanesulphonate (DMPS): 5 mg/kg every 4 hours intravenously for 24 hours with transfer to oral DMPS 400 mg every four hours.
It has been reported to be effective in a severe acute arsenic poisoning (Moore et al., 1994). Because of its relatively few side-effects and proven efficacy in the treatment of arsenic poisoning in animal studies, DMPS may be the preferred agent as an oral chelator for arsenic poisoning (Cullen et al., 1995). Regardless of the chelator that is chosen, therapy can be terminated if the arsenic level is < 5 µg/L after 5 days (Kreppel et al., 1990). Drastic antidote therapy, for instance by BAL, could be limited by measuring the extent of methylation of arsenic (the natural detoxifying mechanism). This can be performed by the determination of monomethylarsenic acid (MMA) and dimethylarsenic acid (DMA) in urine (Mahieu et al., 1981).
10.5.2 Children
<10.5.2>BAL: 3 mg/kg intramuscularly every 4 hours for 2 days, then every 12 hours for 7 to 10 days until recovery or until oral therapy can be started. d-Penicillamine: 25 mg/kg four times per day for a total of 5 days with a maximum of 1 g/day. DMSA: 10 mg/kg or 350 mg/m2 every 8 hours for 5 days. Because of its relatively low in side-effects and proven effective in the treatment of arsenic poisoning in animal studies, DMSA may be the preferred agent as an oral chelator for arsenic poisoning. (Cullen et al., 1995). Regardless of the chelator that is chosen, therapy can be terminated if the arsenic level is < 5 µg/L after

Arsenic (PIM G042) Página 35 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
5 days (Kreppel et al., 1990).
10.6 Management discussion
BAL (re)distribution of arsenic to the brain has to be evaluated. In the mean time the use of the water-soluble dithiols, like DMSA or DMPS, should be preferred as antidotes for arsenic when available. Another advantage of these two drugs is the fact that they cause fewer side-effects.
11. ILLUSTRATIVE CASES
11.1 Case reports from literature
Beer epidemic of 1900 A large outbreak of poisoning by inorganic arsenic, among beer drinkers, was detected in the north of England by the mid of 1900. Among the sources of arsenic contributing to the contamination of beer, we can note (Abbot, 1984): * Sulfuric acid, used to produce glucose for fermentation from various starches and produced from purification of Spanish pyrites, with a high white arsenic (As2O3) content. * Malt, dried or kilned over local gas coke. Recording of deaths among beer-drinkers occurred at mid 1900. Deaths were ascribed to alcoholism and nervous system disturbances (peripheral or multiple neuritis). Inorganic arsenic (contaminated sulfuric acid) as a cause of death was pointed out several months later and the amount of arsenic used in the preparation of beer was estimated to several tons. The total number of cases, recorded in several locations, was estimated to about 6000 and the number of death to about 70. Until the discovery of the other source of arsenic (contaminated malt), once again the diagnosis of arsenic poisoning was difficult to establish based on the symptoms only and was ascribed to alcoholic neuritis. Mass poisoning by sodium arsenite This episode of criminal mass poisoning by inorganic arsenic occurred in Argentina in 1987 (Roses et al., 1991). An acaricide containing an aqueous solution of 45% weight volume of sodium arsenite was intentionally poured over meat, in a butcher's shop. Of the 718 subjects who had purchased contaminated meat, 207 were tested for urine arsenic i.e. symptomatic patients and non symptomatic individuals requesting to have an urinary analysis. No treatment was given to patients having urine arsenic concentration below 75 µg/dL. Patients of other groups (As urine: 76-500 µg/dL and As urine > 500 µg/dL) were treated with BAL. Symptomatology occurred at all levels and abdominal pain was recorded at the lowest urine arsenic levels while vomiting, nausea and
Arsenic (PIM G042) Página 36 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
systemic symptoms tended to increase at higher levels. Follow up of treated patients showed that all were asymptomatic one month after treatment and subsequently an early detection was useful.
Acute oral arsenic trioxide intoxication (Mahieu et al., 1987) Thirty minutes after having voluntarily ingested ten small bags of 1 g of arsenic trioxide (for veterinary purpose) a 27 years old woman was presenting gastrointestinal disturbances: epigastric pain, nausea, vomiting, dysphagia, metallic taste. Three hours later, she was admitted to a local hospital where gastric lavage and intestinal washout (Mannitol 20%) were done. Diuresis (Mannitol 20%) was initiated. BAL (250 mg IM) was administered. Thirteen hours post-ingestion, she was transferred, somnolent, to an university hospital (BP:90/60 mng/Hg) hypovolemia, oliguria). Opacities in digestive bowel were detected with an abdominal X-ray. Main therapeutic measures were the following: * Volume replacement, under the control of a central venous catheter (albumin, plasma) * Large osmotic diuresis (mannitol 20%) * "Intestinal washout" with Mannitol 20% and enema * Duodenal probe, under gastroscopy (aspiration of duodenal content and bile) * Extra-corporeal dialysis (haemodialysis with hemoperfusion): two periods (4 h) at the first and the second day of hospitalization. * BAL treatment, until the 8th day. * Sulfo-adenosyl-L-methionine (Samyr 7), a methyl group donor, given after 48 h by IV, IM and introduodenal routes, with simultaneous administration of vitamin B12 for the last two routes. Evolution of the patient was favourable. * Digestive symptomatology has persisted during 3 days. * At day 3, a diffuse cutaneous erythema was noticed, with a more or less pronounced swelling of the face. * At day 4, hepatalgia with a light cytolysis was noticed. Patient was discharged from the intensive care at day 10. Subacute arsenic poisoning (Kew et al., 1993) A 35-year-old Asian man presented with a three month history of progressive weakness of his hands and legs associated with distal sensory disturbances. The patient had become aware of the symptom six weeks after an Indian ethnic practitioner had started treating him for atopic eczema. On examination Mees lines were present in the finger nails and there was hyperkeratosis of the soles of the feet. Symmetrical wasting and weakness was present in the upper and lower limbs and all tendon reflexes were absent. Cutaneous sensation was impaired
Arsenic (PIM G042) Página 37 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
in a glove and stocking distribution. He could not stand from a sitting position without using his arms and walked
with difficulty unsupported. Electromyography suggested a peripheral sensoria-motor neuropathy. The presence of an increased urinary concentration of inorganic arsenic (63 µg/L; normal < 2 µg/L) and a hair arsenic concentration of 20 µg/g on x-ray fluorescence spectrometry (normal < 1 µg/g) confirmed arsenic intoxication. Chelation therapy with DMPS 100 mg daily for three weeks and later DMSA 400 mg three times daily for two weeks was given without objective improvement in muscle strength. Two years after the onset of symptoms the patient was still unable to return to work.
12. ADDITIONAL INFORMATION
12.1 Specific preventive measures
No relevant information.
12.2 Other
Other useful references: Environmental Protection Agency (EPA), Jacobson-Kram D, Mushak P, Piscator M, Sivulka DJ, Chu M, Gibb HJ, Thorslund TW, Crump KS (1984) Health assessment document for inorganic arsenic. Final report EPA 600/8-83-021F. Environmental Protection Agency, Research Triangle Park.
13. REFERENCES
<13>Abbott H (1984) Fool's gold and the arsenic in beer epidemic of 1900. Chem Ind 13:481-484. Adelson L, Georg R, Mandel A (1961) Acute arsenic intoxication shown by roentgenograms. Arch. Intern Med 107:401-404. Agency for Toxic Substances and Disease Registry (ATSDR) (1998) Toxicological profile for arsenic. ATSDR, Atlanta, Georgia, 349 pp. Agency for Toxic Substances and Disease Registry (ATSDR) (1989) Toxicological profile for arsenic. ATSDR, Atlanta, Georgia, 125 pp. Aldrich CJ (1904) Leuconychia striata arsenicalis transversus: with report of three cases. Am J Med Sci 127:702-709. American Conference of Govermental Industrial Hygienists (ACGIH) (1995) 1995-1996 Threshold Limit Values (TLVsTM) for Chemical Substances and Physical Agents and Biological Exposure Indices (BEIsTM). Second printing. American Conference of Governmental Industrial Hygienists, Cincinnati, OH, 139 pp.

Arsenic (PIM G042) Página 38 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
Aposhian HV (1983) DMSA and DMPS-water soluble antidotes for heavy metal poisonings. Ann Rev Pharmacol Toxicol 23:193-215. Arena JM, Drew RH, Eds (1986) Poisoning. Fifth edition. Charles C Thomas, Springfield, 1128 pp. Armstrong CW, Stroube RB, Rubio T, Siudyla EA, Miller GB Jr (1984) Outbreak of fatal arsenic poisoning caused by contaminated drinking water. Arch Environ Health 39(4):276-279. Axelson O, Dahlgren E, Jansson CD, Rehnlund SO (1978) Arsenic exposure and mortality: a case-referent study from a Swedish copper smelter. Br J Ind Med 35(1):8-15. Bansal SK, Haldar N, Dhang UK (1991) Phrenic neuropathy in arsenic poisoning. Int J Dermatol 30:304-306. Barlow SM, Sullivan FM (1982) Arsenic and its compounds in reproductive hazards of industrial chemicals. Academic Press, London pp. 62-82. Beaudouin AR (1974) Teratogenicity of sodium arsenate in rats. Teratology 10(2):153-158. Beckett WS, Moore JL, Keogh JP, Bleecker ML (1986) Acute encephalopathy due to occupational exposure to arsenic. Br J Ind Med 43(1):66-67.
Beckman KJ, Bauman JL, Pimental PA, Garrard C, Hariman RJ (1991) Arsenic-induced torsade de pointes. Critical Care Med 19(2):290-292. Bhumbla DK, Keefer RF (1994) Arsenic mobilization and bioavailability in soils. Adv. Env. Sci Technol 26:51-82. Blakely BR, Sisodia CS, Mukkur TK (1980) The effect of methylmercury, tetraethyl lead and sodium arsenite on the humoral immune response in mice. Toxicol Appl Pharmacol 52:245-254. Bolliger CT, van Zijl P, Louw JA (1992) Multiple organ failure with the adult respiratory distress syndrome in homicidal arsenic poisoning. Respiration 59(1):57-61. Brouwer OF, Onkenhout W, Edelbrock PM, de Kom JFM, de Wolff FA, Peters ACB (1992) Increased neurotoxicity of arsenic in methylenetetrahydrofolate reductase deficiency. Clin Neurol Neurosurg 94(4):307-310. Buchanan WD (1962) Toxicity of arsenic compounds. Elsevier Publishing Co, New York, Buchet JP, Lauwerys R (1985) Study of inorganic arsenic methylation by rat liver in vitro: relevance for the interpretation of observations in man. Arch Toxicol 57(2):125-129.

Arsenic (PIM G042) Página 39 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
Buchet JP, Lauwerys R, Roels H (1981) Urinary excretion of inorganic arsenic and its metabolites after repeated ingestion of sodium metaarsenite by volunteers. Int Arch Occup Environ Health 48(2):111-118. Campbell JP, Alvarez JA (1989) Acute arsenic intoxication. Am Fam Physician 40(6):93-97. Chen CJ, Hsueh YM, Lai MS, Shyu MP, Chen SY, Wu MM, Kuo TL, Tai TY (1995) Increased prevalence of hypertension and long-term arsenic exposure. Hypertension 25(1):53-60. Crecelius EA (1977) Changes in the chemical speciation of arsenic following ingestion by man. Environ Health Perspect 19:147-150. Cullen NM, Wolf LR, St. Clair D (1995) Pediatric arsenic ingestion. Am J Emerg Med 13(4):432-435. Danan M, Conso F, Dally S, Bertaux L, Chouraki L, Balme R (1985) Intoxication par l'anhydride arsénieux. Neuropathie périphérique et altération des fonctions cognitives. Ann Med Int (Paris) 136(6):479-481.
Dickerson OB (1994) Antimony, arsenic and their compounds In Zenz C, Dickerson OB, Horwath EP Jr (Editors) Occupational medicine. Third edition. Mosby-Year Book, Inc. St-Louis, pp. 468-473. Donofrio PD, Wilbourn AJ, Albers JW, Rogers L, Salanga V, Greenberg HS (1987) Acute arsenic intoxication presenting as Guillain-Barré-like syndrome. Muscle Nerve 10(2):114-120. Ellenhorn MJ (1997) Arsenic In Medical toxicology. Diagnosis and treatment of human poisoning. 2nd Ed Elsevier, Baltimore, pp.1538-1543.
Ellenhorn MJ, Barceloux DG (1988) Arsenic In Medical toxicology. Diagnosis and treatment of human poisoning. Elsevier, New York, pp.1012-1016. Evreux JC, Motin J, Roche L, Vincent V (1968) Arsenic et dérivés, In Précis de toxicologie clinique. Masson et Cie (Editeurs), Paris, pp. 249-252. FAO/WHO (1989) Toxicological evaluation of certain food additives and contaminants. Food and Agricultural Organization/World Health Organization Food additive Series 24, Geneva, pp. 155-162. Feldman RG, Niles CA, Kelly-Hayes M, Sax DS, Dixon WJ, Thompson DJ, Landau E (1979) Peripheral neuropathy in arsenic smelter workers. Neurology 29(7):939-944. Ferm VH, Carpenter SJ (1968) Malformations produced by sodium arsenate. J Reprod Fertil 17:199-201.

Arsenic (PIM G042) Página 40 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
Ferm VH, Saxon A, Smith BM (1971) The teratogenic profile of sodium arsenate in the golden hamster. Arch Environ Health 22:557-560. Fernandez-Sola J, Nogue S, Grau JM, Casademont J, Munne P (1991) Acute arsenical myopathy: morphological description. Clin Toxicol 29(1):131-136. Fincher RM, Koerker RM (1987) Long-term survival in acute arsenic encephalopathy. Follow-up using newer measures of electrophysiologic parameters. Am J Med 82(3):549-553. Foa V, Colombi A, Maroni M, Buratti M (1987) Arsenic In Alessio L, Berlin A, Boni M, Roi R (Editors) Biologic indicators for the assessment of human exposure to industrial chemicals. Commission of the European Communities, Luxembourg, pp. 22-41. Freeman JW, Couch JR (1978) Prolonged encephalopathy with arsenic poisoning. Neurology 28(8):853-855.
Frost DV (1967) Arsenicals in biology retrospect and prospect. Federation Proceedings 26(1):194-208. Garb LG, Hine CH (1977) Arsenical neuropathy: residual effects following acute industrial exposure. J.O.M. 19(8):567-568. Gerhardsson L, Dahlgren E, Ericksson A (1988) Fatal arsenic poisoning - A case report. Scand J Work Environ Health 14(2):130-133. Gerhardt R, Hudson J, Rao R, Sobel R (1978) Chronic renal insufficiency from cortical necrosis induced by arsenic poisoning. Arch Intern Med 138:1267-1269. Goldsmith S (1980) Arsenic induced atypical ventricular tachycardia. N Engl J Med 303:1096-1098. Golub MS (1994) Maternal toxicity and the identification of inorganic arsenic as a developmental toxicant. Reprod Toxicol 8(4):283-295. Gorby MS (1988) Arsenic poisoning-Clinical conference. West J Med 149:308-315.
Gosselin RE, Smith RP, Hodge HC (1984) Arsenic In Clinical toxicology of commercial products, 5th edition. Williams and Wilkins, Baltimore, pp.11142-11147. Gousios AG, Adelson L (1959) Electrocardiographic and radiographic findings in acute arsenic poisoning. Am J Med 27:659-663. Grant WM (1986) Toxicology of the eye. 3rd edition. Charles C Thomas, Springfield, 1083 pp. Gray JR, Khalil A, Prior JC (1989) Acute arsenic toxicity. An

Arsenic (PIM G042) Página 41 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
opaque poisoning. J Can Assoc Radiol 40(4):226-227. Graziano JH, Cuccia D, Friedheim E (1978) The pharmacology of 2,3-dimercaptosuccinic acid and its potential use in arsenic poisoning. J Pharmacol Exp Ther 207(3):1051-1055. Greenberg C, Davies S, McGowan T, Schorer A, Drage C (1979) Acute respiratory failure following severe arsenic poisoning. Chest 76:597-598. Grobe JW (1976) Peripheral circulation disorders and acrocyanosis in arsenic-injured viticulturists. Berufs-Dermatogen 24(3):78-84. Guha Mazumdar DN, Das Gupta J (1991) Arsenic and non-cirrhotic portal hypertension [letter; comment]. J Hepat 13(3):376.
Haguenoer JM, Furon D (1982) Arsenic In Toxicologie et hygiène industrielles Tome 2. Les dérivés minéraux, 2ème partie. Technique et documentation, Paris, pp. 183-236. Hall AH, Robertson WO (1990) Arsenic and other heavy metals In Haddad LM, Winchester JF Clinical management of poisoning and drug overdose. Second edition, WB Saunders Company, Philadelphia, pp. 1024-1034. Hamamoto E (1955) [Infant arsenic poisoning by powdered milk]. Jap Med J 1649:2-12. Hantson P, Verellen-Dumoulin C, Libouton JM, Leonard A, Leonard ED, Mahieu P (1996) Sister chromatid exchanges in human peripheral blood lymphocytes after ingestion of high doses of arsenicals. Int Arch Occup Environ Health 68(5):342-344. Harvey SC (1970) Heavy metals In Goodman LS, Gilman A (Editors) The pharmacological basis of therapeutics. Collier - Macmillan, Toronto, pp. 958-965. Hathaway GJ, Proctor NH, Hughes JP et al (1991) Chemical Hazards of the Workplace. 3rd ed. Van Nostrand Reinhold Company, New York, NY. Hayes WJ (1982) Arsenic In Hayes WJ (Editor) Pesticides studied in man. Williams and Wilkins, Baltimore, pp. 41-50. Hazardous Substances Data Bank (HSDB) Arsenic In Tomes Plus7 Databases. Micromedex, Inc., Emglewood, Colorado (Edition expires 31-01-97). Heaven R, Duncan M, Vukelja SJ (1994) Arsenic intoxication presenting with macrocytosis and peripheral neuropathy, without anemia. Acta Haematol 92(3):142-143. Hilfer RJ, Mandel A (1962) Acute arsenic intoxication diagnosed by roentgenograms. Report of a case with survival. N Engl J Med

Arsenic (PIM G042) Página 42 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
266:663-664. Hindmarsch JT, McCurdy RF (1986) Clinical and environmental aspects of arsenic toxicity. Crit Rev Clin Lab Sci 23(4):315-347. Hindmarsh JT, McLetchie OR, Heffernan LPM, Hayne OA, Ellenberger HA, McCurdy RF, Thiebaux HJ (1977) Electromyographic abnormalities in chronic environmental arsenicalism. J Anal Toxicol 1(6):270-276. Integrated Risk Information System (IRIS) Arsenic, inorganic In Tomes Plus7 Databases. Micromedex, Inc., Emglewood, Colorado (Edition expires 31-01-97).
International Agency for Research on Cancer (IARC) (1990) Arsenic and arsenic compounds In IARC Monographs on the evaluation of the carcinogenic risk of chemicals to humans. Volume 23, Some metals and metallic compounds. World Health Organization, Geneva, pp. 39-141. International Programme on Chemical Safety (IPCS) (1992) Health and Safety Guide NE70: Inorganic arsenic compounds other than arsine. World Health Organization, Geneva, 31 pp. Ishinishi N, Tsuchiya K, Vahter M, Fowler BA (1986) Arsenic In Friberg L, Nordberg GE, Vouk VB (Editors). Handbook on the toxicology of metals. Second edition. Volume II: Specific metals. Elsevier, Amsterdam, pp. 43-83. Jolliffe DM, Budd AJ, Gwilt DJ (1991) Massive acute arsenic poisoning. Anaesthesia 46(4):288-290. Kerr HD, Saryan LA (1986) Arsenic content of homeopathic medicines. Clin Toxicol 24(4):451-459. Kew J, Morris C, Aihie A, Fysh R, Jones S, Brooks D (1993) Arsenic and mercury intoxication due to Indian ethnic remedies. Br Med J 306:506-507. Kjeldsberg CR, Ward HP (1972) Leukemia in arsenic poisoning. Ann Intern Med 77(6):935-937. Kreppel H, Reichl FX, Forth W, Fichtl B (1989) Lack of effectiveness of D-penicillamine in experimental arsenic poisoning. Vet Hum Tox 31(1):1-5. Kreppel H, Reichl FX, Szinicz L, Fichtl B, Forth W (1990) Efficacy of various dithiols compounds in acute As2O3 poisoning in mice. Arch Toxicol 64(5):387-392. Kyle RA, Pease GL (1965) Hematologic aspect aspects of arsenic intoxication. N Eng J Med 273(1):18-23. Labadie H, Stoessel P, Callard P, Beaugrand M (1990) Hepatic

Arsenic (PIM G042) Página 43 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
venooclusive disease and perisinusoidal fibrosis secondary to arsenic poisoning. Gastroenterology 99(4):1140-1143. Lai MS, Hsueh YM, Chen CJ, Shyu MP, Chen SY, Kuo TL, Wu MM, Tai TY (1994) Ingested inorganic arsenic and prevalence of diabetes mellitus. Ann J Epidem 139(5):484-492. Lander JJ, Stanley RJ, Sumner HW, Boswell DC, Aach RD (1975) Angiosarcoma of the liver associated with Fowler's solution (potassium arsenite). Gastroenterology 68(6):1582-1586.
Lee DC, Roberts JR, Kelly JJ, Fishman SM (1995) Whole-bowel irrigation as an adjunct in the treatment of radiopaque arsenic. Am J Emerg Med 13(2):244-245. Lerman BB, Ali N, Green D (1980) Megaloblastic dyserythropoietic anemia following arsenic ingestion. Ann Clin Lab Sci 10:515-517. Levin-Scherz JK, Patrick JD, Weber FH, Garabedian C Jr (1987) Acute arsenic ingestion. Ann Emerg Med 16(6):702-704. Lüchtrath H (1983) The consequences of chronic arsenic poisoning among Moselle wine growers. Pathoanatomical investigations of post-mortem examinations performed between 1960 and 1977. J Cancer Res Clin Oncol 105(2):173-182. Lugo G, Cassady G, Palmisano P (1969) Acute maternal arsenic intoxication with neonatal death. Am J Dis Child 117(3):328-330. Mahieu P, Buchet JP, Lauwerys R (1987) Evolution clinique et biologique d'une intoxication orale aiguë par l'anhydride arsénieux et considérations sur l'attitude thérapeutique. J Tox Clin Exp. 7(4):273-278. Mahieu P, Buchet JP, Roels HA, Lauwerys R (1981) The metabolism of arsenic in humans acutely intoxicated by As2O3. Its significance for the duration of BAL therapy. Clin Toxicol 18(9):1067-1075. Mappes R (1977) Versuche Zur Ausscheidung Von Arsen in Urine. Int Arch Occup Environ Health 40(4):267-272. Mathieu D, Mathieu-Nolf M, Germain-Alonso M, Neviere R, Furon D, Wattel F (1992) Massive arsenic poisoning-effect of hemodialysis and dimercaprol on arsenic kinetics. Intensive Care Med 18(1):47-50. McKinney JD (1992) Metabolism and disposition of inorganic arsenic in laboratory animals and humans. Environ Geochem Health 14: 43-48. Mealey J, Brownell GL, Sweet WH (1959) Radioarsenic in plasma, urine, normal tissues, and intracranial neoplasms. Arch Neurol
Arsenic (PIM G042) Página 44 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
Psychiatr 8: 310-320. Mees RA (1919) Nails with arsenical polyneuritis. Nederl T Geneesk 1:391. Molin L, Wester PO (1976) The estimated daily loss of trace elements from normal skin by desquamation. Scand J Clin Lab Invest 36:679-682.
Monier-Williams GW (1949) Arsenic In Trace elements in Foods. John Wiley & Sons Inc, New York, pp. 162-206. Moore DF, O'Callaghan CA, Berlyne G, Ogg CS, Davies HA, House IM, Henry JA (1994) Acute arsenic poisoning: absence of neuropathy after treatment with 2,3-dimercaptopropanesulphonate (DMPS). J Neurol Neurosurg Psychiat 57:1133-1135. Morton WE, Caron GA (1989) Encephalopathy: an uncommon manifestation of workplace arsenic poisoning? Am J Ind Med 15(1):1-5. Murphy MJ, Lyon LW, Taylor JW (1981) Subacute arsenic neuropathy: Clinical and electrophysiological observations. J Neurol Neurosurg Psychiat 44(10):896-900. National Research Council of Canada (NRCC) (1978) Associated committee on scientific criteria for environmental quality subcommittee on heavy metals and other compounds. Effects of arsenic in the Canadian environment. NRCC, Ottawa, 349 pp. Nevens F, Fevery J, Van Steenbergen W, Sciot R, Desmet V, De Groote J (1990) Arsenic and non-cirrhotic portal hypertension. A report of eight cases. J Hepatol 11:80-85. Nordström (1979) S, Beckman L, Nordenson I (1979) Occupational and environmental risks in and around a smelter in northern Sweden. V. Spontaneous abortion among female employees and decreased birth weight in their offspring. Hereditas 90 ( ):291-296. Poklis A, Saady JJ (1990) Arsenic poisoning: acute or chronic? Suicide or murder? Am J Forensic Med Pathol 11(3):226-232. Prasad GVR, Rossi NF (1995) Arsenic intoxication associated with tubulointerstitial nephritis. Am J Kidney Diseases 26(2):373-376. Pye KG, Kelsey SM, House IM, Newland AC (1992) Severe dyserythropoiesis and autoimmune thrombocytopenia associated with ingestion of kelp supplements. Lancet 339(8808):1540. Quatrehomme G, Ricq O, Lapalus P, Jacomet Y, Ollier A (1992) Acute arsenic intoxication: forensic and toxicologic aspects (an observation) J Forensic Sci 37(4):1163-1171. Regelson W, Kim U, Ospina J (1968) Hemangioendothelial sarcoma of liver from chronic arsenic intoxication by Fowler's solution.
Arsenic (PIM G042) Página 45 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
Cancer 21:514-522. Reynolds JEF (Editor) (1996) Martindale. The Extra Pharmacoepia. Thirty-first edition. Royal Pharmaceutical Society, London, pp. 980-981.
Rezuke WN, Anderson C, Pastuszak WT, Conway SR, Firshein SI (1991) Arsenic intoxication presenting as a myelodysplastic syndrome: a case report. Am J Hematol 36(4):291-293. Robinson TJ (1975) Arsenical polyneuropathy due to caustic arsenical paste. Br Med J 19;3(5976):139 Rosenberg HG (1974) Systemic arterial disease and chronic arsenicism in infants. Arch Pathol 97:360. Roses OE, Garcia Fernandez JC, Villaamil EC (1991) Mass poisoning by sodium arsenite. J Toxicol Clin Toxicol 29(2):209-213. Roth F (1957) Tumoren (hemangiendothelioma). Z Krebsforsch 61:468-503. Sass U, Grosshans E, Simonart JM (1993) Chronic arsenicism: criminal poisoning or drug-intoxication? Report of two cases. Dermatology 186(14):303-305. Schoolmeester WL, White DR (1980) Arsenic poisoning. Review article. Southern Med J 73(2):198-208. Schroeder HA, Balassa JJ (1966) Abnormal trace elements in man: arsenic. J Chron Dis 19:85-78. Selzer PM, Ancel MA (1983) Chronic arsenic poisoning masquerading as pernicious anemia. West J Med 139:219-220. Sheabar FZ, Yannai S, Taitelman U (1989) Efficiency of arsenic clearance from human blood in-vitro and from dogs in-vivo by extracorporeal complexing hemodialysis. Pharmacol Toxicol 64(4):329-333. St-Petery J, Gross, C, Victoria BE (1970) Ventricular fibrillation caused by arsenic poisoning. Am J Dis Child 120:367-371. Tam GKH, Charbonneau SM, Bryce F, Pomroy C, Sandi E (1979) Metabolism of inorganic arsenic (74As) in humans following oral ingestion. Toxicol Appl Pharmacol 50:319-322. Tardieu A, avec la collaboration de Roussin Z (1867) Empoisonnement par l'arsenic In Étude médico-légale et clinique sur l'empoisonnement. Baillière JB et Fils, Paris, pp. 316-426. Terada H, Sasagawa T, Saito H, Shirata H, Sekiya T (1962) Chronic arsenical poisoning and hematopoietic organs. Acta Med Biol 9(4):279-292.

Arsenic (PIM G042) Página 46 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
Tseng WP (1977) Effects and dose-response relationships of skin cancer and Blackfoot disease with arsenic. Environ Health Perspect 19:109-119. Tsutsumi S, Kawaguchi M, Ishii Y, Matsumoto Y (1983) Effects of dimercaprol or thioctic acid on the distribution and excretion of Na3
74AsO3 injected subcutaneously in rats. J Toxicol Sci 8:197-203. Vahter M, Concha G, Nermell B, Nillsson R, Dulout F, Natarajan AT (1995) A unique metabolism of inorganic asenic in native Andean women. Eur J Pharmacol Environ Toxicol Pharmacol Section 293(4-5):455-462. Vahter M (1983) Metabolism of arsenic In Fowler BA (Editor) Biological and Environmental effects of arsenic. Elsevier, Amsterdam, pp. 171-198. Vallee BL, Ulmer DD, Wacker WEC (1960) Arsenic toxicology and biochemistry. A.M.A. Arch. Ind. Health 21:132-151. Van Tongeren JHM, Kunst A, Majoor CLH, Schillings PHM (1965) Folic-acid deficiency in chronic poisoning. Lancet 1:784:786. Vaziri ND, Upham T, Barton CH (1980) Haemodialysis clearance of arsenic. Clin Toxicol 17(3):451-456. Wang BC, Mazzia VDB (1969) Arsenic poisoning as an anaesthetic risk. NY State J Med 69:2911-2912. Wesbey G, Kunis A (1981) Arsenical neuropathy. Ill Med J 160(5):396-398. Westhoff DD, Samaha RJ, Barnes A Jr (1975) Arsenic intoxication as a cause of megaloblastic anemia. Blood 45(2):241-246. Winship KA (1984) Toxicity of inorganic arsenic salts. Adverse Drug React Acute Poisoning Rev 3(3):129-160. World Health Organization (WHO) (1996) Guidelines for drinking water quality. Vol 2: Health criteria and other supporting information, Second edition, Geneva, 973 pp. World Health Organization (WHO) (1989) Environmental Health Criteria 18 - Arsenic. World Health Organization, Geneva, 174 pp. World Health Organization (WHO) (1987) Air quality guidelines for Europe. European Series No 23, Copenhagen, WHO Regional Office for Europe, pp. 171-181.
Zaldivar R, Ghai GL (1980) Clinical epidemiological studies on endemic chronic arsenic poisoning in children and adults,

Arsenic (PIM G042) Página 47 de 47
http://www.inchem.org/documents/pims/chemical/pimg042.htm 29/01/02
including observations on children with high-intake and low-intake of dietary arsenic. Zentrabl Baktoriol 170(5):409-421. Zaldivar R (1974) Arsenic contamination of drinking water and foodstuffs causing endemic chronic poisoning. Beitr Path 151:384-400. Zaloga GP, Deal J, Spurling T, Richter J, Chernow B (1985) Case report: unusual manifestations of arsenic intoxication. Am J Med Sci 289(5):210-214.
14. AUTHOR(S), REVIEWER(S), DATE(S) (INCLUDING UPDATES), COMPLETE ADDRESS(ES)
<14>Author: Jean-Louis Benedetti, M.D. Centre de Toxicologie du Québec Centre Hospitalier Universitaire de Québec (CHUQ) Pavillon Centre Hospitalier de l'Université Laval (CHUL) 2705 Boulevard Laurier Sainte-Foy, Québec Canada, G1V 4G2 Tel: 1-418-6542254 Fax: 1-418-6542148 E-mail: [email protected] Reviewer: Prof. Dr. A.N.P. van Heijst Baarnseweg 42A 3735 MJ Bosch en Duin Netherlands Tel: 31-30-2287178 E-mail:[email protected] Date: July 1996 Peer Reviewed, Sao Paulo INTOX-11, October 21, 1999. (Drs W. Temple, New Zealand- co-ordinator; B. Groszek, Poland; J. de Kom, Surinam; J.C. Rios Bustamante, Chile; J.C. Piola, Argentina).
See Also: Toxicological Abbreviations Arsenic (EHC 18, 1981) Arsenic (ICSC) Arsenic (WHO Food Additives Series 18) Arsenic (WHO Food Additives Series 24) Arsenic (JECFA Evaluation)


![AppNote - PIM - Mitigating Ext. Sources of PIM [11410-00756A]](https://static.fdocuments.us/doc/165x107/55cf9b4e550346d033a5882d/appnote-pim-mitigating-ext-sources-of-pim-11410-00756a.jpg)















