Arrhythmic Risk and Aortic Stenosis - Aritmie Cardiache · Pathophysiology of Aortic Stenosis !...
38
Arrhythmic Risk and Aortic Stenosis
Transcript of Arrhythmic Risk and Aortic Stenosis - Aritmie Cardiache · Pathophysiology of Aortic Stenosis !...
Arrhythmic Risk and Aortic Stenosis
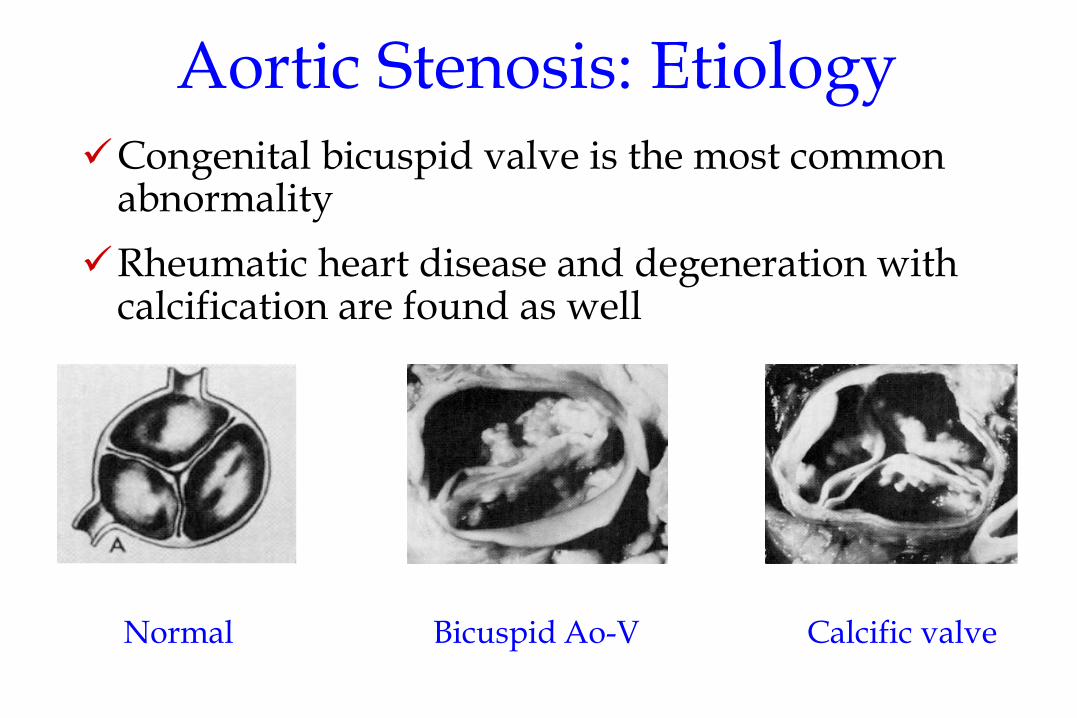
Aortic Stenosis: Etiology ü Congenital bicuspid valve is the most common
abnormality
ü Rheumatic heart disease and degeneration with calcification are found as well
Normal Bicuspid Ao-V Calcific valve
Common Clinical Scenarios ü Younger people
ü Functional murmur vs MVP vs bicuspid AV
ü Older people ü Aortic sclerosis vs aortic
stenosis
Pathophysiology of Aortic Stenosis ü Left ventricular outflow obstruction
ü LV systolic pressure > aortic pressure
ü Concentric left ventricular hypertrophy ü Sustains high LV pressures ü Normalizes wall stress (radius x pressure/wall thickness) ü Eventually results in impaired LV diastolic compliance
ü LA hypertrophy and enlargement
ü Severe stenosis: Limits ability to increase stroke volume on demand
Critical aortic stenosis = fixed cardiac output

Natural History of Aortic Stenosis ü Long asymptomatic “latent” period
ü “Cardinal” symptoms of severe aortic stenosis ü Dyspnea
ü Angina
ü Syncope
ü Sudden death
ü Left ventricular dilatation and contractile failure
ü Endocarditis
ü Arrhythmias ü Ventricular tachycardia
ü Conduction system disease
ü Atrial fibrillation
Mechanisms of Syncope in Aortic Stenosis
ü Fixed cardiac output: Vasodilation (exercise, vagal stimulation, drug induced), inability to augment CO, drop in cerebral perfusion pressure.
ü Heart block: Ca++ deposits in aortic ring encroach upon conduction tissue
ü Ventricular arrhythmias (LVH, ischemia)

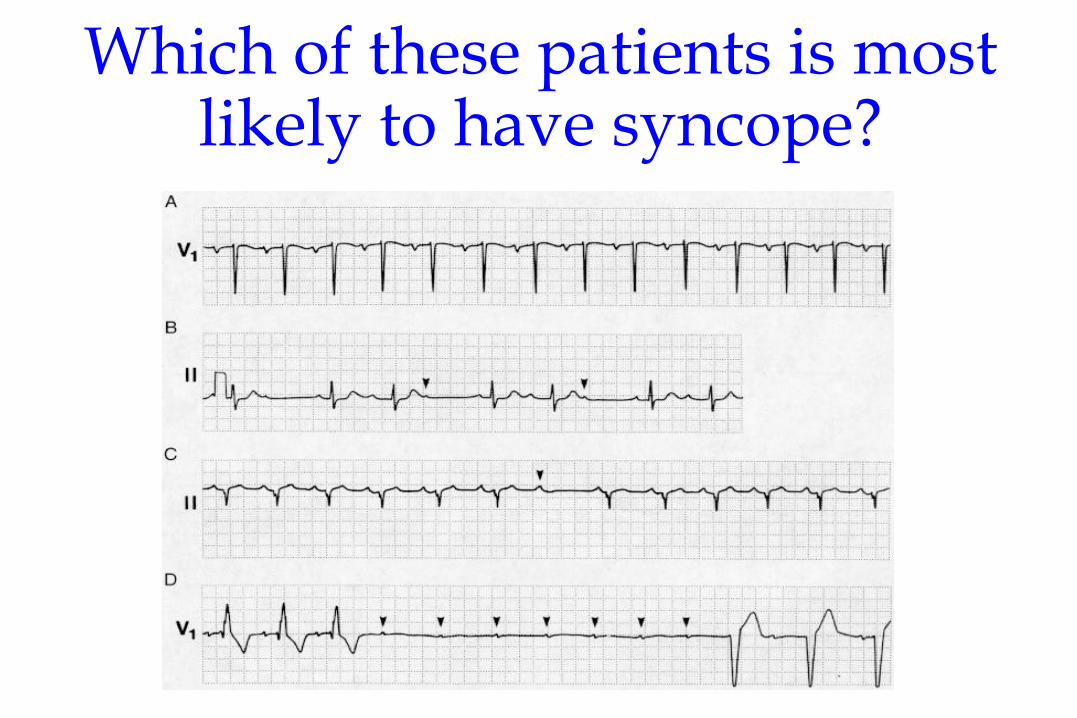
Which of these patients is most likely to have syncope?

A 75 year old man has recurrent seizures. Holter ECG monitoring during a seizure.
What is the appropriate
management?

Predictors of Risk for MI, HF, Death ü Unstable Coronary Syndrome
ü angina, acute or recent MI
ü Decompensated Heart Failure ü new onset, worsening HF, NYHA Class IV
ü Significant Arrhythmias ü high grade AV block, symptomatic or new ventricular
arrhythmia,
ü tachycardia with rate > 100, symptomatic bradycardia
ü Severe Valvular Disease ü severe aortic stenosis, symptomatic mitral stenosis
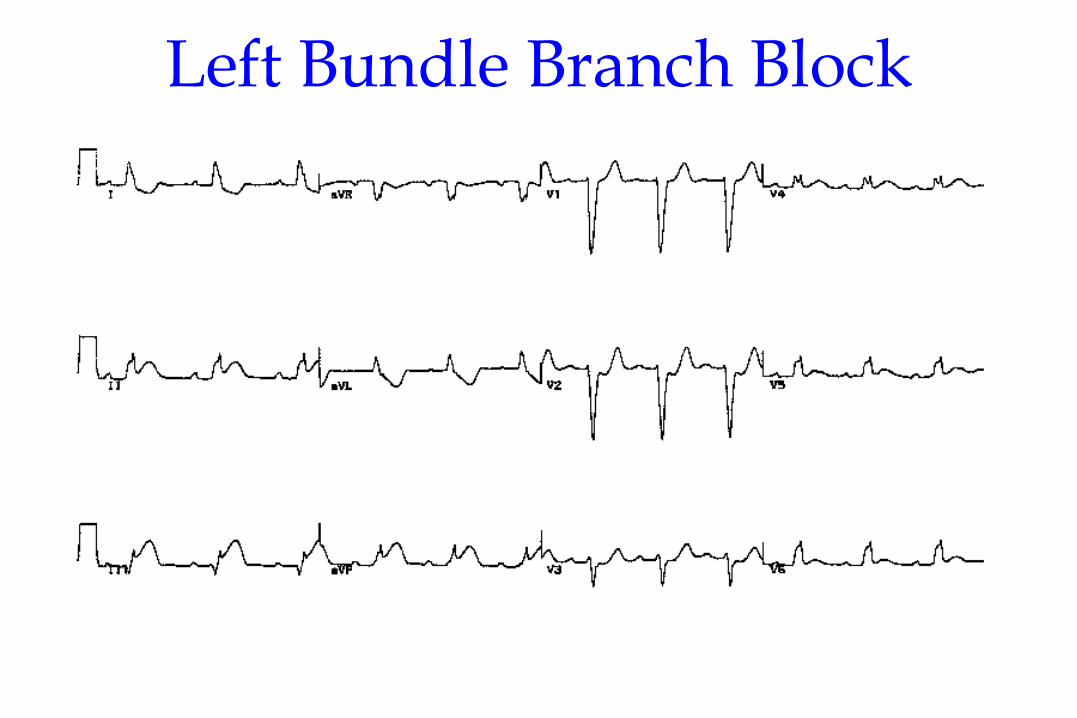
Left Bundle Branch Block
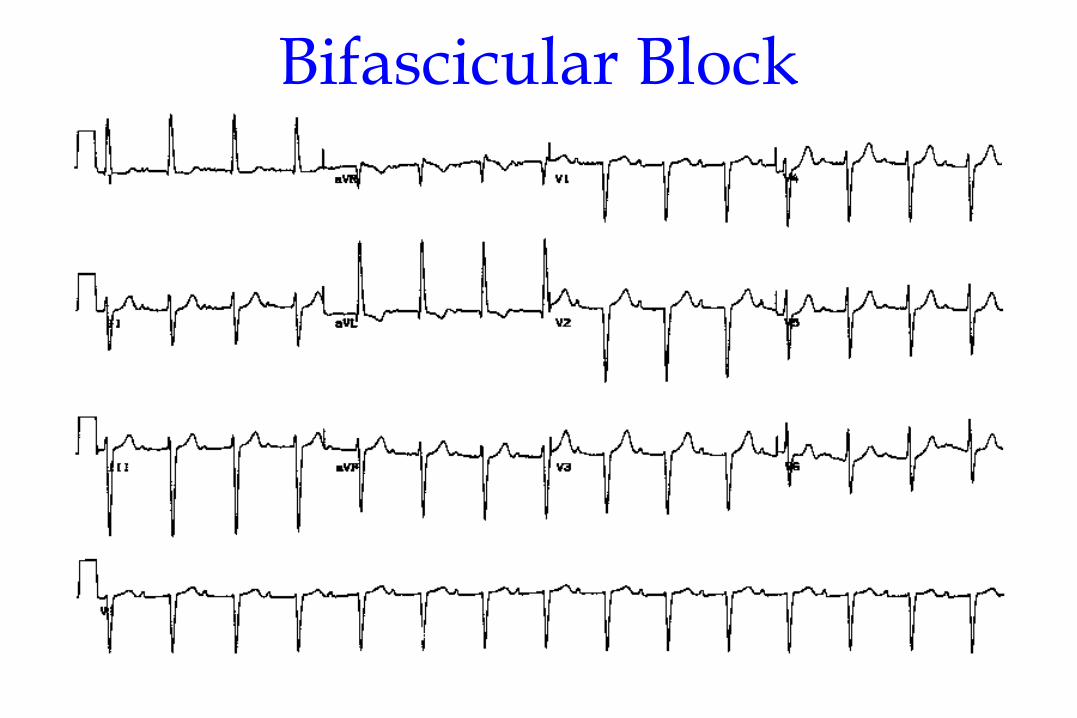
Bifascicular Block

Trifascicular Block
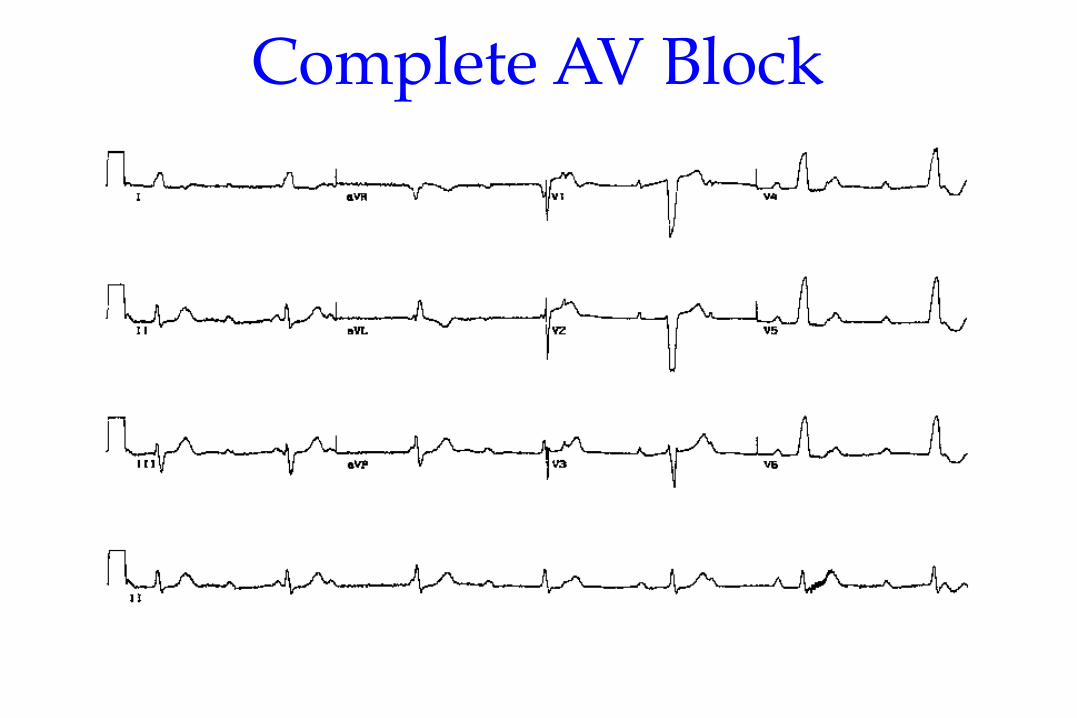
Complete AV Block
Diagnostic Value of ECG
ü Preexisting conduction disturbance
ü WPW Syndrome
ü ECG aspects of genetic syndromes
Oreto G. I Disordini del Ritmo Cardiaco - CSE 1997


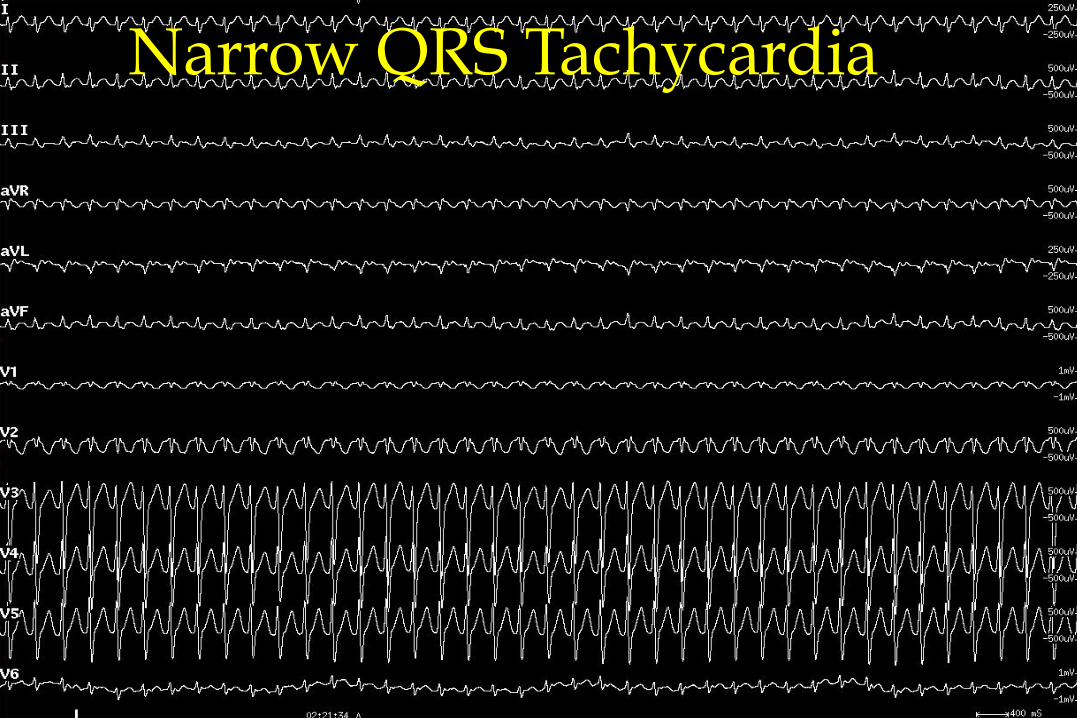
Narrow QRS Tachycardia

Wide QRS Tachycardia
Sherlock Holmes
“…le conclusioni più importanti possono
dipendere da particolari apparentemente trascurabili….”
Oreto G. I Disordini del Ritmo Cardiaco - CSE 1997
Valvular disease and Sudden Death
ü Aortic stenosis (predominate)
ü The mechanism of sudden death is unclear, and both malignant ventricular arrhythmia and bradyarrhythmia have been documented

Bayés de Luna A. Am Heart J. 1989;117:151-159.
Underlying Arrhythmias of SD
Bradycardia 17%
VT 62%
Primary VF 8%
Torsades de Pointes 13%

1 Adapted from Cohn JN. N Engl J Med. 1996;335:490–498.
2 He J, Ogden LG, Bazzano LA, et al. Risk Factors for Congestive Heart Failure in US Men and women: NHANES I epidemiologic follow-up study. Arch Intern Med 2001, 161: 996-1002.
Pathologic remodeling
Low ejection fraction Death
Symptoms: Dyspnea Fatigue Edema
Chronic heart
failure
ü Neurohormonal stimulation
ü Endothelial dysfunction
ü Myocardial toxicity ü Vasoconstriction ü Renal sodium
retention
Arrhythmia
Pump failure
Coronary artery disease
ü Hypertension ü Cardiomyopathy ü Valvular Disease
Left ventricular injury
Pathological Progression of CV Disease
Underlying etiology in ~60% of CHF 1
Underlying etiology in ~40% of CHF 1

LVEF and SCA Incidence
Vreede-Swagemakers JJ. J Am Coll Cardiol. 1997;30:1500-1505.
LVEF
% S
CA
Vic
tims
7.5%
5.1%
2.8%
1.4%
0 1 2 3 4 5 6 7 8
0-30% 31-40% 41-50% >50%
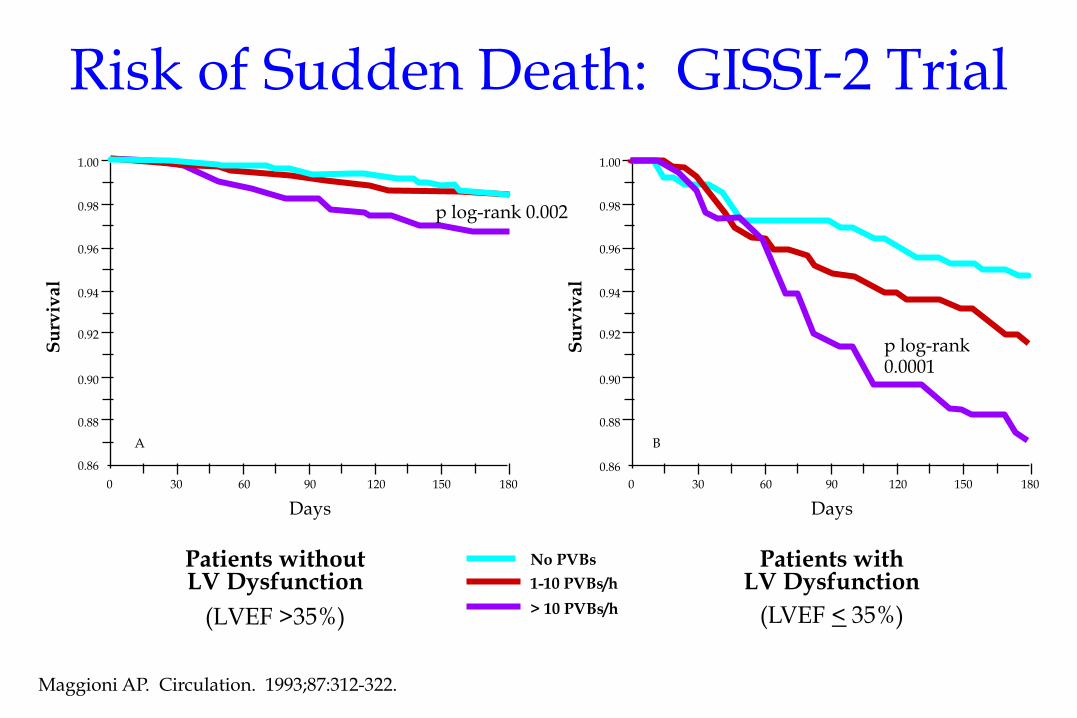
Risk of Sudden Death: GISSI-2 Trial
Patients without LV Dysfunction
(LVEF >35%)
Maggioni AP. Circulation. 1993;87:312-322.
Patients with LV Dysfunction
(LVEF < 35%)
No PVBs
1-10 PVBs/h
> 10 PVBs/h
0.86
A
0.88
0.90
0.92
0.94
0.96
0.98
1.00
0 30 60 90 120 150 180
Days
Su
rviv
al
p log-rank 0.002
0.88
0.90
0.92
0.94
0.96
0.98
1.00
0 30 60 90 120 150 180
Days
Su
rviv
al
B
p log-rank 0.0001
0.86
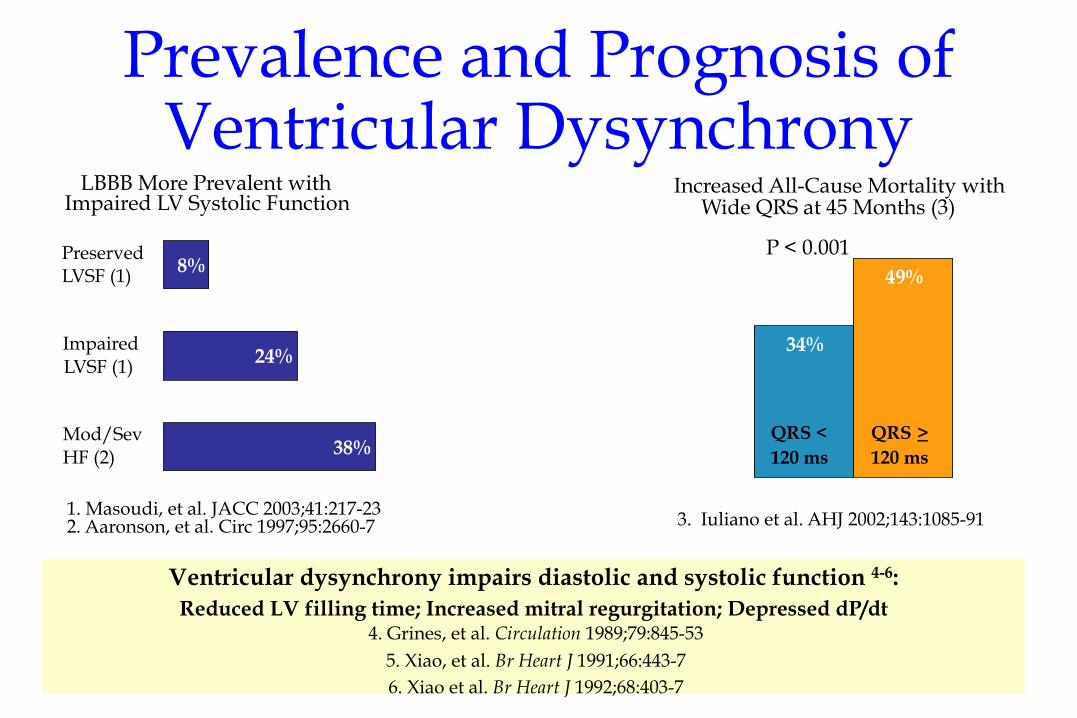
Prevalence and Prognosis of Ventricular Dysynchrony
Ventricular dysynchrony impairs diastolic and systolic function 4-6: Reduced LV filling time; Increased mitral regurgitation; Depressed dP/dt
4. Grines, et al. Circulation 1989;79:845-53 5. Xiao, et al. Br Heart J 1991;66:443-7 6. Xiao et al. Br Heart J 1992;68:403-7
Increased All-Cause Mortality with Wide QRS at 45 Months (3)
34%
49%
QRS < 120 ms
QRS > 120 ms
3. Iuliano et al. AHJ 2002;143:1085-91
P < 0.001
LBBB More Prevalent with Impaired LV Systolic Function
38%
24%
8%
Mod/Sev HF (2)
Impaired LVSF (1)
Preserved LVSF (1)
1. Masoudi, et al. JACC 2003;41:217-23 2. Aaronson, et al. Circ 1997;95:2660-7

Test Appropriate Diagnostic NND
History and physical exam 308 (100%) 47 (15%) 7
ECG 241 (78%) 25 (10%) 10
Holter ECG 82 (27%) 13 (16%) 6
EPS 51 (17%) 14 (27%) 4
Diagnostic Yield
Europace 2002; 4: 351-356


NYHA
VPBs/nsVT
Ischemia
SD
QT d QRS d
FE
EPS
Markers of Arrhythmic Risk
ü Simple “descriptors”
ü Prognostic Indicators
ü Decision-making ?

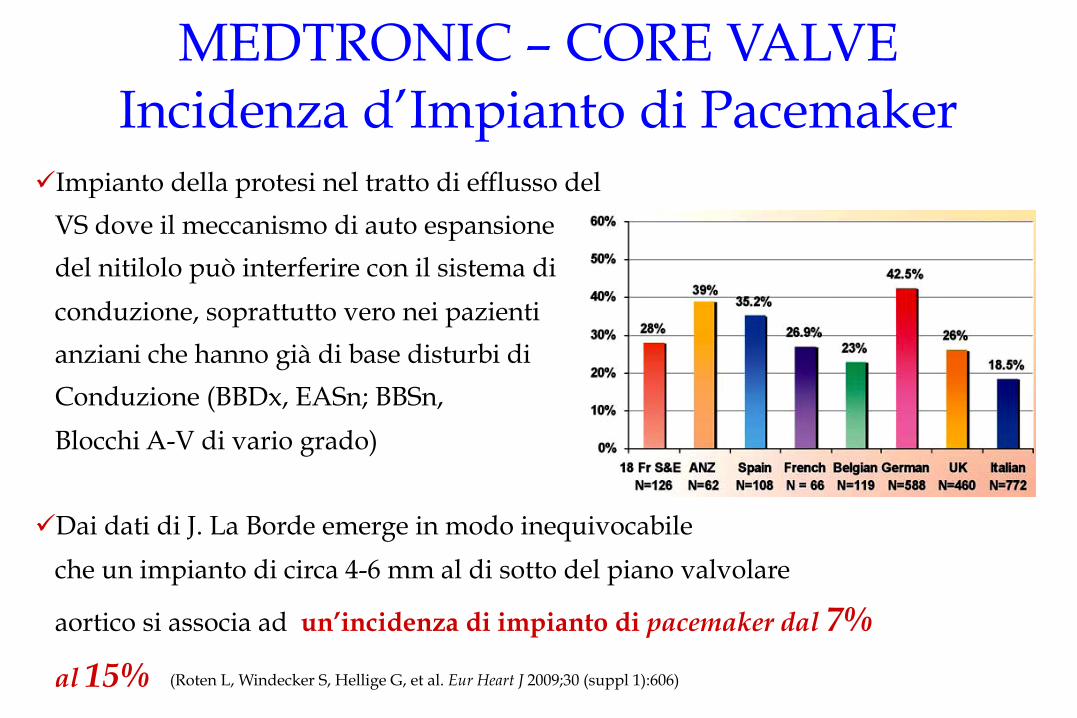
ü Impianto della protesi nel tratto di efflusso del
VS dove il meccanismo di auto espansione
del nitilolo può interferire con il sistema di
conduzione, soprattutto vero nei pazienti
anziani che hanno già di base disturbi di
Conduzione (BBDx, EASn; BBSn,
Blocchi A-V di vario grado)
ü Dai dati di J. La Borde emerge in modo inequivocabile
che un impianto di circa 4-6 mm al di sotto del piano valvolare
aortico si associa ad un’incidenza di impianto di pacemaker dal 7%
al 15%
MEDTRONIC – CORE VALVE Incidenza d’Impianto di Pacemaker
(Roten L, Windecker S, Hellige G, et al. Eur Heart J 2009;30 (suppl 1):606)

FRANCE Registry Complicanze Maggiori a 30 Giorni
PCR 2010

Selection of Pacemaker Systems for Patients With AV Block
Epstein A, et al. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities. J Am Coll Cardiol 2008; 51:e1–62. Figure 1.
AV block
Chronic atrial tachyarrhythmia,
reversion to sinus rhythm not anticipated
Desire for AV
synchrony
Desire for rate response
No Yes
Desire for rate response
No
Desire for atrial pacing
Yes
Ventricular pacemaker
Rate-responsive ventricular pacemaker
No Yes
Single-lead atrial sensing ventricular
pacemaker Desire for rate
response
Dual-chamber pacemaker
Rate-responsive dual-chamber pacemaker
No Yes
No Yes
Ventricular pacemaker
Rate-responsive ventricular pacemaker
No Yes

Yes No
Sinus Node Dysfunction
No
Atrial pacemaker Rate-responsive atrial pacemaker
Rate-responsive dual-chamber
pacemaker
Dual-chamber pacemaker
Ventricular pacemaker
Rate-responsive ventricular pacemaker
Yes
No Yes No Yes
No Yes
Selection of Pacemaker Systems for Patients With Sinus Node Dysfunction
Epstein A, et al. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities. J Am Coll Cardiol 2008; 51:e1–62. Figure 2.
Evidence for impaired AV conduction or concern over future development of AV block
Desire for rate
response
Desire for AV synchrony
Desire for rate
response
Desire for rate
response
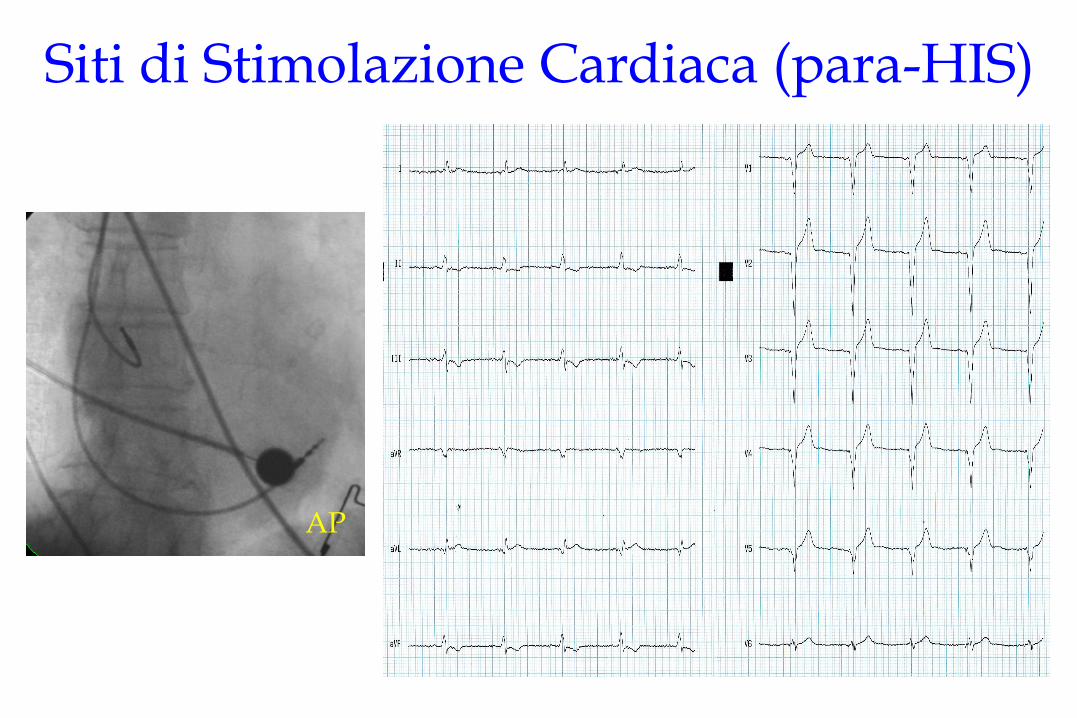
Siti di Stimolazione Cardiaca (para-HIS)
AP
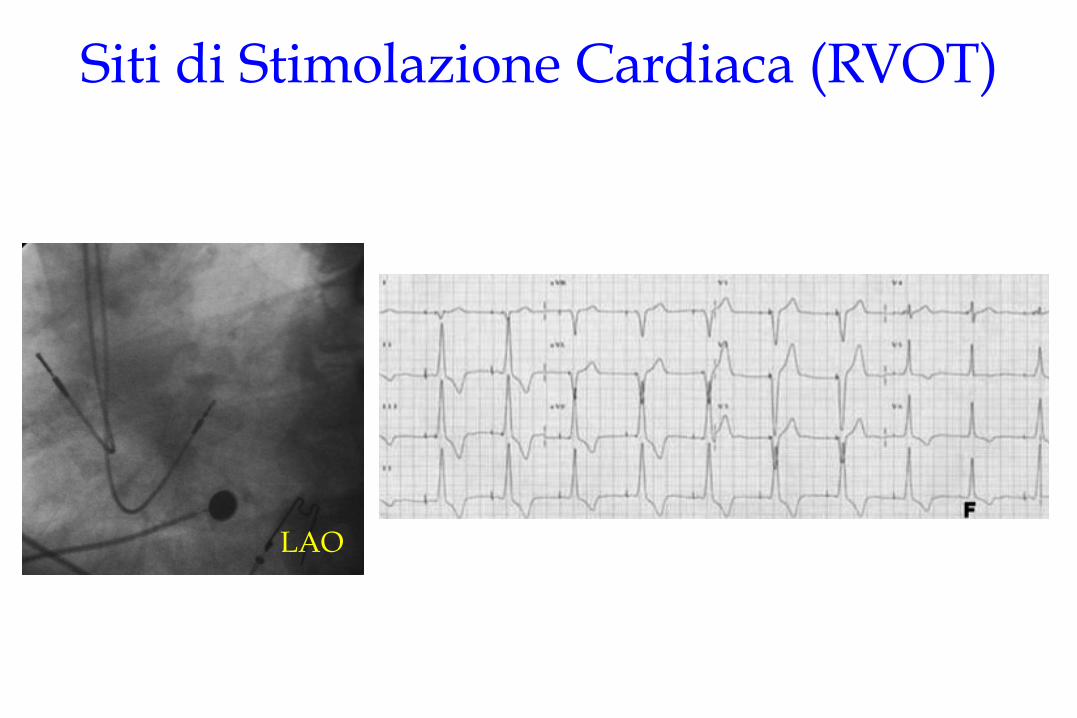
Siti di Stimolazione Cardiaca (RVOT)
LAO

Preoperative Risk Evaluation “Prepares the Patient to TAVI”


















