Are symptomatic guidelines for chemotherapy appropriate to ER-positive screen-detected breast cancer...
10
PRECLINICAL STUDY Are symptomatic guidelines for chemotherapy appropriate to ER-positive screen-detected breast cancer (SDBC)? Nigel J. Bundred • Ramachandran Prasad • Julie Morris • W. Fiona Knox • Ged Byrne • Shan Cheung • Mary Wilson • Gill Lawrence Received: 23 November 2010 / Accepted: 21 June 2011 / Published online: 10 July 2011 Ó Springer Science+Business Media, LLC. 2011 Abstract Oncologists recommend chemotherapy to post- menopausal women with adverse prognostic factors, but predictors of the benefit of chemotherapy are mainly based on mortality from symptomatic cancer trials. From 1990 to 1998, 1475 breast cancers (875 screen detected cancers [SDBCs]: 600 symptomatic) were treated in women aged 50–65 years and prognostic factors compared with cancer mortality. Median follow-up was 110 months. The Not- tingham Prognostic Index (NPI) was calculated for 6737 breast cancers which were part of the Association of Breast Surgery (ABS) 2001/2002 Audit of SDBCs to validate sur- vival figures. Ten year survival was 92.1% for SDBC and 77.6% for symptomatic cancers. Adjusting for baseline factors, SDBCs had a reduced mortality (RR = 0.42 (0.31–0.57), independent of grade, node status and tumour size. Oestrogen receptor (ER) positive SDBC had a lower annual mortality rate (0.6%) compared with symptomatic (4.3%: P \ 0.001) or ER negative SDBC (1.8%). Epithelial proliferation was lower in SDBC in all NPI groups compared with symptomatic cancers (P B 0.001). Grade, node status, ER status, size and mode of detection predicted survival. Survival for each NPI group was better for SDBC. For ER positive SDBC in the Moderate Prognostic Group 1 (MPG1), 10 year mortality was 6.4% compared with 17.6% in symptomatic (P = 0.001). NPI on 6,737 operable SDBC confirmed similar mortality in all groups (4% mortality in MPG1 group). SDBC have lower mortality than symptom- atic due to a lower proliferative index. The use of adjuvant chemotherapy is over-treatment for ER positive SDBCs with Good Prognostic Group (GPG) and MPG1 NPI scores. Keywords Breast cancer Á Epithelial proliferation Á Screening Abbreviations ABS Association of Breast Surgery EBCTCG Early Breast Cancer Trialists’ Collaborative Group Electronic supplementary material The online version of this article (doi:10.1007/s10549-011-1652-6) contains supplementary material, which is available to authorized users. N. J. Bundred (&) Á R. Prasad Á G. Byrne Academic Department of Surgery, University Hospital of South Manchester, 2nd Floor Education and Research Centre, Southmoor Road, Wythenshawe, Manchester M23 9LT, UK e-mail: [email protected] R. Prasad e-mail: [email protected] G. Byrne e-mail: [email protected] J. Morris Academic Department of Statistics, University Hospital of South Manchester, Manchester, UK e-mail: [email protected] W. F. Knox Academic Department of Pathology, University Hospital of South Manchester, Manchester, UK e-mail: [email protected] S. Cheung Á G. Lawrence West Midlands Cancer Intelligence Unit, Manchester, UK e-mail: [email protected] G. Lawrence e-mail: [email protected] M. Wilson Academic Department of Radiology and Statistics, University Hospital of South Manchester, Manchester, UK e-mail: [email protected] 123 Breast Cancer Res Treat (2013) 138:359–368 DOI 10.1007/s10549-011-1652-6
-
Upload
julie-morris -
Category
Documents
-
view
214 -
download
0
Transcript of Are symptomatic guidelines for chemotherapy appropriate to ER-positive screen-detected breast cancer...

PRECLINICAL STUDY
Are symptomatic guidelines for chemotherapy appropriateto ER-positive screen-detected breast cancer (SDBC)?
Nigel J. Bundred • Ramachandran Prasad •
Julie Morris • W. Fiona Knox • Ged Byrne •
Shan Cheung • Mary Wilson • Gill Lawrence
Received: 23 November 2010 / Accepted: 21 June 2011 / Published online: 10 July 2011
� Springer Science+Business Media, LLC. 2011
Abstract Oncologists recommend chemotherapy to post-
menopausal women with adverse prognostic factors, but
predictors of the benefit of chemotherapy are mainly based
on mortality from symptomatic cancer trials. From 1990 to
1998, 1475 breast cancers (875 screen detected cancers
[SDBCs]: 600 symptomatic) were treated in women aged
50–65 years and prognostic factors compared with cancer
mortality. Median follow-up was 110 months. The Not-
tingham Prognostic Index (NPI) was calculated for 6737
breast cancers which were part of the Association of Breast
Surgery (ABS) 2001/2002 Audit of SDBCs to validate sur-
vival figures. Ten year survival was 92.1% for SDBC and
77.6% for symptomatic cancers. Adjusting for baseline
factors, SDBCs had a reduced mortality (RR = 0.42
(0.31–0.57), independent of grade, node status and tumour
size. Oestrogen receptor (ER) positive SDBC had a lower
annual mortality rate (0.6%) compared with symptomatic
(4.3%: P \ 0.001) or ER negative SDBC (1.8%). Epithelial
proliferation was lower in SDBC in all NPI groups compared
with symptomatic cancers (P B 0.001). Grade, node status,
ER status, size and mode of detection predicted survival.
Survival for each NPI group was better for SDBC. For ER
positive SDBC in the Moderate Prognostic Group 1 (MPG1),
10 year mortality was 6.4% compared with 17.6% in
symptomatic (P = 0.001). NPI on 6,737 operable SDBC
confirmed similar mortality in all groups (4% mortality in
MPG1 group). SDBC have lower mortality than symptom-
atic due to a lower proliferative index. The use of adjuvant
chemotherapy is over-treatment for ER positive SDBCs with
Good Prognostic Group (GPG) and MPG1 NPI scores.
Keywords Breast cancer � Epithelial proliferation �Screening
Abbreviations
ABS Association of Breast Surgery
EBCTCG Early Breast Cancer Trialists’ Collaborative
Group
Electronic supplementary material The online version of thisarticle (doi:10.1007/s10549-011-1652-6) contains supplementarymaterial, which is available to authorized users.
N. J. Bundred (&) � R. Prasad � G. Byrne
Academic Department of Surgery, University Hospital of South
Manchester, 2nd Floor Education and Research Centre,
Southmoor Road, Wythenshawe,
Manchester M23 9LT, UK
e-mail: [email protected]
R. Prasad
e-mail: [email protected]
G. Byrne
e-mail: [email protected]
J. Morris
Academic Department of Statistics, University Hospital of South
Manchester, Manchester, UK
e-mail: [email protected]
W. F. Knox
Academic Department of Pathology, University Hospital of
South Manchester, Manchester, UK
e-mail: [email protected]
S. Cheung � G. Lawrence
West Midlands Cancer Intelligence Unit, Manchester, UK
e-mail: [email protected]
G. Lawrence
e-mail: [email protected]
M. Wilson
Academic Department of Radiology and Statistics, University
Hospital of South Manchester, Manchester, UK
e-mail: [email protected]
123
Breast Cancer Res Treat (2013) 138:359–368
DOI 10.1007/s10549-011-1652-6

EPG Excellent Prognostic Group
ER Oestrogen receptor
GPG Good Prognostic Group
MPG1 Moderate Prognostic Group 1
MPG2 Moderate Prognostic Group 2
NHSBSP National Health Service Breast Screening
Programme
NICE National Institute for Health and Clinical
Excellence
NPI Nottingham Prognostic Index
PPG Poor Prognostic Group
PR Progesterone receptor
SDBC Screen detected breast cancer
UHSM University Hospital of South Manchester
WLE Wide local excision
Introduction
Breast screening reduces mortality from breast cancer [1–
3]. Cancers detected by screening should require less
treatment as they are at an earlier stage [1–7]. Survival
figures for the Swedish Two Counties Trial demonstrated
small, node-negative cancers detected by screening had on
average, 8–10% better survival at 15 years compared with
similar-sized node negative, symptomatic cancers; despite
no adjuvant therapy being given [3].
Finnish comparison of palpable and non-palpable T1
cancers indicated a better breast cancer-specific survival in
non-palpable tumours, suggesting an inherent biological
difference in cancers detected by mammographic screening
[6]. Treatment decisions for breast cancer are now based on
molecular phenotype, with Oestrogen receptor (ER) nega-
tive and HER2 positive cancers advised chemotherapy.
Dawson et al. found screen detected luminal A (ER posi-
tive, HER2 negative) breast cancers had a 94% 15 year
survival compared with 84% for symptomatically detected
cancers [7]. Moreover, a UK population-based study found
that cancers detected by screening had a 50% lower mor-
tality than symptomatic cancers [8]. In general, the poorer
breast cancer survival in the UK reflects later diagnosis;
especially in older women [9].
Therapy for SDBC is determined by oncologists using
cancer guidelines developed mainly from trials for symp-
tomatic breast cancer [10, 11]. The Meta-analyses of the
Early Breast Cancer Trialists’ Collaborative Group (EB-
CTCG) recommended adjuvant chemotherapy for women
between 50 and 70 years old with adverse prognostic fac-
tors based on a 10–20% relative reduction in cancer mor-
tality [10] The benefit of chemotherapy is proportionate to
the risk of recurrence but complications of chemotherapy,
which include thrombosis, sepsis and occasionally death,
occur in 1–3% of treated patients and complications
increase with age [10–12]. Late adverse health effects such
as leukaemia and cardiotoxicity occur in 1% of patients
from 5–13 years later [13] The reduction in absolute
mortality from chemotherapy in postmenopausal women
older than 50 years was 3–5% [10] remaining constant at
15 years [10] and occurred within 5 years of chemotherapy
administration. Unless an individual’s risk of death is
greater than 10% at 5 years, no proportionate reduction in
mortality from chemotherapy use greater than 1% is
achievable, and the morbidity from its administration will
equal its benefit. Only breast cancers with an increased
annual hazard rate for mortality of 10% or greater in the
5 years after diagnosis will benefit from chemotherapy.
International Guidelines utilise pathological factors to
recommend chemotherapy [10, 11, 14, 15]. The UK NICE
guidelines recommend the use of Adjuvant! Online [11] to
select for adjuvant therapy. Clinicians use symptomatic
prognostic indices such as the Nottingham Prognostic
Index (NPI) which predicts survival based on histological
grade, lymph node status and 20% of the tumour size;
stratifying women with symptomatic breast cancer into five
different prognostic groups [15, 16]. Chemotherapy is
offered to Moderate (MPG1 and 2) and Poor Prognostic
Groups (PPGs) with overall 10 year survival 85%, 70%
and 36%, respectively [15, 16]. When the NPI was applied
to the 1996/1997 NHS Breast Screening Programme
(NHSBSP) data, the 5 year survival for SDBCs in MPG1, 2
and PPG was 94.2%, 87.4% and 71.5%, respectively [17].
This led us to investigate whether SDBCs have a lower
mortality from cancer, despite the presence of histopa-
thological adverse prognostic factors.
Annual Hazard Rates for mortality in women in the
50–65 year old age group were calculated to determine
within breast cancers with similar prognostic factors,
whether mode of detection is of prognostic value. To
identify women with ER positive SDBC at high risk of
mortality who require adjuvant chemotherapy, we used the
NPI and validated the results on 6737 operable SDBCs
submitted to the NHSBSP/ABS Audit. The ER positive
SDBCs had a better survival than symptomatic cancers
with a low mortality in the first 5 years, despite the omis-
sion of chemotherapy. This survival benefit is due to a
lower epithelial proliferation in SDBC, providing a bio-
logical rationale, and a reason why chemotherapy would be
less effective [18].
Materials and methods
In total, 1475 women with operable breast cancers (875
SDBCs and 600 symptomatic) were diagnosed and treated
360 Breast Cancer Res Treat (2013) 138:359–368
123

in women aged 50–65 years in the Manchester Breast Unit
between 1990 and 1998. Prospective follow-up data were
collected on all women (4.7% [n = 75] were lost to follow-
up). All patients in the Manchester part of the study were
diagnosed and treated by five surgeons in the South Man-
chester breast unit. They consented to follow-up and col-
lection of their data but the study was not submitted for
ethical approval as the data was taken from the outcomes of
the patient National ABS at BASO Audit supported by the
NHSBSP which does not require ethical approval, as the
auditing is done on an annual basis and has been approved
by the Department of Health (Fig. 1).
Pathological data (type, size, grade and node status), ER
and progesterone receptor (PR) status were prospectively
recorded on all patients (using NHSBSP reporting stan-
dards) in the University Hospital of South Manchester
(UHSM) Breast database. Cancer size was measured his-
tologically and expressed in mm. Tumours were graded by
the modified Bloom and Richardson method [19]. Median
follow-up was 110 months (range 15–187).
Women with palpable invasive cancer underwent wide
local excision (WLE) or mastectomy whenever possible.
Impalpable lesions were excised using localisation tech-
niques. Between 1990 and 1998, Unit policy was to per-
form a level III axillary clearance during the primary
procedure, if a pre-operative diagnosis was available or as
a subsequent procedure if no pre-operative diagnosis was
obtained, as sentinel node biopsy was not available in the
U.K. In women who underwent WLE by wire localisation
when grade I and II tumours \10 mm diameter were
removed, no axillary surgery was undertaken [20].
Adjuvant chemotherapy was given to women who had
tumours measuring more than 20 mm, ER negative can-
cers, or with 4 or more involved nodes. Adjuvant
Tamoxifen was given to all women with ER positive
tumours greater than 10 mm until 1995, when it was
offered to all ER positive tumours. The follow-up proto-
col observed was uniform. Women were examined
annually to 10 years with annual mammograms. The ER/
PR status was assessed by immuno-histochemistry on
paraffin slides as previously described [21]. Sections with
more than 5% of cell nuclear staining were considered
ER/PR positive [21]. Epithelial proliferation was assessed
by Ki67 staining and counting the number of cells stained
per 1,000 as previously described [21]. Immunohisto-
chemical detection and scoring of HER2 was as previ-
ously described [21] with scores 3? rated as positive. The
characteristics of the two populations of cancers are
shown in Table 1.
A clinically, radiologically or morphologically-verified
recurrence (any recurrence in the supraclavicular nodes or
beyond) and all deaths from breast cancer, were defined
as distant recurrence in the analysis. After comparing
mortality for SDBC and symptomatic cancers, the NPI
index was employed to determine the risk of mortality
and annual Hazard Rates for death calculated for both
groups.
Table 1 Prognostic factors in SDBC and symptomatic cancers in
Manchester (n = 1475)
Variables Symptomatic
n (%)
N = 600
Screening
n (%)
N = 875
P value
Size
\15 mm 217 (36.2) 536 (61.3)
15–25 mm 287 (47.8) 275 (31.4) P \ 0.001
[25 mm 96 (16.0) 64 (7.3)
Grade
I 165 (27.5) 238 (27.2)
II 258 (43.0) 358 (40.9) P = 0.60
III 177 (29.5) 279 (31.9)
Node status
Negative 392 (65.3) 692 (79.1) P \ 0.001
Positive (1–3 nodes) 149 (24.8) 150 (17.1)
Positive (4? nodes) 59 (9.8) 33 (3.8)
ER positivity 461 (76.8) 677 (77.4) P = 0.86
PR positivity 451 (75.2) 659 (75.3) P = 1.00
HER2 status (n = 786)
0 38 (12.5) 98 (20.3) P = 0.004
1 86 (28.3) 147 (30.5)
2 136 (44.7) 176 (36.5)
3 44 (14.5) 61 (12.7)
Age; mean(SD) 56.9 (4.7) 56.8 (4.6) P = 0.83
Ki67; mean (SD)
(n = 1041) 34.7 (16.0) 21.3 (10.4) P \ 0.001
Ki67 C 20; n (%) 305 (74.6) 341 (54.0) P \ 0.001
Ki67 C 25; n (%) 279 (68.2) 221 (35.0) P \ 0.001
Ki67 C 30; n (%) 246 (60.1) 127 (20.1) P \ 0.001
Chemo (n = 1418) 178 (30.0) 107 (13.0) P \ 0.001
NPI
Excellent 115 (19.2) 187 (21.4) P \ 0.001
Good 166 (27.7) 309 (35.3)
Moderate I 160 (26.7) 242 (27.7)
Moderate II 87 (14.5) 85 (9.7)
Poor 72 (12.0) 52 (5.9)
10-year distant recurrence
%; (95% CI)
19.9 7.9 P \ 0.001
(16.3, 23.5) (5.9, 9.9)
10-year breast cancer
mortality %; (95% CI)
22.4 7.9 P \ 0.001
(18.8, 26.0) (5.9, 9.9)
Comparison of prognostic features, distant recurrence and mortality
between SDBCs and symptomatic cancers. The figures are rounded to
one decimal place. Mortality and distant recurrence figures are
derived from Kaplan–Meier curves and were lower in SDBC com-
pared to symptomatic cancers at 10 years
Breast Cancer Res Treat (2013) 138:359–368 361
123

Mortality data for the operable SDBCs diagnosed in
2001/2002 that were submitted to the NHSBSP/ABS Audit
was utilized to validate our findings. The NHSBSP/ABS
Audit prospectively records data on tumour grade, size and
node status for SDBCs diagnosed in the U.K. Mortality
data are obtained by flagging the patients at cancer regis-
tries and are complete for all patients for a minimum of
5 years follow-up. Chemotherapy use was obtained from
the same dataset in the adjuvant therapy section of the
Audit.
Statistical analysis
Data were analysed using the statistical software package
SPSS version 15.0. The simple chi-square test and the two-
sample t-test were employed to compare the distribution of
pathological features between women with screen-detected
and symptomatic cancers. The assessment of factors
affecting recurrence and survival was made using Kaplan–
Meier plots and the log-rank test. The factors, tumour size
and number of nodes, involved were initially assessed as
continuous variables, to compare recurrence and mortality
between SDBC and symptomatic cancers. Mortality rates
are estimated from the survival proportion estimates at
each uncensored survival time life tables, derived from the
Kaplan–Meier analysis. Smoothed annual mortality rates
were calculated by ER and diagnosis group as described
previously [20]. Subsequently, Cox proportional hazards
regression models were employed to evaluate the inde-
pendent predictive power of diagnostic mode (symptomatic
or SDBC) after adjusting for statistically significant
tumour/patient characteristics (identified from size, grade,
node status, ER and PR status, Ki67, chemotherapy).
Results
After adjusting for tumour grade, size, node and ER status,
diagnosis by screening was associated with an independent
reduced risk of distant recurrence RR = 0.43; (95% CI
0.31–0.57) and breast cancer mortality RR = 0.42
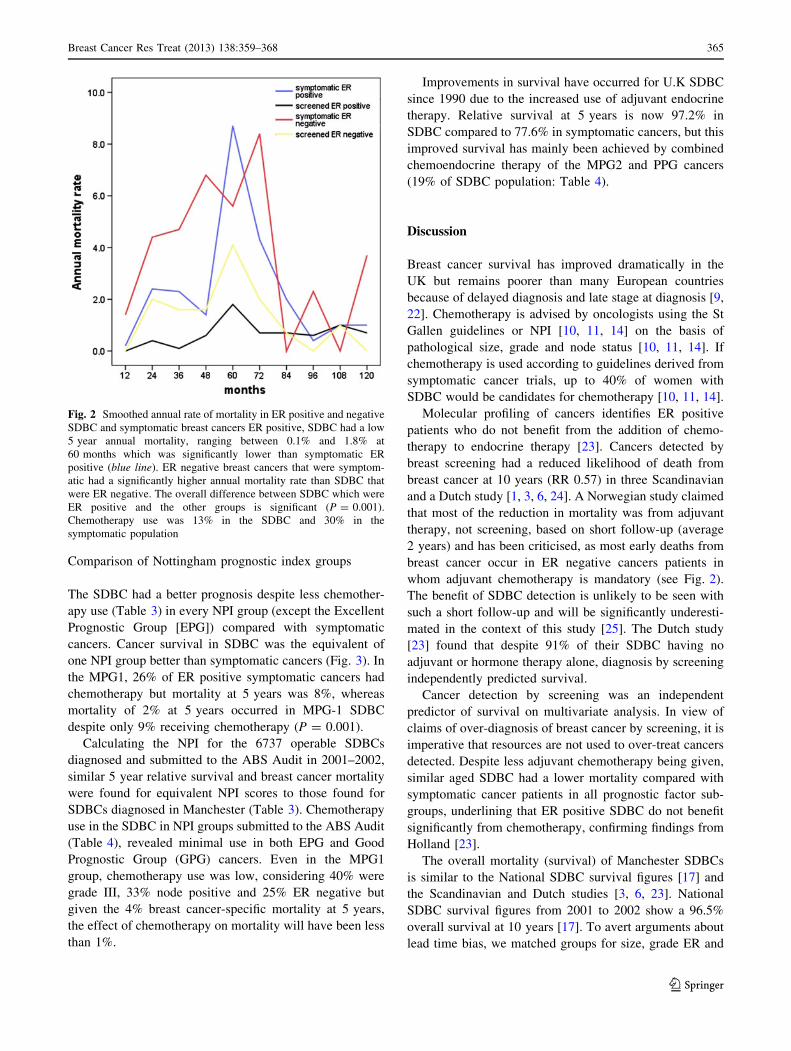
(0.31–0.57) (Table 2). The smoothed annual mortality rates
showed the expected peak for cancer deaths in the 5 years
after surgery for symptomatic cancers (ER negative 5.6%/
year: ER positive 8.7%/year), whereas there was no peak
(increase in mortality or recurrence) in the first 5 years (or
subsequently) in ER positive SDBC (1.8%/year)
(P B 0.001: Fig. 2). Breast Cancer Survival for the study
population was 94% at 5 years. In 875 women with
SDBCs, overall 5 year cancer survival was 96.4%, com-
pared with 87.9% in 600 women with symptomatic cancers
(P \ 0.001).
Fig. 1 CONSORT diagram
362 Breast Cancer Res Treat (2013) 138:359–368
123

Node positivity was higher in symptomatic cancers
(35%) compared with SDBC (21%: P \ 0.001: Table 1).
The SDBCs were smaller (P \ 0.001), but no difference in
grade, ER or PR status was found (Table 1). Adjuvant
chemotherapy was given to 13% of SDBC and 30% of
symptomatic cancers. Distant recurrence was higher in
symptomatic (19.9% at 10 years) compared with SDBC
(7.9%) (P \ 0.001). Amongst SDBCs, regardless of grade
or ER status, only 13 out of 536 (Kaplan–Meier adjusted
percentage 2.5%) women with small tumours (\15 mm)
Table 2 Univariate and
multivariate analysis of breast
cancer survival
Univariate and multivariate
analysis of breast cancer
survival indicating mode of
detection, size, grade, ER
positivity and node status
independently predicted
survival. Ki67 and HER2 were
not available in the early years,
and the number of values is less
Variables (n = 1475) Univariate analysis Multivariate analysis
Hazard ratio (95% CI) P-value Hazard ratio (95% CI) P-value
Mode of detection
Symptomatic 1 1
Screen detected 0.31 (0.23–0.42) \0.001 0.42 (0.31, 0.57) \0.001
Size
\15 mm 1 1
15–25 mm 4.22 (2.85–6.24) \0.001 2.15 (1.43–3.25) \0.001
[25 mm 12.2 (8.05–18.5) \0.001 4.11 (2.62–6.46) \0.001
Grade
I 1 1
II 3.99 (2.16–7.36) \0.001 2.98 (1.61–5.54) 0.001
III 10.2 (5.62–18.5) \0.001 5.90 (3.20–10.8) \0.001
Node status
Negative 1 1
Positive (1–3 nodes) 4.19 (3.01–5.84) \0.001 2.43 (1.71–3.44) \0.001
Positive (4? nodes) 14.0 (9.83–20.1) \0.001 4.87 (3.29–7.20) \0.001
ER status
Negative 1 1
Positive 0.58 (0.43–0.78) \0.001 0.68 (0.50–0.92) 0.012
PR status
Negative 1
Positive 0.60 (0.44–0.81) 0.001
HER2 status (n = 786)
0 1
1 0.81 (0.44–1.49) 0.49
2 0.94 (0.53–1.65) 0.82
3 2.42 (1.33–4.42) 0.004
Age
Each 10 year increase 0.90 (0.66–1.22) 0.49
Ki67 (n = 1041)
Each 10 unit increase 1.47 (1.33–1.63) \0.001
Ki67 \ 20 1
Ki67 C 20 3.63 (2.30–5.72) \0.001
Chemotherapy (n = 1418)
No 1
Yes 6.47 (4.85–8.63) \0.001
NPI
Excellent 1
Good 5.17 (1.55–17.2) 0.007
Moderate I 14.1 (4.41–45.3) \0.001
Moderate II 36.2 (11.3–116) \0.001
Poor 89.3 (28.1–284) \0.001
Breast Cancer Res Treat (2013) 138:359–368 363
123

had evidence of distant recurrence by 60 months compared
with 20/217 (9.7%) symptomatic cancers (Table 2).
Epithelial proliferation
The Ki67 scores were lower in SDBC (see Table 3:
P = 0.001). Even in grade III cancers, SDBC ER positive
tumours (n = 137) had a mean Ki67 of 27.4% (range
5.8–53.1%) compared with 46.3% (range 12.3–78.9%) in
symptomatic cancers (P \ 0.001). In both symptomatic
and SDBC, higher epithelial proliferation (Ki67 score) was
associated with earlier distant recurrence (P = 0.001 and
P = 0.041, respectively) and breast cancer mortality at
5 years (P = 0.005 and P \ 0.001, respectively).
For SDBCs, there was a reduced risk of mortality for ER
positive cancers compared with ER negative tumours
(P = 0.003; log-rank test).
Table 3 NPI index score and mortality in SDBC and symptomatic cancers—ER positive patients only
Index score Screened cohort
N (%) Ki67%
mean (SD)
Grade III
(%)
Node
positive
(%)
Chemo
(%)
10-year distant
recurrence
% (CI)
10-year breast
cancer mortality
% (CI)
5-year overall
mortality
EPG 156 10.7 0 0 0 4.8 0 1.3
(23.0) (4.7) (1.2–8.4)
GPG 256 20.5 0 12 1 5.7 2.6 1.2
(37.3) (8.7) (2.7–8.7) (0.2–5.0)
MPG1 175 24.8 64 23 9 7.4 6.4 2.4
(25.8) (9.7) (3.2–11.6) (2.0–10.8)
MPG2 60 27.5 77 58 38 8.7 21.2 6.7
(8.0) (9.0) (1.3–16.1) (9.0–33.4)
PPG 30 27.5 93 100 89 46.9 49.2 13.3
(4.4) (6.2) (22.9–70.9) (26.6–71.8)
Total 677 20.6 28 20 10 7.5 6.8 2.6
(9.9) (5.3–9.7) (4.6–9.0)
Index score Symptomatic cohort
N (%) Ki67%
mean (SD)
Grade III
(%)
Node
positive
(%)
Chemo
(%)
10-year distant
recurrence
% (CI)
10-year breast
cancer mortality
% (CI)
5-year
overall
mortality
EPG 94 14.9 0 0 0 7.8 1.1 1.1
(20.4) (5.0) (2.2–13.4) (0–3.3)
GPG 132 31.4 0 8 8 14.7 9.3 3.8
(28.6) (12.5) (8.2–21.1) (3.5–15.1)
MPG1 116 40.8 41 36 26 19.4 17.6 8.0
(25.2) (14.9) (11.6–27.2) (10.0–25.2)
MPG2 64 40.8 52 89 82 30 39.8 22.4
(13.9) (13.4) (16.6–43.4) (26.6–53.0)
PPG 55 36.4 76 100 76 59.5 66.4 31.5
(11.9) (15.3) (42.9–76.1) (52.8–80.0)
Total 461 33.7 27 36 29 20.7 20.4 10.1
(15.6) (16.7–24.7) (16.4–24.4)
Log-rank test (distant recurrence): EPG P = 0.33, GPG P = 0.001, MPG1 P = 0.005, MPG2 P = 0.009, PPG P = 0.28
Log-rank test (breast cancer mortality): EPG P = 0.20, GPG P = 0.001, MPG1 P = 0.001, MPG2 P = 0.034, PPG P = 0.015
NPI Index Score and mortality in SDBC and symptomatic cancers in ER positive cancers only. Ki67 was lower for SDBC compared with
symptomatic cancers in every NPI group. Differences in survival for NPI groups for distant recurrence and mortality were seen for SDBC
compared with symptomatic cancers for all scores except in the EPG
364 Breast Cancer Res Treat (2013) 138:359–368
123
Comparison of Nottingham prognostic index groups
The SDBC had a better prognosis despite less chemother-
apy use (Table 3) in every NPI group (except the Excellent
Prognostic Group [EPG]) compared with symptomatic
cancers. Cancer survival in SDBC was the equivalent of
one NPI group better than symptomatic cancers (Fig. 3). In
the MPG1, 26% of ER positive symptomatic cancers had
chemotherapy but mortality at 5 years was 8%, whereas
mortality of 2% at 5 years occurred in MPG-1 SDBC
despite only 9% receiving chemotherapy (P = 0.001).
Calculating the NPI for the 6737 operable SDBCs
diagnosed and submitted to the ABS Audit in 2001–2002,
similar 5 year relative survival and breast cancer mortality
were found for equivalent NPI scores to those found for
SDBCs diagnosed in Manchester (Table 3). Chemotherapy
use in the SDBC in NPI groups submitted to the ABS Audit
(Table 4), revealed minimal use in both EPG and Good
Prognostic Group (GPG) cancers. Even in the MPG1
group, chemotherapy use was low, considering 40% were
grade III, 33% node positive and 25% ER negative but
given the 4% breast cancer-specific mortality at 5 years,
the effect of chemotherapy on mortality will have been less
than 1%.
Improvements in survival have occurred for U.K SDBC
since 1990 due to the increased use of adjuvant endocrine
therapy. Relative survival at 5 years is now 97.2% in
SDBC compared to 77.6% in symptomatic cancers, but this
improved survival has mainly been achieved by combined
chemoendocrine therapy of the MPG2 and PPG cancers
(19% of SDBC population: Table 4).
Discussion
Breast cancer survival has improved dramatically in the
UK but remains poorer than many European countries
because of delayed diagnosis and late stage at diagnosis [9,
22]. Chemotherapy is advised by oncologists using the St
Gallen guidelines or NPI [10, 11, 14] on the basis of
pathological size, grade and node status [10, 11, 14]. If
chemotherapy is used according to guidelines derived from
symptomatic cancer trials, up to 40% of women with
SDBC would be candidates for chemotherapy [10, 11, 14].
Molecular profiling of cancers identifies ER positive
patients who do not benefit from the addition of chemo-
therapy to endocrine therapy [23]. Cancers detected by
breast screening had a reduced likelihood of death from
breast cancer at 10 years (RR 0.57) in three Scandinavian
and a Dutch study [1, 3, 6, 24]. A Norwegian study claimed
that most of the reduction in mortality was from adjuvant
therapy, not screening, based on short follow-up (average
2 years) and has been criticised, as most early deaths from
breast cancer occur in ER negative cancers patients in
whom adjuvant chemotherapy is mandatory (see Fig. 2).
The benefit of SDBC detection is unlikely to be seen with
such a short follow-up and will be significantly underesti-
mated in the context of this study [25]. The Dutch study
[23] found that despite 91% of their SDBC having no
adjuvant or hormone therapy alone, diagnosis by screening
independently predicted survival.
Cancer detection by screening was an independent
predictor of survival on multivariate analysis. In view of
claims of over-diagnosis of breast cancer by screening, it is
imperative that resources are not used to over-treat cancers
detected. Despite less adjuvant chemotherapy being given,
similar aged SDBC had a lower mortality compared with
symptomatic cancer patients in all prognostic factor sub-
groups, underlining that ER positive SDBC do not benefit
significantly from chemotherapy, confirming findings from
Holland [23].
The overall mortality (survival) of Manchester SDBCs
is similar to the National SDBC survival figures [17] and
the Scandinavian and Dutch studies [3, 6, 23]. National
SDBC survival figures from 2001 to 2002 show a 96.5%
overall survival at 10 years [17]. To avert arguments about
lead time bias, we matched groups for size, grade ER and
Fig. 2 Smoothed annual rate of mortality in ER positive and negative
SDBC and symptomatic breast cancers ER positive, SDBC had a low
5 year annual mortality, ranging between 0.1% and 1.8% at
60 months which was significantly lower than symptomatic ER
positive (blue line). ER negative breast cancers that were symptom-
atic had a significantly higher annual mortality rate than SDBC that
were ER negative. The overall difference between SDBC which were
ER positive and the other groups is significant (P = 0.001).
Chemotherapy use was 13% in the SDBC and 30% in the
symptomatic population
Breast Cancer Res Treat (2013) 138:359–368 365
123

node status using the NPI but the observed survival dif-
ferences remained (Table 3). The excellent survival in size
B15 mm ER positive, node negative breast cancer occur-
red in the absence of chemotherapy. The excellent survival
of SDBC in the Excellent Prognostic Group (EPG), GPG
and MPG1 needs to be recognised when deciding adjuvant
therapy. No convergence in survival was evident after
10 years, indicating the difference is unlikely to be due to
lead time bias; a similar finding to others [1, 6, 7]. More-
over, the EBCTCG metaanalysis for the 50–70 year old
age groups shows a 3–5% absolute reduction in breast
cancer mortality in the first 5 years after chemotherapy but
no increased benefit at 15 years; thus even if there is a lead
time bias of 5 years in SDBC, there is no published evi-
dence chemotherapy will affect survival beyond the lead
time. The NHSBSP did not involve oncologists at its
inception because it was only deemed to operate until
cancer diagnosis. Oncologists need to appreciate the better
survival of SDBCs to avoid over-treatment. Effectively,
SDBC MPG1 survival is equivalent to symptomatic GPG
cancers.
Since this data is from several cohort studies, not ran-
domized trials, its interpretation needs some circumspec-
tion, but given the high cure rate in ER positive,
mammographically detected cancers, clinical trials assess-
ing the role of chemotherapy in this setting are unlikely as
they would require a large sample size, at huge economic
cost and would have a high likelihood of returning a neg-
ative result where the endpoint was mortality or recurrence.
Chemotherapy works within 5 years of administration
by killing proliferating cells, reducing the early peak of
mortality seen in symptomatic cancers (Fig. 2). Although
grade takes account of tumour mitotic rate, within grades,
widely different epithelial proliferation rates were seen.
The proliferation rate (Ki67) was a predictor of survival
and was lower in SDBC (i.e. they are slower growing) than
symptomatic cancers. The ER positive SDBC had no early
peak in mortality and a lower annual hazard ratio of death
compared with the ER negative SDBC or symptomatic
cancers. The lower epithelial proliferation in SDBC pro-
vides a biological rationale for their lower mortality, and a
reason why chemotherapy would be less effective [18]. The
21-gene Recurrence Test for ER positive, HER2 negative
breast cancer identifies patients who do not benefit from
chemotherapy on the basis of a high ER/PR score and a low
proliferation score [11].
Most SDBCs, had a Ki67 of\20%, were slow growing
and thus unlikely to benefit from chemotherapy. Since the
reduction in mortality benefit of chemotherapy occurs
within 5 years of treatment, administering chemotherapy to
ER positive SDBC will have no effect on mortality as there
is no early mortality or recurrence peak (Fig. 2).
The addition of chemotherapy to Tamoxifen, in ER
positive, node positive postmenopausal breast cancers led
to reduced mortality, but the benefits were largely confined
to heavily node positive and women\65 years of age [12].
This confirms no benefit will occur in small, node negative,
or less than 4 node positive, ER positive SDBC. Clinical
signs such as a lump are associated with invasiveness,
faster growth and increased mortality [3, 6]. Almost 50%
of SDBC are impalpable, requiring excision by a locali-
zation technique and have a better survival [1–3, 6].
In Manchester, chemotherapy was given to the Poor
Prognostic Groups, until the EBCTCG report in 1998
supporting its wider use in symptomatic cancers [10].
Overall, SDBCs had a survival of 90.7% at 10 years and
Table 4 NHSBSP and ABS at BASO breast screening audit data for invasive SDBCs diagnosed in 2001/2002
NPI 1990–1991 1996–1997 N 2001–2002 Grade
III (%)
Node
positive
(%)
Chemo
(%)
5 year relative
survival
2001–2002
5 year breast cancer
cause specific
mortality (%)
EPG 102.1 100.5 1774 0 0 1 102.2% 0
\2.4 (100.7, 103.6) (99.3–101.7) (101.5, 102.9)
GPG 98.2 98.6 2397 0 10 5 100.1% 1
2.41–3.4 (96.4, 100.1) (97.3–99.9) (99.2, 100.9)
MPG1 93.3 94.2 1470 40 33 32 96.7% 4
[3.4–4.4 (90.5, 96.1) (92.2–96.3) (95.2, 98.1)
MPG2 79.9 87.4 696 52 74 56 92.0% 9
4.41–5.4 (74.8, 85.1) (84.0–90.8) (89.4, 75.3)
PPG 55.8 71.5 400 69 100 64 70.4% 28
[5.4 (47.9, 63.6) (65.5–77.5) (65.4, 75.3)
ABS at BASO Audit data for SDBC diagnosed in 2001/02, NPI scores predicted overall mortality at 5 years. Recurrence and mortality rate
estimates derived from Kaplan–Meier curves. Chemotherapy use in tumours with similar scores 2001/2002 indicates under treatment in MPG2
and PPG nationally. Note improvements in survival in SDBC nationally have mainly come from improved treatment of MPG2 and PPG cancers
by chemo and endocrine therapy
366 Breast Cancer Res Treat (2013) 138:359–368
123

96.4% at 5 years (a figure similar to the 96.5% 5 year
survival of SDBCs in the ABS Audit).
For all groups, where the mortality from breast cancer is
less than 10%, absolute reduction in mortality (1%) pro-
duced by chemotherapy will be outweighed by chemo-
therapy induced morbidity (1–4%) [12, 13]. The lack of
survival benefit has been demonstrated in small, ER posi-
tive SDBCs regardless of grade or node status as 10-year
survival was 99% in the absence of chemotherapy.
Selection criteria for type of adjuvant therapy
The programme Adjuvant! Online is used in the U.S. [11]
and recommended by NICE in the U.K., for making deci-
sions about the kind of adjuvant therapy to prescribe. Using
this programme, a grade III, 15 mm node negative or a
grade II node positive breast cancer would have a survival
of 76.6–80.4% at 10 years, which in an ER positive patient
is improved by approximately 4% using adjuvant endo-
crine therapy. This is in keeping with the survival of the
symptomatic ER positive patients in Manchester. In ER
positive SDBCs (10% received chemotherapy), there was a
breast cancer mortality of 1.7% at 5 years and 6.8% at
10 years, which is three-fold less than that suggested by
Adjuvant! Online. The 5 year data for survival for MPG1
in the ABS Audit shows a mortality of 4%, which is three-
fold lower than expected but consistent with Scandinavian
SDBC survival. Similar data were found in Holland, where
Adjuvant! Online underestimated SDBC survival by 3–5%
[23] in the absence of chemotherapy.
The survival of SDBC, for identical ‘anatomical factors’
(grade, size and node status), is better than symptomatic
cancers, and we must avoid over-treating these cancers. For
ER positive, HER2 negative breast cancer, adjuvant
endocrine therapy is all that is required for those in NPI
EPG, GPG and MPG1. Since this constitutes 70% of
SDBC, the result of treating these patients who are ER
positive and HER2 negative with chemotherapy, in terms
of significant morbidity, has to be weighed with the eco-
nomic costs and the lack of benefit of the treatment.
Consensus guidelines about the management of SDBC
need to be drawn up internationally.
Molecular profiling of breast cancers has been pro-
posed as a method to identify tumours at the risk of early
recurrence to select for chemotherapy [25]. Oncotype DX
uses ER, PR, HER2 and Ki67 to identify a low-risk group
with a recurrence of 14% at 10 years who do not benefit
from chemotherapy, but ER positive SDBC in GPG/
MPG1 have a 7% mortality at 10 years, so its expense
(around £2500 per patient) would not be justified where it
will not add further information in a population at low
risk of mortality.
The SDBC overexpressing HER2 had a higher mortality
(RR 2.84) but the effect of HER2 expression on mortality
was non-significant after adjusting for node status, grade
and tumour size. The SDBCs have a better survival than
symptomatic cancers for all grades, node and ER status.
The individualisation of therapy for breast cancer is now
possible on the basis of mode of detection, ER status and
NPI score at little extra cost.
The need for chemotherapy and hormonal therapy in
SDBC can be targeted with consequent improvement in
quality of life and reduced costs to the NHS.
Acknowledgments The authors appreciate and acknowledge the
contribution of the Association of Breast Surgeons at the British
Association of Surgical Oncology membership for contributing
patients to the ABS at BASO Audit and the contribution of the
members of the NHS Cancer Screening Programmes for the data. The
Follow-up numbers Symptomatic Months 0 12 24 36 48 60 72 84 96 108 120 GPG 132 132 132 131 130 121 108 98 77 58 29 MPG1 116 116 115 115 110 100 88 81 66 53 30 MPG2 64 64 64 60 56 48 37 34 27 17 12 PGP 55 54 53 46 44 38 17 14 12 8 6
SDBCMonths 0 12 24 36 48 60 72 84 96 108 120 GPG 256 156 156 255 253 236 224 218 184 155 115 MPG1 175 175 174 172 170 158 150 136 116 92 60 MPG2 60 60 59 59 57 54 48 44 35 22 13 PGP 30 30 30 29 29 28 19 19 16 12 6
Fig. 3 Breast cancer mortality (ER positives) follow-up numbers.
Proportion of breast cancer survival and NPI scores for ER positive
SDBC and symptomatic cancers plotted by NPI score for SDBC and
symptomatic breast cancers. *Log rank test. (P \ 0.001) Calculation
of NPI between groups revealed, in every group (except the EPG),
that SDBC had a better prognosis despite less chemotherapy use.
Kaplan–Meier curve showing breast cancer survival plotted by NPI.
*Log rank test. (P \ 0.001). Note SDBC have a survival approxi-
mately one NPI group better than symptomatic cancer
Breast Cancer Res Treat (2013) 138:359–368 367
123

authors thank the South Manchester Multi-Disciplinary Team mem-
bers who provided surgical treatment for these patients and the
radiologists who provided diagnosis and detection of the breast
cancers.
Funding Funding was not obtained to carry out this study.
Conflict of interest The authors declare they have no competing
interests.
References
1. Nystrom L, Andersson I, Bjurstam N, Frisell J, Nordenskjold B,
Rutqvist LE (2002) Long-term effects of mammography
screening: updated overview of the Swedish randomised trials.
Lancet 359(9310):909–919 Review. Erratum in: Lancet 2002
Aug 31;360(9334):724
2. Duffy SW, Tabar L, Chen HH, Holmqvist M, Yen MF, Abdsalah
S, Epstein B, Frodis E, Ljungberg E, Hedborg-Melander C,
Sundbom A, Tholin M, Wiege M, Akerlund A, Wu HM, Tung
TS, Chiu YH, Chiu CP, Huang CC, Smith RA, Rosen M, Sten-
beck M, Holmberg L (2002) The impact of organised mam-
mography service screening on breast carcinoma mortality in
seven Swedish counties. Cancer 95(3):458–469
3. Tabar L, Duffy SW, Vitak B, Chen HH, Prevost TC (1999) The
Natural History of Breast Carcinoma. What have we learned from
screening? Cancer 86:449–462
4. Blamey RW, Wilson ARM, Patnick J (2000) ABC of breast
diseases—screening for breast cancer. BMJ 321:689–693
5. Crisp WJ, Higgs MJ, Cowan WK, Cunliffe WJ, Liston J, Lunt
LG, Peakman DJ, Young JR (1993) Screening for breast cancer
detects tumours at an earlier biological stage. Br J Surg
80(7):863–865
6. Joensuu H, Lehtimaki T, Holli K, Elomae L, Turpeenniemi-Hu-
janen T, Kataja V, Anttila A, Lundin M, Isola J, Lundin J (2004)
Risk for distant recurrence of breast cancer detected by mam-
mographic screening or other methods. JAMA 292:1064–1073
7. Dawson SJ, Duffy SW, Blows FM, Driver KE, Provenzano E,
LeQuesne J, Greenberg DC, Pharoah P, Caldas C, Wishart GC
(2009) Molecular characteristics of screen-detected vs. symp-
tomatic breast cancers and their impact on survival. Br J Cancer
101(8):1338–1344
8. Lawrence G, Wallis M, Allgood P, Nagtegaal ID, Warwick J,
Cafferty FH, Houssami N, Kearins O, Tappenden N, O’Sullivan
E, Duffy SW (2009) Population estimates of survival in women
with screen-detected and symptomatic breast cancer taking
account of lead time and length bias. Breast Cancer Res Treat
116(1):179–185 Epub 2008 Jul 12
9. Møller H, Sandin F, Bray F, Klint A, Linklater KM, Purushotham
A, Robinson D, Holmberg L (2010) Breast cancer survival in
England, Norway and Sweden: a population-based comparison.
Int J Cancer 127(11):2630–2638
10. Early Breast Cancer Trialists’ Collaborative Group (2005) Effects
of chemotherapy and hormonal therapy for early breast cancer on
recurrence and 15 year survival: an overview of the randomised
trials. Lancet 365:1687–1717
11. Ravdin PM (1995) A computer based program to assist in adju-
vant therapy decisions for individual breast cancer patients. Bull
Cancer 82 Suppl 5:561s-564s. http://www.adjuvantonline.com
12. Albain KS, Barlow WE, Ravdin PM, Farrar WB, Burton GV,
Ketchel SJ, Cobau CD, Levine EG, Ingle JN, Pritchard KI,
Lichter AS, Schneider DJ, Abeloff MD, Henderson IC, Muss HB,
Green SJ, Lew D, Livingston RB, Martino S, Osborne CK (2009)
Breast Cancer Intergroup of North America. Adjuvant chemo-
therapy and timing of tamoxifen in postmenopausal patients with
endocrine-responsive, node-positive breast cancer: a phase 3,
open-label, randomised controlled trial. Lancet 374(9707):2055–
2063
13. Levine MN, Bramwell VH, Pritchard KI, Norris BD, Shepherd
LE, Abu-Zahra H, Findlay B, Warr D, Bowman D, Myles J,
Arnold A, Vandenberg T, MacKenzie R, Robert J, Ottaway J,
Burnell M, Williams CK, Tu D (1998) Randomized trial of
intensive cyclophosphamide, epirubicin, and fluorouracil che-
motherapy compared with cyclophosphamide, methotrexate, and
fluorouracil in premenopausal women with node-positive breast
cancer. National Cancer Institute of Canada Clinical Trials
Group. J Clin Oncol 16(8):2651–2658
14. Scottish Cancer Therapy Network SIGN Guidelines for breast
cancer women Section 10 Adjuvant Systemic Therapy. Scottish
Intercollegiate Guidelines Network 1998 Breast Cancer. SIGN,
Edinburgh
15. Blamey R (1996) The design and clinical use of the Nottingham
Prognostic Index in breast cancer. Breast 5:154–167
16. Feldman M, Stanford R, Catcheside A, Stotter A (2002) The use
of a prognostic table to aid decision making on adjuvant therapy
for women with early breast cancer. EJSO 28:615–619
17. An audit of SDBCs for the year of screening April 2001 to March
2002. Association of Breast surgery at BASO (British Associa-
tion of Surgical Oncology) 2nd April 2003. NHS Cancer
Screening Programmes 2003 (www.cancerscreening.nhs.uk)
18. Mathieu MC, Rouzier R, Llombart-Cussac A, Sideris L, Kos-
cielny S, Travagli JP, Contesso G, Delaloge S, Spielmann M
(2004) The poor responsiveness of infiltrating lobular breast
carcinomas to neoadjuvant chemotherapy can be explained by
their biological profile. Eur J Cancer 40(3):342–351
19. Elston CW, Ellis IO (1991) The value of histological grade in
breast cancer: experience from a large study with long-term
follow-up. Histopathology (Oxf) 19:403–410
20. Holland PA, Walls J, Boggis CR, Knox F, Baildam AD, Bundred
NJ (1996) A comparison of axillary node status between cancers
detected at the prevalence and first incidence breast screening
rounds. Br J Cancer 74(10):1643–1646
21. Boland G, Butt IS, Prasad R, Knox WF, Bundred NJ (2004)
COX-2 expression is associated with an aggressive phenotype in
ductal cancer in situ. Br J Cancer 90:423–429
22. Coleman MP, Forman D, Bryant H, Butler J, Rachet B, Maringe
C, Nur U, Tracey E, Coory M, Hatcher J, McGahan CE, Turner
D, Marrett L, Gjerstorff ML, Johannesen TB, Adolfsson J, Lambe
M, Lawrence G, Meechan D, Morris EJ, Middleton R, Steward J,
Richards MA, the ICBP Module 1 Working Group (2011) Cancer
survival in Australia, Canada, Denmark, Norway, Sweden, and
the UK, 1995–2007 (the International Cancer Benchmarking
Partnership): an analysis of population-based cancer registry data.
Lancet 377:127–138
23. Mook S, Van’t Veer LJ, Rutgers EJ, Ravdin PM, van de Velde
AO, van Leeuwen FE, Visser O, Schmidt MK (2011) Indepen-
dent prognostic value of screen detection in invasive breast
cancer. J Natl Cancer Inst 103:585–597
24. Howell A, Cuzick J, Baum M, Buzdar A, Dowsett M, Forbes JF,
Hoctin-Boes G, Houghton J, Locker GY, Tobias JS (2005) ATAC
trialists’ group. Results of the ATAC (Arimidex, Tamoxifen,
Alone or in Combination) trial after completion of 5 years’
adjuvant treatment for breast cancer. Lancet 365:60–62
25. Kalager M, Zelen M, Langmark F, Adami H (2010) Effect of
screening mammography on breast-cancer mortality in Norway.
N Engl J Med 363:1203–1210
368 Breast Cancer Res Treat (2013) 138:359–368
123
![Evolving role of chemotherapy in castration-resistant prostate … · 2019-07-12 · age [101]; therefore, we are dealing with a geriat-ric population. For patients with symptomatic](https://static.fdocuments.us/doc/165x107/5f40526d40d9627dc93c24c3/evolving-role-of-chemotherapy-in-castration-resistant-prostate-2019-07-12-age.jpg)