Arboviral infections: clinical syndromes and pathogenicity...
48
CLINICAL SYMPTOMS AND PATHOGENICITY IN HUMANS H. Zeller, MC Georges, I. Schuffenecker, I. Marendat, S. Murri National Reference Centre for Arboviruses and Viral Haemorrhagic Fevers, WHO Collaborating Centre, Institut Pasteur, Lyon, France Luxemburg 20-21 January 2003
Transcript of Arboviral infections: clinical syndromes and pathogenicity...

CLINICAL SYMPTOMS AND PATHOGENICITY IN HUMANS
H. Zeller, MC Georges, I. Schuffenecker,I. Marendat, S. Murri
National Reference Centre for Arboviruses and ViralHaemorrhagic Fevers, WHO Collaborating Centre,
Institut Pasteur, Lyon, France
Luxemburg 20-21 January 2003

CLINICAL SYMPTOMS AND PATHOGENICITY IN HUMANS
Main Arboviruses affecting humans known to circulate in Europe
• TICK BORNE ENCEPHALITIS• CRIMEAN CONGO HAEMORRHAGIC FEVER• WEST NILE• SANDFLY FEVERS NAPLES/SICILIAN• TOSCANA• SINDBIS OCKELBO• TAHYNA • LOUPING-ILL ….

CLINICAL SYMPTOMS AND PATHOGENICITY IN HUMANS
Main syndromes
•Inapparent diseases•Influenza-like illness, dengue-like illness•Febrile disease with rash and arthralgia•Encephalitis, meningitis•Haemorrhagic fever
•Fatality rate (clinical forms): 0-25%

Diseases are inconstant :Emerging part of the iceberg
…Most frequentlyasymptomatic infections
+++

• Incubation period: 2-10 days
Mild dengue-like illness of sudden onset
•fever, lymphadenopathy, headache, abdominal
pain, vomiting, rash, conjunctivitis, eye pain,
anorexia ……
•Duration 3-6 days
Arboviral infection

Main Arboviruses affecting humans known to circulate in Europe
• SANDFLY FEVERS NAPLES/SICILIAN (high fever, headache, joint pains, malaise, and occasionally nausea and vomiting and drowsiness)
• TOSCANA (to aseptic meningitis)
• SINDBIS OCKELBO (fever with rash and polyarthralgia) Reported long lasting athralgia
• TAHYNA (mild febrile illness to aseptic meningitis) ….

TICK BORNE ENCEPHALITIS
Flavivirus
Far Eastern form
Central European form

TICK BORNE ENCEPHALITISTBE infection rate of ticks in a risk region
0.1-5%
Bite
Non symptomaticIllness
Immunity70-90%
10-30% Prodromal phasewith flue-like symptoms
Myelitis/radiculitis 13%
Meningitis 45%
Meningoencephalitis 42%
Recovery70%
Transient/lastingdamage 30%
Death0.5-2%
Oschmann P et al, 1999

TICK BORNE ENCEPHALITISLITHUANIA Kaunas Univ hosp
250 consecutively hospitalized patients with CNS infections (June 1998-May 1999)
133 with TBE infection (53.2 %)
Fever 98.9%General malaise 61.7%Fatigue 62.8%Headache, back limb aches 54.3%Catarrhal symptoms 27.7%
Mickiene et al, CID, 2002, 35:650

TICK BORNE ENCEPHALITISLITHUANIA
133 patients with TBE infectionDisease mild meningeal 43.6%
moderate 43.6% severe 12.8%
Paralytic disease : 3.8%Cranial nerve injury: 5.3%
Fatality rate 0.75%
Mickiene et al, CID, 2002, 35:650Correlation: severity of illness - age r=0.290; P=.001

TICK BORNE ENCEPHALITISLITHUANIA
133 patients with TBE infectionMale 55% 42 yrs Female 45% 49 yrsTick bite: 68%Activities : Forest activity 4%
77 cases: incomplete recovery at 12 weeks34% with objective neurological signs
56 cases with incomplete recovery at 1 year Mickiene et al, CID, 2002, 35:650

TICK BORNE ENCEPHALITIS
Mickiene et al, CID, 2002, 35:650
% of patientsNeurological symptom Acute stage 12 weeks 1 year after
n=133 n=120 n=117
ataxia 26.3 5.0 6.0dysphasia 3.8headache 95.5 31.7 20.5tremor 21.8 15.0 8.5emotional instability 15.0 23.3 18.8decreased concentration 11.3 20.0 15.4decreased memory 9.8 20.8 19.7altered consciousness 18.8hemiparesis 2.6 3.3 3.4cranial nerve paralysis 5.3 0.8spinal nerve paralysis 3.8 3.3 2.6

TICK BORNE ENCEPHALITIS
Critsun el al, J Gen Virol 2003, 77:25
PATHOGENICITY
Case: one patient who died of progressive (2 years) form of TBE (far eastern form) 10 years after being bitten by a tick.
Virological study: Comparative amino-acid alignements
2 amino-acid substitution T277->V and E279->G with theNS1 domain probably responsible for the altered oligomerization of the virus NS1.
Conclusion: Possible increased pathogenicity of the latent virus following spontaneous mutagenesis

WEST NILE

WEST NILE
• Mostly inapparent forms
• Mild form: fever, headache, myalgia…
• Meningitis, meningo-encephalitis or
encephalitis in less than 15%
• others: hepatitis, pancreatitis, myocarditis

Romania 1996
August to October, Bucarest• 835 patients with suspected CNS infection • 393 confirmed patients ( 77%) / 509 tested
352 with acute central nervous system infection
Meningitis 40%Meningo encephalitis 44%Encephalitis 16%
17 (4,3%) fatal cases > 50 years

Romania 1996
August to October, Bucarest
Symptomatic / Non symptomatic forms
1 / 140-320 infections

HUMAN CASES: August-October 2000
cases : 233 hospitalizedDeaths 33 (14.1%)Age 80 54 - 95 (32 patients > 68 yrs)
encephalitis: 57.9%
meningitis 15.9%
febrile disease 24.4%
Israel 2000

HUMAN CASES: August-October 2000
• Risk factors
• Age > 70 years : encephalitis 80% in > 70 yrs41% in < 70 yrs
• level consciousness
• anemia
Israel 2000

5264 HORSES
504 INFECTED = 9.6%
76 ENCEPHALITIS 1.4%
21 EUTHANASIED84.9%
NON SYMPTOMATICOR UNDETECTED DISEASE
4.2% †
15.1%
WEST NILE France 2000

USA New York 1999
Meningitis/meningoencephalitis 62%Meningitis 32%Complete flaccid paralysis 10%
• Confused with Guillain-Barre syndrome• Poliomyelitis-like syndrome
• Other reportsataxia, extrapyramidal signs, cranial nerve abnormalities, myelitis, optic neuritis, seizures
From L. Petersen

Intrauterine West Nile Virus Infection New York Sept 2002
• Index case: woman delevring a live infant 5 weeks after a WN meningoencephalitis.
• Baby with a bilateral chorioretinitis, severe cerebral abnormalities, including severe bilateral white-matter loss in the temporal and occipital lobes and cystic change in one temporal lobe consistent with focal cerebral destruction.
• Specific IgM in infant blood and CSF
Source: MMWR 2002

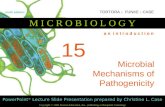
0.1
WN-Romania-1996MWN-Volgograd-1999
WN-Kenya-1998WN-Senegal-1993WN-Italy-1998
WN-Morocco-1996WN-France-2000WN-New-York-1999WN-Israel-1998
WN-Tunisia-1997WN-Algeria-1968
WN-France-1965WN-Egypt-1951
WN-Romania-1996HWN-Cote d’Ivoire-1981
Kunjin-AustraliaWN-India-1980
WN-C.Afr.Rep-1983WN-UgandaWN-Uganda
WN-KenyaWN-Madagascar-1988
JE
Lineage 1
Lineage 2
West Nile: Phylogenetic tree based on nucleic sequence data of E-glycoprotein genefragment of 245 bp
Source: Murgue et al, 2001

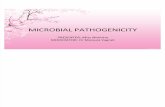
KUNJIN (D00246)
Human RUSSIA 1999 (AF317203)
Cx. pipiens ROMANIA 1997 (AF130362)
WN 0304 ISRAEL 2000WN 0303 ISRAEL 2000
NEW YORK (AF194117)
Gull ISRAEL 1999Horse NY 1999 (AF260967)
Cx. pipiens Conn. 1999 (AF206518)
Human NY 1999 (AF202541)
Flamingo NY 1999 (AF196835)
WN 0043 ISRAEL 2000WN 0247 ISRAEL 2000
Phylogenetic analysis
1662 nt from the PrM,
M, E gene with KUN primers
0.01
Source: Hindiyed et al, EID 2001

Beasley DWC et al, Virology 2002 296 17
Variation in WN virus virulence (1)
Mouse neuroinvasive phenotype of WN virus strainsvaries depending upon virus genotype
Kunjin and Indian strains less evolved strains on lineage II non neuroinvasive or highly attenuated on mice
Neuroinvasive clades branch more distanlty from the rootof the tree
WEST NILE PATHOGENICITY

Beasley DWC et al, Virology 2002 296 17
Variation in WN virus virulence (2)
Lack of age-related resistance to infection in mice for some highly invasive strains
Relationship with glycosylation site?
• neuroinvasive strains EGY50 and SEN 90 with lackof a glycosylation site
IP LD50 10-fold higher than related neuroinvasive strains which encoded the glycosylation site
WEST NILE PATHOGENICITY

WEST NILE PATHOGENICITY
Identification of genes who play a key role in
outcome determination of host-virus interactions
in mice ….
Mashimo T et al, PNAS 2002
Genetic basis of host susceptibility to WN viral infection

Novel Modes of West Nile Virus Transmission, 2002
• Transplanted organs• Transfused blood• Breast milk• Percutaneous, occupational exposure
Lyle R. Petersen CDCLyle R. Petersen CDC

InfectionIllness onset
D4 – D6 illness 1Y after illness
Viremia
IgM
IgG
D14 – D21 illness
Con
cent
ratio
nRevised timing of WNV Viremia and
Antibody Response
L. Petersen, CDC

Crimean-Congo Haemorrhagic Fever
CCHF

KOSOVO
CCHF 2000 / 2001

Disease
May 28: consultation in an outpatient clinicchills, myalgia, nausea, anorexia, vomitingheadache, backhache
Antibiotic therapy: for septic infection?
Day 3: massive hemorrhage with hemathemesis (7-8 times /day)melena, hematuria, metrorrhagia, petechia
Female:17 years-old bitten by a Hyalomma tick on May 2000 in Pristina Kosovo (1)
Drostein et al, J Clin Microbiol 2002, 40 1122

Disease
Day 4 Hospitalization without special isolation measuresfever 39.7°C platelets 30.000/ml bleeding time 120s clotting time 7mn 17s (normal < 6mn)
Day 5 fever 40,1°C, backpain, headachefully oriented patient, …prostrationEpistaxis and gingival bleeding Hemorrhagic conjunctivitisLarge ecchymosis at veinipuncture sites
Female:17 years-old bitten by a Hyalomma tick on May 2000 in Pristina Kosovo (2)
Drostein et al, J Clin Microbiol 2002, 40 1122

Day 8 hemorrhagic diathesis disapear, light residual metrorrhagiaBlood pressure 100/70 mm Hg 60 pulses/mn Recovery
Treatmentsupportive treatment: hydrationno blood transfusion
Nosocomial infections: none
Female:17 years-old bitten by a Hyalomma tick on May 2000 in Pristina Kosovo (3)
Drostein et al, J Clin Microbiol 2002, 40 1122

Kosovska Mitrovica 2000
43 year old female with high fever, headache, nausea, generalized myalgia, disoriented . On day 2 deterioration bleeding from the gastrointestinal tractus
Transferred to Belgrade death a few hours later
The physician who intubated the patient :sick high fever asthenia petechiae, exanthema, pneumonia symptoms, leukopenia, thrombocytopenia
Oral ribavirin treatment : afebrile within 48 h.
CCHF Kosovo
A Papa et al Emerg Inf Dis 2002, 8 852

May July 2001
105 hospitalized suspect cases
30 confirmed cases 24 primairy cases5 secondary cases: 3 deaths
2 nosocomial infectionsone physician, one lab-technician
7 deaths Source: T. Avšič-Županc
CCHF Kosovo

Clinical Features of CCHF (1)Clinical Features of CCHF (1)incubation period: 3 -12 days
1-3 days for tick bite5-6 days for nosocomial or blood exposure
(1-2 days in last Kosovo outbreak 2001)
Sudden onset of fever, malaise, weakness, irritability, anorexia, headache, severe pain in limbs and back, conjunctival injection, hemorrhagic enanthem of soft palate, uvula and pharynx, and a fine petechial rash
Day 3-5 haemorrhage, day 5-14 hepato-renal failure, coma, death
Source: WHO CSR

Clinical Features of CCHF (2)Clinical Features of CCHF (2)
There may be large purpuric areas, bleeding from gums, nose, lungs, uterus and intestine, but in large amounts only in serious or fatal cases, often associated with severe liver damage
Fever persists 5 -12 days (may be biphasic)
Case fatality rate 2% - 50%, convalescence is prolonged
Source: WHO CSR

Clinical Features of CCHF (3)Clinical Features of CCHF (3)
Haemorrhagic phasecutaneous and mucous membrane petechiaespreading cutaneous ecchymosisbleeding from puncture sitesgastrointestinal*, urinary, uterine haemorrhages* sometimes massive haemorrhages
Typically last 5-7 daysAssociated with tachycardia, toxicity, hypotensive and CNS manifestations
Source: WHO CSR

Clinical Features of CCHF (4)Clinical Features of CCHF (4)
EVOLUTIONrecovery:prolonged convalescence with
persistent fatigue and dizziness
DEATHS: Occurred between days 5-14 of illnessHepatorenal failure, severe anemia, shock with pulmonary and cardiac insufficiency
Source: WHO CSR

CCHF : laboratory dataCCHF : laboratory data
LEUCOPENIA, particularly neutropeniaThrombocytopeniaHematocrit increases early then falls downASL, AST levels increasesProteinuria and hematuriaMild azotemia, bilirubine increase
VIREMIA long lasting through the disease
Source: WHO CSR

Treatment of CCHFTreatment of CCHF
Supportive treatmentfluid and electrolytic balancestransfusion, platelets, coagulation factors
Antiviral drugs : ribavirin (Fisher-Hoch SP. 1995 Lancet, 346 (8973): 472-5.
Source: WHO CSR

CCHF : pathogenesisCCHF : pathogenesis
Human : unique host with clinical symptoms

CCHF : pathogenesisCCHF : pathogenesisNot highly cytolyticModest cellular necrosis
Mechanism for haemorrhages not knowClinic evidence of DICHighest incidence of large ecchymoses
Liver: hepatocytes and endothelial cells involvement
Marked clinical improvement at the onset of the immune response

CLINICAL SYMPTOMS OF VHF
Infection Filo RVF CCHF YF DH Lassa AmS HFRS HPS
Incubation 3-10 2-7 2-12 3-7 7-10 >7j >7j >7 >7
Mortality 50-80 0-10 4-30 10-80 1 15 5-50 0-10 50
Haemorrhages ++ ++ +++ ++ + + ++ +Rash ++ + ++ + ++Petechia ++ + +++ ++ ++ ++Ecchymoses + ++ ++ +Melena ++ ++ + +
Shock +++ ++ +++ +++ +++ +++ +++ + ++Involv. Liver + +++ +++ +++ +
kidney + + + ++ + +++ +CNS + ++ + ++ +++
Oedema +++ ++ ++ ++ +++

ARE GENERAL PRACTIONERS AWARE OF
- EUROPEAN ARBOVIRUSES ?
- IMPORTED FROM OUTSIDE EUROPE ?
Information through ENIVD members
Sweden Finland : yes…
Germany, France, Spain, Belgium…
more to be done

MANAGEMENT OF PATIENTS
NOSOCOMIAL TRANSMISSION : CCHF
RISK : BLOOD EXPOSURE
MEASURES :
PROTECTIVE CLOTHING
BARRIER NURSING

This paper was produced for a meeting organized by Health & Consumer Protection DG and represents the views of its author on the subject. These views have not been adopted or in any way approved by the Commission and should not be relied upon as a statement of the Commission's or Health & Consumer Protection DG's views. The European Commission does not guarantee the accuracy of the data included in this paper, nor does it accept responsibility for any use made thereof.