April | June 2013 - Volume 12, Number 2 Could idiopathic
4
Braz J Oral Sci. 12(2):105-108 Original Article Braz J Oral Sci. April | June 2013 - Volume 12, Number 2 Could idiopathic osteosclerosis have correlations with palatally impacted maxillary canines? Cesar Augusto Rodenbusch Poletto 1 , Claudinéia Itiberê 2 , Sérgio Aparecido Ignácio 3 , Lucilia Kuriki 4 , Orlando Motohiro Tanaka 4 , Elisa Camargo 4 1 Area of Orthodontics and Radiology, University of Planalto Catarinense (UNIPLAC), Lages, SC, Brazil and Pontifical Catholic University of Paraná (PUCPR), Curitiba, PR, Brazil 2 Dentist, Curitiba, PR, Brazil 3 Area of Biostatistics, Dental School, Pontifical Catholic University of Paraná (PUCPR), Curitiba, PR, Brazil 4 Area of Orthodontics, Dental School, Pontifical Catholic University of Paraná (PUCPR), Curitiba, PR, Brazil Correspondence to: Cesar Augusto Rodenbusch Poletto Rua Rubens de Almeida, 75, CEP: 88523-180 - Lages, SC, Brasil Phone / fax: +55 49 32232275 E-mail: [email protected] Abstract Aim: To investigate the association between palatally impacted maxillary canines (PIC) and idiopathic osteosclerosis. Methods: A sample of 54 subjects (28 females and 26 males, mean age of 12.98±1.59 years) with PIC was selected from the records of 1,650 orthodontic patients treated at the Discipline of Orthodontics clinics at the Dental School of the Pontifical Catholic University of Paraná (PUCPR), in Curitiba, PR, Brazil. A control group of 54 subjects with normally erupted canines was also selected from the same files (mean age of 12.93±1.58 years). Panoramic, lateral skull, postero-anterior skull, periapical and occlusal radiographs, as well as stone casts of the patients were examined. The Kolmogorov-Smirnov test revealed a normal distribution of gender and age in the groups. The results were analyzed with the Chi-square test (α=0.05). Results: There were no statistically significant differences (p>0.05) between the groups. Four patients from each group had idiopathic osteosclerosis (7.41%), a rate that falls in the prevalence range reported in the literature. Conclusions: No correlation was observed between palatally impacted maxillary canines and idiopathic osteosclerosis. Keywords: diagnosis, tooth, unerupted, osteosclerosis. Introduction Idiopathic osteosclerosis is an asymptomatic, non-expansive and localized increase of bone radiopacity caused by an increase in the width of the bone trabeculae at the expense of medullary space. It is usually located in the mandibular premolar region 1-3 . The lesion has benign characteristics and seems not to increase over time 4 . Peck 5 listed several dental anomalies that seemed to indicate a pattern. Among them were missing teeth, conoid teeth, teeth with reduced size (generalized or localized), delayed tooth formation and eruption (generalized or localized), infra- occlusion (more frequently in primary teeth), palatally impacted canines, maxillary
Transcript of April | June 2013 - Volume 12, Number 2 Could idiopathic

Braz J Oral Sci. 12(2):105-108
Original Article Braz J Oral Sci.April | June 2013 - Volume 12, Number 2
Could idiopathic osteosclerosis havecorrelations with palatally impacted
maxillary canines?Cesar Augusto Rodenbusch Poletto1, Claudinéia Itiberê2, Sérgio Aparecido Ignácio3,
Lucilia Kuriki4, Orlando Motohiro Tanaka4, Elisa Camargo4
1Area of Orthodontics and Radiology, University of Planalto Catarinense (UNIPLAC), Lages, SC, Brazil and
Pontifical Catholic University of Paraná (PUCPR), Curitiba, PR, Brazil2 Dentist, Curitiba, PR, Brazil
3Area of Biostatistics, Dental School, Pontifical Catholic University of Paraná (PUCPR), Curitiba, PR, Brazil4Area of Orthodontics, Dental School, Pontifical Catholic University of Paraná (PUCPR), Curitiba, PR, Brazil
Correspondence to:Cesar Augusto Rodenbusch Poletto
Rua Rubens de Almeida, 75,CEP: 88523-180 - Lages, SC, Brasil
Phone / fax: +55 49 32232275E-mail: [email protected]
Abstract
Aim: To investigate the association between palatally impacted maxillary canines (PIC) andidiopathic osteosclerosis. Methods: A sample of 54 subjects (28 females and 26 males, mean ageof 12.98±1.59 years) with PIC was selected from the records of 1,650 orthodontic patients treatedat the Discipline of Orthodontics clinics at the Dental School of the Pontifical Catholic University ofParaná (PUCPR), in Curitiba, PR, Brazil. A control group of 54 subjects with normally eruptedcanines was also selected from the same files (mean age of 12.93±1.58 years). Panoramic,lateral skull, postero-anterior skull, periapical and occlusal radiographs, as well as stone casts ofthe patients were examined. The Kolmogorov-Smirnov test revealed a normal distribution ofgender and age in the groups. The results were analyzed with the Chi-square test (α=0.05).Results: There were no statistically significant differences (p>0.05) between the groups. Fourpatients from each group had idiopathic osteosclerosis (7.41%), a rate that falls in the prevalencerange reported in the literature. Conclusions: No correlation was observed between palatallyimpacted maxillary canines and idiopathic osteosclerosis.
Keywords: diagnosis, tooth, unerupted, osteosclerosis.
Introduction
Idiopathic osteosclerosis is an asymptomatic, non-expansive and localizedincrease of bone radiopacity caused by an increase in the width of the bonetrabeculae at the expense of medullary space. It is usually located in the mandibularpremolar region1-3. The lesion has benign characteristics and seems not to increaseover time4.
Peck5 listed several dental anomalies that seemed to indicate a pattern. Amongthem were missing teeth, conoid teeth, teeth with reduced size (generalized orlocalized), delayed tooth formation and eruption (generalized or localized), infra-occlusion (more frequently in primary teeth), palatally impacted canines, maxillary

Braz J Oral Sci. 12(2):105-108
106106106106106
canine/premolar transposition, mandibular canine/lateralincisor transposition, and distal angulation of a non-eruptedsecond mandibular premolar. According to this author, otherassociations will be discovered as researchers focus on thegenetic pattern of these anomalies.
After the third molars, the permanent maxillary canineis the most frequently involved tooth in cases of impaction6-7.Palatally impacted maxillary canines seem connected to agenetic condition, and are often associated with other dentaland skeletal disturbances7.
The aim of the present study was to investigate whetheran increased prevalence of idiopathic osteosclerosis existsin patients with palatally impacted maxillary canines.
Material and methods
A total of 1,650 patient records from the files of theDiscipline of Orthodontics of the Dental School of thePontifical Catholic University of Paraná (PUCPR) werereviewed for this study. The Experimental Group (EG)consisted of 54 (3.27%) patients who presented 62 palatallyimpacted maxillary canines; these patients had ages startingat 12 years and 5 months to ensure a definite diagnosis ofpalatal impaction. According to Ericson and Kurol8, the bestage to establish a clinical diagnosis of maxillary canineimpaction using digital palpation and checking for thepresence of a buccal bulge would be starting at 9 yearsbecause the clinical signs are not evident before this age. Asfor gender, 28 cases were observed among females (51.85%)and 26 among males (48.15%).
The Control Group (CG) consisted of 54 patients, 28females and 26 males, with approximately the same age(12.93±1.58 years) as those of the patients in the EG(12.98±1.59 years), with normally erupted canines. TheKolmogorov-Smirnov test indicated normal distribution ofgender and age in the groups.
The patients’ orthodontic documentation, whichincluded a set of radiographs (panoramic, lateral skull,postero-anterior skull, periapical and occlusal), photographsand stone casts, was used for diagnosing the cases ofpalatally impacted maxillary canines. The methods werethe three-dimensional localization using orthogonalradiographs and the Clark method. The canine wasconsidered palatally impacted whenever it was uneruptedand the patient was already in the C5 cervical maturationstage, as proposed by Baccetti9.
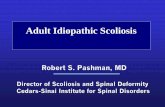
The diagnosis of idiopathic osteosclerosis was alsoestablished based on the patient’s radiographic examinations.Idiopathic osteosclerosis was observed as a bone radiopacityincrease located inside the bone, measuring 3 mm or more,with no radiolucent halo and no apparent cause (Figures 1and 2), as proposed by Langlais et al.1, and White andPharoah3. Radiopaque lesions associated with dental caries,deep restorations or tooth extraction regions were notdiagnosed as idiopathic osteosclerosis, since they could bethe result of condensing osteitis or residual condensingosteitis, when located in a tooth extraction region. Lesions
Fig. 1. Palatally impacted right maxillary canine and idiopathic osteosclerosis inthe right mandibular first premolar region.
located in tooth extraction regions could also be the resultof alveolar sclerosis. Exostoses of the torus type wereexcluded by evaluating the intraoral photographs and thegypsum casts of the orthodontic documentation. Theprojected image of a soft tissue calcification was discardedby analyzing the radiograph with a projection perpendicularto the panoramic radiograph or to the lateral skull radiograph,namely the posteroanterior skull radiograph.
Initially, canine impaction was assessed and idiopathicosteosclerosis was identified in 30 patient records (15 fromthe CG and 15 from the EG), at two time points (day zeroand 30 days later), by a single radiology specialist, and byapplying the Kappa agreement test. The test indicatedagreement between the assessments (p<0.05), obtaining thelowest kappa value of 0.7830 (a value greater than 0.60 isrecommended). All radiographs of both groups were thenanalyzed and the data were tabulated for application of theChi-square statistical test (α=0.05).
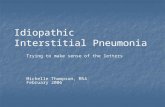
Fig. 2. Periapical view of an idiopathic osteosclerosis.
Could idiopathic osteosclerosis have correlations with palatally impacted maxillary canines?

Braz J Oral Sci. 12(2):105-108
107107107107107
Results
Four cases of osteosclerosis were observed in EG and 4cases CG (7.41%). No significant correlation was foundbetween osteosclerosis and either of the groups (p>0.05).
Discussion
One of the most important requisites for treating andpreventing a disease is to know its etiologic factor. The termidiopathic has been used whenever science has failed todefine the cause of a certain change. Nevertheless, pursuitfor the origin goes on and nowadays several pathologicalconditions have been shown to have a genetic condition asa causal factor. Some changes overlap and often share thesame origin. These associations may help in the earlydiagnosis of some serious disease as the Gardner syndrome,for example. One of its first manifestations in the oral cavityis the presence of osteomas in the maxillary bones. Later on,the patient develops malignant intestinal tumors that are hardto treat and have a more doubtful prognosis. A dentist onthe alert may suspect a new case of Gardner syndrome byobserving atypical osteoma-like lesions in a young patientand referring him/her to medical evaluation10.
Palatally impacted maxillary canines seem to have agenetic etiology6,11, and are frequently associated with otherchanges, such as microdontia of maxillary lateral incisors11-12,delayed tooth eruption13 and fusion of the clinoid processesof the sella turcica14. Idiopathic osteosclerosis is a bone tissuestructural change whose etiologic factor remains unknown.It is also known as enostosis or dense bone island, termsused more frequently by medical literature to describeradiopaque lesions found occasionally, mostly in the longbones. Its most common location in the jaws is the mandible,mainly in the premolar and molar regions.
Although idiopathic osteosclerosis is not a rare entity, littleimportance has been given by orthodontists to its occurrence,as demonstrated by the small number of studies published onthis topic in orthodontic journals. In a study on the incidentalfindings made on panoramic radiographs of orthodontic patients,Bondemark et al.15 observed that idiopathic osteosclerosis wasthe most frequent finding, outnumbering even periapicalinflammatory lesions and marginal bone resorptions.
Diagnosing idiopathic osteosclerosis accurately is adifficult task, since this lesion may be radiographicallymistaken for exostosis, including torus mandibularis andpalatinus, residual condensing osteitis, alveolar calcificationafter exodontia (whether complicated or not), bonearchitectural change in response to occlusal trauma on aninclined tooth, particularly on mandibular second molars,when the first molars are missing. The lesion may even bemistaken for a radiographic projection over bone of a softtissue calcification. The mere presence of teeth, their cariouslesions, occlusal traumas and infectious processes, as well asthe primary teeth shedding process, may also cause bonetissue architectural changes, adding to the abovementionedenostoses and dense bone islands.
The dentist’s approach towards idiopathic osteosclerosisis also not unanimous in the literature. Williams and Brooks4
followed adult patients with idiopathic osteosclerosis for adecade and concluded that it remained stable. McDonald-Jankowski2 studied idiopathic osteosclerosis lesions inradiographic examinations after a 9-year interval and foundthat lesion size may decrease and that that there may becomplete remission in some cases. These findings reinforcethe recommendation for no intervention.
There are, however, reports of complications arising fromthe presence of idiopathic osteosclerosis in the maxillarybones. Bennett and McLaughlin16 warned that bone sclerosismight delay or even obstruct space closure after toothextractions during orthodontic treatment. Nakano et al.17
reported a case of tooth inclination caused by idiopathicosteosclerosis growth. Marques-Silva et al.18 described a casewhere idiopathic osteosclerosis caused deviation of a tootheruption route. This, in turn, led to the resorption of theadjacent tooth. Mah et al.19 suggested that caution shouldbe taken in biomechanical planning and orthodonticmovement in sclerotic bone areas, and also that computerizedtomography examination may aid in this planning.
Alveolar sclerosis is a condition histologically very similarto idiopathic osteosclerosis. Baumgaertel20 reported a veryinteresting case where the tooth movement process throughan alveolus repaired with sclerotic bone was not possible usingthe conventional retraction technique, requiring extraanchorage obtained by means of mini-implants. The patientof that case also displayed agenesis of a maxillary lateralincisor and palatal impaction of a maxillary canine, bothconditions that seem to share the same genetic origin.
Considering the possible difficulty in performing toothmovement when faced with a case of osteosclerosis, theorthodontist should register its presence on the patient’srecords and follow the patient radiographically. If moving atooth through the zone of osteosclerosis is required, cautionmust be taken during the procedure since the lesion mayrender tooth movement difficult.
To the best of our knowledge, no previous study hasinvestigated the association between idiopathic osteosclerosisand palatally impacted permanent maxillary canines. A singlestudy21 was found comparing the prevalence of this lesion incertain malocclusion types, although the criterion adoptedby the authors for diagnosing malocclusion was based solelyon the gypsum model records. The authors did notdistinguished the skeletal from the dental aspects of thesagittal malocclusions, a distinction seemingly relevant whenstudying possible correlations between this malocclusion typeand a bone lesion.
A possible association between a greater prevalence ofidiopathic osteosclerosis among patients with palatallyimpacted maxillary canines could suggest that idiopathicosteosclerosis is a genetic condition and possibly also themanifestation of the complex condition of palatally impactedmaxillary canines.
The prevalence of palatally impacted maxillary caninesfound in the present study (3.27%) and the prevalence of
Could idiopathic osteosclerosis have correlations with palatally impacted maxillary canines?

108108108108108
Braz J Oral Sci. 12(2):105-108
idiopathic osteosclerosis (7.41%) were similar to thosereported elsewhere 22. Finding an identical number ofidiopathic osteosclerosis cases in both groups suggests thatthere is no association of this condition with palatallyimpacted maxillary canines. Also, the small number ofidiopathic osteosclerosis cases observed in this study mayhave interfered with establishing a possible association.Further investigation is required with a greater sample ofpatients to effectively discard an association between thetwo pathologies or possibly demonstrate a common geneticorigin. The results showed no correlation between palatallyimpacted maxillary canines and idiopathic osteosclerosis.
References
1. Anic-Milosevic S, Varga S, Mestrovic S Lapter-Varga M, Slaj M. Dentaland occlusal features in patients with palatally displaced maxillary canines.Eur J Orthod. 2009; 31: 367-73.
2. Baccetti T. Risk indicators and interceptive treatment alternatives for palatallydisplaced canines. Semin Orthod. 2010; 16: 186-92.
3. Bennett J C, Mclaughlin R P. Controlled space closure with preadjustedappliance system. J Clin Orthod. 1990; 4: 251-60.
4. Baumgaertel S. Socket sclerosis- An obstacle for orthodontic spaceclosure? Angle Orthod. 2009; 79: 800-3.
5. Bishara S E. Impacted maxillary canines: A review. Am J Orthod DentofacOrthop. 1992; 101: 159-71.
6. Bondemark L, Jeppsson M, Lindh-Ingildsen L, Rangne K. Incidentalfindings of pathology and abnormality in pretreatment orthodontic panoramicradiographs. Angle Orthod. 2006; 76: 76-98.
7. Cankaya AB, Erdem MA, Isler SC, Cifter M, Olgac V, Kasapoglu C,ET al. Oral and maxillofacial considerations in Gardner’s Syndrome. IntJ Med Sci. 2012; 9: 137-41.
8. Chaushu S, Sharabi S, Becker A. Dental morphologic characteristics ofnormal versus delayed developing dentitions with palatally displacedcanines. Am J Orthod Dentofacial Orthop. 2012; 121: 339-46.
9. Ericson S, Kurol J. Longitudinal study and analysis of clinical supervisionof maxillary canine eruption. Community Dent Oral Epidemiol. 1986; 8:133-40.
10. Garib DG, Alencar BM, Lauris JR, Baccetti T. Agenesis of maxillarylateral incisors and associated dental anomalies. Am J Orthod DentofacialOrthop. 2010; 137: 732-6.
11. Jacoby H. The etiology of maxillary canine impaction. Am J OrthodDentofacial Orthop. 1983; 84: 125-32.
12. Langlais RP, Langland OE, Nortjé CJ. Generalized radiopacities. In:Cooke D, editor. Diagnostic Imaging of the jaws. Baltimore: Williams &Wilkins; 1995. p.565-615.
13. Leonardi R, Barbato E, Vichi M, Caltabiano M. Skeletal anomalies andnormal variants in patients with palatally displaced canines. Angle Orthod.2009; 79: 727-32.
14. Marques-Silva L, Guimarães ALS, Dilascio MLC, Castro WH, GomezRS. A rare complication of idiopathic osteosclerosis. Med Oral Patol OralCir Bucal 2007, 12: E233-4.
15. Mah JK, Yi L, Huang RC, Choo HR. Advanced applications of cone beamcomputed tomography in orthodontics. Semin Orthod. 2011; 17: 57-71.
16. Mcdonald-Jankowski D S. Idiopathic osteosclerosis in the jaws of Britonsand of the Hong Kong Chinese: radiology and systematic review.Dentomaxillofac Radiol. 1999; 28: 357-63.
17. Nakano K, Ogawa T, Sobue S, Ooshima T. Dense bone island: clinicalfeatures and possible complications. Int J Paediatr Dent. 2001; 12: 433-7.
18. Peck S. Dental Anomaly Patterns (DAP): A new way to look atmalocclusion. Angle Orthod. 2009; 19: 1015-6.
19. White SC, Pharoah MJ. Benign tumours of the jaws. In: White SC,Pharoah MJ. Oral radiology: principles and interpretation. Saint Louis:Mosby; 2000. p.378-419.
20. Williams TP, Brooks SL. A longitudinal study of idiopathic osteosclerosisand condensing osteitis. Dentomaxillofac Radiol. 1998; 27: 275-8.
21. Lee S,Park I, Jang I, Choi D, Cha B. A study on the prevalence of theidiopathic osteosclerosis in Korean malocclusion patients. Korean J OralMaxillofac Radiol. 2010; 40: 159-63.
22. Sisman Y, Ertas ET, Ertas H, Sekerci AE. The frequency and distributionof idiopathic osteosclerosis of the jaws. Eur J Dent. 2001; 5: 409-15.
Could idiopathic osteosclerosis have correlations with palatally impacted maxillary canines?