
Apresentaç?o do PowerPoint - IAP-AD · PDF fileSclerosing mucoepidermoid ca with...
111
Thyroid Tumours From Well to Poorly Differentiated and Undifferentiated Carcinomas Algiers, Nov 25, 2008 Porto, Portugal
Transcript of Apresentaç?o do PowerPoint - IAP-AD · PDF fileSclerosing mucoepidermoid ca with...
Thyroid Tumours From Well to Poorly Differentiated and Undifferentiated CarcinomasAlgiers, Nov 25, 2008
Porto, Portugal

WHO book on Endocrine Tumours, 2nd edition, Zurich 1986

THYROID CARCINOMA
Follicular carcinomaPapillary carcinoma(Hürthle cell carcinoma)Medullary carcinomaPoorly differentiated carcinomaUndifferentiated carcinoma
WHO books on Endocrine Tumours, 2nd & 3rd editions, 1988 & 2004


WHO book on Endocrine Tumours, 3rd edition, 2004
THYROID CARCINOMASFollicular carcinomaPapillary carcinoma
Hyalinizing trabecular tumourMucoepidermoid carcinomaSclerosing mucoepidermoid ca
with eosinophilia
Medullary carcinoma Mixed medullary and follicular cell caPoorly differentiated ca
Squamous cell carcinomaMucinous carcinoma
Undifferentiated ca
Questions to be made whenever facing a strange lesion in the thyroid
Is it a primary thyroid tumour?If yes, is it made of follicular or C-cells?
Immunohistochemistry is mandatory: TG and calcitonin (and, if necessary, TTF1)


Thyroglobulin

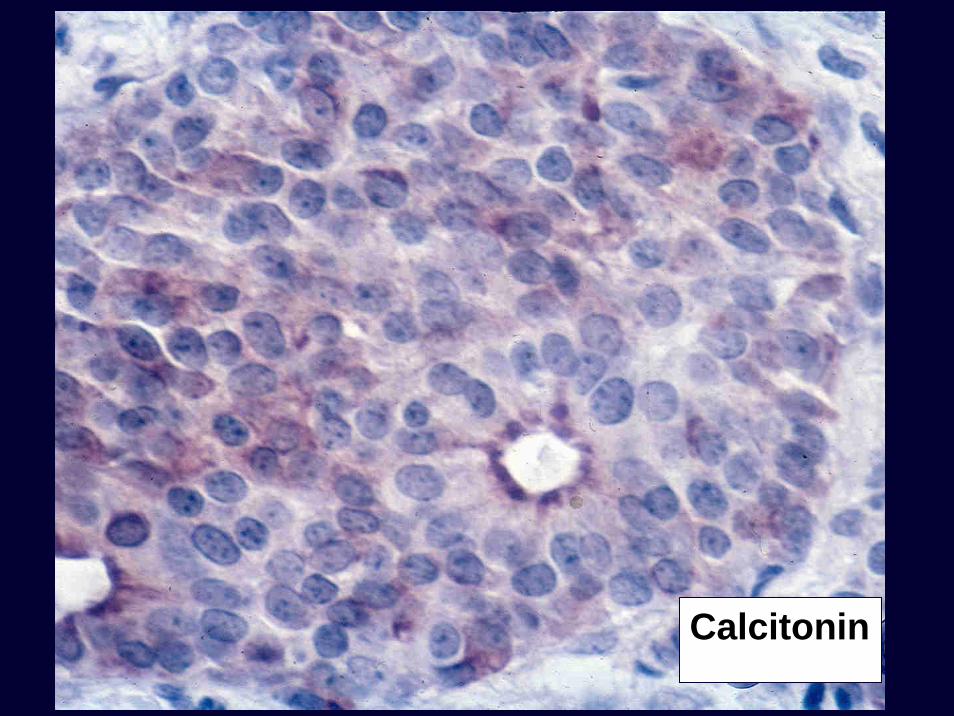
Calcitonin
Most frequent problems of thyroid pathology in a consultancy practice
1. Is there a focus (or some foci) of papillary carcinoma in “this” Hashimoto’s thyroiditis or “this” nodular goiter?2. Is this lesion an adenoma, a follicular carcinoma or a follicular variant of papillary carcinoma?3. How would you classify this Hürthle cell lesion?4. Is this a well differentiated carcinoma with a solid pattern of growth or a poorly differentiated carcinoma?

Diagnosis of (incipient) PTCIn our experience the most frequent doubts arise in four different settings:
a. Hashimoto’s thyroiditisb. Nodular (adenomatous) goiterc. Encapsulated well differentiated neoplasmsd. Oncocytic (Hürthle cell) neoplasms





Microdissected areas with PTC nuclei withinHashimoto’s thyroiditis
RET/PTC rearrangements – contradictory, positive and negative findingsSheils et al, Nikiforov et al, ...
B-RAF mutations – no mutations (n=6) Trovisco et al, 2005



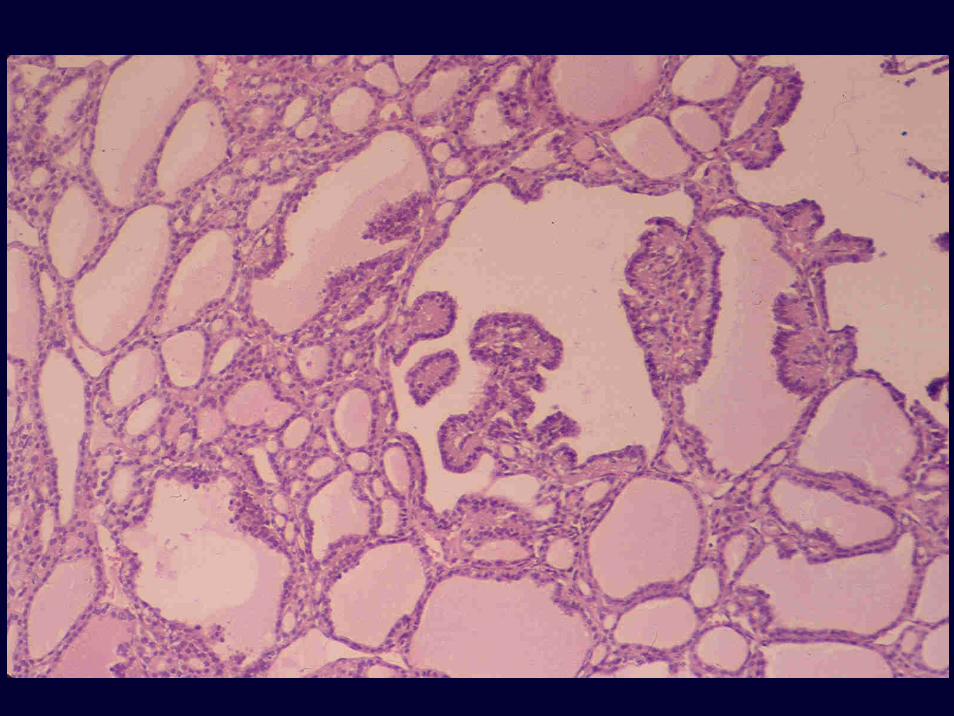
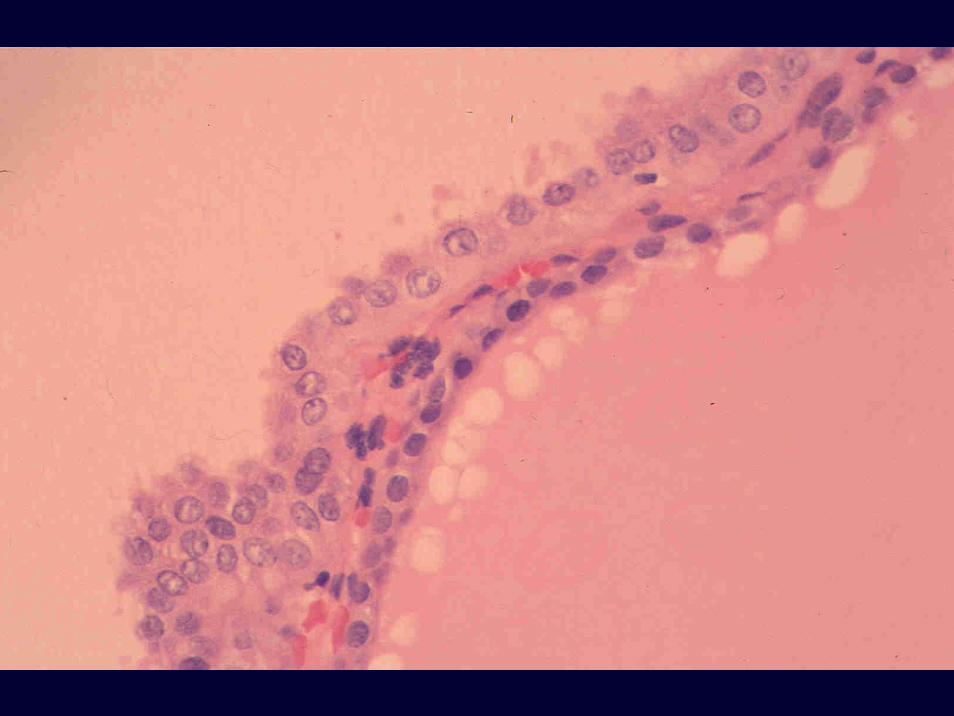
Microdissected areas with PTC nuclei withinadenomas/nodular goiters
RET/PTC rearrangements – Yes Fusco et al, Am J Surg Pathol, 2002
B-RAF mutations – no (?) (few cases) Trovisco et al, 2005

Hashimoto’s thyroiditis and Adenoma/nodular goiter
Dispersed cells with PTC-nucleiwith or without molecular alterations
Clusters of cells with PTC-nuclei forming a microtumourwith or without molecular alterations
CONCLUSION
KEEP THE DIAGNOSIS
PTC




Encapsulated follicular neoplasm

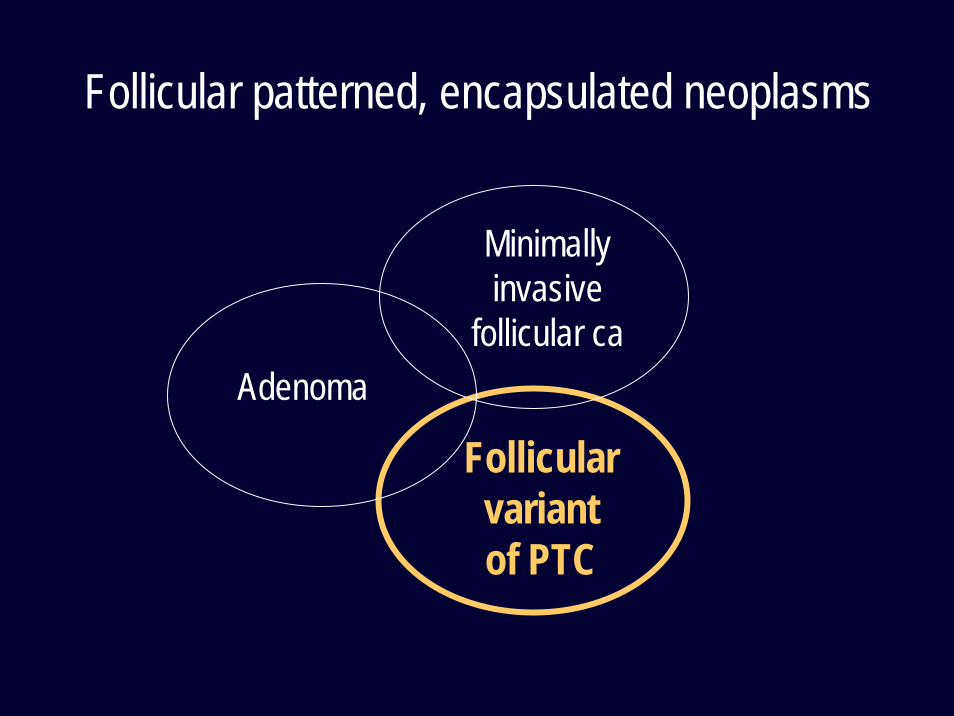
Follicular patterned, encapsulated neoplasms
Adenoma
Follicularvariant of PTC
Minimallyinvasive
follicular ca

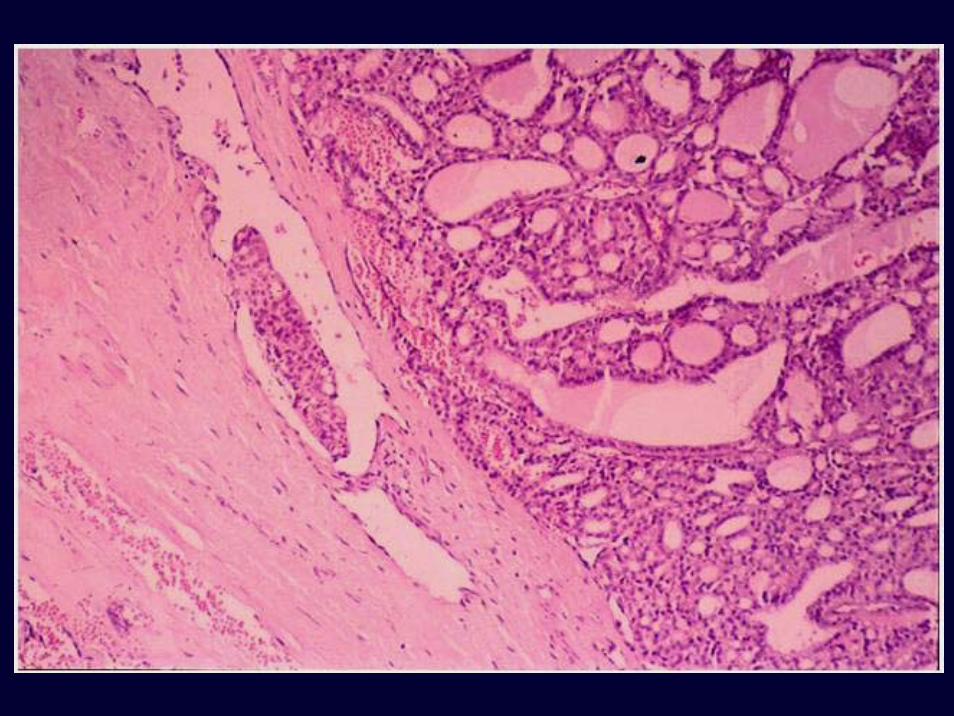
Malignancy in follicular patterned thyroid tumours
Capsular and/or VASCULAR INVASIONSolid, insular, trabecular
Pattern of growth Embryonal, fetalNormofollicularMacrofollicular
Nuclear features PTC NUCLEI
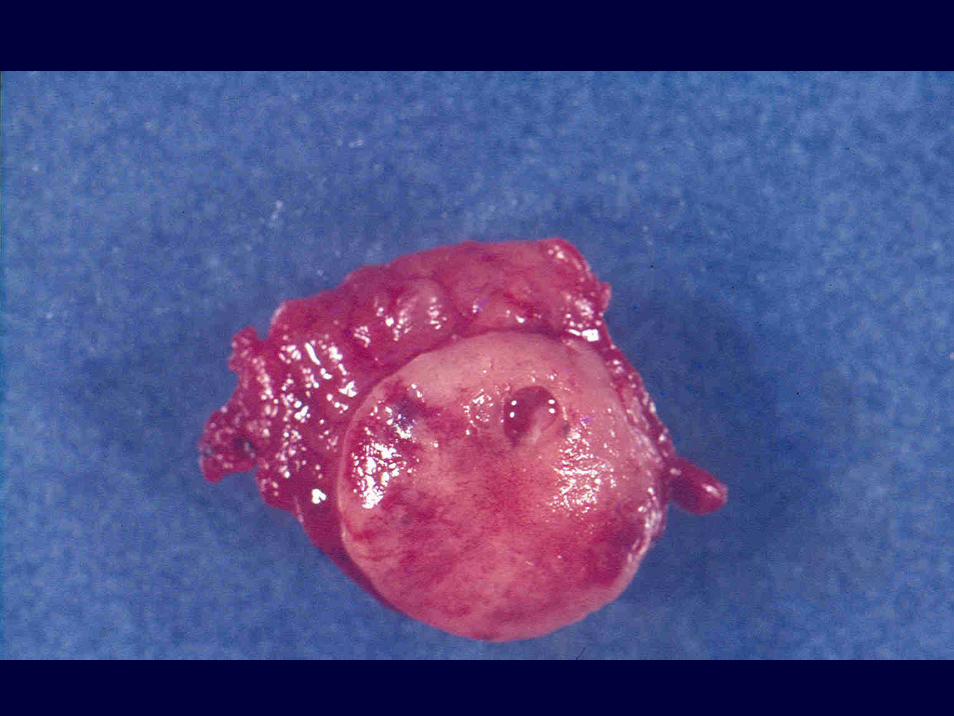
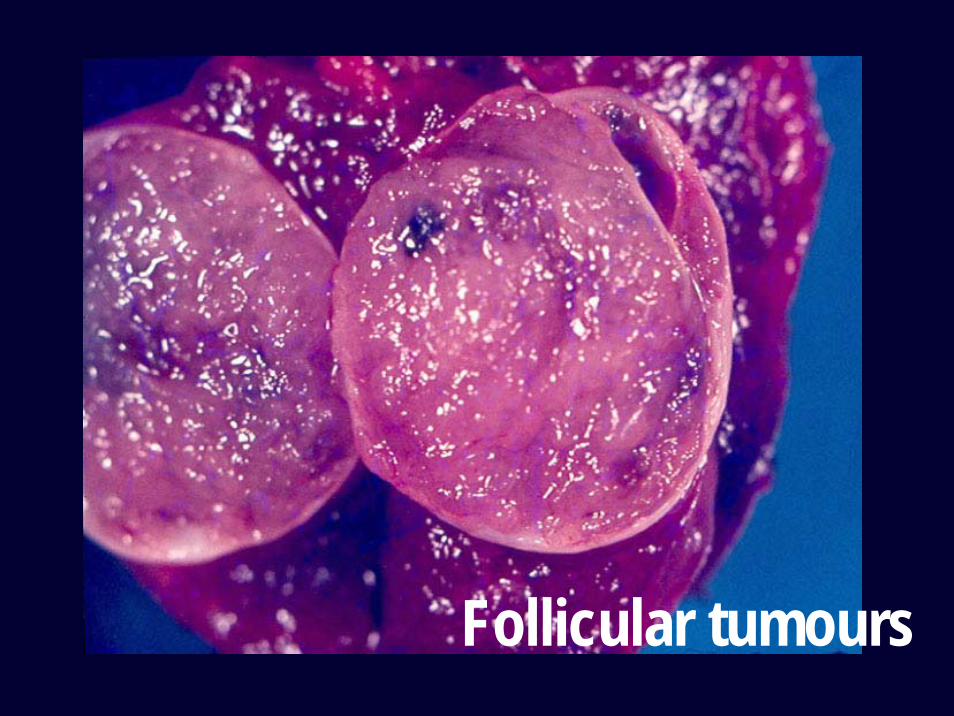
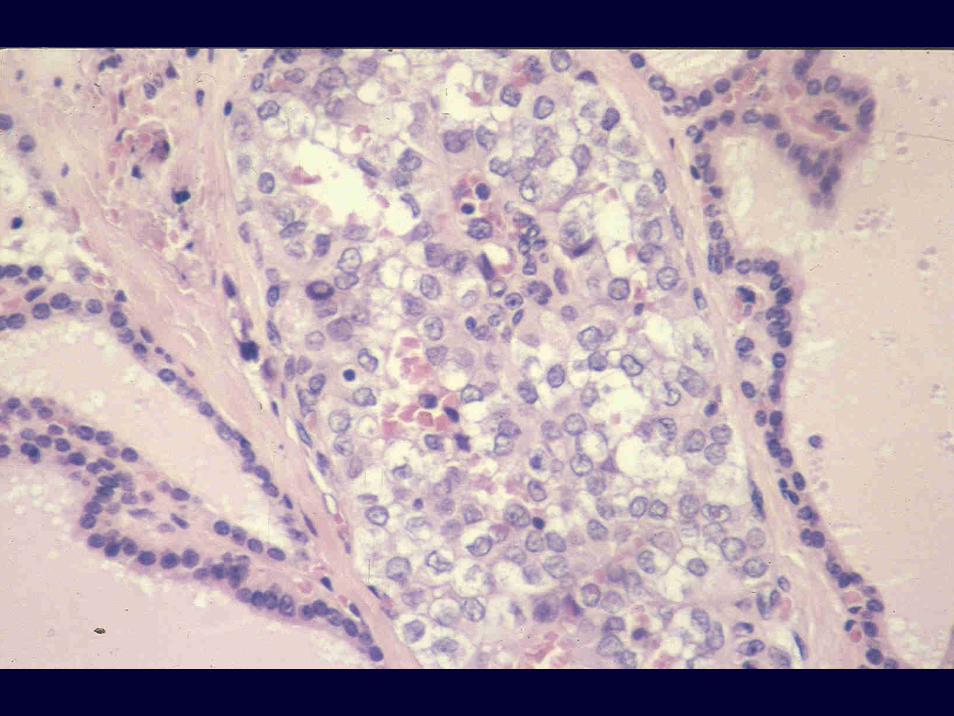
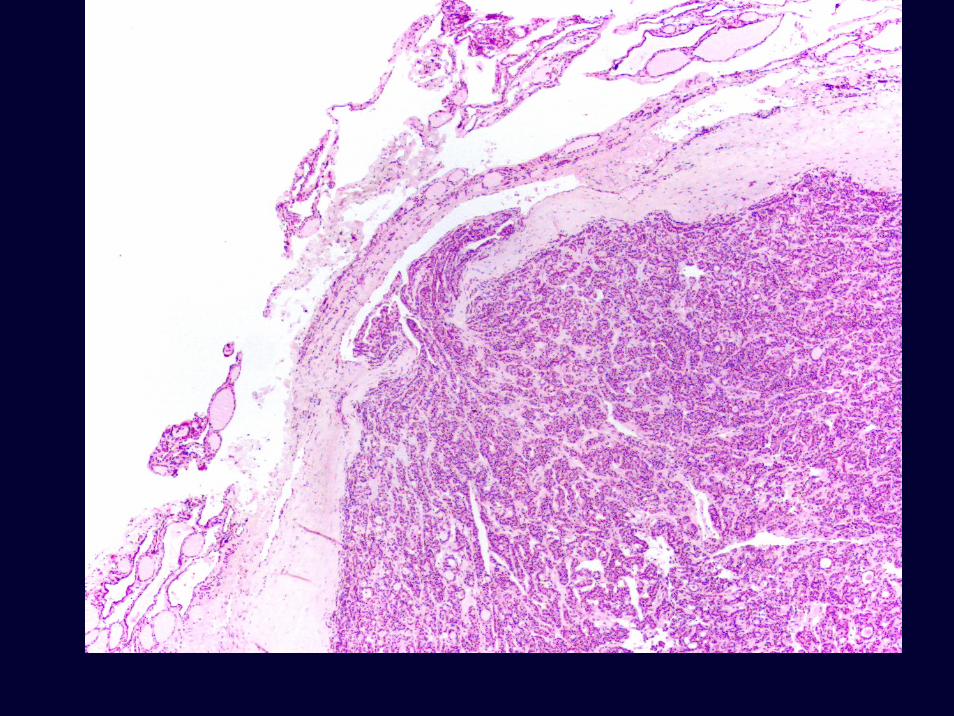
Follicular tumours

RAS activationOther factors
Chromosomalinstability (CINphenotype)Aneuploidy
PAX 8 - PPAR γOther alterations
Adenomaand
Follicular carcinoma
Follicularcell
A preoperative diagnostic test that distinguishes benign from malignant thyroid carcinoma based on gene expressionCerutti et al, J Clin Invest 113:1234, 2004
Follicular adenoma vs follicular carcinoma4 genes – predictive accuracy of 0.832 immunohistochem markers – estimated concordance of 0.76
Conclusion: A simple test based on a combination of these markers might improve preoperative diagnosis of thyroid nodules.

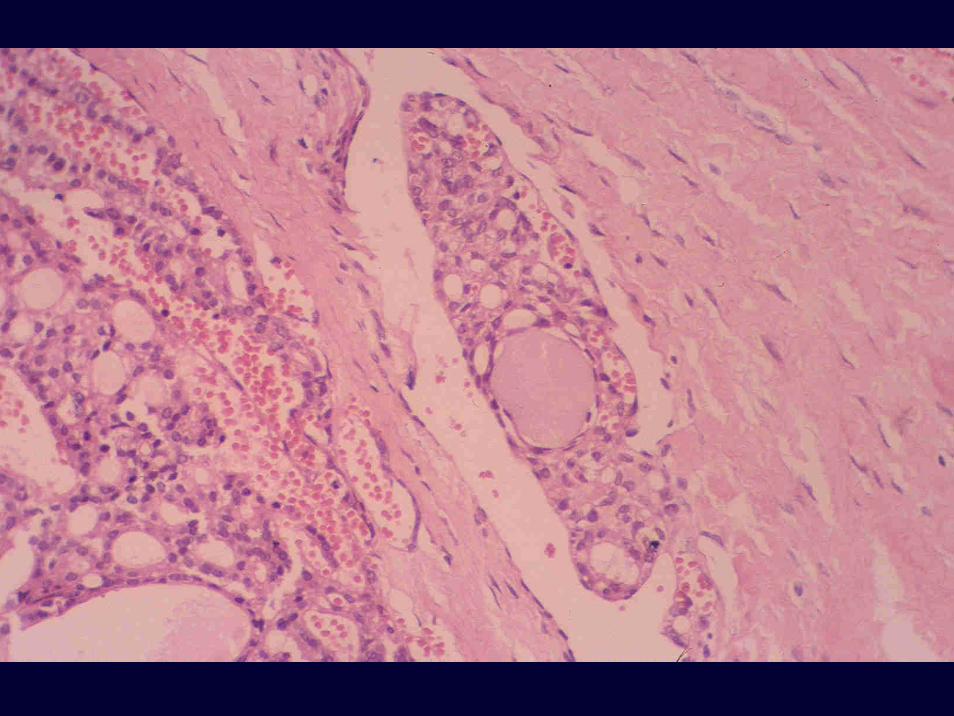
What is the best way to diagnose vascular invasion?
Histopathology Yes
Detection of biomarkers in the May beplasma/blood
High throughput approaches No


Encapsulated follicular tumour
Benign vs Malignant
Follicular adenoma
Follicular tumour of uncertainmalignant potential
Follicular carcinoma
Williams et al, Int J Surg Pathol, 8:181, 2000WHO book on Endocrine Tumours, 3rd ed, 2004

Follicular carcinoma
Minimally invasive
?Widely invasive

Follicular carcinoma
Minimally invasive
Widely invasive
Number and type of invaded vessels
Rosai et al, 2004WHO book on Endocrine Tumours, 2004

Papillary carcinoma
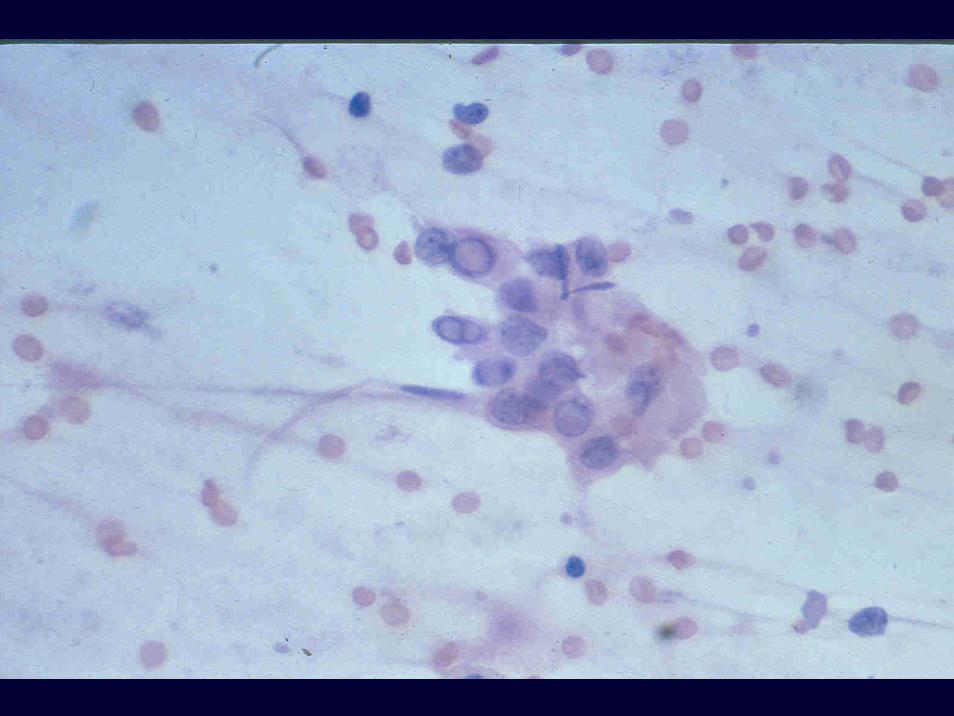
The optically clear nucleus:A reliable sign of papillary carcinoma of the thyroid?
Hapke MR & Dehner LP, Am J Surg Pathol 3:31, 1979



PROGNOSTIC MEANING OF HISTOLOGICAL VARIANTS OF PTC
DIFFUSE SCLEROSING VARIANTTALL CELL VARIANTCOLUMNAR CELL CARCINOMAMULTINODULAR TYPE OF FOLL VAR
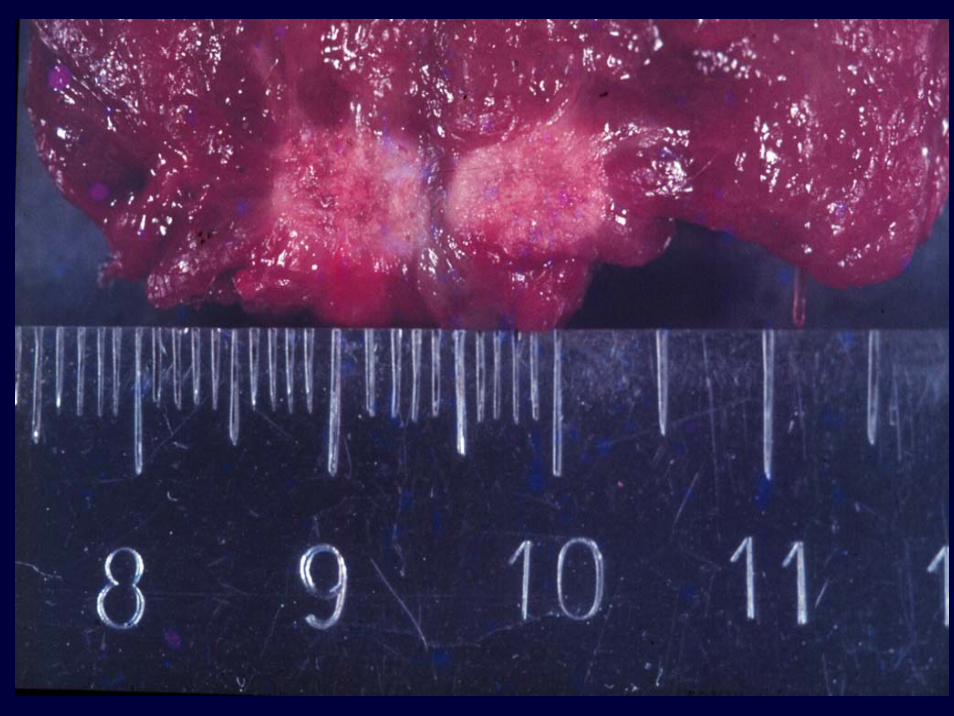
MICROCARCINOMA
Papillary microcarcinomaOccult papillary carcinomaLatent papillary carcinomaSmall papillary carcinomaNonencapsulated thyroid tumourOccult sclerosing carcinomaOccult papillary tumour
Rosai et al Int J Surg Pathol 11:249, 2003

RENAMING PAPILLARY MICROCARCINOMA OF THE THYROID GLAND: THE PORTO PROPOSAL
Juan Rosai, Virginia A. LiVolsi, Manuel Sobrinho-Simões and E.D. Williams
International Journal of Surgical Pathology 11:249-251, 2003

MIB1

Molecular features of papillary thyroid carcinoma
RET/PTC rearrangements (15% - 40%)TRK rearrangements (5% - 10%)MET overexpression (>50% ?)............................................................B-RAF mutations (30% - 50%) [0% - 75%]
Trovisco et al, J Pathol 2004Lima et al, JCEM 89:4267, 2004

RET/PTC rearranged papillary carcinomas display a Bonsai phenotype



PROGNOSTIC MEANING OF HISTOLOGICAL VARIANTS OF PTC
DIFFUSE SCLEROSING VARIANTTALL CELL VARIANTCOLUMNAR CELL CARCINOMAMULTINODULAR TYPE OF FOLL VAR MICROCARCINOMA





PROGNOSTIC FACTORS IN PAPILLARY AND FOLLICULAR THYROID CARCINOMA
Completeness of surgery and responsiveness to radioactive iodine
A – Age M – Distant metastasesE – Extrathyroid extensionS – Size of the tumours
Still debatable: aneuploidy (D…AMES), vascular invasion and molecular features (MIB1, p53)
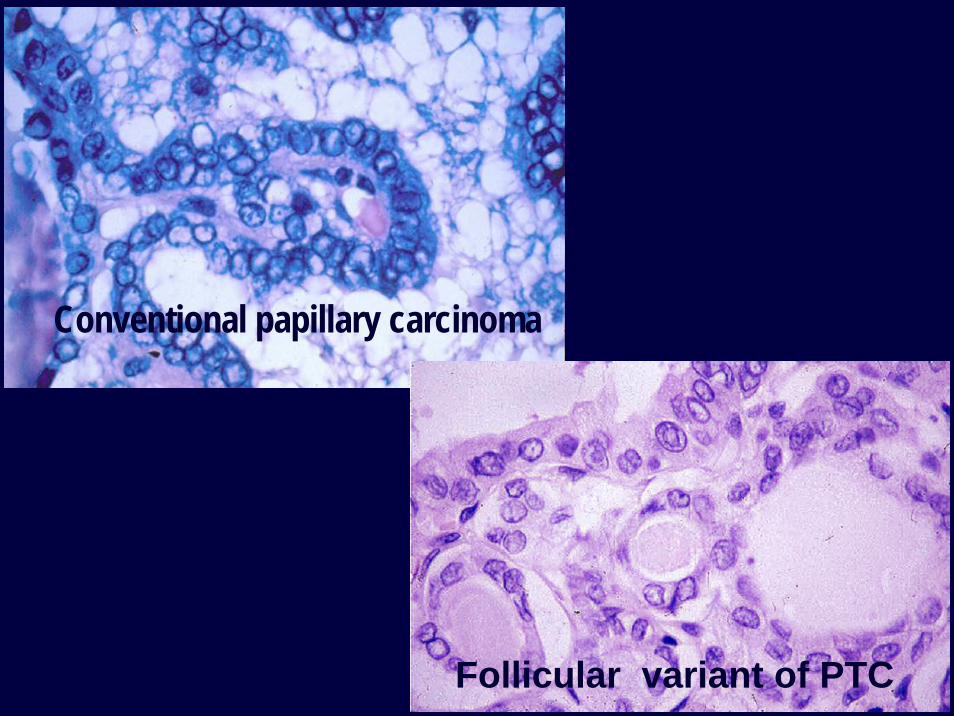
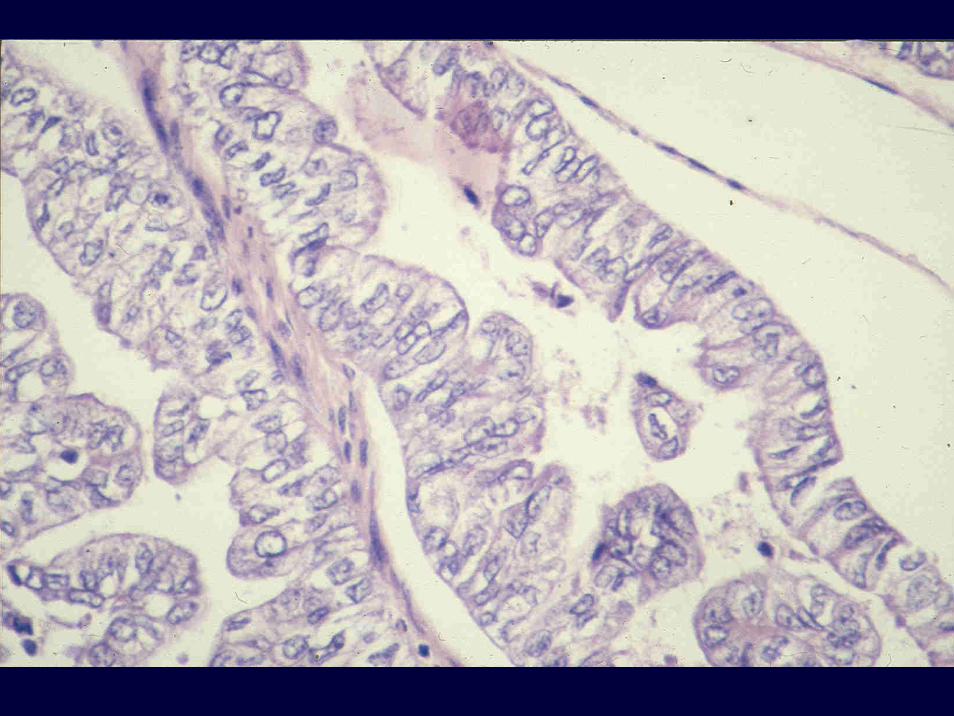
Conventional papillary carcinoma
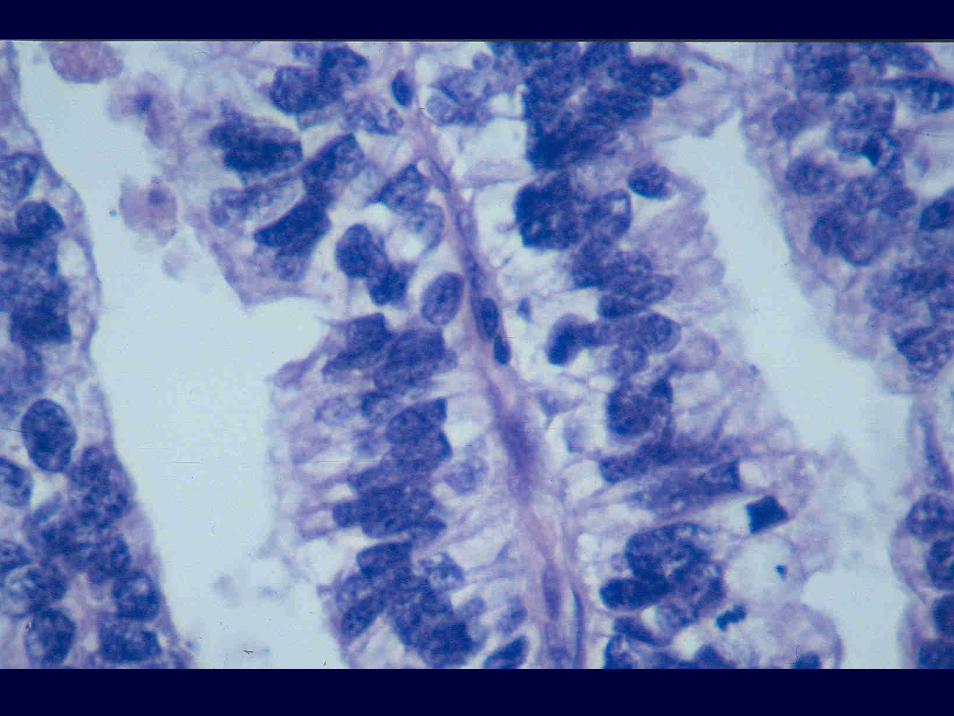
Follicular variant of PTC

Follicular variant of PTC Three problems
1.Questionable diagnosis2.Prognosis3.Relationship with follicular carcinoma
Follicular patterned, encapsulated neoplasms
Adenoma
Follicularvariant of PTC
Minimallyinvasive
follicular ca

Am J Clin Pathol, Jan 2002• Chan JKC: Strict criteria should be applied in the
diagnosis of encapsulated follicular variant of papillary thyroid carcinoma
• Renshaw AA & Gould EW: Why there is the tendency to “overdiagnose” the follicular variant of papillary thyroid carcinoma
• Baloch ZW & LiVolsi VA: Follicular-patterned lesions of the thyroid: the bane of the pathologist

DIAGNOSTIC HINTSCapsular or, more importantly, vascular invasionNuclear features
WHAT ABOUT QUESTIONABLE CASES?
DOES IMMUNOHISTOCHEMISTRY OR MOLECULAR BIOLOGY HELP?
IMMUNOHISTOCHEMICAL MARKERS OF PAPILLARY THYROID CARCINOMA
• Cytokeratin 19• Lewis X and S Lewis X• Galectin 3 • HBME1• Fibronectin 1• ...................

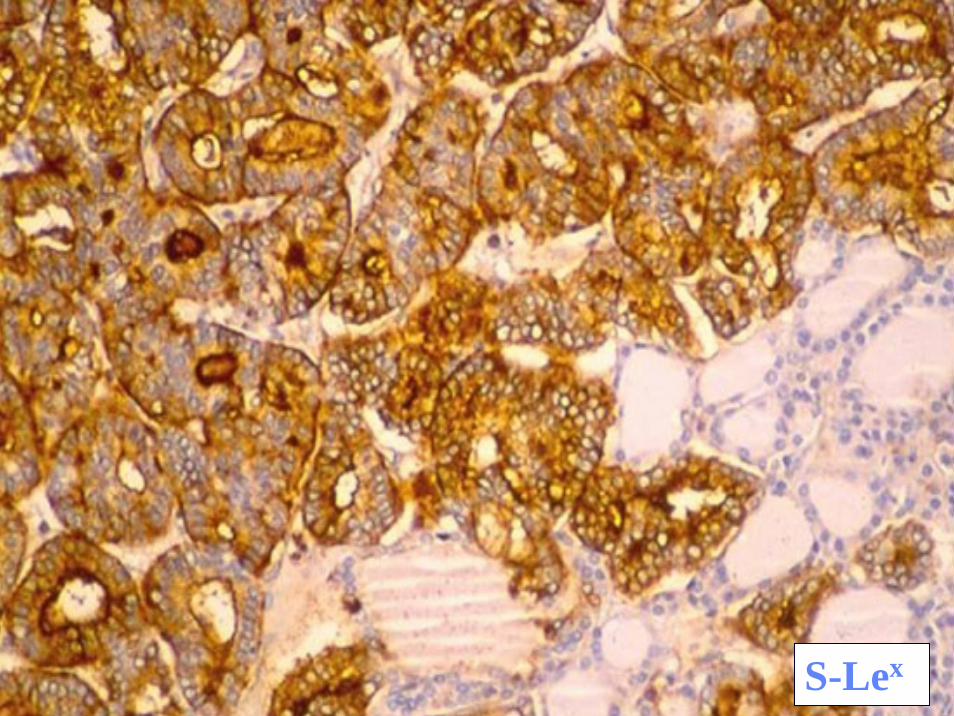
S-Lex


Galectin-3 and HBME-1 expression in well-differentiated thyroid tumors with follicular architecture of uncertain malignant potential
8 cases with questionable invasion13 cases with questionable nuclear changes
GAL3 and HBME1 are more frequently present in the second group (10/13 and 9/13, respectively) than in the first group (3/8 and 5/8, respectively)
Papotti M et al, Mod Pathol 18:541, 2005
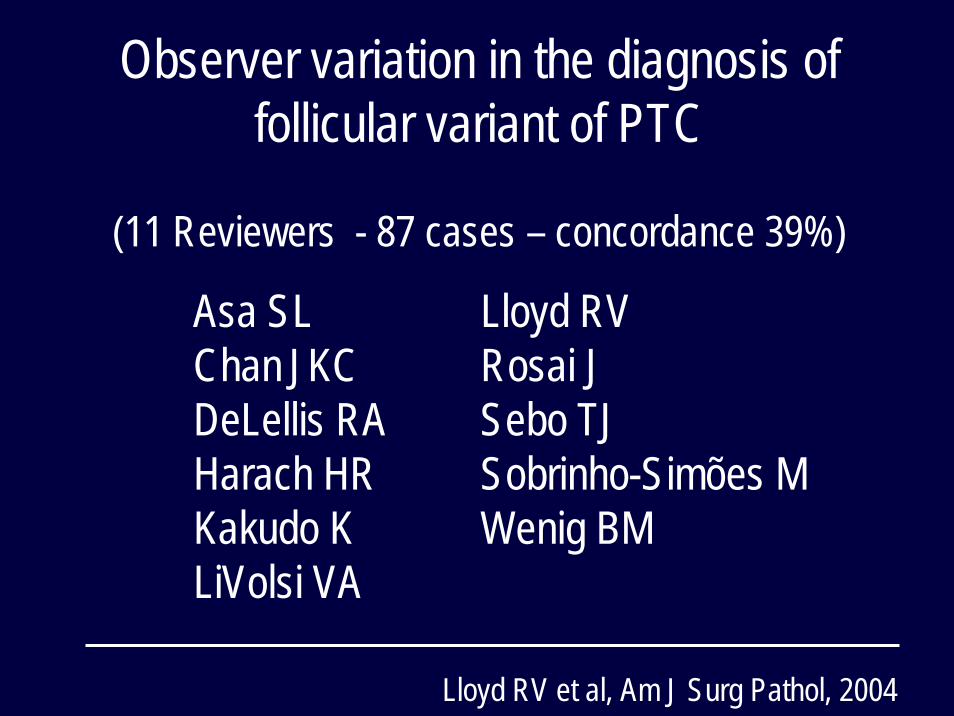
Observer variation in the diagnosis offollicular variant of PTC
(11 Reviewers - 87 cases – concordance 39%)
Asa SL Lloyd RVChan JKC Rosai JDeLellis RA Sebo TJHarach HR Sobrinho-Simões MKakudo K Wenig BMLiVolsi VA
Lloyd RV et al, Am J Surg Pathol, 2004

Usefulness of HBME-1, cytokeratin 19 and galectin-3 immunostaining in the diagnosis of thyroid malignancy
“Unfortunately, in contrast to many reports concerning the differential diagnosis of follicular patterned lesions, we found none of these markers sufficient to confer a sensitive and specific diagnosis”
Matos PS et al, Histopathology 47:391, 2005
B-RAF MUTATIONS IN176 PAPILLARY THYROID CARCINOMAS
Warthin-like PTC > 75%Conventional PTC ~ 50%
Follicular variant PTC < 5%
Soares et al, Oncogene 2003Trovisco et al, J Pathol, 2004
Lima et al, JCEM 89:4267, 2004

• Well differentiated tumor of uncertain malignant potential
• Well differentiated carcinoma, NOS
Williams et al, Int J Surg Pathol 8:181, 2000WHO book on Endocrine Tumours, 3rd edition, 2004
Follicular variant of PTCThree main types:• Encapsulated• Poorly circumscribed• Diffuse, aggressive, multinodular
Multicentricity Vascular invasivenessLung and bone metastases
PROGNOSIS
Diffuse follicular variant of PTCSobrinho-Simões et al, Surg Pathol 3:189, 1990Mikuzami et al, Histopathology 27:575, 1995
Aggressive follicular variant of PTCGuo et al, Lab Invest 79:67A, 1999
Solid variant of PTCNikiforov et al, Am J Surg Pathol 25:1478,2001
Multinodular follicular variant of PTCIvanova et al, Virchows Arch 440: 418, 2002

Encapsulated follicular variant of papillary thyroid carcinoma with bone metastases
5 cases with minimal invasion and distant metastasesBaloch ZW & LiVolsi VA, Mod Pathol 13:861, 2000
RELATIONSHIP WITH FOLLICULAR CARCINOMA

Follicular variant of PTC
Expanding tumours RAS mutationsVascular invasiveness BRAF K601ELung and bone metastases (No BRAF V600E)Less frequent nodal metast PAX8-PPARγ rearr ?
Aneuploidy?
Zhu et al, Am J Clin Pathol 120:71, 2003Trovisco et al, J Pathol 2002:247, 2004Castro P et al, J Clin Endocrinol Metab, 2006Castro P et al, 2008 (submitted)
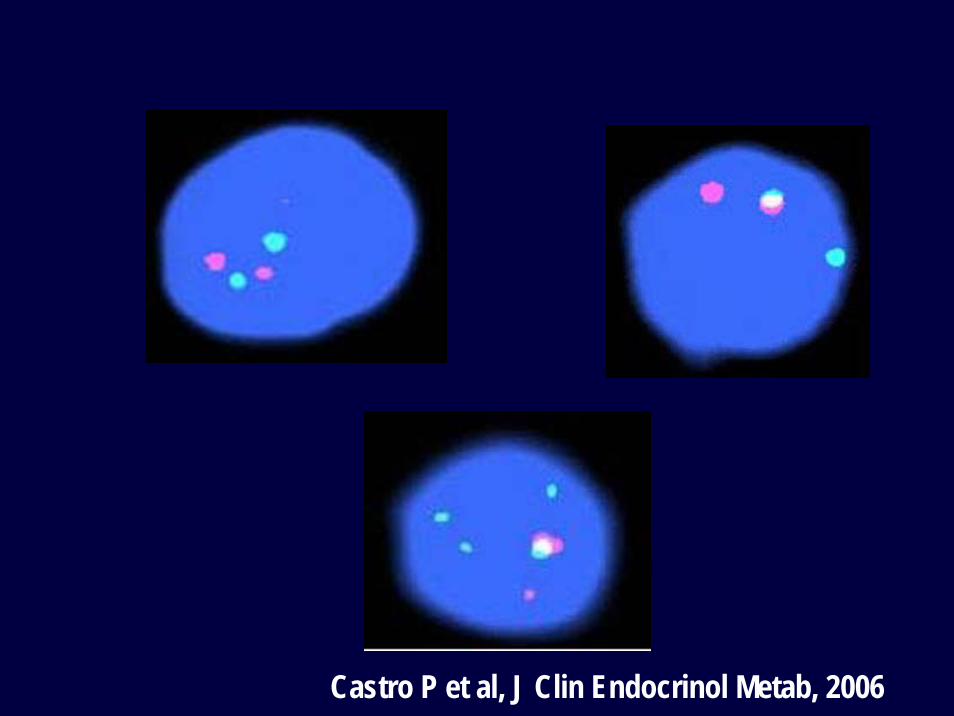
Castro P et al, J Clin Endocrinol Metab, 2006

Follicular variant
Encapsulated follicular variant
PTCPTC
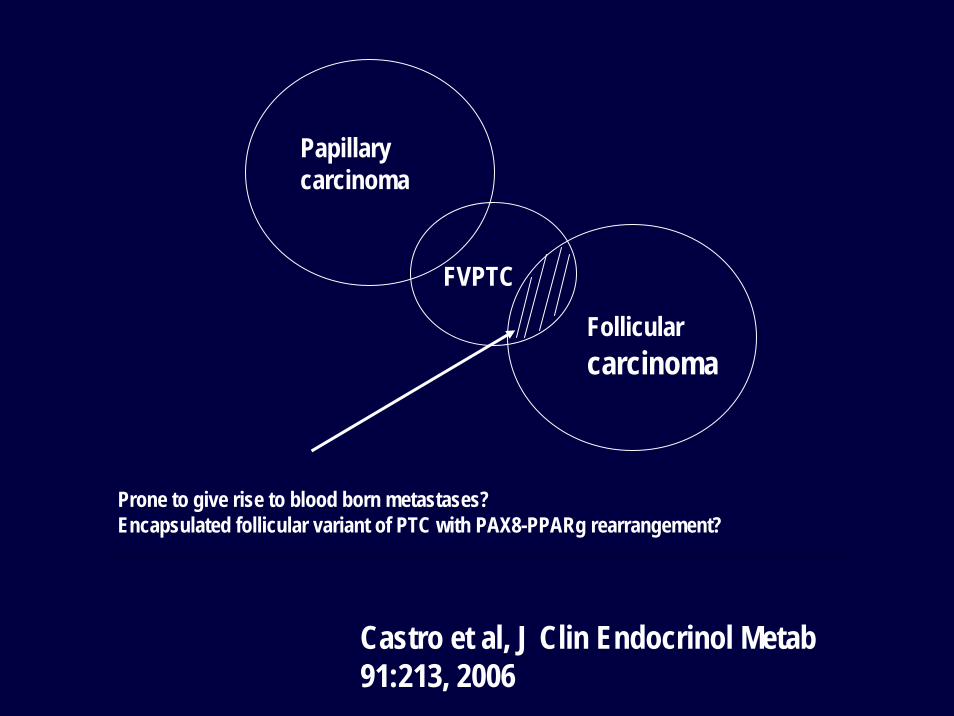
Papillarycarcinoma
Follicularcarcinoma
FVPTC
Prone to give rise to blood born metastases?Encapsulated follicular variant of PTC with PAX8-PPARg rearrangement?
Castro et al, J Clin Endocrinol Metab 91:213, 2006

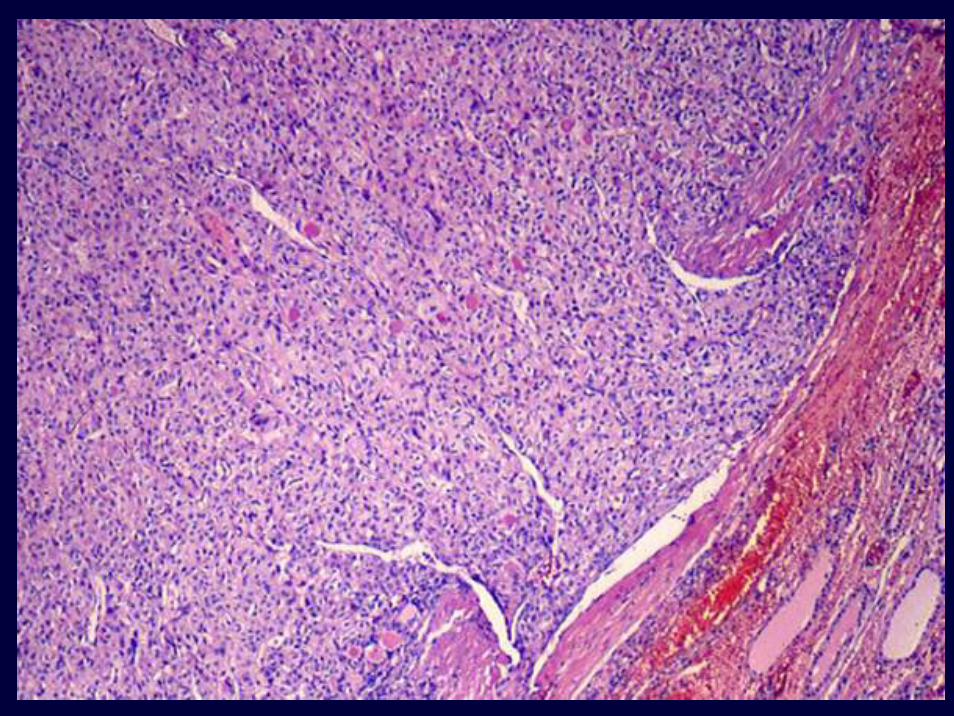
Poorly differentiated carcinoma



Follicular caPoorly diff ca
Undifferentiatedca
Poorly diff ca
Papillary ca
Soares et al, Virchows Arch 444:572, 2004

B-RAF mutations in poorly differentiated carcinomaPure insular carcinoma – no B-RAF mutations
PTC + foci of poorly differentiated ca – with B-RAF mutations
Nikiforova et al, J Clin Endocrinol Metab 88:5399, 2003Soares et al, Virchows Arch 444:572, 2004
MultiMulti--continental study on poorly continental study on poorly differentiated thyroid carcinoma (PDCa)differentiated thyroid carcinoma (PDCa)
Turin, March 3-4 2006

Survival of Data 1:Survival proportions
0 100 200 300 4000
102030405060708090
100110
necrosi 0necrosi 1
Time
Perc
ent s
urvi
val
Survival of Data 1:Survival proportions
0 100 200 300 4000
102030405060708090
100110
mitosi <3mitosi =>3
Time
Perc
ent s
urvi
val
Survival of Data 1:Survival proportions
0 100 200 300 4000
102030405060708090
100110
diagn PDdiagn PTC
Time
Perc
ent s
urvi
val


Volante M et al, Am J Surg Pathol, 2007 (Turin Proposal - Multicontinental study)





IPATIMUP
FACULDADE DE MEDICINA/HOSPITAL S.JOÃO
PORTO, PORTUGAL



















