Approaches for Establishing Clinically Relevant Dissolution Specifications …€¦ · ·...
13
White Paper Approaches for Establishing Clinically Relevant Dissolution Specifications for Immediate Release Solid Oral Dosage Forms Andre Hermans, 1 Andreas M. Abend, 1,10 Filippos Kesisoglou, 1 Talia Flanagan, 2 Michael J. Cohen, 3 Dorys A. Diaz, 3 Y. Mao, 1 Limin Zhang, 4 Gregory K. Webster, 5 Yiqing Lin, 6 David A. Hahn, 7 Carrie A. Coutant, 8 and Haiyan Grady 9 Received 3 February 2017; accepted 16 June 2017; published online 22 August 2017 Abstract. This manuscript represents the perspective of the Dissolution Analytical Working Group of the IQ Consortium. The intent of this manuscript is to highlight the challenges of, and to provide a recommendation on, the development of clinically relevant dissolution specifications (CRS) for immediate release (IR) solid oral dosage forms. A roadmap toward the development of CRS for IR products containing active ingredients with a non-narrow therapeutic window is discussed, within the context of mechanistic dissolution understanding, supported by in-human pharmacokinetic (PK) data. Two case studies present potential outcomes of following the CRS roadmap and setting dissolution specifications. These cases reveal some benefits and challenges of pursuing CRS with additional PK data, in light of current regulatory positions, including that of the US Food and Drug Administration (FDA), who generally favor this approach, but with the understanding that both industry and regulatory agency perspectives are still evolving in this relatively new field. The CRS roadmap discussed in this manuscript also describes a way to develop clinically relevant dissolution specifications based primarily on dissolution data for batches used in pivotal clinical studies, acknowledging that not all IR product development efforts need to be supported by additional PK studies, albeit with the associated risk of potentially unnecessarily tight manufacturing controls. Recommendations are provided on what stages during the life cycle investment into in vivo studies may be valuable. Finally, the opportunities for CRS within the context of post-approval changes, Modeling and Simulation (M&S), and the application of biowaivers, are briefly discussed. KEY WORDS: BCS; biowaivers; clinically relevant dissolution specifications; PBPK modeling; SUPAC. This article was developed with the support of the International Consortium for Innovation and Quality in Pharmaceutical Develop- ment (IQ, www.iqconsortium.org). IQ is a not-for-profit organization of pharmaceutical and biotechnology companies with a mission of advancing science and technology to augment the capability of member companies to develop transformational solutions that benefit patients, regulators, and the broader research and development community. 1 Pharmaceutical Sciences and Clinical Supply, Merck & Co., Inc., West Point, Pennsylvania 19486, USA. 2 Pharmaceutical Technology and Development, AstraZeneca R&D, Macclesfield, Cheshire, UK. 3 Worldwide Research and Development, Global Chemistry and Manufacturing Controls, Pfizer Inc., Eastern Point Road, Groton, Connecticut 06340, USA. 4 Drug Product Science and Technology, Bristol-Myers Squibb Company, New Brunswick, New Jersey 08903, USA. 5 Global Pharmaceutical Research and Development, AbbVie Inc., North Chicago, Illinois 60064, USA. 6 Analytical Development, Biogen Inc., Cambridge, Massachusetts 02142, USA. The AAPS Journal, Vol. 19, No. 6, November 2017 ( # 2017) DOI: 10.1208/s12248-017-0117-1 1537 1550-7416/17/0600-1537/0 # 2017 The Author(s). This article is an open access publication
Transcript of Approaches for Establishing Clinically Relevant Dissolution Specifications …€¦ · ·...

White Paper
Approaches for Establishing Clinically Relevant Dissolution Specificationsfor Immediate Release Solid Oral Dosage Forms
Andre Hermans,1 Andreas M. Abend,1,10 Filippos Kesisoglou,1 Talia Flanagan,2 Michael J. Cohen,3
Dorys A. Diaz,3 Y. Mao,1 Limin Zhang,4 Gregory K. Webster,5 Yiqing Lin,6 David A. Hahn,7
Carrie A. Coutant,8 and Haiyan Grady9
Received 3 February 2017; accepted 16 June 2017; published online 22 August 2017
Abstract. This manuscript represents the perspective of the Dissolution AnalyticalWorking Group of the IQ Consortium. The intent of this manuscript is to highlight thechallenges of, and to provide a recommendation on, the development of clinically relevantdissolution specifications (CRS) for immediate release (IR) solid oral dosage forms. Aroadmap toward the development of CRS for IR products containing active ingredients witha non-narrow therapeutic window is discussed, within the context of mechanistic dissolutionunderstanding, supported by in-human pharmacokinetic (PK) data. Two case studies presentpotential outcomes of following the CRS roadmap and setting dissolution specifications.These cases reveal some benefits and challenges of pursuing CRS with additional PK data, inlight of current regulatory positions, including that of the US Food and Drug Administration(FDA), who generally favor this approach, but with the understanding that both industry andregulatory agency perspectives are still evolving in this relatively new field. The CRSroadmap discussed in this manuscript also describes a way to develop clinically relevantdissolution specifications based primarily on dissolution data for batches used in pivotalclinical studies, acknowledging that not all IR product development efforts need to besupported by additional PK studies, albeit with the associated risk of potentiallyunnecessarily tight manufacturing controls. Recommendations are provided on what stagesduring the life cycle investment into in vivo studies may be valuable. Finally, theopportunities for CRS within the context of post-approval changes, Modeling and Simulation(M&S), and the application of biowaivers, are briefly discussed.
KEY WORDS: BCS; biowaivers; clinically relevant dissolution specifications; PBPK modeling; SUPAC.
This article was developed with the support of the InternationalConsortium for Innovation and Quality in Pharmaceutical Develop-ment (IQ, www.iqconsortium.org). IQ is a not-for-profit organizationof pharmaceutical and biotechnology companies with a mission ofadvancing science and technology to augment the capability ofmember companies to develop transformational solutions that benefitpatients, regulators, and the broader research and developmentcommunity.1 Pharmaceutical Sciences and Clinical Supply, Merck & Co., Inc.,West Point, Pennsylvania 19486, USA.
2 Pharmaceutical Technology and Development, AstraZeneca R&D,Macclesfield, Cheshire, UK.
3Worldwide Research and Development, Global Chemistry andManufacturing Controls, Pfizer Inc., Eastern Point Road, Groton,Connecticut 06340, USA.
4 Drug Product Science and Technology, Bristol-Myers SquibbCompany, New Brunswick, New Jersey 08903, USA.
5Global Pharmaceutical Research and Development, AbbVie Inc.,North Chicago, Illinois 60064, USA.
6Analytical Development, Biogen Inc., Cambridge, Massachusetts02142, USA.
The AAPS Journal, Vol. 19, No. 6, November 2017 (# 2017)DOI: 10.1208/s12248-017-0117-1
1537 1550-7416/17/0600-1537/0 # 2017 The Author(s). This article is an open access publication

PURPOSE
The purpose of this paper is to describe a roadmapfor the development and leverage of clinically relevantdissolution specifications (CRS) for immediate release oralsolid dosage forms of non-narrow therapeutic windowdrugs. There are three objectives for presenting thisroadmap: (1) to describe multiple approaches for estab-lishing clinical relevance for dissolution methodology, (2)to outline how to leverage clinically relevant dissolutionmethodology and specifications for the confirmation of thefinal drug product quality, and (3) to suggest recommen-dations on supporting scale-up and post-approval changesusing the established CRS.
Historically, dissolution specifications have been set bycontrolling the formulation and process within precedentedconditions, and setting the method conditions and acceptancecriteria (=specification) according to current guidance (1).
While this approach is still acceptable, recent ad-vancements in technology and modeling and simulationsignificantly contribute to enhanced product understand-ing. Nevertheless, this enhanced product knowledge hashistorically been underutilized in setting specifications forproduct approval and in support of post-approval changes.Through this approach, the dissolution specification shouldnot only confirm adequate process control but also implyconsistent in vivo performance with respect to efficacy andsafety.
In order to address this gap, we propose a roadmap asdescribed in this article.
BACKGROUND
Since the publication of Janet Woodcock’s final report onpharmaceutical quality for the twenty-first century in 2004(2), pharmaceutical companies have embraced Quality byDesign (QbD) concepts in drug development. Guidance andexpectations are given in regulatory documents includingICH Q8, Q9, and Q10 (3–5). In addition, several publishedarticles, conference talks, and podium discussions are avail-able that discuss this concept at length (6–8). QbD is aprospective approach that provides assurance of robustmanufacture of reliable product quality for patients.
Patients, health care providers, and payers expect medicinesto demonstrate consistent product performance, i.e., safety,quality, and efficacy. A product’s critical quality attributes(CQAs), which are understood during product development,ultimately delineate the boundaries of the product controlstrategy in a registration market application. A product controlstrategy under an enhanced (QbD) approach is represented bythe functional relationship betweenCQAs and the critical processparameters and critical material attributes described in the drugsubstance (also referred to as active pharmaceutical ingredient)and drug product manufacturing processes. Drug substance anddrug product specifications provide confirmation of appropriateprocess control and consistent product quality. However, aproduct control strategy may not assure consistent safety andefficacy unless drug product specifications are clinically relevant.
Clinical relevance requires establishing in vitro acceptancecriteria for dissolution that control against changes in productattributes that could influence in vivo performance as part of thecontrol strategy. This relationship is most simply built byalignment of acceptance criteria against testing results obtainedonmaterials used in pivotal safety and efficacy clinical trials. Forseveral solid oral dosage forms, in vitro dissolution or drugrelease criteria provide a connection to, and serve as a predictorof, in vivo performance. However, this empirical relationshipmay be imprecise depending on, e.g., the BiopharmaceuticsClassification System (BCS) classification of the drug. Recentcommunications from a regulatory perspective have questionedthe clinical relevance of these specifications, and the topic hasbeen the subject of several publications and presentations fromboth regulatory agencies and industry (9–15).
In vitro dissolution testing is used throughout drugproduct development to guide formulation process develop-ment and to control product quality. The goal of thedissolution evaluation is to probe the in vitro rate and extentof drug solubilization to inform selection of formulationcandidates or the impact of process conditions on potentialin vivo performance. At earlier stages of product develop-ment, dissolution experiments under biorelevant conditionsare often applied to rank order formulations for furtherdevelopment or to evaluate if formulation and processvariations could lead to differences in bioperformance. Thehypothesis at this stage of product development is that in vitrodifferences will be reflective of in vivo performance. Thisassumption is continuously tested throughout drug develop-ment as more data are generated that allow for refinement ofthe dissolution method. However, the link between dissolu-tion and in vivo performance is often still theoretic or derivedfrom data from a limited number of batches used in clinicalstudies. It is often difficult to assess whether an observed
Abbreviations: API Active Pharmaceutical Ingredient, AUCArea under Curve, BCS Biopharmaceutical ClassificationSystem, BioRAM Biopharmaceutics Risk AssessmentRoadmap, Cmax Maximal concentration, CMA Critical Mate-rials Attribute, CPP Critical Process Parameter, CQA CriticalQuality Attribute, CRS Clinically Relevant Specifications,EMA European Medicines Agency, FDA Food and DrugAdministration, FIP International Pharmaceutical Federa-tion, ICH International Council for Harmonization of Tech-nical Requirements for Pharmaceuticals for Human Use, IRImmediate Release, IVIVC/R In-vitro-in-vivo correlation/relationship, M&S Modeling and Simulation, MR ModifiedRelease, SUPAC Scale up and Post-Approval Changes,PBPK Model Physiologically Based Pharmacokinetic Model,PD Pharmacodynamic, PK Pharmacokinetic, PSD ParticleSize Distribution, QC Quality Control, QbD Quality byDesign, QRA Quality Risk Assessment, QTPP QualityTarget Product Profile, XR Extended Release
7Genentech, Inc., 1 DNA Way, South San Francisco, California94080, USA.
8 Small Molecule Design & Development, Eli Lilly & Co., LillyCorporate Center, Indianapolis, Indiana 46285, USA.
9 Takeda Development Center Americas, Inc., One Takeda Parkway,Deerfield, Illinois 60015, USA.
10 To whom correspondence should be addressed. (e-mail:[email protected])
1538 Hermans et al.

change in dissolution profile will have a significant impactin vivo. For IR drug products containing highly soluble drugsubstances, a single-point dissolution acceptance criterion forsuitably complete release within 60 min is typically expected.IR tablets formulated with poorly soluble active pharmaceu-tical ingredients (APIs) however often require the addition ofsurfactants to achieve complete release within 60 min whichmay not be reflective of the intraluminal conditions the drugwill experience with oral dosing. In both instances (highly andpoorly soluble drugs), a globally acceptable dissolutionmethod will likely be capable to detect significant process orformulation changes but may not be able to correlate thesewith potential bioperformance changes.
To enhance the understanding of the relevance ofdissolution acceptance criteria to in vivo performance of adrug product, additional investigational work may some-times be needed. For example, identifying which steps inthe manufacturing process are expected to have the mostsignificant impact on the in vivo release rate of the drugproduct may be essential in developing an appropriatein vitro dissolution method to guide drug product devel-opment. The actual capability of such a method todistinguish between batches that meet the desired in vivoperformance needs in vivo investigation to determine whatdissolution changes are significant.
In the past, both industry and regulators acknowl-edged that dissolution product quality Bsameness^ can bedemonstrated by showing similarity factor f2 > 50(SUPAC) (16,17), but neither sameness nor non-sameness may not be clinically relevant, unless thedissolution test is clinically relevant. Thus, using statisticaltools (e.g., f2) to evaluate sameness of product dissolutionmade before and after process and/or formulation changesmay only be meaningful if the method(s) used to monitorthe impact of these changes in vitro is appropriate todetect relevant changes of in vivo exposure. This is a keydriver for developing clinically relevant dissolution tests.
For IR products formulated with a highly soluble drugsubstance (Biopharmaceutical Classification System 1and 3 compounds), a criterion of ≥85% dissolved in 30 or15 min, respectively, is proposed to be acceptable todemonstrate bioequivalence as suggested by the recentdraft FDA dissolution guidance (18). For other immediaterelease solid oral products, the in vivo relevance ofdissolution changes can be addressed by studying the PKbehavior of product made under different compositional orprocess conditions, so-called formulation or process vari-ants, and developing dissolution methods that are sensitiveto changes that are significant. If a PK response is seen forthe different product variants, ideally the next step is to linkthe dissolution data and the observed PK response. Thismay be achieved either with an in vitro/in vivo correlation(IVIVC) that may be established with traditionaldeconvolution/convolution approaches or a physiologicallybased oral absorption/pharmacokinetic model (referred toas oral absorption/PBPK models for the rest of thisdocument). This manuscript describes science-based ap-proaches for establishing clinically relevant specificationsfor immediate release products with a non-narrow thera-peutic window. Some current industry practices for theseapproaches are presented and discussed within the context
of regulatory opinions expressed either during productapplication reviews or in public meetings, publications, etc.
Linking in vitro and in vivo (PK) data with formula-tion and process variants to establish dissolution methodspecifications and to demonstrate that a product will retainits desired bioperformance after formulation or processchanges may present practical challenges in some cases.For instance, drug product developers may find themselvesin situations wherein performing a standalone study toexplore the impact of process variants on in vivo perfor-mance may be difficult or even unethical. Examples includehighly potent compounds that cannot be dosed to healthyvolunteers, such as many small molecule oncology drugs,and controlled substances. In addition, for some drugproducts such as those of orphan drugs or accelerateddevelopment programs, the investment in making multipleproduct variants and performing several relative bioavail-ability studies to support CRS may not be practical. Inthese situations, alternative approaches to ensure that theproposed dissolution method and specification can assuresuitable in vivo performance will be needed, and may relymore heavily on in silico models (typically physiologicallybased pharmacokinetic models) as well as the traditionaluse of dissolution data from materials used during safetyand efficacy studies performed in the clinical program. It isalso worth noting that there may be opportunities forunderstanding formulation behavior (and thus refine disso-lution methods) by leveraging data from other clinicalstudies that are conducted during drug development wheredifferent formulation presentations may be employed. Forexample, it is not uncommon that first-in-human (FIH)studies are conducted with a formulation that differs fromthe formulation which will be developed for further clinicaldevelopment. To determine the most appropriate formula-tion and to support the commercial product, differentformulation variants may be tested in relative bioavailabil-ity studies which may not be dedicated IVIVC studies (19).
CLINICALLY RELEVANT SPECIFICATIONROADMAP
BClinically relevant dissolution specification^ implies thatthe in vitro dissolution method confirms acceptable in vivoperformance of the product. A biorelevant dissolutionmethod, which by a definition suggested by the FIP isperformed in aqueous media resembling the intraluminalenvironment the drug product passes through during admin-istration, can also be clinically relevant. In contrast, aclinically relevant dissolution method can be performed inBnon-biorelevant^ dissolution media as long as the methodand acceptance criteria are capable of confirming orpredicting in vivo performance of the drug (20–22). Everydrug product manufacturing process is subject to variability,and it is expected that a clinically relevant dissolution methodis capable of discriminating if these variations have, or do nothave, an impact on product in vivo performance. The sourcesof this variability may stem from differences in raw materials,including the drug substance and excipients, differences inprocessing conditions, and even changes in the day-to-dayenvironmental conditions. Within the context of thorough
1539Approaches for Establishing Clinically Relevant Dissolution Specifications for Immediate Release Solid Oral Dosage Forms

product development, such variability can be evaluated forsignificance.
It can be challenging to judge if this variability has animpact on product bioperformance by solely relying on adissolution method and acceptance criteria without establish-ing an understanding of the in vivo (in-human) relevance ofthe method, or, alternatively, without establishing tightacceptance criteria to assure similarity. Therefore, under-standing the link of dissolution performance to pharmacoki-netic performance can be a key factor in developing productunderstanding and can play a major part of the developmentstrategy and product life cycle management.
The approaches described below on how to establishclinically relevant dissolution specifications for immediate releasesolid oral dosage forms are based on the interpretation ofmeetingmaterials and publications issued by scientists working forregulatory agencies and in the pharmaceutical industry (9–15).
During development, drug products should be designedwith the patient in mind, wherein the Target Product Profile(TPP) delineates attributes of the product to be delivered tomeet patient safety, efficacy, quality, and suitability for adminis-tration. TheQuality Target Product Profile (QTPP) identifies thespecific product Critical Quality Attributes (CQAs) required todeliver the desired TPP. How to achieve these quality character-istics is evaluated during formulation and process development.Aspects that may significantly impact in vivo performance areoften assessed by in vitro dissolution. Therefore, developing anenhanced understanding of the dissolution mechanism and howformulation and process variables influence dissolution isfundamental for developing clinically relevant criteria.
The role of dissolution testing, and the test employed, maychange during development of the product. Early in development,a variety of explorative approaches (i.e., dissolution in biorelevantmedia (23), multi-stage dissolution (24,25), biphasic/multi-compartmental (gastro-intestinal models) (26), dissolution innon-sink conditions, etc.) or dissolution in multi-pH media canbe used to evaluate the possible impact of formulation and processfactors on the in vivo performance of the dosage form. In earlydevelopment, data from these methods along with other physico-chemical information, such as permeability, can be combined withphysiologically based oral absorption/pharmacokinetic modeling
to predict formulation performance in anticipation of clinicalstudies. These models can be further refined as more data becomeavailable. Application of such models can significantly enhanceformulation and process development and the assessment ofbiopharmaceutics risk factors. The use of this type of physiolog-ically based pharmacokinetic (PBPK) model has been a subject ofseveral recent publications (27,28).
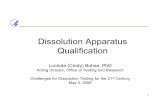
Understanding the dissolution mechanism of a drug productand identifying which aspects of the formulation and manufactur-ing process have themost significant impact on the in vitro releaserate are critical in developing a dissolution method. Figure 1illustrates the mechanistic steps involved when a typical solid oraldosage formdissolves. The dissolution process can be divided intothree steps: tablet erosion/disintegration into granule particles,granule disintegration into primary drug particles, and APIdissolution. Potential CQAs, potential Critical Process Parame-ters (CPPs), and potential Critical Material Attributes (CMAs)are listed for each of the three mechanistic steps. These aretypically the focus of evaluation in development, and build thefoundation of enhanced product understanding.
In early drug product development, where differentformulations and processes are considered, changes in bothcomposition and process can impact each of these dissolutionevents differently. For a given formulation and manufacturingprocess, compositional and process variants may affect one ofthese dissolution steps more strongly than the others.Experimentation such as disintegration, intrinsic API disso-lution, and granule dissolution can help in understanding therelative contribution of each step to the overall dissolutionrate.
If the rates of the mechanistic steps shown in Fig. 1 arevery different, then the slowest step determines the overalldissolution rate. In this case, the effect of variations informulation and process factors likely to impact this slowestdissolution step should be most closely evaluated. CPPs andCMAs can be identified through this process.
As part of selecting the QC dissolution method for theproduct, one is often faced with the challenge of valuing andevaluating the discriminating power of the method. In order toaddress this challenge, one can perhaps study the impact of theaforementioned CPPs and/or CMAs in clinical studies, or one
Tablet GranulesAPI Particles
Solubilized drug
Dosage Form Dissolution
Tablet disintegration controlled dissolution
Granule disintegration controlled dissolution
API controlled dissolution
Cohesive properties of the formulation
Cohesive properties of the granules
Solublization of the API, Wetting of API
Disintegration, Hardness, Tablet porosityCompression force, disintegrant level
Granule PSD, Granule Strengths, Granule porosity, Granulation fluid level, roll pressure
API PSD, API Forms, Crystallization process
Rate Limiting Step
Mechanism of release
CQAs, CPPs, and CMAs(examples)
Precipitation
Fig. 1. Typical dissolution mechanism and factors to explore when developing IR solid oral dosageforms
1540 Hermans et al.

might accept tight specifications and mitigate potential biophar-maceutical risk by setting tight manufacturing controls.
When performing these development activities, the BCSclassification system can aid in estimating if process/formulationvariations and changes in product dissolution are likely to have animpact on in vivo performance (29). The recent draft FDAdissolution guidance (18) suggests that immediate release solid oraldosage forms comprising highly soluble compounds, which achieve≥85% dissolved in 500 mL of 0.01 N HCl with gentle agitation ineither 30 min (BCS class 1) or 15 min (BCS class 3), provideassurance that they will deliver similar bioperformance. In otherwords, aQof 80% (i.e.,≥85%dissolved) in 15min (BCS class 3) or30 min (BCS class 1) should be considered clinically relevant.
In all other cases, such as BCS classes 2 and 4 or BCSclasses 1 and 3 that do not meet the aforementioneddissolution criteria, applying the f2 similarity factor vs. lotsused in pivotal clinical studies can be a useful baseline,although likely conservative, approach to mitigate biophar-maceutical risk if the method is appropriately discriminating.
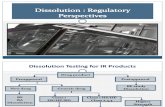
To extend understanding, IVIVC/Rs and/or oralabsorption/PBPK models in conjunction with data frompreclinical (animal) models can also be used to probe theimpact of changes in the dissolution profile (e.g., resultingfrom formulation and process changes) on the PK profile.The results from these simulations can then be used to refineunderstanding of the biopharmaceutical risk. It is also worthemphasizing that this biopharmaceutical risk evaluation iscontinuously facilitated by generated clinical data that allowfor further evaluation of the in vivo relevance of thedissolution method and appropriate refinements as needed.Typically, a sponsor’s strategy to understand and controlbiopharmaceutical risk can be described by two generalapproaches, as depicted in Fig. 2. These approaches aredescribed in more detail below. Approach 1. The sponsormay determine that little additional PK evaluation may beneeded, as processing and compositional controls are avail-able to mitigate against any significant biopharmaceuticalrisk. In this case, in vivo studies using formulation variants
would not be performed and manufacturing would continuewithin established ranges/parameters. For drug productscomprising BCS classes 1 and 3 that exhibit rapid or veryrapid dissolution (i.e., ≥ 85% dissolved in 30 or 15 min,respectively), the dissolution criteria could be set accordingly.For other drug products, the dissolution method and specifi-cation criteria would be established to prevent significantvariations vs. batches used in pivotal clinical trials andregistration stability batches. As these batches would havebeen made under conditions that are representative of thefinal commercial product manufacturing process and theclinical batches would have been used to demonstrate clinicalsafety and efficacy, the dissolution specification would bederived from these batches and thus assure in vitroperformance.
Additionally, if the dissolution specification and methodare established with no additional PK studies of formulationvariants, this may add further challenges for scale-up andpost-approval changes; depending on the level of the change,these changes often require f2 dissolution similarity (either inthe QC method or in multi-pH media, and water) or, if thoserequirements are not met, require a bioequivalency study.Approach 1 may be at risk of generating specification criteriathat are conservative, such that lots that fail the specificationmay not in fact have unacceptable PK performance. Thus,justification of potentially Bwider^ specifications based onenhanced in vivo product understanding as explained belowmay be more desirable.
Approach 2. In this scenario, the sponsor may utilizeadditional bioavailability evaluation in order to furtherexplore the impact of formulation and/or process variabilityand dissolution differences on PK performance. For the PKstudy, ideally, formulation or process variants are chosen toprovide a range of dissolution responses to support a deeperproduct understanding and wider manufacturing conditions.
The outcome of these PK studies can yield informationmeeting the following four scenarios: IVIVC Level A, IVIVC
Sponsor decision to perform in-vivo
studies with process variants?a
Control formulation and process within precedented conditions
Traditional approach
Specification according to current
guidance
Study impact of formulation and/or process variations on in-vivo
performance
2a. Level A IVIVC
Specification based on IVIVC model
2b. Level C IVIVC
Specifications based on IVIVC model
2c. Safe Space
Specifications based on safe space
2d. In-Silico IVIVe
Specifications based on in silico model
No YesApproach 1 Approach 2b
a Sponsor may reevaluate as more data become available and change which approach is most appropriateb When pursuing Approach 2, aspects such as analytical method variability and manufacturing process history will also be taken into account when selecting the final specification within the established window of acceptable clinical performance.
Fig. 2. Decision tree to develop clinically relevant specifications
1541Approaches for Establishing Clinically Relevant Dissolution Specifications for Immediate Release Solid Oral Dosage Forms

Level C, clinically established Bsafe space,^ and establishmentof an in silico IVIVe.
1. An IVIVC Level A can be established if thedissolution method is predictive of in vivo PKperformance. In this case, the method can be used tojustify acceptance criteria and manufacturing condi-tions based on target PK parameters. An IVIVCLevel A supersedes the f2 similarity requirements andis acceptable from a regulatory perspective whenapplying for a biowaiver to support scale-up andpost-approval changes.
2. An IVIVC Level C is established where only one orseveral PK parameters correlate with one or multipledissolution time points. Therefore, the dissolutionmight not be predictive of the entire PK profile. Forimmediate release products, setting a dissolutionspecification for the QC method may be based onthe lower range of the IVIVC model (10% change inPK parameters relative to the target).
3. A clinically established Bsafe space^ for dissolutioncan be established when formulation/process variantsdemonstrate acceptable PK performance, but thedissolution method can discriminate those variants.A dissolution specification for the QC method can bejustified based on the limits of the release profiles usedin the PK studies.
4. In silico IVIVe (in vitro/in vivo extrapolation)—in thisscenario, the link between the in vitro dissolution andthe observed pharmacokinetic response is establishedvia the use of a physiologically based absorption/pharmacokinetic model, and the model is used toidentify dissolution profiles that are projected toensure the desired clinical performance.
There are limited examples of Level A IVIVCs for IRproducts reported in the literature, and any level of IVIVCmay not be expected for BCS 1/3 drugs or BCS 4 drugs withvery low permeability as the dissolution rate in these cases isnot the rate-limiting step to absorption. On the other hand,establishing an IVIVC Level C or a clinically established safespace may be realized for most drug products.
It should be noted that once the window of acceptabledissolution performance from a clinical perspective has beenestablished under approach 2, other aspects of qualityevaluation such as complete release, analytical andmanufacturing process variability, and batch experienceshould also be taken into account when setting the finalspecification criteria within this range; in particular, it isdesirable to avoid specifications set too tightly within thewindow of acceptable clinical performance that could result inthe failure of clinically acceptable batches. A detaileddiscussion of the broader aspects of specification setting isbeyond the scope of this manuscript; however, its impact ishighlighted in the examples below.
In addition to setting clinically relevant dissolutionspecifications for finished product release as described above,similar concepts can be applied to setting acceptance criteriafor formulation/material attributes. For example, the drugsubstance particle size distribution (PSD) often has an impacton drug product dissolution (Fig. 1). According to approach
1, understanding dissolution profiles of drug product madewith API batches covering the expected PSD range of pivotalclinical batches would establish a way to ensure consistentproduct performance. Limits could be applied to the PSDrange to ensure that significant changes in dissolution rate arenot observed supported by in vitro dissolution testing with anappropriately discriminating method. Alternatively, followingthe logic presented in approach 2, drug product variants madewith API batches covering the projected commercial APIPSD range could be studied in vivo and compared to the PKperformance of pivotal clinical studies. In either case, thePSD ranges can be justified; the in vitro dissolution methodcan be correlated with PSD and clinical data, and henceprovide for clinically relevant specifications.
This specification setting strategy can be applied to otherCMAs such as granule particle size, surface area, andlubricant levels, or drug substance properties such as APIform changes and API disproportionation, or direct tabletproperties such as hardness and porosity. Ultimately, thisapproach, which is based on sound product and processunderstanding, might lead developers to set specificationsbased on well-understood underlying CQAs, as opposed todepending on dissolution testing.
As mentioned above, during initial formulation andprocess evaluation and selection, dissolution may be con-ducted with a range of methods including non-traditional andtraditional QC methods. Data from both types of methodscan then be used to explore whether a direct linkage betweendissolution and PK performance can be achieved (approach2). With this information in hand, one can justify selection ofappropriately discriminating method conditions (i.e., surfac-tant levels, pH, agitation speeds) and acceptance criteria for aQC method. If the QC method shows similar clinicalrelevance compared to the more complex method, then onlythe QC method would be used for product release and tojustify formulation and process changes. On the other hand,the QC method, which from a company’s perspective shouldbe globally acceptable, may not be capable to demonstrateacceptable PK performance of extreme process and formula-tion variants. In this case, the QC method conditions andacceptance criteria are set to assure adequate product qualitycontrol for products made under standard/routinemanufacturing conditions. In addition, a sponsor may usethe second, more complex dissolution specification that isindicative of acceptable clinical performance to supportproduct quality investigations or specific post-approvalchanges. The reason for not using the complex dissolutionmethod for routine product release could be based on lack ofmethod robustness or concerns of global regulatory accep-tance when using non-traditional, perhaps novel technology.
It is worth noting that while the discussion above focuseson responding to the outcome of the clinical studies, anotherimportant aspect of the CRS roadmap is to foster improvedclinical study design to achieve this desired outcome. Inparticular, dissolution data, along with oral absorption/PBPKmodeling, guide the rational design of PK studies to establisha likely safe zone or IVIVCs for the critical formulation/process parameters. Following the completion of a PK studyto link in vitro and in vivo performance, any previouslyestablished model(s) can be used (or further refined) tomechanistically understand the output by identifying the key
1542 Hermans et al.

contributing factors for absorption, and characterizing theinterplay between formulation performance and physiologicalfactors. The utility of this approach to establish CRS is brieflydiscussed later in this manuscript.
As more data become available, the sponsor may decideto change the approach as deemed necessary. For example, ifthe sponsor originally embarked on approach 1 but foundthat the appropriate control of one of the critical parameterscould not be guaranteed in a commercial setting, the sponsormay elect to run additional PK studies to support the requiredrange (approach 2). Similarly, if the sponsor originallyembarked on a plan to develop an IVIVC but later assessedthat the bioperformance risks are manageable throughreasonably tight process controls, the sponsor might electinstead to accept the traditional approach of setting specifi-cations according to approach 1. Either of these should beconsidered acceptable.
CASE STUDIES
Two case studies are presented demonstrating outcomes2b and 2c as described in Fig. 2. In case study 1, a multipleLevel C IVIVC was established. This relationship was used tosupport a clinically relevant specification and in-processcontrol on tablet hardness. For case study 2, a pharmacoki-netic safe space was established. This study also highlights thechallenges of applying this approach currently in a globalenvironment.
Case Study 1: Utilization of Dissolution MechanismUnderstanding and Multiple Level C IVIVC to InformClinically Relevant Specifications for Suvorexant SolidDispersion Tablets (30)
Suvorexant is an orexin receptor antagonist approved forthe treatment of insomnia in the USA (Belsomra™). Theactive ingredient is a BCS class 2 compound formulated as anamorphous solid dispersion to enhance its inherently lowcrystalline solubility. Following the principles outlined underthe CRS roadmap, during formulation development increasedemphasis was placed on understanding the dissolutionmechanism. Suvorexant tablets are manufactured via directcompression of a milled solid dispersion intermediate mixedwith excipients. Therefore, the dissolution can be described asa two-step process: tablet erosion or disintegration followedby dissolution of the amorphous intermediate particles.During formulation development and scale-up, tablet erosion,and not API/solid dispersion intermediate dissolution, wasdemonstrated to be the rate-limiting step for overall dissolu-tion of the dosage form. The CMA-controlling tablet erosionfor the suvorexant formulation was found to be tablet solid
fraction, which can be modulated by changes in tablethardness and moisture.
Following the CRS decision tree (Fig. 2), a relativebioavailability study with four batches of tablets with varyinghardness was executed to probe the impact of tablet erosionon in vivo performance. Tablet hardness was selected tobracket the dissolution of phase 3 supplies and to also resultin sufficient dissolution difference1 between batches to enabledevelopment of correlations between dissolution and PK.Given that Level A IVIVCs are generally consideredchallenging for IR products, at the time of study executionthe primary goal was the development of a multiple Level CIVIVC (outcome 2b in the CRS roadmap).
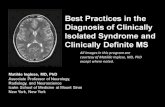
The study outcome and the development of the multipleLevel C IVIVC have been detailed in a previous publication (30).While tablet hardness did not impact the extent of absorption(AUC), modest differences in the rate of absorption (Cmax) wereobserved. Figure 3 shows the target dissolution profile along withtwo sets of boundaries, those set according to the f2 test and thoseset via the IVIVC. The target commercial manufacturingdissolution profile (black line) was based on the dissolutionbehavior observed with the phase 3 formulation. The f2 bounds(+/− 10%) around that profile, which are typically used to assessdissolution similarity for post-approval changes, are representedby the dashed lines. The magenta lines represent the estimatedbounds from the IVIVCmodel that would ensure bioequivalenceas defined by changes in Cmax within ±10% relative to the targetdissolution. It is apparent that applying strict f2 criteria, implying adissolution specification of approximatelyQ= 80% in 20min (i.e.,≥85% dissolved in 20 min), is too conservative and not reflectiveof the in vivo performance of the formulation. The understandingof the dissolution vs. Cmax response led to clinically relevantdissolution bounds outside the f2 range, while still ensuringconsistent bioperformance of future batches.
Furthermore, as a link between formulation properties anddissolution is established, the IVIVC can be further utilized toinformmanufacturing conditions/in-process controls. For the caseof suvorexant tablets, the dissolution data were correlated totablet tensile strength across potencies as described before (Fig.4). This relationship was used to set an upper limit on tablettensile strength and, through that parameter, tablet hardness.Tablet friability was used to set the lower limit. In thismanner, this
1 If f2 was chosen to guide product development and toassess potential future risk with post-approval changes, oneshould consider selecting process variants that would fail thef2 > 50 requirement so that those post-approval changescould be potentially justified provided acceptablebioperformance is demonstrated.
0
20
40
60
80
100
120
0 10 20 30 40 50 60 70
% D
isso
lved
time (min)
Target Dissolution Profile
Upper F2 limit
Lower F2 Limit
Upper IVIVC limit
Lower IVIVC Limit
Fig. 3. Phase 3 Btarget^ dissolution, corresponding f2 range, andIVIVC-estimated bioequivalent dissolution space for suvorexant IRtablets
1543Approaches for Establishing Clinically Relevant Dissolution Specifications for Immediate Release Solid Oral Dosage Forms

approach can contribute to the development of an effectivecontrol strategy where end-product testing (i.e., dissolutiontesting) serves as a final confirmation of the quality and requiredquality is built in at a more fundamental, and earlier, level.
In addition to informing the bioequivalent dissolution spacefor the dissolution specification (and subsequently hardness limits)for the suvorexant tablets, the IVIVC developed was also appliedto project bioequivalence (BE) for different strength tablets(dose/weight multiples). Given the erosion mechanism, lowerstrengths (i.e., smaller tablets) dissolve faster, such that dissolutioncomparisons did not meet the f2 criterion. Given that multiplestrengths were considered at that time of development, demon-strating interchangeability for weight multiple tablets was desiredfor specific markets. To assess the bioequivalence for 2 × 20mg vs.1 × 40 mg and 2 × 15 mg vs. 1 × 30 mg tablets, the IVIVC modelwas applied. Based on the 20-min dissolution time point, themaximal differences projected between 2 × 15 mg and 1 × 30 mgtablets was 9.5% on Cmax (projected differences for 2 × 20 mg vs.1 × 40 mg were smaller). The IVIVC projections were utilizedinternally to design and power a bioequivalence study to compareweightmultiple formulations. As shown in Table I, bioequivalencecriteria weremet for both comparisons attempted (bothAUC andCmax) in line with the predictions of the IVIVC Level C model.The successful prediction of bioequivalence for these tablets canbe also considered an external validation of the IVIVC model.
In summary, the establishment of a multiple Level C IVIVCfor this product enabled a better understanding of the clinical (inthis case pharmacokinetic) impact of process changes and
dissolution. This increased product understanding is at the heartof a QbD strategy. The data from the IVIVC can be used toestablish clinically relevant specifications and adequate in-processcontrols.
Case Study 2: Developing Clinically Relevant Specificationfor a BCS Class 4 Immediate Release Product—Establishinga Pharmacokinetic BSafe Space^
The second case study presented describes the develop-ment of a clinically relevant dissolution test and acceptancecriterion for a BCS class 4 compound, formulated as animmediate release tablet. While the first case study resulted inan IVIVC, this example discusses the demonstration of apharmacokinetic safe space to define the acceptable perfor-mance bounds of formulation changes.
Compound X is a BCS class 4 compound with poorsolubility (<10 μg/mL) in buffers within the physiological pHrange. However, the compound demonstrates solubility of0.5 mg/mL in human intestinal fluid. The physicochemicalproperties of compound X are summarized in Table II.
The first step in establishing a clinically relevant dissolu-tion test for compound X was to identify the most relevantrisks to in vivo dissolution. The product is manufactured by astandard wet granulation process, and the formulationincludes a superdisintegrant to facilitate rapid disintegrationand dissolution. As API particle size and crystalline form hadalready been fixed in an area of low risk, Quality Risk
0102030405060708090
100110
0.00 0.50 1.00 1.50 2.00 2.50 3.00
%D
isso
lved
-20
min
Tensile Strength/SA/V (MPa*mm)
15 mg 20 mg30 mg 40 mgIVIVC - Upper Boundary IVIVC - Lower Boundary
Tablet Image(mg)
Hardness Limit (kP)
Lower Upper
15 11 20
20 8.5 16.5
30 8.5 19.5
40 15 27.5
Fig. 4. Relationship between dissolution and tablet strength and translation to hardness limits for in-process control (30)
Table I. Application of Multiple Level C IVIVC to Estimation of Bioequivalence for Different Strength Suvorexant Tablets and Comparisonto BE Study Outcome
Tablet strength AUC0-t prediction AUC0-t BE results Cmax prediction based on IVIVC(20 min time point)
Cmax results
2 × 20 mg vs.1 × 40 mg
IVIVC not applied. AUC notsensitive to dissolution
102.52% (99.09–106.07) 105.3% 96.58% (90.96–102.55%)
2 × 15 mg vs.1 × 30 mg
IVIVC not applied. AUC notsensitive to dissolution
99.71% (96.66–102.75%) 109.5% 108.74% (101.10–116.95%)
1544 Hermans et al.

Assessment (QRA) had identified granulation parametersand disintegration time (e.g., due to a change in theperformance of the binder or superdisintegrant) as thehighest risks. Process and formulation variants were thenproduced which investigated ranges for these risks, asdescribed in Table III. The critical mechanisms of over-granulation and over-compression were combined to createlarger changes in dissolution performance.
Dissolution tests were conducted to assess the potentialimpact of these highest risk failure mechanisms. The pooraqueous solubility of compound X meant that aqueous buffersat physiologically relevant pHs were unsuitable for use asdissolution media, as less than 10% of the dose would dissolvein a 900-mL volume. Surfactant-containing media were there-fore investigated. Tablet performance was also assessed inFasted State Simulated Intestinal Fluid (FaSSIF), as a knownbiorelevant medium, for comparison. The process and formula-tion variants showed slower dissolution in all of the mediaassessed (Fig. 5); different degrees of discrimination wereobserved, but the rank order of profiles was the same.
The next step was to determine the in vivo impact of thein vitro differences observed. As compound X is characterized
as BCS class 4, a clinical relative bioavailability study wasconducted to evaluate the in vivo impact of the dissolutiondifferences. A study was performed (in healthy volunteers),comparing exposures from the tablet variants to the standardclinical tablet, as well as an oral solution.
All of the tablet variants were found to be bioequivalentto the standard tablet (Table IV). Figure 6 shows thegeometric mean pharmacokinetic profiles obtained. Althoughthe profiles appear to show some differentiation, examinationof individual PK data demonstrated that there was noconsistent rank order for the tablet variants vs. the standardtablet between individual subjects in the study. The oralsolution showed a slightly higher Cmax than the tablets.
These data were then used in conjunction with thediscriminating dissolution methods to allow a specification to beset that assures in vivo performance. The clinical study hadestablished a range of in vitro dissolution profiles within whichbioequivalence was assured, enabling a safe space for dissolutionperformance to be defined (9). The study had shown that thein vitro dissolution methods in Fig. 5 all discriminate for changesin in vitro performance which do not impact in vivo performance,so any of the dissolution methods would be suitable for use as aclinically relevant QC method using the safe space approach. Arelease profile anywhere within the identified region of bio-equivalence in any one of these tests would be suitable to assureclinical quality. In this instance, the project team selected one ofthe surfactant-based media with a similar degree of discrimina-tion to FaSSIF as a QC release test. Preliminary discussions withFDA regarding appropriate discriminating power indicated apreference for a method with more discrimination for the initialrate phase than was seen with surfactant 1.
The clinically relevant dissolution method and specificationwere used during subsequent product and process developmentto assess the impact of lower risk variables that had not beenevaluated in the clinical study. The clinically relevant dissolutiontest and specification are therefore an integral part of the widercontrol strategy, ensuring that every tablet produced duringcommercial manufacture will be bioequivalent to those dosed inthe pivotal safety and efficacy studies.
At the time of filing themarketing applications, a dissolutionspecification of Q = 70% (i.e., ≥75% dissolved) at 45 min wasproposed. This was accepted by all agencies except US FDA,who requested aQ = 80% (i.e.,≥85%dissolved) specification, toprovide assurance of complete release. Following discussion withthe Agency, a two-point specification of Q = 70% at 45 min andQ = 80% at 60 min was agreed; the sponsor stated their intentionto review the need for a two-point specificationwhen a significantbody of commercial batch data was available.
pt?>As more experience of variability during routine com-mercial manufacture was gained, statistical modeling ofmanufacturing process performance identified a risk that clinicallyacceptable batches from within the defined safe space forcompound X could potentially fail specification. This was aparticular risk for the Q = 80% in 60 min US specification, whichwas set relatively tight for such a highly discriminating in vitro test.Based on these data, further dialog was sought with FDA, and theUS specification was successfully re-negotiated to Q = 75% at60min, significantly reducing the risk of failing clinically acceptablebatches. This highlights a key value of a clinically relevantdissolution test and associated pharmacokinetic safe space, asdeveloped for compound X. This also highlights the importance of
Table II. Physicochemical Properties of Compound X
Solubility inaqueous buffers
<10 μg/mL across the physiologicalpH range
Solubility inbiorelevant media
0.5 mg/mL in human intestinal fluid
Permeability Moderate permeability in Caco-2cells; absolute bioavailability 36%
Table III. Tablet Variants Incorporating Highest Risks to In VivoDissolution
Description Dissolution RisksAddressedfrom QRA
Variant A Process variant: over-granulated andover-compressed
Granulation (high risk);compression (mediumrisk); change in fillergrade causing change ingranulation orcompressionbehavior (medium risk)
Variant B Process variant: over-granulated (extreme)and over-compressed,only large (>1 mm)particles used forcompression
Granulation (high risk);compression (mediumrisk); change in fillergrade causing change ingranulation orcompressionbehavior (medium risk)
Variant C Formulation variant:increase the amount ofbinder and reduce theamount of disintegrant toslow tablet disintegration
Binder—change in grade(high risk);disintegrant—changein grade (medium risk)
1545Approaches for Establishing Clinically Relevant Dissolution Specifications for Immediate Release Solid Oral Dosage Forms

considering the constraints of a commercial manufacturing envi-ronment in setting the final specification.
During the development of the above referenced IR tablet,two clinically relevant dissolution methods were identified aspotentially being suitable for routine batch release of this product.One method, using a pH 1.2 aqueous buffer, only discriminatedfor the most slowly dissolving tablet variant. The second methodused a medium containing 0.5% surfactant and was able todiscriminate between all of the variants dosed in the study, similarin discriminatory power to the biorelevant FaSSIF medium. Inthe marketing applications, the sponsor proposed the surfactantmethod with an associated single-point specification. Differingfeedbackwas obtained from regulatory authorities globally on thesuitability of the method and the proposed specification; this hasbeen described by Timko et al. (31). In brief, US FDAagreed thatthe surfactant method was suitable for use as a pharmaceuticaldevelopment tool, but noted that it could be overly sensitive forchanges in product performance that had no impact clinically.FDA requested that the pH 1.2 method be used for batch release,as this was considered to be more biorelevant, while otherregulatory authorities, including EMA and Health Canada,accepted the originally proposed surfactant-based method.
Both methods and acceptance criteria can be consideredclinically relevant, as they would pass clinically acceptable
batches and fail batches with unacceptable bioperformance.This example highlights that there can be differing QCdissolution testing strategies based on country-specific regu-latory expectations. In this case, the divergence in regulatoryexpectations have resulted in a more complex global supplychain, with different QC dissolution tests and specificationsused to release batches in different regions. Taken together,this example and the case study described above illustratethat this is an evolving area of regulatory and pharmaceuticalscience, which warrants further investigation and discussion.
SELECTION OF APPROPRIATE TOOLS FORESTABLISHING CRS
TheCRSprinciples outlined in thismanuscript are in linewiththe FDA’s dissolution guidance from 1997 for IR products and therecently proposed Biopharmaceutics Risk Assessment Roadmap(BioRAM) which calls for the use of preclinical tools and clinicalstudies to gradually develop the product understanding in order tomaximize patient benefit. As discussed in the correspondingBioRAM manuscript (32), generalized delivery scenarios can beassigned to help identify a drug product’s critical performanceattributes. The same concepts could be applied to selecting theappropriate tools for generation of a clinically relevant dissolutionspecification. For example, for MR products, it is generallyaccepted that the entire time course of the plasma concentrationprofile is important in the majority of cases; thus, as reflected incurrent regulatory guidances, Level A IVIVCs are preferred. Incontrast, for IR products where efficacy/safety is typically linked toa summary pharmacokinetic parameter (e.g., AUC,Cmax,Ctrough),Level C IVIVCs (ideally multiple Level C IVIVCs) may beadequate to ensure product performance. The individual drugefficacy/safety characteristics and established margins would needto be taken into account. For certain products and indications, onemay be just looking for a change in Cmax with little effect offormulation variants onAUC. IfCmax is important for efficacy (e.g.,an analgesic drug), CRS should focus on characterizing that
Fig. 5. Dissolution of the tablet variants in FaSSIF and three surfactant-containing media
Table IV. Comparison of Exposures from the Tablet VariantsCompared to the Standard Tablet, According to Standard Bioequiv-
alence Criteria
AUC Gmean
ratio (90% CIs)CmaxGmean
ratio (90% CIs)
Variant A/standard tablet 0.97 (0.90, 1.05) 1.05 (0.95, 1.16)Variant B/standard tablet 1.02 (0.94, 1.10) 1.04 (0.94, 1.15)Variant C/standard tablet 0.97 (0.89, 1.05) 0.91 (0.83, 1.00)
1546 Hermans et al.

relationship to formulation parameters. On the other hand, if thedrug is used for an indication where AUC or Ctrough is important(e.g., anti-viral), the safe space concept applied toAUCmay be thebest surrogate to establish a product specification.
In recent years, utilization of physiologically based oralabsorption/pharmacokinetic models related to biopharmaceuticsand formulation performance has been significantly increasingwithin the industry. Several publications both from industry andfrom regulatory agencies have highlighted the potential use ofsuch models, understanding formulation critical attributes anddissolution performance. For example, Zhang et al. demonstratedhow oral absorption/PBPKmodeling could be used to understandthe in vivo performance of generic IR and XR carbamezepineformulations and identify the important characteristics in therelease mechanisms that should be reflected in a dissolution test(33). More recently, Mitra et al. described the use of models toassess the impact of dissolution differences observed betweenbatches manufactured at different sites for etoricoxib (34). Thesimulations showed that the dissolution differences (outside f2bounds) observed at pH 4.5 and 6.8 during multimedia testingwere not clinically relevant, while the dissolution at pH1.2 (f2 > 50)would be a better predictor of clinical performance. Results from abioequivalence study confirmed the outcome of the simulations.Finally, Pepin et al. recently published their experience withutilizing absorption/PBPK modeling to justify drug productdissolution and drug substance particle size specification forZurampic® (lesinurad) IR tablets (35). While a detailed reviewof the development and application of such physiologically basedoral absorption/pharmacokinetic models is beyond the scope ofthis manuscript, the three examples highlighted demonstrate thepotential utility of modeling in conjunction with the moretraditional IVIVC approaches and the safe space conceptdiscussed in the case studies to develop CRS.
EXECUTION OF CRS DURING CLINICALDEVELOPMENT
The approaches the sponsor can take to demonstrateclinical relevance of the dissolution specification have beendiscussed broadly in presentations given by the FDA andindustry. Furthermore, an aspirational goal would be toenable product release without end-product testing, insofar
as process controls would guarantee product quality. Toachieve this goal, deep product knowledge, including formu-lation components (excipients, API), process, and stability, isrequired, as well as the tools (methods) to probe whetherformulation and process changes impact product quality ornot.
Product formulation and process understanding is evolv-ing throughout clinical development, offering a range ofopportunities for establishing CRS during drug productdevelopment and post-market approval. Early in develop-ment, comprehensive studies of formulation prototypes priorto and during phase 1 are generally not performed, as theformulations used are usually exploratory, and these studiesmay not provide information that is pivotal to the finalproduct. Nevertheless, in-human data generated this early indevelopment may provide valuable bioperformance knowl-edge that may guide formulation platform selection andbetter understanding of API attributes.
When compounds are entering clinical phases 2 and 3,performing PK experiments with formulation variants as partof enhanced product understanding becomes more relevant.It is typically at this stage when the potential need to performPK studies to support process operating ranges becomesclear. In addition, the designs of the actual clinical studies,with respect to the selection of which formulation/processvariants to evaluate, are determined. This is an outcome ofthe ongoing risk assessments. At this stage of productdevelopment, a fundamental understanding of the rate-limiting step in the dissolution mechanism should be avail-able. This allows fine tuning method conditions for traditionaldissolution experiments, or it might, in fact, highlight the needto develop additional methodologies which correlate one ormore formulation material attributes with the observed PKperformance. Furthermore, at this stage, M&S may providesignificant opportunity on its own or as supplement to PKexperimentation to develop CRS.
During phase 3 development, the formulation andprocess is usually Blocked^ which means that the materialsto support pivotal clinical studies have been released andregistration stability with material made at the appropriatescale may have already started. For most programs enteringphase 3 clinical development, the dissolution method
Fig. 6. Plasma concentration time profiles for the standard tablet, oral solution, and tablet variant
1547Approaches for Establishing Clinically Relevant Dissolution Specifications for Immediate Release Solid Oral Dosage Forms

conditions used for clinical batch release, registration stability,and additional scale-up development are in place. However,acceptance criteria for the QC dissolution method2 areusually finalized after all relevant stability and clinical batchdata have been evaluated. Despite the advanced stage of theprogram, targeted PK studies with process and formulationvariants could be conducted to further support clinicallyrelevant specification setting. The scope of such studies maybe narrower than the PK studies conducted earlier indevelopment. In practice though, performing additional PKstudies is often only pursued if risks cannot be mitigatedwithout significant changes in formulation and/or process thatcould potentially question the relevance of the data fromphase 3 clinical efficacy and safety studies. If the additionalclinical PK studies support changes to the dissolution methodand/or changes in the formulation/process conditions, thisinformation could serve as additional justification of theproposed commercial control strategy.
CRS AND POST-APPROVAL CHANGES
Current discussions about CRS dissolution specificationsfocus heavily on product development, but the concept isequally applicable after product approval and for genericproduct development. As clinically relevant dissolution specifi-cations are more likely to identify a potential bioperformancerisk, this should be seen as an opportunity for regulators andindustry to continue working together toward global harmoni-zation on the use of CRS for post-approval changes. Specifically,this means that a clinically relevant dissolution specificationshould be acceptable to support post-approval changes.
Conceptually, the principles outlined in the extendedrelease IVIVC guidance (36) could be applied to immediaterelease dosage forms and CRS in general. However, for mostIR products, the development of a Level A IVIVC is highlyunlikely even if extreme process and formulation variantswere studied in vivo. Based on current regulatory guidances,only a Level A IVIVC would enable the use of the IVIVCpredictive model for post-approval changes and biowaivers.The suvorexant example (case study 1 which followsapproach 2b in the Fig. 2 CRS roadmap), however, demon-strates that a multiple Level C IVIVC can also deliver anappropriate model to accurately predict the Cmax and AUC ofa formulation based on dissolution performance. Therefore,depending on the drug product’s safety and efficacy (PK/PD),a Level C IVIVC, potentially strengthened by oralabsorption/PBPK modeling, should be suitable to appropri-ately predict bioequivalence for post-approval changes (e.g.,SUPAC Level 2 formulation changes) and/or biowaivers.Even in cases of a demonstrated safe space (e.g., case study 2which follows approach 2c), it should be feasible to apply theclinical experience for assessing SUPAC Level 1 and 2formulation changes. In such a case, the clinically relevantdissolution method, rather than a traditional (non-CRS dissomethod) or multimedia dissolution profiles which both
require meeting the f2 ≥ 50 requirements and are currentlymandated by SUPAC IR, should be used to evaluate if thechanges have an impact on bioperformance.
For products developed and commercialized followingapproach 1 (Fig. 2), the current SUPAC guidance seemsappropriate. In this case, if the QRM has been performedrigorously, SUPAC formulation changes up to level 2 andprocess changes are unlikely to have an impact onbioperformance.
RECOMMENDATIONS AND CONCLUSIONS
Dissolution testing remains an important tool for productdevelopment and routine product release. Drug productdissolution comparisons, whether through the use of statisti-cal approaches such as f2 or based on IVIVC type studies, arekey for evaluating if the product meets the desiredbioperformance criteria, thus supporting process develop-ment and post-approval changes. The two case studiespresented in this manuscript illustrate the potential to justifydissolution method conditions and acceptance criteria that areoutside the current regulatory expectation. Given the aspira-tion to continuously improve the fundamental science thatunderpins the discriminating power of the dissolutionmethod, as well as the goal of maximizing understanding ofthe manufacturing process, establishing clinically relevantdissolution specifications, based on process understandingcoupled with PK data, appears to be a best practice.
The following recommendations reflect the currentposition of pharmaceutical companies represented by IQ onclinically relevant dissolution specification:
1. For drug products comprising BCS class 1 and 3compounds that exhibit rapid or very rapid dissolution(i.e., ≥85% dissolved in 30 or 15 min, respectively, inall three media, pH 1.2, 4.5, and 6.8), this is considereda clinically relevant specification and should besufficient to support scale-up and post-approvalchanges without the need to provide dissolution datain additional media for certain changes (e.g., waterand pH 7.5) or demonstrating similarity of dissolutionprofiles for BCS 1 compounds as long as test andreference product dissolve rapidly.
2. For drug products comprising BCS classes 2 and 4, orBCS class 1 and 3 compounds that do not meet thecriteria of rapid or very rapid dissolution, then thecurrent guidance on dissolution specifications andpost-approval changes should be followed (approach1), unless:
3. The sponsor performed studies that evaluated formu-lation variants in vivo, in which case the specificationshould be set accordingly (approach 2). In addition,this same methodology and specification should beconsidered sufficient to support the dissolution aspectsof scale-up and post-approval changes.
ACKNOWLEDGEMENTS
The authors would like to thank the many reviewersfrom the IQ member companies that contributed to thismanuscript.
2 Dissolution method conditions may still evolve even inphase 3 development; however, changes during, for exam-ple, registration stability studies, or to compare individualclinical batches used in pivotal safety and efficacy studiesneed to be carefully justified.
1548 Hermans et al.

Open Access This article is distributed under the terms of theCreative Commons Attribution 4.0 International License(http://creativecommons.org/licenses/by/4.0/), which permitsunrestricted use, distribution, and reproduction in anymedium, provided you give appropriate credit to the originalauthor(s) and the source, provide a link to the CreativeCommons license, and indicate if changes were made.
REFERENCES
1. U.S. Department of Health and Human Services - Food andDrug Administration, Center for Drug Evaluation and Re-search (CDER). Guidance for industry—dissolution testing ofimmediate release solid oral dosage forms. 1997.
2. Woodcock J. The concept of pharmaceutical quality. AmericanPharmaceutical Review. 2004;7(6).
3. International Conference on Harmonization of Technical Re-quirements for Registration of Pharmaceuticals for Human use(ICH). ICH Harmonized Tripartite Guideline: PharmaceuticalDevelopment, ICH Q8 (R2); 2009.
4. International Conference on Harmonization of Technical Re-quirements for Registration of Pharmaceuticals for Human use(ICH). ICH Harmonized Tripartite Guideline: Quality RiskManagement, ICH Q9; 2005.
5. International Conference on Harmonization of Technical Re-quirements for Registration of Pharmaceuticals for Human use(ICH). ICH Harmonized Tripartite Guideline: PharmaceuticalQuality System, ICH Q10; 2005.
6. Yu LX. Pharmaceutical quality by design: product and processdevelopment, understanding, and control. Pharm Res.2008;25(4):781–91.
7. Nasr MM. Implementation of quality by design (QbD)—currentperspectives on opportunities and challenges. FDA PharmaceuticalScience and Clinical Pharmacology Advisory Committee; 2011.
8. Yu LX, Amidon G, Khan MA, Hoag SW, Polli J, Raju GK,et al. Understanding pharmaceutical quality by design. AAPS J.2014;16(4):771–83.
9. Dickinson PA, Lee WW, Stott PW, Townsend AI, Smart JP,Ghahramani P, et al. Clinical relevance of dissolution testing inquality by design. AAPS J. 2008;10(2):380–90.
10. Selen A, Cruanes MT, Mullertz A, Dickinson PA, Cook JA,Polli JE, et al. Meeting report: applied biopharmaceutics andquality by design for dissolution/release specification setting:product quality for patient benefit. AAPS J. 2010;12(3):465–72.
11. Clinically LR. Relevant specifications (CRS): a regulatoryperspective. PQRI: Conference on Evolving Product Quality;Bethesda; 2014.
12. Pope MS. Specifications for QbD-containing applications.AAPS workshop: facilitating oral product development andreducing regulatory burden through novel approaches to assessbioavailability/bioequivalence. Washington; 2011.
13. Suarez-Sharp S. Case studies: models for establishing clinicallyrelevant drug specifications. AAPS Annual Meeting andExposition. Washington; 2011.
14. Suarez-Sharp S. Establishing clinically relevant drug specifica-tions: FDA perspective. AAPS Annual Meeting and Exposition.Chicago; 2012.
15. Norris K, Diaz DA, Ganapathy M, Gold L, Zhang L. Movingtoward clinically relevant dissolution specifications. AAPS NewsMagazine. 2016.
16. U.S. Department of Health andHuman Services—Food andDrugAdministration, Center for Drug Evaluation and Research(CDER). Guidance for industry: Immediate Release Solid OralDosage Forms: Scale-Up and Postapproval Changes: Chemistry,Manufacturing, and Controls; In Vitro Dissolution Testing andIn Vivo Bioequivalence Documentation. 1995.
17. U.S. Department of Health andHuman Services—Food andDrugAdministration, Center for Drug Evaluation and Research(CDER). Guidance for industry: SUPAC-MR: Modified Release
Solid Oral Dosage Forms : Scale-Up and Postapproval Changes:Chemistry, Manufacturing, and Controls; In Vitro DissolutionTesting and In Vivo Bioequivalence Documentation. 1997.
18. U.S. Department of Health and Human Services—Food andDrug Administration, Center for Drug Evaluation and Re-search (CDER). Dissolution Testing and Specification Criteriafor Immediate-Release Solid Oral Dosage Forms ContainingBiopharmaceutics Classification System Class 1 and 3Drugs—Guidance for Industry—Draft Guidance. 2015.
19. Cook JA. Development strategies for IVIVC in an industrialenvironment. Biopharm Drug Dispos. 2012;33(7):349–53.
20. Marroum PJ. Clinically relevant dissolution methods andspecifications. Am Pharm Rev. 2012;15(1):36–41.
21. Marroum P. History and evolution of the dissolution test.Dissolution Technologies. 2014;11–6.
22. Reppas C, Friedel HD, Barker AR, Buhse LF, Cecil TL, Keitel S,et al. Biorelevant in vitro performance testing of orally administereddosage forms-workshop report. Pharm Res. 2014;31(7):1867–76.
23. Nicolaides E, Symillides M, Dressman JB, Reppas C. Biorelevantdissolution testing to predict the plasma profile of lipophilic drugsafter oral administration. Pharm Res. 2001;18(3):380–8.
24. Trasi NS, Purohit HS, Wen H, Sun DD, Taylor LS. Non-sinkdissolution behavior and solubility limit of commercial tacrolimusamorphous formulations. J Pharm Sci. 2017;106(1):264–72.
25. Sun DD, Wen H, Taylor LS. Non-sink dissolution conditions forpredicting product quality and In Vivo performance ofsupersaturating drug delivery systems. J Pharm Sci.2016;105(9):2477–88.
26. Takeuchi S, Tsume Y, Amidon GE, Amidon GL. Evaluation ofa three compartment in vitro gastrointestinal simulator dissolu-tion apparatus to predict in vivo dissolution. J Pharm Sci.2014;103(11):3416–22.
27. Jones HM, Chen Y, Gibson C, Heimbach T, Parrott N, PetersSA, et al. Physiologically based pharmacokinetic modeling indrug discovery and development: a pharmaceutical industryperspective. Clin Pharmacol Ther. 2015;97(3):247–62.
28. Kesisoglou F, Chung J, van Asperen J, Heimbach T. Physiologi-cally based absorption modeling to impact biopharmaceutics andformulation strategies in drug development-industry case studies. JPharm Sci. 2016;105(9):2723–34.
29. U.S. Department of Health and Human Services—Food andDrug Administration, Center for Drug Evaluation and Re-search (CDER). Waiver of In Vivo Bioavailability and Bio-equivalence Studies for Immediate-Release Solid Oral DosageForms Based on a Biopharmaceutics Classification System, Rev1. Guidance for Industry - Draft Guidance. 2015.
30. Kesisoglou F, Hermans A, Neu C, Yee KL, Palcza J, Miller J.Development of in vitro-in vivo correlation for amorphous soliddispersion immediate-release suvorexant tablets and applicationto clinically relevant dissolution specifications and in-processcontrols. J Pharm Sci. 2015;104(9):2913–22.
31. Timko RJ, Dickinson PA, Holt DJ, Montgomery FJ, ReynoldsGK, Stott PW, et al. Quality-by-design: differing dissolutionphilosophies. AAPS Annual Meeting. San Antonio 2013.
32. Selen A, Dickinson PA, Mullertz A, Crison JR, Mistry HB,Cruanes MT, et al. The biopharmaceutics risk assessmentroadmap for optimizing clinical drug product performance. JPharm Sci. 2014;103(11):3377–97.
33. Zhang X, Lionberger RA, Davit BM, Yu LX. Utility ofphysiologically based absorption modeling in implementingquality by design in drug development. AAPS J.2011;13(1):59–71.
34. Mitra A, Kesisoglou F, Dogterom P. Application of absorptionmodeling to predict bioequivalence outcome of two batches ofetoricoxib tablets. AAPS PharmSciTech. 2015;16(1):76–84.
35. Pepin XJ, Flanagan TR, Holt DJ, Eidelman A, Treacy D,Rowlings CE. Justification of drug product dissolution rate anddrug substance particle size specifications based on absorptionPBPK modeling for Lesinurad immediate release tablets. MolPharm. 2016;13(9):3256–69.
36. U.S. Department of Health and Human Services—Food andDrug Administration, Center for Drug Evaluation and Re-search (CDER). Guidance for industry: Extended Release OralDosage Forms: Development, Evaluation, and Application ofIn Vitro/In Vivo Correlations. 1997.
1549Approaches for Establishing Clinically Relevant Dissolution Specifications for Immediate Release Solid Oral Dosage Forms