Approach to Cough
77
APPROACH TO COUGH Jerry V. Pua MD 2 nd year Resident It’s the simple things in life we forget You hear her talkin’ but don’t hear what she said Why do you make something so easy so complicated? Searching for what’s right in front of your face.. - Simple Things by Usher
description
It’s the simple things in life we forget You hear her talkin’ but don’t hear what she said Why do you make something so easy so complicated? Searching for what’s right in front of your face.. - Simple Things by Usher. Approach to Cough. Jerry V. Pua MD 2 nd year Resident. Objectives. - PowerPoint PPT Presentation
Transcript of Approach to Cough
APPROACH TO COUGHJerry V. Pua MD2nd year Resident
It’s the simple things in life we forgetYou hear her talkin’ but don’t hear what she saidWhy do you make something so easy so complicated?Searching for what’s right in front of your face..
- Simple Things by Usher

Objectives To discuss etiology, differential diagnosis
and work up for children presenting with cough
To discuss approach, diagnosis, management, recommendations and prevention of B. pertussis infection

General Data A.E. 6 month old, Female Filipino, Catholic Brgy. Batasan Hills, Quezon City
Consulted at ER last June 15, 2013
Informant: Grandmother Reliability: 80%

Chief Complaint
Cough – 2 weeks duration

History of Present Illness
2 weeks PTA •Non productive cough•No fever nor other associated symptoms•No consult done
5 days PTA •Persistence of recurring bouts of cough•No other associated symptoms•Consulted LHC – Carbocisteine and Amoxicillin (40mkday)

History of Present Illness
3 days PTA • Persistence of continous non productive cough followed by facial cyanosis• Difficulty breathing – alar flaring, tachypnea, ‘seesaw’ breathing
Few hours PTA
•Persistence of symptoms prompted consult at Local Clinic•A> Bronchopneumonia rule out Pertussis•Advised consult at a tertiary institution

Review of Systems Decrease
appetite No failure to
thrive, feeding interruption
No skin lesions No diaphoresis,
no fainting spells
No vomiting, no diarrhea nor constipation
No pallor No facial
redness during bouts of cough
No convulsion No limitation of
movements No bleeding
manifestations

Family History
No heredo-familial disease on both sides of the family
(+) (+)(+) cough
Birth and Maternal History Born to 39 year old G5P4 (4014) non
smoker, non alcoholic beverage drinker mother
No pre natal check up, denies maternal illness
Multivitamins, Ferrous Sulfate intake
Delivered Full term via NSD at home assisted by traditional birth attendant
No feto-maternal complication during and after the delivery

Immunization History No immunization received

Nutritional History Milk Formula – since birth
No milk formula intolerance Complimentary feeding – 6 months old
No interrupted feeding No feeding problems

Growth and Development Motor
Head control – 2 mos. rolls over – 4 mos. sits with support – 6 mos.
Language Imitates sounds – 5mos
Daily Living Put anything at the mouth – 4 mos.
Social/Adaptive Social smile – 2 mos. plays with caregiver – 6
mos

Past Medical History No routine check up No previous hospitalization No previous surgical intervention done. No allergies

Physical Examination Awake, irritable, in mild respiratory
distress. Well hydrated. Weight: 6 kg (z score below 0 ) Height: 65 cm (z score 0 ) BP 80/50HR 122 RR 38 T 37.1
Skin: Warm, Moist, No rashes or other dermatosis. No cyanosis.

Physical Examination HEENT: Normocephalic. Aniceteric sclera; pink
palpebral conjunctivae; no eye discharge (+) intermittent alar flaring. No nasal discharge
nor bleeding. No tragal tenderness, no aural discharge Non hyperemic posterior pharyngeal wall, no
exudates, uvula midline (+) cervical lympadenopathy, bilateral
Chest and Lungs: No chest deformity nor skin lesions at the chest. Symmetrical chest expansion, (+) subcostal and intercostals retractions (+) crackles on both lung fields

Physical Examination Heart: Adynamic precordium, Apex beat at 4th ICS
LMCL, normal rate regular rhythm, no murmur
Abdomen: Globular, No visible veins. Normoactive bowel sounds. Soft, non tender, no organomegaly.
Genitalia: Grossly female Extremities: No preferential movement. Pulses on
all extremities are full and equal. No clubbing, cyanosis of fingers or toes. CRT <2 seconds. No deformities.

Neurologic Examination Mental Status: Awake, irritable. GCS 15 Cranial Nerves: Intact Motor: Good muscle tone, no
fasciculation or atrophy, no involuntary movement. MMT 5/5 on all extremities. DTR’s 2++
Sensory: No deficit. No babinski or clonus.
Cerebellar: No nystagmus Meningeal signs: No Kernig’s, No
Brudzinski, No nuchal rigidity

BRONCHOPNEUMONIARULE OUT PERTUSSISNO STUNTING NO WASTINGAdmitting Impression

SYMPTOMS, SIGN, OR LABORATORY FINDINGS PATHOGNOMONIC OF A DISEASEApproach to Diagnosis

COUGH Most common symptom presenting to
medical practitioners Cough is a forced expulsive maneuver,
usually against a closed glottis Sound of a cough is due to vibration of
larger airways and laryngeal structures during turbulent flow in expiration
Cough quality in children: a comparison of subjective vs. bronchoscopic findingsAnne Bernadette Chang, et. alDept of Paediatrics & Child Health, University of QueenslandDept Respiratory Medicine, Royal Children's Hospital, Brisbane
COUGH Estimating the duration of cough is the
first step in narrowing the list of possible diagnoses
THE DIAGNOSIS AND TREATMENT OF COUGHRICHARDS. IRWIN, M.D.,AND J. MARK MADISON, M.D.The New England Journal of Medicine

Types of Cough (Duration)
Acute Cough -- a recent onset of cough lasting <3 weeks
Subacute Cough (Prolonged acute cough) -- cough slowly resolving over a 3–8-week period
Chronic Cough -- A cough lasting >8 weeks Recurrent Cough -- cough without a cold is
taken as repeated (>2/year) cough episodes, apart from those associated with colds, that each last more than 7–14 days
Recommendations for the assessment and management of cough in childrenM D Shields, A Bush, M L Everard, S McKenzie, R Primhak, on behalf of the British Thoracic Society Cough Guideline Group

ACUTE COUGH Cough lasting for a maximum of 3 weeks Common caused: URTI, acute bronchitis or
tracheobronchitis (bacterial or viral) Such infections is usually self limited and
subsides within one to two weeks along the clearing of the infection
No targets or reliable measures to predict the duration of cough at its onset, also to predict which will persist into sub acute or chronic cough
COUGH MANAGEMENT: A Practical ApproachF. De Blasio, et. al
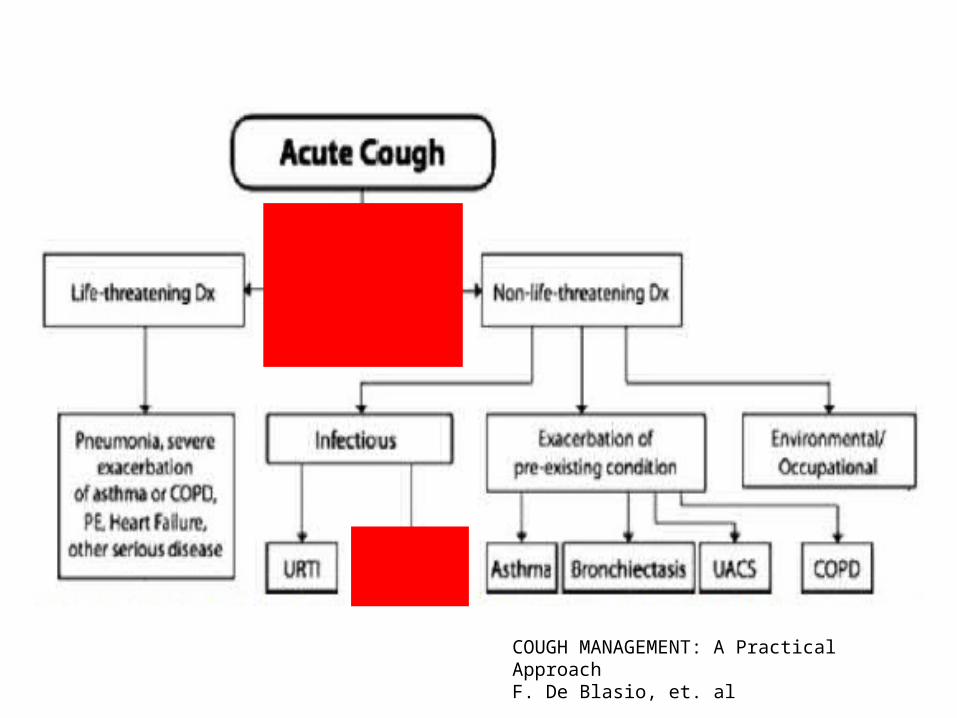
COUGH MANAGEMENT: A Practical ApproachF. De Blasio, et. al

COUGH MANAGEMENT: A Practical ApproachF. De Blasio, et. al

Types of Cough (Causes) Specific Cough -- one in which there is a
clearly identifiable cause Non specific isolated Cough -- typically have a
persistent dry cough, no other respiratory symptoms, well with no signs of chronic lung disease and have a normal chest radiograph
Post viral Cough -- cough originally starting with an upper respiratory tract infection but lasting <3 weeks
Recommendations for the assessment and management of cough in childrenM D Shields, A Bush, M L Everard, S McKenzie, R Primhak, on behalf of the British Thoracic Society Cough Guideline Group

Types of Cough (Quality) Classic Recognizable Cough
Certain cough characteristics classically taught to point to specific etiologies
Dry Cough Wet Cough
Cough in children: definitions and clinical evaluationPosition statement of the Thoracic Society of Australia and New Zealand

Salient Features 6 months old 2 weeks history of
cough No fever Cyanosis at bouts of
cough Difficulty of
breathing Siblings with cough No immunization
received
In mild respiratory distress
Intermittent alar flaring
Intercostal and subcostal retractions
Crackles on both lung fields
Patient: A.E.6 months old, FemaleWorking Impression:
BronchopneumoniaRule out Pertussis
Course at the Ward

1st Hospital DayDiagnostics
Arterial Blood GaspH 7.24 pCO2 26pO2 179 O2sat 99HCO3 11.1 BE - 14.7
CBC w/ PCHgb 37.7 Hct 0.42WBC 35.5 Seg 21Lympho 79 Platelet 647

Case Definitions: Pertussis (WHO) Cough lasting at least 2 wk with at least
1 of the following symptoms: paroxysms of coughing inspiratory whooping posttussive vomiting (ie, vomiting
immediately after coughing) Clinical case: a case that meets the clinical
definition, but is not laboratoryconfirmed Laboratory-confirmed case: a case that meets
the clinical case definition and is laboratory-confirmed
Clinical Definitions of Pertussis: Summary of a Global Pertussis Initiative Roundtable Meeting, February 2011

Clinical Definitions: Pertussis (CDC) Cough illness lasting ≥ 2 weeks with 1 of
the following without apparent cause: Paroxysms of coughing Inspiratory “whoop” Posttussive vomiting
Probable case: symptoms, absence of laboratory confirmation and epidemiologic linkage to a laboratory-confirmed case of pertussis
Confirmed case: symptoms + > 1 following – PCR positive for pertussis or contact with laboratory-confirmed case of pertussis
Clinical Definitions of Pertussis: Summary of a Global Pertussis Initiative Roundtable Meeting, February 2011

Diagnostics Common laboratory diagnostic methods:
Culture – gold standard Direct antigen detection PCR Direct fluorescent antibody (DFA) testing Serologic demonstration enzyme-linked
immunosorbent assay (ELISA) or Western blot with various B. pertussis antigens and agglutination Measuring an increase in titers between acute
and convalescence phase serum specimens or high single serum antibody values
Defining Pertussis EpidemiologyClinical, Microbiologic and Serologic PerspectivesJames D. Cherry, MD, et al Pediatr Infect Dis J 2005

Diagnostics: Serologic Testing
Proper performance of culture, PCR and ELISA to measure increases or decreases in IgG and IgA antibody titers to Pertussis Toxin in paired serum samples, the sensitivity and specificity of the laboratory diagnosis of B. pertussis infection
The greatest sensitivity is obtained when culture, PCR and serologic testing are all performed on individuals with cough illness
Defining Pertussis EpidemiologyClinical, Microbiologic and Serologic PerspectivesJames D. Cherry, MD, et al Pediatr Infect Dis J 2005

Pertussis PCR Key factors for the successful application
of PCR in the diagnosis of infection by Bordetella spp.: Sample collection and processing DNA purification Primer selection Amplification conditions
PCR as a diagnostic tool has the advantage of a much higher sensitivity compared with conventional cultureDefining Pertussis Epidemiology
Clinical, Microbiologic and Serologic PerspectivesJames D. Cherry, MD, et al Pediatr Infect Dis J 2005

Pertussis: PCR A 2.6-fold increase in detection of B.
pertussis using PCR compared with culture PCR results were compared with serologic
diagnosis; PCR had a sensitivity of 61% and a specificity of 88%
Patients with symptoms meeting the CDC clinical case definition for pertussis and who had a specimen positive by PCR or DFA were considered to have true B. pertussis infections Defining Pertussis Epidemiology
Clinical, Microbiologic and Serologic PerspectivesJames D. Cherry, MD, et al Pediatr Infect Dis J 2005

2nd Hospital Day
DiagnosticReferred to Infection Control CommitteeBlood CSNasopharyngeal Pertussis PCR2D Echo with PAP

Complete Blood Counts
06/15/13 06/16/13 06/17/13 06/18/13 06/20/13Hemoglobin 137.7 125.1 126.2 131.4 140.3Hematocrit 0.42 0.38 0.38 0.40 0.43WBC Count 35.5 27.5 25.9 19.2 16.8Diff. CountSegmenterLymphocytesMonocytes
2179
147210
166515
216214
316306
Platelet 647 523 537 539 465

Diagnotics: Complete Blood Count A total count of ≥ 20,000
WBCs/mm3 with ≥ 10,000 lymphocytes/mm3 in a young infant with coryza, cough, apnea or other respiratory distress is indicative of B. pertussis infection
A total count of ≥ 30,000 WBCs/mm3 is cause for concern and the rapidity of the WBC count rise is also an important indicator of worsening condition
Pertussis in Young Infants – Guidance for Clinicians James D. Cherry MD, et. al. May 2010

Microbiology Blood Culture and Sensitivity:
No growth for 5 days of incubation
Nasopharyngeal Bordetella pertussis Polymerase Chain
Reaction POSITIVE for Bordetella pertussis DNA

PERTUSSISBRONCHOPNEUMONIANO STUNTING NO WASTINGFinal Diagnosis

Pertussis Acute respiratory infection caused by
Bordetella pertussis ‘intense cough’ Extremely contagious -- attack rates as
high as 100% in susceptible individuals exposed to aerosol droplets at close range

Bordetella pertussis Tiny, fastidious, gram-negative
coccobacilli that colonize only ciliated epithelium
Expresses pertussis toxin (PT), the major virulence protein
After aerosol acquisition, pertussis organism attaches to ciliated respiratory epithelial cells
Tracheal cytotoxin, adenylate cyclase, and PT appear to inhibit clearance of organisms Responsible for the local epithelial damage

Epidemiology Worldwide, pertussis is a significant
cause of infectious mortality 20 to 40 million cases 200,000 to 400,000 death per years Most of cases and deaths occur in infancy
WHO. Pertussis vaccines. Wkly Epidemiol Rec. 1999;74:137–143
Epidemiology
Philippine Pediatric Society Registry 99 out of 1935660 cases
Philippine Children’s Medical Center 32 cases: Total probable and confirmed
pertussis cases admitted from JANUARY-JUNE 2013

Source of Infection Rate of subclinical infection is as high as 80%
Coughing adolescents and adults -- major reservoir for B. pertussis -- usual sources of infection for infants and children
Household contact with infected adolescent and adults – major source of pertussis infection in not fully immunized infants
Infant Pertussis and Household Transmission n Korea.The Korean Academy of Medical Sciences.

Mode of Transmission
Stages of Pertussis Infection Catarrhal stage (1-2 wk) begins insidiously after
an incubation period (3-12 days)
Paroxysmal stage (2-6 wk) onset marks by coughing Cough begins as a dry, intermittent,
irritative hack and evolves into the inexorable paroxysms
Post-tussive emesis is common, and exhaustion is universal.
Convalescent stage (≥2 wk), the number, severity, and duration of cough episodes diminishes

Stages of Pertussis Infection


Pertussis in Young Infants Catarrhal stage -- characterized by excessive
sneezing or “throat clearing” -- adherence of organism in the ciliated epithelium throughout the respiratory tract – tissue necrosis, production of mucus, and inflammatory cell response
Paroxysmal stage – atypical Acute life-threatening episode is common Spells of cough leading to cyanosis or bradycardia
and limpness as well as apnea Post-tussive vomiting is common
“whoop cough” is rarely present in very young infant
Review: Age-Specific Presentation and Burden of Pertussis by Sarah Long M.D.

1st - 2nd Hospital DayManagement
IsolationD5LR (mild)O2 at 10Lpm
Medications:Ampicillin (100)Erythromycin (40) ---- Azithromycin (10)Salbutamol nebulization every 4 hours
NPO

Goals of hospitalization
Assess progression of disease and likelihood of life-threatening events at peak of disease
Prevent or treat complications Educate parents in the natural history of
the disease and in care that will be given at home

Goals of therapy Limit the number of paroxysms Observe the severity of the cough Provide assistance when necessary Maximize nutrition, rest, and recovery
without sequelae

MedicationsAge Primary Agents Alternate Agents
Azithromycin Erythromycin Clarithro TMP-SMZ<1 mo 10 mg/kg/day in a
single dose for 5 days
(Infantile hypertrophic pyloric stenosis)40-50 mg/kg/day in 4 divided doses for 14 days
Not recommended (safety data unavailable)
Contraindicated for infants aged <2 mo (risk for kernicterus)
1-5 mo 10 mg/kg/day in a single dose for 5 days
40-50 mg/kg/day in 4 divided doses for 14 days
15 mg/kg/d in 2 divided doses for 7 days
Contraindicated at age <2 moFor infants aged ≥2 mo: TMP 8mg/kg/day plus SMZ 40 mg/kg/day in 2 divided doses for 14 days
Infants aged ≥6 mo and child
10 mg/kg in a single dose on day 1 (maximum 500 mg), then 5 mg/kg/day (maximum 250 mg) on days 2-5
40-50 mg/kg/day (maximum 2 g/day) in 4 divided doses for 14 days
15 mg/kg/d in 2 divided doses (maximum 1 g/day) for 7 days
TMP 8 mg/kg/day plus SMZ 40 mg/kg/day in 2 divided doses for 14 days

Pertussis Complications in Young Infants Life-threatening complications are most
common in infants younger than 3 months
Respiratory tract complications: apnea, bacterial pneumonia, and pulmonary hypertension Secondary bacterial pneumonia – leading
identified cause of pertussis-related infection
Review: Age-Specific Presentation and Burden of Pertussis by Sarah Long M.D.

Pertussis Complications in Young Infants Respiratory Failure with Pertussis may
stem from complications of Pneumonia, Pulmonary Hypertension, and Apnea Apnea – due to failure of self-rescue
breathing at the end of a paroxysm of coughing or profound vagal stimulation
Infants intubated due to respiratory failure secondary to apnea have better prognosis than those intubated due to pneumonia or pulmonary hypertension
Review: Age-Specific Presentation and Burden of Pertussis by Sarah Long M.D.

Pertussis Complications in Young Infants Severe Bordetella pertussis consist of
constellation of bronchopneumonia, extreme leukocytosis, refractory hypoxemia, and pulmonary hypertension
White blood cell counts >100 000 in the setting of B. pertussis pneumonia associated with increase mortality
Pertussis Pneumonia, Hypoxemia, Hyperleukocytosis, and Pulmonary Hypertension: Improvement in Oxygenation After a Double Volume Exchange TransfusionMichael J. Romano, et. al. Pediatrics 2004

Pertussis: Proposed Pathologic Course
Infection of tracheal epithelium with Bordetella pertussis
Ciliostasis, epithelial damage and compromised mucociliary clearance
Pulmonary InfectionNecrotizing bronchopneumonia
ARDS
PULMONARY HYPERTENSION
Cardiac Failure and Shock
apnea
hypoxemia
Pulmonary vasoconstriction
Toxin mediated leukocytosis
Increase whole blood mass
Increase vascular resistance
Pathology and Pathogenesis of Fatal Bordetella pertussis Infection in InfantsChristopher D. Paddock, et. al.

3rd -5th Hospital Day The rest of hospital stay patient
completed her antibiotics.
O2 supplementation was titrated down and eventually discontinued.
Patient discharged well and stable.

Indications for ICU referral Infants less than or equal 3 months old
with clinical deterioration White Cell Count more than or equal to
30, 000 or rapidly rising in count (>10,000 in 6 hours)
Respiratory failure or frequent apnea Progressive pneumonic changes in CXR Persistent tachycardia/ cardiovascular
instability Neurological symptoms including seizure
South Thames Retrieval Service Guideline

ICU care Apnea, pneumonia, and seizures are the
most common presenting symptoms requiring ICU care
Leukocytes aggregate within the pulmonary circulation and form a mechanical obstruction to transpulmonary blood flow with the result being severe hypoxemia and pulmonary hypertension
Cardiac failure associated with critical pertussis is likely right sided heart failure secondary to the pulmonary hypertension

Double Volume Exchange Transfusion Multiple authors have reported double
volume exchange transfusion as an effective therapy for the pulmonary hypertension, and secondarily the hypoxemia and cardiac failure
Technique of double volume exchange utilized is the same as performed for the newborn with hyperbilirubinemia
Hypomagnesemia and especially hypocalcemia may occur thus recommended routine calcium supplementationChen H, Lee M, Tsao L. Exchange Transfusion Using Peripheral Vessels Is Safe and Effective in Newborn Infants. Pediatrics 2008

Indications for DVET White cell count more than or equal to
30,000 and rapidly rising count White cell count more than or equal to
30, 000 with pneumonia or hemodynamic instability
White cell count more than or equal 50,000
South Thames Retrieval Service Guideline

Studies shows… Appearance of respiratory symptoms
paralleled the rise in leukocyte count Temporal relationship between the
initiation of exchange transfusion and improvement in oxygenation
Pertussis Pneumonia, Hypoxemia, Hyperleukocytosis, and Pulmonary Hypertension: Improvement in Oxygenation After a Double Volume Exchange TransfusionMichael J. Romano, et. al. Pediatrics 2004

Pertussis Pneumonia, Hypoxemia, Hyperleukocytosis, and Pulmonary Hypertension: Improvement in Oxygenation After a Double Volume Exchange TransfusionMichael J. Romano, et. al. Pediatrics 2004

Criteria for Hospital Discharge Over a 48-hr period disease severity
is unchanged or diminished No intervention is required during
paroxysms Nutrition is adequate No complication has occurred Parents are adequately prepared for care
at home

Prevention: Vaccination Efficacy of the vaccine in reducing
disease severity was 48% among children vaccinated with 3 doses of whole-cell (67%) or acellular (32%)
Pertussis vaccination substantially decrease the severity of breakthrough disease in vaccinated children (3 doses) compared to unvaccinated children Unvaccinated children twice likely to have
severe disease than vaccinated childrenEffects of Pertussis vaccination on Disease: Vaccine Efficacy in Reducing Clinical SeverityPreziosi, Marie-Pierre, et.al. Clinical Infectious Disease 2003

Prevention: Vaccination
DTaP (Diphtheria, tetenus toxoid and acellular Pertussis) contain inactivated PT and 2 or more
other bacterial components (FHA, Pn, and Fim 2 and 3)
4 doses during the 1st 2 years of life 2,4,6 and 15-18 months
5th dose of DTaP recommended for children at 4-6 yr of age

Prevention: Vaccination Tdap (Tetanus toxoid, reduced
diphtheria toxoid, and acellular pertussis vaccine, adsorbed) Preferred age for Tdap vaccination is 11-
12 yr Pregnant adolescents who are in their
2nd or 3rd trimester All adolescents 11-18 yr of age who
received Td, but not Tdap, should receive a single dose of Tdap to provide protection against pertussis

Vaccination of women during pregnancy and newborns
Timing of maternal Tdap immunization is important – administered during the third trimester to have maternal pertussis antigen-specific IgG levels at their peak
Immunization with DTaP or aP vaccines is not recommended in newborns -- controversial
Pertussis re-emergence in the post-vaccination eraChiappini et al. BioMedCentral Infectious Disease 2013
Cocooning strategy Providing indirect protection to infants
who are too young to be immunized or protected by vaccine through immunization of their parents and other family members, caregivers and close contacts
Pertussis re-emergence in the post-vaccination eraChiappini et al. BioMedCentral Infectious Disease 2013
Vaccination of preschool and adolescent Contributes to increase herd immunity Reduce transmission of pertussis to
susceptible population Reduce reservoir of pertussis within
population and indirectly prevent pertussis case in infants and young children
Pertussis re-emergence in the post-vaccination eraChiappini et al. BioMedCentral Infectious Disease 2013

Immunization of health-care workers Pertussis among health-care personnel
has been reported to be 1.7 times higher than the general population
Health-care personnel who have direct contact with patients should receive single dose of TdaP as soon as feasible, if they have not previously received TdaP
Pertussis re-emergence in the post-vaccination eraChiappini et al. BioMedCentral Infectious Disease 2013

Updates Patient follow up at OPD – well,
active Received her first dose of DPT, OPV,
and Hepatitis B Relatives were educated regarding
the importance of immunization as well as proper hygiene to stop the vicious cycle of transmission

Summary A case of 6 month old unimmunized
infant who presented with subacute cough with paroxysms, who after a nasopharyngeal swab PCR was confirmed with Bordetella pertussis
Started on Azithromycin per orem and eventually discharged well and stable
Recommendations for management of pertussis
Emphasized the importance of immunization on preventing vicious transmission cycle

THANK YOU!!!