
Approach to and Evaluation of Sleep Disorders - L.S. Neuro to and Evaluation... · Approach to and...
18
Approach to and Evaluation of Sleep Disorders Anita Valanju Shelgikar, MD; Ronald Chervin, MD, MS, FAASM, FAAN ABSTRACT Purpose of Review: This article provides a framework for the clinical assessment of patients with sleep-related complaints and outlines a systematic approach to a sleep-specific history and physical examination, subjective assessment tools, and diagnostic testing modalities. Recent Findings: Physical examination findings may suggest the presence of a sleep disorder, and obstructive sleep apnea in particular, but the clinical history remains the most important element of the assessment for most sleep problems. While nocturnal polysomnography in a sleep laboratory remains the gold standard for diagnosis of sleep-disordered breathing, out-of-center testing may be considered when the clinician has a high pretest suspicion for obstructive sleep apnea and the patient has no significant cardiopulmonary, neuromuscular, or other sleep disorders. Summary: Sleep-related symptoms are common in adult and pediatric patients. A comprehensive sleep history, physical examination with detailed evaluation of the head and neck, and judicious use of sleep-specific questionnaires guide the decision to pursue diagnostic testing. Understanding of the benefits and limitations of various diagnostic modalities is important as the spectrum of testing options increases. Continuum (Minneap Minn) 2013;19(1):32–49. INTRODUCTION The NIH Sleep Disorders Research Plan, 1 updated in November 2011, indicates a 25% to 30% prevalence of sleep and circadian disorders in the general adult population. The exact prevalence of sleep disorders in neurologic disease is unknown but in some instances may be higher than in the general population. Focused assessment and management of impaired sleep or alertness may im- prove quality of life, improve produc- tivity, reduce accidents, or attenuate progression of a coexisting neurologic disease or facilitate recovery from it. SLEEP HISTORY A detailed sleep history is the central component of the evaluation. Historical information given by the patient should, when possible, be supplemented by a bed partner, family member, or room- mate who may have different insight into the patient’s behavior during sleep or daytime mood and cognitive func- tioning. Whether the presenting sleep complaint is excessive daytime sleepi- ness, poor sleep quality, insomnia (diffi- culty falling or staying asleep), or abnormal behavior during sleep, a uni- form approach to the sleep history facilitates a thorough medical decision- making process. Table 2-1 details the es- sential components of the sleep history. A chief complaint of daytime sleepi- ness should invite questions about its nature and severity, timing, circum- stances, and possible underlying causes. Address correspondence to Dr Anita Valanju Shelgikar, Medical School Sleep Disorders Center, C728 Med Inn Building, 1500 East Medical Center Dr, Ann Arbor, MI 48109-0845, [email protected]. Relationship Disclosure: Dr Shelgikar has received an honorarium from Elsevier for her authorship of a book chapter. Dr Chervin has consulted for Proctor & Gamble and Zansors, LLC; receives compensation for serving on boards from the American Academy of Sleep Medicine, International Pediatric Sleep Association, and the NIH; serves as section editor for and receives royalty payments from UpToDate; receives licensing fees through the University of Michigan from Zansors, LLC; and receives grants from Fisher & Paykel, the NIH, and Philips Respironics. Unlabeled Use of Products/Investigational Use Disclosure: Drs Shelgikar and Chervin report no disclosures. * 2013, American Academy of Neurology. Supplemental digital content: Videos accompanying this ar- ticle are cited in the text as Supplemental Digital Content. Videos may be accessed by clicking on links provided in the HTML, PDF, and iPad versions of this article; the URLs are provided in the print version. Video legends begin on page 48. 32 www.aan.com/continuum February 2013 Review Article Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Transcript of Approach to and Evaluation of Sleep Disorders - L.S. Neuro to and Evaluation... · Approach to and...

Approach to andEvaluation of SleepDisorders
Anita Valanju Shelgikar MD Ronald Chervin MD MS FAASM FAAN
ABSTRACTPurpose of Review This article provides a framework for the clinical assessment ofpatients with sleep-related complaints and outlines a systematic approach to asleep-specific history and physical examination subjective assessment tools anddiagnostic testing modalitiesRecent Findings Physical examination findings may suggest the presence of a sleepdisorder and obstructive sleep apnea in particular but the clinical history remains themost important element of the assessment for most sleep problems While nocturnalpolysomnography in a sleep laboratory remains the gold standard for diagnosis ofsleep-disordered breathing out-of-center testingmay be consideredwhen the clinicianhas a high pretest suspicion for obstructive sleep apnea and the patient has nosignificant cardiopulmonary neuromuscular or other sleep disordersSummary Sleep-related symptoms are common in adult and pediatric patients Acomprehensive sleep history physical examinationwith detailed evaluation of the headand neck and judicious use of sleep-specific questionnaires guide the decision topursue diagnostic testing Understanding of the benefits and limitations of variousdiagnostic modalities is important as the spectrum of testing options increases
Continuum (Minneap Minn) 201319(1)32ndash49
INTRODUCTIONThe NIH Sleep Disorders Research Plan1
updated in November 2011 indicatesa 25 to 30 prevalence of sleep andcircadian disorders in the general adultpopulation The exact prevalence ofsleep disorders in neurologic disease isunknown but in some instances may behigher than in the general populationFocused assessment and managementof impaired sleep or alertness may im-prove quality of life improve produc-tivity reduce accidents or attenuateprogression of a coexisting neurologicdisease or facilitate recovery from it
SLEEP HISTORYA detailed sleep history is the centralcomponent of the evaluation Historical
information given by the patient shouldwhen possible be supplemented by abed partner family member or room-mate who may have different insightinto the patientrsquos behavior during sleepor daytime mood and cognitive func-tioning Whether the presenting sleepcomplaint is excessive daytime sleepi-ness poor sleep quality insomnia (diffi-culty falling or staying asleep) orabnormal behavior during sleep a uni-form approach to the sleep historyfacilitates a thorough medical decision-making process Table 2-1 details the es-sential components of the sleep history
A chief complaint of daytime sleepi-ness should invite questions about itsnature and severity timing circum-stances and possible underlying causes
Address correspondence toDr Anita Valanju ShelgikarMedical School SleepDisorders Center C728 MedInn Building 1500 EastMedical Center DrAnn Arbor MI 48109-0845avalanjumedumichedu
Relationship DisclosureDr Shelgikar has received anhonorarium from Elsevier forher authorship of a bookchapter Dr Chervin hasconsulted for Proctor ampGamble and Zansors LLCreceives compensation forserving on boards from theAmerican Academy of SleepMedicine InternationalPediatric Sleep Associationand the NIH serves as sectioneditor for and receives royaltypayments from UpToDatereceives licensing feesthrough the University ofMichigan from Zansors LLCand receives grants fromFisher amp Paykel the NIH andPhilips Respironics
Unlabeled Use ofProductsInvestigationalUse DisclosureDrs Shelgikar and Chervinreport no disclosures
2013 American Academyof Neurology
Supplemental digital contentVideos accompanying this ar-ticle are cited in the text asSupplemental Digital ContentVideos may be accessed byclicking on links provided inthe HTML PDF and iPadversions of this article theURLs are provided in the printversion Video legends beginon page 48
32 wwwaancomcontinuum February 2013
Review Article
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
Sleepiness is thought to result from neu-robiologic processes that regulate circa-dian rhythms and the drive to sleep2 andsome individuals will clearly articulatesleepiness as a tendency to doze un-intentionally Fatigue is defined aslsquolsquoreversible motor and cognitive impair-ment with reduced motivation and
desire to restrsquorsquo3 and is postulated torepresent a process that is distinct fromsleepiness However patients ofteninterchangeably use the terms lsquolsquotired-nessrsquorsquo lsquolsquosleepinessrsquorsquo and lsquolsquofatiguersquorsquo34 Pa-tients with obstructive sleep apnea (OSA)and possibly other sleep disorders as-sociated with daytime sleepiness may
TABLE 2-1 Components of the Sleep History
b Presenting Sleep-Related Symptom
Onset
Precipitatingpredisposing factors
Duration
Frequency
Severity
b Associated Nocturnal Symptoms
Sleep-disordered breathing
Snoring
Witnessed apneas
Morning headache
Mouth breathing
Acid reflux
Nasal congestion
Nocturia
Erectile dysfunction
Nocturnal dyspnea
Nocturnal behavior
Sleepwalking
Sleeptalking
Sleep eating
Leg movement
Dream enactment
Bruxism
Nocturnal awakenings
Timing in night
Precipitants
Duration
Frequency
Activities while awake
Other symptoms
Leg discomfort
Urge to move
Sleep paralysis
b Time of Symptoms (Time Duringthe Sleep Period That SymptomsOccur)
b Daytime Functioning
Daytime sleepiness
Mood disturbance
Impaired school or workperformance
Decreased alertness while driving
Impaired interpersonalrelationships
Decreased concentration ormemory
Cataplexy or hypnagogic orhypnopompic hallucinations
Leg discomfort urge to moveor spontaneous movements
b Sleep Schedule and Sleep Hygiene
Bed time
Sleep latency
Wake time
Rise time (when patient gets upfrom bed)
Details of bedtime routine
Description of activities duringnocturnal awakenings
b Use of Sleep Aids and Stimulants
Over-the-counter (includingherbal) agents
Prescription medications
Caffeine
Energy drinks
33Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
report fatigue tiredness or lack ofenergy at times even when they denysleepiness4 Interestingly these symp-toms (like sleepiness) appear toimprove with treatment of the under-lying OSA5 A clear understanding ofwhether the patient experiences anoverwhelming urge to sleep duringthe day may help the clinician decidewhich diagnostic studies to pursue andalso guides discussion about potentialdiagnoses that may contribute to thepatientrsquos symptoms Special attentionshould be paid to situations in whichthe patientrsquos sleepiness becomes evi-dent Does the patient doze during con-versation while at work or while drivingIs the patientrsquos concentration or memoryimpaired because of sleepiness Dozingwhile operating heavy machinery or amotor vehicle can lead to devastatingoutcomes and this has both individualand public health implications Daytimesleepiness that impairs a patientrsquos func-tional capabilities can threaten job se-curity and have a negative impact oninterpersonal relationships The con-text of a patientrsquos daytime sleepinesshighlights its severity and impact
The symptom of insomnia is de-fined as difficulty with sleep initiationor maintenance waking too early orsleep that is nonrestorative despiteample opportunity to sleep6 Disordersthat cause insomnia have diagnosticcriteria to specify that the insomniasymptoms should be accompanied byat least one manifestation of daytimeimpairment (such as fatigue mood dis-turbance headaches or gastrointestinalsymptoms in response to sleep loss) orimpaired memory concentration orperformance The point prevalence ofinsomnia is estimated at 6 to 15 inthe general population but is clearlyhigher among certain subgroups suchas patients with psychiatric disease7
Population-based studies done withvaried adult samples from multiple
countries indicate that approximately30 of the general adult populationreports one or more insomnia symp-tom8 Because insomnia is so commonneurologists routinely encounter pa-tients with the symptom As the etiol-ogy of insomnia is often multifactorialthe evaluation can be complex andrequires a detailed history that exploresmany potential contributors
A helpful framework in which to con-sider a patientrsquos insomnia is known asthe lsquolsquo3Prsquorsquo model9 which aids identifica-tion of possible causes of insomnia andhighlights potential targets for treat-ment This model calls for temporalclassification of factors that affect a pa-tientrsquos insomnia characteristics thatpredispose a person to develop in-somnia events that precipitate the in-somnia acutely and behaviors andattitudes that perpetuate insomnia andmay cause it to become chronic Com-mon predisposing factors include per-sonality traits such as excessive worryingor cognitive hyperarousal or the degreeto which a personrsquos preferred sleepingtimes differ from social norms9 Precip-itating factors are often readily identi-fied as major life transitions such aschange in marital status death in thefamily or change in employment How-ever subtler challenges to a personrsquosroutine or environment may also pre-cipitate the onset of insomnia In somesituations the patientrsquos sleep normal-izes upon resolution of the precipitantin other cases behaviors and mindsetsaccrued during the acute phase of theinsomnia can perpetuate the patientrsquossleep disturbance Such perpetuatingfactors can include perceived associa-tions between the sleeping environ-ment and inability to sleep or escalateduse of caffeine throughout the dayOther important details include specif-ics about the patientrsquos insomnia at thepresent time including the latency tosleep timing duration and causes of
KEY POINTS
h Information from thepatient medical recordand any available bedpartner friend orfamily member canclarify the extent andconsequences of thepatientrsquos sleep-relatedsymptoms
h The 3P framework ofinsomnia comprisespredisposingprecipitating andperpetuating factorsDiscussion of all factorsfacilitates identificationof potential treatmenttargets
34 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
nocturnal awakenings behaviors dur-ing nocturnal awakenings and latencyto fall back asleep after each awakeningA useful approach is to ask the patientfor a detailed start-to-finish descriptionof the entire typical sleep period anddaytime period Any medications pre-viously or currently used to facilitatesleep should also be identified
The sleep history should screenfor potentially relevant sleep disordersthat may cause excessive daytime sleep-iness or insomnia (Case 2-1) Thepresence of symptoms such as snor-ing witnessed apneas and morningheadaches raises the suspicion forsleep-disordered breathing (SDB) Leg
discomfort associated with an urge tomove that worsens at night andimproves with leg movement indicatesrestless legs syndrome and may con-tribute to the patientrsquos poor sleepquality and impair daytime functioningSleep paralysis and hypnagogic orhypnopompic hallucinations are notspecific to a particular sleep disorderwhile a history of cataplexy is patho-gnomonic for narcolepsy and must beexplored when a patient presents withreports of central hypersomnia ratherthan SDB When relevant the clinicianshould also ask about nocturnal behav-iors specifically ones that may pose riskof injury to the patient or bed partner
Case 2-1A 44-year-old man with a long-standing history of loud frequent snoringpresented because of his wifersquos concerns related to his snoring His wifehad witnessed him to have occasional pauses in his breathing during sleepand at times he awakened to his snoring He reported frequent acidreflux and morning headaches Approximately once per month he wouldawaken lsquolsquofeeling like my heart is racing and I need to catch my breathrsquorsquoHe had occasional nasal congestion but always awakened with a drymouth and sore throat He denied any leg discomfort but his wife hadtold him that he tossed and turned frequently during sleep
His sleep schedule was the same every night he was in bed by 1000 PMfell asleep immediately without the use of any sleep aids and awakenedat 600 AM feeling tired He had up to four nocturnal awakenings pernight two were attributed to nocturia and the rest were of unknownetiology Each awakening lasted a few minutes and he fell asleep againeasily He had had a few episodes of sleepwalking as a child but none sincethe age of 8 years
He felt sleepy during the day with a propensity to doze unintentionallywhile reading or watching television He denied drowsiness while driving butlimited his driving to his 20-minute commute to and from work his wifedrove for longer distances and hewould often sleep in the passenger seat Hissleepiness was worse in the midafternoon and if given the opportunity hewould nap for 1 hour on the weekends He found naps to be somewhatrefreshing He drank two to three cups of coffee every morning and had a12-oz caffeinated sodawith lunch His sleepiness had not caused him tomakeany mistakes in his job as a physical therapist although he felt that he hadpotential for further improvement in his job performance He also reportedfeeling more irritable in recent months but this had not caused anydifficulties at home or work
Comment This case illustrates the multiple components of a concisebut still detailed sleep history The patientrsquos daytime symptoms provideinsight about the effects of the patientrsquos untreated sleep disorder
35Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
such as sleepwalking driving or cook-ing while asleep or dream-enactmentbehavior If the patient reports suchbehavior further inquiry must be madeabout the frequency of these events andany history of injury sustained due to thesleep-related behavior Details of thesleep history permit a thorough differ-ential diagnosis and can also guide adiscussion of safety concerns
PHYSICAL EXAMINATIONA comprehensive multisystem exami-nation is an important aspect of thesleep evaluation Measurement of theweight height body mass index (BMI)neck circumference and blood pres-sure and heart rate should be per-formed for nearly all patients withsymptoms related to sleep or alertnessOther salient features of the generalexamination include auscultation forany cardiac or respiratory abnormalitiesand identification of peripheral edemaA focused neurologic examinationshould be guided by the patientrsquos his-tory For instance a mental status as-sessment should be considered if apatient with excessive daytime sleepi-ness also complains of memory loss If apatient with a history of diabetes melli-
tus endorses symptoms of restless legssyndrome it is worthwhile to assess forstocking-glove distribution sensory lossand weakness
Detailed examination of the headand neck should be performed as partof a comprehensive sleep evaluationThe patientrsquos facial morphology shouldbe assessed for features of long facesyndrome which includes infraorbitaldarkening mouth breathing elongatedmidface and nasal atrophy10 A 2009review11 reports that previous observa-tional and cross-sectional studies haveshown a relationship between chronicnasal obstruction and OSA Thus a thor-ough nasal examination should be per-formed on patients with sleep-relatedcomplaints Examination of the nasalairway should include evaluation forsymmetry of the nares nasal septum de-viation (Figure 2-1)12 and nasal turbi-nate hypertrophy A bedside assessmentof nasal airflow can be accomplished by
KEY POINT
h Details of facialmorphology nasalairway patency and oralairway crowding arekey features of thesleep-specificexamination
FIGURE 2-1 Nasal septal deviation Thisstructural abnormality canpredispose a patient to havesleep-disordered breathing
Reprinted from Kryger MH Elsevier12 B 2010 withpermission from Elsevier
FIGURE 2-2 Retrognathia Retrognathiais derived from the termslsquolsquoretrorsquorsquo (backward) and
lsquolsquognathosrsquorsquo (jaw) With retrognathia one orboth jaws recede with respect to the frontalplane of the forehead The condition maypredispose a patient to obstruction of theairway and sleep apnea by displacing thetongue against the retropharyngeal regioncompromising airflow Retrognathia issometimes corrected through surgicalrepositioning or advancement of themandible
Reprinted from Kryger MH Elsevier12 B 2010 withpermission from Elsevier
36 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
asking the patient to press the indexfinger against the left nostril and take adeep breath in on the right side thisshould be repeated on the oppositeside as well The patientrsquos facial mor-phology should be assessed for man-dibular retrognathia (Figure 2-2)12 Withthe patientrsquos head in a neutral posi-tion a virtual line is drawn from thevermillion border of the lower lip tothe chin Mandibular retrognathia issuggested if the anterior prominence ofthe chin is 2 mm or more behind thevirtual line13
The modified Mallampati classifica-tion is commonly used for assessmentof the oral airway in patients withsuspected SDB The Mallampati classi-fication14 was developed to identifypatients in whom tracheal intubationwould be difficult the initial description
divided patients into three classes Twoyears later15 this was modified to de-scribe four groups class I class II classIII and class IV Figure 2-3 16 illustratesthe modified Mallampati classificationassessed with the tongue protrudedThe Friedman palate position classifi-cation17 also commonly referencedutilizes the same four categories but isdone with the tongue at rest and notextended Either the Mallampati orFriedman classification may be used todescribe the patency of the oral airway
Tonsils should be classified based onthe degree of hypertrophy (Figure 2-4)12grade I tonsils are inside the tonsillarfossa lateral to the posterior pillarsgrade II tonsils occupy 25 of theoropharynx grade III tonsils occupy50 of the oropharynx and grade IVtonsils occupy at least 75 of the
FIGURE 2-3 Modified Mallampati classification The class is determined by looking at theanatomy of the oral cavity and describes tongue size relative to oropharyngealsize The test is conducted with the patient seated the head held in a neutral
position and the mouth wide open and relaxed The subsequent classification is assigned basedupon the pharyngeal structures that are visible
Reprinted from Huang HH et al BMC Gastroenterol16 B 2011 BioMed Central Ltd wwwbiomedcentralcom1471-230X1112
37Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
oropharynx and nearly meet in the mid-line13 A high-arched narrow hard pal-ate (Figure 2-5)18 may predispose thepatient to have SDB Katz and col-leagues19 have shown that patients withOSA have significantly increased neckcircumference compared to nonapneicsnorers greater distribution of neck fat
may contribute to mass loading on theupper airway in patients with OSA Thepatientrsquos neck circumference should bemeasured at the superior border of thecricothyroid membrane19 A neck cir-cumference greater than 40 cm (157in) has been shown to be predictive ofOSA with 61 sensitivity and 93specificity regardless of sex20
Assessment of the patientrsquos anteriorand posterior dentition can also re-veal anatomic findings that may pre-dispose a person to certain sleepdisorders Two features to note in eval-uation of the anterior dentition areoverjet and overbite (Figure 2-6)21
Overjet as shown in Figure 2-712 isthe horizontal distance between theupper right central incisor and thebuccal surface of the correspondinglower tooth while overbite is the ver-tical distance between these twopoints22 These measurements are typ-ically reported in millimeters The An-gle classification system is used todescribe the first molar position on
FIGURE 2-4 Tonsil size grading Thisstructural abnormality canpredispose a patient to havesleep-disordered breathing
Reprinted from Kryger MH Elsevier12 B 2010 withpermission from Elsevier
FIGURE 2-5 Deficientmaxillarydevelopment inan individual with
Down syndrome leading to highand narrow hard palate
Reprinted with permission from ChengRHW et al InTech18 B 2011 W KeungLeung wwwintechopencombooksprenatal-diagnosis-and-screening-for-down-syndromeoral-health-in-individuals-with-down-syndrome
FIGURE 2-6 Overjet andoverbite Overjetis defined as
increased projection of the upperteeth in front of the lower teethas measured parallel to theocclusal plane Overbite is thevertical overlapping of maxillaryteeth over mandibular teethusually measured perpendicularto the occlusal plane
Reprinted from Saccucci M et al Scoliosis21
B 2011 BioMed Central Ltd wwwscoliosisjournalcomcontent6115
38 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
the mandibular and maxillary dentalarches23 Figure 2-8 shows class I oc-clusion and class II and III malocclu-
sion Of note the mesiobuccal surfaceis the aspect of the tooth that is adja-cent to the cheek mucosa
The Adult Obstructive Sleep ApneaTask Force of the American Academyof Sleep Medicine (AASM) recommen-ded in recent clinical guidelines24 thatthe following physical findings maysuggest the presence of OSA increasedneck circumference (greater than 432cm [17 in] in men greater than 406 cm[16 in] in women) BMI 30 kgm2 orgreater modified Mallampati classifica-tion of III or IV presence of retrognathialateral peritonsillar narrowing macro-glossia tonsillar hypertrophy elongatedenlarged uvula high-archednarrowhard palate nasal abnormalities (egpolyps deviation valve abnormalities
KEY POINT
h Classification of thepatientrsquos dentition helpsto evaluate the positionof the maxillary archrelative to themandibular arch
FIGURE 2-7 OverjetDisplacementof the
mandibular teeth posteriorly inrelationship to the maxillary teethresults inmoreposteriorly crowdedupper airways predisposingpatients for the developmentof obstructive sleep apnea
Reprinted from Kryger MH Elsevier12
B 2010 with permission from Elsevier
FIGURE 2-8 Angle class occlusionmalocclusion A Angle class I occlusion also known asneutrocclusion The mandibular and maxillary dental arches have a normalanterior-posterior relationship The mesiobuccal groove of the mandibular first
molar interdigitates with the mesiobuccal cusp of the maxillary first molar B Angle class IImalocclusion also known as distoclusion The mandibular dental arch is in distal anterior-posteriorrelationship to the maxillary dental arch The mesiobuccal groove of the mandibular first molar isdistal to the mesiobuccal cusp of the maxillary first molar C Angle class III malocclusion alsoknown as mesioclusion The mandibular dental arch is in mesial anterior-posterior relationship tothe maxillary dental arch The mesiobuccal groove of the mandibular first molar is mesial to themesiobuccal cusp of the maxillary first molar
Reprinted fromMorcos SS Patel PK Clin Plast Surg23 B 2007 with permission from Elsevier wwwsciencedirectcomsciencearticlepiiS0094129807000843
39Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
and turbinate hypertrophy) andoroverjet To prevent overlooking thesefindings a thorough head and neckassessment as described in Table 2-2should be incorporated into the phys-ical examination of all patients whopresent with sleep-related complaints
SUBJECTIVE ASSESSMENTSeveral patient-completed question-naires are inexpensive and time-efficient
reasonably well validated and com-monly used They can help to increasestandardization in evaluations of patientsby different clinicians or across centersPerhaps the most well-known andwidely used is the Epworth SleepinessScale25 a subjective assessment of thepatientrsquos daytime sleep propensity inrecent times As shown in Appendix Athe Epworth Sleepiness Scale asks theresponder to use a four-point Likertscale (0 1 2 or 3) to indicate thelikelihood of dozing in eight distinctsedentary conditions A total score of 10or greater out of a possible 24 suggestsexcessive daytime sleepiness25 Whilethe Epworth Sleepiness Scale score canbe easily incorporated into the clinicalevaluation it should not be used as asubstitute for objective measurement ofsleepiness The Epworth Sleepiness Scalescore may correlate to a limited extentwith the presence and severity of OSA26
but some studies have failed to find anystatistically significant association withmean sleep latency on multiple sleep la-tency tests or with severity of OSA27
The most advantageous use of theEpworth Sleepiness Scale may be to followan individualrsquos self-assessment of sleep-iness longitudinally and it may also serveas an indicator of treatment response
Many other questionnaires may beutilized in a clinical sleep evaluationsome pertain to overall sleep qualitywhile others are disorder-specific ThePatient Reported Outcomes Measure-ment Information System (PROMIS) isan NIH-supported system of measuresfor patient-reported health status andincludes questions on sleep disturb-ance The Pittsburgh Sleep QualityIndex (PSQI) is a validated question-naire that inquires about sleep qualityand disturbances over the previousmonth28 The parent-completed Pe-diatric Sleep Questionnaire29 containsa validated reliable 22-item scale tohelp assess risk for SDB in children
KEY POINTS
h The Epworth SleepinessScale apatient-completedquestionnaire assessesthe patientrsquos subjectivetendency to doze duringsedentary situations inrecent times not onlyat the moment thequestionnaire iscompleted
h The Epworth SleepinessScale should not beused in lieu of diagnostictesting but may be avaluable componentof ongoing clinicalevaluation
TABLE 2-2 Head and NeckExamination
b Face
Featuresof long face syndrome
Infraorbital darkening
Mouth breathing
Elongated midface
Nasal atrophy
b Oral Airway
Mandibular retrognathia
Low soft palate (modifiedMallampati classification)
Large or boggy uvula
Erythematous pillars
Tonsillar hypertrophy
High narrow hard palate
Neck circumference
Overjet
Overbite
Angle classification(malocclusion)
Macroglossia
Worn occlusive surfaces(suggestive of bruxism)
b Nasal Airway
Symmetry of the nares
Nasal septum deviation
Nasal airflow
Collapse of nasal alae oninspiration
b Neck
Neck circumference
40 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
The STOP-BANG questionnaire devel-oped and validated in preoperativepatients is a sensitive screening toolfor OSA Four questions address snor-ing tiredness during daytime observedapnea and high blood pressure whereasfour other measures focus on increasedOSA risk factors of BMI (greater than 35kgm2) age (older than 50 years) neckcircumference (greater than 40 cm[1575 in]) and gender (male preva-lence)30 The International RestlessLegs Syndrome Study Group Rating Scale(IRLS) is a validated assessment of dis-ease severity for patients with restlesslegs syndrome31 The patientrsquos perceived
level of insomnia may be assessed withthe Insomnia Severity Index (ISI) avalidated 7-item questionnaire32
A sleep diary (Figure 2-9)33 allows apatient to chart daily sleep and waketimes and should be maintained for atleast 2 consecutive weeks Review ofthis information allows the clinicianto estimate the total amount of sleepthe patient obtains in a 24-hour pe-riod The sleep diary also can provideinsight into the patientrsquos sleep patternIs sleep obtained at the same timesevery day Is the patientrsquos sleep con-solidated or fragmented across 24hours Does the patient sleep and
FIGURE 2-9 Sleep diary completed by a 46-year-old woman who presented with difficulty falling asleep Vertical linesrepresent when the patient went to bed lsquolsquoMrsquorsquo refers to when medication was taken black shading representstime asleep and unshaded white areas are time spent awake
Diary template reprinted from YOURSLEEPaasmnetorg from the American Academy of Sleep Medicine yoursleepaasmnetorgpdfsleepdiarypdf33
41Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
wake at conventional times or doeshe or she appear to be a lsquolsquonight owlrsquorsquoor lsquolsquomorning larkrsquorsquo Answers to thesequestions as provided by the sleepdiary may reveal factors that contrib-ute to sleep-related concerns Use ofsleep diaries can be particularly help-ful in patients with suspected circadianrhythm sleep disorders (including shiftwork) behaviorally induced insufficientsleep or inadequate sleep hygiene
OBJECTIVE MEASURESNocturnal polysomnography (NPSG)or related assessments are indicatedfor the diagnosis and assessment ofSDB and for positive airway titrationin patients with confirmed SDB Theprocedure can also provide informationabout EEG activity nocturnal move-ments cardiac rhythm and oxygen
saturation34 The recommended record-ing montage used in NPSG as shownin Figure 2-10 includes central (C3-A2C4-A1) frontal (F3-A2 F4-A1) andoccipital (O1-A2 O2-A1) EEGs left andright eye electrooculograms mentalsubmental surface EMG and ECG leadsOther recorded parameters includethoracic and abdominal effort oxygensaturation nasaloral airflow and bodyposition Use of a microphone torecord snoring is recommended butnot required34 A full 16-lead EEG(Figure 2-11)35 and video recordingmay be performed when nocturnalseizures are suspected Leg surfaceEMG leads are recommended andadditional arm EMG leads may beapplied when the clinical history sug-gests complex sleep-related motor be-haviors such as dream enactment In
KEY POINT
h A daily sleep diary helpsto summarize a patientrsquossleep-wake schedulemore accurately thanmemory often allowsand can facilitateconstruction ofpersonalized plansfor management ofcircadian rhythm sleepdisorders and insomnia
FIGURE 2-10 A 1-minute epoch from a nocturnal polysomnogram showing obstructive sleepapnea in a 46-year-old man who presented with snoring daytime sleepinessand headaches It depicts the standard recording montage that includes the
following leads central (C3-M2 C4-M1) frontal (F3-M2 F4-M1) and occipital (O1-M2 O2-M1)EEGs left and right eye electrooculograms (E1-M2 E2-M1) mentalsubmental electromyogram(Chin1-Chin2) electrocardiogram (ECG1-ECG2 ECG2-ECG3) snore volume (SNORE) nasalpressure transducer (NPRE) nasaloral airflow (NO) thoracic (THOR) and abdominal (ABD)effort arterial oxyhemoglobin saturation (SpO2) plethysmography (Pleth) and left and right eyeelectromyograms (LAT1-LAT2 RAT1-RAT2)
42 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
most cases the diagnostic NPSG is doneon 1 night although NPSG on 2 con-secutive nights may be considered inthe evaluation of parasomnias
Four categories of sleep monitoringdevices for use in the diagnosis of sleepdisorders have often been described34
These are type 1 standard attended in-laboratory polysomnography type 2comprehensive portable unattendedpolysomnography type 3 modifiedportable sleep apnea testing (often car-diorespiratory studies that do not recordsleep) and type 4 continuous single ordual bioparameter recording (eg pulseoximetry) However this categorizationmay not effectively classify the plethoraof out-of-center testing devices currentlyavailable for clinical use Therefore anew device classification system hasrecently been proposed This schemaknown as the SCOPER system catego-rizes out-of-center testing devices basedon measurement of sleep cardiovascu-
lar oximetry position effort and res-piratory parameters36 Within each ofthe six SCOPER categories a level of 0through 5 is assigned as indicated bythe type of sensor or measurementthat the device uses for that category
The most recent clinical guidelinespublished by the Portable MonitoringTask Force of the AASM37 for use ofunattended portable monitoring inthe diagnosis of OSA in adult patientsrecommend that portable monitoringonly be performed in conjunction witha comprehensive sleep evaluation by(or supervised by) a practitioner board-certified in sleep medicine or eligiblefor the certification examination Theseguidelines state that portable monitor-ing may be used in place of NPSG inpatients with a high pretest probabilityof moderate to severe OSA Portablemonitoring should not be used inpatients with significant medical comor-bidities (including but not limited to
KEY POINT
h The complexclassification of portabletesting devices reflectsthe multitude of designsavailable to cliniciansand will undoubtedlychange as technologyadvances
FIGURE 2-11 A The international 10Y20 system for EEG electrode placement refers to the10 and 20 interelectrode distances Even electrode numbers (2 4 6 8)represent the right hemisphere and odd electrode numbers (1 3 5 7)
represent the left hemisphere B Recommended F4-M1 C4-M1 O2-M1 placements of EEGelectrodes as set forth by the American Academy of Sleep Medicine (AASM)
Adapted from Iber C et al American Academy of SleepMedicine35 Used with permission of the American Academy ofSleep Medicine Darien IL 2012
43Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
moderate to severe pulmonary diseaseneuromuscular disease or congestiveheart failure) in patients with othersleep disorders (including central sleepapnea periodic limb movement disor-der insomnia parasomnias circadianrhythm disorders or narcolepsy) or asa screening tool The use of portablemonitoring may be indicated for thediagnosis of OSA in patients for whomattended NPSG is not possible becauseof immobility safety or critical illnessPortable monitoring may be indi-cated to monitor the response to non-continuous positive airway pressuretreatments for OSA including oralappliances upper airway surgery andweight loss The algorithm shown inAppendix B may help in the determi-nation of an adult patientrsquos candidacyfor out-of-center testing for the diag-nosis of OSA An example of portable(or home) monitoring technology isshown in Supplemental Digital Con-tent 2-1 linkslwwcomCONTA15
Recommended technology for port-able monitoring should record at mini-mum airflow respiratory effort andblood oxygenation the airflow effortand oximetric biosensors typically usedfor attended NPSG should be used37
These guidelines published in 2007will likely continue to evolve as newtechnologies emerge and are found tobe effective The current guidelinesrecommend that out-of-center testingbe performed under the auspices of anAASM-accredited comprehensive sleepmedicine program and that a board-certifiedeligible sleep specialist reviewthe raw data from a portable monitor-ing device All patients who undergoportablemonitoring for the diagnosis ofOSA should have a follow-up visit toreview test results Negative or techni-cally inadequate portable monitoringstudies should be followed by attendedin-laboratory NPSG if the clinical suspi-cion for SDB remains high37
The aforementioned testing proce-dures are primarily used in the evalua-tion of SDB Other testing modalitiesare useful in the diagnosis of othercategories of sleep disorders The mul-tiple sleep latency test (MSLT) and itsvariant the maintenance of wakefulnesstest (MWT) are used in the evaluation ofhypersomnia The conventional record-ing montage is similar to that used fornocturnal polysomnography central fron-tal and occipital EEGs left and right eyeelectrooculograms mentalsubmentalEMG and ECG leads Measurement ofthoracic and abdominal effort oxygensaturation and nasaloral airflow are notrequired but may help explain delayedsleep latencies for patients in whomrespiratory disturbances interfere withsleep onset
The MSLT is a validated tool that isconsidered the de facto standard forobjective assessment of excessive day-time sleepiness38 The recommendedprotocol38 involves five 20-minute napopportunities held at 2-hour intervalsthroughout the day If sleep is ob-served the patient is allowed to sleepfor at least 15 minutes The sleep la-tency for each nap is measured as thetime from the start of the nap trial tothe first epoch of sleep A sleep la-tency of 20 minutes is assigned to naptrials during which no sleep isobserved39 The mean sleep latencycalculated as the average sleep latencyacross all nap trials is the final resultThe presence and number of sleep-onset REM periods (SOREMPs) is alsodetermined as this information canhelp to establish a diagnosis of narco-lepsy without cataplexy or to confirmnarcolepsy with cataplexy
The MSLT should be started 15 to30 hours following completion of anocturnal polysomnogram whichshould record at least 6 hours of sleepin order for determination of the meansleep latency to be valid Drugs that may
KEY POINT
h Careful considerationshould be given tothe indications forout-of-center testingAttended nocturnalpolysomnography isindicated if a portablestudy yields a negativeor technicallyinadequate result
44 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
interfere with sleep latency or REM la-tency should be discontinued 2 weeksbefore testing whenever possible Ascreen may be performed on the day oftesting if there is suspicion that pre-scribed or illicit substances may con-tribute to the patientrsquos sleepiness38
No large multicenter systematicallycollected normative data are availablefor mean sleep latency values on theMSLT38 Nonetheless a mean sleep la-tency of greater than 10 minutes is of-ten considered normal whereas a meansleep latency of 8 to 10 minutes is con-sidered a physiologic gray zone40 Thenormative data for children are classi-fied by Tanner stage of developmentthough the MSLT is typically not per-formed in children aged younger than 6or 7 years because some daytime nap-ping may still be normal in youngchildren41 The second edition of theInternational Classification of SleepDisorders Diagnostic and CodingManual (ICSD-2)42 requires the pres-ence of a mean sleep latency of lessthan 8 minutes and two or moreSOREMPs as part of the diagnosticcriteria for narcolepsy without cata-plexy However the ICSD-2 also notesthat a mean sleep latency of less than 8minutes may occur in up to 30 of thegeneral population Therefore whilethe MSLT is a helpful and widely usedtool it remains an imperfect gold stand-ard in the assessment of daytime sleepi-ness This necessitates that theevaluation of daytime sleepiness notrest on the MSLT results alone butassimilate the clinical history subjectivecomplaints diagnostic study results andother pertinent medical information38
Practice parameters from theAASM state that the MSLT is indicatedfor diagnostic confirmation of sus-pected narcolepsy and may be indi-cated to differentiate idiopathichypersomnia from narcolepsy38 TheMSLT is not indicated for routine
assessment of OSA syndrome or toassess response to treatment of SDBand is not routinely indicated for eval-uation of sleepiness in medical orneurologic disorders (except for narco-lepsy) insomnia or circadian rhythmdisorders
TheMWTprovides an objectivemeas-ure of a patientrsquos ability to remain awakerather than the tendency to fall asleepduring the day The key differencebetween the MWT and the MSLT is thatin the former the patient is asked to tryto stay awake under circumstances con-ducive to sleep rather than to fall asleepThe MWT provides an objective vali-dated assessment of the ability to remainawake for a defined length of time38 Therecommended protocol includes four40-minute trials that begin at 2-hourintervals with the first trial to start 15 to30 hours after the patientrsquos wake-uptime A nocturnal polysomnogram onthe preceding night is not requiredHowever the patient should obtain asufficient amount of sleep during thenight before the MWT Each trial isterminated after 40 minutes if no sleepoccurs or after unequivocal sleep onset(defined as three continuous epochsof stage N1 sleep or one epoch of anyother stage of sleep) has occurred38
One indication for the MWT is to as-sess an individualrsquos ability to remainawake when his or her inability to re-main awake constitutes a public orpersonal safety issue This can becomea pressing issue for individuals em-ployed in the transportation43 con-struction or health care industriesThe MWT may be indicated to assesstreatment response in patients withknown excessive daytime sleepiness
Limited amounts of normative dataare available for the MWT Historicallymultiple testing protocols make syn-thesis of results more challenging TheMWT is used much less often in clinicalpractice compared to the MSLT Patient
KEY POINTS
h The multiple sleeplatency test is the goldstandard for objectiveassessment of daytimesleepiness butinterpretation of theresults must be madewithin the clinicalcontext of the patientrsquoshistory
h In the multiple sleeplatency test the patientis instructed to try tosleep during each naptrial In the maintenanceof wakefulness test thepatient is instructed totry to remain awakeduring the nap trial
h A baseline nocturnalpolysomnogram isrequired before amultiple sleep latencytest and considered butnot required before amaintenance ofwakefulness test
45Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
age may also affect the mean sleep la-tency values on both the MWT and theMSLT43 and may represent evolution ofcircadian rhythm and sleep architec-ture across the lifetime A study of 383patients with narcolepsy with cataplexyexamined the clinical and polysomno-graphic data at the time of diagnosis(age range 5 to 84 years) and found aprogressive decrease in the number ofSOREMPs and a progressive increase inthe mean sleep latency on the MSLT asa function of age44 Given its limita-tions the MWT may thus be used tosupplement the clinical history in theassessment of ability to stay awake butshould not be the sole determinant ofthis parameter
Actigraphy is also used in the clinicalevaluation of patients with sleep disor-ders particularly circadian rhythm sleepdisorders An actigraph is a watchlikedevice that is worn on the wrist for anextended period usually in the range ofweeks The actigraph records move-ment and uses an algorithm to estimatethe amounts of sleep and wake timeduring the recording period Analysissoftware uses movement to estimatewhen sleep and wakefulness haveoccurred Review of the data can pro-vide objective insight into the patientrsquossleep pattern including timing andduration of major sleep disruptionsActigraphy is indicated as part of theevaluation of patients with advancedsleep-phase syndrome delayed sleep-phase syndrome and shift work disor-der and may be indicated in the evalua-tion of jet lag disorder and nonY24-hoursleep-wake syndrome including thatassociated with blindness45 It can alsoserve as a measure of treatment re-sponse in patients with insomnia andcircadian rhythm sleep disorders Forpopulations in which traditional sleepmonitoring may be challenging suchas pediatric or older adult patientsactigraphy may provide valuable infor-
mation about the patientrsquos sleep pat-tern or response to treatment Whenpolysomnography is not availableactigraphy is indicated to estimate totalsleep time in patients with OSA45
OTHER ASSESSMENTMODALITIESLaboratory evaluation and neuroimag-ing with either CT or MRI may beconsidered on an individual basis asindicated by the clinical history Com-plete blood count (CBC) serum chem-istries or measures of thyroid functionmay be obtained if an underlying med-ical disorder is thought to contribute tothe patientrsquos sleep symptoms Forinstance these laboratory studies maybe consideredwhen daytime fatigue is apredominant symptom Serum ironstudies including ferritin level shouldbe checked in patients with restless legssyndrome46 Neuroimaging should beconsidered in patients with antecedenttrauma or for any sleep disorder pa-tient with an abnormal neurologic ex-amination to evaluate for a structuraletiology of the patientrsquos symptoms
APPROACH TO THE PATIENTEvaluation of suspected sleep disordersis best accomplished by a stepwisemultidimensional approach (Case 2-2)A thorough sleep history includes de-tailed description of sleep-related symp-toms nocturnal behaviors the patientrsquossleep schedule level of daytime sleepi-ness and subsequent effects on daytimefunctioning Collateral history from thepatientrsquos bed partner or family is oftennecessary to understand the severity andcontext of the patientrsquos symptoms Sub-jective assessments of sleepiness suchas the Epworth Sleepiness Scale areeasily administered and useful to tracksymptomatic progression or treatmentresponse from one visit to the nextCertain physical examination findingsmay also raise clinical suspicion of
KEY POINTS
h Actigraphy can beuseful in evaluation andtreatment of circadianrhythm sleep disordersand in management ofinsomnia
h Neuroimaging is notroutinely indicated inthe clinical evaluation ofsleep disorders andshould be pursued on acase-by-case basis
46 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
particular sleep disorders For patientsin whom multiple sleep disorders aresuspected systematic use of diagnostictesting allows for accurate identificationof specific diagnoses In a patient withinsomnia and symptoms suggestive ofSDB nocturnal polysomnography shouldbe the first procedure performed Ifthe insomnia persists despite adequatetreatment of SDB further evaluationwith sleep diaries and possibly actigra-
phy may be considered to better char-acterize the patientrsquos sleep patternActigraphy may then again be pursuedto gauge treatment response upon man-agement of the patientrsquos insomnia
The diagnostic modalities availablefor evaluation of sleep disorders arerapidly evolving In-laboratory nocturnalpolysomnography currently remains thegold standard for assessment of SDBHowever the multitude of out-of-center
KEY POINT
h Careful assimilation ofthe clinical history thesleep-specific physicalexamination patientquestionnaires anddiagnostic test resultsleads to the mostaccurate assessment ofpatients with symptomsrelated to sleep oralertness
Case 2-2A 23-year-old woman reported a 4-year history of insomnia Throughoutcollege she was a lsquolsquonight owlrsquorsquo never scheduled classes that started before100 PM and always did well in school During the past 6 months shedeveloped progressive difficulty staying awake in her job as a financialanalyst andwas concerned about how this might affect her job performance
During the week she was in bed by midnight but was unable to fallasleep until 200 AM and awoke with difficulty to an alarm at 600 AMfeeling tired She denied any thought rumination or physical discomfortat bedtime She had tried over-the-counter sleep aids that provided nosymptomatic improvement and worsened morning grogginess Onweekends she slept from 200 AM to 1100 AM and awakened feelinglsquolsquopretty goodrsquorsquo She had nocturia up to once per night and occasionalmorning headaches She had no bed partner but reported gaspingrespirations nocturnal palpitations and snort arousals On about 4 nightsper week she experienced a sensation of needing to move her legswhile trying to fall asleep This sensation was relieved by movement andwas worse at night than during the day Her legs sometimes movedspontaneously at night or while seated quietly for long periods duringthe day She felt sleepy during the afternoon especially while workingat her computer She denied drowsiness while driving She occasionallytook a 30-minute nap on the weekend and found it to be refreshingShe drank one to two cups of coffee every morning and had a 12-oz dietcaffeinated soda at 300 PM Her sleepiness had not caused her to makeany mistakes at work and she denied any mood disturbance
Physical examination was notable for a body mass index of 32 kgm2 neckcircumference of 381 cm (15 in) and modified Mallampati class III oral airwayNasal passages were narrow with turbinate hypertrophy bilaterally andhard palate was high-arched and narrow Nomicrognathia or retrognathia waspresent She had molar occlusion class I bilaterally with no overjet or overbiteThe general cardiac respiratory and neurologic examinations were normal
Comment This case illustrates how discussion of the chief complaint raisessuspicion for multiple sleep disorders The history suggests a circadian rhythmsleep disorder particularly delayed sleep-phase syndrome sleep-disorderedbreathing and restless legs syndrome Diagnostic evaluation should includenocturnal polysomnogramwith consideration toperform testing at the patientrsquospreferred sleep time and serum iron studies Sleep diaries andor actigraphymay be considered for further assessment of the patientrsquos sleep pattern
47Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
testing devices continues to grow andmany may provide useful alternativesthat under appropriate circumstancescould allow more expedient conven-ient and less costly evaluations ofincreased numbers of patients whopreviously had only limited or delayedaccess to sleep services
VIDEO LEGENDSupplemental Digital Content 2-1
Home sleep study Video demonstrates a homesleep study using an unattended type 3 portablemonitoring device The patient is a 56-year-oldman who is experiencing morning headachesand concentration and alertness problems atwork He has a history of mild snoring and ar-terial hypertension His Epworth SleepinessScale score is 18 his neck circumference is19 in he has a Mallampati classification score ofIII and his body mass index is 41 kgm Theapnea-hypopnea index is 84 eventsh Channelsrecorded in this sleep study include arterialoxyhemoglobin saturation heart rate oral-nasalpressure flow snoring inductive plethysmog-raphy for chest efforts and body position
linkslwwcomCONTA15
B 2013 Marcel Hungs MD PhD Used withpermission
REFERENCES1 National Institutes of Health National
Center on Sleep Disorders ResearchSleep disorders research planwwwnhlbinihgovhealthprofsleep201101011NationalSleepDisordersResearch-PlanDHHSPublication11-7820pdf PublishedNovember 2011
2 Dinges DF An overview of sleepiness andaccidents J Sleep Res 19954(S2)4Y14
3 Mills RJ Young CA A medical definitionof fatigue in multiple sclerosis QJM 2008101(1)49Y60
4 Chervin RD Sleepiness fatigue tirednessand lack of energy in obstructive sleepapnea Chest 2000118(2)372Y379
5 Chotinaiwattarakul W OrsquoBrien LM Fan LChervin RD Fatigue tiredness and lack ofenergy improve with treatment for OSAJ Clin Sleep Med 20095(3)222Y227
6 American Academy of Sleep MedicineThe international classification of sleepdisorders diagnostic and coding manual2nd ed Westchester IL American Academyof Sleep Medicine 2005
7 Ebben MR Spielman AJNon-pharmacological treatments forinsomnia J Behav Med 200932(3)244Y254
8 Roth T Insomnia definition prevalenceetiology and consequences J Clin SleepMed 20073(5 suppl)S7YS10
9 Yang CM Spielman AJ Glovinsky PNonpharmacologic strategies in themanagement of insomnia Psychiatr ClinNorth Am 200629(4)895Y919 abstract viii
10 Katz ES DrsquoAmbrosio CM Pediatricobstructive sleep apnea syndrome ClinChest Med 201031(2)221Y234
11 Kohler M Bloch KE Stradling JR The role ofthe nose in the pathogenesis of obstructivesleep apnea Curr Opin Otolaryngol HeadNeck Surg 200917(1)33Y37
12 Kryger MH Atlas of clinical sleep medicinePhiladelphia PA Elsevier 2010
13 Zonato AI Martinho FL Bittencourt LRet al Head and neck physical examinationcomparison between nonapneic andobstructive sleep apnea patientsLaryngoscope 2005115(6)1030Y1034
14 Mallampati SR Gatt SP Gugino LD et alA clinical sign to predict difficult trachealintubation a prospective study Can AnaesthSoc J 198532(4)429Y434
15 Samsoon GL Young JR Difficult trachealintubation a retrospective studyAnaesthesia 198742(5)487Y490
16 Huang HH Lee MS Shih YL et alModified Mallampati classificationas a clinical predictor of peroralesophagogastroduodenoscopy toleranceBMC Gastroenterol 20111112
17 Friedman M Ibrahim H Bass L Clinicalstaging for sleep-disordered breathingOtolaryngol Head Neck Surg 2002127(1)13Y21
18 Cheng RHW Yiu CKY Leung WKOral health in individuals with Downsyndrome In Dey S ed Prenatal diagnosisand screening for down syndromeInTech wwwintechopencombookshowtoreferenceprenatal-diagnosis-and-screening-for-down-syndromeoral-health-in-individuals-with-down-syndromePublished 2011 Accessed August 24 2012
19 Katz I Stradling J Slutsky AS et al Dopatients with obstructive sleep apneahave thick necks Am Rev Respir Dis1990141(5 pt 1)1228Y1231
20 Kushida CA Efron B Guilleminault C Apredictive morphometric model for theobstructive sleep apnea syndrome AnnIntern Med 1997127(8 pt 1)581Y587
48 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
21 Saccucci M Tettamanti L Mummolo S et alScoliosis and dental occlusion a review ofthe literature Scoliosis 2011615
22 Battagel JM Kotecha B Dental side-effectsof mandibular advancement splint wear inpatients who snore Clin Otolaryngol200530(2)149Y156
23 Morcos SS Patel PK The vocabulary ofdentofacial deformities Clin Plast Surg200734(3)589Y599
24 Epstein LJ Kristo D Strollo PJ Jr et alClinical guideline for the evaluationmanagement and long-term care ofobstructive sleep apnea in adults J ClinSleep Med 20095(3)263Y276
25 Johns MW A new method for measuringdaytime sleepiness the Epworth sleepinessscale Sleep 199114(6)540Y545
26 Johns MW Daytime sleepiness snoring andobstructive sleep apnea The EpworthSleepiness Scale Chest 1993103(1)30Y36
27 Chervin RD Aldrich MS The EpworthSleepiness Scale may not reflect objectivemeasures of sleepiness or sleep apneaNeurology 199952(1)125Y131
28 Buysse DJ Reynolds CF 3rd Monk THet al The Pittsburgh Sleep Quality Index anew instrument for psychiatric practice andresearch Psychiatry Res 198928(2)193Y213
29 Chervin RD Hedger K Dillon JE Pituch KJPediatric sleep questionnaire (PSQ) validityand reliability of scales for sleep-disorderedbreathing snoring sleepiness and behavioralproblems Sleep Med 20001(1)21Y32
30 Chung F Yegneswaran B Liao P et al STOPquestionnaire a tool to screen patients forobstructive sleep apnea Anesthesiology2008108(5)812Y821
31 Walters AS LeBrocq C Dhar A et alValidation of the International Restless LegsSyndrome Study Group rating scale forrestless legs syndrome Sleep Med 20034(2)121Y132
32 Bastien CH Vallieres A Morin CMValidation of the Insomnia Severity Indexas an outcome measure for insomniaresearch Sleep Med 20012(4)297Y307
33 YOURSLEEPaasmnetorg from the AmericanAcademy of Sleep Medicine Two weeksleep diary yoursleepaasmnetorgpdfsleepdiarypdf Accessed August 24 2012
34 Kushida CA Littner MR Morgenthaler Tet al Practice parameters for the indicationsfor polysomnography and relatedprocedures an update for 2005 Sleep200528(4)499Y521
35 Iber C Ancoli-Israel S Chesson A et alThe AASM manual for scoring of sleep andassociated events rules terminology andtechnical specifications 1st ed WestchesterIL American Academy of Sleep Medicine2007
36 Collop NA Tracy SL Kapur V et alObstructive sleep apnea devices forout-of-center (OOC) testing technologyevaluation J Clin Sleep Med 20117(5)531Y548
37 Collop NA Anderson WM Boehlecke Bet al Clinical guidelines for the use ofunattended portable monitors in thediagnosis of obstructive sleep apnea in adultpatients Portable Monitoring Task Forceof the American Academy of SleepMedicine J Clin Sleep Med 20073(7)737Y747
38 Littner MR Kushida C Wise M et alStandards of Practice Committee of theAmerican Academy of Sleep MedicinePractice parameters for clinical use of themultiple sleep latency test and themaintenance of wakefulness test Sleep200528(1)113Y121
39 Carskadon MA Dement WC Mitler MMet al Guidelines for the multiple sleeplatency test (MSLT) a standard measure ofsleepiness Sleep 19869(4)519Y524
40 van den Hoed J Kraemer H Guilleminault Cet al Disorders of excessive daytimesomnolence polygraphic and clinical datafor 100 patients Sleep 19814(1)23Y37
41 Hoban TF Chervin RD Assessment ofsleepiness in children Semin PediatrNeurol 20018(4)216Y228
42 ICSD-2 The international classification ofsleep disorders pocket version diagnosticand coding manual 2nd ed WestchesterIL American Academy of Sleep Medicine2005
43 Arand D Bonnet M Hurwitz T et alThe clinical use of the MSLT and MWTSleep 200528(1)123Y144
44 Dauvilliers Y Gosselin A Paquet J et alEffect of age on MSLT results in patientswith narcolepsy-cataplexy Neurology200462(1)46Y50
45 Morgenthaler T Alessi C Friedman Let al Practice parameters for the use ofactigraphy in the assessment of sleep andsleep disorders an update for 2007 Sleep200730(4)519Y529
46 Gamaldo CE Earley CJ Restless legssyndrome a clinical update Chest2006130(5)1596Y1604
49Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited

Sleepiness is thought to result from neu-robiologic processes that regulate circa-dian rhythms and the drive to sleep2 andsome individuals will clearly articulatesleepiness as a tendency to doze un-intentionally Fatigue is defined aslsquolsquoreversible motor and cognitive impair-ment with reduced motivation and
desire to restrsquorsquo3 and is postulated torepresent a process that is distinct fromsleepiness However patients ofteninterchangeably use the terms lsquolsquotired-nessrsquorsquo lsquolsquosleepinessrsquorsquo and lsquolsquofatiguersquorsquo34 Pa-tients with obstructive sleep apnea (OSA)and possibly other sleep disorders as-sociated with daytime sleepiness may
TABLE 2-1 Components of the Sleep History
b Presenting Sleep-Related Symptom
Onset
Precipitatingpredisposing factors
Duration
Frequency
Severity
b Associated Nocturnal Symptoms
Sleep-disordered breathing
Snoring
Witnessed apneas
Morning headache
Mouth breathing
Acid reflux
Nasal congestion
Nocturia
Erectile dysfunction
Nocturnal dyspnea
Nocturnal behavior
Sleepwalking
Sleeptalking
Sleep eating
Leg movement
Dream enactment
Bruxism
Nocturnal awakenings
Timing in night
Precipitants
Duration
Frequency
Activities while awake
Other symptoms
Leg discomfort
Urge to move
Sleep paralysis
b Time of Symptoms (Time Duringthe Sleep Period That SymptomsOccur)
b Daytime Functioning
Daytime sleepiness
Mood disturbance
Impaired school or workperformance
Decreased alertness while driving
Impaired interpersonalrelationships
Decreased concentration ormemory
Cataplexy or hypnagogic orhypnopompic hallucinations
Leg discomfort urge to moveor spontaneous movements
b Sleep Schedule and Sleep Hygiene
Bed time
Sleep latency
Wake time
Rise time (when patient gets upfrom bed)
Details of bedtime routine
Description of activities duringnocturnal awakenings
b Use of Sleep Aids and Stimulants
Over-the-counter (includingherbal) agents
Prescription medications
Caffeine
Energy drinks
33Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
report fatigue tiredness or lack ofenergy at times even when they denysleepiness4 Interestingly these symp-toms (like sleepiness) appear toimprove with treatment of the under-lying OSA5 A clear understanding ofwhether the patient experiences anoverwhelming urge to sleep duringthe day may help the clinician decidewhich diagnostic studies to pursue andalso guides discussion about potentialdiagnoses that may contribute to thepatientrsquos symptoms Special attentionshould be paid to situations in whichthe patientrsquos sleepiness becomes evi-dent Does the patient doze during con-versation while at work or while drivingIs the patientrsquos concentration or memoryimpaired because of sleepiness Dozingwhile operating heavy machinery or amotor vehicle can lead to devastatingoutcomes and this has both individualand public health implications Daytimesleepiness that impairs a patientrsquos func-tional capabilities can threaten job se-curity and have a negative impact oninterpersonal relationships The con-text of a patientrsquos daytime sleepinesshighlights its severity and impact
The symptom of insomnia is de-fined as difficulty with sleep initiationor maintenance waking too early orsleep that is nonrestorative despiteample opportunity to sleep6 Disordersthat cause insomnia have diagnosticcriteria to specify that the insomniasymptoms should be accompanied byat least one manifestation of daytimeimpairment (such as fatigue mood dis-turbance headaches or gastrointestinalsymptoms in response to sleep loss) orimpaired memory concentration orperformance The point prevalence ofinsomnia is estimated at 6 to 15 inthe general population but is clearlyhigher among certain subgroups suchas patients with psychiatric disease7
Population-based studies done withvaried adult samples from multiple
countries indicate that approximately30 of the general adult populationreports one or more insomnia symp-tom8 Because insomnia is so commonneurologists routinely encounter pa-tients with the symptom As the etiol-ogy of insomnia is often multifactorialthe evaluation can be complex andrequires a detailed history that exploresmany potential contributors
A helpful framework in which to con-sider a patientrsquos insomnia is known asthe lsquolsquo3Prsquorsquo model9 which aids identifica-tion of possible causes of insomnia andhighlights potential targets for treat-ment This model calls for temporalclassification of factors that affect a pa-tientrsquos insomnia characteristics thatpredispose a person to develop in-somnia events that precipitate the in-somnia acutely and behaviors andattitudes that perpetuate insomnia andmay cause it to become chronic Com-mon predisposing factors include per-sonality traits such as excessive worryingor cognitive hyperarousal or the degreeto which a personrsquos preferred sleepingtimes differ from social norms9 Precip-itating factors are often readily identi-fied as major life transitions such aschange in marital status death in thefamily or change in employment How-ever subtler challenges to a personrsquosroutine or environment may also pre-cipitate the onset of insomnia In somesituations the patientrsquos sleep normal-izes upon resolution of the precipitantin other cases behaviors and mindsetsaccrued during the acute phase of theinsomnia can perpetuate the patientrsquossleep disturbance Such perpetuatingfactors can include perceived associa-tions between the sleeping environ-ment and inability to sleep or escalateduse of caffeine throughout the dayOther important details include specif-ics about the patientrsquos insomnia at thepresent time including the latency tosleep timing duration and causes of
KEY POINTS
h Information from thepatient medical recordand any available bedpartner friend orfamily member canclarify the extent andconsequences of thepatientrsquos sleep-relatedsymptoms
h The 3P framework ofinsomnia comprisespredisposingprecipitating andperpetuating factorsDiscussion of all factorsfacilitates identificationof potential treatmenttargets
34 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
nocturnal awakenings behaviors dur-ing nocturnal awakenings and latencyto fall back asleep after each awakeningA useful approach is to ask the patientfor a detailed start-to-finish descriptionof the entire typical sleep period anddaytime period Any medications pre-viously or currently used to facilitatesleep should also be identified
The sleep history should screenfor potentially relevant sleep disordersthat may cause excessive daytime sleep-iness or insomnia (Case 2-1) Thepresence of symptoms such as snor-ing witnessed apneas and morningheadaches raises the suspicion forsleep-disordered breathing (SDB) Leg
discomfort associated with an urge tomove that worsens at night andimproves with leg movement indicatesrestless legs syndrome and may con-tribute to the patientrsquos poor sleepquality and impair daytime functioningSleep paralysis and hypnagogic orhypnopompic hallucinations are notspecific to a particular sleep disorderwhile a history of cataplexy is patho-gnomonic for narcolepsy and must beexplored when a patient presents withreports of central hypersomnia ratherthan SDB When relevant the clinicianshould also ask about nocturnal behav-iors specifically ones that may pose riskof injury to the patient or bed partner
Case 2-1A 44-year-old man with a long-standing history of loud frequent snoringpresented because of his wifersquos concerns related to his snoring His wifehad witnessed him to have occasional pauses in his breathing during sleepand at times he awakened to his snoring He reported frequent acidreflux and morning headaches Approximately once per month he wouldawaken lsquolsquofeeling like my heart is racing and I need to catch my breathrsquorsquoHe had occasional nasal congestion but always awakened with a drymouth and sore throat He denied any leg discomfort but his wife hadtold him that he tossed and turned frequently during sleep
His sleep schedule was the same every night he was in bed by 1000 PMfell asleep immediately without the use of any sleep aids and awakenedat 600 AM feeling tired He had up to four nocturnal awakenings pernight two were attributed to nocturia and the rest were of unknownetiology Each awakening lasted a few minutes and he fell asleep againeasily He had had a few episodes of sleepwalking as a child but none sincethe age of 8 years
He felt sleepy during the day with a propensity to doze unintentionallywhile reading or watching television He denied drowsiness while driving butlimited his driving to his 20-minute commute to and from work his wifedrove for longer distances and hewould often sleep in the passenger seat Hissleepiness was worse in the midafternoon and if given the opportunity hewould nap for 1 hour on the weekends He found naps to be somewhatrefreshing He drank two to three cups of coffee every morning and had a12-oz caffeinated sodawith lunch His sleepiness had not caused him tomakeany mistakes in his job as a physical therapist although he felt that he hadpotential for further improvement in his job performance He also reportedfeeling more irritable in recent months but this had not caused anydifficulties at home or work
Comment This case illustrates the multiple components of a concisebut still detailed sleep history The patientrsquos daytime symptoms provideinsight about the effects of the patientrsquos untreated sleep disorder
35Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
such as sleepwalking driving or cook-ing while asleep or dream-enactmentbehavior If the patient reports suchbehavior further inquiry must be madeabout the frequency of these events andany history of injury sustained due to thesleep-related behavior Details of thesleep history permit a thorough differ-ential diagnosis and can also guide adiscussion of safety concerns
PHYSICAL EXAMINATIONA comprehensive multisystem exami-nation is an important aspect of thesleep evaluation Measurement of theweight height body mass index (BMI)neck circumference and blood pres-sure and heart rate should be per-formed for nearly all patients withsymptoms related to sleep or alertnessOther salient features of the generalexamination include auscultation forany cardiac or respiratory abnormalitiesand identification of peripheral edemaA focused neurologic examinationshould be guided by the patientrsquos his-tory For instance a mental status as-sessment should be considered if apatient with excessive daytime sleepi-ness also complains of memory loss If apatient with a history of diabetes melli-
tus endorses symptoms of restless legssyndrome it is worthwhile to assess forstocking-glove distribution sensory lossand weakness
Detailed examination of the headand neck should be performed as partof a comprehensive sleep evaluationThe patientrsquos facial morphology shouldbe assessed for features of long facesyndrome which includes infraorbitaldarkening mouth breathing elongatedmidface and nasal atrophy10 A 2009review11 reports that previous observa-tional and cross-sectional studies haveshown a relationship between chronicnasal obstruction and OSA Thus a thor-ough nasal examination should be per-formed on patients with sleep-relatedcomplaints Examination of the nasalairway should include evaluation forsymmetry of the nares nasal septum de-viation (Figure 2-1)12 and nasal turbi-nate hypertrophy A bedside assessmentof nasal airflow can be accomplished by
KEY POINT
h Details of facialmorphology nasalairway patency and oralairway crowding arekey features of thesleep-specificexamination
FIGURE 2-1 Nasal septal deviation Thisstructural abnormality canpredispose a patient to havesleep-disordered breathing
Reprinted from Kryger MH Elsevier12 B 2010 withpermission from Elsevier
FIGURE 2-2 Retrognathia Retrognathiais derived from the termslsquolsquoretrorsquorsquo (backward) and
lsquolsquognathosrsquorsquo (jaw) With retrognathia one orboth jaws recede with respect to the frontalplane of the forehead The condition maypredispose a patient to obstruction of theairway and sleep apnea by displacing thetongue against the retropharyngeal regioncompromising airflow Retrognathia issometimes corrected through surgicalrepositioning or advancement of themandible
Reprinted from Kryger MH Elsevier12 B 2010 withpermission from Elsevier
36 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
asking the patient to press the indexfinger against the left nostril and take adeep breath in on the right side thisshould be repeated on the oppositeside as well The patientrsquos facial mor-phology should be assessed for man-dibular retrognathia (Figure 2-2)12 Withthe patientrsquos head in a neutral posi-tion a virtual line is drawn from thevermillion border of the lower lip tothe chin Mandibular retrognathia issuggested if the anterior prominence ofthe chin is 2 mm or more behind thevirtual line13
The modified Mallampati classifica-tion is commonly used for assessmentof the oral airway in patients withsuspected SDB The Mallampati classi-fication14 was developed to identifypatients in whom tracheal intubationwould be difficult the initial description
divided patients into three classes Twoyears later15 this was modified to de-scribe four groups class I class II classIII and class IV Figure 2-3 16 illustratesthe modified Mallampati classificationassessed with the tongue protrudedThe Friedman palate position classifi-cation17 also commonly referencedutilizes the same four categories but isdone with the tongue at rest and notextended Either the Mallampati orFriedman classification may be used todescribe the patency of the oral airway
Tonsils should be classified based onthe degree of hypertrophy (Figure 2-4)12grade I tonsils are inside the tonsillarfossa lateral to the posterior pillarsgrade II tonsils occupy 25 of theoropharynx grade III tonsils occupy50 of the oropharynx and grade IVtonsils occupy at least 75 of the
FIGURE 2-3 Modified Mallampati classification The class is determined by looking at theanatomy of the oral cavity and describes tongue size relative to oropharyngealsize The test is conducted with the patient seated the head held in a neutral
position and the mouth wide open and relaxed The subsequent classification is assigned basedupon the pharyngeal structures that are visible
Reprinted from Huang HH et al BMC Gastroenterol16 B 2011 BioMed Central Ltd wwwbiomedcentralcom1471-230X1112
37Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
oropharynx and nearly meet in the mid-line13 A high-arched narrow hard pal-ate (Figure 2-5)18 may predispose thepatient to have SDB Katz and col-leagues19 have shown that patients withOSA have significantly increased neckcircumference compared to nonapneicsnorers greater distribution of neck fat
may contribute to mass loading on theupper airway in patients with OSA Thepatientrsquos neck circumference should bemeasured at the superior border of thecricothyroid membrane19 A neck cir-cumference greater than 40 cm (157in) has been shown to be predictive ofOSA with 61 sensitivity and 93specificity regardless of sex20
Assessment of the patientrsquos anteriorand posterior dentition can also re-veal anatomic findings that may pre-dispose a person to certain sleepdisorders Two features to note in eval-uation of the anterior dentition areoverjet and overbite (Figure 2-6)21
Overjet as shown in Figure 2-712 isthe horizontal distance between theupper right central incisor and thebuccal surface of the correspondinglower tooth while overbite is the ver-tical distance between these twopoints22 These measurements are typ-ically reported in millimeters The An-gle classification system is used todescribe the first molar position on
FIGURE 2-4 Tonsil size grading Thisstructural abnormality canpredispose a patient to havesleep-disordered breathing
Reprinted from Kryger MH Elsevier12 B 2010 withpermission from Elsevier
FIGURE 2-5 Deficientmaxillarydevelopment inan individual with
Down syndrome leading to highand narrow hard palate
Reprinted with permission from ChengRHW et al InTech18 B 2011 W KeungLeung wwwintechopencombooksprenatal-diagnosis-and-screening-for-down-syndromeoral-health-in-individuals-with-down-syndrome
FIGURE 2-6 Overjet andoverbite Overjetis defined as
increased projection of the upperteeth in front of the lower teethas measured parallel to theocclusal plane Overbite is thevertical overlapping of maxillaryteeth over mandibular teethusually measured perpendicularto the occlusal plane
Reprinted from Saccucci M et al Scoliosis21
B 2011 BioMed Central Ltd wwwscoliosisjournalcomcontent6115
38 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
the mandibular and maxillary dentalarches23 Figure 2-8 shows class I oc-clusion and class II and III malocclu-
sion Of note the mesiobuccal surfaceis the aspect of the tooth that is adja-cent to the cheek mucosa
The Adult Obstructive Sleep ApneaTask Force of the American Academyof Sleep Medicine (AASM) recommen-ded in recent clinical guidelines24 thatthe following physical findings maysuggest the presence of OSA increasedneck circumference (greater than 432cm [17 in] in men greater than 406 cm[16 in] in women) BMI 30 kgm2 orgreater modified Mallampati classifica-tion of III or IV presence of retrognathialateral peritonsillar narrowing macro-glossia tonsillar hypertrophy elongatedenlarged uvula high-archednarrowhard palate nasal abnormalities (egpolyps deviation valve abnormalities
KEY POINT
h Classification of thepatientrsquos dentition helpsto evaluate the positionof the maxillary archrelative to themandibular arch
FIGURE 2-7 OverjetDisplacementof the
mandibular teeth posteriorly inrelationship to the maxillary teethresults inmoreposteriorly crowdedupper airways predisposingpatients for the developmentof obstructive sleep apnea
Reprinted from Kryger MH Elsevier12
B 2010 with permission from Elsevier
FIGURE 2-8 Angle class occlusionmalocclusion A Angle class I occlusion also known asneutrocclusion The mandibular and maxillary dental arches have a normalanterior-posterior relationship The mesiobuccal groove of the mandibular first
molar interdigitates with the mesiobuccal cusp of the maxillary first molar B Angle class IImalocclusion also known as distoclusion The mandibular dental arch is in distal anterior-posteriorrelationship to the maxillary dental arch The mesiobuccal groove of the mandibular first molar isdistal to the mesiobuccal cusp of the maxillary first molar C Angle class III malocclusion alsoknown as mesioclusion The mandibular dental arch is in mesial anterior-posterior relationship tothe maxillary dental arch The mesiobuccal groove of the mandibular first molar is mesial to themesiobuccal cusp of the maxillary first molar
Reprinted fromMorcos SS Patel PK Clin Plast Surg23 B 2007 with permission from Elsevier wwwsciencedirectcomsciencearticlepiiS0094129807000843
39Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
and turbinate hypertrophy) andoroverjet To prevent overlooking thesefindings a thorough head and neckassessment as described in Table 2-2should be incorporated into the phys-ical examination of all patients whopresent with sleep-related complaints
SUBJECTIVE ASSESSMENTSeveral patient-completed question-naires are inexpensive and time-efficient
reasonably well validated and com-monly used They can help to increasestandardization in evaluations of patientsby different clinicians or across centersPerhaps the most well-known andwidely used is the Epworth SleepinessScale25 a subjective assessment of thepatientrsquos daytime sleep propensity inrecent times As shown in Appendix Athe Epworth Sleepiness Scale asks theresponder to use a four-point Likertscale (0 1 2 or 3) to indicate thelikelihood of dozing in eight distinctsedentary conditions A total score of 10or greater out of a possible 24 suggestsexcessive daytime sleepiness25 Whilethe Epworth Sleepiness Scale score canbe easily incorporated into the clinicalevaluation it should not be used as asubstitute for objective measurement ofsleepiness The Epworth Sleepiness Scalescore may correlate to a limited extentwith the presence and severity of OSA26
but some studies have failed to find anystatistically significant association withmean sleep latency on multiple sleep la-tency tests or with severity of OSA27
The most advantageous use of theEpworth Sleepiness Scale may be to followan individualrsquos self-assessment of sleep-iness longitudinally and it may also serveas an indicator of treatment response
Many other questionnaires may beutilized in a clinical sleep evaluationsome pertain to overall sleep qualitywhile others are disorder-specific ThePatient Reported Outcomes Measure-ment Information System (PROMIS) isan NIH-supported system of measuresfor patient-reported health status andincludes questions on sleep disturb-ance The Pittsburgh Sleep QualityIndex (PSQI) is a validated question-naire that inquires about sleep qualityand disturbances over the previousmonth28 The parent-completed Pe-diatric Sleep Questionnaire29 containsa validated reliable 22-item scale tohelp assess risk for SDB in children
KEY POINTS
h The Epworth SleepinessScale apatient-completedquestionnaire assessesthe patientrsquos subjectivetendency to doze duringsedentary situations inrecent times not onlyat the moment thequestionnaire iscompleted
h The Epworth SleepinessScale should not beused in lieu of diagnostictesting but may be avaluable componentof ongoing clinicalevaluation
TABLE 2-2 Head and NeckExamination
b Face
Featuresof long face syndrome
Infraorbital darkening
Mouth breathing
Elongated midface
Nasal atrophy
b Oral Airway
Mandibular retrognathia
Low soft palate (modifiedMallampati classification)
Large or boggy uvula
Erythematous pillars
Tonsillar hypertrophy
High narrow hard palate
Neck circumference
Overjet
Overbite
Angle classification(malocclusion)
Macroglossia
Worn occlusive surfaces(suggestive of bruxism)
b Nasal Airway
Symmetry of the nares
Nasal septum deviation
Nasal airflow
Collapse of nasal alae oninspiration
b Neck
Neck circumference
40 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
The STOP-BANG questionnaire devel-oped and validated in preoperativepatients is a sensitive screening toolfor OSA Four questions address snor-ing tiredness during daytime observedapnea and high blood pressure whereasfour other measures focus on increasedOSA risk factors of BMI (greater than 35kgm2) age (older than 50 years) neckcircumference (greater than 40 cm[1575 in]) and gender (male preva-lence)30 The International RestlessLegs Syndrome Study Group Rating Scale(IRLS) is a validated assessment of dis-ease severity for patients with restlesslegs syndrome31 The patientrsquos perceived
level of insomnia may be assessed withthe Insomnia Severity Index (ISI) avalidated 7-item questionnaire32
A sleep diary (Figure 2-9)33 allows apatient to chart daily sleep and waketimes and should be maintained for atleast 2 consecutive weeks Review ofthis information allows the clinicianto estimate the total amount of sleepthe patient obtains in a 24-hour pe-riod The sleep diary also can provideinsight into the patientrsquos sleep patternIs sleep obtained at the same timesevery day Is the patientrsquos sleep con-solidated or fragmented across 24hours Does the patient sleep and
FIGURE 2-9 Sleep diary completed by a 46-year-old woman who presented with difficulty falling asleep Vertical linesrepresent when the patient went to bed lsquolsquoMrsquorsquo refers to when medication was taken black shading representstime asleep and unshaded white areas are time spent awake
Diary template reprinted from YOURSLEEPaasmnetorg from the American Academy of Sleep Medicine yoursleepaasmnetorgpdfsleepdiarypdf33
41Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
wake at conventional times or doeshe or she appear to be a lsquolsquonight owlrsquorsquoor lsquolsquomorning larkrsquorsquo Answers to thesequestions as provided by the sleepdiary may reveal factors that contrib-ute to sleep-related concerns Use ofsleep diaries can be particularly help-ful in patients with suspected circadianrhythm sleep disorders (including shiftwork) behaviorally induced insufficientsleep or inadequate sleep hygiene
OBJECTIVE MEASURESNocturnal polysomnography (NPSG)or related assessments are indicatedfor the diagnosis and assessment ofSDB and for positive airway titrationin patients with confirmed SDB Theprocedure can also provide informationabout EEG activity nocturnal move-ments cardiac rhythm and oxygen
saturation34 The recommended record-ing montage used in NPSG as shownin Figure 2-10 includes central (C3-A2C4-A1) frontal (F3-A2 F4-A1) andoccipital (O1-A2 O2-A1) EEGs left andright eye electrooculograms mentalsubmental surface EMG and ECG leadsOther recorded parameters includethoracic and abdominal effort oxygensaturation nasaloral airflow and bodyposition Use of a microphone torecord snoring is recommended butnot required34 A full 16-lead EEG(Figure 2-11)35 and video recordingmay be performed when nocturnalseizures are suspected Leg surfaceEMG leads are recommended andadditional arm EMG leads may beapplied when the clinical history sug-gests complex sleep-related motor be-haviors such as dream enactment In
KEY POINT
h A daily sleep diary helpsto summarize a patientrsquossleep-wake schedulemore accurately thanmemory often allowsand can facilitateconstruction ofpersonalized plansfor management ofcircadian rhythm sleepdisorders and insomnia
FIGURE 2-10 A 1-minute epoch from a nocturnal polysomnogram showing obstructive sleepapnea in a 46-year-old man who presented with snoring daytime sleepinessand headaches It depicts the standard recording montage that includes the
following leads central (C3-M2 C4-M1) frontal (F3-M2 F4-M1) and occipital (O1-M2 O2-M1)EEGs left and right eye electrooculograms (E1-M2 E2-M1) mentalsubmental electromyogram(Chin1-Chin2) electrocardiogram (ECG1-ECG2 ECG2-ECG3) snore volume (SNORE) nasalpressure transducer (NPRE) nasaloral airflow (NO) thoracic (THOR) and abdominal (ABD)effort arterial oxyhemoglobin saturation (SpO2) plethysmography (Pleth) and left and right eyeelectromyograms (LAT1-LAT2 RAT1-RAT2)
42 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
most cases the diagnostic NPSG is doneon 1 night although NPSG on 2 con-secutive nights may be considered inthe evaluation of parasomnias
Four categories of sleep monitoringdevices for use in the diagnosis of sleepdisorders have often been described34
These are type 1 standard attended in-laboratory polysomnography type 2comprehensive portable unattendedpolysomnography type 3 modifiedportable sleep apnea testing (often car-diorespiratory studies that do not recordsleep) and type 4 continuous single ordual bioparameter recording (eg pulseoximetry) However this categorizationmay not effectively classify the plethoraof out-of-center testing devices currentlyavailable for clinical use Therefore anew device classification system hasrecently been proposed This schemaknown as the SCOPER system catego-rizes out-of-center testing devices basedon measurement of sleep cardiovascu-
lar oximetry position effort and res-piratory parameters36 Within each ofthe six SCOPER categories a level of 0through 5 is assigned as indicated bythe type of sensor or measurementthat the device uses for that category
The most recent clinical guidelinespublished by the Portable MonitoringTask Force of the AASM37 for use ofunattended portable monitoring inthe diagnosis of OSA in adult patientsrecommend that portable monitoringonly be performed in conjunction witha comprehensive sleep evaluation by(or supervised by) a practitioner board-certified in sleep medicine or eligiblefor the certification examination Theseguidelines state that portable monitor-ing may be used in place of NPSG inpatients with a high pretest probabilityof moderate to severe OSA Portablemonitoring should not be used inpatients with significant medical comor-bidities (including but not limited to
KEY POINT
h The complexclassification of portabletesting devices reflectsthe multitude of designsavailable to cliniciansand will undoubtedlychange as technologyadvances
FIGURE 2-11 A The international 10Y20 system for EEG electrode placement refers to the10 and 20 interelectrode distances Even electrode numbers (2 4 6 8)represent the right hemisphere and odd electrode numbers (1 3 5 7)
represent the left hemisphere B Recommended F4-M1 C4-M1 O2-M1 placements of EEGelectrodes as set forth by the American Academy of Sleep Medicine (AASM)
Adapted from Iber C et al American Academy of SleepMedicine35 Used with permission of the American Academy ofSleep Medicine Darien IL 2012
43Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
moderate to severe pulmonary diseaseneuromuscular disease or congestiveheart failure) in patients with othersleep disorders (including central sleepapnea periodic limb movement disor-der insomnia parasomnias circadianrhythm disorders or narcolepsy) or asa screening tool The use of portablemonitoring may be indicated for thediagnosis of OSA in patients for whomattended NPSG is not possible becauseof immobility safety or critical illnessPortable monitoring may be indi-cated to monitor the response to non-continuous positive airway pressuretreatments for OSA including oralappliances upper airway surgery andweight loss The algorithm shown inAppendix B may help in the determi-nation of an adult patientrsquos candidacyfor out-of-center testing for the diag-nosis of OSA An example of portable(or home) monitoring technology isshown in Supplemental Digital Con-tent 2-1 linkslwwcomCONTA15
Recommended technology for port-able monitoring should record at mini-mum airflow respiratory effort andblood oxygenation the airflow effortand oximetric biosensors typically usedfor attended NPSG should be used37
These guidelines published in 2007will likely continue to evolve as newtechnologies emerge and are found tobe effective The current guidelinesrecommend that out-of-center testingbe performed under the auspices of anAASM-accredited comprehensive sleepmedicine program and that a board-certifiedeligible sleep specialist reviewthe raw data from a portable monitor-ing device All patients who undergoportablemonitoring for the diagnosis ofOSA should have a follow-up visit toreview test results Negative or techni-cally inadequate portable monitoringstudies should be followed by attendedin-laboratory NPSG if the clinical suspi-cion for SDB remains high37
The aforementioned testing proce-dures are primarily used in the evalua-tion of SDB Other testing modalitiesare useful in the diagnosis of othercategories of sleep disorders The mul-tiple sleep latency test (MSLT) and itsvariant the maintenance of wakefulnesstest (MWT) are used in the evaluation ofhypersomnia The conventional record-ing montage is similar to that used fornocturnal polysomnography central fron-tal and occipital EEGs left and right eyeelectrooculograms mentalsubmentalEMG and ECG leads Measurement ofthoracic and abdominal effort oxygensaturation and nasaloral airflow are notrequired but may help explain delayedsleep latencies for patients in whomrespiratory disturbances interfere withsleep onset
The MSLT is a validated tool that isconsidered the de facto standard forobjective assessment of excessive day-time sleepiness38 The recommendedprotocol38 involves five 20-minute napopportunities held at 2-hour intervalsthroughout the day If sleep is ob-served the patient is allowed to sleepfor at least 15 minutes The sleep la-tency for each nap is measured as thetime from the start of the nap trial tothe first epoch of sleep A sleep la-tency of 20 minutes is assigned to naptrials during which no sleep isobserved39 The mean sleep latencycalculated as the average sleep latencyacross all nap trials is the final resultThe presence and number of sleep-onset REM periods (SOREMPs) is alsodetermined as this information canhelp to establish a diagnosis of narco-lepsy without cataplexy or to confirmnarcolepsy with cataplexy
The MSLT should be started 15 to30 hours following completion of anocturnal polysomnogram whichshould record at least 6 hours of sleepin order for determination of the meansleep latency to be valid Drugs that may
KEY POINT
h Careful considerationshould be given tothe indications forout-of-center testingAttended nocturnalpolysomnography isindicated if a portablestudy yields a negativeor technicallyinadequate result
44 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
interfere with sleep latency or REM la-tency should be discontinued 2 weeksbefore testing whenever possible Ascreen may be performed on the day oftesting if there is suspicion that pre-scribed or illicit substances may con-tribute to the patientrsquos sleepiness38
No large multicenter systematicallycollected normative data are availablefor mean sleep latency values on theMSLT38 Nonetheless a mean sleep la-tency of greater than 10 minutes is of-ten considered normal whereas a meansleep latency of 8 to 10 minutes is con-sidered a physiologic gray zone40 Thenormative data for children are classi-fied by Tanner stage of developmentthough the MSLT is typically not per-formed in children aged younger than 6or 7 years because some daytime nap-ping may still be normal in youngchildren41 The second edition of theInternational Classification of SleepDisorders Diagnostic and CodingManual (ICSD-2)42 requires the pres-ence of a mean sleep latency of lessthan 8 minutes and two or moreSOREMPs as part of the diagnosticcriteria for narcolepsy without cata-plexy However the ICSD-2 also notesthat a mean sleep latency of less than 8minutes may occur in up to 30 of thegeneral population Therefore whilethe MSLT is a helpful and widely usedtool it remains an imperfect gold stand-ard in the assessment of daytime sleepi-ness This necessitates that theevaluation of daytime sleepiness notrest on the MSLT results alone butassimilate the clinical history subjectivecomplaints diagnostic study results andother pertinent medical information38
Practice parameters from theAASM state that the MSLT is indicatedfor diagnostic confirmation of sus-pected narcolepsy and may be indi-cated to differentiate idiopathichypersomnia from narcolepsy38 TheMSLT is not indicated for routine
assessment of OSA syndrome or toassess response to treatment of SDBand is not routinely indicated for eval-uation of sleepiness in medical orneurologic disorders (except for narco-lepsy) insomnia or circadian rhythmdisorders
TheMWTprovides an objectivemeas-ure of a patientrsquos ability to remain awakerather than the tendency to fall asleepduring the day The key differencebetween the MWT and the MSLT is thatin the former the patient is asked to tryto stay awake under circumstances con-ducive to sleep rather than to fall asleepThe MWT provides an objective vali-dated assessment of the ability to remainawake for a defined length of time38 Therecommended protocol includes four40-minute trials that begin at 2-hourintervals with the first trial to start 15 to30 hours after the patientrsquos wake-uptime A nocturnal polysomnogram onthe preceding night is not requiredHowever the patient should obtain asufficient amount of sleep during thenight before the MWT Each trial isterminated after 40 minutes if no sleepoccurs or after unequivocal sleep onset(defined as three continuous epochsof stage N1 sleep or one epoch of anyother stage of sleep) has occurred38
One indication for the MWT is to as-sess an individualrsquos ability to remainawake when his or her inability to re-main awake constitutes a public orpersonal safety issue This can becomea pressing issue for individuals em-ployed in the transportation43 con-struction or health care industriesThe MWT may be indicated to assesstreatment response in patients withknown excessive daytime sleepiness
Limited amounts of normative dataare available for the MWT Historicallymultiple testing protocols make syn-thesis of results more challenging TheMWT is used much less often in clinicalpractice compared to the MSLT Patient
KEY POINTS
h The multiple sleeplatency test is the goldstandard for objectiveassessment of daytimesleepiness butinterpretation of theresults must be madewithin the clinicalcontext of the patientrsquoshistory
h In the multiple sleeplatency test the patientis instructed to try tosleep during each naptrial In the maintenanceof wakefulness test thepatient is instructed totry to remain awakeduring the nap trial
h A baseline nocturnalpolysomnogram isrequired before amultiple sleep latencytest and considered butnot required before amaintenance ofwakefulness test
45Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
age may also affect the mean sleep la-tency values on both the MWT and theMSLT43 and may represent evolution ofcircadian rhythm and sleep architec-ture across the lifetime A study of 383patients with narcolepsy with cataplexyexamined the clinical and polysomno-graphic data at the time of diagnosis(age range 5 to 84 years) and found aprogressive decrease in the number ofSOREMPs and a progressive increase inthe mean sleep latency on the MSLT asa function of age44 Given its limita-tions the MWT may thus be used tosupplement the clinical history in theassessment of ability to stay awake butshould not be the sole determinant ofthis parameter
Actigraphy is also used in the clinicalevaluation of patients with sleep disor-ders particularly circadian rhythm sleepdisorders An actigraph is a watchlikedevice that is worn on the wrist for anextended period usually in the range ofweeks The actigraph records move-ment and uses an algorithm to estimatethe amounts of sleep and wake timeduring the recording period Analysissoftware uses movement to estimatewhen sleep and wakefulness haveoccurred Review of the data can pro-vide objective insight into the patientrsquossleep pattern including timing andduration of major sleep disruptionsActigraphy is indicated as part of theevaluation of patients with advancedsleep-phase syndrome delayed sleep-phase syndrome and shift work disor-der and may be indicated in the evalua-tion of jet lag disorder and nonY24-hoursleep-wake syndrome including thatassociated with blindness45 It can alsoserve as a measure of treatment re-sponse in patients with insomnia andcircadian rhythm sleep disorders Forpopulations in which traditional sleepmonitoring may be challenging suchas pediatric or older adult patientsactigraphy may provide valuable infor-
mation about the patientrsquos sleep pat-tern or response to treatment Whenpolysomnography is not availableactigraphy is indicated to estimate totalsleep time in patients with OSA45
OTHER ASSESSMENTMODALITIESLaboratory evaluation and neuroimag-ing with either CT or MRI may beconsidered on an individual basis asindicated by the clinical history Com-plete blood count (CBC) serum chem-istries or measures of thyroid functionmay be obtained if an underlying med-ical disorder is thought to contribute tothe patientrsquos sleep symptoms Forinstance these laboratory studies maybe consideredwhen daytime fatigue is apredominant symptom Serum ironstudies including ferritin level shouldbe checked in patients with restless legssyndrome46 Neuroimaging should beconsidered in patients with antecedenttrauma or for any sleep disorder pa-tient with an abnormal neurologic ex-amination to evaluate for a structuraletiology of the patientrsquos symptoms
APPROACH TO THE PATIENTEvaluation of suspected sleep disordersis best accomplished by a stepwisemultidimensional approach (Case 2-2)A thorough sleep history includes de-tailed description of sleep-related symp-toms nocturnal behaviors the patientrsquossleep schedule level of daytime sleepi-ness and subsequent effects on daytimefunctioning Collateral history from thepatientrsquos bed partner or family is oftennecessary to understand the severity andcontext of the patientrsquos symptoms Sub-jective assessments of sleepiness suchas the Epworth Sleepiness Scale areeasily administered and useful to tracksymptomatic progression or treatmentresponse from one visit to the nextCertain physical examination findingsmay also raise clinical suspicion of
KEY POINTS
h Actigraphy can beuseful in evaluation andtreatment of circadianrhythm sleep disordersand in management ofinsomnia
h Neuroimaging is notroutinely indicated inthe clinical evaluation ofsleep disorders andshould be pursued on acase-by-case basis
46 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
particular sleep disorders For patientsin whom multiple sleep disorders aresuspected systematic use of diagnostictesting allows for accurate identificationof specific diagnoses In a patient withinsomnia and symptoms suggestive ofSDB nocturnal polysomnography shouldbe the first procedure performed Ifthe insomnia persists despite adequatetreatment of SDB further evaluationwith sleep diaries and possibly actigra-
phy may be considered to better char-acterize the patientrsquos sleep patternActigraphy may then again be pursuedto gauge treatment response upon man-agement of the patientrsquos insomnia
The diagnostic modalities availablefor evaluation of sleep disorders arerapidly evolving In-laboratory nocturnalpolysomnography currently remains thegold standard for assessment of SDBHowever the multitude of out-of-center
KEY POINT
h Careful assimilation ofthe clinical history thesleep-specific physicalexamination patientquestionnaires anddiagnostic test resultsleads to the mostaccurate assessment ofpatients with symptomsrelated to sleep oralertness
Case 2-2A 23-year-old woman reported a 4-year history of insomnia Throughoutcollege she was a lsquolsquonight owlrsquorsquo never scheduled classes that started before100 PM and always did well in school During the past 6 months shedeveloped progressive difficulty staying awake in her job as a financialanalyst andwas concerned about how this might affect her job performance
During the week she was in bed by midnight but was unable to fallasleep until 200 AM and awoke with difficulty to an alarm at 600 AMfeeling tired She denied any thought rumination or physical discomfortat bedtime She had tried over-the-counter sleep aids that provided nosymptomatic improvement and worsened morning grogginess Onweekends she slept from 200 AM to 1100 AM and awakened feelinglsquolsquopretty goodrsquorsquo She had nocturia up to once per night and occasionalmorning headaches She had no bed partner but reported gaspingrespirations nocturnal palpitations and snort arousals On about 4 nightsper week she experienced a sensation of needing to move her legswhile trying to fall asleep This sensation was relieved by movement andwas worse at night than during the day Her legs sometimes movedspontaneously at night or while seated quietly for long periods duringthe day She felt sleepy during the afternoon especially while workingat her computer She denied drowsiness while driving She occasionallytook a 30-minute nap on the weekend and found it to be refreshingShe drank one to two cups of coffee every morning and had a 12-oz dietcaffeinated soda at 300 PM Her sleepiness had not caused her to makeany mistakes at work and she denied any mood disturbance
Physical examination was notable for a body mass index of 32 kgm2 neckcircumference of 381 cm (15 in) and modified Mallampati class III oral airwayNasal passages were narrow with turbinate hypertrophy bilaterally andhard palate was high-arched and narrow Nomicrognathia or retrognathia waspresent She had molar occlusion class I bilaterally with no overjet or overbiteThe general cardiac respiratory and neurologic examinations were normal
Comment This case illustrates how discussion of the chief complaint raisessuspicion for multiple sleep disorders The history suggests a circadian rhythmsleep disorder particularly delayed sleep-phase syndrome sleep-disorderedbreathing and restless legs syndrome Diagnostic evaluation should includenocturnal polysomnogramwith consideration toperform testing at the patientrsquospreferred sleep time and serum iron studies Sleep diaries andor actigraphymay be considered for further assessment of the patientrsquos sleep pattern
47Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
testing devices continues to grow andmany may provide useful alternativesthat under appropriate circumstancescould allow more expedient conven-ient and less costly evaluations ofincreased numbers of patients whopreviously had only limited or delayedaccess to sleep services
VIDEO LEGENDSupplemental Digital Content 2-1
Home sleep study Video demonstrates a homesleep study using an unattended type 3 portablemonitoring device The patient is a 56-year-oldman who is experiencing morning headachesand concentration and alertness problems atwork He has a history of mild snoring and ar-terial hypertension His Epworth SleepinessScale score is 18 his neck circumference is19 in he has a Mallampati classification score ofIII and his body mass index is 41 kgm Theapnea-hypopnea index is 84 eventsh Channelsrecorded in this sleep study include arterialoxyhemoglobin saturation heart rate oral-nasalpressure flow snoring inductive plethysmog-raphy for chest efforts and body position
linkslwwcomCONTA15
B 2013 Marcel Hungs MD PhD Used withpermission
REFERENCES1 National Institutes of Health National
Center on Sleep Disorders ResearchSleep disorders research planwwwnhlbinihgovhealthprofsleep201101011NationalSleepDisordersResearch-PlanDHHSPublication11-7820pdf PublishedNovember 2011
2 Dinges DF An overview of sleepiness andaccidents J Sleep Res 19954(S2)4Y14
3 Mills RJ Young CA A medical definitionof fatigue in multiple sclerosis QJM 2008101(1)49Y60
4 Chervin RD Sleepiness fatigue tirednessand lack of energy in obstructive sleepapnea Chest 2000118(2)372Y379
5 Chotinaiwattarakul W OrsquoBrien LM Fan LChervin RD Fatigue tiredness and lack ofenergy improve with treatment for OSAJ Clin Sleep Med 20095(3)222Y227
6 American Academy of Sleep MedicineThe international classification of sleepdisorders diagnostic and coding manual2nd ed Westchester IL American Academyof Sleep Medicine 2005
7 Ebben MR Spielman AJNon-pharmacological treatments forinsomnia J Behav Med 200932(3)244Y254
8 Roth T Insomnia definition prevalenceetiology and consequences J Clin SleepMed 20073(5 suppl)S7YS10
9 Yang CM Spielman AJ Glovinsky PNonpharmacologic strategies in themanagement of insomnia Psychiatr ClinNorth Am 200629(4)895Y919 abstract viii
10 Katz ES DrsquoAmbrosio CM Pediatricobstructive sleep apnea syndrome ClinChest Med 201031(2)221Y234
11 Kohler M Bloch KE Stradling JR The role ofthe nose in the pathogenesis of obstructivesleep apnea Curr Opin Otolaryngol HeadNeck Surg 200917(1)33Y37
12 Kryger MH Atlas of clinical sleep medicinePhiladelphia PA Elsevier 2010
13 Zonato AI Martinho FL Bittencourt LRet al Head and neck physical examinationcomparison between nonapneic andobstructive sleep apnea patientsLaryngoscope 2005115(6)1030Y1034
14 Mallampati SR Gatt SP Gugino LD et alA clinical sign to predict difficult trachealintubation a prospective study Can AnaesthSoc J 198532(4)429Y434
15 Samsoon GL Young JR Difficult trachealintubation a retrospective studyAnaesthesia 198742(5)487Y490
16 Huang HH Lee MS Shih YL et alModified Mallampati classificationas a clinical predictor of peroralesophagogastroduodenoscopy toleranceBMC Gastroenterol 20111112
17 Friedman M Ibrahim H Bass L Clinicalstaging for sleep-disordered breathingOtolaryngol Head Neck Surg 2002127(1)13Y21
18 Cheng RHW Yiu CKY Leung WKOral health in individuals with Downsyndrome In Dey S ed Prenatal diagnosisand screening for down syndromeInTech wwwintechopencombookshowtoreferenceprenatal-diagnosis-and-screening-for-down-syndromeoral-health-in-individuals-with-down-syndromePublished 2011 Accessed August 24 2012
19 Katz I Stradling J Slutsky AS et al Dopatients with obstructive sleep apneahave thick necks Am Rev Respir Dis1990141(5 pt 1)1228Y1231
20 Kushida CA Efron B Guilleminault C Apredictive morphometric model for theobstructive sleep apnea syndrome AnnIntern Med 1997127(8 pt 1)581Y587
48 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
21 Saccucci M Tettamanti L Mummolo S et alScoliosis and dental occlusion a review ofthe literature Scoliosis 2011615
22 Battagel JM Kotecha B Dental side-effectsof mandibular advancement splint wear inpatients who snore Clin Otolaryngol200530(2)149Y156
23 Morcos SS Patel PK The vocabulary ofdentofacial deformities Clin Plast Surg200734(3)589Y599
24 Epstein LJ Kristo D Strollo PJ Jr et alClinical guideline for the evaluationmanagement and long-term care ofobstructive sleep apnea in adults J ClinSleep Med 20095(3)263Y276
25 Johns MW A new method for measuringdaytime sleepiness the Epworth sleepinessscale Sleep 199114(6)540Y545
26 Johns MW Daytime sleepiness snoring andobstructive sleep apnea The EpworthSleepiness Scale Chest 1993103(1)30Y36
27 Chervin RD Aldrich MS The EpworthSleepiness Scale may not reflect objectivemeasures of sleepiness or sleep apneaNeurology 199952(1)125Y131
28 Buysse DJ Reynolds CF 3rd Monk THet al The Pittsburgh Sleep Quality Index anew instrument for psychiatric practice andresearch Psychiatry Res 198928(2)193Y213
29 Chervin RD Hedger K Dillon JE Pituch KJPediatric sleep questionnaire (PSQ) validityand reliability of scales for sleep-disorderedbreathing snoring sleepiness and behavioralproblems Sleep Med 20001(1)21Y32
30 Chung F Yegneswaran B Liao P et al STOPquestionnaire a tool to screen patients forobstructive sleep apnea Anesthesiology2008108(5)812Y821
31 Walters AS LeBrocq C Dhar A et alValidation of the International Restless LegsSyndrome Study Group rating scale forrestless legs syndrome Sleep Med 20034(2)121Y132
32 Bastien CH Vallieres A Morin CMValidation of the Insomnia Severity Indexas an outcome measure for insomniaresearch Sleep Med 20012(4)297Y307
33 YOURSLEEPaasmnetorg from the AmericanAcademy of Sleep Medicine Two weeksleep diary yoursleepaasmnetorgpdfsleepdiarypdf Accessed August 24 2012
34 Kushida CA Littner MR Morgenthaler Tet al Practice parameters for the indicationsfor polysomnography and relatedprocedures an update for 2005 Sleep200528(4)499Y521
35 Iber C Ancoli-Israel S Chesson A et alThe AASM manual for scoring of sleep andassociated events rules terminology andtechnical specifications 1st ed WestchesterIL American Academy of Sleep Medicine2007
36 Collop NA Tracy SL Kapur V et alObstructive sleep apnea devices forout-of-center (OOC) testing technologyevaluation J Clin Sleep Med 20117(5)531Y548
37 Collop NA Anderson WM Boehlecke Bet al Clinical guidelines for the use ofunattended portable monitors in thediagnosis of obstructive sleep apnea in adultpatients Portable Monitoring Task Forceof the American Academy of SleepMedicine J Clin Sleep Med 20073(7)737Y747
38 Littner MR Kushida C Wise M et alStandards of Practice Committee of theAmerican Academy of Sleep MedicinePractice parameters for clinical use of themultiple sleep latency test and themaintenance of wakefulness test Sleep200528(1)113Y121
39 Carskadon MA Dement WC Mitler MMet al Guidelines for the multiple sleeplatency test (MSLT) a standard measure ofsleepiness Sleep 19869(4)519Y524
40 van den Hoed J Kraemer H Guilleminault Cet al Disorders of excessive daytimesomnolence polygraphic and clinical datafor 100 patients Sleep 19814(1)23Y37
41 Hoban TF Chervin RD Assessment ofsleepiness in children Semin PediatrNeurol 20018(4)216Y228
42 ICSD-2 The international classification ofsleep disorders pocket version diagnosticand coding manual 2nd ed WestchesterIL American Academy of Sleep Medicine2005
43 Arand D Bonnet M Hurwitz T et alThe clinical use of the MSLT and MWTSleep 200528(1)123Y144
44 Dauvilliers Y Gosselin A Paquet J et alEffect of age on MSLT results in patientswith narcolepsy-cataplexy Neurology200462(1)46Y50
45 Morgenthaler T Alessi C Friedman Let al Practice parameters for the use ofactigraphy in the assessment of sleep andsleep disorders an update for 2007 Sleep200730(4)519Y529
46 Gamaldo CE Earley CJ Restless legssyndrome a clinical update Chest2006130(5)1596Y1604
49Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited

report fatigue tiredness or lack ofenergy at times even when they denysleepiness4 Interestingly these symp-toms (like sleepiness) appear toimprove with treatment of the under-lying OSA5 A clear understanding ofwhether the patient experiences anoverwhelming urge to sleep duringthe day may help the clinician decidewhich diagnostic studies to pursue andalso guides discussion about potentialdiagnoses that may contribute to thepatientrsquos symptoms Special attentionshould be paid to situations in whichthe patientrsquos sleepiness becomes evi-dent Does the patient doze during con-versation while at work or while drivingIs the patientrsquos concentration or memoryimpaired because of sleepiness Dozingwhile operating heavy machinery or amotor vehicle can lead to devastatingoutcomes and this has both individualand public health implications Daytimesleepiness that impairs a patientrsquos func-tional capabilities can threaten job se-curity and have a negative impact oninterpersonal relationships The con-text of a patientrsquos daytime sleepinesshighlights its severity and impact
The symptom of insomnia is de-fined as difficulty with sleep initiationor maintenance waking too early orsleep that is nonrestorative despiteample opportunity to sleep6 Disordersthat cause insomnia have diagnosticcriteria to specify that the insomniasymptoms should be accompanied byat least one manifestation of daytimeimpairment (such as fatigue mood dis-turbance headaches or gastrointestinalsymptoms in response to sleep loss) orimpaired memory concentration orperformance The point prevalence ofinsomnia is estimated at 6 to 15 inthe general population but is clearlyhigher among certain subgroups suchas patients with psychiatric disease7
Population-based studies done withvaried adult samples from multiple
countries indicate that approximately30 of the general adult populationreports one or more insomnia symp-tom8 Because insomnia is so commonneurologists routinely encounter pa-tients with the symptom As the etiol-ogy of insomnia is often multifactorialthe evaluation can be complex andrequires a detailed history that exploresmany potential contributors
A helpful framework in which to con-sider a patientrsquos insomnia is known asthe lsquolsquo3Prsquorsquo model9 which aids identifica-tion of possible causes of insomnia andhighlights potential targets for treat-ment This model calls for temporalclassification of factors that affect a pa-tientrsquos insomnia characteristics thatpredispose a person to develop in-somnia events that precipitate the in-somnia acutely and behaviors andattitudes that perpetuate insomnia andmay cause it to become chronic Com-mon predisposing factors include per-sonality traits such as excessive worryingor cognitive hyperarousal or the degreeto which a personrsquos preferred sleepingtimes differ from social norms9 Precip-itating factors are often readily identi-fied as major life transitions such aschange in marital status death in thefamily or change in employment How-ever subtler challenges to a personrsquosroutine or environment may also pre-cipitate the onset of insomnia In somesituations the patientrsquos sleep normal-izes upon resolution of the precipitantin other cases behaviors and mindsetsaccrued during the acute phase of theinsomnia can perpetuate the patientrsquossleep disturbance Such perpetuatingfactors can include perceived associa-tions between the sleeping environ-ment and inability to sleep or escalateduse of caffeine throughout the dayOther important details include specif-ics about the patientrsquos insomnia at thepresent time including the latency tosleep timing duration and causes of
KEY POINTS
h Information from thepatient medical recordand any available bedpartner friend orfamily member canclarify the extent andconsequences of thepatientrsquos sleep-relatedsymptoms
h The 3P framework ofinsomnia comprisespredisposingprecipitating andperpetuating factorsDiscussion of all factorsfacilitates identificationof potential treatmenttargets
34 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
nocturnal awakenings behaviors dur-ing nocturnal awakenings and latencyto fall back asleep after each awakeningA useful approach is to ask the patientfor a detailed start-to-finish descriptionof the entire typical sleep period anddaytime period Any medications pre-viously or currently used to facilitatesleep should also be identified
The sleep history should screenfor potentially relevant sleep disordersthat may cause excessive daytime sleep-iness or insomnia (Case 2-1) Thepresence of symptoms such as snor-ing witnessed apneas and morningheadaches raises the suspicion forsleep-disordered breathing (SDB) Leg
discomfort associated with an urge tomove that worsens at night andimproves with leg movement indicatesrestless legs syndrome and may con-tribute to the patientrsquos poor sleepquality and impair daytime functioningSleep paralysis and hypnagogic orhypnopompic hallucinations are notspecific to a particular sleep disorderwhile a history of cataplexy is patho-gnomonic for narcolepsy and must beexplored when a patient presents withreports of central hypersomnia ratherthan SDB When relevant the clinicianshould also ask about nocturnal behav-iors specifically ones that may pose riskof injury to the patient or bed partner
Case 2-1A 44-year-old man with a long-standing history of loud frequent snoringpresented because of his wifersquos concerns related to his snoring His wifehad witnessed him to have occasional pauses in his breathing during sleepand at times he awakened to his snoring He reported frequent acidreflux and morning headaches Approximately once per month he wouldawaken lsquolsquofeeling like my heart is racing and I need to catch my breathrsquorsquoHe had occasional nasal congestion but always awakened with a drymouth and sore throat He denied any leg discomfort but his wife hadtold him that he tossed and turned frequently during sleep
His sleep schedule was the same every night he was in bed by 1000 PMfell asleep immediately without the use of any sleep aids and awakenedat 600 AM feeling tired He had up to four nocturnal awakenings pernight two were attributed to nocturia and the rest were of unknownetiology Each awakening lasted a few minutes and he fell asleep againeasily He had had a few episodes of sleepwalking as a child but none sincethe age of 8 years
He felt sleepy during the day with a propensity to doze unintentionallywhile reading or watching television He denied drowsiness while driving butlimited his driving to his 20-minute commute to and from work his wifedrove for longer distances and hewould often sleep in the passenger seat Hissleepiness was worse in the midafternoon and if given the opportunity hewould nap for 1 hour on the weekends He found naps to be somewhatrefreshing He drank two to three cups of coffee every morning and had a12-oz caffeinated sodawith lunch His sleepiness had not caused him tomakeany mistakes in his job as a physical therapist although he felt that he hadpotential for further improvement in his job performance He also reportedfeeling more irritable in recent months but this had not caused anydifficulties at home or work
Comment This case illustrates the multiple components of a concisebut still detailed sleep history The patientrsquos daytime symptoms provideinsight about the effects of the patientrsquos untreated sleep disorder
35Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
such as sleepwalking driving or cook-ing while asleep or dream-enactmentbehavior If the patient reports suchbehavior further inquiry must be madeabout the frequency of these events andany history of injury sustained due to thesleep-related behavior Details of thesleep history permit a thorough differ-ential diagnosis and can also guide adiscussion of safety concerns
PHYSICAL EXAMINATIONA comprehensive multisystem exami-nation is an important aspect of thesleep evaluation Measurement of theweight height body mass index (BMI)neck circumference and blood pres-sure and heart rate should be per-formed for nearly all patients withsymptoms related to sleep or alertnessOther salient features of the generalexamination include auscultation forany cardiac or respiratory abnormalitiesand identification of peripheral edemaA focused neurologic examinationshould be guided by the patientrsquos his-tory For instance a mental status as-sessment should be considered if apatient with excessive daytime sleepi-ness also complains of memory loss If apatient with a history of diabetes melli-
tus endorses symptoms of restless legssyndrome it is worthwhile to assess forstocking-glove distribution sensory lossand weakness
Detailed examination of the headand neck should be performed as partof a comprehensive sleep evaluationThe patientrsquos facial morphology shouldbe assessed for features of long facesyndrome which includes infraorbitaldarkening mouth breathing elongatedmidface and nasal atrophy10 A 2009review11 reports that previous observa-tional and cross-sectional studies haveshown a relationship between chronicnasal obstruction and OSA Thus a thor-ough nasal examination should be per-formed on patients with sleep-relatedcomplaints Examination of the nasalairway should include evaluation forsymmetry of the nares nasal septum de-viation (Figure 2-1)12 and nasal turbi-nate hypertrophy A bedside assessmentof nasal airflow can be accomplished by
KEY POINT
h Details of facialmorphology nasalairway patency and oralairway crowding arekey features of thesleep-specificexamination
FIGURE 2-1 Nasal septal deviation Thisstructural abnormality canpredispose a patient to havesleep-disordered breathing
Reprinted from Kryger MH Elsevier12 B 2010 withpermission from Elsevier
FIGURE 2-2 Retrognathia Retrognathiais derived from the termslsquolsquoretrorsquorsquo (backward) and
lsquolsquognathosrsquorsquo (jaw) With retrognathia one orboth jaws recede with respect to the frontalplane of the forehead The condition maypredispose a patient to obstruction of theairway and sleep apnea by displacing thetongue against the retropharyngeal regioncompromising airflow Retrognathia issometimes corrected through surgicalrepositioning or advancement of themandible
Reprinted from Kryger MH Elsevier12 B 2010 withpermission from Elsevier
36 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
asking the patient to press the indexfinger against the left nostril and take adeep breath in on the right side thisshould be repeated on the oppositeside as well The patientrsquos facial mor-phology should be assessed for man-dibular retrognathia (Figure 2-2)12 Withthe patientrsquos head in a neutral posi-tion a virtual line is drawn from thevermillion border of the lower lip tothe chin Mandibular retrognathia issuggested if the anterior prominence ofthe chin is 2 mm or more behind thevirtual line13
The modified Mallampati classifica-tion is commonly used for assessmentof the oral airway in patients withsuspected SDB The Mallampati classi-fication14 was developed to identifypatients in whom tracheal intubationwould be difficult the initial description
divided patients into three classes Twoyears later15 this was modified to de-scribe four groups class I class II classIII and class IV Figure 2-3 16 illustratesthe modified Mallampati classificationassessed with the tongue protrudedThe Friedman palate position classifi-cation17 also commonly referencedutilizes the same four categories but isdone with the tongue at rest and notextended Either the Mallampati orFriedman classification may be used todescribe the patency of the oral airway
Tonsils should be classified based onthe degree of hypertrophy (Figure 2-4)12grade I tonsils are inside the tonsillarfossa lateral to the posterior pillarsgrade II tonsils occupy 25 of theoropharynx grade III tonsils occupy50 of the oropharynx and grade IVtonsils occupy at least 75 of the
FIGURE 2-3 Modified Mallampati classification The class is determined by looking at theanatomy of the oral cavity and describes tongue size relative to oropharyngealsize The test is conducted with the patient seated the head held in a neutral
position and the mouth wide open and relaxed The subsequent classification is assigned basedupon the pharyngeal structures that are visible
Reprinted from Huang HH et al BMC Gastroenterol16 B 2011 BioMed Central Ltd wwwbiomedcentralcom1471-230X1112
37Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
oropharynx and nearly meet in the mid-line13 A high-arched narrow hard pal-ate (Figure 2-5)18 may predispose thepatient to have SDB Katz and col-leagues19 have shown that patients withOSA have significantly increased neckcircumference compared to nonapneicsnorers greater distribution of neck fat
may contribute to mass loading on theupper airway in patients with OSA Thepatientrsquos neck circumference should bemeasured at the superior border of thecricothyroid membrane19 A neck cir-cumference greater than 40 cm (157in) has been shown to be predictive ofOSA with 61 sensitivity and 93specificity regardless of sex20
Assessment of the patientrsquos anteriorand posterior dentition can also re-veal anatomic findings that may pre-dispose a person to certain sleepdisorders Two features to note in eval-uation of the anterior dentition areoverjet and overbite (Figure 2-6)21
Overjet as shown in Figure 2-712 isthe horizontal distance between theupper right central incisor and thebuccal surface of the correspondinglower tooth while overbite is the ver-tical distance between these twopoints22 These measurements are typ-ically reported in millimeters The An-gle classification system is used todescribe the first molar position on
FIGURE 2-4 Tonsil size grading Thisstructural abnormality canpredispose a patient to havesleep-disordered breathing
Reprinted from Kryger MH Elsevier12 B 2010 withpermission from Elsevier
FIGURE 2-5 Deficientmaxillarydevelopment inan individual with
Down syndrome leading to highand narrow hard palate
Reprinted with permission from ChengRHW et al InTech18 B 2011 W KeungLeung wwwintechopencombooksprenatal-diagnosis-and-screening-for-down-syndromeoral-health-in-individuals-with-down-syndrome
FIGURE 2-6 Overjet andoverbite Overjetis defined as
increased projection of the upperteeth in front of the lower teethas measured parallel to theocclusal plane Overbite is thevertical overlapping of maxillaryteeth over mandibular teethusually measured perpendicularto the occlusal plane
Reprinted from Saccucci M et al Scoliosis21
B 2011 BioMed Central Ltd wwwscoliosisjournalcomcontent6115
38 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
the mandibular and maxillary dentalarches23 Figure 2-8 shows class I oc-clusion and class II and III malocclu-
sion Of note the mesiobuccal surfaceis the aspect of the tooth that is adja-cent to the cheek mucosa
The Adult Obstructive Sleep ApneaTask Force of the American Academyof Sleep Medicine (AASM) recommen-ded in recent clinical guidelines24 thatthe following physical findings maysuggest the presence of OSA increasedneck circumference (greater than 432cm [17 in] in men greater than 406 cm[16 in] in women) BMI 30 kgm2 orgreater modified Mallampati classifica-tion of III or IV presence of retrognathialateral peritonsillar narrowing macro-glossia tonsillar hypertrophy elongatedenlarged uvula high-archednarrowhard palate nasal abnormalities (egpolyps deviation valve abnormalities
KEY POINT
h Classification of thepatientrsquos dentition helpsto evaluate the positionof the maxillary archrelative to themandibular arch
FIGURE 2-7 OverjetDisplacementof the
mandibular teeth posteriorly inrelationship to the maxillary teethresults inmoreposteriorly crowdedupper airways predisposingpatients for the developmentof obstructive sleep apnea
Reprinted from Kryger MH Elsevier12
B 2010 with permission from Elsevier
FIGURE 2-8 Angle class occlusionmalocclusion A Angle class I occlusion also known asneutrocclusion The mandibular and maxillary dental arches have a normalanterior-posterior relationship The mesiobuccal groove of the mandibular first
molar interdigitates with the mesiobuccal cusp of the maxillary first molar B Angle class IImalocclusion also known as distoclusion The mandibular dental arch is in distal anterior-posteriorrelationship to the maxillary dental arch The mesiobuccal groove of the mandibular first molar isdistal to the mesiobuccal cusp of the maxillary first molar C Angle class III malocclusion alsoknown as mesioclusion The mandibular dental arch is in mesial anterior-posterior relationship tothe maxillary dental arch The mesiobuccal groove of the mandibular first molar is mesial to themesiobuccal cusp of the maxillary first molar
Reprinted fromMorcos SS Patel PK Clin Plast Surg23 B 2007 with permission from Elsevier wwwsciencedirectcomsciencearticlepiiS0094129807000843
39Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
and turbinate hypertrophy) andoroverjet To prevent overlooking thesefindings a thorough head and neckassessment as described in Table 2-2should be incorporated into the phys-ical examination of all patients whopresent with sleep-related complaints
SUBJECTIVE ASSESSMENTSeveral patient-completed question-naires are inexpensive and time-efficient
reasonably well validated and com-monly used They can help to increasestandardization in evaluations of patientsby different clinicians or across centersPerhaps the most well-known andwidely used is the Epworth SleepinessScale25 a subjective assessment of thepatientrsquos daytime sleep propensity inrecent times As shown in Appendix Athe Epworth Sleepiness Scale asks theresponder to use a four-point Likertscale (0 1 2 or 3) to indicate thelikelihood of dozing in eight distinctsedentary conditions A total score of 10or greater out of a possible 24 suggestsexcessive daytime sleepiness25 Whilethe Epworth Sleepiness Scale score canbe easily incorporated into the clinicalevaluation it should not be used as asubstitute for objective measurement ofsleepiness The Epworth Sleepiness Scalescore may correlate to a limited extentwith the presence and severity of OSA26
but some studies have failed to find anystatistically significant association withmean sleep latency on multiple sleep la-tency tests or with severity of OSA27
The most advantageous use of theEpworth Sleepiness Scale may be to followan individualrsquos self-assessment of sleep-iness longitudinally and it may also serveas an indicator of treatment response
Many other questionnaires may beutilized in a clinical sleep evaluationsome pertain to overall sleep qualitywhile others are disorder-specific ThePatient Reported Outcomes Measure-ment Information System (PROMIS) isan NIH-supported system of measuresfor patient-reported health status andincludes questions on sleep disturb-ance The Pittsburgh Sleep QualityIndex (PSQI) is a validated question-naire that inquires about sleep qualityand disturbances over the previousmonth28 The parent-completed Pe-diatric Sleep Questionnaire29 containsa validated reliable 22-item scale tohelp assess risk for SDB in children
KEY POINTS
h The Epworth SleepinessScale apatient-completedquestionnaire assessesthe patientrsquos subjectivetendency to doze duringsedentary situations inrecent times not onlyat the moment thequestionnaire iscompleted
h The Epworth SleepinessScale should not beused in lieu of diagnostictesting but may be avaluable componentof ongoing clinicalevaluation
TABLE 2-2 Head and NeckExamination
b Face
Featuresof long face syndrome
Infraorbital darkening
Mouth breathing
Elongated midface
Nasal atrophy
b Oral Airway
Mandibular retrognathia
Low soft palate (modifiedMallampati classification)
Large or boggy uvula
Erythematous pillars
Tonsillar hypertrophy
High narrow hard palate
Neck circumference
Overjet
Overbite
Angle classification(malocclusion)
Macroglossia
Worn occlusive surfaces(suggestive of bruxism)
b Nasal Airway
Symmetry of the nares
Nasal septum deviation
Nasal airflow
Collapse of nasal alae oninspiration
b Neck
Neck circumference
40 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
The STOP-BANG questionnaire devel-oped and validated in preoperativepatients is a sensitive screening toolfor OSA Four questions address snor-ing tiredness during daytime observedapnea and high blood pressure whereasfour other measures focus on increasedOSA risk factors of BMI (greater than 35kgm2) age (older than 50 years) neckcircumference (greater than 40 cm[1575 in]) and gender (male preva-lence)30 The International RestlessLegs Syndrome Study Group Rating Scale(IRLS) is a validated assessment of dis-ease severity for patients with restlesslegs syndrome31 The patientrsquos perceived
level of insomnia may be assessed withthe Insomnia Severity Index (ISI) avalidated 7-item questionnaire32
A sleep diary (Figure 2-9)33 allows apatient to chart daily sleep and waketimes and should be maintained for atleast 2 consecutive weeks Review ofthis information allows the clinicianto estimate the total amount of sleepthe patient obtains in a 24-hour pe-riod The sleep diary also can provideinsight into the patientrsquos sleep patternIs sleep obtained at the same timesevery day Is the patientrsquos sleep con-solidated or fragmented across 24hours Does the patient sleep and
FIGURE 2-9 Sleep diary completed by a 46-year-old woman who presented with difficulty falling asleep Vertical linesrepresent when the patient went to bed lsquolsquoMrsquorsquo refers to when medication was taken black shading representstime asleep and unshaded white areas are time spent awake
Diary template reprinted from YOURSLEEPaasmnetorg from the American Academy of Sleep Medicine yoursleepaasmnetorgpdfsleepdiarypdf33
41Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
wake at conventional times or doeshe or she appear to be a lsquolsquonight owlrsquorsquoor lsquolsquomorning larkrsquorsquo Answers to thesequestions as provided by the sleepdiary may reveal factors that contrib-ute to sleep-related concerns Use ofsleep diaries can be particularly help-ful in patients with suspected circadianrhythm sleep disorders (including shiftwork) behaviorally induced insufficientsleep or inadequate sleep hygiene
OBJECTIVE MEASURESNocturnal polysomnography (NPSG)or related assessments are indicatedfor the diagnosis and assessment ofSDB and for positive airway titrationin patients with confirmed SDB Theprocedure can also provide informationabout EEG activity nocturnal move-ments cardiac rhythm and oxygen
saturation34 The recommended record-ing montage used in NPSG as shownin Figure 2-10 includes central (C3-A2C4-A1) frontal (F3-A2 F4-A1) andoccipital (O1-A2 O2-A1) EEGs left andright eye electrooculograms mentalsubmental surface EMG and ECG leadsOther recorded parameters includethoracic and abdominal effort oxygensaturation nasaloral airflow and bodyposition Use of a microphone torecord snoring is recommended butnot required34 A full 16-lead EEG(Figure 2-11)35 and video recordingmay be performed when nocturnalseizures are suspected Leg surfaceEMG leads are recommended andadditional arm EMG leads may beapplied when the clinical history sug-gests complex sleep-related motor be-haviors such as dream enactment In
KEY POINT
h A daily sleep diary helpsto summarize a patientrsquossleep-wake schedulemore accurately thanmemory often allowsand can facilitateconstruction ofpersonalized plansfor management ofcircadian rhythm sleepdisorders and insomnia
FIGURE 2-10 A 1-minute epoch from a nocturnal polysomnogram showing obstructive sleepapnea in a 46-year-old man who presented with snoring daytime sleepinessand headaches It depicts the standard recording montage that includes the
following leads central (C3-M2 C4-M1) frontal (F3-M2 F4-M1) and occipital (O1-M2 O2-M1)EEGs left and right eye electrooculograms (E1-M2 E2-M1) mentalsubmental electromyogram(Chin1-Chin2) electrocardiogram (ECG1-ECG2 ECG2-ECG3) snore volume (SNORE) nasalpressure transducer (NPRE) nasaloral airflow (NO) thoracic (THOR) and abdominal (ABD)effort arterial oxyhemoglobin saturation (SpO2) plethysmography (Pleth) and left and right eyeelectromyograms (LAT1-LAT2 RAT1-RAT2)
42 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
most cases the diagnostic NPSG is doneon 1 night although NPSG on 2 con-secutive nights may be considered inthe evaluation of parasomnias
Four categories of sleep monitoringdevices for use in the diagnosis of sleepdisorders have often been described34
These are type 1 standard attended in-laboratory polysomnography type 2comprehensive portable unattendedpolysomnography type 3 modifiedportable sleep apnea testing (often car-diorespiratory studies that do not recordsleep) and type 4 continuous single ordual bioparameter recording (eg pulseoximetry) However this categorizationmay not effectively classify the plethoraof out-of-center testing devices currentlyavailable for clinical use Therefore anew device classification system hasrecently been proposed This schemaknown as the SCOPER system catego-rizes out-of-center testing devices basedon measurement of sleep cardiovascu-
lar oximetry position effort and res-piratory parameters36 Within each ofthe six SCOPER categories a level of 0through 5 is assigned as indicated bythe type of sensor or measurementthat the device uses for that category
The most recent clinical guidelinespublished by the Portable MonitoringTask Force of the AASM37 for use ofunattended portable monitoring inthe diagnosis of OSA in adult patientsrecommend that portable monitoringonly be performed in conjunction witha comprehensive sleep evaluation by(or supervised by) a practitioner board-certified in sleep medicine or eligiblefor the certification examination Theseguidelines state that portable monitor-ing may be used in place of NPSG inpatients with a high pretest probabilityof moderate to severe OSA Portablemonitoring should not be used inpatients with significant medical comor-bidities (including but not limited to
KEY POINT
h The complexclassification of portabletesting devices reflectsthe multitude of designsavailable to cliniciansand will undoubtedlychange as technologyadvances
FIGURE 2-11 A The international 10Y20 system for EEG electrode placement refers to the10 and 20 interelectrode distances Even electrode numbers (2 4 6 8)represent the right hemisphere and odd electrode numbers (1 3 5 7)
represent the left hemisphere B Recommended F4-M1 C4-M1 O2-M1 placements of EEGelectrodes as set forth by the American Academy of Sleep Medicine (AASM)
Adapted from Iber C et al American Academy of SleepMedicine35 Used with permission of the American Academy ofSleep Medicine Darien IL 2012
43Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
moderate to severe pulmonary diseaseneuromuscular disease or congestiveheart failure) in patients with othersleep disorders (including central sleepapnea periodic limb movement disor-der insomnia parasomnias circadianrhythm disorders or narcolepsy) or asa screening tool The use of portablemonitoring may be indicated for thediagnosis of OSA in patients for whomattended NPSG is not possible becauseof immobility safety or critical illnessPortable monitoring may be indi-cated to monitor the response to non-continuous positive airway pressuretreatments for OSA including oralappliances upper airway surgery andweight loss The algorithm shown inAppendix B may help in the determi-nation of an adult patientrsquos candidacyfor out-of-center testing for the diag-nosis of OSA An example of portable(or home) monitoring technology isshown in Supplemental Digital Con-tent 2-1 linkslwwcomCONTA15
Recommended technology for port-able monitoring should record at mini-mum airflow respiratory effort andblood oxygenation the airflow effortand oximetric biosensors typically usedfor attended NPSG should be used37
These guidelines published in 2007will likely continue to evolve as newtechnologies emerge and are found tobe effective The current guidelinesrecommend that out-of-center testingbe performed under the auspices of anAASM-accredited comprehensive sleepmedicine program and that a board-certifiedeligible sleep specialist reviewthe raw data from a portable monitor-ing device All patients who undergoportablemonitoring for the diagnosis ofOSA should have a follow-up visit toreview test results Negative or techni-cally inadequate portable monitoringstudies should be followed by attendedin-laboratory NPSG if the clinical suspi-cion for SDB remains high37
The aforementioned testing proce-dures are primarily used in the evalua-tion of SDB Other testing modalitiesare useful in the diagnosis of othercategories of sleep disorders The mul-tiple sleep latency test (MSLT) and itsvariant the maintenance of wakefulnesstest (MWT) are used in the evaluation ofhypersomnia The conventional record-ing montage is similar to that used fornocturnal polysomnography central fron-tal and occipital EEGs left and right eyeelectrooculograms mentalsubmentalEMG and ECG leads Measurement ofthoracic and abdominal effort oxygensaturation and nasaloral airflow are notrequired but may help explain delayedsleep latencies for patients in whomrespiratory disturbances interfere withsleep onset
The MSLT is a validated tool that isconsidered the de facto standard forobjective assessment of excessive day-time sleepiness38 The recommendedprotocol38 involves five 20-minute napopportunities held at 2-hour intervalsthroughout the day If sleep is ob-served the patient is allowed to sleepfor at least 15 minutes The sleep la-tency for each nap is measured as thetime from the start of the nap trial tothe first epoch of sleep A sleep la-tency of 20 minutes is assigned to naptrials during which no sleep isobserved39 The mean sleep latencycalculated as the average sleep latencyacross all nap trials is the final resultThe presence and number of sleep-onset REM periods (SOREMPs) is alsodetermined as this information canhelp to establish a diagnosis of narco-lepsy without cataplexy or to confirmnarcolepsy with cataplexy
The MSLT should be started 15 to30 hours following completion of anocturnal polysomnogram whichshould record at least 6 hours of sleepin order for determination of the meansleep latency to be valid Drugs that may
KEY POINT
h Careful considerationshould be given tothe indications forout-of-center testingAttended nocturnalpolysomnography isindicated if a portablestudy yields a negativeor technicallyinadequate result
44 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
interfere with sleep latency or REM la-tency should be discontinued 2 weeksbefore testing whenever possible Ascreen may be performed on the day oftesting if there is suspicion that pre-scribed or illicit substances may con-tribute to the patientrsquos sleepiness38
No large multicenter systematicallycollected normative data are availablefor mean sleep latency values on theMSLT38 Nonetheless a mean sleep la-tency of greater than 10 minutes is of-ten considered normal whereas a meansleep latency of 8 to 10 minutes is con-sidered a physiologic gray zone40 Thenormative data for children are classi-fied by Tanner stage of developmentthough the MSLT is typically not per-formed in children aged younger than 6or 7 years because some daytime nap-ping may still be normal in youngchildren41 The second edition of theInternational Classification of SleepDisorders Diagnostic and CodingManual (ICSD-2)42 requires the pres-ence of a mean sleep latency of lessthan 8 minutes and two or moreSOREMPs as part of the diagnosticcriteria for narcolepsy without cata-plexy However the ICSD-2 also notesthat a mean sleep latency of less than 8minutes may occur in up to 30 of thegeneral population Therefore whilethe MSLT is a helpful and widely usedtool it remains an imperfect gold stand-ard in the assessment of daytime sleepi-ness This necessitates that theevaluation of daytime sleepiness notrest on the MSLT results alone butassimilate the clinical history subjectivecomplaints diagnostic study results andother pertinent medical information38
Practice parameters from theAASM state that the MSLT is indicatedfor diagnostic confirmation of sus-pected narcolepsy and may be indi-cated to differentiate idiopathichypersomnia from narcolepsy38 TheMSLT is not indicated for routine
assessment of OSA syndrome or toassess response to treatment of SDBand is not routinely indicated for eval-uation of sleepiness in medical orneurologic disorders (except for narco-lepsy) insomnia or circadian rhythmdisorders
TheMWTprovides an objectivemeas-ure of a patientrsquos ability to remain awakerather than the tendency to fall asleepduring the day The key differencebetween the MWT and the MSLT is thatin the former the patient is asked to tryto stay awake under circumstances con-ducive to sleep rather than to fall asleepThe MWT provides an objective vali-dated assessment of the ability to remainawake for a defined length of time38 Therecommended protocol includes four40-minute trials that begin at 2-hourintervals with the first trial to start 15 to30 hours after the patientrsquos wake-uptime A nocturnal polysomnogram onthe preceding night is not requiredHowever the patient should obtain asufficient amount of sleep during thenight before the MWT Each trial isterminated after 40 minutes if no sleepoccurs or after unequivocal sleep onset(defined as three continuous epochsof stage N1 sleep or one epoch of anyother stage of sleep) has occurred38
One indication for the MWT is to as-sess an individualrsquos ability to remainawake when his or her inability to re-main awake constitutes a public orpersonal safety issue This can becomea pressing issue for individuals em-ployed in the transportation43 con-struction or health care industriesThe MWT may be indicated to assesstreatment response in patients withknown excessive daytime sleepiness
Limited amounts of normative dataare available for the MWT Historicallymultiple testing protocols make syn-thesis of results more challenging TheMWT is used much less often in clinicalpractice compared to the MSLT Patient
KEY POINTS
h The multiple sleeplatency test is the goldstandard for objectiveassessment of daytimesleepiness butinterpretation of theresults must be madewithin the clinicalcontext of the patientrsquoshistory
h In the multiple sleeplatency test the patientis instructed to try tosleep during each naptrial In the maintenanceof wakefulness test thepatient is instructed totry to remain awakeduring the nap trial
h A baseline nocturnalpolysomnogram isrequired before amultiple sleep latencytest and considered butnot required before amaintenance ofwakefulness test
45Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
age may also affect the mean sleep la-tency values on both the MWT and theMSLT43 and may represent evolution ofcircadian rhythm and sleep architec-ture across the lifetime A study of 383patients with narcolepsy with cataplexyexamined the clinical and polysomno-graphic data at the time of diagnosis(age range 5 to 84 years) and found aprogressive decrease in the number ofSOREMPs and a progressive increase inthe mean sleep latency on the MSLT asa function of age44 Given its limita-tions the MWT may thus be used tosupplement the clinical history in theassessment of ability to stay awake butshould not be the sole determinant ofthis parameter
Actigraphy is also used in the clinicalevaluation of patients with sleep disor-ders particularly circadian rhythm sleepdisorders An actigraph is a watchlikedevice that is worn on the wrist for anextended period usually in the range ofweeks The actigraph records move-ment and uses an algorithm to estimatethe amounts of sleep and wake timeduring the recording period Analysissoftware uses movement to estimatewhen sleep and wakefulness haveoccurred Review of the data can pro-vide objective insight into the patientrsquossleep pattern including timing andduration of major sleep disruptionsActigraphy is indicated as part of theevaluation of patients with advancedsleep-phase syndrome delayed sleep-phase syndrome and shift work disor-der and may be indicated in the evalua-tion of jet lag disorder and nonY24-hoursleep-wake syndrome including thatassociated with blindness45 It can alsoserve as a measure of treatment re-sponse in patients with insomnia andcircadian rhythm sleep disorders Forpopulations in which traditional sleepmonitoring may be challenging suchas pediatric or older adult patientsactigraphy may provide valuable infor-
mation about the patientrsquos sleep pat-tern or response to treatment Whenpolysomnography is not availableactigraphy is indicated to estimate totalsleep time in patients with OSA45
OTHER ASSESSMENTMODALITIESLaboratory evaluation and neuroimag-ing with either CT or MRI may beconsidered on an individual basis asindicated by the clinical history Com-plete blood count (CBC) serum chem-istries or measures of thyroid functionmay be obtained if an underlying med-ical disorder is thought to contribute tothe patientrsquos sleep symptoms Forinstance these laboratory studies maybe consideredwhen daytime fatigue is apredominant symptom Serum ironstudies including ferritin level shouldbe checked in patients with restless legssyndrome46 Neuroimaging should beconsidered in patients with antecedenttrauma or for any sleep disorder pa-tient with an abnormal neurologic ex-amination to evaluate for a structuraletiology of the patientrsquos symptoms
APPROACH TO THE PATIENTEvaluation of suspected sleep disordersis best accomplished by a stepwisemultidimensional approach (Case 2-2)A thorough sleep history includes de-tailed description of sleep-related symp-toms nocturnal behaviors the patientrsquossleep schedule level of daytime sleepi-ness and subsequent effects on daytimefunctioning Collateral history from thepatientrsquos bed partner or family is oftennecessary to understand the severity andcontext of the patientrsquos symptoms Sub-jective assessments of sleepiness suchas the Epworth Sleepiness Scale areeasily administered and useful to tracksymptomatic progression or treatmentresponse from one visit to the nextCertain physical examination findingsmay also raise clinical suspicion of
KEY POINTS
h Actigraphy can beuseful in evaluation andtreatment of circadianrhythm sleep disordersand in management ofinsomnia
h Neuroimaging is notroutinely indicated inthe clinical evaluation ofsleep disorders andshould be pursued on acase-by-case basis
46 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
particular sleep disorders For patientsin whom multiple sleep disorders aresuspected systematic use of diagnostictesting allows for accurate identificationof specific diagnoses In a patient withinsomnia and symptoms suggestive ofSDB nocturnal polysomnography shouldbe the first procedure performed Ifthe insomnia persists despite adequatetreatment of SDB further evaluationwith sleep diaries and possibly actigra-
phy may be considered to better char-acterize the patientrsquos sleep patternActigraphy may then again be pursuedto gauge treatment response upon man-agement of the patientrsquos insomnia
The diagnostic modalities availablefor evaluation of sleep disorders arerapidly evolving In-laboratory nocturnalpolysomnography currently remains thegold standard for assessment of SDBHowever the multitude of out-of-center
KEY POINT
h Careful assimilation ofthe clinical history thesleep-specific physicalexamination patientquestionnaires anddiagnostic test resultsleads to the mostaccurate assessment ofpatients with symptomsrelated to sleep oralertness
Case 2-2A 23-year-old woman reported a 4-year history of insomnia Throughoutcollege she was a lsquolsquonight owlrsquorsquo never scheduled classes that started before100 PM and always did well in school During the past 6 months shedeveloped progressive difficulty staying awake in her job as a financialanalyst andwas concerned about how this might affect her job performance
During the week she was in bed by midnight but was unable to fallasleep until 200 AM and awoke with difficulty to an alarm at 600 AMfeeling tired She denied any thought rumination or physical discomfortat bedtime She had tried over-the-counter sleep aids that provided nosymptomatic improvement and worsened morning grogginess Onweekends she slept from 200 AM to 1100 AM and awakened feelinglsquolsquopretty goodrsquorsquo She had nocturia up to once per night and occasionalmorning headaches She had no bed partner but reported gaspingrespirations nocturnal palpitations and snort arousals On about 4 nightsper week she experienced a sensation of needing to move her legswhile trying to fall asleep This sensation was relieved by movement andwas worse at night than during the day Her legs sometimes movedspontaneously at night or while seated quietly for long periods duringthe day She felt sleepy during the afternoon especially while workingat her computer She denied drowsiness while driving She occasionallytook a 30-minute nap on the weekend and found it to be refreshingShe drank one to two cups of coffee every morning and had a 12-oz dietcaffeinated soda at 300 PM Her sleepiness had not caused her to makeany mistakes at work and she denied any mood disturbance
Physical examination was notable for a body mass index of 32 kgm2 neckcircumference of 381 cm (15 in) and modified Mallampati class III oral airwayNasal passages were narrow with turbinate hypertrophy bilaterally andhard palate was high-arched and narrow Nomicrognathia or retrognathia waspresent She had molar occlusion class I bilaterally with no overjet or overbiteThe general cardiac respiratory and neurologic examinations were normal
Comment This case illustrates how discussion of the chief complaint raisessuspicion for multiple sleep disorders The history suggests a circadian rhythmsleep disorder particularly delayed sleep-phase syndrome sleep-disorderedbreathing and restless legs syndrome Diagnostic evaluation should includenocturnal polysomnogramwith consideration toperform testing at the patientrsquospreferred sleep time and serum iron studies Sleep diaries andor actigraphymay be considered for further assessment of the patientrsquos sleep pattern
47Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
testing devices continues to grow andmany may provide useful alternativesthat under appropriate circumstancescould allow more expedient conven-ient and less costly evaluations ofincreased numbers of patients whopreviously had only limited or delayedaccess to sleep services
VIDEO LEGENDSupplemental Digital Content 2-1
Home sleep study Video demonstrates a homesleep study using an unattended type 3 portablemonitoring device The patient is a 56-year-oldman who is experiencing morning headachesand concentration and alertness problems atwork He has a history of mild snoring and ar-terial hypertension His Epworth SleepinessScale score is 18 his neck circumference is19 in he has a Mallampati classification score ofIII and his body mass index is 41 kgm Theapnea-hypopnea index is 84 eventsh Channelsrecorded in this sleep study include arterialoxyhemoglobin saturation heart rate oral-nasalpressure flow snoring inductive plethysmog-raphy for chest efforts and body position
linkslwwcomCONTA15
B 2013 Marcel Hungs MD PhD Used withpermission
REFERENCES1 National Institutes of Health National
Center on Sleep Disorders ResearchSleep disorders research planwwwnhlbinihgovhealthprofsleep201101011NationalSleepDisordersResearch-PlanDHHSPublication11-7820pdf PublishedNovember 2011
2 Dinges DF An overview of sleepiness andaccidents J Sleep Res 19954(S2)4Y14
3 Mills RJ Young CA A medical definitionof fatigue in multiple sclerosis QJM 2008101(1)49Y60
4 Chervin RD Sleepiness fatigue tirednessand lack of energy in obstructive sleepapnea Chest 2000118(2)372Y379
5 Chotinaiwattarakul W OrsquoBrien LM Fan LChervin RD Fatigue tiredness and lack ofenergy improve with treatment for OSAJ Clin Sleep Med 20095(3)222Y227
6 American Academy of Sleep MedicineThe international classification of sleepdisorders diagnostic and coding manual2nd ed Westchester IL American Academyof Sleep Medicine 2005
7 Ebben MR Spielman AJNon-pharmacological treatments forinsomnia J Behav Med 200932(3)244Y254
8 Roth T Insomnia definition prevalenceetiology and consequences J Clin SleepMed 20073(5 suppl)S7YS10
9 Yang CM Spielman AJ Glovinsky PNonpharmacologic strategies in themanagement of insomnia Psychiatr ClinNorth Am 200629(4)895Y919 abstract viii
10 Katz ES DrsquoAmbrosio CM Pediatricobstructive sleep apnea syndrome ClinChest Med 201031(2)221Y234
11 Kohler M Bloch KE Stradling JR The role ofthe nose in the pathogenesis of obstructivesleep apnea Curr Opin Otolaryngol HeadNeck Surg 200917(1)33Y37
12 Kryger MH Atlas of clinical sleep medicinePhiladelphia PA Elsevier 2010
13 Zonato AI Martinho FL Bittencourt LRet al Head and neck physical examinationcomparison between nonapneic andobstructive sleep apnea patientsLaryngoscope 2005115(6)1030Y1034
14 Mallampati SR Gatt SP Gugino LD et alA clinical sign to predict difficult trachealintubation a prospective study Can AnaesthSoc J 198532(4)429Y434
15 Samsoon GL Young JR Difficult trachealintubation a retrospective studyAnaesthesia 198742(5)487Y490
16 Huang HH Lee MS Shih YL et alModified Mallampati classificationas a clinical predictor of peroralesophagogastroduodenoscopy toleranceBMC Gastroenterol 20111112
17 Friedman M Ibrahim H Bass L Clinicalstaging for sleep-disordered breathingOtolaryngol Head Neck Surg 2002127(1)13Y21
18 Cheng RHW Yiu CKY Leung WKOral health in individuals with Downsyndrome In Dey S ed Prenatal diagnosisand screening for down syndromeInTech wwwintechopencombookshowtoreferenceprenatal-diagnosis-and-screening-for-down-syndromeoral-health-in-individuals-with-down-syndromePublished 2011 Accessed August 24 2012
19 Katz I Stradling J Slutsky AS et al Dopatients with obstructive sleep apneahave thick necks Am Rev Respir Dis1990141(5 pt 1)1228Y1231
20 Kushida CA Efron B Guilleminault C Apredictive morphometric model for theobstructive sleep apnea syndrome AnnIntern Med 1997127(8 pt 1)581Y587
48 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
21 Saccucci M Tettamanti L Mummolo S et alScoliosis and dental occlusion a review ofthe literature Scoliosis 2011615
22 Battagel JM Kotecha B Dental side-effectsof mandibular advancement splint wear inpatients who snore Clin Otolaryngol200530(2)149Y156
23 Morcos SS Patel PK The vocabulary ofdentofacial deformities Clin Plast Surg200734(3)589Y599
24 Epstein LJ Kristo D Strollo PJ Jr et alClinical guideline for the evaluationmanagement and long-term care ofobstructive sleep apnea in adults J ClinSleep Med 20095(3)263Y276
25 Johns MW A new method for measuringdaytime sleepiness the Epworth sleepinessscale Sleep 199114(6)540Y545
26 Johns MW Daytime sleepiness snoring andobstructive sleep apnea The EpworthSleepiness Scale Chest 1993103(1)30Y36
27 Chervin RD Aldrich MS The EpworthSleepiness Scale may not reflect objectivemeasures of sleepiness or sleep apneaNeurology 199952(1)125Y131
28 Buysse DJ Reynolds CF 3rd Monk THet al The Pittsburgh Sleep Quality Index anew instrument for psychiatric practice andresearch Psychiatry Res 198928(2)193Y213
29 Chervin RD Hedger K Dillon JE Pituch KJPediatric sleep questionnaire (PSQ) validityand reliability of scales for sleep-disorderedbreathing snoring sleepiness and behavioralproblems Sleep Med 20001(1)21Y32
30 Chung F Yegneswaran B Liao P et al STOPquestionnaire a tool to screen patients forobstructive sleep apnea Anesthesiology2008108(5)812Y821
31 Walters AS LeBrocq C Dhar A et alValidation of the International Restless LegsSyndrome Study Group rating scale forrestless legs syndrome Sleep Med 20034(2)121Y132
32 Bastien CH Vallieres A Morin CMValidation of the Insomnia Severity Indexas an outcome measure for insomniaresearch Sleep Med 20012(4)297Y307
33 YOURSLEEPaasmnetorg from the AmericanAcademy of Sleep Medicine Two weeksleep diary yoursleepaasmnetorgpdfsleepdiarypdf Accessed August 24 2012
34 Kushida CA Littner MR Morgenthaler Tet al Practice parameters for the indicationsfor polysomnography and relatedprocedures an update for 2005 Sleep200528(4)499Y521
35 Iber C Ancoli-Israel S Chesson A et alThe AASM manual for scoring of sleep andassociated events rules terminology andtechnical specifications 1st ed WestchesterIL American Academy of Sleep Medicine2007
36 Collop NA Tracy SL Kapur V et alObstructive sleep apnea devices forout-of-center (OOC) testing technologyevaluation J Clin Sleep Med 20117(5)531Y548
37 Collop NA Anderson WM Boehlecke Bet al Clinical guidelines for the use ofunattended portable monitors in thediagnosis of obstructive sleep apnea in adultpatients Portable Monitoring Task Forceof the American Academy of SleepMedicine J Clin Sleep Med 20073(7)737Y747
38 Littner MR Kushida C Wise M et alStandards of Practice Committee of theAmerican Academy of Sleep MedicinePractice parameters for clinical use of themultiple sleep latency test and themaintenance of wakefulness test Sleep200528(1)113Y121
39 Carskadon MA Dement WC Mitler MMet al Guidelines for the multiple sleeplatency test (MSLT) a standard measure ofsleepiness Sleep 19869(4)519Y524
40 van den Hoed J Kraemer H Guilleminault Cet al Disorders of excessive daytimesomnolence polygraphic and clinical datafor 100 patients Sleep 19814(1)23Y37
41 Hoban TF Chervin RD Assessment ofsleepiness in children Semin PediatrNeurol 20018(4)216Y228
42 ICSD-2 The international classification ofsleep disorders pocket version diagnosticand coding manual 2nd ed WestchesterIL American Academy of Sleep Medicine2005
43 Arand D Bonnet M Hurwitz T et alThe clinical use of the MSLT and MWTSleep 200528(1)123Y144
44 Dauvilliers Y Gosselin A Paquet J et alEffect of age on MSLT results in patientswith narcolepsy-cataplexy Neurology200462(1)46Y50
45 Morgenthaler T Alessi C Friedman Let al Practice parameters for the use ofactigraphy in the assessment of sleep andsleep disorders an update for 2007 Sleep200730(4)519Y529
46 Gamaldo CE Earley CJ Restless legssyndrome a clinical update Chest2006130(5)1596Y1604
49Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited

nocturnal awakenings behaviors dur-ing nocturnal awakenings and latencyto fall back asleep after each awakeningA useful approach is to ask the patientfor a detailed start-to-finish descriptionof the entire typical sleep period anddaytime period Any medications pre-viously or currently used to facilitatesleep should also be identified
The sleep history should screenfor potentially relevant sleep disordersthat may cause excessive daytime sleep-iness or insomnia (Case 2-1) Thepresence of symptoms such as snor-ing witnessed apneas and morningheadaches raises the suspicion forsleep-disordered breathing (SDB) Leg
discomfort associated with an urge tomove that worsens at night andimproves with leg movement indicatesrestless legs syndrome and may con-tribute to the patientrsquos poor sleepquality and impair daytime functioningSleep paralysis and hypnagogic orhypnopompic hallucinations are notspecific to a particular sleep disorderwhile a history of cataplexy is patho-gnomonic for narcolepsy and must beexplored when a patient presents withreports of central hypersomnia ratherthan SDB When relevant the clinicianshould also ask about nocturnal behav-iors specifically ones that may pose riskof injury to the patient or bed partner
Case 2-1A 44-year-old man with a long-standing history of loud frequent snoringpresented because of his wifersquos concerns related to his snoring His wifehad witnessed him to have occasional pauses in his breathing during sleepand at times he awakened to his snoring He reported frequent acidreflux and morning headaches Approximately once per month he wouldawaken lsquolsquofeeling like my heart is racing and I need to catch my breathrsquorsquoHe had occasional nasal congestion but always awakened with a drymouth and sore throat He denied any leg discomfort but his wife hadtold him that he tossed and turned frequently during sleep
His sleep schedule was the same every night he was in bed by 1000 PMfell asleep immediately without the use of any sleep aids and awakenedat 600 AM feeling tired He had up to four nocturnal awakenings pernight two were attributed to nocturia and the rest were of unknownetiology Each awakening lasted a few minutes and he fell asleep againeasily He had had a few episodes of sleepwalking as a child but none sincethe age of 8 years
He felt sleepy during the day with a propensity to doze unintentionallywhile reading or watching television He denied drowsiness while driving butlimited his driving to his 20-minute commute to and from work his wifedrove for longer distances and hewould often sleep in the passenger seat Hissleepiness was worse in the midafternoon and if given the opportunity hewould nap for 1 hour on the weekends He found naps to be somewhatrefreshing He drank two to three cups of coffee every morning and had a12-oz caffeinated sodawith lunch His sleepiness had not caused him tomakeany mistakes in his job as a physical therapist although he felt that he hadpotential for further improvement in his job performance He also reportedfeeling more irritable in recent months but this had not caused anydifficulties at home or work
Comment This case illustrates the multiple components of a concisebut still detailed sleep history The patientrsquos daytime symptoms provideinsight about the effects of the patientrsquos untreated sleep disorder
35Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
such as sleepwalking driving or cook-ing while asleep or dream-enactmentbehavior If the patient reports suchbehavior further inquiry must be madeabout the frequency of these events andany history of injury sustained due to thesleep-related behavior Details of thesleep history permit a thorough differ-ential diagnosis and can also guide adiscussion of safety concerns
PHYSICAL EXAMINATIONA comprehensive multisystem exami-nation is an important aspect of thesleep evaluation Measurement of theweight height body mass index (BMI)neck circumference and blood pres-sure and heart rate should be per-formed for nearly all patients withsymptoms related to sleep or alertnessOther salient features of the generalexamination include auscultation forany cardiac or respiratory abnormalitiesand identification of peripheral edemaA focused neurologic examinationshould be guided by the patientrsquos his-tory For instance a mental status as-sessment should be considered if apatient with excessive daytime sleepi-ness also complains of memory loss If apatient with a history of diabetes melli-
tus endorses symptoms of restless legssyndrome it is worthwhile to assess forstocking-glove distribution sensory lossand weakness
Detailed examination of the headand neck should be performed as partof a comprehensive sleep evaluationThe patientrsquos facial morphology shouldbe assessed for features of long facesyndrome which includes infraorbitaldarkening mouth breathing elongatedmidface and nasal atrophy10 A 2009review11 reports that previous observa-tional and cross-sectional studies haveshown a relationship between chronicnasal obstruction and OSA Thus a thor-ough nasal examination should be per-formed on patients with sleep-relatedcomplaints Examination of the nasalairway should include evaluation forsymmetry of the nares nasal septum de-viation (Figure 2-1)12 and nasal turbi-nate hypertrophy A bedside assessmentof nasal airflow can be accomplished by
KEY POINT
h Details of facialmorphology nasalairway patency and oralairway crowding arekey features of thesleep-specificexamination
FIGURE 2-1 Nasal septal deviation Thisstructural abnormality canpredispose a patient to havesleep-disordered breathing
Reprinted from Kryger MH Elsevier12 B 2010 withpermission from Elsevier
FIGURE 2-2 Retrognathia Retrognathiais derived from the termslsquolsquoretrorsquorsquo (backward) and
lsquolsquognathosrsquorsquo (jaw) With retrognathia one orboth jaws recede with respect to the frontalplane of the forehead The condition maypredispose a patient to obstruction of theairway and sleep apnea by displacing thetongue against the retropharyngeal regioncompromising airflow Retrognathia issometimes corrected through surgicalrepositioning or advancement of themandible
Reprinted from Kryger MH Elsevier12 B 2010 withpermission from Elsevier
36 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
asking the patient to press the indexfinger against the left nostril and take adeep breath in on the right side thisshould be repeated on the oppositeside as well The patientrsquos facial mor-phology should be assessed for man-dibular retrognathia (Figure 2-2)12 Withthe patientrsquos head in a neutral posi-tion a virtual line is drawn from thevermillion border of the lower lip tothe chin Mandibular retrognathia issuggested if the anterior prominence ofthe chin is 2 mm or more behind thevirtual line13
The modified Mallampati classifica-tion is commonly used for assessmentof the oral airway in patients withsuspected SDB The Mallampati classi-fication14 was developed to identifypatients in whom tracheal intubationwould be difficult the initial description
divided patients into three classes Twoyears later15 this was modified to de-scribe four groups class I class II classIII and class IV Figure 2-3 16 illustratesthe modified Mallampati classificationassessed with the tongue protrudedThe Friedman palate position classifi-cation17 also commonly referencedutilizes the same four categories but isdone with the tongue at rest and notextended Either the Mallampati orFriedman classification may be used todescribe the patency of the oral airway
Tonsils should be classified based onthe degree of hypertrophy (Figure 2-4)12grade I tonsils are inside the tonsillarfossa lateral to the posterior pillarsgrade II tonsils occupy 25 of theoropharynx grade III tonsils occupy50 of the oropharynx and grade IVtonsils occupy at least 75 of the
FIGURE 2-3 Modified Mallampati classification The class is determined by looking at theanatomy of the oral cavity and describes tongue size relative to oropharyngealsize The test is conducted with the patient seated the head held in a neutral
position and the mouth wide open and relaxed The subsequent classification is assigned basedupon the pharyngeal structures that are visible
Reprinted from Huang HH et al BMC Gastroenterol16 B 2011 BioMed Central Ltd wwwbiomedcentralcom1471-230X1112
37Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
oropharynx and nearly meet in the mid-line13 A high-arched narrow hard pal-ate (Figure 2-5)18 may predispose thepatient to have SDB Katz and col-leagues19 have shown that patients withOSA have significantly increased neckcircumference compared to nonapneicsnorers greater distribution of neck fat
may contribute to mass loading on theupper airway in patients with OSA Thepatientrsquos neck circumference should bemeasured at the superior border of thecricothyroid membrane19 A neck cir-cumference greater than 40 cm (157in) has been shown to be predictive ofOSA with 61 sensitivity and 93specificity regardless of sex20
Assessment of the patientrsquos anteriorand posterior dentition can also re-veal anatomic findings that may pre-dispose a person to certain sleepdisorders Two features to note in eval-uation of the anterior dentition areoverjet and overbite (Figure 2-6)21
Overjet as shown in Figure 2-712 isthe horizontal distance between theupper right central incisor and thebuccal surface of the correspondinglower tooth while overbite is the ver-tical distance between these twopoints22 These measurements are typ-ically reported in millimeters The An-gle classification system is used todescribe the first molar position on
FIGURE 2-4 Tonsil size grading Thisstructural abnormality canpredispose a patient to havesleep-disordered breathing
Reprinted from Kryger MH Elsevier12 B 2010 withpermission from Elsevier
FIGURE 2-5 Deficientmaxillarydevelopment inan individual with
Down syndrome leading to highand narrow hard palate
Reprinted with permission from ChengRHW et al InTech18 B 2011 W KeungLeung wwwintechopencombooksprenatal-diagnosis-and-screening-for-down-syndromeoral-health-in-individuals-with-down-syndrome
FIGURE 2-6 Overjet andoverbite Overjetis defined as
increased projection of the upperteeth in front of the lower teethas measured parallel to theocclusal plane Overbite is thevertical overlapping of maxillaryteeth over mandibular teethusually measured perpendicularto the occlusal plane
Reprinted from Saccucci M et al Scoliosis21
B 2011 BioMed Central Ltd wwwscoliosisjournalcomcontent6115
38 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
the mandibular and maxillary dentalarches23 Figure 2-8 shows class I oc-clusion and class II and III malocclu-
sion Of note the mesiobuccal surfaceis the aspect of the tooth that is adja-cent to the cheek mucosa
The Adult Obstructive Sleep ApneaTask Force of the American Academyof Sleep Medicine (AASM) recommen-ded in recent clinical guidelines24 thatthe following physical findings maysuggest the presence of OSA increasedneck circumference (greater than 432cm [17 in] in men greater than 406 cm[16 in] in women) BMI 30 kgm2 orgreater modified Mallampati classifica-tion of III or IV presence of retrognathialateral peritonsillar narrowing macro-glossia tonsillar hypertrophy elongatedenlarged uvula high-archednarrowhard palate nasal abnormalities (egpolyps deviation valve abnormalities
KEY POINT
h Classification of thepatientrsquos dentition helpsto evaluate the positionof the maxillary archrelative to themandibular arch
FIGURE 2-7 OverjetDisplacementof the
mandibular teeth posteriorly inrelationship to the maxillary teethresults inmoreposteriorly crowdedupper airways predisposingpatients for the developmentof obstructive sleep apnea
Reprinted from Kryger MH Elsevier12
B 2010 with permission from Elsevier
FIGURE 2-8 Angle class occlusionmalocclusion A Angle class I occlusion also known asneutrocclusion The mandibular and maxillary dental arches have a normalanterior-posterior relationship The mesiobuccal groove of the mandibular first
molar interdigitates with the mesiobuccal cusp of the maxillary first molar B Angle class IImalocclusion also known as distoclusion The mandibular dental arch is in distal anterior-posteriorrelationship to the maxillary dental arch The mesiobuccal groove of the mandibular first molar isdistal to the mesiobuccal cusp of the maxillary first molar C Angle class III malocclusion alsoknown as mesioclusion The mandibular dental arch is in mesial anterior-posterior relationship tothe maxillary dental arch The mesiobuccal groove of the mandibular first molar is mesial to themesiobuccal cusp of the maxillary first molar
Reprinted fromMorcos SS Patel PK Clin Plast Surg23 B 2007 with permission from Elsevier wwwsciencedirectcomsciencearticlepiiS0094129807000843
39Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
and turbinate hypertrophy) andoroverjet To prevent overlooking thesefindings a thorough head and neckassessment as described in Table 2-2should be incorporated into the phys-ical examination of all patients whopresent with sleep-related complaints
SUBJECTIVE ASSESSMENTSeveral patient-completed question-naires are inexpensive and time-efficient
reasonably well validated and com-monly used They can help to increasestandardization in evaluations of patientsby different clinicians or across centersPerhaps the most well-known andwidely used is the Epworth SleepinessScale25 a subjective assessment of thepatientrsquos daytime sleep propensity inrecent times As shown in Appendix Athe Epworth Sleepiness Scale asks theresponder to use a four-point Likertscale (0 1 2 or 3) to indicate thelikelihood of dozing in eight distinctsedentary conditions A total score of 10or greater out of a possible 24 suggestsexcessive daytime sleepiness25 Whilethe Epworth Sleepiness Scale score canbe easily incorporated into the clinicalevaluation it should not be used as asubstitute for objective measurement ofsleepiness The Epworth Sleepiness Scalescore may correlate to a limited extentwith the presence and severity of OSA26
but some studies have failed to find anystatistically significant association withmean sleep latency on multiple sleep la-tency tests or with severity of OSA27
The most advantageous use of theEpworth Sleepiness Scale may be to followan individualrsquos self-assessment of sleep-iness longitudinally and it may also serveas an indicator of treatment response
Many other questionnaires may beutilized in a clinical sleep evaluationsome pertain to overall sleep qualitywhile others are disorder-specific ThePatient Reported Outcomes Measure-ment Information System (PROMIS) isan NIH-supported system of measuresfor patient-reported health status andincludes questions on sleep disturb-ance The Pittsburgh Sleep QualityIndex (PSQI) is a validated question-naire that inquires about sleep qualityand disturbances over the previousmonth28 The parent-completed Pe-diatric Sleep Questionnaire29 containsa validated reliable 22-item scale tohelp assess risk for SDB in children
KEY POINTS
h The Epworth SleepinessScale apatient-completedquestionnaire assessesthe patientrsquos subjectivetendency to doze duringsedentary situations inrecent times not onlyat the moment thequestionnaire iscompleted
h The Epworth SleepinessScale should not beused in lieu of diagnostictesting but may be avaluable componentof ongoing clinicalevaluation
TABLE 2-2 Head and NeckExamination
b Face
Featuresof long face syndrome
Infraorbital darkening
Mouth breathing
Elongated midface
Nasal atrophy
b Oral Airway
Mandibular retrognathia
Low soft palate (modifiedMallampati classification)
Large or boggy uvula
Erythematous pillars
Tonsillar hypertrophy
High narrow hard palate
Neck circumference
Overjet
Overbite
Angle classification(malocclusion)
Macroglossia
Worn occlusive surfaces(suggestive of bruxism)
b Nasal Airway
Symmetry of the nares
Nasal septum deviation
Nasal airflow
Collapse of nasal alae oninspiration
b Neck
Neck circumference
40 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
The STOP-BANG questionnaire devel-oped and validated in preoperativepatients is a sensitive screening toolfor OSA Four questions address snor-ing tiredness during daytime observedapnea and high blood pressure whereasfour other measures focus on increasedOSA risk factors of BMI (greater than 35kgm2) age (older than 50 years) neckcircumference (greater than 40 cm[1575 in]) and gender (male preva-lence)30 The International RestlessLegs Syndrome Study Group Rating Scale(IRLS) is a validated assessment of dis-ease severity for patients with restlesslegs syndrome31 The patientrsquos perceived
level of insomnia may be assessed withthe Insomnia Severity Index (ISI) avalidated 7-item questionnaire32
A sleep diary (Figure 2-9)33 allows apatient to chart daily sleep and waketimes and should be maintained for atleast 2 consecutive weeks Review ofthis information allows the clinicianto estimate the total amount of sleepthe patient obtains in a 24-hour pe-riod The sleep diary also can provideinsight into the patientrsquos sleep patternIs sleep obtained at the same timesevery day Is the patientrsquos sleep con-solidated or fragmented across 24hours Does the patient sleep and
FIGURE 2-9 Sleep diary completed by a 46-year-old woman who presented with difficulty falling asleep Vertical linesrepresent when the patient went to bed lsquolsquoMrsquorsquo refers to when medication was taken black shading representstime asleep and unshaded white areas are time spent awake
Diary template reprinted from YOURSLEEPaasmnetorg from the American Academy of Sleep Medicine yoursleepaasmnetorgpdfsleepdiarypdf33
41Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
wake at conventional times or doeshe or she appear to be a lsquolsquonight owlrsquorsquoor lsquolsquomorning larkrsquorsquo Answers to thesequestions as provided by the sleepdiary may reveal factors that contrib-ute to sleep-related concerns Use ofsleep diaries can be particularly help-ful in patients with suspected circadianrhythm sleep disorders (including shiftwork) behaviorally induced insufficientsleep or inadequate sleep hygiene
OBJECTIVE MEASURESNocturnal polysomnography (NPSG)or related assessments are indicatedfor the diagnosis and assessment ofSDB and for positive airway titrationin patients with confirmed SDB Theprocedure can also provide informationabout EEG activity nocturnal move-ments cardiac rhythm and oxygen
saturation34 The recommended record-ing montage used in NPSG as shownin Figure 2-10 includes central (C3-A2C4-A1) frontal (F3-A2 F4-A1) andoccipital (O1-A2 O2-A1) EEGs left andright eye electrooculograms mentalsubmental surface EMG and ECG leadsOther recorded parameters includethoracic and abdominal effort oxygensaturation nasaloral airflow and bodyposition Use of a microphone torecord snoring is recommended butnot required34 A full 16-lead EEG(Figure 2-11)35 and video recordingmay be performed when nocturnalseizures are suspected Leg surfaceEMG leads are recommended andadditional arm EMG leads may beapplied when the clinical history sug-gests complex sleep-related motor be-haviors such as dream enactment In
KEY POINT
h A daily sleep diary helpsto summarize a patientrsquossleep-wake schedulemore accurately thanmemory often allowsand can facilitateconstruction ofpersonalized plansfor management ofcircadian rhythm sleepdisorders and insomnia
FIGURE 2-10 A 1-minute epoch from a nocturnal polysomnogram showing obstructive sleepapnea in a 46-year-old man who presented with snoring daytime sleepinessand headaches It depicts the standard recording montage that includes the
following leads central (C3-M2 C4-M1) frontal (F3-M2 F4-M1) and occipital (O1-M2 O2-M1)EEGs left and right eye electrooculograms (E1-M2 E2-M1) mentalsubmental electromyogram(Chin1-Chin2) electrocardiogram (ECG1-ECG2 ECG2-ECG3) snore volume (SNORE) nasalpressure transducer (NPRE) nasaloral airflow (NO) thoracic (THOR) and abdominal (ABD)effort arterial oxyhemoglobin saturation (SpO2) plethysmography (Pleth) and left and right eyeelectromyograms (LAT1-LAT2 RAT1-RAT2)
42 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
most cases the diagnostic NPSG is doneon 1 night although NPSG on 2 con-secutive nights may be considered inthe evaluation of parasomnias
Four categories of sleep monitoringdevices for use in the diagnosis of sleepdisorders have often been described34
These are type 1 standard attended in-laboratory polysomnography type 2comprehensive portable unattendedpolysomnography type 3 modifiedportable sleep apnea testing (often car-diorespiratory studies that do not recordsleep) and type 4 continuous single ordual bioparameter recording (eg pulseoximetry) However this categorizationmay not effectively classify the plethoraof out-of-center testing devices currentlyavailable for clinical use Therefore anew device classification system hasrecently been proposed This schemaknown as the SCOPER system catego-rizes out-of-center testing devices basedon measurement of sleep cardiovascu-
lar oximetry position effort and res-piratory parameters36 Within each ofthe six SCOPER categories a level of 0through 5 is assigned as indicated bythe type of sensor or measurementthat the device uses for that category
The most recent clinical guidelinespublished by the Portable MonitoringTask Force of the AASM37 for use ofunattended portable monitoring inthe diagnosis of OSA in adult patientsrecommend that portable monitoringonly be performed in conjunction witha comprehensive sleep evaluation by(or supervised by) a practitioner board-certified in sleep medicine or eligiblefor the certification examination Theseguidelines state that portable monitor-ing may be used in place of NPSG inpatients with a high pretest probabilityof moderate to severe OSA Portablemonitoring should not be used inpatients with significant medical comor-bidities (including but not limited to
KEY POINT
h The complexclassification of portabletesting devices reflectsthe multitude of designsavailable to cliniciansand will undoubtedlychange as technologyadvances
FIGURE 2-11 A The international 10Y20 system for EEG electrode placement refers to the10 and 20 interelectrode distances Even electrode numbers (2 4 6 8)represent the right hemisphere and odd electrode numbers (1 3 5 7)
represent the left hemisphere B Recommended F4-M1 C4-M1 O2-M1 placements of EEGelectrodes as set forth by the American Academy of Sleep Medicine (AASM)
Adapted from Iber C et al American Academy of SleepMedicine35 Used with permission of the American Academy ofSleep Medicine Darien IL 2012
43Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
moderate to severe pulmonary diseaseneuromuscular disease or congestiveheart failure) in patients with othersleep disorders (including central sleepapnea periodic limb movement disor-der insomnia parasomnias circadianrhythm disorders or narcolepsy) or asa screening tool The use of portablemonitoring may be indicated for thediagnosis of OSA in patients for whomattended NPSG is not possible becauseof immobility safety or critical illnessPortable monitoring may be indi-cated to monitor the response to non-continuous positive airway pressuretreatments for OSA including oralappliances upper airway surgery andweight loss The algorithm shown inAppendix B may help in the determi-nation of an adult patientrsquos candidacyfor out-of-center testing for the diag-nosis of OSA An example of portable(or home) monitoring technology isshown in Supplemental Digital Con-tent 2-1 linkslwwcomCONTA15
Recommended technology for port-able monitoring should record at mini-mum airflow respiratory effort andblood oxygenation the airflow effortand oximetric biosensors typically usedfor attended NPSG should be used37
These guidelines published in 2007will likely continue to evolve as newtechnologies emerge and are found tobe effective The current guidelinesrecommend that out-of-center testingbe performed under the auspices of anAASM-accredited comprehensive sleepmedicine program and that a board-certifiedeligible sleep specialist reviewthe raw data from a portable monitor-ing device All patients who undergoportablemonitoring for the diagnosis ofOSA should have a follow-up visit toreview test results Negative or techni-cally inadequate portable monitoringstudies should be followed by attendedin-laboratory NPSG if the clinical suspi-cion for SDB remains high37
The aforementioned testing proce-dures are primarily used in the evalua-tion of SDB Other testing modalitiesare useful in the diagnosis of othercategories of sleep disorders The mul-tiple sleep latency test (MSLT) and itsvariant the maintenance of wakefulnesstest (MWT) are used in the evaluation ofhypersomnia The conventional record-ing montage is similar to that used fornocturnal polysomnography central fron-tal and occipital EEGs left and right eyeelectrooculograms mentalsubmentalEMG and ECG leads Measurement ofthoracic and abdominal effort oxygensaturation and nasaloral airflow are notrequired but may help explain delayedsleep latencies for patients in whomrespiratory disturbances interfere withsleep onset
The MSLT is a validated tool that isconsidered the de facto standard forobjective assessment of excessive day-time sleepiness38 The recommendedprotocol38 involves five 20-minute napopportunities held at 2-hour intervalsthroughout the day If sleep is ob-served the patient is allowed to sleepfor at least 15 minutes The sleep la-tency for each nap is measured as thetime from the start of the nap trial tothe first epoch of sleep A sleep la-tency of 20 minutes is assigned to naptrials during which no sleep isobserved39 The mean sleep latencycalculated as the average sleep latencyacross all nap trials is the final resultThe presence and number of sleep-onset REM periods (SOREMPs) is alsodetermined as this information canhelp to establish a diagnosis of narco-lepsy without cataplexy or to confirmnarcolepsy with cataplexy
The MSLT should be started 15 to30 hours following completion of anocturnal polysomnogram whichshould record at least 6 hours of sleepin order for determination of the meansleep latency to be valid Drugs that may
KEY POINT
h Careful considerationshould be given tothe indications forout-of-center testingAttended nocturnalpolysomnography isindicated if a portablestudy yields a negativeor technicallyinadequate result
44 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
interfere with sleep latency or REM la-tency should be discontinued 2 weeksbefore testing whenever possible Ascreen may be performed on the day oftesting if there is suspicion that pre-scribed or illicit substances may con-tribute to the patientrsquos sleepiness38
No large multicenter systematicallycollected normative data are availablefor mean sleep latency values on theMSLT38 Nonetheless a mean sleep la-tency of greater than 10 minutes is of-ten considered normal whereas a meansleep latency of 8 to 10 minutes is con-sidered a physiologic gray zone40 Thenormative data for children are classi-fied by Tanner stage of developmentthough the MSLT is typically not per-formed in children aged younger than 6or 7 years because some daytime nap-ping may still be normal in youngchildren41 The second edition of theInternational Classification of SleepDisorders Diagnostic and CodingManual (ICSD-2)42 requires the pres-ence of a mean sleep latency of lessthan 8 minutes and two or moreSOREMPs as part of the diagnosticcriteria for narcolepsy without cata-plexy However the ICSD-2 also notesthat a mean sleep latency of less than 8minutes may occur in up to 30 of thegeneral population Therefore whilethe MSLT is a helpful and widely usedtool it remains an imperfect gold stand-ard in the assessment of daytime sleepi-ness This necessitates that theevaluation of daytime sleepiness notrest on the MSLT results alone butassimilate the clinical history subjectivecomplaints diagnostic study results andother pertinent medical information38
Practice parameters from theAASM state that the MSLT is indicatedfor diagnostic confirmation of sus-pected narcolepsy and may be indi-cated to differentiate idiopathichypersomnia from narcolepsy38 TheMSLT is not indicated for routine
assessment of OSA syndrome or toassess response to treatment of SDBand is not routinely indicated for eval-uation of sleepiness in medical orneurologic disorders (except for narco-lepsy) insomnia or circadian rhythmdisorders
TheMWTprovides an objectivemeas-ure of a patientrsquos ability to remain awakerather than the tendency to fall asleepduring the day The key differencebetween the MWT and the MSLT is thatin the former the patient is asked to tryto stay awake under circumstances con-ducive to sleep rather than to fall asleepThe MWT provides an objective vali-dated assessment of the ability to remainawake for a defined length of time38 Therecommended protocol includes four40-minute trials that begin at 2-hourintervals with the first trial to start 15 to30 hours after the patientrsquos wake-uptime A nocturnal polysomnogram onthe preceding night is not requiredHowever the patient should obtain asufficient amount of sleep during thenight before the MWT Each trial isterminated after 40 minutes if no sleepoccurs or after unequivocal sleep onset(defined as three continuous epochsof stage N1 sleep or one epoch of anyother stage of sleep) has occurred38
One indication for the MWT is to as-sess an individualrsquos ability to remainawake when his or her inability to re-main awake constitutes a public orpersonal safety issue This can becomea pressing issue for individuals em-ployed in the transportation43 con-struction or health care industriesThe MWT may be indicated to assesstreatment response in patients withknown excessive daytime sleepiness
Limited amounts of normative dataare available for the MWT Historicallymultiple testing protocols make syn-thesis of results more challenging TheMWT is used much less often in clinicalpractice compared to the MSLT Patient
KEY POINTS
h The multiple sleeplatency test is the goldstandard for objectiveassessment of daytimesleepiness butinterpretation of theresults must be madewithin the clinicalcontext of the patientrsquoshistory
h In the multiple sleeplatency test the patientis instructed to try tosleep during each naptrial In the maintenanceof wakefulness test thepatient is instructed totry to remain awakeduring the nap trial
h A baseline nocturnalpolysomnogram isrequired before amultiple sleep latencytest and considered butnot required before amaintenance ofwakefulness test
45Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
age may also affect the mean sleep la-tency values on both the MWT and theMSLT43 and may represent evolution ofcircadian rhythm and sleep architec-ture across the lifetime A study of 383patients with narcolepsy with cataplexyexamined the clinical and polysomno-graphic data at the time of diagnosis(age range 5 to 84 years) and found aprogressive decrease in the number ofSOREMPs and a progressive increase inthe mean sleep latency on the MSLT asa function of age44 Given its limita-tions the MWT may thus be used tosupplement the clinical history in theassessment of ability to stay awake butshould not be the sole determinant ofthis parameter
Actigraphy is also used in the clinicalevaluation of patients with sleep disor-ders particularly circadian rhythm sleepdisorders An actigraph is a watchlikedevice that is worn on the wrist for anextended period usually in the range ofweeks The actigraph records move-ment and uses an algorithm to estimatethe amounts of sleep and wake timeduring the recording period Analysissoftware uses movement to estimatewhen sleep and wakefulness haveoccurred Review of the data can pro-vide objective insight into the patientrsquossleep pattern including timing andduration of major sleep disruptionsActigraphy is indicated as part of theevaluation of patients with advancedsleep-phase syndrome delayed sleep-phase syndrome and shift work disor-der and may be indicated in the evalua-tion of jet lag disorder and nonY24-hoursleep-wake syndrome including thatassociated with blindness45 It can alsoserve as a measure of treatment re-sponse in patients with insomnia andcircadian rhythm sleep disorders Forpopulations in which traditional sleepmonitoring may be challenging suchas pediatric or older adult patientsactigraphy may provide valuable infor-
mation about the patientrsquos sleep pat-tern or response to treatment Whenpolysomnography is not availableactigraphy is indicated to estimate totalsleep time in patients with OSA45
OTHER ASSESSMENTMODALITIESLaboratory evaluation and neuroimag-ing with either CT or MRI may beconsidered on an individual basis asindicated by the clinical history Com-plete blood count (CBC) serum chem-istries or measures of thyroid functionmay be obtained if an underlying med-ical disorder is thought to contribute tothe patientrsquos sleep symptoms Forinstance these laboratory studies maybe consideredwhen daytime fatigue is apredominant symptom Serum ironstudies including ferritin level shouldbe checked in patients with restless legssyndrome46 Neuroimaging should beconsidered in patients with antecedenttrauma or for any sleep disorder pa-tient with an abnormal neurologic ex-amination to evaluate for a structuraletiology of the patientrsquos symptoms
APPROACH TO THE PATIENTEvaluation of suspected sleep disordersis best accomplished by a stepwisemultidimensional approach (Case 2-2)A thorough sleep history includes de-tailed description of sleep-related symp-toms nocturnal behaviors the patientrsquossleep schedule level of daytime sleepi-ness and subsequent effects on daytimefunctioning Collateral history from thepatientrsquos bed partner or family is oftennecessary to understand the severity andcontext of the patientrsquos symptoms Sub-jective assessments of sleepiness suchas the Epworth Sleepiness Scale areeasily administered and useful to tracksymptomatic progression or treatmentresponse from one visit to the nextCertain physical examination findingsmay also raise clinical suspicion of
KEY POINTS
h Actigraphy can beuseful in evaluation andtreatment of circadianrhythm sleep disordersand in management ofinsomnia
h Neuroimaging is notroutinely indicated inthe clinical evaluation ofsleep disorders andshould be pursued on acase-by-case basis
46 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
particular sleep disorders For patientsin whom multiple sleep disorders aresuspected systematic use of diagnostictesting allows for accurate identificationof specific diagnoses In a patient withinsomnia and symptoms suggestive ofSDB nocturnal polysomnography shouldbe the first procedure performed Ifthe insomnia persists despite adequatetreatment of SDB further evaluationwith sleep diaries and possibly actigra-
phy may be considered to better char-acterize the patientrsquos sleep patternActigraphy may then again be pursuedto gauge treatment response upon man-agement of the patientrsquos insomnia
The diagnostic modalities availablefor evaluation of sleep disorders arerapidly evolving In-laboratory nocturnalpolysomnography currently remains thegold standard for assessment of SDBHowever the multitude of out-of-center
KEY POINT
h Careful assimilation ofthe clinical history thesleep-specific physicalexamination patientquestionnaires anddiagnostic test resultsleads to the mostaccurate assessment ofpatients with symptomsrelated to sleep oralertness
Case 2-2A 23-year-old woman reported a 4-year history of insomnia Throughoutcollege she was a lsquolsquonight owlrsquorsquo never scheduled classes that started before100 PM and always did well in school During the past 6 months shedeveloped progressive difficulty staying awake in her job as a financialanalyst andwas concerned about how this might affect her job performance
During the week she was in bed by midnight but was unable to fallasleep until 200 AM and awoke with difficulty to an alarm at 600 AMfeeling tired She denied any thought rumination or physical discomfortat bedtime She had tried over-the-counter sleep aids that provided nosymptomatic improvement and worsened morning grogginess Onweekends she slept from 200 AM to 1100 AM and awakened feelinglsquolsquopretty goodrsquorsquo She had nocturia up to once per night and occasionalmorning headaches She had no bed partner but reported gaspingrespirations nocturnal palpitations and snort arousals On about 4 nightsper week she experienced a sensation of needing to move her legswhile trying to fall asleep This sensation was relieved by movement andwas worse at night than during the day Her legs sometimes movedspontaneously at night or while seated quietly for long periods duringthe day She felt sleepy during the afternoon especially while workingat her computer She denied drowsiness while driving She occasionallytook a 30-minute nap on the weekend and found it to be refreshingShe drank one to two cups of coffee every morning and had a 12-oz dietcaffeinated soda at 300 PM Her sleepiness had not caused her to makeany mistakes at work and she denied any mood disturbance
Physical examination was notable for a body mass index of 32 kgm2 neckcircumference of 381 cm (15 in) and modified Mallampati class III oral airwayNasal passages were narrow with turbinate hypertrophy bilaterally andhard palate was high-arched and narrow Nomicrognathia or retrognathia waspresent She had molar occlusion class I bilaterally with no overjet or overbiteThe general cardiac respiratory and neurologic examinations were normal
Comment This case illustrates how discussion of the chief complaint raisessuspicion for multiple sleep disorders The history suggests a circadian rhythmsleep disorder particularly delayed sleep-phase syndrome sleep-disorderedbreathing and restless legs syndrome Diagnostic evaluation should includenocturnal polysomnogramwith consideration toperform testing at the patientrsquospreferred sleep time and serum iron studies Sleep diaries andor actigraphymay be considered for further assessment of the patientrsquos sleep pattern
47Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
testing devices continues to grow andmany may provide useful alternativesthat under appropriate circumstancescould allow more expedient conven-ient and less costly evaluations ofincreased numbers of patients whopreviously had only limited or delayedaccess to sleep services
VIDEO LEGENDSupplemental Digital Content 2-1
Home sleep study Video demonstrates a homesleep study using an unattended type 3 portablemonitoring device The patient is a 56-year-oldman who is experiencing morning headachesand concentration and alertness problems atwork He has a history of mild snoring and ar-terial hypertension His Epworth SleepinessScale score is 18 his neck circumference is19 in he has a Mallampati classification score ofIII and his body mass index is 41 kgm Theapnea-hypopnea index is 84 eventsh Channelsrecorded in this sleep study include arterialoxyhemoglobin saturation heart rate oral-nasalpressure flow snoring inductive plethysmog-raphy for chest efforts and body position
linkslwwcomCONTA15
B 2013 Marcel Hungs MD PhD Used withpermission
REFERENCES1 National Institutes of Health National
Center on Sleep Disorders ResearchSleep disorders research planwwwnhlbinihgovhealthprofsleep201101011NationalSleepDisordersResearch-PlanDHHSPublication11-7820pdf PublishedNovember 2011
2 Dinges DF An overview of sleepiness andaccidents J Sleep Res 19954(S2)4Y14
3 Mills RJ Young CA A medical definitionof fatigue in multiple sclerosis QJM 2008101(1)49Y60
4 Chervin RD Sleepiness fatigue tirednessand lack of energy in obstructive sleepapnea Chest 2000118(2)372Y379
5 Chotinaiwattarakul W OrsquoBrien LM Fan LChervin RD Fatigue tiredness and lack ofenergy improve with treatment for OSAJ Clin Sleep Med 20095(3)222Y227
6 American Academy of Sleep MedicineThe international classification of sleepdisorders diagnostic and coding manual2nd ed Westchester IL American Academyof Sleep Medicine 2005
7 Ebben MR Spielman AJNon-pharmacological treatments forinsomnia J Behav Med 200932(3)244Y254
8 Roth T Insomnia definition prevalenceetiology and consequences J Clin SleepMed 20073(5 suppl)S7YS10
9 Yang CM Spielman AJ Glovinsky PNonpharmacologic strategies in themanagement of insomnia Psychiatr ClinNorth Am 200629(4)895Y919 abstract viii
10 Katz ES DrsquoAmbrosio CM Pediatricobstructive sleep apnea syndrome ClinChest Med 201031(2)221Y234
11 Kohler M Bloch KE Stradling JR The role ofthe nose in the pathogenesis of obstructivesleep apnea Curr Opin Otolaryngol HeadNeck Surg 200917(1)33Y37
12 Kryger MH Atlas of clinical sleep medicinePhiladelphia PA Elsevier 2010
13 Zonato AI Martinho FL Bittencourt LRet al Head and neck physical examinationcomparison between nonapneic andobstructive sleep apnea patientsLaryngoscope 2005115(6)1030Y1034
14 Mallampati SR Gatt SP Gugino LD et alA clinical sign to predict difficult trachealintubation a prospective study Can AnaesthSoc J 198532(4)429Y434
15 Samsoon GL Young JR Difficult trachealintubation a retrospective studyAnaesthesia 198742(5)487Y490
16 Huang HH Lee MS Shih YL et alModified Mallampati classificationas a clinical predictor of peroralesophagogastroduodenoscopy toleranceBMC Gastroenterol 20111112
17 Friedman M Ibrahim H Bass L Clinicalstaging for sleep-disordered breathingOtolaryngol Head Neck Surg 2002127(1)13Y21
18 Cheng RHW Yiu CKY Leung WKOral health in individuals with Downsyndrome In Dey S ed Prenatal diagnosisand screening for down syndromeInTech wwwintechopencombookshowtoreferenceprenatal-diagnosis-and-screening-for-down-syndromeoral-health-in-individuals-with-down-syndromePublished 2011 Accessed August 24 2012
19 Katz I Stradling J Slutsky AS et al Dopatients with obstructive sleep apneahave thick necks Am Rev Respir Dis1990141(5 pt 1)1228Y1231
20 Kushida CA Efron B Guilleminault C Apredictive morphometric model for theobstructive sleep apnea syndrome AnnIntern Med 1997127(8 pt 1)581Y587
48 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
21 Saccucci M Tettamanti L Mummolo S et alScoliosis and dental occlusion a review ofthe literature Scoliosis 2011615
22 Battagel JM Kotecha B Dental side-effectsof mandibular advancement splint wear inpatients who snore Clin Otolaryngol200530(2)149Y156
23 Morcos SS Patel PK The vocabulary ofdentofacial deformities Clin Plast Surg200734(3)589Y599
24 Epstein LJ Kristo D Strollo PJ Jr et alClinical guideline for the evaluationmanagement and long-term care ofobstructive sleep apnea in adults J ClinSleep Med 20095(3)263Y276
25 Johns MW A new method for measuringdaytime sleepiness the Epworth sleepinessscale Sleep 199114(6)540Y545
26 Johns MW Daytime sleepiness snoring andobstructive sleep apnea The EpworthSleepiness Scale Chest 1993103(1)30Y36
27 Chervin RD Aldrich MS The EpworthSleepiness Scale may not reflect objectivemeasures of sleepiness or sleep apneaNeurology 199952(1)125Y131
28 Buysse DJ Reynolds CF 3rd Monk THet al The Pittsburgh Sleep Quality Index anew instrument for psychiatric practice andresearch Psychiatry Res 198928(2)193Y213
29 Chervin RD Hedger K Dillon JE Pituch KJPediatric sleep questionnaire (PSQ) validityand reliability of scales for sleep-disorderedbreathing snoring sleepiness and behavioralproblems Sleep Med 20001(1)21Y32
30 Chung F Yegneswaran B Liao P et al STOPquestionnaire a tool to screen patients forobstructive sleep apnea Anesthesiology2008108(5)812Y821
31 Walters AS LeBrocq C Dhar A et alValidation of the International Restless LegsSyndrome Study Group rating scale forrestless legs syndrome Sleep Med 20034(2)121Y132
32 Bastien CH Vallieres A Morin CMValidation of the Insomnia Severity Indexas an outcome measure for insomniaresearch Sleep Med 20012(4)297Y307
33 YOURSLEEPaasmnetorg from the AmericanAcademy of Sleep Medicine Two weeksleep diary yoursleepaasmnetorgpdfsleepdiarypdf Accessed August 24 2012
34 Kushida CA Littner MR Morgenthaler Tet al Practice parameters for the indicationsfor polysomnography and relatedprocedures an update for 2005 Sleep200528(4)499Y521
35 Iber C Ancoli-Israel S Chesson A et alThe AASM manual for scoring of sleep andassociated events rules terminology andtechnical specifications 1st ed WestchesterIL American Academy of Sleep Medicine2007
36 Collop NA Tracy SL Kapur V et alObstructive sleep apnea devices forout-of-center (OOC) testing technologyevaluation J Clin Sleep Med 20117(5)531Y548
37 Collop NA Anderson WM Boehlecke Bet al Clinical guidelines for the use ofunattended portable monitors in thediagnosis of obstructive sleep apnea in adultpatients Portable Monitoring Task Forceof the American Academy of SleepMedicine J Clin Sleep Med 20073(7)737Y747
38 Littner MR Kushida C Wise M et alStandards of Practice Committee of theAmerican Academy of Sleep MedicinePractice parameters for clinical use of themultiple sleep latency test and themaintenance of wakefulness test Sleep200528(1)113Y121
39 Carskadon MA Dement WC Mitler MMet al Guidelines for the multiple sleeplatency test (MSLT) a standard measure ofsleepiness Sleep 19869(4)519Y524
40 van den Hoed J Kraemer H Guilleminault Cet al Disorders of excessive daytimesomnolence polygraphic and clinical datafor 100 patients Sleep 19814(1)23Y37
41 Hoban TF Chervin RD Assessment ofsleepiness in children Semin PediatrNeurol 20018(4)216Y228
42 ICSD-2 The international classification ofsleep disorders pocket version diagnosticand coding manual 2nd ed WestchesterIL American Academy of Sleep Medicine2005
43 Arand D Bonnet M Hurwitz T et alThe clinical use of the MSLT and MWTSleep 200528(1)123Y144
44 Dauvilliers Y Gosselin A Paquet J et alEffect of age on MSLT results in patientswith narcolepsy-cataplexy Neurology200462(1)46Y50
45 Morgenthaler T Alessi C Friedman Let al Practice parameters for the use ofactigraphy in the assessment of sleep andsleep disorders an update for 2007 Sleep200730(4)519Y529
46 Gamaldo CE Earley CJ Restless legssyndrome a clinical update Chest2006130(5)1596Y1604
49Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited

such as sleepwalking driving or cook-ing while asleep or dream-enactmentbehavior If the patient reports suchbehavior further inquiry must be madeabout the frequency of these events andany history of injury sustained due to thesleep-related behavior Details of thesleep history permit a thorough differ-ential diagnosis and can also guide adiscussion of safety concerns
PHYSICAL EXAMINATIONA comprehensive multisystem exami-nation is an important aspect of thesleep evaluation Measurement of theweight height body mass index (BMI)neck circumference and blood pres-sure and heart rate should be per-formed for nearly all patients withsymptoms related to sleep or alertnessOther salient features of the generalexamination include auscultation forany cardiac or respiratory abnormalitiesand identification of peripheral edemaA focused neurologic examinationshould be guided by the patientrsquos his-tory For instance a mental status as-sessment should be considered if apatient with excessive daytime sleepi-ness also complains of memory loss If apatient with a history of diabetes melli-
tus endorses symptoms of restless legssyndrome it is worthwhile to assess forstocking-glove distribution sensory lossand weakness
Detailed examination of the headand neck should be performed as partof a comprehensive sleep evaluationThe patientrsquos facial morphology shouldbe assessed for features of long facesyndrome which includes infraorbitaldarkening mouth breathing elongatedmidface and nasal atrophy10 A 2009review11 reports that previous observa-tional and cross-sectional studies haveshown a relationship between chronicnasal obstruction and OSA Thus a thor-ough nasal examination should be per-formed on patients with sleep-relatedcomplaints Examination of the nasalairway should include evaluation forsymmetry of the nares nasal septum de-viation (Figure 2-1)12 and nasal turbi-nate hypertrophy A bedside assessmentof nasal airflow can be accomplished by
KEY POINT
h Details of facialmorphology nasalairway patency and oralairway crowding arekey features of thesleep-specificexamination
FIGURE 2-1 Nasal septal deviation Thisstructural abnormality canpredispose a patient to havesleep-disordered breathing
Reprinted from Kryger MH Elsevier12 B 2010 withpermission from Elsevier
FIGURE 2-2 Retrognathia Retrognathiais derived from the termslsquolsquoretrorsquorsquo (backward) and
lsquolsquognathosrsquorsquo (jaw) With retrognathia one orboth jaws recede with respect to the frontalplane of the forehead The condition maypredispose a patient to obstruction of theairway and sleep apnea by displacing thetongue against the retropharyngeal regioncompromising airflow Retrognathia issometimes corrected through surgicalrepositioning or advancement of themandible
Reprinted from Kryger MH Elsevier12 B 2010 withpermission from Elsevier
36 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
asking the patient to press the indexfinger against the left nostril and take adeep breath in on the right side thisshould be repeated on the oppositeside as well The patientrsquos facial mor-phology should be assessed for man-dibular retrognathia (Figure 2-2)12 Withthe patientrsquos head in a neutral posi-tion a virtual line is drawn from thevermillion border of the lower lip tothe chin Mandibular retrognathia issuggested if the anterior prominence ofthe chin is 2 mm or more behind thevirtual line13
The modified Mallampati classifica-tion is commonly used for assessmentof the oral airway in patients withsuspected SDB The Mallampati classi-fication14 was developed to identifypatients in whom tracheal intubationwould be difficult the initial description
divided patients into three classes Twoyears later15 this was modified to de-scribe four groups class I class II classIII and class IV Figure 2-3 16 illustratesthe modified Mallampati classificationassessed with the tongue protrudedThe Friedman palate position classifi-cation17 also commonly referencedutilizes the same four categories but isdone with the tongue at rest and notextended Either the Mallampati orFriedman classification may be used todescribe the patency of the oral airway
Tonsils should be classified based onthe degree of hypertrophy (Figure 2-4)12grade I tonsils are inside the tonsillarfossa lateral to the posterior pillarsgrade II tonsils occupy 25 of theoropharynx grade III tonsils occupy50 of the oropharynx and grade IVtonsils occupy at least 75 of the
FIGURE 2-3 Modified Mallampati classification The class is determined by looking at theanatomy of the oral cavity and describes tongue size relative to oropharyngealsize The test is conducted with the patient seated the head held in a neutral
position and the mouth wide open and relaxed The subsequent classification is assigned basedupon the pharyngeal structures that are visible
Reprinted from Huang HH et al BMC Gastroenterol16 B 2011 BioMed Central Ltd wwwbiomedcentralcom1471-230X1112
37Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
oropharynx and nearly meet in the mid-line13 A high-arched narrow hard pal-ate (Figure 2-5)18 may predispose thepatient to have SDB Katz and col-leagues19 have shown that patients withOSA have significantly increased neckcircumference compared to nonapneicsnorers greater distribution of neck fat
may contribute to mass loading on theupper airway in patients with OSA Thepatientrsquos neck circumference should bemeasured at the superior border of thecricothyroid membrane19 A neck cir-cumference greater than 40 cm (157in) has been shown to be predictive ofOSA with 61 sensitivity and 93specificity regardless of sex20
Assessment of the patientrsquos anteriorand posterior dentition can also re-veal anatomic findings that may pre-dispose a person to certain sleepdisorders Two features to note in eval-uation of the anterior dentition areoverjet and overbite (Figure 2-6)21
Overjet as shown in Figure 2-712 isthe horizontal distance between theupper right central incisor and thebuccal surface of the correspondinglower tooth while overbite is the ver-tical distance between these twopoints22 These measurements are typ-ically reported in millimeters The An-gle classification system is used todescribe the first molar position on
FIGURE 2-4 Tonsil size grading Thisstructural abnormality canpredispose a patient to havesleep-disordered breathing
Reprinted from Kryger MH Elsevier12 B 2010 withpermission from Elsevier
FIGURE 2-5 Deficientmaxillarydevelopment inan individual with
Down syndrome leading to highand narrow hard palate
Reprinted with permission from ChengRHW et al InTech18 B 2011 W KeungLeung wwwintechopencombooksprenatal-diagnosis-and-screening-for-down-syndromeoral-health-in-individuals-with-down-syndrome
FIGURE 2-6 Overjet andoverbite Overjetis defined as
increased projection of the upperteeth in front of the lower teethas measured parallel to theocclusal plane Overbite is thevertical overlapping of maxillaryteeth over mandibular teethusually measured perpendicularto the occlusal plane
Reprinted from Saccucci M et al Scoliosis21
B 2011 BioMed Central Ltd wwwscoliosisjournalcomcontent6115
38 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
the mandibular and maxillary dentalarches23 Figure 2-8 shows class I oc-clusion and class II and III malocclu-
sion Of note the mesiobuccal surfaceis the aspect of the tooth that is adja-cent to the cheek mucosa
The Adult Obstructive Sleep ApneaTask Force of the American Academyof Sleep Medicine (AASM) recommen-ded in recent clinical guidelines24 thatthe following physical findings maysuggest the presence of OSA increasedneck circumference (greater than 432cm [17 in] in men greater than 406 cm[16 in] in women) BMI 30 kgm2 orgreater modified Mallampati classifica-tion of III or IV presence of retrognathialateral peritonsillar narrowing macro-glossia tonsillar hypertrophy elongatedenlarged uvula high-archednarrowhard palate nasal abnormalities (egpolyps deviation valve abnormalities
KEY POINT
h Classification of thepatientrsquos dentition helpsto evaluate the positionof the maxillary archrelative to themandibular arch
FIGURE 2-7 OverjetDisplacementof the
mandibular teeth posteriorly inrelationship to the maxillary teethresults inmoreposteriorly crowdedupper airways predisposingpatients for the developmentof obstructive sleep apnea
Reprinted from Kryger MH Elsevier12
B 2010 with permission from Elsevier
FIGURE 2-8 Angle class occlusionmalocclusion A Angle class I occlusion also known asneutrocclusion The mandibular and maxillary dental arches have a normalanterior-posterior relationship The mesiobuccal groove of the mandibular first
molar interdigitates with the mesiobuccal cusp of the maxillary first molar B Angle class IImalocclusion also known as distoclusion The mandibular dental arch is in distal anterior-posteriorrelationship to the maxillary dental arch The mesiobuccal groove of the mandibular first molar isdistal to the mesiobuccal cusp of the maxillary first molar C Angle class III malocclusion alsoknown as mesioclusion The mandibular dental arch is in mesial anterior-posterior relationship tothe maxillary dental arch The mesiobuccal groove of the mandibular first molar is mesial to themesiobuccal cusp of the maxillary first molar
Reprinted fromMorcos SS Patel PK Clin Plast Surg23 B 2007 with permission from Elsevier wwwsciencedirectcomsciencearticlepiiS0094129807000843
39Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
and turbinate hypertrophy) andoroverjet To prevent overlooking thesefindings a thorough head and neckassessment as described in Table 2-2should be incorporated into the phys-ical examination of all patients whopresent with sleep-related complaints
SUBJECTIVE ASSESSMENTSeveral patient-completed question-naires are inexpensive and time-efficient
reasonably well validated and com-monly used They can help to increasestandardization in evaluations of patientsby different clinicians or across centersPerhaps the most well-known andwidely used is the Epworth SleepinessScale25 a subjective assessment of thepatientrsquos daytime sleep propensity inrecent times As shown in Appendix Athe Epworth Sleepiness Scale asks theresponder to use a four-point Likertscale (0 1 2 or 3) to indicate thelikelihood of dozing in eight distinctsedentary conditions A total score of 10or greater out of a possible 24 suggestsexcessive daytime sleepiness25 Whilethe Epworth Sleepiness Scale score canbe easily incorporated into the clinicalevaluation it should not be used as asubstitute for objective measurement ofsleepiness The Epworth Sleepiness Scalescore may correlate to a limited extentwith the presence and severity of OSA26
but some studies have failed to find anystatistically significant association withmean sleep latency on multiple sleep la-tency tests or with severity of OSA27
The most advantageous use of theEpworth Sleepiness Scale may be to followan individualrsquos self-assessment of sleep-iness longitudinally and it may also serveas an indicator of treatment response
Many other questionnaires may beutilized in a clinical sleep evaluationsome pertain to overall sleep qualitywhile others are disorder-specific ThePatient Reported Outcomes Measure-ment Information System (PROMIS) isan NIH-supported system of measuresfor patient-reported health status andincludes questions on sleep disturb-ance The Pittsburgh Sleep QualityIndex (PSQI) is a validated question-naire that inquires about sleep qualityand disturbances over the previousmonth28 The parent-completed Pe-diatric Sleep Questionnaire29 containsa validated reliable 22-item scale tohelp assess risk for SDB in children
KEY POINTS
h The Epworth SleepinessScale apatient-completedquestionnaire assessesthe patientrsquos subjectivetendency to doze duringsedentary situations inrecent times not onlyat the moment thequestionnaire iscompleted
h The Epworth SleepinessScale should not beused in lieu of diagnostictesting but may be avaluable componentof ongoing clinicalevaluation
TABLE 2-2 Head and NeckExamination
b Face
Featuresof long face syndrome
Infraorbital darkening
Mouth breathing
Elongated midface
Nasal atrophy
b Oral Airway
Mandibular retrognathia
Low soft palate (modifiedMallampati classification)
Large or boggy uvula
Erythematous pillars
Tonsillar hypertrophy
High narrow hard palate
Neck circumference
Overjet
Overbite
Angle classification(malocclusion)
Macroglossia
Worn occlusive surfaces(suggestive of bruxism)
b Nasal Airway
Symmetry of the nares
Nasal septum deviation
Nasal airflow
Collapse of nasal alae oninspiration
b Neck
Neck circumference
40 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
The STOP-BANG questionnaire devel-oped and validated in preoperativepatients is a sensitive screening toolfor OSA Four questions address snor-ing tiredness during daytime observedapnea and high blood pressure whereasfour other measures focus on increasedOSA risk factors of BMI (greater than 35kgm2) age (older than 50 years) neckcircumference (greater than 40 cm[1575 in]) and gender (male preva-lence)30 The International RestlessLegs Syndrome Study Group Rating Scale(IRLS) is a validated assessment of dis-ease severity for patients with restlesslegs syndrome31 The patientrsquos perceived
level of insomnia may be assessed withthe Insomnia Severity Index (ISI) avalidated 7-item questionnaire32
A sleep diary (Figure 2-9)33 allows apatient to chart daily sleep and waketimes and should be maintained for atleast 2 consecutive weeks Review ofthis information allows the clinicianto estimate the total amount of sleepthe patient obtains in a 24-hour pe-riod The sleep diary also can provideinsight into the patientrsquos sleep patternIs sleep obtained at the same timesevery day Is the patientrsquos sleep con-solidated or fragmented across 24hours Does the patient sleep and
FIGURE 2-9 Sleep diary completed by a 46-year-old woman who presented with difficulty falling asleep Vertical linesrepresent when the patient went to bed lsquolsquoMrsquorsquo refers to when medication was taken black shading representstime asleep and unshaded white areas are time spent awake
Diary template reprinted from YOURSLEEPaasmnetorg from the American Academy of Sleep Medicine yoursleepaasmnetorgpdfsleepdiarypdf33
41Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
wake at conventional times or doeshe or she appear to be a lsquolsquonight owlrsquorsquoor lsquolsquomorning larkrsquorsquo Answers to thesequestions as provided by the sleepdiary may reveal factors that contrib-ute to sleep-related concerns Use ofsleep diaries can be particularly help-ful in patients with suspected circadianrhythm sleep disorders (including shiftwork) behaviorally induced insufficientsleep or inadequate sleep hygiene
OBJECTIVE MEASURESNocturnal polysomnography (NPSG)or related assessments are indicatedfor the diagnosis and assessment ofSDB and for positive airway titrationin patients with confirmed SDB Theprocedure can also provide informationabout EEG activity nocturnal move-ments cardiac rhythm and oxygen
saturation34 The recommended record-ing montage used in NPSG as shownin Figure 2-10 includes central (C3-A2C4-A1) frontal (F3-A2 F4-A1) andoccipital (O1-A2 O2-A1) EEGs left andright eye electrooculograms mentalsubmental surface EMG and ECG leadsOther recorded parameters includethoracic and abdominal effort oxygensaturation nasaloral airflow and bodyposition Use of a microphone torecord snoring is recommended butnot required34 A full 16-lead EEG(Figure 2-11)35 and video recordingmay be performed when nocturnalseizures are suspected Leg surfaceEMG leads are recommended andadditional arm EMG leads may beapplied when the clinical history sug-gests complex sleep-related motor be-haviors such as dream enactment In
KEY POINT
h A daily sleep diary helpsto summarize a patientrsquossleep-wake schedulemore accurately thanmemory often allowsand can facilitateconstruction ofpersonalized plansfor management ofcircadian rhythm sleepdisorders and insomnia
FIGURE 2-10 A 1-minute epoch from a nocturnal polysomnogram showing obstructive sleepapnea in a 46-year-old man who presented with snoring daytime sleepinessand headaches It depicts the standard recording montage that includes the
following leads central (C3-M2 C4-M1) frontal (F3-M2 F4-M1) and occipital (O1-M2 O2-M1)EEGs left and right eye electrooculograms (E1-M2 E2-M1) mentalsubmental electromyogram(Chin1-Chin2) electrocardiogram (ECG1-ECG2 ECG2-ECG3) snore volume (SNORE) nasalpressure transducer (NPRE) nasaloral airflow (NO) thoracic (THOR) and abdominal (ABD)effort arterial oxyhemoglobin saturation (SpO2) plethysmography (Pleth) and left and right eyeelectromyograms (LAT1-LAT2 RAT1-RAT2)
42 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
most cases the diagnostic NPSG is doneon 1 night although NPSG on 2 con-secutive nights may be considered inthe evaluation of parasomnias
Four categories of sleep monitoringdevices for use in the diagnosis of sleepdisorders have often been described34
These are type 1 standard attended in-laboratory polysomnography type 2comprehensive portable unattendedpolysomnography type 3 modifiedportable sleep apnea testing (often car-diorespiratory studies that do not recordsleep) and type 4 continuous single ordual bioparameter recording (eg pulseoximetry) However this categorizationmay not effectively classify the plethoraof out-of-center testing devices currentlyavailable for clinical use Therefore anew device classification system hasrecently been proposed This schemaknown as the SCOPER system catego-rizes out-of-center testing devices basedon measurement of sleep cardiovascu-
lar oximetry position effort and res-piratory parameters36 Within each ofthe six SCOPER categories a level of 0through 5 is assigned as indicated bythe type of sensor or measurementthat the device uses for that category
The most recent clinical guidelinespublished by the Portable MonitoringTask Force of the AASM37 for use ofunattended portable monitoring inthe diagnosis of OSA in adult patientsrecommend that portable monitoringonly be performed in conjunction witha comprehensive sleep evaluation by(or supervised by) a practitioner board-certified in sleep medicine or eligiblefor the certification examination Theseguidelines state that portable monitor-ing may be used in place of NPSG inpatients with a high pretest probabilityof moderate to severe OSA Portablemonitoring should not be used inpatients with significant medical comor-bidities (including but not limited to
KEY POINT
h The complexclassification of portabletesting devices reflectsthe multitude of designsavailable to cliniciansand will undoubtedlychange as technologyadvances
FIGURE 2-11 A The international 10Y20 system for EEG electrode placement refers to the10 and 20 interelectrode distances Even electrode numbers (2 4 6 8)represent the right hemisphere and odd electrode numbers (1 3 5 7)
represent the left hemisphere B Recommended F4-M1 C4-M1 O2-M1 placements of EEGelectrodes as set forth by the American Academy of Sleep Medicine (AASM)
Adapted from Iber C et al American Academy of SleepMedicine35 Used with permission of the American Academy ofSleep Medicine Darien IL 2012
43Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
moderate to severe pulmonary diseaseneuromuscular disease or congestiveheart failure) in patients with othersleep disorders (including central sleepapnea periodic limb movement disor-der insomnia parasomnias circadianrhythm disorders or narcolepsy) or asa screening tool The use of portablemonitoring may be indicated for thediagnosis of OSA in patients for whomattended NPSG is not possible becauseof immobility safety or critical illnessPortable monitoring may be indi-cated to monitor the response to non-continuous positive airway pressuretreatments for OSA including oralappliances upper airway surgery andweight loss The algorithm shown inAppendix B may help in the determi-nation of an adult patientrsquos candidacyfor out-of-center testing for the diag-nosis of OSA An example of portable(or home) monitoring technology isshown in Supplemental Digital Con-tent 2-1 linkslwwcomCONTA15
Recommended technology for port-able monitoring should record at mini-mum airflow respiratory effort andblood oxygenation the airflow effortand oximetric biosensors typically usedfor attended NPSG should be used37
These guidelines published in 2007will likely continue to evolve as newtechnologies emerge and are found tobe effective The current guidelinesrecommend that out-of-center testingbe performed under the auspices of anAASM-accredited comprehensive sleepmedicine program and that a board-certifiedeligible sleep specialist reviewthe raw data from a portable monitor-ing device All patients who undergoportablemonitoring for the diagnosis ofOSA should have a follow-up visit toreview test results Negative or techni-cally inadequate portable monitoringstudies should be followed by attendedin-laboratory NPSG if the clinical suspi-cion for SDB remains high37
The aforementioned testing proce-dures are primarily used in the evalua-tion of SDB Other testing modalitiesare useful in the diagnosis of othercategories of sleep disorders The mul-tiple sleep latency test (MSLT) and itsvariant the maintenance of wakefulnesstest (MWT) are used in the evaluation ofhypersomnia The conventional record-ing montage is similar to that used fornocturnal polysomnography central fron-tal and occipital EEGs left and right eyeelectrooculograms mentalsubmentalEMG and ECG leads Measurement ofthoracic and abdominal effort oxygensaturation and nasaloral airflow are notrequired but may help explain delayedsleep latencies for patients in whomrespiratory disturbances interfere withsleep onset
The MSLT is a validated tool that isconsidered the de facto standard forobjective assessment of excessive day-time sleepiness38 The recommendedprotocol38 involves five 20-minute napopportunities held at 2-hour intervalsthroughout the day If sleep is ob-served the patient is allowed to sleepfor at least 15 minutes The sleep la-tency for each nap is measured as thetime from the start of the nap trial tothe first epoch of sleep A sleep la-tency of 20 minutes is assigned to naptrials during which no sleep isobserved39 The mean sleep latencycalculated as the average sleep latencyacross all nap trials is the final resultThe presence and number of sleep-onset REM periods (SOREMPs) is alsodetermined as this information canhelp to establish a diagnosis of narco-lepsy without cataplexy or to confirmnarcolepsy with cataplexy
The MSLT should be started 15 to30 hours following completion of anocturnal polysomnogram whichshould record at least 6 hours of sleepin order for determination of the meansleep latency to be valid Drugs that may
KEY POINT
h Careful considerationshould be given tothe indications forout-of-center testingAttended nocturnalpolysomnography isindicated if a portablestudy yields a negativeor technicallyinadequate result
44 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
interfere with sleep latency or REM la-tency should be discontinued 2 weeksbefore testing whenever possible Ascreen may be performed on the day oftesting if there is suspicion that pre-scribed or illicit substances may con-tribute to the patientrsquos sleepiness38
No large multicenter systematicallycollected normative data are availablefor mean sleep latency values on theMSLT38 Nonetheless a mean sleep la-tency of greater than 10 minutes is of-ten considered normal whereas a meansleep latency of 8 to 10 minutes is con-sidered a physiologic gray zone40 Thenormative data for children are classi-fied by Tanner stage of developmentthough the MSLT is typically not per-formed in children aged younger than 6or 7 years because some daytime nap-ping may still be normal in youngchildren41 The second edition of theInternational Classification of SleepDisorders Diagnostic and CodingManual (ICSD-2)42 requires the pres-ence of a mean sleep latency of lessthan 8 minutes and two or moreSOREMPs as part of the diagnosticcriteria for narcolepsy without cata-plexy However the ICSD-2 also notesthat a mean sleep latency of less than 8minutes may occur in up to 30 of thegeneral population Therefore whilethe MSLT is a helpful and widely usedtool it remains an imperfect gold stand-ard in the assessment of daytime sleepi-ness This necessitates that theevaluation of daytime sleepiness notrest on the MSLT results alone butassimilate the clinical history subjectivecomplaints diagnostic study results andother pertinent medical information38
Practice parameters from theAASM state that the MSLT is indicatedfor diagnostic confirmation of sus-pected narcolepsy and may be indi-cated to differentiate idiopathichypersomnia from narcolepsy38 TheMSLT is not indicated for routine
assessment of OSA syndrome or toassess response to treatment of SDBand is not routinely indicated for eval-uation of sleepiness in medical orneurologic disorders (except for narco-lepsy) insomnia or circadian rhythmdisorders
TheMWTprovides an objectivemeas-ure of a patientrsquos ability to remain awakerather than the tendency to fall asleepduring the day The key differencebetween the MWT and the MSLT is thatin the former the patient is asked to tryto stay awake under circumstances con-ducive to sleep rather than to fall asleepThe MWT provides an objective vali-dated assessment of the ability to remainawake for a defined length of time38 Therecommended protocol includes four40-minute trials that begin at 2-hourintervals with the first trial to start 15 to30 hours after the patientrsquos wake-uptime A nocturnal polysomnogram onthe preceding night is not requiredHowever the patient should obtain asufficient amount of sleep during thenight before the MWT Each trial isterminated after 40 minutes if no sleepoccurs or after unequivocal sleep onset(defined as three continuous epochsof stage N1 sleep or one epoch of anyother stage of sleep) has occurred38
One indication for the MWT is to as-sess an individualrsquos ability to remainawake when his or her inability to re-main awake constitutes a public orpersonal safety issue This can becomea pressing issue for individuals em-ployed in the transportation43 con-struction or health care industriesThe MWT may be indicated to assesstreatment response in patients withknown excessive daytime sleepiness
Limited amounts of normative dataare available for the MWT Historicallymultiple testing protocols make syn-thesis of results more challenging TheMWT is used much less often in clinicalpractice compared to the MSLT Patient
KEY POINTS
h The multiple sleeplatency test is the goldstandard for objectiveassessment of daytimesleepiness butinterpretation of theresults must be madewithin the clinicalcontext of the patientrsquoshistory
h In the multiple sleeplatency test the patientis instructed to try tosleep during each naptrial In the maintenanceof wakefulness test thepatient is instructed totry to remain awakeduring the nap trial
h A baseline nocturnalpolysomnogram isrequired before amultiple sleep latencytest and considered butnot required before amaintenance ofwakefulness test
45Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
age may also affect the mean sleep la-tency values on both the MWT and theMSLT43 and may represent evolution ofcircadian rhythm and sleep architec-ture across the lifetime A study of 383patients with narcolepsy with cataplexyexamined the clinical and polysomno-graphic data at the time of diagnosis(age range 5 to 84 years) and found aprogressive decrease in the number ofSOREMPs and a progressive increase inthe mean sleep latency on the MSLT asa function of age44 Given its limita-tions the MWT may thus be used tosupplement the clinical history in theassessment of ability to stay awake butshould not be the sole determinant ofthis parameter
Actigraphy is also used in the clinicalevaluation of patients with sleep disor-ders particularly circadian rhythm sleepdisorders An actigraph is a watchlikedevice that is worn on the wrist for anextended period usually in the range ofweeks The actigraph records move-ment and uses an algorithm to estimatethe amounts of sleep and wake timeduring the recording period Analysissoftware uses movement to estimatewhen sleep and wakefulness haveoccurred Review of the data can pro-vide objective insight into the patientrsquossleep pattern including timing andduration of major sleep disruptionsActigraphy is indicated as part of theevaluation of patients with advancedsleep-phase syndrome delayed sleep-phase syndrome and shift work disor-der and may be indicated in the evalua-tion of jet lag disorder and nonY24-hoursleep-wake syndrome including thatassociated with blindness45 It can alsoserve as a measure of treatment re-sponse in patients with insomnia andcircadian rhythm sleep disorders Forpopulations in which traditional sleepmonitoring may be challenging suchas pediatric or older adult patientsactigraphy may provide valuable infor-
mation about the patientrsquos sleep pat-tern or response to treatment Whenpolysomnography is not availableactigraphy is indicated to estimate totalsleep time in patients with OSA45
OTHER ASSESSMENTMODALITIESLaboratory evaluation and neuroimag-ing with either CT or MRI may beconsidered on an individual basis asindicated by the clinical history Com-plete blood count (CBC) serum chem-istries or measures of thyroid functionmay be obtained if an underlying med-ical disorder is thought to contribute tothe patientrsquos sleep symptoms Forinstance these laboratory studies maybe consideredwhen daytime fatigue is apredominant symptom Serum ironstudies including ferritin level shouldbe checked in patients with restless legssyndrome46 Neuroimaging should beconsidered in patients with antecedenttrauma or for any sleep disorder pa-tient with an abnormal neurologic ex-amination to evaluate for a structuraletiology of the patientrsquos symptoms
APPROACH TO THE PATIENTEvaluation of suspected sleep disordersis best accomplished by a stepwisemultidimensional approach (Case 2-2)A thorough sleep history includes de-tailed description of sleep-related symp-toms nocturnal behaviors the patientrsquossleep schedule level of daytime sleepi-ness and subsequent effects on daytimefunctioning Collateral history from thepatientrsquos bed partner or family is oftennecessary to understand the severity andcontext of the patientrsquos symptoms Sub-jective assessments of sleepiness suchas the Epworth Sleepiness Scale areeasily administered and useful to tracksymptomatic progression or treatmentresponse from one visit to the nextCertain physical examination findingsmay also raise clinical suspicion of
KEY POINTS
h Actigraphy can beuseful in evaluation andtreatment of circadianrhythm sleep disordersand in management ofinsomnia
h Neuroimaging is notroutinely indicated inthe clinical evaluation ofsleep disorders andshould be pursued on acase-by-case basis
46 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
particular sleep disorders For patientsin whom multiple sleep disorders aresuspected systematic use of diagnostictesting allows for accurate identificationof specific diagnoses In a patient withinsomnia and symptoms suggestive ofSDB nocturnal polysomnography shouldbe the first procedure performed Ifthe insomnia persists despite adequatetreatment of SDB further evaluationwith sleep diaries and possibly actigra-
phy may be considered to better char-acterize the patientrsquos sleep patternActigraphy may then again be pursuedto gauge treatment response upon man-agement of the patientrsquos insomnia
The diagnostic modalities availablefor evaluation of sleep disorders arerapidly evolving In-laboratory nocturnalpolysomnography currently remains thegold standard for assessment of SDBHowever the multitude of out-of-center
KEY POINT
h Careful assimilation ofthe clinical history thesleep-specific physicalexamination patientquestionnaires anddiagnostic test resultsleads to the mostaccurate assessment ofpatients with symptomsrelated to sleep oralertness
Case 2-2A 23-year-old woman reported a 4-year history of insomnia Throughoutcollege she was a lsquolsquonight owlrsquorsquo never scheduled classes that started before100 PM and always did well in school During the past 6 months shedeveloped progressive difficulty staying awake in her job as a financialanalyst andwas concerned about how this might affect her job performance
During the week she was in bed by midnight but was unable to fallasleep until 200 AM and awoke with difficulty to an alarm at 600 AMfeeling tired She denied any thought rumination or physical discomfortat bedtime She had tried over-the-counter sleep aids that provided nosymptomatic improvement and worsened morning grogginess Onweekends she slept from 200 AM to 1100 AM and awakened feelinglsquolsquopretty goodrsquorsquo She had nocturia up to once per night and occasionalmorning headaches She had no bed partner but reported gaspingrespirations nocturnal palpitations and snort arousals On about 4 nightsper week she experienced a sensation of needing to move her legswhile trying to fall asleep This sensation was relieved by movement andwas worse at night than during the day Her legs sometimes movedspontaneously at night or while seated quietly for long periods duringthe day She felt sleepy during the afternoon especially while workingat her computer She denied drowsiness while driving She occasionallytook a 30-minute nap on the weekend and found it to be refreshingShe drank one to two cups of coffee every morning and had a 12-oz dietcaffeinated soda at 300 PM Her sleepiness had not caused her to makeany mistakes at work and she denied any mood disturbance
Physical examination was notable for a body mass index of 32 kgm2 neckcircumference of 381 cm (15 in) and modified Mallampati class III oral airwayNasal passages were narrow with turbinate hypertrophy bilaterally andhard palate was high-arched and narrow Nomicrognathia or retrognathia waspresent She had molar occlusion class I bilaterally with no overjet or overbiteThe general cardiac respiratory and neurologic examinations were normal
Comment This case illustrates how discussion of the chief complaint raisessuspicion for multiple sleep disorders The history suggests a circadian rhythmsleep disorder particularly delayed sleep-phase syndrome sleep-disorderedbreathing and restless legs syndrome Diagnostic evaluation should includenocturnal polysomnogramwith consideration toperform testing at the patientrsquospreferred sleep time and serum iron studies Sleep diaries andor actigraphymay be considered for further assessment of the patientrsquos sleep pattern
47Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
testing devices continues to grow andmany may provide useful alternativesthat under appropriate circumstancescould allow more expedient conven-ient and less costly evaluations ofincreased numbers of patients whopreviously had only limited or delayedaccess to sleep services
VIDEO LEGENDSupplemental Digital Content 2-1
Home sleep study Video demonstrates a homesleep study using an unattended type 3 portablemonitoring device The patient is a 56-year-oldman who is experiencing morning headachesand concentration and alertness problems atwork He has a history of mild snoring and ar-terial hypertension His Epworth SleepinessScale score is 18 his neck circumference is19 in he has a Mallampati classification score ofIII and his body mass index is 41 kgm Theapnea-hypopnea index is 84 eventsh Channelsrecorded in this sleep study include arterialoxyhemoglobin saturation heart rate oral-nasalpressure flow snoring inductive plethysmog-raphy for chest efforts and body position
linkslwwcomCONTA15
B 2013 Marcel Hungs MD PhD Used withpermission
REFERENCES1 National Institutes of Health National
Center on Sleep Disorders ResearchSleep disorders research planwwwnhlbinihgovhealthprofsleep201101011NationalSleepDisordersResearch-PlanDHHSPublication11-7820pdf PublishedNovember 2011
2 Dinges DF An overview of sleepiness andaccidents J Sleep Res 19954(S2)4Y14
3 Mills RJ Young CA A medical definitionof fatigue in multiple sclerosis QJM 2008101(1)49Y60
4 Chervin RD Sleepiness fatigue tirednessand lack of energy in obstructive sleepapnea Chest 2000118(2)372Y379
5 Chotinaiwattarakul W OrsquoBrien LM Fan LChervin RD Fatigue tiredness and lack ofenergy improve with treatment for OSAJ Clin Sleep Med 20095(3)222Y227
6 American Academy of Sleep MedicineThe international classification of sleepdisorders diagnostic and coding manual2nd ed Westchester IL American Academyof Sleep Medicine 2005
7 Ebben MR Spielman AJNon-pharmacological treatments forinsomnia J Behav Med 200932(3)244Y254
8 Roth T Insomnia definition prevalenceetiology and consequences J Clin SleepMed 20073(5 suppl)S7YS10
9 Yang CM Spielman AJ Glovinsky PNonpharmacologic strategies in themanagement of insomnia Psychiatr ClinNorth Am 200629(4)895Y919 abstract viii
10 Katz ES DrsquoAmbrosio CM Pediatricobstructive sleep apnea syndrome ClinChest Med 201031(2)221Y234
11 Kohler M Bloch KE Stradling JR The role ofthe nose in the pathogenesis of obstructivesleep apnea Curr Opin Otolaryngol HeadNeck Surg 200917(1)33Y37
12 Kryger MH Atlas of clinical sleep medicinePhiladelphia PA Elsevier 2010
13 Zonato AI Martinho FL Bittencourt LRet al Head and neck physical examinationcomparison between nonapneic andobstructive sleep apnea patientsLaryngoscope 2005115(6)1030Y1034
14 Mallampati SR Gatt SP Gugino LD et alA clinical sign to predict difficult trachealintubation a prospective study Can AnaesthSoc J 198532(4)429Y434
15 Samsoon GL Young JR Difficult trachealintubation a retrospective studyAnaesthesia 198742(5)487Y490
16 Huang HH Lee MS Shih YL et alModified Mallampati classificationas a clinical predictor of peroralesophagogastroduodenoscopy toleranceBMC Gastroenterol 20111112
17 Friedman M Ibrahim H Bass L Clinicalstaging for sleep-disordered breathingOtolaryngol Head Neck Surg 2002127(1)13Y21
18 Cheng RHW Yiu CKY Leung WKOral health in individuals with Downsyndrome In Dey S ed Prenatal diagnosisand screening for down syndromeInTech wwwintechopencombookshowtoreferenceprenatal-diagnosis-and-screening-for-down-syndromeoral-health-in-individuals-with-down-syndromePublished 2011 Accessed August 24 2012
19 Katz I Stradling J Slutsky AS et al Dopatients with obstructive sleep apneahave thick necks Am Rev Respir Dis1990141(5 pt 1)1228Y1231
20 Kushida CA Efron B Guilleminault C Apredictive morphometric model for theobstructive sleep apnea syndrome AnnIntern Med 1997127(8 pt 1)581Y587
48 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
21 Saccucci M Tettamanti L Mummolo S et alScoliosis and dental occlusion a review ofthe literature Scoliosis 2011615
22 Battagel JM Kotecha B Dental side-effectsof mandibular advancement splint wear inpatients who snore Clin Otolaryngol200530(2)149Y156
23 Morcos SS Patel PK The vocabulary ofdentofacial deformities Clin Plast Surg200734(3)589Y599
24 Epstein LJ Kristo D Strollo PJ Jr et alClinical guideline for the evaluationmanagement and long-term care ofobstructive sleep apnea in adults J ClinSleep Med 20095(3)263Y276
25 Johns MW A new method for measuringdaytime sleepiness the Epworth sleepinessscale Sleep 199114(6)540Y545
26 Johns MW Daytime sleepiness snoring andobstructive sleep apnea The EpworthSleepiness Scale Chest 1993103(1)30Y36
27 Chervin RD Aldrich MS The EpworthSleepiness Scale may not reflect objectivemeasures of sleepiness or sleep apneaNeurology 199952(1)125Y131
28 Buysse DJ Reynolds CF 3rd Monk THet al The Pittsburgh Sleep Quality Index anew instrument for psychiatric practice andresearch Psychiatry Res 198928(2)193Y213
29 Chervin RD Hedger K Dillon JE Pituch KJPediatric sleep questionnaire (PSQ) validityand reliability of scales for sleep-disorderedbreathing snoring sleepiness and behavioralproblems Sleep Med 20001(1)21Y32
30 Chung F Yegneswaran B Liao P et al STOPquestionnaire a tool to screen patients forobstructive sleep apnea Anesthesiology2008108(5)812Y821
31 Walters AS LeBrocq C Dhar A et alValidation of the International Restless LegsSyndrome Study Group rating scale forrestless legs syndrome Sleep Med 20034(2)121Y132
32 Bastien CH Vallieres A Morin CMValidation of the Insomnia Severity Indexas an outcome measure for insomniaresearch Sleep Med 20012(4)297Y307
33 YOURSLEEPaasmnetorg from the AmericanAcademy of Sleep Medicine Two weeksleep diary yoursleepaasmnetorgpdfsleepdiarypdf Accessed August 24 2012
34 Kushida CA Littner MR Morgenthaler Tet al Practice parameters for the indicationsfor polysomnography and relatedprocedures an update for 2005 Sleep200528(4)499Y521
35 Iber C Ancoli-Israel S Chesson A et alThe AASM manual for scoring of sleep andassociated events rules terminology andtechnical specifications 1st ed WestchesterIL American Academy of Sleep Medicine2007
36 Collop NA Tracy SL Kapur V et alObstructive sleep apnea devices forout-of-center (OOC) testing technologyevaluation J Clin Sleep Med 20117(5)531Y548
37 Collop NA Anderson WM Boehlecke Bet al Clinical guidelines for the use ofunattended portable monitors in thediagnosis of obstructive sleep apnea in adultpatients Portable Monitoring Task Forceof the American Academy of SleepMedicine J Clin Sleep Med 20073(7)737Y747
38 Littner MR Kushida C Wise M et alStandards of Practice Committee of theAmerican Academy of Sleep MedicinePractice parameters for clinical use of themultiple sleep latency test and themaintenance of wakefulness test Sleep200528(1)113Y121
39 Carskadon MA Dement WC Mitler MMet al Guidelines for the multiple sleeplatency test (MSLT) a standard measure ofsleepiness Sleep 19869(4)519Y524
40 van den Hoed J Kraemer H Guilleminault Cet al Disorders of excessive daytimesomnolence polygraphic and clinical datafor 100 patients Sleep 19814(1)23Y37
41 Hoban TF Chervin RD Assessment ofsleepiness in children Semin PediatrNeurol 20018(4)216Y228
42 ICSD-2 The international classification ofsleep disorders pocket version diagnosticand coding manual 2nd ed WestchesterIL American Academy of Sleep Medicine2005
43 Arand D Bonnet M Hurwitz T et alThe clinical use of the MSLT and MWTSleep 200528(1)123Y144
44 Dauvilliers Y Gosselin A Paquet J et alEffect of age on MSLT results in patientswith narcolepsy-cataplexy Neurology200462(1)46Y50
45 Morgenthaler T Alessi C Friedman Let al Practice parameters for the use ofactigraphy in the assessment of sleep andsleep disorders an update for 2007 Sleep200730(4)519Y529
46 Gamaldo CE Earley CJ Restless legssyndrome a clinical update Chest2006130(5)1596Y1604
49Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited

asking the patient to press the indexfinger against the left nostril and take adeep breath in on the right side thisshould be repeated on the oppositeside as well The patientrsquos facial mor-phology should be assessed for man-dibular retrognathia (Figure 2-2)12 Withthe patientrsquos head in a neutral posi-tion a virtual line is drawn from thevermillion border of the lower lip tothe chin Mandibular retrognathia issuggested if the anterior prominence ofthe chin is 2 mm or more behind thevirtual line13
The modified Mallampati classifica-tion is commonly used for assessmentof the oral airway in patients withsuspected SDB The Mallampati classi-fication14 was developed to identifypatients in whom tracheal intubationwould be difficult the initial description
divided patients into three classes Twoyears later15 this was modified to de-scribe four groups class I class II classIII and class IV Figure 2-3 16 illustratesthe modified Mallampati classificationassessed with the tongue protrudedThe Friedman palate position classifi-cation17 also commonly referencedutilizes the same four categories but isdone with the tongue at rest and notextended Either the Mallampati orFriedman classification may be used todescribe the patency of the oral airway
Tonsils should be classified based onthe degree of hypertrophy (Figure 2-4)12grade I tonsils are inside the tonsillarfossa lateral to the posterior pillarsgrade II tonsils occupy 25 of theoropharynx grade III tonsils occupy50 of the oropharynx and grade IVtonsils occupy at least 75 of the
FIGURE 2-3 Modified Mallampati classification The class is determined by looking at theanatomy of the oral cavity and describes tongue size relative to oropharyngealsize The test is conducted with the patient seated the head held in a neutral
position and the mouth wide open and relaxed The subsequent classification is assigned basedupon the pharyngeal structures that are visible
Reprinted from Huang HH et al BMC Gastroenterol16 B 2011 BioMed Central Ltd wwwbiomedcentralcom1471-230X1112
37Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
oropharynx and nearly meet in the mid-line13 A high-arched narrow hard pal-ate (Figure 2-5)18 may predispose thepatient to have SDB Katz and col-leagues19 have shown that patients withOSA have significantly increased neckcircumference compared to nonapneicsnorers greater distribution of neck fat
may contribute to mass loading on theupper airway in patients with OSA Thepatientrsquos neck circumference should bemeasured at the superior border of thecricothyroid membrane19 A neck cir-cumference greater than 40 cm (157in) has been shown to be predictive ofOSA with 61 sensitivity and 93specificity regardless of sex20
Assessment of the patientrsquos anteriorand posterior dentition can also re-veal anatomic findings that may pre-dispose a person to certain sleepdisorders Two features to note in eval-uation of the anterior dentition areoverjet and overbite (Figure 2-6)21
Overjet as shown in Figure 2-712 isthe horizontal distance between theupper right central incisor and thebuccal surface of the correspondinglower tooth while overbite is the ver-tical distance between these twopoints22 These measurements are typ-ically reported in millimeters The An-gle classification system is used todescribe the first molar position on
FIGURE 2-4 Tonsil size grading Thisstructural abnormality canpredispose a patient to havesleep-disordered breathing
Reprinted from Kryger MH Elsevier12 B 2010 withpermission from Elsevier
FIGURE 2-5 Deficientmaxillarydevelopment inan individual with
Down syndrome leading to highand narrow hard palate
Reprinted with permission from ChengRHW et al InTech18 B 2011 W KeungLeung wwwintechopencombooksprenatal-diagnosis-and-screening-for-down-syndromeoral-health-in-individuals-with-down-syndrome
FIGURE 2-6 Overjet andoverbite Overjetis defined as
increased projection of the upperteeth in front of the lower teethas measured parallel to theocclusal plane Overbite is thevertical overlapping of maxillaryteeth over mandibular teethusually measured perpendicularto the occlusal plane
Reprinted from Saccucci M et al Scoliosis21
B 2011 BioMed Central Ltd wwwscoliosisjournalcomcontent6115
38 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
the mandibular and maxillary dentalarches23 Figure 2-8 shows class I oc-clusion and class II and III malocclu-
sion Of note the mesiobuccal surfaceis the aspect of the tooth that is adja-cent to the cheek mucosa
The Adult Obstructive Sleep ApneaTask Force of the American Academyof Sleep Medicine (AASM) recommen-ded in recent clinical guidelines24 thatthe following physical findings maysuggest the presence of OSA increasedneck circumference (greater than 432cm [17 in] in men greater than 406 cm[16 in] in women) BMI 30 kgm2 orgreater modified Mallampati classifica-tion of III or IV presence of retrognathialateral peritonsillar narrowing macro-glossia tonsillar hypertrophy elongatedenlarged uvula high-archednarrowhard palate nasal abnormalities (egpolyps deviation valve abnormalities
KEY POINT
h Classification of thepatientrsquos dentition helpsto evaluate the positionof the maxillary archrelative to themandibular arch
FIGURE 2-7 OverjetDisplacementof the
mandibular teeth posteriorly inrelationship to the maxillary teethresults inmoreposteriorly crowdedupper airways predisposingpatients for the developmentof obstructive sleep apnea
Reprinted from Kryger MH Elsevier12
B 2010 with permission from Elsevier
FIGURE 2-8 Angle class occlusionmalocclusion A Angle class I occlusion also known asneutrocclusion The mandibular and maxillary dental arches have a normalanterior-posterior relationship The mesiobuccal groove of the mandibular first
molar interdigitates with the mesiobuccal cusp of the maxillary first molar B Angle class IImalocclusion also known as distoclusion The mandibular dental arch is in distal anterior-posteriorrelationship to the maxillary dental arch The mesiobuccal groove of the mandibular first molar isdistal to the mesiobuccal cusp of the maxillary first molar C Angle class III malocclusion alsoknown as mesioclusion The mandibular dental arch is in mesial anterior-posterior relationship tothe maxillary dental arch The mesiobuccal groove of the mandibular first molar is mesial to themesiobuccal cusp of the maxillary first molar
Reprinted fromMorcos SS Patel PK Clin Plast Surg23 B 2007 with permission from Elsevier wwwsciencedirectcomsciencearticlepiiS0094129807000843
39Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
and turbinate hypertrophy) andoroverjet To prevent overlooking thesefindings a thorough head and neckassessment as described in Table 2-2should be incorporated into the phys-ical examination of all patients whopresent with sleep-related complaints
SUBJECTIVE ASSESSMENTSeveral patient-completed question-naires are inexpensive and time-efficient
reasonably well validated and com-monly used They can help to increasestandardization in evaluations of patientsby different clinicians or across centersPerhaps the most well-known andwidely used is the Epworth SleepinessScale25 a subjective assessment of thepatientrsquos daytime sleep propensity inrecent times As shown in Appendix Athe Epworth Sleepiness Scale asks theresponder to use a four-point Likertscale (0 1 2 or 3) to indicate thelikelihood of dozing in eight distinctsedentary conditions A total score of 10or greater out of a possible 24 suggestsexcessive daytime sleepiness25 Whilethe Epworth Sleepiness Scale score canbe easily incorporated into the clinicalevaluation it should not be used as asubstitute for objective measurement ofsleepiness The Epworth Sleepiness Scalescore may correlate to a limited extentwith the presence and severity of OSA26
but some studies have failed to find anystatistically significant association withmean sleep latency on multiple sleep la-tency tests or with severity of OSA27
The most advantageous use of theEpworth Sleepiness Scale may be to followan individualrsquos self-assessment of sleep-iness longitudinally and it may also serveas an indicator of treatment response
Many other questionnaires may beutilized in a clinical sleep evaluationsome pertain to overall sleep qualitywhile others are disorder-specific ThePatient Reported Outcomes Measure-ment Information System (PROMIS) isan NIH-supported system of measuresfor patient-reported health status andincludes questions on sleep disturb-ance The Pittsburgh Sleep QualityIndex (PSQI) is a validated question-naire that inquires about sleep qualityand disturbances over the previousmonth28 The parent-completed Pe-diatric Sleep Questionnaire29 containsa validated reliable 22-item scale tohelp assess risk for SDB in children
KEY POINTS
h The Epworth SleepinessScale apatient-completedquestionnaire assessesthe patientrsquos subjectivetendency to doze duringsedentary situations inrecent times not onlyat the moment thequestionnaire iscompleted
h The Epworth SleepinessScale should not beused in lieu of diagnostictesting but may be avaluable componentof ongoing clinicalevaluation
TABLE 2-2 Head and NeckExamination
b Face
Featuresof long face syndrome
Infraorbital darkening
Mouth breathing
Elongated midface
Nasal atrophy
b Oral Airway
Mandibular retrognathia
Low soft palate (modifiedMallampati classification)
Large or boggy uvula
Erythematous pillars
Tonsillar hypertrophy
High narrow hard palate
Neck circumference
Overjet
Overbite
Angle classification(malocclusion)
Macroglossia
Worn occlusive surfaces(suggestive of bruxism)
b Nasal Airway
Symmetry of the nares
Nasal septum deviation
Nasal airflow
Collapse of nasal alae oninspiration
b Neck
Neck circumference
40 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
The STOP-BANG questionnaire devel-oped and validated in preoperativepatients is a sensitive screening toolfor OSA Four questions address snor-ing tiredness during daytime observedapnea and high blood pressure whereasfour other measures focus on increasedOSA risk factors of BMI (greater than 35kgm2) age (older than 50 years) neckcircumference (greater than 40 cm[1575 in]) and gender (male preva-lence)30 The International RestlessLegs Syndrome Study Group Rating Scale(IRLS) is a validated assessment of dis-ease severity for patients with restlesslegs syndrome31 The patientrsquos perceived
level of insomnia may be assessed withthe Insomnia Severity Index (ISI) avalidated 7-item questionnaire32
A sleep diary (Figure 2-9)33 allows apatient to chart daily sleep and waketimes and should be maintained for atleast 2 consecutive weeks Review ofthis information allows the clinicianto estimate the total amount of sleepthe patient obtains in a 24-hour pe-riod The sleep diary also can provideinsight into the patientrsquos sleep patternIs sleep obtained at the same timesevery day Is the patientrsquos sleep con-solidated or fragmented across 24hours Does the patient sleep and
FIGURE 2-9 Sleep diary completed by a 46-year-old woman who presented with difficulty falling asleep Vertical linesrepresent when the patient went to bed lsquolsquoMrsquorsquo refers to when medication was taken black shading representstime asleep and unshaded white areas are time spent awake
Diary template reprinted from YOURSLEEPaasmnetorg from the American Academy of Sleep Medicine yoursleepaasmnetorgpdfsleepdiarypdf33
41Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
wake at conventional times or doeshe or she appear to be a lsquolsquonight owlrsquorsquoor lsquolsquomorning larkrsquorsquo Answers to thesequestions as provided by the sleepdiary may reveal factors that contrib-ute to sleep-related concerns Use ofsleep diaries can be particularly help-ful in patients with suspected circadianrhythm sleep disorders (including shiftwork) behaviorally induced insufficientsleep or inadequate sleep hygiene
OBJECTIVE MEASURESNocturnal polysomnography (NPSG)or related assessments are indicatedfor the diagnosis and assessment ofSDB and for positive airway titrationin patients with confirmed SDB Theprocedure can also provide informationabout EEG activity nocturnal move-ments cardiac rhythm and oxygen
saturation34 The recommended record-ing montage used in NPSG as shownin Figure 2-10 includes central (C3-A2C4-A1) frontal (F3-A2 F4-A1) andoccipital (O1-A2 O2-A1) EEGs left andright eye electrooculograms mentalsubmental surface EMG and ECG leadsOther recorded parameters includethoracic and abdominal effort oxygensaturation nasaloral airflow and bodyposition Use of a microphone torecord snoring is recommended butnot required34 A full 16-lead EEG(Figure 2-11)35 and video recordingmay be performed when nocturnalseizures are suspected Leg surfaceEMG leads are recommended andadditional arm EMG leads may beapplied when the clinical history sug-gests complex sleep-related motor be-haviors such as dream enactment In
KEY POINT
h A daily sleep diary helpsto summarize a patientrsquossleep-wake schedulemore accurately thanmemory often allowsand can facilitateconstruction ofpersonalized plansfor management ofcircadian rhythm sleepdisorders and insomnia
FIGURE 2-10 A 1-minute epoch from a nocturnal polysomnogram showing obstructive sleepapnea in a 46-year-old man who presented with snoring daytime sleepinessand headaches It depicts the standard recording montage that includes the
following leads central (C3-M2 C4-M1) frontal (F3-M2 F4-M1) and occipital (O1-M2 O2-M1)EEGs left and right eye electrooculograms (E1-M2 E2-M1) mentalsubmental electromyogram(Chin1-Chin2) electrocardiogram (ECG1-ECG2 ECG2-ECG3) snore volume (SNORE) nasalpressure transducer (NPRE) nasaloral airflow (NO) thoracic (THOR) and abdominal (ABD)effort arterial oxyhemoglobin saturation (SpO2) plethysmography (Pleth) and left and right eyeelectromyograms (LAT1-LAT2 RAT1-RAT2)
42 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
most cases the diagnostic NPSG is doneon 1 night although NPSG on 2 con-secutive nights may be considered inthe evaluation of parasomnias
Four categories of sleep monitoringdevices for use in the diagnosis of sleepdisorders have often been described34
These are type 1 standard attended in-laboratory polysomnography type 2comprehensive portable unattendedpolysomnography type 3 modifiedportable sleep apnea testing (often car-diorespiratory studies that do not recordsleep) and type 4 continuous single ordual bioparameter recording (eg pulseoximetry) However this categorizationmay not effectively classify the plethoraof out-of-center testing devices currentlyavailable for clinical use Therefore anew device classification system hasrecently been proposed This schemaknown as the SCOPER system catego-rizes out-of-center testing devices basedon measurement of sleep cardiovascu-
lar oximetry position effort and res-piratory parameters36 Within each ofthe six SCOPER categories a level of 0through 5 is assigned as indicated bythe type of sensor or measurementthat the device uses for that category
The most recent clinical guidelinespublished by the Portable MonitoringTask Force of the AASM37 for use ofunattended portable monitoring inthe diagnosis of OSA in adult patientsrecommend that portable monitoringonly be performed in conjunction witha comprehensive sleep evaluation by(or supervised by) a practitioner board-certified in sleep medicine or eligiblefor the certification examination Theseguidelines state that portable monitor-ing may be used in place of NPSG inpatients with a high pretest probabilityof moderate to severe OSA Portablemonitoring should not be used inpatients with significant medical comor-bidities (including but not limited to
KEY POINT
h The complexclassification of portabletesting devices reflectsthe multitude of designsavailable to cliniciansand will undoubtedlychange as technologyadvances
FIGURE 2-11 A The international 10Y20 system for EEG electrode placement refers to the10 and 20 interelectrode distances Even electrode numbers (2 4 6 8)represent the right hemisphere and odd electrode numbers (1 3 5 7)
represent the left hemisphere B Recommended F4-M1 C4-M1 O2-M1 placements of EEGelectrodes as set forth by the American Academy of Sleep Medicine (AASM)
Adapted from Iber C et al American Academy of SleepMedicine35 Used with permission of the American Academy ofSleep Medicine Darien IL 2012
43Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
moderate to severe pulmonary diseaseneuromuscular disease or congestiveheart failure) in patients with othersleep disorders (including central sleepapnea periodic limb movement disor-der insomnia parasomnias circadianrhythm disorders or narcolepsy) or asa screening tool The use of portablemonitoring may be indicated for thediagnosis of OSA in patients for whomattended NPSG is not possible becauseof immobility safety or critical illnessPortable monitoring may be indi-cated to monitor the response to non-continuous positive airway pressuretreatments for OSA including oralappliances upper airway surgery andweight loss The algorithm shown inAppendix B may help in the determi-nation of an adult patientrsquos candidacyfor out-of-center testing for the diag-nosis of OSA An example of portable(or home) monitoring technology isshown in Supplemental Digital Con-tent 2-1 linkslwwcomCONTA15
Recommended technology for port-able monitoring should record at mini-mum airflow respiratory effort andblood oxygenation the airflow effortand oximetric biosensors typically usedfor attended NPSG should be used37
These guidelines published in 2007will likely continue to evolve as newtechnologies emerge and are found tobe effective The current guidelinesrecommend that out-of-center testingbe performed under the auspices of anAASM-accredited comprehensive sleepmedicine program and that a board-certifiedeligible sleep specialist reviewthe raw data from a portable monitor-ing device All patients who undergoportablemonitoring for the diagnosis ofOSA should have a follow-up visit toreview test results Negative or techni-cally inadequate portable monitoringstudies should be followed by attendedin-laboratory NPSG if the clinical suspi-cion for SDB remains high37
The aforementioned testing proce-dures are primarily used in the evalua-tion of SDB Other testing modalitiesare useful in the diagnosis of othercategories of sleep disorders The mul-tiple sleep latency test (MSLT) and itsvariant the maintenance of wakefulnesstest (MWT) are used in the evaluation ofhypersomnia The conventional record-ing montage is similar to that used fornocturnal polysomnography central fron-tal and occipital EEGs left and right eyeelectrooculograms mentalsubmentalEMG and ECG leads Measurement ofthoracic and abdominal effort oxygensaturation and nasaloral airflow are notrequired but may help explain delayedsleep latencies for patients in whomrespiratory disturbances interfere withsleep onset
The MSLT is a validated tool that isconsidered the de facto standard forobjective assessment of excessive day-time sleepiness38 The recommendedprotocol38 involves five 20-minute napopportunities held at 2-hour intervalsthroughout the day If sleep is ob-served the patient is allowed to sleepfor at least 15 minutes The sleep la-tency for each nap is measured as thetime from the start of the nap trial tothe first epoch of sleep A sleep la-tency of 20 minutes is assigned to naptrials during which no sleep isobserved39 The mean sleep latencycalculated as the average sleep latencyacross all nap trials is the final resultThe presence and number of sleep-onset REM periods (SOREMPs) is alsodetermined as this information canhelp to establish a diagnosis of narco-lepsy without cataplexy or to confirmnarcolepsy with cataplexy
The MSLT should be started 15 to30 hours following completion of anocturnal polysomnogram whichshould record at least 6 hours of sleepin order for determination of the meansleep latency to be valid Drugs that may
KEY POINT
h Careful considerationshould be given tothe indications forout-of-center testingAttended nocturnalpolysomnography isindicated if a portablestudy yields a negativeor technicallyinadequate result
44 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
interfere with sleep latency or REM la-tency should be discontinued 2 weeksbefore testing whenever possible Ascreen may be performed on the day oftesting if there is suspicion that pre-scribed or illicit substances may con-tribute to the patientrsquos sleepiness38
No large multicenter systematicallycollected normative data are availablefor mean sleep latency values on theMSLT38 Nonetheless a mean sleep la-tency of greater than 10 minutes is of-ten considered normal whereas a meansleep latency of 8 to 10 minutes is con-sidered a physiologic gray zone40 Thenormative data for children are classi-fied by Tanner stage of developmentthough the MSLT is typically not per-formed in children aged younger than 6or 7 years because some daytime nap-ping may still be normal in youngchildren41 The second edition of theInternational Classification of SleepDisorders Diagnostic and CodingManual (ICSD-2)42 requires the pres-ence of a mean sleep latency of lessthan 8 minutes and two or moreSOREMPs as part of the diagnosticcriteria for narcolepsy without cata-plexy However the ICSD-2 also notesthat a mean sleep latency of less than 8minutes may occur in up to 30 of thegeneral population Therefore whilethe MSLT is a helpful and widely usedtool it remains an imperfect gold stand-ard in the assessment of daytime sleepi-ness This necessitates that theevaluation of daytime sleepiness notrest on the MSLT results alone butassimilate the clinical history subjectivecomplaints diagnostic study results andother pertinent medical information38
Practice parameters from theAASM state that the MSLT is indicatedfor diagnostic confirmation of sus-pected narcolepsy and may be indi-cated to differentiate idiopathichypersomnia from narcolepsy38 TheMSLT is not indicated for routine
assessment of OSA syndrome or toassess response to treatment of SDBand is not routinely indicated for eval-uation of sleepiness in medical orneurologic disorders (except for narco-lepsy) insomnia or circadian rhythmdisorders
TheMWTprovides an objectivemeas-ure of a patientrsquos ability to remain awakerather than the tendency to fall asleepduring the day The key differencebetween the MWT and the MSLT is thatin the former the patient is asked to tryto stay awake under circumstances con-ducive to sleep rather than to fall asleepThe MWT provides an objective vali-dated assessment of the ability to remainawake for a defined length of time38 Therecommended protocol includes four40-minute trials that begin at 2-hourintervals with the first trial to start 15 to30 hours after the patientrsquos wake-uptime A nocturnal polysomnogram onthe preceding night is not requiredHowever the patient should obtain asufficient amount of sleep during thenight before the MWT Each trial isterminated after 40 minutes if no sleepoccurs or after unequivocal sleep onset(defined as three continuous epochsof stage N1 sleep or one epoch of anyother stage of sleep) has occurred38
One indication for the MWT is to as-sess an individualrsquos ability to remainawake when his or her inability to re-main awake constitutes a public orpersonal safety issue This can becomea pressing issue for individuals em-ployed in the transportation43 con-struction or health care industriesThe MWT may be indicated to assesstreatment response in patients withknown excessive daytime sleepiness
Limited amounts of normative dataare available for the MWT Historicallymultiple testing protocols make syn-thesis of results more challenging TheMWT is used much less often in clinicalpractice compared to the MSLT Patient
KEY POINTS
h The multiple sleeplatency test is the goldstandard for objectiveassessment of daytimesleepiness butinterpretation of theresults must be madewithin the clinicalcontext of the patientrsquoshistory
h In the multiple sleeplatency test the patientis instructed to try tosleep during each naptrial In the maintenanceof wakefulness test thepatient is instructed totry to remain awakeduring the nap trial
h A baseline nocturnalpolysomnogram isrequired before amultiple sleep latencytest and considered butnot required before amaintenance ofwakefulness test
45Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
age may also affect the mean sleep la-tency values on both the MWT and theMSLT43 and may represent evolution ofcircadian rhythm and sleep architec-ture across the lifetime A study of 383patients with narcolepsy with cataplexyexamined the clinical and polysomno-graphic data at the time of diagnosis(age range 5 to 84 years) and found aprogressive decrease in the number ofSOREMPs and a progressive increase inthe mean sleep latency on the MSLT asa function of age44 Given its limita-tions the MWT may thus be used tosupplement the clinical history in theassessment of ability to stay awake butshould not be the sole determinant ofthis parameter
Actigraphy is also used in the clinicalevaluation of patients with sleep disor-ders particularly circadian rhythm sleepdisorders An actigraph is a watchlikedevice that is worn on the wrist for anextended period usually in the range ofweeks The actigraph records move-ment and uses an algorithm to estimatethe amounts of sleep and wake timeduring the recording period Analysissoftware uses movement to estimatewhen sleep and wakefulness haveoccurred Review of the data can pro-vide objective insight into the patientrsquossleep pattern including timing andduration of major sleep disruptionsActigraphy is indicated as part of theevaluation of patients with advancedsleep-phase syndrome delayed sleep-phase syndrome and shift work disor-der and may be indicated in the evalua-tion of jet lag disorder and nonY24-hoursleep-wake syndrome including thatassociated with blindness45 It can alsoserve as a measure of treatment re-sponse in patients with insomnia andcircadian rhythm sleep disorders Forpopulations in which traditional sleepmonitoring may be challenging suchas pediatric or older adult patientsactigraphy may provide valuable infor-
mation about the patientrsquos sleep pat-tern or response to treatment Whenpolysomnography is not availableactigraphy is indicated to estimate totalsleep time in patients with OSA45
OTHER ASSESSMENTMODALITIESLaboratory evaluation and neuroimag-ing with either CT or MRI may beconsidered on an individual basis asindicated by the clinical history Com-plete blood count (CBC) serum chem-istries or measures of thyroid functionmay be obtained if an underlying med-ical disorder is thought to contribute tothe patientrsquos sleep symptoms Forinstance these laboratory studies maybe consideredwhen daytime fatigue is apredominant symptom Serum ironstudies including ferritin level shouldbe checked in patients with restless legssyndrome46 Neuroimaging should beconsidered in patients with antecedenttrauma or for any sleep disorder pa-tient with an abnormal neurologic ex-amination to evaluate for a structuraletiology of the patientrsquos symptoms
APPROACH TO THE PATIENTEvaluation of suspected sleep disordersis best accomplished by a stepwisemultidimensional approach (Case 2-2)A thorough sleep history includes de-tailed description of sleep-related symp-toms nocturnal behaviors the patientrsquossleep schedule level of daytime sleepi-ness and subsequent effects on daytimefunctioning Collateral history from thepatientrsquos bed partner or family is oftennecessary to understand the severity andcontext of the patientrsquos symptoms Sub-jective assessments of sleepiness suchas the Epworth Sleepiness Scale areeasily administered and useful to tracksymptomatic progression or treatmentresponse from one visit to the nextCertain physical examination findingsmay also raise clinical suspicion of
KEY POINTS
h Actigraphy can beuseful in evaluation andtreatment of circadianrhythm sleep disordersand in management ofinsomnia
h Neuroimaging is notroutinely indicated inthe clinical evaluation ofsleep disorders andshould be pursued on acase-by-case basis
46 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
particular sleep disorders For patientsin whom multiple sleep disorders aresuspected systematic use of diagnostictesting allows for accurate identificationof specific diagnoses In a patient withinsomnia and symptoms suggestive ofSDB nocturnal polysomnography shouldbe the first procedure performed Ifthe insomnia persists despite adequatetreatment of SDB further evaluationwith sleep diaries and possibly actigra-
phy may be considered to better char-acterize the patientrsquos sleep patternActigraphy may then again be pursuedto gauge treatment response upon man-agement of the patientrsquos insomnia
The diagnostic modalities availablefor evaluation of sleep disorders arerapidly evolving In-laboratory nocturnalpolysomnography currently remains thegold standard for assessment of SDBHowever the multitude of out-of-center
KEY POINT
h Careful assimilation ofthe clinical history thesleep-specific physicalexamination patientquestionnaires anddiagnostic test resultsleads to the mostaccurate assessment ofpatients with symptomsrelated to sleep oralertness
Case 2-2A 23-year-old woman reported a 4-year history of insomnia Throughoutcollege she was a lsquolsquonight owlrsquorsquo never scheduled classes that started before100 PM and always did well in school During the past 6 months shedeveloped progressive difficulty staying awake in her job as a financialanalyst andwas concerned about how this might affect her job performance
During the week she was in bed by midnight but was unable to fallasleep until 200 AM and awoke with difficulty to an alarm at 600 AMfeeling tired She denied any thought rumination or physical discomfortat bedtime She had tried over-the-counter sleep aids that provided nosymptomatic improvement and worsened morning grogginess Onweekends she slept from 200 AM to 1100 AM and awakened feelinglsquolsquopretty goodrsquorsquo She had nocturia up to once per night and occasionalmorning headaches She had no bed partner but reported gaspingrespirations nocturnal palpitations and snort arousals On about 4 nightsper week she experienced a sensation of needing to move her legswhile trying to fall asleep This sensation was relieved by movement andwas worse at night than during the day Her legs sometimes movedspontaneously at night or while seated quietly for long periods duringthe day She felt sleepy during the afternoon especially while workingat her computer She denied drowsiness while driving She occasionallytook a 30-minute nap on the weekend and found it to be refreshingShe drank one to two cups of coffee every morning and had a 12-oz dietcaffeinated soda at 300 PM Her sleepiness had not caused her to makeany mistakes at work and she denied any mood disturbance
Physical examination was notable for a body mass index of 32 kgm2 neckcircumference of 381 cm (15 in) and modified Mallampati class III oral airwayNasal passages were narrow with turbinate hypertrophy bilaterally andhard palate was high-arched and narrow Nomicrognathia or retrognathia waspresent She had molar occlusion class I bilaterally with no overjet or overbiteThe general cardiac respiratory and neurologic examinations were normal
Comment This case illustrates how discussion of the chief complaint raisessuspicion for multiple sleep disorders The history suggests a circadian rhythmsleep disorder particularly delayed sleep-phase syndrome sleep-disorderedbreathing and restless legs syndrome Diagnostic evaluation should includenocturnal polysomnogramwith consideration toperform testing at the patientrsquospreferred sleep time and serum iron studies Sleep diaries andor actigraphymay be considered for further assessment of the patientrsquos sleep pattern
47Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
testing devices continues to grow andmany may provide useful alternativesthat under appropriate circumstancescould allow more expedient conven-ient and less costly evaluations ofincreased numbers of patients whopreviously had only limited or delayedaccess to sleep services
VIDEO LEGENDSupplemental Digital Content 2-1
Home sleep study Video demonstrates a homesleep study using an unattended type 3 portablemonitoring device The patient is a 56-year-oldman who is experiencing morning headachesand concentration and alertness problems atwork He has a history of mild snoring and ar-terial hypertension His Epworth SleepinessScale score is 18 his neck circumference is19 in he has a Mallampati classification score ofIII and his body mass index is 41 kgm Theapnea-hypopnea index is 84 eventsh Channelsrecorded in this sleep study include arterialoxyhemoglobin saturation heart rate oral-nasalpressure flow snoring inductive plethysmog-raphy for chest efforts and body position
linkslwwcomCONTA15
B 2013 Marcel Hungs MD PhD Used withpermission
REFERENCES1 National Institutes of Health National
Center on Sleep Disorders ResearchSleep disorders research planwwwnhlbinihgovhealthprofsleep201101011NationalSleepDisordersResearch-PlanDHHSPublication11-7820pdf PublishedNovember 2011
2 Dinges DF An overview of sleepiness andaccidents J Sleep Res 19954(S2)4Y14
3 Mills RJ Young CA A medical definitionof fatigue in multiple sclerosis QJM 2008101(1)49Y60
4 Chervin RD Sleepiness fatigue tirednessand lack of energy in obstructive sleepapnea Chest 2000118(2)372Y379
5 Chotinaiwattarakul W OrsquoBrien LM Fan LChervin RD Fatigue tiredness and lack ofenergy improve with treatment for OSAJ Clin Sleep Med 20095(3)222Y227
6 American Academy of Sleep MedicineThe international classification of sleepdisorders diagnostic and coding manual2nd ed Westchester IL American Academyof Sleep Medicine 2005
7 Ebben MR Spielman AJNon-pharmacological treatments forinsomnia J Behav Med 200932(3)244Y254
8 Roth T Insomnia definition prevalenceetiology and consequences J Clin SleepMed 20073(5 suppl)S7YS10
9 Yang CM Spielman AJ Glovinsky PNonpharmacologic strategies in themanagement of insomnia Psychiatr ClinNorth Am 200629(4)895Y919 abstract viii
10 Katz ES DrsquoAmbrosio CM Pediatricobstructive sleep apnea syndrome ClinChest Med 201031(2)221Y234
11 Kohler M Bloch KE Stradling JR The role ofthe nose in the pathogenesis of obstructivesleep apnea Curr Opin Otolaryngol HeadNeck Surg 200917(1)33Y37
12 Kryger MH Atlas of clinical sleep medicinePhiladelphia PA Elsevier 2010
13 Zonato AI Martinho FL Bittencourt LRet al Head and neck physical examinationcomparison between nonapneic andobstructive sleep apnea patientsLaryngoscope 2005115(6)1030Y1034
14 Mallampati SR Gatt SP Gugino LD et alA clinical sign to predict difficult trachealintubation a prospective study Can AnaesthSoc J 198532(4)429Y434
15 Samsoon GL Young JR Difficult trachealintubation a retrospective studyAnaesthesia 198742(5)487Y490
16 Huang HH Lee MS Shih YL et alModified Mallampati classificationas a clinical predictor of peroralesophagogastroduodenoscopy toleranceBMC Gastroenterol 20111112
17 Friedman M Ibrahim H Bass L Clinicalstaging for sleep-disordered breathingOtolaryngol Head Neck Surg 2002127(1)13Y21
18 Cheng RHW Yiu CKY Leung WKOral health in individuals with Downsyndrome In Dey S ed Prenatal diagnosisand screening for down syndromeInTech wwwintechopencombookshowtoreferenceprenatal-diagnosis-and-screening-for-down-syndromeoral-health-in-individuals-with-down-syndromePublished 2011 Accessed August 24 2012
19 Katz I Stradling J Slutsky AS et al Dopatients with obstructive sleep apneahave thick necks Am Rev Respir Dis1990141(5 pt 1)1228Y1231
20 Kushida CA Efron B Guilleminault C Apredictive morphometric model for theobstructive sleep apnea syndrome AnnIntern Med 1997127(8 pt 1)581Y587
48 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
21 Saccucci M Tettamanti L Mummolo S et alScoliosis and dental occlusion a review ofthe literature Scoliosis 2011615
22 Battagel JM Kotecha B Dental side-effectsof mandibular advancement splint wear inpatients who snore Clin Otolaryngol200530(2)149Y156
23 Morcos SS Patel PK The vocabulary ofdentofacial deformities Clin Plast Surg200734(3)589Y599
24 Epstein LJ Kristo D Strollo PJ Jr et alClinical guideline for the evaluationmanagement and long-term care ofobstructive sleep apnea in adults J ClinSleep Med 20095(3)263Y276
25 Johns MW A new method for measuringdaytime sleepiness the Epworth sleepinessscale Sleep 199114(6)540Y545
26 Johns MW Daytime sleepiness snoring andobstructive sleep apnea The EpworthSleepiness Scale Chest 1993103(1)30Y36
27 Chervin RD Aldrich MS The EpworthSleepiness Scale may not reflect objectivemeasures of sleepiness or sleep apneaNeurology 199952(1)125Y131
28 Buysse DJ Reynolds CF 3rd Monk THet al The Pittsburgh Sleep Quality Index anew instrument for psychiatric practice andresearch Psychiatry Res 198928(2)193Y213
29 Chervin RD Hedger K Dillon JE Pituch KJPediatric sleep questionnaire (PSQ) validityand reliability of scales for sleep-disorderedbreathing snoring sleepiness and behavioralproblems Sleep Med 20001(1)21Y32
30 Chung F Yegneswaran B Liao P et al STOPquestionnaire a tool to screen patients forobstructive sleep apnea Anesthesiology2008108(5)812Y821
31 Walters AS LeBrocq C Dhar A et alValidation of the International Restless LegsSyndrome Study Group rating scale forrestless legs syndrome Sleep Med 20034(2)121Y132
32 Bastien CH Vallieres A Morin CMValidation of the Insomnia Severity Indexas an outcome measure for insomniaresearch Sleep Med 20012(4)297Y307
33 YOURSLEEPaasmnetorg from the AmericanAcademy of Sleep Medicine Two weeksleep diary yoursleepaasmnetorgpdfsleepdiarypdf Accessed August 24 2012
34 Kushida CA Littner MR Morgenthaler Tet al Practice parameters for the indicationsfor polysomnography and relatedprocedures an update for 2005 Sleep200528(4)499Y521
35 Iber C Ancoli-Israel S Chesson A et alThe AASM manual for scoring of sleep andassociated events rules terminology andtechnical specifications 1st ed WestchesterIL American Academy of Sleep Medicine2007
36 Collop NA Tracy SL Kapur V et alObstructive sleep apnea devices forout-of-center (OOC) testing technologyevaluation J Clin Sleep Med 20117(5)531Y548
37 Collop NA Anderson WM Boehlecke Bet al Clinical guidelines for the use ofunattended portable monitors in thediagnosis of obstructive sleep apnea in adultpatients Portable Monitoring Task Forceof the American Academy of SleepMedicine J Clin Sleep Med 20073(7)737Y747
38 Littner MR Kushida C Wise M et alStandards of Practice Committee of theAmerican Academy of Sleep MedicinePractice parameters for clinical use of themultiple sleep latency test and themaintenance of wakefulness test Sleep200528(1)113Y121
39 Carskadon MA Dement WC Mitler MMet al Guidelines for the multiple sleeplatency test (MSLT) a standard measure ofsleepiness Sleep 19869(4)519Y524
40 van den Hoed J Kraemer H Guilleminault Cet al Disorders of excessive daytimesomnolence polygraphic and clinical datafor 100 patients Sleep 19814(1)23Y37
41 Hoban TF Chervin RD Assessment ofsleepiness in children Semin PediatrNeurol 20018(4)216Y228
42 ICSD-2 The international classification ofsleep disorders pocket version diagnosticand coding manual 2nd ed WestchesterIL American Academy of Sleep Medicine2005
43 Arand D Bonnet M Hurwitz T et alThe clinical use of the MSLT and MWTSleep 200528(1)123Y144
44 Dauvilliers Y Gosselin A Paquet J et alEffect of age on MSLT results in patientswith narcolepsy-cataplexy Neurology200462(1)46Y50
45 Morgenthaler T Alessi C Friedman Let al Practice parameters for the use ofactigraphy in the assessment of sleep andsleep disorders an update for 2007 Sleep200730(4)519Y529
46 Gamaldo CE Earley CJ Restless legssyndrome a clinical update Chest2006130(5)1596Y1604
49Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited

oropharynx and nearly meet in the mid-line13 A high-arched narrow hard pal-ate (Figure 2-5)18 may predispose thepatient to have SDB Katz and col-leagues19 have shown that patients withOSA have significantly increased neckcircumference compared to nonapneicsnorers greater distribution of neck fat
may contribute to mass loading on theupper airway in patients with OSA Thepatientrsquos neck circumference should bemeasured at the superior border of thecricothyroid membrane19 A neck cir-cumference greater than 40 cm (157in) has been shown to be predictive ofOSA with 61 sensitivity and 93specificity regardless of sex20
Assessment of the patientrsquos anteriorand posterior dentition can also re-veal anatomic findings that may pre-dispose a person to certain sleepdisorders Two features to note in eval-uation of the anterior dentition areoverjet and overbite (Figure 2-6)21
Overjet as shown in Figure 2-712 isthe horizontal distance between theupper right central incisor and thebuccal surface of the correspondinglower tooth while overbite is the ver-tical distance between these twopoints22 These measurements are typ-ically reported in millimeters The An-gle classification system is used todescribe the first molar position on
FIGURE 2-4 Tonsil size grading Thisstructural abnormality canpredispose a patient to havesleep-disordered breathing
Reprinted from Kryger MH Elsevier12 B 2010 withpermission from Elsevier
FIGURE 2-5 Deficientmaxillarydevelopment inan individual with
Down syndrome leading to highand narrow hard palate
Reprinted with permission from ChengRHW et al InTech18 B 2011 W KeungLeung wwwintechopencombooksprenatal-diagnosis-and-screening-for-down-syndromeoral-health-in-individuals-with-down-syndrome
FIGURE 2-6 Overjet andoverbite Overjetis defined as
increased projection of the upperteeth in front of the lower teethas measured parallel to theocclusal plane Overbite is thevertical overlapping of maxillaryteeth over mandibular teethusually measured perpendicularto the occlusal plane
Reprinted from Saccucci M et al Scoliosis21
B 2011 BioMed Central Ltd wwwscoliosisjournalcomcontent6115
38 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
the mandibular and maxillary dentalarches23 Figure 2-8 shows class I oc-clusion and class II and III malocclu-
sion Of note the mesiobuccal surfaceis the aspect of the tooth that is adja-cent to the cheek mucosa
The Adult Obstructive Sleep ApneaTask Force of the American Academyof Sleep Medicine (AASM) recommen-ded in recent clinical guidelines24 thatthe following physical findings maysuggest the presence of OSA increasedneck circumference (greater than 432cm [17 in] in men greater than 406 cm[16 in] in women) BMI 30 kgm2 orgreater modified Mallampati classifica-tion of III or IV presence of retrognathialateral peritonsillar narrowing macro-glossia tonsillar hypertrophy elongatedenlarged uvula high-archednarrowhard palate nasal abnormalities (egpolyps deviation valve abnormalities
KEY POINT
h Classification of thepatientrsquos dentition helpsto evaluate the positionof the maxillary archrelative to themandibular arch
FIGURE 2-7 OverjetDisplacementof the
mandibular teeth posteriorly inrelationship to the maxillary teethresults inmoreposteriorly crowdedupper airways predisposingpatients for the developmentof obstructive sleep apnea
Reprinted from Kryger MH Elsevier12
B 2010 with permission from Elsevier
FIGURE 2-8 Angle class occlusionmalocclusion A Angle class I occlusion also known asneutrocclusion The mandibular and maxillary dental arches have a normalanterior-posterior relationship The mesiobuccal groove of the mandibular first
molar interdigitates with the mesiobuccal cusp of the maxillary first molar B Angle class IImalocclusion also known as distoclusion The mandibular dental arch is in distal anterior-posteriorrelationship to the maxillary dental arch The mesiobuccal groove of the mandibular first molar isdistal to the mesiobuccal cusp of the maxillary first molar C Angle class III malocclusion alsoknown as mesioclusion The mandibular dental arch is in mesial anterior-posterior relationship tothe maxillary dental arch The mesiobuccal groove of the mandibular first molar is mesial to themesiobuccal cusp of the maxillary first molar
Reprinted fromMorcos SS Patel PK Clin Plast Surg23 B 2007 with permission from Elsevier wwwsciencedirectcomsciencearticlepiiS0094129807000843
39Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
and turbinate hypertrophy) andoroverjet To prevent overlooking thesefindings a thorough head and neckassessment as described in Table 2-2should be incorporated into the phys-ical examination of all patients whopresent with sleep-related complaints
SUBJECTIVE ASSESSMENTSeveral patient-completed question-naires are inexpensive and time-efficient
reasonably well validated and com-monly used They can help to increasestandardization in evaluations of patientsby different clinicians or across centersPerhaps the most well-known andwidely used is the Epworth SleepinessScale25 a subjective assessment of thepatientrsquos daytime sleep propensity inrecent times As shown in Appendix Athe Epworth Sleepiness Scale asks theresponder to use a four-point Likertscale (0 1 2 or 3) to indicate thelikelihood of dozing in eight distinctsedentary conditions A total score of 10or greater out of a possible 24 suggestsexcessive daytime sleepiness25 Whilethe Epworth Sleepiness Scale score canbe easily incorporated into the clinicalevaluation it should not be used as asubstitute for objective measurement ofsleepiness The Epworth Sleepiness Scalescore may correlate to a limited extentwith the presence and severity of OSA26
but some studies have failed to find anystatistically significant association withmean sleep latency on multiple sleep la-tency tests or with severity of OSA27
The most advantageous use of theEpworth Sleepiness Scale may be to followan individualrsquos self-assessment of sleep-iness longitudinally and it may also serveas an indicator of treatment response
Many other questionnaires may beutilized in a clinical sleep evaluationsome pertain to overall sleep qualitywhile others are disorder-specific ThePatient Reported Outcomes Measure-ment Information System (PROMIS) isan NIH-supported system of measuresfor patient-reported health status andincludes questions on sleep disturb-ance The Pittsburgh Sleep QualityIndex (PSQI) is a validated question-naire that inquires about sleep qualityand disturbances over the previousmonth28 The parent-completed Pe-diatric Sleep Questionnaire29 containsa validated reliable 22-item scale tohelp assess risk for SDB in children
KEY POINTS
h The Epworth SleepinessScale apatient-completedquestionnaire assessesthe patientrsquos subjectivetendency to doze duringsedentary situations inrecent times not onlyat the moment thequestionnaire iscompleted
h The Epworth SleepinessScale should not beused in lieu of diagnostictesting but may be avaluable componentof ongoing clinicalevaluation
TABLE 2-2 Head and NeckExamination
b Face
Featuresof long face syndrome
Infraorbital darkening
Mouth breathing
Elongated midface
Nasal atrophy
b Oral Airway
Mandibular retrognathia
Low soft palate (modifiedMallampati classification)
Large or boggy uvula
Erythematous pillars
Tonsillar hypertrophy
High narrow hard palate
Neck circumference
Overjet
Overbite
Angle classification(malocclusion)
Macroglossia
Worn occlusive surfaces(suggestive of bruxism)
b Nasal Airway
Symmetry of the nares
Nasal septum deviation
Nasal airflow
Collapse of nasal alae oninspiration
b Neck
Neck circumference
40 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
The STOP-BANG questionnaire devel-oped and validated in preoperativepatients is a sensitive screening toolfor OSA Four questions address snor-ing tiredness during daytime observedapnea and high blood pressure whereasfour other measures focus on increasedOSA risk factors of BMI (greater than 35kgm2) age (older than 50 years) neckcircumference (greater than 40 cm[1575 in]) and gender (male preva-lence)30 The International RestlessLegs Syndrome Study Group Rating Scale(IRLS) is a validated assessment of dis-ease severity for patients with restlesslegs syndrome31 The patientrsquos perceived
level of insomnia may be assessed withthe Insomnia Severity Index (ISI) avalidated 7-item questionnaire32
A sleep diary (Figure 2-9)33 allows apatient to chart daily sleep and waketimes and should be maintained for atleast 2 consecutive weeks Review ofthis information allows the clinicianto estimate the total amount of sleepthe patient obtains in a 24-hour pe-riod The sleep diary also can provideinsight into the patientrsquos sleep patternIs sleep obtained at the same timesevery day Is the patientrsquos sleep con-solidated or fragmented across 24hours Does the patient sleep and
FIGURE 2-9 Sleep diary completed by a 46-year-old woman who presented with difficulty falling asleep Vertical linesrepresent when the patient went to bed lsquolsquoMrsquorsquo refers to when medication was taken black shading representstime asleep and unshaded white areas are time spent awake
Diary template reprinted from YOURSLEEPaasmnetorg from the American Academy of Sleep Medicine yoursleepaasmnetorgpdfsleepdiarypdf33
41Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
wake at conventional times or doeshe or she appear to be a lsquolsquonight owlrsquorsquoor lsquolsquomorning larkrsquorsquo Answers to thesequestions as provided by the sleepdiary may reveal factors that contrib-ute to sleep-related concerns Use ofsleep diaries can be particularly help-ful in patients with suspected circadianrhythm sleep disorders (including shiftwork) behaviorally induced insufficientsleep or inadequate sleep hygiene
OBJECTIVE MEASURESNocturnal polysomnography (NPSG)or related assessments are indicatedfor the diagnosis and assessment ofSDB and for positive airway titrationin patients with confirmed SDB Theprocedure can also provide informationabout EEG activity nocturnal move-ments cardiac rhythm and oxygen
saturation34 The recommended record-ing montage used in NPSG as shownin Figure 2-10 includes central (C3-A2C4-A1) frontal (F3-A2 F4-A1) andoccipital (O1-A2 O2-A1) EEGs left andright eye electrooculograms mentalsubmental surface EMG and ECG leadsOther recorded parameters includethoracic and abdominal effort oxygensaturation nasaloral airflow and bodyposition Use of a microphone torecord snoring is recommended butnot required34 A full 16-lead EEG(Figure 2-11)35 and video recordingmay be performed when nocturnalseizures are suspected Leg surfaceEMG leads are recommended andadditional arm EMG leads may beapplied when the clinical history sug-gests complex sleep-related motor be-haviors such as dream enactment In
KEY POINT
h A daily sleep diary helpsto summarize a patientrsquossleep-wake schedulemore accurately thanmemory often allowsand can facilitateconstruction ofpersonalized plansfor management ofcircadian rhythm sleepdisorders and insomnia
FIGURE 2-10 A 1-minute epoch from a nocturnal polysomnogram showing obstructive sleepapnea in a 46-year-old man who presented with snoring daytime sleepinessand headaches It depicts the standard recording montage that includes the
following leads central (C3-M2 C4-M1) frontal (F3-M2 F4-M1) and occipital (O1-M2 O2-M1)EEGs left and right eye electrooculograms (E1-M2 E2-M1) mentalsubmental electromyogram(Chin1-Chin2) electrocardiogram (ECG1-ECG2 ECG2-ECG3) snore volume (SNORE) nasalpressure transducer (NPRE) nasaloral airflow (NO) thoracic (THOR) and abdominal (ABD)effort arterial oxyhemoglobin saturation (SpO2) plethysmography (Pleth) and left and right eyeelectromyograms (LAT1-LAT2 RAT1-RAT2)
42 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
most cases the diagnostic NPSG is doneon 1 night although NPSG on 2 con-secutive nights may be considered inthe evaluation of parasomnias
Four categories of sleep monitoringdevices for use in the diagnosis of sleepdisorders have often been described34
These are type 1 standard attended in-laboratory polysomnography type 2comprehensive portable unattendedpolysomnography type 3 modifiedportable sleep apnea testing (often car-diorespiratory studies that do not recordsleep) and type 4 continuous single ordual bioparameter recording (eg pulseoximetry) However this categorizationmay not effectively classify the plethoraof out-of-center testing devices currentlyavailable for clinical use Therefore anew device classification system hasrecently been proposed This schemaknown as the SCOPER system catego-rizes out-of-center testing devices basedon measurement of sleep cardiovascu-
lar oximetry position effort and res-piratory parameters36 Within each ofthe six SCOPER categories a level of 0through 5 is assigned as indicated bythe type of sensor or measurementthat the device uses for that category
The most recent clinical guidelinespublished by the Portable MonitoringTask Force of the AASM37 for use ofunattended portable monitoring inthe diagnosis of OSA in adult patientsrecommend that portable monitoringonly be performed in conjunction witha comprehensive sleep evaluation by(or supervised by) a practitioner board-certified in sleep medicine or eligiblefor the certification examination Theseguidelines state that portable monitor-ing may be used in place of NPSG inpatients with a high pretest probabilityof moderate to severe OSA Portablemonitoring should not be used inpatients with significant medical comor-bidities (including but not limited to
KEY POINT
h The complexclassification of portabletesting devices reflectsthe multitude of designsavailable to cliniciansand will undoubtedlychange as technologyadvances
FIGURE 2-11 A The international 10Y20 system for EEG electrode placement refers to the10 and 20 interelectrode distances Even electrode numbers (2 4 6 8)represent the right hemisphere and odd electrode numbers (1 3 5 7)
represent the left hemisphere B Recommended F4-M1 C4-M1 O2-M1 placements of EEGelectrodes as set forth by the American Academy of Sleep Medicine (AASM)
Adapted from Iber C et al American Academy of SleepMedicine35 Used with permission of the American Academy ofSleep Medicine Darien IL 2012
43Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
moderate to severe pulmonary diseaseneuromuscular disease or congestiveheart failure) in patients with othersleep disorders (including central sleepapnea periodic limb movement disor-der insomnia parasomnias circadianrhythm disorders or narcolepsy) or asa screening tool The use of portablemonitoring may be indicated for thediagnosis of OSA in patients for whomattended NPSG is not possible becauseof immobility safety or critical illnessPortable monitoring may be indi-cated to monitor the response to non-continuous positive airway pressuretreatments for OSA including oralappliances upper airway surgery andweight loss The algorithm shown inAppendix B may help in the determi-nation of an adult patientrsquos candidacyfor out-of-center testing for the diag-nosis of OSA An example of portable(or home) monitoring technology isshown in Supplemental Digital Con-tent 2-1 linkslwwcomCONTA15
Recommended technology for port-able monitoring should record at mini-mum airflow respiratory effort andblood oxygenation the airflow effortand oximetric biosensors typically usedfor attended NPSG should be used37
These guidelines published in 2007will likely continue to evolve as newtechnologies emerge and are found tobe effective The current guidelinesrecommend that out-of-center testingbe performed under the auspices of anAASM-accredited comprehensive sleepmedicine program and that a board-certifiedeligible sleep specialist reviewthe raw data from a portable monitor-ing device All patients who undergoportablemonitoring for the diagnosis ofOSA should have a follow-up visit toreview test results Negative or techni-cally inadequate portable monitoringstudies should be followed by attendedin-laboratory NPSG if the clinical suspi-cion for SDB remains high37
The aforementioned testing proce-dures are primarily used in the evalua-tion of SDB Other testing modalitiesare useful in the diagnosis of othercategories of sleep disorders The mul-tiple sleep latency test (MSLT) and itsvariant the maintenance of wakefulnesstest (MWT) are used in the evaluation ofhypersomnia The conventional record-ing montage is similar to that used fornocturnal polysomnography central fron-tal and occipital EEGs left and right eyeelectrooculograms mentalsubmentalEMG and ECG leads Measurement ofthoracic and abdominal effort oxygensaturation and nasaloral airflow are notrequired but may help explain delayedsleep latencies for patients in whomrespiratory disturbances interfere withsleep onset
The MSLT is a validated tool that isconsidered the de facto standard forobjective assessment of excessive day-time sleepiness38 The recommendedprotocol38 involves five 20-minute napopportunities held at 2-hour intervalsthroughout the day If sleep is ob-served the patient is allowed to sleepfor at least 15 minutes The sleep la-tency for each nap is measured as thetime from the start of the nap trial tothe first epoch of sleep A sleep la-tency of 20 minutes is assigned to naptrials during which no sleep isobserved39 The mean sleep latencycalculated as the average sleep latencyacross all nap trials is the final resultThe presence and number of sleep-onset REM periods (SOREMPs) is alsodetermined as this information canhelp to establish a diagnosis of narco-lepsy without cataplexy or to confirmnarcolepsy with cataplexy
The MSLT should be started 15 to30 hours following completion of anocturnal polysomnogram whichshould record at least 6 hours of sleepin order for determination of the meansleep latency to be valid Drugs that may
KEY POINT
h Careful considerationshould be given tothe indications forout-of-center testingAttended nocturnalpolysomnography isindicated if a portablestudy yields a negativeor technicallyinadequate result
44 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
interfere with sleep latency or REM la-tency should be discontinued 2 weeksbefore testing whenever possible Ascreen may be performed on the day oftesting if there is suspicion that pre-scribed or illicit substances may con-tribute to the patientrsquos sleepiness38
No large multicenter systematicallycollected normative data are availablefor mean sleep latency values on theMSLT38 Nonetheless a mean sleep la-tency of greater than 10 minutes is of-ten considered normal whereas a meansleep latency of 8 to 10 minutes is con-sidered a physiologic gray zone40 Thenormative data for children are classi-fied by Tanner stage of developmentthough the MSLT is typically not per-formed in children aged younger than 6or 7 years because some daytime nap-ping may still be normal in youngchildren41 The second edition of theInternational Classification of SleepDisorders Diagnostic and CodingManual (ICSD-2)42 requires the pres-ence of a mean sleep latency of lessthan 8 minutes and two or moreSOREMPs as part of the diagnosticcriteria for narcolepsy without cata-plexy However the ICSD-2 also notesthat a mean sleep latency of less than 8minutes may occur in up to 30 of thegeneral population Therefore whilethe MSLT is a helpful and widely usedtool it remains an imperfect gold stand-ard in the assessment of daytime sleepi-ness This necessitates that theevaluation of daytime sleepiness notrest on the MSLT results alone butassimilate the clinical history subjectivecomplaints diagnostic study results andother pertinent medical information38
Practice parameters from theAASM state that the MSLT is indicatedfor diagnostic confirmation of sus-pected narcolepsy and may be indi-cated to differentiate idiopathichypersomnia from narcolepsy38 TheMSLT is not indicated for routine
assessment of OSA syndrome or toassess response to treatment of SDBand is not routinely indicated for eval-uation of sleepiness in medical orneurologic disorders (except for narco-lepsy) insomnia or circadian rhythmdisorders
TheMWTprovides an objectivemeas-ure of a patientrsquos ability to remain awakerather than the tendency to fall asleepduring the day The key differencebetween the MWT and the MSLT is thatin the former the patient is asked to tryto stay awake under circumstances con-ducive to sleep rather than to fall asleepThe MWT provides an objective vali-dated assessment of the ability to remainawake for a defined length of time38 Therecommended protocol includes four40-minute trials that begin at 2-hourintervals with the first trial to start 15 to30 hours after the patientrsquos wake-uptime A nocturnal polysomnogram onthe preceding night is not requiredHowever the patient should obtain asufficient amount of sleep during thenight before the MWT Each trial isterminated after 40 minutes if no sleepoccurs or after unequivocal sleep onset(defined as three continuous epochsof stage N1 sleep or one epoch of anyother stage of sleep) has occurred38
One indication for the MWT is to as-sess an individualrsquos ability to remainawake when his or her inability to re-main awake constitutes a public orpersonal safety issue This can becomea pressing issue for individuals em-ployed in the transportation43 con-struction or health care industriesThe MWT may be indicated to assesstreatment response in patients withknown excessive daytime sleepiness
Limited amounts of normative dataare available for the MWT Historicallymultiple testing protocols make syn-thesis of results more challenging TheMWT is used much less often in clinicalpractice compared to the MSLT Patient
KEY POINTS
h The multiple sleeplatency test is the goldstandard for objectiveassessment of daytimesleepiness butinterpretation of theresults must be madewithin the clinicalcontext of the patientrsquoshistory
h In the multiple sleeplatency test the patientis instructed to try tosleep during each naptrial In the maintenanceof wakefulness test thepatient is instructed totry to remain awakeduring the nap trial
h A baseline nocturnalpolysomnogram isrequired before amultiple sleep latencytest and considered butnot required before amaintenance ofwakefulness test
45Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
age may also affect the mean sleep la-tency values on both the MWT and theMSLT43 and may represent evolution ofcircadian rhythm and sleep architec-ture across the lifetime A study of 383patients with narcolepsy with cataplexyexamined the clinical and polysomno-graphic data at the time of diagnosis(age range 5 to 84 years) and found aprogressive decrease in the number ofSOREMPs and a progressive increase inthe mean sleep latency on the MSLT asa function of age44 Given its limita-tions the MWT may thus be used tosupplement the clinical history in theassessment of ability to stay awake butshould not be the sole determinant ofthis parameter
Actigraphy is also used in the clinicalevaluation of patients with sleep disor-ders particularly circadian rhythm sleepdisorders An actigraph is a watchlikedevice that is worn on the wrist for anextended period usually in the range ofweeks The actigraph records move-ment and uses an algorithm to estimatethe amounts of sleep and wake timeduring the recording period Analysissoftware uses movement to estimatewhen sleep and wakefulness haveoccurred Review of the data can pro-vide objective insight into the patientrsquossleep pattern including timing andduration of major sleep disruptionsActigraphy is indicated as part of theevaluation of patients with advancedsleep-phase syndrome delayed sleep-phase syndrome and shift work disor-der and may be indicated in the evalua-tion of jet lag disorder and nonY24-hoursleep-wake syndrome including thatassociated with blindness45 It can alsoserve as a measure of treatment re-sponse in patients with insomnia andcircadian rhythm sleep disorders Forpopulations in which traditional sleepmonitoring may be challenging suchas pediatric or older adult patientsactigraphy may provide valuable infor-
mation about the patientrsquos sleep pat-tern or response to treatment Whenpolysomnography is not availableactigraphy is indicated to estimate totalsleep time in patients with OSA45
OTHER ASSESSMENTMODALITIESLaboratory evaluation and neuroimag-ing with either CT or MRI may beconsidered on an individual basis asindicated by the clinical history Com-plete blood count (CBC) serum chem-istries or measures of thyroid functionmay be obtained if an underlying med-ical disorder is thought to contribute tothe patientrsquos sleep symptoms Forinstance these laboratory studies maybe consideredwhen daytime fatigue is apredominant symptom Serum ironstudies including ferritin level shouldbe checked in patients with restless legssyndrome46 Neuroimaging should beconsidered in patients with antecedenttrauma or for any sleep disorder pa-tient with an abnormal neurologic ex-amination to evaluate for a structuraletiology of the patientrsquos symptoms
APPROACH TO THE PATIENTEvaluation of suspected sleep disordersis best accomplished by a stepwisemultidimensional approach (Case 2-2)A thorough sleep history includes de-tailed description of sleep-related symp-toms nocturnal behaviors the patientrsquossleep schedule level of daytime sleepi-ness and subsequent effects on daytimefunctioning Collateral history from thepatientrsquos bed partner or family is oftennecessary to understand the severity andcontext of the patientrsquos symptoms Sub-jective assessments of sleepiness suchas the Epworth Sleepiness Scale areeasily administered and useful to tracksymptomatic progression or treatmentresponse from one visit to the nextCertain physical examination findingsmay also raise clinical suspicion of
KEY POINTS
h Actigraphy can beuseful in evaluation andtreatment of circadianrhythm sleep disordersand in management ofinsomnia
h Neuroimaging is notroutinely indicated inthe clinical evaluation ofsleep disorders andshould be pursued on acase-by-case basis
46 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
particular sleep disorders For patientsin whom multiple sleep disorders aresuspected systematic use of diagnostictesting allows for accurate identificationof specific diagnoses In a patient withinsomnia and symptoms suggestive ofSDB nocturnal polysomnography shouldbe the first procedure performed Ifthe insomnia persists despite adequatetreatment of SDB further evaluationwith sleep diaries and possibly actigra-
phy may be considered to better char-acterize the patientrsquos sleep patternActigraphy may then again be pursuedto gauge treatment response upon man-agement of the patientrsquos insomnia
The diagnostic modalities availablefor evaluation of sleep disorders arerapidly evolving In-laboratory nocturnalpolysomnography currently remains thegold standard for assessment of SDBHowever the multitude of out-of-center
KEY POINT
h Careful assimilation ofthe clinical history thesleep-specific physicalexamination patientquestionnaires anddiagnostic test resultsleads to the mostaccurate assessment ofpatients with symptomsrelated to sleep oralertness
Case 2-2A 23-year-old woman reported a 4-year history of insomnia Throughoutcollege she was a lsquolsquonight owlrsquorsquo never scheduled classes that started before100 PM and always did well in school During the past 6 months shedeveloped progressive difficulty staying awake in her job as a financialanalyst andwas concerned about how this might affect her job performance
During the week she was in bed by midnight but was unable to fallasleep until 200 AM and awoke with difficulty to an alarm at 600 AMfeeling tired She denied any thought rumination or physical discomfortat bedtime She had tried over-the-counter sleep aids that provided nosymptomatic improvement and worsened morning grogginess Onweekends she slept from 200 AM to 1100 AM and awakened feelinglsquolsquopretty goodrsquorsquo She had nocturia up to once per night and occasionalmorning headaches She had no bed partner but reported gaspingrespirations nocturnal palpitations and snort arousals On about 4 nightsper week she experienced a sensation of needing to move her legswhile trying to fall asleep This sensation was relieved by movement andwas worse at night than during the day Her legs sometimes movedspontaneously at night or while seated quietly for long periods duringthe day She felt sleepy during the afternoon especially while workingat her computer She denied drowsiness while driving She occasionallytook a 30-minute nap on the weekend and found it to be refreshingShe drank one to two cups of coffee every morning and had a 12-oz dietcaffeinated soda at 300 PM Her sleepiness had not caused her to makeany mistakes at work and she denied any mood disturbance
Physical examination was notable for a body mass index of 32 kgm2 neckcircumference of 381 cm (15 in) and modified Mallampati class III oral airwayNasal passages were narrow with turbinate hypertrophy bilaterally andhard palate was high-arched and narrow Nomicrognathia or retrognathia waspresent She had molar occlusion class I bilaterally with no overjet or overbiteThe general cardiac respiratory and neurologic examinations were normal
Comment This case illustrates how discussion of the chief complaint raisessuspicion for multiple sleep disorders The history suggests a circadian rhythmsleep disorder particularly delayed sleep-phase syndrome sleep-disorderedbreathing and restless legs syndrome Diagnostic evaluation should includenocturnal polysomnogramwith consideration toperform testing at the patientrsquospreferred sleep time and serum iron studies Sleep diaries andor actigraphymay be considered for further assessment of the patientrsquos sleep pattern
47Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
testing devices continues to grow andmany may provide useful alternativesthat under appropriate circumstancescould allow more expedient conven-ient and less costly evaluations ofincreased numbers of patients whopreviously had only limited or delayedaccess to sleep services
VIDEO LEGENDSupplemental Digital Content 2-1
Home sleep study Video demonstrates a homesleep study using an unattended type 3 portablemonitoring device The patient is a 56-year-oldman who is experiencing morning headachesand concentration and alertness problems atwork He has a history of mild snoring and ar-terial hypertension His Epworth SleepinessScale score is 18 his neck circumference is19 in he has a Mallampati classification score ofIII and his body mass index is 41 kgm Theapnea-hypopnea index is 84 eventsh Channelsrecorded in this sleep study include arterialoxyhemoglobin saturation heart rate oral-nasalpressure flow snoring inductive plethysmog-raphy for chest efforts and body position
linkslwwcomCONTA15
B 2013 Marcel Hungs MD PhD Used withpermission
REFERENCES1 National Institutes of Health National
Center on Sleep Disorders ResearchSleep disorders research planwwwnhlbinihgovhealthprofsleep201101011NationalSleepDisordersResearch-PlanDHHSPublication11-7820pdf PublishedNovember 2011
2 Dinges DF An overview of sleepiness andaccidents J Sleep Res 19954(S2)4Y14
3 Mills RJ Young CA A medical definitionof fatigue in multiple sclerosis QJM 2008101(1)49Y60
4 Chervin RD Sleepiness fatigue tirednessand lack of energy in obstructive sleepapnea Chest 2000118(2)372Y379
5 Chotinaiwattarakul W OrsquoBrien LM Fan LChervin RD Fatigue tiredness and lack ofenergy improve with treatment for OSAJ Clin Sleep Med 20095(3)222Y227
6 American Academy of Sleep MedicineThe international classification of sleepdisorders diagnostic and coding manual2nd ed Westchester IL American Academyof Sleep Medicine 2005
7 Ebben MR Spielman AJNon-pharmacological treatments forinsomnia J Behav Med 200932(3)244Y254
8 Roth T Insomnia definition prevalenceetiology and consequences J Clin SleepMed 20073(5 suppl)S7YS10
9 Yang CM Spielman AJ Glovinsky PNonpharmacologic strategies in themanagement of insomnia Psychiatr ClinNorth Am 200629(4)895Y919 abstract viii
10 Katz ES DrsquoAmbrosio CM Pediatricobstructive sleep apnea syndrome ClinChest Med 201031(2)221Y234
11 Kohler M Bloch KE Stradling JR The role ofthe nose in the pathogenesis of obstructivesleep apnea Curr Opin Otolaryngol HeadNeck Surg 200917(1)33Y37
12 Kryger MH Atlas of clinical sleep medicinePhiladelphia PA Elsevier 2010
13 Zonato AI Martinho FL Bittencourt LRet al Head and neck physical examinationcomparison between nonapneic andobstructive sleep apnea patientsLaryngoscope 2005115(6)1030Y1034
14 Mallampati SR Gatt SP Gugino LD et alA clinical sign to predict difficult trachealintubation a prospective study Can AnaesthSoc J 198532(4)429Y434
15 Samsoon GL Young JR Difficult trachealintubation a retrospective studyAnaesthesia 198742(5)487Y490
16 Huang HH Lee MS Shih YL et alModified Mallampati classificationas a clinical predictor of peroralesophagogastroduodenoscopy toleranceBMC Gastroenterol 20111112
17 Friedman M Ibrahim H Bass L Clinicalstaging for sleep-disordered breathingOtolaryngol Head Neck Surg 2002127(1)13Y21
18 Cheng RHW Yiu CKY Leung WKOral health in individuals with Downsyndrome In Dey S ed Prenatal diagnosisand screening for down syndromeInTech wwwintechopencombookshowtoreferenceprenatal-diagnosis-and-screening-for-down-syndromeoral-health-in-individuals-with-down-syndromePublished 2011 Accessed August 24 2012
19 Katz I Stradling J Slutsky AS et al Dopatients with obstructive sleep apneahave thick necks Am Rev Respir Dis1990141(5 pt 1)1228Y1231
20 Kushida CA Efron B Guilleminault C Apredictive morphometric model for theobstructive sleep apnea syndrome AnnIntern Med 1997127(8 pt 1)581Y587
48 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
21 Saccucci M Tettamanti L Mummolo S et alScoliosis and dental occlusion a review ofthe literature Scoliosis 2011615
22 Battagel JM Kotecha B Dental side-effectsof mandibular advancement splint wear inpatients who snore Clin Otolaryngol200530(2)149Y156
23 Morcos SS Patel PK The vocabulary ofdentofacial deformities Clin Plast Surg200734(3)589Y599
24 Epstein LJ Kristo D Strollo PJ Jr et alClinical guideline for the evaluationmanagement and long-term care ofobstructive sleep apnea in adults J ClinSleep Med 20095(3)263Y276
25 Johns MW A new method for measuringdaytime sleepiness the Epworth sleepinessscale Sleep 199114(6)540Y545
26 Johns MW Daytime sleepiness snoring andobstructive sleep apnea The EpworthSleepiness Scale Chest 1993103(1)30Y36
27 Chervin RD Aldrich MS The EpworthSleepiness Scale may not reflect objectivemeasures of sleepiness or sleep apneaNeurology 199952(1)125Y131
28 Buysse DJ Reynolds CF 3rd Monk THet al The Pittsburgh Sleep Quality Index anew instrument for psychiatric practice andresearch Psychiatry Res 198928(2)193Y213
29 Chervin RD Hedger K Dillon JE Pituch KJPediatric sleep questionnaire (PSQ) validityand reliability of scales for sleep-disorderedbreathing snoring sleepiness and behavioralproblems Sleep Med 20001(1)21Y32
30 Chung F Yegneswaran B Liao P et al STOPquestionnaire a tool to screen patients forobstructive sleep apnea Anesthesiology2008108(5)812Y821
31 Walters AS LeBrocq C Dhar A et alValidation of the International Restless LegsSyndrome Study Group rating scale forrestless legs syndrome Sleep Med 20034(2)121Y132
32 Bastien CH Vallieres A Morin CMValidation of the Insomnia Severity Indexas an outcome measure for insomniaresearch Sleep Med 20012(4)297Y307
33 YOURSLEEPaasmnetorg from the AmericanAcademy of Sleep Medicine Two weeksleep diary yoursleepaasmnetorgpdfsleepdiarypdf Accessed August 24 2012
34 Kushida CA Littner MR Morgenthaler Tet al Practice parameters for the indicationsfor polysomnography and relatedprocedures an update for 2005 Sleep200528(4)499Y521
35 Iber C Ancoli-Israel S Chesson A et alThe AASM manual for scoring of sleep andassociated events rules terminology andtechnical specifications 1st ed WestchesterIL American Academy of Sleep Medicine2007
36 Collop NA Tracy SL Kapur V et alObstructive sleep apnea devices forout-of-center (OOC) testing technologyevaluation J Clin Sleep Med 20117(5)531Y548
37 Collop NA Anderson WM Boehlecke Bet al Clinical guidelines for the use ofunattended portable monitors in thediagnosis of obstructive sleep apnea in adultpatients Portable Monitoring Task Forceof the American Academy of SleepMedicine J Clin Sleep Med 20073(7)737Y747
38 Littner MR Kushida C Wise M et alStandards of Practice Committee of theAmerican Academy of Sleep MedicinePractice parameters for clinical use of themultiple sleep latency test and themaintenance of wakefulness test Sleep200528(1)113Y121
39 Carskadon MA Dement WC Mitler MMet al Guidelines for the multiple sleeplatency test (MSLT) a standard measure ofsleepiness Sleep 19869(4)519Y524
40 van den Hoed J Kraemer H Guilleminault Cet al Disorders of excessive daytimesomnolence polygraphic and clinical datafor 100 patients Sleep 19814(1)23Y37
41 Hoban TF Chervin RD Assessment ofsleepiness in children Semin PediatrNeurol 20018(4)216Y228
42 ICSD-2 The international classification ofsleep disorders pocket version diagnosticand coding manual 2nd ed WestchesterIL American Academy of Sleep Medicine2005
43 Arand D Bonnet M Hurwitz T et alThe clinical use of the MSLT and MWTSleep 200528(1)123Y144
44 Dauvilliers Y Gosselin A Paquet J et alEffect of age on MSLT results in patientswith narcolepsy-cataplexy Neurology200462(1)46Y50
45 Morgenthaler T Alessi C Friedman Let al Practice parameters for the use ofactigraphy in the assessment of sleep andsleep disorders an update for 2007 Sleep200730(4)519Y529
46 Gamaldo CE Earley CJ Restless legssyndrome a clinical update Chest2006130(5)1596Y1604
49Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
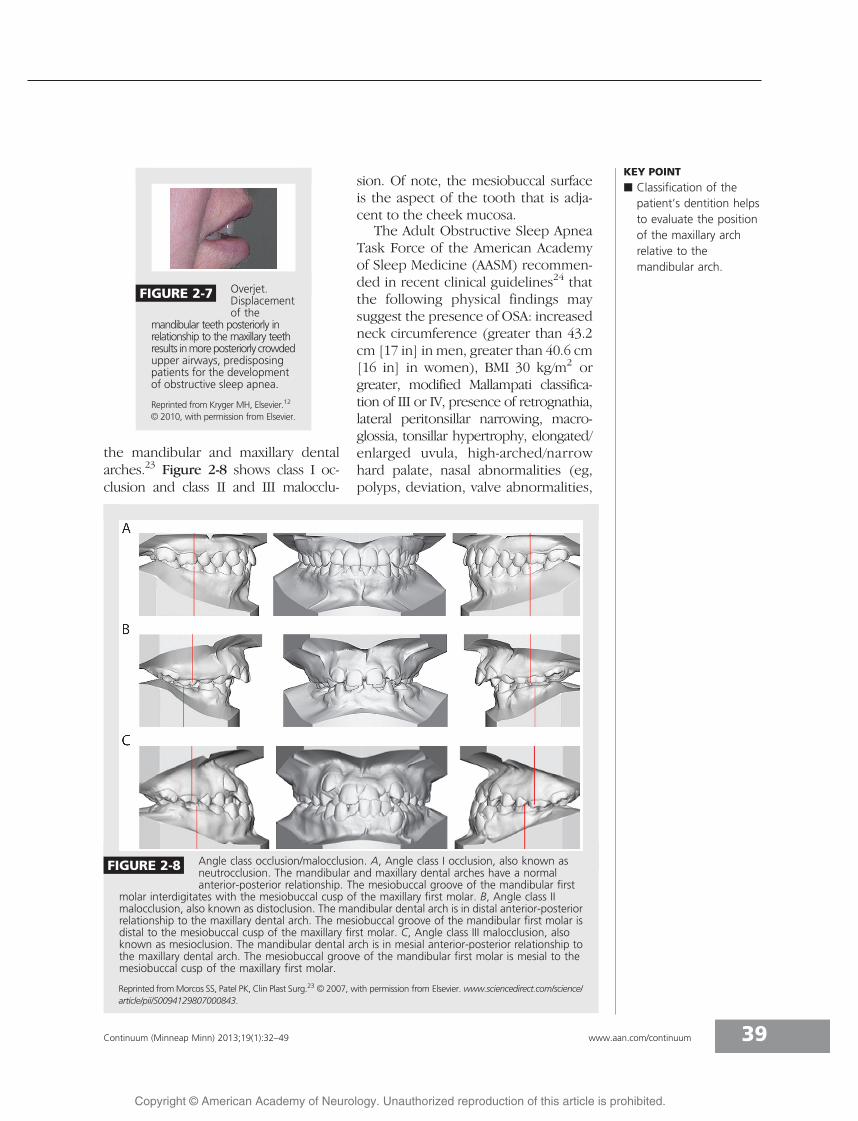
the mandibular and maxillary dentalarches23 Figure 2-8 shows class I oc-clusion and class II and III malocclu-
sion Of note the mesiobuccal surfaceis the aspect of the tooth that is adja-cent to the cheek mucosa
The Adult Obstructive Sleep ApneaTask Force of the American Academyof Sleep Medicine (AASM) recommen-ded in recent clinical guidelines24 thatthe following physical findings maysuggest the presence of OSA increasedneck circumference (greater than 432cm [17 in] in men greater than 406 cm[16 in] in women) BMI 30 kgm2 orgreater modified Mallampati classifica-tion of III or IV presence of retrognathialateral peritonsillar narrowing macro-glossia tonsillar hypertrophy elongatedenlarged uvula high-archednarrowhard palate nasal abnormalities (egpolyps deviation valve abnormalities
KEY POINT
h Classification of thepatientrsquos dentition helpsto evaluate the positionof the maxillary archrelative to themandibular arch
FIGURE 2-7 OverjetDisplacementof the
mandibular teeth posteriorly inrelationship to the maxillary teethresults inmoreposteriorly crowdedupper airways predisposingpatients for the developmentof obstructive sleep apnea
Reprinted from Kryger MH Elsevier12
B 2010 with permission from Elsevier
FIGURE 2-8 Angle class occlusionmalocclusion A Angle class I occlusion also known asneutrocclusion The mandibular and maxillary dental arches have a normalanterior-posterior relationship The mesiobuccal groove of the mandibular first
molar interdigitates with the mesiobuccal cusp of the maxillary first molar B Angle class IImalocclusion also known as distoclusion The mandibular dental arch is in distal anterior-posteriorrelationship to the maxillary dental arch The mesiobuccal groove of the mandibular first molar isdistal to the mesiobuccal cusp of the maxillary first molar C Angle class III malocclusion alsoknown as mesioclusion The mandibular dental arch is in mesial anterior-posterior relationship tothe maxillary dental arch The mesiobuccal groove of the mandibular first molar is mesial to themesiobuccal cusp of the maxillary first molar
Reprinted fromMorcos SS Patel PK Clin Plast Surg23 B 2007 with permission from Elsevier wwwsciencedirectcomsciencearticlepiiS0094129807000843
39Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
and turbinate hypertrophy) andoroverjet To prevent overlooking thesefindings a thorough head and neckassessment as described in Table 2-2should be incorporated into the phys-ical examination of all patients whopresent with sleep-related complaints
SUBJECTIVE ASSESSMENTSeveral patient-completed question-naires are inexpensive and time-efficient
reasonably well validated and com-monly used They can help to increasestandardization in evaluations of patientsby different clinicians or across centersPerhaps the most well-known andwidely used is the Epworth SleepinessScale25 a subjective assessment of thepatientrsquos daytime sleep propensity inrecent times As shown in Appendix Athe Epworth Sleepiness Scale asks theresponder to use a four-point Likertscale (0 1 2 or 3) to indicate thelikelihood of dozing in eight distinctsedentary conditions A total score of 10or greater out of a possible 24 suggestsexcessive daytime sleepiness25 Whilethe Epworth Sleepiness Scale score canbe easily incorporated into the clinicalevaluation it should not be used as asubstitute for objective measurement ofsleepiness The Epworth Sleepiness Scalescore may correlate to a limited extentwith the presence and severity of OSA26
but some studies have failed to find anystatistically significant association withmean sleep latency on multiple sleep la-tency tests or with severity of OSA27
The most advantageous use of theEpworth Sleepiness Scale may be to followan individualrsquos self-assessment of sleep-iness longitudinally and it may also serveas an indicator of treatment response
Many other questionnaires may beutilized in a clinical sleep evaluationsome pertain to overall sleep qualitywhile others are disorder-specific ThePatient Reported Outcomes Measure-ment Information System (PROMIS) isan NIH-supported system of measuresfor patient-reported health status andincludes questions on sleep disturb-ance The Pittsburgh Sleep QualityIndex (PSQI) is a validated question-naire that inquires about sleep qualityand disturbances over the previousmonth28 The parent-completed Pe-diatric Sleep Questionnaire29 containsa validated reliable 22-item scale tohelp assess risk for SDB in children
KEY POINTS
h The Epworth SleepinessScale apatient-completedquestionnaire assessesthe patientrsquos subjectivetendency to doze duringsedentary situations inrecent times not onlyat the moment thequestionnaire iscompleted
h The Epworth SleepinessScale should not beused in lieu of diagnostictesting but may be avaluable componentof ongoing clinicalevaluation
TABLE 2-2 Head and NeckExamination
b Face
Featuresof long face syndrome
Infraorbital darkening
Mouth breathing
Elongated midface
Nasal atrophy
b Oral Airway
Mandibular retrognathia
Low soft palate (modifiedMallampati classification)
Large or boggy uvula
Erythematous pillars
Tonsillar hypertrophy
High narrow hard palate
Neck circumference
Overjet
Overbite
Angle classification(malocclusion)
Macroglossia
Worn occlusive surfaces(suggestive of bruxism)
b Nasal Airway
Symmetry of the nares
Nasal septum deviation
Nasal airflow
Collapse of nasal alae oninspiration
b Neck
Neck circumference
40 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
The STOP-BANG questionnaire devel-oped and validated in preoperativepatients is a sensitive screening toolfor OSA Four questions address snor-ing tiredness during daytime observedapnea and high blood pressure whereasfour other measures focus on increasedOSA risk factors of BMI (greater than 35kgm2) age (older than 50 years) neckcircumference (greater than 40 cm[1575 in]) and gender (male preva-lence)30 The International RestlessLegs Syndrome Study Group Rating Scale(IRLS) is a validated assessment of dis-ease severity for patients with restlesslegs syndrome31 The patientrsquos perceived
level of insomnia may be assessed withthe Insomnia Severity Index (ISI) avalidated 7-item questionnaire32
A sleep diary (Figure 2-9)33 allows apatient to chart daily sleep and waketimes and should be maintained for atleast 2 consecutive weeks Review ofthis information allows the clinicianto estimate the total amount of sleepthe patient obtains in a 24-hour pe-riod The sleep diary also can provideinsight into the patientrsquos sleep patternIs sleep obtained at the same timesevery day Is the patientrsquos sleep con-solidated or fragmented across 24hours Does the patient sleep and
FIGURE 2-9 Sleep diary completed by a 46-year-old woman who presented with difficulty falling asleep Vertical linesrepresent when the patient went to bed lsquolsquoMrsquorsquo refers to when medication was taken black shading representstime asleep and unshaded white areas are time spent awake
Diary template reprinted from YOURSLEEPaasmnetorg from the American Academy of Sleep Medicine yoursleepaasmnetorgpdfsleepdiarypdf33
41Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
wake at conventional times or doeshe or she appear to be a lsquolsquonight owlrsquorsquoor lsquolsquomorning larkrsquorsquo Answers to thesequestions as provided by the sleepdiary may reveal factors that contrib-ute to sleep-related concerns Use ofsleep diaries can be particularly help-ful in patients with suspected circadianrhythm sleep disorders (including shiftwork) behaviorally induced insufficientsleep or inadequate sleep hygiene
OBJECTIVE MEASURESNocturnal polysomnography (NPSG)or related assessments are indicatedfor the diagnosis and assessment ofSDB and for positive airway titrationin patients with confirmed SDB Theprocedure can also provide informationabout EEG activity nocturnal move-ments cardiac rhythm and oxygen
saturation34 The recommended record-ing montage used in NPSG as shownin Figure 2-10 includes central (C3-A2C4-A1) frontal (F3-A2 F4-A1) andoccipital (O1-A2 O2-A1) EEGs left andright eye electrooculograms mentalsubmental surface EMG and ECG leadsOther recorded parameters includethoracic and abdominal effort oxygensaturation nasaloral airflow and bodyposition Use of a microphone torecord snoring is recommended butnot required34 A full 16-lead EEG(Figure 2-11)35 and video recordingmay be performed when nocturnalseizures are suspected Leg surfaceEMG leads are recommended andadditional arm EMG leads may beapplied when the clinical history sug-gests complex sleep-related motor be-haviors such as dream enactment In
KEY POINT
h A daily sleep diary helpsto summarize a patientrsquossleep-wake schedulemore accurately thanmemory often allowsand can facilitateconstruction ofpersonalized plansfor management ofcircadian rhythm sleepdisorders and insomnia
FIGURE 2-10 A 1-minute epoch from a nocturnal polysomnogram showing obstructive sleepapnea in a 46-year-old man who presented with snoring daytime sleepinessand headaches It depicts the standard recording montage that includes the
following leads central (C3-M2 C4-M1) frontal (F3-M2 F4-M1) and occipital (O1-M2 O2-M1)EEGs left and right eye electrooculograms (E1-M2 E2-M1) mentalsubmental electromyogram(Chin1-Chin2) electrocardiogram (ECG1-ECG2 ECG2-ECG3) snore volume (SNORE) nasalpressure transducer (NPRE) nasaloral airflow (NO) thoracic (THOR) and abdominal (ABD)effort arterial oxyhemoglobin saturation (SpO2) plethysmography (Pleth) and left and right eyeelectromyograms (LAT1-LAT2 RAT1-RAT2)
42 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
most cases the diagnostic NPSG is doneon 1 night although NPSG on 2 con-secutive nights may be considered inthe evaluation of parasomnias
Four categories of sleep monitoringdevices for use in the diagnosis of sleepdisorders have often been described34
These are type 1 standard attended in-laboratory polysomnography type 2comprehensive portable unattendedpolysomnography type 3 modifiedportable sleep apnea testing (often car-diorespiratory studies that do not recordsleep) and type 4 continuous single ordual bioparameter recording (eg pulseoximetry) However this categorizationmay not effectively classify the plethoraof out-of-center testing devices currentlyavailable for clinical use Therefore anew device classification system hasrecently been proposed This schemaknown as the SCOPER system catego-rizes out-of-center testing devices basedon measurement of sleep cardiovascu-
lar oximetry position effort and res-piratory parameters36 Within each ofthe six SCOPER categories a level of 0through 5 is assigned as indicated bythe type of sensor or measurementthat the device uses for that category
The most recent clinical guidelinespublished by the Portable MonitoringTask Force of the AASM37 for use ofunattended portable monitoring inthe diagnosis of OSA in adult patientsrecommend that portable monitoringonly be performed in conjunction witha comprehensive sleep evaluation by(or supervised by) a practitioner board-certified in sleep medicine or eligiblefor the certification examination Theseguidelines state that portable monitor-ing may be used in place of NPSG inpatients with a high pretest probabilityof moderate to severe OSA Portablemonitoring should not be used inpatients with significant medical comor-bidities (including but not limited to
KEY POINT
h The complexclassification of portabletesting devices reflectsthe multitude of designsavailable to cliniciansand will undoubtedlychange as technologyadvances
FIGURE 2-11 A The international 10Y20 system for EEG electrode placement refers to the10 and 20 interelectrode distances Even electrode numbers (2 4 6 8)represent the right hemisphere and odd electrode numbers (1 3 5 7)
represent the left hemisphere B Recommended F4-M1 C4-M1 O2-M1 placements of EEGelectrodes as set forth by the American Academy of Sleep Medicine (AASM)
Adapted from Iber C et al American Academy of SleepMedicine35 Used with permission of the American Academy ofSleep Medicine Darien IL 2012
43Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
moderate to severe pulmonary diseaseneuromuscular disease or congestiveheart failure) in patients with othersleep disorders (including central sleepapnea periodic limb movement disor-der insomnia parasomnias circadianrhythm disorders or narcolepsy) or asa screening tool The use of portablemonitoring may be indicated for thediagnosis of OSA in patients for whomattended NPSG is not possible becauseof immobility safety or critical illnessPortable monitoring may be indi-cated to monitor the response to non-continuous positive airway pressuretreatments for OSA including oralappliances upper airway surgery andweight loss The algorithm shown inAppendix B may help in the determi-nation of an adult patientrsquos candidacyfor out-of-center testing for the diag-nosis of OSA An example of portable(or home) monitoring technology isshown in Supplemental Digital Con-tent 2-1 linkslwwcomCONTA15
Recommended technology for port-able monitoring should record at mini-mum airflow respiratory effort andblood oxygenation the airflow effortand oximetric biosensors typically usedfor attended NPSG should be used37
These guidelines published in 2007will likely continue to evolve as newtechnologies emerge and are found tobe effective The current guidelinesrecommend that out-of-center testingbe performed under the auspices of anAASM-accredited comprehensive sleepmedicine program and that a board-certifiedeligible sleep specialist reviewthe raw data from a portable monitor-ing device All patients who undergoportablemonitoring for the diagnosis ofOSA should have a follow-up visit toreview test results Negative or techni-cally inadequate portable monitoringstudies should be followed by attendedin-laboratory NPSG if the clinical suspi-cion for SDB remains high37
The aforementioned testing proce-dures are primarily used in the evalua-tion of SDB Other testing modalitiesare useful in the diagnosis of othercategories of sleep disorders The mul-tiple sleep latency test (MSLT) and itsvariant the maintenance of wakefulnesstest (MWT) are used in the evaluation ofhypersomnia The conventional record-ing montage is similar to that used fornocturnal polysomnography central fron-tal and occipital EEGs left and right eyeelectrooculograms mentalsubmentalEMG and ECG leads Measurement ofthoracic and abdominal effort oxygensaturation and nasaloral airflow are notrequired but may help explain delayedsleep latencies for patients in whomrespiratory disturbances interfere withsleep onset
The MSLT is a validated tool that isconsidered the de facto standard forobjective assessment of excessive day-time sleepiness38 The recommendedprotocol38 involves five 20-minute napopportunities held at 2-hour intervalsthroughout the day If sleep is ob-served the patient is allowed to sleepfor at least 15 minutes The sleep la-tency for each nap is measured as thetime from the start of the nap trial tothe first epoch of sleep A sleep la-tency of 20 minutes is assigned to naptrials during which no sleep isobserved39 The mean sleep latencycalculated as the average sleep latencyacross all nap trials is the final resultThe presence and number of sleep-onset REM periods (SOREMPs) is alsodetermined as this information canhelp to establish a diagnosis of narco-lepsy without cataplexy or to confirmnarcolepsy with cataplexy
The MSLT should be started 15 to30 hours following completion of anocturnal polysomnogram whichshould record at least 6 hours of sleepin order for determination of the meansleep latency to be valid Drugs that may
KEY POINT
h Careful considerationshould be given tothe indications forout-of-center testingAttended nocturnalpolysomnography isindicated if a portablestudy yields a negativeor technicallyinadequate result
44 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
interfere with sleep latency or REM la-tency should be discontinued 2 weeksbefore testing whenever possible Ascreen may be performed on the day oftesting if there is suspicion that pre-scribed or illicit substances may con-tribute to the patientrsquos sleepiness38
No large multicenter systematicallycollected normative data are availablefor mean sleep latency values on theMSLT38 Nonetheless a mean sleep la-tency of greater than 10 minutes is of-ten considered normal whereas a meansleep latency of 8 to 10 minutes is con-sidered a physiologic gray zone40 Thenormative data for children are classi-fied by Tanner stage of developmentthough the MSLT is typically not per-formed in children aged younger than 6or 7 years because some daytime nap-ping may still be normal in youngchildren41 The second edition of theInternational Classification of SleepDisorders Diagnostic and CodingManual (ICSD-2)42 requires the pres-ence of a mean sleep latency of lessthan 8 minutes and two or moreSOREMPs as part of the diagnosticcriteria for narcolepsy without cata-plexy However the ICSD-2 also notesthat a mean sleep latency of less than 8minutes may occur in up to 30 of thegeneral population Therefore whilethe MSLT is a helpful and widely usedtool it remains an imperfect gold stand-ard in the assessment of daytime sleepi-ness This necessitates that theevaluation of daytime sleepiness notrest on the MSLT results alone butassimilate the clinical history subjectivecomplaints diagnostic study results andother pertinent medical information38
Practice parameters from theAASM state that the MSLT is indicatedfor diagnostic confirmation of sus-pected narcolepsy and may be indi-cated to differentiate idiopathichypersomnia from narcolepsy38 TheMSLT is not indicated for routine
assessment of OSA syndrome or toassess response to treatment of SDBand is not routinely indicated for eval-uation of sleepiness in medical orneurologic disorders (except for narco-lepsy) insomnia or circadian rhythmdisorders
TheMWTprovides an objectivemeas-ure of a patientrsquos ability to remain awakerather than the tendency to fall asleepduring the day The key differencebetween the MWT and the MSLT is thatin the former the patient is asked to tryto stay awake under circumstances con-ducive to sleep rather than to fall asleepThe MWT provides an objective vali-dated assessment of the ability to remainawake for a defined length of time38 Therecommended protocol includes four40-minute trials that begin at 2-hourintervals with the first trial to start 15 to30 hours after the patientrsquos wake-uptime A nocturnal polysomnogram onthe preceding night is not requiredHowever the patient should obtain asufficient amount of sleep during thenight before the MWT Each trial isterminated after 40 minutes if no sleepoccurs or after unequivocal sleep onset(defined as three continuous epochsof stage N1 sleep or one epoch of anyother stage of sleep) has occurred38
One indication for the MWT is to as-sess an individualrsquos ability to remainawake when his or her inability to re-main awake constitutes a public orpersonal safety issue This can becomea pressing issue for individuals em-ployed in the transportation43 con-struction or health care industriesThe MWT may be indicated to assesstreatment response in patients withknown excessive daytime sleepiness
Limited amounts of normative dataare available for the MWT Historicallymultiple testing protocols make syn-thesis of results more challenging TheMWT is used much less often in clinicalpractice compared to the MSLT Patient
KEY POINTS
h The multiple sleeplatency test is the goldstandard for objectiveassessment of daytimesleepiness butinterpretation of theresults must be madewithin the clinicalcontext of the patientrsquoshistory
h In the multiple sleeplatency test the patientis instructed to try tosleep during each naptrial In the maintenanceof wakefulness test thepatient is instructed totry to remain awakeduring the nap trial
h A baseline nocturnalpolysomnogram isrequired before amultiple sleep latencytest and considered butnot required before amaintenance ofwakefulness test
45Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
age may also affect the mean sleep la-tency values on both the MWT and theMSLT43 and may represent evolution ofcircadian rhythm and sleep architec-ture across the lifetime A study of 383patients with narcolepsy with cataplexyexamined the clinical and polysomno-graphic data at the time of diagnosis(age range 5 to 84 years) and found aprogressive decrease in the number ofSOREMPs and a progressive increase inthe mean sleep latency on the MSLT asa function of age44 Given its limita-tions the MWT may thus be used tosupplement the clinical history in theassessment of ability to stay awake butshould not be the sole determinant ofthis parameter
Actigraphy is also used in the clinicalevaluation of patients with sleep disor-ders particularly circadian rhythm sleepdisorders An actigraph is a watchlikedevice that is worn on the wrist for anextended period usually in the range ofweeks The actigraph records move-ment and uses an algorithm to estimatethe amounts of sleep and wake timeduring the recording period Analysissoftware uses movement to estimatewhen sleep and wakefulness haveoccurred Review of the data can pro-vide objective insight into the patientrsquossleep pattern including timing andduration of major sleep disruptionsActigraphy is indicated as part of theevaluation of patients with advancedsleep-phase syndrome delayed sleep-phase syndrome and shift work disor-der and may be indicated in the evalua-tion of jet lag disorder and nonY24-hoursleep-wake syndrome including thatassociated with blindness45 It can alsoserve as a measure of treatment re-sponse in patients with insomnia andcircadian rhythm sleep disorders Forpopulations in which traditional sleepmonitoring may be challenging suchas pediatric or older adult patientsactigraphy may provide valuable infor-
mation about the patientrsquos sleep pat-tern or response to treatment Whenpolysomnography is not availableactigraphy is indicated to estimate totalsleep time in patients with OSA45
OTHER ASSESSMENTMODALITIESLaboratory evaluation and neuroimag-ing with either CT or MRI may beconsidered on an individual basis asindicated by the clinical history Com-plete blood count (CBC) serum chem-istries or measures of thyroid functionmay be obtained if an underlying med-ical disorder is thought to contribute tothe patientrsquos sleep symptoms Forinstance these laboratory studies maybe consideredwhen daytime fatigue is apredominant symptom Serum ironstudies including ferritin level shouldbe checked in patients with restless legssyndrome46 Neuroimaging should beconsidered in patients with antecedenttrauma or for any sleep disorder pa-tient with an abnormal neurologic ex-amination to evaluate for a structuraletiology of the patientrsquos symptoms
APPROACH TO THE PATIENTEvaluation of suspected sleep disordersis best accomplished by a stepwisemultidimensional approach (Case 2-2)A thorough sleep history includes de-tailed description of sleep-related symp-toms nocturnal behaviors the patientrsquossleep schedule level of daytime sleepi-ness and subsequent effects on daytimefunctioning Collateral history from thepatientrsquos bed partner or family is oftennecessary to understand the severity andcontext of the patientrsquos symptoms Sub-jective assessments of sleepiness suchas the Epworth Sleepiness Scale areeasily administered and useful to tracksymptomatic progression or treatmentresponse from one visit to the nextCertain physical examination findingsmay also raise clinical suspicion of
KEY POINTS
h Actigraphy can beuseful in evaluation andtreatment of circadianrhythm sleep disordersand in management ofinsomnia
h Neuroimaging is notroutinely indicated inthe clinical evaluation ofsleep disorders andshould be pursued on acase-by-case basis
46 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
particular sleep disorders For patientsin whom multiple sleep disorders aresuspected systematic use of diagnostictesting allows for accurate identificationof specific diagnoses In a patient withinsomnia and symptoms suggestive ofSDB nocturnal polysomnography shouldbe the first procedure performed Ifthe insomnia persists despite adequatetreatment of SDB further evaluationwith sleep diaries and possibly actigra-
phy may be considered to better char-acterize the patientrsquos sleep patternActigraphy may then again be pursuedto gauge treatment response upon man-agement of the patientrsquos insomnia
The diagnostic modalities availablefor evaluation of sleep disorders arerapidly evolving In-laboratory nocturnalpolysomnography currently remains thegold standard for assessment of SDBHowever the multitude of out-of-center
KEY POINT
h Careful assimilation ofthe clinical history thesleep-specific physicalexamination patientquestionnaires anddiagnostic test resultsleads to the mostaccurate assessment ofpatients with symptomsrelated to sleep oralertness
Case 2-2A 23-year-old woman reported a 4-year history of insomnia Throughoutcollege she was a lsquolsquonight owlrsquorsquo never scheduled classes that started before100 PM and always did well in school During the past 6 months shedeveloped progressive difficulty staying awake in her job as a financialanalyst andwas concerned about how this might affect her job performance
During the week she was in bed by midnight but was unable to fallasleep until 200 AM and awoke with difficulty to an alarm at 600 AMfeeling tired She denied any thought rumination or physical discomfortat bedtime She had tried over-the-counter sleep aids that provided nosymptomatic improvement and worsened morning grogginess Onweekends she slept from 200 AM to 1100 AM and awakened feelinglsquolsquopretty goodrsquorsquo She had nocturia up to once per night and occasionalmorning headaches She had no bed partner but reported gaspingrespirations nocturnal palpitations and snort arousals On about 4 nightsper week she experienced a sensation of needing to move her legswhile trying to fall asleep This sensation was relieved by movement andwas worse at night than during the day Her legs sometimes movedspontaneously at night or while seated quietly for long periods duringthe day She felt sleepy during the afternoon especially while workingat her computer She denied drowsiness while driving She occasionallytook a 30-minute nap on the weekend and found it to be refreshingShe drank one to two cups of coffee every morning and had a 12-oz dietcaffeinated soda at 300 PM Her sleepiness had not caused her to makeany mistakes at work and she denied any mood disturbance
Physical examination was notable for a body mass index of 32 kgm2 neckcircumference of 381 cm (15 in) and modified Mallampati class III oral airwayNasal passages were narrow with turbinate hypertrophy bilaterally andhard palate was high-arched and narrow Nomicrognathia or retrognathia waspresent She had molar occlusion class I bilaterally with no overjet or overbiteThe general cardiac respiratory and neurologic examinations were normal
Comment This case illustrates how discussion of the chief complaint raisessuspicion for multiple sleep disorders The history suggests a circadian rhythmsleep disorder particularly delayed sleep-phase syndrome sleep-disorderedbreathing and restless legs syndrome Diagnostic evaluation should includenocturnal polysomnogramwith consideration toperform testing at the patientrsquospreferred sleep time and serum iron studies Sleep diaries andor actigraphymay be considered for further assessment of the patientrsquos sleep pattern
47Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
testing devices continues to grow andmany may provide useful alternativesthat under appropriate circumstancescould allow more expedient conven-ient and less costly evaluations ofincreased numbers of patients whopreviously had only limited or delayedaccess to sleep services
VIDEO LEGENDSupplemental Digital Content 2-1
Home sleep study Video demonstrates a homesleep study using an unattended type 3 portablemonitoring device The patient is a 56-year-oldman who is experiencing morning headachesand concentration and alertness problems atwork He has a history of mild snoring and ar-terial hypertension His Epworth SleepinessScale score is 18 his neck circumference is19 in he has a Mallampati classification score ofIII and his body mass index is 41 kgm Theapnea-hypopnea index is 84 eventsh Channelsrecorded in this sleep study include arterialoxyhemoglobin saturation heart rate oral-nasalpressure flow snoring inductive plethysmog-raphy for chest efforts and body position
linkslwwcomCONTA15
B 2013 Marcel Hungs MD PhD Used withpermission
REFERENCES1 National Institutes of Health National
Center on Sleep Disorders ResearchSleep disorders research planwwwnhlbinihgovhealthprofsleep201101011NationalSleepDisordersResearch-PlanDHHSPublication11-7820pdf PublishedNovember 2011
2 Dinges DF An overview of sleepiness andaccidents J Sleep Res 19954(S2)4Y14
3 Mills RJ Young CA A medical definitionof fatigue in multiple sclerosis QJM 2008101(1)49Y60
4 Chervin RD Sleepiness fatigue tirednessand lack of energy in obstructive sleepapnea Chest 2000118(2)372Y379
5 Chotinaiwattarakul W OrsquoBrien LM Fan LChervin RD Fatigue tiredness and lack ofenergy improve with treatment for OSAJ Clin Sleep Med 20095(3)222Y227
6 American Academy of Sleep MedicineThe international classification of sleepdisorders diagnostic and coding manual2nd ed Westchester IL American Academyof Sleep Medicine 2005
7 Ebben MR Spielman AJNon-pharmacological treatments forinsomnia J Behav Med 200932(3)244Y254
8 Roth T Insomnia definition prevalenceetiology and consequences J Clin SleepMed 20073(5 suppl)S7YS10
9 Yang CM Spielman AJ Glovinsky PNonpharmacologic strategies in themanagement of insomnia Psychiatr ClinNorth Am 200629(4)895Y919 abstract viii
10 Katz ES DrsquoAmbrosio CM Pediatricobstructive sleep apnea syndrome ClinChest Med 201031(2)221Y234
11 Kohler M Bloch KE Stradling JR The role ofthe nose in the pathogenesis of obstructivesleep apnea Curr Opin Otolaryngol HeadNeck Surg 200917(1)33Y37
12 Kryger MH Atlas of clinical sleep medicinePhiladelphia PA Elsevier 2010
13 Zonato AI Martinho FL Bittencourt LRet al Head and neck physical examinationcomparison between nonapneic andobstructive sleep apnea patientsLaryngoscope 2005115(6)1030Y1034
14 Mallampati SR Gatt SP Gugino LD et alA clinical sign to predict difficult trachealintubation a prospective study Can AnaesthSoc J 198532(4)429Y434
15 Samsoon GL Young JR Difficult trachealintubation a retrospective studyAnaesthesia 198742(5)487Y490
16 Huang HH Lee MS Shih YL et alModified Mallampati classificationas a clinical predictor of peroralesophagogastroduodenoscopy toleranceBMC Gastroenterol 20111112
17 Friedman M Ibrahim H Bass L Clinicalstaging for sleep-disordered breathingOtolaryngol Head Neck Surg 2002127(1)13Y21
18 Cheng RHW Yiu CKY Leung WKOral health in individuals with Downsyndrome In Dey S ed Prenatal diagnosisand screening for down syndromeInTech wwwintechopencombookshowtoreferenceprenatal-diagnosis-and-screening-for-down-syndromeoral-health-in-individuals-with-down-syndromePublished 2011 Accessed August 24 2012
19 Katz I Stradling J Slutsky AS et al Dopatients with obstructive sleep apneahave thick necks Am Rev Respir Dis1990141(5 pt 1)1228Y1231
20 Kushida CA Efron B Guilleminault C Apredictive morphometric model for theobstructive sleep apnea syndrome AnnIntern Med 1997127(8 pt 1)581Y587
48 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
21 Saccucci M Tettamanti L Mummolo S et alScoliosis and dental occlusion a review ofthe literature Scoliosis 2011615
22 Battagel JM Kotecha B Dental side-effectsof mandibular advancement splint wear inpatients who snore Clin Otolaryngol200530(2)149Y156
23 Morcos SS Patel PK The vocabulary ofdentofacial deformities Clin Plast Surg200734(3)589Y599
24 Epstein LJ Kristo D Strollo PJ Jr et alClinical guideline for the evaluationmanagement and long-term care ofobstructive sleep apnea in adults J ClinSleep Med 20095(3)263Y276
25 Johns MW A new method for measuringdaytime sleepiness the Epworth sleepinessscale Sleep 199114(6)540Y545
26 Johns MW Daytime sleepiness snoring andobstructive sleep apnea The EpworthSleepiness Scale Chest 1993103(1)30Y36
27 Chervin RD Aldrich MS The EpworthSleepiness Scale may not reflect objectivemeasures of sleepiness or sleep apneaNeurology 199952(1)125Y131
28 Buysse DJ Reynolds CF 3rd Monk THet al The Pittsburgh Sleep Quality Index anew instrument for psychiatric practice andresearch Psychiatry Res 198928(2)193Y213
29 Chervin RD Hedger K Dillon JE Pituch KJPediatric sleep questionnaire (PSQ) validityand reliability of scales for sleep-disorderedbreathing snoring sleepiness and behavioralproblems Sleep Med 20001(1)21Y32
30 Chung F Yegneswaran B Liao P et al STOPquestionnaire a tool to screen patients forobstructive sleep apnea Anesthesiology2008108(5)812Y821
31 Walters AS LeBrocq C Dhar A et alValidation of the International Restless LegsSyndrome Study Group rating scale forrestless legs syndrome Sleep Med 20034(2)121Y132
32 Bastien CH Vallieres A Morin CMValidation of the Insomnia Severity Indexas an outcome measure for insomniaresearch Sleep Med 20012(4)297Y307
33 YOURSLEEPaasmnetorg from the AmericanAcademy of Sleep Medicine Two weeksleep diary yoursleepaasmnetorgpdfsleepdiarypdf Accessed August 24 2012
34 Kushida CA Littner MR Morgenthaler Tet al Practice parameters for the indicationsfor polysomnography and relatedprocedures an update for 2005 Sleep200528(4)499Y521
35 Iber C Ancoli-Israel S Chesson A et alThe AASM manual for scoring of sleep andassociated events rules terminology andtechnical specifications 1st ed WestchesterIL American Academy of Sleep Medicine2007
36 Collop NA Tracy SL Kapur V et alObstructive sleep apnea devices forout-of-center (OOC) testing technologyevaluation J Clin Sleep Med 20117(5)531Y548
37 Collop NA Anderson WM Boehlecke Bet al Clinical guidelines for the use ofunattended portable monitors in thediagnosis of obstructive sleep apnea in adultpatients Portable Monitoring Task Forceof the American Academy of SleepMedicine J Clin Sleep Med 20073(7)737Y747
38 Littner MR Kushida C Wise M et alStandards of Practice Committee of theAmerican Academy of Sleep MedicinePractice parameters for clinical use of themultiple sleep latency test and themaintenance of wakefulness test Sleep200528(1)113Y121
39 Carskadon MA Dement WC Mitler MMet al Guidelines for the multiple sleeplatency test (MSLT) a standard measure ofsleepiness Sleep 19869(4)519Y524
40 van den Hoed J Kraemer H Guilleminault Cet al Disorders of excessive daytimesomnolence polygraphic and clinical datafor 100 patients Sleep 19814(1)23Y37
41 Hoban TF Chervin RD Assessment ofsleepiness in children Semin PediatrNeurol 20018(4)216Y228
42 ICSD-2 The international classification ofsleep disorders pocket version diagnosticand coding manual 2nd ed WestchesterIL American Academy of Sleep Medicine2005
43 Arand D Bonnet M Hurwitz T et alThe clinical use of the MSLT and MWTSleep 200528(1)123Y144
44 Dauvilliers Y Gosselin A Paquet J et alEffect of age on MSLT results in patientswith narcolepsy-cataplexy Neurology200462(1)46Y50
45 Morgenthaler T Alessi C Friedman Let al Practice parameters for the use ofactigraphy in the assessment of sleep andsleep disorders an update for 2007 Sleep200730(4)519Y529
46 Gamaldo CE Earley CJ Restless legssyndrome a clinical update Chest2006130(5)1596Y1604
49Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited

and turbinate hypertrophy) andoroverjet To prevent overlooking thesefindings a thorough head and neckassessment as described in Table 2-2should be incorporated into the phys-ical examination of all patients whopresent with sleep-related complaints
SUBJECTIVE ASSESSMENTSeveral patient-completed question-naires are inexpensive and time-efficient
reasonably well validated and com-monly used They can help to increasestandardization in evaluations of patientsby different clinicians or across centersPerhaps the most well-known andwidely used is the Epworth SleepinessScale25 a subjective assessment of thepatientrsquos daytime sleep propensity inrecent times As shown in Appendix Athe Epworth Sleepiness Scale asks theresponder to use a four-point Likertscale (0 1 2 or 3) to indicate thelikelihood of dozing in eight distinctsedentary conditions A total score of 10or greater out of a possible 24 suggestsexcessive daytime sleepiness25 Whilethe Epworth Sleepiness Scale score canbe easily incorporated into the clinicalevaluation it should not be used as asubstitute for objective measurement ofsleepiness The Epworth Sleepiness Scalescore may correlate to a limited extentwith the presence and severity of OSA26
but some studies have failed to find anystatistically significant association withmean sleep latency on multiple sleep la-tency tests or with severity of OSA27
The most advantageous use of theEpworth Sleepiness Scale may be to followan individualrsquos self-assessment of sleep-iness longitudinally and it may also serveas an indicator of treatment response
Many other questionnaires may beutilized in a clinical sleep evaluationsome pertain to overall sleep qualitywhile others are disorder-specific ThePatient Reported Outcomes Measure-ment Information System (PROMIS) isan NIH-supported system of measuresfor patient-reported health status andincludes questions on sleep disturb-ance The Pittsburgh Sleep QualityIndex (PSQI) is a validated question-naire that inquires about sleep qualityand disturbances over the previousmonth28 The parent-completed Pe-diatric Sleep Questionnaire29 containsa validated reliable 22-item scale tohelp assess risk for SDB in children
KEY POINTS
h The Epworth SleepinessScale apatient-completedquestionnaire assessesthe patientrsquos subjectivetendency to doze duringsedentary situations inrecent times not onlyat the moment thequestionnaire iscompleted
h The Epworth SleepinessScale should not beused in lieu of diagnostictesting but may be avaluable componentof ongoing clinicalevaluation
TABLE 2-2 Head and NeckExamination
b Face
Featuresof long face syndrome
Infraorbital darkening
Mouth breathing
Elongated midface
Nasal atrophy
b Oral Airway
Mandibular retrognathia
Low soft palate (modifiedMallampati classification)
Large or boggy uvula
Erythematous pillars
Tonsillar hypertrophy
High narrow hard palate
Neck circumference
Overjet
Overbite
Angle classification(malocclusion)
Macroglossia
Worn occlusive surfaces(suggestive of bruxism)
b Nasal Airway
Symmetry of the nares
Nasal septum deviation
Nasal airflow
Collapse of nasal alae oninspiration
b Neck
Neck circumference
40 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
The STOP-BANG questionnaire devel-oped and validated in preoperativepatients is a sensitive screening toolfor OSA Four questions address snor-ing tiredness during daytime observedapnea and high blood pressure whereasfour other measures focus on increasedOSA risk factors of BMI (greater than 35kgm2) age (older than 50 years) neckcircumference (greater than 40 cm[1575 in]) and gender (male preva-lence)30 The International RestlessLegs Syndrome Study Group Rating Scale(IRLS) is a validated assessment of dis-ease severity for patients with restlesslegs syndrome31 The patientrsquos perceived
level of insomnia may be assessed withthe Insomnia Severity Index (ISI) avalidated 7-item questionnaire32
A sleep diary (Figure 2-9)33 allows apatient to chart daily sleep and waketimes and should be maintained for atleast 2 consecutive weeks Review ofthis information allows the clinicianto estimate the total amount of sleepthe patient obtains in a 24-hour pe-riod The sleep diary also can provideinsight into the patientrsquos sleep patternIs sleep obtained at the same timesevery day Is the patientrsquos sleep con-solidated or fragmented across 24hours Does the patient sleep and
FIGURE 2-9 Sleep diary completed by a 46-year-old woman who presented with difficulty falling asleep Vertical linesrepresent when the patient went to bed lsquolsquoMrsquorsquo refers to when medication was taken black shading representstime asleep and unshaded white areas are time spent awake
Diary template reprinted from YOURSLEEPaasmnetorg from the American Academy of Sleep Medicine yoursleepaasmnetorgpdfsleepdiarypdf33
41Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
wake at conventional times or doeshe or she appear to be a lsquolsquonight owlrsquorsquoor lsquolsquomorning larkrsquorsquo Answers to thesequestions as provided by the sleepdiary may reveal factors that contrib-ute to sleep-related concerns Use ofsleep diaries can be particularly help-ful in patients with suspected circadianrhythm sleep disorders (including shiftwork) behaviorally induced insufficientsleep or inadequate sleep hygiene
OBJECTIVE MEASURESNocturnal polysomnography (NPSG)or related assessments are indicatedfor the diagnosis and assessment ofSDB and for positive airway titrationin patients with confirmed SDB Theprocedure can also provide informationabout EEG activity nocturnal move-ments cardiac rhythm and oxygen
saturation34 The recommended record-ing montage used in NPSG as shownin Figure 2-10 includes central (C3-A2C4-A1) frontal (F3-A2 F4-A1) andoccipital (O1-A2 O2-A1) EEGs left andright eye electrooculograms mentalsubmental surface EMG and ECG leadsOther recorded parameters includethoracic and abdominal effort oxygensaturation nasaloral airflow and bodyposition Use of a microphone torecord snoring is recommended butnot required34 A full 16-lead EEG(Figure 2-11)35 and video recordingmay be performed when nocturnalseizures are suspected Leg surfaceEMG leads are recommended andadditional arm EMG leads may beapplied when the clinical history sug-gests complex sleep-related motor be-haviors such as dream enactment In
KEY POINT
h A daily sleep diary helpsto summarize a patientrsquossleep-wake schedulemore accurately thanmemory often allowsand can facilitateconstruction ofpersonalized plansfor management ofcircadian rhythm sleepdisorders and insomnia
FIGURE 2-10 A 1-minute epoch from a nocturnal polysomnogram showing obstructive sleepapnea in a 46-year-old man who presented with snoring daytime sleepinessand headaches It depicts the standard recording montage that includes the
following leads central (C3-M2 C4-M1) frontal (F3-M2 F4-M1) and occipital (O1-M2 O2-M1)EEGs left and right eye electrooculograms (E1-M2 E2-M1) mentalsubmental electromyogram(Chin1-Chin2) electrocardiogram (ECG1-ECG2 ECG2-ECG3) snore volume (SNORE) nasalpressure transducer (NPRE) nasaloral airflow (NO) thoracic (THOR) and abdominal (ABD)effort arterial oxyhemoglobin saturation (SpO2) plethysmography (Pleth) and left and right eyeelectromyograms (LAT1-LAT2 RAT1-RAT2)
42 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
most cases the diagnostic NPSG is doneon 1 night although NPSG on 2 con-secutive nights may be considered inthe evaluation of parasomnias
Four categories of sleep monitoringdevices for use in the diagnosis of sleepdisorders have often been described34
These are type 1 standard attended in-laboratory polysomnography type 2comprehensive portable unattendedpolysomnography type 3 modifiedportable sleep apnea testing (often car-diorespiratory studies that do not recordsleep) and type 4 continuous single ordual bioparameter recording (eg pulseoximetry) However this categorizationmay not effectively classify the plethoraof out-of-center testing devices currentlyavailable for clinical use Therefore anew device classification system hasrecently been proposed This schemaknown as the SCOPER system catego-rizes out-of-center testing devices basedon measurement of sleep cardiovascu-
lar oximetry position effort and res-piratory parameters36 Within each ofthe six SCOPER categories a level of 0through 5 is assigned as indicated bythe type of sensor or measurementthat the device uses for that category
The most recent clinical guidelinespublished by the Portable MonitoringTask Force of the AASM37 for use ofunattended portable monitoring inthe diagnosis of OSA in adult patientsrecommend that portable monitoringonly be performed in conjunction witha comprehensive sleep evaluation by(or supervised by) a practitioner board-certified in sleep medicine or eligiblefor the certification examination Theseguidelines state that portable monitor-ing may be used in place of NPSG inpatients with a high pretest probabilityof moderate to severe OSA Portablemonitoring should not be used inpatients with significant medical comor-bidities (including but not limited to
KEY POINT
h The complexclassification of portabletesting devices reflectsthe multitude of designsavailable to cliniciansand will undoubtedlychange as technologyadvances
FIGURE 2-11 A The international 10Y20 system for EEG electrode placement refers to the10 and 20 interelectrode distances Even electrode numbers (2 4 6 8)represent the right hemisphere and odd electrode numbers (1 3 5 7)
represent the left hemisphere B Recommended F4-M1 C4-M1 O2-M1 placements of EEGelectrodes as set forth by the American Academy of Sleep Medicine (AASM)
Adapted from Iber C et al American Academy of SleepMedicine35 Used with permission of the American Academy ofSleep Medicine Darien IL 2012
43Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
moderate to severe pulmonary diseaseneuromuscular disease or congestiveheart failure) in patients with othersleep disorders (including central sleepapnea periodic limb movement disor-der insomnia parasomnias circadianrhythm disorders or narcolepsy) or asa screening tool The use of portablemonitoring may be indicated for thediagnosis of OSA in patients for whomattended NPSG is not possible becauseof immobility safety or critical illnessPortable monitoring may be indi-cated to monitor the response to non-continuous positive airway pressuretreatments for OSA including oralappliances upper airway surgery andweight loss The algorithm shown inAppendix B may help in the determi-nation of an adult patientrsquos candidacyfor out-of-center testing for the diag-nosis of OSA An example of portable(or home) monitoring technology isshown in Supplemental Digital Con-tent 2-1 linkslwwcomCONTA15
Recommended technology for port-able monitoring should record at mini-mum airflow respiratory effort andblood oxygenation the airflow effortand oximetric biosensors typically usedfor attended NPSG should be used37
These guidelines published in 2007will likely continue to evolve as newtechnologies emerge and are found tobe effective The current guidelinesrecommend that out-of-center testingbe performed under the auspices of anAASM-accredited comprehensive sleepmedicine program and that a board-certifiedeligible sleep specialist reviewthe raw data from a portable monitor-ing device All patients who undergoportablemonitoring for the diagnosis ofOSA should have a follow-up visit toreview test results Negative or techni-cally inadequate portable monitoringstudies should be followed by attendedin-laboratory NPSG if the clinical suspi-cion for SDB remains high37
The aforementioned testing proce-dures are primarily used in the evalua-tion of SDB Other testing modalitiesare useful in the diagnosis of othercategories of sleep disorders The mul-tiple sleep latency test (MSLT) and itsvariant the maintenance of wakefulnesstest (MWT) are used in the evaluation ofhypersomnia The conventional record-ing montage is similar to that used fornocturnal polysomnography central fron-tal and occipital EEGs left and right eyeelectrooculograms mentalsubmentalEMG and ECG leads Measurement ofthoracic and abdominal effort oxygensaturation and nasaloral airflow are notrequired but may help explain delayedsleep latencies for patients in whomrespiratory disturbances interfere withsleep onset
The MSLT is a validated tool that isconsidered the de facto standard forobjective assessment of excessive day-time sleepiness38 The recommendedprotocol38 involves five 20-minute napopportunities held at 2-hour intervalsthroughout the day If sleep is ob-served the patient is allowed to sleepfor at least 15 minutes The sleep la-tency for each nap is measured as thetime from the start of the nap trial tothe first epoch of sleep A sleep la-tency of 20 minutes is assigned to naptrials during which no sleep isobserved39 The mean sleep latencycalculated as the average sleep latencyacross all nap trials is the final resultThe presence and number of sleep-onset REM periods (SOREMPs) is alsodetermined as this information canhelp to establish a diagnosis of narco-lepsy without cataplexy or to confirmnarcolepsy with cataplexy
The MSLT should be started 15 to30 hours following completion of anocturnal polysomnogram whichshould record at least 6 hours of sleepin order for determination of the meansleep latency to be valid Drugs that may
KEY POINT
h Careful considerationshould be given tothe indications forout-of-center testingAttended nocturnalpolysomnography isindicated if a portablestudy yields a negativeor technicallyinadequate result
44 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
interfere with sleep latency or REM la-tency should be discontinued 2 weeksbefore testing whenever possible Ascreen may be performed on the day oftesting if there is suspicion that pre-scribed or illicit substances may con-tribute to the patientrsquos sleepiness38
No large multicenter systematicallycollected normative data are availablefor mean sleep latency values on theMSLT38 Nonetheless a mean sleep la-tency of greater than 10 minutes is of-ten considered normal whereas a meansleep latency of 8 to 10 minutes is con-sidered a physiologic gray zone40 Thenormative data for children are classi-fied by Tanner stage of developmentthough the MSLT is typically not per-formed in children aged younger than 6or 7 years because some daytime nap-ping may still be normal in youngchildren41 The second edition of theInternational Classification of SleepDisorders Diagnostic and CodingManual (ICSD-2)42 requires the pres-ence of a mean sleep latency of lessthan 8 minutes and two or moreSOREMPs as part of the diagnosticcriteria for narcolepsy without cata-plexy However the ICSD-2 also notesthat a mean sleep latency of less than 8minutes may occur in up to 30 of thegeneral population Therefore whilethe MSLT is a helpful and widely usedtool it remains an imperfect gold stand-ard in the assessment of daytime sleepi-ness This necessitates that theevaluation of daytime sleepiness notrest on the MSLT results alone butassimilate the clinical history subjectivecomplaints diagnostic study results andother pertinent medical information38
Practice parameters from theAASM state that the MSLT is indicatedfor diagnostic confirmation of sus-pected narcolepsy and may be indi-cated to differentiate idiopathichypersomnia from narcolepsy38 TheMSLT is not indicated for routine
assessment of OSA syndrome or toassess response to treatment of SDBand is not routinely indicated for eval-uation of sleepiness in medical orneurologic disorders (except for narco-lepsy) insomnia or circadian rhythmdisorders
TheMWTprovides an objectivemeas-ure of a patientrsquos ability to remain awakerather than the tendency to fall asleepduring the day The key differencebetween the MWT and the MSLT is thatin the former the patient is asked to tryto stay awake under circumstances con-ducive to sleep rather than to fall asleepThe MWT provides an objective vali-dated assessment of the ability to remainawake for a defined length of time38 Therecommended protocol includes four40-minute trials that begin at 2-hourintervals with the first trial to start 15 to30 hours after the patientrsquos wake-uptime A nocturnal polysomnogram onthe preceding night is not requiredHowever the patient should obtain asufficient amount of sleep during thenight before the MWT Each trial isterminated after 40 minutes if no sleepoccurs or after unequivocal sleep onset(defined as three continuous epochsof stage N1 sleep or one epoch of anyother stage of sleep) has occurred38
One indication for the MWT is to as-sess an individualrsquos ability to remainawake when his or her inability to re-main awake constitutes a public orpersonal safety issue This can becomea pressing issue for individuals em-ployed in the transportation43 con-struction or health care industriesThe MWT may be indicated to assesstreatment response in patients withknown excessive daytime sleepiness
Limited amounts of normative dataare available for the MWT Historicallymultiple testing protocols make syn-thesis of results more challenging TheMWT is used much less often in clinicalpractice compared to the MSLT Patient
KEY POINTS
h The multiple sleeplatency test is the goldstandard for objectiveassessment of daytimesleepiness butinterpretation of theresults must be madewithin the clinicalcontext of the patientrsquoshistory
h In the multiple sleeplatency test the patientis instructed to try tosleep during each naptrial In the maintenanceof wakefulness test thepatient is instructed totry to remain awakeduring the nap trial
h A baseline nocturnalpolysomnogram isrequired before amultiple sleep latencytest and considered butnot required before amaintenance ofwakefulness test
45Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
age may also affect the mean sleep la-tency values on both the MWT and theMSLT43 and may represent evolution ofcircadian rhythm and sleep architec-ture across the lifetime A study of 383patients with narcolepsy with cataplexyexamined the clinical and polysomno-graphic data at the time of diagnosis(age range 5 to 84 years) and found aprogressive decrease in the number ofSOREMPs and a progressive increase inthe mean sleep latency on the MSLT asa function of age44 Given its limita-tions the MWT may thus be used tosupplement the clinical history in theassessment of ability to stay awake butshould not be the sole determinant ofthis parameter
Actigraphy is also used in the clinicalevaluation of patients with sleep disor-ders particularly circadian rhythm sleepdisorders An actigraph is a watchlikedevice that is worn on the wrist for anextended period usually in the range ofweeks The actigraph records move-ment and uses an algorithm to estimatethe amounts of sleep and wake timeduring the recording period Analysissoftware uses movement to estimatewhen sleep and wakefulness haveoccurred Review of the data can pro-vide objective insight into the patientrsquossleep pattern including timing andduration of major sleep disruptionsActigraphy is indicated as part of theevaluation of patients with advancedsleep-phase syndrome delayed sleep-phase syndrome and shift work disor-der and may be indicated in the evalua-tion of jet lag disorder and nonY24-hoursleep-wake syndrome including thatassociated with blindness45 It can alsoserve as a measure of treatment re-sponse in patients with insomnia andcircadian rhythm sleep disorders Forpopulations in which traditional sleepmonitoring may be challenging suchas pediatric or older adult patientsactigraphy may provide valuable infor-
mation about the patientrsquos sleep pat-tern or response to treatment Whenpolysomnography is not availableactigraphy is indicated to estimate totalsleep time in patients with OSA45
OTHER ASSESSMENTMODALITIESLaboratory evaluation and neuroimag-ing with either CT or MRI may beconsidered on an individual basis asindicated by the clinical history Com-plete blood count (CBC) serum chem-istries or measures of thyroid functionmay be obtained if an underlying med-ical disorder is thought to contribute tothe patientrsquos sleep symptoms Forinstance these laboratory studies maybe consideredwhen daytime fatigue is apredominant symptom Serum ironstudies including ferritin level shouldbe checked in patients with restless legssyndrome46 Neuroimaging should beconsidered in patients with antecedenttrauma or for any sleep disorder pa-tient with an abnormal neurologic ex-amination to evaluate for a structuraletiology of the patientrsquos symptoms
APPROACH TO THE PATIENTEvaluation of suspected sleep disordersis best accomplished by a stepwisemultidimensional approach (Case 2-2)A thorough sleep history includes de-tailed description of sleep-related symp-toms nocturnal behaviors the patientrsquossleep schedule level of daytime sleepi-ness and subsequent effects on daytimefunctioning Collateral history from thepatientrsquos bed partner or family is oftennecessary to understand the severity andcontext of the patientrsquos symptoms Sub-jective assessments of sleepiness suchas the Epworth Sleepiness Scale areeasily administered and useful to tracksymptomatic progression or treatmentresponse from one visit to the nextCertain physical examination findingsmay also raise clinical suspicion of
KEY POINTS
h Actigraphy can beuseful in evaluation andtreatment of circadianrhythm sleep disordersand in management ofinsomnia
h Neuroimaging is notroutinely indicated inthe clinical evaluation ofsleep disorders andshould be pursued on acase-by-case basis
46 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
particular sleep disorders For patientsin whom multiple sleep disorders aresuspected systematic use of diagnostictesting allows for accurate identificationof specific diagnoses In a patient withinsomnia and symptoms suggestive ofSDB nocturnal polysomnography shouldbe the first procedure performed Ifthe insomnia persists despite adequatetreatment of SDB further evaluationwith sleep diaries and possibly actigra-
phy may be considered to better char-acterize the patientrsquos sleep patternActigraphy may then again be pursuedto gauge treatment response upon man-agement of the patientrsquos insomnia
The diagnostic modalities availablefor evaluation of sleep disorders arerapidly evolving In-laboratory nocturnalpolysomnography currently remains thegold standard for assessment of SDBHowever the multitude of out-of-center
KEY POINT
h Careful assimilation ofthe clinical history thesleep-specific physicalexamination patientquestionnaires anddiagnostic test resultsleads to the mostaccurate assessment ofpatients with symptomsrelated to sleep oralertness
Case 2-2A 23-year-old woman reported a 4-year history of insomnia Throughoutcollege she was a lsquolsquonight owlrsquorsquo never scheduled classes that started before100 PM and always did well in school During the past 6 months shedeveloped progressive difficulty staying awake in her job as a financialanalyst andwas concerned about how this might affect her job performance
During the week she was in bed by midnight but was unable to fallasleep until 200 AM and awoke with difficulty to an alarm at 600 AMfeeling tired She denied any thought rumination or physical discomfortat bedtime She had tried over-the-counter sleep aids that provided nosymptomatic improvement and worsened morning grogginess Onweekends she slept from 200 AM to 1100 AM and awakened feelinglsquolsquopretty goodrsquorsquo She had nocturia up to once per night and occasionalmorning headaches She had no bed partner but reported gaspingrespirations nocturnal palpitations and snort arousals On about 4 nightsper week she experienced a sensation of needing to move her legswhile trying to fall asleep This sensation was relieved by movement andwas worse at night than during the day Her legs sometimes movedspontaneously at night or while seated quietly for long periods duringthe day She felt sleepy during the afternoon especially while workingat her computer She denied drowsiness while driving She occasionallytook a 30-minute nap on the weekend and found it to be refreshingShe drank one to two cups of coffee every morning and had a 12-oz dietcaffeinated soda at 300 PM Her sleepiness had not caused her to makeany mistakes at work and she denied any mood disturbance
Physical examination was notable for a body mass index of 32 kgm2 neckcircumference of 381 cm (15 in) and modified Mallampati class III oral airwayNasal passages were narrow with turbinate hypertrophy bilaterally andhard palate was high-arched and narrow Nomicrognathia or retrognathia waspresent She had molar occlusion class I bilaterally with no overjet or overbiteThe general cardiac respiratory and neurologic examinations were normal
Comment This case illustrates how discussion of the chief complaint raisessuspicion for multiple sleep disorders The history suggests a circadian rhythmsleep disorder particularly delayed sleep-phase syndrome sleep-disorderedbreathing and restless legs syndrome Diagnostic evaluation should includenocturnal polysomnogramwith consideration toperform testing at the patientrsquospreferred sleep time and serum iron studies Sleep diaries andor actigraphymay be considered for further assessment of the patientrsquos sleep pattern
47Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
testing devices continues to grow andmany may provide useful alternativesthat under appropriate circumstancescould allow more expedient conven-ient and less costly evaluations ofincreased numbers of patients whopreviously had only limited or delayedaccess to sleep services
VIDEO LEGENDSupplemental Digital Content 2-1
Home sleep study Video demonstrates a homesleep study using an unattended type 3 portablemonitoring device The patient is a 56-year-oldman who is experiencing morning headachesand concentration and alertness problems atwork He has a history of mild snoring and ar-terial hypertension His Epworth SleepinessScale score is 18 his neck circumference is19 in he has a Mallampati classification score ofIII and his body mass index is 41 kgm Theapnea-hypopnea index is 84 eventsh Channelsrecorded in this sleep study include arterialoxyhemoglobin saturation heart rate oral-nasalpressure flow snoring inductive plethysmog-raphy for chest efforts and body position
linkslwwcomCONTA15
B 2013 Marcel Hungs MD PhD Used withpermission
REFERENCES1 National Institutes of Health National
Center on Sleep Disorders ResearchSleep disorders research planwwwnhlbinihgovhealthprofsleep201101011NationalSleepDisordersResearch-PlanDHHSPublication11-7820pdf PublishedNovember 2011
2 Dinges DF An overview of sleepiness andaccidents J Sleep Res 19954(S2)4Y14
3 Mills RJ Young CA A medical definitionof fatigue in multiple sclerosis QJM 2008101(1)49Y60
4 Chervin RD Sleepiness fatigue tirednessand lack of energy in obstructive sleepapnea Chest 2000118(2)372Y379
5 Chotinaiwattarakul W OrsquoBrien LM Fan LChervin RD Fatigue tiredness and lack ofenergy improve with treatment for OSAJ Clin Sleep Med 20095(3)222Y227
6 American Academy of Sleep MedicineThe international classification of sleepdisorders diagnostic and coding manual2nd ed Westchester IL American Academyof Sleep Medicine 2005
7 Ebben MR Spielman AJNon-pharmacological treatments forinsomnia J Behav Med 200932(3)244Y254
8 Roth T Insomnia definition prevalenceetiology and consequences J Clin SleepMed 20073(5 suppl)S7YS10
9 Yang CM Spielman AJ Glovinsky PNonpharmacologic strategies in themanagement of insomnia Psychiatr ClinNorth Am 200629(4)895Y919 abstract viii
10 Katz ES DrsquoAmbrosio CM Pediatricobstructive sleep apnea syndrome ClinChest Med 201031(2)221Y234
11 Kohler M Bloch KE Stradling JR The role ofthe nose in the pathogenesis of obstructivesleep apnea Curr Opin Otolaryngol HeadNeck Surg 200917(1)33Y37
12 Kryger MH Atlas of clinical sleep medicinePhiladelphia PA Elsevier 2010
13 Zonato AI Martinho FL Bittencourt LRet al Head and neck physical examinationcomparison between nonapneic andobstructive sleep apnea patientsLaryngoscope 2005115(6)1030Y1034
14 Mallampati SR Gatt SP Gugino LD et alA clinical sign to predict difficult trachealintubation a prospective study Can AnaesthSoc J 198532(4)429Y434
15 Samsoon GL Young JR Difficult trachealintubation a retrospective studyAnaesthesia 198742(5)487Y490
16 Huang HH Lee MS Shih YL et alModified Mallampati classificationas a clinical predictor of peroralesophagogastroduodenoscopy toleranceBMC Gastroenterol 20111112
17 Friedman M Ibrahim H Bass L Clinicalstaging for sleep-disordered breathingOtolaryngol Head Neck Surg 2002127(1)13Y21
18 Cheng RHW Yiu CKY Leung WKOral health in individuals with Downsyndrome In Dey S ed Prenatal diagnosisand screening for down syndromeInTech wwwintechopencombookshowtoreferenceprenatal-diagnosis-and-screening-for-down-syndromeoral-health-in-individuals-with-down-syndromePublished 2011 Accessed August 24 2012
19 Katz I Stradling J Slutsky AS et al Dopatients with obstructive sleep apneahave thick necks Am Rev Respir Dis1990141(5 pt 1)1228Y1231
20 Kushida CA Efron B Guilleminault C Apredictive morphometric model for theobstructive sleep apnea syndrome AnnIntern Med 1997127(8 pt 1)581Y587
48 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
21 Saccucci M Tettamanti L Mummolo S et alScoliosis and dental occlusion a review ofthe literature Scoliosis 2011615
22 Battagel JM Kotecha B Dental side-effectsof mandibular advancement splint wear inpatients who snore Clin Otolaryngol200530(2)149Y156
23 Morcos SS Patel PK The vocabulary ofdentofacial deformities Clin Plast Surg200734(3)589Y599
24 Epstein LJ Kristo D Strollo PJ Jr et alClinical guideline for the evaluationmanagement and long-term care ofobstructive sleep apnea in adults J ClinSleep Med 20095(3)263Y276
25 Johns MW A new method for measuringdaytime sleepiness the Epworth sleepinessscale Sleep 199114(6)540Y545
26 Johns MW Daytime sleepiness snoring andobstructive sleep apnea The EpworthSleepiness Scale Chest 1993103(1)30Y36
27 Chervin RD Aldrich MS The EpworthSleepiness Scale may not reflect objectivemeasures of sleepiness or sleep apneaNeurology 199952(1)125Y131
28 Buysse DJ Reynolds CF 3rd Monk THet al The Pittsburgh Sleep Quality Index anew instrument for psychiatric practice andresearch Psychiatry Res 198928(2)193Y213
29 Chervin RD Hedger K Dillon JE Pituch KJPediatric sleep questionnaire (PSQ) validityand reliability of scales for sleep-disorderedbreathing snoring sleepiness and behavioralproblems Sleep Med 20001(1)21Y32
30 Chung F Yegneswaran B Liao P et al STOPquestionnaire a tool to screen patients forobstructive sleep apnea Anesthesiology2008108(5)812Y821
31 Walters AS LeBrocq C Dhar A et alValidation of the International Restless LegsSyndrome Study Group rating scale forrestless legs syndrome Sleep Med 20034(2)121Y132
32 Bastien CH Vallieres A Morin CMValidation of the Insomnia Severity Indexas an outcome measure for insomniaresearch Sleep Med 20012(4)297Y307
33 YOURSLEEPaasmnetorg from the AmericanAcademy of Sleep Medicine Two weeksleep diary yoursleepaasmnetorgpdfsleepdiarypdf Accessed August 24 2012
34 Kushida CA Littner MR Morgenthaler Tet al Practice parameters for the indicationsfor polysomnography and relatedprocedures an update for 2005 Sleep200528(4)499Y521
35 Iber C Ancoli-Israel S Chesson A et alThe AASM manual for scoring of sleep andassociated events rules terminology andtechnical specifications 1st ed WestchesterIL American Academy of Sleep Medicine2007
36 Collop NA Tracy SL Kapur V et alObstructive sleep apnea devices forout-of-center (OOC) testing technologyevaluation J Clin Sleep Med 20117(5)531Y548
37 Collop NA Anderson WM Boehlecke Bet al Clinical guidelines for the use ofunattended portable monitors in thediagnosis of obstructive sleep apnea in adultpatients Portable Monitoring Task Forceof the American Academy of SleepMedicine J Clin Sleep Med 20073(7)737Y747
38 Littner MR Kushida C Wise M et alStandards of Practice Committee of theAmerican Academy of Sleep MedicinePractice parameters for clinical use of themultiple sleep latency test and themaintenance of wakefulness test Sleep200528(1)113Y121
39 Carskadon MA Dement WC Mitler MMet al Guidelines for the multiple sleeplatency test (MSLT) a standard measure ofsleepiness Sleep 19869(4)519Y524
40 van den Hoed J Kraemer H Guilleminault Cet al Disorders of excessive daytimesomnolence polygraphic and clinical datafor 100 patients Sleep 19814(1)23Y37
41 Hoban TF Chervin RD Assessment ofsleepiness in children Semin PediatrNeurol 20018(4)216Y228
42 ICSD-2 The international classification ofsleep disorders pocket version diagnosticand coding manual 2nd ed WestchesterIL American Academy of Sleep Medicine2005
43 Arand D Bonnet M Hurwitz T et alThe clinical use of the MSLT and MWTSleep 200528(1)123Y144
44 Dauvilliers Y Gosselin A Paquet J et alEffect of age on MSLT results in patientswith narcolepsy-cataplexy Neurology200462(1)46Y50
45 Morgenthaler T Alessi C Friedman Let al Practice parameters for the use ofactigraphy in the assessment of sleep andsleep disorders an update for 2007 Sleep200730(4)519Y529
46 Gamaldo CE Earley CJ Restless legssyndrome a clinical update Chest2006130(5)1596Y1604
49Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
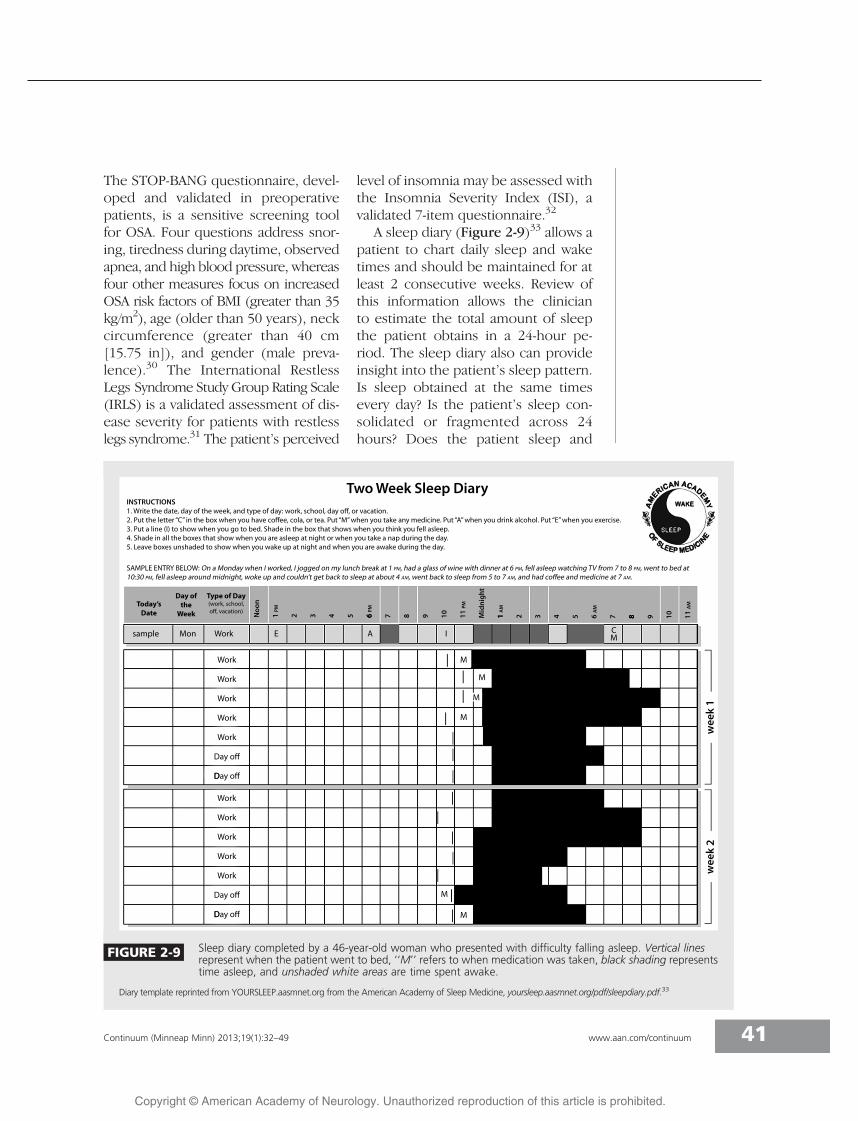
The STOP-BANG questionnaire devel-oped and validated in preoperativepatients is a sensitive screening toolfor OSA Four questions address snor-ing tiredness during daytime observedapnea and high blood pressure whereasfour other measures focus on increasedOSA risk factors of BMI (greater than 35kgm2) age (older than 50 years) neckcircumference (greater than 40 cm[1575 in]) and gender (male preva-lence)30 The International RestlessLegs Syndrome Study Group Rating Scale(IRLS) is a validated assessment of dis-ease severity for patients with restlesslegs syndrome31 The patientrsquos perceived
level of insomnia may be assessed withthe Insomnia Severity Index (ISI) avalidated 7-item questionnaire32
A sleep diary (Figure 2-9)33 allows apatient to chart daily sleep and waketimes and should be maintained for atleast 2 consecutive weeks Review ofthis information allows the clinicianto estimate the total amount of sleepthe patient obtains in a 24-hour pe-riod The sleep diary also can provideinsight into the patientrsquos sleep patternIs sleep obtained at the same timesevery day Is the patientrsquos sleep con-solidated or fragmented across 24hours Does the patient sleep and
FIGURE 2-9 Sleep diary completed by a 46-year-old woman who presented with difficulty falling asleep Vertical linesrepresent when the patient went to bed lsquolsquoMrsquorsquo refers to when medication was taken black shading representstime asleep and unshaded white areas are time spent awake
Diary template reprinted from YOURSLEEPaasmnetorg from the American Academy of Sleep Medicine yoursleepaasmnetorgpdfsleepdiarypdf33
41Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
wake at conventional times or doeshe or she appear to be a lsquolsquonight owlrsquorsquoor lsquolsquomorning larkrsquorsquo Answers to thesequestions as provided by the sleepdiary may reveal factors that contrib-ute to sleep-related concerns Use ofsleep diaries can be particularly help-ful in patients with suspected circadianrhythm sleep disorders (including shiftwork) behaviorally induced insufficientsleep or inadequate sleep hygiene
OBJECTIVE MEASURESNocturnal polysomnography (NPSG)or related assessments are indicatedfor the diagnosis and assessment ofSDB and for positive airway titrationin patients with confirmed SDB Theprocedure can also provide informationabout EEG activity nocturnal move-ments cardiac rhythm and oxygen
saturation34 The recommended record-ing montage used in NPSG as shownin Figure 2-10 includes central (C3-A2C4-A1) frontal (F3-A2 F4-A1) andoccipital (O1-A2 O2-A1) EEGs left andright eye electrooculograms mentalsubmental surface EMG and ECG leadsOther recorded parameters includethoracic and abdominal effort oxygensaturation nasaloral airflow and bodyposition Use of a microphone torecord snoring is recommended butnot required34 A full 16-lead EEG(Figure 2-11)35 and video recordingmay be performed when nocturnalseizures are suspected Leg surfaceEMG leads are recommended andadditional arm EMG leads may beapplied when the clinical history sug-gests complex sleep-related motor be-haviors such as dream enactment In
KEY POINT
h A daily sleep diary helpsto summarize a patientrsquossleep-wake schedulemore accurately thanmemory often allowsand can facilitateconstruction ofpersonalized plansfor management ofcircadian rhythm sleepdisorders and insomnia
FIGURE 2-10 A 1-minute epoch from a nocturnal polysomnogram showing obstructive sleepapnea in a 46-year-old man who presented with snoring daytime sleepinessand headaches It depicts the standard recording montage that includes the
following leads central (C3-M2 C4-M1) frontal (F3-M2 F4-M1) and occipital (O1-M2 O2-M1)EEGs left and right eye electrooculograms (E1-M2 E2-M1) mentalsubmental electromyogram(Chin1-Chin2) electrocardiogram (ECG1-ECG2 ECG2-ECG3) snore volume (SNORE) nasalpressure transducer (NPRE) nasaloral airflow (NO) thoracic (THOR) and abdominal (ABD)effort arterial oxyhemoglobin saturation (SpO2) plethysmography (Pleth) and left and right eyeelectromyograms (LAT1-LAT2 RAT1-RAT2)
42 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
most cases the diagnostic NPSG is doneon 1 night although NPSG on 2 con-secutive nights may be considered inthe evaluation of parasomnias
Four categories of sleep monitoringdevices for use in the diagnosis of sleepdisorders have often been described34
These are type 1 standard attended in-laboratory polysomnography type 2comprehensive portable unattendedpolysomnography type 3 modifiedportable sleep apnea testing (often car-diorespiratory studies that do not recordsleep) and type 4 continuous single ordual bioparameter recording (eg pulseoximetry) However this categorizationmay not effectively classify the plethoraof out-of-center testing devices currentlyavailable for clinical use Therefore anew device classification system hasrecently been proposed This schemaknown as the SCOPER system catego-rizes out-of-center testing devices basedon measurement of sleep cardiovascu-
lar oximetry position effort and res-piratory parameters36 Within each ofthe six SCOPER categories a level of 0through 5 is assigned as indicated bythe type of sensor or measurementthat the device uses for that category
The most recent clinical guidelinespublished by the Portable MonitoringTask Force of the AASM37 for use ofunattended portable monitoring inthe diagnosis of OSA in adult patientsrecommend that portable monitoringonly be performed in conjunction witha comprehensive sleep evaluation by(or supervised by) a practitioner board-certified in sleep medicine or eligiblefor the certification examination Theseguidelines state that portable monitor-ing may be used in place of NPSG inpatients with a high pretest probabilityof moderate to severe OSA Portablemonitoring should not be used inpatients with significant medical comor-bidities (including but not limited to
KEY POINT
h The complexclassification of portabletesting devices reflectsthe multitude of designsavailable to cliniciansand will undoubtedlychange as technologyadvances
FIGURE 2-11 A The international 10Y20 system for EEG electrode placement refers to the10 and 20 interelectrode distances Even electrode numbers (2 4 6 8)represent the right hemisphere and odd electrode numbers (1 3 5 7)
represent the left hemisphere B Recommended F4-M1 C4-M1 O2-M1 placements of EEGelectrodes as set forth by the American Academy of Sleep Medicine (AASM)
Adapted from Iber C et al American Academy of SleepMedicine35 Used with permission of the American Academy ofSleep Medicine Darien IL 2012
43Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
moderate to severe pulmonary diseaseneuromuscular disease or congestiveheart failure) in patients with othersleep disorders (including central sleepapnea periodic limb movement disor-der insomnia parasomnias circadianrhythm disorders or narcolepsy) or asa screening tool The use of portablemonitoring may be indicated for thediagnosis of OSA in patients for whomattended NPSG is not possible becauseof immobility safety or critical illnessPortable monitoring may be indi-cated to monitor the response to non-continuous positive airway pressuretreatments for OSA including oralappliances upper airway surgery andweight loss The algorithm shown inAppendix B may help in the determi-nation of an adult patientrsquos candidacyfor out-of-center testing for the diag-nosis of OSA An example of portable(or home) monitoring technology isshown in Supplemental Digital Con-tent 2-1 linkslwwcomCONTA15
Recommended technology for port-able monitoring should record at mini-mum airflow respiratory effort andblood oxygenation the airflow effortand oximetric biosensors typically usedfor attended NPSG should be used37
These guidelines published in 2007will likely continue to evolve as newtechnologies emerge and are found tobe effective The current guidelinesrecommend that out-of-center testingbe performed under the auspices of anAASM-accredited comprehensive sleepmedicine program and that a board-certifiedeligible sleep specialist reviewthe raw data from a portable monitor-ing device All patients who undergoportablemonitoring for the diagnosis ofOSA should have a follow-up visit toreview test results Negative or techni-cally inadequate portable monitoringstudies should be followed by attendedin-laboratory NPSG if the clinical suspi-cion for SDB remains high37
The aforementioned testing proce-dures are primarily used in the evalua-tion of SDB Other testing modalitiesare useful in the diagnosis of othercategories of sleep disorders The mul-tiple sleep latency test (MSLT) and itsvariant the maintenance of wakefulnesstest (MWT) are used in the evaluation ofhypersomnia The conventional record-ing montage is similar to that used fornocturnal polysomnography central fron-tal and occipital EEGs left and right eyeelectrooculograms mentalsubmentalEMG and ECG leads Measurement ofthoracic and abdominal effort oxygensaturation and nasaloral airflow are notrequired but may help explain delayedsleep latencies for patients in whomrespiratory disturbances interfere withsleep onset
The MSLT is a validated tool that isconsidered the de facto standard forobjective assessment of excessive day-time sleepiness38 The recommendedprotocol38 involves five 20-minute napopportunities held at 2-hour intervalsthroughout the day If sleep is ob-served the patient is allowed to sleepfor at least 15 minutes The sleep la-tency for each nap is measured as thetime from the start of the nap trial tothe first epoch of sleep A sleep la-tency of 20 minutes is assigned to naptrials during which no sleep isobserved39 The mean sleep latencycalculated as the average sleep latencyacross all nap trials is the final resultThe presence and number of sleep-onset REM periods (SOREMPs) is alsodetermined as this information canhelp to establish a diagnosis of narco-lepsy without cataplexy or to confirmnarcolepsy with cataplexy
The MSLT should be started 15 to30 hours following completion of anocturnal polysomnogram whichshould record at least 6 hours of sleepin order for determination of the meansleep latency to be valid Drugs that may
KEY POINT
h Careful considerationshould be given tothe indications forout-of-center testingAttended nocturnalpolysomnography isindicated if a portablestudy yields a negativeor technicallyinadequate result
44 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
interfere with sleep latency or REM la-tency should be discontinued 2 weeksbefore testing whenever possible Ascreen may be performed on the day oftesting if there is suspicion that pre-scribed or illicit substances may con-tribute to the patientrsquos sleepiness38
No large multicenter systematicallycollected normative data are availablefor mean sleep latency values on theMSLT38 Nonetheless a mean sleep la-tency of greater than 10 minutes is of-ten considered normal whereas a meansleep latency of 8 to 10 minutes is con-sidered a physiologic gray zone40 Thenormative data for children are classi-fied by Tanner stage of developmentthough the MSLT is typically not per-formed in children aged younger than 6or 7 years because some daytime nap-ping may still be normal in youngchildren41 The second edition of theInternational Classification of SleepDisorders Diagnostic and CodingManual (ICSD-2)42 requires the pres-ence of a mean sleep latency of lessthan 8 minutes and two or moreSOREMPs as part of the diagnosticcriteria for narcolepsy without cata-plexy However the ICSD-2 also notesthat a mean sleep latency of less than 8minutes may occur in up to 30 of thegeneral population Therefore whilethe MSLT is a helpful and widely usedtool it remains an imperfect gold stand-ard in the assessment of daytime sleepi-ness This necessitates that theevaluation of daytime sleepiness notrest on the MSLT results alone butassimilate the clinical history subjectivecomplaints diagnostic study results andother pertinent medical information38
Practice parameters from theAASM state that the MSLT is indicatedfor diagnostic confirmation of sus-pected narcolepsy and may be indi-cated to differentiate idiopathichypersomnia from narcolepsy38 TheMSLT is not indicated for routine
assessment of OSA syndrome or toassess response to treatment of SDBand is not routinely indicated for eval-uation of sleepiness in medical orneurologic disorders (except for narco-lepsy) insomnia or circadian rhythmdisorders
TheMWTprovides an objectivemeas-ure of a patientrsquos ability to remain awakerather than the tendency to fall asleepduring the day The key differencebetween the MWT and the MSLT is thatin the former the patient is asked to tryto stay awake under circumstances con-ducive to sleep rather than to fall asleepThe MWT provides an objective vali-dated assessment of the ability to remainawake for a defined length of time38 Therecommended protocol includes four40-minute trials that begin at 2-hourintervals with the first trial to start 15 to30 hours after the patientrsquos wake-uptime A nocturnal polysomnogram onthe preceding night is not requiredHowever the patient should obtain asufficient amount of sleep during thenight before the MWT Each trial isterminated after 40 minutes if no sleepoccurs or after unequivocal sleep onset(defined as three continuous epochsof stage N1 sleep or one epoch of anyother stage of sleep) has occurred38
One indication for the MWT is to as-sess an individualrsquos ability to remainawake when his or her inability to re-main awake constitutes a public orpersonal safety issue This can becomea pressing issue for individuals em-ployed in the transportation43 con-struction or health care industriesThe MWT may be indicated to assesstreatment response in patients withknown excessive daytime sleepiness
Limited amounts of normative dataare available for the MWT Historicallymultiple testing protocols make syn-thesis of results more challenging TheMWT is used much less often in clinicalpractice compared to the MSLT Patient
KEY POINTS
h The multiple sleeplatency test is the goldstandard for objectiveassessment of daytimesleepiness butinterpretation of theresults must be madewithin the clinicalcontext of the patientrsquoshistory
h In the multiple sleeplatency test the patientis instructed to try tosleep during each naptrial In the maintenanceof wakefulness test thepatient is instructed totry to remain awakeduring the nap trial
h A baseline nocturnalpolysomnogram isrequired before amultiple sleep latencytest and considered butnot required before amaintenance ofwakefulness test
45Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
age may also affect the mean sleep la-tency values on both the MWT and theMSLT43 and may represent evolution ofcircadian rhythm and sleep architec-ture across the lifetime A study of 383patients with narcolepsy with cataplexyexamined the clinical and polysomno-graphic data at the time of diagnosis(age range 5 to 84 years) and found aprogressive decrease in the number ofSOREMPs and a progressive increase inthe mean sleep latency on the MSLT asa function of age44 Given its limita-tions the MWT may thus be used tosupplement the clinical history in theassessment of ability to stay awake butshould not be the sole determinant ofthis parameter
Actigraphy is also used in the clinicalevaluation of patients with sleep disor-ders particularly circadian rhythm sleepdisorders An actigraph is a watchlikedevice that is worn on the wrist for anextended period usually in the range ofweeks The actigraph records move-ment and uses an algorithm to estimatethe amounts of sleep and wake timeduring the recording period Analysissoftware uses movement to estimatewhen sleep and wakefulness haveoccurred Review of the data can pro-vide objective insight into the patientrsquossleep pattern including timing andduration of major sleep disruptionsActigraphy is indicated as part of theevaluation of patients with advancedsleep-phase syndrome delayed sleep-phase syndrome and shift work disor-der and may be indicated in the evalua-tion of jet lag disorder and nonY24-hoursleep-wake syndrome including thatassociated with blindness45 It can alsoserve as a measure of treatment re-sponse in patients with insomnia andcircadian rhythm sleep disorders Forpopulations in which traditional sleepmonitoring may be challenging suchas pediatric or older adult patientsactigraphy may provide valuable infor-
mation about the patientrsquos sleep pat-tern or response to treatment Whenpolysomnography is not availableactigraphy is indicated to estimate totalsleep time in patients with OSA45
OTHER ASSESSMENTMODALITIESLaboratory evaluation and neuroimag-ing with either CT or MRI may beconsidered on an individual basis asindicated by the clinical history Com-plete blood count (CBC) serum chem-istries or measures of thyroid functionmay be obtained if an underlying med-ical disorder is thought to contribute tothe patientrsquos sleep symptoms Forinstance these laboratory studies maybe consideredwhen daytime fatigue is apredominant symptom Serum ironstudies including ferritin level shouldbe checked in patients with restless legssyndrome46 Neuroimaging should beconsidered in patients with antecedenttrauma or for any sleep disorder pa-tient with an abnormal neurologic ex-amination to evaluate for a structuraletiology of the patientrsquos symptoms
APPROACH TO THE PATIENTEvaluation of suspected sleep disordersis best accomplished by a stepwisemultidimensional approach (Case 2-2)A thorough sleep history includes de-tailed description of sleep-related symp-toms nocturnal behaviors the patientrsquossleep schedule level of daytime sleepi-ness and subsequent effects on daytimefunctioning Collateral history from thepatientrsquos bed partner or family is oftennecessary to understand the severity andcontext of the patientrsquos symptoms Sub-jective assessments of sleepiness suchas the Epworth Sleepiness Scale areeasily administered and useful to tracksymptomatic progression or treatmentresponse from one visit to the nextCertain physical examination findingsmay also raise clinical suspicion of
KEY POINTS
h Actigraphy can beuseful in evaluation andtreatment of circadianrhythm sleep disordersand in management ofinsomnia
h Neuroimaging is notroutinely indicated inthe clinical evaluation ofsleep disorders andshould be pursued on acase-by-case basis
46 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
particular sleep disorders For patientsin whom multiple sleep disorders aresuspected systematic use of diagnostictesting allows for accurate identificationof specific diagnoses In a patient withinsomnia and symptoms suggestive ofSDB nocturnal polysomnography shouldbe the first procedure performed Ifthe insomnia persists despite adequatetreatment of SDB further evaluationwith sleep diaries and possibly actigra-
phy may be considered to better char-acterize the patientrsquos sleep patternActigraphy may then again be pursuedto gauge treatment response upon man-agement of the patientrsquos insomnia
The diagnostic modalities availablefor evaluation of sleep disorders arerapidly evolving In-laboratory nocturnalpolysomnography currently remains thegold standard for assessment of SDBHowever the multitude of out-of-center
KEY POINT
h Careful assimilation ofthe clinical history thesleep-specific physicalexamination patientquestionnaires anddiagnostic test resultsleads to the mostaccurate assessment ofpatients with symptomsrelated to sleep oralertness
Case 2-2A 23-year-old woman reported a 4-year history of insomnia Throughoutcollege she was a lsquolsquonight owlrsquorsquo never scheduled classes that started before100 PM and always did well in school During the past 6 months shedeveloped progressive difficulty staying awake in her job as a financialanalyst andwas concerned about how this might affect her job performance
During the week she was in bed by midnight but was unable to fallasleep until 200 AM and awoke with difficulty to an alarm at 600 AMfeeling tired She denied any thought rumination or physical discomfortat bedtime She had tried over-the-counter sleep aids that provided nosymptomatic improvement and worsened morning grogginess Onweekends she slept from 200 AM to 1100 AM and awakened feelinglsquolsquopretty goodrsquorsquo She had nocturia up to once per night and occasionalmorning headaches She had no bed partner but reported gaspingrespirations nocturnal palpitations and snort arousals On about 4 nightsper week she experienced a sensation of needing to move her legswhile trying to fall asleep This sensation was relieved by movement andwas worse at night than during the day Her legs sometimes movedspontaneously at night or while seated quietly for long periods duringthe day She felt sleepy during the afternoon especially while workingat her computer She denied drowsiness while driving She occasionallytook a 30-minute nap on the weekend and found it to be refreshingShe drank one to two cups of coffee every morning and had a 12-oz dietcaffeinated soda at 300 PM Her sleepiness had not caused her to makeany mistakes at work and she denied any mood disturbance
Physical examination was notable for a body mass index of 32 kgm2 neckcircumference of 381 cm (15 in) and modified Mallampati class III oral airwayNasal passages were narrow with turbinate hypertrophy bilaterally andhard palate was high-arched and narrow Nomicrognathia or retrognathia waspresent She had molar occlusion class I bilaterally with no overjet or overbiteThe general cardiac respiratory and neurologic examinations were normal
Comment This case illustrates how discussion of the chief complaint raisessuspicion for multiple sleep disorders The history suggests a circadian rhythmsleep disorder particularly delayed sleep-phase syndrome sleep-disorderedbreathing and restless legs syndrome Diagnostic evaluation should includenocturnal polysomnogramwith consideration toperform testing at the patientrsquospreferred sleep time and serum iron studies Sleep diaries andor actigraphymay be considered for further assessment of the patientrsquos sleep pattern
47Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
testing devices continues to grow andmany may provide useful alternativesthat under appropriate circumstancescould allow more expedient conven-ient and less costly evaluations ofincreased numbers of patients whopreviously had only limited or delayedaccess to sleep services
VIDEO LEGENDSupplemental Digital Content 2-1
Home sleep study Video demonstrates a homesleep study using an unattended type 3 portablemonitoring device The patient is a 56-year-oldman who is experiencing morning headachesand concentration and alertness problems atwork He has a history of mild snoring and ar-terial hypertension His Epworth SleepinessScale score is 18 his neck circumference is19 in he has a Mallampati classification score ofIII and his body mass index is 41 kgm Theapnea-hypopnea index is 84 eventsh Channelsrecorded in this sleep study include arterialoxyhemoglobin saturation heart rate oral-nasalpressure flow snoring inductive plethysmog-raphy for chest efforts and body position
linkslwwcomCONTA15
B 2013 Marcel Hungs MD PhD Used withpermission
REFERENCES1 National Institutes of Health National
Center on Sleep Disorders ResearchSleep disorders research planwwwnhlbinihgovhealthprofsleep201101011NationalSleepDisordersResearch-PlanDHHSPublication11-7820pdf PublishedNovember 2011
2 Dinges DF An overview of sleepiness andaccidents J Sleep Res 19954(S2)4Y14
3 Mills RJ Young CA A medical definitionof fatigue in multiple sclerosis QJM 2008101(1)49Y60
4 Chervin RD Sleepiness fatigue tirednessand lack of energy in obstructive sleepapnea Chest 2000118(2)372Y379
5 Chotinaiwattarakul W OrsquoBrien LM Fan LChervin RD Fatigue tiredness and lack ofenergy improve with treatment for OSAJ Clin Sleep Med 20095(3)222Y227
6 American Academy of Sleep MedicineThe international classification of sleepdisorders diagnostic and coding manual2nd ed Westchester IL American Academyof Sleep Medicine 2005
7 Ebben MR Spielman AJNon-pharmacological treatments forinsomnia J Behav Med 200932(3)244Y254
8 Roth T Insomnia definition prevalenceetiology and consequences J Clin SleepMed 20073(5 suppl)S7YS10
9 Yang CM Spielman AJ Glovinsky PNonpharmacologic strategies in themanagement of insomnia Psychiatr ClinNorth Am 200629(4)895Y919 abstract viii
10 Katz ES DrsquoAmbrosio CM Pediatricobstructive sleep apnea syndrome ClinChest Med 201031(2)221Y234
11 Kohler M Bloch KE Stradling JR The role ofthe nose in the pathogenesis of obstructivesleep apnea Curr Opin Otolaryngol HeadNeck Surg 200917(1)33Y37
12 Kryger MH Atlas of clinical sleep medicinePhiladelphia PA Elsevier 2010
13 Zonato AI Martinho FL Bittencourt LRet al Head and neck physical examinationcomparison between nonapneic andobstructive sleep apnea patientsLaryngoscope 2005115(6)1030Y1034
14 Mallampati SR Gatt SP Gugino LD et alA clinical sign to predict difficult trachealintubation a prospective study Can AnaesthSoc J 198532(4)429Y434
15 Samsoon GL Young JR Difficult trachealintubation a retrospective studyAnaesthesia 198742(5)487Y490
16 Huang HH Lee MS Shih YL et alModified Mallampati classificationas a clinical predictor of peroralesophagogastroduodenoscopy toleranceBMC Gastroenterol 20111112
17 Friedman M Ibrahim H Bass L Clinicalstaging for sleep-disordered breathingOtolaryngol Head Neck Surg 2002127(1)13Y21
18 Cheng RHW Yiu CKY Leung WKOral health in individuals with Downsyndrome In Dey S ed Prenatal diagnosisand screening for down syndromeInTech wwwintechopencombookshowtoreferenceprenatal-diagnosis-and-screening-for-down-syndromeoral-health-in-individuals-with-down-syndromePublished 2011 Accessed August 24 2012
19 Katz I Stradling J Slutsky AS et al Dopatients with obstructive sleep apneahave thick necks Am Rev Respir Dis1990141(5 pt 1)1228Y1231
20 Kushida CA Efron B Guilleminault C Apredictive morphometric model for theobstructive sleep apnea syndrome AnnIntern Med 1997127(8 pt 1)581Y587
48 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
21 Saccucci M Tettamanti L Mummolo S et alScoliosis and dental occlusion a review ofthe literature Scoliosis 2011615
22 Battagel JM Kotecha B Dental side-effectsof mandibular advancement splint wear inpatients who snore Clin Otolaryngol200530(2)149Y156
23 Morcos SS Patel PK The vocabulary ofdentofacial deformities Clin Plast Surg200734(3)589Y599
24 Epstein LJ Kristo D Strollo PJ Jr et alClinical guideline for the evaluationmanagement and long-term care ofobstructive sleep apnea in adults J ClinSleep Med 20095(3)263Y276
25 Johns MW A new method for measuringdaytime sleepiness the Epworth sleepinessscale Sleep 199114(6)540Y545
26 Johns MW Daytime sleepiness snoring andobstructive sleep apnea The EpworthSleepiness Scale Chest 1993103(1)30Y36
27 Chervin RD Aldrich MS The EpworthSleepiness Scale may not reflect objectivemeasures of sleepiness or sleep apneaNeurology 199952(1)125Y131
28 Buysse DJ Reynolds CF 3rd Monk THet al The Pittsburgh Sleep Quality Index anew instrument for psychiatric practice andresearch Psychiatry Res 198928(2)193Y213
29 Chervin RD Hedger K Dillon JE Pituch KJPediatric sleep questionnaire (PSQ) validityand reliability of scales for sleep-disorderedbreathing snoring sleepiness and behavioralproblems Sleep Med 20001(1)21Y32
30 Chung F Yegneswaran B Liao P et al STOPquestionnaire a tool to screen patients forobstructive sleep apnea Anesthesiology2008108(5)812Y821
31 Walters AS LeBrocq C Dhar A et alValidation of the International Restless LegsSyndrome Study Group rating scale forrestless legs syndrome Sleep Med 20034(2)121Y132
32 Bastien CH Vallieres A Morin CMValidation of the Insomnia Severity Indexas an outcome measure for insomniaresearch Sleep Med 20012(4)297Y307
33 YOURSLEEPaasmnetorg from the AmericanAcademy of Sleep Medicine Two weeksleep diary yoursleepaasmnetorgpdfsleepdiarypdf Accessed August 24 2012
34 Kushida CA Littner MR Morgenthaler Tet al Practice parameters for the indicationsfor polysomnography and relatedprocedures an update for 2005 Sleep200528(4)499Y521
35 Iber C Ancoli-Israel S Chesson A et alThe AASM manual for scoring of sleep andassociated events rules terminology andtechnical specifications 1st ed WestchesterIL American Academy of Sleep Medicine2007
36 Collop NA Tracy SL Kapur V et alObstructive sleep apnea devices forout-of-center (OOC) testing technologyevaluation J Clin Sleep Med 20117(5)531Y548
37 Collop NA Anderson WM Boehlecke Bet al Clinical guidelines for the use ofunattended portable monitors in thediagnosis of obstructive sleep apnea in adultpatients Portable Monitoring Task Forceof the American Academy of SleepMedicine J Clin Sleep Med 20073(7)737Y747
38 Littner MR Kushida C Wise M et alStandards of Practice Committee of theAmerican Academy of Sleep MedicinePractice parameters for clinical use of themultiple sleep latency test and themaintenance of wakefulness test Sleep200528(1)113Y121
39 Carskadon MA Dement WC Mitler MMet al Guidelines for the multiple sleeplatency test (MSLT) a standard measure ofsleepiness Sleep 19869(4)519Y524
40 van den Hoed J Kraemer H Guilleminault Cet al Disorders of excessive daytimesomnolence polygraphic and clinical datafor 100 patients Sleep 19814(1)23Y37
41 Hoban TF Chervin RD Assessment ofsleepiness in children Semin PediatrNeurol 20018(4)216Y228
42 ICSD-2 The international classification ofsleep disorders pocket version diagnosticand coding manual 2nd ed WestchesterIL American Academy of Sleep Medicine2005
43 Arand D Bonnet M Hurwitz T et alThe clinical use of the MSLT and MWTSleep 200528(1)123Y144
44 Dauvilliers Y Gosselin A Paquet J et alEffect of age on MSLT results in patientswith narcolepsy-cataplexy Neurology200462(1)46Y50
45 Morgenthaler T Alessi C Friedman Let al Practice parameters for the use ofactigraphy in the assessment of sleep andsleep disorders an update for 2007 Sleep200730(4)519Y529
46 Gamaldo CE Earley CJ Restless legssyndrome a clinical update Chest2006130(5)1596Y1604
49Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
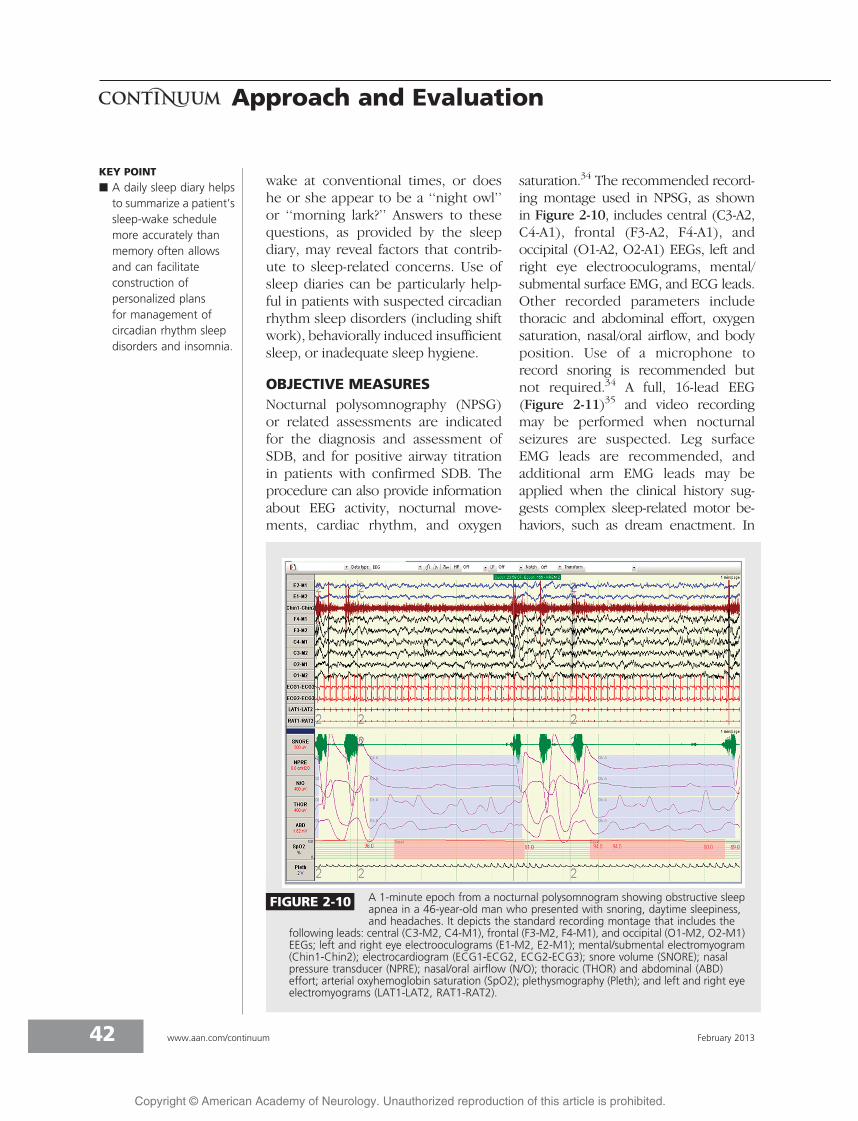
wake at conventional times or doeshe or she appear to be a lsquolsquonight owlrsquorsquoor lsquolsquomorning larkrsquorsquo Answers to thesequestions as provided by the sleepdiary may reveal factors that contrib-ute to sleep-related concerns Use ofsleep diaries can be particularly help-ful in patients with suspected circadianrhythm sleep disorders (including shiftwork) behaviorally induced insufficientsleep or inadequate sleep hygiene
OBJECTIVE MEASURESNocturnal polysomnography (NPSG)or related assessments are indicatedfor the diagnosis and assessment ofSDB and for positive airway titrationin patients with confirmed SDB Theprocedure can also provide informationabout EEG activity nocturnal move-ments cardiac rhythm and oxygen
saturation34 The recommended record-ing montage used in NPSG as shownin Figure 2-10 includes central (C3-A2C4-A1) frontal (F3-A2 F4-A1) andoccipital (O1-A2 O2-A1) EEGs left andright eye electrooculograms mentalsubmental surface EMG and ECG leadsOther recorded parameters includethoracic and abdominal effort oxygensaturation nasaloral airflow and bodyposition Use of a microphone torecord snoring is recommended butnot required34 A full 16-lead EEG(Figure 2-11)35 and video recordingmay be performed when nocturnalseizures are suspected Leg surfaceEMG leads are recommended andadditional arm EMG leads may beapplied when the clinical history sug-gests complex sleep-related motor be-haviors such as dream enactment In
KEY POINT
h A daily sleep diary helpsto summarize a patientrsquossleep-wake schedulemore accurately thanmemory often allowsand can facilitateconstruction ofpersonalized plansfor management ofcircadian rhythm sleepdisorders and insomnia
FIGURE 2-10 A 1-minute epoch from a nocturnal polysomnogram showing obstructive sleepapnea in a 46-year-old man who presented with snoring daytime sleepinessand headaches It depicts the standard recording montage that includes the
following leads central (C3-M2 C4-M1) frontal (F3-M2 F4-M1) and occipital (O1-M2 O2-M1)EEGs left and right eye electrooculograms (E1-M2 E2-M1) mentalsubmental electromyogram(Chin1-Chin2) electrocardiogram (ECG1-ECG2 ECG2-ECG3) snore volume (SNORE) nasalpressure transducer (NPRE) nasaloral airflow (NO) thoracic (THOR) and abdominal (ABD)effort arterial oxyhemoglobin saturation (SpO2) plethysmography (Pleth) and left and right eyeelectromyograms (LAT1-LAT2 RAT1-RAT2)
42 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
most cases the diagnostic NPSG is doneon 1 night although NPSG on 2 con-secutive nights may be considered inthe evaluation of parasomnias
Four categories of sleep monitoringdevices for use in the diagnosis of sleepdisorders have often been described34
These are type 1 standard attended in-laboratory polysomnography type 2comprehensive portable unattendedpolysomnography type 3 modifiedportable sleep apnea testing (often car-diorespiratory studies that do not recordsleep) and type 4 continuous single ordual bioparameter recording (eg pulseoximetry) However this categorizationmay not effectively classify the plethoraof out-of-center testing devices currentlyavailable for clinical use Therefore anew device classification system hasrecently been proposed This schemaknown as the SCOPER system catego-rizes out-of-center testing devices basedon measurement of sleep cardiovascu-
lar oximetry position effort and res-piratory parameters36 Within each ofthe six SCOPER categories a level of 0through 5 is assigned as indicated bythe type of sensor or measurementthat the device uses for that category
The most recent clinical guidelinespublished by the Portable MonitoringTask Force of the AASM37 for use ofunattended portable monitoring inthe diagnosis of OSA in adult patientsrecommend that portable monitoringonly be performed in conjunction witha comprehensive sleep evaluation by(or supervised by) a practitioner board-certified in sleep medicine or eligiblefor the certification examination Theseguidelines state that portable monitor-ing may be used in place of NPSG inpatients with a high pretest probabilityof moderate to severe OSA Portablemonitoring should not be used inpatients with significant medical comor-bidities (including but not limited to
KEY POINT
h The complexclassification of portabletesting devices reflectsthe multitude of designsavailable to cliniciansand will undoubtedlychange as technologyadvances
FIGURE 2-11 A The international 10Y20 system for EEG electrode placement refers to the10 and 20 interelectrode distances Even electrode numbers (2 4 6 8)represent the right hemisphere and odd electrode numbers (1 3 5 7)
represent the left hemisphere B Recommended F4-M1 C4-M1 O2-M1 placements of EEGelectrodes as set forth by the American Academy of Sleep Medicine (AASM)
Adapted from Iber C et al American Academy of SleepMedicine35 Used with permission of the American Academy ofSleep Medicine Darien IL 2012
43Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
moderate to severe pulmonary diseaseneuromuscular disease or congestiveheart failure) in patients with othersleep disorders (including central sleepapnea periodic limb movement disor-der insomnia parasomnias circadianrhythm disorders or narcolepsy) or asa screening tool The use of portablemonitoring may be indicated for thediagnosis of OSA in patients for whomattended NPSG is not possible becauseof immobility safety or critical illnessPortable monitoring may be indi-cated to monitor the response to non-continuous positive airway pressuretreatments for OSA including oralappliances upper airway surgery andweight loss The algorithm shown inAppendix B may help in the determi-nation of an adult patientrsquos candidacyfor out-of-center testing for the diag-nosis of OSA An example of portable(or home) monitoring technology isshown in Supplemental Digital Con-tent 2-1 linkslwwcomCONTA15
Recommended technology for port-able monitoring should record at mini-mum airflow respiratory effort andblood oxygenation the airflow effortand oximetric biosensors typically usedfor attended NPSG should be used37
These guidelines published in 2007will likely continue to evolve as newtechnologies emerge and are found tobe effective The current guidelinesrecommend that out-of-center testingbe performed under the auspices of anAASM-accredited comprehensive sleepmedicine program and that a board-certifiedeligible sleep specialist reviewthe raw data from a portable monitor-ing device All patients who undergoportablemonitoring for the diagnosis ofOSA should have a follow-up visit toreview test results Negative or techni-cally inadequate portable monitoringstudies should be followed by attendedin-laboratory NPSG if the clinical suspi-cion for SDB remains high37
The aforementioned testing proce-dures are primarily used in the evalua-tion of SDB Other testing modalitiesare useful in the diagnosis of othercategories of sleep disorders The mul-tiple sleep latency test (MSLT) and itsvariant the maintenance of wakefulnesstest (MWT) are used in the evaluation ofhypersomnia The conventional record-ing montage is similar to that used fornocturnal polysomnography central fron-tal and occipital EEGs left and right eyeelectrooculograms mentalsubmentalEMG and ECG leads Measurement ofthoracic and abdominal effort oxygensaturation and nasaloral airflow are notrequired but may help explain delayedsleep latencies for patients in whomrespiratory disturbances interfere withsleep onset
The MSLT is a validated tool that isconsidered the de facto standard forobjective assessment of excessive day-time sleepiness38 The recommendedprotocol38 involves five 20-minute napopportunities held at 2-hour intervalsthroughout the day If sleep is ob-served the patient is allowed to sleepfor at least 15 minutes The sleep la-tency for each nap is measured as thetime from the start of the nap trial tothe first epoch of sleep A sleep la-tency of 20 minutes is assigned to naptrials during which no sleep isobserved39 The mean sleep latencycalculated as the average sleep latencyacross all nap trials is the final resultThe presence and number of sleep-onset REM periods (SOREMPs) is alsodetermined as this information canhelp to establish a diagnosis of narco-lepsy without cataplexy or to confirmnarcolepsy with cataplexy
The MSLT should be started 15 to30 hours following completion of anocturnal polysomnogram whichshould record at least 6 hours of sleepin order for determination of the meansleep latency to be valid Drugs that may
KEY POINT
h Careful considerationshould be given tothe indications forout-of-center testingAttended nocturnalpolysomnography isindicated if a portablestudy yields a negativeor technicallyinadequate result
44 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
interfere with sleep latency or REM la-tency should be discontinued 2 weeksbefore testing whenever possible Ascreen may be performed on the day oftesting if there is suspicion that pre-scribed or illicit substances may con-tribute to the patientrsquos sleepiness38
No large multicenter systematicallycollected normative data are availablefor mean sleep latency values on theMSLT38 Nonetheless a mean sleep la-tency of greater than 10 minutes is of-ten considered normal whereas a meansleep latency of 8 to 10 minutes is con-sidered a physiologic gray zone40 Thenormative data for children are classi-fied by Tanner stage of developmentthough the MSLT is typically not per-formed in children aged younger than 6or 7 years because some daytime nap-ping may still be normal in youngchildren41 The second edition of theInternational Classification of SleepDisorders Diagnostic and CodingManual (ICSD-2)42 requires the pres-ence of a mean sleep latency of lessthan 8 minutes and two or moreSOREMPs as part of the diagnosticcriteria for narcolepsy without cata-plexy However the ICSD-2 also notesthat a mean sleep latency of less than 8minutes may occur in up to 30 of thegeneral population Therefore whilethe MSLT is a helpful and widely usedtool it remains an imperfect gold stand-ard in the assessment of daytime sleepi-ness This necessitates that theevaluation of daytime sleepiness notrest on the MSLT results alone butassimilate the clinical history subjectivecomplaints diagnostic study results andother pertinent medical information38
Practice parameters from theAASM state that the MSLT is indicatedfor diagnostic confirmation of sus-pected narcolepsy and may be indi-cated to differentiate idiopathichypersomnia from narcolepsy38 TheMSLT is not indicated for routine
assessment of OSA syndrome or toassess response to treatment of SDBand is not routinely indicated for eval-uation of sleepiness in medical orneurologic disorders (except for narco-lepsy) insomnia or circadian rhythmdisorders
TheMWTprovides an objectivemeas-ure of a patientrsquos ability to remain awakerather than the tendency to fall asleepduring the day The key differencebetween the MWT and the MSLT is thatin the former the patient is asked to tryto stay awake under circumstances con-ducive to sleep rather than to fall asleepThe MWT provides an objective vali-dated assessment of the ability to remainawake for a defined length of time38 Therecommended protocol includes four40-minute trials that begin at 2-hourintervals with the first trial to start 15 to30 hours after the patientrsquos wake-uptime A nocturnal polysomnogram onthe preceding night is not requiredHowever the patient should obtain asufficient amount of sleep during thenight before the MWT Each trial isterminated after 40 minutes if no sleepoccurs or after unequivocal sleep onset(defined as three continuous epochsof stage N1 sleep or one epoch of anyother stage of sleep) has occurred38
One indication for the MWT is to as-sess an individualrsquos ability to remainawake when his or her inability to re-main awake constitutes a public orpersonal safety issue This can becomea pressing issue for individuals em-ployed in the transportation43 con-struction or health care industriesThe MWT may be indicated to assesstreatment response in patients withknown excessive daytime sleepiness
Limited amounts of normative dataare available for the MWT Historicallymultiple testing protocols make syn-thesis of results more challenging TheMWT is used much less often in clinicalpractice compared to the MSLT Patient
KEY POINTS
h The multiple sleeplatency test is the goldstandard for objectiveassessment of daytimesleepiness butinterpretation of theresults must be madewithin the clinicalcontext of the patientrsquoshistory
h In the multiple sleeplatency test the patientis instructed to try tosleep during each naptrial In the maintenanceof wakefulness test thepatient is instructed totry to remain awakeduring the nap trial
h A baseline nocturnalpolysomnogram isrequired before amultiple sleep latencytest and considered butnot required before amaintenance ofwakefulness test
45Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
age may also affect the mean sleep la-tency values on both the MWT and theMSLT43 and may represent evolution ofcircadian rhythm and sleep architec-ture across the lifetime A study of 383patients with narcolepsy with cataplexyexamined the clinical and polysomno-graphic data at the time of diagnosis(age range 5 to 84 years) and found aprogressive decrease in the number ofSOREMPs and a progressive increase inthe mean sleep latency on the MSLT asa function of age44 Given its limita-tions the MWT may thus be used tosupplement the clinical history in theassessment of ability to stay awake butshould not be the sole determinant ofthis parameter
Actigraphy is also used in the clinicalevaluation of patients with sleep disor-ders particularly circadian rhythm sleepdisorders An actigraph is a watchlikedevice that is worn on the wrist for anextended period usually in the range ofweeks The actigraph records move-ment and uses an algorithm to estimatethe amounts of sleep and wake timeduring the recording period Analysissoftware uses movement to estimatewhen sleep and wakefulness haveoccurred Review of the data can pro-vide objective insight into the patientrsquossleep pattern including timing andduration of major sleep disruptionsActigraphy is indicated as part of theevaluation of patients with advancedsleep-phase syndrome delayed sleep-phase syndrome and shift work disor-der and may be indicated in the evalua-tion of jet lag disorder and nonY24-hoursleep-wake syndrome including thatassociated with blindness45 It can alsoserve as a measure of treatment re-sponse in patients with insomnia andcircadian rhythm sleep disorders Forpopulations in which traditional sleepmonitoring may be challenging suchas pediatric or older adult patientsactigraphy may provide valuable infor-
mation about the patientrsquos sleep pat-tern or response to treatment Whenpolysomnography is not availableactigraphy is indicated to estimate totalsleep time in patients with OSA45
OTHER ASSESSMENTMODALITIESLaboratory evaluation and neuroimag-ing with either CT or MRI may beconsidered on an individual basis asindicated by the clinical history Com-plete blood count (CBC) serum chem-istries or measures of thyroid functionmay be obtained if an underlying med-ical disorder is thought to contribute tothe patientrsquos sleep symptoms Forinstance these laboratory studies maybe consideredwhen daytime fatigue is apredominant symptom Serum ironstudies including ferritin level shouldbe checked in patients with restless legssyndrome46 Neuroimaging should beconsidered in patients with antecedenttrauma or for any sleep disorder pa-tient with an abnormal neurologic ex-amination to evaluate for a structuraletiology of the patientrsquos symptoms
APPROACH TO THE PATIENTEvaluation of suspected sleep disordersis best accomplished by a stepwisemultidimensional approach (Case 2-2)A thorough sleep history includes de-tailed description of sleep-related symp-toms nocturnal behaviors the patientrsquossleep schedule level of daytime sleepi-ness and subsequent effects on daytimefunctioning Collateral history from thepatientrsquos bed partner or family is oftennecessary to understand the severity andcontext of the patientrsquos symptoms Sub-jective assessments of sleepiness suchas the Epworth Sleepiness Scale areeasily administered and useful to tracksymptomatic progression or treatmentresponse from one visit to the nextCertain physical examination findingsmay also raise clinical suspicion of
KEY POINTS
h Actigraphy can beuseful in evaluation andtreatment of circadianrhythm sleep disordersand in management ofinsomnia
h Neuroimaging is notroutinely indicated inthe clinical evaluation ofsleep disorders andshould be pursued on acase-by-case basis
46 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
particular sleep disorders For patientsin whom multiple sleep disorders aresuspected systematic use of diagnostictesting allows for accurate identificationof specific diagnoses In a patient withinsomnia and symptoms suggestive ofSDB nocturnal polysomnography shouldbe the first procedure performed Ifthe insomnia persists despite adequatetreatment of SDB further evaluationwith sleep diaries and possibly actigra-
phy may be considered to better char-acterize the patientrsquos sleep patternActigraphy may then again be pursuedto gauge treatment response upon man-agement of the patientrsquos insomnia
The diagnostic modalities availablefor evaluation of sleep disorders arerapidly evolving In-laboratory nocturnalpolysomnography currently remains thegold standard for assessment of SDBHowever the multitude of out-of-center
KEY POINT
h Careful assimilation ofthe clinical history thesleep-specific physicalexamination patientquestionnaires anddiagnostic test resultsleads to the mostaccurate assessment ofpatients with symptomsrelated to sleep oralertness
Case 2-2A 23-year-old woman reported a 4-year history of insomnia Throughoutcollege she was a lsquolsquonight owlrsquorsquo never scheduled classes that started before100 PM and always did well in school During the past 6 months shedeveloped progressive difficulty staying awake in her job as a financialanalyst andwas concerned about how this might affect her job performance
During the week she was in bed by midnight but was unable to fallasleep until 200 AM and awoke with difficulty to an alarm at 600 AMfeeling tired She denied any thought rumination or physical discomfortat bedtime She had tried over-the-counter sleep aids that provided nosymptomatic improvement and worsened morning grogginess Onweekends she slept from 200 AM to 1100 AM and awakened feelinglsquolsquopretty goodrsquorsquo She had nocturia up to once per night and occasionalmorning headaches She had no bed partner but reported gaspingrespirations nocturnal palpitations and snort arousals On about 4 nightsper week she experienced a sensation of needing to move her legswhile trying to fall asleep This sensation was relieved by movement andwas worse at night than during the day Her legs sometimes movedspontaneously at night or while seated quietly for long periods duringthe day She felt sleepy during the afternoon especially while workingat her computer She denied drowsiness while driving She occasionallytook a 30-minute nap on the weekend and found it to be refreshingShe drank one to two cups of coffee every morning and had a 12-oz dietcaffeinated soda at 300 PM Her sleepiness had not caused her to makeany mistakes at work and she denied any mood disturbance
Physical examination was notable for a body mass index of 32 kgm2 neckcircumference of 381 cm (15 in) and modified Mallampati class III oral airwayNasal passages were narrow with turbinate hypertrophy bilaterally andhard palate was high-arched and narrow Nomicrognathia or retrognathia waspresent She had molar occlusion class I bilaterally with no overjet or overbiteThe general cardiac respiratory and neurologic examinations were normal
Comment This case illustrates how discussion of the chief complaint raisessuspicion for multiple sleep disorders The history suggests a circadian rhythmsleep disorder particularly delayed sleep-phase syndrome sleep-disorderedbreathing and restless legs syndrome Diagnostic evaluation should includenocturnal polysomnogramwith consideration toperform testing at the patientrsquospreferred sleep time and serum iron studies Sleep diaries andor actigraphymay be considered for further assessment of the patientrsquos sleep pattern
47Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
testing devices continues to grow andmany may provide useful alternativesthat under appropriate circumstancescould allow more expedient conven-ient and less costly evaluations ofincreased numbers of patients whopreviously had only limited or delayedaccess to sleep services
VIDEO LEGENDSupplemental Digital Content 2-1
Home sleep study Video demonstrates a homesleep study using an unattended type 3 portablemonitoring device The patient is a 56-year-oldman who is experiencing morning headachesand concentration and alertness problems atwork He has a history of mild snoring and ar-terial hypertension His Epworth SleepinessScale score is 18 his neck circumference is19 in he has a Mallampati classification score ofIII and his body mass index is 41 kgm Theapnea-hypopnea index is 84 eventsh Channelsrecorded in this sleep study include arterialoxyhemoglobin saturation heart rate oral-nasalpressure flow snoring inductive plethysmog-raphy for chest efforts and body position
linkslwwcomCONTA15
B 2013 Marcel Hungs MD PhD Used withpermission
REFERENCES1 National Institutes of Health National
Center on Sleep Disorders ResearchSleep disorders research planwwwnhlbinihgovhealthprofsleep201101011NationalSleepDisordersResearch-PlanDHHSPublication11-7820pdf PublishedNovember 2011
2 Dinges DF An overview of sleepiness andaccidents J Sleep Res 19954(S2)4Y14
3 Mills RJ Young CA A medical definitionof fatigue in multiple sclerosis QJM 2008101(1)49Y60
4 Chervin RD Sleepiness fatigue tirednessand lack of energy in obstructive sleepapnea Chest 2000118(2)372Y379
5 Chotinaiwattarakul W OrsquoBrien LM Fan LChervin RD Fatigue tiredness and lack ofenergy improve with treatment for OSAJ Clin Sleep Med 20095(3)222Y227
6 American Academy of Sleep MedicineThe international classification of sleepdisorders diagnostic and coding manual2nd ed Westchester IL American Academyof Sleep Medicine 2005
7 Ebben MR Spielman AJNon-pharmacological treatments forinsomnia J Behav Med 200932(3)244Y254
8 Roth T Insomnia definition prevalenceetiology and consequences J Clin SleepMed 20073(5 suppl)S7YS10
9 Yang CM Spielman AJ Glovinsky PNonpharmacologic strategies in themanagement of insomnia Psychiatr ClinNorth Am 200629(4)895Y919 abstract viii
10 Katz ES DrsquoAmbrosio CM Pediatricobstructive sleep apnea syndrome ClinChest Med 201031(2)221Y234
11 Kohler M Bloch KE Stradling JR The role ofthe nose in the pathogenesis of obstructivesleep apnea Curr Opin Otolaryngol HeadNeck Surg 200917(1)33Y37
12 Kryger MH Atlas of clinical sleep medicinePhiladelphia PA Elsevier 2010
13 Zonato AI Martinho FL Bittencourt LRet al Head and neck physical examinationcomparison between nonapneic andobstructive sleep apnea patientsLaryngoscope 2005115(6)1030Y1034
14 Mallampati SR Gatt SP Gugino LD et alA clinical sign to predict difficult trachealintubation a prospective study Can AnaesthSoc J 198532(4)429Y434
15 Samsoon GL Young JR Difficult trachealintubation a retrospective studyAnaesthesia 198742(5)487Y490
16 Huang HH Lee MS Shih YL et alModified Mallampati classificationas a clinical predictor of peroralesophagogastroduodenoscopy toleranceBMC Gastroenterol 20111112
17 Friedman M Ibrahim H Bass L Clinicalstaging for sleep-disordered breathingOtolaryngol Head Neck Surg 2002127(1)13Y21
18 Cheng RHW Yiu CKY Leung WKOral health in individuals with Downsyndrome In Dey S ed Prenatal diagnosisand screening for down syndromeInTech wwwintechopencombookshowtoreferenceprenatal-diagnosis-and-screening-for-down-syndromeoral-health-in-individuals-with-down-syndromePublished 2011 Accessed August 24 2012
19 Katz I Stradling J Slutsky AS et al Dopatients with obstructive sleep apneahave thick necks Am Rev Respir Dis1990141(5 pt 1)1228Y1231
20 Kushida CA Efron B Guilleminault C Apredictive morphometric model for theobstructive sleep apnea syndrome AnnIntern Med 1997127(8 pt 1)581Y587
48 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
21 Saccucci M Tettamanti L Mummolo S et alScoliosis and dental occlusion a review ofthe literature Scoliosis 2011615
22 Battagel JM Kotecha B Dental side-effectsof mandibular advancement splint wear inpatients who snore Clin Otolaryngol200530(2)149Y156
23 Morcos SS Patel PK The vocabulary ofdentofacial deformities Clin Plast Surg200734(3)589Y599
24 Epstein LJ Kristo D Strollo PJ Jr et alClinical guideline for the evaluationmanagement and long-term care ofobstructive sleep apnea in adults J ClinSleep Med 20095(3)263Y276
25 Johns MW A new method for measuringdaytime sleepiness the Epworth sleepinessscale Sleep 199114(6)540Y545
26 Johns MW Daytime sleepiness snoring andobstructive sleep apnea The EpworthSleepiness Scale Chest 1993103(1)30Y36
27 Chervin RD Aldrich MS The EpworthSleepiness Scale may not reflect objectivemeasures of sleepiness or sleep apneaNeurology 199952(1)125Y131
28 Buysse DJ Reynolds CF 3rd Monk THet al The Pittsburgh Sleep Quality Index anew instrument for psychiatric practice andresearch Psychiatry Res 198928(2)193Y213
29 Chervin RD Hedger K Dillon JE Pituch KJPediatric sleep questionnaire (PSQ) validityand reliability of scales for sleep-disorderedbreathing snoring sleepiness and behavioralproblems Sleep Med 20001(1)21Y32
30 Chung F Yegneswaran B Liao P et al STOPquestionnaire a tool to screen patients forobstructive sleep apnea Anesthesiology2008108(5)812Y821
31 Walters AS LeBrocq C Dhar A et alValidation of the International Restless LegsSyndrome Study Group rating scale forrestless legs syndrome Sleep Med 20034(2)121Y132
32 Bastien CH Vallieres A Morin CMValidation of the Insomnia Severity Indexas an outcome measure for insomniaresearch Sleep Med 20012(4)297Y307
33 YOURSLEEPaasmnetorg from the AmericanAcademy of Sleep Medicine Two weeksleep diary yoursleepaasmnetorgpdfsleepdiarypdf Accessed August 24 2012
34 Kushida CA Littner MR Morgenthaler Tet al Practice parameters for the indicationsfor polysomnography and relatedprocedures an update for 2005 Sleep200528(4)499Y521
35 Iber C Ancoli-Israel S Chesson A et alThe AASM manual for scoring of sleep andassociated events rules terminology andtechnical specifications 1st ed WestchesterIL American Academy of Sleep Medicine2007
36 Collop NA Tracy SL Kapur V et alObstructive sleep apnea devices forout-of-center (OOC) testing technologyevaluation J Clin Sleep Med 20117(5)531Y548
37 Collop NA Anderson WM Boehlecke Bet al Clinical guidelines for the use ofunattended portable monitors in thediagnosis of obstructive sleep apnea in adultpatients Portable Monitoring Task Forceof the American Academy of SleepMedicine J Clin Sleep Med 20073(7)737Y747
38 Littner MR Kushida C Wise M et alStandards of Practice Committee of theAmerican Academy of Sleep MedicinePractice parameters for clinical use of themultiple sleep latency test and themaintenance of wakefulness test Sleep200528(1)113Y121
39 Carskadon MA Dement WC Mitler MMet al Guidelines for the multiple sleeplatency test (MSLT) a standard measure ofsleepiness Sleep 19869(4)519Y524
40 van den Hoed J Kraemer H Guilleminault Cet al Disorders of excessive daytimesomnolence polygraphic and clinical datafor 100 patients Sleep 19814(1)23Y37
41 Hoban TF Chervin RD Assessment ofsleepiness in children Semin PediatrNeurol 20018(4)216Y228
42 ICSD-2 The international classification ofsleep disorders pocket version diagnosticand coding manual 2nd ed WestchesterIL American Academy of Sleep Medicine2005
43 Arand D Bonnet M Hurwitz T et alThe clinical use of the MSLT and MWTSleep 200528(1)123Y144
44 Dauvilliers Y Gosselin A Paquet J et alEffect of age on MSLT results in patientswith narcolepsy-cataplexy Neurology200462(1)46Y50
45 Morgenthaler T Alessi C Friedman Let al Practice parameters for the use ofactigraphy in the assessment of sleep andsleep disorders an update for 2007 Sleep200730(4)519Y529
46 Gamaldo CE Earley CJ Restless legssyndrome a clinical update Chest2006130(5)1596Y1604
49Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited

most cases the diagnostic NPSG is doneon 1 night although NPSG on 2 con-secutive nights may be considered inthe evaluation of parasomnias
Four categories of sleep monitoringdevices for use in the diagnosis of sleepdisorders have often been described34
These are type 1 standard attended in-laboratory polysomnography type 2comprehensive portable unattendedpolysomnography type 3 modifiedportable sleep apnea testing (often car-diorespiratory studies that do not recordsleep) and type 4 continuous single ordual bioparameter recording (eg pulseoximetry) However this categorizationmay not effectively classify the plethoraof out-of-center testing devices currentlyavailable for clinical use Therefore anew device classification system hasrecently been proposed This schemaknown as the SCOPER system catego-rizes out-of-center testing devices basedon measurement of sleep cardiovascu-
lar oximetry position effort and res-piratory parameters36 Within each ofthe six SCOPER categories a level of 0through 5 is assigned as indicated bythe type of sensor or measurementthat the device uses for that category
The most recent clinical guidelinespublished by the Portable MonitoringTask Force of the AASM37 for use ofunattended portable monitoring inthe diagnosis of OSA in adult patientsrecommend that portable monitoringonly be performed in conjunction witha comprehensive sleep evaluation by(or supervised by) a practitioner board-certified in sleep medicine or eligiblefor the certification examination Theseguidelines state that portable monitor-ing may be used in place of NPSG inpatients with a high pretest probabilityof moderate to severe OSA Portablemonitoring should not be used inpatients with significant medical comor-bidities (including but not limited to
KEY POINT
h The complexclassification of portabletesting devices reflectsthe multitude of designsavailable to cliniciansand will undoubtedlychange as technologyadvances
FIGURE 2-11 A The international 10Y20 system for EEG electrode placement refers to the10 and 20 interelectrode distances Even electrode numbers (2 4 6 8)represent the right hemisphere and odd electrode numbers (1 3 5 7)
represent the left hemisphere B Recommended F4-M1 C4-M1 O2-M1 placements of EEGelectrodes as set forth by the American Academy of Sleep Medicine (AASM)
Adapted from Iber C et al American Academy of SleepMedicine35 Used with permission of the American Academy ofSleep Medicine Darien IL 2012
43Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
moderate to severe pulmonary diseaseneuromuscular disease or congestiveheart failure) in patients with othersleep disorders (including central sleepapnea periodic limb movement disor-der insomnia parasomnias circadianrhythm disorders or narcolepsy) or asa screening tool The use of portablemonitoring may be indicated for thediagnosis of OSA in patients for whomattended NPSG is not possible becauseof immobility safety or critical illnessPortable monitoring may be indi-cated to monitor the response to non-continuous positive airway pressuretreatments for OSA including oralappliances upper airway surgery andweight loss The algorithm shown inAppendix B may help in the determi-nation of an adult patientrsquos candidacyfor out-of-center testing for the diag-nosis of OSA An example of portable(or home) monitoring technology isshown in Supplemental Digital Con-tent 2-1 linkslwwcomCONTA15
Recommended technology for port-able monitoring should record at mini-mum airflow respiratory effort andblood oxygenation the airflow effortand oximetric biosensors typically usedfor attended NPSG should be used37
These guidelines published in 2007will likely continue to evolve as newtechnologies emerge and are found tobe effective The current guidelinesrecommend that out-of-center testingbe performed under the auspices of anAASM-accredited comprehensive sleepmedicine program and that a board-certifiedeligible sleep specialist reviewthe raw data from a portable monitor-ing device All patients who undergoportablemonitoring for the diagnosis ofOSA should have a follow-up visit toreview test results Negative or techni-cally inadequate portable monitoringstudies should be followed by attendedin-laboratory NPSG if the clinical suspi-cion for SDB remains high37
The aforementioned testing proce-dures are primarily used in the evalua-tion of SDB Other testing modalitiesare useful in the diagnosis of othercategories of sleep disorders The mul-tiple sleep latency test (MSLT) and itsvariant the maintenance of wakefulnesstest (MWT) are used in the evaluation ofhypersomnia The conventional record-ing montage is similar to that used fornocturnal polysomnography central fron-tal and occipital EEGs left and right eyeelectrooculograms mentalsubmentalEMG and ECG leads Measurement ofthoracic and abdominal effort oxygensaturation and nasaloral airflow are notrequired but may help explain delayedsleep latencies for patients in whomrespiratory disturbances interfere withsleep onset
The MSLT is a validated tool that isconsidered the de facto standard forobjective assessment of excessive day-time sleepiness38 The recommendedprotocol38 involves five 20-minute napopportunities held at 2-hour intervalsthroughout the day If sleep is ob-served the patient is allowed to sleepfor at least 15 minutes The sleep la-tency for each nap is measured as thetime from the start of the nap trial tothe first epoch of sleep A sleep la-tency of 20 minutes is assigned to naptrials during which no sleep isobserved39 The mean sleep latencycalculated as the average sleep latencyacross all nap trials is the final resultThe presence and number of sleep-onset REM periods (SOREMPs) is alsodetermined as this information canhelp to establish a diagnosis of narco-lepsy without cataplexy or to confirmnarcolepsy with cataplexy
The MSLT should be started 15 to30 hours following completion of anocturnal polysomnogram whichshould record at least 6 hours of sleepin order for determination of the meansleep latency to be valid Drugs that may
KEY POINT
h Careful considerationshould be given tothe indications forout-of-center testingAttended nocturnalpolysomnography isindicated if a portablestudy yields a negativeor technicallyinadequate result
44 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
interfere with sleep latency or REM la-tency should be discontinued 2 weeksbefore testing whenever possible Ascreen may be performed on the day oftesting if there is suspicion that pre-scribed or illicit substances may con-tribute to the patientrsquos sleepiness38
No large multicenter systematicallycollected normative data are availablefor mean sleep latency values on theMSLT38 Nonetheless a mean sleep la-tency of greater than 10 minutes is of-ten considered normal whereas a meansleep latency of 8 to 10 minutes is con-sidered a physiologic gray zone40 Thenormative data for children are classi-fied by Tanner stage of developmentthough the MSLT is typically not per-formed in children aged younger than 6or 7 years because some daytime nap-ping may still be normal in youngchildren41 The second edition of theInternational Classification of SleepDisorders Diagnostic and CodingManual (ICSD-2)42 requires the pres-ence of a mean sleep latency of lessthan 8 minutes and two or moreSOREMPs as part of the diagnosticcriteria for narcolepsy without cata-plexy However the ICSD-2 also notesthat a mean sleep latency of less than 8minutes may occur in up to 30 of thegeneral population Therefore whilethe MSLT is a helpful and widely usedtool it remains an imperfect gold stand-ard in the assessment of daytime sleepi-ness This necessitates that theevaluation of daytime sleepiness notrest on the MSLT results alone butassimilate the clinical history subjectivecomplaints diagnostic study results andother pertinent medical information38
Practice parameters from theAASM state that the MSLT is indicatedfor diagnostic confirmation of sus-pected narcolepsy and may be indi-cated to differentiate idiopathichypersomnia from narcolepsy38 TheMSLT is not indicated for routine
assessment of OSA syndrome or toassess response to treatment of SDBand is not routinely indicated for eval-uation of sleepiness in medical orneurologic disorders (except for narco-lepsy) insomnia or circadian rhythmdisorders
TheMWTprovides an objectivemeas-ure of a patientrsquos ability to remain awakerather than the tendency to fall asleepduring the day The key differencebetween the MWT and the MSLT is thatin the former the patient is asked to tryto stay awake under circumstances con-ducive to sleep rather than to fall asleepThe MWT provides an objective vali-dated assessment of the ability to remainawake for a defined length of time38 Therecommended protocol includes four40-minute trials that begin at 2-hourintervals with the first trial to start 15 to30 hours after the patientrsquos wake-uptime A nocturnal polysomnogram onthe preceding night is not requiredHowever the patient should obtain asufficient amount of sleep during thenight before the MWT Each trial isterminated after 40 minutes if no sleepoccurs or after unequivocal sleep onset(defined as three continuous epochsof stage N1 sleep or one epoch of anyother stage of sleep) has occurred38
One indication for the MWT is to as-sess an individualrsquos ability to remainawake when his or her inability to re-main awake constitutes a public orpersonal safety issue This can becomea pressing issue for individuals em-ployed in the transportation43 con-struction or health care industriesThe MWT may be indicated to assesstreatment response in patients withknown excessive daytime sleepiness
Limited amounts of normative dataare available for the MWT Historicallymultiple testing protocols make syn-thesis of results more challenging TheMWT is used much less often in clinicalpractice compared to the MSLT Patient
KEY POINTS
h The multiple sleeplatency test is the goldstandard for objectiveassessment of daytimesleepiness butinterpretation of theresults must be madewithin the clinicalcontext of the patientrsquoshistory
h In the multiple sleeplatency test the patientis instructed to try tosleep during each naptrial In the maintenanceof wakefulness test thepatient is instructed totry to remain awakeduring the nap trial
h A baseline nocturnalpolysomnogram isrequired before amultiple sleep latencytest and considered butnot required before amaintenance ofwakefulness test
45Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
age may also affect the mean sleep la-tency values on both the MWT and theMSLT43 and may represent evolution ofcircadian rhythm and sleep architec-ture across the lifetime A study of 383patients with narcolepsy with cataplexyexamined the clinical and polysomno-graphic data at the time of diagnosis(age range 5 to 84 years) and found aprogressive decrease in the number ofSOREMPs and a progressive increase inthe mean sleep latency on the MSLT asa function of age44 Given its limita-tions the MWT may thus be used tosupplement the clinical history in theassessment of ability to stay awake butshould not be the sole determinant ofthis parameter
Actigraphy is also used in the clinicalevaluation of patients with sleep disor-ders particularly circadian rhythm sleepdisorders An actigraph is a watchlikedevice that is worn on the wrist for anextended period usually in the range ofweeks The actigraph records move-ment and uses an algorithm to estimatethe amounts of sleep and wake timeduring the recording period Analysissoftware uses movement to estimatewhen sleep and wakefulness haveoccurred Review of the data can pro-vide objective insight into the patientrsquossleep pattern including timing andduration of major sleep disruptionsActigraphy is indicated as part of theevaluation of patients with advancedsleep-phase syndrome delayed sleep-phase syndrome and shift work disor-der and may be indicated in the evalua-tion of jet lag disorder and nonY24-hoursleep-wake syndrome including thatassociated with blindness45 It can alsoserve as a measure of treatment re-sponse in patients with insomnia andcircadian rhythm sleep disorders Forpopulations in which traditional sleepmonitoring may be challenging suchas pediatric or older adult patientsactigraphy may provide valuable infor-
mation about the patientrsquos sleep pat-tern or response to treatment Whenpolysomnography is not availableactigraphy is indicated to estimate totalsleep time in patients with OSA45
OTHER ASSESSMENTMODALITIESLaboratory evaluation and neuroimag-ing with either CT or MRI may beconsidered on an individual basis asindicated by the clinical history Com-plete blood count (CBC) serum chem-istries or measures of thyroid functionmay be obtained if an underlying med-ical disorder is thought to contribute tothe patientrsquos sleep symptoms Forinstance these laboratory studies maybe consideredwhen daytime fatigue is apredominant symptom Serum ironstudies including ferritin level shouldbe checked in patients with restless legssyndrome46 Neuroimaging should beconsidered in patients with antecedenttrauma or for any sleep disorder pa-tient with an abnormal neurologic ex-amination to evaluate for a structuraletiology of the patientrsquos symptoms
APPROACH TO THE PATIENTEvaluation of suspected sleep disordersis best accomplished by a stepwisemultidimensional approach (Case 2-2)A thorough sleep history includes de-tailed description of sleep-related symp-toms nocturnal behaviors the patientrsquossleep schedule level of daytime sleepi-ness and subsequent effects on daytimefunctioning Collateral history from thepatientrsquos bed partner or family is oftennecessary to understand the severity andcontext of the patientrsquos symptoms Sub-jective assessments of sleepiness suchas the Epworth Sleepiness Scale areeasily administered and useful to tracksymptomatic progression or treatmentresponse from one visit to the nextCertain physical examination findingsmay also raise clinical suspicion of
KEY POINTS
h Actigraphy can beuseful in evaluation andtreatment of circadianrhythm sleep disordersand in management ofinsomnia
h Neuroimaging is notroutinely indicated inthe clinical evaluation ofsleep disorders andshould be pursued on acase-by-case basis
46 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
particular sleep disorders For patientsin whom multiple sleep disorders aresuspected systematic use of diagnostictesting allows for accurate identificationof specific diagnoses In a patient withinsomnia and symptoms suggestive ofSDB nocturnal polysomnography shouldbe the first procedure performed Ifthe insomnia persists despite adequatetreatment of SDB further evaluationwith sleep diaries and possibly actigra-
phy may be considered to better char-acterize the patientrsquos sleep patternActigraphy may then again be pursuedto gauge treatment response upon man-agement of the patientrsquos insomnia
The diagnostic modalities availablefor evaluation of sleep disorders arerapidly evolving In-laboratory nocturnalpolysomnography currently remains thegold standard for assessment of SDBHowever the multitude of out-of-center
KEY POINT
h Careful assimilation ofthe clinical history thesleep-specific physicalexamination patientquestionnaires anddiagnostic test resultsleads to the mostaccurate assessment ofpatients with symptomsrelated to sleep oralertness
Case 2-2A 23-year-old woman reported a 4-year history of insomnia Throughoutcollege she was a lsquolsquonight owlrsquorsquo never scheduled classes that started before100 PM and always did well in school During the past 6 months shedeveloped progressive difficulty staying awake in her job as a financialanalyst andwas concerned about how this might affect her job performance
During the week she was in bed by midnight but was unable to fallasleep until 200 AM and awoke with difficulty to an alarm at 600 AMfeeling tired She denied any thought rumination or physical discomfortat bedtime She had tried over-the-counter sleep aids that provided nosymptomatic improvement and worsened morning grogginess Onweekends she slept from 200 AM to 1100 AM and awakened feelinglsquolsquopretty goodrsquorsquo She had nocturia up to once per night and occasionalmorning headaches She had no bed partner but reported gaspingrespirations nocturnal palpitations and snort arousals On about 4 nightsper week she experienced a sensation of needing to move her legswhile trying to fall asleep This sensation was relieved by movement andwas worse at night than during the day Her legs sometimes movedspontaneously at night or while seated quietly for long periods duringthe day She felt sleepy during the afternoon especially while workingat her computer She denied drowsiness while driving She occasionallytook a 30-minute nap on the weekend and found it to be refreshingShe drank one to two cups of coffee every morning and had a 12-oz dietcaffeinated soda at 300 PM Her sleepiness had not caused her to makeany mistakes at work and she denied any mood disturbance
Physical examination was notable for a body mass index of 32 kgm2 neckcircumference of 381 cm (15 in) and modified Mallampati class III oral airwayNasal passages were narrow with turbinate hypertrophy bilaterally andhard palate was high-arched and narrow Nomicrognathia or retrognathia waspresent She had molar occlusion class I bilaterally with no overjet or overbiteThe general cardiac respiratory and neurologic examinations were normal
Comment This case illustrates how discussion of the chief complaint raisessuspicion for multiple sleep disorders The history suggests a circadian rhythmsleep disorder particularly delayed sleep-phase syndrome sleep-disorderedbreathing and restless legs syndrome Diagnostic evaluation should includenocturnal polysomnogramwith consideration toperform testing at the patientrsquospreferred sleep time and serum iron studies Sleep diaries andor actigraphymay be considered for further assessment of the patientrsquos sleep pattern
47Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
testing devices continues to grow andmany may provide useful alternativesthat under appropriate circumstancescould allow more expedient conven-ient and less costly evaluations ofincreased numbers of patients whopreviously had only limited or delayedaccess to sleep services
VIDEO LEGENDSupplemental Digital Content 2-1
Home sleep study Video demonstrates a homesleep study using an unattended type 3 portablemonitoring device The patient is a 56-year-oldman who is experiencing morning headachesand concentration and alertness problems atwork He has a history of mild snoring and ar-terial hypertension His Epworth SleepinessScale score is 18 his neck circumference is19 in he has a Mallampati classification score ofIII and his body mass index is 41 kgm Theapnea-hypopnea index is 84 eventsh Channelsrecorded in this sleep study include arterialoxyhemoglobin saturation heart rate oral-nasalpressure flow snoring inductive plethysmog-raphy for chest efforts and body position
linkslwwcomCONTA15
B 2013 Marcel Hungs MD PhD Used withpermission
REFERENCES1 National Institutes of Health National
Center on Sleep Disorders ResearchSleep disorders research planwwwnhlbinihgovhealthprofsleep201101011NationalSleepDisordersResearch-PlanDHHSPublication11-7820pdf PublishedNovember 2011
2 Dinges DF An overview of sleepiness andaccidents J Sleep Res 19954(S2)4Y14
3 Mills RJ Young CA A medical definitionof fatigue in multiple sclerosis QJM 2008101(1)49Y60
4 Chervin RD Sleepiness fatigue tirednessand lack of energy in obstructive sleepapnea Chest 2000118(2)372Y379
5 Chotinaiwattarakul W OrsquoBrien LM Fan LChervin RD Fatigue tiredness and lack ofenergy improve with treatment for OSAJ Clin Sleep Med 20095(3)222Y227
6 American Academy of Sleep MedicineThe international classification of sleepdisorders diagnostic and coding manual2nd ed Westchester IL American Academyof Sleep Medicine 2005
7 Ebben MR Spielman AJNon-pharmacological treatments forinsomnia J Behav Med 200932(3)244Y254
8 Roth T Insomnia definition prevalenceetiology and consequences J Clin SleepMed 20073(5 suppl)S7YS10
9 Yang CM Spielman AJ Glovinsky PNonpharmacologic strategies in themanagement of insomnia Psychiatr ClinNorth Am 200629(4)895Y919 abstract viii
10 Katz ES DrsquoAmbrosio CM Pediatricobstructive sleep apnea syndrome ClinChest Med 201031(2)221Y234
11 Kohler M Bloch KE Stradling JR The role ofthe nose in the pathogenesis of obstructivesleep apnea Curr Opin Otolaryngol HeadNeck Surg 200917(1)33Y37
12 Kryger MH Atlas of clinical sleep medicinePhiladelphia PA Elsevier 2010
13 Zonato AI Martinho FL Bittencourt LRet al Head and neck physical examinationcomparison between nonapneic andobstructive sleep apnea patientsLaryngoscope 2005115(6)1030Y1034
14 Mallampati SR Gatt SP Gugino LD et alA clinical sign to predict difficult trachealintubation a prospective study Can AnaesthSoc J 198532(4)429Y434
15 Samsoon GL Young JR Difficult trachealintubation a retrospective studyAnaesthesia 198742(5)487Y490
16 Huang HH Lee MS Shih YL et alModified Mallampati classificationas a clinical predictor of peroralesophagogastroduodenoscopy toleranceBMC Gastroenterol 20111112
17 Friedman M Ibrahim H Bass L Clinicalstaging for sleep-disordered breathingOtolaryngol Head Neck Surg 2002127(1)13Y21
18 Cheng RHW Yiu CKY Leung WKOral health in individuals with Downsyndrome In Dey S ed Prenatal diagnosisand screening for down syndromeInTech wwwintechopencombookshowtoreferenceprenatal-diagnosis-and-screening-for-down-syndromeoral-health-in-individuals-with-down-syndromePublished 2011 Accessed August 24 2012
19 Katz I Stradling J Slutsky AS et al Dopatients with obstructive sleep apneahave thick necks Am Rev Respir Dis1990141(5 pt 1)1228Y1231
20 Kushida CA Efron B Guilleminault C Apredictive morphometric model for theobstructive sleep apnea syndrome AnnIntern Med 1997127(8 pt 1)581Y587
48 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
21 Saccucci M Tettamanti L Mummolo S et alScoliosis and dental occlusion a review ofthe literature Scoliosis 2011615
22 Battagel JM Kotecha B Dental side-effectsof mandibular advancement splint wear inpatients who snore Clin Otolaryngol200530(2)149Y156
23 Morcos SS Patel PK The vocabulary ofdentofacial deformities Clin Plast Surg200734(3)589Y599
24 Epstein LJ Kristo D Strollo PJ Jr et alClinical guideline for the evaluationmanagement and long-term care ofobstructive sleep apnea in adults J ClinSleep Med 20095(3)263Y276
25 Johns MW A new method for measuringdaytime sleepiness the Epworth sleepinessscale Sleep 199114(6)540Y545
26 Johns MW Daytime sleepiness snoring andobstructive sleep apnea The EpworthSleepiness Scale Chest 1993103(1)30Y36
27 Chervin RD Aldrich MS The EpworthSleepiness Scale may not reflect objectivemeasures of sleepiness or sleep apneaNeurology 199952(1)125Y131
28 Buysse DJ Reynolds CF 3rd Monk THet al The Pittsburgh Sleep Quality Index anew instrument for psychiatric practice andresearch Psychiatry Res 198928(2)193Y213
29 Chervin RD Hedger K Dillon JE Pituch KJPediatric sleep questionnaire (PSQ) validityand reliability of scales for sleep-disorderedbreathing snoring sleepiness and behavioralproblems Sleep Med 20001(1)21Y32
30 Chung F Yegneswaran B Liao P et al STOPquestionnaire a tool to screen patients forobstructive sleep apnea Anesthesiology2008108(5)812Y821
31 Walters AS LeBrocq C Dhar A et alValidation of the International Restless LegsSyndrome Study Group rating scale forrestless legs syndrome Sleep Med 20034(2)121Y132
32 Bastien CH Vallieres A Morin CMValidation of the Insomnia Severity Indexas an outcome measure for insomniaresearch Sleep Med 20012(4)297Y307
33 YOURSLEEPaasmnetorg from the AmericanAcademy of Sleep Medicine Two weeksleep diary yoursleepaasmnetorgpdfsleepdiarypdf Accessed August 24 2012
34 Kushida CA Littner MR Morgenthaler Tet al Practice parameters for the indicationsfor polysomnography and relatedprocedures an update for 2005 Sleep200528(4)499Y521
35 Iber C Ancoli-Israel S Chesson A et alThe AASM manual for scoring of sleep andassociated events rules terminology andtechnical specifications 1st ed WestchesterIL American Academy of Sleep Medicine2007
36 Collop NA Tracy SL Kapur V et alObstructive sleep apnea devices forout-of-center (OOC) testing technologyevaluation J Clin Sleep Med 20117(5)531Y548
37 Collop NA Anderson WM Boehlecke Bet al Clinical guidelines for the use ofunattended portable monitors in thediagnosis of obstructive sleep apnea in adultpatients Portable Monitoring Task Forceof the American Academy of SleepMedicine J Clin Sleep Med 20073(7)737Y747
38 Littner MR Kushida C Wise M et alStandards of Practice Committee of theAmerican Academy of Sleep MedicinePractice parameters for clinical use of themultiple sleep latency test and themaintenance of wakefulness test Sleep200528(1)113Y121
39 Carskadon MA Dement WC Mitler MMet al Guidelines for the multiple sleeplatency test (MSLT) a standard measure ofsleepiness Sleep 19869(4)519Y524
40 van den Hoed J Kraemer H Guilleminault Cet al Disorders of excessive daytimesomnolence polygraphic and clinical datafor 100 patients Sleep 19814(1)23Y37
41 Hoban TF Chervin RD Assessment ofsleepiness in children Semin PediatrNeurol 20018(4)216Y228
42 ICSD-2 The international classification ofsleep disorders pocket version diagnosticand coding manual 2nd ed WestchesterIL American Academy of Sleep Medicine2005
43 Arand D Bonnet M Hurwitz T et alThe clinical use of the MSLT and MWTSleep 200528(1)123Y144
44 Dauvilliers Y Gosselin A Paquet J et alEffect of age on MSLT results in patientswith narcolepsy-cataplexy Neurology200462(1)46Y50
45 Morgenthaler T Alessi C Friedman Let al Practice parameters for the use ofactigraphy in the assessment of sleep andsleep disorders an update for 2007 Sleep200730(4)519Y529
46 Gamaldo CE Earley CJ Restless legssyndrome a clinical update Chest2006130(5)1596Y1604
49Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited

moderate to severe pulmonary diseaseneuromuscular disease or congestiveheart failure) in patients with othersleep disorders (including central sleepapnea periodic limb movement disor-der insomnia parasomnias circadianrhythm disorders or narcolepsy) or asa screening tool The use of portablemonitoring may be indicated for thediagnosis of OSA in patients for whomattended NPSG is not possible becauseof immobility safety or critical illnessPortable monitoring may be indi-cated to monitor the response to non-continuous positive airway pressuretreatments for OSA including oralappliances upper airway surgery andweight loss The algorithm shown inAppendix B may help in the determi-nation of an adult patientrsquos candidacyfor out-of-center testing for the diag-nosis of OSA An example of portable(or home) monitoring technology isshown in Supplemental Digital Con-tent 2-1 linkslwwcomCONTA15
Recommended technology for port-able monitoring should record at mini-mum airflow respiratory effort andblood oxygenation the airflow effortand oximetric biosensors typically usedfor attended NPSG should be used37
These guidelines published in 2007will likely continue to evolve as newtechnologies emerge and are found tobe effective The current guidelinesrecommend that out-of-center testingbe performed under the auspices of anAASM-accredited comprehensive sleepmedicine program and that a board-certifiedeligible sleep specialist reviewthe raw data from a portable monitor-ing device All patients who undergoportablemonitoring for the diagnosis ofOSA should have a follow-up visit toreview test results Negative or techni-cally inadequate portable monitoringstudies should be followed by attendedin-laboratory NPSG if the clinical suspi-cion for SDB remains high37
The aforementioned testing proce-dures are primarily used in the evalua-tion of SDB Other testing modalitiesare useful in the diagnosis of othercategories of sleep disorders The mul-tiple sleep latency test (MSLT) and itsvariant the maintenance of wakefulnesstest (MWT) are used in the evaluation ofhypersomnia The conventional record-ing montage is similar to that used fornocturnal polysomnography central fron-tal and occipital EEGs left and right eyeelectrooculograms mentalsubmentalEMG and ECG leads Measurement ofthoracic and abdominal effort oxygensaturation and nasaloral airflow are notrequired but may help explain delayedsleep latencies for patients in whomrespiratory disturbances interfere withsleep onset
The MSLT is a validated tool that isconsidered the de facto standard forobjective assessment of excessive day-time sleepiness38 The recommendedprotocol38 involves five 20-minute napopportunities held at 2-hour intervalsthroughout the day If sleep is ob-served the patient is allowed to sleepfor at least 15 minutes The sleep la-tency for each nap is measured as thetime from the start of the nap trial tothe first epoch of sleep A sleep la-tency of 20 minutes is assigned to naptrials during which no sleep isobserved39 The mean sleep latencycalculated as the average sleep latencyacross all nap trials is the final resultThe presence and number of sleep-onset REM periods (SOREMPs) is alsodetermined as this information canhelp to establish a diagnosis of narco-lepsy without cataplexy or to confirmnarcolepsy with cataplexy
The MSLT should be started 15 to30 hours following completion of anocturnal polysomnogram whichshould record at least 6 hours of sleepin order for determination of the meansleep latency to be valid Drugs that may
KEY POINT
h Careful considerationshould be given tothe indications forout-of-center testingAttended nocturnalpolysomnography isindicated if a portablestudy yields a negativeor technicallyinadequate result
44 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
interfere with sleep latency or REM la-tency should be discontinued 2 weeksbefore testing whenever possible Ascreen may be performed on the day oftesting if there is suspicion that pre-scribed or illicit substances may con-tribute to the patientrsquos sleepiness38
No large multicenter systematicallycollected normative data are availablefor mean sleep latency values on theMSLT38 Nonetheless a mean sleep la-tency of greater than 10 minutes is of-ten considered normal whereas a meansleep latency of 8 to 10 minutes is con-sidered a physiologic gray zone40 Thenormative data for children are classi-fied by Tanner stage of developmentthough the MSLT is typically not per-formed in children aged younger than 6or 7 years because some daytime nap-ping may still be normal in youngchildren41 The second edition of theInternational Classification of SleepDisorders Diagnostic and CodingManual (ICSD-2)42 requires the pres-ence of a mean sleep latency of lessthan 8 minutes and two or moreSOREMPs as part of the diagnosticcriteria for narcolepsy without cata-plexy However the ICSD-2 also notesthat a mean sleep latency of less than 8minutes may occur in up to 30 of thegeneral population Therefore whilethe MSLT is a helpful and widely usedtool it remains an imperfect gold stand-ard in the assessment of daytime sleepi-ness This necessitates that theevaluation of daytime sleepiness notrest on the MSLT results alone butassimilate the clinical history subjectivecomplaints diagnostic study results andother pertinent medical information38
Practice parameters from theAASM state that the MSLT is indicatedfor diagnostic confirmation of sus-pected narcolepsy and may be indi-cated to differentiate idiopathichypersomnia from narcolepsy38 TheMSLT is not indicated for routine
assessment of OSA syndrome or toassess response to treatment of SDBand is not routinely indicated for eval-uation of sleepiness in medical orneurologic disorders (except for narco-lepsy) insomnia or circadian rhythmdisorders
TheMWTprovides an objectivemeas-ure of a patientrsquos ability to remain awakerather than the tendency to fall asleepduring the day The key differencebetween the MWT and the MSLT is thatin the former the patient is asked to tryto stay awake under circumstances con-ducive to sleep rather than to fall asleepThe MWT provides an objective vali-dated assessment of the ability to remainawake for a defined length of time38 Therecommended protocol includes four40-minute trials that begin at 2-hourintervals with the first trial to start 15 to30 hours after the patientrsquos wake-uptime A nocturnal polysomnogram onthe preceding night is not requiredHowever the patient should obtain asufficient amount of sleep during thenight before the MWT Each trial isterminated after 40 minutes if no sleepoccurs or after unequivocal sleep onset(defined as three continuous epochsof stage N1 sleep or one epoch of anyother stage of sleep) has occurred38
One indication for the MWT is to as-sess an individualrsquos ability to remainawake when his or her inability to re-main awake constitutes a public orpersonal safety issue This can becomea pressing issue for individuals em-ployed in the transportation43 con-struction or health care industriesThe MWT may be indicated to assesstreatment response in patients withknown excessive daytime sleepiness
Limited amounts of normative dataare available for the MWT Historicallymultiple testing protocols make syn-thesis of results more challenging TheMWT is used much less often in clinicalpractice compared to the MSLT Patient
KEY POINTS
h The multiple sleeplatency test is the goldstandard for objectiveassessment of daytimesleepiness butinterpretation of theresults must be madewithin the clinicalcontext of the patientrsquoshistory
h In the multiple sleeplatency test the patientis instructed to try tosleep during each naptrial In the maintenanceof wakefulness test thepatient is instructed totry to remain awakeduring the nap trial
h A baseline nocturnalpolysomnogram isrequired before amultiple sleep latencytest and considered butnot required before amaintenance ofwakefulness test
45Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
age may also affect the mean sleep la-tency values on both the MWT and theMSLT43 and may represent evolution ofcircadian rhythm and sleep architec-ture across the lifetime A study of 383patients with narcolepsy with cataplexyexamined the clinical and polysomno-graphic data at the time of diagnosis(age range 5 to 84 years) and found aprogressive decrease in the number ofSOREMPs and a progressive increase inthe mean sleep latency on the MSLT asa function of age44 Given its limita-tions the MWT may thus be used tosupplement the clinical history in theassessment of ability to stay awake butshould not be the sole determinant ofthis parameter
Actigraphy is also used in the clinicalevaluation of patients with sleep disor-ders particularly circadian rhythm sleepdisorders An actigraph is a watchlikedevice that is worn on the wrist for anextended period usually in the range ofweeks The actigraph records move-ment and uses an algorithm to estimatethe amounts of sleep and wake timeduring the recording period Analysissoftware uses movement to estimatewhen sleep and wakefulness haveoccurred Review of the data can pro-vide objective insight into the patientrsquossleep pattern including timing andduration of major sleep disruptionsActigraphy is indicated as part of theevaluation of patients with advancedsleep-phase syndrome delayed sleep-phase syndrome and shift work disor-der and may be indicated in the evalua-tion of jet lag disorder and nonY24-hoursleep-wake syndrome including thatassociated with blindness45 It can alsoserve as a measure of treatment re-sponse in patients with insomnia andcircadian rhythm sleep disorders Forpopulations in which traditional sleepmonitoring may be challenging suchas pediatric or older adult patientsactigraphy may provide valuable infor-
mation about the patientrsquos sleep pat-tern or response to treatment Whenpolysomnography is not availableactigraphy is indicated to estimate totalsleep time in patients with OSA45
OTHER ASSESSMENTMODALITIESLaboratory evaluation and neuroimag-ing with either CT or MRI may beconsidered on an individual basis asindicated by the clinical history Com-plete blood count (CBC) serum chem-istries or measures of thyroid functionmay be obtained if an underlying med-ical disorder is thought to contribute tothe patientrsquos sleep symptoms Forinstance these laboratory studies maybe consideredwhen daytime fatigue is apredominant symptom Serum ironstudies including ferritin level shouldbe checked in patients with restless legssyndrome46 Neuroimaging should beconsidered in patients with antecedenttrauma or for any sleep disorder pa-tient with an abnormal neurologic ex-amination to evaluate for a structuraletiology of the patientrsquos symptoms
APPROACH TO THE PATIENTEvaluation of suspected sleep disordersis best accomplished by a stepwisemultidimensional approach (Case 2-2)A thorough sleep history includes de-tailed description of sleep-related symp-toms nocturnal behaviors the patientrsquossleep schedule level of daytime sleepi-ness and subsequent effects on daytimefunctioning Collateral history from thepatientrsquos bed partner or family is oftennecessary to understand the severity andcontext of the patientrsquos symptoms Sub-jective assessments of sleepiness suchas the Epworth Sleepiness Scale areeasily administered and useful to tracksymptomatic progression or treatmentresponse from one visit to the nextCertain physical examination findingsmay also raise clinical suspicion of
KEY POINTS
h Actigraphy can beuseful in evaluation andtreatment of circadianrhythm sleep disordersand in management ofinsomnia
h Neuroimaging is notroutinely indicated inthe clinical evaluation ofsleep disorders andshould be pursued on acase-by-case basis
46 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
particular sleep disorders For patientsin whom multiple sleep disorders aresuspected systematic use of diagnostictesting allows for accurate identificationof specific diagnoses In a patient withinsomnia and symptoms suggestive ofSDB nocturnal polysomnography shouldbe the first procedure performed Ifthe insomnia persists despite adequatetreatment of SDB further evaluationwith sleep diaries and possibly actigra-
phy may be considered to better char-acterize the patientrsquos sleep patternActigraphy may then again be pursuedto gauge treatment response upon man-agement of the patientrsquos insomnia
The diagnostic modalities availablefor evaluation of sleep disorders arerapidly evolving In-laboratory nocturnalpolysomnography currently remains thegold standard for assessment of SDBHowever the multitude of out-of-center
KEY POINT
h Careful assimilation ofthe clinical history thesleep-specific physicalexamination patientquestionnaires anddiagnostic test resultsleads to the mostaccurate assessment ofpatients with symptomsrelated to sleep oralertness
Case 2-2A 23-year-old woman reported a 4-year history of insomnia Throughoutcollege she was a lsquolsquonight owlrsquorsquo never scheduled classes that started before100 PM and always did well in school During the past 6 months shedeveloped progressive difficulty staying awake in her job as a financialanalyst andwas concerned about how this might affect her job performance
During the week she was in bed by midnight but was unable to fallasleep until 200 AM and awoke with difficulty to an alarm at 600 AMfeeling tired She denied any thought rumination or physical discomfortat bedtime She had tried over-the-counter sleep aids that provided nosymptomatic improvement and worsened morning grogginess Onweekends she slept from 200 AM to 1100 AM and awakened feelinglsquolsquopretty goodrsquorsquo She had nocturia up to once per night and occasionalmorning headaches She had no bed partner but reported gaspingrespirations nocturnal palpitations and snort arousals On about 4 nightsper week she experienced a sensation of needing to move her legswhile trying to fall asleep This sensation was relieved by movement andwas worse at night than during the day Her legs sometimes movedspontaneously at night or while seated quietly for long periods duringthe day She felt sleepy during the afternoon especially while workingat her computer She denied drowsiness while driving She occasionallytook a 30-minute nap on the weekend and found it to be refreshingShe drank one to two cups of coffee every morning and had a 12-oz dietcaffeinated soda at 300 PM Her sleepiness had not caused her to makeany mistakes at work and she denied any mood disturbance
Physical examination was notable for a body mass index of 32 kgm2 neckcircumference of 381 cm (15 in) and modified Mallampati class III oral airwayNasal passages were narrow with turbinate hypertrophy bilaterally andhard palate was high-arched and narrow Nomicrognathia or retrognathia waspresent She had molar occlusion class I bilaterally with no overjet or overbiteThe general cardiac respiratory and neurologic examinations were normal
Comment This case illustrates how discussion of the chief complaint raisessuspicion for multiple sleep disorders The history suggests a circadian rhythmsleep disorder particularly delayed sleep-phase syndrome sleep-disorderedbreathing and restless legs syndrome Diagnostic evaluation should includenocturnal polysomnogramwith consideration toperform testing at the patientrsquospreferred sleep time and serum iron studies Sleep diaries andor actigraphymay be considered for further assessment of the patientrsquos sleep pattern
47Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
testing devices continues to grow andmany may provide useful alternativesthat under appropriate circumstancescould allow more expedient conven-ient and less costly evaluations ofincreased numbers of patients whopreviously had only limited or delayedaccess to sleep services
VIDEO LEGENDSupplemental Digital Content 2-1
Home sleep study Video demonstrates a homesleep study using an unattended type 3 portablemonitoring device The patient is a 56-year-oldman who is experiencing morning headachesand concentration and alertness problems atwork He has a history of mild snoring and ar-terial hypertension His Epworth SleepinessScale score is 18 his neck circumference is19 in he has a Mallampati classification score ofIII and his body mass index is 41 kgm Theapnea-hypopnea index is 84 eventsh Channelsrecorded in this sleep study include arterialoxyhemoglobin saturation heart rate oral-nasalpressure flow snoring inductive plethysmog-raphy for chest efforts and body position
linkslwwcomCONTA15
B 2013 Marcel Hungs MD PhD Used withpermission
REFERENCES1 National Institutes of Health National
Center on Sleep Disorders ResearchSleep disorders research planwwwnhlbinihgovhealthprofsleep201101011NationalSleepDisordersResearch-PlanDHHSPublication11-7820pdf PublishedNovember 2011
2 Dinges DF An overview of sleepiness andaccidents J Sleep Res 19954(S2)4Y14
3 Mills RJ Young CA A medical definitionof fatigue in multiple sclerosis QJM 2008101(1)49Y60
4 Chervin RD Sleepiness fatigue tirednessand lack of energy in obstructive sleepapnea Chest 2000118(2)372Y379
5 Chotinaiwattarakul W OrsquoBrien LM Fan LChervin RD Fatigue tiredness and lack ofenergy improve with treatment for OSAJ Clin Sleep Med 20095(3)222Y227
6 American Academy of Sleep MedicineThe international classification of sleepdisorders diagnostic and coding manual2nd ed Westchester IL American Academyof Sleep Medicine 2005
7 Ebben MR Spielman AJNon-pharmacological treatments forinsomnia J Behav Med 200932(3)244Y254
8 Roth T Insomnia definition prevalenceetiology and consequences J Clin SleepMed 20073(5 suppl)S7YS10
9 Yang CM Spielman AJ Glovinsky PNonpharmacologic strategies in themanagement of insomnia Psychiatr ClinNorth Am 200629(4)895Y919 abstract viii
10 Katz ES DrsquoAmbrosio CM Pediatricobstructive sleep apnea syndrome ClinChest Med 201031(2)221Y234
11 Kohler M Bloch KE Stradling JR The role ofthe nose in the pathogenesis of obstructivesleep apnea Curr Opin Otolaryngol HeadNeck Surg 200917(1)33Y37
12 Kryger MH Atlas of clinical sleep medicinePhiladelphia PA Elsevier 2010
13 Zonato AI Martinho FL Bittencourt LRet al Head and neck physical examinationcomparison between nonapneic andobstructive sleep apnea patientsLaryngoscope 2005115(6)1030Y1034
14 Mallampati SR Gatt SP Gugino LD et alA clinical sign to predict difficult trachealintubation a prospective study Can AnaesthSoc J 198532(4)429Y434
15 Samsoon GL Young JR Difficult trachealintubation a retrospective studyAnaesthesia 198742(5)487Y490
16 Huang HH Lee MS Shih YL et alModified Mallampati classificationas a clinical predictor of peroralesophagogastroduodenoscopy toleranceBMC Gastroenterol 20111112
17 Friedman M Ibrahim H Bass L Clinicalstaging for sleep-disordered breathingOtolaryngol Head Neck Surg 2002127(1)13Y21
18 Cheng RHW Yiu CKY Leung WKOral health in individuals with Downsyndrome In Dey S ed Prenatal diagnosisand screening for down syndromeInTech wwwintechopencombookshowtoreferenceprenatal-diagnosis-and-screening-for-down-syndromeoral-health-in-individuals-with-down-syndromePublished 2011 Accessed August 24 2012
19 Katz I Stradling J Slutsky AS et al Dopatients with obstructive sleep apneahave thick necks Am Rev Respir Dis1990141(5 pt 1)1228Y1231
20 Kushida CA Efron B Guilleminault C Apredictive morphometric model for theobstructive sleep apnea syndrome AnnIntern Med 1997127(8 pt 1)581Y587
48 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
21 Saccucci M Tettamanti L Mummolo S et alScoliosis and dental occlusion a review ofthe literature Scoliosis 2011615
22 Battagel JM Kotecha B Dental side-effectsof mandibular advancement splint wear inpatients who snore Clin Otolaryngol200530(2)149Y156
23 Morcos SS Patel PK The vocabulary ofdentofacial deformities Clin Plast Surg200734(3)589Y599
24 Epstein LJ Kristo D Strollo PJ Jr et alClinical guideline for the evaluationmanagement and long-term care ofobstructive sleep apnea in adults J ClinSleep Med 20095(3)263Y276
25 Johns MW A new method for measuringdaytime sleepiness the Epworth sleepinessscale Sleep 199114(6)540Y545
26 Johns MW Daytime sleepiness snoring andobstructive sleep apnea The EpworthSleepiness Scale Chest 1993103(1)30Y36
27 Chervin RD Aldrich MS The EpworthSleepiness Scale may not reflect objectivemeasures of sleepiness or sleep apneaNeurology 199952(1)125Y131
28 Buysse DJ Reynolds CF 3rd Monk THet al The Pittsburgh Sleep Quality Index anew instrument for psychiatric practice andresearch Psychiatry Res 198928(2)193Y213
29 Chervin RD Hedger K Dillon JE Pituch KJPediatric sleep questionnaire (PSQ) validityand reliability of scales for sleep-disorderedbreathing snoring sleepiness and behavioralproblems Sleep Med 20001(1)21Y32
30 Chung F Yegneswaran B Liao P et al STOPquestionnaire a tool to screen patients forobstructive sleep apnea Anesthesiology2008108(5)812Y821
31 Walters AS LeBrocq C Dhar A et alValidation of the International Restless LegsSyndrome Study Group rating scale forrestless legs syndrome Sleep Med 20034(2)121Y132
32 Bastien CH Vallieres A Morin CMValidation of the Insomnia Severity Indexas an outcome measure for insomniaresearch Sleep Med 20012(4)297Y307
33 YOURSLEEPaasmnetorg from the AmericanAcademy of Sleep Medicine Two weeksleep diary yoursleepaasmnetorgpdfsleepdiarypdf Accessed August 24 2012
34 Kushida CA Littner MR Morgenthaler Tet al Practice parameters for the indicationsfor polysomnography and relatedprocedures an update for 2005 Sleep200528(4)499Y521
35 Iber C Ancoli-Israel S Chesson A et alThe AASM manual for scoring of sleep andassociated events rules terminology andtechnical specifications 1st ed WestchesterIL American Academy of Sleep Medicine2007
36 Collop NA Tracy SL Kapur V et alObstructive sleep apnea devices forout-of-center (OOC) testing technologyevaluation J Clin Sleep Med 20117(5)531Y548
37 Collop NA Anderson WM Boehlecke Bet al Clinical guidelines for the use ofunattended portable monitors in thediagnosis of obstructive sleep apnea in adultpatients Portable Monitoring Task Forceof the American Academy of SleepMedicine J Clin Sleep Med 20073(7)737Y747
38 Littner MR Kushida C Wise M et alStandards of Practice Committee of theAmerican Academy of Sleep MedicinePractice parameters for clinical use of themultiple sleep latency test and themaintenance of wakefulness test Sleep200528(1)113Y121
39 Carskadon MA Dement WC Mitler MMet al Guidelines for the multiple sleeplatency test (MSLT) a standard measure ofsleepiness Sleep 19869(4)519Y524
40 van den Hoed J Kraemer H Guilleminault Cet al Disorders of excessive daytimesomnolence polygraphic and clinical datafor 100 patients Sleep 19814(1)23Y37
41 Hoban TF Chervin RD Assessment ofsleepiness in children Semin PediatrNeurol 20018(4)216Y228
42 ICSD-2 The international classification ofsleep disorders pocket version diagnosticand coding manual 2nd ed WestchesterIL American Academy of Sleep Medicine2005
43 Arand D Bonnet M Hurwitz T et alThe clinical use of the MSLT and MWTSleep 200528(1)123Y144
44 Dauvilliers Y Gosselin A Paquet J et alEffect of age on MSLT results in patientswith narcolepsy-cataplexy Neurology200462(1)46Y50
45 Morgenthaler T Alessi C Friedman Let al Practice parameters for the use ofactigraphy in the assessment of sleep andsleep disorders an update for 2007 Sleep200730(4)519Y529
46 Gamaldo CE Earley CJ Restless legssyndrome a clinical update Chest2006130(5)1596Y1604
49Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited

interfere with sleep latency or REM la-tency should be discontinued 2 weeksbefore testing whenever possible Ascreen may be performed on the day oftesting if there is suspicion that pre-scribed or illicit substances may con-tribute to the patientrsquos sleepiness38
No large multicenter systematicallycollected normative data are availablefor mean sleep latency values on theMSLT38 Nonetheless a mean sleep la-tency of greater than 10 minutes is of-ten considered normal whereas a meansleep latency of 8 to 10 minutes is con-sidered a physiologic gray zone40 Thenormative data for children are classi-fied by Tanner stage of developmentthough the MSLT is typically not per-formed in children aged younger than 6or 7 years because some daytime nap-ping may still be normal in youngchildren41 The second edition of theInternational Classification of SleepDisorders Diagnostic and CodingManual (ICSD-2)42 requires the pres-ence of a mean sleep latency of lessthan 8 minutes and two or moreSOREMPs as part of the diagnosticcriteria for narcolepsy without cata-plexy However the ICSD-2 also notesthat a mean sleep latency of less than 8minutes may occur in up to 30 of thegeneral population Therefore whilethe MSLT is a helpful and widely usedtool it remains an imperfect gold stand-ard in the assessment of daytime sleepi-ness This necessitates that theevaluation of daytime sleepiness notrest on the MSLT results alone butassimilate the clinical history subjectivecomplaints diagnostic study results andother pertinent medical information38
Practice parameters from theAASM state that the MSLT is indicatedfor diagnostic confirmation of sus-pected narcolepsy and may be indi-cated to differentiate idiopathichypersomnia from narcolepsy38 TheMSLT is not indicated for routine
assessment of OSA syndrome or toassess response to treatment of SDBand is not routinely indicated for eval-uation of sleepiness in medical orneurologic disorders (except for narco-lepsy) insomnia or circadian rhythmdisorders
TheMWTprovides an objectivemeas-ure of a patientrsquos ability to remain awakerather than the tendency to fall asleepduring the day The key differencebetween the MWT and the MSLT is thatin the former the patient is asked to tryto stay awake under circumstances con-ducive to sleep rather than to fall asleepThe MWT provides an objective vali-dated assessment of the ability to remainawake for a defined length of time38 Therecommended protocol includes four40-minute trials that begin at 2-hourintervals with the first trial to start 15 to30 hours after the patientrsquos wake-uptime A nocturnal polysomnogram onthe preceding night is not requiredHowever the patient should obtain asufficient amount of sleep during thenight before the MWT Each trial isterminated after 40 minutes if no sleepoccurs or after unequivocal sleep onset(defined as three continuous epochsof stage N1 sleep or one epoch of anyother stage of sleep) has occurred38
One indication for the MWT is to as-sess an individualrsquos ability to remainawake when his or her inability to re-main awake constitutes a public orpersonal safety issue This can becomea pressing issue for individuals em-ployed in the transportation43 con-struction or health care industriesThe MWT may be indicated to assesstreatment response in patients withknown excessive daytime sleepiness
Limited amounts of normative dataare available for the MWT Historicallymultiple testing protocols make syn-thesis of results more challenging TheMWT is used much less often in clinicalpractice compared to the MSLT Patient
KEY POINTS
h The multiple sleeplatency test is the goldstandard for objectiveassessment of daytimesleepiness butinterpretation of theresults must be madewithin the clinicalcontext of the patientrsquoshistory
h In the multiple sleeplatency test the patientis instructed to try tosleep during each naptrial In the maintenanceof wakefulness test thepatient is instructed totry to remain awakeduring the nap trial
h A baseline nocturnalpolysomnogram isrequired before amultiple sleep latencytest and considered butnot required before amaintenance ofwakefulness test
45Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
age may also affect the mean sleep la-tency values on both the MWT and theMSLT43 and may represent evolution ofcircadian rhythm and sleep architec-ture across the lifetime A study of 383patients with narcolepsy with cataplexyexamined the clinical and polysomno-graphic data at the time of diagnosis(age range 5 to 84 years) and found aprogressive decrease in the number ofSOREMPs and a progressive increase inthe mean sleep latency on the MSLT asa function of age44 Given its limita-tions the MWT may thus be used tosupplement the clinical history in theassessment of ability to stay awake butshould not be the sole determinant ofthis parameter
Actigraphy is also used in the clinicalevaluation of patients with sleep disor-ders particularly circadian rhythm sleepdisorders An actigraph is a watchlikedevice that is worn on the wrist for anextended period usually in the range ofweeks The actigraph records move-ment and uses an algorithm to estimatethe amounts of sleep and wake timeduring the recording period Analysissoftware uses movement to estimatewhen sleep and wakefulness haveoccurred Review of the data can pro-vide objective insight into the patientrsquossleep pattern including timing andduration of major sleep disruptionsActigraphy is indicated as part of theevaluation of patients with advancedsleep-phase syndrome delayed sleep-phase syndrome and shift work disor-der and may be indicated in the evalua-tion of jet lag disorder and nonY24-hoursleep-wake syndrome including thatassociated with blindness45 It can alsoserve as a measure of treatment re-sponse in patients with insomnia andcircadian rhythm sleep disorders Forpopulations in which traditional sleepmonitoring may be challenging suchas pediatric or older adult patientsactigraphy may provide valuable infor-
mation about the patientrsquos sleep pat-tern or response to treatment Whenpolysomnography is not availableactigraphy is indicated to estimate totalsleep time in patients with OSA45
OTHER ASSESSMENTMODALITIESLaboratory evaluation and neuroimag-ing with either CT or MRI may beconsidered on an individual basis asindicated by the clinical history Com-plete blood count (CBC) serum chem-istries or measures of thyroid functionmay be obtained if an underlying med-ical disorder is thought to contribute tothe patientrsquos sleep symptoms Forinstance these laboratory studies maybe consideredwhen daytime fatigue is apredominant symptom Serum ironstudies including ferritin level shouldbe checked in patients with restless legssyndrome46 Neuroimaging should beconsidered in patients with antecedenttrauma or for any sleep disorder pa-tient with an abnormal neurologic ex-amination to evaluate for a structuraletiology of the patientrsquos symptoms
APPROACH TO THE PATIENTEvaluation of suspected sleep disordersis best accomplished by a stepwisemultidimensional approach (Case 2-2)A thorough sleep history includes de-tailed description of sleep-related symp-toms nocturnal behaviors the patientrsquossleep schedule level of daytime sleepi-ness and subsequent effects on daytimefunctioning Collateral history from thepatientrsquos bed partner or family is oftennecessary to understand the severity andcontext of the patientrsquos symptoms Sub-jective assessments of sleepiness suchas the Epworth Sleepiness Scale areeasily administered and useful to tracksymptomatic progression or treatmentresponse from one visit to the nextCertain physical examination findingsmay also raise clinical suspicion of
KEY POINTS
h Actigraphy can beuseful in evaluation andtreatment of circadianrhythm sleep disordersand in management ofinsomnia
h Neuroimaging is notroutinely indicated inthe clinical evaluation ofsleep disorders andshould be pursued on acase-by-case basis
46 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
particular sleep disorders For patientsin whom multiple sleep disorders aresuspected systematic use of diagnostictesting allows for accurate identificationof specific diagnoses In a patient withinsomnia and symptoms suggestive ofSDB nocturnal polysomnography shouldbe the first procedure performed Ifthe insomnia persists despite adequatetreatment of SDB further evaluationwith sleep diaries and possibly actigra-
phy may be considered to better char-acterize the patientrsquos sleep patternActigraphy may then again be pursuedto gauge treatment response upon man-agement of the patientrsquos insomnia
The diagnostic modalities availablefor evaluation of sleep disorders arerapidly evolving In-laboratory nocturnalpolysomnography currently remains thegold standard for assessment of SDBHowever the multitude of out-of-center
KEY POINT
h Careful assimilation ofthe clinical history thesleep-specific physicalexamination patientquestionnaires anddiagnostic test resultsleads to the mostaccurate assessment ofpatients with symptomsrelated to sleep oralertness
Case 2-2A 23-year-old woman reported a 4-year history of insomnia Throughoutcollege she was a lsquolsquonight owlrsquorsquo never scheduled classes that started before100 PM and always did well in school During the past 6 months shedeveloped progressive difficulty staying awake in her job as a financialanalyst andwas concerned about how this might affect her job performance
During the week she was in bed by midnight but was unable to fallasleep until 200 AM and awoke with difficulty to an alarm at 600 AMfeeling tired She denied any thought rumination or physical discomfortat bedtime She had tried over-the-counter sleep aids that provided nosymptomatic improvement and worsened morning grogginess Onweekends she slept from 200 AM to 1100 AM and awakened feelinglsquolsquopretty goodrsquorsquo She had nocturia up to once per night and occasionalmorning headaches She had no bed partner but reported gaspingrespirations nocturnal palpitations and snort arousals On about 4 nightsper week she experienced a sensation of needing to move her legswhile trying to fall asleep This sensation was relieved by movement andwas worse at night than during the day Her legs sometimes movedspontaneously at night or while seated quietly for long periods duringthe day She felt sleepy during the afternoon especially while workingat her computer She denied drowsiness while driving She occasionallytook a 30-minute nap on the weekend and found it to be refreshingShe drank one to two cups of coffee every morning and had a 12-oz dietcaffeinated soda at 300 PM Her sleepiness had not caused her to makeany mistakes at work and she denied any mood disturbance
Physical examination was notable for a body mass index of 32 kgm2 neckcircumference of 381 cm (15 in) and modified Mallampati class III oral airwayNasal passages were narrow with turbinate hypertrophy bilaterally andhard palate was high-arched and narrow Nomicrognathia or retrognathia waspresent She had molar occlusion class I bilaterally with no overjet or overbiteThe general cardiac respiratory and neurologic examinations were normal
Comment This case illustrates how discussion of the chief complaint raisessuspicion for multiple sleep disorders The history suggests a circadian rhythmsleep disorder particularly delayed sleep-phase syndrome sleep-disorderedbreathing and restless legs syndrome Diagnostic evaluation should includenocturnal polysomnogramwith consideration toperform testing at the patientrsquospreferred sleep time and serum iron studies Sleep diaries andor actigraphymay be considered for further assessment of the patientrsquos sleep pattern
47Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
testing devices continues to grow andmany may provide useful alternativesthat under appropriate circumstancescould allow more expedient conven-ient and less costly evaluations ofincreased numbers of patients whopreviously had only limited or delayedaccess to sleep services
VIDEO LEGENDSupplemental Digital Content 2-1
Home sleep study Video demonstrates a homesleep study using an unattended type 3 portablemonitoring device The patient is a 56-year-oldman who is experiencing morning headachesand concentration and alertness problems atwork He has a history of mild snoring and ar-terial hypertension His Epworth SleepinessScale score is 18 his neck circumference is19 in he has a Mallampati classification score ofIII and his body mass index is 41 kgm Theapnea-hypopnea index is 84 eventsh Channelsrecorded in this sleep study include arterialoxyhemoglobin saturation heart rate oral-nasalpressure flow snoring inductive plethysmog-raphy for chest efforts and body position
linkslwwcomCONTA15
B 2013 Marcel Hungs MD PhD Used withpermission
REFERENCES1 National Institutes of Health National
Center on Sleep Disorders ResearchSleep disorders research planwwwnhlbinihgovhealthprofsleep201101011NationalSleepDisordersResearch-PlanDHHSPublication11-7820pdf PublishedNovember 2011
2 Dinges DF An overview of sleepiness andaccidents J Sleep Res 19954(S2)4Y14
3 Mills RJ Young CA A medical definitionof fatigue in multiple sclerosis QJM 2008101(1)49Y60
4 Chervin RD Sleepiness fatigue tirednessand lack of energy in obstructive sleepapnea Chest 2000118(2)372Y379
5 Chotinaiwattarakul W OrsquoBrien LM Fan LChervin RD Fatigue tiredness and lack ofenergy improve with treatment for OSAJ Clin Sleep Med 20095(3)222Y227
6 American Academy of Sleep MedicineThe international classification of sleepdisorders diagnostic and coding manual2nd ed Westchester IL American Academyof Sleep Medicine 2005
7 Ebben MR Spielman AJNon-pharmacological treatments forinsomnia J Behav Med 200932(3)244Y254
8 Roth T Insomnia definition prevalenceetiology and consequences J Clin SleepMed 20073(5 suppl)S7YS10
9 Yang CM Spielman AJ Glovinsky PNonpharmacologic strategies in themanagement of insomnia Psychiatr ClinNorth Am 200629(4)895Y919 abstract viii
10 Katz ES DrsquoAmbrosio CM Pediatricobstructive sleep apnea syndrome ClinChest Med 201031(2)221Y234
11 Kohler M Bloch KE Stradling JR The role ofthe nose in the pathogenesis of obstructivesleep apnea Curr Opin Otolaryngol HeadNeck Surg 200917(1)33Y37
12 Kryger MH Atlas of clinical sleep medicinePhiladelphia PA Elsevier 2010
13 Zonato AI Martinho FL Bittencourt LRet al Head and neck physical examinationcomparison between nonapneic andobstructive sleep apnea patientsLaryngoscope 2005115(6)1030Y1034
14 Mallampati SR Gatt SP Gugino LD et alA clinical sign to predict difficult trachealintubation a prospective study Can AnaesthSoc J 198532(4)429Y434
15 Samsoon GL Young JR Difficult trachealintubation a retrospective studyAnaesthesia 198742(5)487Y490
16 Huang HH Lee MS Shih YL et alModified Mallampati classificationas a clinical predictor of peroralesophagogastroduodenoscopy toleranceBMC Gastroenterol 20111112
17 Friedman M Ibrahim H Bass L Clinicalstaging for sleep-disordered breathingOtolaryngol Head Neck Surg 2002127(1)13Y21
18 Cheng RHW Yiu CKY Leung WKOral health in individuals with Downsyndrome In Dey S ed Prenatal diagnosisand screening for down syndromeInTech wwwintechopencombookshowtoreferenceprenatal-diagnosis-and-screening-for-down-syndromeoral-health-in-individuals-with-down-syndromePublished 2011 Accessed August 24 2012
19 Katz I Stradling J Slutsky AS et al Dopatients with obstructive sleep apneahave thick necks Am Rev Respir Dis1990141(5 pt 1)1228Y1231
20 Kushida CA Efron B Guilleminault C Apredictive morphometric model for theobstructive sleep apnea syndrome AnnIntern Med 1997127(8 pt 1)581Y587
48 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
21 Saccucci M Tettamanti L Mummolo S et alScoliosis and dental occlusion a review ofthe literature Scoliosis 2011615
22 Battagel JM Kotecha B Dental side-effectsof mandibular advancement splint wear inpatients who snore Clin Otolaryngol200530(2)149Y156
23 Morcos SS Patel PK The vocabulary ofdentofacial deformities Clin Plast Surg200734(3)589Y599
24 Epstein LJ Kristo D Strollo PJ Jr et alClinical guideline for the evaluationmanagement and long-term care ofobstructive sleep apnea in adults J ClinSleep Med 20095(3)263Y276
25 Johns MW A new method for measuringdaytime sleepiness the Epworth sleepinessscale Sleep 199114(6)540Y545
26 Johns MW Daytime sleepiness snoring andobstructive sleep apnea The EpworthSleepiness Scale Chest 1993103(1)30Y36
27 Chervin RD Aldrich MS The EpworthSleepiness Scale may not reflect objectivemeasures of sleepiness or sleep apneaNeurology 199952(1)125Y131
28 Buysse DJ Reynolds CF 3rd Monk THet al The Pittsburgh Sleep Quality Index anew instrument for psychiatric practice andresearch Psychiatry Res 198928(2)193Y213
29 Chervin RD Hedger K Dillon JE Pituch KJPediatric sleep questionnaire (PSQ) validityand reliability of scales for sleep-disorderedbreathing snoring sleepiness and behavioralproblems Sleep Med 20001(1)21Y32
30 Chung F Yegneswaran B Liao P et al STOPquestionnaire a tool to screen patients forobstructive sleep apnea Anesthesiology2008108(5)812Y821
31 Walters AS LeBrocq C Dhar A et alValidation of the International Restless LegsSyndrome Study Group rating scale forrestless legs syndrome Sleep Med 20034(2)121Y132
32 Bastien CH Vallieres A Morin CMValidation of the Insomnia Severity Indexas an outcome measure for insomniaresearch Sleep Med 20012(4)297Y307
33 YOURSLEEPaasmnetorg from the AmericanAcademy of Sleep Medicine Two weeksleep diary yoursleepaasmnetorgpdfsleepdiarypdf Accessed August 24 2012
34 Kushida CA Littner MR Morgenthaler Tet al Practice parameters for the indicationsfor polysomnography and relatedprocedures an update for 2005 Sleep200528(4)499Y521
35 Iber C Ancoli-Israel S Chesson A et alThe AASM manual for scoring of sleep andassociated events rules terminology andtechnical specifications 1st ed WestchesterIL American Academy of Sleep Medicine2007
36 Collop NA Tracy SL Kapur V et alObstructive sleep apnea devices forout-of-center (OOC) testing technologyevaluation J Clin Sleep Med 20117(5)531Y548
37 Collop NA Anderson WM Boehlecke Bet al Clinical guidelines for the use ofunattended portable monitors in thediagnosis of obstructive sleep apnea in adultpatients Portable Monitoring Task Forceof the American Academy of SleepMedicine J Clin Sleep Med 20073(7)737Y747
38 Littner MR Kushida C Wise M et alStandards of Practice Committee of theAmerican Academy of Sleep MedicinePractice parameters for clinical use of themultiple sleep latency test and themaintenance of wakefulness test Sleep200528(1)113Y121
39 Carskadon MA Dement WC Mitler MMet al Guidelines for the multiple sleeplatency test (MSLT) a standard measure ofsleepiness Sleep 19869(4)519Y524
40 van den Hoed J Kraemer H Guilleminault Cet al Disorders of excessive daytimesomnolence polygraphic and clinical datafor 100 patients Sleep 19814(1)23Y37
41 Hoban TF Chervin RD Assessment ofsleepiness in children Semin PediatrNeurol 20018(4)216Y228
42 ICSD-2 The international classification ofsleep disorders pocket version diagnosticand coding manual 2nd ed WestchesterIL American Academy of Sleep Medicine2005
43 Arand D Bonnet M Hurwitz T et alThe clinical use of the MSLT and MWTSleep 200528(1)123Y144
44 Dauvilliers Y Gosselin A Paquet J et alEffect of age on MSLT results in patientswith narcolepsy-cataplexy Neurology200462(1)46Y50
45 Morgenthaler T Alessi C Friedman Let al Practice parameters for the use ofactigraphy in the assessment of sleep andsleep disorders an update for 2007 Sleep200730(4)519Y529
46 Gamaldo CE Earley CJ Restless legssyndrome a clinical update Chest2006130(5)1596Y1604
49Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited

age may also affect the mean sleep la-tency values on both the MWT and theMSLT43 and may represent evolution ofcircadian rhythm and sleep architec-ture across the lifetime A study of 383patients with narcolepsy with cataplexyexamined the clinical and polysomno-graphic data at the time of diagnosis(age range 5 to 84 years) and found aprogressive decrease in the number ofSOREMPs and a progressive increase inthe mean sleep latency on the MSLT asa function of age44 Given its limita-tions the MWT may thus be used tosupplement the clinical history in theassessment of ability to stay awake butshould not be the sole determinant ofthis parameter
Actigraphy is also used in the clinicalevaluation of patients with sleep disor-ders particularly circadian rhythm sleepdisorders An actigraph is a watchlikedevice that is worn on the wrist for anextended period usually in the range ofweeks The actigraph records move-ment and uses an algorithm to estimatethe amounts of sleep and wake timeduring the recording period Analysissoftware uses movement to estimatewhen sleep and wakefulness haveoccurred Review of the data can pro-vide objective insight into the patientrsquossleep pattern including timing andduration of major sleep disruptionsActigraphy is indicated as part of theevaluation of patients with advancedsleep-phase syndrome delayed sleep-phase syndrome and shift work disor-der and may be indicated in the evalua-tion of jet lag disorder and nonY24-hoursleep-wake syndrome including thatassociated with blindness45 It can alsoserve as a measure of treatment re-sponse in patients with insomnia andcircadian rhythm sleep disorders Forpopulations in which traditional sleepmonitoring may be challenging suchas pediatric or older adult patientsactigraphy may provide valuable infor-
mation about the patientrsquos sleep pat-tern or response to treatment Whenpolysomnography is not availableactigraphy is indicated to estimate totalsleep time in patients with OSA45
OTHER ASSESSMENTMODALITIESLaboratory evaluation and neuroimag-ing with either CT or MRI may beconsidered on an individual basis asindicated by the clinical history Com-plete blood count (CBC) serum chem-istries or measures of thyroid functionmay be obtained if an underlying med-ical disorder is thought to contribute tothe patientrsquos sleep symptoms Forinstance these laboratory studies maybe consideredwhen daytime fatigue is apredominant symptom Serum ironstudies including ferritin level shouldbe checked in patients with restless legssyndrome46 Neuroimaging should beconsidered in patients with antecedenttrauma or for any sleep disorder pa-tient with an abnormal neurologic ex-amination to evaluate for a structuraletiology of the patientrsquos symptoms
APPROACH TO THE PATIENTEvaluation of suspected sleep disordersis best accomplished by a stepwisemultidimensional approach (Case 2-2)A thorough sleep history includes de-tailed description of sleep-related symp-toms nocturnal behaviors the patientrsquossleep schedule level of daytime sleepi-ness and subsequent effects on daytimefunctioning Collateral history from thepatientrsquos bed partner or family is oftennecessary to understand the severity andcontext of the patientrsquos symptoms Sub-jective assessments of sleepiness suchas the Epworth Sleepiness Scale areeasily administered and useful to tracksymptomatic progression or treatmentresponse from one visit to the nextCertain physical examination findingsmay also raise clinical suspicion of
KEY POINTS
h Actigraphy can beuseful in evaluation andtreatment of circadianrhythm sleep disordersand in management ofinsomnia
h Neuroimaging is notroutinely indicated inthe clinical evaluation ofsleep disorders andshould be pursued on acase-by-case basis
46 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
particular sleep disorders For patientsin whom multiple sleep disorders aresuspected systematic use of diagnostictesting allows for accurate identificationof specific diagnoses In a patient withinsomnia and symptoms suggestive ofSDB nocturnal polysomnography shouldbe the first procedure performed Ifthe insomnia persists despite adequatetreatment of SDB further evaluationwith sleep diaries and possibly actigra-
phy may be considered to better char-acterize the patientrsquos sleep patternActigraphy may then again be pursuedto gauge treatment response upon man-agement of the patientrsquos insomnia
The diagnostic modalities availablefor evaluation of sleep disorders arerapidly evolving In-laboratory nocturnalpolysomnography currently remains thegold standard for assessment of SDBHowever the multitude of out-of-center
KEY POINT
h Careful assimilation ofthe clinical history thesleep-specific physicalexamination patientquestionnaires anddiagnostic test resultsleads to the mostaccurate assessment ofpatients with symptomsrelated to sleep oralertness
Case 2-2A 23-year-old woman reported a 4-year history of insomnia Throughoutcollege she was a lsquolsquonight owlrsquorsquo never scheduled classes that started before100 PM and always did well in school During the past 6 months shedeveloped progressive difficulty staying awake in her job as a financialanalyst andwas concerned about how this might affect her job performance
During the week she was in bed by midnight but was unable to fallasleep until 200 AM and awoke with difficulty to an alarm at 600 AMfeeling tired She denied any thought rumination or physical discomfortat bedtime She had tried over-the-counter sleep aids that provided nosymptomatic improvement and worsened morning grogginess Onweekends she slept from 200 AM to 1100 AM and awakened feelinglsquolsquopretty goodrsquorsquo She had nocturia up to once per night and occasionalmorning headaches She had no bed partner but reported gaspingrespirations nocturnal palpitations and snort arousals On about 4 nightsper week she experienced a sensation of needing to move her legswhile trying to fall asleep This sensation was relieved by movement andwas worse at night than during the day Her legs sometimes movedspontaneously at night or while seated quietly for long periods duringthe day She felt sleepy during the afternoon especially while workingat her computer She denied drowsiness while driving She occasionallytook a 30-minute nap on the weekend and found it to be refreshingShe drank one to two cups of coffee every morning and had a 12-oz dietcaffeinated soda at 300 PM Her sleepiness had not caused her to makeany mistakes at work and she denied any mood disturbance
Physical examination was notable for a body mass index of 32 kgm2 neckcircumference of 381 cm (15 in) and modified Mallampati class III oral airwayNasal passages were narrow with turbinate hypertrophy bilaterally andhard palate was high-arched and narrow Nomicrognathia or retrognathia waspresent She had molar occlusion class I bilaterally with no overjet or overbiteThe general cardiac respiratory and neurologic examinations were normal
Comment This case illustrates how discussion of the chief complaint raisessuspicion for multiple sleep disorders The history suggests a circadian rhythmsleep disorder particularly delayed sleep-phase syndrome sleep-disorderedbreathing and restless legs syndrome Diagnostic evaluation should includenocturnal polysomnogramwith consideration toperform testing at the patientrsquospreferred sleep time and serum iron studies Sleep diaries andor actigraphymay be considered for further assessment of the patientrsquos sleep pattern
47Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
testing devices continues to grow andmany may provide useful alternativesthat under appropriate circumstancescould allow more expedient conven-ient and less costly evaluations ofincreased numbers of patients whopreviously had only limited or delayedaccess to sleep services
VIDEO LEGENDSupplemental Digital Content 2-1
Home sleep study Video demonstrates a homesleep study using an unattended type 3 portablemonitoring device The patient is a 56-year-oldman who is experiencing morning headachesand concentration and alertness problems atwork He has a history of mild snoring and ar-terial hypertension His Epworth SleepinessScale score is 18 his neck circumference is19 in he has a Mallampati classification score ofIII and his body mass index is 41 kgm Theapnea-hypopnea index is 84 eventsh Channelsrecorded in this sleep study include arterialoxyhemoglobin saturation heart rate oral-nasalpressure flow snoring inductive plethysmog-raphy for chest efforts and body position
linkslwwcomCONTA15
B 2013 Marcel Hungs MD PhD Used withpermission
REFERENCES1 National Institutes of Health National
Center on Sleep Disorders ResearchSleep disorders research planwwwnhlbinihgovhealthprofsleep201101011NationalSleepDisordersResearch-PlanDHHSPublication11-7820pdf PublishedNovember 2011
2 Dinges DF An overview of sleepiness andaccidents J Sleep Res 19954(S2)4Y14
3 Mills RJ Young CA A medical definitionof fatigue in multiple sclerosis QJM 2008101(1)49Y60
4 Chervin RD Sleepiness fatigue tirednessand lack of energy in obstructive sleepapnea Chest 2000118(2)372Y379
5 Chotinaiwattarakul W OrsquoBrien LM Fan LChervin RD Fatigue tiredness and lack ofenergy improve with treatment for OSAJ Clin Sleep Med 20095(3)222Y227
6 American Academy of Sleep MedicineThe international classification of sleepdisorders diagnostic and coding manual2nd ed Westchester IL American Academyof Sleep Medicine 2005
7 Ebben MR Spielman AJNon-pharmacological treatments forinsomnia J Behav Med 200932(3)244Y254
8 Roth T Insomnia definition prevalenceetiology and consequences J Clin SleepMed 20073(5 suppl)S7YS10
9 Yang CM Spielman AJ Glovinsky PNonpharmacologic strategies in themanagement of insomnia Psychiatr ClinNorth Am 200629(4)895Y919 abstract viii
10 Katz ES DrsquoAmbrosio CM Pediatricobstructive sleep apnea syndrome ClinChest Med 201031(2)221Y234
11 Kohler M Bloch KE Stradling JR The role ofthe nose in the pathogenesis of obstructivesleep apnea Curr Opin Otolaryngol HeadNeck Surg 200917(1)33Y37
12 Kryger MH Atlas of clinical sleep medicinePhiladelphia PA Elsevier 2010
13 Zonato AI Martinho FL Bittencourt LRet al Head and neck physical examinationcomparison between nonapneic andobstructive sleep apnea patientsLaryngoscope 2005115(6)1030Y1034
14 Mallampati SR Gatt SP Gugino LD et alA clinical sign to predict difficult trachealintubation a prospective study Can AnaesthSoc J 198532(4)429Y434
15 Samsoon GL Young JR Difficult trachealintubation a retrospective studyAnaesthesia 198742(5)487Y490
16 Huang HH Lee MS Shih YL et alModified Mallampati classificationas a clinical predictor of peroralesophagogastroduodenoscopy toleranceBMC Gastroenterol 20111112
17 Friedman M Ibrahim H Bass L Clinicalstaging for sleep-disordered breathingOtolaryngol Head Neck Surg 2002127(1)13Y21
18 Cheng RHW Yiu CKY Leung WKOral health in individuals with Downsyndrome In Dey S ed Prenatal diagnosisand screening for down syndromeInTech wwwintechopencombookshowtoreferenceprenatal-diagnosis-and-screening-for-down-syndromeoral-health-in-individuals-with-down-syndromePublished 2011 Accessed August 24 2012
19 Katz I Stradling J Slutsky AS et al Dopatients with obstructive sleep apneahave thick necks Am Rev Respir Dis1990141(5 pt 1)1228Y1231
20 Kushida CA Efron B Guilleminault C Apredictive morphometric model for theobstructive sleep apnea syndrome AnnIntern Med 1997127(8 pt 1)581Y587
48 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
21 Saccucci M Tettamanti L Mummolo S et alScoliosis and dental occlusion a review ofthe literature Scoliosis 2011615
22 Battagel JM Kotecha B Dental side-effectsof mandibular advancement splint wear inpatients who snore Clin Otolaryngol200530(2)149Y156
23 Morcos SS Patel PK The vocabulary ofdentofacial deformities Clin Plast Surg200734(3)589Y599
24 Epstein LJ Kristo D Strollo PJ Jr et alClinical guideline for the evaluationmanagement and long-term care ofobstructive sleep apnea in adults J ClinSleep Med 20095(3)263Y276
25 Johns MW A new method for measuringdaytime sleepiness the Epworth sleepinessscale Sleep 199114(6)540Y545
26 Johns MW Daytime sleepiness snoring andobstructive sleep apnea The EpworthSleepiness Scale Chest 1993103(1)30Y36
27 Chervin RD Aldrich MS The EpworthSleepiness Scale may not reflect objectivemeasures of sleepiness or sleep apneaNeurology 199952(1)125Y131
28 Buysse DJ Reynolds CF 3rd Monk THet al The Pittsburgh Sleep Quality Index anew instrument for psychiatric practice andresearch Psychiatry Res 198928(2)193Y213
29 Chervin RD Hedger K Dillon JE Pituch KJPediatric sleep questionnaire (PSQ) validityand reliability of scales for sleep-disorderedbreathing snoring sleepiness and behavioralproblems Sleep Med 20001(1)21Y32
30 Chung F Yegneswaran B Liao P et al STOPquestionnaire a tool to screen patients forobstructive sleep apnea Anesthesiology2008108(5)812Y821
31 Walters AS LeBrocq C Dhar A et alValidation of the International Restless LegsSyndrome Study Group rating scale forrestless legs syndrome Sleep Med 20034(2)121Y132
32 Bastien CH Vallieres A Morin CMValidation of the Insomnia Severity Indexas an outcome measure for insomniaresearch Sleep Med 20012(4)297Y307
33 YOURSLEEPaasmnetorg from the AmericanAcademy of Sleep Medicine Two weeksleep diary yoursleepaasmnetorgpdfsleepdiarypdf Accessed August 24 2012
34 Kushida CA Littner MR Morgenthaler Tet al Practice parameters for the indicationsfor polysomnography and relatedprocedures an update for 2005 Sleep200528(4)499Y521
35 Iber C Ancoli-Israel S Chesson A et alThe AASM manual for scoring of sleep andassociated events rules terminology andtechnical specifications 1st ed WestchesterIL American Academy of Sleep Medicine2007
36 Collop NA Tracy SL Kapur V et alObstructive sleep apnea devices forout-of-center (OOC) testing technologyevaluation J Clin Sleep Med 20117(5)531Y548
37 Collop NA Anderson WM Boehlecke Bet al Clinical guidelines for the use ofunattended portable monitors in thediagnosis of obstructive sleep apnea in adultpatients Portable Monitoring Task Forceof the American Academy of SleepMedicine J Clin Sleep Med 20073(7)737Y747
38 Littner MR Kushida C Wise M et alStandards of Practice Committee of theAmerican Academy of Sleep MedicinePractice parameters for clinical use of themultiple sleep latency test and themaintenance of wakefulness test Sleep200528(1)113Y121
39 Carskadon MA Dement WC Mitler MMet al Guidelines for the multiple sleeplatency test (MSLT) a standard measure ofsleepiness Sleep 19869(4)519Y524
40 van den Hoed J Kraemer H Guilleminault Cet al Disorders of excessive daytimesomnolence polygraphic and clinical datafor 100 patients Sleep 19814(1)23Y37
41 Hoban TF Chervin RD Assessment ofsleepiness in children Semin PediatrNeurol 20018(4)216Y228
42 ICSD-2 The international classification ofsleep disorders pocket version diagnosticand coding manual 2nd ed WestchesterIL American Academy of Sleep Medicine2005
43 Arand D Bonnet M Hurwitz T et alThe clinical use of the MSLT and MWTSleep 200528(1)123Y144
44 Dauvilliers Y Gosselin A Paquet J et alEffect of age on MSLT results in patientswith narcolepsy-cataplexy Neurology200462(1)46Y50
45 Morgenthaler T Alessi C Friedman Let al Practice parameters for the use ofactigraphy in the assessment of sleep andsleep disorders an update for 2007 Sleep200730(4)519Y529
46 Gamaldo CE Earley CJ Restless legssyndrome a clinical update Chest2006130(5)1596Y1604
49Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited

particular sleep disorders For patientsin whom multiple sleep disorders aresuspected systematic use of diagnostictesting allows for accurate identificationof specific diagnoses In a patient withinsomnia and symptoms suggestive ofSDB nocturnal polysomnography shouldbe the first procedure performed Ifthe insomnia persists despite adequatetreatment of SDB further evaluationwith sleep diaries and possibly actigra-
phy may be considered to better char-acterize the patientrsquos sleep patternActigraphy may then again be pursuedto gauge treatment response upon man-agement of the patientrsquos insomnia
The diagnostic modalities availablefor evaluation of sleep disorders arerapidly evolving In-laboratory nocturnalpolysomnography currently remains thegold standard for assessment of SDBHowever the multitude of out-of-center
KEY POINT
h Careful assimilation ofthe clinical history thesleep-specific physicalexamination patientquestionnaires anddiagnostic test resultsleads to the mostaccurate assessment ofpatients with symptomsrelated to sleep oralertness
Case 2-2A 23-year-old woman reported a 4-year history of insomnia Throughoutcollege she was a lsquolsquonight owlrsquorsquo never scheduled classes that started before100 PM and always did well in school During the past 6 months shedeveloped progressive difficulty staying awake in her job as a financialanalyst andwas concerned about how this might affect her job performance
During the week she was in bed by midnight but was unable to fallasleep until 200 AM and awoke with difficulty to an alarm at 600 AMfeeling tired She denied any thought rumination or physical discomfortat bedtime She had tried over-the-counter sleep aids that provided nosymptomatic improvement and worsened morning grogginess Onweekends she slept from 200 AM to 1100 AM and awakened feelinglsquolsquopretty goodrsquorsquo She had nocturia up to once per night and occasionalmorning headaches She had no bed partner but reported gaspingrespirations nocturnal palpitations and snort arousals On about 4 nightsper week she experienced a sensation of needing to move her legswhile trying to fall asleep This sensation was relieved by movement andwas worse at night than during the day Her legs sometimes movedspontaneously at night or while seated quietly for long periods duringthe day She felt sleepy during the afternoon especially while workingat her computer She denied drowsiness while driving She occasionallytook a 30-minute nap on the weekend and found it to be refreshingShe drank one to two cups of coffee every morning and had a 12-oz dietcaffeinated soda at 300 PM Her sleepiness had not caused her to makeany mistakes at work and she denied any mood disturbance
Physical examination was notable for a body mass index of 32 kgm2 neckcircumference of 381 cm (15 in) and modified Mallampati class III oral airwayNasal passages were narrow with turbinate hypertrophy bilaterally andhard palate was high-arched and narrow Nomicrognathia or retrognathia waspresent She had molar occlusion class I bilaterally with no overjet or overbiteThe general cardiac respiratory and neurologic examinations were normal
Comment This case illustrates how discussion of the chief complaint raisessuspicion for multiple sleep disorders The history suggests a circadian rhythmsleep disorder particularly delayed sleep-phase syndrome sleep-disorderedbreathing and restless legs syndrome Diagnostic evaluation should includenocturnal polysomnogramwith consideration toperform testing at the patientrsquospreferred sleep time and serum iron studies Sleep diaries andor actigraphymay be considered for further assessment of the patientrsquos sleep pattern
47Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
testing devices continues to grow andmany may provide useful alternativesthat under appropriate circumstancescould allow more expedient conven-ient and less costly evaluations ofincreased numbers of patients whopreviously had only limited or delayedaccess to sleep services
VIDEO LEGENDSupplemental Digital Content 2-1
Home sleep study Video demonstrates a homesleep study using an unattended type 3 portablemonitoring device The patient is a 56-year-oldman who is experiencing morning headachesand concentration and alertness problems atwork He has a history of mild snoring and ar-terial hypertension His Epworth SleepinessScale score is 18 his neck circumference is19 in he has a Mallampati classification score ofIII and his body mass index is 41 kgm Theapnea-hypopnea index is 84 eventsh Channelsrecorded in this sleep study include arterialoxyhemoglobin saturation heart rate oral-nasalpressure flow snoring inductive plethysmog-raphy for chest efforts and body position
linkslwwcomCONTA15
B 2013 Marcel Hungs MD PhD Used withpermission
REFERENCES1 National Institutes of Health National
Center on Sleep Disorders ResearchSleep disorders research planwwwnhlbinihgovhealthprofsleep201101011NationalSleepDisordersResearch-PlanDHHSPublication11-7820pdf PublishedNovember 2011
2 Dinges DF An overview of sleepiness andaccidents J Sleep Res 19954(S2)4Y14
3 Mills RJ Young CA A medical definitionof fatigue in multiple sclerosis QJM 2008101(1)49Y60
4 Chervin RD Sleepiness fatigue tirednessand lack of energy in obstructive sleepapnea Chest 2000118(2)372Y379
5 Chotinaiwattarakul W OrsquoBrien LM Fan LChervin RD Fatigue tiredness and lack ofenergy improve with treatment for OSAJ Clin Sleep Med 20095(3)222Y227
6 American Academy of Sleep MedicineThe international classification of sleepdisorders diagnostic and coding manual2nd ed Westchester IL American Academyof Sleep Medicine 2005
7 Ebben MR Spielman AJNon-pharmacological treatments forinsomnia J Behav Med 200932(3)244Y254
8 Roth T Insomnia definition prevalenceetiology and consequences J Clin SleepMed 20073(5 suppl)S7YS10
9 Yang CM Spielman AJ Glovinsky PNonpharmacologic strategies in themanagement of insomnia Psychiatr ClinNorth Am 200629(4)895Y919 abstract viii
10 Katz ES DrsquoAmbrosio CM Pediatricobstructive sleep apnea syndrome ClinChest Med 201031(2)221Y234
11 Kohler M Bloch KE Stradling JR The role ofthe nose in the pathogenesis of obstructivesleep apnea Curr Opin Otolaryngol HeadNeck Surg 200917(1)33Y37
12 Kryger MH Atlas of clinical sleep medicinePhiladelphia PA Elsevier 2010
13 Zonato AI Martinho FL Bittencourt LRet al Head and neck physical examinationcomparison between nonapneic andobstructive sleep apnea patientsLaryngoscope 2005115(6)1030Y1034
14 Mallampati SR Gatt SP Gugino LD et alA clinical sign to predict difficult trachealintubation a prospective study Can AnaesthSoc J 198532(4)429Y434
15 Samsoon GL Young JR Difficult trachealintubation a retrospective studyAnaesthesia 198742(5)487Y490
16 Huang HH Lee MS Shih YL et alModified Mallampati classificationas a clinical predictor of peroralesophagogastroduodenoscopy toleranceBMC Gastroenterol 20111112
17 Friedman M Ibrahim H Bass L Clinicalstaging for sleep-disordered breathingOtolaryngol Head Neck Surg 2002127(1)13Y21
18 Cheng RHW Yiu CKY Leung WKOral health in individuals with Downsyndrome In Dey S ed Prenatal diagnosisand screening for down syndromeInTech wwwintechopencombookshowtoreferenceprenatal-diagnosis-and-screening-for-down-syndromeoral-health-in-individuals-with-down-syndromePublished 2011 Accessed August 24 2012
19 Katz I Stradling J Slutsky AS et al Dopatients with obstructive sleep apneahave thick necks Am Rev Respir Dis1990141(5 pt 1)1228Y1231
20 Kushida CA Efron B Guilleminault C Apredictive morphometric model for theobstructive sleep apnea syndrome AnnIntern Med 1997127(8 pt 1)581Y587
48 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
21 Saccucci M Tettamanti L Mummolo S et alScoliosis and dental occlusion a review ofthe literature Scoliosis 2011615
22 Battagel JM Kotecha B Dental side-effectsof mandibular advancement splint wear inpatients who snore Clin Otolaryngol200530(2)149Y156
23 Morcos SS Patel PK The vocabulary ofdentofacial deformities Clin Plast Surg200734(3)589Y599
24 Epstein LJ Kristo D Strollo PJ Jr et alClinical guideline for the evaluationmanagement and long-term care ofobstructive sleep apnea in adults J ClinSleep Med 20095(3)263Y276
25 Johns MW A new method for measuringdaytime sleepiness the Epworth sleepinessscale Sleep 199114(6)540Y545
26 Johns MW Daytime sleepiness snoring andobstructive sleep apnea The EpworthSleepiness Scale Chest 1993103(1)30Y36
27 Chervin RD Aldrich MS The EpworthSleepiness Scale may not reflect objectivemeasures of sleepiness or sleep apneaNeurology 199952(1)125Y131
28 Buysse DJ Reynolds CF 3rd Monk THet al The Pittsburgh Sleep Quality Index anew instrument for psychiatric practice andresearch Psychiatry Res 198928(2)193Y213
29 Chervin RD Hedger K Dillon JE Pituch KJPediatric sleep questionnaire (PSQ) validityand reliability of scales for sleep-disorderedbreathing snoring sleepiness and behavioralproblems Sleep Med 20001(1)21Y32
30 Chung F Yegneswaran B Liao P et al STOPquestionnaire a tool to screen patients forobstructive sleep apnea Anesthesiology2008108(5)812Y821
31 Walters AS LeBrocq C Dhar A et alValidation of the International Restless LegsSyndrome Study Group rating scale forrestless legs syndrome Sleep Med 20034(2)121Y132
32 Bastien CH Vallieres A Morin CMValidation of the Insomnia Severity Indexas an outcome measure for insomniaresearch Sleep Med 20012(4)297Y307
33 YOURSLEEPaasmnetorg from the AmericanAcademy of Sleep Medicine Two weeksleep diary yoursleepaasmnetorgpdfsleepdiarypdf Accessed August 24 2012
34 Kushida CA Littner MR Morgenthaler Tet al Practice parameters for the indicationsfor polysomnography and relatedprocedures an update for 2005 Sleep200528(4)499Y521
35 Iber C Ancoli-Israel S Chesson A et alThe AASM manual for scoring of sleep andassociated events rules terminology andtechnical specifications 1st ed WestchesterIL American Academy of Sleep Medicine2007
36 Collop NA Tracy SL Kapur V et alObstructive sleep apnea devices forout-of-center (OOC) testing technologyevaluation J Clin Sleep Med 20117(5)531Y548
37 Collop NA Anderson WM Boehlecke Bet al Clinical guidelines for the use ofunattended portable monitors in thediagnosis of obstructive sleep apnea in adultpatients Portable Monitoring Task Forceof the American Academy of SleepMedicine J Clin Sleep Med 20073(7)737Y747
38 Littner MR Kushida C Wise M et alStandards of Practice Committee of theAmerican Academy of Sleep MedicinePractice parameters for clinical use of themultiple sleep latency test and themaintenance of wakefulness test Sleep200528(1)113Y121
39 Carskadon MA Dement WC Mitler MMet al Guidelines for the multiple sleeplatency test (MSLT) a standard measure ofsleepiness Sleep 19869(4)519Y524
40 van den Hoed J Kraemer H Guilleminault Cet al Disorders of excessive daytimesomnolence polygraphic and clinical datafor 100 patients Sleep 19814(1)23Y37
41 Hoban TF Chervin RD Assessment ofsleepiness in children Semin PediatrNeurol 20018(4)216Y228
42 ICSD-2 The international classification ofsleep disorders pocket version diagnosticand coding manual 2nd ed WestchesterIL American Academy of Sleep Medicine2005
43 Arand D Bonnet M Hurwitz T et alThe clinical use of the MSLT and MWTSleep 200528(1)123Y144
44 Dauvilliers Y Gosselin A Paquet J et alEffect of age on MSLT results in patientswith narcolepsy-cataplexy Neurology200462(1)46Y50
45 Morgenthaler T Alessi C Friedman Let al Practice parameters for the use ofactigraphy in the assessment of sleep andsleep disorders an update for 2007 Sleep200730(4)519Y529
46 Gamaldo CE Earley CJ Restless legssyndrome a clinical update Chest2006130(5)1596Y1604
49Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited

testing devices continues to grow andmany may provide useful alternativesthat under appropriate circumstancescould allow more expedient conven-ient and less costly evaluations ofincreased numbers of patients whopreviously had only limited or delayedaccess to sleep services
VIDEO LEGENDSupplemental Digital Content 2-1
Home sleep study Video demonstrates a homesleep study using an unattended type 3 portablemonitoring device The patient is a 56-year-oldman who is experiencing morning headachesand concentration and alertness problems atwork He has a history of mild snoring and ar-terial hypertension His Epworth SleepinessScale score is 18 his neck circumference is19 in he has a Mallampati classification score ofIII and his body mass index is 41 kgm Theapnea-hypopnea index is 84 eventsh Channelsrecorded in this sleep study include arterialoxyhemoglobin saturation heart rate oral-nasalpressure flow snoring inductive plethysmog-raphy for chest efforts and body position
linkslwwcomCONTA15
B 2013 Marcel Hungs MD PhD Used withpermission
REFERENCES1 National Institutes of Health National
Center on Sleep Disorders ResearchSleep disorders research planwwwnhlbinihgovhealthprofsleep201101011NationalSleepDisordersResearch-PlanDHHSPublication11-7820pdf PublishedNovember 2011
2 Dinges DF An overview of sleepiness andaccidents J Sleep Res 19954(S2)4Y14
3 Mills RJ Young CA A medical definitionof fatigue in multiple sclerosis QJM 2008101(1)49Y60
4 Chervin RD Sleepiness fatigue tirednessand lack of energy in obstructive sleepapnea Chest 2000118(2)372Y379
5 Chotinaiwattarakul W OrsquoBrien LM Fan LChervin RD Fatigue tiredness and lack ofenergy improve with treatment for OSAJ Clin Sleep Med 20095(3)222Y227
6 American Academy of Sleep MedicineThe international classification of sleepdisorders diagnostic and coding manual2nd ed Westchester IL American Academyof Sleep Medicine 2005
7 Ebben MR Spielman AJNon-pharmacological treatments forinsomnia J Behav Med 200932(3)244Y254
8 Roth T Insomnia definition prevalenceetiology and consequences J Clin SleepMed 20073(5 suppl)S7YS10
9 Yang CM Spielman AJ Glovinsky PNonpharmacologic strategies in themanagement of insomnia Psychiatr ClinNorth Am 200629(4)895Y919 abstract viii
10 Katz ES DrsquoAmbrosio CM Pediatricobstructive sleep apnea syndrome ClinChest Med 201031(2)221Y234
11 Kohler M Bloch KE Stradling JR The role ofthe nose in the pathogenesis of obstructivesleep apnea Curr Opin Otolaryngol HeadNeck Surg 200917(1)33Y37
12 Kryger MH Atlas of clinical sleep medicinePhiladelphia PA Elsevier 2010
13 Zonato AI Martinho FL Bittencourt LRet al Head and neck physical examinationcomparison between nonapneic andobstructive sleep apnea patientsLaryngoscope 2005115(6)1030Y1034
14 Mallampati SR Gatt SP Gugino LD et alA clinical sign to predict difficult trachealintubation a prospective study Can AnaesthSoc J 198532(4)429Y434
15 Samsoon GL Young JR Difficult trachealintubation a retrospective studyAnaesthesia 198742(5)487Y490
16 Huang HH Lee MS Shih YL et alModified Mallampati classificationas a clinical predictor of peroralesophagogastroduodenoscopy toleranceBMC Gastroenterol 20111112
17 Friedman M Ibrahim H Bass L Clinicalstaging for sleep-disordered breathingOtolaryngol Head Neck Surg 2002127(1)13Y21
18 Cheng RHW Yiu CKY Leung WKOral health in individuals with Downsyndrome In Dey S ed Prenatal diagnosisand screening for down syndromeInTech wwwintechopencombookshowtoreferenceprenatal-diagnosis-and-screening-for-down-syndromeoral-health-in-individuals-with-down-syndromePublished 2011 Accessed August 24 2012
19 Katz I Stradling J Slutsky AS et al Dopatients with obstructive sleep apneahave thick necks Am Rev Respir Dis1990141(5 pt 1)1228Y1231
20 Kushida CA Efron B Guilleminault C Apredictive morphometric model for theobstructive sleep apnea syndrome AnnIntern Med 1997127(8 pt 1)581Y587
48 wwwaancomcontinuum February 2013
Approach and Evaluation
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
21 Saccucci M Tettamanti L Mummolo S et alScoliosis and dental occlusion a review ofthe literature Scoliosis 2011615
22 Battagel JM Kotecha B Dental side-effectsof mandibular advancement splint wear inpatients who snore Clin Otolaryngol200530(2)149Y156
23 Morcos SS Patel PK The vocabulary ofdentofacial deformities Clin Plast Surg200734(3)589Y599
24 Epstein LJ Kristo D Strollo PJ Jr et alClinical guideline for the evaluationmanagement and long-term care ofobstructive sleep apnea in adults J ClinSleep Med 20095(3)263Y276
25 Johns MW A new method for measuringdaytime sleepiness the Epworth sleepinessscale Sleep 199114(6)540Y545
26 Johns MW Daytime sleepiness snoring andobstructive sleep apnea The EpworthSleepiness Scale Chest 1993103(1)30Y36
27 Chervin RD Aldrich MS The EpworthSleepiness Scale may not reflect objectivemeasures of sleepiness or sleep apneaNeurology 199952(1)125Y131
28 Buysse DJ Reynolds CF 3rd Monk THet al The Pittsburgh Sleep Quality Index anew instrument for psychiatric practice andresearch Psychiatry Res 198928(2)193Y213
29 Chervin RD Hedger K Dillon JE Pituch KJPediatric sleep questionnaire (PSQ) validityand reliability of scales for sleep-disorderedbreathing snoring sleepiness and behavioralproblems Sleep Med 20001(1)21Y32
30 Chung F Yegneswaran B Liao P et al STOPquestionnaire a tool to screen patients forobstructive sleep apnea Anesthesiology2008108(5)812Y821
31 Walters AS LeBrocq C Dhar A et alValidation of the International Restless LegsSyndrome Study Group rating scale forrestless legs syndrome Sleep Med 20034(2)121Y132
32 Bastien CH Vallieres A Morin CMValidation of the Insomnia Severity Indexas an outcome measure for insomniaresearch Sleep Med 20012(4)297Y307
33 YOURSLEEPaasmnetorg from the AmericanAcademy of Sleep Medicine Two weeksleep diary yoursleepaasmnetorgpdfsleepdiarypdf Accessed August 24 2012
34 Kushida CA Littner MR Morgenthaler Tet al Practice parameters for the indicationsfor polysomnography and relatedprocedures an update for 2005 Sleep200528(4)499Y521
35 Iber C Ancoli-Israel S Chesson A et alThe AASM manual for scoring of sleep andassociated events rules terminology andtechnical specifications 1st ed WestchesterIL American Academy of Sleep Medicine2007
36 Collop NA Tracy SL Kapur V et alObstructive sleep apnea devices forout-of-center (OOC) testing technologyevaluation J Clin Sleep Med 20117(5)531Y548
37 Collop NA Anderson WM Boehlecke Bet al Clinical guidelines for the use ofunattended portable monitors in thediagnosis of obstructive sleep apnea in adultpatients Portable Monitoring Task Forceof the American Academy of SleepMedicine J Clin Sleep Med 20073(7)737Y747
38 Littner MR Kushida C Wise M et alStandards of Practice Committee of theAmerican Academy of Sleep MedicinePractice parameters for clinical use of themultiple sleep latency test and themaintenance of wakefulness test Sleep200528(1)113Y121
39 Carskadon MA Dement WC Mitler MMet al Guidelines for the multiple sleeplatency test (MSLT) a standard measure ofsleepiness Sleep 19869(4)519Y524
40 van den Hoed J Kraemer H Guilleminault Cet al Disorders of excessive daytimesomnolence polygraphic and clinical datafor 100 patients Sleep 19814(1)23Y37
41 Hoban TF Chervin RD Assessment ofsleepiness in children Semin PediatrNeurol 20018(4)216Y228
42 ICSD-2 The international classification ofsleep disorders pocket version diagnosticand coding manual 2nd ed WestchesterIL American Academy of Sleep Medicine2005
43 Arand D Bonnet M Hurwitz T et alThe clinical use of the MSLT and MWTSleep 200528(1)123Y144
44 Dauvilliers Y Gosselin A Paquet J et alEffect of age on MSLT results in patientswith narcolepsy-cataplexy Neurology200462(1)46Y50
45 Morgenthaler T Alessi C Friedman Let al Practice parameters for the use ofactigraphy in the assessment of sleep andsleep disorders an update for 2007 Sleep200730(4)519Y529
46 Gamaldo CE Earley CJ Restless legssyndrome a clinical update Chest2006130(5)1596Y1604
49Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited
21 Saccucci M Tettamanti L Mummolo S et alScoliosis and dental occlusion a review ofthe literature Scoliosis 2011615
22 Battagel JM Kotecha B Dental side-effectsof mandibular advancement splint wear inpatients who snore Clin Otolaryngol200530(2)149Y156
23 Morcos SS Patel PK The vocabulary ofdentofacial deformities Clin Plast Surg200734(3)589Y599
24 Epstein LJ Kristo D Strollo PJ Jr et alClinical guideline for the evaluationmanagement and long-term care ofobstructive sleep apnea in adults J ClinSleep Med 20095(3)263Y276
25 Johns MW A new method for measuringdaytime sleepiness the Epworth sleepinessscale Sleep 199114(6)540Y545
26 Johns MW Daytime sleepiness snoring andobstructive sleep apnea The EpworthSleepiness Scale Chest 1993103(1)30Y36
27 Chervin RD Aldrich MS The EpworthSleepiness Scale may not reflect objectivemeasures of sleepiness or sleep apneaNeurology 199952(1)125Y131
28 Buysse DJ Reynolds CF 3rd Monk THet al The Pittsburgh Sleep Quality Index anew instrument for psychiatric practice andresearch Psychiatry Res 198928(2)193Y213
29 Chervin RD Hedger K Dillon JE Pituch KJPediatric sleep questionnaire (PSQ) validityand reliability of scales for sleep-disorderedbreathing snoring sleepiness and behavioralproblems Sleep Med 20001(1)21Y32
30 Chung F Yegneswaran B Liao P et al STOPquestionnaire a tool to screen patients forobstructive sleep apnea Anesthesiology2008108(5)812Y821
31 Walters AS LeBrocq C Dhar A et alValidation of the International Restless LegsSyndrome Study Group rating scale forrestless legs syndrome Sleep Med 20034(2)121Y132
32 Bastien CH Vallieres A Morin CMValidation of the Insomnia Severity Indexas an outcome measure for insomniaresearch Sleep Med 20012(4)297Y307
33 YOURSLEEPaasmnetorg from the AmericanAcademy of Sleep Medicine Two weeksleep diary yoursleepaasmnetorgpdfsleepdiarypdf Accessed August 24 2012
34 Kushida CA Littner MR Morgenthaler Tet al Practice parameters for the indicationsfor polysomnography and relatedprocedures an update for 2005 Sleep200528(4)499Y521
35 Iber C Ancoli-Israel S Chesson A et alThe AASM manual for scoring of sleep andassociated events rules terminology andtechnical specifications 1st ed WestchesterIL American Academy of Sleep Medicine2007
36 Collop NA Tracy SL Kapur V et alObstructive sleep apnea devices forout-of-center (OOC) testing technologyevaluation J Clin Sleep Med 20117(5)531Y548
37 Collop NA Anderson WM Boehlecke Bet al Clinical guidelines for the use ofunattended portable monitors in thediagnosis of obstructive sleep apnea in adultpatients Portable Monitoring Task Forceof the American Academy of SleepMedicine J Clin Sleep Med 20073(7)737Y747
38 Littner MR Kushida C Wise M et alStandards of Practice Committee of theAmerican Academy of Sleep MedicinePractice parameters for clinical use of themultiple sleep latency test and themaintenance of wakefulness test Sleep200528(1)113Y121
39 Carskadon MA Dement WC Mitler MMet al Guidelines for the multiple sleeplatency test (MSLT) a standard measure ofsleepiness Sleep 19869(4)519Y524
40 van den Hoed J Kraemer H Guilleminault Cet al Disorders of excessive daytimesomnolence polygraphic and clinical datafor 100 patients Sleep 19814(1)23Y37
41 Hoban TF Chervin RD Assessment ofsleepiness in children Semin PediatrNeurol 20018(4)216Y228
42 ICSD-2 The international classification ofsleep disorders pocket version diagnosticand coding manual 2nd ed WestchesterIL American Academy of Sleep Medicine2005
43 Arand D Bonnet M Hurwitz T et alThe clinical use of the MSLT and MWTSleep 200528(1)123Y144
44 Dauvilliers Y Gosselin A Paquet J et alEffect of age on MSLT results in patientswith narcolepsy-cataplexy Neurology200462(1)46Y50
45 Morgenthaler T Alessi C Friedman Let al Practice parameters for the use ofactigraphy in the assessment of sleep andsleep disorders an update for 2007 Sleep200730(4)519Y529
46 Gamaldo CE Earley CJ Restless legssyndrome a clinical update Chest2006130(5)1596Y1604
49Continuum (Minneap Minn) 201319(1)32ndash49 wwwaancomcontinuum
Copyright American Academy of Neurology Unauthorized reproduction of this article is prohibited


















