Application Type Completion Goal Date - Food and Drug ... Goal Date April 7, 2014 Division / Office...
88
Statistical Reviewer: Tammy Massie, PhD STN: 125473 Page i Application Type Original BLA STN 125473 CBER Received Date January 25, 2013 Completion Goal Date April 7, 2014 Division / Office CBER/OBE/DB/VEB Priority Review n/a Reviewer Name(s) Tammy J. Massie, PhD Review Completion Date / Stamped Date Supervisory Concurrence A. Dale Horne, DrPH, Branch Chief VEB Lihan Yan, PhD, Team Leader BAT Applicant Merck, Inc. Established Name (Proposed) Trade Name Grastek® Pharmacologic Class Allergenic Extract (Timothy Grass) Formulation(s), including Adjuvants, etc Tablet Dosage Form(s) and Route(s) of Administration Sub-lingual (placed under tongue until dissolved) Dosing Regimen 2,800 Bioequivalent Allergy Unit (BAU) of the drug substance (per tablet), once per day. Proposed Indication(s) and Intended Population(s) Grastek ® (MK-7243) is indicated for the disease modifying treatment of diagnosed Timothy and related grass pollen induced allergic rhinitis, with or without conjunctivitis, in adults and children 5 years of age and older.
Transcript of Application Type Completion Goal Date - Food and Drug ... Goal Date April 7, 2014 Division / Office...

Statistical Reviewer: Tammy Massie, PhD STN: 125473
Page i
Application Type Original BLA
STN 125473
CBER Received Date January 25, 2013
Completion Goal Date April 7, 2014
Division / Office CBER/OBE/DB/VEB
Priority Review n/a
Reviewer Name(s) Tammy J. Massie, PhD
Review Completion Date / Stamped Date
Supervisory Concurrence A. Dale Horne, DrPH, Branch Chief VEB
Lihan Yan, PhD, Team Leader BAT
Applicant Merck, Inc.
Established Name
(Proposed) Trade Name Grastek®
Pharmacologic Class Allergenic Extract (Timothy Grass)
Formulation(s), including Adjuvants, etc
Tablet
Dosage Form(s) and Route(s) of Administration
Sub-lingual (placed under tongue until dissolved)
Dosing Regimen 2,800 Bioequivalent Allergy Unit (BAU) of the drug substance (per tablet), once per day.
Proposed Indication(s) and Intended Population(s)
Grastek ® (MK-7243) is indicated for the disease modifying treatment of diagnosed Timothy and related grass pollen induced allergic rhinitis, with or without conjunctivitis, in adults and children 5 years of age and older.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
Page ii
Table of Contents
Glossary ............................................................................................................................. 1
1. Executive Summary ...................................................................................................... 3
2. Clinical and Regulatory Background........................................................................ 11
2.1 Disease or Health-Related Condition(s) Studied .........................................................................12 2.2 Currently Available, Pharmacologically Unrelated Treatment(s)/Intervention(s) for the
Proposed Indication(s) ..................................................................................................................12 2.4 Previous Human Experience with the Product (Including Foreign Experience) ......................12 2.5 Summary of Pre- and Post-submission Regulatory Activity Related to the Submission .........14
3. Submission Quality and Good Clinical Practices .................................................... 14
3.1 Submission Quality and Completeness .........................................................................................14 3.2 Compliance with Good Clinical Practices and Data Integrity ....................................................14
4. Significant Efficacy/Safety Issues Related to Other Review Disciplines................ 14
5. Sources of Clinical Data and Other Information Considered in the Review ........ 15
5.1 Review Strategy ..............................................................................................................................15 5.2 BLA/IND Documents That Serve as the Basis for the Statistical Review ..................................17 5.3 Table of Studies/Clinical Trials .....................................................................................................18 5.4 Consultations ..................................................................................................................................23
5.4.1 Advisory Committee Meeting ................................................................................................23 5.5 Literature Reviewed .......................................................................................................................23
6. Discussion of Individual Studies/Clinical Trials ...................................................... 23
6.1 Trial #1: P05238-US and Canadian Adult Phase III Field Study ..............................................29 6.1.1 Objectives (Primary, Secondary, etc) .....................................................................................29 6.1.2 Design Overview ....................................................................................................................29 6.1.3 Population ..............................................................................................................................31 6.1.4 Study Treatments or Agents Mandated by the Protocol .........................................................31 6.1.6 Sites and Centers ....................................................................................................................31 6.1.7 Surveillance/Monitoring .........................................................................................................31 6.1.8 Endpoints and Criteria for Study Success ..............................................................................31 6.1.9 Statistical Considerations & Statistical Analysis Plan ...........................................................32 6.1.10 Study Population and Disposition ........................................................................................34 6.1.11 Efficacy Analyses .................................................................................................................37 6.1.12 Safety Analyses ....................................................................................................................44
6.2 Trial #2: P05239-US and Canadian Pediatric Phase III Field Study .........................................48 6.2.1 Objectives (Primary, Secondary, etc.) ....................................................................................48 6.2.2 Design Overview ....................................................................................................................49 6.2.3 Population ..............................................................................................................................50 6.2.4 Study Treatments or Agents Mandated by the Protocol .........................................................50 6.2.6 Sites and Centers ....................................................................................................................50 6.2.7 Surveillance/Monitoring .........................................................................................................51 6.2.8 Endpoints and Criteria for Study Success ..............................................................................51 6.2.9 Statistical Considerations & Statistical Analysis Plan ...........................................................51 6.2.10 Study Population and Disposition ........................................................................................51 6.2.11 Efficacy Analyses .................................................................................................................55 6.2.12 Safety Analyses ....................................................................................................................60

Statistical Reviewer: Tammy Massie, PhD STN: 125473
Page iii
7. Integrated Overview of Efficacy ................................................................................ 64
7.1 Indication #1 ...................................................................................................................................64 7.1.1 Methods of Integration ...........................................................................................................64 7.1.2 Demographics and Baseline Characteristics ..........................................................................67 7.1.3 Analysis of Primary Endpoint(s) ............................................................................................69 7.1.4 Analysis of Secondary Endpoint(s) ........................................................................................71 7.1.6 Other Endpoints .....................................................................................................................73 7.1.7 Subpopulations .......................................................................................................................74 7.1.10 Additional Efficacy Issues/Analyses ....................................................................................75 7.1.11 Efficacy Conclusions ............................................................................................................76
8. Integrated Overview of Safety ................................................................................... 76
8.1 Safety Assessment Methods ...........................................................................................................77 8.2 Safety Database ..............................................................................................................................77
8.2.1 Studies/Clinical Trials Used to Evaluate Safety .....................................................................77 8.2.2 Overall Exposure, Demographics of Pooled Safety Populations ...........................................77
8.3 Caveats Introduced by Pooling of Data across Studies/Clinical Trials......................................79 8.4 Safety Results ..................................................................................................................................80
8.4.1 Deaths .....................................................................................................................................82 8.4.2 Nonfatal Serious Adverse Events ...........................................................................................82 8.4.3 Study Dropouts/Discontinuations ...........................................................................................83 8.4.4 Common Adverse Events .......................................................................................................83 8.4.5 Clinical Test Results...............................................................................................................83 8.4.6 Systemic Adverse Events .......................................................................................................83 8.4.7 Local Reactogenicity ..............................................................................................................83 8.4.8 Adverse Events of Special Interest .........................................................................................84
8.5 Additional Safety Evaluations .......................................................................................................84 8.6 Safety Conclusions ..........................................................................................................................84
9. Additional Statistical Issues ....................................................................................... 84
9.1 Special Populations.........................................................................................................................84 9.1.1 Human Reproduction and Pregnancy Data ............................................................................84 9.1.2 Use During Lactation .............................................................................................................84 9.1.3 Pediatric Use and PREA Considerations ................................................................................84 9.1.4 Immunocompromised Patients ...............................................................................................84 9.1.5 Geriatric Use ..........................................................................................................................85 9.2 Aspect(s) of the Statistical Evaluation Not Previously Covered ...............................................85
10. Conclusions ................................................................................................................ 85
10.1 Statistical Issues and Collective Evidence ..................................................................................85 10.2 Conclusions and Recommendations............................................................................................85

Statistical Reviewer: Tammy Massie, PhD STN: 125473
Page 1
GLOSSARY
2M Patients received active treatment starting 2 months prior to the pollen season
4M Patients received active treatment starting 4 months prior to the pollen season
AASS Average Adjusted Symptom Score ASS Adjusted Symptom Score ACS Average Combined Score ANCOVA Analysis of Covariance ARIA GA2LEN Allergic Rhinitis and its Impact on Asthma Global Allergy and
Asthma European Network ARMS Average Rescue Medication Score ARTSS Average Rhinoconjunctivitis Total Symptom Score AUC Area Under the Curve BMI Body Mass Index CA Complementary Analysis CI (or % CI) Confidence Interval (or % Confidence Interval) CID Clinically Important Difference CMH Cochran-Mantel-Haenszel CS Combined Score CSR Clinical Study Report DRM Data Review Meeting DSMB Data and Safety Monitoring Board EMA European Medicines Agency EU European Union FAS Full Analysis Set FDA Food and Drug Administration GES Global Evaluation Score GLM Generalized Linear Model ICH International Conference on Harmonisation Ig Immunoglobulin IR Index of Reactivity ITT Intention-To-Treat LS Least Squares LOCF Last Observation Carried Forward MCID Minimal Clinically Important Difference MIVQUE0 Minimum Variance Quadratic Unbiased Estimation ML Maximum Likelihood ND Not Determined NS Not Significant PP Per Protocol PPS Per Protocol Set PRO Patient-Reported Outcome RC Rhinoconjunctivitis

Statistical Reviewer: Tammy Massie, PhD STN: 125473
Page 2
REML Restricted Maximum Likelihood RMS Rescue Medication Score RQLQ Rhinoconjunctivitis Quality of Life Questionnaire RRTSS Retrospective Rhinoconjunctivitis Total Symptom Score RTSS Rhinoconjunctivitis Total Symptom Score SAP Statistical Analysis Plan SAS Statistical Analysis System SD Standard Deviation SEM Standard Error of the Mean SLIT Sublingual Immunotherapy SIT Specific Immunotherapy TEAE Treatment Emergent Adverse Event VO Voie Orale (i.e., oral route in French) WAO World Allergy Organization

Statistical Reviewer: Tammy Massie, PhD STN: 125473
Page 3
1. EXECUTIVE SUMMARY Merck conducted a multinational clinical development program for MK-7243/Grastek® Timothy grass pollen extract sublingual tablet for the treatment of allergic rhinoconjunctivitis in patients with clinical symptoms due to Timothy grass pollen allergy. MK-7243/GRASTEK contains allergen extracts of the following grass pollen: Timothy (Phleum pratense L.). As per the applicant, this product, MK-7243/Grastek®, is indicated for: “the disease modifying treatment of diagnosed Timothy and related grass pollen induced allergic rhinitis, with or without conjunctivitis, in adults and children 5 years of age and older.” Overall, approximately ~2000 subjects 18 to 65 years of age and nearly 500 children 5-18 years of age participated in the clinical development program of MK-7243/Grastek®, which consisted of a total of fourteen clinical trials in the MK-7243/Grastek® Clinical Development program. The effectiveness and safety of MK-7243/Grastek® was evaluated in the following clinical trials from Phase I to Phase III:
• Five Phase 1 trials (GT-01, GT-03 and GT-04 in adults; GT-09 and GT-11 in children);
• One Phase 2 safety and efficacy trial in adults with AR and asthma (GT-07); • One dose-finding Phase 2/3 efficacy and safety trial in adults (GT-02); and • Six Phase 3 efficacy and safety trials (GT-08 in adults in Europe, GT-14 in adults
in the US, P05238 in adults in North America, GT-12 and P05239 in children in Germany and North America, respectively, and P08067 in adults/children in North America).
The majority of these studies were performed over one allergy season. However, a single long-term extension over several allergy seasons within the Phase 3 adult GT-08 trial was performed over up to 5 years and was completed in 2009; data from the 3 treatment years and the 2 follow-up years are provided in the applicant provided application. A summary of the thirteen efficacy studies, including the purpose of the study and the number of patients exposed to various doses of the Merck MK-7243/Grastek® product, is provided in the table below NOTE: in the following tables acronyms were utilized including: AIT = allergy immunotherapy tablet; Approx = approximately; BAU = Bioequivalent Allergen Unit; DB = double-blind; MC = multicenter; MD = multiple dose; OL = open label; PC = placebo-controlled; PG = parallel-group; QD = once daily; R = randomized; SD = single dose; SQ-T = standardized quality tablet; SQ-U = standardized quality unit; PD= pharmacodynamic; GPS = grass pollen season; IgE = immunoglobulin E.
Table 1: Summary of Clinical Studies

Statistical Reviewer: Tammy Massie, PhD STN: 125473
4
Type of Study
Study Identifier
Objective(s) of the Study
Study Design and Type of
Control
Test Product(s); Dosage Regimen; Route of
Administration
Number of Subjects
Healthy Subjects or Diagnosis of Patients
Duration of Treatment
Study Status; Type of Report
Efficacy and Safety
P05238 Efficacy and Safety
MC, R, DB, PG, PC; Phase 3
Grastek 2,800 BAU QD Placebo Sublingual tablet
438 (213 active; 225 placebo)
Clinical history of significant grass pollen-induced allergic rhinoconjunctivitis; Ages 18 to 65 years; Positive skin prick test and specific IgE to Phleum pratense
Approx 16 weeks prior to and then during the entire 2009 GPS (total of approx 24 weeks)
Completed Full
Efficacy and Safety
P05239 Efficacy and Safety
MC, R, DB, PC, PG; Phase 3
Grastek 2,800 BAU QD Placebo Sublingual tablet
344 (175 active; 169 placebo)
Clinical history of significant grass pollen-induced allergic rhinoconjunctivitis; Ages 5 to <18 years; Positive skin prick test and specific IgE to Phleum pratense
Approx 16 weeks prior to and then during the entire 2009 GPS (total of approx 24 weeks)
Completed Full
Safety GT-01 Safety Period 1: R, DB, PC, SD stepwise, dose escalation
Periods 2 and 3: R, DB, PC, MD, PG
Period 4: follow-up visit Phase 1
Grastek 93 BAU a
(2,500 SQ-U) QD Grastek 933 BAU (25,000 SQ-U) QD Grastek 2,800 BAU (75,000 SQ-U) QD Grastek 4,699 BAU (125,000 SQ-U) QD Grastek 14,097 BAU (375,000 SQ-U) QD Placebo Sublingual tablet
Period 1: 47 (39 active; 8 placebo)
Period 2, 3, and 4: 48 (36 active, 12 placebo)
Clinical history of grass pollen-induced seasonal moderate- to-severe allergic rhinoconjunctivitis; Ages 18 to 65 years; Positive skin prick test and specific IgE to Phleum pratense
Period 1: single dose (outside GPS)
Period 2: 8 weeks (outside GPS)
Period 3: 15 weeks (approx 4 weeks prior to the GPS and during the 2002 GPS)
Period 4: follow-up visit; planned to take place 3 months after the last visit of Period 3
Completed Full

Statistical Reviewer: Tammy Massie, PhD STN: 125473
5
Type of Study
Study Identifier
Objective(s) of the Study
Study Design and Type of
Control
Test Product(s); Dosage Regimen; Route of
Administration
Number of Subjects
Healthy Subjects or Diagnosis of Patients
Duration of Treatment
Study Status; Type of Report
Efficacy and safety
GT-02 Efficacy and Safety
MC, R, DB, dose ranging, PG, PC; Phase 2/3
Grastek 93 BAU (2,500 SQ-U)a QD Grastek 933 BAU (25,000 SQ-U) QD Grastek 2,800 BAU (75,000 SQ-U) QD Placebo Sublingual tablet
855 (569 active; 286 placebo)
Clinical history of significant grass pollen-induced allergic rhinoconjunctivitis (≥2 years); Ages 18 to 65 years; Positive skin prick test and specific IgE to Phleum pratense; Adequate level of symptomatology in the previous pollen season (observational year 2002)
Approx 8 weeks prior to and during the 2003 GPS (maximum duration of treatment was 24 weeks)
Completed Full
Safety GT-03 Safety R, DB, PC, MD, dose- escalation; Phase 1
Grastek 933 BAU (25,000 SQ-U) QD Grastek 2,800 BAU (75,000 SQ-U) QD Grastek 5,600 BAU (150,000 SQ-U) QD Grastek 11,200 BAU (300,000 SQ-U) QD Grastek 18,666 BAU (500,000 SQ-U) QD Grastek 28,194 BAU (750,000 SQ-U) QD Grastek 37,592 BAU (1,000,000 SQ-U) QD Placebo Sublingual tablet
84 (63 active; 21 placebo)
Clinical history of significant grass pollen-induced seasonal allergic rhinoconjunctivitis (≥2 years); Ages 18 to 65 years; Positive skin prick test and specific IgE to Phleum pratense
28 days (outside the GPS)
Completed Full

Statistical Reviewer: Tammy Massie, PhD STN: 125473
6
Type of Study
Study Identifier
Objective(s) of the Study
Study Design and Type of
Control
Test Product(s); Dosage Regimen; Route of
Administration
Number of Subjects
Healthy Subjects or Diagnosis of Patients
Duration of Treatment
Study Status; Type of Report
Safety GT-04 Safety R, DB, PC, MD, dose- escalation; Phase 1
Grastek 2,800 BAU (75,000 SQ-T) QD Grastek 5,600 BAU (150,000 SQ-T) QD Grastek 11,200 BAU (300,000 SQ-T) QD Grastek 18,666 BAU (500,000 SQ-T) QD Placebo Sublingual tablet
43 (32 active; 11 placebo)
Clinical history of significant grass pollen-induced allergic rhinoconjunctivitis (≥2 years) and mild- to-moderate asthma (last 2 years, symptoms in GPS); Ages 18 to 65 years; Positive skin prick test and specific IgE to Phleum pratense
28 days (outside the GPS) Completed Full
Efficacy and Safety
GT-07 Efficacy and Safety
MC, R, DB, PG, PC; Phase 2
Grastek 2,800 BAU (75,000 SQ-T) QD Placebo Sublingual tablet
114 (74 active; 40 placebo)
Clinical history of significant grass pollen-induced allergic rhinoconjunctivitis (≥2 years) and grass pollen-induced mild- to-moderate asthma (last 2 years, symptoms in GPS); Ages 18 to 65 years; Positive skin prick test and specific IgE to Phleum pratense
12±2 weeks prior to and during the 2004 GPS; (maximum duration of treatment was 24 weeks)
Completed Full

Statistical Reviewer: Tammy Massie, PhD STN: 125473
7
Type of Study
Study Identifier
Objective(s) of the Study
Study Design and Type of
Control
Test Product(s); Dosage Regimen; Route of
Administration
Number of Subjects
Healthy Subjects or Diagnosis of Patients
Duration of Treatment
Study Status; Type of Report
Efficacy and Safety
GT-08 Efficacy and safety
MC, R, DB, PG, PC; Phase 3
Years 1 to 3b: Grastek 2,800 BAU (75,000 SQ-T) QD Placebo
Years 4 and 5: No treatment Sublingual tablet
Year 1: 634 (316 active; 318 placebo) Year 2: 351 (189 active; 162 placebo)
Year 3: 308 (170 active; 138 placebo)
Year 4: 283 (157 active; 126 placebo)c
Year 5: 258 (145 active; 113 placebo)c
Clinical history of grass pollen-induced allergic rhinoconjunctivitis (≥2 years); Ages 18 to 65 years; Positive skin prick test and specific IgE to Phleum pratense
Year 1: 4 to 6 months prior to the GPS and during the 2005 GPS
Year 2 and 3: Extensions of GT-08 to the end of the 2006 and 2007 GPS, respectively
Year 4 and 5: No treatment follow-up extensions of GT-08 to the end of the 2008 and 2009 GPS, respectively
Completed Full
Safety GT-09 Safety MC, R, DB, PC, PG; Phase 1
Grastek 2,800 BAU (75,000 SQ-T) QD Placebo Sublingual tablet
30 (23 active; 7 placebo)
Clinical history of grass pollen-induced allergic rhinoconjunctivitis; Ages 5 to 12 years; Positive skin prick test and specific IgE to Phleum pratense
28 days (outside the GPS)
Completed Full

Statistical Reviewer: Tammy Massie, PhD STN: 125473
8
Type of Study
Study Identifier
Objective(s) of the Study
Study Design and Type of
Control
Test Product(s); Dosage Regimen; Route of
Administration
Number of Subjects
Healthy Subjects or Diagnosis of Patients
Duration of Treatment
Study Status; Type of Report
Compliance and Safety
GT-10 Compliance and Safety
MC, R, PG, OL; Phase 3
Grastek 2,800 BAU (75,000 SQ-T) QD Sublingual tablet
460 (460 active)
Clinical history of grass pollen-induced allergic rhinoconjunctivitis; Ages 18 to 65 years; Positive skin prick test to Phleum pratense
Approx 6 to 12 weeks prior to and during the 2006 GPS
Completed Full
Safety GT-11 Safety MC, R, DB, PC, PG; Phase 1
Grastek 2,800 BAU (75,000 SQ-T) QD Placebo Sublingual tablet
30 (22 active; 8 placebo)
Clinical history of grass pollen-induced allergic rhinoconjunctivitis; Ages 5 to 12 years; Positive skin prick test and specific IgE to Phleum pratense
28 days (outside the GPS) Completed Full
Efficacy and Safety
GT-12 Efficacy and Safety
MC, R, DB, PC, PG; Phase 3
Grastek 2,800 BAU (75,000 SQ-T) QD Placebo Sublingual tablet
253 (126 active; 127 placebo)
Clinical history of grass pollen-induced allergic rhinoconjunctivitis; Ages 5 to 16 years; Positive skin prick test and specific IgE to Phleum pratense
At least 16 weeks prior to and then during the entire 2007 GPS
Completed Full
Efficacy and Safety
GT-14 Efficacy and Safety
MC, R, DB, PG, PC; Phase 3
Grastek 2,800 BAU (75,000 SQ-T) QD Placebo Sublingual tablet
329 (163 active; 166 placebo)
Clinical history of grass pollen-induced allergic rhinoconjunctivitis (≥ 2 years); Ages 18 to 65 years; Positive skin prick test and specific IgE to Phleum pratense
At least 8 to 16 weeks prior to and during the 2007 GPS
Completed Full

Statistical Reviewer: Tammy Massie, PhD STN: 125473
9
Type of Study
Study Identifier
Objective(s) of the Study
Study Design and Type of
Control
Test Product(s); Dosage Regimen; Route of
Administration
Number of Subjects
Healthy Subjects or Diagnosis of Patients
Duration of Treatment
Study Status; Type of Report
Safety and tolerance
GT-15 Observational safety and tolerance
MC, R, OL; Phase 4
Grastek 2,800 BAU (75,000 SQ-T) QD Sublingual tablet
628 d
(628 active)
Presenting with grass pollen-induced allergic rhinitis; Ages >18 years; Previous positive skin prick test and/or specific IgE to Phleum pratense
At least 4 months prior to and during the 2008 GPS (maximum 10 months)
Completed Full
Immunology GT-16 Investigate changes in immunological parameters and cutaneous reactivity
MC, R, DB, PC, PG; Phase 3b
Grastek 2,800 BAU (75,000 SQ-T) QD Placebo Sublingual tablet
78 (52 active; 26 placebo)
Clinical history of grass pollen-induced allergic rhinitis (≥ 1 year); Ages 18 to 65 years;e
Positive skin prick test and specific IgE to Phleum pratense
Approx 2 to 4 months prior to and during the 2007 GPS
Completed Full
Compliance GT-17 Compliance MC, R, PG, OL Phase 4
Grastek 2,800 BAU (75,000 SQ-T) QD Sublingual tablet
261 (261 active)
Clinical history of grass pollen-induced allergic rhinoconjunctivitis (≥ 2 years); Ages >18 to <65 years; Positive skin prick test and specific IgE to Phleum pratense
Approx 48 weeks of treatment
Completed Full
Immunology GT-18 Investigate PD effect and tolerability of Grastek
MC, R, DB, PC, PG; Phase 3
Grastek 2,800 BAU (75,000 SQ-T) QD Placebo Sublingual tablet
276 (219 active; 57 placebo)
Clinical history of moderate-to-severe persistent grass pollen-induced allergic rhinoconjunctivitis (≥ 2 years); Ages 18 to 65 years; Positive skin prick test and specific IgE to Phleum pratense
At least 8 weeks of treatment initiated during the GPS
Completed Full

Statistical Reviewer: Tammy Massie, PhD STN: 125473
10
Type of Study
Study Identifier
Objective(s) of the Study
Study Design and Type of
Control
Test Product(s); Dosage Regimen; Route of
Administration
Number of Subjects
Healthy Subjects or Diagnosis of Patients
Duration of Treatment
Study Status; Type of Report
Safety GT-19 Safety (local allergic reactions) of Grastek in combination with desloratadine
R, DB, Crossover;
Phase 3
Grastek
2,800 BAU (75,000 SQ-T; sublingual tablet) SD
+ desloratadine 2.5
mg or placebo
(melting tablet) SD
46
(all subjects received single doses of each treatment)
Clinical history of moderate-to-severe persistent grass pollen-induced allergic rhinoconjunctivitis (≥2 years);
Ages 18 to 65 years; Positive skin prick test
and specific IgE to Phleum pratense;
Treatment-related local application site reaction in mouth
Single doses Completed
Full
Efficacy and
Safety
P08067 Efficacy and
Safety
MC, R, DB, PG, PC;
Phase 3
MK-7243
2,800 BAU QD Placebo Sublingual tablet
1501
(752 active;
749 placebo)
Clinical history of significant allergic rhinoconjunctivitis to grass (with or without asthma);
Ages 5 to 65 years; Positive skin prick test
and specific IgE to Phleum pratense
Approx 12 weeks prior to and then during the entire 2012
GPS
(total of approx
24 weeks)
Completed
Full
Table summarizes data provided within applicant provided datasets: -------------------------------------(b)(4)------------------------------------------------------

Statistical Reviewer: Tammy Massie, PhD STN: 125473
11
The studies provided in this submission appear to support the applicant’s conjecture that the Grastek® 2800 BAU product is safe and effective in the treatment of allergic rhinoconjunctivitis, using CBER’s pre-specified criterion for efficacy based on the Combined Symptom Score that incorporates both rescue medication and symptom scores. Furthermore, similar positive trends are observed for the individual endpoints of Total Symptom Scores as well as the Total Rescue Medication Scores. Based on the data submitted and reviewed, Grastek® 2800 BAU per dose, appears to be effective for immunotherapy treatment of allergic rhinoconjunctivitis due to sensitivity to the Timothy grass pollen included in the product for both youths 5-18 years of age as well as adults 18-65 years of age. Furthermore, the product appears to be safe for youths 5-18 years of age as well as adults 18-65 years of age, based on the statistical analyses examined and performed by the reviewing statistician.
2. CLINICAL AND REGULATORY BACKGROUND Allergic rhinoconjunctivitis (ARC) is a worldwide disease affecting over 500 million people, including approximately 30 million Americans. Grass pollen is a major seasonal allergen in the Unites States. Untreated or inadequately treated ARC can cause sleep disturbance, daytime fatigue, and somnolence as well as depressed mood, irritability, and behavioral problems. Societal costs include absenteeism from work or school and decreased productivity when at work. Currently, treatments for ARC include allergen avoidance, pharmaceutical treatment options including pharmacologic therapy such as oral antihistamines and nasal corticosteroids (which provide temporary relief from allergy symptoms but are not effective in all patients, and are not disease-modifying) and administration is subcutaneous injection (SCIT) (which is a treatment that modifies the immune response and treats the cause rather than the symptoms). An alternative to SCIT is sublingual immunotherapy (SLIT) in which treatment is administered orally rather than by injection. Two items to note with SLIT treatment presented in the literature include 1) the incidence of severe or serious AE associated with SLIT is significantly lower than with SCIT such that SLIT may be self-administered at home by the patient, and 2) safe use of SCIT requires administration in a clinic that is capable of responding to systemic allergic reactions. In Europe, Merck markets one solution for SLIT as a “named patient product,” and the sublingual immunotherapy tablet, Grazax®/Grastek®, that is the subject of this BLA. Grazax®/Grastek® is a tablet comprised of extracts from one single grass pollen Timothy (Phleum pratense L.). This grass belongs to the taxonomic (botanical) family Poaceae (formerly known as Gramineae) and subfamily Pooideae and is among the standardized grasses approved by CBER for the skin-test diagnosis and SCIT.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
12
Grastek® is currently marketed throughout the European Union (under the trade name Grazax®), and has successfully completed Phase 3 testing in the U.S. The applicant proposes the following indication:
“GRASTEK® is indicated for the disease modifying treatment of diagnosed Timothy and related grass pollen induced allergic rhinitis, with or without conjunctivitis, in adults and children 5 years of age and older.”
As in Europe, the dosage of the tablets to be used in the U.S. is 2800 BAU (Bioequivalent Allergy Units) -- an in-house potency measurement, which is discussed further in the clinical review of this product. Adults will initiate therapy at 2800 BAUs per day (one tablet, sublingually administered per day). The first dose of Grastek® should only be administered in a healthcare setting under the supervision of a physician with experience in the diagnosis and treatment of allergic diseases. After receiving the first dose, the patient should be kept under observation for 30 minutes to monitor for signs or symptoms of a severe systemic or severe local allergic reaction. If the first dose is adequately tolerated, subsequent doses may be taken at home. Grastek® should only be administered to children under adult supervision. Finally, treatment with Grastek® can be initiated at any time during the year. For symptom improvement during the first grass pollen season, treatment with Grastek® should be initiated at least 8 to 12 weeks prior to the season.
2.1 Disease or Health-Related Condition(s) Studied Allergic rhinitis (AR) is characterized by red, itchy eyes, a blocked and runny nose, and sneezing. The most common causes of allergic rhinitis are different pollens (grass and tree), house dust mites, mold, and animal dander. Allergic rhinitis can be intermittent (such as hay fever) or persistent (all year round). Often AR is accompanied by allergic conjunctivitis (AC), and may be accompanied by allergic asthma. About 10% of adults and children in the United States have AR.
2.2 Currently Available, Pharmacologically Unrelated Treatment(s)/Intervention(s) for the Proposed Indication(s) A comprehensive listing of products that are approved to treat AR can be found in the medical officer’s review. These include both pharmaceutical drugs (prescription as well as over the counter) as well as SCIT (subcutaneous injections).
2.4 Previous Human Experience with the Product (Including Foreign Experience) There are no allergenic products for grasses licensed or approved for administration in adults or children via SLIT in the U.S. However, several European countries have approved SLIT products for grasses as well as other extracts including Merck’s Grazax® (the European equivalent to Grastek®/MK-7243).

Statistical Reviewer: Tammy Massie, PhD STN: 125473
13
A total of 13 clinical trials comprise the Grastek® Clinical Program conducted to evaluate the efficacy and safety of Grastek®. This included five Phase 1 trials (GT-01, GT-03 and GT-04 in adults; GT-09 and GT-11 in children); one Phase 2 safety and efficacy trial in adults with AR and asthma (GT-07); one dose-finding Phase 2/3 efficacy and safety trial in adults (GT-02); and six Phase 3 efficacy and safety trials (GT-08 in adults in Europe, GT-14 in adults in the US, P05238 in adults in North America, GT-12 and P05239 in children in Germany and North America, respectively, and P08067 in adults/children in North America). A comprehensive list of all studies including the location of the study, allocation of patients to treatment or placebo treatment arm, as well as the age range of patients can be observed in the following table. Table 2.4.1. Number of Subjects Included in the 13 Studies Comprising the MK-7243 Clinical Development Program by Study and Age Range
Clinical Studies in Adult Subjects Study Number
Phase Study Location
Number of Subjects Total
Number of Subjects Active
Number of Subjects Placebo
Age Range (Years)
GT-01 1 EU 47 39 8 20 to 57 GT-03 1 EU 84 63 21 20 to 61 GT-04 1 EU 43 32 11 18 to 42 GT-02 2/3 Dose
finding EU 855 569 286 18 to 66
GT-07 2 EU 114 74 40 18 to 64 GT-08 Year 1 3 EU 634 316 318 18 to 65 Year 2 3 EU 351 189 162 18 to 63 Year 3 3 EU 308 170 138 18 to 63 Year 4 3 EU 283 157 126 18 to 63 Year 5 3 EU 258 145 113 18 to 63 GT-14 3 US 329 163 166 18 to 65 P05238 3 North
America 438 213 225 18 to 63
P08067 3 Norm America
1218 608 610 18 to ≥65
Total Number of Adult Subjects Enrolled
3762 2077 1685 18 to 66
Clinical Studies in Pediatric Subjects Study Number
Phase Study Location
Number of Subjects Total
Number of Subjects Active
Number of Subjects Placebo
Age Range (Years)
GT-09 1 EU 30 23 7 5 to 12 GT-11 1 EU 30 22 8 5 to 12

Statistical Reviewer: Tammy Massie, PhD STN: 125473
14
GT-12 3 Germany 253 126 127 5 to 16 P05239 3 North
344 175 169 5 to 18b
P08067 3 North
283 144 139 5 to <18 Total Number of Pediatric Subjects Enrolled
940 490 450 5 to 18
Source: Table created by reviewing statistician utilizing data provided in: -----------------------------------(b)(4)------------------------------------------------------- Additional experience can be found in the medical officer’s review.
2.5 Summary of Pre- and Post-submission Regulatory Activity Related to the Submission Additional information related to the Pre- and Post-submission Regulatory Activity related to this submission can be found in the medical officer’s and project manager’s reviews.
3. SUBMISSION QUALITY AND GOOD CLINICAL PRACTICES This submission includes the summary of thirteen (13) pre-marketing studies of which nine (9) studies included efficacy endpoints, and all thirteen (13) pre-marketing studies gathered safety data. These studies included approximately 2,500 subjects exposed to the Grastek® product, with study product administered prior to allergy season then efficacy data collected up to a year post dose. One study, GT-08, an adult phase 3 study performed in Europe, was completed in 2009 and included 5 years of safety and efficacy data collected. Two large Phase III studies were performed under US-IND, while the majority of the remaining studies were not performed under US-IND; however, these studies had similar endpoints and time frames.
3.1 Submission Quality and Completeness The submission was adequately organized for conducting a complete statistical review. The efficacy and safety data were presented within the Integrated Summary of Safety (ISS) section of the submission, which is unusual. Additionally, the applicant elected not to provide an integrated summary of efficacy. Thus, all efficacy data had to be gleaned from each individual study report.
3.2 Compliance with Good Clinical Practices and Data Integrity Based on the submitted material and current analysis, it appears the clinical trials were conducted in accordance with acceptable ethical standards.
4. SIGNIFICANT EFFICACY/SAFETY ISSUES RELATED TO OTHER REVIEW DISCIPLINES

Statistical Reviewer: Tammy Massie, PhD STN: 125473
15
At this point, no issues have been identified that would impact the statistical review or influence the conclusions made based on the studies which examined this product.
5. SOURCES OF CLINICAL DATA AND OTHER INFORMATION CONSIDERED IN THE REVIEW The BLA submission provided by Merck can be found in the following location: -------------------------------(b)(4)-------------------------------- This file path includes the clinical overview, summary of safety, summary of efficacy, as well as datasets for the 9 efficacy studies and 13 safety studies that were examined and analyzed by the reviewing statistician in the evaluation of this product. The datasets were SAS datasets. A comprehensive “define” document was provided by the applicant and included descriptions of the various datasets as well as variables within each dataset. In addition to the raw data collected from the Case Report Forms (CRFs) and Patient Reported Outcomes (PROs), the applicant also provided derived datasets. These datasets were confirmed by the reviewing statistician, utilizing a variety of methods, including comparisons of PROC FREQ results.
5.1 Review Strategy The applicant provided a summary and detailed results as well as the datasets of 9 efficacy studies and 13 safety studies. The primary studies of interest include the Phase III study under US IND. The data and the detailed and comprehensive write up of the studies are found within Module 2 and Module 4 of the original submission of this BLA, 125473 amendment 0, submitted to CBER on January 18, 2013. This BLA includes the following 13 clinical trials that comprise the clinical program which were conducted to evaluate the efficacy and safety of MK-7243:
• Five Phase I trials o Adults
GT-01 Europe GT-03 Europe GT-04 Europe
o Children GT-09 Europe GT-11 Europe
• One Phase II safety and efficacy trial in o Adults with Allergic Rhinitis (AR) and asthma
GT-07 Europe • One dose-finding Phase II/III efficacy and safety trial in
o Adults GT-02 Europe
• Six Phase III efficacy and safety trials:

Statistical Reviewer: Tammy Massie, PhD STN: 125473
16
o Adults: GT-08 Europe GT-14 US P05238 North America (US & Canada)
o Children: GT-12 Germany P05239 North America (US & Canada)
o Adults and Children P08067 North America (US & Canada).
The Phase I/II studies contribute data and information to the overall safety of this product and will only be discussed briefly in the safety section of this review. The Phase III studies that are of most interest were the studies performed under US-IND. These include: P05238 (Adults), P05239 (Children), P08067 (Adults and Children), and GT-14 (adults). Although GT-14 was a 12-month study conducted in the US including adults 18-65 years of age in 2006, it failed to demonstrate efficacy, and thus is not comprehensively reviewed in this document. Additionally, Study P05238 was a 12-month study conducted in the US and Canada, including adults 18-65 years of age conducted in 2009. While the point estimate of the difference between treatment and placebo groups suggested that the product was effective, the 95% Confidence Interval did not meet the pre-specified criterion for efficacy. The study is considered supportive, but did not meet its primary endpoint and thus is not comprehensively reviewed in this document. Study P05239 was a 12-month study of children 5-17 years old and demonstrated efficacy based on pre-specified criteria related to total combined symptom score. Additionally, Study P08067 was a 12-month study conducted in the U.S. and Canada in 2012 in children and adults 5-65 years of age. The data collected and analyzed from Study P08067 demonstrated efficacy among all subjects and in the subsets of children 5-17 years of age, and adults 18-65 years of age. The applicant also submitted, under the heading “Other Study Reports,” brief summaries and data from six additional studies that the applicant does not consider as pertinent to the claimed indication; however, they do provide additional insight into the Grastek® product. While safety data from these studies will be included in the overall safety evaluation, the individual studies will not be discussed in detail in this review. These studies are:
• GT-10, P05440, an open-label Phase 3 trial to assess treatment compliance with Grastek® (in adults with grass-induced ARC)
• GT-15, P07022; Observational national clinical trial of safety and tolerance in patients suffering from an allergic grass pollen rhinitis and treated by GRAZAX® in real life settings

Statistical Reviewer: Tammy Massie, PhD STN: 125473
17
• GT-16, P06990; A randomized, double-blind, placebo-controlled Phase 3b study investigating changes in immunological parameters and cutaneous reactivity induced by a short course immunotherapy with ALK grass tablets
• GT-17, P06991; A randomized, parallel-group, Phase 4, open-label trial evaluating compliance to the treatment with Grastek® tablets in patients with seasonal grass pollen rhinoconjunctivitis
• GT-18, P06744; A Phase 3 trial assessing the pharmacodynamic effect and the tolerability of Grastek® treatment initiated in the grass pollen season in subjects with seasonal grass pollen induced rhinoconjunctivitis
5.2 BLA/IND Documents That Serve as the Basis for the Statistical Review The BLA submitted by the applicant is stored in the following location: --------------------------------(b)(4)--------------------------------- This includes the clinical and non-clinical information, background material, protocol(s), case report forms, and datasets of all studies submitted by the applicant. The datasets are located in the file paths: ------------------------------------------(b)(4)--------------------------------------- ------------------------------------------(b)(4)--------------------------------------- ------------------------------------------(b)(4)--------------------------------------- ------------------------------------------(b)(4)--------------------------------------- ------------------------------------------(b)(4)--------------------------------------- ------------------------------------------(b)(4)--------------------------------------- ------------------------------------------(b)(4)--------------------------------------- ------------------------------------------(b)(4)--------------------------------------- ------------------------------------------(b)(4)--------------------------------------- ------------------------------------------(b)(4)--------------------------------------- ------------------------------------------(b)(4)--------------------------------------- ------------------------------------------(b)(4)--------------------------------------- ------------------------------------------(b)(4)--------------------------------------- ------------------------------------------(b)(4)--------------------------------------- ------------------------------------------(b)(4)--------------------------------------- ------------------------------------------(b)(4)--------------------------------------- ------------------------------------------(b)(4)--------------------------------------- --------------------------------------(b)(4)----------------------------------- --------------------------------------(b)(4)----------------------------------- Additionally, the applicant provided several publications related to the studies submitted within this BLA application.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
18
5.3 Table of Studies/Clinical Trials The following table lists a brief summary of the efficacy studies provided within this submission:

Statistical Reviewer: Tammy Massie, PhD STN: 125473
19
Table 5.3.a. Summary of Efficacy Studies Performed to Examine the Effect of Merck Grastek®: 2800 BAU dose
Study # Location Years/ Age Range Study Type Treatment
Dose Number of
Subjects
GT-08 EU 2004-2009 18-65 year
Safety/Efficacy Field
2800 BAU Placebo
316 318
P08067 US, Canada 2012 5-56 year
Safety/Efficacy Field
2,800 BAU Placebo
752 749
GT-14 US 2006-2007 18-65year
Safety/Efficacy Field
2,800 BAU Placebo
166 163
P05238 US, Canada 2008-2009 18-65year
Safety/Efficacy Field
2,800 BAU Placebo
166 163
GT-12 Germany 2006–2007 5-16 year
Safety/Efficacy Field
2,800 BAU Placebo
126 127
P05239 US, Canada 2008–2009 5-18 year
Safety/Efficacy Field
2,800 BAU Placebo
175 169
Table summarizes data provided within applicant provided datasets: ------------------------------------(b)(4)---------------------------------------
All studies examined within this submission were single-season field studies that examined subjects’ responses for only one allergy season. These utilized studies collected safety data; however, there were several additional studies explicitly designed to provide insight into safety/tolerability of this product. A summary of the safety studies can be examined in the following table:

Statistical Reviewer: Tammy Massie, PhD STN: 125473
20
Table 5.3.b. Grastek® Sublingual Tablet Clinical Studies and Design Features
Study # Location Age Range Study Type Treatment Dose Number of Subjects
GT-01 EU 18-65 years old Phase 1 Safety/Tolerability
2800 BAU Placebo
Period 1 Period 2/3/4 39 36 8 12
GT-03 EU 18-65 years old Phase 1 Dose Escalation
Safety/Tolerability
933 BAU 2800 BAU 5600 BAU
11,200 BAU 18,666 BAU 28,194 BAU 37,592 BAU
Placebo
9 9 9 9 9 9 9 21
GT-04 EU 18-65 years old Phase 1 Dose Escalation
Safety/Tolerability
2800 BAU 5600 BAU
11,200 BAU 18,666 BAU
Placebo
8 8 8 8 11
GT-02 EU 18-65 years old Phase 2 Dose Finding
Safety/Tolerability
93 BAU 933 BAU
28,000 BAU Placebo
189 189 190 286
GT-07 EU 18-65 years old Phase 2 Efficacy
Safety/Tolerability
28,000 BAU Placebo
74 40
GT-08 EU 18-65 years old Phase 3 Safety/Efficacy
Field
2800 BAU Placebo
316 318
P08067 US, Canada
5-56 yeasr old Phase 3 Safety/Efficacy
Field
2,800 BAU Placebo
752 749
GT-14 US 18-65year Phase3 Safety/Efficacy
Field
2,800 BAU Placebo
166 163
P05238 US, Canada
18-65year Phase 3 Safety/Efficacy
Field
2,800 BAU Placebo
166 163
GT-12 Germany 5-16 year Phase 3 Safety/Efficacy
Field
2,800 BAU Placebo
126 127
P05239 US, Canada
5-18 year Phase 3 Safety/Efficacy
Field
2,800 BAU Placebo
175 169
Table summarizes data provided within applicant provided datasets: -------------------------------(b)(4)---------------------------------------------

Statistical Reviewer: Tammy Massie, PhD STN: 125473
21
A summary of the analyses based on the Combined Score for the first year of all efficacy studies is provided in Table 5.3.c, below. Table 5.3.c. Grastek® Summary of Primary Efficacy Results Based on Combined Medication and Symptom Score
Study # Location Age Range
Treatment Dose
Number of
Subjects
Met US-FDA
Criteria for
Efficacy*
% Difference TCS
(*)
Pt Est (95% CI)
GT-08 EU 18-65yr 2800 BAU Placebo
316 318
Yes -34% (-42, -26%)
P08067 US, Canada
5-56yr 2,800 BAU
Placebo
752 749
Yes -23% (-36%, -13%)
GT-14 US 18-65yr 2,800 BAU
Placebo
166 163
No -10% (-24%, 4%)
P05238 US, Canada
18-65yr 2,800 BAU
Placebo
166 163
No -21% (-33%, -6%)
GT-12 Germany 5-16yr 2,800 BAU
Placebo
126 127
No -24% (-41%, -4%)
P05239 US, Canada
5-18yr 2,800 BAU
Placebo
175 169
Yes -26% (-45, -14%)
Source: Table summarizes data provided within applicant provided datasets: ------------------------------(b)(4)-------------------------------------------- * Based on the Upper Limit of the 95% CI of the % difference between placebo and treatment being less than -10%

Statistical Reviewer: Tammy Massie, PhD STN: 125473
22
Table 5.3.d Grastek® Summary of Primary Efficacy Results Based on Combined Medication and Symptom Score, Daily Symptom Score, and Daily Medication Score
Source: sBLA 125473/000; Summary of Clinical Efficacy, Page 154 Source: sBLA 125473/000; Summary of Clinical Efficacy, Page 154

Statistical Reviewer: Tammy Massie, PhD STN: 125473
23
Figure 5.3.e. Grastek® Summary of Primary Efficacy Results Based on Combined Medication and Symptom Score
Source: sBLA 125473/000; Summary of Clinical Efficacy, Page 164
5.4 Consultations
5.4.1 Advisory Committee Meeting
An Advisory Committee meeting was held on December 12, 2013 to discuss Merck’s Grastek® product. The Advisory Committee voting results suggested that the data for this product support the contention of adequate safety and efficacy in individuals 18-65 years of age.
5.5 Literature Reviewed Within this submission the applicant provided several articles related to the studies performed. These articles have extensive references of which the statistician utilized several journal articles as well as websites (in particular World Allergy Organization-WAO published suggested standards for allergenic products).
6. DISCUSSION OF INDIVIDUAL STUDIES/CLINICAL TRIALS This submission included the results of fourteen randomized, double blind, placebo controlled clinical trials to examine the safety/tolerability and efficacy of Grastek®. Specifically, the applicant submitted the data and summaries of the following safety/tolerability and efficacy studies:
• GT-07 (Phase II/III: European safety/tolerability and efficacy in Adults) • GT-02 (Phase II/III: European safety/tolerability and Dose finding study in
Adults)

Statistical Reviewer: Tammy Massie, PhD STN: 125473
24
• GT-08 (Phase III: European safety/tolerability and efficacy study in Adults) • GT-14 (Phase III: US safety/tolerability and efficacy study in Adults) • P05238 (Phase III: North American safety/tolerability and efficacy study in
Adults) • P05238 (Phase III: North American safety/tolerability and efficacy study in
Adults) • P05239 (Phase III: North American and German safety/tolerability and efficacy
study in Children) • P08067 (Phase III: North American safety/tolerability and efficacy study in
Adults and Children)
Additionally, the applicant examined the safety/tolerability of this product in five additional studies that included either Adults or Children.
• GT-01 (Phase I: European safety study in Adults) • GT-03 (Phase I: European safety study in Adults) • GT-04 (Phase I: European safety study in Adults) • GT-09 (Phase I: European safety study in Children) • GT-11 (Phase I: European safety study in Children)
The studies of primary interest in the examination of the efficacy of this product, Grastek®, are the Phase III studies performed under US-IND:
• P05238 (Phase III: North American safety/tolerability and efficacy study in Adults)
• P05239 (Phase III: North American and German safety/tolerability and efficacy study in Children)
• P08067 (Phase III: North American safety/tolerability and efficacy study in Adults and Children)
Key design features for the studies that were consistent among the majority of studies include the following components. Data were to be collected to determine the safety and the efficacy of this product. This included efficacy endpoints related to Total Daily Symptom Scores (DSS), Total Daily Rescue Medication Scores (DMS), and Total Combined Symptoms (TCS) which combines the Daily Symptom Scores and Daily Rescue Medication Scores. Additionally, the total Rhinoconjunctivitis Quality of Life Questionnaire (RQLQ) was to gather scores related to general lifestyle prior to and during the pollen season. Randomization In all studies, patients who fulfilled all the inclusion criteria and none of the exclusion criteria were randomized to active therapy or placebo, with a treatment assignment ratio (or allocation ratio) typically leading to groups of equal size (ratio 1:1, 1:1:1, 1:1:1:1 for studies with placebo and one, two, or three dosage levels of active treatment, respectively). Once the final dosage of 2,800 BAU was selected as the optimal dose, all

Statistical Reviewer: Tammy Massie, PhD STN: 125473
25
future studies randomized patients in a 1:1 ratio. A computer-generated randomization list was prepared for each study. All multicenter studies were stratified by study center by allocating complete blocks to each center. Control treatment The efficacy studies were placebo-controlled. The placebo tablets appeared identical to the active treatment tablets with respect to physical characteristics (i.e., color, weight, taste, size, and shape), the number of tablets per treatment box, and the number of tablets to be taken daily. The excipients were also the same as those used in the active treatment tablets. Furthermore, both the treatment and placebo dose were quick-release tablets that would dissolve within 5 seconds on the tongue, ensuring a similar feel and dissolution rate for both placebo and treatment tablets. Blinding All studies addressed in this document were double-blind. The issue of blinding specific immunotherapy studies is raised in the Food and Drug Administration (FDA) Guidance for Industry: Allergic Rhinitis, Clinical Development Programs for Drug Products (April 2000) and in the EMA Guideline [EMA, 2008]: “. . . superiority versus placebo or any other comparator has to be shown. Since local allergic adverse events are frequent in specific immunotherapy, a placebo preparation with histamine may be considered to keep the blinding.” Treatment Schedules The various study treatment schedules were not consistent between all studies; thus, separate discussions of individual studies will be provided when examining specific studies. However, in general there was a baseline time period in which subjects’ allergic symptoms were collected. Subsequent administration of product occurred 16 to 12 weeks prior to the anticipated pollen season, and during the pollen season, subjects noted their allergic symptoms within daily diary cards. Additionally, during and after the treatment dosing time frame, adverse events were collected within diary cards or during clinic visits. Patient population The patients enrolled in the clinical development program included both adults and/or children, depending on the study and were consistent with the population consulting allergy practices for treatment of grass pollen-related allergic rhinoconjunctivitis. Choice and description of study endpoints The clinical development program of Grastek® sublingual tablet began by Merck (originally ALK Abello) in 2001. The efficacy endpoints chosen for the Phase 3 program were in accordance with FDA and EMA guidances on evaluations for AR and the EMA guideline on the clinical development of products for specific immunotherapy for the treatment of allergic disease.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
26
According to these guidelines, an accepted demonstration of efficacy in rhinoconjunctivitis is based on alleviation of symptoms as measured by subject symptom score, use of rescue medication, and in vitro parameters. However, based on advice provided during the May 2011 Allergenic Product Advisory Committee, endpoints were utilized that reflect symptoms adjusted by rescue medication usage. Thus, the efficacy endpoints chosen for the Phase 3 program were in accordance with these guidelines on evaluations for AR trials and included rhinoconjunctivitis daily symptom score (DSS), daily medication score (DMS), and the total combined symptom and medication score (TCS: the sum of DSS and DMS). The total Rhinoconjunctivitis Quality of Life Questionnaire with standardized activities (RQLQ) score was a key secondary endpoint. Throughout the program, the applicant designed the studies in line with appropriate health authority guidelines, including the US-FDA with respect to the single study performed under US-IND. The field exposure studies provided in this submission had similar endpoints and time frames for administration and data collection, while the safety studies had similar endpoints with safety data collected over time spans consisting of 28 days from initial exposure to Oralair® through up to 3 years post-exposure to the product. Symptom Score Daily rhinoconjunctivitis symptoms, including the four nasal symptoms of runny nose, stuffy nose, sneezing, and itchy nose, and the two non-nasal symptoms of gritty/itchy eyes and watery eyes, were measured on a scale of 0 (none) to 3 (severe) in accordance with the FDA and EMA guidance, as well as clinical guidance from the WAO. A description of the score to be reported by patients is provided in the following table. Table 6.a. Daily Symptom Score
Score Severity Description
0 Absent symptoms No sign/symptom evident
1 Mild symptoms Sign/symptom clearly present, but minimal awareness; easily tolerated
2 Moderate symptoms Definite awareness of sign/symptom, which is bothersome but tolerable
3 Severe symptoms Sign/symptom that is hard to tolerate, may cause interference with activities of daily living and/or sleeping
Table summarizes the definition of symptom scores based on definitions provided within summary of clinical efficacy: -----------------------------------------(b)(4)------------------------------------------------------- Daily Medication Score In natural field studies, in order to manage severe rhinoconjunctivitis symptoms, patients were permitted to take rescue medication according to a stepwise regimen described in each protocol. The Daily Rescue Medication Score (DMS) was defined by Merck based on the hypothesis that a nasal corticosteroid is more efficient than an antihistamine and an oral corticosteroid is more efficient than a nasal corticosteroid, leading to a derived ordinal score that can be seen in the following table. Additionally, it was suggested to the randomized patients to utilize rescue medication based on a stepwise manner that

Statistical Reviewer: Tammy Massie, PhD STN: 125473
27
would escalate the use of rescue medication as the symptoms developed and became more severe. Table 6.b. Daily Rescue Medication Score
Rescue Medication for Rhinoconjunctivitis symptoms Score/Dose Unit Maximum Daily Score
Loratadine syrup 1 mg/mL – 5 mL QD (5 to <6 years) 6 (per 5 mL) 6
Loratadine RediTabs tablet 10 mg – 1 tablet QD ≥ 18 years); Claritin syrup 1 mg/mL – 10 mL QD (≥6 to <18 years)
6 (per tablet or 10 mL)
6
Olopatadine hydrochloride 0.1% ophthalmic solution - 1 drop in the affected eye BID
1.5 (per drop) 6
Mometasone furoate monohydrate nasal spray 50 mcg – 1 spray in each nostril QD (5 to <12 years of age)
4 (per spray) 8
Mometasone furoate monohydrate nasal spray 50 mcg - 2 sprays in each nostril QD (≥12 years of age)
2 (per spray) 8
Prednisone tablet 5 mg (Day 1 - 1 mg/kg/day, Max 50 mg/day)
1.6 (per tablet) 16
Prednisone tablet 5 mg (Day 2+ - 0.5 mg/kg/day, Max 25 mg/day)
1.6 x 2 (per tablet) 16
Maximum daily rhinoconjunctivitis medication score 36
Source: Adapted from applicant’s Table 4 Clinical Overview Page 25 Total Combined Symptom and Medication Score This combined score incorporated both the daily symptom scores and the combined symptom score. The daily Total Combined Score (TCS) is a score taking into account the DDS and DMS and assuming equivalent importance of symptoms and medications scores. This score is the combination of the daily symptom score and daily rescue medication score and is calculated for each day for each patient as: TCS = DSS + DMS. General Statistical approach For each study in the clinical development program, all analyses were pre-specified in the respective protocol and detailed in the associated Statistical Analysis Plan (SAP) and its amendments. Each SAP also described the models to be used for the endpoint analyses, validity assumptions, handling of missing data, and how potential statistical issues were to be addressed. In the Phase 2 and 3 studies of Grastek®, the key efficacy endpoints of clinical interest, TCS, DSS, and DMS, were computed as the average of the available daily scores over specified GPS (entire or peak GPS). The daily TCS was computed as the sum of daily DSS and DMS scores.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
28
In the majority of studies that included efficacy endpoints, the key efficacy endpoints were to be analyzed using linear mixed models. The specific model to be utilized for each study adjusted for factors such as site/region effect, asthma status, and baseline scores, and these details are outlined in each individual study report. The least squares mean and 2-sided 95% confidence interval (CI) for the between-treatment differences were estimated from the models, with the associated p-values reported. In addition, the percentage reduction relative to placebo effect was calculated as (Grastek®-placebo) / placebo x 100% using the within-group least squares means for the Grastek® group and the placebo group. The normality assumption of the ANOVA model was examined for the key efficacy endpoints. When the normality assumption was severely violated, analysis based on appropriate parametric methods (e.g., square root and log transformation of the data, and a zero-inflated log-normal model) or nonparametric analysis (e.g., Wilcoxon rank sums test and Hodges-Lehmann analysis of median differences) was adopted as the primary efficacy analysis. In addition, when ANOVA remained as the primary analysis approach, sensitivity analyses using such transformed data or non- parametric methods were utilized to corroborate the results for the primary ANOVA analysis approach. Further, the interaction of treatment with other model covariates was examined via subgroup analyses by each level of the covariates. The efficacy analyses were based on the full analysis set (FAS), which generally includes all randomized subjects in accordance with the International Conference on Harmonization (ICH) intention-to-treat principles. Additional analyses based on a per-protocol approach were also performed to corroborate the results of the key efficacy endpoints. In the Phase 2/3 studies of Grastek®, the safety analyses were performed based on all randomized subjects. Subjects were counted in the treatment group for which treatment they actually received. The adverse experiences were summarized by treatment group for the frequency distribution (number and percentage). The vital signs were summarized by treatment group, including the means and standard deviations for changes from baseline. Additional details are provided in individual study reports. In addition to the safety summary of the individual studies, the data were pooled across studies, separately for the adult and pediatric populations, to provide an integrated summary of safety profile of Grastek® treatment. Analysis sets In the natural field studies, consistent with the ICH E9 Guideline (Statistical Principles for Clinical Trials), the applicant planned to utilize the analysis set which is as complete as possible and as close as possible to the Intention-To-Treat ideal of including all randomized subjects. The primary efficacy analysis included data from all patients who received at least one dose of the investigational product and had recorded the primary efficacy measure on at least one day during the pollen period while on treatment. Thus, the primary analysis set is appropriately termed “Full Analysis Set” (FAS).

Statistical Reviewer: Tammy Massie, PhD STN: 125473
29
6.1 Trial #1: P05238-US and Canadian Adult Phase III Field Study Merck’s trial P05238 was submitted to CBER under US-IND to be “a multi-center, double-blind, randomized, placebo controlled, parallel-group study evaluating the efficacy and safety of grass (Phleum Pratense) sublingual tablet (SCH 697243) in adult subjects with a history of grass pollen induced rhinoconjunctivitis with or without asthma.”
6.1.1 Objectives (Primary, Secondary, etc)
The objectives of this study were to evaluate the efficacy and safety of sublingual tablets of grass pollen allergen extract compared with placebo for reduction of rhinoconjunctivitis symptoms and rescue medication usage. Primary Objective: To evaluate the efficacy of grass sublingual tablet (Grastek®) versus placebo in the treatment of grass pollen-induced rhinoconjunctivitis based on the combined sum (CS) of rhinoconjunctivitis daily symptom scores (DSS) and rhinoconjunctivitis daily medication scores (DMS) averaged over the entire grass pollen season (GPS). Key Secondary Objectives: To assess overall safety and to compare the following between the Grastek® and placebo groups:
• The average rhinoconjunctivitis DSS for the entire GPS. • The average rhinoconjunctivitis DMS for the entire GPS. • The average weekly rhinoconjunctivitis quality of life total score for the entire
GPS.
6.1.2 Design Overview
This was a multicenter, double-blind, randomized, placebo-controlled, parallel-group study in subjects 18 to 65 years of age, of either sex and of any race, with a history of grass pollen-induced rhinoconjunctivitis with or without asthma. There was an observational grass pollen season period in year 2008 where no investigational medicinal product (IMP) was administered. Open-label rescue medications for the rhinoconjunctivitis and asthma symptoms were provided during this year. Eligible subjects were to visit the study site for at least 6 visits: Screening, Post-screening, Pre-season, On-season, End-of-season, and Off-season Visits, and at Unscheduled Visits as appropriate. Additional Off-season Visits were scheduled depending on the timing of the Randomization Visit in relation to the anticipated start of the Grass Pollen Season (GPS). Qualified subjects were to be randomized into the treatment period.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
30
In the treatment period, the subjects were treated once daily with either Grastek® (Timothy grass allergy immunotherapy tablet [grass AIT]) or placebo for approximately 16 weeks prior to the GPS and during the GPS. At the Randomization Visit, subjects were supplied with self-injectable epinephrine together with instructions on how and when to use it. Open-label rescue medications for the rhinoconjunctivitis and asthma symptoms were to be provided. Subjects were to visit the study site for at least 9 visits: Screening (2 visits), Randomization (3 visits), Off-season, Pre-season, On-season, and End-of-season Visits, and at Unscheduled Visits as appropriate. The first three consecutive daily doses of IMP were administered at the study site, and the subjects were monitored at the site for 30 minutes following dosing. Subsequent administration of IMP was done once daily at home at approximately the same time each day. A telephone contact between the investigator/designee and the subject occurred once daily for the first 4 days of at-home administration of IMP to monitor adverse events (AEs) and once approximately 1 week after the End-of-season Visit. A summary of the study visits and data collection points for this study are illustrated in the following study design diagram. Figure 6.1.2.a. Study Design Diagram
Source: Original BLA 125473/000 Clinical Study Report P05238 page 35 This study was conducted in conformity with Good Clinical Practice. A data safety monitoring committee (DSMC) was established prior to the start of the treatment period. The purpose of the DSMC was to evaluate adverse event data and to provide recommendations regarding the conduct of the study to ensure the safety of the subjects. Reviewer Comment: The study as proposed and implemented was acceptable to the statistical reviewer. Initially, CBER had suggested a different and more stringent threshold for the upper bound of the 95% confidence interval; however, based upon feedback from many applicants and discussions held during the May 2011 APAC, it was

Statistical Reviewer: Tammy Massie, PhD STN: 125473
31
determined that a -10% margin for the upper bound of the 95% CI was sufficient. This revised upper bound threshold was agreeable to CBER, and it was utilized as the standard criterion for efficacy for all field studies for seasonal allergies caused by grass pollens.
6.1.3 Population
The treatment population consisted of male or female patients aged 18 to 65 years (inclusive) in the United States and Canada with documented grass pollen-related allergic rhinoconjunctivitis, based on a clinical history of significant allergic rhinoconjunctivitis to grass (with or without asthma) diagnosed by a physician and who had received treatment for their disease for the previous grass pollen season, had a positive SPT to Timothy grass (wheal diameter ≥ 5 mm, greater than the negative control), and were positive for specific IgE against Phleum pratense (≥ IgE Class 2; ≥ 0.7 kAU/L) at the screening visit.
6.1.4 Study Treatments or Agents Mandated by the Protocol
In this study, two treatments were to be examined and compared: 2800 BAU Grastek® tablets and Placebo tablets that matched the 2800 BAU Grastek® tablets. Both the active treatment and placebo were to be administered sublingually (under the tongue) every day at the same time during the approximate 4 to 6-month treatment period, depending on the location of the treatment site.
6.1.6 Sites and Centers
This study was to include 59 centers in various locations within the United States and 10 centers within Canada with expected exposure to grass pollen.
6.1.7 Surveillance/Monitoring
A detailed synopsis of the surveillance and monitoring of the study can be found in the medical officer’s and epidemiologist’s reviews. However, a data safety monitoring committee (DSMC) was set up to ensure adequate safety monitoring of the study with pre-specified plans to examine and stop the study in case of unexpected safety issues.
6.1.8 Endpoints and Criteria for Study Success
There are several primary and secondary endpoints in this study that were utilized to assess how well the Grastek® product reduced symptoms related to grass allergies, as well as reduced the need to take medications to treat or prevent symptoms associated with grass allergies. The primary criterion for success was the combined symptom score (CS), which consisted of the patient’s daily symptom scores (DSS) and daily rescue medication scores (DMS). Primary efficacy variable: The daily combined symptom score (CS) is a daily patient-specific score taking into account the patient’s daily rhinoconjunctivitis symptom scores (DSS) and daily rescue

Statistical Reviewer: Tammy Massie, PhD STN: 125473
32
medication scores (DMS), assuming equivalent importance of symptoms and medication scores. The TCS score is calculated as: TCS = DSS + DMS. The DSS is described in Section 6, including tables that specifically provide the scoring mechanisms and methods. Secondary efficacy variables:
- Daily Symptom Scores (DSS): The DSS is the sum of the six (non-missing) rhinoconjunctivitis symptom scores as evaluated by the patient using a score from 0 to 3.
- Daily Rescue Medication Score (DMS): The DMS was assigned daily to the different medications used as rescue medication.
- Rhinoconjunctivitis symptoms (RSS): The severity of each of the six individual rhinoconjunctivitis symptoms was scored daily.
In addition to examining the various scores, TCS, DSS, DMS, during the entire grass pollen season, these scores were also computed and compared for the worst pollen period while the patient was on treatment. Additionally, the following tertiary endpoints were examined:
- The proportion of patients who used rescue medication during the pollen period and worst pollen period while on treatment.
- The proportion of days rescue medication was used during the pollen period and worst pollen period while on treatment.
- Proportion of Symptom-Controlled Days (PSCD) as defined by a DSS score of “0.”
- Overall Rhinoconjunctivitis Quality of Life Questionnaire (RQLQ) score. - Global assessment and evaluation of the efficacy of the treatment by the patient. - Asthma status and severity. - Immunological markers (IgE and IgG4 specific for Timothy grass pollen allergen)
and Skin Prick Test (SPT) results. Safety variables: - Adverse events (AEs).
- Laboratory assessments. - Physical examinations. - Vital signs.
6.1.9 Statistical Considerations & Statistical Analysis Plan
Analysis sets: For the purpose of this study, three analysis sets were defined, namely, the Safety Set, the Full Analysis Set (FAS), and the Per Protocol Analysis Set (PPS), which were pre-specified and defined as follows:

Statistical Reviewer: Tammy Massie, PhD STN: 125473
33
- The Safety Set includes all patients who received at least one dose of the investigational product.
- The FAS includes all patients who received at least one dose of investigational product and had at least one TCS while on treatment during the grass pollen season (GPS). The FAS was regarded as the primary population for the efficacy analyses.
- The PPS includes all patients from the FAS who had valid TCS during the GPS while on treatment and who completed the study according to the protocol and had no major protocol deviations.
The primary efficacy endpoint of the total combined (sum of) rhinoconjunctivitis DSS and DMS averaged over the entire GPS was evaluated using a linear model with asthma status, study site, and treatment group as fixed effects. For the primary endpoint, subjects with at least one post-baseline diary record with DSS and DMS within the defined pollen season were included. The combined average score was to be based on all available data during the GPS for each subject. A 2-sided 95% confidence interval of the difference in adjusted means between the two treatment groups was presented. Also, the difference in adjusted means between the two treatment groups relative to the adjusted mean of the placebo group was presented as a percentage with corresponding confidence intervals. Secondary Efficacy Endpoints: The secondary endpoints were evaluated using a linear model with asthma status, treatment, and study site effects in the model. For the following key secondary endpoints, the type 1 error rate was controlled using the Hochberg procedure:
• SCH 697243 vs placebo on the average rhinoconjunctivitis DSS for the entire GPS
• SCH 697243 vs placebo on the average rhinoconjunctivitis DMS for the entire GPS
• SCH 697243 vs placebo on the average weekly rhinoconjunctivitis quality of life total score for the entire GPS.
The secondary endpoints were adjusted for multiplicity using the Benjamini and Hochberg method to control the overall alpha level of 0.05 among the secondary efficacy tests of interest. The key secondary analyses were to be performed only if the primary analysis was statistically significant at two-sided alpha = 0.05. Safety Analysis: The number of subjects reporting any adverse events, the incidence of specific adverse events, and discontinuations due to adverse events were tabulated by treatment group. Laboratory and vital sign data were listed and summarized, and values outside the reference ranges were flagged. Missing Data: For the primary analysis, there was no imputation of missing data. The combined average score was based on the available data. However, the primary analysis was supplemented by sensitivity analyses using various imputation techniques to ensure the robustness of the conclusions made via the primary analysis methods.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
34
Determination of sample size: In the observational period, up to 450 subjects were to be enrolled. Assuming 25% dropout from the observational period, approximately 340 subjects were to be enrolled in the treatment period the following year. New subjects were also to be enrolled after the start of the Year 1 (2008) observational period GPS if additional subjects were needed to meet the targeted sample size. In the treatment period, the subjects were to be randomized in a 1:1 ratio to either Grastek® or placebo. With approximately 170 subjects per group, the study was able to detect the following difference from placebo in the primary endpoint with 88% power at a 5% level of significance (2-sided test). This sample size was based on an estimated placebo effect of the combined score (CS) of 7.07, an estimated pooled standard deviation of 4.77, and a difference of effect from placebo to treatment of 1.62 (or 23%), all of which were estimated based on prior Phase I/II studies of Grastek®. Reviewer Comment: The applicant initially proposed utilizing a point estimate in which an improvement of greater than 20% based on the combined score of the Grastek® treated individuals over the placebo comparator was to be considered the primary endpoint. This was agreeable to CBER; however, it was suggested that the study also meet a clinically meaningful margin of -10% for the upper bound of the 95% CI. This study was created in 2007 and started in 2008, well before the feedback provided and issues discussed during the May 2011 APAC meeting in which this advice for standards for field studies was presented in a public format.
6.1.10 Study Population and Disposition
The study population and baseline demographics of the enrolled patients are similar for both treatment groups. In this study, 439 patients were randomized to treatment.
6.1.10.1 Populations Enrolled/Analyzed The following table illustrates the population distribution in study P05238. Table 6.1.10.1.1. Summary of Patient Population
Grastek 2800 BAU N (%)
Placebo N (%)
Total N (%)
Patients Randomized 213 (100%)
225 (100%)
438 (100%)
Patients in Safety Set 213 (100%)
225 (100%)
438 (100%)
Patients in Full Analysis Set 213 (100%)
225 (100%)
438 (100%)
Protocol Evaluable Data Set 164 (77%)
188 (84%)
352 (80%)
Source: Table created by reviewing statistician utilizing data provided in: ------------------------------(b)(4)----------------------------------------------
6.1.10.1.1 Demographics

Statistical Reviewer: Tammy Massie, PhD STN: 125473
35
The demographics of the individuals included in this study can be seen in the following table. Within the table the number of individuals and percent of individuals is noted for each treatment group, based on the demographic variables of gender, age, and race. This table illustrates that the baseline characteristics were similar for both treatment groups. Table 6.1.10.1.1 Baseline Demographics of the Patient Population Baseline Demographic 2800 BAU
N=213 Placebo N=225
Total N=438
Gender [n (%)] Female 109 (51) 112 (50) 221 (50) Male 104 (49) 113 (50) 217 (50) Age (years) Range 18 – 63 18 – 61 18 – 63 Race [n (%)]
White/Caucasian 182 (85) 187 (83) 369 (84) Black or African American 21 (10) 21 (9) 42 (10) Asian 4 (2) 9 (4) 13 (3) American Indian/Alaska Native/Pacific Islander 0 (0) 3 (1) 3 (1) Other 6 (3) 5 (2) 11 (3) Source: Table created by reviewing statistician utilizing data provided in:
------------------------------(b)(4)-------------------------------------------
6.1.10.1.2 Medical/Behavioral Characterization of the Enrolled Population The medical/behavioral characteristics of the individuals included in this study can be seen in the following table. Within the table, the mean and standard deviation of various relevant medical/behavioral characteristics are noted for each treatment group based on the BMI, height, and weight. This table illustrates that these characteristics were similar for both treatment groups. Table 6.1.10.1.2 Baseline Medical/Behavioral Characteristics of the Patient Population Baseline Demographic 2800 BAU
N=213 Placebo N=225
Total N=438
BMI (kg/m²) Mean (SD) 27.5 (5.7) 27.9 (6.0) 27.8 (5.9) Range 17-47.8 11.6-48.4 11.6-48.4 Asthma Status [n (%)] Asthmatic 45 (21%) 56 (26%) 104 (24%) Non-Asthmatic 168 (79%) 166 (74%) 334 (76%) Sensitization [n (%)] Grass 213 (100%) 225 (100%) 438 (100%) Other Allergens 181 (85%) 191 (85%) 372 (85%)
Source: Table created by reviewing statistician utilizing data provided in: ------------------------------(b)(4)------------------------------------------
6.1.10.1.3 Subject Disposition

Statistical Reviewer: Tammy Massie, PhD STN: 125473
36
The following figure illustrates the randomization, allocation, and withdrawal of patients for this study. This graphic notes which treatment arm subjects were randomized to and subsequently lists the reason for dropout, including the number of subjects and percentage of subjects that withdrew prior to study completion. It is of interest to note the adverse event rate is slightly higher in the active treatment group; however, other reasons for dropout were fairly similar between the placebo and treatment groups. Table 6.1.10.1.3.1. Patient Disposition through Randomization
Source: Original BLA 125473/000 Clinical Study Report P05238 page 82 The disposition of subjects can be further examined in the following table that illustrates which randomized subjects were followed throughout the entire study period. Considering the tabulation of subjects that discontinued or were lost to follow-up within the study, it appears that the placebo and treated group had similar dropout patterns. Table 6.1.10.1.3.2. Patient Disposition after Randomization

Statistical Reviewer: Tammy Massie, PhD STN: 125473
37
Source: Original BLA 125473/000 Clinical Study Report P05238 page 83
6.1.11 Efficacy Analyses
The applicant proposed and implemented the following efficacy analysis within this study. Primary Efficacy Analysis The primary efficacy variable to address the treatment effect for this study was the Total Combined Score (TCS) based upon the combined (sum of) rhinoconjunctivitis daily symptom score (DSS) and daily medication score (DMS) averaged over the entire Grass Pollen Season (GPS). For the treatment period, the primary efficacy endpoint of the combined (sum of) rhinoconjunctivitis DSS and DMS averaged over the entire GPS was to be evaluated using a linear model with asthma status, study site, and treatment group as fixed effects. This model was to allow for heterogeneous variance estimates for the treatment groups, with appropriate adjustments made. For the primary endpoint, subjects with at least one post-baseline diary record with DSS and DMS within the defined pollen season were to be included. The combined average score was to be based on all available data during the GPS for each subject. A 2-sided 95% confidence interval for the difference in the adjusted means (adjusted for asthma status, and study site) between the two treatment groups was to be presented. Also the difference in adjusted means between the two treatment groups relative to the adjusted mean of the placebo group was to be presented as a percentage with corresponding confidence interval. Secondary Efficacy Analysis The secondary efficacy variable to address the treatment effect for this study was the DSS and DMS. The DSS is composed of six rhinoconjunctivitis symptoms recorded daily, including runny nose, blocked nose, sneezing, itchy nose, gritty feeling/red/itchy eyes, and watery eyes; the symptoms were measured on a scale of 0 (no symptoms) to 3 (severe symptoms), and a higher score indicated a higher level of symptoms. The DMS is

Statistical Reviewer: Tammy Massie, PhD STN: 125473
38
composed of a sum of the scores associated with rescue medication use per day, where a lower medication score indicated less use of rescue medication. The DSS and DMS data were collected during the GPS in which the duration of the GPS was defined as the total number of days for which a subject had data during the GPS. Safety Analysis The safety endpoints (treatment-emergent, treatment-related AEs; local AEs; discontinuations due to AEs) were to be based on the All-Treated set, and were to be summarized by treatment group and asthma status for the frequency distribution (N and percentage).
6.1.11.1 Analyses of Primary Endpoint(s) The primary efficacy endpoint is the Total Combined Score (TCS) during the grass pollen season (GPS) while on treatment. The primary analysis was performed for the Full Analysis Set (FAS), which included all patients who received at least one dose of the investigational product. The TCS was analyzed using a linear model with asthma status, study site, and treatment group as fixed effects and also adjusting for heterogeneous variance between treatment groups. The TCS score was based on all available data during the GPS for each subject within the FAS. A 2-sided 95% confidence interval for the difference in adjusted means between the two treatment groups was provided. Also, the difference in adjusted means between the two treatment groups relative to the adjusted mean of the placebo group was presented as a percentage with corresponding confidence interval. The linear model results for the primary efficacy analysis of the TCS during the pollen period for the FAS are summarized below. The point estimate is the LS Means difference between 2800 BAU and placebo, and the relative LS Means difference is equal to (LS Mean difference/LS Mean for the Placebo group) x 100. For the tables provided in this review the calculations were performed utilizing SAS Proc MIXED, with the specific model noted within the footnotes. If additional methods were used to compute the 95% CI to verify and confirm the robustness of results, the methods are noted in the table footnotes. The mixed model is a combination of fixed and random effects parameters and is written as follows: y=Xβ+Zγ+ε where y denotes the vector of observed yij’s, X is the known matrix of xij’s, β is the unknown fixed effects parameter vector. Z is the known design matrix of zij’s, γ is the

Statistical Reviewer: Tammy Massie, PhD STN: 125473
39
vector of unknown random effects parameters, and ε is the unobserved vector of independent and identically distributed Gaussian random errors. The results in the third and fourth columns of Table 6.1.11.1.a. below are the estimates from the mixed model, including the linear estimate for the contrast vector (L) and the approximate standard error for the LS Mean (computed as the square root of L(X’V-1X)-
1L’, where V is the variance/covariance structure). As an additional method to ensure robustness of results, the reviewing statistician utilized the delta method to estimate the 95% CI for the difference between the treatment and placebo group. Additionally, the reviewing statistician also utilized different variance/covariance structures within the model to ensure robustness of the results of the statistical tests and conclusions drawn from them. These results of statistical analysis of the primary endpoint, which can be seen in the below table, confirmed the applicant’s results and provided an additional analysis supporting the applicant’s conjecture that this product reduces the combined symptom and rescue medication score when compared to placebo. Table 6.1.11.1.a. Primary Efficacy Analysis: ANCOVA of the TCS during the Pollen Period – FAS Treatment
n LS
Mean LS Mean difference vs Placebo
Point Est
LS Mean difference vs
Placebo
95% CI
Relative LS Mean
difference (%)
Point Est
Relative LS Mean
difference (%)
95% CI
Relative LS Mean difference
(%)
95% CI (using the delta
method) Grastek® 184 5.08 -1.31 [-2.22, -0.40] -20% [-33%, -6%] [-34%, -5%]
Placebo 207 6.39 Source: Table created by reviewing statistician utilizing data provided in: -------------------------------(b)(4)--------------------------------------------- Model utilized: ANCOVA with patient/subject ID, pooled (geographically) center, asthma status, and treatment group using SAS: PROC MIXED procedure. As an additional analysis method, the delta method was used to calculate the confidence intervals. The difference in LS means of the daily TCS during the entire grass pollen period between the 3400 BAU group and the Placebo group was statistically significant. The treatment effect was estimated as the difference in LS means of -1.31, corresponding to a relative LS Mean difference of -20% from placebo. The 95% CI expressed as percentages was [-33%, -6%]. Furthermore, utilizing the delta method, the 95% CI expressed as percentages was [-34%, -5%], which does not satisfy CBER’s suggested criterion of meeting a 10% threshold for reduction of combined symptom scores, nor does it meet the applicant’s pre-specified treatment difference of 23%. However, both the point estimate and the upper confidence bound of the 95% CI do suggest a positive trend for reducing treatment symptoms and rescue medication when comparing Grastek® to placebo.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
40
6.1.11.2 Analyses of Secondary Endpoints In addition to the primary endpoint of interest, the total combined symptom and rescue medication score (TCS) during the entire GPS, several secondary endpoints were of interest. These include but are not limited to the daily symptom scores, as well as use of rescue medication during the pre-specified grass pollen season and the TCS during the peak pollen season. Table 6.1.11.2.a. illustrates the difference between the placebo and treatment groups for the entire grass pollen season. Within this table the DDS, and DMS sample size in each treatment arm, point estimate of the LS Mean per treatment arm as well as LS Mean difference, 95% CI of the LS Mean and relative LS Mean Difference are presented. Table 6.1.11.2.a Secondary Efficacy Analysis: ANCOVA of the DDS and DMS during the Grass Pollen Season (GPS) – FAS
Treatment n LS Mean
LS Mean difference vs
Placebo
Point Est (95% CI)
Relative LS Mean difference vs Placebo (%)
Pt Est
Relative LS Mean difference vs Placebo (%)
95% CI
DDS Grastek® 184 3.8 -0.9 18% (-29%, -6%) Placebo 207 4.7 (-1.5, -0.3) DMS
Grastek® 184 1.3 -0.5 -25% (-49, -5%) Placebo 207 1.7 (-1.0, -0.1)
Source: Table created by reviewing statistician utilizing data provided in: -------------------------------(b)(4)--------------------------------------------- Model utilized: ANCOVA with patient/subject ID, pooled (geographically) center, asthma status using SAS Proc MIXED procedure. Table 6.1.11.2.b. illustrates the difference between the placebo and treatment groups for the peak grass pollen season. Within this table the TCS, DDS, and DMS sample size in each treatment arm, point estimate of the LS Mean per treatment arm as well as LS Mean difference, 95% CI of the LS Mean and relative LS Mean Difference are presented. This is a secondary analysis in which the study was not powered to detect differences between treatment groups nor were alpha adjustments made for these hypothesis tests; however, the trends observed within the table suggest that the treatment reduces the symptoms, use of rescue medication, or the combination of both when compared to individuals randomized to the placebo treated group.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
41
Table 6.1.11.2.b. Secondary Efficacy Analysis: ANCOVA of the TCS, DDS and DMS during the Peak Grass Pollen Season – FAS
Treatment n LS Mean
LS Mean difference vs
Placebo
Point Est (95% CI)
Relative LS Mean difference vs Placebo (%)
Pt Est
Relative LS Mean difference vs Placebo (%)
95% CI
TCS Grastek® 184 5.8 -1.6 -21% (-36%, -4%) Placebo 207 7.3 (-2.8, -0.4)
DDS Grastek® 184 4.2 -1.1 -21% (-32%, -7%) Placebo 207 5.2 (-1.8, -0.4) DMS
Grastek® 184 1.6 -0.5 -22% (-50%, 16%) Placebo 207 2.1 (-1.2, 0.3)
Source: Table created by reviewing statistician utilizing data provided in: -------------------------------(b)(4)------------------------------------------ Model utilized: ANCOVA with patient/subject ID, pooled (geographically) center, asthma status using SAS Proc MIXED procedure.
6.1.11.3 Subpopulation Analyses Several subpopulations were of interest to the review team: grass pollen sensitivity, geographic location, and asthma status. Additionally, based on current regulations, there should be analyses based on gender, age, and race. In this study, nearly 85% of the enrolled subjects were Caucasian/white; thus, subgroup analysis of the primary endpoint based on specific races is not expected to be informative. However, comparisons of the treatment response when considering male vs female outcomes as well as those from 18-50 years of age (at study enrollment) versus those 50 to 65 years of age were performed by the reviewing statistician. These results provide consistent positive trends that demonstrate Grastek® reduces total combined symptom and rescue medication scores when compared to placebo. From Figure 6.1.11.3.1 below, it can be seen that there is an observable positive treatment effect for both male and female subjects, but the effect appears to be slightly greater among males. Other comparisons of groups, including sensitivity to grasses, asthma status, and geographic location are presented and illustrate positive trends in the effect of the Grastek® treatment in reducing symptoms.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
42
Figure 6.1.11.3.1. Subpopulation Analysis for Age, Gender, Race, Grass Sensitivity, and Region when examining the TCS during GPS including mean and 95% Confidence Interval
Source: Original BLA 125473/000 Clinical Study Report P05238 page 136 results confirmed by reviewing statistician
6.1.11.4 Dropouts and/or Discontinuations For the average scores of TCS in each of the four study periods (preseason, GPS, peak season, and post-season), there was no imputation of missing diary data. The average score for each subject and study period was based on the available data within the period. However, for rhinoconjunctivitis DMS, if rescue medication use was missing on any single day of the diary card, it was assumed to be “no use,” and a score of zero was assigned in such cases as a convention. For each of the primary and key secondary endpoints of TCS, DSS, and DMS, 11% (24/208) of subjects in the Grastek® group and 8% (18/225) of subjects in the placebo group had no data during GPS. The dropouts in each of the treatment arms were within the expected dropout/missing values suggested within the IND phase of the study (10%). Consistent with the primary analysis methodology, the primary endpoint and two of three key secondary endpoints meet the criterion for declaring significant difference between the active group and placebo group using the non-parametric methods. Sensitivity Analysis based on Missing Values

Statistical Reviewer: Tammy Massie, PhD STN: 125473
43
To see how robust the result is for the primary endpoint when dealing with missing values and other definitions of the pollen season, three different sensitivity analyses were implemented. These analyses included:
1. LOCF (Last Observation Carried Forward) method – Impute any missing daily values of TCS by the last observed non-missing daily value of TCS carried forward until next non-missing daily TCS value is found.
2. Worst Case Scenario – Impute missing values of TCS on a given day by the opposite treatment group’s mean value for TCS in GPS. Thus, a subject in the active group with a missing value in TCS on a given day will have that missing value replaced by the mean TCS value for the placebo group and vice versa.
3. Alternative definition of the pollen season – Instead of using the method described in the protocol to define the pollen season (i.e., first day of 3 consecutive days of pollen counts >=10 grains/m**3 through last day of the last of 3 consecutive days with pollen count >=10 grains/m**3), an alternative approach was explored. This method selected the four weeks, where each week started on Monday and ended on Sunday, with the highest pollen counts in the pollen season.
Analyses of the primary efficacy data utilizing the various imputation methodologies demonstrate consistent positive results with respect to the point estimate, as well as the 95% CI of the relative difference between the active group and placebo group. In the following table, it can be seen that the point estimates for the % relative difference based on the different imputation mechanisms are: -19%, -12%, and -20%. The “worst case scenario” sensitivity analysis does not meet the -10% upper bound for the 95% CI of the relative difference; however, the other imputation methods would have met CBER’s criterion for success.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
44
Figure 6.1.11.4.1. Sensitivity Analysis of Primary Variables during GPS
Source: Original BLA 125473/000 Clinical Study Report P05238 page 2497 results of LOCF and Worst case confirmed by reviewing statistician. Reviewer comment: The proposed treatment of exclusions and missing values is acceptable. In addition, comparisons of missing value rates were made and were deemed comparable for both treatment groups for primary endpoints as well as key secondary endpoints.
6.1.11.5 Exploratory and Post Hoc Analyses The applicant provided a variety of exploratory and post hoc analyses. These analyses included but were not limited to comparisons of combined score, rescue medication score, symptom scores for IgG4, IgE, as well as examination of secondary endpoint analyses over the peak and entire pollen season. A variety of these analyses were confirmed by the reviewing statistician. The analysis of the IgG4 and IgE scores appeared to be positively affected by the use of the active treatment when compared to placebo treated individuals; however, there was a large amount of variability. Additionally, analyses of selected endpoints, time frames, and analysis sets revealed trends in which the active treatment reduced the use of rescue medication, and reduced the severity based on symptom scores of a variety of nasal and oral endpoints. This finding was observed for the full pollen season as well as the peak grass pollen season and for different analysis sets that were available
6.1.12 Safety Analyses
Safety data were collected for the entire study period. Subjects were able to note safety events on the daily diary cards, and also received periodic follow-up from study personnel. Overall, there were slightly more adverse events in the treatment group compared to the placebo group; however, there were no serious adverse events noted in either the treatment or placebo group. A summary of the adverse events can be seen in the applicant’s following Table 6.1.12.a, which includes the number (and percentage) of subjects experiencing adverse events, stratified by the treatment group (confirmed via JMP tabulations by the reviewing statistician).

Statistical Reviewer: Tammy Massie, PhD STN: 125473
45
Table 6.1.12.a. Summary of Adverse Events Observed in the Treated and Placebo Groups during the Entire Study Period
Source: Original BLA 125473/000 Clinical Study Report P05238 page 145 (confirmed by reviewing statistician). A summary of the types of serious adverse events observed during the study can be seen in the following table that was confirmed by the reviewing statistician via JMP. Within Table 6.1.12.b shows that 9 patients had SAEs in the Placebo group and 7 patients had SAEs within the Grastek® group. Additionally, other less serious adverse events are included within the table, showing similar trends in adverse events occurring in both the active treated and placebo treatment groups.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
46
Table 6.1.12.b. Summary of Serious Adverse Events
Source: Original BLA 125473/000 Clinical Study Report P05238 Section 12.2.1.1 Table 36 Page 146, results confirmed by reviewing statistician.
Additional details related to safety events can be seen in the medical officer’s and epidemiologist’s reviews. Reviewer’s comment: Overall, the treatment group had slightly more adverse events than the placebo; however, as an active treatment designed to elicit a response via the

Statistical Reviewer: Tammy Massie, PhD STN: 125473
47
product instead of the pollens during the pollen season, this finding is not surprising. Additional and more detailed comments can be found in the medical officer’s and epidemiologist’s reviews.
6.1.12.1 Methods The safety data analysis consisted of examining observed Adverse Events provided by the applicant. Tabulations were utilized to compare the effect of treatment versus placebo on the observation of adverse events. No pre-specified hypothesis tests were to be performed for either organ classes or specific adverse events. For further details and additional discussion, the statistician defers to the medical officer.
6.1.12.3 Deaths One death was observed in this study but was considered by the applicant as well as the medical officer to be unrelated to study drug, as the subject suffered a multiple drug overdose of non-study drugs several months after the study drug was discontinued. Further details and discussion can be found in the medical officer’s review.
6.1.12.4 Nonfatal Serious Adverse Events No important findings were noted in the 16 observed non-fatal serious adverse events. The number of SAE’s were fairly balanced between the two treatment groups: 9 placebo and 7 active treatment, representing less than 5% of study subjects. Furthermore, all serious adverse events were self-limiting and were resolved upon discontinuation of study treatment. For further details and additional discussion, please refer to the medical officer’s review.
6.1.12.5 Adverse Events of Special Interest (AESI) The statistician defers to the medical officer.
6.1.12.6 Clinical Test Results Clinical test results including IgG, IgE, and other tests performed throughout the study had results that were expected and not considered outside of normal ranges. For further details and additional discussion, the reviewing statistician defers to the medical officer.
6.1.12.7 Dropouts and/or Discontinuations
A total of 43 subjects prematurely withdrew from the study: 17 (7.1%) from the placebo group and 11 (11.2%) from the study drug group. Two of the dropouts in the placebo group and 15 subjects in the study drug group withdrew because of AEs.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
48
Summary and conclusion: Although Study P05238 did not meet its objectives with respect to the primary efficacy endpoint, this study provided supportive evidence that this product reduces the TCS, DDS, and DMS scores when comparing Grastek® treated individuals to those treated with placebo. The safety profile of Grastek® in this study appears to be acceptable, with only 16 documented serious adverse events that were all self-limiting, resolved, and had comparable rates when considering the placebo versus Grastek® treated subjects. One death occurred due to ingestion of multiple drugs including hydrocodone, meprobamate, and carisoprodol; the subject had not taken study medication for approximately 1 month prior to the event. Furthermore, the adverse events observed during the study treatment period were similar to other similar allergenic products or those experiencing symptoms related to exposure to the grass allergens.
6.2 Trial #2: P05239-US and Canadian Pediatric Phase III Field Study Merck’s trial P05239 was submitted to CBER under US-IND to be “a multi-center, double-blind, randomized, placebo controlled, parallel-group study evaluating the efficacy and safety of grass (Phleum Pratense) sublingual tablet (SCH 697243) in children 5 to <18 years of age with a history of grass pollen induced rhinoconjunctivitis with or without asthma.”
6.2.1 Objectives (Primary, Secondary, etc.)
The objectives of this study were to evaluate the efficacy and safety of sublingual tablets of grass pollen allergen extract compared with placebo for reduction of rhinoconjunctivitis symptoms and rescue medication usage. Primary Objective: To evaluate the efficacy of grass sublingual tablet (Grastek®) versus placebo in the treatment of grass pollen-induced rhinoconjunctivitis based on the combined sum (CS) of rhinoconjunctivitis daily symptom score (DSS) and rhinoconjunctivitis daily medication score (DMS) averaged over the entire grass pollen season (GPS). Key Secondary Objectives: To assess overall safety and to compare the following between the Grastek® and placebo groups:
• The average rhinoconjunctivitis DSS for the entire GPS.
• The average rhinoconjunctivitis DMS for the entire GPS.
• The average weekly rhinoconjunctivitis quality of life total score for the entire GPS.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
49
6.2.2 Design Overview
This was a multicenter, double-blind, randomized, placebo-controlled, parallel-group study in subjects 5 to <18 years of age, of either sex and of any race with a history of grass pollen-induced rhinoconjunctivitis with or without asthma. There was an observational grass pollen season period in year 2008 where no investigational medicinal product (IMP) was administered and a second year in 2009 in which the experimental treatment was administered. Open-label rescue medications for the rhinoconjunctivitis and asthma symptoms were provided during this first year. Eligible subjects were to visit the study site for at least 6 visits: Screening, Post-screening, Pre-season, On-season, End-of-season, and Off-season Visits, and at Unscheduled Visits as appropriate. Additional Off-season Visits were scheduled depending on the timing of the Randomization Visit in relation to the anticipated start of the Grass Pollen Season (GPS). Qualified subjects were to be randomized into the treatment period. In the treatment period, the subjects were treated once daily with either Grastek® (Timothy grass allergy immunotherapy tablet [grass AIT]) or placebo for approximately 16 weeks prior to the GPS and during the GPS. At the Randomization Visit, subjects were supplied with self-injectable epinephrine together with instructions on how and when to use it. Open-label rescue medications for the rhinoconjunctivitis and asthma symptoms were to be provided. Subjects were to visit the study site for at least 9 visits: Screening (2 visits), Randomization (3 visits), Off-season, Pre-season, On-season, and End-of-season Visits, and at Unscheduled Visits as appropriate. The first three consecutive daily doses of IMP were administered at the study site, and the subjects were monitored at the site for 30 minutes following dosing. Subsequent administration of IMP was done once daily at home at approximately the same time each day. A telephone contact between the investigator/designee and the subject occurred once daily for the first 4 days of at-home administration of IMP to monitor adverse events (AEs) and once approximately 1 week after the End-of-season Visit. A summary of the study visits and data collection points for this study are illustrated in the following study design diagram.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
50
Figure 6.2.2.a. Study Design Diagram
Source: Original BLA 125473/000 Clinical Study Report P05239 page 35 This study was conducted in conformity with Good Clinical Practice. A data safety monitoring committee (DSMC) was established prior to the start of the treatment period. The purpose of the DSMC was to evaluate adverse event data and to provide recommendations regarding the conduct of the study to ensure the safety of the subjects.
6.2.3 Population
The treatment population consisted of male and female patients aged 5 to <18 years in the United States and Canada with documented grass pollen-related allergic rhinoconjunctivitis, based on a clinical history of significant allergenic rhinoconjunctivitis to grass (with or without asthma) diagnosed by a physician and who had received treatment for their disease for the previous grass pollen season, had a positive SPT to Timothy grass (wheal diameter ≥ 5 mm, greater than the negative control), and were positive for specific IgE against Phleum pratense (≥ IgE Class 2; ≥ 0.7 kAU/L) at the screening visit.
6.2.4 Study Treatments or Agents Mandated by the Protocol
In this study, two treatments were to be examined and compared: 2800 BAU Grastek® tablets and Placebo tablets that matched the 2800 BAU Grastek® tablets. Both the active treatment and placebo were to be administered sublingually (under the tongue) every day at the same time during the approximate 4 to 6-month treatment period, depending on the location of the treatment site.
6.2.6 Sites and Centers
This study was to include 52 centers in various locations within the United States and 10 centers within Canada with expected exposure to grass pollen.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
51
6.2.7 Surveillance/Monitoring
A detailed synopsis of the surveillance and monitoring of the study can be found in the medical officer’s and epidemiologist’s reviews. However, a data safety monitoring committee (DSMC) was set up to ensure adequate safety monitoring of the study, with pre-specified plans to examine and stop the study in case of unexpected safety issues.
6.2.8 Endpoints and Criteria for Study Success
There are several primary and secondary endpoints in this study that were utilized to assess how well the Grastek® product reduced symptoms related to grass allergies, as well as reduced the need to take medications to treat or prevent symptoms associated with grass allergies. The primary criterion for success was the combined symptom score (CS), which consisted of the patient’s daily symptom scores (DSS) and daily rescue medication scores (DMS). A comprehensive summary of the endpoints and criteria for study success can be seen in Section 6.1.8., an adult study that was nearly identical to this pediatric study.
6.2.9 Statistical Considerations & Statistical Analysis Plan
Analysis sets: For the purpose of this study, three analysis sets were defined, namely, the Safety Set, the Full Analysis Set (FAS), and the Per Protocol Analysis Set (PPS). A comprehensive summary of the analysis for this study can be seen in Section 6.1.9., an adult study that was nearly identical to this pediatric study.
6.2.10 Study Population and Disposition
The study population and baseline demographics of the enrolled patients are similar for both treatment groups. In this study, 344 patients were randomized to treatment.
6.2.10.1 Populations Enrolled/Analyzed The following table displays the population distribution in study P05239.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
52
Table 6.2.10.1.1. Summary of Patient Population Grastek® 2800 BAU
N (%) Placebo N (%)
Total N (%)
Patients Randomized 175 (100%)
169 (100%)
344 (100%)
Patients in Safety Set 175 (100%)
169 (100%)
344 (100%)
Patients in Full Analysis Set 175 (100%)
169 (100%)
344 (100%)
Protocol Evaluable Data Set 135 (77%)
124 (73%)
259 (75%)
Source: Table created by reviewing statistician utilizing data provided in: -------------------------------(b)(4)-------------------------------------------- 6.2.10.1.1 Demographics The demographics of the individuals included in this study can be seen in the following table. The number and percentage of individuals are noted for each treatment group based on the demographic variables of gender, age, and race. This table shows that the baseline characteristics were similar for both treatment groups. Table 6.2.10.1.1 Baseline Demographics of the Patient Population
Baseline Demographic Grastek® N=175
Placebo N=169
Total N=344
Gender [n (%)]
Female 57 (33%) 64 (38%) 121 (35%) Male 118 (67%) 105 (62%) 223 (65%) Age (years) Mean (SD) 12.1 (3.0) 12.6 (3.0) 12.3 (3.0) Range 6-17 5-18 5-18 Race [n (%)]
White/Caucasian 153 (87%) 149 (88%) 302 (88%) Black or African American 12 (7%) 13 (8%) 25 (7%) Asian 5 (3%) 1 (1%) 6 (2%) American Indian/Alaska Native/Pacific Islander 1 (1%) 1 (1%) 2 (1%) Other 4 (2%) 5 (3%) 9 (3%)
Source: Table created by reviewing statistician utilizing data provided in: -------------------------------(b)(4)-------------------------------------------- 6.2.10.1.2 Medical/Behavioral Characterization of the Enrolled Population The medical/behavioral characteristics of the individuals included in this study can be seen in the following table. The mean and standard deviation of various relevant medical/behavioral characteristics are noted for each treatment group based on the BMI, height, and weight. This table reveals that these characteristics were similar for both treatment groups.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
53
Table 6.2.10.1.2 Baseline Medical/Behavioral Characteristics of the Patient Population Baseline Demographic Grastek®
N=175 Placebo N=169
Total N=344
BMI (kg/m²) Mean (SD) 20.3 (5.0) 20.7 (4.2) 20.5 (4.6) Range 13.5-48.8 13.8-37.1 13.5-48.8 Asthma Status [n (%)] Asthmatic 46 (26%) 44 (26%) 90 (26%) Non-Asthmatic 129 (74%) 125 (74%) 254 (74%) Sensitization [n (%)] Grass 174 (99%) 168 (99%) 342 (99%) Other Allergens 152 (87%) 154 (91%) 306 (89%)
Source: Table created by reviewing statistician utilizing data provided in: -------------------------------(b)(4)-------------------------------------------- 6.2.10.1.3 Subject Disposition The following figure illustrates the randomization, allocation, and withdrawal of patients for this study. This graphic notes which treatment arm subjects were randomized to and subsequently lists the reason for dropout, including the number of subjects and percentage of subjects that withdrew prior to study completion. It is of interest to note the adverse event rate is slightly higher in the active treatment group; however, other reasons for dropout were fairly similar between the placebo and treatment groups.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
54
Table 6.2.10.1.3.1. Patient Disposition through Randomization
Source: Original BLA 125473/000 Clinical Study Report P05239 page 85 The disposition of subjects can be further examined in the following table that shows which randomized subjects were followed throughout the entire study period. Considering the tabulation of subjects that discontinued or were lost to follow-up within the study, it appears that the placebo and treated group had similar dropout patterns.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
55
Table 6.2.10.1.3.2. Patient Disposition after Randomization
Source: Original BLA 125473/000 Clinical Study Report P05239 page 88
6.2.11 Efficacy Analyses
The applicant proposed and implemented the following efficacy analyses within this study. Primary Efficacy Analysis The primary efficacy variable to address the treatment effect for this study was the Total Combined Score (TCS) based upon the combined (sum of) rhinoconjunctivitis daily symptom score (DSS) and daily medication score (DMS) averaged over the entire Grass Pollen Season (GPS). A more detailed and comprehensive summary of the analysis and criteria for study success for the primary efficacy, secondary efficacy, and safety analysis can be seen in Section 6.1.11, the adult study that was nearly identical to this pediatric study.
6.2.11.1 Analyses of Primary Endpoint(s) The primary efficacy endpoint is the Total Combined Score (CS) during the grass pollen season (GPS) while on treatment. The primary analysis was performed for the Full Analysis Set (FAS), which included all patients who received at least one dose of the investigational product. The TCS was analyzed using a linear model with asthma status, study site, and treatment group as fixed effects and also adjusting for heterogeneous variance between treatment groups. The TCS score will be based on all available data during the GPS for each subject within the FAS. A comprehensive and detailed summary of the endpoints and analyses as well as the criteria for study success can be seen in Section 6.1.11.1., an adult study that was nearly identical to this pediatric study. These results of statistical analysis of the primary endpoint comparing the TCS scores of the Grastek® treated group versus the placebo group can be seen in the below table.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
56
These results confirmed the applicant’s results and provided an additional analysis supporting the applicant’s conjecture that the Grastek® product reduces the total combined symptom and rescue medication score when compared to placebo. Table 6.2.11.1.a. Primary Efficacy Analysis: ANCOVA of the TCS during the Grass Pollen Season – FAS Treatment
n LS
Mean LS Mean difference vs Placebo
Point Est
LS Mean difference vs
Placebo
95% CI
Relative LS Mean
difference (%)
Point Est
Relative LS Mean
difference (%)
95% CI
Relative LS Mean difference
(%)
95% CI (using the delta
method) Grastek® 149 4.62 -1.63 [-2.60, -0.66] -26% [-38%, -10%] [-37.%, -11%]
Placebo 158 6.25 Source: Table created by reviewing statistician utilizing data provided in: -------------------------------(b)(4)------------------------------------------ Model utilized: ANCOVA with patient/subject ID, pooled (geographically) center, asthma status. SAS: PROC MIXED with repeated effect based on Subject and Compound Symmetry as Variance/Covariance structure. As an additional analysis method, the delta method was used to calculate the confidence intervals. The difference in LS means of the daily TCS during the entire grass pollen period between the Grastek® group and the Placebo group was statistically significant. The treatment effect was estimated as the difference in LS means of -1.63, corresponding to a relative LS Mean difference of -26% from placebo. The 95% CI expressed as percentages was [-38%, -10%]. Furthermore, utilizing the delta method, the 95% CI expressed as percentages was [-37%, -11%], which satisfies CBER’s suggested criterion of meeting a 10% threshold for reduction of combined symptom scores, and it also meets the applicant’s pre-specified treatment difference of 20%. The positive effect of the treatment in reduction of TCS scores compared to placebo were obtained with other variance/covariance structures, including AR(1), as well as other methods for estimation including Fieller’s method, when considering data analyzed from this pediatric study, P05239.
6.2.11.2 Analyses of Secondary Endpoints In addition to the primary endpoint of interest, the total combined symptom and rescue medication score (TCS) during the entire GPS, several secondary endpoints were of interest. These include but are not limited to the daily symptom scores (DDS) as well as use of rescue medication (DMS) during the pre-specified grass pollen season as well as the TCS during the peak pollen season.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
57
Table 6.2.11.2.a Secondary Efficacy Analysis: ANCOVA of the DDS and DMS during the Grass Pollen Season (GPS) – FAS
Treatment n LS Mean
LS Mean difference vs
Placebo
Point Est (95% CI)
Relative LS Mean difference vs Placebo (%)
Pt Est
Relative LS Mean difference vs Placebo (%)
95% CI
DDS Grastek® 149 3.7 -1.2 -25% (-36%, -9%) Placebo 158 4.9 (-1.95, -0.5) DMS
Grastek® 149 0.9 -0.4 -32% (-58, -4%) Placebo 158 1.3 (-0.9, 0.0*)
Source: Table created by reviewing statistician utilizing data provided in: -------------------------------(b)(4)------------------------------------------ Model utilized: ANCOVA with patient/subject ID, pooled (geographically) center, asthma status. SAS: PROC MIXED with repeated effect based on Subject and Compound Symmetry as Variance/Covariance structure. (*): the computed value is 0.03, not 0, Table 6.2.11.2.c illustrates the difference between the placebo and treatment groups for the peak grass pollen season. Within this table the TCS, DDS, and DMS, sample size in each treatment arm, point estimate of the LS Mean per treatment arm, as well as LS Mean difference, Relative LS Mean Difference, and 95% CI for the Relative LS Mean Difference are presented. This is a secondary analysis in which the study was not powered to detect differences between treatment groups, nor were alpha adjustments made for these hypothesis tests; however, the trends observed within the table indicate that the treatment reduces the symptoms, use of rescue medication or the combination of both when compared to individuals randomized to the placebo treated group. Table 6.2.11.2.c Secondary Efficacy Analysis: ANCOVA of the TCS, DDS and DMS during the Peak Grass Pollen Season – FAS
Treatment n LS Mean
LS Mean difference vs
Placebo
Point Est (95% CI)
Relative LS Mean difference vs Placebo (%)
Pt Est
Relative LS Mean difference vs Placebo (%)
95% CI
TCS Grastek® 147 4.7 -2.1 -31% (-48%, -14%) Placebo 153 6.9 (-3.3, -0.9)
DDS Grastek® 147 3.8 -1.5 -28% (-43%, -13%) Placebo 153 5.3 (-2.3, -0.7) DMS
Grastek® 147 0.9 -0.5 -41% (-81%, 0%) Placebo 153 1.6 (-1.3, 0.0)
Source: Table created by reviewing statistician utilizing data provided in: ------------------------------(b)(4)------------------------------------------- Model utilized: ANCOVA with patient/subject ID, pooled (geographically) center, asthma status. SAS: PROC MIXED with repeated effect based on Subject and Compound Symmetry as Variance/Covariance structure.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
58
6.2.11.3 Subpopulation Analyses Several subpopulations were of interest to the review team: grass pollen sensitivity, geographic location, and asthma status. Additionally, based on current regulations, there should be subgroup analyses based on gender, age, and race. In this study, nearly 90% of the enrolled subjects were Caucasian/white; thus, subgroup analysis of the primary endpoint based on specific races is not necessarily informative. However, comparisons of the treatment response when considering male vs female outcomes, as well as those from 5 to <12 years of age (at study enrollment) versus those 12 to 18 years of age were performed by the reviewing statistician, confirming the results presented by the applicant. These results provide consistent positive trends that demonstrate Grastek® reduces total combined symptom and rescue medication scores when compared to placebo. From the graphic below, there is an observable positive treatment effect for both male and female subjects, but the effect appears to be slightly greater among males. Other comparisons of groups including sensitivity to grasses, asthma status, and geographic location are presented and illustrate positive trends in the effect of the Grastek® treatment in reducing symptoms. Figure 6.2.11.3.1. Subpopulation Analysis for Age, Gender, Race, Grass Sensitivity, and Region when examining the TCS during GPS, including mean and 95% Confidence Interval
Source: Original BLA 125473/000 Clinical Study Report P05239 page 141 results confirmed by reviewing statistician

Statistical Reviewer: Tammy Massie, PhD STN: 125473
59
6.2.11.4 Dropouts and/or Discontinuations For the average scores of TCS in each of the four study periods (pre-season, GPS, peak season, and post-season), there was no imputation of missing diary data. The average score for each subject and study period was based on the available data in the period. However, for rhinoconjunctivitis DMS, if rescue medication use was missing on any single day of the diary card, it was assumed to be “no use” and a score of zero was assigned in such cases as a convention. For each of the primary and key secondary endpoints of TCS, DSS, and DMS, 14% (24/173) of subjects in the Grastek® group and 9% (9/167) of subjects in the placebo group had no data recorded during the Grass Pollen Season (GPS). The dropouts in each of the treatment arms were within the expected dropout/missing values anticipated during the IND phase of the study (15%). Although there is a slight imbalance in the missing values in treatment arms, sensitivity analyses were performed to determine if the missing values may have influenced the results and conclusions (see below). The primary endpoint and two of three key secondary endpoints met the criterion for declaring that there was a statistically significant and clinically meaningful difference between the active group and placebo group. Sensitivity Analyses based on Missing Values To see how robust the result is for the primary endpoint when dealing with missing values and other definitions of the pollen season, three different sensitivity analyses were employed. These analyses included:
1. LOCF (Last Observation Carried Forward) method – Impute any missing daily value of TCS by the last observed non-missing daily value of TCS carried forward until next non-missing daily TCS value is found.
2. Worst Case Scenario – Impute missing values of TCS on a given day by the opposite treatment group’s mean value for TCS in GPS. Thus, a subject in the active group with a missing value in TCS on a given day will have that missing value replaced by the mean TCS value for the placebo group and vice versa.
3. Alternative definition of the pollen season – Instead of using the method described in the protocol to define the pollen season (i.e., first day of 3 consecutive days of pollen counts >=10 grains/m**3 through last day of the last of 3 consecutive days with pollen count >=10 grains/m**3), an alternative approach was explored. This method selected the four weeks, where each week starts on Monday and ends on Sunday, with the highest pollen counts in the pollen season.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
60
Analyses of the primary efficacy data utilizing the various imputation methodologies demonstrate consistent positive results with respect to the point estimate, as well as the 95% CI of the relative difference between the active group and placebo group. In the following table, it can be seen that the point estimate for each of the imputation mechanisms described above are: -26%, -14%, and -32%. The “worst case scenario” sensitivity analysis does not meet the -10% upper bound for the 95% CI of the relative difference; however, the other imputation methods would have met CBER’s criterion for success. Figure 6.2.11.4.1. Sensitivity Analysis of Primary Variables during GPS
Source: Original BLA 125473/000 Clinical Study Report P05239 page 2238 results of LOCF and Worst case confirmed by reviewing statistician. Reviewer comment: The proposed treatment of exclusions and missing values was deemed acceptable to the reviewing statistician. Comparisons of missing value rates were made and revealed slight differences between the treatment groups. However, sensitivity analyses demonstrated similar trends and conclusions for the primary endpoint and key secondary endpoints, supporting the contention that the Grastek® product improves the TCS scores when compared to placebo treated individuals.
6.2.11.5 Exploratory and Post Hoc Analyses The applicant provided a variety of exploratory and post hoc analyses. These analyses included but were not limited to comparisons of combined score, rescue medication score, symptom scores for IgG4, IgE, as well as examination of secondary endpoints over the peak and entire pollen season. A variety of these analyses were confirmed by the reviewing statistician. The analyses of the IgG4 and IgE scores suggested that these scores were positively affected by the use of the active treatment when compared to placebo treated individuals; however, there was a large amount of variability. Additionally, analyses of selected endpoints, time frames, and analysis sets confirmed the trends observed in which the active treatment reduced the use of rescue medication, and reduced the severity based on symptom scores of a variety of nasal and oral endpoints. This finding was observed for the full pollen season as well as the peak grass pollen season and for different analysis sets that were available
6.2.12 Safety Analyses
Safety data were collected for the entire study period. Subjects were able to note safety events on the daily diary cards, and also received periodic follow-up from study personnel. Overall, there were slightly more adverse events in the treatment group compared to the placebo group; however, there were no serious adverse events noted in
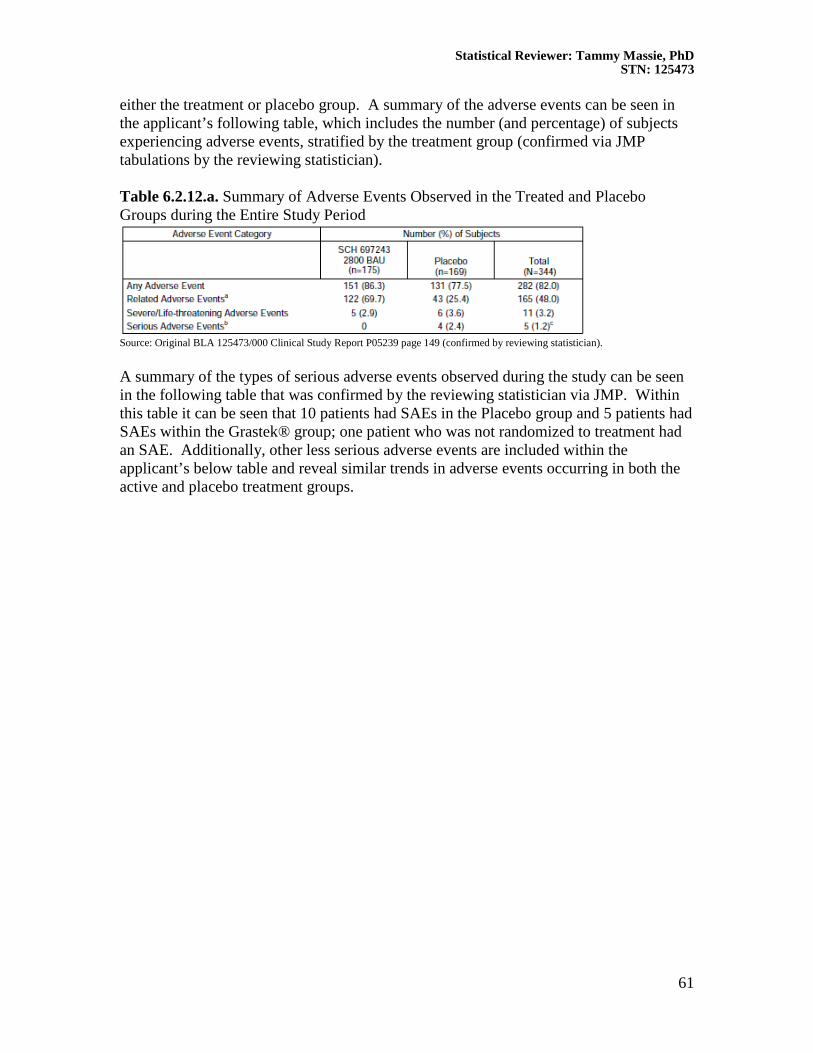
Statistical Reviewer: Tammy Massie, PhD STN: 125473
61
either the treatment or placebo group. A summary of the adverse events can be seen in the applicant’s following table, which includes the number (and percentage) of subjects experiencing adverse events, stratified by the treatment group (confirmed via JMP tabulations by the reviewing statistician). Table 6.2.12.a. Summary of Adverse Events Observed in the Treated and Placebo Groups during the Entire Study Period
Source: Original BLA 125473/000 Clinical Study Report P05239 page 149 (confirmed by reviewing statistician). A summary of the types of serious adverse events observed during the study can be seen in the following table that was confirmed by the reviewing statistician via JMP. Within this table it can be seen that 10 patients had SAEs in the Placebo group and 5 patients had SAEs within the Grastek® group; one patient who was not randomized to treatment had an SAE. Additionally, other less serious adverse events are included within the applicant’s below table and reveal similar trends in adverse events occurring in both the active and placebo treatment groups.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
62
Table 6.2.12.b. Summary of Serious Adverse Events
Source: Original BLA 125473/000 Clinical Study Report P05239 Page 150, results confirmed by reviewing statistician.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
63
Additional details related to safety events can be seen in the medical officer’s and epidemiologist’s reviews. Reviewers comment: Overall, the treatment group had slightly more adverse events than the placebo; however, as an active treatment designed to elicit a response via the product instead of the pollens during the pollen season, this finding is not surprising. Additional and more detailed comments can be found in the medical officer’s and epidemiologist’s reviews.
6.2.12.1 Methods The safety data analysis consisted of examining observed Adverse Events provided by the applicant. Tabulations of adverse events were utilized to compare the effect of treatment versus placebo on the observation of adverse events. No pre-specified hypothesis tests were to be performed for either organ classes or specific adverse events. For further details and additional discussion, the reviewing statistician defers to the medical officer.
6.2.12.3 Deaths No deaths were observed in this study.
6.2.12.4 Nonfatal Serious Adverse Events No important findings were noted in the 16 observed non-fatal serious adverse events. The number of SAE’s were fairly balanced between the two treatment groups: 9 placebo and 7 active treatment, representing less than 5% of study subjects. Furthermore, all serious adverse events were self-limiting and were resolved upon discontinuation of study treatment. For further details and additional discussion, please refer to the medical officer’s review.
6.2.12.5 Adverse Events of Special Interest (AESI) The statistician defers to the medical officer.
6.2.12.6 Clinical Test Results Clinical tests including IgG, IgE, and other tests performed throughout the study had results that were expected and not considered outside of normal ranges. For further details and additional discussion, the statistician defers to the medical officer.
6.2.12.7 Dropouts and/or Discontinuations

Statistical Reviewer: Tammy Massie, PhD STN: 125473
64
A total of 19 subjects (4.7%) discontinued from the treatment period due to AEs; a slightly higher number of subjects in the Grastek® group (13 subjects [7.4%] than in the placebo group (5 subjects [3%]) discontinued from the trial due to an AE. In addition, one subject not randomized to any treatment also discontinued from the study due to an adverse event. Summary and conclusion: Study P05239 met its objectives with respect to the primary efficacy endpoint based on an acceptable point estimate of a 26% reduction in combined symptom and rescue medication scores (TCS). The study also met CBER’s criterion for efficacy based on a clinically meaningful difference defined as an upper bound of the 95% CI of at least -10% (observed to be -14% in this study). Additionally, this study provided supportive evidence that this product does reduce the TCS, DDS, and DMS scores when comparing Grastek® treated individuals to those treated with placebo. The safety profile of Grastek® in this study appears to be acceptable, with only 16 total documented serious adverse events (including one patient that had not received any treatment) that were all self-limiting, resolved, and had comparable rates between the placebo and Grastek® treated subjects. No deaths occurred in this study. Furthermore, the adverse events observed during the study treatment period were consistent with those elicited by other similar allergenic products or symptoms related to exposure to the grass allergens.
7. INTEGRATED OVERVIEW OF EFFICACY The following section summarizes the totality of evidence from all studies submitted by the applicant to this BLA. Based on the results presented by the applicant and confirmed by the reviewing statistician, it appears that this product reduces daily symptom scores, reduces the use of daily rescue medication, and reduces the combined symptom score that incorporates both the daily allergic symptoms as well as the use of rescue medication.
7.1 Indication #1 Based on the applicant provided Label and Package Insert, the following is the proposed indication for this product: MK-7243 is indicated for the disease modifying treatment of diagnosed Timothy and related grass pollen induced allergic rhinitis, with or without conjunctivitis, in adults and children 5 years of age and older.
7.1.1 Methods of Integration
Overall, approximately 2000 subjects 18 to 65 years of age and nearly 500 children 5-18 years of age participated in the clinical development program of MK-7243, which consisted of fourteen clinical trials. The effectiveness and safety of MK-7243 was evaluated in the following clinical trials from Phase I to Phase III:
• Five Phase 1 trials (GT-01, GT-03, and GT-04 in adults; GT-09 and GT-11 in children);

Statistical Reviewer: Tammy Massie, PhD STN: 125473
65
• One Phase 2 safety and efficacy trial in adults with AR and asthma (GT-07); • One dose-finding Phase 2/3 efficacy and safety trial in adults (GT-02); and • Six Phase 3 efficacy and safety trials (GT-08 in adults in Europe, GT-14 in adults
in the US, P05238 in adults in North America, GT-12 and P05239 in children in Germany and North America, respectively, and P08067 in adults/children in North America).
The majority of these studies were performed over one allergy season. However, a single long-term extension over several allergy seasons within the Phase 3 adult GT-08 trial was conducted over up to 5 years and was completed in 2009; data from the 3 treatment years and the 2 follow-up years are included in the applicant provided submission. A summary of the thirteen efficacy studies, including the purpose of the study and number of patients exposed to various doses of the Merck Grastek® product, is provided in the table below.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
66
Table 7.1.1.a. Efficacy Studies provided within the BLA for Merck’s Grastek®
Source: Original BLA 125473/000 Clinical Overview page 20-21 From the above table and previously examined studies in this review, it can be seen that the majority of the studies of this product consisted of natural exposure field studies after 2-4 months of treatment over one grass pollen season. The primary measure of efficacy, as per CBER Standards, is the (CS) combined score, which incorporates both the rescue medication score and the rhinoconjunctivitis symptom score during the pollen season. It is important to note that since many of these studies were performed internationally and not under US-IND, the pre-specified primary efficacy endpoints varied among studies. Integration of results was to incorporate both the primary endpoints as well as secondary endpoints of the various studies in order to utilize and compare the TCS as the primary

Statistical Reviewer: Tammy Massie, PhD STN: 125473
67
efficacy endpoint. Furthermore, the clinically meaningful difference was to be set utilizing the US standard, based on the May 2011 Advisory Committee agreed upon standard of -10% as the clinically meaningful upper bound for the % difference between treatment and placebo responses in the TCS endpoint. The following table provides a summary of endpoints based on protocols submitted by the applicant and consists of all studies considered within the integrated study of efficacy. This table includes a listing of primary and key secondary endpoints, the study, as well as the type of analysis performed. Table 7.1.1.b. Summary of Endpoints based on Protocols submitted by Merck and considered for the Integrated Study of Efficacy for Grastek® Endpoint Adults
Phase 3 Trials GT-08
Adults Phase 3 Trials P05238
Adults Phase 3 Trials GT-14
Adults Phase 2 Trials GT-02
Adults Phase 2 Trials GT-07
Pediatrics Phase 3 Trials GT-12
Pediatrics Phase 3 Trials P05239
Adult & Pediatrics Phase 3 Trial P08067
TCS entire GPS TCS peak GPS
S P S
S S
S S
P P KS
DSS entire GPS DSS peak GPS
P S
KS S
P S
P KS
S P KS
KS S
KS S
DMS entire GPS DMS peak GPS
P S
KS S
KS S
P KS
S P KS
KS S
KS S
RQLQ entire GPS RQLQ peak GPS*
S KS KS KS KS
Notes: DSS=daily symptom score; DMS=daily medication score; GPS=grass pollen season; P=primary; KS=key secondary; S=secondary; RQLQ= Rhinoconjunctivitis Quality of Life Questionnaire; TCS=total combined score
*for subjects ≥12 years of age Source: Statistical Summary based on SAPs provided in BLA 125473/000
In all studies, the primary efficacy endpoint (i.e., the symptom score or symptom/rescue medication score) was analyzed using a linear model, specifically an ANCOVA with treatment as main effect, pooled study center/geographic location as stratification factor for the multicenter studies, and several covariates (including: baseline symptom, baseline rescue medication scores, asthma status, and potentially other covariates depending on study) which could potentially impact the clinical score.
7.1.2 Demographics and Baseline Characteristics
Across studies, no notable differences in demographic characteristics were observed between the active and placebo treatment groups. The racial profile of subjects was predominantly white/Caucasian (85-90%) in all studies performed by the applicant. In various studies, the distribution of gender did slightly differ, as can be seen in the below table (in which males tended to be more predominant, with 52% to 62% of participants and females varied from 38% to 48% of participants); however, between the randomized treatment groups, no imbalances were noted. Specific details related to demographic and baseline characteristics can be seen in the following table, which examines the number and percentage of individuals in the Full Analysis set stratified by treatment group, age, gender, race/ethnicity, BMI, asthma status, sensitivity to grass pollens, and baseline retrospective symptom scores.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
68
Table 7.1.2.a. Summary of Demographic and Baseline Characteristics
Source: Original BLA 125473/000 Clinical Overview page 68-71

Statistical Reviewer: Tammy Massie, PhD STN: 125473
69
7.1.3 Analysis of Primary Endpoint(s)
Considering the results of the primary and secondary analyses (depending on the study examined), it can be seen that when comparing the study treatment at a dose of Grastek® to placebo, the study treatment group had a lower point estimate of TCS than placebo. The primary efficacy endpoint (dependent variable), TCS score, was analyzed using a linear model, specifically an ANCOVA with treatment as main effect, pooled study center as stratification factor for the multicenter studies, and several covariates (including: baseline symptom/rescue medication scores, asthma status, and other covariates-depending on the study) which could potentially impact the clinical score. It is important to note that each study utilized its own statistical model that was pre-specified in the protocol rather than a common model for all the studies. The table below summarizes the difference in LS Means (and 95% CI) of the treated group versus placebo as well as the relative LS Mean difference (and 95% CI) utilizing the TCS endpoint for all of the field studies that collected efficacy data provided in this submission. The results demonstrate that the treatment (particularly the dosage proposed of 2800 BAU Grastek®) reduces the TCS score when compared to placebo, based on both the point estimate of the difference as well as the 95% CI considering the LS Mean values. Across the trials a consistent trend in favor of Grastek® was observed, with some variation in overall magnitude of effect as expected in seasonal allergic rhinitis trials. One trial did not achieve statistical significance over placebo (GT-14 Trial), although the numerical trends in the results favored treatment with Grastek®. As a consequence of this study which did not meet the pre-specified success criterion, Merck conducted three additional trials (P05238, P05239, and P08067) in North America. The last trial was powered based on the upper 95% confidence limit of the relative difference in scores between placebo and Grastek® groups being no less than -10%, yielding a study of approximately 1500 individuals. Although results of the first two trials were statistically significant, the adult study did not meet CBER’s criterion stated in the May 2011 Allergenic Advisory Committee meeting of -10% for the upper bound of the relative % difference between treatment and placebo based on the 95% CI. Although not powered for such, the pediatric trial (P05239) met this clinically meaningful criterion based on the 95% CI. The last trial (P08067), in children and adults, demonstrated that Grastek® improved the TCS more than placebo during the entire grass pollen season (treatment difference relative to placebo -23%, 95% CI: -36% to -13%). Therefore, the results of 3 of 6 confirmatory trials also met the statistical criterion based on the 95% confidence limit, set by CBER’s review team: an upper bound of -10%. Specific results for the TCS, DDS, and DMS from the Phase III studies can be seen in the following table.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
70
Table 7.1.3.a. Summary of all Phase III studies based on the Analysis for the Grass Pollen Season for the TCS, DSS, and DMS
Source: Original BLA 125473/000 Clinical Overview page 34-35 (results confirmed by reviewing statistician) A corresponding forest plot for the primary endpoint of interest to the Agency, TCS, is provided below.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
71
Figure 7.1.4.a. Analysis of the (TCS), the Combined Total Daily Symptom Score and Rescue Medication Score: Summary of Studies based on Phase III studies submitted by Merck-FAS
Source: Original BLA 125473/000 Clinical Overview page 52 (confirmed by reviewing statistician) The data from each of the field studies can be combined and pooled with similar positive results, illustrating that this product reduces both the symptoms as well as the use of rescue medication. Table 7.1.3.b. Summary of a Pooled Analysis for the Grass Pollen Season for the TCS, DSS, and DMS based on all the Phase III Studies submitted by the applicant
Source: Original BLA 125473/000 Clinical Overview page 36 (confirmed by reviewing statistician) From the tabulations and the forest plot, it can be observed that the studies provided within this BLA suggest there is a consistent trend of a reduction of symptoms and use of rescue medication based on the TCS score in the active treatment group compared to the placebo group.
7.1.4 Analysis of Secondary Endpoint(s)
Although the applicant considered a variety of endpoints in the different studies to be secondary endpoints, when given the opportunity for feedback within the IND phase of studies, the review team within CBER consistently proposed Daily Rhinoconjunctivitis

Statistical Reviewer: Tammy Massie, PhD STN: 125473
72
Symptom Scores (DSS) and Daily Rescue Medication Scores (DMS) to be secondary endpoints. Thus, in this integrated summary of efficacy, these results of the DSS and DMS will be presented. As in the above analysis for the primary TCS endpoint, the members of the review team agree that utilizing the pre-specified ANCOVA model provided within the protocol is considered appropriate for each study and is preferable to using one single post-hoc model for all the studies. However, other models, including covariates such as treatment group, baseline scores, geographic region, and various other fixed and random effects, were examined and yielded similar results and conclusions. Table 7.1.3.a. summarizes the difference in LS Means (and 95% CI) of the treated group versus placebo as well as the Relative LS Mean difference (and 95% CI) utilizing the DSS endpoints for the field studies. The results demonstrate that the treatment (particularly the dosage proposed of 2800 BAU of the Grastek® product) reduces the DSS score when compared to placebo, based on both the point estimate of the difference as well as the 95% CI considering the LS Mean values. A forest plot of these values can be seen in Figure 7.1.4.a., which illustrates the effect of the treatment versus placebo difference for DSS. It is of note that the applicant has included both the 95% CI bars as well as a line denoting a difference of “0.” CBER’s preferred clinically meaningful difference is based on the % relative difference of -10%, based on the upper bound of a 95% CI (which can be compared to the final column in the presented values below). Figure 7.1.5.a. Analysis of the Daily Symptom Score (DSS): Summary of Studies based on Phase III studies submitted by Merck-FAS
Source: Original BLA 125473/000 Clinical Overview page 53 (confirmed by reviewing FDA statistician)

Statistical Reviewer: Tammy Massie, PhD STN: 125473
73
Comparisons of Rescue Medication Scores based on treatment administered can be seen in Table 7.1.4.a. in the previous section. These results suggest that again there is a reduction in the rescue medication scores in the Grastek® treated individuals compared to the placebo control individuals. The results also demonstrate that the treatment (particularly the dosage proposed of 2800 BAU of Grastek®) reduces the RMS score when compared to placebo, based on both the point estimate of the difference as well as the 95% CI considering the LS Mean values. A forest plot of these values, provided by the applicant, illustrates the effect of the treatment versus placebo difference for RTSS. This figure provided by the applicant shows both the 95% CI of the Difference in LS Means as well as the relative location with respect to the line denoting “0” or no difference. Also provided are the 95% CIs of the Relative Difference, which can be compared to CBER’s standard for the upper bound of -10%. Figure 7.1.5.b. Forest Plot of the Daily Rescue Medication Score (DMS): Summary of Studies based on Phase III studies submitted by Merck-FAS
Source: Original BLA 125473/000 Clinical Overview page 54 (confirmed by reviewing FDA statistician) The results and figures included in this section provide evidence that Grastek® reduces the use of daily relief medication (DMS) as well as the daily symptom score (DSS) for the LS Means, utilizing the pre-specified model. This finding is consistent with the results found regarding the primary efficacy endpoint.
7.1.6 Other Endpoints
Analyses of exploratory and additional endpoints have little impact on the evaluation of the product, and thus will not be addressed in the Integrated Analysis of Efficacy. However, other exploratory analyses based on other endpoints, including clinical and symptom scores, different analysis sets, and other subset analyses yield similar trends that demonstrate the positive effect of this treatment when compared to placebo.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
74
7.1.7 Subpopulations
Based on the results provided by the applicant and select analyses performed by the reviewing statistician, there do not appear to be significant differences in efficacy between subjects who were mono-sensitized (defined as sensitive to the group of five-grass pollen allergens), and between Caucasians and non-Caucasians. In addition, there were no significant differences in efficacy between subjects with and without asthma, or between children and adults. Differences were noticeable when comparing regions (North America versus Europe), but this finding may be due to differences in pollen season as well as different standards of care. Results of the subset analyses are presented in Figure 7.1.7.a and 7.1.7.b. for adult subjects and pediatric subjects, respectively. Figure 7.1.7.a. Point Estimate and 95% CI for the Difference in the Total Combined Symptom and Rescue Medication Score (TCS) in select subgroups during the Grass Pollen Season-ITT Analysis Population in Adult Studies
Source: Original BLA 125473/000 Summary of Clinical Efficacy page 185 Table 7.1.7.b. Point Estimate and 95% CI for the Difference in the Total Combined Symptom and Rescue Medication Score (TCS) in select subgroups during the Grass Pollen Season-ITT Analysis Population in Pediatric Phase III Studies

Statistical Reviewer: Tammy Massie, PhD STN: 125473
75
Source: Original BLA 125473/000 Summary of Clinical Efficacy page 186 Overall subgroup analyses of the pooled studies provide supportive evidence that the Grastek® product reduces the TCS for a variety of subgroups, including age, gender, race, asthma status, and geographic location.
7.1.10 Additional Efficacy Issues/Analyses
There are no additional efficacy issues or analyses that provide additional insight into the effect of this product. The statistical reviewer did perform additional subset analyses on the applicant provided data to determine if there may have been a specific group that had efficacy results that did not yield similar conclusions regarding the positive effect of this treatment. These subsets included (but are not limited to) baseline skin prick test values, asthma status, dichotomization based on use of rescue medication, and geographic region. Since this study was not powered to examine these subsets nor were any alpha adjustments made, these subgroup-specific results are not presented here; however, the trends consistently supported that this treatment improves the combined symptom score and daily medication score. Furthermore, the reviewing statistician also performed sensitivity analyses of the primary and key secondary endpoints for both the individual studies and pooled studies, utilizing a variety of variance/covariance structures, examining several different methods for estimation of 95% CI, various analysis sets, as well as subgroups. In addition to the reduction of allergy symptoms, this product in general appears to reduce the use of rescue medication.
Statistical Reviewer: Tammy Massie, PhD STN: 125473
76
7.1.11 Efficacy Conclusions
The overall results of the efficacy data suggest that there is a reduction in symptoms and use of rescue medication when comparing individuals who were randomized and received Grastek® study treatment compared to individuals who received a nearly identical placebo product. The applicant’s proposed indication is: “Grastek® (MK-7243) is indicated for the disease modifying treatment of diagnosed Timothy and related grass pollen induced allergic rhinitis, with or without conjunctivitis, in adults and children 5 years of age and older..” Based on the applicant’s data and analyses, which were confirmed by the reviewing statistician, this indication appears to be supported. However, it is important to note that no study included patients greater than 65 years of age. The statistical analyses of the various efficacy studies suggest that the product reduced the use of daily rescue medication (DMS) as well as Daily Symptom Score (DSS), based on LS Means utilizing pre-specified ANCOVA models. Furthermore, since CBER consistently recommended a total combined score (TCS), incorporating both symptoms and rescue medication, regardless of the applicant’s primary endpoint, this combined score was considered the primary endpoint for this review. This issue is particularly relevant to the non-US IND studies, which may have been planned and implemented without CBER’s input. Since this methodology was consistently recommended and implemented by CBER, type I error should not be affected by the change in endpoint. An additional challenge that was influenced by the non-US-IND studies is the definition of a clinically meaningful endpoint. Several of these studies were designed simply to meet a simple difference between treatment groups (H0:µT - µP <0) with a p-value less than 0.05. CBER had a more stringent criterion, requiring the upper bound of the 95% CI of the Relative Difference meeting a clinically meaningful margin of -10%. Many of the non-US studies were not designed or powered for this endpoint. However, it is important to note that several of these studies did meet the US criterion, and other studies demonstrated trends suggesting that the Grastek® treatment group reduces combined scores when compared to the placebo treated group. Overall, the statistical reviewer agrees with the applicant’s statement that Grastek® is effective for immunotherapy for the reduction of rhinoconjuctivis symptoms and use of rescue medication due to grass allergy.
8. INTEGRATED OVERVIEW OF SAFETY

Statistical Reviewer: Tammy Massie, PhD STN: 125473
77
8.1 Safety Assessment Methods The safety methods incorporated a variety of active and passive adverse event reporting mechanisms depending on the study. Subjects were provided daily diary cards in which adverse event symptoms could be noted. Additionally, regular clinic visits were scheduled for the various studies in which subjects were to be asked questions to assess if any symptoms that could be considered adverse events had occurred. All subjects were to be administered the initial dose of Grastek® within a physician’s office and observed for a minimum of 30 minutes to 1 hour, depending on the study. During this time frame all individuals were observed and queried for potential symptoms and adverse events. Additional details related to safety assessment methods can be seen in the medical officer’s and epidemiologist’s review.
8.2 Safety Database
8.2.1 Studies/Clinical Trials Used to Evaluate Safety
The safety datasets provided in this submission include the efficacy datasets described in Section 1, Table 1. Within Table 1, information about each of the safety studies is provided, including the protocol, time of study, study title, study design and objectives, study population, treatment doses and schedule, number of patients exposed, and treatment duration.
8.2.2 Overall Exposure, Demographics of Pooled Safety Populations
The overall exposure and demographics of the safety database based on the treatment groups were provided by the applicant and confirmed by the reviewing statistician via JMP. The results of the tabulations of the pooled exposure to treatment or placebo can be seen within tables provided within this section of this review. The following table summarizes the extent of exposure to any treatment (including placebo and dosages of Grastek® not submitted for consideration in this BLA) in all studies provided within this BLA. This table includes the number of patients, mean exposure, and range of exposure for adults as well as children and adolescents. Table 8.2.a. Exposure to Treatment or Placebo of All Subjects Stratified by Age groups
Source: Original BLA 125473/000 Summary of Clinical Safety page 24 The previous table can be further examined by considering the extent of exposure to treatment. It is important to note that the primary dosage of interest is 2800 BAU of the Grastek® product.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
78
Table 8.2.b. Extent of Exposure to Treatment or Placebo for All Subjects ADULTS
CHILDREN
Source: Original BLA 125473/000 Summary of Clinical Safety page 26 The following table provides insight into the demographics of individuals in the studies provided within this submission. The table includes the sample size (n) and percentage of individuals for the Safety Analysis set based on age, gender, height, weight, and BMI stratified by treatment group. Overall, the demographics appear to be similar between the treatment groups when pooling all the studies that collected safety data; however, as can be seen in the below table, it is of note that there are slightly more males in these studies than females (52% and 55% for the active and placebo treated groups in the Adult studies and 66 and 64% for the active and placebo treated groups in the Pediatric studies, respectively).

Statistical Reviewer: Tammy Massie, PhD STN: 125473
79
Table 8.2.c. Demographic and Baseline Characteristics of Subjects Randomized to Treatment or Placebo for All Subjects in Phase II/III Studies
Source: Original BLA 125473/000 Summary of Clinical Safety page 37 Based on the above table it, appears there is balance between the two treatment groups for the majority of baseline characteristics (gender being the only subgroup trait that may be slightly imbalanced; however, the predominance of males, particularly in the pediatric subjects, is consistent between the treatment and placebo groups).
8.3 Caveats Introduced by Pooling of Data across Studies/Clinical Trials Since these studies were performed in a variety of locations and under different INDs (some non-US INDs), caution should be used when interpreting results. However, considering that the results and trends were consistent regardless of studies, this may be less of a concern than if conclusions depended on the individual study.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
80
8.4 Safety Results A summary of the adverse events can be seen in the table below. Based on the tabulated values, similar trends of adverse events can be seen in both the treatment and placebo treated patients (82% and 68%, respectively, for adults and 82% versus 79% for pediatric subjects). The table below provides a brief description of the adverse event, the count, and % of observed subjects with the Adverse Event, stratified by treatment group. It is important to note that this table combines all treatment doses of the active treatment. Table 8.4.1.a Overview of Adverse Events-Safety Analysis Set-All Doses from All Studies- Adult Subjects
Source: Original BLA 125473/000 Summary of Clinical Safety page 55 Table 8.4.1.b Overview of Adverse Events-Safety Analysis Set-All Doses from All Studies-Pediatric Subjects
Source: Original BLA 125473/000 Summary of Clinical Safety page 56 Considering treatment emergent adverse events listed in the table above, the treated group had a greater likelihood of TEAEs with 66% versus 23% (Adults) and 58% versus 24% (Pediatric subjects), when comparing the treatment group to the placebo treated individuals. The types of adverse events observed during this study can be seen in the following tables, which include events common (>3% of subjects experiencing the adverse event) in Adult and Pediatric subjects.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
81
Table 8.4.2.a Summary of Adverse Events-Adult Subjects
Source: Original BLA 125473/000 Summary of Clinical Safety page 85

Statistical Reviewer: Tammy Massie, PhD STN: 125473
82
Table 8.4.2.a Summary of Adverse Events-Adult Subjects
Source: Original BLA 125473/000 Summary of Clinical Safety page 86 Additional comments related to global AEs for the pooled results can be seen in the medical officer’s and epidemiologist’s reviews.
8.4.1 Deaths
One death was reported by the applicant; however, this death was caused by a multiple drug overdose several months after study drug was discontinued and was deemed by the medical officer as unlikely to be related to treatment. Further details regarding this patient and their medical history can be found in the medical officer’s review.
8.4.2 Nonfatal Serious Adverse Events
Limited non-fatal serious Adverse Events were reported. Within the adult studies, there were 20 (1.2%) serious adverse events in the treated group, while there were 20 (1.2%) serious adverse events in the placebo group. Within the pediatric studies, there were 3 (0.7%) serious adverse events in the treated group and 4 (0.9%) serious adverse events in

Statistical Reviewer: Tammy Massie, PhD STN: 125473
83
the placebo group. All serious adverse events were noted to be self-limiting and resolved. Additional details can be found in the medical officer’s and epidemiologist’s review.
8.4.3 Study Dropouts/Discontinuations
Within all studies submitted by the applicant, approximately 16% of treated subjects and approximately 13% of placebo treated subjects discontinued treatment. The reason for discontinuation varied, but the predominant reason for dropping out was local side effects, including swelling and irritation in the mouth/tongue and oral region. A detailed discussion related to dropouts and discontinuations is deferred to the medical officer and epidemiologist.
8.4.4 Common Adverse Events
The majority of adverse events that were observed and noted within the various studies were related to allergies (i.e., rhinoconjunctivitis symptoms) for both active treated and placebo treated patients. Overall, approximately 70-80% and 60-70% of subjects in the treatment and placebo groups, respectively, experienced adverse events. The majority of these adverse events were local reactions that involved the throat, nasal, and oral regions as well as the GI tract, which is to be expected when considering grass allergic individuals with symptoms noted at baseline. Further discussion and details related to common adverse events is deferred to the medical officer and epidemiologist.
8.4.5 Clinical Test Results
Clinical test results varied between and within the studies. However, endpoints including IgG, IgE, and other tests performed had results that were expected and not considered outside of normal ranges.
8.4.6 Systemic Adverse Events
There were few episodes of anaphylaxis or anaphylactic shock observed in any subjects within the submitted studies, with all issues resolving with epinephrine administration. Rarely (less than 1% of individuals) were uticaria and systemic rashes observed. Additional details related to systemic adverse events can be found in the medical officer’s review.
8.4.7 Local Reactogenicity
There were local reactions noted in both the treated and placebo treated individuals, up to 80% and up to 70%, respectively, depending on the study. The majority of these adverse reactions were either gastro-intestinal or were irritation located in the administration site: the throat. The majority of these events were mild or moderate and all were self-limiting. Additional details related to systemic adverse events can be found in the medical officer’s review.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
84
8.4.8 Adverse Events of Special Interest
No adverse events of special interest were noted in the submitted studies.
8.5 Additional Safety Evaluations Although this product had adverse events noted, these were to be expected since this product is composed of the allergen the individuals are allergic to. All issues associated with these adverse events were self-limiting and resolved by study completion
8.6 Safety Conclusions Based on the observed safety data including AEs, this product frequently causes local AEs in the oral region that are known to be associated with SLIT (since it is administered by mouth) in both adult and pediatric subjects. The data reviewed support the general conclusion that the incidence of severe or serious AE associated with SLIT is non-life-threatening and self-limiting. Additional details can be seen in the medical officer’s and epidemiologist’s reviews.
9. ADDITIONAL STATISTICAL ISSUES No additional statistical issues were noted during the examination and re-analysis of the efficacy and safety data provided by the applicant.
9.1 Special Populations No special populations were examined in any studies submitted within this BLA.
9.1.1 Human Reproduction and Pregnancy Data
There are no data regarding human reproduction or pregnancy provided within this submission.
9.1.2 Use During Lactation
There are no data regarding the use of this product in lactating individuals provided within this submission.
9.1.3 Pediatric Use and PREA Considerations
This submission included a North American study designed exclusively to examine pediatric subjects (P05239) as well as a study that included both pediatric and adult subjects in Canada and the US. Safety and efficacy data from these studies were similar to the efficacy data acquired in the adult studies.
9.1.4 Immunocompromised Patients
There are no data regarding individuals with compromised immunity provided within this submission, particularly since immunocompromised subjects were excluded from the studies.

Statistical Reviewer: Tammy Massie, PhD STN: 125473
85
9.1.5 Geriatric Use
There are no data regarding geriatric use in individuals older than 65 years of age provided within any studies submitted by the applicant.
9.2 Aspect(s) of the Statistical Evaluation Not Previously Covered
The reviewer has no additional comments.
10. CONCLUSIONS
10.1 Statistical Issues and Collective Evidence
The data from the studies provided in this submission appear to support the applicant’s conjecture that the Grastek® 2800 BAU product is safe and effective in the treatment of allergic rhinoconjunctivitis, using CBER’s pre-specified criterion for efficacy based on the Combined Symptom score that incorporates both rescue medication and symptom scores.
10.2 Conclusions and Recommendations Based on the data submitted and reviewed, Grastek® 2800 BAU per dose, appears to be safe and effective for immunotherapy of allergic rhinoconjunctivitis due to sensitivity to any combination of the five grass pollens included in the product. The product appears to be safe and effective for pediatric subjects 5-18 years of age and adults 18-65 years of age. The statistical analyses performed and examined by the reviewing statistician support the safety and efficacy of this product.