Appendix D FORMS - WV DHHR · • To choose the agency which will provide services agreed upon. •...
54
Appendix D FORMS 101 – Vitamin/Iron Order Form ............................................................................................................... 1 R001A – Client Tracking Sheet ................................................................................................................. 2 R003 – Client Request for Records Release .............................................................................................. 3 R004 – Client Rights and Responsibilities ................................................................................................. 4 R004A – Spanish Client Rights and Responsibilities .................................................................................. 5 R006 – DCC Contact Letter #2 .................................................................................................................. 6 R006 – Spanish DCC Contact Letter #2 ..................................................................................................... 7 R007 – DCC Contact Letter #1 .................................................................................................................. 8 R007 – Spanish DCC Contact Letter #1 ..................................................................................................... 9 R009 – Provider Non-Enrollment Letter ................................................................................................. 10 R010 – Provider Enrollment Letter ......................................................................................................... 11 R011a – Service Care Plan...................................................................................................................... 12 R011c – Service Care Plan Blank Form ................................................................................................... 13 R015 – Progress Notes ........................................................................................................................... 14 R019 – Alternate Entry Referral OF Infants/Prenatals to RFTS ................................................................ 15 R022 – Outcome Measures At Case Closure........................................................................................... 16 R025 – RFTS/WIC Participant Request for Information ........................................................................... 17 R036a – Initial Client Assessment – Prenatal .......................................................................................... 18 R036b – Initial Client Assessment – Infant ............................................................................................. 19 R038A – High Birth Score Referral and Tracking Form ............................................................................ 20 R039 – Provider Letter ........................................................................................................................... 21 R040 – Quality Assurance Report ........................................................................................................... 22 R041A – Regional Care Coordinators Time Sheet ................................................................................... 23 R041B – Regional Clerk Time Sheet........................................................................................................ 24 R042 – DCC Contact Letter #3 ................................................................................................................ 25 R042 – Spanish DCC Contact Letter #3 ................................................................................................... 26 R060 – Enhanced Services Education Report.......................................................................................... 27 R065 – Edinburgh Postnatal Depression Scale........................................................................................ 28 TS001 – Tobacco Screening Form .......................................................................................................... 29 TS002 – Tobacco Follow-up Form .......................................................................................................... 30 TS006 – SCRIPT Intervention Form......................................................................................................... 31 Part A Designated Care Coordinators and Enhanced Services Providers ................................................. 32 Part B DCC Agency Caseload Projection ................................................................................................. 33 Infant Anticipatory Guidelines ............................................................................................................... 34 Prenatal Anticipatory Guidelines ........................................................................................................... 35 WV Birth Score – Development Risk Screen and Newborn Hearing Screen............................................. 36 WV Prenatal Risk Screening Instrument ................................................................................................. 37 NICU Care Coordination Referral form ................................................................................................... 38 Designated Care Coordinator Training Certification ............................................................................... 39
-
Upload
nguyenkhanh -
Category
Documents
-
view
214 -
download
0
Transcript of Appendix D FORMS - WV DHHR · • To choose the agency which will provide services agreed upon. •...

Appendix D FORMS 101 – Vitamin/Iron Order Form ............................................................................................................... 1 R001A – Client Tracking Sheet ................................................................................................................. 2 R003 – Client Request for Records Release .............................................................................................. 3 R004 – Client Rights and Responsibilities ................................................................................................. 4 R004A – Spanish Client Rights and Responsibilities .................................................................................. 5 R006 – DCC Contact Letter #2 .................................................................................................................. 6 R006 – Spanish DCC Contact Letter #2 ..................................................................................................... 7 R007 – DCC Contact Letter #1 .................................................................................................................. 8 R007 – Spanish DCC Contact Letter #1 ..................................................................................................... 9 R009 – Provider Non-Enrollment Letter ................................................................................................. 10 R010 – Provider Enrollment Letter ......................................................................................................... 11 R011a – Service Care Plan ...................................................................................................................... 12 R011c – Service Care Plan Blank Form ................................................................................................... 13 R015 – Progress Notes ........................................................................................................................... 14 R019 – Alternate Entry Referral OF Infants/Prenatals to RFTS ................................................................ 15 R022 – Outcome Measures At Case Closure........................................................................................... 16 R025 – RFTS/WIC Participant Request for Information ........................................................................... 17 R036a – Initial Client Assessment – Prenatal .......................................................................................... 18 R036b – Initial Client Assessment – Infant ............................................................................................. 19 R038A – High Birth Score Referral and Tracking Form ............................................................................ 20 R039 – Provider Letter ........................................................................................................................... 21 R040 – Quality Assurance Report ........................................................................................................... 22 R041A – Regional Care Coordinators Time Sheet ................................................................................... 23 R041B – Regional Clerk Time Sheet ........................................................................................................ 24 R042 – DCC Contact Letter #3 ................................................................................................................ 25 R042 – Spanish DCC Contact Letter #3 ................................................................................................... 26 R060 – Enhanced Services Education Report.......................................................................................... 27 R065 – Edinburgh Postnatal Depression Scale ........................................................................................ 28 TS001 – Tobacco Screening Form .......................................................................................................... 29 TS002 – Tobacco Follow-up Form .......................................................................................................... 30 TS006 – SCRIPT Intervention Form ......................................................................................................... 31 Part A Designated Care Coordinators and Enhanced Services Providers ................................................. 32 Part B DCC Agency Caseload Projection ................................................................................................. 33 Infant Anticipatory Guidelines ............................................................................................................... 34 Prenatal Anticipatory Guidelines ........................................................................................................... 35 WV Birth Score – Development Risk Screen and Newborn Hearing Screen ............................................. 36 WV Prenatal Risk Screening Instrument ................................................................................................. 37 NICU Care Coordination Referral form ................................................................................................... 38 Designated Care Coordinator Training Certification ............................................................................... 39

DHHR/BPH/OMCFH/RFTS/101 Revised 8/2010
VITAMIN/IRON ORDER FORM Please forward orders to: Office of Maternal, Child and Family Health Right From The Start Program MATERIALS MANAGEMENT OFFICE 900 Bullitt Street Charleston, West Virginia 25301 (304) 558-3417 TOLL FREE: 1-800-642-8522 FAX: (304) 558-1524
ATTENTION
Orders are shipped via UPS. Street address is required. ALLOW NO LESS THAN A 2 WEEK LEAD TIME FOR PROCESSING AND DELIVERY OF YOUR ORDER. For inventory maintenance purposes, all orders must be submitted on form OMCFH/RFTS/101. NO EXCEPTIONS.
Provider Name: ___________________________________________ Provider Number: 5050__________________ STREET ADDRESS: ______________________________________________________________________________ _______________________________________________________________________________________________ Contact Person: __________________________________________ Telephone: _____________________________ Date: ______________________________ RFTS/101 Vitamin Request Forms: ________________ (Amount Requested)
CODE ITEM AMOUNT PER CASE CASES ON HAND
CASES ORDERED
QUANTITY APPROVED
M100 Prenatal Vitamins w/ Folic Acid
12 bottles/case 100 tablets/bottle
M150 Prenatal Iron 12 bottles/case
100 tablets/bottle
NOTE: We reserve the right to alter your request based on current inventory. Requested by: _____________________________________ Approved by: __________________________________ (County Health Office or Clinic Physician) (OMCFH) Please check expiration date on vitamins presently in stock. We recommend vitamin and iron supplies be rotated with attention to the date of expiration. Expired vitamins and iron should be returned to the Materials Management Warehouse. The Medicaid Program Regulation MA-91-07, issued July 1, 1991, allows for the coverage of the purchase of non-prescription prenatal vitamins and ferrous sulfate, gluconate, and fumarate. Under this allowance, a recipient of WV Medicaid card may receive vitamins and/or iron tablets from a pharmacy with a written prescription from their physician/provider. The policy of Right From The Start Maternity Services for the distribution of vitamins/iron is as follows: Give one bottle at the time of positive pregnancy determination or first OB visit to: 1) minors (19 years of age and under) 2) non-citizens 3) clients who have not yet applied for or been approved for Medicaid 4) clients denied Medicaid and not yet approved for Right From The Start Maternity Services As soon as a patient is enrolled in: Medicaid - provide her with a prescription for future vitamin/iron needs OMCFH - provide her with two (2) additional bottles of vitamins.
PLEASE RESERVE RIGHT FROM THE START MATERNITY SERVICES
SUPPLIES FOR THESE CATEGORIES OF OB PATIENTS ONLY!

OFFICE OF MATERNAL, CHILD AND FAMILY HEALTH RIGHT FROM THE START PROGRAM
CLIENT TRACKING SHEET
WVDHHR/BPH/OMCFBH/DPWH/PP/RFTS/ROO1A//6-2012
Enhanced Services Only Prenatal Infant Birth Score ID:
Name: Name: Last Name First Name (MI) Last Name First Name (MI) Name Change: Name Change: Last Name First Name
(MI) Last Name First Name (MI)
Prenatal SS#: SS#: Birthdate: Birthdate: EDC: Guardian’s Name: Change in EDC: Delivery Date: Guardian’s SS#:
Medicaid #: RFTS Maternity Services #: HMO Name: HMO #: Service Date: Face to Face: Yes No Place: Home Office Clinic Other:
S5190HD ASSESSMENT/SERVICE CARE PLAN Prenatal Only - 1 Per Case
T1016HD CARE COORDINATION (#15 Minute Units) Infant ( PHB Curriculum addressed)
Prenatal ( PHB Curriculum addressed) First 6 Months Months 7-12 1st Trimester Mo. 4 Mo. 5 Mo. 6 Mo. 7 Mo. 8 Mo. 9 1 2 3 4 5 6 7 8 9 10 11 12
Referrals to: Care Coordination:
A01 DHHR A14 Health Check C Monitoring Q Environment: Infant Stimulation A02 HUD A15 Birth to Three E Revise Plan/Assessment R Environment: Safety A03 WIC A16 Children’s Specialty Care F Birth Score S Well Child Care A04 Parenting Education A17 Family Planning G Advocacy T Acute Care For Infants A05 Preventive Self Care Ed A18 Genetics H Transportation U Newborn Hearing Screening A06 Childbirth Education A19 Nutrition J Financial: Infant Care Items V Baby Bottle Tooth Decay/Oral Health A07 Community Agency A21 Systems Point of Entry K Financial: Access to Phone W Tobacco Dependence Treatment A09 Medical Provider A22 CHIP L Financial: Utilities X Developmental Progress A10 Child Care A23 Other M Financial: Money Management Y Nutrition Assessment A11 School A24 WV Quitline N Environment: Adequate Housing Z Day One A12 Clergy BN F/U Missed Appointment O Environment: Safe Drinking Water AA Depression Screening A13 Law Enforcement BY F/U Kept Appointment P Environment: Electrical Circuitry AB Family Planning Education
ENHANCED SERVICES – PRENATALS ONLY – 1 SESSION PER DAY Progress Notes: Time: In Out
S9442HD CHILDBIRTH CLASSES A Maternal/Infant Development D Relaxation/Breathing Tech. B Nutrition/Fitness/Drugs E Postpatum/FamilyPlanning C Physiology of Labor/Delivery F Newborn Care/ Breastfeeding
S9444HD PARENTING EDUCATION
A Infant Care D Child Safety B Preventive Care E Newborn Development C S/S Acute Illness
S9445HD PREVENTIVE SELF CARE EDUCATION
A Physical/Emotional Changes E Breastfeeding B Warning Signs in Pregnancy F Contraceptive Care C Healthful Behaviors H Smoking Assessment D Eating Habits I Safety/Domestic Violence
S9452HD NUTRITIONAL EVALUATION/COUNSELING (RD only)
"I received a home visit by the DCC today." Client Signature:
DCC Signature:
Agency:
County:
A - COMPLETED PROGRAM
B-INCOMPLETE
B1. Spontaneous Abortion B9. Lost to Follow-up B2. Induced Abortion B10. Transferred Within Region B3. Moved Out-of-State B11. Did Not Meet Program Protocol B4. Transferred Out-Of-Region B13. Pre-term Delivery B8. Death B15. Closed by RCC
Original: DCC Copy: RCC Copy: Billing

OMCFH/RFTS-R003 White: DCC Revised: 8/2010 Yellow: RCC Pink: Client
WEST VIRGINIA DEPARTMENT OF HEALTH AND HUMAN RESOURCES BUREAU FOR PUBLIC HEALTH
OFFICE OF MATERNAL, CHILD AND FAMILY HEALTH RIGHT FROM THE START PROGRAM
350 Capitol Street, Room 427 Charleston, West Virginia 25301-3714
Toll Free in WV: 1-800-642-8522
CLIENT REQUEST FOR RECORD RELEASE I, ____________________________________________________ do hereby request:
(Client’s Name)
To review my Right From The Start Program case record. A copy of my Right From The Start Program case record. A copy of my Right From The Start Program case record be released to:
___________________________________________________________ __________________________________ ___________________________________ Signature of Client Date Witness Date ______________________________________________ Title/Agency

OMCFH/RFTS-R004 White: DCC Revised:8/2010 Yellow:
RCC Pink: Client
Goldenrod: Medical Provider
RIGHT FROM THE START PROGRAM CLIENT RIGHTS AND RESPONSIBILITIES
NAME: ________________________________________ SSN: ______________________________________________ (Last) (First) (MI)
RIGHTS RESPONSIBILITIES • To receive professional treatment and consideration. • To participate in development of the care plan and
selection of services. • To choose the agency which will provide services
agreed upon. • To question any planned action. • To decline any or all services offered. • To withdraw from care coordination at any time without
penalty or loss of any other program eligibility. • To review or receive a copy of your RFTS records. • To participate in RFTS any time during the eligibility
period even if services have previously been refused.
• To keep all medical appointments. • To keep all appointments for other services identified in
the care plan and agreed upon by the client. • To obtain all medically-ordered laboratory procedures. • To report any change in address or telephone number. • To report any changes in health condition. • To report any changes in home environment which
affect health condition. • To provide Care Coordinator with a safe environment for
visits.
TO REPORT ANY PROBLEMS OR CHANGES, PLEASE CALL: _________________________________________________
If you believe you have been denied any of the above rights, you may contact the Right From The Start Program by phone at 1-800-642-8522 or mail at 350 Capitol Street, Room 427, Charleston, West Virginia 25301-3714.
CLIENT: I have read and understand my responsibilities and rights and do hereby give permission for my/my infant’s RFTS record to be
released by the Care Coordinator to agencies participating in my care. I also give my permission for agencies participating in
my/my infant’s care to release information to the RFTS staff.
______________________________________________________________________________________________________(Signature) (Date) DESIGNATED CARE COORDINATOR: I have reviewed the rights and responsibilities with this client.
______________________________________________________________________________________________________ (Signature) (Date) CAREGIVER PERMISSION I, ___________________________________________Parent/Guardian of _________________________________________
(Infant) give permission to ____________________________________________ to discuss and plan care for my infant in my absence (Designated Care Coordinator) with _________________________________________________. (Caregiver) ________________________________________________________________________________________ (Parent/Guardian Signature) (Date) ________________________________________________________________________________________ (Designated Care Coordinator Signature) (Date) COMMENTS:___________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
*Please identify additional person/persons who may be caregivers.

WVDHHR/BPH/OMCFH/RFTS-R004-A Blanco: DCC
Revisado: 11/08 Amarillo: RCC Rosa: Client
Oro: el Proveedor Médico
PROYECTO DERECHO DESDE EL PRINCIPIO WEST VIRGINIA DEPARTAMENTO DE SALUD Y RECURSOS HUMANOS
DERECHOS Y RESPONSABILIDADES DE LA CLIENTE
NOMBRE: SSN: ________________________________________________ (Last) (First) (MI)
DERECHOS
RESPONSABILIDADES Recibir tratamiento y consideración profesionales. Participar en el desarrollo del plan de cuidado y en la
selección de servicios. Elegir la agencia que proveerá los servicios seleccionados. Dudar de cualquier acción planificada. Rechazar todo o cualquier servicio. Quitar la coordinación de cuidado a toda hora sin pena y sin
perder elegibilidad de cualquier otro programa. Rever or recibir una copia de sus récords. Participar a toda hora durante el período elegible aunque haya
rechazado los servicios de antes.
Quedarse con toda cita médica. Quedarse con toda cita por otros servicios identificados en el
plan de cuidado y seleccionados por la cliente. Obtener todas las pruebas médicas pedidas. Informarnos de cualquier cambio de señas o de número de
teléfono. Informarnos de cualquier cambio en su condición médica. Informarnos de cualquier cambio en su ambiente casera que
afecte su condición médica. Para proveerie a la trabajadora – Care Coordinator – un
ambiente seguro para las visitas.
PARA INFORMARNOS DE PROBLEMA O CAMBIO, POR FAVOR LLAME: ____________________________________________ Si cree que se le ha negado cualquier de estos derechos, puede hablar con el Proyecto Derecho Desde El Principio por teléfono a 1-800-642-8522 o por correo a 350 Capitol Street, Room 427, Charleston, West Virginia 25301-3714.
CLIENTE: He leído y entiendo mis responsabilidades y derechos y desde ahora permito que mi récord de Derecho Desde El Principio o el récord de mi niño sea mandado por el Coordenador de Cuidado a las agencias que particpan en mi cuidado. __________________________________________________________________________________________________________ (Firma) (Fecha) COORDENADOR DE CUIDADO DESIGNADO: He revisto los derechos y responsabilidades con esta cliente. __________________________________________________________________________________________________________
(Firma) (Fecha)
PERMISO PARA CUIDANIÑOS Yo, ______________________________________________ Padre/Guardian de ___________________________________________,
(Niño)
permito que ____________________________________________________________ hable de y planifique el cuidado de mi niño en (Coordenador de Cuidado Designado)

WVDHHR/BPH/OMCFH/RFTS-R004-A Blanco: DCC
Revisado: 11/08 Amarillo: RCC Rosa: Client
Oro: el Proveedor Médico
mi ausencia con ___________________________________________. (Cuidaniños)
__________________________________________________________________________________________________________ (Firma de Padre/Guardian de) (Fecha) ________________________________________________________________________________________________________________________ (Firma de Coordenador de Cuidado Designado) (Fecha)
COMMENTS: *
________________________________________________________________________________________________________
______________________________________________________________________________________________________________
______________________________________________________________________________________________________________
______________________________________________________________________________________________________________
______________________________________________________________________________________________________________
________________________________________________________________________________
*Por favor identifique otra(s) persona(s) que le(s) permite ser cuidaniños.

OMCFH/RFTS-R006-DCC Contact Letter #2 White: Client Revised: 6/2011 Yellow: DCC
Earl Ray Tomblin Governor
Michael J. Lewis, M.D. Ph.D. Cabinet Secretary
STATE OF WEST VIRGINIA DEPARTMENT OF HEALTH AND HUMAN RESOURCES
RIGHT FROM THE START PROGRAM
______________________________ (Date) Dear ________________________________: You recently received a letter about the Right From The Start Program’s free services for you and your baby. Social workers and nurses from the Right From The Start Program can offer pregnant women and their babies resources and services to help keep them healthy. Right From The Start may be able to assist you with housing needs, transportation to doctor’s appointments, health care, items for your baby and WIC (Women’s, Infants and Children Program) benefits. The Right From the Start Program has information about:
• how being pregnant may make you feel bad • how your body changes when you’re pregnant • things that shouldn’t happen during pregnancy (like having contractions before your due date) • baby blues • how to tell when things are not normal • how to tell if your baby is sick • easy ways to take care of your baby • colic • how to tell if your baby has a fever • when to call your or your baby’s doctor
All Right From The Start Program services are free and offered in your home or at some other place of your choosing. Pregnant women and new moms decide the services they want. There is also information available for dads. Having a baby can be a happy event. But at times, taking care of a baby can be very hard. Having someone to talk with and to offer ideas may make things easier. Please call or email me to let me know if you would like services from the Right From The Start Program. Sincerely, Designated Care Coordinator
________________________________ DCC Name (Please Print)
________________________________ Agency
________________________________ Agency Address
________________________________
________________________________ Telephone/Email
OFFICE OF MATERNAL, CHILD AND FAMILY HEALTH Bureau for Public Health
350 Capitol Street, Room 427 Charleston, WV 25301-3714
Phone: (304) 558-5388 Toll-Free (in WV): 1-800-642-8522 or 1-800-642-9704 FAX: (304) 558-7164

OMCFH/RFTS-R006-DCC Contact Letter #2 White : Client Revised: 6-2011 Yellow: DCC
Michael J. Lewis, M.D. Ph.D. Cabinet Secretary
Earl Ray Tomblin Governor
ESTADO DE WEST VIRGINIA EL DEPARTAMENTO DE SALUD Y LOS RECURSOS HUMANOS
PROGRAMA DESDE EL PRINCIPIO
______________________________ (Fecha/Date) Estimada ________________________________: Recientemente le mande una carta sobre el program Desde el Principio y come puede obtener ayuda valde para usted y su Bebé. West Virginia tiene asistentes sociales y enfermeras que pueden ofrecer a las mujeres embarazadas y a sus bebés ayuda en mantenerlos sanos. Estas enfermeras y asistentes sociales pueden asistir en encontrar cosas que usted puede necesitar como WIC, un lugar para vivir, maneras para conseguir al doctor, cosas para su bebé y cuidado médico. Pueden ayudarle a aprender:
• cómo estando embarazada puede hacerle sentir mal • cómo su cuerpo cambia cuando usted está embarazada • cosas que no deben suceder durante el embarazo (como tener contracciones antes de su fecha debida) • depresión postparto • sabiendo cuándo las cosas no son normales • sabiendo si su bebé esta enfermo • maneras fáciles de tomar cuidado de su bebé • colico • cómo saber si su bebé tiene una fiebre • cuándo debe de llamar al medico
Estos servicios, llamados “Desde el Principio,” son gratis y pueden visitarle en su hogar o en otro lugar. Las mujeres embarazadas y las nuevas mamás consiguen eligenlos servicios que ellas quieren. Hasta hay información disponible para los papás. Me gustaría hablar con usted del programa Desde el Principio. Tener un bebé puede ser un tiempo muy feliz, pero puede ser realmente duro. Tener a alguien con quien hablar y para ofrecer ideas puede a veces hacer cosas más fáciles. Por favor llámeme o envíe por correo electrónico y déjeme saber independientemente si usted quiere usar el programa Desde el Principio. Sinceramente, ________________________________ Designated Care Coordinator
________________________________ DCC Name (Please Print)
________________________________ Agency
________________________________ Agency Address
________________________________ Telephone/Email
OFICINA DE LA SALUD MATERNAL, DEL NIÑO Y DE LA FAMILIA
Oficina para la salud pública 350 Capitol Street, Room 427 Charleston, WV 25301-3714
Telephono: (304) 558-5388 Gratis (en WV): 1-800-642-8522 or 1-800-642-9704 FAX: (304) 558-7164
OMCFH/RFTS-R007-DCC Contact Letter #1 White: Client Revised: 6/2011 Yellow: DCC
Michael J. Lewis, M.D. Ph.D. Cabinet Secretary
Earl Ray Tomblin Governor
STATE OF WEST VIRGINIA DEPARTMENT OF HEALTH AND HUMAN RESOURCES
RIGHT FROM THE START PROGRAM
________________________________
(Date) Dear : Having a baby can be a very happy time, but can also be really hard. Having someone to talk to and offer ideas can sometimes make things easier. West Virginia has social workers and nurses who can offer pregnant women and their babies help to keep them healthy. These nurses and social workers can help you find things you may need like WIC, a place to live, a way to get to the doctor, things for your baby and health care. They can help you learn about:
• how being pregnant may make you feel bad • how your body changes when you’re pregnant • things that shouldn’t happen during pregnancy (like having contractions before your due date) • baby blues • how to tell when things are not normal • how to tell if your baby is sick • easy ways to take care of your baby • colic • how to tell if your baby has a fever • when to call your or your baby’s doctor
These services, called Right From The Start, are free and can be held in your home or at some other place. Pregnant women and new moms get to choose which services they want. There is even information available for dads. Helping West Virginia’s pregnant women and babies stay healthy is our goal. We hope to hear from you so we can talk about what services you may like to have. Please call or email me to let me know whether or not you want Right From The Start. Sincerely, Designated Care Coordinator
_________________________________ DCC Name (Please Print)
______________________________________ Agency
______________________________________ Agency Address
______________________________________
______________________________________ Telephone/Email
OFFICE OF MATERNAL, CHILD AND FAMILY HEALTH Bureau for Public Health
350 Capitol Street, Room 427 Charleston, WV 25301-3714
Phone: (304) 558-5388 Toll-Free (in WV): 1-800-642-8522 or 1-800-642-9704 FAX: (304) 558-7164

OMCFH/RFTS-R007-DCC Contact Letter #1 White: Client Revised: 6-2011 Yellow: DCC
Michael J. Lewis, M.D. Ph.D. Cabinet Secretary
Earl Ray Tomblin Governor
ESTADO DE WEST VIRGINIA EL DEPARTAMENTO DE SALUD Y LOS RECURSOS HUMANOS
PROGRAMA DESDE EL PRINCIPIO
________________________________
(Fecha/Date) Estimada : Tener un bebé puede ser un tiempo muy feliz, pero puede también ser realmente duro. Tener alguien con quien hablar y que le ofrezca ideas puede a veces hacer cosas más fáciles. West Virginia tiene asistentes sociales y enfermeras que pueden ofrecer a las mujeres embarazadas y a sus bebés ayuda en mantenerlos sanos. Estas enfermeras y asistentes sociales pueden asistir en encontrar cosas que usted puede necesitar como WIC, un lugar para vivir, maneras para conseguir al doctor, cosas para su bebé y cuidado médico. Pueden ayudarle a aprender:
• cómo estando embarazada puede hacerle sentir mal • cómo su cuerpo cambia cuando usted está embarazada • cosas que no deben suceder durante el embarazo (como tener contracciones antes de su fecha debida) • depresión postparto • sabiendo cuándo las cosas no son normales • sabiendo si su bebé esta enfermo • maneras fáciles de tomar cuidado de su bebé • colico • cómo saber si su bebé tiene una fiebre • cuándo debe de llamar al medico
Estos servicios, llamados “Desde el Principio,” son gratis y pueden visitarle en su hogar o en otro lugar. Las mujeres embarazadas y las nuevas mamás eligen los servicios que ellas quieren. Hasta hay información disponible para los papás. Ayudando Las mujeres embarazadas y los bebés de West Virginia quedarse sanos es nuestra meta. Esperamos oír de usted para hablar de qué servicios usted puede usar. Llámeme o envíe por correo electrónico por favor dejerme saber independientemente si usted quiere usar el programa Desde el Principio. Sinceramente, ________________________________ Designated Care Coordinator
________________________________ DCC Name (Please Print)
________________________________ Agency
________________________________ Agency Address
________________________________ Telephone/Email
OFICINA DE LA SALUD MATERNAL, DEL NIÑO Y DE LA FAMILIA
Oficina para la salud pública 350 Capitol Street, Room 427 Charleston, WV 25301-3714
Telephono: (304) 558-5388 Gratis (en WV): 1-800-642-8522 or 1-800-642-9704 FAX: (304) 558-7164

OFFICE OF MATERNAL, CHILD AND FAMILY HEALTH
Bureau for Public Health 350 Capitol Street, Room 427 Charleston, WV 25301-3714
Phone: (304) 558-5388 Toll-Free (in WV): 1-800-642-8522 or 1-800-642-9704 FAX: (304) 558-7164 OMCFH/RFTS-R009-Provider Non-Enrollment Letter White: Provider Revised: 6/2011 Yellow: RCC
Michael J. Lewis, M.D. Ph.D. Cabinet Secretary
Earl Ray Tomblin Governor
STATE OF WEST VIRGINIA DEPARTMENT OF HEALTH AND HUMAN RESOURCES
RIGHT FROM THE START PROGRAM _______________________________ (Date) Dear Provider:
This is to inform you that your client, _________________________________________
will not be receiving care coordination at this time for the following reason(s):
∼ Does not meet eligibility requirements.
∼ Past EDC
∼ No Care Coordination Provider available. (Will assign as provider becomes
available.)
∼ Refused
Please call if you have questions or concerns.
Sincerely,
___________________________________
Regional Care Coordinator Agency Name: __________________________
Address: _______________________________
______________________________________
Agency Telephone: ______________________

OFFICE OF MATERNAL, CHILD AND FAMILY HEALTH
Bureau for Public Health 350 Capitol Street, Room 427 Charleston, WV 25301-3714
Phone: (304) 558-5388 Toll-Free (in WV): 1-800-642-8522 or 1-800-642-9704 FAX: (304) 558-7164 OMCFH/RFTS-R010-Provider Enrollment Letter White: Provider Revised: 9-2011 Yellow: DCC
Earl Ray Tomblin Governor
Michael J. Lewis, M.D. Ph.D. Cabinet Secretary
STATE OF WEST VIRGINIA DEPARTMENT OF HEALTH AND HUMAN RESOURCES
RIGHT FROM THE START PROGRAM
___________________________________________ (Date)
RE: ____________________________________ (Client Name)
____________________________________
(Social Security Number)
Dear Provider:
The State of West Virginia provides money so that social workers and nurses from local health departments, community health centers and other community agencies can offer pregnant women and their newborns support services to improve well-being. These nurses and social workers are knowledgeable on how to locate community resources, depending on the need, such as WIC, housing assistance, transportation to doctor appointments, infant care items and the availability of medical care. They offer information on pregnancy discomforts and body changes that occur during pregnancy. They can help the pregnant woman learn to recognize warning signs of such complications as preterm labor, postpartum blues and when to call their doctor. The nurses and social workers also offer parenting support and information on baby care such as colic, dealing with a fever and how to determine if the baby is sick.
These services, called Right From The Start, are provided at no cost to the family and are offered
in the family’s home or other setting. Pregnant women or new moms who participate in Right From The Start choose which services they want. There is even information available for dads.
The above referenced client has been evaluated and is eligible for Right From The Start services. With the assistance of the client, a service plan has been developed for management of the client’s needs. Should you wish to recommend any modifications to the service plan at any time, please call me at the number listed below. Sincerely,
Designated Care Coordinator
____________________________________ Phone Number
____________________________________ Agency Name
____________________________________ Address
____________________________________ City, State & Zip
Enclosure

OMCFH/RFTS-R011A White: DCC Revised: 12-2011 Pink: RCC Yellow Client Goldenrod: Provider
RIGHT FROM THE START PROGRAM
SERVICE CARE PLAN
Closure Date: Closure Code: A
B
CLIENT NAME MEDICAID NO. SOC. SECURITY # PRENATAL (Last) (First) (MI)
INFANT
IDENTIFIED NEEDS Prenatal DCC Client Infant DCC Client
Childbirth education Parenting education Obstetrical care Pediatric care Parenting education Nutrition WIC Anticipatory guidance Anticipatory guidance Safety Safety DCC/guardian trusting relationship DCC/Client trusting relationship Coordination of services Coordination of services Transportation to medical appointments Transportation to medical appointments Infant care items Choose method of infant feeding Please List Others Infant care items
Please list others:
GOALS TO BE COMPLETED TO MEET IDENTIFIED NEEDS TARGET DATE
COMPLETED DATE Prenatal Infant
To have a full term, healthy pregnancy To promote optimal infant health to age one year To choose a family planning method To ensure safety To provide parenting education To educate on coping skills To provide anticipatory guidance To educate about sign/symptoms of maternal depression To obtain postpartum care To provide parenting education To assist with locating resources To provide anticipatory guidance To provide benefits of breast vs. bottle feeding To assist with locating resources To establish trusting DCC/client relationship To establish trusting DCC/guardian relationship
Please list others: Please list others
ACTIVITIES TO BE COMPLETED TO MEET GOALS TARGET DATE
COMPLETED DATE Prenatal Infant
Client will: Client will: Keep all doctor appointments Choose a doctor and keep appointments Keep all WIC appointments Keep all WIC appointments Eat a nutritious diet recommended for pregnancy Get all immunizations according to schedule Remain tobacco, alcohol and drug free Maintain diet recommended for age Maintain a smoke free environment Provide a smoke free environment Recognize signs/ symptoms of pre-term labor Practice safe sleeping Maintain safe environment Provide safe care during feeding, changing and transportation Report any health concerns to DCC and physician Bond with infant and provide adequate stimulation for growth and development Keep Medicaid card and HMO current Recognize signs/symptoms of illness and seek medical care
DCC will: Report any health concerns to DCC and physician Screen for depression and help client recognize signs/symptoms DCC will: Promote oral health Promote oral health Teach about components of adequate prenatal care Promote mother/infant bonding Provide education on labor and delivery Make referrals as needed Provide education on family planning choices Establish trusting DCC/client relationship Make referrals as needed Please list others: Establish trusting DCC/client relationship
Please list others: Copy of completed, signed and dated Service Care Plan to be given to client on the date client signs the plan. __________________________________________________________________________________________________________________________________________ Client Signature Date DCC Signature Date Service Care Plan Revision: __________________________________________________________________________________________________________________________________________ Client Signature Date DCC Signature Date

OMCFH/RFTS-R011C-Blank White: DCC Revised: 12/2011 Pink: RCC Yellow Client Goldenrod: Provider
RIGHT FROM THE START PROGRAM
SERVICE CARE PLAN Closure Date: Closure Code: A B
CLIENT NAME MEDICAID NO. SOC. SECURITY # PRENATAL
(Last) (First) (MI)
INFANT
IDENTIFIED NEEDS
Prenatal DCC Client Infant DCC Client
GOALS TO BE COMPLETED TO MEET IDENTIFIED NEEDS TARGET
DATE COMPLETED
DATE Prenatal Infant
ACTIVITIES TO BE COMPLETED TO MEET GOALS TARGET DATE
COMPLETEDDATE Prenatal Infant
Copy of completed, signed and dated Service Care Plan to be given to client on the date client signs the plan. __________________________________________________________________________________________________________________________________________ Client Signature Date DCC Signature Date Service Care Plan Revision: __________________________________________________________________________________________________________________________________________ Client Signature Date DCC Signature Date

Office of Maternal, Child and Family HealthRIGHT FROM THE START PROGRAM
Progress Notes
WVDHHR/BPH/OMCFH/DPWH/PP/RFTS/R015-Progress Notes(Savable) Revised 5-12 DCC-Original/RCC-Copy
MI
*DCC Signature required for each entry
Prenatal Infant
Name: DCC:
SSN: Agency:
Date Time In/Out Comments
First TitleLast

*SEPARATE FORMS FOR MULTIPLE BIRTHS White:RCC OMCFH/RFTS-R019 Yellow:DCC Revised 5-2012 (Infants only) Pink:HMO
Goldenrod:RCC
RIGHT FROM THE START PROGRAM ALTERNATE ENTRY REFERRAL OF INFANTS/PRENATALS TO RFTS*
*Infant's Name: _________________________________ (Last) (First) (MI)
SSN: _________________________________________
Birth Score ID #: ____________________________________
Hospital of Delivery:_______________________________________
*Date of Birth: ____/___/_____ Sex: Female Male
Birth Weight: ___________ Birth Score: _____________
*Mother/Guardian Name: _____________________________
Address: __________________________________________
__________________________________________________
Mother/Guardian SSN: _______________________________
Mother/Guardian DOB: __________ County: _____________
Telephone: ________________________________________
Medicaid Number: __________________________________
Child Mother/Guardian Effective Date: ___________
HMO Plan: _________________________________________
HMO No.: __________________________________________
Effective Date: _____________________________________
Name & Address of Physician:________________________
__________________________________________________
__________________________________________________
Telephone: ________________________________________
Concerns: _________________________________________
__________________________________________________
__________________________________________________
Newborn Hearing Screening Pass Fail Unknown
*Prenatal Name: _____________________________________ (Last) (First) (MI)
SSN: ______________________________________________
Address: ___________________________________________
___________________________________________________
Telephone: _________________________________________
*Date of Birth: _____/_____/_____
EDC: ____/______/______
County: ___________________________________________
RFTS Maternity Services Medicaid Insurance
RFTS/Medicaid No.: ________________________________
Effective Date: ______________________________________
HMO Plan: _________________________________________
HMO No.: __________________________________________
Effective Date: ______________________________________
Name & Address of Physician:
___________________________________________________
___________________________________________________
___________________________________________________
Telephone: _________________________________________
Concerns: __________________________________________
___________________________________________________
___________________________________________________
___________________________________________________
___________________________________________________ Referral Closure Codes (For DCC Use) Date:______________ B-01 Spontaneous Abortion B-06 Unable to Establish contact B-02 Induced Abortion B-07 Refused Services B-03 Moved out of state B-08 Death B-04 Transferred out of region B-14 Did not meet eligibility
Protective Service Referral: _________________________________ Case Worker: ___________________________________
Referred to RFTS by: ___________________________________________________ Date: ______________________________
Site: _________________________________________________________________ Telephone: _________________________
Date Received: ___________________________________________ Date of Approval: ________________________________
Referred to (DCC Agency): __________________________________________________________________________________
Recommendations: ________________________________________________________________________________________
Signature: _________________________________________________________ Date: ________________________________ (Regional Care Coordinator)
DCC is to return a copy of form to RCC with appropriate code checked if unable to complete the Initial Client Assessment (R036) * Required fields
OMCFH/RFTS-R022 White - DCC Revised 6-2012 Yellow - RCC
Pink - Provider
OFFICE OF MATERNAL, CHILD AND FAMILY HEALTH RIGHT FROM THE START PROGRAM
OUTCOME MEASURES AT CASE CLOSURE
__________________________________________________________________________________________________________ *Last Name *First Name (MI)
_________________________________________________ *Birthdate: __________________ *Social Security No. (Mother) *Coverage Type: Medicaid
*Medical Card No.: ______________________________________ RFTS Maternity Services HMO PRENATAL OUTCOME MEASURES AT CASE CLOSURE Closure: Complete Incomplete *PHYSIOLOGY OF LABOR AND DELIVERY Delivery Date: _________ Maternal complications during labor and delivery: Yes No
List:____________________________________________________
If yes, did patient deliver at a Tertiary Care Center? Yes No
*NUTRITION/FITNESS/DRUGS Maternal Alcohol and/or Drug Abuse: Yes No Gestational Diabetes Yes No
Did patient miscarry? Yes No *POSTPARTUM CARE Kept postpartum appointment Yes No Referred: ___________________________________________________
*CONTRACEPTIVE CARE Did the mother start a method of birth control after delivery? Yes No If no, Family Planning Referral: Yes No
Referred to:_________________________________________________
*SMOKING CESSATION (Self reported) Remained quit Yes No ETS exposure at closure Yes No Referred to WV Quitline Yes No
Infant 1 Female Male Infant 2 Female Male Infant 3 Female Male Infant 4 Female Male
Vag C-S VBAC Gest. Age (Wks) Birth Defects Yes No NICU Stay # Days: ______ Infant Death
Vag C-S VBAC Gest. Age ________(Wks) Birth Defects Yes No NICU Stay # Days: ______ Infant Death
Vag C-S VBAC Gest. Age ________(Wks) Birth Defects Yes No NICU Stay # Days: ______ Infant Death
Vag C-S VBAC Gest. Age _______(Wks) Birth Defects Yes No NICU Stay # Days: ______ Infant Death
Did the mother breastfeed at hospital discharge? Yes No Breastfeeding at closure? Yes No Number of weeks breastfed: <1 1-6 7+
Did the mother breastfeed at hospital discharge? Yes No Breastfeeding at closure? Yes No Number of weeks breastfed: <1 1-6 7+
Did the mother breastfeed at hospital discharge? Yes No Breastfeeding at closure? Yes No Number of weeks breastfed: <1 1-6 7+
Did the mother breastfeed at hospital discharge? Yes No Breastfeeding at closure? Yes No Number of weeks breastfed: <1 1-6 7+
Was the infant’s birth weight: Very Low Birth Weight <1500 gm Low Birth Weight 1500-2500 gm
Normal Birth Weight >2500 gm Weight: ______________(lbs/ozs) ______________(Grams)
Was the infant’s birth weight: Very Low Birth Weight <1500 gm Low Birth Weight 1500-2500 gm
Normal Birth Weight >2500 gm Weight: ______________(lbs/ozs) ______________(Grams)
Was the infant’s birth weight: Very Low Birth Weight <1500 gm Low Birth Weight 1500-2500 gm
Normal Birth Weight >2500 gm Weight: ______________(lbs/ozs) ______________(Grams)
Was the infant’s birth weight: Very Low Birth Weight <1500 gm Low Birth Weight 1500-2500 gm
Normal Birth Weight >2500 gm Weight: ______________(lbs/ozs) ______________(Grams)
Type of Infant Risk Score? Low Birth Score < 99 High Birth Score > 100 Developmental Risk Hearing Impairment
Type of Infant Risk Score? Low Birth Score < 99 High Birth Score > 100 Developmental Risk Hearing Impairment
Type of Infant Risk Score? Low Birth Score < 99 High Birth Score > 100 Developmental Risk Hearing Impairment
Type of Infant Risk Score? Low Birth Score < 99 High Birth Score > 100 Developmental Risk Hearing Impairment
Use of safety seat for infant transport: Yes No
Use of safety seat for infant transport: Yes No
Use of safety seat for infant transport: Yes No
Use of safety seat for infant transport: Yes No
INFANT OUTCOME MEASURES AT CASE CLOSURE Closure: Complete Incomplete
*WELL CHILD CARE
Has child kept 5 well child visits with Pediatric Care Provider? Yes No Immunizations up to date: Yes No If no, referred: Yes No CHIP referral Yes No PCP at closure Yes No If no, referred Yes No
*SAFETY Does mother use a child safety seat to transport child? Yes No
*NICU STAY Yes No
Tertiary Care Center: __________________________________________
*BREASTFED Months <1 1-6 7+
DCC Signature: _________________________________________________________________ *Service Date: __________________________ Agency: _______________________________________________________________________ *County: ______________________________ (Do not complete on client transfers – DCC who receives transferred case to complete upon case closure)
* Required Fields

OMCFH/RFTS-R025 White: WIC Revised: 3/2012 Yellow: DCC Pink: RCC
RIGHT FROM THE START PROGRAM RFTS/WIC PARTICIPANT REQUEST FOR INFORMATION
(TO BE COMPLETED BY THE RIGHT FROM THE START DESIGNATED CARE COORDINATOR)
PRENATALS
Participant Name: ____________________________________________ Last Name First Name (MI)
Participant Address: __________________________________________
____________________________________________________________
INFANTS
Parent's Name: ______________________________________________ Last Name First Name (MI)
Parent's Address: ____________________________________________
SPECIFIC INFORMATION REQUESTED
Diet History
24 Hour Recall
Height/Length
Weight
Hemoglobin/Hematocrit
Head Circumference
Birth Weight
Weight Gain During
Pregnancy
Pre-Pregnancy Weight
Verification of Appointments
Current Status as WIC
Participant
Breastfeeding Status
____________________________________________________ ______________________ Signature - RFTS Designated Care Coordinator Date
PLEASE SEND REQUESTED
INFORMATION TO
____________________________________________________________ ____________________________________________________________ ____________________________________________________________ ____________________________________________________________
(For completion by WIC Staff)
Check if verbal request ______________________________ Date request received
____________________________________________ ______________________________
Signature of WIC Staff Date responded to request

WVDHHR/BPH/OMCFH/DPWH/RFTS/R036a – Initial Client Assessment Prenatal/Revised 9-19-2011 Page 1
Right From The Start Program Initial Client Assessment – Prenatal
Name: Last First MI Date of Birth: Age: Social Security #:
Address: Street City State Zip Code
County of Residence: Telephone #: Alternate #: Current Address: (if not staying at home) Street City Zip Code
Directions to home:
Race: White Black/African American Asian American Indian/Alaska Native Native Hawaiian/Pacific Islander Ethnicity: Hispanic/Latino Not Hispanic/Latino (Check all that apply)
U.S. Citizen: Yes No
Marital Status: Single Married Separated Widow Divorced
Employed: Yes No Medicaid/RFTS Maternity Services/HMO Name & Number:
OB Provider Name & Number:
Emergency Contact: Telephone #: Relationship to Client:
Address: Street City Zip Code
PREGNANCY HISTORY Gravida Para #Abortions (insert # in box) # Living Children Past Deliveries (insert # in box) Spontaneous: Vaginal: VBAC: C-Section:
Induced: Reason for C-Section:
Complications with Past Deliveries:
CURRENT PREGNANCY
Estimated Date of Delivery (EDD): Trimester for initial prenatal visit: 1st 2nd 3rd Present illness (non-pregnancy related):
Current Medications (prescription or OTC):
MEDICAL HISTORY
Illness/Disease Yes No Assistance Needed Referred To Diabetes
Gestational Diabetes
History of Gestational Diabetes
Heart Disease/Defect
Birth Defect
Physical Impairment/Disability
Mental Impairment/Disability
High/Low Blood Pressure
Seizures
Stressful Life Event
STDs
History or Risk of Depression
History of Postpartum Depression
History Psychiatric Illness
Past Date: Diagnosis:
Present Date: Diagnosis:
Therapist:
WVDHHR/BPH/OMCFH/DPWH/RFTS/R036a – Initial Client Assessment Prenatal/Revised 9-19-2011 Page 2
MATERNAL LEGAL HISTORY Issue Yes No Assistance Needed Referred To
Is client a minor? If yes, who is your legal guardian?
CPS Involvement? Past Current Self Child(ren)
Describe:
Involvement with criminal justice system? If yes, Past Current
Self Partner Other
Describe (charges, dates, findings, incarceration, probation):
EDUCATION
Issue Yes No Assistance Needed Referred To Currently in school?
Name of School: Purpose:
Years of school completed (list number in box): 1-12 12+
Degree obtained: GED High School Diploma Certification College Degree
Learning Style: Visual Auditory Tactile Unknown
Special Education History:
Future Education Plans:
Employment Goals:
SUPPORT SYSTEM Father of Baby: Last First MI
Age: Supportive: Yes No Living with Client: Yes No
Other household members:
Name Age Relationship to client
Other Support:
Children living outside home:
Name Age In custody of
LIVING ARRANGEMENTS Where client lives √ Monthly Expenses √ Amount Total monthly family income √ Amount
Own Home House Payment Employment
Mobile Home Rent Payment Disability
Apartment Utilities Child Support
Public Housing Loans Spousal Support
Foster Home Car Payment Food Stamps
Parent’s Home Other Loans
Friend’s Home Settlement
Shelter None
Homeless Other
Other

WVDHHR/BPH/OMCFH/DPWH/RFTS/R036a – Initial Client Assessment Prenatal/Revised 9-19-2011 Page 3
ENHANCED SERVICES - NUTRITION
Issue Yes No Assistance Needed Referred To Med. condition requiring dietary modification
Nausea/Vomiting
Non-food cravings (if yes, list below)
(Type):
Frequently skips meals/fasts/binges
Bulimia/Anorexia or History
Food allergy or intolerance
Prior nutritional counseling
Dental impairment affecting diet
ENHANCED SERVICES – PREVENTIVE SELF CARE/CHILDBIRTH EDUCATION
Issue Yes No Assistance Needed Referred To Poor previous pregnancy experience
Significant apprehension/anxiety
Poor pregnancy information
Lack of knowledge of risk factors
Lack of knowledge of prescribed Tx
Non-compliant with prescribed Tx
Unrealistic expectations for infant
Desires parenting/infant care education
Desires information on infant development
Non-stimulating environment for infant
Desires childbirth education
HOME/FAMILY NEEDS ASSESSMENT
Issue Yes No Assistance Needed Referred To Adequate housing
Safe neighborhood
Adequate space
Heating/cooling adequate
Environmental Tobacco Smoke
CPR Training
Transportation
Bathtub/Shower
Hot water
Concern about unsafe water (if yes, list below)
(Concerns):
Toilet Facilities
Enrolled in WIC
Safe Crib/Bedding
Baby care items needed
Working fire extinguisher
Working smoke detector
Working Carbon Monoxide Detector
Fire escape plan
Refrigerator
Cooking facilities
Telephone access
Washer/Dryer
Pets (explain dangers of cat litter)
Child care plan (if no, refer)
Adequate support system
Service providers in home (if yes, list below)
(Service providers in home):

WVDHHR/BPH/OMCFH/DPWH/RFTS/R036a – Initial Client Assessment Prenatal/Revised 9-19-2011 Page 4
HOME/FAMILY NEEDS ASSESSMENT – Con’t Issue Yes No Assistance Needed Referred To
Bed sharing
Risks explained
Co-sleeping (room sharing)
Concern about mother’s feelings regarding pregnancy/parenting/infant
Unplanned Unwanted Ambivalent Happy Nervous
Concern about biological father/partner’s feelings regarding pregnancy/parenting/infant
Accepting Denying Rejecting Unable to assess Happy
Recent loss of partner
Abandonment Separation/divorce Death Other
Current conflict in home
Parent(s) Partner Other
Dysfunctional family relations
Abuse in past year
Physical Verbal Sexual Other
Religious/ethnic/cultural factors affecting pregnancy outcome
Two (2) or more preschool children in home
Poor/ineffective parenting
Difficulty budgeting money/food stamps
Handicapped/disabled family member
Illiteracy (self)
Illiteracy (partner)
Smoker
CPD: SCRIPT presented: Yes No SCRIPT Refused:
CO level obtained
Refused CO Breathalyzer:
2nd hand smoke exposure
Current medications
Alcohol/Drug use (If yes, describe)
(Describe):
Special needs for child(ren)
Adequate food
Past surgery(ies)
OTHER REFERRALS/NOTES
DCC Signature: Title: Agency: Region: Date:
Please remember to forward a signed copy to RCC.
WVDHHR/BPH/OMCFH/DPWH/RFTS/R036b – Initial Client Assessment Infant/Revised 9-19-2011 Page 1
Right From The Start Program Initial Client Assessment – Infant
Name: Last First MI Date of Birth: Male Female Social Security #:
Address: Street City State Zip Code
County of Residence: Telephone #: Alternate #:
Current Address: (if not staying at home) Street City State Zip Code
Directions to home:
Medicaid/HMO Name: Medicaid/HMO #:
Birth Score (high or low):
U.S. Citizen: Yes No
Race: White Black/African American Asian American Indian/Alaska Native Native Hawaiian/Pacific Islander Ethnicity: Hispanic/Latino Not Hispanic/Latino (Check all that apply)
Birth Weight:
Birth Score ID:
Apgar: 1 min. 5 min. Gestational Age (#wks)
Birth Facility:
Parent/Guardian Last First MI If not parent, relationship to infant:
Pediatrician Phone#:
Name of Emergency Contact: Telephone #: Relationship to Client:
Address: Street City State Zip Code
Father of infant: Last First MI Age: Living with client
MEDICAL HISTORY
Issue Yes No Assistance Needed Referred To
Illnesses/Conditions:
Respiratory Distress
Hyperbilirubinemia
Seizures
IVH
Visual Impairment
Hearing Impairment
Herpes
Chlamydia
Hepatitis
HIV
Sickle Cell
Down’s Syndrome
Cystic Fibrosis
Genetic Disorder
WVDHHR/BPH/OMCFH/DPWH/RFTS/R036b – Initial Client Assessment Infant/Revised 9-19-2011 Page 2
MEDICAL HISTORY – Con’t Issue Yes No Assistance Needed Referred To
Drug Addicted
Past Surgery(ies)
Other
NICU stay Days Weeks Months (Check one)
High Risk Clinic
Need for Specialty Physician(s)
History Psychiatric Illness (mother/father)
Breast Feeding
Bottle Feeding
Formula changes
Fluoride Supplement
Feeding Problems
Diarrhea/Constipation
Started Solid Foods Type: Started:
Other Beverages Type: Started:
Current Medicines Type: How Often:
Techonology Dependent Type:
Newborn Hearing Screening Done
Date L Passed Failed R Passed Failed
Rescreen Date L Passed Failed R Passed Failed
If failed rescreen, date referred: Audiologist Sky Hi* BTT CSHCN
Other health issues (list):
LIVING ARRANGEMENTS
Where client lives √ Family monthly expenses √ Amount Total monthly family income √ Amount Parents Own Home House Payment Employment
Mobile Home Rent Payment Disability
Apartment Utilities Child Support
Public Housing Loans Spousal Support
Foster Home Car Payment Food Stamps
Friend’s Home Other Loans
Shelter Settlement
Homeless None
Other Other

WVDHHR/BPH/OMCFH/DPWH/RFTS/R036b – Initial Client Assessment Infant/Revised 9-19-2011 Page 3
HOME/FAMILY NEEDS ASSESSMENT
Issue Yes No Assistance Needed Referred To
Adequate housing
Safe neighborhood
Adequate space
Heating/cooling adequate
Environmental Tobacco Smoke
Parent(s) CPR Training
Transportation
Bathtub/Shower
Hot water
Concern about unsafe water (if yes, list below)
(Concerns):
Toilet Facilities
Enrolled in WIC
Safe Crib/Bedding
Baby care items needed
Working fire extinguisher
Working smoke detector
Working Carbon Monoxide Detector
Fire escape plan
Refrigerator
Cooking facilities
Telephone access
Washer/Dryer
Pets
Child care plan (if no, refer)
Adequate support system
Service providers in home (if yes, list below)
(Service providers in home):
CPS Involvement (Parent/Guardian) Past Present If yes, describe
Bed sharing
Risks explained
Co-sleeping (room sharing)
Concern about mother/guardian’s feelings regarding parenting/infant
Unplanned Unwanted Nervous Ambivalent Happy
WVDHHR/BPH/OMCFH/DPWH/RFTS/R036b – Initial Client Assessment Infant/Revised 9-19-2011 Page 4
HOME/FAMILY NEEDS ASSESSMENT – Con’t
Issue Yes No Assistance Needed Referred To Concern about biological father/guardian’s feelings regarding parenting/infant
Accepting Denying Rejecting Unable to assess Happy
Parent’s recent loss of partner
Abandonment Separation/divorce Death Other
Current conflict in home
Parent(s)/guardian Partner of parent Grandparents Other
Dysfunctional family relations
Abuse in past year (mother of infant)
Physical Verbal Sexual Other
Religious/ethnic/cultural factors affecting access to healthcare
Two (2) or more preschool children in home
Poor/ineffective parenting
Family difficulty budgeting money/food stamps (inappropriate spending)
Handicapped/disabled family member
Illiteracy (parent/guardian)
2nd hand smoke exposure
Provide education on smoke free environment Refused
Parent/guardian alcohol/drug use
(If yes, describe):
Special healthcare needs
Adequate food for family
Parent/guardian significant apprehension/anxiety
Lack of knowledge for prescribed Tx
Non-compliant with prescribed Tx
Unrealistic expectations for infant
Desires parenting/infant care education
Desires information on infant development
Non-stimulating environment for infant
OTHER REFERRALS/NOTES
DCC Signature: Title: Agency: Region: Date:
Please remember to forward a signed copy to RCC.

West Virginia Birth Score Program High Birth Score Referral and Tracking Form
Date of Birth Mother's SSN: Address:
Pay Type:
Case ID: Birth Score:
Mother's Name:
Phone:
Birth Hospital:
Primary Care Physician: PCP Phone:
GA Type
BWt. Grams Mom's Age Sex Feeding Prev. Preg Mom Ed. Nicotine
Factors
DCC/Health Check Worker Signature: Date:
Abnormality Left Ear:
Dev. Risk: VLBW APGAR <3 Hearing Screen Results: Test Type: Right Ear:
Transfer Hosp:
First Birth Score Surveillance Visit: Kept: Not Kept Unknown: (Within 3 weeks after discharge) Second Birth Score Surveillance Visit: Kept: Not Kept Unknown: (4-6 weeks after discharge) Enrolled in WIC: Enrolled in Health Check: Yes: No: Yes: No:
If infants PCP is not the same as above make corrections here and notify Birth Score Office: Infant's PCP/Clinic: PCP Phone PCP/Clinic Address:
Tracking Outcome: (Check all that apply for High Birth Tracking only) High Score Tracking Complete Moved Out of State Infant Death
Lost to Follow-up Refused High Score Follow-up Other: (Explain)
Agency: RCC County: Date Received From BSO: RCC Region:
Infant's Name:
Unable to Locate
R038A - High Birth Score Referral and Tracking Form WVDHHR/BPH/OMCHF/DPWH/RFTS/1-09
Birth Score Office
West Virginia University Birth Score Developmental Risk & Newborn Hearing Screen Program
Department of Pediatrics Post Office Box 9214
Morgantown, WV 26506-9214
DO NOT COPY BLANK FORM
Client Record RCC
Copy to:
Complete and submit to:

OFFICE OF MATERNAL, CHILD AND FAMILY HEALTH
Bureau for Public Health 350 Capitol Street, Room 427 Charleston, WV 25301-3714
Phone: (304) 558-5388 Toll-Free (in WV): 1-800-642-8522 or 1-800-642-9704 FAX: (304) 558-7164 OMCFH/RFTS-R039 White: Provider Revised: 6-2011 Yellow: DCC Pink: RCC
Michael J. Lewis, M.D. Ph.D. Cabinet Secretary
Earl Ray Tomblin Governor
STATE OF WEST VIRGINIA DEPARTMENT OF HEALTH AND HUMAN RESOURCES
RIGHT FROM THE START PROGRAM
_________________________________ (Date)
Re: ________________________________________ S. S. Number: _______________________________ Dear Provider, This is to inform you that this client's case record is being closed for Right From The Start services as of
_______________________________________. The reason for closure is indicated below:
REASON
Completed Program
Program Incomplete (If incomplete, please indicate reason below) Spontaneous Aborted Pregnancy Induced Aborted Pregnancy Moved Out-of-State Transferred Out of Region Death Lost to Follow-up Did not Meet Program Protocols Preterm Delivery Closed at RCC Level
Enhanced Services Only Sincerely, _____________________________________________ Designated Care Coordinator
_____________________________________________ Agency Name _____________________________________________ Agency Address _____________________________________________ Agency Telephone Number

OMCFH/RFTS-R040 White: DCC Revised 12-2011 Pink: RCC
Right From The Start Program QUALITY ASSURANCE REPORT (10 Infants and 10 Prenatals Quarterly)
PROVIDER AGENCY
PERSON COMPLETING THE FORM
Title: RN GN LSW TLSW Please indicate Y (Yes), N (No), or N/A (Not Applicable)
Client Name (Active File)
Dat
e R
ecei
ved
from
Reg
iona
l Le
ad A
genc
y
Doc
umen
tatio
n of
con
tact
w
ithin
10
wor
king
day
s
Ass
essm
ent &
Se
rvic
e C
are
Plan
com
plet
e
Rig
hts
&
Res
pons
ibili
ties
sign
ed a
nd in
ch
art
Mon
thly
co
ntac
ts
docu
men
ted
(A
t lea
st o
ne
HV)
Trac
king
she
ets
code
s &
uni
ts
prop
erly
use
d
Form
s se
nt to
R
CC
with
in fi
ve
(5) w
orki
ng
days
of s
ervi
ce
date
SCR
IPT
Form
s co
mpl
eted
Edin
burg
h Po
st
Nat
al
Dep
ress
ion
Scal
e (E
PDS)
Pre
nata
l
Pos
tpar
tum
Cas
es c
lose
d in
ap
prop
riate
m
anne
r with
cl
osur
e co
des
Out
com
es &
Ev
alua
tions
D
ocum
ente
d
1)
2)
3)
4)
5)
6)
7)
8)
9)
10)
11)
12)
13)
14)
15)
16)
17)
18)
19)
20)

REGIONAL CARE COORDINATORS TIME SHEET
WVDHHR/BPH/OMCFH/DPWH/PP/RFTS/R041A/10-06 Copy to OMCFH
ACTIVITY CODE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31MONTHLY TOTALS
Project Eligibility 1
Referral for Services/Tracking 2
Project Development/Training/ Technical Assistance
3
Client Tracking 4
Community Activities 5
Reports/Surveys/Billing /Budget Preparation 6
Outreach/Certification of Service Providers/Provider Recruitment
7
Time Off 8
Newborn Hearing Screening 9
Miscellaneous(Must include explanation of activities)
10
Daily Totals
REGIONDATES
STAFF PERSON AGENCY MONTH

REGIONAL CARE COORDINATORS TIME SHEET
WVDHHR/BPH/OMCFH/DPWH/PP/RFTS/R041A/10-06 Copy to OMCFH
DATE Miscellaneous Activity Explanations

REGIONAL CLERK TIME SHEET
WVDHHR/BPH/OMCFH/DPWH/PP/RFTS/R041B/10-06 Copy to OMCFH
ACTIVITY CODE 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31MONTHLY TOTALS
Computer Input100
Technical Assistance 101
Typing102
Copying103
Records104
Reports 105
Appointments106
Billing107
Training108
Tracking109
Time Off 115
Miscellaneous (Must include explanation of activities)
116
Daily Totals
REGIONDATES
STAFF PERSON AGENCY MONTH

REGIONAL CLERK TIME SHEET
WVDHHR/BPH/OMCFH/DPWH/PP/RFTS/R041B/10-06 Copy to OMCFH
Miscellaneous Activity ExplanationsDATE

OMCFH/RFTS-R042-DCC Contact Letter #3 White: Client Revised: 6/2011 Yellow: DCC
Earl Ray Tomblin Governor
Michael J. Lewis, M.D. Ph.D. Cabinet Secretary
STATE OF WEST VIRGINIA DEPARTMENT OF HEALTH AND HUMAN RESOURCES
RIGHT FROM THE START PROGRAM
_____________________________ (Date) Dear : We have not heard from you about Right From The Start. Right From The Start offers pregnant women and their babies free services to help keep them healthy. We can help you find things in your area that you may need, like WIC, a place to live, a way to get to the doctor, baby care items and other things you may need during this happy, but sometimes hard time. We can help you learn about things like:
• baby care • how to tell if your baby has a fever • how/why you may feel different when you’re pregnant • what you should eat • baby blues • and much more
If we do not hear from you by ______________________, we will know you are not interested in RFTS. I hope you will call about these free services. I look forward to hearing from you.
Sincerely,
Designated Care Coordinator
______________________________________ DCC Name (Please Print)
______________________________________ Agency
______________________________________ Agency Address
______________________________________
______________________________________ Telephone/Email
OFFICE OF MATERNAL, CHILD AND FAMILY HEALTH
Bureau for Public Health 350 Capitol Street, Room 427 Charleston, WV 25301-3714
Phone: (304) 558-5388 Toll-Free (in WV): 1-800-642-8522 or 1-800-642-9704 FAX: (304) 558-7164
OMCFH/RFTS-R042-DCC Contact Letter #3 White: Client Revised: 6-2011 Yellow: DCC
Michael J. Lewis, M.D. Ph.D. Cabinet Secretary
Earl Ray Tomblin Governor
ESTADO DE WEST VIRGINIA EL DEPARTAMENTO DE SALUD Y LOS RECURSOS HUMANOS
PROGRAMA DESDE EL PRINCIPIO
________________________________
(Fecha/Date) Estimada : No hemos oído de usted sobre el programa Desde el Principio. Desde el Principio puede asistirle a usted y su bebé encontrar cosas gratis que usted puede necesitar como WIC, un lugar para vivir, maneras para conseguir al doctor, cosas para su bebé y otros servicios que a lo mejor le falta durante este tiempo feliz aunque a veces difícil. Pueden ayudarle a aprender:
• maneras fáciles de tomar cuidado de su bebé • cómo saber si su bebé tiene una fiebre • porque se siente diferente cuando usted está embarazada • Lo que debe de comer • depresión postparto • y mucho mas
Si no comunicamos por el día ______________________, sabremos que no le interesa el programa Desde el Principio. Tengo esperanza que usted llamara sobre estos servicios gratuitos. Sinceramente, ________________________________ Designated Care Coordinator
________________________________ DCC Name (Please Print)
________________________________ Agency
________________________________ Agency Address
________________________________ Telephone/Email
OFICINA DE LA SALUD MATERNAL, DEL NIÑO Y DE LA FAMILIA Oficina para la salud pública 350 Capitol Street, Room 427 Charleston, WV 25301-3714
Telephono: (304) 558-5388 Gratis (en WV): 1-800-642-8522 or 1-800-642-9704 FAX: (304) 558-7164
RIGHT FROM THE START PROGRAMENHANCED SERVICES EDUCATION REPORT
WVDHHR/BPH/OMCFH/DPWH/PP/RFTS/R060 - SavableRevised 1-2010
Original: Enhanced Service ProviderCopy: OB (At case closure)
RCC (At case closure)RCC(Initial Assessment)
(S9442 HD)
Enhanced Services DCC Signature:
Verbal Approval Received from RCC on This
Date: No Refused
DCC’s Initials
Date:
Service Provider:
Referred for Right From the Start Care Coordination:
DCCs should complete a Tracking Sheet (RFTS-R001A) for each client encounter and submit it to the RCC within 5 working days.
(FOR USE BY AGENCIES THAT ONLY PROVIDE ENHANCED SERVICES EDUCATION)
Region #:RLA Name:
Medicaid: HMO #:
RFTS Maternity Services
Nutritional Evaluation/Counseling
Health Education
(S9452 HD)
(S9445 HD)
Childbirth Education
Parenting Education (S9444 HD)
Service Provided Date(s) CompletedEnhanced Service
RCC Name:
Yes
SS#:
Birth Date: Telephone #:
EDC:
Patient’s Name:
Address:
City State Zip
Last First MI

White: DCC Yellow: RCC WVDHHR/BPH/OMCFH/PWH/PP/RFTS/R065 Pink: OB Provider 4/2012 Goldenrod: Client
RIGHT FROM THE START PROGRAM EDINBURGH POSTNATAL DEPRESSION SCALE (EPDS)
*Name: _____________________________________________________________ Last First MI
*Social Security #: ___________________________ *DOB: ___________________
*Prenatal *Pregnancy Due Date: __________________ *Postpartum *Baby’s DOB: __________________________
Because you are pregnant or you have recently had a baby, which can often result in mood changes, we would like to know how you are feeling. Please underline the answer which comes closest to how you have felt IN THE PAST SEVEN (7) DAYS, not just how you feel today. Please complete all ten items.
1. I have been able to laugh and see the funny side of things.
As much as I always could Not quite so much now Definitely not so much now Not at all
_________
Score
2. I have looked forward with enjoyment to things.
As much as I ever did Rather less than I used to Definitely less than I used to Hardly at all
_________
Score
3. I have blamed myself unnecessarily when things went wrong.(*)
Yes, most of the time Yes, some of the time Not very often No, never
_________
Score
4. I have been anxious or worried for no good reason.
No, not at all Hardly ever Yes, sometimes Yes, very often
_________
Score
5. I have felt scared or panicky for no very good reason. (*)
Yes, quite a lot Yes, sometimes No, not much No, not at all
_________
Score
6. Things have been getting the best of me. (*)
Yes, most of the time I haven’t been able to cope at all Yes, sometimes I haven’t been coping as well as usual No, most of the time I have coped quite well No, I have been coping as well as ever
_________
Score
7. I have been so unhappy that I have had difficulty sleeping. (*)
Yes, most of the time Yes, sometimes Not very often No, not at all
_________
Score
8. I have felt sad or miserable. (*) Yes, most of the time Yes, quite often Not very often No, not at all
_________
Score
9. I have been so unhappy that I have been crying. (*)
Yes, most of the time Yes, quite often Only occasionally No, never
_________ Score
10. The thought of harming myself has occurred to me. (*)
Yes, quite often Sometimes Hardly ever Never
_________
Score
Client’s Signature: ______________________________________________________________ Date: ________________________
DCC Signature: ________________________________________________________________ Date: ________________________
DCC Agency: _________________________________________________________________________________________________
*EPDS Score: *Referred to : Medical Provider *Date: ____________________________ Emergency Room
*Required Fields

White: DCC Yellow: RCC WVDHHR/BPH/OMCFH/PWH/PS/RFTS/R065
Pink: OB Provider
1-03 Goldenrod: Client
Edinburgh Post-Partum Depression Screen Information (EPDS)
Instructions for Users: 1. The mother is asked to underline the response which comes closest to how she has been feeling in the
previous seven (7) days. 2. All ten (10) items must be completed. 3. Care should be taken to avoid the possibility of the mother discussing her answers with others. 4. The mother should complete the scale herself, unless she has limited English or has difficulty with
reading. Scoring Response categories are scored 0, 1, 2, 3 according to increased severity of the symptoms. Items marked with an asterisk (*) are reverse scored (i.e. 3, 2, 1 & 0). The total score is calculated by adding together the scores for each of the ten items. Use Users may reproduce the scale without further permission providing they respect copyright by quotinga the names of the authors, the title and the source of the paper in all reproduced copies. Interpretation ⊄ Women who score above the threshold of 12 to 13 are likely experiencing an episode of depression and
must be referred to a physician or mental health care provider. If evidence of suicidal tendencies/hopelessness exists, establish a safety plan with the client/family and arrange urgent (24 - 48 hrs.) or emergency evaluation at a Mental Health Center or Emergency Room based on your assessment.
⊄ A score of 9-11 might indicate depression. A careful assessment should be carried out to confirm the
diagnosis, and in uncertain cases it may be useful to repeat the EPDS after two (2) weeks. ⊄ A score of 0 - 8 may indicate minimal/mild depression. The client should be carefully assessed and the
RFTS individualized service care plan followed. If questions or concerns arise, the screen should be repeated.
a Reprint with permission from: Cox, J. L., Holder, J. M., & Sagovsky, R. (1987). Detection of postnatal depression: Development of the 10-item Edinburgh Postnatal Depression Scale. British Journal of Psychiatry, 150, 782 - 786.

WVDHHR/BPH/OMCFH/DPWH/PP/RFTS TS001 Page 1 of 1 June 11, 2008
RIGHT FROM THE START PROJECT (RFTS) TS001 TOBACCO SCREENING FORM
Prenatal CO VALUE PPM Postpartum Refused
# of weeks: Equipment Problem Date: / / Explanation in Progress Notes MM DD YYYY
Date of Birth: / / SSN: - -
Name: Last Name MI First Name
County: Region: DCC ID#: DCC Name: Agency Name:
1. Which statements best describes your tobacco use now? (choose all that apply) I have never smoked cigarettes. (Mark here if you have only tried smoking) I stopped smoking BEFORE I found out I was pregnant - I am not smoking. I stopped smoking AFTER I found out I was pregnant - I am not smoking. I dip, chew, or use smokeless tobacco. I smoke regularly now-about the same number BEFORE I became pregnant.
Number of cigarettes I smoke each day: I smoke, but I cut down on the number of cigarettes I smoke AFTER I became pregnant.
Number of cigarettes I smoke each day: I have increased smoking since I found out I was pregnant. I have started smoking since I found out I was pregnant.
2. How many cigarette smokers live in the same house with you? (choose only one) 0 1 2 or more
3. How is cigarette smoking handled where you live? (choose only one) No one smokes where I live - they smoke outside. People may only smoke in certain rooms where I live. People may smoke anywhere I live.
4. How many of your family and friends are cigarette smokers? (choose only one). None A few Some Most
If Never Smoked or Recently Quit - STOP HERE / Continue ONLY if Currently Smoking
5. How soon after you wake up do you usually use tobacco? (choose only one). 5 minutes or less 6 to 30 minutes 31 to 59 minutes 1 to 2 hours Greater than 2 hours
6. How sure are you that you could/can stop smoking for 24 hours? (choose only one). Low 1 2 3 4 5 6 7 8 9 10 High
7. How harmful do you feel cigarette smoking or smokeless tobacco is to you? (choose only one). Low 1 2 3 4 5 6 7 8 9 10 High
8. How harmful do you feel cigarette smoking or smokeless tobacco is to your baby? (choose only one). Low 1 2 3 4 5 6 7 8 9 10 High
9. Do you want to quit? Yes No
10. The SCRIPT Program provided me with: (choose all that apply). Guide Counseling Time Spent (in minutes)
11. My doctor advised me to quit. Yes No
12. I have used the WV Quitline. Yes No
RCC DCC OB Provider Client
WVDHHR/BPH/OMCFH/DPWH/PP/RFTS TS002 Page 1 of 1 June 11, 2008
RIGHT FROM THE START PROJECT (RFTS) TS002 TOBACCO FOLLOW-UP FORM
Prenatal CO VALUE PPM Postpartum Refused
Follow-Up #: Equipment Problem Date: / / Explanation in Progress Notes MM DD YYYY
Date of Birth: / / SSN: - -
Name: Last Name MI First Name
County: Region: DCC ID#: DCC Name: Agency Name:
1. Have you smoked a cigarette, even one puff, within the last 7 days? (choose only one) Yes No Never Smoked
2. Since you started maternity care with the Right From The Start Project (RFTS) has the smoking pattern changed where you live? (choose all that apply)
No change. I have started/increased smoking since pregnant. No one smokes where I live – they People may smoke anywhere I live. smoke outside. People may smoke in certain rooms.
If Never Smoked - STOP HERE
3. Since your first RFTS home visit, which statements best describes your cigarette smoking? I smoke about the same number. Number of cigarettes smoked each day: I smoke, but I have cut down on the number of cigarettes. Number of cigarettes smoked each day: I have started/increased smoking. Number of cigarettes smoked each day: I dip, chew, or use smokeless tobacco. I have quit!
4. If you are a smoker, how many times since your first RFTS visit have you made a serious attempt to stop smoking (went without a cigarette for at least 24 hours). (choose only one)
0 1 2 3 I have quit!
5. How soon after you wake up do you usually smoke your first cigarette or use other tobacco? (choose only one) 5 minutes or less 6 to 30 minutes 31-59 minutes 1 to 2 hours Greater than 2 hours I am not smoking!
6. Since you started RFTS, has your DCC provided the following: (choose only those methods provided) I received no information. I watched the "Commit To Quit" video. My Right From The Start worker counseled me to quit. I was advised to call the WV Quitline. I was given A Pregnant Woman's Guide To Quit Smoking. My DCC called me on my quit date.
7. a. My doctor advised me to quit. Yes No b. My doctor advised me to call the WV Quitline. Yes No c. I called the WV Quitline. Yes No d. The WV Quitline called me. Yes No
8. I found the SCRIPT Program helpful? (choose only one). Low 1 2 3 4 5 6 7 8 9 10 High
9. During this pregnancy, has anyone who is living with you: a. Tried to quit smoking. Yes No b. Successfully quit smoking. Yes No
RCC DCC OB Provider Client
WVDHHR/BPH/OMCFH/DPWH/PP/RFTS TS006 Page 1 of 1 April 2012
RIGHT FROM THE START PROGRAM (RFTS) TS006 SCRIPT INTERVENTION FORM
Prenatal CO VALUE PPM Postpartum Record CO value if not measured
Date: at Screening Visit MM DD YYYY
Date of Birth: SSN:
Name: Last Name MI First Name
County: Region: DCC ID#: DCC Name: Agency Name:
1. ASK < 1 Minute
Document smoking status and number of cigarettes per day (CPD): (# cigarettes per day) A. Quit since screening visit B. Smoker
Response A. Congratulate her on success - stop home and social ETS exposure Response B. ASSESS, ADVISE, ASSIST AND ARRANGE
2. ASSESS < 1 Minute
Readiness to quit Yes No (If No, stop here)
3. ADVISE < 1 Minute
Provide clear, strong messages about risks of smoking to mother/fetus Yes No • Provide clear, strong and personal advice to quit and stay quit • Advise client to stop ETS exposure • Review "Commit to Quit" Video
4. ASSIST > 15-20 Minutes Provide SCRIPT Overview • Provide A Pregnant Woman's Guide to Quit Smoking Briefly review cessation skills in the "Commit To Quit" Video and the Guide: • STEP 1: Review Agreement to Quit, sign the contract and set Quit Date (Page 3) • STEP 2: Review Smoking Diary - #cpd (Page 4) • STEP 3: Review Scheduled Smoking (Page 5) • STEP 4: Review Yuck Jar (Page 6) • STEP 5: Promote Deep Breathing (Page 6) • STEP 6 & 7: Review Stop Smoking Buddy (Pages 8 to 11) • STEP 8: Learn Smoke - Tasting (Page 13) • STEP 9: Review Smoking Alternatives (Page 14) • STEP 10: Review Smoking Habits (Page 16) Express confidence that use of the Guide and methods will help them quit • Build Self-Efficacy (Page 19)
5. ARRANGE < 1 Minute
• Remind client of next visit and label as "smoker" in notes • Explain/schedule DCC follow-up telephone call(s) • Recommend call WV Quitline • Recommend talk with doctor about quitting
Summarize counseling session:
RCC DCC OB Provider Client

WVDHHR/BPH/OMCFH/DPWH/PP/RFTS/9-2010 1
Regional Care Coordinator:
Counties Served:
Add, Delete or Continue
County Codes Served by DCC
RN FT Yes Yes Yes
LSW PT No No No
TLSW
RN FT Yes Yes Yes
LSW PT No No No
TLSW
RN FT Yes Yes Yes
LSW PT No No No
TLSW
RN FT Yes Yes Yes
LSW PT No No No
TLSW
RN FT Yes Yes Yes
LSW PT No No No
TLSW
RN FT Yes Yes Yes
LSW PT No No NoTLSW
Date Date
PART ARIGHT FROM THE START PROGRAM
DESIGNATED CARE COORDINATORS AND ENHANCED SERVICES PROVIDERS
*Provider/Agency must complete a "Part A" for each region they serve or each site within the same region.
Region : Please indicate: FT = Full Time or 2080 Hours a Year (100% RFTS) PT = Part Time (< 100% RFTS)
Provider Agency:
Street Address:
City/State/Zip:
City/State/Zip:
Regional Lead Agency:
Address:
As you have additions or deletions to this listing, please send an updated copy to the Regional Lead Agency. RCC must send a copy of each Part A including additions/deletions to the OMCFH/RFTS office. NEW DCCs MAY NOT PROVIDE SERVICES UNTIL APPROVED AND TRAINED BY THE RCC. New Agencies may not provide services until approved by OMCFH, WV Medicaid and Health Maintenance Organizations (HMOs).
DCC Email Address
"I certify that the individual(s) listed above meet the qualifications outlined in the OMCFH RFTS Program Policy and Procedures Manual and will provide services to RFTS eligible clients according to protocol outlined in the Manual."
License or Certificate Expiration
Date
Administrative Person Viewing Licensure (DCC Agency) Regional Care Coordinator
Enhanced Services
Care Coord. Prenatals
Care Coord. Infants
Full or Part TimeName of DCC Title
Telephone/Fax#:
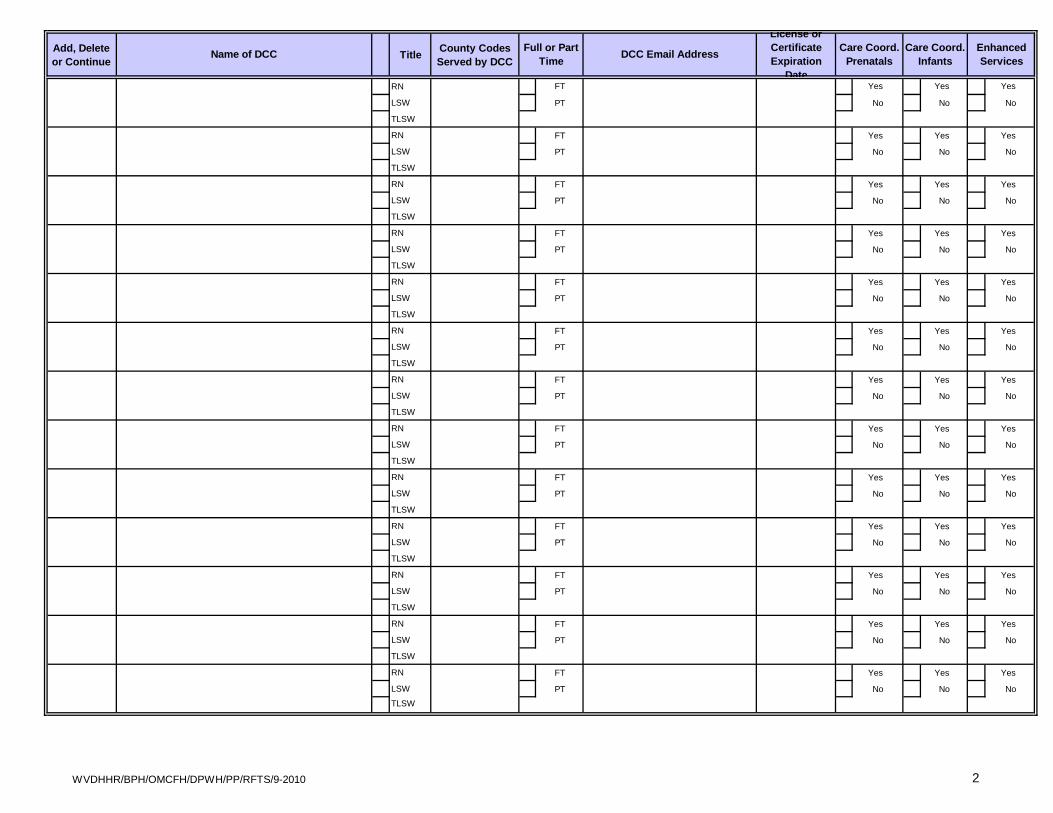
WVDHHR/BPH/OMCFH/DPWH/PP/RFTS/9-2010 2
Add, Delete or Continue Title County Codes
Served by DCC
RN FT Yes Yes Yes
LSW PT No No No
TLSW
RN FT Yes Yes Yes
LSW PT No No No
TLSW
RN FT Yes Yes Yes
LSW PT No No No
TLSW
RN FT Yes Yes Yes
LSW PT No No No
TLSW
RN FT Yes Yes Yes
LSW PT No No No
TLSW
RN FT Yes Yes Yes
LSW PT No No No
TLSW
RN FT Yes Yes Yes
LSW PT No No No
TLSW
RN FT Yes Yes Yes
LSW PT No No No
TLSW
RN FT Yes Yes Yes
LSW PT No No No
TLSW
RN FT Yes Yes Yes
LSW PT No No No
TLSW
RN FT Yes Yes Yes
LSW PT No No No
TLSW
RN FT Yes Yes Yes
LSW PT No No No
TLSW
RN FT Yes Yes Yes
LSW PT No No No
TLSW
DCC Email Address Care Coord. Prenatals
Care Coord. Infants
Enhanced ServicesName of DCC Full or Part
Time
License or Certificate Expiration
Date

WVDHHR/BPH/OMCFH/DPWH/PP/RFTS/8-2010
Health Education:
Health Education:
Date Date
You must notify the Regional Care Coordinator of changes in your caseload or Designated Care Coordinators.
Preventive Self Care
Childbirth Education
Nutrition:
ANNUAL CASELOAD PROJECTION(estimate total of all levels of care for contract year)
ENHANCED SERVICES ONLY
Parenting
Preventive Self Care
Childbirth Education
Nutrition:
(received in last contract year) (received in last contract year) (in last contract year) (in last contract year)
PRENATALS ANNUAL CASELOAD PROJECTION(estimate total of all levels of care for contract year)
PART BRIGHT FROM THE START
DCC AGENCY CASELOAD PROJECTIONNumber of Prental Referrals: Number of Infant Referrals: Number of Prenatals Served: Number of Infants Served:
Assessment/Service Care Plan:
Administrative Person Viewing Licensure (DCC Agency) Regional Care Coordinator
Care Coordination:
INFANTS ANNUAL CASELOAD PROJECTION(estimate total of all levels of care for contract year)
Parenting
Assessment/Service Care Plan:
Care Coordination:
Enhanced Services:

RIGHT FROM THE STARTINFANT ANTICIPATORY GUIDELINES
WVDHHR/BPH/OMCFH/DPWH/PP/RFTS 10/04/2011 Partners for a Healthy Baby Curriculum-FSU
Client Name: SS #: Service Date:
DCC
Purpose Sheet # Handout #(s) Initials
53, 77, 87 1, 2, 57, 75, 82
1, 7, 17, 31, 53, 65 9, 24, 35, 38, 39, 58, 61, 67
1, 53 1, 2, 39, 58, 59, 60, 75
23, 31 30, 31, 40
7, 17, 41, 65 10, 47, 48
7, 17, 23 11, 67
17, 41, 53, 65 25, 49
23 NONE
41 NONE
41 47
41 NONE
NONE NONE
1, 7, 17, 41, 53, 65, 77 4, 5, 12, 13, 14, 15, 26, 50, 62, 63
1, 7, 17, 41, 65 6, 15, 16, 26, 44, 63
53, 87 63, 76, 83, 84, 86
7, 17, 41, 65, 77, 87 17, 69
1, 7, 17, 31, 41 3, 19, 20, 21, 27, 41, 52, 58
7, 17, 23, 31, 41, 65, 87 18, 28, 32, 33, 70
1, 7, 23, 53, 65, 77, 877, 8, 18, 22, 34, 35, 36, 51, 56, 64, 70, 76, 85, 86, 90
7, 17, 31, 53 23, 43, 71
17, 23, 31, 41, 77, 87 29, 35, 37, 46, 51, 56, 77, 78 100, 121, 135, 136, 137, 156, 185, 186
31, 41, 53, 65, 77, 87 42, 44, 45, 46, 53, 54, 55, 65, 66, 71, 72, 73, 74, 79, 80, 81, 87, 88, 89
DCC Signature: Agency:
FAMILY DEVELOPMENT
Empowerment
Purpose Sheet #
30, 60, 92, 120, 144
Months 0-6 Months 7-12 Prenatal
Family Planning
Sex & STDs
Depression
Diet & Exercise
Health Care
Alcohol, Drugs & Tobacco
Relationships & Support
Planning & Problem Solving
Career Development & Finances
MOTHER'S NEEDS
Physical Changes & Discomforts
Emotional Changes
Health Care
Common Concerns
BABY'S DEVELOPMENT
Bonding & Attachment
Responding to Baby's Cues
Infant Development
CARING FOR BABY
Breastfeeding
Bottle Feeding
Nutrition
Sleeping
Daily Care Routines
31, 61, 93, 121, 145
3, 31, 61, 93, 121, 145
3, 31, 61, 93, 121, 145
93
NONE
3, 31, 61, 93, 121
61, 93, 121
3, 31, 121
Handout #(s)
1, 2, 3, 4, 31, 49, 81
57, 58
29, 30, 81
37, 55
3, 31, 61, 121, 145
3, 31, 61, 93, 145
2, 60, 144
30, 60
2
2, 30, 60, 92
30, 120
92
2, 30, 60, 92, 120, 144
2, 30, 60, 92
2, 30, 60, 92, 120, 144
NONE
60, 92, 144
NONE
NONE
10, 63, 62
152
NONE
116, 165
153
96, 117
97, 131, 132, 166, 167, 168, 169, 181
114, 129
95
113, 128
115, 164
NONE
106, 107, 125, 141, 142, 143, 159, 174
90, 91, 92, 108, 109, 110, 144, 145, 155, 160, 161, 162, 175
93, 111, 126, 146, 147
93, 94, 112, 127, 130, 148, 163, 176
NONE
130, 150, 151 ,177
NONE
NONE
NONE
NONE
Handout #(s)
98, 99, 118, 133, 154, 182, 183
119, 120, 134, 155, 170, 184
101, 102, 103, 104, 105, 122, 123, 124, 138, 139, 140, 157, 158, 171, 172, 173, 187, 188
10, 62, 63
62
NONE
NONE
NONE
NONE
NONE
10, 62, 63
NONE
49
NONE
40
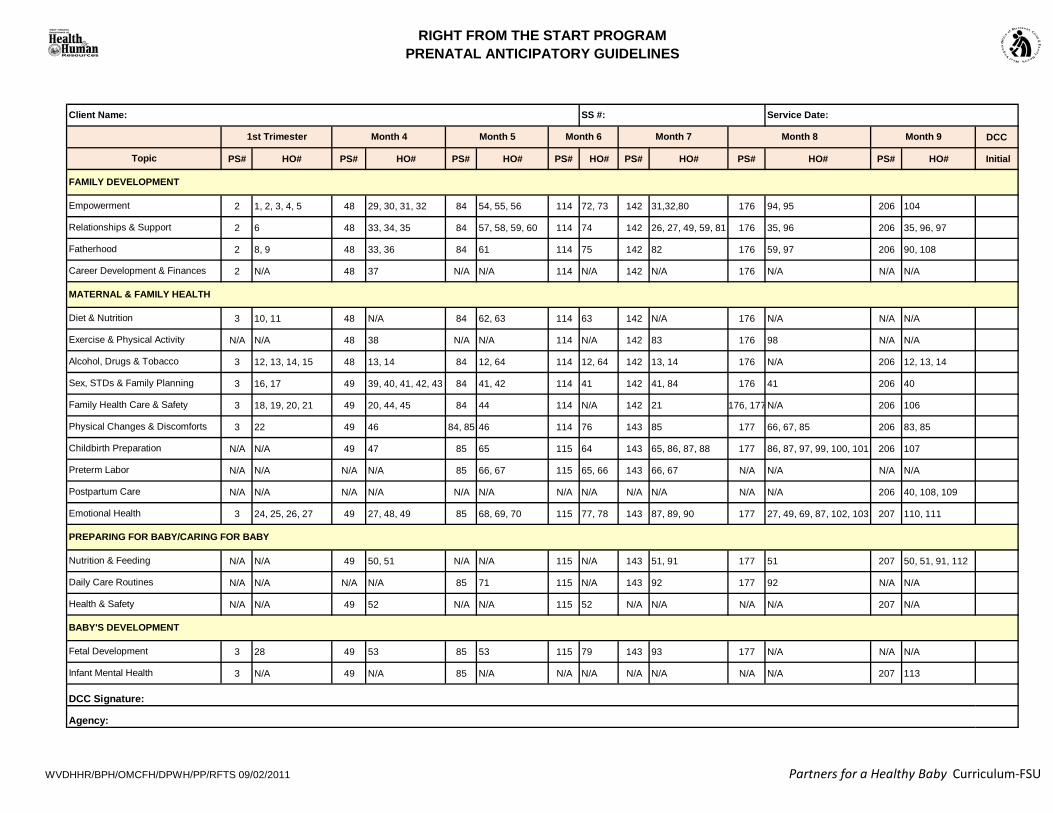
RIGHT FROM THE START PROGRAMPRENATAL ANTICIPATORY GUIDELINES
WVDHHR/BPH/OMCFH/DPWH/PP/RFTS 09/02/2011 Partners for a Healthy Baby Curriculum-FSU
DCC
PS# HO# PS# HO# PS# HO# PS# HO# PS# HO# PS# HO# PS# HO# Initial
2 1, 2, 3, 4, 5 48 29, 30, 31, 32 84 54, 55, 56 114 72, 73 142 31,32,80 176 94, 95 206 104
2 6 48 33, 34, 35 84 57, 58, 59, 60 114 74 142 26, 27, 49, 59, 81 176 35, 96 206 35, 96, 97
2 8, 9 48 33, 36 84 61 114 75 142 82 176 59, 97 206 90, 108
2 N/A 48 37 N/A N/A 114 N/A 142 N/A 176 N/A N/A N/A
3 10, 11 48 N/A 84 62, 63 114 63 142 N/A 176 N/A N/A N/A
N/A N/A 48 38 N/A N/A 114 N/A 142 83 176 98 N/A N/A
3 12, 13, 14, 15 48 13, 14 84 12, 64 114 12, 64 142 13, 14 176 N/A 206 12, 13, 14
3 16, 17 49 39, 40, 41, 42, 43 84 41, 42 114 41 142 41, 84 176 41 206 40
3 18, 19, 20, 21 49 20, 44, 45 84 44 114 N/A 142 21 176, 177 N/A 206 106
3 22 49 46 84, 85 46 114 76 143 85 177 66, 67, 85 206 83, 85
N/A N/A 49 47 85 65 115 64 143 65, 86, 87, 88 177 86, 87, 97, 99, 100, 101 206 107
N/A N/A N/A N/A 85 66, 67 115 65, 66 143 66, 67 N/A N/A N/A N/A
N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A 206 40, 108, 109
3 24, 25, 26, 27 49 27, 48, 49 85 68, 69, 70 115 77, 78 143 87, 89, 90 177 27, 49, 69, 87, 102, 103 207 110, 111
N/A N/A 49 50, 51 N/A N/A 115 N/A 143 51, 91 177 51 207 50, 51, 91, 112
N/A N/A N/A N/A 85 71 115 N/A 143 92 177 92 N/A N/A
N/A N/A 49 52 N/A N/A 115 52 N/A N/A N/A N/A 207 N/A
3 28 49 53 85 53 115 79 143 93 177 N/A N/A N/A
3 N/A 49 N/A 85 N/A N/A N/A N/A N/A N/A N/A 207 113
Fetal Development
Infant Mental Health
Nutrition & Feeding
Diet & Nutrition
Month 7
Empowerment
1st Trimester
Relationships & Support
Fatherhood
FAMILY DEVELOPMENT
Career Development & Finances
Topic
Client Name: SS #: Service Date:
Month 4 Month 5 Month 6 Month 8 Month 9
DCC Signature:
Agency:
MATERNAL & FAMILY HEALTH
PREPARING FOR BABY/CARING FOR BABY
BABY'S DEVELOPMENT
Daily Care Routines
Exercise & Physical Activity
Alcohol, Drugs & Tobacco
Sex, STDs & Family Planning
Family Health Care & Safety
Physical Changes & Discomforts
Childbirth Preparation
Preterm Labor
Postpartum Care
Emotional Health
Health & Safety

Prenatal Month 4 Prenatal Month 6 Prenatal Month 8FAMILY DEVELOPMENT FAMILY DEVELOPMENT FAMILY DEVELOPMENT
Empowerment Empowerment EmpowermentRelationships & Support Relationships & Support Relationships & SupportFatherhood Fatherhood FatherhoodCareer Development & Finances Career Development & Finances Career Development & Finances
MATERNAL & FAMILY HEALTH MATERNAL & FAMILY HEALTH MATERNAL & FAMILY HEALTHDiet & Nutrition Diet & Nutrition Diet & NutritionExercise & Physical Activity Exercise & Physical Activity Exercise & Physical ActivityAlcohol, Drugs & Tobacco Alcohol, Drugs & Tobacco Alcohol, Drugs & TobaccoSex, STDs & Family Planning Sex, STDs & Family Planning Sex, STDs & Family PlanningFamily Health Care & Safety Family Health Care & Safety Family Health Care & SafetyPhysical Changes & Discomforts Physical Changes & Discomforts Physical Changes & DiscomfortsChildbirth Preparation Childbirth Preparation Childbirth PreparationPreterm Labor Preterm Labor Preterm LaborPostpartum Care Postpartum Care Postpartum CareEmotional Health Emotional Health Emotional Health
PREPARING FOR BABY/CARING FOR BABY
PREPARING FOR BABY/CARING FOR BABY
PREPARING FOR BABY/CARING FOR BABY
Nutrition & Feeding Nutrition & Feeding Nutrition & FeedingDaily Care Routines Daily Care Routines Daily Care RoutinesHealth & Safety Health & Safety Health & Safety
BABY'S DEVELOPMENT BABY'S DEVELOPMENT BABY'S DEVELOPMENTFetal Development Fetal Development Fetal DevelopmentInfant Mental Health Infant Mental Health Infant Mental Health

No (0)Yes (12)
Mother's Last Name
Mother's First Name
Insurance WV Medicaid Self-Pay Other
Payment Method
Mother's Maiden Name
Infant's Last Name
Infant's First Name
WV Birth Score-DevelopmentalRisk Screen And Newborn
Hearing Screen
Street Address City
/ /Infant's Birth Date
Gestational Age
Mother's Race
WhiteBlackAsian
HispanicMixed RaceOther
<1501 (90)1501-2000 (77)2001-2500 (55)2501-3000 (10)>3000 (0)
Birth Weight (grams)
<17 (75)17-19 (60)>19 (0)
Maternal Age
Infant's Sex Male (40)Female (0)
Breast Only (0)Bottle or Both (36)
FeedingIntention
None (0)1-3 (3)4-6 (12)7-8 (18)9 or more (21)
PreviousPregnancies
10th grade or lower (12)
11th grade or above (0)MaternalEducation
Nicotine useduring pregnancy
Zip Code
ITEM ANSWER CODE SCORE
- -Parent Phone
- -
PRIMARY CARE PHYSICIAN/CLINIC
WVKYMD
OHPAVA
Other
City
Was infant transferred to NICU?NO YES
Cabell Huntington WVU Hospital Women & Childrens Other
NEWBORN HEARING
1. Type of Test:
2. Test Results:
3. Reason if not screened:
ABR OAELeft EarRight Ear
Pass Fail Not ScreenedPass Fail Not Screened
Infant Death Parent Refusal Equipment Failure Other
My baby's Birth Score, Developmental Risk Screen and Newborn Hearing Screenhave been explained to me. I understand my baby may be eligible for a specialservice such as case management or early intervention.
Parent/guardian signature Date
Witness' signature Date
For Office Use____RFTS Region _____ ______Outreach county _____________Birth to Three Site ___________OMCFH Hearing Referral_______
Packet Sent _______Yes ______ NoDate _______________ Initials _________
Distribution Copies: BirthScore Office, Chart,Parent/Guardian
Birth Score Total
DEVELOPMENTAL RISK Automatic High Score Answer each. Definition of abnormalities on back.
YES NO
Birth Weight 1500 gms or less
5 Minute APGAR 3 or less
YES NO Congenital Abnormalities
Which of the following substances / drugs have you used during pregnancy?
alcoholcocaineheroinother opioids
marijuanamethadonemethamphatamine
Mother's SS #
WVKYMD
OHPAVA
Other
Zip CodeOffice Phone
High Birth Score is above 99.
QUESTIONS FOR MOTHER:
SmokingOral tobaccoPatch
Delivery Hospital
Please indicate if you experienced prolongedperiods of stress during your pregnancy:
Not at allYes, moderate stressYes, very stressed
All in all, would you say your health is:ExcellentGoodFairPoor
Have you ever been diagnosed by aphysician with the following conditions?
No, I have never been diagnosed with diabetesType I diabetes (juvenile type)Type II diabetes (adult onset)
Gestational diabetes (pregnancy related)
Pre-DeliveryAdmission WeightHeight - self reported by mom
ft inches lbs
33892

E018672
Typewritten Text
SAMPLE
E018672
Typewritten Text
E018672
Typewritten Text

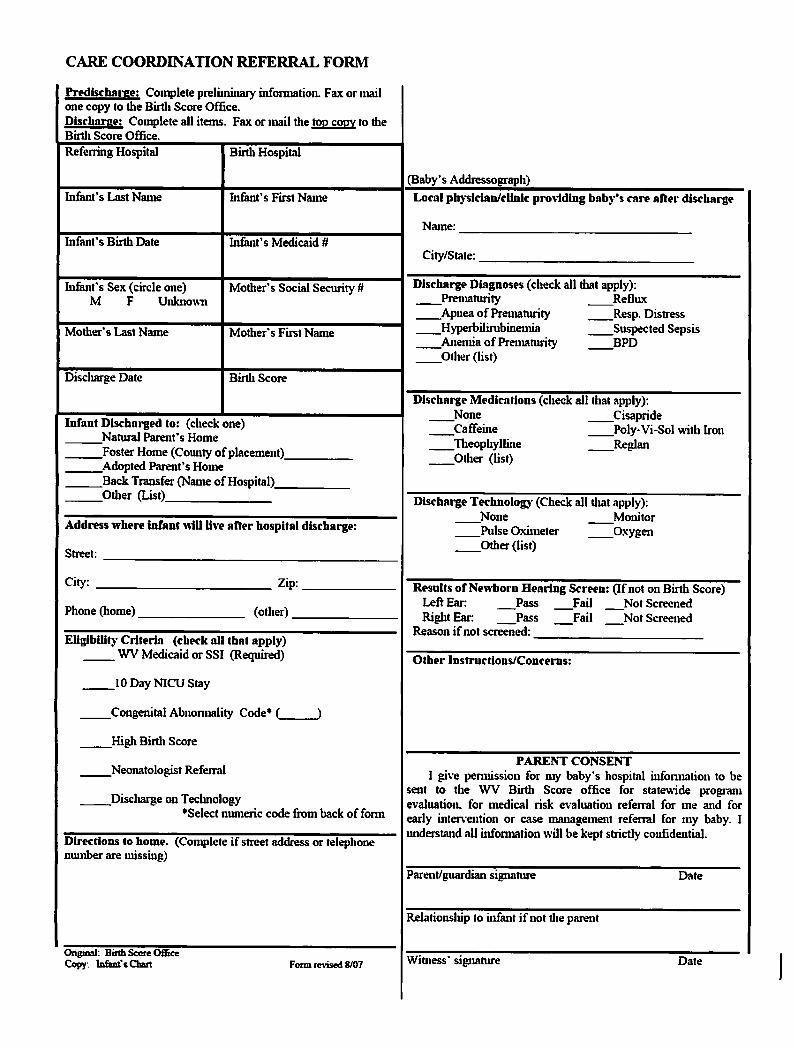


WVDHHR/BPH/OMCFH/DPWH/PP/RFTS/12-2011DCC Training Certificate
DCC received the following training:
Health EducationParenting EducationChildbirth EducationNutritional Evaluation/Counseling (RD Only)
cc: OMCFH/Perinatal Programs Director
TelephoneFace to Face
This certifies that (DCC Name and Title)
Address:
Right From The Start ProgramOffice of Maternal, Child and Family Health
350 Capitol Street, Room 427Charleston, West Virginia 25301-3714
304-558-5388 or 1-800-642-8522Fax: 304-558-7164
Designated Care Coordinator Training CertificationAgency Name: Region (1-8)
Registered Nurse Social Worker CBE RDDCC License Number: (Observed by RCC No
Service Care PlanAppropriate Documentation/Record Keeping
Newborn Hearing Screening
Client Eligibility (Medicaid & Maternity Services)
Depression Screening
Counties to be served by this DCC are:
Other:(Specify)
"I agree to return assigned equipment to Regional Lead Agency upon termniation."
(To be placed on file at RLA)
Spent
Information and Referral
Serial #:Date:
Learning Community ResourcesQuarterly DCC Training Attendance
Equipment Assigned: Teaching Dolls
NICU
Client Referral TypesPRSIAlternate EntryBirth Score
How to Conduct a Home VisitHow to Open a Case
Required Visits
Other
Access to RFTS Forms/Literature (Materials Management)
Billable/Nonbillable Services & Instructions
Interviewing Techniques
Reporting RequirementsSCRIPT (Tobacco Cessation & CO Monitor)
Quality AssuranceCase Closure
Enhanced Services
received initial Right From The Start Program training on(Date)
RFTS Forms
HIPAA RegulationsRFTS Program Overview DCC Job Description/ResponsibilitiesRFTS Policy and Procedure Manual
DVD Player and AccessoriesCO Monitor
Yes
RCC Signature: Training Completion Date:
Care Coordination
days of field training with a qualified DCC
InfantPrenatalTwo Day PHB Curriculum Training
DCC Signature: Training Completion Date:
Newborn Hearing ScreeningBirth ScoreTransportation Assistance
Standards of Care