Appendicitis Super Dooper Mega Final Case Study
69
I. INTRODUCTION Appendicitis is an inflammation of the vermiform appendix that develops most commonly in adolescents and young adults. It can occur at any age but is rare in clients younger than 2 years and reaches a peak incidence in clients between 20 and 30 years. It is not common in older adults; however, when it does occur in such clients, rupture of the appendix is most common(Medical – Surgical Nursing: Clinical Management for Positive Outcome 8 th by Joyce Black and Jane Hokanson Hawks, page 683). It is classified as a medical emergency and many cases require removal of the inflamed appendix, either by laparoscopy or laparotomy. If left untreated, mortality is high, mainly because of peritonitis (inflammation of the peritoneum) and shock. (http://www.wikipedia.org/wiki/Appendicitis? wasRedirected=true) There is no specific test for appendicitis, but blood tests such as a white blood cell count and x – rays may help a physician make a diagnosis. Abdominal ultrasound has proven to be useful in differentiating causes of abdominal pain. (http://www.healthscout.com/ency/68/658/main.html) The most specific physical finding is rebound tenderness, pain on percussion, Rovsing’s sign (Right Lower Quadrant pain with palpation of the Left Lower Quadrant), Psoas sign (Right Lower Quadrant pain is felt with hyperextension of the right hip) are present in the patients with acute appendicitis. (http://www.ufs.ph/tinig/mayjun02/05060225.html) 1
Transcript of Appendicitis Super Dooper Mega Final Case Study

I. INTRODUCTION
Appendicitis is an inflammation of the vermiform appendix that develops most
commonly in adolescents and young adults. It can occur at any age but is rare in clients younger
than 2 years and reaches a peak incidence in clients between 20 and 30 years. It is not common
in older adults; however, when it does occur in such clients, rupture of the appendix is most
common(Medical – Surgical Nursing: Clinical Management for Positive Outcome 8 th by Joyce
Black and Jane Hokanson Hawks, page 683). It is classified as a medical emergency and many
cases require removal of the inflamed appendix, either by laparoscopy or laparotomy. If left
untreated, mortality is high, mainly because of peritonitis (inflammation of the peritoneum) and
shock. (http://www.wikipedia.org/wiki/Appendicitis?wasRedirected=true)
There is no specific test for appendicitis, but blood tests such as a white blood cell count
and x – rays may help a physician make a diagnosis. Abdominal ultrasound has proven to be
useful in differentiating causes of abdominal pain.
(http://www.healthscout.com/ency/68/658/main.html) The most specific physical finding is
rebound tenderness, pain on percussion, Rovsing’s sign (Right Lower Quadrant pain with
palpation of the Left Lower Quadrant), Psoas sign (Right Lower Quadrant pain is felt with
hyperextension of the right hip) are present in the patients with acute appendicitis.
(http://www.ufs.ph/tinig/mayjun02/05060225.html)
Anecdotal reports describe the success of intravenous antibiotics in treating acute
appendicitis in patients without access to surgical interventions
(http://www.ufs.ph/tinig/mayjun02/05060225.html). But in most cases, a surgical removal of the
appendix is more advisable to relieve the recurrence of pain and to prevent bursting of the
appendix. The surgery that corrects the appendicitis, called an appendectomy, is a procedure with
relatively little risk. Many surgeons are performing laparoscopic appendectomy in which the
appendix is removed through three small incisions less than an inch long using special
instrument and a special camera. With laparoscopic appendectomy, most patients can go home
within 24 hours of the operation. (http://www.healthscout.com/ency/68/658/main.html) Appendix
can also be removed through laparotomy. The surgeon makes a small incision at the Mcburney’s
point (Mcburney’s incision) to remove the appendix. Appendectomy is done under a general or
1

regional anesthesia, which means the patient will not feel any pain during the procedure.
(http://www.nlm.nih.gov/medlineplus/ency/arcticle/002921.html)
The incidence rate of appendicitis in the United States is approximately 680, 000 per year
or 56, 000 per month (http://www.diagnosis.com/a/acute_appendicitis/prevalence.html). In the
Philippines, there are approximately 215, 604 cases recorded annually (in the estimated
population of 88, 241, 697).
(http://wiki.answers.com/Q/What_is_the_appendicitis_rate_in_the_Philippines)
To gather more information about appendicitis and appendectomy, the group chose this case
for presentation; and to help future patients in improving their lives, and also this case study may
be used as reference for future researchers.
2

OBJECTIVES
Student – Nurse Centered
General Objectives
To gather additional knowledge from the patient’s condition and give proper nursing care
on her post – operative state to prevent complications through the use of the nursing process.
Specific Objectives
At the end of the study the student nurse will:
Understand and be knowledgeable about the patient’s condition.
Assess the needs for care of the patient.
Plan appropriate interventions related to the patient’s needs.
Implement the planned nursing interventions.
Evaluate whether the goals are met or not.
Reassess if the care of plan was effective.
Patient – Centered
General Objectives
The patient will be knowledgeable about the proper care needed on her post – operative
state, to attain maximum level of care, and to prevent complications.
Specific Objectives
At the end of the study, the patient will:
Be knowledgeable about her condition.
Understand the extent of restrictions of food and activities.
3

Achieve the needed nursing care appropriate for her age and condition.
Decrease the anxiety she is experiencing after the surgery and possible complications.
Respond to the prescribed treatments or managements.
Become better and will live normally like with other people.
4

I. NURSING PROCESS
A. ASSESSMENT
1. Personal Data
a. Demographic Data
Name : Adding J
Age : 12 years old
Sex : Male
Birthday :
Address : baldios, Sta. Ignacia Tarlac
Religion : Roman Catholic
Nationality : Filipino
Civil Status : Single
Occupation : N/A
Height :
Weight :
Chief Complaint : Abdominal pain – Right Lower Quadrant
Date of Admission : January 4, 2011
Admitting Diagnosis : t/c Appendicitis
Final Diagnosis : Acute Appendicitis
5

b. Environmental Status
Ading J resides at Baldios,Sta. Ignacia, Tarlac. Their house was a bungalow type which is
made up of bamboo where there are mango trees around it. There are two rooms in their house
which they use for sleeping. They are five living in their house. There is available sari – sari
stores available in their place. The available means of transportation in their area are thru
jeepney, tricycle and mini bus. They also have a forced pump located at their backyard which
they also use for their drinking water. They have 2 cats and a dog which they allow to stay inside
their house. They said that they have a good relationship with their neighborhood.
c. Lifestyle
Ading J is a grade six student. He usually sleeps at 8 or 9 in the evening and wakes up at
around 6 in the morning to prepare his self to school. Every day, he plays basketball as his
exercise and past time. According to his sister, their mother usually cooks meat or pork dishes,
and sometimes vegetables. He usually drinks 8 - 10 glasses of water a day. Right after he eats, he
goes back to his friends to play basketball. He takes a bath every day, usually every morning
before he goes to school. His sister also stated that adding J started eating junk foods and soft
drinks every afternoon.
6

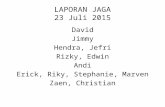
2. FAMILY HISTORY OF HEALTH AND ILLNESS
7
87
81
74
5477
48
69
63
78
CA
ASTHMA
76
71 60 6967
64
LEGEND
BOY
GIRL
X DECEASED
PATIENT
APPENDICITIS
CA Cancer
V/A Vehicular Accident
43
49
47
MATERNALPATERNAL
41
v/a

3. History of Past Illness
According to Ading J this is his second time of hospitalization. He was 5 years old when
he was first hospitalized, that was when some of his body part (specifically his armpit) burned
because of the explosion of the gasoline when his parents was cooking. He already had Chicken
Pox and measles. Ading J did not know if he was fully immunized, he does not have any
allergies to any foods, medication and pets. Cough and Colds, Diarrhea and fever are the usual
condition that he acquired and his mother buys over the counter drugs like paracetamol, neozep
and loperamide.
4. History of Present Illness
Two weeks prior to admission, the patient felt an abdominal pain at the right lower
quadrant. Though Ading J experienced pain, he can still tolerate it and continued to play
basketball.
One week prior to admission, abdominal pain was still present and his mother decided to
seek consultation to Gilberto O. Teodoro Memorial Hospital Emergency Room. He was
diagnosed with Appendicitis and his physician prescribed cefalexin as the first course of
treatment.
After one week, she went to another clinic which is the Iglesia Clinic in Camiling, Tarlac.
The findings were also Appendicitis, and the physician prescribed diclofenac. She was referred
to Tarlac Provincial Hospital for further laboratory examination. Urinalysis was ordered, after
reading the result the physician decided to admit her for more evaluation. After certain
laboratory tests, the physician subjected the patient for appendectomy.
5. 13 AREAS OF ASSESSMENT
I. SOCIAL STATUS
8

Ading J is the third of the six siblings. The family resides at Baldios, Sta Ignacia Tarlac.
Ading J belongs to a nuclear family. He is a Roman Catholic and a grade six student. His mother
is a house wife and his father works in Tuguegarao as an auto technician earning P1,200 a week,
which they spend for their foods and groceries, electric bill, cellular phone load, and daily school
allowance of their children. Ading J’s medical expenses are supported by his family, relatives
and health insurance (philhealth). He usually goes to talk with their neighbors and play
basketball with his playmates. He has a good relationship with their neighbors.
NORMS
Social status included family relationship that serves as his support system especially at
times of need and stress related conditions. It meets a fundamental human need for social ties
making life less anxious. Also social support system buffers the negative effect of stress as
means of achievement of a good health. (Friedman and Smith 1988)
ANALYSIS
Ading J has a normal social status because he is able to mingle with the other people and
do the usual things a typical child does. They are also able to provide their basic needs.
II. MENTAL STATUS
Adding J is conscious and coherent. Oriented to time and date, he is able to read and
write and follow instructions, able to maintain eye to eye contact. He is open to any questions,
approachable and is able to converse but slowly with the student nurses. During the assessment,
Ading J talks about his past memories showing that his long term memories are still active.
9

NORMSTo consider a person’s mental status is normal, he should be oriented. He should be able
to evaluate and act appropriately in situations regarding judgment. (Health Assessment and
Physical Examination 3rd Edition by Mary Ellen Zator Ester)
ANALYSIS
Ading J’s mental status is normal, it is usual that a patient in pain has a hard time when
talking.
III. EMOTIONAL STATUS
Prior to hospitalization according to his sister, he is very cheerful; he loves to make
conversations with his playmates, and siblings. His sister also stated that they have financial
problems but since their family and relatives are very supportive not just financially but also
emotionally along with the health insurance they are able to lessen their burden regarding their
expenses in the hospital. This shows that they have a good relationship status with her family.
Ading J’s after the procedure was still asleep due to the anesthesia. When Ading J’s was awake,
he stated that she can feel the pain on the incision site, which is a normal response several hours
after the operation.
NORMS
Integrity manifests with wisdom and feelings of satisfaction with one’s life while despair
arises from remorse about what could have been. The presence of despair causes life to be
viewed as meaningless. (Source: Nursing CEU.com: The process of human development)
Carrying out emotional feelings through words and facial expressions are normal signs that client
was aware of his physical conditions. (Nursing Fundamentals, Rick Daniels) Expression of self
control and self perception is just normal (Fundamentals of Nursing, Kozier, Erb, Berman, and
Synder).
10

ANALYSIS
Ading J’s emotional status is considered normal, due to his condition it is normal to feel
pain and become unresponsive in some instances.
IV. SENSORY PERCEPTION
VISION
In assessing the vision, Ading J is instructed to look straight to observe the general
appearance of her eyes. His eyes are almond in shape, irises are black in color and scleras are
whitish in color, eyebrows and eye lashes are equally distributed. His conjunctiva is pale and
moist. Ading J was also instructed to follow the direction of a finger with his eyes following six
cardinal positions. And his eyes were able to move in full ranges of motion and in all directions.
With the use of penlight pupils are assessed, pupils are equally round and reactive to light
accommodation. Ading J does not use eyeglasses or contact lenses.
Visual acuity was assessed by asking Ading J to read the word written on a piece of paper
with a font size of approximately 12 at about 3 feet away from his using the right eye first then
the left eye and then both eyes. Mrs. F read all the samples correctly during the test.
NORMS
For the test of the Cardinal Fields of Gaze, the extra ocular muscle movements are being
assessed. Normally, both eyes of the patient should move smoothly and symmetrically in each of
the six fields. Light and accommodation reading is possible in the distance of 14 inches for the
assessment of near vision. (Health Assessment and Physical Examination 3rd edition by Estes)
Analysis
The patient’s visual capacity or status is normal, extra ocular muscle movements and
papillary response and visual acuity are normal.
11

SMELL
Ading J’s nose has no deviations in terms of shape and size. Nose is pointed and no
discharges were seen during the assessment. According to the patient he doesn’t have any history
of sinus infection or epistaxis (nose bleeding). Before the next procedure, permission was asked
to Ading J to do another test. Using a perfume and an orange peel without the patient’s
knowledge we ask him to identify the 2 samples by smelling. After smelling he correctly
identifies the perfume and orange peel. Test shows that there are no abnormalities or obstructions
were identified in his sense of smell.
Norms
Nose must be symmetrical and along of the face. Each nostril must be patent and
recognize the smell of an object. (Health assessment and physical examination, Mary Ellen
Zator Estes)
Analysis
Client was able to recognize the odor. He has normal sense of smell but he has difficulty
of breathing that leads to the need of oxygen therapy.
HEARING
General appearance of Ading J’s ears was parallel, symmetrically proportional to the size
of the head, bean shape, has a firm cartilage and with the presence of cerumen. In assessing the
hearing acuity of the patient, Ading J is instructed to repeat the words that will be whisper at a
distance of 2 feet away on the left ear first, and then the right after the test he was able to repeat
the whispered words. Another test by the use of the beeping sound of the digital thermometer at
the distance of 4 feet away and still he was able to hear the sound. He verbalized that he has no
known auditory deficits nor ear infection history and unusual sensations like ringing or buzzing.
12

Norms
For the auditory acuity, the patient should be able to repeat the whispered words from a
distance of two feet. (Health assessment and physical examination, Mary Ellen Zator Estes)
Analysis
Based on the given data, patient’s auditory acuity is normal.
TASTE
Ading J’s lips are dry and symmetrical in shape, tongue is pale in color, no presence of
tooth decay, but there is a presence of tooth cavities, no false dentures and no teeth loss, no sign
of gingivitis, buccal area are pale. The patient was asked to open his mouth widely to assess the
entire mouth. To assess his sense of taste, patient was asked to do some taste test. He was ask to
taste a cotton ball soak with orange juice and cotton ball soaked in water with salt without
knowing what the two samples are. After patting the cotton balls on the lips of the patient, Ading
J identified the 2 samples correctly.
Norms
Taste is intact in the posterior one third of the tongue. (Health Assessment and Physical
Examination, Mary Ellen Zator Estes)
Analysis
Client’s sense of taste is normal.
TOUCH
In assessing’s sense Ading J’s of touch, he was asked to close his eyes a cotton ball was
stroke to the back of his neck. Then using another cotton ball we poured alcohol on it and rub it
on the same area. He stated that he felt a sensation of wet and cold on his skin.
13

Norms
The skin contains receptors for pain, touch, pressure and temperature. Sensory signals are
transmitted along rapid sensory pathways, and less distinct signals such as pressure of localized
touch are sent via slower sensory pathways. (Health Assessment and Physical Examination,
Mary Ellen Zator Estes)
Analysis
Ading J’s sensory transmission functions well as manifested by the data presented, it is
considered normal.
V. MOTOR STABILITY
Several hours after the surgery, the patient was asked to perform ROM exercise on the
upper and lower extremities. He was asked to raise both of his arms. He performed it with ease
and freely moved without any difficulty. He can bend and straightened his elbows and extend
and spread his fingers. He performed it with ease. According to the patient he felt pain in the
right lower quadrant of his abdomen when raising his right leg and cannot move it freely. There
is no presence of deformity. There are also proper symmetry between left and right on each
extremity. Early ambulation was encouraged. Patient can bend his legs with limited range of
motion and needs assistance when standing and going to the comfort room.
NORMS
Fine motor skills involve the small muscle of the body that enables such functions as
writing, grasping objects and fastening of clothes. Fine motor skill involves strength, fine motor
controls and dexterity. Gross motor skills involve the large muscles of the body that enable such
functions as walking, kicking, sitting upright, lifting and throwing a ball. A person’s gross motor
skills depend on both muscle tone and strength.
Low muscle tone is characteristics disabling conditions such as Down syndrome, genetics
or muscle disorders, or central nervous system disorders.
ANALYSIS
14

Ading J’s motor ability is not in good condition due to the presence of pain in the right
lower quadrant of the abdomen when raising the right legs.
VI. BODY TEMPERATURE
The table below shows the temperature of Mrs. F during the shift
DATE TIME TEMPERATURE ANALYSISJanuary 4, 2011
January 5, 2011
January 6, 2011
8:00 am
9:00 am2:00 pm
3:00 pm
8:00 pm
36.7C
36.9C36.8C
38.5C
37C
Normal
NormalNormal
Above normal
Normal
INTERPRETATION
Ading J’s temperature at January 4 was normal, on January 5, he was febrile. On January
6, his temperature returned to normal.
NORMS
Normal temperature for axilla is within 35.4-37.4c (Fundamentals of Nursing by Kozier
and Erbs 7th edition)
ANALYSIS
According to the data gathered on September 30, 2010 at 6:00 pm Ading J’s body
temperature is on normal range. The patient had altered body temperature on October 1, 2010 at
3:00 pm up to 6:00 pm, and became normal at 10:00 pm.
VII. Respiratory Rate
15

DATE T IMERESPIRATORY RATE
ANALYSIS
January 4, 2010
8:00 am
9:00 am
2:00 pm
20cpm
18cpm
19cpm
Normal
January 5, 2010 9:30 pm 20 cpm Normal
January 6, 2010 8:00 am 19 cmp Normal
Norms
Respiration in the resting adult, the normal respiratory rate is 12 to 20 breaths per minute.
This type of breathing is termed eupnea, or normal breathing.
(Health Assessment and Physical Examination, 3rd edition by Estes, page 455)
(Analysis is presented on the table above)
VIII. Circulatory Rate
DATE TIME B.P ANALYSISSeptember 30, 2010
October 01, 2010
September 30, 2010
October 01, 2010
3:35 pm
9:30 pm
3:35 pm
9:30 pm
90/70
100/80P.R
64
70
Normal
Normal
Normal
Normal
Norms
Pulse
Normal pulse rate vary with age. The table below shows the normal range of pulse rate
according to age:
16

AGE RESTING PULSE RATE AVERAGE
10 years 70 – 110 bpm 90
14 years 60 – 110 bpm 85 – 90
Adult 60 – 100 bpm 72
Source: Health Assessment and Physical Examination, 3rd edition by Estes, page 253
Normal blood pressure varies with age. As a person ages, blood pressure generally
increases. The table below shows the general ranges of normal blood pressure at different ages
and gender:
BLOOD PRESSURE: Normal Range According to Age and Gender
Female
AGE SYSTOLIC (mm Hg) DIASTOLIC (mm Hg)5
1015
≥18
103 – 109
112 – 118120 – 127
<120
66 – 70
73 – 7678 – 81
<80
Male
AGE SYSTOLIC (mm Hg) DIASTOLIC (mm Hg)5
1015
≥18
104 – 102
111 – 119122 – 131
<120
65 – 70
73 – 7876 – 81
<80
17

Source: Health Assessment and Physical Examination, 3rd edition by Estes, page 260
IX. Nutritional Status
Before he was confined to the hospital, adding J eats 3 to 4 times per day and drinks 8 to
10 glasses of fluids. He also eats fruits like banana and mango. When the patient was admitted in
the hospital, he was on a nothing by mouth state. His BMI is in normal range.
BMI COMPUTATION:
Weight: 48kg
Height: 5”1’
BMI = WEIGHT IN KILOGRAMS
HEIGHT IN METER SQUARED
= 48kg
2.4006 m
BMI =19.99 - NORMAL
Norms
According to the Health Asian Diet Pyramid, there should be a daily intake of rice,
grains, bread, fruit and vegetables; optional daily for fish, shellfish, and dairy products; weekly
for sweets, eggs and poultry, and monthly for meat.
There should be an increase intake of a wide variety of fruits and vegetables. Include in
the diet foods higher in vitamins C and E, and omega-3 fatty acid rich foods. (www.webmd.com)
Analysis
Mrs. F nutritional status was affected because of the surgical procedure done to her
(appendectomy). Her BMI is in the normal range.
18

X. Elimination Status
Mrs. F usually defecates once every day with hard stools bur not painful and urinates 4 to 5
times per day with an approximately 30 to 40 cc of urine per urination. When she was admitted
she voids 4 times and defecates once.
Norms
The frequency of defecation is highly individual, varying from several times per day to
two or three times per week. The amount defecated also varies from person to person.
(Fundamentals of Nursing 7th edition by Kozier, et. Al., page 1126)
Average Daily Urine Output by Age
AGE AMOUNT(mL)5 to 8 years
8 to 14 years14 years through adulthood
Older adulthood
700 – 1000
800 – 14001500
1500 or less
Source: Fundamentals of Nursing 7th edition by Kozier, ET. Al., page 1261
ANALYSIS
Mrs. F elimination status is affected. Because she was on nothing by mouth state after the
operation, she has nothing to defecate.
XI. Reproductive Status
Ading J had his circumcision at the age of 10. He does not had any sexual experience.
Norms:
(Maternal and Child health Nursing 4th Edition by Pilliteri)
19

ANALYSIS
Based on the statement above Ading J has a normal reproductive status. He doesn’t have
sexually transmitted disease.
XII. Sleep – Rest Pattern
He usually sleeps at 8 to 9 in the evening and wakes up at 6 in the morning. He watches
television during his rest hours or play basketball with friends. He also spends time to be with his
family and playmates. But when he was confined his sleep pattern was always interrupted.
Norms
CATEGORY
NORMAL HOURS OF
SLEEP PER DAYNewborns
InfantsToddlers
PreschoolersSchool – age children
Young adultsMiddle – aged adults
Elders
16 to 18
12 to 1410 to 1211 to 128 to 127 to 86 to 8
About 6 hours
Source: Fundamentals of Nursing 7th edition by Kozier, ET. Al., page 1116
ANALYSISBecause of his condition, Ading J's sleep pattern was affected.
XIII. State of Skin and Appendages
20

Ading J’s skin is brown in color. His skin in the foot is dry, some calluses are observed. He
complains of some itchiness on his lower extremities. His conjunctiva is pale. He has some scar
on his lower extremities. His nails are pale, short and clean. His nail beds are slightly pale. His
capillary refill time is 2 seconds.
NORMS
The palpebral conjunctiva should appear pink and moist. Normally the skin is a uniform
whitish pink or brown color depending on the patient's race. Normally, the nails have pink cast
light skinned individuals and are brown in dark-skinned individuals. (Health assessment and
Physical Examination, 3rd edition by Mary Ellen Zator Estes).
AnalysisAding J’s skin appendages are affected due to decreased oxygen supply. The patient’s dry
skin was due to restriction in fluid and any food. The Patient’s capillary refill is normal.
6. Laboratory and Diagnostic Procedures
DATE ORDERED: September 29, 2010
Urinalysis
INDICATION RESULT NORMAL RANGE ANALYSIS
21

>to detect renal and metabolic diseases.
>diagnosis of diseases or disorders of the kidney or urinary tract.
Color: Yellow
Transparency: TurbidLeukocytes/Nitrates: NegativeUrobilirogen: NormalProtein: TracepH: 6.0Blood cells: negativeSpecific gravity: 1.010Ketone: NegativeBilirubin: NegativeGlucose: NegativeMucus threads: ModeratePus cells: 3 - 4
RBC: 0 - 1Epitheleal Cells: ModerateBacteria: Rare
Urates/Phosphates: Moderate
Straw yellow – amber
Transparent – turbidAbsent0.2 – 1. 0 mg/dlAbsent - Trace5.0 – 8.5Absent1.010 – 1.015AbsentAbsentAbsentNegative or fewFew
0 – 3/ HPFFewNegative or Few
Few
Normal
NormalNormalNormalNormalNormalNormalNormalNormalNormalNormalNormalHigh. An indicator that there is an infection present in the urinary tract.NormalNormalNormal
Normal
NURSING RESPONSIBILITIES
Prior to procedure:
Explain the procedure to the patient and family/relatives.
Provide for patient’s privacy.
Instruct the patient to go to the laboratory with the request form.
Instruct the patient to dispose the first urine and catch the midstream urine.
Educate the patient not to contaminate the inside part of the container.
Instruct the patient to send the specimen to the laboratory immediately
During the procedure:
Maintain the sterility of the specimen container by not touching the inside part.
22

Maintain the freshness and sterility of the urine specimen.
After the procedure:
Interpret the result
Refer to the physician if abnormalities are noted.
DATE ORDERED: September 29, 2010
Complete Blood Count
INDICATION RESULT NORMAL RANGE ANALYSIS
>to detect/diagnose blood disorders.
>to detect presence of infection.
BLOOD TYPE: A+
WBC: 13.9 G/L
LYM: 1.8 R2 12.9%L*MID: 0.8 5.5%MGRAN:7.0 81.6%GRBC: 4.17 T/LHGB: 113 g/LHCT: .373 L/L
4.1 – 10.9 G/L
0.6 – 4.1 10.0– 58.5%L0.0 – 1.8 0.1 – 24 %M2.0 – 7.8 37.0–92.0 %G4.20 – 6.30 T/L120 – 180 g/L.370 - .510 L/L
WBC is high because of the presence of infection. WBC defends our body against infection.
NormalNormalNormalNormal
23

>to screen for fluid and electrolyte problem.
MCV: 82.6 fLMCH: 27.1 pgMCHC: 328 g/L
PLT: 379 G/L
80.0 – 97.0 fL26.0 – 32.0 pg310 – 360 g/L11.5 – 14.5 %
140 – 440 G/L
NormalNormalNormalNormalNormalNormal
Normal
NURSING RESPONSIBILITIES
Prior to procedure:
Explain the procedure to the patient and family/relatives. Educate the patient about what to expect during the procedure.
During the procedure:
Advise the patient to relax during the procedure.
After the procedure:
Interpret the result Refer to the physician if abnormalities are noted.
24

7. Anatomy and Physiology
The Appendix
The appendix averages 10 cm in length, but can range from 2 to 20 cm. The diameter of
the appendix is usually between 7 and 8 mm. The appendix is located in the lower quadrant of
the abdomen, or, more specifically, the right iliac fossa. Its position within the abdomen
corresponds to a point on the surface known as McBurney's point (see below). While the base of
the appendix is at a fairly constant location, 2 cm below the ileocecal valve, the location of the
tip of the appendix can vary from being retrocecal (74%) to being in the pelvis to being
25

extraperitoneal. In rare individuals with situs inversus, the appendix may be located in the lower
left side.
New studies propose that the appendix may harbor and protect bacteria that are beneficial
in the function of the human colon. Some researchers argue that the appendix has a function in
fetuses and adults.[7] Endocrine cells have been found in the appendix of 11-week-old fetuses that
contribute to "biological control (homeostatic) mechanisms." In adults, Martin argues that the
appendix acts as a lymphatic organ. The appendix is experimentally verified as being rich in
infection-fighting lymphoid cells, suggesting that it might play a role in the immune system.
Although it was long accepted that the immune tissue, called gut associated lymphoid tissue,
surrounding the appendix and elsewhere in the gut carries out a number of important functions,
explanations were lacking for the distinctive shape of the appendix and its apparent lack of
importance as judged by an absence of side-effects following appendectomy.
8. PATHOPHYSIOLOGY
Book based
26
Non modifiable risk factors:
>age
>gender
Modifiable risk factors:
>constipation
>activity
>low fiber dietSeverity of symptoms is related to
the degree of inflammation
present.
The inflammatory process ranges
from mild to severe appendiceal
swelling and obstruction.
Concurrent infection can cause mucosal
ulceration and subsequent development of
abscess, necrosis or rupture.
Abdominal pain is present, usually
described as being in the right lower
quadrant, localized at Mcburney’s point.
Appendectomy is often
suggested by the
physician.
Other common
symptoms include
anorexia, nausea and
vomiting, low grade
fever, elevated WBC

Patient – based
27
Modifiable Factors
Constipation Low Fiber – Diet
Nausea and loss of appetite
Acute abdominal pain at the Mcburney’s point.
Start of the inflammatory process
Increased intra luminal pressure in the appendix
Occlusion of appendix by fecalith
Non Modifiable Factors
AgeGender
Appendectomy Inflammation of appendix (appendicitis)
Low grade fever

B. PLANNING
NURSING CARE PLAN
Acute Pain
Assessment Planning Intervention Expected outcome
Subjective: “Masakit ang sugat ko” P/S is 6/10.Objectives:
facial grimace increase ability to perspire
irritable at times
guarding behavior
limited movements and range of motion.
assisted with the significant others when turning in other position.
Within 30 minutes to 1 hour of giving proper nursing interventions, the patient will verbalize reduction of pain.
Monitor the pain scale. (to know if there is an improvement)
Position on a semi-fowlers position.(for the patient to feel comfortable)
Provide a clean bed. (to have a good relaxation.)
Encourage to have a bed rest.( to gain energy)
Encourage to continue limiting body movements. (to prevent pain)
Educate the importance of deep breathing exercises. (for the patient to feel calm and relax)
Within 30 minutes to 1 hour of giving proper nursing interventions, the patient will:
-verbalize a decrease of pain.-can move freely without assistance.-free from irritability.
-facial grimace will be absent.
28

Nursing Diagnosis:Acute pain related to surgical incision on the abdomen.Scientific Explanation:
Unpleasant sensory and emotional experience arising fromactual or potential tissue damage or described in terms of such damage (International Association for the Study of Pain); sudden or slow onset of any intensity frommild to severe with an anticipated or predictable end and a duration of less than 6 months. (Nurse’s Pocket Guide Edition 11 by F.A Davis, page 498)
Divert attention by instructing to read books.(to lessen and divert pain)
Instruct to increase fluid intake.(to prevent dehydration)
Instruct to guard the site when coughing. (to prevent from opening of the site)
Instruct to take medications that are prescribed by the physician. (for the patient safety to drugs)
Educate the patient to clean the site regularly. (to prevent any complications and infection)
Hyperthermia
Assessment Planning InterventionsExpected Outcomes
29

Subjective:Ø
Objective:
warm to touch diaphoretic
weak in appearance
irritable at times
vital signs taken as follows:
BP-90/70 mmHgRR-20 cpmPR-64 bpmTemp- 38.5°c
Diagnosis:Altered body temperature related to inflammatory process.
Scientific Explanation:Hyperthermia is an elevated body temperature due to failed thermoregulation. Hyperthermia occurs when the body produces or absorbs more heat than it can dissipate. It may also occur as assign of infection.
Within 1 hour of proper nursing interventions, the patient’s temperature will subside to 37.5 °c from 38.5 °c.
Monitor vital signs especially temperature. (To know if it has an improvement of the patient’s temperature.)
Perform Tepid Sponge bath. (To lower body temperature.)
Provide clean and comfortable bed. (for the patient to have a good rest and feel comfortable)
Provide clean and comfortable clothing. (for the patient not to feel irritable)
Instruct to increase fluid intake after NPO. (to prevent dehydration)
Instruct to eat nutritious foods like green leafy vegetables after NPO. (to gain more energy)
Instruct to take medications that are prescribed by the physician. (For safety purposes.)
Within 1 hour of proper nursing interventions, the patient’s temperature will subside to 37.5 °c from 38.5 °c.
30

Risk for Infection
ASSESMENT PLANNING INTERVENTION AND RATIONALE
EXPECTED OUTCOME
S O
O
Irritable Poor hygiene Long fingernails Dirty surroundings Incision on the right
lower quadrant of the abdomen
DiagnosisRisk for infection related to surgical incision on the right lower quadrant of the abdomen
SCIENTIFIC EXPLANATION
There’s a risk for infection for a client who undergone a surgical incision because there is a break in the tissue or that would serve as an opening that can be
Within 2 hours of proper nursing intervention the client risk for infection will decrease to achieve timely wound healing
Instruct in good hand washing(Reduces risk of spread of bacteria)
Instruct good body hygiene(Reduces risk of spread of bacteria and promote relaxation)
Demonstrate aseptic wound care(Reduces risk of spread of bacteria)
Inspect incision and dressings(Provides for early detection of developing infections process)
Encourage to cut the fingernails(Reduce risk of spread of bacteria)
Encourage to keep the surroundings of the patient clean(To minimize the chance of getting infection through microorganisms around the ward)
After 2 hours of proper nursing intervention the client risk for infection is decrease to achieve timely wound healing as evidenced by:
a. Washing the hands using soap
b. Good body hygiene
c. Well kept surrounding
d. Short fingernails
31

invaded by different kind of microorganisms.
Impaired Skin Integrity
ASSESSMENT PLANNING INTERVENTIONSEXPECTED OUTCOME
S
“nangangati ang sugat ko”O
with surgical incision at the mcburney’s point
with suture noted
with surgical dressing intact
poor skin turgor
limited movement
Within 1 hour of proper nursing interventions, the patient will regain integrity of the skin and demonstrate measures to protect care and heal the skin lesion.
Assess site of skin impairment (the cause of the wound must be determined before appropriate interventions can be implemented).
Monitor site of skin impairment for color change, redness, swelling, warmth, pain, or other signs of infections (systematic inspection can identify impending problem early).
Clean the site aseptically (to decrease the production of bacteria).
Select a topical treatment that will maintain a moist wound – healing environment and that is balanced with the need to absorb exudates ( keep peri wound skin dry and control
After 1 hour of rendering proper nursing interventions, the patient will regain integrity of the skin and demonstrate measures to protect care and heal the skin lesion.
32

DiagnosisImpaired skin integrity related to tissue damage.Scientific explanation
Invasion of body structures, destruction of skin layers (dermis), disruption of skin surface (epidermis).
exudates and eliminate dead space) Avoid massaging around the site of
skin impairment and over bony prominences (massage may lead to tissue trauma).
Monitor nutritional intake (Altered nutrition can prevent wound healing and put at risk for further skin breakdown).
Fatigue
Assessment Planning Interventions Expected OutcomesSubjective: Nanghihina ako”
Objective:
with limited body movements
weak in appearance
slow and low voice noted
diaphoretic
vital signs taken as follows:
BP-80/70 mmHg
Within 1 hour of proper nursing interventions, the patient will verbalize increase body strength.
Obtain vital signs. (for baseline purposes)
Maintain on a flat position as an order of the physician.
Encourage to have adequate rest. (to gain energy)
Encourage to ask some help to the nurse or significant others if she want to move or change in position. (for the patients safety)
Instruct to increase fluid intake after
Within 1 hour of proper nursing interventions, the patient will verbalize increase body strength.
33

RR-20 cpmPR-64 bpmTemp- 35.8 °cDiagnosis:Fatigue related to post surgical procedure.Scientific Explanation:
An overwhelming sustained sense of exhaustion and decreased capacity for physical and mental work at usual level.
NPO. (to prevent dehydration)
Instruct to eat nutritious foods like green leafy vegetables after NPO. (to gain more energy)
Educate about the significant others to assist the patient when moving. (for safety and for the patient to move easily)
Instruct to take medications that are prescribed by the physician. (To avoid any drug accident such as overdosing.)
34

C. IMPLEMENTATION
1. DRUGSName of Drug Date
AdministeredRoute and
AdministrationGeneral Action Indication Client’s actual
response to medication
Cefoxitin October 1, 2010
6:00pm
IVP
1gq 8 hours
Bactericidal: Inhibits synthesis of bacterial cell
wall, causing cell death.
Perioperative prophylaxis.
Presence of pain was noted on the IV insertion site during the drug administration.
Nursing Responsibilities:
Check the doctor’s order. Check the right drug, right patient, right time, right frequency and right route of drug administration. Explain to the patient and/or relatives the purpose of the drug. Document The Drug administration done. Check the patient for any possible adverse reaction to the drug.
35

Name of Drug Date Administered Route and Administration
General Action Indication Client’s actual response to medication
Ketorolac September 30, 2010
6:00pm
IVP
30mgq 6 hours
anti-inflammatory, antipyretic and analgesic effects is the inhibition of prostaglandin synthesis by competitive blocking of the enzyme cyclooxygenase (COX)
Short-term management of pain due to surgical procedure done
Pain scale of 8/10 decreases to 4/10 which is consider as bearable pain.
Nursing Responsibilities:
Check the doctor’s order. Check the right drug, right patient, right time, right frequency and right route of drug administration. Explain to the patient and/or relatives the purpose of the drug. Document The Drug administration done. Check the patient for any possible adverse reaction to the drug.
36

Name of Drug Date Administered
Route and Administration
General Action Indication Client’s actual response to medication
Omeprazole September 30, 2010
6:00pm
IVP
40mgq 12 hours
Gastric acid-pump inhibitor. Suppresses gastric acid secretion by specific inhibition of the hydrogen-potassium ATPase enzyme system at the secretory surface of the gastric parietal cells; blocks the final step of acid production.
Perioperative client who is NPO
Pain due to hypersecretion of hydrochloric acid in the stomach is lessen.
Nursing Responsibilities:
37

Check the doctor’s order. Check the right drug, right patient, right time, right frequency and right route of drug administration. Explain to the patient and/or relatives the purpose of the drug. Document The Drug administration done. Check the patient for any possible adverse reaction to the drug.
Name of Drug Date Administered
Route and Administration
General Action Indication Client’s actual response to medication
Paracetamol October 1, 2010
6:00pm
IVP
30mgPRN
The main mechanism of action of paracetamol is considered to be the inhibition of cyclooxygenase (COX)
For client who has elevated temperature (hyperthermia)
Client’s temperature of 38.5oc decreases to 37.5oc
Nursing Responsibilities:
38

Check the doctor’s order. Check the right drug, right patient, right time, right frequency and right route of drug administration. Explain to the patient and/or relatives the purpose of the drug. Document The Drug administration done. Check the patient for any possible adverse reaction to the drug.
2. MEDICAL MANAGEMENT
Medical Management
Date Ordered/ Performed/ Changed/ Discontinued
General Description Indication/s or purpose/s
Client’s reaction to treatment
Intravenous FluidD5LRS @
Changed: September 30, 2010 at 10:28 pm.
D5LR is actually 5% dextrose in lactated ringer's solution. It is a hypertonic solution which
This solution is indicated for use in adults and
The patient was hydrated. The fluid and electrolytes level
39

20gtts/min means it pulls fluid out of the cells into the intravascular space (veins).
5% Dextrose in Lactated Ringer's Injection provides electrolytes and calories, and is a source of water for hydration. It is capable of inducing diuresis depending on the clinical condition of the patient. This solution also contains lactate which produces a metabolic alkalinizing effect.
pediatric patients as a source of electrolytes, calories and water for hydration.
of her body is maintained.
40

Nursing Management
Prior
Before starting I.V therapy, consider duration of therapy, type of infusion condition
of veins and medical condition of the patient to assist in choosing in I.V site and type
of catheter.
Ensure that you are competent in initiating the type of I.V therapy decided on and
familiar with institutional policy and procedure before initiating therapy.
Explain the procedure to the client and why is it necessary.
During
Monitor the insertion site for signs of phlebitis or infiltration.
Monitor the flow rate of the IV fluid.
Maintain the cleanliness of the plaster.
After
After initiation of I.V therapy, monitor the patient frequently for:
1. Signs of infiltration of sluggish flow
2. Signs of phlebitis or infection
3. Correct solution, medication, volume and rate
4. Dwell time of catheter and need to be replace
5. Condition of catheter dressing and frequency of change
6. Fluid and electrolyte balance
7. Signs of fluid overload or dehydration
8. Patient satisfaction with mode therapy
41

MedicalManagement
Date Ordered/Performed
Changed/discontinuedGeneral Description Indication/s or purpose/s
Client’s reaction to treatment
Oxygen Therapy 09-30-2010
08-30-2010
Oxygen may be classified as an element, a gas, and a drug. Oxygen therapy is the administration of oxygen at concentrations greater than that in room air to treat or prevent hypoxemia (not enough oxygen in the blood). Oxygen delivery systems are classified as stationary, portable, or ambulatory. Oxygen can be administered by nasal cannula, mask, and tent. Hyperbaric oxygen therapy involves placing the patient in an airtight chamber with oxygen under pressure.
The body is constantly taking in oxygen and releasing carbon dioxide. If this process is inadequate, oxygen levels in the blood decrease and the patient may need supplemental oxygen. Oxygen therapy is a key treatment in respiratory care. The purpose is to increase oxygen saturation in tissues where the saturation levels are too low due to illness or injury.
Breathing prescribed oxygen increases the amount of oxygen in the blood, reduces the extra work of the heart, and decreases shortness of breath. Oxygen therapy is frequently ordered in the home care setting, as well as in acute (urgent) care facilities.
The patient’s oxygen need was sustained. Airway becomes easier. Breathing pattern becomes normal.
42

43

3. Surgical Management
DATE PERFORMED: September 30, 2010 – 11:45 a.m
Name of Procedure Brief Description Indication/ PurposeClient’s Response to
Operation
Appendectomy Surgical removal of the Appendix
To remove the inflamed appendix to prevent rupture - this will eventually lead to peritonitis.
The patient was asleep after the operation.
The patient was lying flat on bed 6 – 8 hours after the surgery.
The patient had chills few hours after the operation.
The patient had fever 1 day after the operation.
Nursing Responsibilities
Prior to the Surgery
Check the vital signs for baseline data.
Instruct the patient to be on nothing per Orem 8 hours prior to surgery.
Educate the patient the patient about coughing, deep breathing exercises and turning side
– to – side after the surgery.
Let the patient voice out what she feels to relieve anxiety.
Listen to what the patient says.
During the surgery
Promote sterility on the sterile field.
Monitor the patient’s well being.
44

Monitor patient’s vital signs
After the Surgery
Keep the patient on NPO for 6 to 8 hours or until peristalsis occurs.
Keep the patient lie flat on bed without pillow for 6 to 8 hours.
Monitor for bleeding and signs of shock.
Monitor for signs of infection.
45

4. DIET
46

5. ACTIVITY/EXERCISE
47

D. EVALUATION
III. CONCLUSION
The group’s grand case study is about ruptured appendicitis. It was a good learning
experience for our group to handle such case.
The client manifest hyperthermia, fatigue, impaired physical mobility, and impaired skin
integrity, the group therefore concludes that nursing intervention should be done to alleviate
predicament on the client’s health. The highlight of our principle is to provide optimum nursing
care primarily to our client and the significant others as well. The group believes that the first
thing to consider for our client’s wellness to make them feel special and be sincere in rendering
quality services.
Susceptibility of the client to acquire complication is greatly at risk. Hence, client should
be monitor carefully and medications must be maintained ideally.
IV. RECOMMENDATION
The group recommends providing wound care aseptically as frequently as possible to
prevent infection and apply cold compress to the abdomen when abdominal pain is experience.
Advice regular consultation to the physician for it can be a factor for recovery and assess the
patient’s progress. Advised the client who has to religiously take his medication prescribed to
alleviate symptoms and prevent further complications. Instruct the patient normal activities can
be resumed within a few days, but it takes four to six weeks for full recovery. Heavy lifting and
strenuous activities should be avoided during recovery. Encourage continuous range of motion
exercises. Eat healthy foods from all of the five food groups; fruits, vegetables, breads, dairy
products, meats, fishes. Eating healthy foods may help the patient feel better and have more
energy and also help recover faster from sickness. Emphasize the importance of increase dietary
intake of fiber and vitamin C. Avoid foods that can cause constipation such as apple, guava and
star apple. Encourage to increase fluid intake to maintain hydration and electrolyte balance.
48

V. REVIEW OF RELATED LITERATURE
Viral Infections Linked to Appendicitis
By Rajshri on January 19, 2010 at 6:55 PM
A new study by UT Southwestern Medical Center surgeons and physicians says that appendicitis may also be caused by a virus and that you can actually "catch" it.
The researchers evaluated data over a 36-year period from the National Hospital Discharge Survey and concluded in a paper appearing in the January issue of Archives of Surgery that appendicitis may be caused by undetermined viral infection or infections, said Dr. Edward Livingston, chief of GI/endocrine surgery at UT Southwestern and senior author of the report.
The review of hospital discharge data runs counter to traditional thought, suggesting that appendicitis doesn't necessarily lead to a burst appendix if the organ is not removed quickly, Dr. Livingston said.
"Just as the traditional appendix scar across the abdomen is fast becoming history, thanks to new single-incision surgery techniques that hide a tiny scar in the bellybutton, so too may the conventional wisdom that patients with appendicitis need to be operated on as soon as they enter the hospital," said Dr. Livingston. "Patients still need to be seen quickly by a physician, but emergency surgery is now in question."
Appendicitis is the most common reason for emergency general surgery, leading to some 280,000 appendectomies being performed annually.
Appendicitis was first identified in 1886. Since then, doctors
have presumed quick removal of the appendix was a necessity to avoid a subsequent bursting,
which can be an emergency. Because removing the appendix solves the problems and is
generally safe, removal became the standard medical practice in the early 20th century.
SOURCE: http://www.medindia.net/news/Viral-Infections-Linked-to-Appendicitis-63833-1.htm
49

VI. BIBLIOGRAPHY
Published Materials
Medical – Surgical Nursing: Clinical Management for Positive Outcome 8th by Joyce Black and
Jane Hokanson Hawks,
Fundamentals of Nursing Practice 7th edition by Kozier and Erbs
Health Assessment and Physical Examination 3rd edition by Estes
Medical – Surgical Nursing 8th edition by Joyce Black
2010 Lippincotts Nursing Drug Guide by Amy Karch
Prentice Hall Nursing Diagnosis Handbook by Judith M. Wilkinson and Nancy R. Ahern
Unpublished Materials
http://www.wikipedia.org/wiki/Appendicitis?wasRedirected=true
http://www.healthscout.com/ency/68/658/main.html
http://www.ufs.ph/tinig/mayjun02/05060225.html
http://www.nlm.nih.gov/medlineplus/ency/arcticle/002921.html
http://www.diagnosis.com/a/acute_appendicitis/prevalence.html
http://wiki.answers.com/Q/What_is_the_appendicitis_rate_in_the_Philippines
50

51