Aplastic Anemia: Current Thinking LGL on the Disease ... AA Current... · aplastic anemia = low...
14
3/23/2015 1 Aplastic Anemia: Current Thinking on the Disease, Diagnosis, and Non-Transplant Treatment Bogdan Dumitriu, MD Hematology Branch National, Heart, Lung and Blood Institute National Institutes of Health BONE MARROW FAILURE SYNDROMES SDS DKC LGL AA AA/PNH PNH MDS hypocellular MDS AML AID: MS, IBD, uveitis, DM type 1, etc. Hemoglobin – variable, around 7-8 g/dL (>13 g/dL) weakness, fatigue, shortness of breath, lack of energy Neutrophils – under 500/uL (>1500/uL) infections, mouth ulcers Platelets – under 10.000/uL (>150.000/uL) bleeding (gums, nose, skin) APLASTIC ANEMIA = LOW BLOOD COUNTS CLINICAL MANIFESTATIONS OF BONE MAROW FAILURE anemia, bleeding, infection AGE AT DIAGNOSIS Aplastic Anemia Admissions to NIH Clinical Center Years Camitta et al, Blood 53:504, 1979 Williams et al, Sem Hematol 10:195, 1973 6 5 4 3 2 1 0 0 60 80 100 20 40 Utah, extrapolated severe “NATURAL HISTORY” OF APLASTIC ANEMIA % Surviving AA Study Group, non-transplanted (n = 63) Utah, total (n = 99) Severity Criteria (two of three): platelets <20k/uL reticulocytes <1% (60k/uL) ANC <500/uL Very severe: ANC <200/uL
Transcript of Aplastic Anemia: Current Thinking LGL on the Disease ... AA Current... · aplastic anemia = low...
3/23/2015
1
Aplastic Anemia: Current Thinking
on the Disease, Diagnosis, and
Non-Transplant Treatment
Bogdan Dumitriu, MD
Hematology Branch
National, Heart, Lung and Blood Institute
National Institutes of Health
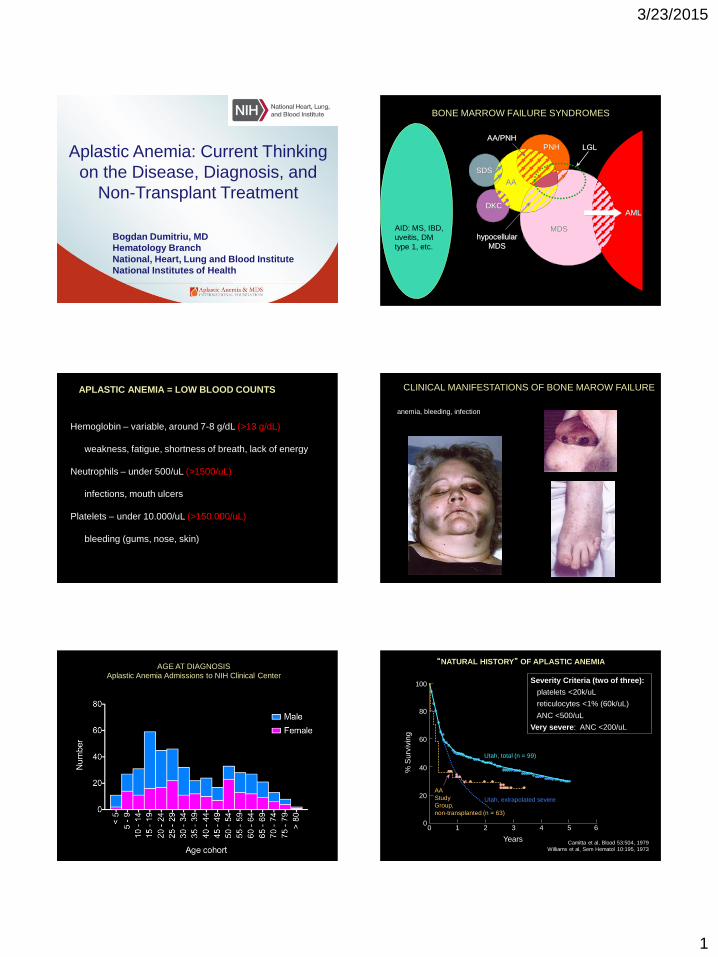
BONE MARROW FAILURE SYNDROMES
SDS
DKC
LGL
AA
AA/PNH
PNH
MDShypocellular
MDS
AML
AID: MS, IBD,
uveitis, DM
type 1, etc.
Hemoglobin – variable, around 7-8 g/dL (>13 g/dL)
weakness, fatigue, shortness of breath, lack of energy
Neutrophils – under 500/uL (>1500/uL)
infections, mouth ulcers
Platelets – under 10.000/uL (>150.000/uL)
bleeding (gums, nose, skin)
APLASTIC ANEMIA = LOW BLOOD COUNTS CLINICAL MANIFESTATIONS OF BONE MAROW FAILURE
anemia, bleeding, infection
AGE AT DIAGNOSIS
Aplastic Anemia Admissions to NIH Clinical Center
YearsCamitta et al, Blood 53:504, 1979
Williams et al, Sem Hematol 10:195, 1973
65432100
60
80
100
20
40
Utah, extrapolated severe
“NATURAL HISTORY” OF APLASTIC ANEMIA
% S
urv
ivin
g
AA
Study
Group,
non-transplanted (n = 63)
Utah, total (n = 99)
Severity Criteria (two of three):
platelets <20k/uL
reticulocytes <1% (60k/uL)
ANC <500/uL
Very severe: ANC <200/uL
3/23/2015
2
Normal
bone
marrow
Aplastic
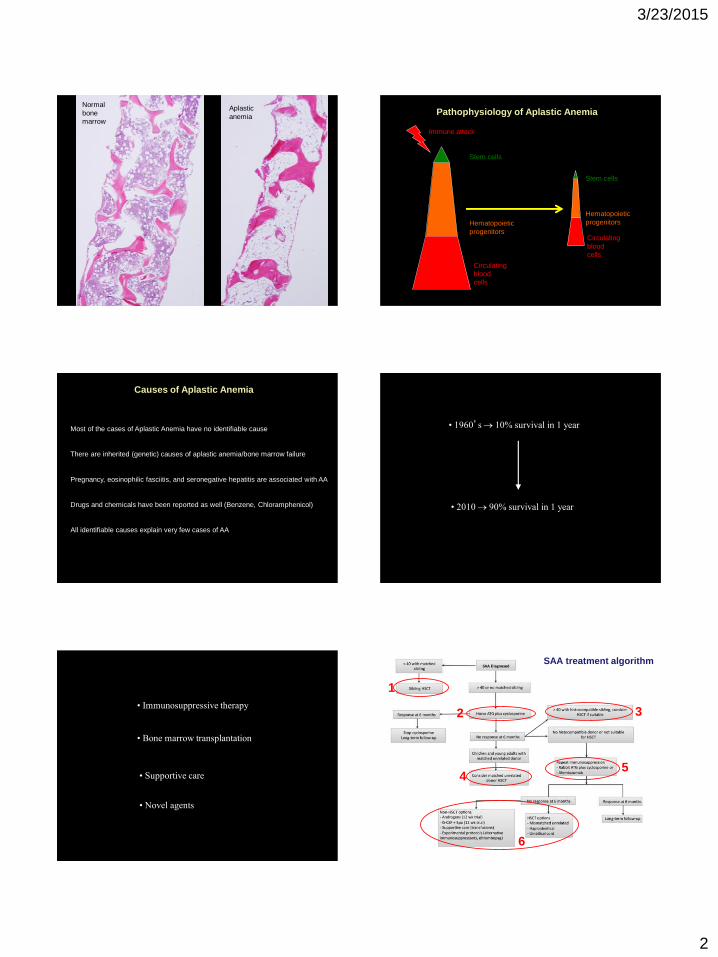
anemiaPathophysiology of Aplastic Anemia
Stem cells
Hematopoietic
progenitors
Immune attack
Circulating
blood
cells
Stem cells
Hematopoietic
progenitors
Circulating
blood
cells
Most of the cases of Aplastic Anemia have no identifiable cause
There are inherited (genetic) causes of aplastic anemia/bone marrow failure
Pregnancy, eosinophilic fasciitis, and seronegative hepatitis are associated with AA
Drugs and chemicals have been reported as well (Benzene, Chloramphenicol)
All identifiable causes explain very few cases of AA
Causes of Aplastic Anemia
• 1960’s 10% survival in 1 year
• 2010 90% survival in 1 year
• Immunosuppressive therapy
• Bone marrow transplantation
• Supportive care
• Novel agents
2
1
3
45
6
SAA treatment algorithm
3/23/2015
3
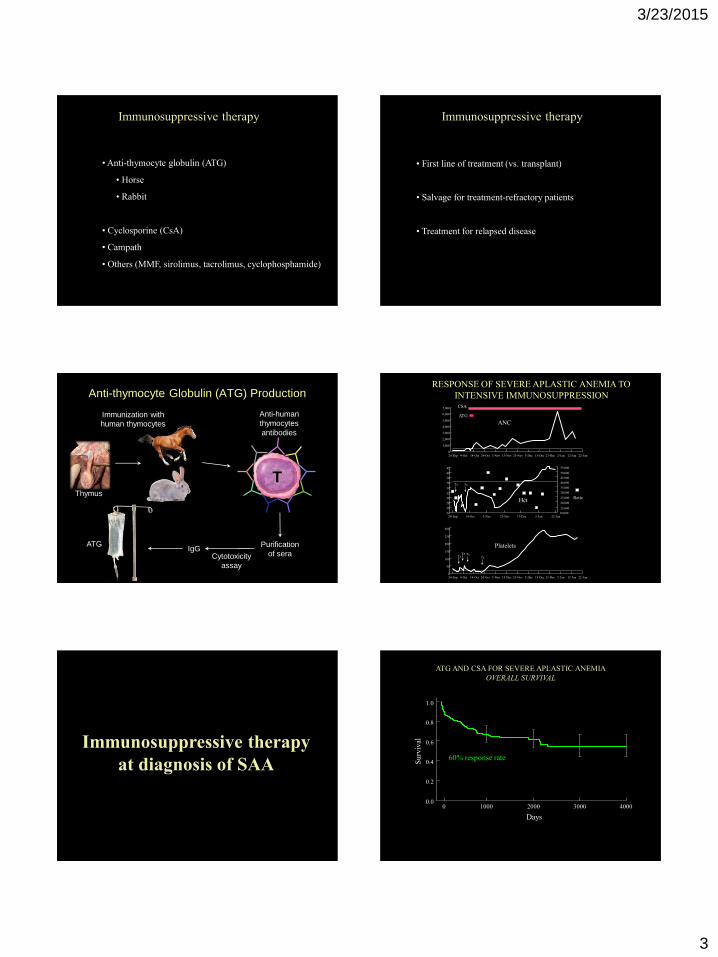
•Anti-thymocyte globulin (ATG)
• Horse
• Rabbit
• Cyclosporine (CsA)
• Campath
• Others (MMF, sirolimus, tacrolimus, cyclophosphamide)
Immunosuppressive therapy
• First line of treatment (vs. transplant)
• Salvage for treatment-refractory patients
• Treatment for relapsed disease
Immunosuppressive therapy
Cytotoxicity
assay
Immunization with
human thymocytes
Anti-human
thymocytes
antibodies
T
Purification
of seraIgG
ATG
Anti-thymocyte Globulin (ATG) Production
Thymus
RESPONSE OF SEVERE APLASTIC ANEMIA TO
INTENSIVE IMMUNOSUPPRESSION
7,000
6,000
5,000
4,000
3,000
2,000
1,000
024-Sep 4-Oct 14-Oct 24-Oct 3-Nov 13-Nov 23-Nov 3-Dec 13-Dec 23-Dec 2-Jan 12-Jan 22-Jan
300
250
200
150
100
50
024-Sep 4-Oct 14-Oct 24-Oct 3-Nov 13-Nov 23-Nov 3-Dec 13-Dec 23-Dec 2-Jan 12-Jan 22-Jan
TxTx Tx
Tx
CSA
ATG
42
40
38
34
32
30
26
2424-Sep 14-Oct 3-Nov 23-Nov 13-Dec 2-Jan 22-Jan
36
28
10,000
15,000
20,000
25,000
30,000
35,000
40,000
45,000
50,000
55,000
Tx Tx
ANC
Platelets
ReticHct
Immunosuppressive therapy
at diagnosis of SAA
ATG AND CSA FOR SEVERE APLASTIC ANEMIA
OVERALL SURVIVAL
1.0
0.8
0.6
0.4
0.2
0.00 1000 2000 3000
Days
4000
Su
rviv
al
60% response rate
3/23/2015
4
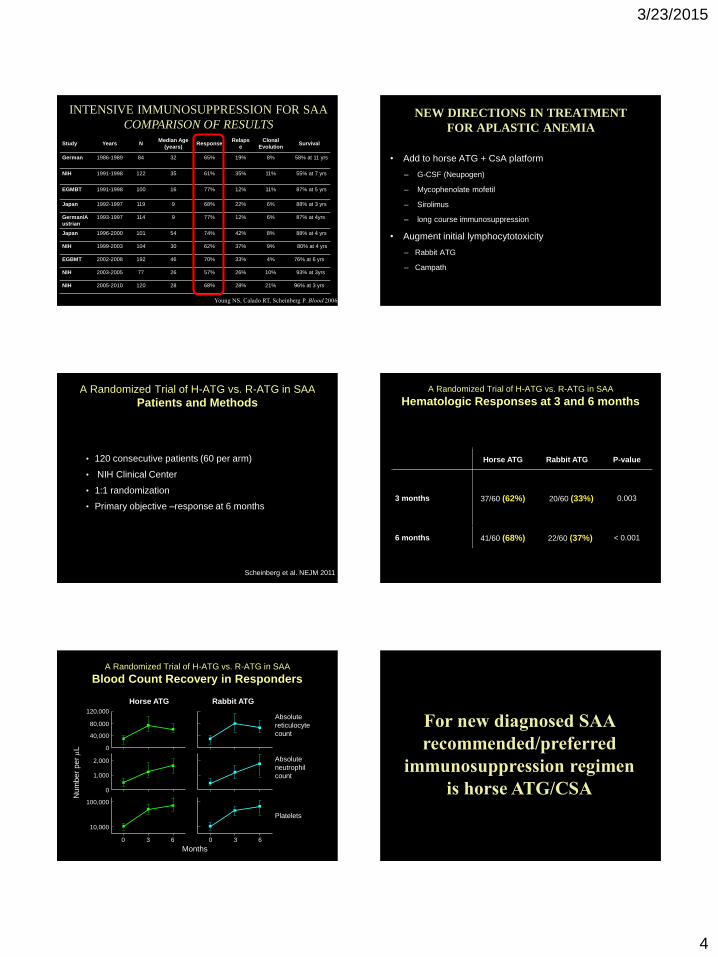
Study Years NMedian Age
(years)Response
Relaps
e
Clonal
EvolutionSurvival
German 1986-1989 84 32 65% 19% 8% 58% at 11 yrs
NIH 1991-1998 122 35 61% 35% 11% 55% at 7 yrs
EGMBT 1991-1998 100 16 77% 12% 11% 87% at 5 yrs
Japan 1992-1997 119 9 68% 22% 6% 88% at 3 yrs
German/A
ustrian
1993-1997 114 9 77% 12% 6% 87% at 4yrs
Japan 1996-2000 101 54 74% 42% 8% 88% at 4 yrs
NIH 1999-2003 104 30 62% 37% 9% 80% at 4 yrs
EGBMT 2002-2008 192 46 70% 33% 4% 76% at 6 yrs
NIH 2003-2005 77 26 57% 26% 10% 93% at 3yrs
NIH 2005-2010 120 28 68% 28% 21% 96% at 3 yrs
Young NS, Calado RT, Scheinberg P. Blood 2006
INTENSIVE IMMUNOSUPPRESSION FOR SAA
COMPARISON OF RESULTS
• Add to horse ATG + CsA platform
– G-CSF (Neupogen)
– Mycophenolate mofetil
– Sirolimus
– long course immunosuppression
• Augment initial lymphocytotoxicity
– Rabbit ATG
– Campath
NEW DIRECTIONS IN TREATMENT
FOR APLASTIC ANEMIA
A Randomized Trial of H-ATG vs. R-ATG in SAA
Patients and Methods
• 120 consecutive patients (60 per arm)
• NIH Clinical Center
• 1:1 randomization
• Primary objective –response at 6 months
Scheinberg et al. NEJM 2011
Horse ATG Rabbit ATG P-value
3 months 37/60 (62%) 20/60 (33%) 0.003
6 months 41/60 (68%) 22/60 (37%) < 0.001
A Randomized Trial of H-ATG vs. R-ATG in SAA
Hematologic Responses at 3 and 6 months
A Randomized Trial of H-ATG vs. R-ATG in SAA
Blood Count Recovery in Responders
Months
Horse ATG Rabbit ATG
Absolute
reticulocyte
count
Absolute
neutrophil
count
Platelets
630630
120,000
80,000
40,000
0
0
1,000
2,000
100,000
10,000
Num
ber
per L
For new diagnosed SAA
recommended/preferred
immunosuppression regimen
is horse ATG/CSA
3/23/2015
5
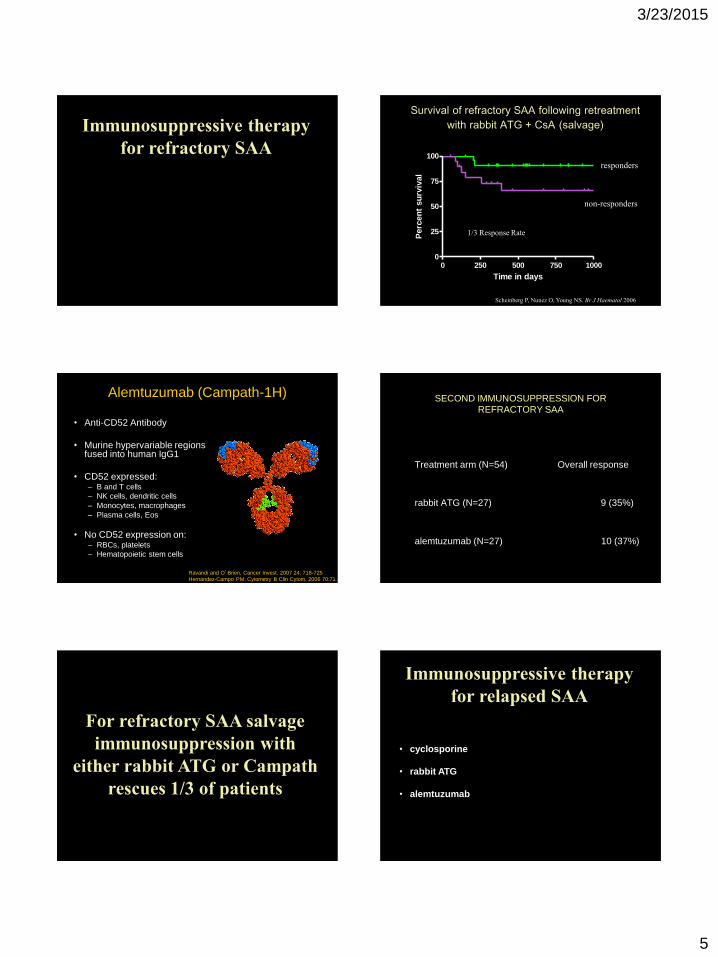
Immunosuppressive therapy
for refractory SAA
• rabbit ATG
• Campath
0 250 500 750 10000
25
50
75
100
Time in days
Perc
en
t su
rviv
al
Survival of refractory SAA following retreatment
with rabbit ATG + CsA (salvage)
responders
non-responders
Scheinberg P, Nunez O, Young NS. Br J Haematol 2006
1/3 Response Rate
Alemtuzumab (Campath-1H)
• Anti-CD52 Antibody
• Murine hypervariable regions fused into human IgG1
• CD52 expressed:– B and T cells
– NK cells, dendritic cells
– Monocytes, macrophages
– Plasma cells, Eos
• No CD52 expression on:– RBCs, platelets
– Hematopoietic stem cells
Ravandi and O’Brien, Cancer Invest. 2007 24: 718-725
Hernández-Campo PM, Cytometry B Clin Cytom. 2006 70:71
SECOND IMMUNOSUPPRESSION FOR
REFRACTORY SAA
Treatment arm (N=54) Overall response
rabbit ATG (N=27) 9 (35%)
alemtuzumab (N=27) 10 (37%)
For refractory SAA salvage
immunosuppression with
either rabbit ATG or Campath
rescues 1/3 of patients
Immunosuppressive therapy
for relapsed SAA
• cyclosporine
• rabbit ATG
• alemtuzumab
3/23/2015
6
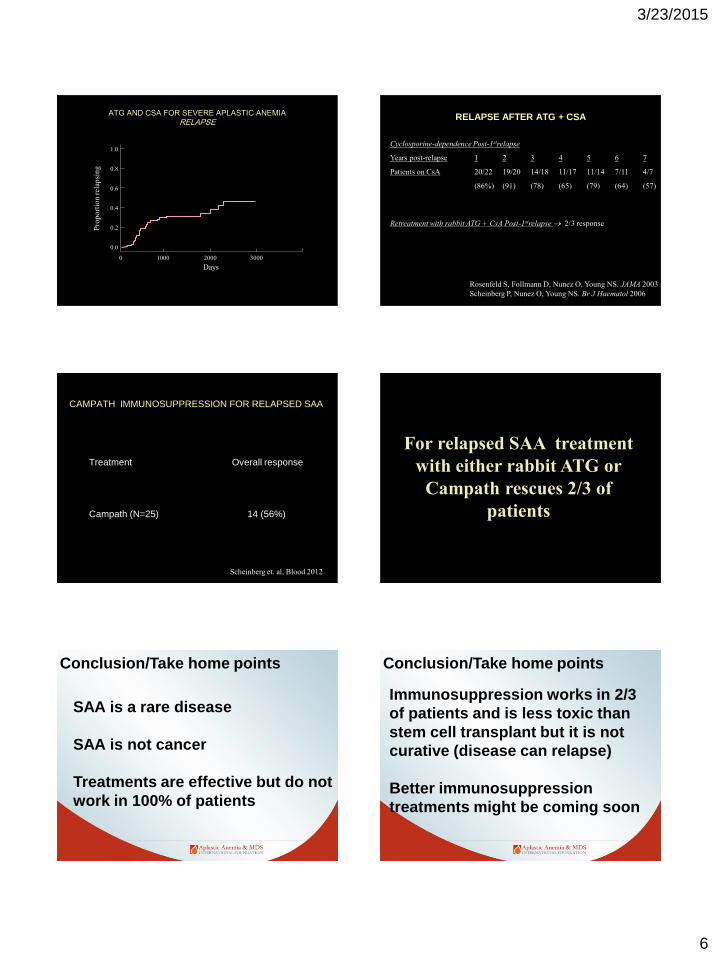
ATG AND CSA FOR SEVERE APLASTIC ANEMIA
RELAPSE
1.0
0.8
0.6
0.4
0.2
0.0
0 1000 2000 3000
Days
4000
0
Pro
po
rtio
n r
elap
sin
g
RELAPSE AFTER ATG + CSA
Cyclosporine-dependence Post-1strelapse
Years post-relapse 1 2 3 4 5 6 7
Patients on CsA 20/22 19/20 14/18 11/17 11/14 7/11 4/7
(86%) (91) (78) (65) (79) (64) (57)
Retreatment with rabbit ATG + CsA Post-1strelapse 2/3 response
Rosenfeld S, Follmann D, Nunez O, Young NS. JAMA 2003
Scheinberg P, Nunez O, Young NS. Br J Haematol 2006
CAMPATH IMMUNOSUPPRESSION FOR RELAPSED SAA
Treatment Overall response
Campath (N=25) 14 (56%)
Scheinberg et. al, Blood 2012
For relapsed SAA treatment
with either rabbit ATG or
Campath rescues 2/3 of
patients
Conclusion/Take home points
SAA is a rare disease
SAA is not cancer
Treatments are effective but do not
work in 100% of patients
Conclusion/Take home points
Immunosuppression works in 2/3
of patients and is less toxic than
stem cell transplant but it is not
curative (disease can relapse)
Better immunosuppression
treatments might be coming soon
3/23/2015
7
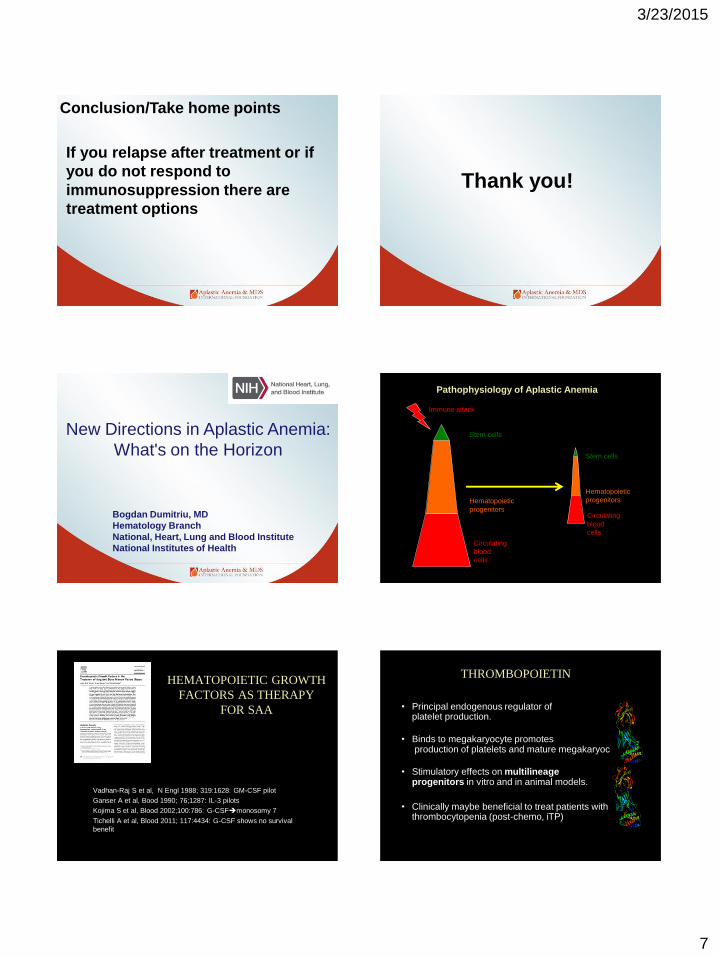
Conclusion/Take home points
If you relapse after treatment or if
you do not respond to
immunosuppression there are
treatment options
Thank you!
New Directions in Aplastic Anemia:
What's on the Horizon
Bogdan Dumitriu, MD
Hematology Branch
National, Heart, Lung and Blood Institute
National Institutes of Health
Pathophysiology of Aplastic Anemia
Stem cells
Hematopoietic
progenitors
Immune attack
Circulating
blood
cells
Stem cells
Hematopoietic
progenitors
Circulating
blood
cells
HEMATOPOIETIC GROWTH
FACTORS AS THERAPY
FOR SAA
Vadhan-Raj S et al, N Engl 1988; 319:1628: GM-CSF pilot
Ganser A et al, Bood 1990; 76;1287: IL-3 pilots
Kojima S et al, Blood 2002;100:786: G-CSFmonosomy 7
Tichelli A et al, Blood 2011; 117:4434: G-CSF shows no survival
benefit
THROMBOPOIETIN
• Principal endogenous regulator of platelet production.
• Binds to megakaryocyte promotes production of platelets and mature megakaryocytes.
• Stimulatory effects on multilineageprogenitors in vitro and in animal models.
• Clinically maybe beneficial to treat patients with thrombocytopenia (post-chemo, iTP)
3/23/2015
8
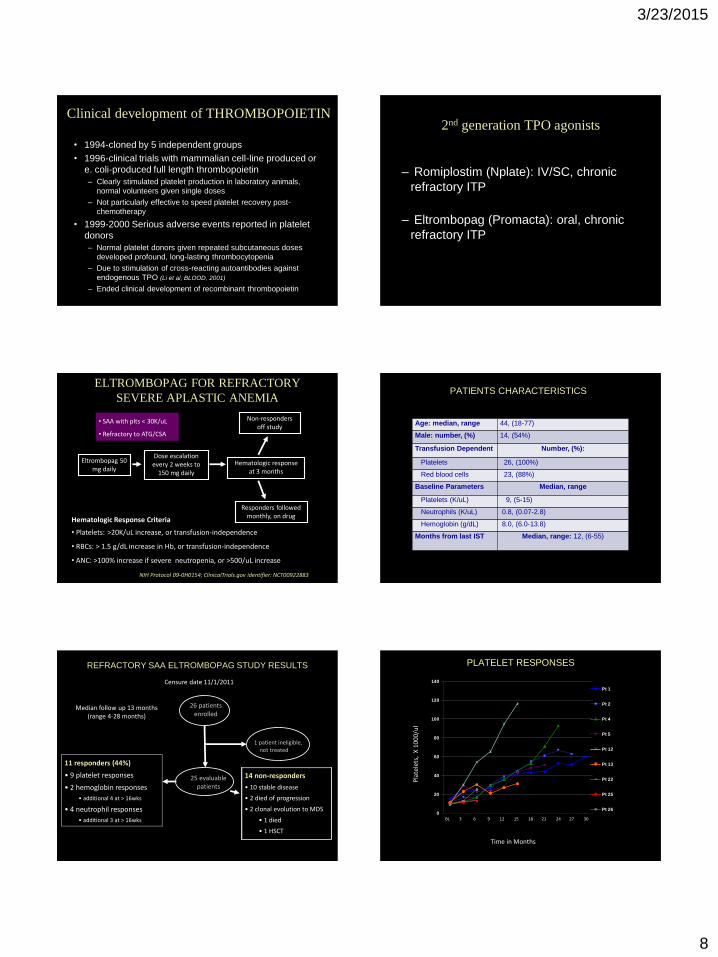
Clinical development of THROMBOPOIETIN
• 1994-cloned by 5 independent groups
• 1996-clinical trials with mammalian cell-line produced or
e. coli-produced full length thrombopoietin
– Clearly stimulated platelet production in laboratory animals,
normal volunteers given single doses
– Not particularly effective to speed platelet recovery post-
chemotherapy
• 1999-2000 Serious adverse events reported in platelet
donors
– Normal platelet donors given repeated subcutaneous doses
developed profound, long-lasting thrombocytopenia
– Due to stimulation of cross-reacting autoantibodies against
endogenous TPO (Li et al, BLOOD, 2001)
– Ended clinical development of recombinant thrombopoietin
2nd generation TPO agonists
– Romiplostim (Nplate): IV/SC, chronic
refractory ITP
– Eltrombopag (Promacta): oral, chronic
refractory ITP
ELTROMBOPAG FOR REFRACTORY
SEVERE APLASTIC ANEMIA
Eltrombopag 50 mg daily
Dose escalation every 2 weeks to
150 mg daily
Hematologic responseat 3 months
Non-responders off study
Responders followedmonthly, on drug
NIH Protocol 09-0H0154; ClinicalTrials.gov identifier: NCT00922883
Hematologic Response Criteria
• Platelets: >20K/uL increase, or transfusion-independence
• RBCs: > 1.5 g/dL increase in Hb, or transfusion-independence
• ANC: >100% increase if severe neutropenia, or >500/uL increase
• SAA with plts < 30K/uL
• Refractory to ATG/CSA
PATIENTS CHARACTERISTICS
Age: median, range 44, (18-77)
Male: number, (%) 14, (54%)
Transfusion Dependent Number, (%):
Platelets 26, (100%)
Red blood cells 23, (88%)
Baseline Parameters Median, range
Platelets (K/uL) 9, (5-15)
Neutrophils (K/uL) 0.8, (0.07-2.8)
Hemoglobin (g/dL) 8.0, (6.0-13.8)
Months from last IST Median, range: 12, (6-55)
REFRACTORY SAA ELTROMBOPAG STUDY RESULTS
11 responders (44%)
• 9 platelet responses
• 2 hemoglobin responses
• additional 4 at > 16wks
• 4 neutrophil responses
• additional 3 at > 16wks
26 patientsenrolled
25 evaluablepatients
1 patient ineligible, not treated
14 non-responders
• 10 stable disease
• 2 died of progression
• 2 clonal evolution to MDS
• 1 died
• 1 HSCT
Median follow up 13 months(range 4-28 months)
Censure date 11/1/2011
Pla
tele
ts,
X 1
000/
ul
0
20
40
60
80
100
120
140
1 2 3 4 5 6 7 8 9 10 11
Pt 1
Pt 2
Pt 4
Pt 5
Pt 12
Pt 13
Pt 22
Pt 25
Pt 26
Time in Months
PLATELET RESPONSES
BL 3 6 9 12 15 18 21 24 27 30
3/23/2015
9
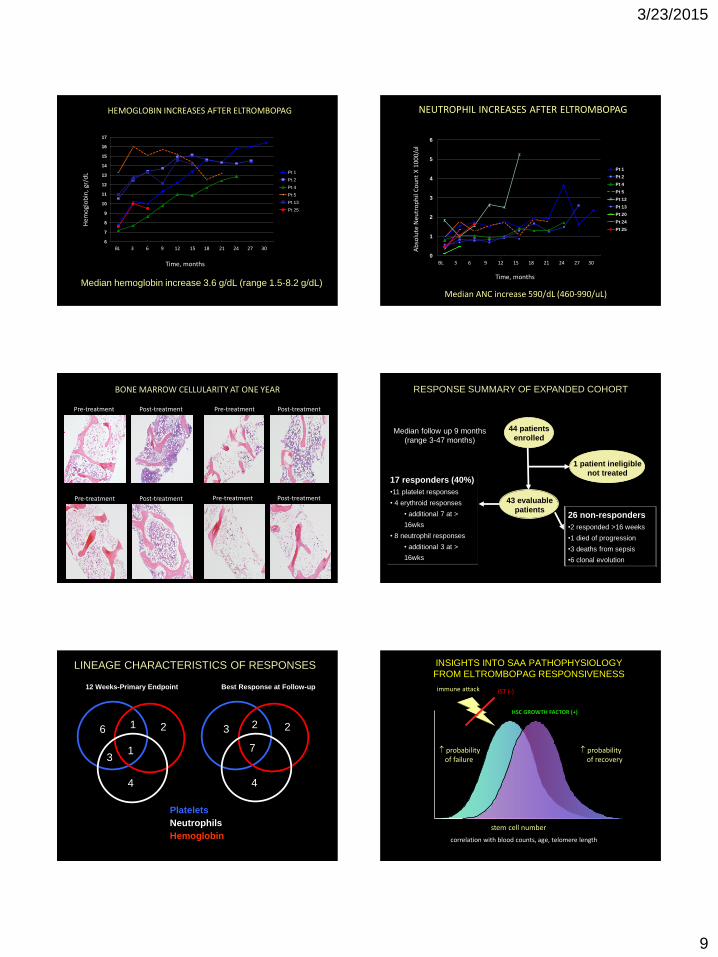
Hem
ogl
ob
in,
gr/d
L
Time, months
6
7
8
9
10
11
12
13
14
15
16
17
1 2 3 4 5 6 7 8 9 10 11
Pt 1
Pt 2
Pt 4
Pt 5
Pt 13
Pt 25
HEMOGLOBIN INCREASES AFTER ELTROMBOPAG
Median hemoglobin increase 3.6 g/dL (range 1.5-8.2 g/dL)
BL 3 6 9 12 15 18 21 24 27 30 Ab
solu
te N
eu
tro
ph
il C
ou
nt
X 1
00
0/u
l
Time, months
0
1
2
3
4
5
6
1 2 3 4 5 6 7 8 9 10 11
Pt 1
Pt 2
Pt 4
Pt 5
Pt 12
Pt 13
Pt 20
Pt 24
Pt 25
NEUTROPHIL INCREASES AFTER ELTROMBOPAG
Median ANC increase 590/dL (460-990/uL)
BL 3 6 9 12 15 18 21 24 27 30
BONE MARROW CELLULARITY AT ONE YEAR
Pre-treatment Post-treatment Pre-treatment Post-treatment
Pre-treatment Post-treatment Post-treatmentPre-treatment
RESPONSE SUMMARY OF EXPANDED COHORT
17 responders (40%)
•11 platelet responses
• 4 erythroid responses
• additional 7 at >
16wks
• 8 neutrophil responses
• additional 3 at >
16wks
44 patients
enrolled
43 evaluable
patients
1 patient ineligible,
not treated
26 non-responders
•2 responded >16 weeks
•1 died of progression
•3 deaths from sepsis
•6 clonal evolution
Median follow up 9 months
(range 3-47 months)
1 patient ineligible
not treated
16
Platelets
Neutrophils
Hemoglobin
4
3
3
4
7
12 Weeks-Primary Endpoint Best Response at Follow-up
LINEAGE CHARACTERISTICS OF RESPONSES
2 2 2
1
INSIGHTS INTO SAA PATHOPHYSIOLOGY
FROM ELTROMBOPAG RESPONSIVENESS
stem cell number
probability of failure
correlation with blood counts, age, telomere length
probability of recovery
HSC GROWTH FACTOR (+)
immune attack IST (-)
3/23/2015
10
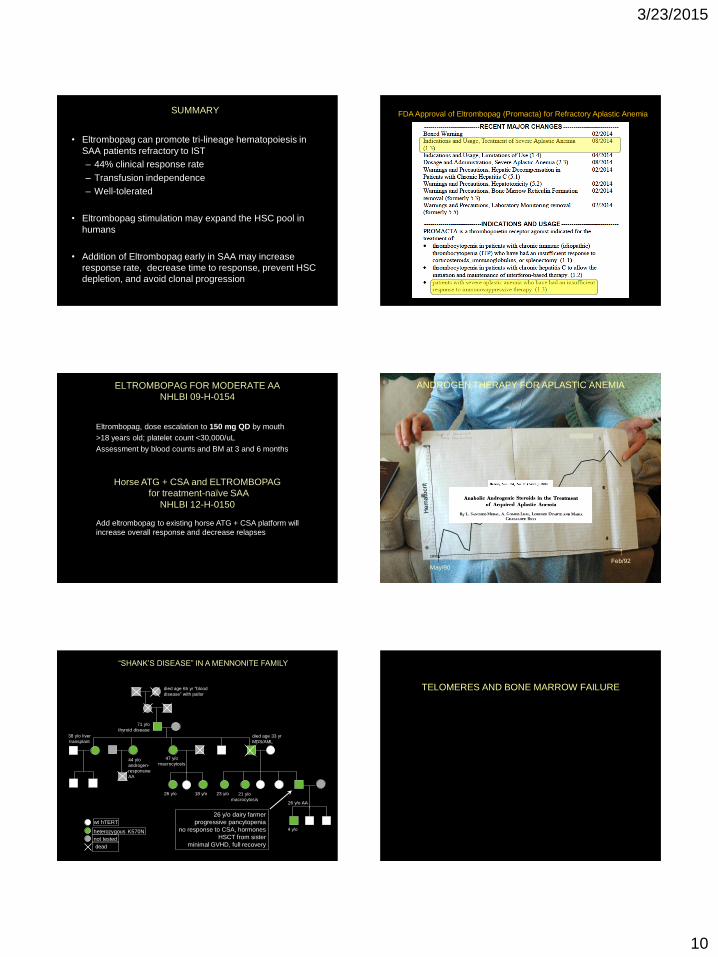
SUMMARY
• Eltrombopag can promote tri-lineage hematopoiesis in
SAA patients refractory to IST
– 44% clinical response rate
– Transfusion independence
– Well-tolerated
• Eltrombopag stimulation may expand the HSC pool in
humans
• Addition of Eltrombopag early in SAA may increase
response rate, decrease time to response, prevent HSC
depletion, and avoid clonal progression
FDA Approval of Eltrombopag (Promacta) for Refractory Aplastic Anemia
ELTROMBOPAG FOR MODERATE AA
NHLBI 09-H-0154
Eltrombopag, dose escalation to 150 mg QD by mouth
>18 years old; platelet count <30,000/uL
Assessment by blood counts and BM at 3 and 6 months
Horse ATG + CSA and ELTROMBOPAG
for treatment-naïve SAA
NHLBI 12-H-0150
Add eltrombopag to existing horse ATG + CSA platform will
increase overall response and decrease relapses
ANDROGEN THERAPY FOR APLASTIC ANEMIA
May/90Feb/92
16%
48%
38 y/o liver
transplant
26 y/o AA
47 y/o
macrocytosis
21 y/o
macrocytosis
71 y/o
thyroid disease
44 y/o
androgen-
responsive
AA
died age 33 yr
MDS/AML
26 y/o 18 y/o
4 y/o
died age 65 yr “blood
disease” with pallor
wt hTERT
heterozygous K570N
not tested
“SHANK’S DISEASE” IN A MENNONITE FAMILY
23 y/o
dead
26 y/o dairy farmer
progressive pancytopenia
no response to CSA, hormones
HSCT from sister
minimal GVHD, full recovery
TELOMERES AND BONE MARROW FAILURE
3/23/2015
11
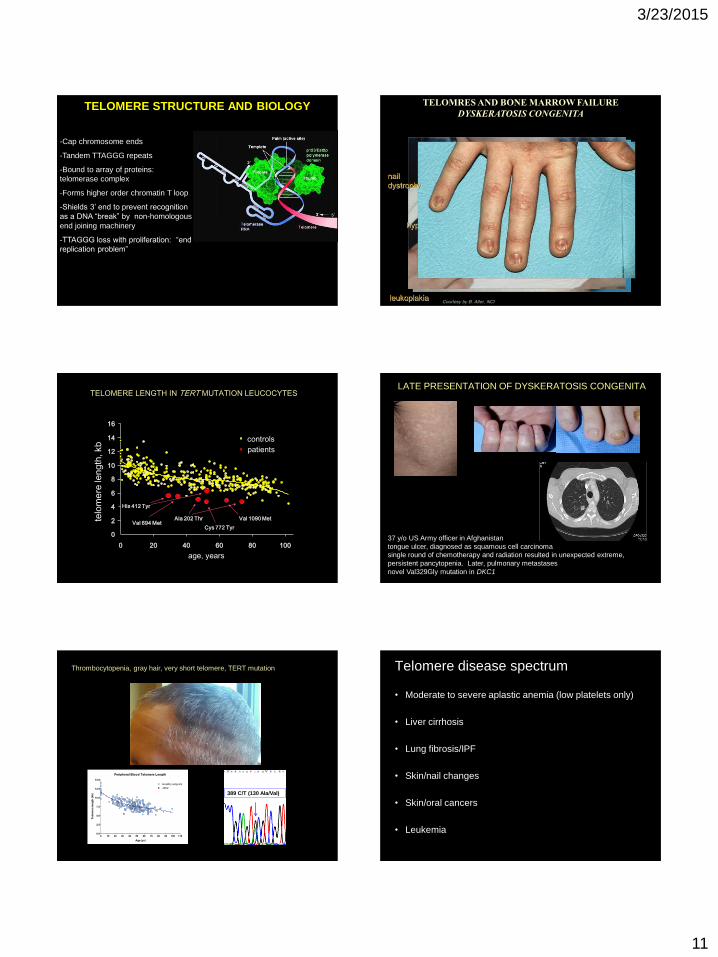
TELOMERE STRUCTURE AND BIOLOGY
-Cap chromosome ends
-Tandem TTAGGG repeats
-Bound to array of proteins:
telomerase complex
-Forms higher order chromatin T loop
-Shields 3’ end to prevent recognition
as a DNA “break” by non-homologous
end joining machinery
-TTAGGG loss with proliferation: “end
replication problem”
Autosomal Dominant DKC
Mutations in TERC:
RNA component of the telomerase
complex, the template for telomere
elongation
X-linked DKC
Mutations in DKC1:
encodes dyskerin, a protein
component of telomerase complex
leukoplakia
hyperpigmentation
nail
dystrophy
Courtesy by B. Alter, NCI
TELOMRES AND BONE MARROW FAILURE
DYSKERATOSIS CONGENITA
0
2
4
6
8
10
12
14
16
0 20 40 60 80 100
controls
age, years
telo
me
re le
ng
th, kb
His 412 Tyr
Val 694 MetAla 202 Thr
Cys 772 Tyr
Val 1090 Met
patients
TELOMERE LENGTH IN TERT MUTATION LEUCOCYTESLATE PRESENTATION OF DYSKERATOSIS CONGENITA
37 y/o US Army officer in Afghanistan
tongue ulcer, diagnosed as squamous cell carcinoma
single round of chemotherapy and radiation resulted in unexpected extreme,
persistent pancytopenia. Later, pulmonary metastases
novel Val329Gly mutation in DKC1
Peripheral Blood Telomere Length
0 10 20 30 40 50 60 70 80 90 100 1100.0
2.5
5.0
7.5
10.0
12.5
15.0
Healthy subjects
1952
Age (yr)
Te
lom
ere
le
ng
th (kb
)
Thrombocytopenia, gray hair, very short telomere, TERT mutation
389 C/T (130 Ala/Val)
Telomere disease spectrum
• Moderate to severe aplastic anemia (low platelets only)
• Liver cirrhosis
• Lung fibrosis/IPF
• Skin/nail changes
• Skin/oral cancers
• Leukemia
3/23/2015
12
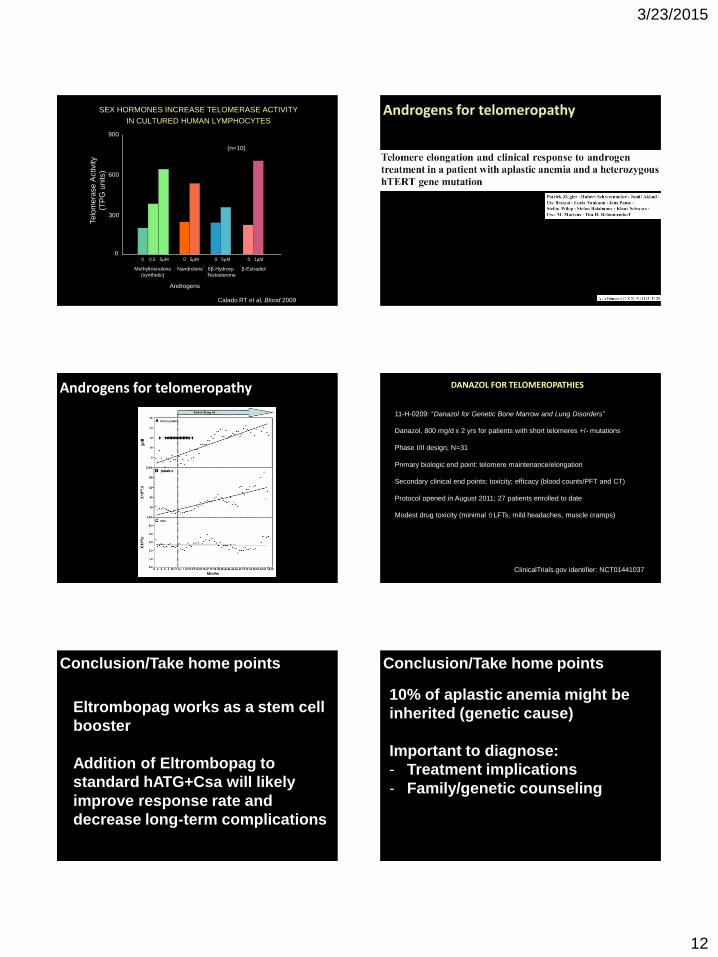
SEX HORMONES INCREASE TELOMERASE ACTIVITY
IN CULTURED HUMAN LYMPHOCYTES
(n=10)
900
600
Telo
mera
se A
ctivity
(TP
G u
nits)
Methyltrienolone
(synthetic)
300
0
Nandrolone 6β-Hydroxy-
Testosterone
β-Estradiol
0 0.5 5μM 0 5μM 0 5μM 0 1μM
Androgens
Calado RT et al, Blood 2009
Androgens for telomeropathy
Androgens for telomeropathy DANAZOL FOR TELOMEROPATHIES
11-H-0209: “Danazol for Genetic Bone Marrow and Lung Disorders”
Danazol, 800 mg/d x 2 yrs for patients with short telomeres +/- mutations
Phase I/II design, N=31
Primary biologic end point: telomere maintenance/elongation
Secondary clinical end points: toxicity; efficacy (blood counts/PFT and CT)
Protocol opened in August 2011; 27 patients enrolled to date
Modest drug toxicity (minimal LFTs, mild headaches, muscle cramps)
ClinicalTrials.gov identifier: NCT01441037
Conclusion/Take home points
Eltrombopag works as a stem cell
booster
Addition of Eltrombopag to
standard hATG+Csa will likely
improve response rate and
decrease long-term complications
Conclusion/Take home points
10% of aplastic anemia might be
inherited (genetic cause)
Important to diagnose:
- Treatment implications
- Family/genetic counseling
3/23/2015
13
Thank you!
NCT01623167“Eltrombopag with Standard Immunosuppression for Aplastic Anemia”
Indication: SAA
Exclusions: Prior Treatment (ATG, high dose cyclophosphamide, alemtuzumab),
Fanconi Anemia, liver cirrhosis
Inclusions:
• > 2yrs
• Bone marrow cellularity < 30%
• At least two of the following:
ANC < 500/microL
Platelets < 20,000/microL
ARC < 60,000/microL
Purpose: To improve hematologic response by adding eltrombopag (oral growth
factor) to standard immunosuppressive therapy
Type: Inpatient and Outpatient, Non-Randomized
Duration: 10-14 days inpatient for horse-ATG, CSA+ eltrombopag for 6 months, with 3
month, 6 month and annual follow-up visits
Severe Aplastic Anemia (SAA)Treatment-Naive
NCT00922883 “ A Pilot Study of a Thrombopoietin-receptor Agonist (TPO-R agonist),
Eltrombopag, in Aplastic Anemia Patients with Immunosuppressive-therapy Refractory
Thrombocytopenia”
Indication: SAA with refractory thrombocytopenia following at least one treatment course of
horse or rabbit ATG/cyclosporine.
Exclusions: Treatment with horse or rabbit ATG or Campath within 6 months of study entry,
Fanconi Anemia, liver cirrhosis, PNH clone size greater than 50%.
Inclusions:
• Diagnosis of aplastic anemia, with refractory thrombocytopenia following at least one
treatment course of horse or rabbit ATG/cyclosporine.
• Platelet count ≤ 30,000/mL
• Age ≥ 18 years old
Purpose: To improve platelet counts with eltrombopag (oral growth factor) in patients with
thrombocytopenia after immunosuppressive therapy
Type: Outpatient, Non-Randomized
Duration: 3 months of therapy. Monthly visits to NIH.
Severe Aplastic Anemia (SAA)Refractory
NCT01328587 “Eltrombopag for Moderate Aplastic Anemia”
Indication: MAA with thrombocytopenia or anemia.
Exclusions: Fanconi Anemia, liver cirrhosis, PNH clone size greater than 50%.
Inclusions: Current diagnosis of moderate aplastic anemia and
• Age ≥ 18 years old
• One or more of platelet count less than or equal to 30,000/microL, Hemoglobin less
than or equal to 8.5g/dl OR platelet and/or red cell transfusion dependent
Purpose: To improve platelet counts with eltrombopag (oral growth factor).
Type: Outpatient, Non-Randomized.
Duration: 4 months of therapy. Monthly visits to NIH.
Moderate Aplastic Anemia (MAA)
NCT00345345 “Alemtuzumab to Treat T-Large Granular Lymphocytosis”
Indication: T-LGL, Neutropenia, Anemia
Inclusions:
1. T-LGL clone detectable by peripheral blood flow cytometry and TCR gene
rearrangements
2. At least one cytopenia:
• ANC < 500/uL
• Platelets < 20 k/uL or < 50 k/uL with bleeding
• Hemoglobin < 9 g/dL or anemia requiring >2 units of RBCs/month transfusions
Purpose: To characterize response (improvement of blood counts) to immunosuppression
(Campath) in patients with T-LGL
Type: Inpatient and Outpatient, Non-Randomized
Duration: 11 days inpatient, with 3 month, 6 month and annual follow-up visits
T-cell Large Granular Lymphocytosis (T-LGL)
• A Pilot Study of a Thrombopoietin-Receptor Agonist, Eltrombopag, in Patients With Low to Int-2 Risk MDS
• NCT00961064
• Purpose of this study is to see if eltrombopag can increase platelet counts in patients with MDS
• Inclusion criteria:– Patients 18 years of age and older who have platelet count of less than 30
that has not responded to conventional treatment
• Outpatient study: – Treatment with eltrombopag once per day for 16 weeks
– Evaluations at NIH every 4 weeks
– If response, then follow up every 3 months
– If no response then follow up at 1 and 6 months off drug
Myelodysplastic syndrome (MDS)

3/23/2015
14
Clofarabine followed by high-dose lenalidomide for high risk MDS, CMMoland AML
NCT01629082
• PhaseI
• Single course of IV clofarabine (5mg/m2/d x5) for cytoreduction
• Oral lenalidomide consolidation with dose escalation from 25 mg daily for 21/28 days for 1 cycle in the first cohort up to 50 mg daily for 28/28 days for 2 cycles in the fourth cohort.
• Oral lenalidomide maintenance, starting at a dose of 10 mg daily in 28 day cycles, with dose adjustments, for up to 12 cycles.
• Inclusion criteria:
– MDS: Int-2 IPSS and higher
– CMMoL
– AML
– ECOG 0 to 2
– Unresponsive to, or unable to receive, DNA hypomethylating agents or standard intensive induction chemotherapy (i.e. “7+3” cytarabine/anthracycline chemotherapy)
• Outpatient study:
– Needs to stay locally for monthly revlimid prescription refills.
Myelodysplastic syndrome (MDS)