APHA 09.30.11 - MSPRS
1
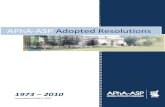
•Peer review - essential tool for evaluating and improving medical staff’s quality of care •Recent requirement by Joint Commission - Ongoing Professional Practice Evaluation A Medical Staff Peer Review System in a Public Teaching Hospital – An Internal Quality Improvement Tool Linda S Chan PhD, Manal Elabiad MS, Ling Zheng MD PhD, Brittany Wagman BS, Garren Low MS, Roger Chang, MA, Nicholas Testa MD, Stephanie L Hall MD Los Angeles County + University of Southern California Medical Center, Los Angeles, California CHALLENGES ENCOUNTERED RESULTS – MORTALITY PEER REVIEWS •Largest public teaching hospital in the west serving the indigent population •Licensed for 724 beds; transferred to its new state-of- the-art facilities in November 2008 •Trains about 1,500 medical professionals daily of which 870 are medical residents Technical Challenges •Lack of a electronic medical record •Lack of universal access to the hospital intranet .Procedural Challenges •Uneven distribution of peer review workload •Timeliness in processing peer reviews Cultural Challenges •Variable degree of acceptability and seriousness • The “punitive” nature deterred unbiased reviews Institutional Challenges •Inadequate staffing, inadequate funding for computer hardware and software •Poor medical records system •Slow implementation of corrective actions MEDICAL STAFF PEER REVIEW SYSTEM LESSONS LEARNED •Must have adequate staffing, adequate infrastructure, electronic medical records system, universal web entry, continuous in-service, monitoring and improvement •All clinical departments must support the process •The peer review instrument and process must be improved to reduce the variation and bias PURPOSE OF THE STUDY •Present the development, implementation, and management of an electronic Medical Staff Peer Review System (MS-PRS) as well as challenges encountered and lessons learned RESULTS – MEASURE OF POTENTIAL IMPACT LAC+USC MEDICAL CENTER Peer Review Levels and Bodies •1 st level: discharge department •2 nd level: Small Peer Review Committee (SPRC) •3 rd level: Executive Peer Review Committee (EPRC) Feedback and Reporting •Weekly operational reports •Quarterly summary trend reports •Letters to accountable providers and departments Confidentiality of Peer Reviews •Only accessible to quality improvement staff •All names are kept confidential through out review process Staffing •A full-time computer engineer •A half-time coordinator •A half-time programmer analyst. •Assistance from Quality INTRODUCTION DISCUSSION •Number of cases requiring improvement has decreased •Significant decrease in medical malpractice claim rate could be related only in part to MS-PRS •Direct impact of MS-PRS is difficult to measure as it is an integral part of the quality improvement effort of our institution •MS-PRS scored about 70% using a published self-evaluation tool (mean 45%, range: 0 to 86%) (Edwards MT. Peer Review: A New Tool for Quality Improvement. Physician Exec. 2009;25:54-59) RESULTS – IMPROVEMENTS TAKEN Opportunities for Improvement (OFI) 2007 2008 2009 2010 # mortalities reviewed # Had OFI (Level 1 review) 841 44 785 34 723 30 737 18 # OFI status not finalized # Had OFE (Status finalized) 0 12 2 14 3 5 5 1 Im provem entActions Taken,2007-2010 0 5 10 15 20 25 30 35 40 45 50 N um b er of Im provem entA cti Num berofM edicalM alpractice per 100,000 PatientE ncounters 0 20 40 60 80 100 120 N u m b er o f M edicalM alp ra ctices p e r 1 0
-
Upload
garren-low -
Category
Health & Medicine
-
view
51 -
download
1
Transcript of APHA 09.30.11 - MSPRS

•Peer review - essential tool for evaluating and improving medical staff’s quality of care •Recent requirement by Joint Commission - Ongoing Professional Practice Evaluation
A Medical Staff Peer Review System in a Public Teaching Hospital – An Internal Quality Improvement Tool
Linda S Chan PhD, Manal Elabiad MS, Ling Zheng MD PhD, Brittany Wagman BS, Garren Low MS, Roger Chang, MA, Nicholas Testa MD, Stephanie L Hall MD
Los Angeles County + University of Southern California Medical Center, Los Angeles, California
CHALLENGES ENCOUNTERED
RESULTS – MORTALITY PEER REVIEWS
•Largest public teaching hospital in the west serving the indigent population•Licensed for 724 beds; transferred to its new state-of-the-art facilities in November 2008 •Trains about 1,500 medical professionals daily of which 870 are medical residents
Technical Challenges•Lack of a electronic medical record •Lack of universal access to the hospital intranet .Procedural Challenges•Uneven distribution of peer review workload•Timeliness in processing peer reviewsCultural Challenges•Variable degree of acceptability and seriousness• The “punitive” nature deterred unbiased reviews Institutional Challenges•Inadequate staffing, inadequate funding for computer hardware and software •Poor medical records system•Slow implementation of corrective actions
MEDICAL STAFF PEER REVIEW SYSTEM
LESSONS LEARNED
•Must have adequate staffing, adequate infrastructure, electronic medical records system, universal web entry, continuous in-service, monitoring and improvement •All clinical departments must support the process•The peer review instrument and process must be improved to reduce the variation and bias•Culture of peer review must be changed from a punitive to a rewarding philosophy
PURPOSE OF THE STUDY
•Present the development, implementation, and management of an electronic Medical Staff Peer Review System (MS-PRS) as well as challenges encountered and lessons learned
RESULTS – MEASURE OF POTENTIAL IMPACT
LAC+USC MEDICAL CENTER
Peer Review Levels and Bodies•1st level: discharge department•2nd level: Small Peer Review Committee (SPRC)•3rd level: Executive Peer Review Committee (EPRC) Feedback and Reporting•Weekly operational reports•Quarterly summary trend reports•Letters to accountable providers and departmentsConfidentiality of Peer Reviews•Only accessible to quality improvement staff •All names are kept confidential through out review processStaffing•A full-time computer engineer•A half-time coordinator •A half-time programmer analyst. •Assistance from Quality Improvement Managers (QIM) and QI support as needed
INTRODUCTION DISCUSSION
•Number of cases requiring improvement has decreased•Significant decrease in medical malpractice claim rate could be related only in part to MS-PRS •Direct impact of MS-PRS is difficult to measure as it is an integral part of the quality improvement effort of our institution •MS-PRS scored about 70% using a published self-evaluation tool (mean 45%, range: 0 to 86%) (Edwards MT. Peer Review: A New Tool for Quality Improvement. Physician Exec. 2009;25:54-59)
RESULTS – IMPROVEMENTS TAKEN
Opportunities for Improvement (OFI)
2007 2008 2009 2010
# mortalities reviewed# Had OFI (Level 1 review)
84144
78534
72330
73718
# OFI status not finalized# Had OFE (Status finalized)
012
2 14
3 5
5 1
Improvement Actions Taken, 2007-2010
0
5
10
15
20
25
30
35
40
45
50
Nu
mb
er
of
Imp
rovem
en
t A
cti
on
s
Number of Medical Malpractice per 100,000 Patient Encounters
0
20
40
60
80
100
120
Nu
mb
er
of
Me
dic
al M
alp
rac
tic
es
pe
r 1
00
,00
0