APELLIS R&D DAY
137
APELLIS R&D DAY June 30, 2021 A N D T H E Y ’ R E O F F !
Transcript of APELLIS R&D DAY

APELLISR&D DAYJune 30, 2021
A N D T H E Y ’ R E O F F !

APELLISR&D DAY
A N D T H E Y ’ R E O F F ! Welcome!
Cedric Francois, M.D., Ph.D.
Chief Executive Officer
Apellis Pharmaceuticals
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

3
Statements in this presentation about future expectations, plans
and prospects, as well as any other statements regarding matters
that are not historical facts, may constitute “forward-looking
statements” within the meaning of The Private Securities Litigation
Reform Act of 1995. These statements include, but are not limited
to, statements relating to the implications of preliminary clinical
data. The words “anticipate,” “believe,” “continue,” “could,”
“estimate,” “expect,” “intend,” “may,” “plan,” “potential,” “predict,”
“project,” “should,” “target,” “will,” “would” and similar expressions
are intended to identify forward-looking statements, although not all
forward-looking statements contain these identifying words. Actual
results may differ materially from those indicated by such forward-
looking statements as a result of various important factors,
including: whether the company’s clinical trials will be fully enrolled
and completed when anticipated; whether preliminary or interim
results from a clinical trial will be predictive of the final results of the
trial; whether results obtained in preclinical studies and clinical
trials will be indicative of results that will be generated in future
clinical trials; whether pegcetacoplan will successfully advance
through the clinical trial process on a timely basis, or at all; whether
the results of the company’s clinical trials will warrant regulatory
submissions and whether pegcetacoplan will receive approval from
the FDA or equivalent foreign regulatory agencies for GA, PNH,
CAD, C3G, IC-MPGN, ALS or any other indication when expected
or at all; whether, if Apellis’ products receive approval, they will be
successfully distributed and marketed; and other factors discussed
in the “Risk Factors” section of Apellis’ Annual Report on Form 10-
K filed with the Securities and Exchange Commission on April 28,
2021 and the risks described in other filings that Apellis may make
with the Securities and Exchange Commission. Any forward-
looking statements contained in this press release speak only as of
the date hereof, and Apellis specifically disclaims any obligation to
update any forward-looking statement, whether as a result of new
information, future events or otherwise.
Forward-Looking Statements
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

4
Disclosures
B r u n o F a t t i z z o , M . D . Consultancy honoraria: Alexion, Amgen, Apellis, Momenta, and Novartis
A n g e l a G e n g e , M . D . Executive director CRU Montreal Neurological Institute and ALS center of Excellence
On Advisory boards of following companies: Alexion, Apellis, AL-S Pharma, ArgenX, Biogen, Amylyx,
Calico, UCB, Roche, Sanofi, Regeneron, UCB, MTPA
On DSMB:AZT therapeutics, Clene
Consulting CMO: Quralis
Chair Scientific Advisory Committee of CATALIS
N a n c y M . H o l e k am p , M . D .
Consultant: Allergan, Acucela, Apellis, Bayer, Lineage Cell Therapeutics, Clearside Biosciences,
Gemini, Genentech, Gyroscope, Katalyst Surgical, Nacuity, Notal Vision, Novartis, Polyactiva, Regeneron
• Speakers Bureau: Allergan, Genentech, Novartis, Regeneron, Spark
• Contracted Research: Genentech, Gemini, Gyroscope, Notal Vision
• Intellectual Property/Patent: Katalyst Surgical
M a t t hew P i c k e r i ng , P h . D . ,
M . B . , B . S .
Apellis Pharmaceuticals, Alexion Pharmaceuticals, Gemini Therapeutics, Gyroscope Therapeutics
I l e n e W e i t z , M . D . Honoraria, consultancy: Alexion, Apellis
Speakers bureau: Alexion
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

5
Disclosures
C h a r l e s W yk o f f , M . D . , P h . D . Consulting: Adverum, Aerie Pharmaceuticals, Allergan, Allgenesis, Apellis, Arctic Vision, Arrowhead
Pharmaceuticals, Bausch + Lomb, Bayer, Bionic Vision Technologies, Chengdu Kanghong
Biotechnologies (KHB), Clearside Biomedical, EyePoint Pharmaceuticals, Genentech, Gyroscope, IVERIC
Bio, Kato Pharmaceuticals, Kodiak Sciences, Long Bridge Medical, NGM Biopharmaceuticals, Novartis,
OccuRx, Ocular Therapeutix, ONL Therapeutics, Opthea Limited, Oxurion, Palatin, PolyPhotonix,
RecensMedical, Regeneron, RegenXBio, Roche, SAI MedPartners, Surrozen Takeda, Verana Health
Research: Adverum, Aerie Pharmaceuticals, Aldeyra, Alimera Sciences, Allergan, Amgen, Apellis, Asclepix,
Bayer, Boehringer Ingelheim, Chengdu Kanghong Biotechnology, Clearside Biomedical, Gemini,
Genentech, Graybug Vision, Gyroscope, IONIS Pharmaceutical, iRENIX, IVERIC bio, Kodiak Sciences,
LMRI, Neurotech Pharmaceuticals, NGM Biopharmaceuticals, Novartis, Oxurion, RecensMedical,
Regeneron, RegenXBio, Roche, SamChunDang Pharm, Taiwan Liposome Company, Xbrane BioPharma
Ownership/Stock: ONL Therapeutics, PolyPhotonix, RecensMedical, Visgenx
A p e l l i s / S o b i C o l l a b o ra t i on Sobi has global co-development and ex-U.S. commercialization rights for systemic pegcetacoplan
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

6
Growing Our Pipeline for Long-Term Leadership in Complement
Transforming Treatment
across Rare, Complement-
Driven Diseases Be #1 in the Retina
Building a Portfolio
of Brain-Active
Complement Therapies
APELLIS:
Global Leader
in Complement
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

7
• EMPAVELI™ (pegcetacoplan) launch off to strong start
• Platform potential for EMPAVELI with four new registrational programs
• New molecular entities in development to sustain long-term growth in existing and new indications
Global Leader in Complement, Today and Tomorrow
R A R E D I S E A S E
N E U R O L O G Y
O P H T H A L M O L O G Y
• Optimistic heading into DERBY and OAKS readout in September 2021
• Significant unmet need and blockbuster opportunity
• New molecular entities in development in GA, wet and intermediate AMD
• C3 plays a key role in a wide range of neurodegenerative conditions
• Apellis to pioneer targeted C3 therapies in neurodegeneration
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
APELLISR&D DAY
A N D T H E Y ’ R E O F F !
Transforming Treatment
across Rare, Complement-
Driven Diseases
Victoria Brown
Senior Vice President, Rare Disease Program Executive
Apellis Pharmaceuticals
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

9
Transforming Treatment Across Rare,
Complement-Driven Diseases
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

10
• Advance four additional
registrational programs
Expand Rare Disease
Portfolio
Transforming Treatment Across Rare, Complement-Driven
Diseases
• Ensure access for adults
with PNH
Establish EMPAVELI in PNH
• Launch Enable device
• Develop siRNA +
EMPAVELI
• Develop oral alternative
pathway inhibitor
Enhance Patient Experience
& New Indications
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

11
• Advance four additional
registrational programs
Expand Rare Disease
Portfolio
Transforming Treatment Across Rare, Complement-Driven
Diseases
• Ensure access for adults
with PNH
Establish EMPAVELI in PNH
• Launch Enable device
• Develop siRNA +
EMPAVELI
• Develop oral alternative
pathway inhibitor
Enhance Patient Experience
& New Indications
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

IC-MPGN
/ C3GPNH ALS HSCT-TMACAD
Paroxysmal Nocturnal
Hemoglobinuria (PNH)
David Acheson
Senior Vice President, North America Commercial
Apellis Pharmaceuticals
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
13
U.S. Launch Priorities Driving Strategic Activities
Ensure EMPAVELI commercial supply
Establish Apellis & the PNH unmet need
Ensure patient access and reimbursement
Leverage the clinical data to differentiate the brand
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
14
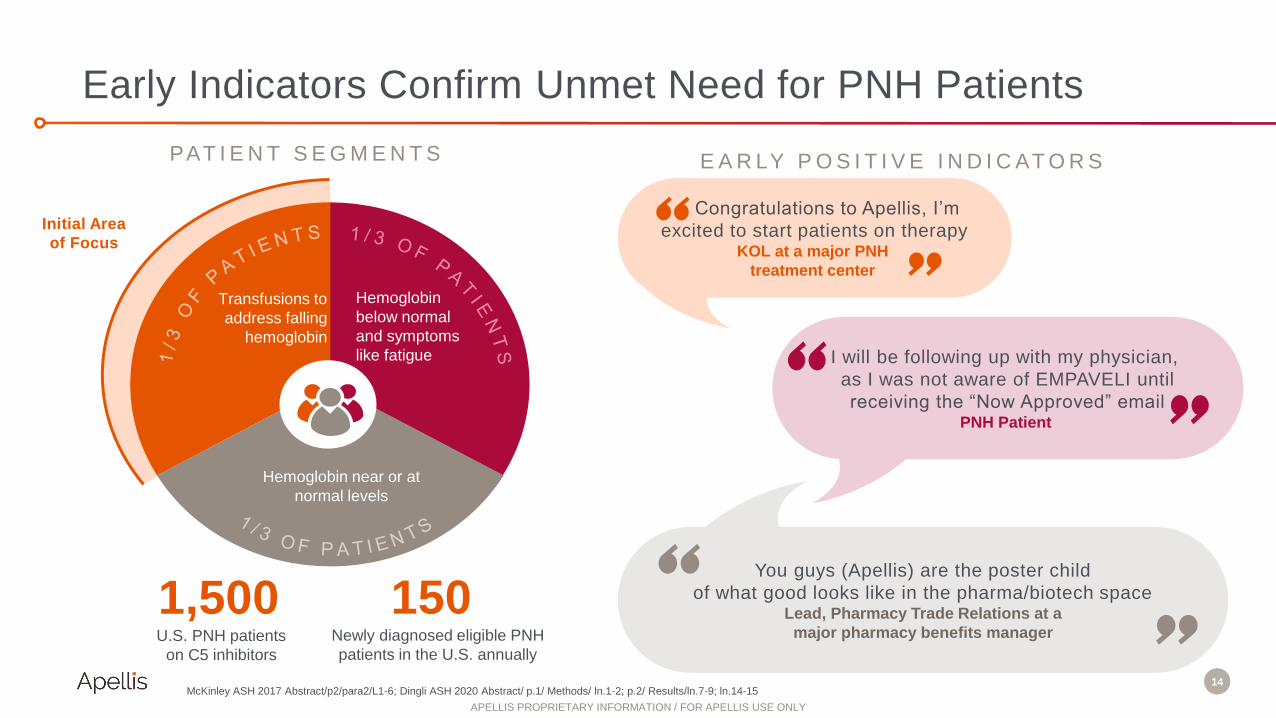
Early Indicators Confirm Unmet Need for PNH Patients
McKinley ASH 2017 Abstract/p2/para2/L1-6; Dingli ASH 2020 Abstract/ p.1/ Methods/ ln.1-2; p.2/ Results/ln.7-9; ln.14-15
14
E A R LY P O S I T I V E I N D I C AT O R SPAT I E N T S E G M E N T S
Congratulations to Apellis, I’m
excited to start patients on therapy KOL at a major PNH
treatment center
I will be following up with my physician,
as I was not aware of EMPAVELI until
receiving the “Now Approved” emailPNH Patient
You guys (Apellis) are the poster child
of what good looks like in the pharma/biotech spaceLead, Pharmacy Trade Relations at a
major pharmacy benefits manager
Hemoglobin near or at
normal levels
Transfusions to
address falling
hemoglobin
Hemoglobin
below normal
and symptoms
like fatigue
Initial Area
of Focus
U.S. PNH patients
on C5 inhibitors
1,500Newly diagnosed eligible PNH
patients in the U.S. annually
150
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
15
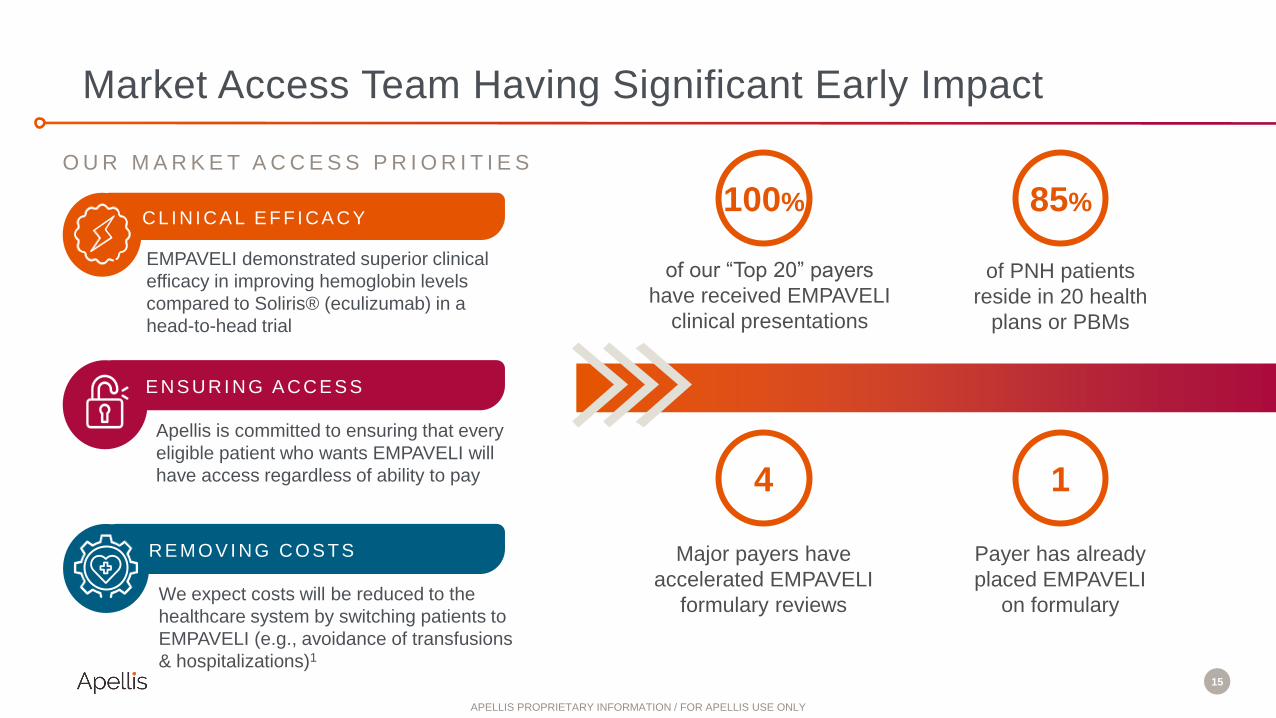
Market Access Team Having Significant Early Impact
15
O U R M A R K E T A C C E S S P R I O R I T I E S
EMPAVELI demonstrated superior clinical
efficacy in improving hemoglobin levels
compared to Soliris® (eculizumab) in a
head-to-head trial
We expect costs will be reduced to the
healthcare system by switching patients to
EMPAVELI (e.g., avoidance of transfusions
& hospitalizations)1
Apellis is committed to ensuring that every
eligible patient who wants EMPAVELI will
have access regardless of ability to pay
E NS URI NG A CCE S S
C L I N I C A L E F F I C A C Y
R E M O V I N G C O S T S
of our “Top 20” payers
have received EMPAVELI
clinical presentations
of PNH patients
reside in 20 health
plans or PBMs
Major payers have
accelerated EMPAVELI
formulary reviews
4
85%100%
Payer has already
placed EMPAVELI
on formulary
1
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

16
Patient Journey & Early Lead Indicators
25%
50%
25%
EMPAVELI-Treated Patients
by Payer Segment
Early Launch Days from
Prescription to First Dose
Physician Enrollment in REMS
Since Launch
7-10 >50
MEDICAID MEDICARE
COMMERCIAL
Have had RXs from all three payer channels
submitted & approved
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

17
Great Start for EMPAVELI Launch
17
Product in channel within 5 days
90% of top payers have received clinical
presentations
Sales organization live meetings have
increased to 38% from 8% post-PDUFA
>50 physicians have enrolled in REMS
90% of payer formulary reviews to be
complete
Engage 100% of priority accounts via
Apellis sales organization
T O D A Y Q 4 2 0 2 1
Engage 85% of priority physicians via
Apellis sales organization
Maintain & enhance high patient
confidence score for self-infusion within
2 weeks on therapy
ApellisAssist early operational
effectiveness is rated high by patients
O R G A N I Z A T I O N F O C U S I S O N 2 K H C P S & 9 0 T A R G E T E D T R E A T M E N T C E N T E R S
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

Q&A with Dr. Ilene Weitz
Ilene Weitz, M.D.
Hematology Specialist, Professor of Clinical
Medicine
Keck School of Medicine at the University of
Southern California
Monica Fay
Senior Vice President, Medical Affairs
Apellis Pharmaceuticals
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

19
• Advance four additional
registrational programs
Expand Rare Disease
Portfolio
Transforming Treatment Across Rare, Complement-Driven
Diseases
• Ensure access for adults
with PNH
Establish EMPAVELI in PNH
• Launch Enable device
• Develop siRNA +
EMPAVELI
• Develop oral alternative
pathway inhibitor
Enhance Patient Experience
& New Indications
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

IC-MPGN
/ C3GPNH HSCT-TMACAD
Immune Complex Membranoproliferative
Glomerulonephritis (IC-MPGN) /
C3 Glomerulopathy (C3G)
ALS
Matthew Pickering, Ph.D., M.B., B.S.
Professor of Rheumatology and Wellcome Trust Senior Fellow in Clinical Science
Imperial College London via Imperial Consultants
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

21
IC-MPGN and C3G are Rare, Chronic, Complement-Mediated
Glomerular Diseases Resulting in Kidney Damage and Failure
• MPGN pattern of injury
• Complement alternative and
classical pathway implicated
• Immunoglobulin deposition
dominant or co-dominant
with C3
• Complement alternative pathway
implicated
• C3-dominant glomerular deposits
• Two subtypes
– DDD
– C3GN
• Similar clinical presentation, features, and disease course
• Heterogenous disease pathology (i.e., genetic or acquired)
M P G N C 3 G L O M E R U L O PAT H Y
C3 & immunoglobulin
depositionDominant C3 deposition
Overlap of MPGN and C3 Glomerulopathy
Dense
deposit
disease
FHR5
nephropathy
Adapted from: JASN January 2018, 29 (1) 9-1
C3GN
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

22
Key Clinical Signs and Symptoms
• Proteinuria and/or hematuria
• Low serum C3
• Decreased GFR
• High blood pressure
Key Pathological Findings
• Positive C3 staining
– C3G and IC-MPGN
• IC-MPGN also has Ig deposition
No Disease-Modifying Treatments
No Approved Treatments for IC-MPGN or C3G
Illustrative. Adapted from Kidney International (2014) 85, 450–456
C3
IgG
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

23
• ~18,000 patients in US and EU with primary C3G or
IC-MPGN
• ~50% of patients progress to ESRD in 5-10 years and
require chronic dialysis or transplant
• Kidney transplantation is not curative. Disease
recurrence has been reported in as many as 85%
transplanted patients
• Proteinuria is an important marker of renal
damage and the key clinical marker, along with GFR,
used by clinicians to measure progression of the
disease
IC-MPGN and C3G Represent Areas of High Unmet Need
Garam et al. Clin Kidney J. 2020
C3GN
DDD
IC-MPGN
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

24
IC-MPGN/C3G Interferes with Life Physically and Emotionally
“Physically, I gained weight in the beginning because of this
disease.”
“With C3G being such a rare disease, I am often faced with
new challenges that do not have solutions.”
“Mentally, the medication that I was taking made it hard
for me to focus.”
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

25
EMPAVELI Targets C3 for Comprehensive Control of
IC-MPGN and C3G
C3
Alternative
Pathway
Classical
Pathway
Lectin
Pathway
C3a Structural damage to kidney
MAC
C3b
C5a C5b
C5
STOP STOP
STOP STOP
E M PAV E L I
Inflammation
Inflammation
Co
ntro
ls a
ll do
wn
stre
am
effe
cts
Structural damage to kidney
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

26
Phase 2 DISCOVERY Design and Study Goals
C3G, C3 glomerulopathy; CKD-EPI, Chronic Kidney Disease Epidemiology Collaboration; eGFR, estimated glomerular filtration rate; Q2W, every 2 weeks; QD, once daily; TEAE,
treatment-emergent adverse event; uPCR, urine protein to creatinine ratio.
1. Levey et al. Ann Intern Med. 2009;150:604-612.
48 weeks
EMPAVELI 360 mg QD SCTransition to 1080 mg Q2W ≥week 24N=8 C3G patients
Primary
endpoint
readoutScreening
4 weeks 24 weeks
Long-term
extension
APL2-201; NCT03453619
Population: Biopsy-confirmed adult
or adolescent patients with C3G or
biopsy-confirmed adult patients with
IgAN, LN, or primary MN
Primary endpoint: Change from
baseline in proteinuria as quantified
by uPCR
Secondary endpoints include:
Change in estimated glomerular
filtration rate and serum complement
markers, including C3
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

27
EMPAVELI Demonstrated 73% Reduction in Mean Proteinuria
as Measured by 24h uPCR at Week 48 in DISCOVERY
Treatment with EMPAVELI resulted in proteinuria reduction at week 48
Figure error bars represent standard error. Five patients were included at each time point.
CFB, change from baseline; uPCR, urine protein to creatinine ratio. A Normal ranges for each parameter: first morning uPCR, <0.200 mg/mg, serum albumin, 3.5 -5.50 g/dL; B Baseline was the most recent result before the first dose.C eGFR was calculated using the CKD-EPI creatinine equation
Parameter, mean (SE), [range]a
Baselineb
(N=5)
Week 48
(N=5)
24-hour uPCR, mg/mg 3.48 (0.82)
[1.74, 6.55]
0.93 (0.27)
[0.34, 1.69]
Percentage CFB in 24-hour
uPCR
NA -67.73 (10.50)
[-94.12, -37.31]
Serum albumin, g/dL 3.50 (0.30)
[2.40, 4.10]
4.08 (0.24)
[3.30, 4.60]
eGFRc, mL/min/1.73 m2 88.00 (22.61)
[29.00, 138.00]
86.60 (20.44)
[41.00, 142.00]
Decreased uPCR, increased serum albumin, and
stable renal function were observed at week 48
-100
-80
-60
-40
-20
0
0 48
Cha
nge
fro
m b
ase
line
in m
ea
n 2
4-h
ou
r u
PC
R, %
Week
Patient 1
Patient 2
Patient 3
Patient 4
Patient 9
Mean
APL2-201; NCT03453619
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

28
Phase 2 DISCOVERY Study: EMPAVELI Targets Underlying
Disease Process of C3G
Serum C3 levels increased after initiation of EMPAVELI
Graphed error bars represent standard error. Normal ranges are indicated by shading: serum C3, 90 -180 mg/dL
a Normal ranges for each of the biomarkers: serum C3, 0.94 -1.66 mg/mL; CH50, 176-382 U/mL; AH50, 77-159 U/mL. b Baseline was the most recent result before the
first dose.
Biomarker, mean (SD), [range]a Baselineb Week 48
Serum C3, mg/mL 61.60 (20.42)
[11.00, 116.00]
252.00 (52.82)
[82.00, 407.00]
Serum C4, mg/dL 19.20 (4.22)
[5.00, 31.00]
17.75 (2.17)
[14.00, 22.00]
CH50, U/mL 183.40 (53.17)
[23.00, 298.00]
214.00 (12.52)
[190.00, 248.00]
AH50, U/mL 62.00 (25.59)
[0.00, 113.00]
60.75 (22.40)
[0.00, 96.00]
Levels of key complement biomarkers increased from baseline to week 48
0
100
200
300
400
500
-4 0 4 8 12 16 20 24 28 32 36 40 44 48
Se
rum
C3
, m
g/d
L
Week
APL2-201; NCT03453619
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

29
EMPAVELI Safety Profile in C3G Cohort of DISCOVERY
There were no discontinuations due to treatment emergent adverse events
(TEAEs) and no serious or severe adverse events
The majority of TEAEs were considered unrelated to study drug
APL2-201; NCT03453619
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
30
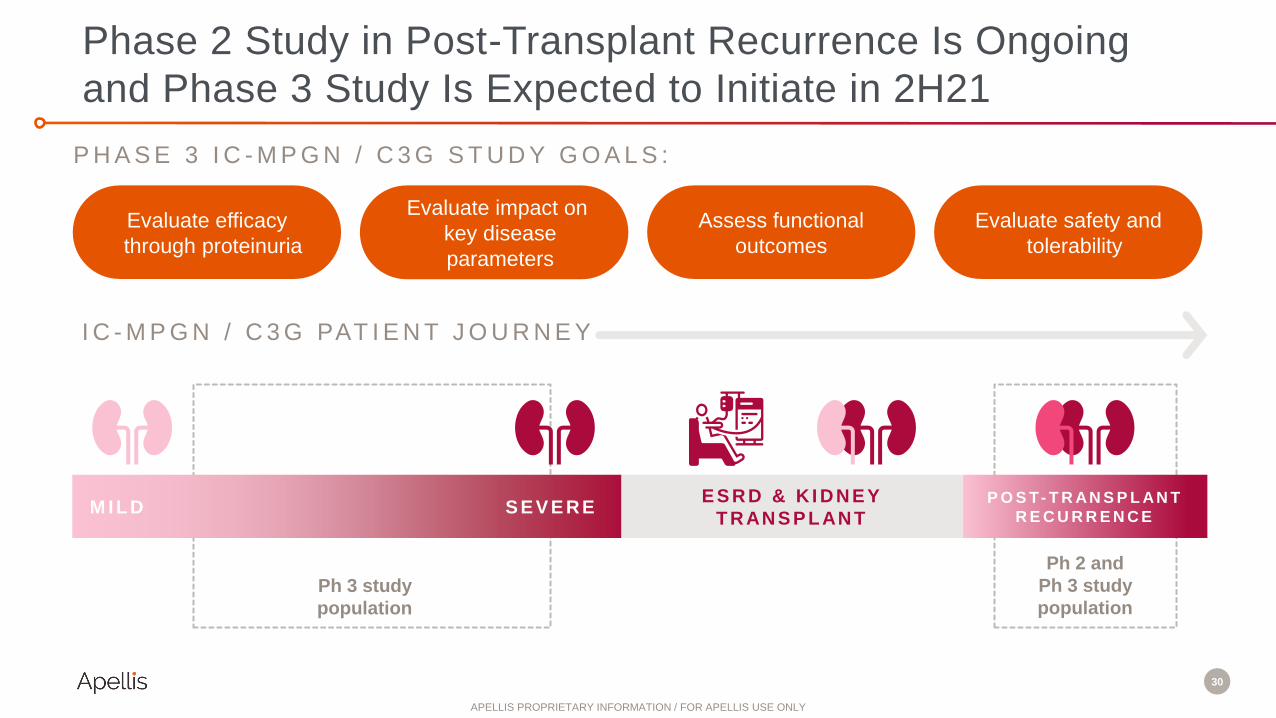
Phase 2 Study in Post-Transplant Recurrence Is Ongoing
and Phase 3 Study Is Expected to Initiate in 2H21
I C - M P G N / C 3 G PAT I E N T J O U R N E Y
S E V E R EP O S T- T R AN S P L AN T
R E C U R R E N C E
Ph 3 study
population
Ph 2 and
Ph 3 study
population
E S R D & K I D N E Y
T R AN S P L AN T
P H A S E 3 I C - M P G N / C 3 G S T U D Y G O A L S :
Assess functional
outcomes
Evaluate impact on
key disease
parameters
Evaluate efficacy
through proteinuria
Evaluate safety and
tolerability
M I L D
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

31
Key Takeaways
IC-MPGN and C3G are rare, chronic, complement-mediated diseases resulting in
kidney damage and failure with no approved therapies
Excessive deposition of C3 breakdown products in the kidney is the primary driver of
kidney damage in patients with IC-MPGN and C3G
EMPAVELI achieved proof of concept in C3G by demonstrating a 73% reduction in
mean proteinuria at 48 weeks
Phase 2 study ongoing; Phase 3 expected to initiate in 2H21
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

IC-MPGN
/ C3GPNH ALS HSCT-TMACAD
Amyotrophic Lateral
Sclerosis (ALS)
Angela Genge, M.D., FRCP(C)
Executive Director, Clinical Research Unit & Director of ALS Center of Excellence
Montreal Neurological Institute
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

33
2/3 initially present with muscle weakness of the limbs2
1/3 initially present with difficulty with speech and swallowing2
1 Brown RH and Al-Chalabi A. N Engl J Med 2017; 377:162-72. Arthur KC, et al. Nat Commun 2015 Aug 11;7:12408. Brown RH and Al-Chalabi A. N Engl J Med 2017;377:162-72
Significant Unmet Need for People Living with ALS
ALS is a fatal neurodegenerative disorder, characterized by
progressive loss of upper and lower motor neurons1
Currently, no treatment targets the neuroinflammation
caused by an overactive immune response
ALS affects 225,000 people globally. ~90% of cases are
sporadic and death typically occurs 3-5 years from
disease onset1,2
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

34
Extensive evidence suggests that complement activation plays a role in disease progression:
• Disease progression is correlated with elevated C3
• Complement C3 is elevated in the serum, brain, and spinal cord compared to nonaffected controls
• Individuals with ALS have high levels of activated C3 at the neuromuscular junction where neurons communicate directly to muscle cells
Kjældgaard AL, Pilely K, Olsen KS, et al. J Inflamm Res. 2021;14:1043-1053; Sta M, et al. Neurobiol Dis. 2011;42(3):211-220; Goldknopf IL, et al. Biochem Biophys Res Commun. 2006;342(4):1034-1039;
Ganesalingam J, et al. J Neurochem. 2011;117(3):528-537’ El Idrissi NB, et al. J Neuroinflamm. 2016;13(1):72.
Complement-Mediated Neuroinflammation Is a Key Driver of
Neurodegeneration
Brain
Spinal Cord
N E U R O M U S C U L A R S Y S T E M
Peripheral nerves
NMJ
Terminal
Schwann Cell
Muscle
C3
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

35El Idrissi N, et al. J Neuroinflammation. 2016;13(1):72
Complement C3 and its Breakdown Products Are Deposited at
the Neuromuscular Junctions of People with ALS
Control ALS
Motor Nerve Terminal Motor nerve terminal + C3/C3b
Terminal Schwann Cell
Terminal Schwann Cell + C3/C3b
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

36
EMPAVELI Targets C3 to Slow Disease Progression in ALS
C3
Alternative
Pathway
Classical
Pathway
Lectin
Pathway
C3a Neurodegeneration
MAC
C3b
C5a C5b
C5
STOP STOP
STOP STOP
Co
ntro
ls a
ll do
wn
stre
am
effe
cts
E M PAV E L I
Neuroinflammation
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
37
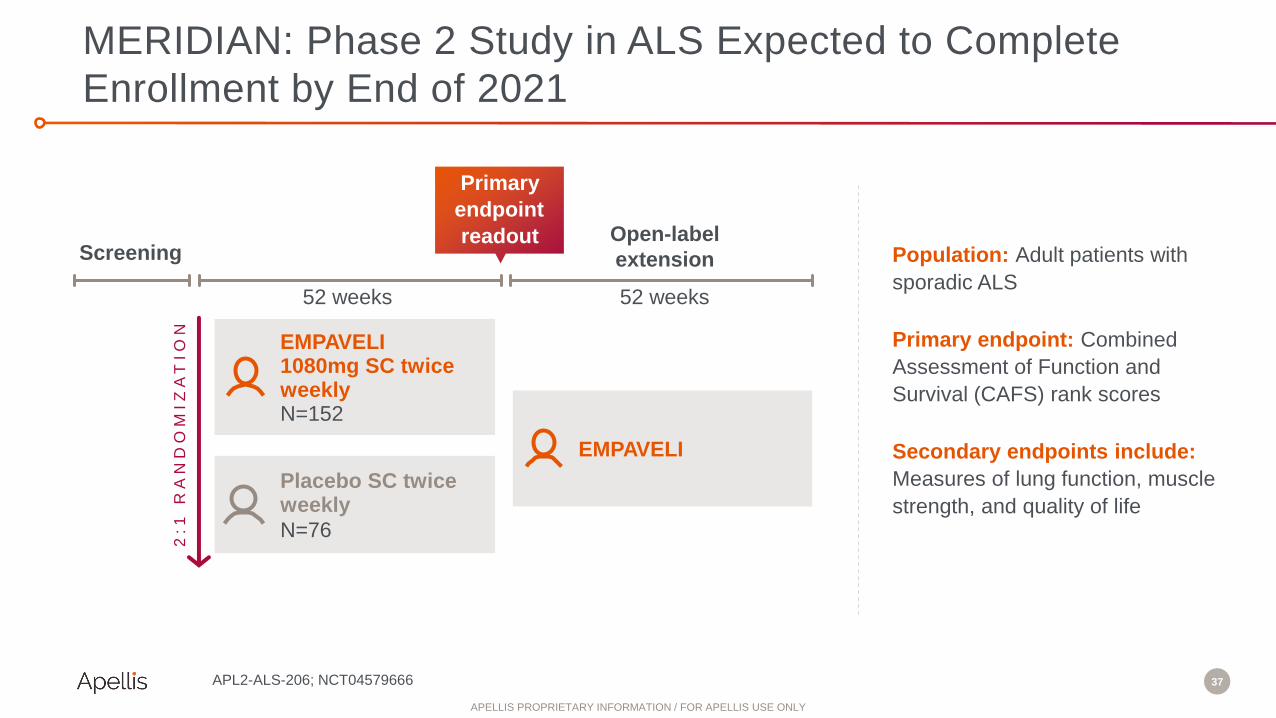
MERIDIAN: Phase 2 Study in ALS Expected to Complete
Enrollment by End of 2021
EMPAVELI1080mg SC twice weekly N=152
Primary
endpoint
readoutScreening
52 weeks
Open-label
extension
Placebo SC twice weekly
N=76
2:1
R
AN
DO
MIZ
AT
IO
N
52 weeks
EMPAVELI
APL2-ALS-206; NCT04579666
Population: Adult patients with
sporadic ALS
Primary endpoint: Combined
Assessment of Function and
Survival (CAFS) rank scores
Secondary endpoints include:
Measures of lung function, muscle
strength, and quality of life
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

38
Key Takeaways
Urgent and significant need for treatments for ALS, a fatal neurodegenerative disorder
Evidence suggests complement activation and elevated levels of C3 play a role in
disease progression
Controlling complement activation centrally at C3 with EMPAVELI may have the
potential to slow the progression of ALS
Phase 2 enrollment completion expected by the end of 2021
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
IC-MPGN
/ C3GPNH HSCT-TMACAD
Cold Agglutinin Disease
(CAD)
Bruno Fattizzo, M.D.
Professor, Consultant Hematologist and Clinical Researcher
Fondazione IRCCS Ca' Granda Policlinico Hospital, Milan, Italy
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
40
D I S E A S E B A C K G R O U N D :
• Chronic and severe red blood disorder
• Exacerbation of the condition in a cold environment
• Primarily affects older adults (age 50+)
• Symptoms include
– Hemolytic anemia and fatigue
– Transfusion requirements
– Cold-induced circulatory symptoms
– Increased risk of thrombotic events like stroke or heart attack
Cold Agglutinin Disease (CAD) Is a Chronic and Severe
Blood Disorder with No Approved Therapies
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

41
Phase 2 PLAUDIT Study Design
48 weeks
Randomized 1:1
EMPAVELI Daily 360mg QD SC
N=6
EMPAVELI Daily 270mg QD SCN=7
Primary
endpoint
readoutScreening
All
subjects
RA
ND
OM
IZ
AT
IO
N
APL2-CP-AIHA-208; NCT03226678
Population: CAD patients with
hemoglobin (Hb) levels <11 g/dL,
signs of hemolysis, and positive
direct antiglobulin test (DAT) for IgG
and/or complement C3
Primary endpoints:
• Safety
• Change in hematologic and blood
chemistry parameters and FACIT
PLAUDIT study also includes a parallel cohort of patients with warm antibody autoimmune hemolytic anemia (wAIHA)
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

42
PLAUDIT: Efficacy and Safety Results Support Further
Clinical Development of EMPAVELI in CAD
EMPAVELI Increased Hemoglobin within the First Weeks of
Treatment with Sustained Benefit with Longer Exposure
168 days of treatment
Hemoglobin (g/dL)
Additional Efficacy Outcomes
• 77% (n=10) patients were transfusion free at month 12
• FACIT score increased by 7.7 points from baseline to
week 24
Safety Profile Was Generally Consistent with Other
Studies
• All 13 CAD subjects experienced ≥1 treatment-emergent
adverse event (TEAE), mainly mild to moderate in severity
• Five subjects reported 13 serious adverse events (SAEs)
unrelated to EMPAVELI
• EMPAVELI was generally well tolerated
*FACIT- Clinically significant increase is 3 or more points
APL2-CP-AIHA-208; NCT03226678
CSR 11.4.1.1.2 PRBC Transfusions; CSR Table 21: Summary of FACIT-Fatigue Total Score by Visit—ITT Set; Fattizzo B, et al. European Hematology Association. June 13-16, 2019.
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

43
Key Takeaways
CAD is a chronic and severe blood disorder with no approved therapies
EMPAVELI may be able to control hemolysis in CAD by controlling complement
EMPAVELI demonstrated meaningful efficacy results across multiple hematologic
parameters and was well tolerated in PLAUDIT study
Sobi expects to initiate a Phase 3 study in H2 2021
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

IC-MPGN
/ C3GPNH HSCT-TMACAD
Hematopoietic Stem Cell Transplant
Thrombotic Microangiopathy (HSCT-TMA)
Bruno Fattizzo, M.D.
Professor, Consultant Hematologist and Clinical Researcher
Fondazione IRCCS Ca' Granda Policlinico Hospital, Milan, Italy
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

45
• Multi-system disease characterized by microangiopathic
hemolytic anemia, consumptive thrombocytopenia and
microvascular thrombosis
• Patients who develop organ damage as a result of
HSCT-TMA are associated with high mortality rates
• C3 is believed to play a critical role in TMA based on
proinflammatory and procoagulant properties of C3a and
C3b
• sC5b9 is a high-risk feature of HSCT-TMA
C3 Plays a Critical Role in HSCT-TMA, a Multi-System
Disease
Khosla , Hematopoietic stem cell transplant-associated thrombotic microangiopathy: current paradigm and novel therapies, Bone Marrow Transplantation 2018; The EBMT handbook
2019; Moiseev, Clinical and morphological practices in the diagnosis of transplant associated microangiopathy: a study on behalf of Transpla nt Complications Working Party of the EBMT,
Bone Marrow Transplantation 2018
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

46
• ~9,000 and ~18,000 allogeneic transplants
conducted in U.S. and EU+ annually.1,2
• TMA incidence can be up to ~40% of allogenic
transplants3
• ~50% of HSCT-TMA cases can be severe3
• ~90% or more of severe HSCT-TMA is fatal3
1. Current Uses and Outcomes of Hematopoietic Cell Transplantation (HCT): CIBMTR Summary Slide; 2. Passweg et al, BMT. 2019, 38: 1575–1585; 3. Jodele et al, Blood. 2014,
124(4): 645–653
HSCT-TMA Is Associated with Very Poor Outcomes
He
ma
tolo
gy
HSCT without TMA
HSCT-TMA
HSCT without TMA:
Median survival 79.7 months
HSCT with TMA (HSCT-TMA):
Median survival 5.8 months
Kraft S, et al. Bone Marrow Transplant. 2019, 54, 540–548
1.0
0.8
0.6
0.4
0.2
0
Ove
rall
su
rviv
al
0 12 24 36 48 60 72 84 96 108
Follow-up (months)
P=9.82E-16
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

47
Endothelial Damage
Amplification Loop
Loss of Control & Detrimental Effects
Extremely High Levels of Complement Activation Post-Transplant
Leads to Severe Complement Dysregulation in HSCT-TMA
C3
Alternative
Pathway
Classical
Pathway
Lectin
Pathway
C3a
MAC
C3b
C5a C5b
C5
Blood Clots/Organ DamageInflammation
Blood Clots/Organ DamageInflammation
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

48
EMPAVELI Targets C3 to Control Complement Activation in
HSCT-TMA
C3
Alternative
Pathway
Classical
Pathway
Lectin
Pathway
C3a
MAC
C3b
C5a C5b
C5
STOP STOP
STOP STOP
Co
ntro
ls a
ll do
wn
stre
am
effe
cts
E M PAV E L I
Blood Clots/Organ DamageInflammation
Blood Clots/Organ DamageInflammation
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
49
Key Takeaways
HSCT-TMA is a multi-system disease associated with high mortality rates
EMPAVELI has the potential to control the extremely high levels of complement
activation associated with HSCT-TMA
Sobi expects to initiate a potentially registrational Phase 2 study in H2 2021
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

50
EMPAVELI: Comprehensive Control of Complement with
Broad Platform Potential
IC -MPGN
/ C3G
ALS CAD HSCT-TMA
First patient dosed
in Phase 3 study in
2H21 (Apellis)
Complete
enrollment by end
of 2021 (Apellis)Initiate Phase 3 trial
in 2H21 (Sobi)
Initiate potentially
registrational Phase
2 study in 2H21
(Sobi)
Protect organ
function and prevent
mortality
Increase survival
and slow the
progression of
symptoms
Best-in-class therapy
for late-stage and
transplant patients
Improve hemoglobin
levels and reduce
transfusion
dependency
PNH
~1,500*
The new
standard
of care
~5,000** ~5,000** ~4,000****~19,000***
*Based on complement-treated patient population
**Based on severe patient population
***Based on sporadic only, patients seeking treatment, and non-monotherapy patients
****Based on high-risk patients for developing TMA
Sobi has global co-development and ex-U.S. commercialization rights for systemic
pegcetacoplan
PNH: Hill A, et al. Blood. 2006; 108(11):985. CAD: Catenion using physician and literature consensus. TMA:
Current Uses and Outcomes of Hematopoietic Cell Transplantation (HCT): CIBMTR Summary Slides.Passweg
et al, BMT. 2019, 38: 1575–1585 . Jodele et al, Blood. 2014, 124(4): 645–653. C3G: ClearView Analysis using
physician and literature consensus. ALS: ClearView Analysis based on physician interviews
EMPAVELI
Ambition
U.S. launch is
ongoingKEY
UPCOMING
MILESTONES
U.S. PATIENTS
NEEDING
TREATMENT
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
51
• Advance four additional
registrational programs
Expand Rare Disease
Portfolio
Transforming Treatment Across Rare, Complement-Driven
Diseases
• Ensure access for adults
with PNH
Establish EMPAVELI in PNH
• Launch Enable device
• Develop siRNA +
EMPAVELI
• Develop oral alternative
pathway inhibitor
Enhance Patient Experience
& New Indications
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

Launch Enable Device
Victoria Brown
Senior Vice President, Rare Disease Program Executive
Apellis Pharmaceuticals
• Launch Enable device
• Develop siRNA +
EMPAVELI
• Develop oral alternative
pathway inhibitor
Enhance Patient Experience
& New Indications
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

53
Advancing Patient-Centered Device Innovation for 2022
Source: Consultant analysis of PNH focus groups unique
PAT I E N T S R E S P O N D E D P O S I T I V E LY T O A N E X T - G E N E R AT I O N D E V I C E :
Administers with a few simple steps
Allows discreet self-administration
Alleviates needle fear
Increases mobility and independence
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
Develop siRNA + EMPAVELI
for Less-Frequent Dosing
Lukas Scheibler, Ph.D.
Chief Innovation Officer
Apellis Pharmaceuticals
• Launch Enable device
• Develop siRNA +
EMPAVELI
• Develop oral alternative
pathway inhibitor
Enhance Patient Experience
& New Indications
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

55
C3
Receptor-mediated
endocytosis
RISC
loadingPassenger
strand
degradation
C3 mRNA target
recognition
AGO2 cleavage
of C3 mRNA
Ribosome/
tRNA protein
synthesis
Endosomal
escape
Receptor
recycling
Endosomal
trafficking
• EMPAVELI dose and posology is driven
by high C3 concentration in blood
• Silencing C3 expression in the liver with
siRNA reduces circulating C3
concentration
• GalNAc-conjugated siRNAs have been
shown to target the liver and are
approved in variety of indications
– Patisiran, givosiran, inclisiran are
approved
– 19 GalNAc-siRNA development
programs exist
Silencing C3 Expression Could Reduce EMPAVELI Posology
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

56
Apellis siRNA Silenced 90% of C3
3 mg/kg 10 mg/kg 30 mg/kg
mRNA Day 15 KD 89% 97% 99%
Protein max KD 77% 85% 94%
15 46 79 113 156 1900.0
0.5
1.0
1.5
2.0
Days post-dose
NHP Liver Biopsy C3 mRNA
0 50 100 150 2000
50
100
150
Days post-dose
NHP Serum C3 Protein to Day 172
Vehicle 3 mg/kg 10 mg/kg 30 mg/kg
Rela
tive
C3 g
en
e e
xp
res
sio
n
Vehicle 3 mg/kg 10 mg/kg 30 mg/kg
C3 %
of
ba
se
lin
e
0 – 10%
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

57
Complement Targets Require Silencing & Inhibition
C5 siRNA in monotherapy
does not control PNH in
Phase 1 study
• “Maximal reductions in LDH, an
exploratory objective, of 37-50%
were observed in eculizumab-
naïve patients, and LDH levels
remained above the goal of
<1.5xULN.” – Badri et al 2020
• “... residual levels of C5 … were
sufficient to cause intravascular
hemolysis.” - Harris et al 2018
C5 siRNA in combination with eculizumab controls PNH with less-frequent dosing in Phase
1 study
• “All patients receiving cemdisiranachieved LDH <1.5xULN on reduced doses and/or frequency of eculizumab.” – Badri et al 2020
siRNA enables less frequent dosing:
• “In combination with Cemdisiran, the total cumulative yearly maintenance dose of eculizumab can potentially be reduced to approximately 70%.” – Badri et al 2020
Single dose ALN-CC5 reduced classical pathway
hemolytic activity by 65-70% to day 71 in nonhuman
primates. – Badri et al 2020; Kusner et al 2019
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

58
Apellis siRNA + EMPAVELI: Improving Treatment Experience
with Less-Frequent Dosing
Silencing C3 expression in the liver may reduce treatment frequency of EMPAVELI
Apellis siRNA silenced C3 expression >90% over 3+ months in NHP and significantly
reduced complement activity
IND for siRNA program anticipated in 2022
Results support potential to reduce dosing frequency of EMPAVELI
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

Oral Alternative Pathway
Inhibitor
Lukas Scheibler, Ph.D.
Chief Innovation Officer
Apellis Pharmaceuticals
• Launch Enable device
• Develop siRNA +
EMPAVELI
• Develop oral alternative
pathway inhibitor
Enhance Patient Experience
& New Indications
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
60
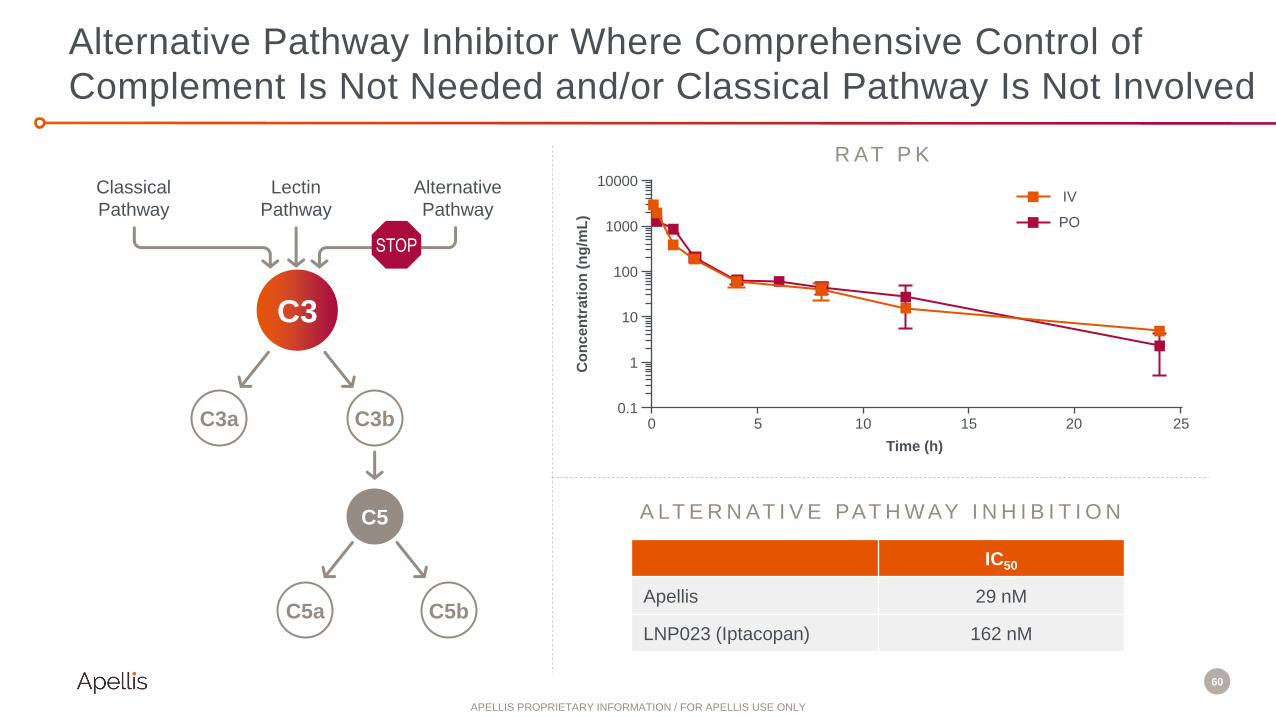
Alternative Pathway Inhibitor Where Comprehensive Control of
Complement Is Not Needed and/or Classical Pathway Is Not Involved
R AT P K
A LT E R N AT I V E PAT H W AY I N H I B I T I O N
IC50
Apellis 29 nM
LNP023 (Iptacopan) 162 nM
C3
Alternative
Pathway
Classical
Pathway
Lectin
Pathway
C3a C3b
C5a C5b
C5
10000
1000
100
10
1
0.1
Co
nc
en
tra
tio
n (
ng
/mL
)
Time (h)
0 5 10 15 20 25
IV
PO
STOP
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

61
Oral Alternative Pathway Inhibitor for Indications Where
Comprehensive Control of Complement Is Not Needed
C 3 G
S E V E R EP O S T- T R AN S P L AN T
R E C U R R E N C E
EMPAVELI
targetEMPAVELI
target
E S R D & K I D N E Y
T R AN S P L AN TM I L D
Oral
alternative
pathway
inhibitor
target
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

62
Transforming Treatment Across Rare,
Complement-Driven Diseases
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

APELLISR&D DAY
A N D T H E Y ’ R E O F F ! Rare Disease Q&A
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

APELLISR&D DAY
A N D T H E Y ’ R E O F F ! Lunch Break
Boxed lunches are in the lobby. The presentation
will resume in 20 minutes.
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
APELLISR&D DAY
A N D T H E Y ’ R E O F F !
Building a Portfolio of
Brain-Active
Complement Therapies
Lukas Scheibler, Ph.D.
Chief Innovation Officer
Apellis Pharmaceuticals
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
66
The Retina as a Window to the Brain
Picture: discoveryeye.org
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

67
C3 Therapy for Neurodegeneration Is an Extension of the
Neuroprotective Effects of Pegcetacoplan in the Retina
Geographic Atrophy Is a
C3-Dependent Neuropathology
Phase 2 FILLY Study:
Pegcetacoplan Reduced GA Lesion Growth
*,†Square root. Modified intention-to-treat (mITT) population was used for the efficacy analysis; defined as all patients who received at least 1 injection and underwent at least 1 follow-up examination at month 2 or
later at which primary efficacy data were collected. 2-sided t tests at the alpha = 0.1 level
Liao DS, et al. Ophthalmology. 2020;127:186-95. Holz et al. JAMA Ophthalmol. 2018
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

Role of C3 in
Neurodegeneration
Angela Genge, M.D., FRCP(C)
Executive Director, Clinical Research Unit & Director of ALS Center of Excellence
Montreal Neurological Institute
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

69
Multiple Preclinical Studies Demonstrate that C3 Inhibition Is
Neuroprotective in Aging and Neurodegenerative Diseases
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

70
Aberrant C3-Mediated Pruning Leads to Synaptic and
Cognitive Dysfunction in Multiple Neurologic Diseases
Stephen, Barres and Stevens, Annu Rev Neurosci 2012 https://joannamoncrieff.com/2017/11/27/philosophy-part-6-are-mental-
disorders-brain-diseases-in-waiting/
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

71
C3 Protein Is Elevated in Alzheimer’s Disease Patient CSF;
C3 Knockout Is Synaptoprotective in AD Animal Models
C3 and Processed C3 Protein (C3b, iC3b and C3c)
Is Increased in AD Patient CSF
M O U S E M O D E L O F A DA D PAT I E N T S
C3 Knockout Is Protective of Synapses
in an Amyloid Mouse Model
Wu, 2019 Wu, et al 2019
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

72
C3 Is Upregulated in Rapidly Progressing Tauopathies
such as PSP, CBD and FTD
C3 KO Prevents Cortical Atrophy in a
Mouse Tauopathy Model
C3 mRNA Is Elevated in CBD
and PSP Patient Brains
Litvinchuk et al., 2018
CBD – Corticobasal Degeneration
PSP – Progressive Supranuclear Palsy
FTD – Frontotemporal Dementia
Wu et al., 2019
6
5
4
3
2
1
0
Rela
tive C
3 m
RN
A l
evel
NCI CBD Pick PSP
n.s.
**
*
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
73
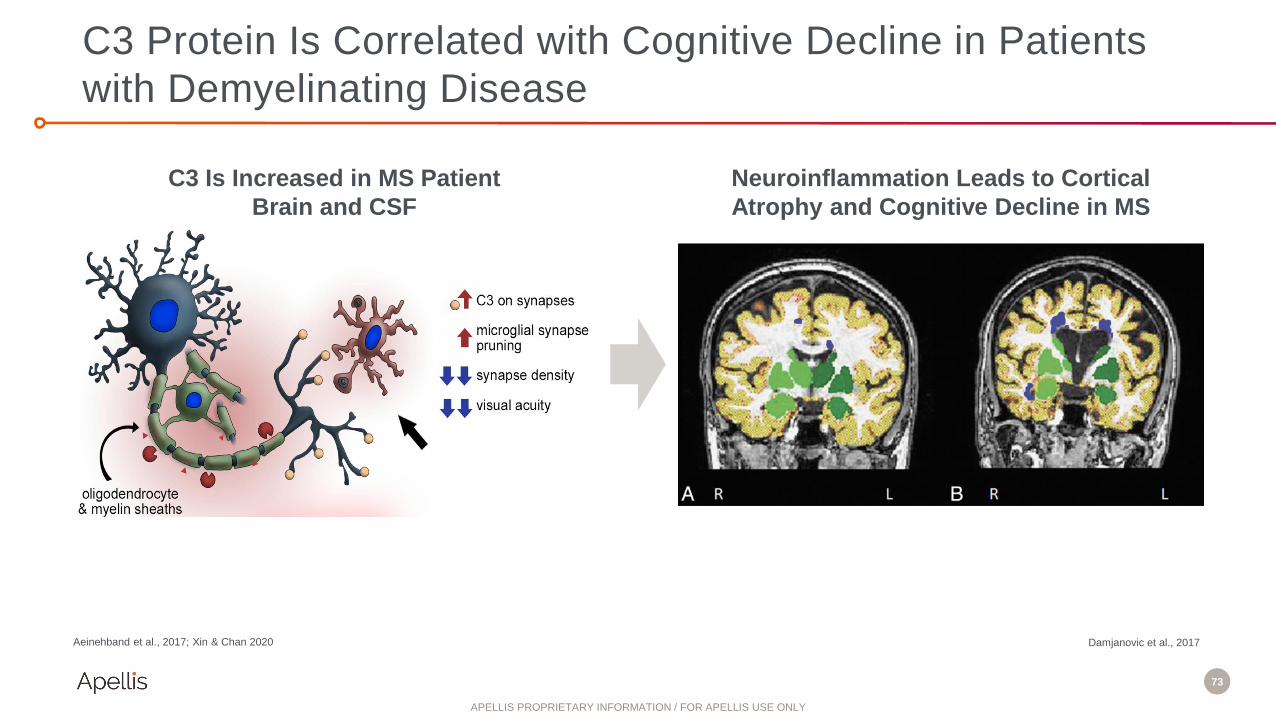
C3 Protein Is Correlated with Cognitive Decline in Patients
with Demyelinating Disease
C3 Is Increased in MS Patient
Brain and CSF
Neuroinflammation Leads to Cortical
Atrophy and Cognitive Decline in MS
Aeinehband et al., 2017; Xin & Chan 2020 Damjanovic et al., 2017
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

74
Rationale for C3 Inhibition as a Treatment for
Neurodegenerative Diseases
C3 regulation is required for synaptic refinement, learning, and memory in neural
development and throughout life
C3 dysregulation results in synaptic loss and dysfunction, a primary cause of
cognitive decline in aging and many neurologic diseases including ALS, Alzheimer’s
disease, multiple sclerosis, and tauopathies.
Restoring C3 regulation with Apellis’ proprietary molecules aims to improve cognitive
function in multiple neurodegenerative diseases
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

Pioneering C3 in
Neurodegeneration
David Eyerman, Ph.D.
Vice President, Translational Neurology
Apellis Pharmaceuticals
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

76
A Large Challenge in Treating CNS Diseases Is Getting
Pharmacologic Treatment Across the Blood Brain Barrier
Zhou et al., 2017
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

77
• Brain-shuttle enabled
biologic inhibitors
Next-Gen Brain-Active
C3 Inhibitors • Brain-delivered
APL-1030 secretors
• Brain-delivered C3 gene
knockdown
Gene Therapies
• Intrathecal APL-1030
First-in-Class Brain-Active
C3 Inhibitor
Building a Portfolio of Brain-Active Complement Therapies
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

78
• Brain-shuttle enabled
biologic inhibitors
Next-Gen Brain-Active
C3 Inhibitors • Brain-delivered
APL-1030 secretors
• Brain-delivered C3 gene
knockdown
Gene Therapies
• Intrathecal APL-1030
First-in-Class Brain-Active
C3 Inhibitor
Building a Portfolio of Brain-Active Complement Therapies
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

79
APL-1030: A Novel Molecular Entity C3 Inhibitor
• 64 amino acids, highly water soluble
• Binds to same epitope of C3/C3b as
pegcetacoplan
• Binding affinity and inhibition equal to
pegcetacoplan
• High thermal stability
• Recombinant and synthetic manufacture is
feasible
• C- and/or N-terminus accessible to
modification without impact on function
C3
Alternative
Pathway
Classical
Pathway
Lectin
Pathway
C3a
MAC
C3b
C5a C5b
C5
STOP STOP
STOP STOP
Co
ntro
ls a
ll do
wn
stre
am
effe
cts
A P L - 1 0 3 0
Neuroinflammation
Neurodegeneration
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

80
APL-1030 Is a Novel C3 & C3b Inhibitor for Intrathecal
Delivery to the Brain
• Good tolerability and high
brain concentrations
following 5-day intrathecal
pump infusion in rats
• Enters brain interstitial fluid
in rats
• Enters brain and inhibits C3
in human primates (NHPs)
I N V I V O P K / P DDrug
Delivery
Pump
APL-1030 Delivery to
CSF and Brain
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

81
High CSF Concentrations and Good Tolerability in NHPs
Following Intrathecal Administration of APL-1030
CSF Levels of APL-1030
0 24 48 72 96 120 1440.1
1
10
100
1000
Hours of Infusion
Pump
Shutoff
Plasma Levels of APL-1030
0 24 48 72 96 120 1440.01
0.1
1
10
100
1000
Hours of Infusion
CSF 0.8 mg/day CSF 2.0 mg/day
CSF 8 mg/day CSF 20 mg/day
CS
F [
AP
L-1
03
0]
µg
/mL
Pla
sm
a [
AP
L-1
03
0]
µg
/mL
Pump
Shutoff
Plasma 0.8 mg/day Plasma 2.0 mg/day
Plasma 8 mg/day Plasma 20 mg/day
20-NPK-001
• Dose escalating exposure in CSF up to ~500ug/mL
• SS CSF achieved within 8-24 hours of infusion
• T1/2 of APL-1030 post-pump shutoff = 3-6h in CSF and ~20h in plasma
• Plasma concentrations are 10-15X lower than CSF
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

82
APL-1030 Distributes Across the Brain of NHPs Following
5 Days of Intrathecal Administration
Pre
fronta
l Cort
ex
Occ
ipita
l Cort
ex
Ento
rhin
al C
ortex
Par
ieta
l Cort
ex
Hip
pocam
pus CA1
Hip
pocam
pus CA2
Hip
pocam
pus CA3
Cau
date
Puta
men
Subst
antia
Nig
ra
Glo
bus Pal
lidus
Am
ygdal
a
Thalam
us
Cer
ebel
lum
0.1
1
10
100
1000
AP
L-1
030 (
ug
/g)
APL-1030 (2 mg/day)
Cortex Hippocampus Basal Ganglia Other
Pre
fronta
l Cort
ex
Occ
ipita
l Cort
ex
Ento
rhin
al C
ortex
Par
ieta
l Cort
ex
Hip
pocam
pus CA1
Hip
pocam
pus CA2
Hip
pocam
pus CA3
Cau
date
Puta
men
Subst
antia
Nig
ra
Glo
bus Pal
lidus
Am
ygdal
a
Thalam
us
Cer
ebel
lum
0.1
1
10
100
1000
APL-1030 (20 mg/day)
AP
L-1
030 (
ug
/g)
Cortex Hippocampus Basal Ganglia Other
Brain Tissue Concentrations of APL-1030
Target Tissue
Concentration
20-NPK-001
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

83
PFC EC CA1 CA3
0
1
2
3
4
5
6
C3a n
g/g
, B
rain
Tis
su
e Vehicle
APL-1030 (20 mg/day)
APL-1030 (2 mg/day)
Functional Inhibition of C3 Breakdown in Cognition-Relevant
Brain Regions of NHPs Treated with APL-1030
Brain Tissue Levels of the C3 Breakdown Product C3a Following
Intrathecal Infusion with APL-1030 for 5 Days
Prefrontal
CortexHippocampus
CA1
Hippocampus
CA3 20-NPK-001
Entorhinal
Cortex
LOD
(0.12 ng/mL)
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
84
APL-1030: Advancing First-in-Class, Brain-Active C3 Inhibitor
IND planned in H1 2022
Potential to treat multiple neurodegenerative disorders
Inhibits C3 breakdown in brain of nonhuman primates
Distributes throughout the brain
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

85
• Brain-shuttle enabled
biologic inhibitors
Next-Gen Brain-Active
C3 Inhibitors • Brain-delivered
APL-1030 secretors
• Brain-delivered C3 gene
knockdown
Gene Therapies
• Intrathecal APL-1030
First-in-Class Brain-Active
C3 Inhibitor
Building a Portfolio of Brain-Active Complement Therapies
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

86
Small Biological Building Blocks Replicating Pegcetacoplan
Pharmacology Will Yield New Therapies for Neurologic Diseases
Salvia et al., 2016
Brain Shuttle Mediated Delivery
via Systemic ROA
C3/C3b Complement Inhibitors
and Bifunctional NBEs
Gene Therapy Secretion in Brain
with Long Durability of Effect
LNP / AAV
https://engage.utsouthwestern.edu/pages/stories/donor-
story-gene-therapy
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

87
Hal
f Bra
in
Stria
tum
Cer
ebel
lum
Hip
pocam
pus
Cort
ex
0.0
0.5
1.0
1.5
2.0
Test A
rtic
le u
g/g
Brain-Shuttle Enabled C3 Inhibitor to Treat CNS Indications
C3/C3bPharmacologically-
active moiety
Brain
Shuttle
Brain ShuttleBrain delivery via
trojan horse
Brain-Shuttle Enabled C3 Inhibitor in Rat Brain
Following a Single IV Administration
Target
Concentration
10mg/kg; IV route of administration;
24 hours post dose
Data on file
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

88
• Brain-shuttle enabled
biologic inhibitors
Next-Gen Brain-Active
C3 Inhibitors • Brain-delivered
APL-1030 secretors
• Brain-delivered C3 gene
knockdown
Gene Therapies
• Intrathecal APL-1030
First-in-Class Brain-Active
C3 Inhibitor
Building a Portfolio of Brain-Active Complement Therapies
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

89Salvia et al., 2016
Brain Shuttle Mediated Delivery
via Systemic ROA
C3/C3b Complement Inhibitors
and Bifunctional NBEs
Gene Therapy Secretion in Brain
with Long Durability of Effect
LNP / AAV
https://engage.utsouthwestern.edu/pages/stories/donor-
story-gene-therapy
Small Biological Building Blocks Replicating Pegcetacoplan
Pharmacology Will Yield New Therapies for Neurologic Diseases
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
90
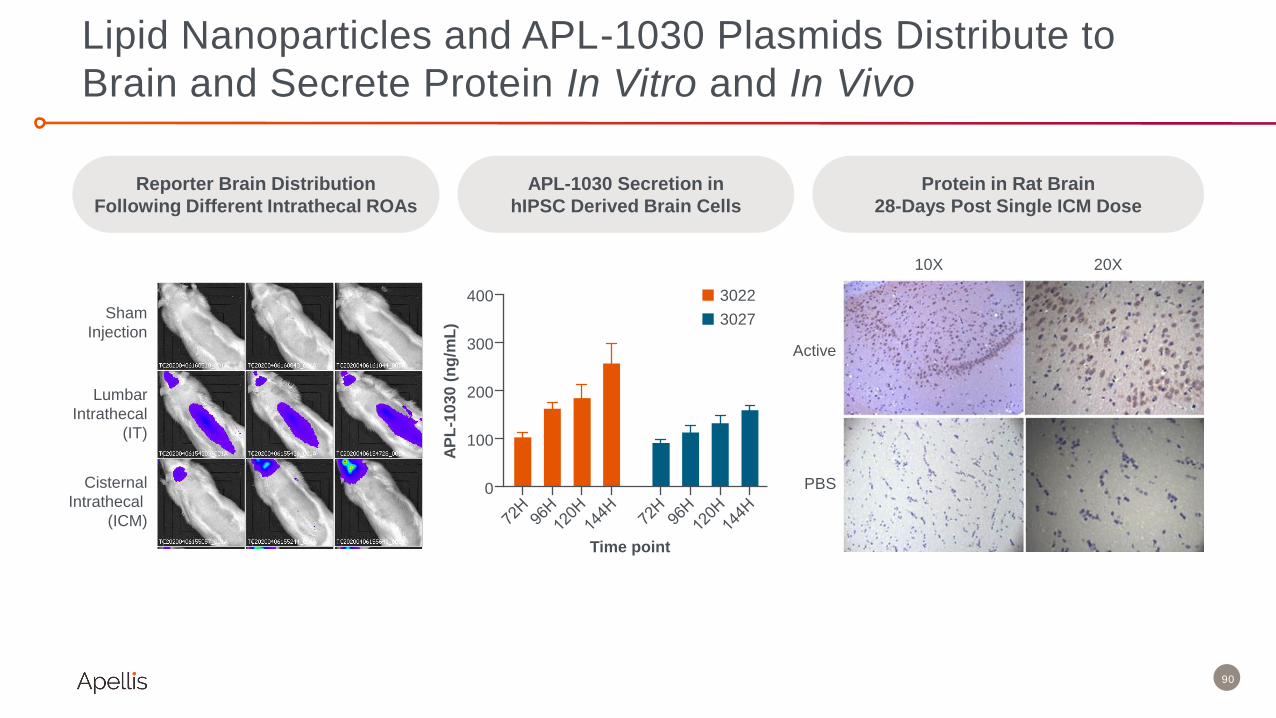
Lipid Nanoparticles and APL-1030 Plasmids Distribute to
Brain and Secrete Protein In Vitro and In Vivo
Protein in Rat Brain
28-Days Post Single ICM Dose
APL-1030 Secretion in
hIPSC Derived Brain Cells
Sham
Injection
Lumbar
Intrathecal
(IT)
Cisternal
Intrathecal
(ICM)
Reporter Brain Distribution
Following Different Intrathecal ROAs
Active
PBS
10X 20X
0
100
200
300
400 3022
3027
Time point
AP
L-1
03
0 (
ng
/mL
)

91
Building a Portfolio of Brain-Active Complement Therapies
TECHNOLOGYDRUG
CANDIDATEDISCOVERY
IND
ENABLING
EARLY
CLINICAL
Biologic
APL-1030 - IT
C3/C3b
Brain Shuttle
Gene
therapy
C3/C3b
Secretor
• Potential to treat multiple
neurodegenerative diseases by
targeting C3
• APL-1030 is a first-in-class, brain-
active C3 inhibitor
– Preclinical pharmacodynamic
response at dose levels expected
to translate to humans
– IND submission in H1 2022
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

APELLISR&D DAY
A N D T H E Y ’ R E O F F ! Be #1 in the Retina
Cedric Francois, M.D., Ph.D.
Chief Executive Officer
Apellis Pharmaceuticals
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

93
• Pegcetacoplan
• APL-2006: anti-VEGF
plus anti-C3
Next-Gen Wet AMD
Apellis: Be #1 in the Retina
• Gene therapies for all
forms of AMD
Gene Therapy
Geographic Atrophy and
Intermediate AMD
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
94
• Pegcetacoplan
• APL-2006: anti-VEGF
plus anti-C3
Next-Gen Wet AMD
Apellis: Be #1 in the Retina
• Gene therapies for all
forms of AMD
Gene Therapy
Geographic Atrophy and
Intermediate AMD
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
95
We believe that GA is the consequence of a failure to clean up C3 deposition in the retina.
Single pathway inhibitors are insufficient to correct this failure .
Pegcetacoplan, a targeted C3 therapy, has the potential to accomplish this with its broad,
multi-point control of complement across all three pathways.
“Other complement
inhibitors have failed.
Why should
pegcetacoplan work?”
• Visual acuity charts don't reflect the real impact of GA in vision due to foveal sparing.
• GA is a relentless, progressive disease that severely impairs patients’ visual function and quality
of life.
• A leading cause of blindness, GA has no approved treatments and remains the most significant
unmet need in the retina.
• The need and desire for treatment was reflected in the speed of enrollment in DERBY and
OAKS.
“Pegcetacoplan has no
impact on visual acuity. It
will take years to notice a
difference. Why would
people take this drug?”
Key Misconceptions Dispelled
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

96
• The FILLY study met its primary endpoint, demonstrated a dose response, and the sham group
progressed at the expected rate.
• Dropouts were in line with other GA trials. 242 out of 246 patients (modified intent-to-
treat: mITT) were included in the primary analysis population, which accounted for missing data with
the well-established mixed-effect model for repeated measures (MMRM).
• All sensitivity analyses confirmed the efficacy results.
• Post hoc analyses also showed that lesion growth slowed in treated eyes vs. contralateral eyes in
patients with bilateral GA and that pegcetacoplan slowed progression from intermediate AMD to GA.
“How can we trust the
FILLY data?”
• The FILLY trial had no safety findings that limited DERBY and OAKS, which studies the same
broad patient population.
• Exudations are an expected occurrence in GA. No classical CNV was detected and there was
no clinically significant impact on vision.
• FILLY was single-masked, which may have led to greater reporting of exudations in subjects
randomized to pegcetacoplan than in subjects randomized to sham. DERBY and OAKS are
double masked to further minimize potential bias.
• Two cases of infectious endophthalmitis out of ~1,500 intravitreal injections are consistent with
reported incidence rates in published studies involving intravitreal injection.
“FILLY had safety issues.
Pegcetacoplan causes
‘wet AMD' and had two
cases of infectious
endophthalmitis.”
Key Misconceptions Dispelled
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

97
Geographic Atrophy Is a Leading Cause of Blindness
Impacting 5M Patients Worldwide
2,741,000
2,035,000
588,000
1,296,000
907,000
257,000
4,037,000
2,942,000
845,000
Prevalent Patients Diagnosed Patients Treated by any DMT
US
Europe
Estimated future commercial opportunity across US and Europe
Global Prevalence
5,000,000
1.Boyer DS et al., Retina 2017 2 2. Wong WL, et al. Lancet Glob Health. 2014;2:e106-16; 3. Global Data AMD Global Drug Forecast and Market Analysis, JAMA Ophthalmology, Gibson 2012 American Journal of
Preventative Medicine, ZS Associates Demand Forecast Market Research, APLS internal analysis and assumptions
Current global prevalence
Europe includes 31 countries in southern, northern, and western Europe. US and EU figures represent future years. DMT: Disease Modifying Therapies
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

What Is the Unmet Need in
Geographic Atrophy?
Charles Wykoff, M.D., Ph.D.
Director of Research
Retina Consultants of Texas
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

99
• There are 5 million people living with GA
worldwide; 1 million are in the US1
• GA accounts for 20% of all legal blindness
attributed to AMD2, 3
• There is no approved treatment for GA1
1. Boyer DS et al., Retina 2017.
2. Ferris FL 3rd et al., Arch Ophthalmol. 1984
3. Klaver CC, et al., Arch Ophthalmol. 1998
Image from Holz FG et al., Ophthalmology 2014.
There Is No Treatment for GA, a Leading Cause of Blindness
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
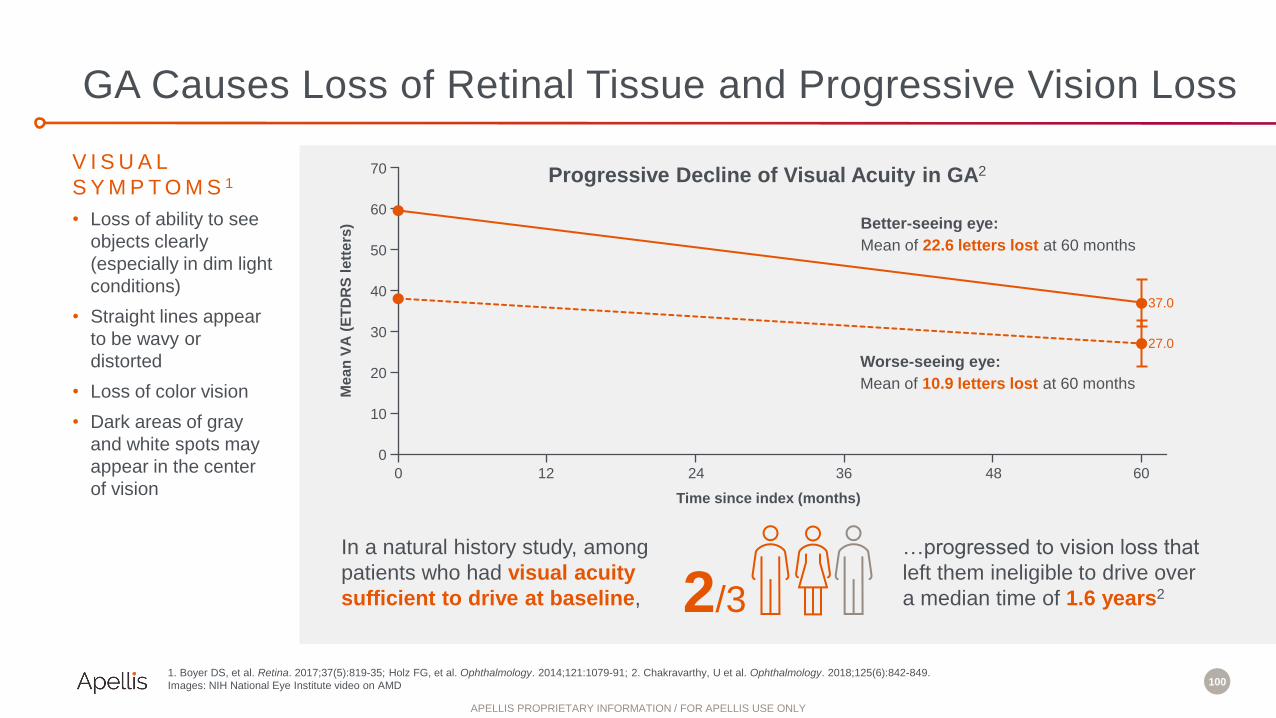
100
V I S U A L
S Y M P T O M S 1
• Loss of ability to see
objects clearly
(especially in dim light
conditions)
• Straight lines appear
to be wavy or
distorted
• Loss of color vision
• Dark areas of gray
and white spots may
appear in the center
of vision
1. Boyer DS, et al. Retina. 2017;37(5):819-35; Holz FG, et al. Ophthalmology. 2014;121:1079-91; 2. Chakravarthy, U et al. Ophthalmology. 2018;125(6):842-849.
Images: NIH National Eye Institute video on AMD
In a natural history study, among
patients who had visual acuity
sufficient to drive at baseline, 2/3
…progressed to vision loss that
left them ineligible to drive over
a median time of 1.6 years2
70
60
50
40
30
20
10
0
Me
an
VA
(E
TD
RS
le
tte
rs)
0 12
Time since index (months)
24 36 48 60
Better-seeing eye:
Mean of 22.6 letters lost at 60 months
Worse-seeing eye:
Mean of 10.9 letters lost at 60 months
Progressive Decline of Visual Acuity in GA2
37.0
27.0
GA Causes Loss of Retinal Tissue and Progressive Vision Loss
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

101
Living with GA:
Q&A with Rob
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

Pegcetacoplan: Phase 2 FILLY Results
Charles Wykoff, M.D., Ph.D.
Director of Research
Retina Consultants of Texas
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

103
Phase 2 FILLY Study: Design
*Confirmed by the central reading center using fundus autofluorescence images. †Not counting the 3 satellite sites
Liao DS, et al. Ophthalmology. 2020;127
Sham groups were pooled
for all analyses
PEGCETACOPLAN
15 mg/0.1 mL
every other month (n=79)
PEGCETACOPLAN
15 mg/0.1 mL
monthly (n=86)Population: patients with
geographic atrophy*
secondary to AMD
Design: single masked,
randomized 2:1:2:1
Duration: 18 months
Randomized 2:2:1:1
ELIGIBLE PATIENTS
WITH GA*
246 subjects
in 43 sites†
SHAM
every other month (n=40)
SHAM
monthly (n=41)
Single masked
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

104
Phase 2 FILLY Study: Timeline and Endpoints
Liao DS, et al. Ophthalmology. 2020;127
0 6
months
12months
18months
2
months
Images
taken at Primary safety endpoint
Number and severity of local and
systemic treatment emergent
adverse events (TEAEs)
Primary efficacy endpoint
Change in geographic
atrophy (GA) lesion size
from baseline at month 12
Treatment
period
No
injections
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
105
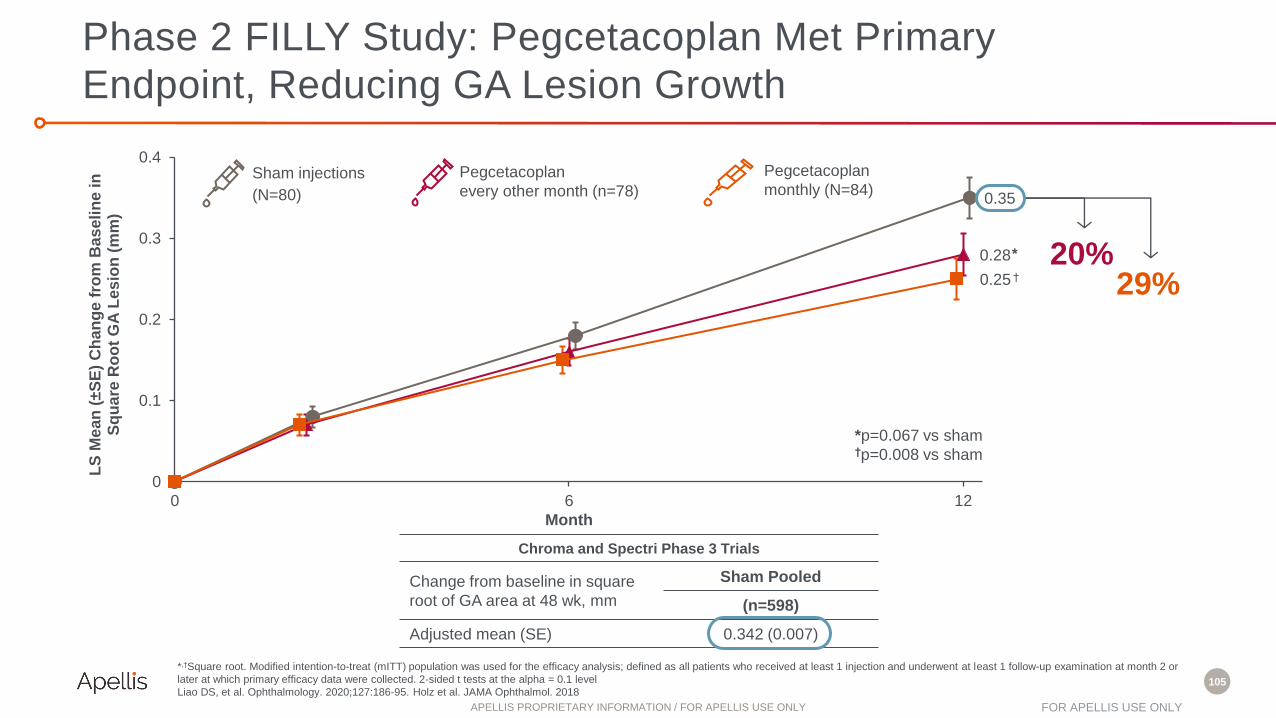
Chroma and Spectri Phase 3 Trials
Change from baseline in square
root of GA area at 48 wk, mm
Sham Pooled
(n=598)
Adjusted mean (SE) 0.342 (0.007)
*p=0.067 vs sham†p=0.008 vs sham
*
†
0.35
0.28
0.25
0
0.1
0.2
0.3
0.4
0 6 12
LS
Me
an
(±S
E)
Ch
an
ge f
rom
Bas
eli
ne
in
S
qu
are
Ro
ot
GA
Le
sio
n (
mm
)
Month
20%29%
Phase 2 FILLY Study: Pegcetacoplan Met Primary
Endpoint, Reducing GA Lesion Growth
*,†Square root. Modified intention-to-treat (mITT) population was used for the efficacy analysis; defined as all patients who received at least 1 injection and underwent at least 1 follow-up examination at month 2 or
later at which primary efficacy data were collected. 2-sided t tests at the alpha = 0.1 level
Liao DS, et al. Ophthalmology. 2020;127:186-95. Holz et al. JAMA Ophthalmol. 2018
Sham injections
(N=80)
Pegcetacoplan
every other month (n=78)
Pegcetacoplan
monthly (N=84)
FOR APELLIS USE ONLYAPELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

106
Phase 2 FILLY Study: Impact of Pegcetacoplan on Absolute
GA Lesion Growth Is Consistent with the Primary Endpoint
1.47
2.13
0
0.5
1
1.5
2
2.5
0 6 12
20%30%
*** p=0.068 vs sham
††† p=0.005 vs sham
†††
*Nominal p values
mITT, Observed, Mixed-Effect Model
A mixed effect model with main effects of treatment, visit and GA lesion at baseline, and interactions of treatment × visit, visit ×
baseline.
M12DBL Data
LS
Mean
(±S
E)
Ch
an
ge f
rom
Baselin
e in
Sq
uare
Ro
ot
GA
Lesio
n (
mm
)
LS
Mean
(±S
E)
Ch
an
ge f
rom
Baselin
e
in G
A L
esio
n (
mm
2)
Sham injections
(N=80)
Pegcetacoplan
every other month (n=78)
Pegcetacoplan
monthly (N=84)
Month Month
0.25
0
0.1
0.2
0.3
0.4
0 6 12
20%29%
** p=0.067 vs sham
†† p=0.008 vs sham
††
P R I M A R Y E N D P O I N T
( S Q U A R E R O O T T R A N S F O R M E D
L E S I O N G R O W T H )
A B S O L U T E ( U N T R A N S F O R M E D )
L E S I O N S I Z E *
0.28**
0.35
1.70***
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

107
• Exudations at 12 Months (treatment period):
– 16% monthly, 6% every other month, 1% sham
– 0 cases of classical CNV
– No clinically significant impact on vision
– Patients discontinued pegcetacoplan; most treated with anti-VEGF therapy
• Safety in line with other studies of intravitreally administered agents
• Serious adverse events in the study eye were reported in 4 of 86 (4.7%)
(2 endophthalmitis, 1 IOP increase, 1 retinal detachment), 2 of 79 (2.5%)
(endophthalmitis, IOP increase), and 1 of 81 (1.2%) (dry AMD) of patients in the
pegcetacoplan monthly, pegcetacoplan every other month, and sham groups,
respectively
Liao DS, et al. Ophthalmology. 2020;127:186-95.
Wykoff CC, et al. Ophthalmology. 2021; in press.
GA
Phase 2 FILLY Study: Safety
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

108
• Intermediate AMD (iAMD) is characterized
by the presence of large drusen and
pigmentary abnormalities in the macula
• Associated with visual impairment,
especially in low-light condition
• Similar to GA, dysregulation of the
complement system is implicated in iAMD
• No approved therapy to prevent the
progression of iAMD to advanced AMD
Longitudinal Analysis of Structural and Functional Changes in Presence of Reticular Pseudodrusen Associated With Age -Related Macular Degeneration.
Intermediate AMD
Geographic Atrophy Wet AMD
A d v a n c e d A M D
Pegcetacoplan: Opportunity for Earlier Intervention in AMD
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

109
iRORA: incomplete RPE and outer retinal atrophy; cRORA: complete RPE and
outer retinal atrophy; RPE: retinal pigment epithelium
Sadda et al., EURETINA 2020 late-breaking presentation.
cRORAMonth 12
iRORAMonth 0
• Therapeutic trials for geographic atrophy are focused
on the end-stage (complete RPE and outer retinal
atrophy or cRORA); e.g., GA lesions
• Earlier endpoints in the atrophy pathway have been
defined: incomplete RPE and outer retinal atrophy
(iRORA); e.g., consistent with intermediate AMD
Earlier Endpoints for Retinal Atrophy
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

110
Pearson Chi-Square:
Month 6 - P=0.08 for PM; P=0.32 for PEOM;
*Month 12 - P=0.02 for PM; P=0.03 for PEOM
Relative risk:
Month 12 - 0.61 (0.37- 1.00) for PM; 0.70 (0.50 – 0.98) for PEOM
cRORA
iRORA
Residual
RPE
Phase 2 FILLY Post Hoc Analysis: Pegcetacoplan Slowed
Progression from Intermediate AMD to GA
Ip et al., Macula Society 2021.
All p-values are nominal.
P R O G R E S S I O N F R O M i R O R A T O c R O R A
27.8%
50.0%
40.6%
57.6%53.1%
81.8%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Month 6 Month 12
Pegcetacoplan Monthly (n=18)
Pegcetacoplan Every Other Month (n=33)
Sham (33)
*P=0.02
*P=0.03
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

111
Key Takeaways
Pegcetacoplan met the primary endpoint in the Phase 2 FILLY study, reducing GA lesion
growth with benefit shown across GA phenotypes
Demonstrated a dose response with sham group progressing at expected rate
Phase 2 FILLY safety in line with other studies of intravitreally administered agents
Slowed progression from intermediate AMD to GA; potential for earlier intervention in
the course of GA
Urgent and significant need for treatments for GA, a disease that leads to blindness
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

Pegcetacoplan: Advancing the First
Potential Treatment for GA
Jeffrey Eisele, Ph.D.
Executive Vice President, Ophthalmology Program Lead
Apellis Pharmaceuticals
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

113
94% believe that GA poses a significant
burden to patients’ quality of life1*
84% believe that slowing lesion growth is the
most important goal for preserving vision in GA1*
“I think APL-2 is the most promising of any of the
agents in development so far.” – Retina KOL2
“All three complement pathways converge on C3,
which makes APL-2 much more promising than
lampalizumab’s factor D inhibitor.”– Retina Specialist2
“Apellis designed these trials really well. If it shows
benefit, I think APL-2 will get a lot of uptake pretty quickly.”
– Retina Specialist2
1BEESY Strategy Global GA ECP ATU (n=488) | *Rating 5, 6 and 7-point scale where 1= completely disagree and 7= completely agree2Health Advances Commercial Assessment & Analysis (n=31)
“Anything over 20% [reduction in lesion growth rate]
would be significant in my mind.” – Retina Specialist2
These statements include only the opinions of a limited sample of retina specialists and do not necessarily reflect the opinions of all retina specialists.
Retina Specialists Are Enthusiastic About the Prospect of
Pegcetacoplan as the First-Ever GA Therapy
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

114
DERBY and OAKS: Two Phase 3 Studies of
Pegcetacoplan in Patients with GA (n=1,258)
Same study population
and trial design as FILLY
Population: patients with
geographic atrophy*
secondary to AMD
Primary endpoint: change
in total area of GA lesion(s)
based on fundus
autofluorescence (FAF) at
month 12
Design: single masked,
randomized 2:1:2:1
Duration: 2 years
Randomized 2:1:2:1
ELIGIBLE PATIENTS
WITH GA*
>600 subjects
from approx. 100
multinational sites
per study
PEGCETACOPLAN
15 mg/0.1 mL
monthly (n=200)
PEGCETACOPLAN
15 mg/0.1 mL
every other month (n=200)
SHAM INJECTIONS
pooled (n=200)
Double masked Primary endpoint
read out
1 year 1 year
NCT03525600, NCT03525613
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

115
DERBY and OAKS: Key Efficacy Endpoints
BCVA=best-corrected visual acuity; FAF=fundus autofluorescence; LL-BCVA=low-luminance BCVA.
NCT03525600, NCT03525613
P R I M A RY
• Change from baseline to Month 12 in total area of GA lesion(s) in the study eye
(in mm2) based on FAF
S E C O N D A RY
• BCVA, LL-BCVA
• Reading speed
• Microperimetry (OAKS study only) —
Macular Integrity Assessment
(MAIA) device
• National Eye Institute Visual
Functioning Questionnaire 25-Item
Version (NEI VFQ-25)
• Functional Reading Independence
Index (FRI) composite score
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
116
DERBY and OAKS: Top-Line Results Expected in September
P R I M A R Y E N D P O I N T
Change in lesion growthS A F E T Y
Monthly treatment
with pegcetacoplan
Every-other-month treatment
with pegcetacoplan
• Safety profile including rate
of exudations and
intraocular inflammation
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
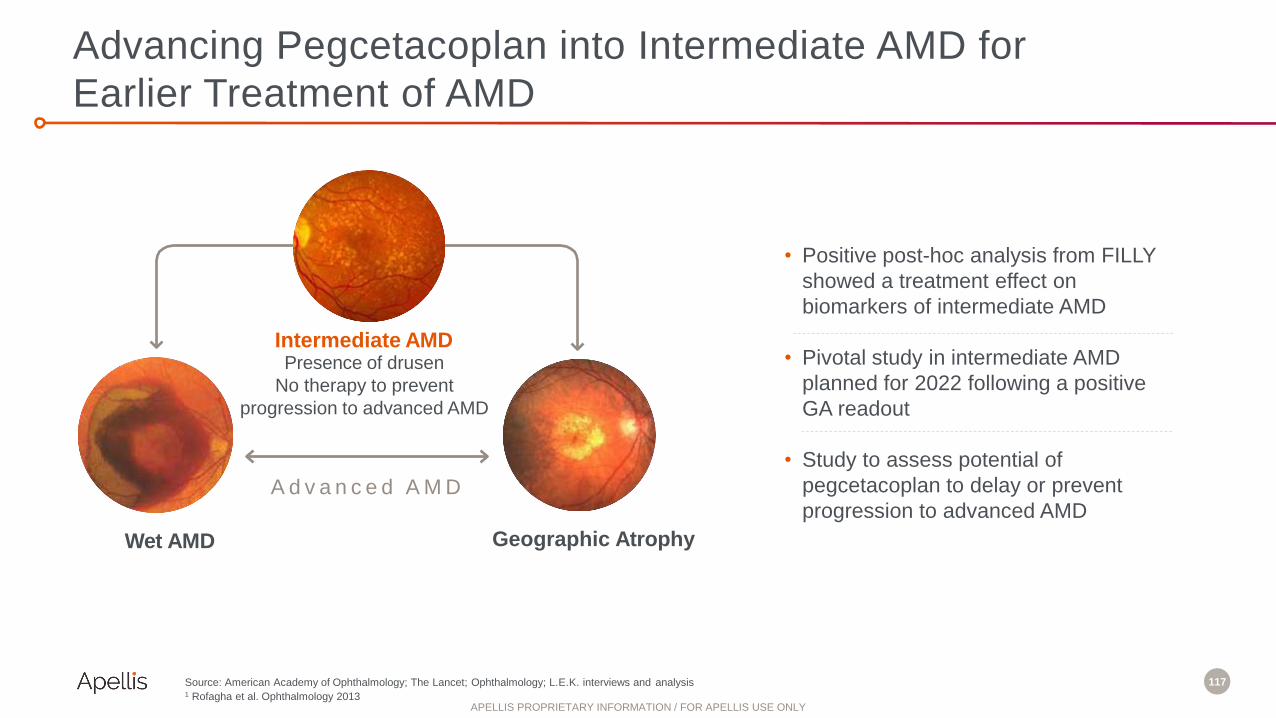
117
Advancing Pegcetacoplan into Intermediate AMD for
Earlier Treatment of AMD
Source: American Academy of Ophthalmology; The Lancet; Ophthalmology; L.E.K. interviews and analysis1 Rofagha et al. Ophthalmology 2013
Intermediate AMDPresence of drusen
No therapy to prevent
progression to advanced AMD
Geographic Atrophy Wet AMD
A d v a n c e d A M D
• Positive post-hoc analysis from FILLY
showed a treatment effect on
biomarkers of intermediate AMD
• Pivotal study in intermediate AMD
planned for 2022 following a positive
GA readout
• Study to assess potential of
pegcetacoplan to delay or prevent
progression to advanced AMD
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
Next-Gen Wet AMD
Lukas Scheibler, Ph.D.
Chief Innovation Officer
Apellis Pharmaceuticals
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

119
• Pegcetacoplan
• APL-2006: anti-VEGF
plus anti-C3
Next-Gen Wet AMD
Apellis: Be #1 in the Retina
• Gene therapies for all
forms of AMD
Gene Therapy
Geographic Atrophy and
Intermediate AMD
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

120
US and Europe Prevalence of Patients with AMD
Source: Health Advances analysis, UN Population Projections, Friedman 2004, EUREYE 2006, Kang and Kim 2019, Song 2017, Mathenge 2013, Grunwald 2013 Ophthal,
Sadda 2018 Ophthal, Domalpally 2018 Ophthalmol Retina, Klein 2008 Am J Ophthalmal, Mitchell 2002 Ophthal, Wong 2014 Lancet Glob Health, Colijn 2017 Oph, Gibson
2012 Am J Prev Med, Wu 2014 Ophthalmology, Wu 2015 IOVS, Wu 2016 IOVS, Augood 2006 Arch Ophthalmol (EUREYE).
A D VA N C E D A M D
GA +
WET AMD
~1.3 million at
highest risk of
progression to GA~4 million ~6 million
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

121
Wet AMD patients treated with anti-
VEGF therapy develop GA
Complement levels increase after anti-
VEGF therapy in eyes with wet AMDVisual function outcome declines over
time despite anti-VEGF treatment
0
5
10
15
20
25
30
35
40
Baseline Month 24
Proportion of patients with GA (%)
Lucentis (n=141) Eylea (n= 137)
https://www.aaojournal.org/article/S0161-6420(19)31954-2/fulltext https://doi.org/10.1038/s41598-021-87340-6 https://www.aaojournal.org/article/S0161-6420(18)30947-3/fulltext
C3 + Anti-VEGF Therapy May Be Superior to Anti-VEGF Alone
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
122
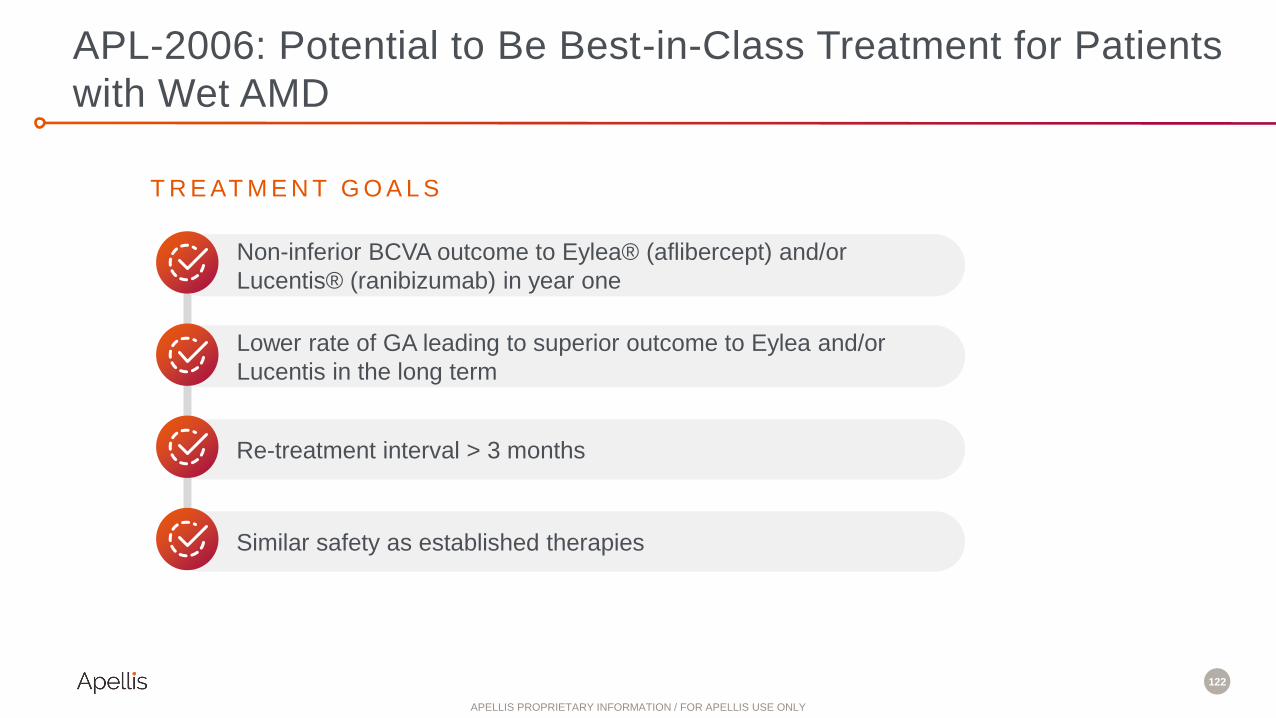
Lower rate of GA leading to superior outcome to Eylea and/or
Lucentis in the long term
T R E AT M E N T G O A L S
Non-inferior BCVA outcome to Eylea® (aflibercept) and/or
Lucentis® (ranibizumab) in year one
Re-treatment interval > 3 months
Similar safety as established therapies
APL-2006: Potential to Be Best-in-Class Treatment for Patients
with Wet AMD
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

123
APL-2006: Next-Generation Wet AMD Therapy
• Potential to provide superior
treatment for patients with
wet AMD and GA
• Less frequent dosing
• IND anticipated late 2022
Ranibizumab – VEGF inhibitor
VH
CH
VL
CL
LA
1030
LA
1030
Long Acting – 2x half-life over
Lucentis in NHP
APL-1030 – C3 / C3b inhibitor
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

124
APL-2006: Potent Bispecific C3 and VEGF Inhibitor
Complement Inhibition Potency VEGF Inhibition vs. Lucentis
HUVEC Proliferation Assay
0.20
0.15
0.10
0.05
0
Ab
s.
(69
0n
m –
57
0 n
m)
Lucentis
APL-2006
Pegcetacoplan
APL-2006
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

125
• Pegcetacoplan
• APL-2006: anti-VEGF
plus anti-C3
Next-Gen Wet AMD
Apellis: Be #1 in the Retina
• Gene therapies for all
forms of AMD
Gene Therapy
Geographic Atrophy and
Intermediate AMD
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

126
Goal: Develop Gene Therapy to Secrete APL-1030 or
APL-2006 in the Retina
In vivo / rabbit studyIn vitro data in ARPE19 cells
Plasmid copy number GC/ng DNAAPL-1030 protein in media
of transfected ARPE19 cells
1500
1000
500
0
AP
L-1
03
0 i
n m
ed
ia (
ng
/mL
)
0.02 0.06 0.20
Dose (µg)
Sham 0.1 10 30
Dose (µg)
1 100
4000
3000
0
GC
/ng
DN
A
2000
1000
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
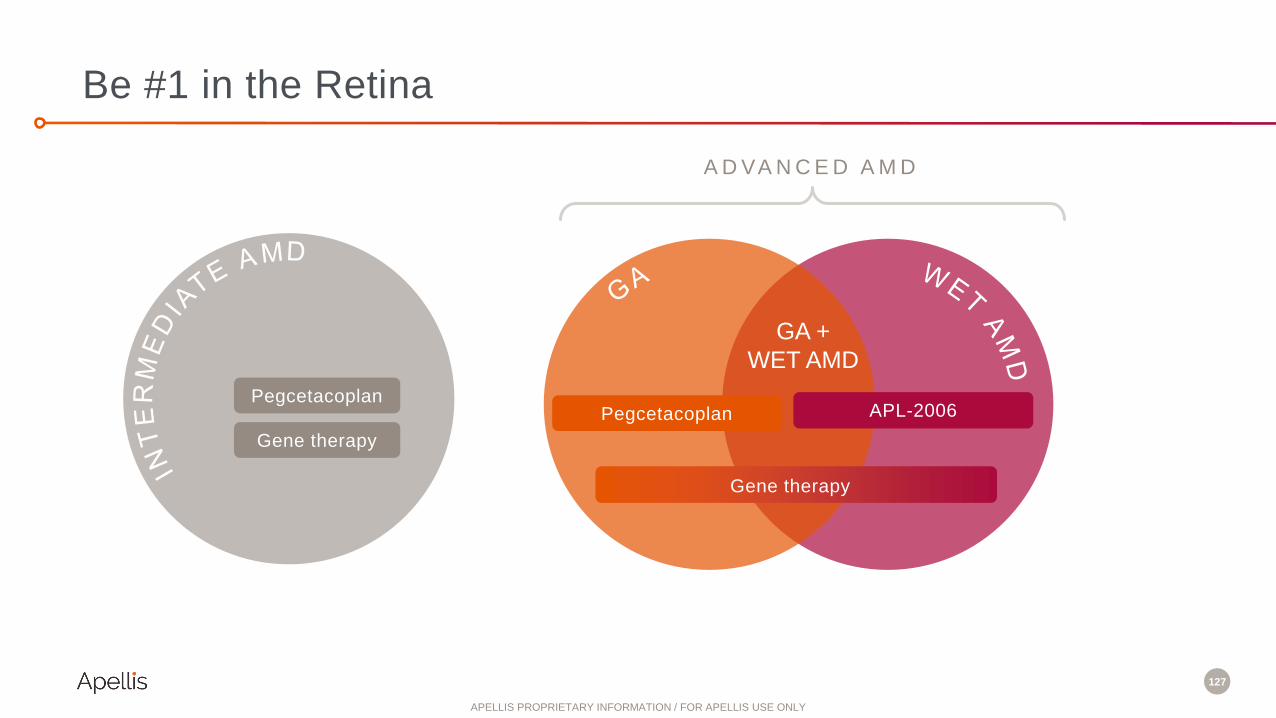
127
Be #1 in the Retina
A D VA N C E D A M D
GA +
WET AMD
PegcetacoplanPegcetacoplan APL-2006
Gene therapy
Gene therapy
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
APELLISR&D DAY
A N D T H E Y ’ R E O F F !
Neurology/Ophthalmology
Q&A
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
APELLISR&D DAY
A N D T H E Y ’ R E O F F !
Cedric Francois, M.D., Ph.D.
Chief Executive Officer
Apellis Pharmaceuticals
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

130
EXCLUSIVE RESEARCH COLLABORATIONto apply base editing to discover novel therapies for complement-driven diseases

131
P O S I T I O N S A P E L L I S F O R L O N G - T E R M L E A D E R S H I P I N C O M P L E M E N T
EXCLUSIVE RESEARCH COLLABORATION
6 research programs
over 5 years: vision for
one-time, curative
therapies
Base editing technology
to discover precision
medicines for diseases of
the eye, liver, and brain
Focused on C3
and other
complement targets
Modulating
a complex biological
system

132
BASE EDIT ING IS A NEW APPROACH TO GENE EDIT ING
Nuclease editingCreation of double-stranded breaks in DNA at a target
location to disrupt, delete, insert, or modify genes
Base editingDirect conversion of one base pair to another at a
target location, without double-stranded breaks
CRISPR → Guide RNA-driven targeting
• Leverages established DNA targeting ability of CRISPR
• Modified to not cause double-stranded breaks
Deaminase → Single base editing
• Completes predictable chemical modification at target DNA base
• Adenine Deaminase for A-to-G editor (“ABE”)
• Cytidine Deaminase for C-to-T editor (“CBE”)
Two components fused as a single protein:
A
A
T▲

APELLISR&D DAY
A N D T H E Y ’ R E O F F ! Beam Collaboration Q&A
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

134
• EMPAVELI launch off to strong start
• Platform potential for EMPAVELI with four new registrational programs
• New molecular entities in development to sustain long-term growth in existing and new indications
Global Leader in Complement, Today and Tomorrow
R A R E D I S E A S E
N E U R O L O G Y
O P H T H A L M O L O G Y
• C3 plays a key role in a wide range of neurodegenerative conditions
• Apellis to pioneer targeted C3 therapies in neurodegeneration
• Optimistic heading into DERBY and OAKS readout in September 2021
– Significant unmet need and blockbuster opportunity
• Data from monthly dosing believed to be sufficient for NDA submission
– Primary endpoint on monthly dosing minimally affected by missed visits due to COVID-19
– Primary endpoint on every-other-month dosing may be affected by missed visits due to COVID-19
• New molecular entities in development in GA, wet and intermediate AMD
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

135
PRODUCT DISEASE PRECLINICAL PHASE 1 PHASE 2 PHASE 3 LAUNCH
Rare Disease
EMPAVELI™ (systemic
pegcetacoplan)*
PNH
IC-MPGN / C3G
ALS
CAD
HSCT-TMA
siRNA + EMPAVELI** Existing + new indications
Ophthalmology
Intravitreal pegcetacoplanGA
Intermediate AMD***
APL-2006 GA & Wet AMD
Gene therapies Wet AMD, Intermediate AMD & GA
Neurology
APL-1030 Undisclosed
Brain shuttle Undisclosed
Gene therapies Undisclosed
Multiple
Therapeutic
Areas
APL-9 Control of host attack for gene therapies
Oral alternative pathway inhibitor Mild C3G and other indications
Gene-edited therapies (Beam) Undisclosed
*Sobi has global co-development and ex-U.S. commercialization rights for systemic pegcetacoplan **Initial IND for siRNA *** Pending regulatory feedback
Growing Pipeline in Rare Disease, Ophthalmology, and Neurology
Marketed in the US
IND in ‘22
IND in ‘22
IND in ‘22
Initiate Ph 3 in H2’21
Initiate Ph 2 in H2’21
Initiate Ph 3 in ’22
Initiate Ph 3 in H2’21
Potential to be registrational*
*
*
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY
APELLISR&D DAY
A N D T H E Y ’ R E O F F ! THANK YOU!
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY

APELLISR&D DAYJune 30, 2021
A N D T H E Y ’ R E O F F !
APELLIS PROPRIETARY INFORMATION / FOR APELLIS USE ONLY