Ape thumb deformity to publish
42
Dr. M KASI VISWANADHAM DEPT. OF ORTHO RMC ,KAKINDA
-
Upload
kasi-mogali -
Category
Health & Medicine
-
view
133 -
download
0
Transcript of Ape thumb deformity to publish

Dr. M KASI VISWANADHAM
DEPT. OF ORTHO
RMC ,KAKINDA

According to evolutionary biologists, one of the more singular factors elevating man as a higher mammal, as compared to any other, is
the modification in the functional capability of the thumb.
The human thumb stands alone in its talent to 'oppose'.
Anatomically, 'opposition' implies the movement by which you can touch the tip of your thumb to the tips of other fingers of the same hand.
No animal except the human kind has a truly opposable thumb

Ape thumb deformity
who cannot move the thumb away from the
rest of the hand due to paralysis of thenar
muscles due to median nerve injury or polio
or leprosy

The median nerve is derived from medial and lateral cords of the brachial plexus It contains fibres from all five roots (C5-T1).
After originating from the brachial plexus in the axilla, the median nerve descends down the arm, initially lateral to thebrachialartery.

Halfway down the
arm, the nerve
crosses over the
brachial artery, and
becomes situated
medially.
The median nerve
enters the anterior
compartment of the
forearm via the
cubital fossa.

In the forearm, the nerve travels between the flexor digitorum profundus and flexor digitorumsuperficialis muscles.
The median nerve gives rise to two major branches in the forearm:
Anterior interosseousnerve
Palmar cutaneousnerve Innervates the skin of the lateral palm.

The median nerve enters the hand via the carpal tunnel, where it terminates by dividing into two branches:
Recurrent branch –Innervates the thenarmuscles.
Palmar digital branch –Innervates the palmarsurface and fingertips of the lateral three and half digits. Also innervates the lateral two lumbricalmuscles.

Motor Functions
The median nerve innervates the
muscles in the anterior forearm, and
some intrinsic hand muscles.
The Anterior Forearm
innervates muscles in the superficial
and intermediate layers:
Superficial layer: PT, PL,FCR
Intermediate layer:FDS
The median nerve also gives rise to
the anterior interosseous nerve, which
supplies the deep flexors:
Deep layer: lateral half of FDP,FPL,PQ

The Hand
Innervates some of the muscles in the hand via two branches.
The recurrent branch of the median nerve innervates the thenarmuscles
The palmar digital branch innervates the lateral two lumbricals –these muscles perform flexion at the metacarpophalangeal joints of the index and middle fingers

Sensory Functions
cutaneous innervation of part of the hand. This is achieved via two branches:
Palmar cutaneous branch – Arises in the forearm and travels into the hand. It innervates the lateral aspect of the palm. This nerve does not pass through the carpal tunnel, and is spared in carpal tunnel syndrome.
Palmar digital cutaneous branch – Arises
in the hand. Innervates the palmar
surface and fingertips of the lateral three
and half digits.

Median nerve injuries are classified as
high or low
depending on whether the lesion is
proximal or distal to the origin of the anterior
interosseous nerve in the proximal forearm.
In low injuries, the thenar intrinsic muscles
innervated by the median nerve APB
opponens pollicis & superficial head of the
FPB are paralyzed.
In high injuries in addition all flexor muscles
except FCU & medial half of FDP are involved


Thumb opposition is a complex movement requiring trapeziometacarpal joint
Abduction of the thumb from the palmar surface of the index finger
Flexion of the metacarpophalangeal joint
Internal rotation or pronation
Radial deviation of the proximal phalanx
Thumb motion toward the fingers.
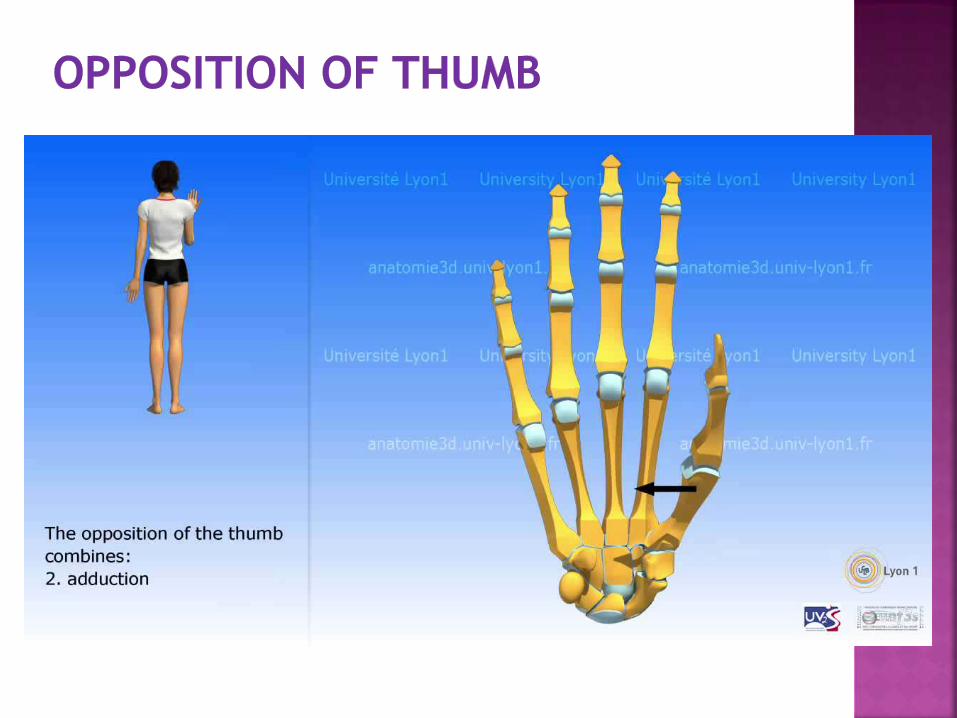

Axial thumb rotation, usually 90 degrees of
pronation and 60 degrees of supination,
occurs on the spheroid area of the saddle-
shaped trapezial articular surface
The prime muscle of thumb opposition is
the APB, although both the opponens
pollicis and FPB also produce some
opposition.

Steindler is credited with performing the
first opponensplasty in 1917.
He attached a radial slip of the FPL tendon
onto the dorsum of the base of the thumb
proximal phalanx.
To maximize thumb opposition, Bunnell
recommended passing the transferred
tendon through a pulley on the ulnar border
of the wrist so that it ran subcutaneously
across the palm to its thumb insertion

A theoretic alternative to opponensplasty is
nerve transfer, joining the anterior
interosseous nerve in the distal forearm to
the thenar branch of the median nerve,
possibly with an intervening nerve graft.

To restore thumb function properly
deformities or disabilities of thumb must be
correct preopertively

As a substitute for opposition
adduction and extension of the thumb occur as a single function in which the flexed tip of the thumb is brought against the base of the proximal phalanx of the index finger by the pull of the long thumb extensor toward Lister’s tubercle.

To pick up an object
Abduction of shoulder
Elevating the elbow
Pronation of wrist
Pinch occurs at the base of a finger
instead of at its tip

The long thumb extensor tendon, acting as an adductor, gradually migrates into the web space between the thumb and index finger
Fixed adduction and external rotational deformity of the thumb must be corrected

Dividing the fascia in the web
space between the index and
thumb metacarpals
Z-plasty of the web
Rotational osteotomy and
release of the web space
Arthrodesis of the 1 st
carpometacarpal joint
Excision of the trapezium

To restore thumb opposition functionb
satisfactorly
Tendon transfers to the
long thumb flexor
long thumb extensor
long thumb abductor may be necessary to
stabilize the thumb dynamically if the
transfer

must be expendable and strength and
potential excursion should be similar to
that of the APB and OP

If a tendon transfer does not run in a
straight line, increased force is expended
to overcome friction
True thumb opposition is best restored by
transfers that run subcutaneously across
the palm parallel to the APB muscle
All extrinsic opponensplasties should pass
around a stout, fixed pulley in the region of
the pisiform on the ulnar border of the
wrist.

In the area of the pisiform
Under or through the transverse carpal
ligament
Through Guyon’s tunnel
Around the palmar fascia
Around the PL
Around the FCU tendon

single and dual insertion techniques
In single insertion tech
Attaching the opponensplasty to the APB
insertion on the radial aspect of the thumb
MP joint---- isolated median nerve palsy
Dual insertions into the APB insertion and
either the dorsal MP joint capsule or the
thumb extensor expansion---- combined
median and ulnar nerve palsies

Abductor pollicis brevis tendon
Extensor pollicis brevis
Extensor pollicis longus
Dorsoulnar base of thumb proximal phalanx
Thumb metacarpal neck
Adductor pollicis tendon
Superficial head of flexor pollicis brevis tendon

Sublimus opponenplasty
EIP opponenplasty
Abd. Digiti mini opponenplasty
PL opponenplasty

First described by Krukenberg in 1921
Bunnel in 1924 described sublimus transfer
and emphasized and defined the role of pully
in this transfer
Thompson 1942
Riordan 1960
Brand 1966

Motor unit ring finger sublimustendon
Pulley---FCU tendon fixed pulley
Insertion site---dorsal ulnar cortex to the radial cortex of the base of the proximal phalanx

Motor unit ring finger sublimus tendon
Pulley---- distal transverse carpal ligament
ulnar border of the palmar aponeurosis
Insertion site---APB insertion site
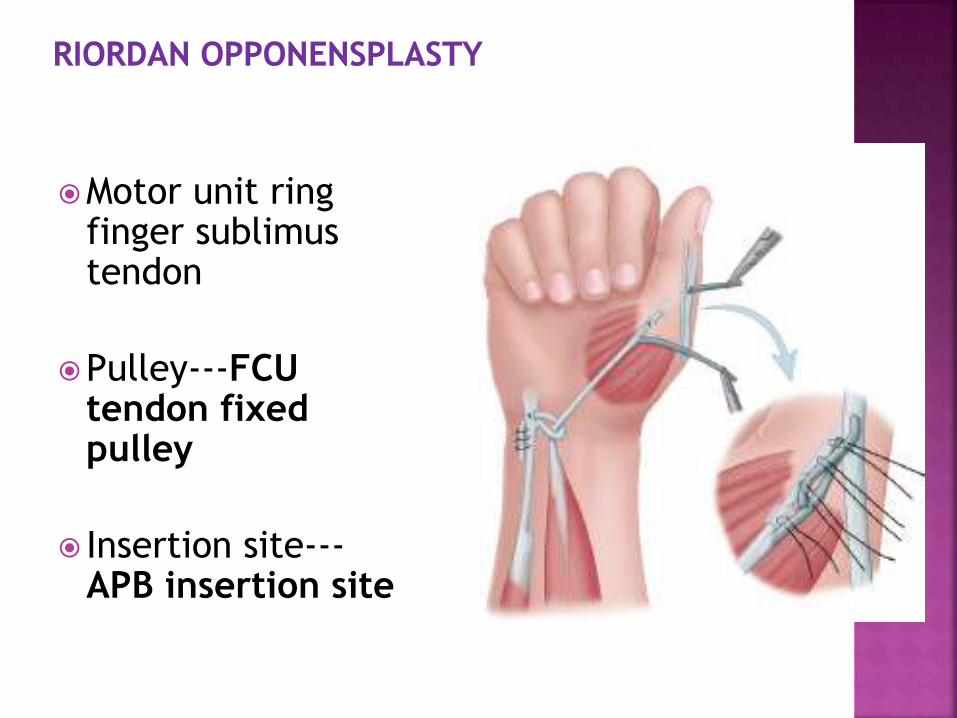
Motor unit ring finger sublimustendon
Pulley---FCU tendon fixed pulley
Insertion site---APB insertion site

Motor unit ring finger
sublimus tendon
Pulley----GUYONS canal
Insertion site----by two
slips
one into ulnar side MCP
another into APL & EPB
tendons

Described by Burkhalter
The EIP opponensplasty is popular in high
median nerve palsy and other situations in
which the ring and middle finger FDS tendons
are unavailable.
It is increasingly preferred to superficialis
transfer in low median nerve palsies because
it does not weaken grip and causes little if any
functional disability
Burkhalter W, Christensen RC, Brown P: Extensor indicis proprius opponensplasty. J Bone
Joint Surg Am 1973; 55:725-732


The ADM opponensplasty described
independently by Huber and Nicolaysen
Popularized by Littler and Cooley
Improves the hand's appearance by
increasing the bulk of the thenar
eminence.
Littler JW, Cooley SGE: Opposition of the thumb and its restoration by abductor digiti
quinti transfer. J Bone Joint Surg Am 1963; 45:1389-1484.

Littler transfer of abducto digiti quinti to restore opposition.A, Two skin
incisions.Intervening skin (shaded area) Is undermined, creating pocket to receive
transfer. B, AnatomY of abductor digiti quinti. Neurovascular bundle is located
proximally on deep surface of muscle. Muscle inserts on proximal phalanx
(1) and extensor tendon (2) of little nger. C,Origin of muscleis freed
from pisiform butnot from exor carpi ulnaris tendon. Muscle is folded
over about 170 degrees and is passed subcutaneously to thenar area, and its
two tendons of insertion(1 and 2) are sutured to abductor
pollicis brevis tendon. .

The Camitz palmaris longus opponensplasty
is a simple transfer that is usually
performed for loss of abduction and
opposition occurring as a complication of
severe carpal tunnel syndrome.

The thumb is immobilized in opposition for 3
weeks after most opponensplasties, and the
wrist should also be immobilized if the tendon
transfer crosses the flexor surface of this joint