AOTA Adaptation to Macular Escotomas in Persons With Low Vision
7
Click here to load reader
-
Upload
adelitaperez -
Category
Documents
-
view
213 -
download
1
Transcript of AOTA Adaptation to Macular Escotomas in Persons With Low Vision

Adaptation to Macular Scotomas in Persons With Low Vision
Ronald A. Schuchard
Key Words: visual perception
Persons with scotomas in their central 20° of vision of ten do not notice these blind spots within their visual field and have visual performance difficulties far exceeding what would be expected from standard vision tests. Before persons with macular scotomas can be assisted to optimally use their remaining vision for a better quality of lzfe, more must be known about how the visual system adapts to a macular scotoma. Important issues include spatial and temporal characteristics o.rperceptua/ completion and metamorphopsia, development ofpreferred retinal loci for fixation and visual search, and dynamics of the preferred retinal locus development in terms of the changes in the eye movement system, With a full understanding of the visual system's adaptation to macular scotomas, new low vision devices and training techniques can be proposed to promote independence in activities or daily living for the person with low vision.
Ronald A. Schuchard, PhD. is A,sistant Professor of Ophthalmology and Assistant Professor of Physics, University of Missouri-Kansas City, 2300 ITolmes, Kansas City, iVlissouri 641082634.
This a?-licle was accepted/or publication April 28. 1995.
I t is not uncommon to hear comments such as the folloWing from persons in a low vision rehabilitation clinical service:
•� "When] try to catch fly balls while playing baseball, the ball disappears and then reappears but not always in time for me to catch it."
•� "W11en ] look at a door or a window frame, it appears bent."
•� "W11en] look at a word or part of a sentence on a page, the letters or words to the right of where I am looking are so blurry that] cannot recognize them."
•� "] cannot seem to walk straight or walk without things hitting me; things (chairs, fences, and so forth) seem to leap out and hit me."
•� "Outdoors in the evening or when] go indoors, more of the objects (signs, faces, and so forth) become bent or blurry."
•� "My vision has not become any worse (and my physician agrees), but] cannot read as well as] did before, even with my low vision device."
These persons are probably trying to perform activities of daily living (ADL) with one or more macular scotomas (sometimes called blind spots) unknown to them or their health specialists. W11y are some persons with low vision aware that they have these blind spots, whereas others with low vision perform ADL completely unaware that their problems in visual performance are due to macular
scotomas'
Characteristics of Macular Scotomas
Macular scotomas are retinal areas with reduced light sensitivity (compared with sensitivity results of persons with normal vision) in the central 20° of the visual field. Macular scotomas are specified by the retinal location in that central scotomas are retinal areas with reduced light sensitivity involving the fovea, whereas paracentral scotomas are retinal areas with reduced light sensitivity Within the central 20° of the visual field but do not involve the fovea. Macular scotomas are further defined by the light intensity used to map out their extent. For example, dense scotomas (sometimes labeled ahsolute scotomas) are retinal areas that are insensitive to very bright objects, whereas relative scotomas are retinal areas that are insensitive to a light level relatively less than the very bright object. Most clinical services and studies of the central visual field have used standard clinical perimetry equipment (Amsler grid, tangent screen, and Humphrey Visual Field Analyzer 1). Recent results have indicated that macular perimetry with the scanning laser ophthalmoscope (SLO) is more sensitive in detecting smalllocaJizcd scotomas than standard clinical perimetry equipment (Schu
'Manufactured bv Humrhrey Instrumcnts, lnc., 2992 Alvarado Streel, San Lcandro, CA 94')77-0700,
October 1995, Volume 49, Numbe'- 9 870

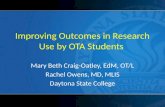
chard, 1993; Schuchard & Hu, 1994). Therefore, these small (maybe 50 and less) macular scotomas more than likely have gone undetected by health specialists in low vision rehabilitation services and investigators in studies of the central visual field. Figure 1 shows an example of these types of macular scotomas in a patient with traumatic brain injury
Macular scotomas are associated with mOSl of the common low vision medical conditions such as agerelated macular degeneration, diabetic retinopathy, and glaucoma, as well as less common medical conditions such as postchiasmal central nervous system disorders. In a typical low vision rehabilitation service, 83% of patient eyes were found by SLO macular perimetry to have dense macular scotomas present in the central visual field (Fletcher, Schuchard, Livingstone, Crane, & Hu, 1994) This prevalence of den~e macular scotomas is nearly equal to the 80% of patient eyes found bv SLO macular perimetry to have dense macular scotomas in a low vision research study (Schuchard. 1993). Fewer than half of these research subjects with low vision were documented, either by their referring clinician or Jow vision specialist, as haVing macular scotomas. Central scotomas, with a wide range of acuities, were found in 40% of the research subjects, whereas 50% of the J1atients with macular scotomas had central scotomas. Paracentral macular scotomas with no central scotoma (and thus often with fairly good acuity) were additionally found III 40% of all the research subjects, whereas 50% of patients with macular scotomas had paracentral macular scotomas. In the low VIsion rehabilitation study (Fletcher et aI., 1994), only 169'0 of the patients with macular scotomas had scotomas of less than 50 in size. Most of the persons with macular scotomas (84%) referred to the low vision rehabIlitation ~ervice had scotomas greater than 50 in size that ~ubstantially affected their ADL. We may never know the true prevalence of macular scotomas in the general population: many per
sons may have scotomas less than 50 in size and never know about them. Regardless, the prevalence of persons with low vision who have macular scotomas (especially paracentral scotomas because central scotomas are easier to document) is considerably greater than suspected by most low vision specialists.
Perception With a Macular Scotoma
One would think that persons with low vision would see black holes where their macular scotomas fall in the central visual field if the visual system was not able to adapt to
macular scotomas. Instead, recent research has shown that the visual system has a great capacity to adapt to macular scotomas (Ramachandran, 1.992; Schuchard, 1993, 1995) Thu~. most persons with macular scotomas do not perceive a black ~pot in the visual field where the scotoma is located. Persons with normal vision do nOI perceive a black spot when viewing the visual world with one eye closed. Figure 2 demonstrates both the phenomena of having smaJJ objects jumping into and out of view and of larger object~ alway~ being in view withoUl gars, which shows thai even persons with normal vision do nor perceive a black spot in the visual field where the scotoma is located
In another example, scotomas from laser treatments of retinal diseases are ~ometimes deSCrIbed by patients as "large black spot~" or "bouJders," but over a period of months, these spots fade and can no longer be localized without macular penmetry testing. Even when persons with low vision 31-e continuously aware of theIr scotomas, the visual world does not fall into a "black hole"; rather, these persons often see 3 blurry, hazy, dark or light area and a smaller blind spot size than the actual scotoma size (Sch uchard, 1993)
The mapping of object space into perceptual space by observers with a scotoma can include warping or
TSf)�
Figure 1. Annotated SLO pictures of a patient with traumatic brain injury showing dense scotomas (OS), threshold scotomas (TS), and preferred retinal locus (PRL, white cross). Persons can have a variety of scotoma characteristics mcludmg a Simple central scotoma in the foveal area with 20/15 visual acuity (Figure 1a) and a ring scotoma with 20/40 visual acuity where the PRL is surrounded by dense scotoma (Figure 1b).
Tbe American]ournal oj" Occupa/lonal Tbempr 871

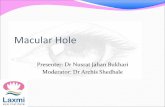
+ •� Figure 2. First hold the text of this paper close to your right eye with your left eye closed. Look at the first word, at the very left, of a line of text in the middle of the page. Notice that the words to the right may appear blurry and unreadable, but there are no words missing and no gap in the text. Next look at the cross in this figure with your right eye, again with your left eye closed. Move the cross closer and further from your right eye and notice that the dot disappears and then reappears. The dot is moving into and out of your physiological blind spot and cannot be "seen" by the visual system.
sewing-up (metamorphopsia) or both, as well as filling in (perceptual completion). Metam01phojJsiu is defined as a perception in which objects appear distorted or larger or smaJler than their actual size. Perceplual comple/ion is defined as a perception in which objects appear complete or filled in, without missing visual information, when part of the object falls in a scotoma. Even though perceptual completion has been documented in observers with scotomas, perceptual completion across SCOtomas is a poorly understood phenomenon. Perceptual completion of uniform surrounding fields has been documented with artificial scotomas (Gerrits, De Haan, & Vendrik, 1966; Ramachandran & Gregory, 1991), physiological blind spots (Schuchard, 1993; Sergent, 1988), and macular scotomas (Craik, 1966; Gerrits & Timmerman, 1969; Schuchard, 1993). Perceptual com pletion of si mpie geometric objects (such as lines and crosses) has been documented with physiological blind spots (Schuchard, 1991; Sergent, 1988) and macular scotomas (Craik, 1966; Schuchard, 1991). However, a lack of perceptual completion has been reported in observers with macular scotomas (Gerrits & Timmerman, 1969; Schuchard, 1991).
Craik (1966) documented his perception with a 1° central scotoma that had been produced by fLxa[jng the noonday summer sun with the right eye for a period of 2 min. SeveraJ days later, he reported that the scotoma was subjectively filled in with the prevailing color of the border around the scotoma such thal the scotoma nearly escapcd notice Only a cloudiness, visible in both monocular and binocular vision, occasionally called attention to the scotoma. Small black objects or moderately bright points subtending less than 20 min. ofarc were completely invisible when in the scotoma. Thin wires appeared with a gap as if broken. However, thicker rods were filled
in across the scotoma, although the thick rods were perceived to have a somewhat smaller thickness and less precise edges than when seen away from the scotoma. RcmarkabJy, this report is probably the most complete
documentation of perceptual Completion development in a person adapting to a macular scotoma. Other reports show perceptual completion with cortical scotomas, but even in this literature, there is disagreement as to whether perceptual completion or uncontrolled experimental factors like poor fIxation stability are actually producing the perception of complete objects (Sergent, 1988). As earlyas 1941, the filling in of physiological blind spots and of scotomas was thought to represent some intrinsic organizing function of the cortex (Lashley, 1941). Recent studies have indicated that filling in occurs extraretinally by interpolation of the visual information from the borders of the scotoma (Gerrits & Timmerman, 1969; Piantanida, 198'); Ramachandran & Gregory, 1991; Spillmann & Kurtenback, 1992) Perceptual completion can be regarded as a type of visual ilJusion (as a perception that does not represent the character of an object or a misconception of a sensory impression) (Gassel & Williams, 1963). For example, persons with normal vision will perceive edges or borders where no contrast exists (see Figure 3),
Persons with low vision can have different perceptions depending on the expected visual target. Figure 4 shows examples of letters placed briefly over macular scotomas with an SLO. Jfrold before the presentation that they will be seeing geometric objects (Jines, circles, and so forth), persons with low vision wilJ report that they see two parallel lines (for the H) and a cone or upside-down V (for the A). However, if told beforehand that they will he presented with letters, these same persons wilJ almost always report thal they see a complete H (with no breaks or irregularities) and then an A. Thus, the expected visual target plays an important part in the visual perception of persons with macular scotomas, as it cloes for persons with normal vision who can be tricked into diffcrent visual perceptions by visual illusions.
Preferred Retinal Loci With Central Scotomas
In an eye with a central scotoma, the development of one or more eccentric preferred retinal loci (PRL) naturally and reliably occurs (Culham, Fitzke, Timberlake, & Mar
shall, 1993; Cummings, Whittaker, Watson, & Budd, 198'); Fletcher et aI., 1994; Guez, Francois, Rigauclicre, & O'Regan, 1993; Schuchard, 1993; Schuchard & Fletcher, 1994; Schuchard & Raasch, 1992; Timberlake et aI., 1986; Timberlake, Peli, Essock, & Augliere, 1987; White & Bedell, 1990; Whittaker, Budd, & Cummings, 1988; Whittaker & Cummings, 1986). The term PRL is normally reserved for those persons whose visuaJ system has chosen an eccentric retinal area to act as a pseudofovea for visual tasks that were performed with the fovea, The mechanisms
October 1995. Vo/ume 49. Number 9 872

a b
7c v
Figure 3. Examples of illusionary contours. Notice that there is a strong perception of a contrast edge or shape (white bar in Figure 3a and white triangle in Figure 3b) even where no contrast exists (white on white).
that decide the specific retinal location or the time course for PRL development have not been discovered. Regardless, the retinal location of PRL relative to the macular scotoma, and thus the position of gaze relative to the blind spot, is often critical for success of visual performance in persons with macular scotomas. Even the relative location of paracentral macular scotomas to the fovea can have drastic consequences for ADL. For example. persons with ring scotomas can have very poor reading rates (Plas, Fletcher, & Schuchard, 1995). In a typical low vision rehabilitation service, 51% of eyes were found to have the PRL to the left or right of a macular scotoma. These persons typically cannot see ahead or scan hack to the beginning of a line while reading.
The only accurate means for determining the location of the PRl relative to macular scotomas, the physiological blind spot, or any other retinal landmark is to use a device like the SLO. For example, although one might think that, because the acuity is relatively poorer, the PRJ. is relatively farther away from the nonfunctioning fovea, the eccentric retinal location of the PRL cannot be determined by visual acuity alone (Schuchard & Raasch, 1992).
The PRL ability, besides the PRL retin31 characteristics, has profound effects on ADL. In an eve with a functioning fovea (for example, paracentral scotoma), ,Fxation is the act of directing the eve toward the visual object of regard, causing the image of the object to be within the fovea. Eccentric/ixation refers to fixation performance in which the person has the sensation of looking directly at the visual object during fixation with the eccentric PRL. Eccentric viewing, on the other hand, re
fers to fL'(ation performance in which the person has the sensation of looking above, below, or to either side of the object during fL'(ation with the fovea or PRL. A shift from the fovea to an eccentric PRL in the perception of looking directly at an object is possible in persons with bilateral central scotomas (Schuchard & Raasch, 1992; White & I3edeiL 1990) In a similar manner, the fovea or PRL controls large eye movements. How well the PRJ. develops should predict the ability fOt" the person with a central scotoma to successfully perform ADL involving eve movements (slIch as fIXation and visual search). When persons with low vision are asked to fixate (look directly at) small objects. they may use different retinal locations and therefore exhibit multiple PRls. These persons with low vision may not even be con~ciously aware that they are looking at small objects such as words with different retinal locations. These different retinal locations can have different acuity capabilities as weJl as contrast and other visual function capabilities. When asked to keep their fIXcltion on a small object (fixation stabilitv), persons with Jow vision will often use a retinal area that is much larger than that usecl by a normally sighted person. The SLO has shown that persons with low vision can have PRl as small as that of persons with normal vision (1°_2°) and as large as 9°.
Persons with low vision mllst use their PRl when searching for objects during scanning Or other eye movements. \X!hen asked to follow or track a moving object, the person with low vision may have difficulty if the object is moving into the macular scotoma. Additionally, the macular scotoma may inhibit their visual search capabilities
The American journal 01' Occu/Jalional 'lbera/JI' 873

Figure 4. Illustration of two letters, H and A, projected onto the retina so that the images of the cross bars of both letters (black pattern) are falling into the dense macular scotomas (gray pattern). Persons with low vision can report two different perceptions - two parallel lines or an H versus an upside-down V or an A, depending on what type of object the person with low vision is expecting to see.
when these persons make large eye movementS (saccadic eye movements) to focus on a new point of interest. The ability of persons with low vision to use their PRl for fixation stability, pursuit, and saccadic eye movements has been found to be more highly correlated to reading rate than to other visual test results (Fletcher, Schuchard, Warren, Crane, & Lashkari, 1993). In addition, the existence of a macular scotoma, at any retinal location, always delayed the identification of objects during a visual search task (Schuchard & Fletcher, 1994). Persons with central
scotomas have heen found to place the center of a large object at their PRL, even when verbal instructiom were given to place the center of the large object at their nonfunctioning fovea (Schuchard & Raasch, 1992; White & Bedell, 1990).
Up to this point, the discussion of PRls has ignored the fact that persons with low vbion exist in a binocular visual world, whereas most of the concepts of the PRl have been developed monocularly. In a study investigating binocular correspondence, 80% of the 67 subjects saw objects with only one eye (monocular perception) while performing a simple free viewing binocular visual task (Schuchard, Tekwani, & Hu, 1995). However, this study does not conclude that the subjects are seeing the world with only one eye. The task was to fixate small visual targets at the PRllocation. Subjects reported seeing the world with both eyes, although not always appreciating that, when looking at a small object (such as a number, letter, or word), the small object was only seen by one eye. Previous studies of PRL abilities in eye movements (Schuchard & Fletcher, 1994; Whittaker & Cummings, 1986; Whittaker & Cummings, 1990; Whittaker, Cummings, & Swieson, 1991) have used similar tasks. Typically, the subject is asked to fixate, saccade to, or follow a small object. The eye used by the visual system in binocular tasks may be the dominant eye, whereas the fellow eye is actually following the lead of the dominant eye in eye movement and other visual tasks. Therefore, the poor results in the aforementioned PRl studies may be due to forcing the fellow eye to perform eye movement tasks without the dominant eye. The study by Schuchard et a!. (1995) implied that the visual system does not (cannot?) tvpically retain binocular correspondence because only 20% of the subjects saw the object with both eyes (one subject retained binocular perception with anomalous retinal correspondence). This lack of binocular correspondence has dramatiC implications for persons with low vision in ADL, possibly including the loss of visual function such as depth perception from disparity and rivalry, diplopia, or suppression instead of fusion when viewing binocular objects.
ADL and Macular Scotomas
Clearly the visual system has a great capacity for plasticity in adapting to macular scotomas. Persons can adapt to
central blind spots by developing PRLs to perform foveal tasks (such as fixation and reading) on eccentric retinal areas. This adaptation may occur without the conscious knowledge of the person with low vision and may nOt be detected by the low vision specialist. Thus, the person with low vision may experience strange or unusual visual sensations during ADI.. What are the possible visual circumstances that could lead to the comments by persons with low vision stated at the beginning of the article?
October 199'5, Volume 49. Number 9 874

"When I Try to Catch Fly Balls While Playing Baseball, the Ball Disappears and Then Reappears but Not Always in Time for Me to Catch It. "
Persons with small paracentral scotomas often have good acuity with small blind spots just above the fixation location in the visual field. Balls or other small objects flying in the air that are in the visual field corresponding to the macular scotoma cannot be seen until the image falls on healthy retina. Because the person does not see a black hole, there is no perception of a hole in his or her vision. Thus objects appear to dance into and then out of view, without any understanding of why this perception is occurring.
"When 1 Look at a Door or a Window Frame, It Appears Bent. "
A person with similar visual field conditions as described for the balls can look at large objects and "see" the whole object. However, if the person cannot fully adapt to the macular scotoma, or the macular scotoma is toO large for the perceptual completion mechanisms to successfully fill in the visual information, the perception of the large object can be distorted. This perception is especially noticeable when the object has straight edges that the person with low vision knows should be uniform straight lines.
"When 1 Look at a Word or Part of a Sentence on a Page, the Letters or Words to the Right of Where 1Am Looking Are So Bluny That J Cannot Recognize Them."
Persons with a central scotoma to the right of the PRL or with a paracentral scOtoma immediately to the right of the fovea may not be aware of the blind spot caused by the sCotuma. The perceptual completion process naturally fills in the type of visual information that is expected (letters or words), but the visual system will not know the specific information that is at the spatial location of the scotoma. Thus the perception is often of blurry objects with no gap that are generally correct but without specific visual information. For example, the person perceives a blurry unrecognizable letter or word because the specific letters or words inside the scotoma cannOt be "seen" by the visual system.
"I Cannot Seem to Walk Straight or \Valk Without Things Hitting Me; Things (Chairs, Fences, and So Forth) Seem to Leap Out and Hit Me "
Persons with a central scotoma to the right or left of the PRIor persons with a paracentral scotoma to the right or left of the fovea may have large scotomas without an appreciatiun of the true extent of the blind Spot. Thus,
The American Journal Of Occupatiunal Therapv
the perceptual completion process will fill in the edge of the blind spot that gives the perception that the path is clear, whereas in reality the chair that is just inside the blind spot is not seen until the last second, when the image of the chair falls on healthy retina outside of the scotoma.
"Outdoors in the Evening or When I Co Indoors, More of the Objects (Signs, Faces, and So Forth) Become Bent or BlunJ!. "
Because relative scotomas are often larger than dense scotomas, the blind spot will suddenly become bigger when the person with a macular scotoma moves from the outdoors or any other well-lit environment ro a dimly lit environment. Thus the light level of the environment can change the visual perception and exacerbate difficulties in ADL for the person with low vision.
"MY Vision Has Not Become Any \Xlorse (and My Physician Agrees), but 1 Cannot Read as Well as 1Did Before, Even With Jl!~y Low Vision Device. "
Unfortunately, macular scotomas can increase in size with the progression of many macular diseases, but this increase in the blind spOtS may not change the results of other vision tests. For example, a ring scotoma could substantially increase in size without affecting the center of the ring (the fovea), and thus visual acuity and contrast sensitivity would remain relatively unchanged. This change in size of the macular scotoma may nor be detected by the low vision specialist, and thus the patient is left wondering what, besides a vision change, is causing the increased difficulties in ADL.
Conclusion
Persons with macular scotomas have visual performance difficulties far exceeding what would be expected from standard vision tests Before professionals can assist these persuns to optimally use their remaining vision for a better quality of life, we must know how the visual system adapts to a macular scotoma. Questions worth investigating are: (a) What are the limitations of the visual system's plasticity in adapting to macular scotomas' (b) Why do only some persons develop PRL with relatively good ability? (c) Is there one PRL for all visual tasks or ADL? (d) Does the ability of the PRL in visual tasks predict rehabilitation potential? Because potentially four of five persons with low vision are performing ADL with macular scotomas, only when the answers to these types of questions are found anel made available to low vision specialists, including occupational therapists, will these persons have thorough low vision rehabilitation care.•
875

References
Craik, K. J W. (1966). Tbe nature of psycbologv. Cambridge, United Kingdom: University Pres~.
Culham, L. E, Fitzke, F W., Timberlake, G L & Marshall.J
(1993). Assessment of fIXation stability in normal ~ubjects and patients llsing a scanning laser ophthalmoscope. Clinical Vision Sciences, 8, 551-56l.
Cummings, R. W., Whittaker, S. G.. Watson, G. R., & Budd, ]. M. (1985). Scanning characters and reading with a central scotoma. American Journal of OptometlJI and Physiological Optics, 62, 833-843
Fletcher, D. C, Schuchard, R. A., Livingstone, C L., Crane, W. G., & Hu, S. Y. (1994). Scanning laser ophthalmoscope (SLO) macular perimetry and applications for low vision rehabilitation clinicians. In A. Colenbrander & D. C Fletcher (Eds.), Low vision and vision rehabilitation. Opbtbalmology Clinics of North America (Vol 7, pp. 257-265). Philadelphia: Saunders.
Fletcher, D. C, Schuchard, R. A., Warren, M. L., Crane, W. G., & Lashkari, K. (1993). A scanning laser ophthalmoscope preferred retinal locus scoring system compared with reading speed and accuracy. investigative Opbthalmology & Visual Science, 34, 787.
Gassel. M. 1'.1., & Williams, D. (1963). Visual function in patients with homonymous hemianopia. Part Ill. The completion phenomenon; insight and attitude to the defect; and visual functional efficiency. Brain, 86, 229-260.
Gerrits, H.]. I'vl., De Haan, B., & Vendrik, A]. H (1966) Experiments with retinal stabilized images: Relations between the observations and neural data. Vision Research, 6, 427-440.
Gerrits, H.]. 1'.1., & Timmerman, G. J. M. E N. (1969). The filling-in process in patients with retinal scotomata. Vision Research, 9, 439-442.
Guez,]. E, Francois,]. F., Rigaudiere, F., & O'Regan,]. K. (1993). Is there a systematic location for the pseudo-fovea in patients with central scotoma' Vision Researcb, 33, 1271-1279.
Lashley, K. S. (1941). Patterns of cerebral integration indicated by the scotomas of migraine. Archives ofNeurology and PsycbiatlJ!, 46, 331-339
Piantanida, T P. (1985). Temporal modulation sensitivity of the blue mechanism: Measurements made with extraretinal chromatic adaptation. Vision Research, 25, 1439-1444.
Plas, R., Fletcher, D C, & Schuchard, R. A. (1995). Ringshaped macular scotomata Effects on actiuities ofdailv liuing. Manuscript submitted for publication.
Ramachandran, V. S. (1992). Blind Spots. SCientific Amen'can, 266, 86-91
Ramachandran, V. S., & Gregory, R. L. (1991). Perceptual filling in of artificially induced scotomas in human vision. Nature, 350, 699-702
Schuchard, R. A. (1991). Perception of straight Jine objects
A UPDATE�
across a scotoma inuestigatiue Opbthalmology & Visual Science. 32. 816.
Schuchard. R. A. (1993). Validity and interpretation of Am~ler grid reports. Arcbiues ofOphthalmology, 111, 776-780.
Schuchard, R. A (1995) Perception of simple objects across natural and artificial scotomas. Manuscript submitted for publication.
Schuchard, R. A, & Fletcher, D. C. (1994). Preferred retinal locus: A review with applications in low vi~ion rehabilitation. In A. Colenbrander & D. C. Fletcher (Eds.), Low vision and vision rehabilitation. Opbtbalmology Clinics ofNorth America (Vol 7, pp. 243-256). Philadelphia: Saunders.
Schuchard, R. A., & Hu, S. Y (1994). Macular perimetry: Static perimetry compared to fundus perimetry. Vision Science and its Applications (OSA Tecbnical Digest Series), 2, 262-265.
Schuchard, R. A., & Raasch, T. W. (1992). Retinal locus for fixation: Pericentral fLxation targets. Clinical Vision Sciences, 7, 511-620.
Schuchard, R. A., Tekwani, N., & Hu, S. Y. (1995). Binocular preferred retinal loci: Relationship of visual factors to binocular perception. Vision Science and its Applications (OSA Technical Digest Series), 1, 332-335.
Sergent,]. (1988). An investigation into perceptual completion in blind areas of the visual field. Brain, 111, 347-37 3.
Spill mann, L., & Kurtenback, A (1992). Dynamic noise backgrounds facilitate target fading Vision Research, 32, 19411946
Timberlake, G. T., Mainster, M. A, Peli, E., Augliere, R. A, Essock, E. A, & Arend, L. E. (1986). Reading with a macular scotoma. 1. Retinal location ofscotoma and fIXation area. investigative Ophtbalmology & Visual Science, 27, 1137-1147
Timberlake, G. T., Peli, E" Essock, E. A, & Augliere, R. A. (1987). Reading with a macular scotoma. Ii. Retinal locus for scanning text. investigative Ophtbalmology & Visual Science, 28, 1268-1274.
White,]' M., & Bedell, H. E (1990). The oculomotor reference in humans with bilateral macular disease. inuestigative Opbtbalmology & Visual Science, 31(6), 1149-1161
\X!hittaker, S. G., Budd,]. 1'.1., & Cummings, R. W. (1988). Eccentric fixation with macular scotoma. investigative Ophthalmologv & Visual Science, 29, 268-278.
Whittaker, S. G., & Cummings, R. W. (1986). Redevelopment of fIXation and scanning eye movements following the loss offoveal function In S. R. Hilfer &]. B Sheffield (Eds.), Development of order in tbe visual system (pp. 175-191). New York: Springer-Verlag.
Whittaker, S. G., & Cummings, R. W. (1990). Foveating saccades. Vision Research, 30, 1363-1366.
Whittaker, S. G., Cummings, R. W, & Swieson, L. R. (1991). Saccade control without a fovea. Vision Research, 31, 22092218
Coming in Novelnber/December AOTA ArchivatIssue
• Official documents
• 1995 Eleanor Clarke Slagle Lecture
• Listing of Educational Programs in Occupational Therapy
• Stereotypes, stigma, and mental illness
Turn to AJOT for the latest information on occupational
therapy treatment modalities, aids and eqUipment, legal and
social issues, education, and research.
Octoher 1995, Volume 49, Number 9 876