
ANZONA Conference 2013
18
Atypical Femoral Fracture ANZONA Conference 2013 “Racing to the Challenge” Anita Taylor, ONP, RAH Cheryl Kimber, ONP, FMC
Transcript of ANZONA Conference 2013

Atypical Femoral Fracture
ANZONA Conference 2013 “Racing to the Challenge”
Anita Taylor, ONP, RAH
Cheryl Kimber, ONP, FMC

Overview
• Aetiology
• Case Series
• Case Study 1&2 - RAH
• Case Study 3&4 - FMC
• Patient Education
• Implications for Practice

Aetiology • Incidence
– Estimated to be 7̴8 cases in 100 000 patients taking oral bisphosphonates
(Yil 2013 quoting Dell et al 2010)
– 1 per 1000 per year (Rizzoli et al, 2010)
• Risk Benefit – Fracture prevention whilst on
bisphosphonates 1/100 (Rizzoli et al, 2010)
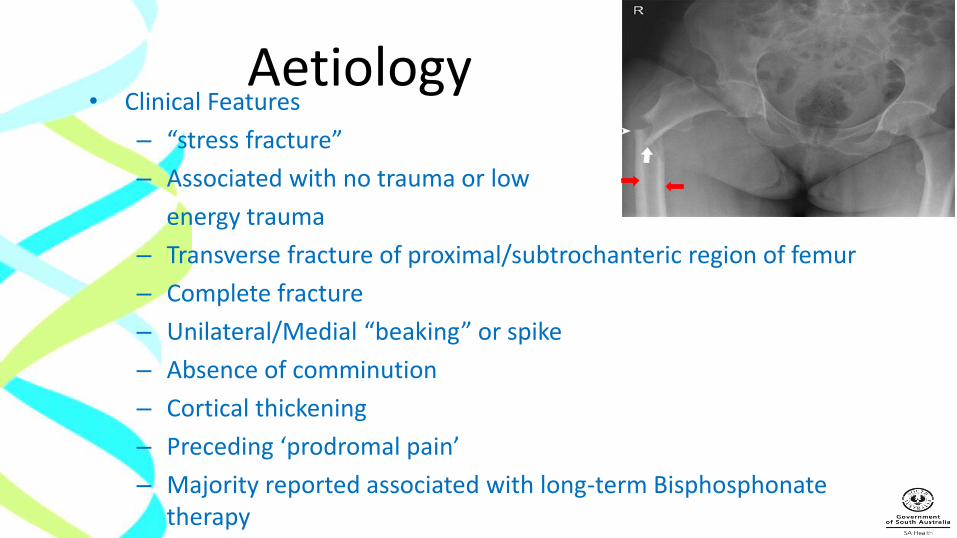
Aetiology • Clinical Features
– “stress fracture”
– Associated with no trauma or low
energy trauma
– Transverse fracture of proximal/subtrochanteric region of femur
– Complete fracture
– Unilateral/Medial “beaking” or spike
– Absence of comminution
– Cortical thickening
– Preceding ‘prodromal pain’
– Majority reported associated with long-term Bisphosphonate therapy

Why-Bisphosphonates?
• Increase bone strength and decrease fracture risk by suppressing excessive bone remodelling/turnover
• However - reduction remodelling associated with increased micro damage accumulation as cracks are not removed efficiently
• Similar age related reductions in bone turnover – increase micro damage accumulation
• BPs may exacerbate damage accumulation • Impair targeted remodelling → extent that remodelling not
targeted to damage repair • Allowing micro damage to persist for longer compared with
untreated bone

Case Series Design: • Retrospective review from January 2011 – June 2013: a
30 month period
Setting • 2 Level 1 Trauma Centres in Adelaide region
Sample • RAH n= 11; N= 88 (60+yrs) N=21 (50-60yrs)
0.5% of ALL SOF# • FMC n= 5; N= 31 (60+yrs) N=34 (50-60yrs)
0.14% of ALL SOF#

RAH Sample

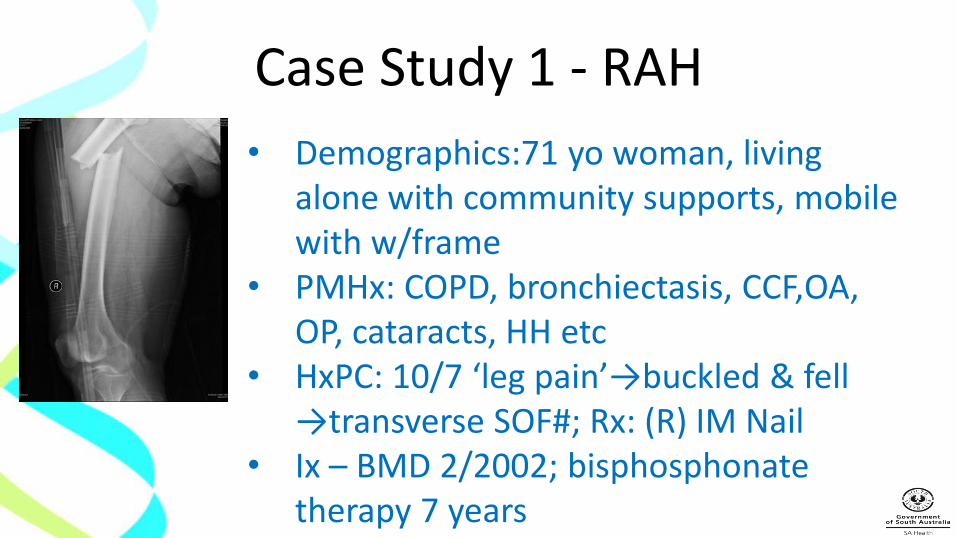
Case Study 1 - RAH
• Demographics:71 yo woman, living
alone with community supports, mobile with w/frame
• PMHx: COPD, bronchiectasis, CCF,OA, OP, cataracts, HH etc
• HxPC: 10/7 ‘leg pain’→buckled & fell →transverse SOF#; Rx: (R) IM Nail
• Ix – BMD 2/2002; bisphosphonate therapy 7 years

Case Study 2 - RAH • Demographics: 88yo male living alone, 4WW,
drives car, MOW, cleaning & podiatry, ACAT-LLOC
• PMHx: prostate Ca(Androgen), HT, CCF, GORD, AF(Dabigatran), mild AR & MR, OP, glaucoma etc
• HxPC: Fell visiting wife in NH→(L)LGN. c/o (R)hip & thigh pain→distal femur →nil fall
• Ix – CT(R)hip; Bone tumour opinion; BoneBx
• Rx:(L)LGN & (R)LGN for contra-lateral, atypical subtrochanteric femoral # sustained in-hospital.
• Orthogeriatric opinion: “bisphosphonate related atypical #’s (seems likely) …”
FMC Sample

Case Study 3 - FMC • 68 yr lady, very mobile • PMHx – breast Ca + radiotherapy, NIDDM, HTN,
Osteoporosis • HxPC: bumped by friend and fell “heard crack” • Shortened leg, pain • Alendronate 14 yrs Management • Surgery: Long IM nail • Bone biopsy • Ceased Bisphosphonate, commenced strontium


Case Study 4 - FMC • 2013
• Trip fall - fracture
• Bone density -1.7 (2012)
• Back on alendronate as strontium caused reflux?
• Management - IM Nail, strontium ranelate and referral to endocrinologist

Patient Education In addition to usual discharge advice: post- operative care & follow up, bone health, falls risk minimisation etc. • Bisphosphonate use: dental care, ONJ • Immediate review of pain in hip, thigh or femur:
“typically sharp, well-localized to the mid or upper thigh, for several weeks to months prior to the fracture” (Yil 2013 quoting Giusti et al 2010)
• Discuss bisphosphonate cessation/‘drug holiday’ with medical officer/pharmacist
• Co-morbid conditions- Vitamin D deficiency, RA, hypophosphatasia, glucocorticoids
Implications for Practice
• Nurse awareness
• Identify risk factors amongst this in-patient population
• Standard definition of fracture type is required
• Research: Larger & longer studies to gather more information about this phenomenon
• International collaboration

Summary • Atypical femoral fractures are rare
• May be associated with long term bisphosphonate use
• Benefit of bisphosphonate for fracture prevention outweighs risk
• Subtrochanteric # is an expected finding in patients with osteoporosis
• Nursing awareness and knowledge is important
• Ongoing research is needed

References • Black,D., Kelly, M, Genant, M. et al, Bisphosphonates and Fractures of the
Subtrochanteric or Diaphyseal Femur, The New England Journal of Medicine 2010, May13, pp1761-71
• Neviaser, Lane, Lenart, Folorunsho Edobor-Osula, Lorich. Low-Energy Femoral Shaft Fractures Associated With Alendronate Use. Journal of Orthopaedic Trauma, 2008;22(5):346–350.
• Rizzoli, Akesson, Bouxsein, Kanis, Napoli, Papapoulos, Reginister, Cooper. Subtrochanteric fractures after long-term treatment with bisphosphonates: a European Society on Clinical and Economic Aspects of Osteoporosis and Osteoarthritis, and International Osteoporosis Foundation Working Group Report. Osteoporosis International, 2010. DOI 10.1007/s00198-010-1453-5. Available from Source URL:
http://www.iofbonehealth.org/iof-and-esceo-issue-position-paper-atypical-femoral-fractures-and-long-term-bisphosphonate-use
• Yil Ryun Jo,Hye Won Kim,Seock Ho Moon,Young Jin Ko. A Case Report of Long-Term Bisphosphonate Therapy and Atypical Stress Fracture of Bilateral Femur. Annals of Rehabilitation Medicine, 2013;37(3):430-432. pISSN: 2234-0645. eISSN: 2234-0653. http://dx.doi.org/10.5535/arm.2013.37.3.430


















