Antimicrobial Therapy David H. Spach, MD Professor of Medicine Division of Infectious Diseases...
51
Antimicrobial Therapy David H. Spach, MD Professor of Medicine Division of Infectious Diseases University of Washington, Seattle
-
Upload
bruno-blair -
Category
Documents
-
view
237 -
download
2
Transcript of Antimicrobial Therapy David H. Spach, MD Professor of Medicine Division of Infectious Diseases...

Antimicrobial Therapy
David H. Spach, MDProfessor of Medicine
Division of Infectious DiseasesUniversity of Washington, Seattle

Use of Antimicrobials
• Treat Infections
• Prevent Infections
• Cost
• Resistance

Antibiotic Use and Resistance
Community Use
Hospital Use
Agricultural Use

Antibiotic Use and Resistance
Community Use
Hospital Use
Agricultural Use

Antibiotic Resistance
Antibiotic Development

Infectious Diseases
36. Tamiflu
60. Zostavax
77. Truvada
84. Norvir
97. Atripla
2014 Most Prescribed Drugs
Source: IMS National Prescription Audit, IMS Health.

Infectious Diseases
15. Atripla (HIV)
22. Truvada (HIV)
32. Solvaldi (Hepatitis C)
49. Prezista (HIV)
51. Isentress (HIV)
59. Reyataz (HIV)
71. Prevnar 13 (Vaccine)
75. Stribild (HIV)
81. Zyvox (Antibacterial)
84. Complera (HIV)
87. Gardasil (Vaccine)
88. Zostavax (Vaccine)
93. Cubicin (Antibacterial)
97. Viread (HIV)
2014 Most Profitable Drugs
Source: IMS National Prescription Audit, IMS Health.

Source: IDSA. Clin Infect Dis. 2010:50:1081-3.

Source: IDSA. Clin Infect Dis. 2010:50:1081-3.
“Our audacious but noble aim is the creation of a sustainable global antibacterial drug R&D enterprise with the power in the short-term to develop 10 new, safe, and effective antibiotics by 2020.”

“ESKAPE” Pathogens
· Enterococcus faecalis
· Staphylococcus aureus
· Klebsiella pneumoniae
· Acinetobacter baumannii
· Pseudomonas aeruginosa
· Enterobacter species

Structure of Gram-Positive Bacteria
Cell WallCell Membrane
Penicillin Binding Proteins
DNA
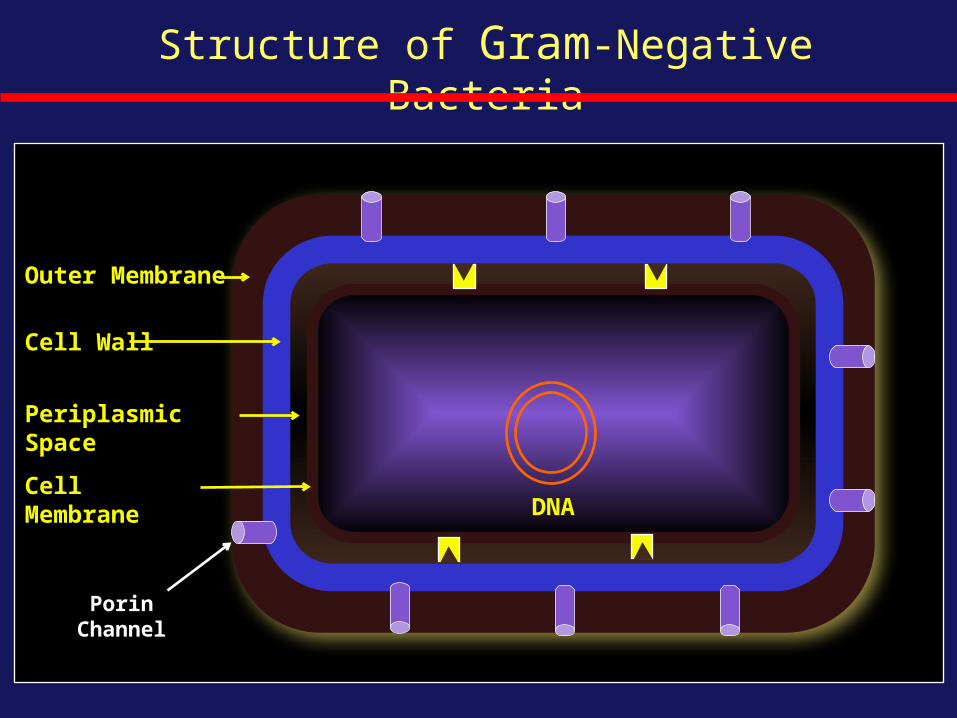
Structure of Gram-Negative Bacteria
Porin Channel
Outer Membrane
Cell Wall
Periplasmic Space
Cell MembraneDNA

Antimicrobials: Site of Action
Cell Wall
Cytoplasm 23 S Ribosome 30S Ribosome 50S Ribosome
DNA Inhibitor
Cell Membrane

Systemic Antibacterials: Recent FDA Approvals
· 2009 -Telavancin (Vibativ): SSTI
· 2010- Ceftaroline (Teflaro): SSTI, CAP
· 2011- Fidaxomicin (Dificid): Clostridium difficile
· 2013- Telavancin (Vibativ): HAP/VAP
· 2014 Tedizolid (Sivextro): SSTIDalbavancin (Dalvance): SSTIOritavancin (Orbactiv): SSTI

Telavancin (Vibativ)

Telavancin: Mechanism of Action
Cell Wall SynthesisTelavancin
DNA

Telavancin: Mechanism of Action (1)
Ligase
Tripeptide Intermediate
Cell Wall Pentapeptide Precursor
Telavancin
D-Ala D-Ala
D-AlaD-Ala
D-Ala D-Ala

Telavancin: Mechanism of Action (2)
Telavancin
Lipid II(cell wall precursor)

· FDA Status: approved for SSTI 2009, HAP in 2013
· Clinical Indication: 1) complicated SSTI caused by gram-positive bacteria (MSSA, MRSA, S. pyogenes, S. agalactiae, S. anginosus group, E. faecalis)2) VAP and HAP caused by MSSA or MRSA
· Mechanism: Lipoglycopeptide vancomycin semisynthetic derivative --inhibits cell wall synthesis and binds to membrane lipid II molecules
· Dosing: 10 mg IV q24 hours
· Dose Reduction: - For CrCl 30-50: 7.5 mg/kg q24 - For CrCl 10-30: 10 mg/kg q48
· Adverse Effects: nephrotoxicity, diarrhea, “red man”, foamy urine
Telavancin (Vibativ)
Source: Damodaron SE, Madhan S. J Pharmacol Pharmacother. 2011;2:135-7.

Telavacin versus Vancomcyin for Complicated SSTIATLAS Trial
· Methods (N = 1867) - Two Phase 3 trials- Randomized, double blind - Patients with complicated SSTI- Suspected or confirmed gram+- N = 579 with MRSA - Adults
· Regimens - Telavancin: 10 mg/kg IV q24h - Vancomycin: 1g IV q12h
Study Design Overall Success Rate*
Source: Stryjewski ME, et al. Clin Infect Dis. 2008;46:1683-93.
All0
20
40
60
80
10091
86
Telavancin Vancomycin
Pa
tie
nts
%
*7-14 days after receipt of last antibiotic dose

Telavacin versus Vancomcyin for HAP with Gram+ATTAIN Trial
· Methods (N = 1503) - Two Phase 3 trials- Randomized, double blind - Patients with HAP, including VAP- Suspected or confirmed gram+- Adults
· Regimens (duration 7-21 days) - Telavacin: 10 mg/kg IV q24h - Vancomycin: 1g IV q12h - Concomitant therapy for Gram- allowed
Study Design Results
Source: Rubinstein E, et al. Clin Infect Dis. 2011;52:31-40.
Cure Rate Mortality0
20
40
60
80
100
82
22
81
17
Telavancin Vancomycin
Pa
tie
nts
%

Ceftaroline (Teflaro)

Beta-Lactams: Mechanism of Action
Cell WallCell Membrane
Penicillin Binding Proteins
DNA
TranspeptidationCarboxypeptidation
Ceftaroline

Ceftaroline (Teflaro): Mechanism of Action
Altered Penicillin Binding Protein Ceftaroline
DNA
PBP 2a
PBP 2a

Ceftaroline (Teflaro)
· FDA Status: approved 2010
· Indication: SSTI, CAP
· Class: Cephalosporin (“5th Generation”)
· Mechanism: Inhibits cell wall synthesis (binds to PBP, including PBP2a)
· Dose: 600 mg IV q12 hours
· Activity: - Broad gram-positive activity: MSSA, MRSA, VISA, DRSP- Gram-negative: Enterobacteriaceae- Not active against Pseudomonas sp. or Proteus sp., or E. faecium
· Adverse Effects: seroconversion to positive direct Coombs’ test
Source: Saravolatz LD, et al. Clin Infect Dis. 2011;52:1156-63.

Cetaroline for Complicated SSTICANVAS 1 and 2
· Methods - Pooled analysis of 2 phase 3 trials - Double-blind trial - N = 1378 enrolled - Complicated SSTI
· Regimens (5-14 days) Ceftaroline: 600 mg IV q12h or Vancomycin: 1g IV q12h + Aztreonam: 1 g IV q12h
Study Design Clinical Cure
Source: Corey GR, et al. Clin Infect Dis. 2012;56:641-50.
All MRSA0
20
40
60
80
10092 9393 94
Ceftaroline Vancomycin-Aztreonzam
Pa
tie
nts
%

Cetaroline vs. Ceftriaxone for CAPFocus1 and 2
· Methods - Pooled analysis of 2 phase 3 trials - Double-blind trial - N = 1228 enrolled - Community acquired pneumonia - Patients hospitalized
· Regimens (5-14 days) Ceftaroline: 600 mg IV q12h x 5-7d or Ceftriaxone: 1g IV q12h x 5-7d
Study Design Clinical Cure Rate
Source: File TM, et al. Clin Infect Dis. 2010;51:1395-405.
FOCUS 1: received 2 doses of clarithromycin on d1 Series10
20
40
60
80
100
8478
Ceftaroline Ceftriaxone
Pa
tie
nts
%

Tedizolid (Sivextro)

Protein Synthesis
50S
fMet-tRNA
50 S Ribosome
30S
30 S Ribosome
DNA
23S
70 S Initiation Complex
23S

Tedizolid (Zyvox): Mechanism of Action
50S
fMet-tRNA
50 S Ribosome
30S
70 S Initiation Complex
30 S Ribosome
DNA23S
Tedizolid
23S

Tedizolid (Sivextro)
· FDA Status: approved June 20, 2014
· Clinical Indication: approved for SSTI caused by susceptible bacteria
MSSA, MRSA, S. pyogenes, S. agalactiae, S. anginosus group, E. faecalis
· Class: Oxazolidinone; binds to 23S rRNA of 50S subunit
· Mechanism: Inhibits protein synthesis (blocks ribosomal initiation complex)
· Dose: 200 mg IV or PO once daily
· Adverse Effects: nausea, headache, diarrhea
Source: Tedizolid Package Insert

Tedizolid versus Linezolid for SSTI: Oral TherapyESTABLISH-1
· Methods
- Randomized, double blind, phase 3
trial
- 81 study centers
- N = 667 adults
- Acute bacterial SSTI
· Regimens
- Tedizolid: 200 mg PO qd x 6d
- Linezolid: 600 mg PO bid x 10 days
Study Design (ESTABLISH-1) Early Clinical Response
Source: Prokocimer P, et al. JAMA. 2013;309:559-69.
Series10
20
40
60
80
100
80 79
Tedizolid Linezolid
Pa
tie
nts
%

· Methods - Randomized, double blind, phase 3 trial - 58 centers in 9 countries - N = 666 adults - Acute bacterial SSTI
· Regimens* - Tedizolid: 200 mg IV/PO qd x 6d - Linezolid: 600 mg IV/PO bid x 10 days
Study Design (ESTABLISH-2) Early Clinical Response
Source: Moran GJ, et al. Lancet Infect Dis 2014;14:696-705.
Series10
20
40
60
80
100
85 83
Tedizolid Linezolid
Pa
tie
nts
%*required to receive IV therapy for minimum of 1 day, then could step down to PO
Tedizolid versus Linezolid for SSTI: IV/Oral TherapyESTABLISH-2

Dalbavancin (Dalvance)

Dalbavancin (Dalvance): Mechanism of Action
DalbavancinCell Wall Synthesis
DNA
Dimer
Dimer
Dimer

· FDA Status: approved May 23, 2014
· Clinical Indication: approved for SSTI caused by gram-positive bacteria(MSSA, MRSA, S. pyogenes, S. agalactiae, S. anginosus group)
· Mechanism: Lipoglycopeptide that inhibits cell wall synthesis
· 2 Dose Regimen: 1000 mg IV followed 1 week later by 500 mg IV
· Dose Reduction: - Regular hemodialysis: no dose change- For CrCl < 30 ml/min and no hemodialysis: 750 mg then 375 mg
· Adverse Effects: nausea, headache, diarrhea
Dalbavancin (Dalvance)
Source: Dalbavancin Package Insert

Dalbavancin versus Vancomycin for SSTIDISCOVER 1 and DISCOVER 2
· Methods - Pooled analysis of 2 phase 3 trials* - Randomized trials - N = 659 adults - Acute bacterial SSTI
· Regimens - Dalbavancin 1000 mg d1, 500 mg d8 - Vancomycin IV for ≥3 days, then oral linezolid 600 mg bid to complete 10-14d
Study Design Clinical Response to Therapy
Source: Babinchak T, et al. Clin Infect Dis 2005;41:S354-7.
*DISCOVER 1 and DISCOVER 2
1° End Point 2° End Point 0
20
40
60
80
100
80
91
80
92
Dalbavancin Vancomycin-Linezolid
Pa
tie
nts
%
1° End Point = Success rate at 48 to 72 hours 2° End Point = Success rate at end of therapy

· Mechanism of Action- Improved PBP binding due to hydrophobic side chain- More stable binding due to formation of dalbavancin dimers
· Dalbavancin bactericidal and vancomycin bacteriostatic
· Differences in dosing and dose reductions
How is Dalbavancin Different from Vancomycin
Source: Guskey MT, et al. Pharmacotherapy. 2010;30:80-94.

Catheter-Related Bloodstream InfectionsDalbavancin versus Vancomycin
· Methods (N 75) - Phase 2, randomized, controlled - Patients with catheter-related BSI - Randomized, open-labeled - Catheter-related BSI cause by Gram+ - Catheters removed for MSSA & MRSA - MRSA identified in 51% of patients
· Regimens - Dalbavancin: 1.0 g IV d1; 0.5 g IV d8 - Vancomycin: 1g bid IV x 14d
Study Design Overall Success Rate
Source: Raad I, et al. Clin Infect Dis 2005;40:374-80.
INVESTIGATIONAL-Dalbavancin not FDA approved for treatment of bloodstream infections
Series10
20
40
60
80
10087
50
Dalbavancin Vancomycin
Pa
tie
nts
%

Oritavancin (Orbactiv)

· FDA Status: approved August 6, 2014
· Clinical Indication: approved for acute SSTI caused by gram-positive bacteria (MSSA, MRSA, various streptococcal species, and Enterococcus faecalis)
· Mechanism: Lipoglycopeptide with multiple mechanisms: inhibits transglycolation, inhibits transpeptidation, and disrupts cell membranes
· Single Dose Regimen: 1200 mg IV (infused over 3 hours)
· Dose Reduction: - Mild or moderate renal impairment: no dose change- Severe renal impairment or hemodialysis: unknown
· Adverse Effects: nausea, headache, diarrhea, vomiting
Oritavancin (Orbactiv)

Oritavancin versus Vancomycin for SSTISOLO-I
· Methods
- Randomized, double blind, phase 3
trial
- N = 954 adults
- Acute bacterial SSTI
· Regimens
- Oritavancin: 1200 mg IV x 1
- Vancomycin: 1g IV q12h x 7-10 days
Study Design (ESTABLISH-1) Investigator-Assessed Clinical Cure
Source: Corey R, et al. N Engl J Med. 2013;370:2180-90.
Series10
20
40
60
80
100
80 80
Oritavancin Vancomcyin
Pa
tie
nts
%

Fidaxomicin (Dificid)

Fidaxomicin (Dificid)
FDA Status: Approved in May 2011 Indication: Clostridium difficile-associated diarrhea Class: macrocyclic antibiotic Mechanism: inhibits RNA polymerase and transcription Dose: 200 mg bid x 10 days In vitro C. difficile activity: 8x more active than vancomycin Absorption: Minimal oral absorption Adverse Effects: nausea, vomiting, abdominal pain

Treatment Arms
Clostridium difficile : Fidaxomicin vs VancomycinStudy Design
From: Louie TJ, et al. N Engl J Med. 2011;364:422-31.
Study Design
Protocol
- N = 629 enrolled (548 evaluated)
- Double-blind, prospective, randomized trial
- Phase 3 trial
- Conducted from 2006-2008
- Age: 16 years and older
- Acute symptoms of C. diff and +stool toxin
- Randomized to fidaxomicin or vancomycin
Fidaxomicin200 mg PO BID X 10 days
Vancomycin125 mg PO QID x 10 days

Clostridium difficile: Fidaxomicin vs VancomycinResults
From: Louie TJ, et al. N Engl J Med. 2011;364:422-31.
Clinical Cure* Recurrence^0
20
40
60
80
10088.2
15.4
85.8
25.3
Fidaxomicin
Vancomycin
Pat
ien
ts %
Clinical Cure = resolution of symptoms and no need for further therapyRecurrence = diarrhea and positive stool test within 4 weeks after treatment
P < 0.005

Treatment of Gram-Negative Infections

Source: Boucher HW, et al. Clin Infect Dis. 2013:56:1685-94.

Source: Boucher HW, et al. Clin Infect Dis. 2013:56:1685-94.
“Our survey demonstrates some progress in
development of new antibacterial drugs that target
infections caused by resistant GNB, but progress
remains alarmingly elusive.”

Source: Centers for Disease Control and Prevention (CDC)

· Antibiotic development has dramatically fallen off
· Antibiotics are lower priority for pharmaceutical development
· Most recently approved antibiotics are for Gram+ infections
· New antibiotics with favorable dosing characteristics
· Huge need for antibiotics for multi-resistant gram negative pathogens
Conclusions