Antimicrobial Susceptibility Testing – are we heading towards … · •Antimicrobial...
44
EUCAST The European Committee on Antimicrobial Susceptibility Testing Gunnar Kahlmeter EUCAST and ESCMID
Transcript of Antimicrobial Susceptibility Testing – are we heading towards … · •Antimicrobial...

EUCAST
The European Committee on Antimicrobial Susceptibility Testing
Gunnar Kahlmeter EUCAST and ESCMID

ESCMID
• How many of you are ESCMID members?
• How many have been to an ECCMID?
• How many are planning to attend ECCMID in April 2015?
• Is your department an ESCMID Collaborative Centre?
• Have you thought about applying for an ESCMID Observership?
• ESCMID Post Graduate course or Summer school?

EUCAST
• Is your lab on EUCAST?
• Is your lab on CLSI?
• Is your lab on CDS?
• Is your lab thinking about changing to EUCAST?

Antimicrobial Susceptibility Testing - main principles and methods
- and some history

Methods for susceptibility testing
1. Phenotypic test methods – MIC determination (broth micro dilution, gradient tests, disk diffusion, automated and
semiautomated systems such as Vitek2, Phoenix, Microscan)
– based on antimicrobial activity (MIC) and breakpoints
– Predict susceptibility and resistance.
– Quantifiable.
– Require standardisation.
– Require breakpoints.
2. Genotypic test methods
3. Expert rules

Milestones in the development of phenotypic AST
• Beijerinck in 1889 used agar diffusion to study the effect of different auxins (plant growth hormones) on bacterial growth.
• Fleming in 1924 introduced the use of the ditch plate technique for evaluating antimicrobial qualities of antiseptic solutions.
• Fleming later developed a broth dilution technique with turbidity as end point.
• The WHO commissioned the ICS published in 1971 (Ericsson and Sherris) but soon after denounced their own initiative.
• The 1970ies - the formation of national breakpoint committees (DIN, NCCLS, and others).
• EUCAST formed 1997 and revamped 2001
• ISO 20776-1 (2006) – International reference for broth microdilution MIC determination in non-fastidious bacteria.

Hans Ericsson (Sweden)
John Sherris (USA)

Ericsson and Sherris (International Collaborative Study, 1971) were critizised for recommending rigorous standardisation
• Balows, head of CDC 1972: “…a level of standardisation that might result in violation of property rights”.
• Garrod, leading UK microbiologist in the mid 1900s: “The ICS demands a degree of standardisation which I believe to be impracticable”.
• DIN, Germany: “The ICS approach is too complicated given conditions in German laboratories”.

In the beginning there was one table for everything - one zone diameter breakpoint and a corresponding MIC value for all purposes.

CLSI S1 (First Supplement, 1981)
NCCLS First Supplement, 1981 - “useful for anything that would grow”
1. EUCAST – structure, remit, national committees (NACs)

It is now >40 years later and much more complicated
Tools for determining breakpoints more sophisticated
• Species related breakpoints
• Disease related breakpoints (UTI, meningitis, pneumonia)
• Dose related breakpoints

Phenotypic susceptibility testing is based on
MIC + breakpoints
Agreement Breakpoint committees
Medicine agencies
Standardisation ISO standard

The MIC
• The MIC can be standardised to the degree where many people start thinking it is an absolute value which can be compared to body fluid concentrations.
• But with simple means (changing inoculum, incubation time, temperature, pH, cat ion content etc) it can easily be “manipulated”

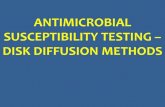
MIC determination Broth microdilution according to the
ISO-standard*
16 8 4 2 1 .5 .25 .12 .06 .03 C
See the ISO, CLSI or EUCAST websites

All other tests are surrogate tests calibrated to the ISO method
Gradient MIC test: Several manufacturers:
bioMerieux (Etest)
Oxoid (M.I.C.E.)
Liofilchem (MIC-strip)
Disk diffusion’ Agar dilution

Which mehods can be automated?
• Broth microdilution (BMD) – Micro Scan, Phoenix, Vitek2
• Agar dilution – Semi-automated in-house
• Gradient tests – Semi-automated (inoculation, application, reader)
– Etest (bioMerieux), M.I.C.E. (Thermofisher), MIC Test Strip (Liofilchem)
• Disk diffusion (or tablet diffusion) – Semi-automated (automated 6 – 8 h)
– Biomic, Sirscan, Osiris
All other tests are surrogate tests calibrated to the ISO method

Clinical breakpoints
AST is based on a highly standardised, reproducible, but relative MIC-value related to
breakpoints determined for that specific system.
S ≤Y mg/L R >Y mg/L (CLSI R ≥ Z mg/L)

Clinical breakpoints are always a compromise and therefore sometimes a disappointment….
• People differ (age, pharmacokinetics, immune competence)
• Infections differ (site, severity, bacterial virulence etc)
• …
When we get it wrong, we were almost always over optimistic!

─ Dose and mode of administration ─ Clinical targets (indications) ─ Target organisms (indications) ─ MIC distributions of target organisms ─ Resistance mechanisms of clinical importance in
target organisms ─ Pharmacokinetics of agent in target patients ─ Pharmacodynamics of agent in relation to target
organism ─ Clinical outcome data for target infections.
Tools for determining clinical breakpoints

S I R
1. Determine the SIR-category of the wild type (S, I or R) 2. If wild type is “S”, determine the S-breakpoint (PK/PD, Clinical outcome related to
MIC etc) 3. If dose can be increased (or agent concentrated), define R-breakpoint.

S I R
1. If wild type is “intermediate”, determine the R- breakpoint. 2. If wild type “resistant”, decide whether or not a “high-level resistant” category is
needed.

S, I and R • Susceptible (S)
– a micro-organism is defined as susceptible by a level of
antimicrobial activity associated with a high likelihood of
therapeutic success
• Intermediate (I)
– a micro-organism is defined as intermediate by a level of
antimicrobial agent activity associated with uncertain therapeutic
effect.
It implies that an infection due to the isolate may be
appropriately treated in body sites where the drugs are
physically concentrated or when a high dosage of drug can be
used; (it also indicates a buffer zone that should prevent small,
uncontrolled, technical factors from causing major discrepancies
in interpretations.)
• Resistant
– a micro-organism is defined as resistant by a level of
antimicrobial activity associated with a high likelihood of
therapeutic failure.

1. Medicines agencies (EMA, FDA) 2. Breakpoint committees
Colleagues who know better
Breakpoints are determined by:
Pharmaceutical companies AST companies

Breakpoint committees 1970 – 2001
EUCAST was reorganised in 2001 and united the national breakpoint
committees of Europe
Committee Country Disk diffusion
BSAC United Kingdom Yes
CA-SFM France Yes
CRG The Netherlands No
DIN Germany Yes
NWGA Norway No
SRGA Sweden Yes
NCCLS (CLSI) USA Yes

EUCAST General Committee NACs from European Countries + Australia + USA + …
Meets once yearly + formal consultations
EUCAST Steering Committee 5 two day meetings per year
Subcommittees Antifungal susceptibility testing
Anaerobes
Expert Rules and Intrinsic Resistance
Detection of resistance mechanisms
The relationship between phenotype and genotype
Veterinary breakpoints (VetCAST)
Expert groups • M.tuberculosis • Helicobacter • C.difficile • etc

National AST Committee (NAC)
• Antimicrobial susceptibility testing – Coherent strategy at national level
– Implementation of breakpoints and methods
– Education (national workshops, websites)
– Translation of documents
– Liaison and consultation with EUCAST – via the General Committee and open consultations
– Liaison with other national groups involved in antimicrobial stewardship or surveillance of resistance.
– QA
• (Antimicrobial Policies)
• (Antimicrobial Resistance Surveillance)
• (Antimicrobial Consumption and Stewardship)

Denmark
Finland
Poland
France
Germany
Spain Portugal
Greece
Italy Turkey
Switzer- land
Austria
Czech Republic
Estonia
Latvia
Lithuania
Belarus
Ukraine
Romania Hungary
Slovakia Moldova
Bulgaria
Russia
Ireland
Great Britain
Monte- negro
Serbia
Slovenia Croatia
Bosnia- Herze- govina
Mace- donia
Albania
Norway
Nether-
lands
Malta
Belgium
Luxembourg
Sweden
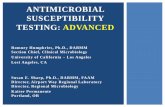
National AST Committees (NACs), August 2014
Yes
No
In the process of forming a NAC
No information
Australia Iceland Israel Countries not on this map: South Africa USA Brazil Morocco

• Representatives of national breakpoint committees (6) and General Committee (3)
• Observers from EMA and ECDC
• Industry is invited to present “their case” but is not part of the decision
• Convenes 5 times per year (2 days)
• A part time scientific secretary
EUCAST Steering Committee

EUCAST decision process
• Steering Committee evaluates available data and proposes breakpoints
(and other decisions).
• Consultation with general committee members and national committees
(NACs) on proposed decision – revision of the proposal.
• Public consultation (EUCAST webpage) after which criticism and
responses are published – revision of proposed decision.
• Final decision (and for breakpoints rationale document) published.

EUCAST strives to be transparent
• Open, public consultation as part of the decision process with published comments and rebuttals (on website)
• Rationale documents for breakpoint decisions (on website)
• Decision on zone diameter breakpoints and how they relate to MIC values available (on website)
• EUCAST secretariate responds to 500 – 1000 queries per year, mostly within a few days (FAQ on website).

Consultation on document

A breakpoint decision on a new agent normally takes 5 Steering Committee
meetings = 1 year

Breakpoints from EUCAST
– Existing agents - harmonization of European breakpoints (2002 – 2008) for antibiotics commonly used and available in most countries:
Penicillins, cephalosporins, carbapenems, aminoglycosides, fluoroquinolones, tetracyclines, glycopeptides, macrolides etc
– New agents - together with EMA (2003 - ) – Daptomycin
– Tigecycline
– Doripenem
– Telavancin
– Ceftaroline
– Ceftobiprole
– Bedaquiline, Delaminid
– New glycopeptides, cefalosporine/inhibitor agents, and more
• Review of established breakpoints (2009 - ): Glycopeptides, Carbapenems, Colistin, Doripenem

Bacteria without breakpoints
• Aerococcus spp - 2015
• Kingella kingae - 2015
• M.tuberculosis - ongoing
• Actinomyces spp
• Nocardia spp
• ….

Antibiotics without breakpoints
• Spiramycin
• Josamycin
• Cefoperazone-sulbactam
• ….
• Currently EUCAST is preparing a list of “all” globally available antibiotics with the rationale for why they were not given breakpoints

EUCAST regular review of
breakpoints
• New resistance mechanisms
• New agent in class
• New clinical data
• Extended indications
• Change in dosing or administration
• Change in target organisms

Review
• Glycopeptides
• Carbapenems
• Colistin – ongoing (together with CLSI and others)
• Fluoroquinolones - ongoing
• Tigecycline - ongoing
• Aminoglycosides - planned

Denmark
Finland
Poland
France
Germany
Spain
Portugal
Greece
Italy Turkey
Switzer- land
Austria
Czech Republic
Estonia
Latvia
Lithuania
Belarus
Ukraine
Romania Hungary
Slovakia Moldova
Bulgaria
Russia
Ireland
Great Britain
Monte- negro
Serbia
Slovenia
Croatia Bosnia- Herze- govina
Mace- donia
Albania
Norway
Nether-
lands
Malta
Belgium
Luxembourg
Sweden
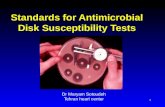
Implementation of EUCAST breakpoints, January 2014
>50%
<10%
10-50%
No information
Australia Iceland Israel Countries not on this map:
% Laboratories
South Africa USA Brazil Morocco

Antimicrobial susceptibility testing guidelines and methods used in the UK (201
laboratories), Dec 2013 Derek Brown and Christine Walton, UKNEQAS
Guideline Method Number of laboratories
England Wales Scotland N. Ireland Total
BSAC Automated 9 1 1 0 11
Disk diffusion 75 3 3 0 81
Breakpoint 4 0 0 0 4
Multiple 10 0 0 0 10
Stokes Disk diffusion 1 0 0 0 1
EUCAST Automated 36 2 18 3 56
Disk diffusion 10 4 0 2 16
Etest 1 0 0 0 1
Multiple 3 0 0 0 3
CLSI Automated 12 0 1 0 13
Disk diffusion 1 0 1 0 2
Multiple 1 0 0 0 1
Not stated 2 0 0 0 2
BSAC has decided to abandon the BSAC disk diffusion technique based on ISA and
semi-confluent inoculum 2015-12-31

Other disk diffusion methods
• The Dutch and the Germans abandoned their methods years ago (<2005).
• SRGA abandoned the Swedish method 2010.
• CA-SFM abandoned method 1 January 2015.
• BSAC abandons method 1 january 2016

EUCAST Websites
EUCAST websites • www.eucast.org • Free of charge • No login • Updated weekly • Previous versions of
documents are online • Newsflow (RSS) • MIC wild type
distributions • >50 000 visits/month

9. The Future Will there be internationally agreed breakpoints?
• If by action – who takes the initiative?
– WHO, UN, ISO?
– EUCAST or CLSI?
– Financing? Business model?
• If by evolution and “survival of the fittest” – is it then between EUCAST and CLSI when judged on…
• Science/credibility?
• Decision model?
• Influence/transparence?
• Availability to the international community?

Acknowledgement • Derek Brown and Rafael Canton,
companions and hard EUCAST workers.
• The EUCAST Steering Committee 2001 –
• Erika Matuschek and Jenny Åhman who are responsible for technical developments and the EUCAST Network Laboratories
• John Turnidge and Ron Jones for always being supportive and helpful