Antimicrobial Resistance and Risk Factors of Urinary Tract ...ipna-online.org/Media/Junior...
36
2 nd IPNA ESPN MASTER for JUNIOR CLASSES CYSTINOSIS Prof.Dr. Rezan Topaloglu Hacettepe University Faculty of Medicine Department of Pediatric Nephrology Ankara Turkey R.Topaloglu
Transcript of Antimicrobial Resistance and Risk Factors of Urinary Tract ...ipna-online.org/Media/Junior...

2nd IPNA ESPN MASTER for
JUNIOR CLASSES
CYSTINOSIS
Prof.Dr. Rezan Topaloglu Hacettepe University Faculty of Medicine
Department of Pediatric Nephrology Ankara Turkey
R.Topaloglu

Cystinosis Rare autosomal recessive disorder estimated incidence
1/ 100.000 live births
Lysosomal storage disease
Types Classical, Infantile, Nephropathic cystinosis
Late onset cystinosis Juvenile or Intermediate form
Ocular non nephropatic form Adult or Bening form
R.Topaloglu

Clinical Findings of Nephropatic Cystinosis According to Age
Age Presentation
Birth Normal
Infancy Renal Tubular Fanconi syndrome
-Dehydration, polyuria, polydipsia
-Metabolic acidosis
-Hypokalemi
-Hypophosphatemic rickets
-Hypocalcemic tetany
Growth retardation Vomiting
Early childhood Photophobia
Pre-adolescence Renal failure
Renal osteodystrophy
Hypothyroidism
Pediatr Nephrol 2008;28:863 R.Topaloglu

Late onset cystinosis Juvenile or Intermediate form
Onset at a later age. Often does not presents with Fanconi syndrome Renal failure occurs usually between ages 15-25 years
Presents with photophobia, crystals form in cornea
Ocular- Non nephropathic form or Bening form
R.Topaloglu

Metabolic defect
Autosomal recessive disorder characterized by
intra lysosomal accumulation of cystine due to
a defect in the lysosomal transport of cystine
Lysosomal transporter-CYSTINOSIN
coded by CTNS gene
R.Topaloglu

KI 2012: 81;127-129
R.Topaloglu

LOCALIZATION &
IDENTICATION OF CTNS GENE
R.Topaloglu

1. Letter
Nature Genetics 10, 246 - 248 (1995) doi:10.1038/ng0695-246
Linkage of the gene for cystinosis to markers on the short arm of
chromosome 17
The Cystinosis Collaborative Research Group
Geraldine A. McDowell1, ,8, William A. Gahl1, ,8, Leah A. Stephenson1, ,8, Jerry A.
Schneider2, ,8, Jean Weissenbach3, ,8, Mihael H. Polymeropoulos4, ,8, Margaret M.
Town5, ,9, William van't Hoff6, ,9, Martin Farrall7, ,9 & Christopher G. Mathew5, ,9
Cystinosis gene located on Chromosome 17 short arm p13.3
linkage of the cystinosis gene to markers on the short arm of chromosome 17
(Zmax=10.89, =0.03) for marker D17S1584. Multipoint analysis and haplotypes
in recombinant families suggest that the gene is located between markers
D17S1583 and D17S796 -4cM interval
D17S1798 D17S1828 1 cM
2. Am J Hum Genet 1996; 58:535-543 Jean G et al
Reduced the interval to 1 cM
R.Topaloglu

• In 1998, a large deletion was detected in the homozygous state in over a third of affected european individuals.
• a 13 kb deletion in a single family, • searching for the causative gene to the region of overlap. • novel gene is identified by using a positional cloning strategy in this
region • the various mutations were detected within its coding region in
affected individuals validated it as the gene responsible for cystinosis
• It is named as CTNS gene
R.Topaloglu

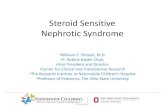
CTNS gene
structure
2
Cytoplasm
Lysosomal membrane
Lysosome
N-terminus
C-terminus
GY-DQ-L CTNS product Cystinosin predicted structure
367 aa
YFPQA
R.Topaloglu

Mutations in CTNS gene
More than 110 mutations have been reported
Big deletion 57 kb
Small deletions (13kb, 4 kb deletions)
Insertions
Missense or nonsense mutations
Splicing mutations
Partial replication of exon 9, a skipping of exon 5 (85 bp)
R.Topaloglu

•The size of this deletion was determined to be 57 kb Am J Hum Genet 1998;63:1352-
1362
•57kb deletion that covers the first 9 exons and introns and intrups exon 10
•57 kb deletion extends into CARKL and TRPV1 gene causing more complex
phenotypes
•76 % of patients European origin have this deletion either in heterozygous or
homozygous state
•In the US and Northren European populations 50 % of individuals with nephropathic
cystinosis is homozygous for this deletion
57 Kb deletion

Clinical Findings of Nephropatic Cystinosis According to Age
Age Presentation
Birth Normal
Infancy Renal Tubular Fanconi syndrome
-Dehydration, polyuria, polydipsia
-Metabolic acidosis
-Hypokalemi
-Hypophosphatemic rickets
-Hypocalcemic tetany
Growth retardation
Vomiting
Early childhood Photophobia
Pre-adolescence Renal failure
Renal osteodystrophy
Hypothyroidism
Pediatr Nephrol 2008;28:863 R.Topaloglu

Diagnosis confirmation
The diagnosis can be confirmed by
measurement of leukocyte cystine levels
demonstration of corneal cystine crystals by the slit lamp exam and
genetic analysis of the CTNS gene.
R.Topaloglu

Renal Disease
Main Predictor of prognosis
R.Topaloglu

Renal Disease Characteristics
Proximal RTA
Renal loss of Na and K - Hyponatremia & Hypokalemia
Hyperuricosuria-Hypourecemia
Carnitinuria- Decrease plasma carnitine
hypercalciuria & hyperphosphaturia- Medullary nephrocalsinosis
Increased protein excretion
albuminuria
LMW proteinuria- Vit D binding protein, α1 microglobulin, β2 microglobulin, RBP
High molecular weight prt-IgG
R.Topaloglu

Renal disease Characteristics
Generalized aa uria 10 times normal values
Urinary cystine concentration is elevated
No cystine stones Why ?
Diluted urine
Alkaline Urine
In late childhood medullary nephrocalsinosis due to hypercalsiuria and hyperhosphaturia
N Eng J Med 2002; 347:111-121 R.Topaloglu

Renal Pathology Typical swan neck deformity of
proximal convulated tubules seen at 6 monts
Other typical features: irregularities of proximal tubular cells (flat cells without brush boarder and large cells with hyperchromatic cytoplasm)
Gl may appear normal generally contain giant multinucleated podocytes
Cystine crystals located in the lysosomes or in cytoplasm seen within interstitial cells rarely within podocytes
Late stage Progressive tubulo-interstitial lesions interstitial fibrosis, tubular atrophy
NEJM 2002 ; 347:111 Am J Kidney Dis 2008;51:893 KI 2008; 73:782
Glomerulus with multiple
multinucleated podocytes and parietal
epithelial cells (HE).
Interstitial cells display
cytoplasmic crystalline
inclusions (toluidine bluestain)
Interstitial cells containing multiple
clear, elongated, needle-shaped and
rhomboid cytoplasmic
inclusions(EM )
R.Topaloglu

Renal functions
In infancy or early childhood serum Cr is generally not elevated
In the absence of Rx creatinin clearance decreases
Among 205 European patients before cystiamine threapy end Stage renal failure developed at mean age 9.2 years
Some have unexplained pleteaus in the renal functions for months to years
Some have rapid deteriotions triggered by an acute infection or by dehydration
Proc Eur Dial Transplant Assoc 1983;19:582-589
R.Topaloglu

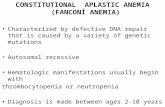
Renal Function treated and Untreated Cystinosis Patients, According to Age
●33 untreated patients (1960-1992) ▲ 28 patients treated during at least 10 years, beginning before age 3 (mean age : 17m) Age at which serum creatinine reaches 10 mg/dl has been shifted from 10y to 23y NEJM 2002
R.Topaloglu

Renal transplantation in cystinosis
No recurrence of cystinosis in renal graft
• graft biopsies: cystine crystals in invading host cells, but not in tubular or glomerular epithelium
Living-related transplantation with heterozygote parent’s kidney is allowed
R.Topaloglu

Superior renal graft survival in
cystinosis
Broyer et al. 1981, EDTA paediatric registry • n=47 patients with cystinosis
• 1 year patient and graft survival compared to other primary renal diseases: 89% versus 81% and 81% versus 67%
Kashtan et al. 1995, NAPRTCS data • superior survival of renal grafts in cystinosis
Niaudet, 2006, DIVAT, France • n=23 patients with cystinosis
• at 16 years follow-up graft survival in cystinosis 80% versus 65 % in other primary renal diseases
Van Strelan et all 2011, ESPN and ERA-EDTA Registry • n-=245 patients
• 5 year graft survival compared to other renal diseases (94% versus 84 % )
• Improved 5 year graft survival and the renal function over the last 20 years among NC patients before 1990 graft survival 86% after 2000 100%
R.Topaloglu

Extrarenal complications and long term complications
Endocrine system: Growth Retardation, Hypothyroidism, Diabetes Mellitus, Male Hypogonadism
Eye involvement
Myopaty, Swallowing difficulty
Pulmonary dysfunction
CNS inolvement
R.Topaloglu

Eye Involvement
Band keratopathy which can impair vision Pigmentary retinopathy – impaired color vision and impaired night vision
corneal cyristals
R.Topaloglu

GI Complications
Untreated or undertreated patients develop GI symptoms in 2nd or 3rd decade of life
Spectrum of involvement diverse
77% have feeding abnormalities- reflux, dysmotility, pseudo obstruction, swallowing dysfunction
Mild hepatomegaly , portal hypertension
Exocrine pancreatic insufficiency
Inflamatory bowel disease
R.Topaloglu

CNS involvement in children
intra cranial pressure may increase due to cystine deposition
Pseudotumor cerebri
CSF normal except elevetad intracranial pressure
In some cases acetazolamide is enough in some ventriculo peritoneal shunt is needed
Convulsions, spasticity
Some have abnormal EEG without seizures
Low visual memory may be related to cortical atrophy
Phycosocial difficulties
R.Topaloglu

Late CNS Involvement
Most commonly a generalized cerebral atrophy on CT
Occasionaly calsifications of basal ganglia
Extensive demyelination
Cystinotic encephalopathy - cerebellar and pyramidal signs, mental deterirotion , pseudo-bulbar palsy
- stroke like episodes
Correlates directly with age
Pediatr Nephrol 2008;28:863
Pathogenesis could be related to neuro toxicity involving oligodendrocytes
R.Topaloglu

TREATMENT
Treatment of Fanconi Syndrome
Treatment of cystine accumulation-Cystine depleting treatment
R.Topaloglu

Symptomatic Treatment for Fanconi
syndrome
This treatment may delay kidney failure and improve growth
provision of large amounts of water and sufficient food
nasogastric tube or gastrostomy in infants
potassium and sodium as bicarbonate (or citrate) , in 3-4 doses
Phosphate supplement, serum phosphate level = 3-3.5mg/dl
Ca supplementation
1α OH D3 to cure rickets 0.5-1.5 µg/d
to prevent rickets 0.1-0.3 µg/d
Carnitine supplementation 100mg/kg/day ?
Indomethasine -effects on polyuria & electrolyte supplement Starting age usually 9 months
R.Topaloglu

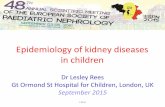
Cystine Depleting Therapy
Cysteamine
In cysteamine-treated lysosomes (c), cysteamine combines with half-cystine (cysteine) to form a
mixed disulfide cysteine-cysteamine, which uses the lysine transporter to exit the lysosome
Gahl et al, NEJM 2002
R.Topaloglu

Adequet treatment with cystine depleting agent
Significantly reduces the rate of progression to ESRF
Improves growth retardation
Postpones even prevents the extrarenal complications
hypothyroidism,
myopathy
pulmonary dysfunction,
DM
Cysteamine does not influence
Delayed puberty
Primary hypogonadism in male
Male infertility
Systemic cysteamine does not prevent corneal cysteine crystals , a need for topical cysteamine eye drops
R.Topaloglu

Monitorising the treatment
Leukocyte cystine levels
Adjust dose to maintain leukocytes cystine at less than 1 nmol ½ cystine /mg protein
R.Topaloglu


New treatment options
Anti inflammatory drugs? (jasn 25:1163;2014)
Inhibition of intracellular Clusterin and increasing cell viability attenuation of apoptosis in cystinosis cells (jasn 26:612;2015)
Treating chaperon mediated autophagy impairment that contributes to cell malfunction in cystinosis (EMBO Molecular Medicine 7:158;2015)
N acetyl cysteine- oxidative stress was reduce and renal function significantly improved during 3 months period (Ped Nephrol 29:1097;2014)
Folate pro-drug of cystamine as an enhanced treatment for nephropathic cystinosis (Bioorg Med Chem Lett. 21:2502; 2011)
Bone marrow transplantation (Blood 114:2542;2009 Kidney Int 79:1198;2011)
Hematopoeitic stem cell (Stem cell 33:301;2015)
Gene therapy
Gene repair
R.Topaloglu

Summary
Early diagnosis and adequate treatment is the key factor
Cystine depleting treatment slows down the progression of renal and extra-renal symptoms of cystinosis and should be administered as early as possible after the diagnosis and should be continued life-long (also after renal transplantation)
The administration of the recommended doses of cysteamine should be given
Ongoing research on new treatment modalities will improve the future of patients with cystinosis
R.Topaloglu

Questions
How one can suspect cystinosis in an infant ?
What is cystinosin ?
What is the most common endocrine
complication in cystinosis
Could the parents be donor ?
How is the graft survival in cystinotic patients
?
R.Topaloglu