Antiinflammatory drugs
79
Drugs affecting the immune system Chapters 43,44,45,46
-
Upload
many87 -
Category
Health & Medicine
-
view
1.075 -
download
6
description
Transcript of Antiinflammatory drugs

Drugs affecting the immune system
Chapters 43,44,45,46

NSAIDs Large and chemically diverse
group of drugs with the following properties: Analgesic Anti-inflammatory Antipyretic Antirheumatic

NSAIDs: Indications Analgesia (mild to moderate) Antigout effects Anti-inflammatory effects Antipyretic effects Relief of vascular headaches Platelet inhibition (ASA) Various bone, joint, and muscle pain Osteoarthritis Rheumatoid arthritis Dysmenorrhea

NSAIDs: Mechanism of Action Analgesia—treatment of
headaches, mild to moderate pain, and inflammation
Antipyretic: reduce fever Inhibit prostaglandin E2 within the area of
the brain that controls temperature Salicylates also have antiplatelet
activity Inhibit platelet aggregation

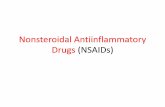
Figure 43-1 Arachidonic acid pathway.

NSAIDS: Mechanism of action• Inflammation: response to tissue injury and infection• Cardinal signs of inflammation• Chemical Mediators
– Prostaglandins• Vasodilation, relaxation of smooth muscles, increased capillary
permeability & sensitization of nerve cells to pain– Cyclooxygenase (COX)
• COX-1 & COX-2• Enzyme responsible for conversion of arachidonic acid into
prostaglandins -Leukotrienes

Chemical Categories of NSAIDs
Seven structurally related groups1. Acetic acids2. Carboxylic acids (salicylates)
Acetylated and nonacetylated
3. Propionic acids4. COX-2 inhibitors5. Fenamic acids6. Napthylalkanones (nonacidic)7. Oxicams

NSAIDs: Acetic Acid diclofenac sodium, Voltaren Indomethacin, indocin Sulindac, Clinoril tolmetin

NSAIDs: Carboxylic Acids
Acetylated acetylsalicytic acid diflunisal , Dolobid
Nonacetylated Ketorolac, Toradol sodium salicylate

NSAIDs: Propionic Acids Flurbiprofen, Ansaid Ibuprofen, (Advil, Motrin) Ketoprofen(Orudis) Naproxen(Aleve, Anaprox,
Naprosyn)

NSAIDs: Other Agents
COX-2 inhibitors Celebrex Vioxx (removed in 2004)

NSAIDs: Other Agents (cont’d)
Oxicams Meloxicam, Mobic piroxicam
Fenamic acids mefenamic acid
Nonacidic compounds nabumetone

NSAIDs: Salicylates
salicylates (aspirin) More potent effect on platelet aggregation
and thermal regulatory centre in the brain Analgesic Antipyretic Anti-inflammatory
Antithrombotic effect: used in the treatment of MI and other thromboembolic disorders

NSAIDs: Antigout Agents Gout: condition that results from
inappropriate uric acid metabolism Underexcretion of uric acid Overproduction of uric acid
Uric acid crystals are deposited in tissues and joints, resulting in pain

NSAIDs: Antigout Agents (cont’d)
allopurinol Used to reduce production of uric acid
colchicine Reduces inflammatory response to the
deposits of urate crystals
probenecid, sulfinpyrazone Increase excretion of uric acid in the urine

NSAIDs: Side EffectsGastrointestinal Dyspepsia, heartburn, epigastric distress,
nausea GI bleeding* Mucosal lesions* (erosions or ulcerations)
*misoprostol (Cytotec) can be used to reduce these dangerous effects
Renal Reductions in creatinine clearance Acute tubular necrosis with renal failure

NSAIDs Salicylate Toxicity Adults: tinnitus and hearing loss Children: hyperventilation and CNS
effects Effects arise when serum levels
exceed 300 mcg/mL Metabolic acidosis and respiratory
alkalosis may be present

NSAIDs: Nursing Implications Before beginning therapy, assess for
conditions that may be contraindications to therapy, especially: GI lesions or peptic ulcer disease Bleeding disorders
Assess also for conditions that require cautious use
Perform laboratory studies as indicated (cardiac, renal, liver studies, CBC, platelet count)

Nursing Implications Perform a medication history to assess
for potential drug interactions. Several serious drug interactions exist
Alcohol Heparin Phenytoin Oral anticoagulants Steroids Sulfonamides

Nursing Implications (cont’d) Salicylates are NOT to be given to
children under age 12 because of the risk of Reye’s syndrome
Because these agents generally cause GI distress, they are often better tolerated if taken with food, milk, or an antacid to avoid irritation
Explain to clients that therapeutic effects may not be seen for 3 to 4 weeks

Nursing Implications (cont’d) Educate clients about the various side
effects of NSAIDs, and to notify their physician if these effects become severe or if bleeding or GI pain occurs
Clients should watch closely for the occurrence of any unusual bleeding, such as in the stool
Enteric-coated tablets should not be crushed or chewed

Nursing Implications (cont’d) Monitor for therapeutic effects,
which vary according to the condition being treated Decrease in swelling, pain,
stiffness, and tenderness of a joint or muscle area

Case Study: NSAIDS Mrs Jones is 78 years old and has been
discharged from hospital following an open reduction internal fixation of her Right tib/fibula.
She has a remote history of GI bleed in her 60’s
Her orthopedic surgeon prescribes: Cytotec, ASA 81 mg Celebrex

Your discharge instructions will be:
ASA:
Celebrex:
Cytotec:

Client teaching about NSAIDS:
Take with food/milk
Check stools for blood
Report stomach pain
Report to other health care
providers (ie dentist)

Immune System Defends the body against invading
pathogens, foreign antigens, and its own cells that become cancerous
Can also sometimes attack itself, causing “autoimmune diseases” or immune-mediated diseases
Participates in analphylaxis & tissue/organ rejection

Immunosuppressants Agents that decrease or prevent
an immune response, thus suppressing the immune system
Used to prevent or treat rejection of transplanted organs

Immunosuppressants (cont’d) All suppress certain T-lymphocyte
cells lines, preventing their involvement in the immune response
Result: a pharmacologically immunocompromised state
Mechanisms of action vary according to agent

Immunosuppressants (cont’d)
Corticosteroids azathioprine muromonab-
CD3 daclizumab sirolimus
cyclophosphamide
cyclosporine tacrolimus basiliximab glatiramer
acetate

Immunosuppressants (cont’d) Indications vary from agent to
agent Primarily indicated for the
prevention of organ rejection Some also used for immunological
diseases such as rheumatoid arthritis and multiple sclerosis

Immunosuppressants (cont’d) azathioprine
Used as an adjunct medication to prevent rejection of kidney transplants
Also used in the treatment of rheumatoid arthritis

Immunosuppressants (cont’d) cyclosporine
Primary agent used in the prevention of kidney, liver, heart, and bone marrow transplant rejection
May be used for other autoimmune disorders
tacrolimus Used for the prevention of liver and
kidney transplant rejection

Immunosuppressants (cont’d) glatiramer acetate
The only immunosuppressant agent used for the treatment of multiple sclerosis (MS)
Used to reduce the frequency of MS relapses (exacerbations) in relapsing-remitting multiple sclerosis (RRMS)

Immunosuppressants (cont’d) Side effects vary according to
agents, and may be devastating
**All immunosuppressed clients have a heightened susceptibility to
opportunistic infections**

Nursing Implications Thorough assessment should be
performed before administering these agents Renal, liver, and cardiovascular
function Respiratory assessment Baseline vital signs Baseline laboratory studies, including
hemoglobin, hematocrit, WBC, and platelet counts

Nursing Implications (cont’d) Assess for contraindications, drug
allergies Monitor WBC counts throughout
therapy; if the count drops below 3.0 x 109/L the drug should be discontinued, but only after contacting the physician

Nursing Implications (cont’d) Oral immunosuppressants should be taken
with food to minimize GI upset Oral forms are used when possible to
decrease the risk of infection that may occur with parenteral injections
Oral antifungal agents are usually given with these agents to treat oral candidiasis that may occur
Observe the oral cavity often for white patches on the tongue, mucous membranes, and oral pharynx

Nursing Implications (cont’d) Follow guidelines for parenteral
administration carefully Clients need to be told that lifelong
therapy with immunosuppressants is indicated with organ transplantation

Nursing Implications (cont’d) Clients taking immunosuppressants
should be encouraged to take measures to reduce the risk of infection Avoiding crowds Avoiding people with colds or other infections
Clients should be told to report any fever, sore throat, chills, joint pain, fatigue, or other signs of a severe infection immediately

Immunity Immune response
Antigens Antibodies
Active immunization Passive immunization

Table 45-1 Active versus passive immunity

Immunizing Biologicals Biological antimicrobial agents
Also called biologicals Antitoxins Serum Toxoids Vaccines Used to prevent, treat, or cure
infectious diseases

Toxoids Antigenic (foreign) preparations or bacterial
exotoxins Detoxified with chemicals or heat Cannot revert back to a toxic form Stimulate one’s immune system to produce
a specific antibody The production of these antibodies protect
against future exposures to the antigen Ex. Tetanus

Vaccines Suspensions of live, attenuated
(weakened) or killed (inactivated) micro-organisms
The weakened form prevents the person from contracting the disease

Vaccines (cont’d) Also stimulate the production of
antigens against a specific antibody Vaccinations with live bacteria or
virus provide lifelong immunity Vaccinations with killed bacteria or
virus provide partial immunity, and booster shots are needed periodically

Active Immunization The body is exposed to a relatively
harmless form of an antigen The immune system is stimulated,
and “remembers” this antigen if subsequent exposures occur
The immunizations do not cause a full-blown infection

Examples of Active Immunizing Agents BCG vaccine (tuberculosis) Diphtheria,tetanus, and pertussis toxoids,
several forms Cholera vaccine Haemophilus influenzae type b conjugate
vaccine Hepatitis A and B virus vaccines Measles, mumps, and rubella virus
vaccine, live—several forms Poliovirus vaccine, several forms

Examples of Active Immunizing Agents (cont’d) Rabies virus vaccine Smallpox virus vaccine Tetanus toxoid Varicella virus vaccine (chicken
pox) Yellow fever virus vaccine

Indications Active immunization
Prevents infection caused by bacterial toxins or viruses
Provides long-lasting or permanent immunity
“Herd immunity”

Passive Immunization Serum or concentrated immune
globulins from humans or animals are injected into a person
The substances needed to fight off invading micro-organisms are given directly to a person
The immune system is bypassed Short-lived compared with active
immunization, but works faster

Passive Immunization (cont’d) Naturally acquired passive immunity
From mother to fetus through the placenta From mother to infant through breast milk
Artificially acquired passive immunity Acquired from an external source, such as
injection of antibodies or immunoglobulins

Examples of Passive Immunizing Agents Antivenins Diphtheria antitoxin Hepatitis B immune globulin Immune globulin, various forms Rabies immune globulin (human) Rh0(D) immune globulin (RhoGAM) Tetanus immune globulin Varicella zoster immune globulin
(chicken pox/shingles)

Indications (cont’d) Passive immunization
Antitoxins, antivenins, immune globulins Minimizes effects of poisoning by the
venoms of spiders and certain snakes Provides quick immunity before a
person’s own immune system has a chance to make antibodies (such as in cases of exposure to hepatitis B or rabies viruses)

Indications (cont’d) National Advisory Committee on
Immunization recommendations for adult and pediatric immunizations (Canada) Provide specific dosages and intervals
for immunizations

Mechanism of action:vaccinesAnitgens: foreign substancesAnitbodies: immunoglobulinsOnce the vaccine is administered the body
produces immunoglobulins: IgG, IgA, IgE, IgD, IgM to attack and kill the foreign invader
Anitbody titre: the amount of immunoglobulin in the body that must be present to protect the body against the pathogen
Booster shot: given when antibody titre reveals low levels

Side Effects Range from mild and transient to
very serious or life threatening Minor effects
Fever, minor rash, soreness at injection site, itching
Severe effects Fever >38° C, encephalitis, convulsions,
anaphylactic reaction, dyspnea, others

Immunization schedule

Side Effects (cont’d) Minor reactions
Treated with acetaminophen and rest Serious or unusual reactions
Serum sickness Report serious or unusual reactions to
the Canadian Adverse Events Following Immunization Surveillance System

Nursing Implications Assess client’s health history,
medication history, allergies, pregnancy status
Assess previous reactions and responses to immunizations
Assess for contraindications, including immunosuppression

Nursing Implications (cont’d) Before giving any agent, recheck
the specific protocols for administration and schedules for administration
Follow manufacturer’s guidelines for drug storage, administration, routes, and site of administration

Nursing Implications (cont’d) If discomfort occurs at the injection
site, apply warm compresses and give acetaminophen
Do not give acetylsalicylate acid to children
Monitor for therapeutic responses and adverse reactions

Cancer Cellular transformation Uncontrolled and rapid cellular
growth Invasion into surrounding tissue Metastasis to other tissues or
organs

Cancer (cont’d) Cancerous cells do not have:
Growth control mechanisms Positive physiological function
Cancer cells either: Grow and invade adjacent tissues Break away from original tumour
mass and travel by means of blood or lymphatic system to distant sites

Cancer (cont’d) Metastasis
Uncontrolled cell growth Neoplasm
Mass of new cells; tumour Tumour
Benign Malignant (cancer)

Table 46-2 Tumour classification based on specific tissue of origin

Etiology of Cancer Age- and sex-related differences Genetic factors Ethnic factors Oncogenic factors (viruses) Occupational and environmental
carcinogens Radiation Immunological factors

Chemotherapy Pharmacological treatment of
cancer Antineoplastic agents Divided into two groups based on
where in the cellular life cycle they work Cell cycle nonspecific (CCNS) Cell cycle specific (CCS)

Chemotherapy (cont’d) Drugs have a narrow therapeutic
index Combination of agents is usually
more effective than single-agent therapy
Nearly all agents cause side effects and adverse effects
Dose-limiting side effects

Chemotherapy (cont’d) Harmful to all rapidly growing cells
Harmful cancer cells Healthy, normal human cells
Hair follicles GI cells Bone marrow cells

Chemotherapy:Contraindications
Few given the fatal outcome of
cancer
Low wbc
Infectious process

Extravasation Leaking of an antineoplastic drug into
surrounding tissues during IV administration
Can result in permanent damage to nerves, tendons, muscles, loss of limbs
Skin grafting or amputations may be necessary
Prevention is essential, Continuous monitoring of the IV site is essential

Extravasation (cont’d) If suspected, stop the IV infusion
immediately but do not remove the IV tube If possible, aspirate remaining drug or blood
from the tube Follow instructions for giving the
appropriate antidote (if one exists) through the existing IV tube, then remove the catheter
Some antidotes are not given through the IV catheter

Extravasation (cont’d) Cover area with sterile, occlusive
dressing Apply warm or cold compresses,
depending on the extravasated agent
Elevate the limb

Nursing Implications Assess baseline blood counts before
giving any antineoplastic agents Follow specific administration guidelines
for each antineoplastic agent Remember that all rapidly dividing cells
(both normal and cancer cells) are affected Mucous membranes Hair follicles Bone marrow component

Nursing Implications (cont’d) Monitor for complications
GI mucous membranes: stomatitis, altered bowel function with high risk for poor appetite, nausea, vomiting, diarrhea, and inflammation and possible ulcerations of GI mucosa

Nursing Implications (cont’d) Monitor for complications
Hair follicles: loss of hair (alopecia)
Bone marrow components:
dangerously low (life-threatening)
blood cell counts

Nursing Implications (cont’d) Implement measures to monitor
for and prevent infection in clients with neutropenia
Implement measures to monitor for and prevent bleeding in clients with thrombocytopenia and anemia
Keep in mind that anemia may result in severe fatigue

Nursing Implications (cont’d) Monitor for stomatitis (oral inflammation
and ulcerations) and implement measures to reduce the effects if it occurs
Anticipate nausea and vomiting and implement measures to reduce these effects
Women of childbearing age will need to use a nondrug form of contraception during therapy

Nursing Implications (cont’d) In addition to physical measures,
keep in mind the need for emotional support during this time for both the client and family
Monitor for therapeutic responses to antineoplastic therapies and the many possible side/adverse effects