Antidiuretic Hormone ADH ADH Hypertonic Interstitial Fluid Collecting Duct H2OH2O Urine.
34
Antidiuretic Hormone ADH ADH Hypertonic Interstitial Fluid Collecti ng Duct H 2 O Urine
-
Upload
meghan-gilmore -
Category
Documents
-
view
237 -
download
0
Transcript of Antidiuretic Hormone ADH ADH Hypertonic Interstitial Fluid Collecting Duct H2OH2O Urine.
Antidiuretic HormoneADH
ADH
Hypertonic Interstitial Fluid
Collecting Duct
H2O
Urine
Calcitonin
Calcium
Estrogen
Calcium

Parathormone
Calcium

Blood pH = 7.4(7.35-7.45)
Blood pH regulated by1. Kidneys2. Lungs
3. Buffers in blood
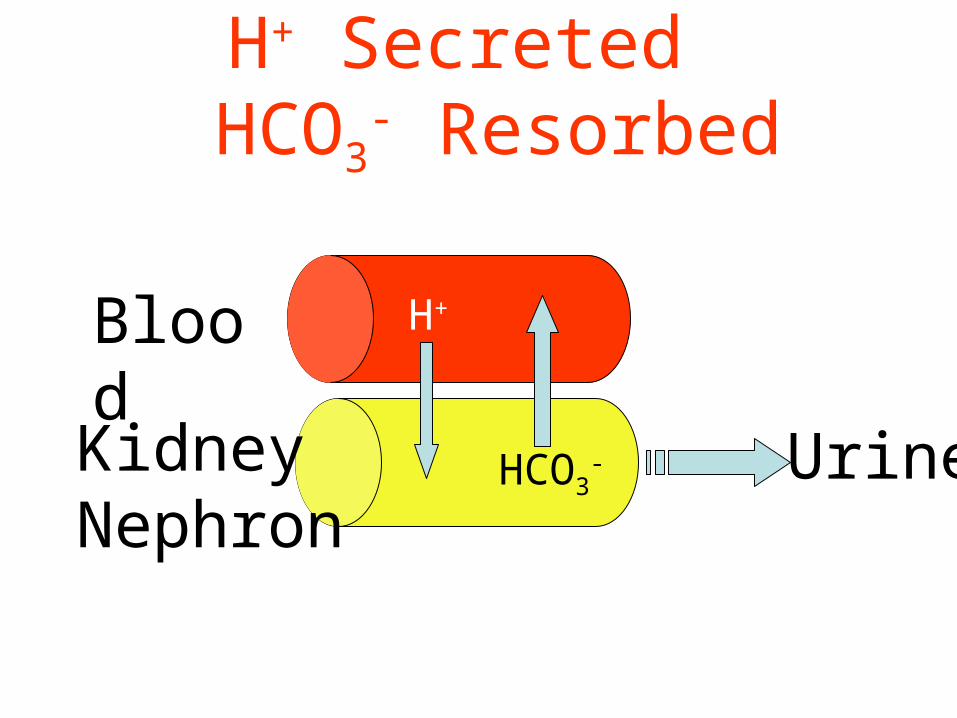
H+ Secreted HCO3
- Resorbed
Blood
Kidney Nephron
HCO3-
H+
Urine
Kidneys Regulate pH
• Excreting excess hydrogen ions, retain bicarbonate– if pH is too low
• Retaining hydrogen ions, excrete bicarbonate– if pH is too high
Lungs Regulate pH
• Breathe faster to get rid of excess carbon dioxide if pH is too low– Carbon dioxide forms carbonic acid in the
blood
• Breathe slower to retain carbon dioxide if pH is too high
Carbon Dioxide and Acid
CO2 + H2O H2CO3 H+ + HCO3-
Carbonic Acid
More Carbon Dioxide = More Acid = Lower pH
• Breathing slower will retain CO2 , pH will– decrease (more acid)
• Breathing faster will eliminate more CO2 pH will– increase (less acid)
Blood pH Drops to 7.3How does the body compensate?
• Breathe faster to get rid of carbon dioxide– eliminates acid
Blood pH Increases to 7.45How does the body compensate?
• Breathe slower to retain more carbon dioxide– retains more acid

The role of ADH:
• ADH = urinary concentration• ADH = secreted in response to ⇑
osmolality;
= secreted in response to ⇓ vol;• ADH acts on DCT / CD to reabsorb water• Acts via V2 receptors & aquaporin 2• Acts only on WATER
PG

Calculation of osmolality
• Difficult: measure & add all active osmoles
• Easy = [ sodium x 2 ] + urea + glucose
• Normal = 280 - 290 mosm / kg
PG
Fluid shifts in disease
• Fluid loss:– GI: diarrhoea, vomiting, etc.– Renal: diuresis– Vascular: haemorrhage– Skin: burns,sweat
• Fluid gain:– Iatrogenic:– Heart / liver / kidney failure:
PG

Prescribing fluids:
• Crystalloids:– 0.9% saline - not “normal” !– 5% dextrose– 0.18% saline + 0.45% dextrose– Others
• Colloids:– Blood– Plasma / albumin– Synthetics eg gelofusion
PG
The rules of fluid replacement:
• Replace blood with blood• Replace plasma with colloid• Resuscitate with crystalloid or colloid• Replace ECF depletion with saline• Rehydrate with dextrose
PG

How much fluid to give ?
• What is your starting point ?– Euvolaemia ? ( normal )– Hypovolaemia ? ( dry )– Hypervolaemia ? ( wet )
• What are the expected losses ?• What are the expected gains ?
PG
Signs of hypo / hypervolaemia:
Signs of …Volume depletion Volume overloadPostural hypotension Hypertension
Tachycardia Tachycardia
Absence of JVP @ 45o Raised JVP / gallop rhythm
Decreased skin turgor Oedema
Dry mucosae Pleural effusions
Supine hypotension Pulmonary oedema
Oliguria Ascites
Organ failure Organ failure
PG
What are the expected losses ?
• Measurable:– urine ( measure hourly if necessary )– GI ( stool, stoma, drains, tubes )
• Insensible:– sweat– exhaled
PG
• Electrolyte (Na+, K+, Ca++) Steady State• Amount Ingested = Amount Excreted.• Normal entry: Mainly ingestion in food. • Clinical entry: Can include parenteral
administration.

Case 1:
• A 62 year old man is 2 days post-colectomy. He is euvolaemic, and is allowed to drink 500ml. His urine output is 63 ml/hour:
1. How much IV fluid does he need today ?
2. What type of IV fluid does he need ?
PG

Case 2:
• 3 days after her admission, a 43 year old woman with diabetic ketoacidosis has a blood pressure of 88/46 mmHg & pulse of 110 bpm. Her charts show that her urine output over the last 3 days was 26.5 litres, whilst her total intake was 18 litres:
1. How much fluid does she need to regain a normal BP ?
2. What fluids would you use ?
PG
Case 3:
• An 85 year old man receives IV fluids for 3 days following a stroke; he is not allowed to eat. He has ankle oedema and a JVP of +5 cms; his charts reveal a total input of 9 l and a urine output of 6 litres over these 3 days.
1. How much excess fluid does he carry ?
2. What would you do with his IV fluids ?
PG
Case 4:
• 5 days after a liver transplant, a 48 year old man has a pyrexia of 40.8oC. His charts for the last 24 hours reveal:
• urine output: 2.7 litres• drain output: 525 ml• nasogastric output: 1.475 litres• blood transfusion: 2 units (350 ml
each)• IV crystalloid: 2.5 litres• oral fluids: 500 ml
PG
Case 4 cont:
• On examination he is tachycardic; his supine BP is OK, but you can’t sit him up to check his erect BP. His serum [ Na+ ] is 140 mmol/l.
• How much IV fluid does he need ?• What fluid would you use ?
PG

Case 5
• 30yo girl• SOB, moist cough, chest pain• ESKD• Very little urine output• Has missed dialysis last 3 sessions
Case 5
• What next?
– Current weight 78kg– IBW 68kg– JVP twitching her ear– No peripheral oedema– Coarse crackles to mid zones– BP 240/110– P 100– Gallop rhythm– 4cm of liver in RUQ

Case 5
• Assessment– Acute significant overload– Probably about 10kg
Case 6
• 55yo lady• Presents to dialysis for her routine session• BP 78/30
• History of dizziness for the last 6 hours• Current weight 58kg• IBW 59kg

Case 6
• P 120• Chest clear• HS dual• No oedema• Admits to 24hours of diarrhoea• Thirsty• No JVP visible
Case 6
• Dehydrated• Volume constricted• Hypotensive due to decreased circulating
fluid volume• Resuscitation?

The EndThe End
Acknowledgements
• Paddy Gibson – 4th year teaching ppt 2009
• Robert Harris – Fluid Balance ppt 2009• Heather Laird-Fick – Fluid and electrolyte
disorders ppt 2009• JXZhang Lecture 14 – ppt 2009• Dennis Wormington – fundamentals of
fluid assessment ppt 2009
![7.6: Water Balance Antidiuretic hormone (ADH): causes the kidneys to increase water reabsorption Regulating ADH: 1.water intake 2.[blood solute] 3.blood.](https://static.fdocuments.us/doc/165x107/56649d205503460f949f504f/76-water-balance-antidiuretic-hormone-adh-causes-the-kidneys-to-increase.jpg)